Upload
others
View
0
Download
0
Embed Size (px)
Citation preview
Review Article
Indoor aerosols: from personal exposure to risk assessment
Abstract Motivated by growing considerations of the scale, severity, and risksassociated with human exposure to indoor particulate matter, this workreviewed existing literature to: (i) identify state-of-the-art experimentaltechniques used for personal exposure assessment; (ii) compare exposurelevels reported for domestic/school settings in different countries (excludingexposure to environmental tobacco smoke and particulate matter from biomasscooking in developing countries); (iii) assess the contribution of outdoorbackground vs indoor sources to personal exposure; and (iv) examine scientificunderstanding of the risks posed by personal exposure to indoor aerosols.Limited studies assessing integrated daily residential exposure to just oneparticle size fraction, ultrafine particles, show that the contribution of indoorsources ranged from 19% to 76%. This indicates a strong dependence onresident activities, source events and site specificity, and highlights theimportance of indoor sources for total personal exposure. Further, it wasassessed that 10–30% of the total burden of disease from particulate matterexposure was due to indoor-generated particles, signifying that indoorenvironments are likely to be a dominant environmental factor affecting humanhealth. However, due to challenges associated with conducting epidemiologicalassessments, the role of indoor-generated particles has not been fullyacknowledged, and improved exposure/risk assessment methods are stillneeded, together with a serious focus on exposure control.
L. Morawska1,2, A. Afshari3,G. N. Bae4, G. Buonanno1,5,C. Y. H. Chao6, O. H€anninen7,W. Hofmann8, C. Isaxon9,E. R. Jayaratne1,2, P. Pasanen10,T. Salthammer1,11, M. Waring12,A. Wierzbicka9
1International Laboratory for Air Quality and Health,Queensland University of Technology, Brisbane, Qld,Australia, 2Institute of Health and BiomedicalInnovation, Queensland University of Technology,Brisbane, Qld, Australia, 3Department of Energy andEnvironment, Danish Building Research Institute/AalborgUniversity, Dr. Neergaards Vej, Denmark, 4Center forEnvironment, Health and Welfare Research, KoreaInstitute of Science and Technology, Seoul, Korea,5Department of Civil and Mechanical Engineering,University of Cassino and Southern Lazio, Cassino, FR,Italy, 6Department of Mechanical Engineering, HongKong University of Science and Technology, Kowloon,Hong Kong, 7Department of Environmental Health,National Institute for Health and Welfare, Kuopio,Finland, 8Department of Materials Research and Physics,University of Salzburg, Salzburg, Austria, 9Division ofErgonomics and Aerosol Technology, Lund University,Lund, Sweden, 10Department of Environmental Science,University of Eastern Finland, Kuopio, Finland,11Department of Material Analysis and IndoorChemistry, Fraunhofer WKI, Braunschweig, Germany,12Department of Civil, Architectural and EnvironmentalEngineering, Drexel University, Philadelphia, PA, USA
Key words: Indoor particulate matter; Personal exposure;Domestic indoor particulate matter; School indoorparticulate matter; Burden of disease from particulatematter exposure; Methods for personal exposureassessment.
L. MorawskaInternational Laboratory for Air Quality and HealthQueensland University of Technology2 George St, Brisbane, 4001 QldAustraliaTel.: +61-7-3138-2616Fax: +61-3138-9079e-mail: [email protected]
Received for review 13 December 2012. Accepted forpublication 26 March 2013.
462
Indoor Air 2013; 23: 462–487 © 2013 John Wiley & Sons A/S. Published by John Wiley & Sons Ltdwileyonlinelibrary.com/journal/inaPrinted in Singapore. All rights reserved INDOOR AIR
doi:10.1111/ina.12044
Practical ImplicationsThe indoor source contribution can be the dominant fraction of the integrated daily residential exposure to particles(especially UFP and PM2.5), strongly depending on resident activities, source events, and site specificity. Up to 30%of the burden of disease from particulate matter, exposure can be attributed to indoor-generated particles, which arethus one of the dominant environmental factors affecting human health globally. Improved exposure and risk assess-ment methods are needed, together with a serious focus on exposure control, to reduce the severity and risks associ-ated with human exposure to indoor particulate matter.
Introduction
Throughout their entire lives, each and every person isexposed to the aerosols omnipresent in indoor air.Given that most people spend the majority of theirlives indoors, the consequences of this exposure rangefrom insignificant to fatal and depend on the type ofaerosols present, type of indoor environment, durationof time spent, age, gender, susceptibility, and manyother factors (Adgate et al., 2003; Brasche and Bischof,2005; Lai et al., 2004; Leech et al., 2002). With theincreasing contemporary focus on indoor exposure, itis worth noting that it has been known for centuriesthat exposure to certain types of aerosols constitute atleast some level of risk and should be controlled(Miller, 1998).
Considering the scale of the problem and the poten-tial severity of the associated risks, the need for goodcharacterization and quantification of exposure toindoor aerosols appears obvious. Yet, while the pastdecade has seen an increase in the body of literaturepublished on this topic, there are still major challengesto be addressed, to fully understand and quantify themagnitude of both individual and population exposureto air pollution in different types of indoor microenvi-ronments. There are several reasons for this. Firstly,exposure is often confused with concentration, and it ispollutant concentration, not human exposure that isusually characterized or quantified. It does not helpthat the term ‘exposure’ belongs equally in the domainof everyday language and in the scientific vocabulary,and in the former it does not have a precise meaning. Itis this vague understanding of exposure that is oftenadopted in indoor sciences. Secondly, ambient particu-late matter (PM) presents a special challenge, and ithas not even been established conclusively which of itscharacteristics are the most significant in relation tohealth. Thirdly, apportioning indoor exposure tothe two components essential for exposure control,including: (i) PM of outdoor origin (which haspenetrated indoors) and (ii) PM generated by indoorsources, is a complexity with which many studies havestruggled. These three aspects are discussed in moredetail below.
Exposure is a vital element of risk assessment, a pro-cess which is initiated upon identification of a hazard,
and evidence that exposure constitutes risk to humanhealth. While a detailed discussion of this process isoutside the scope of this review, and more informationon the Predictive Risk Equation can be found inUSEPA (1991) or Naugle and Pierson (1991), it is veryimportant to understand the terms used and the indi-vidual elements of this process. In particular, pollutantconcentration is the numerical value of the amount ofan individual pollutant per unit volume of air at a par-ticular point in time or averaged over a period of time.Exposure is a product of the pollutant concentrationand the time over which a person is in contact with thatpollutant. When concentration varies with time, thetime-averaged concentration is used for exposure cal-culation. Two types of exposures are of special impor-tance in health risk assessments: (i) lifetime exposure,which is the sum of exposures which occurred in differ-ent environments – this is particularly important forcarcinogenic pollutants; and (ii) short-term exposure toelevated concentrations. Dose is a product of exposureand dosimetry factors (such as inhalation rate, regionalsurface area of the lung or breathing pattern), andquantifies the amount of substance available for inter-ference with metabolic processes or biologically signifi-cant receptors. Dose-response is the magnitude of theresponse of an individual to a given dose of a pollu-tant. Lifetime individual risk (which applies specificallyto carcinogenic pollutants) is a product of lifetime aver-age daily dose and dose-response. Risk to exposed popu-lation is a quantitative assessment which takes intoaccount lifetime individual risk of the populationgroups affected and specific exposure scenarios of thepopulation. The main objective of health risk assess-ment is to link the hazard with the risk to the exposedpopulation in a quantitative way, and thus provide thebasis for risk management.
In the context of this discussion, exposure assess-ment includes: (i) identification of sources of indoorpollution and specifically PM; (ii) characterization(through measurements, surveys, questionnaires, etc)of indoor air pollutants and contributing factors suchas concentration, duration, frequency, distributionroute, time frame, and geography; and (iii) modelingexposure for different occupancy and lifestyle scenar-ios. To quantify personal exposure to PM, three meth-ods are frequently used: (i) direct personal exposure
463
Indoor aerosols
measurements, which are the best and most accuratemeasure of exposure (Jantunen et al., 2002); (ii) mea-suring microenvironmental concentrations and thetime spent in these microenvironments; and (iii) per-sonal activity information (Meng et al., 2005). The lat-ter involves gathering personal activity informationfrom questionnaires and has been used in both regres-sion and analysis of variance models to describesources and activities impacting exposure and indoorair quality (Baxter et al., 2007; Koistinen et al., 2001).
Regarding the second of the above listed methods,the existing exposure models adopt one of two generalapproaches: (i) a time series approach that estimatesthe microenvironmental exposure of individuals basedon the instantaneous concentration at any moment; or(ii) a time-averaged approach that estimates the micro-environmental exposure using average pollutant con-centrations and the total time spent in eachmicroenvironment (USEPA, 2004). Expressions for thetwo exposure evaluation methods are described inEquations (1) and (2), respectively:
Eðt1; t2Þ ¼Zt¼t2
t¼t1
CsðtÞdt ð1Þ
Eðt1; t2Þ ¼ �Csðt2 � t1Þ ð2Þ
where t1 and t2 denote the start and stop times of theinvestigated time interval; E(t1, t2) is the exposure dur-ing this period; Cs(t) is the instantaneous microenvi-ronmental concentration at any moment between t1and t2; and �Cs is the average pollutant concentrationduring the time period t2–t1. The units of both equa-tions are [pollutant concentration 9 time].
It is noteworthy that different definitions have beenused for exposure, and for example, Zartarian et al.(1997) defined exposure as the contact between anagent and a target that takes place at a contact bound-ary over an exposure period. According to their defini-tion, time-averaged inhalation exposure is in units ofconcentration (at the breathing zone boundary), whileintegrated exposure is in units of concentration 9 time.To avoid confusion, if there is only concentration dataavailable, we propose that one should refer to the con-centration to which a person is/would be exposed. How-ever, in the case of actual exposure data, which alwayshas a duration (with the minimum duration being onesingle breath), then the units should be: [pollutant con-centration 9 duration of exposure]. Otherwise, it wouldbe difficult to avoid confusion between ‘time-averagedinhalation exposure’ and ‘integrated exposure’ (overtime), with each having different units.
Exposure to particles is a special challenge, due totheir multifactorial nature and their highly variablesize. Airborne particles range in size over five orders of
magnitude, from molecular dimensions to the sizes thatare distinguishable with the naked eye (from about0.001 lm to about 100 lm; Baron and Willeke, 2001),which constitutes a big challenge in the choice andavailability of instrumental techniques, particularly forpersonal exposure monitoring. Other characteristicsinclude: number concentration, number size distribu-tion, mass concentration mass size distribution, surfacearea, shape, chemical composition, electrical charge, orlight-scattering properties. Usually, only some of theseproperties are measured, and almost never all of them,simultaneously.
In relation to some of these metrics, in particularnumber concentration of ultrafine particles(UFP < 0.1 lm) or their surface area, while there isample evidence of the hazardous nature of these parti-cles provided by toxicological studies, epidemiologicstudies have not yet established an exposure–responserelationship (Fissan et al., 2007; Shin et al., 2007;WHO, 2005). In contrast, for PM2.5 and PM10 (massconcentration of particles with aerodynamic diameterssmaller than 2.5 and 10 lm, respectively), and totalsuspended particulate matter (TSP), not only has theirhazardous nature been established, but epidemiologicstudies have quantified exposure–response relation-ships (WHO, 2005). However, whether the effects areindependent or dependent and therefore only some ofthem need to be measured (and regulated) are openquestions at present. Thus, in the absence of a well-established exposure–response relationship, the selec-tion of parameters for investigation is not a trivialaspect.
Indoor and outdoor source contribution to indoor exposure to aerosols
Indoor particles are a mix of ambient particles thathave infiltrated indoors, particles emitted indoors andparticles formed indoors through reactions of gas-phase precursors emitted both indoors and outdoors(Meng et al., 2005; Morawska and Salthammer, 2003;Uhde and Salthammer, 2007). Therefore, the composi-tion and toxicity of indoor particles is very complex,with similarities but also differences to outdoor aero-sols. These differences reflect particle origin, as well aspostformation physicochemical processes, in bothindoor and outdoor environments. Epidemiologicalassociations between PM and various health outcomesare based predominantly on ambient air measurements(WHO, 2005); however, poor correlations have beenfound between ambient PM concentrations and per-sonal exposure to PM. This is due to the contributionof many other pollution sources to personal exposure,including work related, in-vehicle and/or leisure activi-ties (Meng et al., 2005). This initiated a debate as towhether ambient PM is a good surrogate for exposureto PM and in some recent work assessing personalexposure to PM, a division of personal exposure into
464
Morawska et al.
ambient and nonambient sources has been considered(Wilson and Brauer, 2006; Wallace and Williams,2005).
Infiltration of outdoor particles is significantly modi-fied by particle size-specific differences in the penetra-tion efficiency and indoor deposition rate. The latteralso directly affects the concentrations generated byindoor sources. Both coarse and ultrafine particles arerapidly removed from the air, but by different mecha-nisms: coarse particles by gravimetric settling, andultrafine (e.g., those generated by gas cooking or can-dles) by thermokinetic deposition. Accumulation modeparticles, which dominate outdoor background con-centrations, have the highest penetration and infiltra-tion rates (Long et al., 2000). To account for particleswhich infiltrated from outside, indoor to outdoorratios for particle concentration are often calculated(I/O). Many studies have reported I/O ratios both withand without operating indoor sources, and on the basisof comparisons between several published articles,Morawska and Salthammer (2003) concluded that, fornaturally ventilated buildings in the absence of indoorsources, I/O ratios for PM10 and PM2.5 ranged from0.5 to 0.98 (with a median value of 0.7) and 0.54 to1.08 (median, 0.91), respectively. This highlights theimportance of the contribution of outdoor air as asource of particles encountered in indoor environ-ments. However, when indoor sources are present, I/Oratios for PM10 and PM2.5 range from 1.14 to 3.91(median, 1.47), and 1 to 2.4 (median, 1.21), respec-tively, demonstrating the significance of indoor sourcecontributions.
Indoor sources of ultrafine particles [contributing toparticle number (PN), rather than mass concentration]have been identified as tobacco smoking, cooking (fry-ing, grilling, baking, barbequing, boiling water, toast-ing, cooking soup, etc), the use of gas and electricstoves, electric toasters, gas-powered clothes dryers,candle and incense burning, photocopiers, laser print-ers, hair spray, cleaning products, and furniture polishcontaining terpenes (which form secondary aerosolswhen in the presence of ozone) (Abt et al., 2000;Dennekamp et al., 2001; He et al., 2004; Husseinet al., 2006; Lee and Hsu, 2007; Li et al., 1993; Longet al., 2000; Ogulei et al., 2006; Wallace, 2005, 2006;Weschler, 2003; Wainman et al., 2000). Largerindoor particles (contributing to particle mass con-centration, PM2.5 and/or PM10) have been identifiedas coming from sweeping, hovering, dusting, humanmovement (walking, dancing, children playing), sit-ting on upholstered furniture, resuspension fromclothes (folding clothes, blankets, making a bed),washing powder residues (zeolite), resuspension fromcarpets and the pouring of kitty litter (Abt et al.,2000; Ferro et al., 2004; Gudmundsson et al., 2007;Koistinen et al., 2004; Long et al., 2000; Oguleiet al., 2006).
Some of these sources, such as frying (Abt et al.,2000;) or physically stirring foods that are saut�eing infats and liquids (Long et al., 2000), can contribute toboth the smaller and larger particle concentrations. Ithas been reported that indoor sources can periodicallygenerate particles that, in terms of number and massconcentrations, significantly exceed background levels(Abt et al., 2000; He et al., 2004; Long et al., 2000)and that indoor particle events are site and time spe-cific, and can also be brief, intermittent and highly var-iable (Hussein et al., 2005; Long et al., 2000; Nazaroff,2004). A phenomenon which also needs to be men-tioned in relation to human exposure is the ‘personalcloud’. As discussed by Wallace (1996), the personalcloud effect is an observed elevation in personal expo-sure when measured by a personal monitor relative toindoor concentration measured by a fixed room moni-tor. While the exact nature of this phenomenon hasnot been explained, a review by Wallace (1996) hasrevealed that it can elevate personal exposure by up to50%.
Aim and scope of this work
The aim of this study was to review the existing litera-ture on personal exposure to indoor aerosols and therisk it poses to the following: (i) identify the state ofthe art in experimental techniques used for personalexposure assessment; (ii) compare the exposure levelsreported by studies conducted in different settings andin different countries; (iii) assess the overall role of out-door background versus indoor sources in contributingto personal exposure; and (iv) examine scientific under-standing of risk due to personal exposure to indooraerosols. The special focus of the review was on expo-sure in domestic and school environments due to theirimportance to overall human exposure. Exposure inother important microenvironments, such as in-transit,has already attracted separate reviews (Knibbs et al.,2011), or are sufficiently complex and diverse to war-rant separate reviews (in particular industrial and non-industrial workplace, healthcare facilities, or facilitiesmanufacturing or handling engineered particles). Inaddition, not included in this review were studiesreporting indoor concentrations or exposures in devel-oping countries, where wood, coal, agricultural resi-dues, dung, and biogas are used as fuels, becausedifferences in household characteristics, type of fuel,cooking appliances and ventilation conditions makecomparisons difficult. Another exclusion were environ-ments affected by environment tobacco smoke. Indeveloping countries, indoor exposure to particles fromburning biomass fuels is a major health concern, andthe reported concentrations are substantially higherin comparison with those reported in developedcountries, with indoor PM10 shown to range from 104to 2500 lg/m3 and PM2.5 201–304 lg/m
3 in developing
465
Indoor aerosols
countries (Begum et al., 2009; Morawska et al., 2011a;Wang et al., 2010). Again, this is a topic for a separatereview.
The authors of this review identified studies pub-lished in English, between January 1989 and October2012, using ScienceDirect, EBSCOhost, Web ofScience and Wiley Interscience search engines. The fol-lowing key words were used: personal exposure, indoorenvironments, PM10, PM2.5, PM1, and UFP. Addi-tional studies were identified from the references ofthese publications, and on the basis of personal knowl-edge of the authors of this review.
Methods for monitoring personal exposure to indoor particulatematter
General approaches to PM monitoring for the purposeof personal exposure assessment include the following:(a) measurements carried out in outdoor microenviron-ments, usually at fixed outdoor stations, to assess com-pliance with national ambient air quality standards. Asdiscussed above, this approach fails to account for allcomponents of exposure and is also a poor predictor ofpersonal exposure to outdoor PM, due to its large spa-tial and temporal variations, especially in urban envi-ronments (e.g., Kousa et al., 2002); (b) monitoringcarried out simultaneously at indoor and outdoor sites(Williams et al., 2003), including single or multipleindoor microenvironments (Rodes, 2011). In suchstudies, the sampler inlet is usually placed 1.0–1.5 mabove the floor to simulate a seated breathing height,and in a location not unduly influenced by potentialnearby aerosol sources (Adgate et al., 2002); and (c)direct personal exposure monitoring.
Table S1 summarizes the existing methods that havebeen used for PM characterization for approaches (a)and (b), as discussed above, including particle mass(Almeida et al., 2011; Andresen et al., 2005; Brani�set al., 2005; Crist et al., 2008; Ekmekcioglu and Ke-skin, 2007; Jo and Lee, 2006; Landis et al., 2001; Leeet al., 2002; Monn et al., 1997; Morawska et al., 2001,2003; Reff et al., 2007; Williams et al., 2000), PN(Bhangar et al., 2011; Diapouli et al., 2007; He et al.,2007; and Hoek et al., 2008; Marra et al., 2010; Mat-son, 2004; Morawska et al., 2001, 2003; Mullen et al.,2011a; Wallace and Ott, 2011), surface area (Buonannoet al., 2010) and size distribution measurements(Almeida et al., 2011; Buonanno et al., 2010; Liaoet al., 2006; Marple, 2004; Massey et al., 2012; Mora-wska et al., 2001; Saraga et al., 2011; Wan et al., 2011;Williams et al., 2003), as well as that of particle com-position (Chao and Wong, 2002; Hoek et al., 2008;Janssen et al., 2001, 2003; John et al., 2007; Lai et al.,2004; Landis et al., 2001; Moln�ar et al., 2007a,b;Reff et al., 2007; Roorda-Knape et al., 1998; Strangeret al., 2008; Titcombe and Simcik, 2011; Williamset al., 2003; Wilson et al., 1995). It should be noted
that this is not an exhaustive review of all availablemethods – for a comprehensive review of particle mon-itoring methods the reader is directed to Morawskaet al. (2008). In general terms, the methods can bedivided into online and off-line techniques. Some ofthese methods are suitable for both indoor and out-door application, while others are more appropriatefor outdoor environments (due to high flow rates orthe excessive noise they generate). It can be seen fromTable S1 that there is a large range of instrumentationavailable for particle mass concentration measure-ments, which is not surprising because many types ofinstruments are necessary for standard compliancemonitoring. Inertial impactors have been used since1860 to collect particle samples for chemical and gravi-metric analysis (Marple, 2004). The cascade impactorwas developed in the 1940s, and today, there are preci-sion cascade impactors for high accuracy aerosol sam-pling to collect size-fractionated airborne particlesamples. For example, the 125B Rotating Micro-Ori-fice Uniform Deposit Impactor (MOUDI) from MSPCorp is designed for high concentration aerosol sam-pling in 13 stages, from 10 nm to 18 um (MSP Corp,2011). Once collected on an impactor or filter, the par-ticulate mass is determined by thermally equilibratingand weighing the sample. Subsequently, chemical anal-ysis may be carried out by several techniques such asatomic absorption spectrometry, atomic fluorescencespectrometry, inductively couple plasma spectroscopy,and X-ray fluorescence spectroscopy (XRFS). Particlemass concentration is not only monitored by the classicmethod of collecting particles on filters, but it isincreasingly monitored using online methods, in partic-ular photometers, which calibrate aerosol light-scatter-ing responses for a specific challenge aerosol to providereal-time mass concentration readings (Rodes, 2011).Light-scattering techniques have been applied to moni-tor size-fractionated mass concentrations such asPM10, PM5, PM2.5, and PM1 (Massey et al., 2012). Itcan be further concluded from Table S1 that in addi-tion to several instruments available for PN concentra-tion and size distribution monitoring, there are two PNpersonal monitors and only one instrument for surfacearea monitoring. In consequence, there is very littleinformation available to assess personal exposure tosurface area, with only a handful of investigations con-ducted in occupational settings (Wang et al., 2010),including one in a pizzeria (Buonanno et al., 2010).Today, there are a number of techniques available forcollecting samples for elemental and carbon analysis[organic carbon (OC) and elemental carbon (EC)] anda selection of these are listed in Table S1.
While microenvironment monitoring can provideestimates of personal exposure, accurate results requirethe use of monitoring devices that can be carried on orby the participants, for direct personal exposure moni-toring [point (c) above]. This is important to avoid mis-
466
Morawska et al.
classification, noncompliance, and to improve the fidel-ity of the data in general. The first large-scale probabil-ity-based study of personal exposure to particles wasconducted in 1990 by the Harvard University Schoolof Public Health (HSPH) who designed and con-structed a battery-operated personal monitor for bothPM10 and PM2.5 (Ozkaynak et al., 1996). The monitorwas worn over 24 h by 178 participants. The two majorindoor particle sources were found to be smoking andcooking. However, even in the presence of thesesources, the majority of indoor particles came fromoutdoors. Yet, indoor concentrations were only weaklycorrelated with outdoor concentrations, and the corre-lation between personal exposures outdoor concentra-tions was even weaker.
Hand-held ultrafine particle monitors are now com-mercially available, including the TSI 3007 Condensa-tion Particle Counter (CPC) (Wallace and Ott, 2011).Recent advances in the miniaturization of opticalbenches used for nephelometry have produced com-pact real-time aerosol sensors that can be worn or car-ried to characterize acute exposure levels (Rodes,2011). Two real-time PN and size monitoring devicesthat are being used at present are the Nanotracer Mon-itor from Philips (Marra et al., 2010) and the Mini Dif-fusion Size Classifier (DiSC) from the University ofApplied Sciences, Windisch, Switzerland (Fierz et al.,2007). In June 2012, Philips ceased production ofNanotracers, however, the DiSC is still commerciallyavailable. In addition, Naneos Particle Solutions, Swit-zerland, is presently introducing a pocket size/postcardsize particle detector, providing the lung-deposited sur-face area of aerosol particles with a time resolution of5 s (Naneos, 2012). These personal exposure monitorsare small, self-contained, battery-powered devices thatcan be carried by an individual to mimic the proximityof the breathing zone, defined as 30 cm in diameteraround the head, to local sources or spatial concentra-tion gradients (Jensen and O’Brien, 1993). Contempo-rary personal aerosol exposure monitoring may bedirect reading or time integrated sampling systems.They generally consist of two parts – (i) the aerosol siz-ing and collection unit, which includes the sample inlet,an impactor or a cyclone for aerodynamic sizing andthe filter cassette holder, if applicable, and (ii) the flowcontrol, electronics and sensors unit, which includes amini-pump and battery pack for the purpose of flowmanagement (power management, flow control, timingfunctions, and start/stop functions). Some devices maybe fitted with built-in supplementary features for com-pliance and activity level sensing, Global PositioningSystem sensing, QC data capture and sensors for tem-perature and humidity. Typically, participants carrythe personal samplers in small foam-insulated bagswith a shoulder strap that has the inlet mounted on thefront (Broich et al., 2011). During sampling sessions,participants are requested to wear or carry the expo-
sure monitors whenever possible and to place thembeside them while seated or sleeping (Adgate et al.,2002; Jayaratne et al., 2011). During sampling, partici-pants are also asked to fill out a time–activity diary,recording the time periods spent in primary microenvi-ronments such as at home, outside the home, insideother than home, outside other than home, and in-transit. They also record data on exposure to tobaccosmoke and other potential modifiers of exposure, suchas occupation, cooking, outdoor activities, and thenumber of hours that doors and windows were open ina residence (Mazaheri et al., 2012). There have beenmany investigations of personal exposure conductedwith portable devices and, in Table 1, we present sev-eral such examples.
Personal exposure levels
Residential environment
People in developed countries spend approximately65% of our time in our residences (Brasche and Bisc-hof, 2005; Leech et al., 2002). Studies that assess con-centrations measured in residences, outdoors,concentrations from personal monitoring and inte-grated daily residential exposure are given in Table S2.Residences with smoking have been excluded, astobacco smoking is a known source of fine particlesthat can dramatically influence indoor concentrations.For example, indoor PM2.5 mass concentration wasreported to increase by 58–130% due to smoking(Breysse et al., 2005; Stranger et al., 2007). Studiesassessing the particle concentration and emission fac-tors of a given indoor activity or cooking event havenot been included in this review. In the reviewed stud-ies (Table S2), simultaneous indoor and outdoor con-centration data are most commonly given. Fourteenstudies reported integrated mass concentration valuesfrom direct personal monitoring with varying averag-ing times (note that in the original articles these valuesare presented as ‘personal exposure concentrations’but given that exposure is a product of concentrationand exposure duration, and for consistency within thisreview, we will refer to them as ‘concentrations frompersonal monitoring’) for PM2.5 (Adgate et al., 2002;Johannesson et al., 2007; Koistinen et al., 2004; Laiet al., 2004; Landis et al., 2001; Meng et al., 2005;Moln�ar et al., 2005; Rodes et al., 2010; Turpin et al.,2007; Wallace et al., 2006), PM1.5 (Williams et al.,2000) and PM10 (Lioy et al., 1990; Monn et al., 1997).Only three studies give values for daily residentialexposure to UFP in units of number concentration perhour per day (Bhangar et al., 2011; Mullen et al.,2011b; Wallace and Ott, 2011). Average PM2.5 frompersonal monitoring in the listed studies rangesfrom 10.6 to 54 lg/m3, with average and medianvalues of 27.3 and 26.5 lg/m3, respectively. These
467
Indoor aerosols
concentrations are given for different averaging times,including 24 h, 48 h, or 7 days, incorporate time spentoutdoors, and comprise both adults and children.Bhangar et al. (2011), Mullen et al. (2011a,b), andWallace and Ott (2011) present an elegant way of cal-culating indoor residential (i.e., while occupants are athome) daily integrated exposure to UFP in units ofparticles per cm3�h/day. The daily integrated exposureis a normalized form of integrated exposure and mayserve as a useful single metric for comparative pur-poses. The average indoor residential daily integratedexposure per person reported in these three studies ran-ged from 11.5 9 104 to 29.6 9 104 particles/cm3�h/day. On the basis of values reported by Wallace andOtt (2011), the average integrated daily residentialexposure (cooking + indoor background due to infil-tration of particles from outdoors) constitutes 67% ofthe total daily integrated personal exposure. Addition-ally, in these three studies, each occupant’s daily inte-grated residential UFP exposure was apportioned intocontributions from outdoor, episodic and continuousindoor sources, on the basis of continuous indoor andoutdoor measurements, occupant activity logs andquestionnaires. The indoor source contribution to theaverage residential daily UFP exposure was 59%(ranging from 38% to 76% in seven residences) inBhangar et al. (2011) and 30.5% (ranging from 19% to42% in two residences) in Mullen et al. (2011a,b).Recalculating values given by Wallace and Ott (2011),cooking (dominant indoor source) contributed to 47%of residential exposure (one residence). Wallace (2006)attributed 55% of particles found indoors to indoor
sources. These studies point to a strong dependence onresident activities, source events and site specificity, butalso highlights the importance of indoor sources intotal personal exposure.
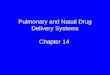
In Figure 1, the statistics (minimum values, 1st quar-tile, median, 3rd quartile, and maximum values)obtained from average values reported in the reviewedstudies are given for outdoor and indoor PM10 andPM2.5, and for PM2.5 from personal monitoring.The purpose of Figure 1 is to give an indication ofthe range of measured concentrations, given that theapplied averaging times varied to a great degree, as didthe measurement methods and instrumentation used.For example, the averaging times ranged from hours(8, 24, 48 h) to days, seasons and years, and someincluded nonoccupancy time. In terms of assessing per-sonal exposure to particles in residences, the most rele-vant average would be during the time the occupant ispresent in the residence (occupancy time). Inclusion ofnonoccupancy time (when no-one is present in theresidence) underestimates the concentration relevantfor personal exposure assessment. Median values ofreported indoor PM10 concentrations are slightlyhigher than outdoors (i.e., 34.7 and 30.2 lg/m3, respec-tively), while median indoor and outdoor values forPM2.5 are the same (17.6 lg/m
3), with higher varia-tions seen indoors. The median value of PM2.5 frompersonal monitoring accounts for 26.5 lg/m3 and ishigher than indoor and outdoor concentrations. Thiscan be explained by the fact that people spend time inother microenvironments where concentrations can behigher than at indoor and outdoor measurement sites
Table 1 Summary of personal exposure monitoring studies using portable devices
Metrics Size Instruments References
Particle mass PM10 Personal Environmental Monitor (SKC) Scapellato et al. (2009)Grimm Aerosol Spectrometer 1.109 Broich et al. (2011)Battery-operated personal monitor (Harvard School of Public Health) Ozkaynak et al., 1996;
PM2.5 Personal Environmental Monitor model 200 (MSP Corp) Andresen et al. (2005)Filter Sampler URG-2000-25F (URG) Crist et al. (2008)PM2.5 Personal sampler (BGI) Reff et al. (2007)Personal environmental monitoring sampler (PEMS) (Harvard School of Public Health) Jedrychowski et al. (2006)SidePak Portable nephelometer model AM510 (TSI) Borgini et al. (2011)Battery-operated personal monitor (Harvard School of Public Health) Ozkaynak et al., 1996;
PM1 Grimm Aerosol Spectrometer 1.109 Broich et al. (2011)Personal exposure monitor PMON (Model URG-2000-15, URG) Williams et al. (2000)
Particle number and average size Nanotracer Monitor (Philips) Jayaratne et al. (2011)Mazaheri et al. (2012)Buonanno et al. (2012a)
MiniDiSC (Windisch) Fierz et al. (2007)Particle surface area Nanoparticle Dosimeter (Naneos Particle Solutions) Naneos (2012)Particle size distribution Not availableElemental composition PM2.5 GK2.05 cyclone sampler (KTL, BGI) Lai et al. (2004)
Personal Environmental Monitor (PEM) (MSP) Landis et al. (2001)Black carbon PM2.5 Reflectometer EEL 43 Roosbroeck et al. (2007)Light scattering TSP Nephelometer MIE pDR Williams et al. (2003)
Portable nephelometer SidePak model AM510 (TSI) Borgini et al. (2011)Polycyclic Aromatic Hydrocarbons PM2.5 Personal microenvironment Aerosol Speciation Samplers PMASS model 240 (MSP Corp) Titcombe and Simcik (2011)
468
Morawska et al.
(e.g., smoky bar, restaurant, in-transit, woodworkingsite, etc) or they can be in closer proximity to indoorsources than the indoor monitor (Meng et al., 2005;Turpin et al., 2007).
Eight studies assessing indoor and outdoor PN con-centrations were found and have been included inTable S2. However, due to differences in minimummeasured size (between 6 and 15 nm) and the varietyof averaging times (based on the whole monitoring per-iod, occupancy, activity, and nonactivity periods), theirdirect comparison did not seem meaningful. Only twostudies (Bhangar et al., 2011; Mullen et al., 2011a,b)reported directly measured values for occupancy time(while awake and asleep) and used instruments withthe same lower size limit (6 nm). On the basis of thesetwo studies (seven single family houses and four apart-ments), the average concentration for occupancy timeindoors accounts for 16.1 9 103 (ranging from5.3 9 103 to 34.7 9 103) particles/cm3, while outdoorsaccounts for 19.0 9 103 (ranging from 8.9 9 103 to22.4 9 103) particles/cm3.
Similarity of the indoor to outdoor concentrations(in Figure 1 and the text above) may be misleadingand may suggest that there is not a pressing need tosupplement ambient air-based exposure proxies with amore detailed assessment of personal exposures. How-ever, when comparing indoor and outdoor concentra-tions, one has to bear in mind that: (a) the buildingsfilter a substantial fraction of outdoor particles (i.e.,infiltration of particles originating from outdoors issignificantly modified by particle size-specific differ-ences in the penetration efficiency and indoor deposi-tion rate), thus modifying exposure to ambientparticles; (b) in addition to particles of an ambient ori-gin, particles can also originate from indoor sources,and these may differ significantly from outdoor parti-cles in terms of both composition (as they have differ-ent sources) and temporal patterns; (c) personalexposure is further modified by both outdoor (e.g., in
traffic) and indoor (e.g., in kitchen) near-field activities,which may not be captured properly by stationarymicroenvironmental monitoring.
Some activities, including smoking, woodwork, andcooking, were reported to have a dramatic influence onfine indoor PN concentrations (Hussein et al., 2006;Wallace et al., 2006) and on personal PM2.5 exposure(Meng et al., 2005; Turpin et al., 2007; Wallace et al.,2006). Reported peak number concentrations due tocooking activities ranged from 1.6 9 104 to 6.3 9 105
particles/cm3 (He et al., 2004; Wan et al., 2011), andthese are much higher than reported outdoor maxi-mum concentrations. Sources of indoor-generated par-ticulate matter are not well characterized, withcontributions from a range of vastly different activities,including cooking, cleaning, combustion devices, can-dles, photochemistry, printers, and the use of variousconsumer products such as aerosols, detergents,sprays, etc.; however, their quantitative contributionshave not been determined on a population representa-tive basis.
In addition, the impact of particle size-dependentphysical processes has not been sufficiently investigated,in terms of their impact on PM exposure and uptake,particularly when particle composition is consideredin addition to physical characteristics. For example,particles of different chemical composition tend to havecharacteristic size distributions, and it is not knownwhether the differences observed in composition studies(e.g., Levy et al., 2012) are only partly or completelyattributable to the physical characteristics. To determinewhether the observed differences may also be attribut-able to composition or exposure, and whether dosedifferences are due to particle size distributions, requiresnew research applying innovative approaches to expo-sure and dose characterization, based on integratedmonitoring and modeling approaches. This is discussedfurther in section ‘Chemical’.
Epidemiological studies attempting to investigate thehealth effects of exposure to indoor-generated particlesare typically limited to small cohorts or very inaccuratequestionnaire-based exposure assessment. Europeandata on indoor concentrations of indoor- and outdoor-generated particles showed that while the outdoorcomponent ranged from 6 to 20 lg/m3, the contribu-tion of indoor sources in non-smoking homes was3–5 lg/m3, representing 20–30% of the total concen-trations (H€anninen et al., 2004).
Schools
The focus of this section is personal exposure assess-ment in relation to airborne particle concentrations inschools, in particular PM10, PM2.5, and UFP. Schoolsare complex indoor environments with very specificbuilding designs, ventilation conditions, indoor andoutdoor pollution sources, and types of activities
0
50
100
150
200
250
PM10outdoors
PM10indoors
PM2.5outdoors
PM2.5indoors
PM2.5personalmonitoring
Mas
s con
cent
ratio
n (μ
g/m
3 )
Fig. 1 Summary of particle mass (PM10 and PM2.5) obtainedfrom average values reported in the studies included in TableS2. Box plots denote minimum values, 1st quartile, median, 3rdquartile and maximum values
469
Indoor aerosols
conducted (Daisey et al., 2003; Lee and Chang, 2000).Therefore, the monitoring of school exposures is chal-lenging and can be conducted in many different ways,as reported by the recent reviews on this topic (Lin andPeng, 2010; Mej�ıa et al., 2011). On the other hand, thecharacterization of these microenvironments is consid-ered important to estimate the total exposure of chil-dren. Children are a population subgroup verysensitive to air pollution, because they receive a higherdose of airborne particles relative to lung size com-pared with adults (Farhat et al., 2005), and at the sametime, their physiological and immunological systemsare still in the process of developing.
Generally speaking, air quality in schools can bemeasured on three scales, depending on the spatial unitof analysis (Mej�ıa et al., 2011): (i) ‘city scale’, thebroadest and most common scale characterizes airquality across several city blocks using remote mea-surements; (ii) ‘school scale’, which characterizes airquality in schools from data collected by ground-levelmonitors or samplers installed in school buildings,school yards and/or around the perimeter of theschool; or (iii) ‘personal scale’, which measures airquality by attaching individual portable instruments tochildren, to assess their exposure.
Within this review, a literature search was conductedfor articles reporting data relevant for assessing the airquality in and around schools. The most important cri-terion for inclusion was that the collected air qualitydata were used for indicating or representing pollutantconcentrations in school environments. In the past dec-ade, there has been a large body of literature publishedon the concentration levels of airborne PM in schoolclassrooms, specifically PM10 and PM2.5. Dataextracted from about 40 original papers are summa-rized in Table S3.
A number of studies examining PM levels in class-rooms, mainly in Asia and Europe, reported high levelsof PM10 and PM2.5 (Almeida et al., 2011; Borginiet al., 2011; Diapouli et al., 2008; Ekmekcioglu andKeskin, 2007; Fromme et al., 2005, 2007; Goyal andKhare, 2009; Janssen et al., 1997; Lahrz et al., 2003;Lee and Chang, 2000; Liu et al., 2004; Roorda-Knapeet al., 1998; Stranger et al., 2007, 2008; Yang et al.,2009), ranging from 30 to 1181.1 lg/m3 and 13 to360 lg/m3, respectively. Other studies carried out inthe United States and Northern Europe (Brunekreefet al., 1997; Gauvin et al., 2002; Janssen et al., 2001,2003; John et al., 2007; Keeler et al., 2002; Link et al.,2004; Moln�ar et al., 2007a; Parker et al., 2008;Shaughnessy et al., 2002; Weichenthal et al., 2008)reported lower levels of PM10 (average value 23 lg/m
3)and PM2.5 (14 lg/m
3) than other published literature(Table S3). The wide range of PM10 and PM2.5 concen-trations indicate a great potential for their reduction,as well as a need for identifying the factors responsiblefor this variability.
On the other hand, there are only a few studiesreporting on indoor UFP concentrations in schoolclassrooms, and even less which investigated the corre-lation with outdoor traffic or indoor processes (Buon-anno et al., 2013; Diapouli et al., 2008; Guo et al.,2008; Morawska et al., 2009a; Mullen et al., 2011a,b;Weichenthal et al., 2008). Only one paper reported thedaily personal exposure of children and the contribu-tion of the school microenvironment to daily dose (Bu-onanno et al., 2012a). In general, classroom UFPconcentrations decreased with a reduced degree of traf-fic density and urbanization, indicating that, in theabsence of significant indoor sources, vehicular emis-sion greatly influenced the indoor UFP concentrationlevels.
It should be noted that articles included in thisreview varied in their design and approach, becausepersonal exposure assessment was not the main focusof all studies. The main differences can be summa-rized as follows: (i) the averaging time (school time,24 h, 3 weeks, etc); (ii) selection of schools (randomor based on defined conditions); (iii) the spatial unitof analysis (city, school or personal scale); (iv) iden-tification of the major sources of local air pollutionand the corresponding thermodynamic processes(some techniques include meteorological or localtraffic data); (v) statistics (summary, correlation,principal component, and time series analyses arecommonly applied in the schools); and (vi) analysisof the main parameters influencing indoor concentra-tions (building age, seasons, ventilation rates, andindoor activities).
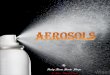
In Figure 2, the statistics (minimum values, 1st quar-tile, median, 3rd quartile and maximum values) of theparticle mass (PM10 and PM2.5) and number concen-trations obtained from the studies included in Table S3are reported. In terms of PM10, the median valuefor all schools was significantly higher indoors(102 lg/m3) than outside the schools (37 lg/m3). Thisincrement is largely due to indoor sources like resus-
Fig. 2 Distribution of the particle mass (PM10 and PM2.5) andnumber concentrations obtained from the studies included inTable S3
470
Morawska et al.
pension, which mainly influence the coarse fraction(Brani�s et al., 2005; Kingham et al., 2008). The corre-sponding wide range of indoor PM10 (higher than out-door PM10) indicates an important potential forreduction and the need to determine the main influen-tial parameters for this variability. This confirms that,to assess the personal exposure of children in schools,indoor PM10 measurements are vital, along with thecomplete characterization of indoor sources and chil-dren’s activities.
PM2.5 data were similar for both indoor and outdoorsampling sites, with a median value equal to about23 lg/m3. This variability is slightly higher in indoorenvironments, confirming a reduced influence ofindoor activities (mainly resuspension) on the fine frac-tion.
In Figure 2, negligible differences between the out-door and indoor measurements (8.2 9 103 particles/cm3 and 7.0 9 103 particles/cm3, respectively) are alsoreported for P) concentrations. This is due to the majorinfluence of UFP sources (mainly traffic) on outdoormonitoring sites, where, in the absence of relevantindoor UFP sources, the building envelope smothersthe ‘fresh’ outdoor peaks. Therefore, to assess the per-sonal exposure of children in schools to UFPs, outdoormeasurements are very important and have to beincluded in the experimental design. In terms of per-sonal exposure, the data were limited to particle massconcentration measurements reported in three of thereviewed papers (Borgini et al., 2011; Gauvin et al.,2002; Janssen et al., 1997), and therefore, it was insuffi-cient for performing any statistical analysis. It shouldbe noted that the data presented in Figure 2 do notaccount for differences in how the data were averaged,with the concentrations reported in Table S3 beingbased on a variety of averaging times (school time,daily, weekly, etc). Therefore, the main conclusion thatcan be drawn from the data presented in Figure 2, thatindoor PM10 and UFP concentrations are higher andlower than outdoor levels, respectively, would be fur-ther enhanced if only data for school times were con-sidered.
To assess personal exposure, data are needed thatcharacterize concentrations when a specific person ispresent in a given space. Concentrations given as dailyor weekly averages are not suitable, as these concentra-tions capture times when pupils are not at school, andconsequently, they are generally lower than specificschool time concentrations.
From data available in the reviewed articles, it canbe concluded that, in classrooms, PM10 concentrationsduring school hours were higher than outdoor concen-trations, whereas UFPs significantly increased withincreasing truck traffic density and significantlydecreased with increasing distance from the road. Ingeneral, the scientific literature is largely insufficientwith respect to: (i) monitoring personal exposure to
particles in schools; ii) UFP monitoring (limited to fewpapers); (iii) concentrations based on an averaging timethat only captures when the person in question is pres-ent in a given space (i.e., children are at school); (iv)the relationship between ambient concentration andpersonal exposure; and (v) the contribution of schoolexposure to a child’s daily exposure, with respect toother sources (transportation, home, outdoors, etc).
Particle composition
Chemical
As discussed in the previous chapters, particulate mat-ter in the indoor environment may be generated bymany different indoor and outdoor sources. The com-position of airborne particles is generally subject toconsiderable time and location-related fluctuations,due to these differing types of emission sources, as wellas different atmospheric conditions (Turner and Col-beck, 2008). Particles are generally composed of a fewmain, and many trace constituents, and the predomi-nant chemical components are sulfate, nitrate, ammo-nium, sea salt, minerals, OC, and EC (P€oschl, 2005).
Air exchange between a buildings indoor and out-door environment can lead to changes in the mixtureof particles found in indoor air, and this process oftenleads to correlations between indoor and outdoor con-centrations. For instance, Geller et al. (2002) foundindoor/outdoor (I/O) correlations in EC, sulfate, alu-minium, silicon, calcium, iron, titanium, zinc, andpotassium for desert aerosols in California. However,these correlations are not always strong, and the com-position of indoor and outdoor air particles can differgreatly, as demonstrated by Conner et al. (2001), in astudy conducted in Baltimore, MD in the UnitedStates. In addition to building air exchange rate, thefollowing processes influence the I/O ratio for the dif-ferent chemical species in particles:
• Particle penetration from outdoors through mechan-ical system ventilation ducts, or through cracks inwindows, doors, and building walls (Nazaroff,2004).
• Particle generation due to primary sources, such asfrom combustion processes, heating, cooking (Evanset al., 2008), household activities (G�ehin et al.,2008), hobbies, mechanical wear, biogenic sub-stances, skin, hair, pets, etc.
• Particle generation or alteration due to secondaryimpacts, such as partitioning of semivolatile organiccompounds (SVOCs) and chemical processes such assecondary organic aerosol (SOA) formation.
• Particle deposition and resuspension.In many outdoor particles, elements and metals can
be found which allow an insight into their origin. Forinstance, iron, silicon, aluminium, calcium, and potas-
471
Indoor aerosols
sium usually originate from natural sources, and tin,lead and transition metals are generally anthropogenic.Also, certain compounds tend to exist predominatelyin particles of particular sizes. Anlauf et al. (2006) ana-lyzed inorganic aerosol components as a function ofthe particle aerodynamic diameter. Ammonium andsulfate tended to be present in groups with a smallerdiameter, and nitrate, sodium. and chloride were foundmore often in the larger particle groups. The distribu-tion of metals in aerosols was investigated by Allenet al. (2001). Cadmium, tin, lead, and selenium tendedto be found in smaller particles, while nickel, zinc, cop-per, cobalt, manganese, and mercury were spreadacross a wide range of sizes, and iron, strontium andbarium tended to be found more in larger particles.Karanasiou et al. (2007) examined aerosols in the cityair in Athens for nine metals in different particle sizes.Anthropogenic components, such as cadmium andvanadium, were found in smaller size groups, whilecopper, chrome, iron, and aluminium were generallyfound in the larger aerosols. There were no clear ten-dencies for lead, nickel, and manganese, which can alsobe attributed to anthropogenic sources. Extensiveinvestigations into heavy metal pollution in airborneparticles have been carried out by Amato et al. (2009)and Klumpp et al. (2009).
Given that these outdoor particles infiltrate into theindoor environment, these relationships often hold forindoor particles as well. For instance, Chao and Wong(2002) demonstrated the dependency of elemental com-position on particle size for PM2.5 and PM10 in indoorair. Indoor processes affect this composition as well,with both Morawska et al. (2009a,b) and Barthel et al.(2011) finding small quantities of metals in aerosolsthat were emitted by laser printers. Grgic (2008) alsosummarized papers concerning the analysis of metalsin aerosols in a review article, which stated that theconcentration of metals in aerosols and their bioavail-ability (Voutsa and Samara, 2002) is influenced by aplethora of factors, such as the pH value, aerosol typeand size, organic material, and EC content (Desboeufset al., 2005).
The particles produced by indoor sources can havecompletely different compositions depending on theirorigin. For example, while OC and EC are alwaysreleased in combustion processes, Hedberg et al.(2002) found that polycyclic aromatic hydrocarbons(PAH), aluminium, silicon, phosphor, sulfate, andchlorine are also released when burning beech wood ina household oven. Burning candles were examined byPagels et al. (2009) and depending on the product,phosphate, sulfate, sodium, and potassium were foundto be significant aerosol components, besides EC andOC. Another strong source of emissions is incensesticks, which are often burned for religious reasons.Depending on the type if incense burned, the particlescan contain large quantities of EC, OC, anions, and
main, and transition elements (See and Balasubramani-an, 2011).
Nanosprays are a relatively new particle source inindoor environments. Norgaard et al. (2009) analyzedthe aerosols from a number of different sprays used forcleaning surfaces and found high levels of cyclic andperfluorinated siloxanes in the air both during andafter their use. Many sprays contain silver as an anti-bacterial active ingredient, and Quadros and Marr(2011) found that the emission of silver correlated withthat of chlorine in many of the spray aerosols. The par-ticles released by photocopiers do not, as previouslyspeculated, consist of toner carbon (Wensing et al.,2011), but they mainly arise through condensation ofSVOCs. Similarly, Wensing et al. (2008) found siliconand higher alkanes (C31–C45) in printer-generatedaerosols, which indicates secondary formation pro-cesses, and it is also assumed that the particles foundto be released by household electrical appliances arisevia SVOCs released by heat (Schripp et al., 2011).
In addition to this, chemical reactions betweenunsaturated organic substances and ozone take placeindoors in a similar way to which they do in atmo-spheric chemistry and lead to the formation of SOAs.Monoterpenes, such as d-limonene and a-pinene, areusually involved in this process, and these compoundsoriginate from indoor and outdoor sources, due to theuse of consumer products and wood off-gassing,respectively. Ozone/monoterpene reactions result inmany compounds, including: reactive intermediatessuch as hydroxyl radicals, alkylperoxy radicals, andCriegee biradicals; high volatility products such as car-bon dioxide or formaldehyde; and semivolatile prod-ucts such as carboxylic acids and hydroperoxides,which may yield SOAs (Kroll and Seinfeld, 2008).Indoors, SOA formation may be due to nucleation orgas-to-particle partitioning, and indoor formationinfluences particle distributions in the ultrafine and finesize ranges. Enhanced particle formation also mayoccur via polymerization reactions of the oxidationproducts within the particle phase. Particular analysiswas performed on the SOA formation potential of nat-ural paints (Lamorena et al., 2007), wood productsand natural paints (Schripp et al., 2012; Toftum et al.,2008), air fresheners (Lamorena and Lee, 2008), house-hold products (Coleman et al., 2008), and controlledterpene mixtures (Waring et al., 2011).
Few studies have ascertained the personal exposureof building occupants to different compositional ele-ments of indoor particles, and those that have, ana-lyzed integrated gravimetric filter samples. Forinstance, Zhao et al. (2006b) collected 24-h personalexposure samples for 38 individuals in four differentenvironments and attributed various sources to levelsof exposure to different compounds. The compositionof indoor particles was a function of the building airexchange rate, with indoor sources dominating the
472
Morawska et al.
fractional contribution to the composition at lower airexchange conditions. Sulfur, iron, lead, and EC weremainly attributed to outdoor sources (e.g., vehicleemissions), so the presence of these compoundsincreased with the air exchange rate. The most exten-sive study to measure personal exposure to particlecomposition was the RIOPA study, which measuredoutdoor, indoor, and personal exposure to particlesand volatile organic gases for 100 residents within 100different homes in three US cities (Weisel et al., 2005).Functional group and elemental analysis were per-formed on the personal exposure samples. The RIOPAstudy inferred that personal exposures were frequentlymodified by indoor sources that generated organicmaterial with a strong aliphatic character (Turpinet al., 2007).
Biological
Bioaerosols contain an heterogeneous mixture of par-ticles from microorganisms (fungi, bacteria, viruses),plants and animals (Dillon et al., 1996). The size ofthese particles varies significantly, ranging fromviruses (20–300 nm) to typical bacterial cells (0.5–3 lm), fungal spores (1.5–30 lm), and pollen grains(10–400 lm) (Reponen et al., 2001). In the literature,bioaerosols most often refer to fungal and bacterialaerosols, but in indoor air, it also includes particlesfrom house dust-mites, cockroaches, and insects andpets, as well as skin cells from humans and pets(Flannigan, 2001).
In general, outdoor air is the main source of fungalbioaerosols, and therefore, the tightness of a building’senvelope and the performance of filtration in a ventila-tion system will determine the I/O ratio in a givenbuilding, which is expected to be less than one. How-ever, in areas where the ground is frozen or coveredwith snow at various times throughout the year, indoorsources become the most significant contributor toindoor bioaerosol concentrations. In these situations, ahigh I/O does not necessarily indicate the presence ofexceptional sources and exposure. Many human activi-ties can affect bioaerosol concentrations, such as han-dling firewood, root vegetables and plants, which havebeen shown to elevate fungal spore concentrations(Hunter et al., 1988; Lehtonen et al., 1993). In relationto bacteria, humans themselves can be an importantindoor source (Nevalainen 1989; Qian et al., 2012),and humans or pets can also carry bioaerosols fromthe outdoors (Lehtonen et al., 1993) or from highlycontaminated environments, like cow barns (Pasanenet al., 1989). Resuspension also elevates indoor bio-aerosol concentrations, during activities such as clean-ing indoor surfaces.
In most studies, personal exposure to bioaerosols isassessed indirectly by measuring the concentration ofbioaerosols in occupied rooms or spaces. This indirect
method has been found to underestimate exposure toboth fungal and bacterial bioaerosols (Wang et al.,2012). One possible explanation for this the role ofhuman occupancy as a source of indoor biologicalaerosols. For example, Qian et al. (2012) reportedsize-resolved, per person-hour emission rates for bio-logical particles based on a mass-balance modelingapproach and illustrated the extent to which being inan occupied room results in exposure to bacteria thatare associated with previous or current human occu-pants. Recently, the qPCR methodology was devel-oped to assess viruses in the air, but like othermethods, it does not give precise information aboutpersonal exposure (Ziros et al., 2011). Fragments orconstituents measured in dust samples have also beenused as an indicator for assessing exposure to dust-mite allergens (Pauli et al., 1988).
One group of researchers used Button InhalableSamplers to measure the personal exposure of teachersto bioaerosols during winter in Finland. The overallaverage particle mass concentration was found to be57 lg/m3, with a total fungi count of 12.2 9 103
spores/m3 and 33 viable fungi colony-formingunits/m3. Corresponding values in the home and work-place (classroom) were 17 lg/m3, 10.8 9 103 spores/m3 and 30 cfu/m3, and 34 lg/m3, 12.0 9 103 spores/m3 and 19 cfu/m3, respectively. Bacteria concentra-tions in the classroom (14.5 9 104 spores/m3,1090 cfu/m3) were found to be higher than in the home(60.6 9 103 spores/m3, 340 cfu/m3), as well as higherthan overall average personal exposure (86.0 9 103
spores/m3, 720 cfu/m3) (Toivola, 2004; Toivola et al.,2002, 2004). Fungi concentrations were generallyhigher in the classrooms with a higher number ofpupils, as well as in homes with dogs that lived insideor those that reported the occasional condensation ofwater of inner window surfaces. Personal exposure tobacteria was found to be higher for men than womenand for people in younger age groups (27–40 and 40–48) compared with older ones (>48 years) (Toivola,2004; Toivola et al., 2004).
From the point of view of health outcomes, exposureassessment to causative agents is also important. Someof these are present in microbial cell walls (b-glucans)and can be analyzed as whole spores and also as frag-ments of cell walls. Adhikari et al. (2013) assessed theendotoxin and fungal fragments in 15 homes usingcyclone samplers which divided particles into threeranges: 1.8 lm. Accordingto enzyme activity and limulus amebocyte lysate tests,the
compared to stationary liquid impingers (Tolchinskyet al., 2011).
Intake/uptake and deposition in the lungs
Lung deposition modeling
In the indirect dose assessment approach, the daily PNor surface area deposited dose in tracheobronchial andalveolar airways for a given age group can be com-puted as: the product of the inhalation rate of a givenage group depending on the human activity; the frac-tional deposition depending on inhalation rate andparticle diameter, integrated over the whole PN sizedistribution; and the time spent for a given activity in adefined location (Buonanno et al., 2011, 2012b). Thus,to relate the inhaled ambient aerosol to bronchial andalveolar doses requires knowledge of the fractionaldeposition efficiencies of inhaled particles in differentregions of the human respiratory tract. Particle deposi-tion is determined by biological factors, such as lungmorphology and breathing patterns, and physical fac-tors such as fluid dynamics, particle properties anddeposition mechanisms (Hofmann, 2011).
At present, the direct experimental in situ determina-tion of particle deposition in human subjects is limitedto total deposition during a single breath for a widerange of particle sizes and flow rates (Hofmann et al.,2009; L€ondahl et al., 2006, 2008, 2009; Morawskaet al., 2005; ICRP, 1994; Heyder et al., 1986). Bron-chial and alveolar deposition as a function of particlesize and flow rate can only be derived indirectlyand with less accuracy from subsequent retentionmeasurements of radiolabeled aerosols (Heyder et al.,1986) or from the analysis of serial bolus depositiondata (Kim and Hu, 1998). However, health risk assess-ment for inhaled particles requires information onlocal deposition patterns within the lungs and suchinformation can only be provided by computationalmodeling.
Current particle deposition models can be groupedinto two categories, referring to the region of interestin the lung: (i) deposition in the whole lung (whole-lung models); or (ii) deposition in a localized region ofthe lung (local-scale models) (Hofmann, 2011). Inwhole-lung models, particle deposition in individualairways is computed by analytical equations for parti-cle deposition efficiencies under specific flow conditions(analytical approach). In local-scale models, particletransport and deposition equations are solved by Com-putational Fluid and Particle Dynamics (CFDP)methods (numerical models). At present, analyticalwhole-lung models are the most appropriate depositionmodels for the study of health effects in the whole lung.
At the onset of inhalation, particles pass through theextrathoracic region, bronchial and alveolated airways,and after a short breath-hold time, follow the same
path back during the exhalation phase. Their depth ofpenetration into the lungs depends on the time duringthe inhalation phase at which they are inhaled. Interms of deposition calculations, this transportscenario requires the computation of deposition effi-ciencies in extrathoracic, cylindrical bronchial and al-veolated airways, and quasi-hemispherical alveoli forthe whole breathing cycle. The two primary differencesbetween current models of inhaled particle depositionin the whole lung are the choice of the selected mor-phometric lung model, and the applied computationaltechniques, generally related to the complexity of theselected morphometric model. In general, five differentclasses of conceptual models with respect to lung mor-phometry and mathematical modeling technique havebeen recognized: (1) semiempirical regional compart-ment models (ICRP, 1994), (2) one-dimensional cross-section or ‘trumpet’ models (Taulbee and Yu, 1975),(3) deterministic symmetric generation or ‘single/typi-cal path’ models (Yeh and Schum, 1980), (4) determin-istic asymmetric generation or ‘multiple path’ models(Asgharian et al., 2001), and (5) stochastic asymmetricgeneration or ‘multiple path’ models (Koblinger andHofmann, 1990). Models 2–5 are often termed ‘mecha-nistic models’, as they are based on a mechanisticunderstanding of physiological and physical mecha-nisms, while Model 1 is based primarily on mathemati-cal fits to experimental data.
Indirect dose assessment approach
Several approaches exist for estimating human expo-sure. Direct methods involve exposure measures per-formed at the point of contact or uptake when theexposure occurs, while indirect methods involveextrapolating exposure estimates from other measuresand existing data. A number of indirect exposuremodels (AERMOD, CALTOX, SHEDS, UKADMS,etc) are described by Fryer et al. (2006). In Buonannoet al. (2011, 2012b), activity pattern data were com-bined with microenvironmental data (human activitiesand PN size distributions) using an indirect MonteCarlo method simulation approach, to evaluate thedoses of alveolar and tracheobronchial-deposited PNand surface area experienced by different age groupsin Cassino (South Italy) and Brisbane (Australia). Itwas found that females received higher doses thanmales, as a result of their different lifestyle patterns,with females spending more time in indoor environ-ments where higher exposure levels are experienced.With regard to age, adults (in particular, people aged19–40) received considerably higher doses than teen-agers (aged 15–18) and seniors (>65 years). This wasalso due to different lifestyle patterns, because theinhalation rates and other characteristics of the differ-ent age groups were found to have a negligible effecton dose. Overall, Italian daily alveolar PN and sur-
474
Morawska et al.
face area dose for all of the age groups was equal to1.5 9 1011 particles and 2.5 9 103 mm2, while thealveolar PN and surface area dose received by allAustralian age groups was equal to 3.0 9 1010 parti-cles and 4.5 9 102 mm2, respectively.
The main reason for the significant impact of life-style on received particle doses is due to the differentparticle exposure levels experienced in different mic-roenvironments. In particular, the highest dose intensi-ties were found during cooking and transportationactivities, including both indoor (car and bus) and out-door (pedestrian and bike) means. Higher doses werereceived by Italian people compared with Australians,mainly because in Italy, particle concentration levelswere significantly higher during eating, cooking, andtransportation activities. When particle deposition as afunction of the available air-tissue interface for differ-ent age groups is considered, infants and children (typi-cally receiving a lower absolute dose) turned out to beexposed to higher normalized doses than those experi-enced by working adults.
Risk assessment of indoor aerosols
Previous chapters have illustrated published methodsfor monitoring personal exposure to indoor aerosols,their composition and the levels of human exposure, aswell as the tools for dose assessment. They provide theinformation required for analyzing the potentialimpact that indoor aerosols may have on humanhealth. While indoor epidemiology is challenged by dif-ficulties in collecting exposure data from sufficientlylarge target populations, risk assessment can be con-ducted if an exposure–response relationship is avail-able for the exposure metric selected for the riskassessment. General risk assessment methodologies arewell established. However, there are specific challengesin applying these methods in the indoor environment,which makes the justification to give an overview ofthe general methodology in this particular context: ouraim is to summarize how the methods have been specif-ically used for indoor exposures.
There are four major steps in risk assessment proce-dure for both carcinogens and noncarcinogens: (i)hazard identification, (ii) exposure assessment, (iii)dose-response assessment, and (iv) risk characteriza-tion (United States National Research Council, 1983;USEPA, 1992, 2005).
Hazard identification refers to identifying the pollu-tants of concern, and their potential adverse healtheffects, on the basis of the results of epidemiologic,clinical, toxicological, and environmental research. PMmetrics and components identified as hazardousinclude PM2.5 and PM10 mass concentrations, PN con-centration (of ultrafine particles), PAH compounds,heavy metals (including Ni, Cd, Hg, Pb, V), elementalorganic carbon, etc.
Exposure assessment quantifies the amount of theconcerned pollutants that the receptor has beenexposed to for a certain duration. The exposure valueis then used to calculate the intake dose. It can beexpressed in the terms of chronic daily intake (CDI,mg/kg day), given by:
CDI
¼ Average Exposure Conc:� Inhalation Rate�Uptake FractionBody Weight
ð3Þ
where the inhalation rate and body weight arecommonly assumed to be 20 m3/day and 70 kg.
Dose-response assessment refers to estimating theprobability and frequency illnesses occur. The potencyfactor is used as an indicator for the severity of adversehealth effects. The values for commonly found pollu-tants can be found on the ‘Integrated Risk InformationSystem’ (IRIS, USEPA, 1998). It can also be namedthe inhalation UR (UR) and can be expressed in termsof the slope factor (SF), where SF = Potencyfactors 9 (body weight/inhalation rate).
Risk characterization combines the results from thedose-response and exposure assessments. The risk esti-mation methods for carcinogens and noncarcinogensare different. For carcinogens, with linear extrapola-tions, excess lifetime cancer risk can be calculated as:
ELCR ¼ SF� CDI. ð4ÞA commonly used acceptable value of ELCR is
defined by USEPA as 1 9 10�6 (USEPA, 2005).For noncarcinogens, with nonlinear extrapolations,
risk can be expressed as a hazard quotient (HQ) (USEP-A, 1992):
HQ ¼ CDIRfD
or HQ ¼ CDIRfC
ð5Þ
where RfD and RfC are the inhalation chronic refer-ence dose and inhalation chronic reference concentra-tion, respectively. The acceptable level of HQ is 1.
These provide a general procedure for estimating therisks of exposure to any known pollutant, when the‘risk potential’ (SF or dose-response) of the particularagent is known. For example, in research conducted byGuo et al. (2004), which estimated the ELCR ofVOCs, the CDI was expressed by the authors as:
CDI ¼ ðCA IR ED EF LÞðBW ATL NY) ð6Þ
where CA is the mean contaminant concentration (mg/m3); IR is the inhalation rate (m3/h); ED, EF, and Lare described as the total exposure duration in a year(hr); BW is the body weight (kg); ATL is the averagelifespan (years); and NY is the number of days in a
475
Indoor aerosols
year (365 days/year). CDI applies the unit of mg/kg/day. Potency factors are taken from the ‘IntegratedRisk Information System’ (IRIS, USEPA, 1998). Thestandard values suggested by USEPA (1994) to assistin these calculations are as follows: (i) 20 m3 inhaledair per day, with an average body weight of 70 and60 kg for adult men and women, respectively; (ii) 5 m3
inhaled air per day, with an average body weight of10 kg for a child; and (iii) an average lifespan of70 years.
The World Health Organization is using an environ-mental burden of disease approach and quantifyingboth carcinogenic and noncarcinogenic health risksusing disability adjusted life years (DALY). Thismethodology was recently applied for a number ofstressors, including ambient PM2.5 in European coun-tries in the ‘Environmental Burden of Disease inEuropean Countries’ (EBoDE) study (H€anninen et al.,2011). The approach was further specifically appliedto indoor exposures of PM2.5, mold particles and sec-ond-hand smoke (H€anninen et al., 2012). DALY isthe measure of health impact due to a disease and isgiven by:
DALY ¼ YLLþYLD ð7Þ
where YLL is the years of life loss due to prematuremortality and YLD is the years of lost due to disabilitycaused by morbidity. The primary model used in thisstudy is a three-step process for obtaining DALY, asoutlined below.
Relative risk identification means to provide a quan-tified level of risk due to the level of exposure:
RR ¼ expð EE�
lnRR�Þ ð8Þ
where RR° is the relative risk per unit exposure of E°,and E is the exposure threshold.
Population attribution fraction (PAF) is the reduc-tion in disease that would have occurred if the entirepopulation was not exposed to the risk. This is givenby:
PAF ¼ f� ðRR� 1Þf� ðRR� 1Þ þ 1 ð9Þ
where f is the fraction of population exposed.Environmental Burden of Disease is the final result
which is given by:
EBD ¼ PAF� BoD ð10Þ
where BoD is the burden of the target disease in ques-tion, in years, given by the WHO. This gives the totalDALY from a disease for the entire population, due toexposure to selected PM fraction. Currently, the
required RR parameters are well defined for PM2.5,PM10, and BC and are emerging for a number of otherPM components.
In the EBoDE study, the burden of disease forPM2.5 included cardiopulmonary mortality, lung can-cer mortality, total nonviolent mortality, chronic bron-chitis, and restricted activity days. For PM10, thediseases used for analysis included lower respiratorysymptoms and new cases of chronic bronchitis. Resultsshowed that the inhalation of suspended particularmatter posed the most severe health risk, with a DALYof 6000–10 000 per one million people. This was amuch higher burden of disease when compared withother indoor exposures like second-hand smoke (600–1200) and radon (600–900).
These examples illustrate how some specific chal-lenges can be handled for risk estimation in indoorenvironments. Also, exposure assessment in risk analy-sis is highly relevant and linked with the interpretationof E-R coefficients obtained in epidemiological set-tings. The net error in the assessment depends on thefactor variability in the exposure measurement. Fullhandling of the complexity of exposure metrics andindicators would need to be linked with the personalexposure levels discussed in section ‘Personal exposurelevels’ and the intake/uptake and deposition in the lungdiscussed in section ‘Intake/uptake and deposition inthe lungs’.
Studies on the risk assessment of indoor aerosols
This section reviews studies performed by researcherson the estimation of risks induced by carcinogens in anindoor environment. There were studies that compliedwith the given guidelines, as explained in the previoussections, and some which used modified methods forcalculating the risks.
Studies following the guidelines. Studies that performedrisk assessments, which complied with the given guide-lines, included a study on the ELCR for various car-cinogenic PAHs in Chinese, Malay and Indian foodstalls (See et al., 2006). It used the same methodsgiven by the USEPA, as illustrated by the variousequations discussed above, for calculating exposureand dose for the PAHs contained in airborne parti-cles. They reported that the ELCRs were 4.08 9 10�3,1.21 9 10�2, and 1.07 9 10�3 for Chinese, Malay,and Indian cooking stalls, respectively, which is higherthan the acceptable ELCR value provided by theUSEPA.
It must be noted that cancer may also be caused bycarcinogens in a gaseous form. The USEPA guidelinesare comprehensive and are applicable in such cases.Studies using USEPA guidelines for gaseous carcino-gens, including formaldehyde and acetaldehyde, havebeen conducted by Sousa et al. (2011), Cavalcante
476
Morawska et al.
et al. (2006), and Feng et al. (2006). They were per-formed in different environments in different countries.According to their findings, the cancer risks or ELCRs,ranged from the order of 10�8 in libraries in Brazil to10�4 in hotel ballrooms in China.
Studies which modified the methods used in the guide-lines. On the other hand, a few studies modified themethods used for exposure estimation and risk assess-ment, to adapt them to their assumptions and scenar-ios. See and Balasubramanian (2006) carried out a riskassessment for three metal noncarcinogens (Al, Cr, andMn) and four metal carcinogens (As, Cd, Cr, and Ni)which were emitted by cooking activities in indoorenvironments. The physical and chemical properties ofPM2.5 were investigated for a Chinese food stall in Sin-gapore that used gas stoves, and the average mass con-centrations of metals were measured to estimate therisks. In addition to the four basic steps described inthe guidelines above, the authors included a respiratorydeposition factor to improve the accuracy of the expo-sure assessment. The deposition factions of differentsized PMs were considered with an interpolated equa-tion:
Ei ¼ �0:081þ 0:23 lnðDpÞ2 þ 0:23ffiffiffiffiffiffiDp
p ð11Þwhere Ei is the deposition faction of particle size i, andDp was the diameter of the particle.
Then, the overall deposition faction (f) was calcu-lated using:
f ¼PðFiEiÞ
Fð12Þ
where F and Fi are the number concentrations of allparticles with an aerodynamic diameter
5–13 months experience shortness of breath and pleu-ral effusion. After a careful examination of the lung tis-sues, pulmonary fibrosis and pulmonary inflammationwere diagnosed. However, factory conditions are unli-kely to be the same as those in an ambient domesticenvironment, and therefore, these results are notdirectly useful for the public. In addition, it has beenshown that for patients with cardiovascular disease,the inhalation of UFP from diesel engines poses a highrisk of heart attacks (Miller et al., 2009). Althoughthere are currently no studies proving a direct linkbetween heart attacks and indoor UFP sources, it wasfound that people living close to traffic have a higherrisk of suffering from coronary arteriosclerosis, whichcauses heart attacks (Hoffmann et al., 2007).
General cancer risk assessments involve analyzingthe mass fraction of the chemical components ofinhaled particles and calculating the individual cancerrisks of the different chemical compounds, character-ized by the potency factor. However, there are cur-rently only a limited number of studies on the riskassessment of UFPs, resulting in a lack of data to con-struct the UFP equivalent of the potency factor. Someresearchers endeavored to carry out a risk assessmenton UFP by avoiding the dependency on potency factorusing odds ratios to estimate the probability of cancerrisk when exposed to UFP (Zalk et al., 2009; Zhaoet al., 2006a,b). Another proposed method is to statis-tically estimate the probability of cancer based onexposure to different number and surface concentra-tions of UFPs by analyzing the number of affectedpatients (Chio and Liao, 2008; Liao et al., 2011).
Recently, a study by Sze-To et al. (2012) attemptedto use the same approach used for PM to estimate theELCR of UFPs generated and inhaled when cooking,based on the following equation:
ELCR ¼ C� SF�QBW
ð13Þ
where C is the exposure concentration, SF is the inha-lation SF, Q is the daily inhalation rate (m3/day) andBW is the body weight (and 70 kg is used). Further-more, the equation was modified to suit the features ofUFP. The modified ELCR (for the UFP-related part)was expressed as:
ELCR ¼ SFmQBW
Cf
Zdp
CUFPðdpÞbðdpÞddp" #
ð14Þ
where SFm is the SF of the UFP mixture, cf is theconversion coefficient (in mg/nm2) for diesel engineexhaust data (which was recently recognized as a car-cinogen by the WHO (2012)), and CUFP is the parti-cle surface area concentration of UFP (nm2/m3).They reported that the average ELCR contributed by
UFP was 1.52 9 10�4 and 1.01 9 10�4 for cookingoccupants and other occupants, respectively, whichyielded results similar to some referencedepidemiological results (Wang et al., 2009b; Zhonget al., 1999).
Summary of the state of knowledge and recommendations forfuture research
This work was motivated by growing consideration ofthe scale, potential severity, and risks associated withhuman exposure to indoor PM. There have been sev-eral challenges identified, making the entire process ofrisk assessment, as well as its individual components,particularly complex. These include: (i) the vagueunderstanding of the term exposure, as it is oftenadopted in indoor sciences; (ii) the intrinsic challengesof PM investigations and the still incomplete under-standing of its overall impact on health; and (iii) thecontribution from both indoor and outdoor sources toexposures occurring indoors. Indoor exposure to PM isoften divided into two components, differing signifi-cantly in composition, temporal patterns, and theirrelationship to personal time–activity patterns: (I) par-ticles from outdoors, which can significantly affect PMlevels in indoor and traffic related microenvironments;and (II) particles from indoor sources, which have thepotential to generate very high levels of PM that donot correlate with outdoor levels on a temporal basis.Health responses associated with PM originate mostlyfrom ambient epidemiological studies, which are notsuitable for evaluating the composition-specific toxicityof indoor-generated particles. However, in studiesattempting to identify the difference constituents inambient PM, the results are very vague and heteroge-neous, suggesting that particle mass, and not composi-tion, may be the best indicator of PM toxicity. If thisindirect finding is expanded to indoor-generated parti-cles, partly supported by their similar composition,indoor-generated exposures should be treated just asseriously as exposure to ambient PM.
This review shows that personal exposure to indoorparticulate matter has traditionally been determinedfrom measurements carried out at fixed locations, inambient outdoor or indoor microenvironments (seesection ‘Methods for monitoring personal exposure toindoor particulate matter’). Even if such estimates arecommonly used, these are not as reliable or as accurateas monitoring by personal samplers that are worn orcarried by the subjects. In this article, we have provideda general summary of the various methods and instru-ments which have been used for the characterization ofPM in indoor microenvironments, for the purpose ofmeasuring personal exposure. With the advances intechnology, particularly miniaturization, there hasbeen a rapid proliferation of compact instruments thatcan be used for personal monitoring. While hand-held
478
Morawska et al.
instruments for monitoring gases, such as carbon diox-ide and carbon monoxide, have been around for manyyears, these are now being matched in size byinstruments that can measure particle mass, number,and surface area. In the near future, we can no doubtexpect to see instruments that measure gases, such asnitrogen dioxides, and a range of other chemical spe-cies.
There is a growing body of literature available onexposure to indoor aerosols in the residential environ-ment. Even so, not all of the results from these studiescan be directly compared, due to the differences instudy design and instrumentation; however, a generalpicture of the magnitudes and trends in exposure isstarting to emerge (as discussed in section ‘Residentialenvironment’). In particular, it has been shown that,in limited studies assessing daily integrated residentialexposure to UFPs, the contribution of indoor sourceswas ~50% (ranging from 19% to 76%). This not onlyindicates a strong dependence on resident activities,source events and site specificity, but it also highlightsthe importance of indoor sources for total personalexposure. Median values of reported indoor PM10concentrations have been shown to be slightly higherthan outdoor concentrations, while median indoorand outdoor values for PM2.5 were similar, but withhigher variations seen indoors. In addition, the med-ian value PM2.5 concentrations from personal moni-toring is also higher than indoor and outdoorconcentrations. On the basis of the reviewed articles, ageneral need is evident for: (i) characterization ofindoor residential sources by means of particle chemi-cal composition, toxicity, size-dependant physicalproperties affecting exposure and dose characteristics;(ii) personal exposure monitoring with portabledevices for better characterization of exposure (allow-ing for the capture of near-field exposures that are notwell characterized by stationary monitoring); (iii)apportionment of the contribution of indoor residen-tial and outdoor particles to personal exposure andtheir quantitative assessment on population represen-tative basis; (iv) modification of outdoor particles bybuildings and the effect on exposure (composition,size, dose, etc); (v) use of a normalized metric for inte-grated personal exposure assessment to enable mean-ingful comparisons (concentration h/day); (vi)characteri