Embed Size (px)
Citation preview

Hindawi Publishing CorporationJournal of Nutrition and MetabolismVolume 2012, Article ID 470656, 13 pagesdoi:10.1155/2012/470656
Review Article
Folate Intake and Markers of Folate Status in Womenof Reproductive Age, Pregnant and Lactating Women:A Meta-Analysis
Cristiana Berti,1 Katalin Fekete,2 Carla Dullemeijer,3 Monica Trovato,1
Olga W. Souverein,3 Adrienne Cavelaars,3 Rosalie Dhonukshe-Rutten,3 Maddalena Massari,1
Tamas Decsi,2 Pieter van’t Veer,3 and Irene Cetin1
1 Unit of Obstetrics and Gynecology, Department of Clinical Sciences Hospital ‘L. Sacco’ and Center for Fetal ResearchGiorgio Pardi, University of Milan, 20157 Milan, Italy
2 University of Pecs, H-7623 Pecs, Hungary3 Division of Human Nutrition, Wageningen University and Research Centre, P.O. Box 8129,6700 EV Wageningen, The Netherlands
Correspondence should be addressed to Irene Cetin, [email protected]
Received 13 January 2012; Accepted 24 May 2012
Academic Editor: Cornelia M. Witthoft
Copyright © 2012 Cristiana Berti et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Background. Pregnant and breastfeeding women are at risk for folate deficiency. Folate supplementation has been shown to beassociated with enhanced markers of folate status. However, dose-response analyses for adult women are still lacking. Objective.To assess the dose-response relationship between total folate intake (folic acid plus dietary folate) and markers of folate status(plasma/serum folate, red blood cell folate, and plasma homocysteine); to evaluate potential differences between women inchildbearing age, pregnant and lactating women. Methods. Electronic literature searches were carried out on three databases untilFebruary 2010. The overall pooled regression coefficient (β) and SE(β) were calculated using meta-analysis on a double-log scale.Results. The majority of data was based on nonpregnant, nonlactating women in childbearingage. The pooled estimate of therelationship between folate intake and serum/plasma folate was 0.56 (95% CI = 0.40–0.72, P < 0.00001); that is, the doubling offolate intake increases the folate level in serum/plasma by 47%. For red blood cell folate, the pooled-effect estimate was 0.30 (95%CI = 0.22–0.38, P < 0.00001), that is, +23% for doubling intake. For plasma-homocysteine it was –0.10 (95% = –0.17 to –0.04,P = 0.001), that is, –7% for doubling the intake. Associations tended to be weaker in pregnant and lactating women. Conclusion.Significant relationships between folate intake and serum/plasma folate, red blood cell folate, and plasma homocysteine werequantified. This dose-response methodology may be applied for setting requirements for women in childbearing age, as well as forpregnant and lactating women.
1. Introduction
Folate is involved in one-carbon transfer reactions, whichare fundamental for DNA and RNA synthesis, amino acidmetabolism, and formate oxidation [1]. Plasma or serumfolate, red blood cell (RBC) folate, and homocysteine(tHcy) are used as biomarkers of folate status and reflectreliably changes in folate intakes [2, 3]. Serum folate reflectsprimarily recent intake, whereas erythrocyte folate levelsreflect time-integrated intake and are considered to be a
measure of long-term folate status [4]. Plasma homocysteineis an indicator of low or deficient folate status, and thereforeconsidered as an indicator of folate adequacy [5] on the basisthat normal homocysteine metabolism requires an adequatesupply of folate [6].
Folate intake and status play a crucial role duringpregnancy [7]. Pregnant and breastfeeding women are atrisk for folate deficiency due to an increased need forfolate. Previously, a longitudinal study showed low folatestatus among participants, especially in late pregnancy and

2 Journal of Nutrition and Metabolism
during lactation [3]. Moreover, a meta-analysis includingtwenty-one controlled trials on folate supplementation inpregnant women showed that compared to placebo orno supplementation, folate supplementation was associatedwith strongly increased serum folate levels and red cellfolate levels [8]. Regarding breastfeeding, a review of theliterature indicates that apparently healthy women, who donot receive folic acid supplementation, can already becomefolate depleted in the early postpartum [9].
Deriving a dose-response association may help to addressthe above issues and identify major modifiers of the intake-status relationship, useful to address questions on the“optimal” level of a folate biomarker and to recommend-ing intake of folic acid/folate for mother’s and newborn’shealth. Actually, the adequate folate intake during pregnancyhas not been clearly stated yet. Six hundred μg/day DFEs(Dietary Folate Equivalents) are considered sufficient tomaintain adequate folate status in pregnant women [10–12]. Nordic Nutrition Recommendations [13] recommend500 μg/day DFE while the dietary reference intakes of totalfolate are 400 μg/day in Italy [14] and 300 μg/day in UK[15]. Internationally, women are advised to use folic acidsupplements during the periconceptional period on the basisof the well-recognized link between maternal folate statusand neural tube defects (NTDs) [16]. Some debate alsoexists regarding the proper daily dosage of folic acid/folatefor preventing NTDs [17]. The current recommendation tosupplement 400 μg folic acid daily starting at least 4 weeksbefore conception which seems to be not enough to achieveoptimal-red-cell-folate levels within 4 weeks, because thisrequires at least 8–12 weeks of daily intake [18]. In contrast,with 800 μg folic acid, the health criterion is reached withinan average of 4 weeks after the start of supplementation[19]. Regarding lactating women, for example, Mackey andPicciano [20] found that folate status in lactating womenwas preserved with 1 mg/day of supplemental folate for threemonths.
However, the strength of the dose-response relationshipbetween folate intake and folate biomarkers has not beenestablished yet, except for the relation with risk of NTDs inwomen aged 20–65 years [21]. Consequently, we used meta-analysis to model folate status as a function of supplementalfolate intake. We conducted a meta-analysis of data fromrandomised controlled studies (RCTs) that examined theeffect of folate exposure on folate status in women inchildbearing age, pregnant and lactating women, in order toquantitatively assess folate dose-response relationships.
2. Methods
This research is part of a project within the EuropeanMicronutrient Recommendations Aligned (EURRECA) Net-work of Excellence that aims to identify micronutrientrequirements for optimal health in European populations[22]. The review here reported was part of a wider reviewprocess to identify studies assessing the effect of folate intakeon both different markers of folate status as well as healthoutcomes.
3. Electronic Searches
The methodology here used is based on a standard method-ology developed for EURRECA reviews [23]. A protocol wasprovided outlining specific linkages among the populationsof interest, exposures, modifying factors, biological role offolate, and outcomes of interest, in order to define studyeligibility criteria prior to starting the literature search andin order to interpret relevant studies once they are identified.The general search strategy included terms for randomisedcontrolled trials in humans AND (intake or status) AND(folate or folic acid or vitamin B9). Electronic searcheswere carried out over all years until February 2010. Bothindexing and text terms were used and each search strategywas further adapted for the individual databases searched(Ovid EMBASE, Ovid Medline, and Cochrane Central). Thereference lists of collected articles and of published reviewswere also checked for relevant studies to be included into thescreening and data extraction process.
4. Data Collection
The results of the searches were combined, and papers werescreened on the basis of title and abstract; references clearlynot meeting the review criteria were excluded. This task wasdivided between two independent reviewers (K. Fekete andC. Berti), with a minimum of 10% overlapping in order toharmonise the process. Once potentially relevant literaturewas identified, full-text articles were retrieved and reviewedfor inclusion on the basis of the predetermined inclu-sion/exclusion criteria (Table 1). Only papers meeting allcriteria were included and extracted onto an Access databaseby a single reviewer (C. Berti). Corresponding authors ofpapers were contacted to obtain values or data when datain the original articles were not clear or presented as graph.Information pertaining to bibliographic details, and studycharacteristics, as well as nutrient supplement informationsuch as intake/dose, source of micronutrient, chemical form,mode of delivery, duration of delivery, chemical analysis,measures of prior nutritional status, level of the nutrientin the background diet, method used to estimate intake,and analytical methods used to assess nutrient status werecollated.
5. Assessment of Internal Validity
In order to assess the risk of bias of the studies, thefollowing indicators of internal validity specific to the RCTmethodology were collected during data extraction: (1)method of sequence generation and allocation, (2) blinding,(3) potential funding bias, (4) number of participants atstart, (5) dropouts and dropout reasons, (6) dose check,(7) dietary intake data reported, (8) outcome comparabilityand reproducibility, and (9) similarity of most and leastexposed groups at baseline. Based on these indicators, tworeviewers decided on the overall risk of bias. Disagreementswere resolved by discussion. The criteria for judging theseindicators were adapted from the Cochrane Handbook [38].

Journal of Nutrition and Metabolism 3
Table 1: Inclusion criteria followed to select potentially relevantpapers for data extraction.
Populationcharacteristics
Apparently healthy participants at baseline
Study design Randomised controlled trial
InterventionSupplements or fortified foods or naturaldiet intakes versus a placebo or untreatedgroup
Duration 4 weeks
OutcomesMust report the following relationships:intake-status
Intake measuresReport of intake from supplements orfortified foods or natural food sources
Statusmeasurements
Red blood cell (RBC) folatePlasma/serum folateHomocysteine (tHcy)
Baselineinformation
Baseline data must be present for allreported outcomes
6. Data Analysis
The effect of total folate intake (folic acid plus dietary folate),expressed as μg/d DFEs [39], was investigated through meta-analysis of the intervention group compared with the controlgroup for all included studies that assessed the specifiedbiomarkers of folate status. Based on the assumption that thebioavailability of folic acid added to food is greater than thatof natural food folate by a factor of 1.7, the amounts of folicacid from supplements/fortified foods were transformed intoamounts of folate by multiplying × 1.7 [6, 39]. In the studiesevaluating the effects of supplements or fortified foods, whendietary intake was not provided, the mean dietary folateintake of 247 μg/day from other comparable studies was usedin the calculation. If required, concentration data expressedas nmol/l were converted to the SI units conventional μg/L(i.e., ng/mL) by dividing by the conversion factor (i.e., 2.266).
We calculated an intake-status regression coefficient
(β) and the corresponding standard error (SE) for eachindividual study [40]. The intake-status relationship wasassumed to be linear on the ln-ln-scale (natural logarithm ofintake versus natural logarithm of status). This assumptionis based upon our hypothesis that within the range ofobservations, the true intake-status relationship for folatecan be described by a monotonic concave curve, which slowlygrows to positive infinity as intake increases and rapidly goesto negative infinity as intake approaches 0. We calculatedthe overall pooled β and its SE using random effectsmeta-analysis, which estimates the between-study varianceusing the method of DerSimonian and Laird [41] and usesthis estimate to modify the weights used to calculate thesummary estimate. Residual heterogeneity between studieswas evaluated using the I2 statistic. A priori defined subgroupanalyses according to dose, duration of supplementation,and population group were carried out to try to explainthe heterogeneity. Meta-analysis was carried out with ReviewManager (RevMan) 5.0 (Copenhagen: The Nordic CochraneCentre, The Cochrane Collaboration, 2008).
7. Results
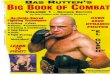
Figure 1 shows the flow diagram outlining the search resultsfor pregnant and lactating women. Of the overall 4067 hitsrecovered through the general search, after the removal ofduplicates and titles and abstracts highly unlikely to berelevant for the aims of this paper (data not shown), a totalof 283 titles and abstracts were potentially available. Afterinclusion of studies from bibliographic searches, title andabstract were screened, 136 were collected as full-text articles,and 15 articles fulfilled the inclusion criteria. Papers wereexcluded because they were review articles, or dealt with notinterventional studies, or with trial inappropriately designedor with intervention studies including other populationgroups or nonhealthy women or without the minimalduration or dealt with combined intervention where theeffects could not be attributed solely to folic acid. Also, paperswith incomplete data not obtainable from the authors wereexcluded.
Characteristics of the included studies are summarisedin Table 2. Eight studies compared the placebo group withmore than one intervention group [18, 24–31, 36]. Themajority of interventions assessed the effect of folic acidfrom supplements (n = 14), while only one used fortifiedfoods [32]. Four studies [18, 30, 31, 36] were designed asthree-arm trials, comparing placebo to both folic acid and 5-methyltetrahydrofolate or [6S]-5-methyltetrahydrofolate (5-MTHF) or racemic MTHF. We analysed the two types ofsupplement separately.
Ten studies included women in childbearing age, threewere on pregnant women [33–35] and two included lactatingwomen [20, 36]. Placebo was used in the control group in themajority of studies except for two studies [27, 33] in whichthe control group did not undergo any treatment. Only onestudy included pregnant adolescents [35]. Most of the trials(i.e., ten) were conducted in Europe, two in New Zealand [24,32], one was in Brazil [35], one in Canada [36], and one inthe USA [20].
The majority of the studies (e.g., 12 out of 15) presenteda moderate risk of bias (data not shown). The most commonreason for this was an overall lack of information aboutthe method of randomization (i.e., inadequate or unclearsequence generation and/or allocation) and/or unclearsource of funding. In contrast, most of the trials reportedreasons for dropouts and numbers of dropouts, as well asinformation on compliance (i.e., methods, number of nocompliants or dose check).
8. Serum/Plasma Folate
We identified nine studies that reported the effect of specifieddoses of folic acid up to 1.0 mg/day plus dietary folateon serum/plasma folate. Three trials were in pregnantwomen, four in women in childbearing age, and two studiesduring the postpartum period. Overall, 632 participants wereincluded in the studies with a duration ranging from 4 to 25weeks. For further details on the characteristics of includedstudies, see Table 2.

4 Journal of Nutrition and Metabolism
Ta
ble
2:G
ener
alch
arac
teri
stic
sof
the
incl
ude
dst
udi
esan
deff
ects
onth
ebi
omar
kers
offo
late
inte
rven
tion
inw
omen
ofch
ildbe
arin
gag
e,pr
egn
ant
and
lact
atin
gw
omen
,wit
hre
spec
tto
the
con
trol
/pla
cebo
acco
rdin
gto
the
orig
inal
pape
r.
Au
thor
,yea
rC
oun
try
Popu
lati
on(n
.in
clu
ded)
Des
crip
tion
ofsu
pply
N.i
nin
terv
enti
on(F
A)
and
inco
ntr
olgr
oups
(P)
atla
test
tim
e
Stu
dyde
sign
Bio
mar
kers
repo
rted
Pva
lue
Ada
nk
etal
.,20
03[2
4]N
ewZ
eala
nd
Ch
ildbe
arin
gag
ew
omen
(239
)
Folic
acid
caps
ule=
400μ
g/da
y.Fo
licac
idca
psu
le=
2800
μg/
wee
k.P
lace
boca
psu
le
FA(4
00)=
36P=
44
Dou
ble
blin
d.D
ura
tion
:12
wks
.D
ieta
ryas
sess
men
t
RB
Cfo
late
(nm
ol/L
)(M
icro
tite
rte
chn
iqu
e,L
.C
asei
).P
lasm
ah
omoc
yste
ine
(μm
ol/L
)(fl
uor
esce
nce
pola
riza
tion
imm
un
oass
ay).
<0.
001
<0.
05
Bro
uwer
etal
.,19
991
[25]
Net
her
lan
ds
Ch
ildbe
arin
gag
ew
omen
(144
)
Folic
acid
tabl
et=
250μ
g/da
y(5
00μ
gfo
licac
idan
da
plac
ebo
tabl
etev
ery
seco
nd
day)
.Fo
licac
idta
blet
=50
0μ
g/da
y.P
lace
bota
blet
.
FA(2
50)=
50FA
(500
)=
45P=
49
Dou
ble
blin
d,2
con
tain
ers
ofin
dist
ingu
ish
able
tabl
ets:
one
red
mar
ked,
one
yello
wm
arke
d.D
ura
tion
:4w
ks.
Die
tary
asse
ssm
ent
RB
Cfo
late
(nm
ol/L
)(I
mx
auto
mat
edim
mu
noa
ssay
syst
em).
Pla
sma
fola
te(I
mx
auto
mat
edim
mu
noa
ssay
syst
em).
FA(2
50):
a<
0.01
FA(5
00):
a<
0.00
1FA
(250
):a<
0.00
1FA
(500
):a<
0.00
1
Bro
uwer
etal
.,19
992
[26]
Net
her
lan
ds
Ch
ildbe
arin
gag
ew
omen
(144
)
Folic
acid
tabl
et=
250μ
g/da
y(5
00μ
gfo
licac
idev
ery
the
2nd
day)
.Fo
licac
idta
blet
=50
0μ
g/da
y.P
lace
bota
blet
.
FA(2
50)=
50FA
(500
)=
45P=
49
Dou
ble
blin
d,2
con
tain
ers
ofin
dist
ingu
ish
able
tabl
ets:
one
red-
mar
ked,
one
yello
w-m
arke
d.D
ura
tion
:4w
ks.
Die
tary
asse
ssm
ent
Pla
sma
hom
ocys
tein
e(μ
mol
/L)
(HP
LCan
dfl
uor
imet
ric
dete
ctio
n)
FA(2
50):
a<
0.01
FA(5
00):
a<
0.00
1
Cu
skel
lyet
al.,
1996
[27]
UK
Ch
ildbe
arin
gag
ew
omen
(49)
Folic
acid
caps
ule=
400μ
g/da
y.Fo
lic-a
cid-
fort
ified
food
spl
us
400μ
g/da
y(F
A-f
).D
ieta
ryfo
late
plu
s40
0μ
g/da
y(F
A-d
).D
ieta
ryad
vice
(DA
)C
ontr
olgr
oup:
no
trea
tmen
t
FA=
9FA
-f=
6FA
-d=
10D
A=
7P=
9
Du
rati
on:1
2w
ksm
os.
Die
tary
asse
ssm
ent
RB
Cfo
late
(μg/
L)
(mic
robi
olog
ical
assa
y)
Dal
yet
al.,
1997
[28]
Irel
and
Ch
ildbe
arin
gag
ew
omen
(110
)Fo
licac
idta
blet
=20
0–40
0μ
g/da
y.P
lace
bota
blet
FA(1
00)=
22FA
(200
)=
28FA
(400
)=
26P=
19
Dou
ble
blin
d,id
enti
cal
tabl
ets.
Du
rati
on:2
4w
ks
RB
Cfo
late
(μg/
L)
(mic
robi
olog
ical
assa
y)
Dal
yet
al.,
2002
[29]
Irel
and
Ch
ildbe
arin
gag
ew
omen
(110
)Fo
licac
idta
blet
=20
0–40
0μ
g/da
y.P
lace
bota
blet
FA(1
00)=
21FA
(200
)=
28FA
(400
)=
26P=
19
Dou
ble
blin
d,id
enti
cal
tabl
ets.
Du
rati
on:1
0w
ks
Pla
sma
hom
ocys
tein
e(μ
mol
/L)
(au
tom
ated
flu
ores
cen
ce-p
olar
izat
ion
met
hod
).
Lam
ers
etal
.,20
04[3
0]G
erm
any
Ch
ildbe
arin
gag
ew
omen
(144
)
Folic
acid
caps
ule=
400μ
g/da
y.[6S]
-5-M
TH
Fca
psu
le=
416μ
g/da
y.[6S]
-5-M
TH
Fca
psu
le=
208μ
g/da
y.P
lace
boca
psu
le
FA=
34Lo
wM
TH
F=
32H
igh
MT
HF=
35P=
34
Dou
ble
blin
d,h
ard
gela
tin
eca
psu
les
Du
rati
on:2
4w
ks
Pla
sma
hom
ocys
tein
e(μ
mol
/L)
(im
mu
noa
ssay
onA
xSY
Man
alys
er).
FA:a
<0.
01Lo
wM
TH
F:a<
0.01
Hig
hM
TH
F:a<
0.01

Journal of Nutrition and Metabolism 5T
abl
e2:
Con
tin
ued
.
Au
thor
,yea
rC
oun
try
Popu
lati
on(n
.in
clu
ded)
Des
crip
tion
ofsu
pply
N.i
nin
terv
enti
on(F
A)
and
inco
ntr
olgr
oups
(P)
atla
test
tim
e
Stu
dyde
sign
Bio
mar
kers
repo
rted
Pva
lue
Lam
ers
etal
.,20
06∗
[18]
Ger
man
y
Ch
ildbe
arin
gag
ew
omen
(144
)
Folic
acid
caps
ule=
400μ
g/da
y.[6S]
-5-M
TH
Fca
psu
le=
416μ
g/da
y.[6S]
-5-M
TH
Fca
psu
le=
208μ
g/da
y.P
lace
boca
psu
le
FA=
34Lo
wM
TH
F=
33H
igh
MT
HF=
35P=
34
Dou
ble
blin
d,h
ard
gela
tin
eca
psu
les.
Du
rati
on:2
4w
ks.
Red
bloo
dce
llfo
late
(nm
ol/L
)({
(wh
ole
bloo
dfo
late×
100)
–(p
lasm
afo
late×
(100
–h
emat
ocri
t))}
).P
lasm
afo
late
(nm
ol/L
)(m
icro
biol
ogic
alas
say)
Foh
ret
al.,
2002
[31]
Ger
man
y
Ch
ildbe
arin
gag
ew
omen
(163
)
Folic
acid
caps
ule=
400μ
g/da
y.M
TH
F(r
acem
icm
ixtu
re)
caps
ule=
480μ
g/da
y.P
lace
boca
psu
le
FA=
51M
TH
F=
52P=
57
Dou
ble
blin
d.D
ura
tion
:8w
ks.
RB
Cfo
late
(nm
ol/L
)(i
mm
un
oass
ayki
tfo
rIM
xan
alys
er).
Pla
sma
fola
te(n
mol
/L)
(im
mu
noa
ssay
kit
for
IMx
anal
yser
).P
lasm
ah
omoc
yste
ine
(μm
ol/L
)(r
ever
sed-
phas
eH
PLC
).
Gre
enet
al.,
2005
[32]
New
Zea
lan
d
Ch
ildbe
arin
gag
ew
omen
(73)
75g
pow
dere
dm
ilkda
ily.
Fort
ified
milk
=37
5μ
gfo
licac
id/d
ay.
Con
trol
milk
FA=
36P=
37
Dou
ble
blin
d.D
ura
tion
:12
wks
.D
ieta
ryas
sess
men
t
RB
Cfo
late
(nm
ol/L
)(f
rom
wh
ole
bloo
dfo
late
bysu
btra
ctin
gpl
asm
afo
late
and
corr
ecti
ng
for
hem
atoc
rit)
.P
lasm
afo
late
(nm
ol/L
)(m
icro
tite
rte
chn
iqu
e,ch
lora
mph
enic
olre
sist
ant,
L.C
asei
).P
lasm
ah
omoc
yste
ine
(μm
ol/L
)(I
mx
anal
yzer
).
Elli
son
etal
.,20
04[3
3]U
KP
regn
ant
wom
en(3
0)Fo
licac
idca
psu
le=
400μ
g/da
y.C
ontr
olgr
oup:
no
trea
tmen
t.FA
=15
P=
15D
ura
tion
:24
wks
.
Pla
ma
fola
te(n
g/m
L).
Pla
sma
hom
ocys
tein
e(μ
mol
/L)
(en
zym
eim
mu
noa
ssay
).
<0.
05
Lira
etal
.,19
89[3
4]Sp
ain
Pre
gnan
tw
omen
(153
)
Mu
ltiv
itam
inca
psu
les.
Supp
lem
ent=
350μ
gfo
licac
id,1
05m
gfe
rrou
ssu
lph
ate,
500
mg
asco
rbic
acid
,da
ily.
Pla
cebo
=10
5m
gfe
rrou
ssu
lph
ate,
500
mg
asco
rbic
acid
,dai
ly.
FA=
75P=
78
Ran
ge:0
–350
μg/
day.
Du
rati
on:2
5w
ks.
RB
Cfo
late
(μg/
L)(L
.Cas
eim
icro
biol
ogic
alas
say)
.Se
rum
fola
te(μ
g/L
)(L
.C
asei
mic
robi
olog
ical
assa
y).
<0.
001
<0.
001
Nog
uei
raet
al.,
2003
[35]
Bra
zil
Pre
gnan
tw
omen
(114
)
Min
eral
tabl
ets.
Supp
lem
ent=
250μ
gfo
licac
id,1
20m
gir
onsu
lph
ate/
day.
Pla
cebo
:120
iron
sulp
hat
e/da
y.
FA=
15P=
16D
ura
tion
:22
wks
.P
lasm
afo
late
(mg/
mL)
(Rad
ioim
mu
noa
ssay
-Io
do12
5).

6 Journal of Nutrition and Metabolism
Ta
ble
2:C
onti
nu
ed.
Au
thor
,yea
rC
oun
try
Popu
lati
on(n
.in
clu
ded)
Des
crip
tion
ofsu
pply
N.i
nin
terv
enti
on(F
A)
and
inco
ntr
olgr
oups
(P)
atla
test
tim
e
Stu
dyde
sign
Bio
mar
kers
repo
rted
Pva
lue
Hou
ghto
net
al.,
2006
[36]
Can
ada
Lac
tati
ng
wom
en(6
9)
Folic
acid
caps
ule=
400μ
g/da
y.[6S]
-5-M
TH
Fca
psu
le=
416μ
g/da
y.P
lace
boca
psu
le
FA=
21M
TH
F=
21P=
22
Dou
ble
blin
d.D
ura
tion
:16
wks
.D
ieta
ryas
sess
men
t
RB
C(n
mol
/L)
(fro
mth
ew
hol
e-bl
ood
fola
teby
subt
ract
ing
plas
ma
fola
tean
dco
rrec
tin
gfo
rh
emat
ocri
t).
Pla
sma
fola
te(n
mol
/L)
(L.
rham
nos
us
mic
robi
olog
ical
assa
y).
Pla
sma
hom
ocys
tein
e(μ
mol
/L)
(HP
LC)
FA:<
0.00
2M
TH
F:<
0.00
01M
TH
F:<
0.00
2
Mac
key
and
Pic
cian
o,19
99[2
0]U
SAL
acta
tin
gw
omen
(42)
Folic
acid
caps
ule
s=
1m
g/da
y.P
lace
bota
blet
FA=
21P=
21
Dou
ble
blin
d,fo
licac
idta
blet
sin
dist
ingu
ish
able
from
plac
ebo
tabl
ets.
Du
rati
on:1
2w
ks.
Die
tary
asse
ssm
ent
RB
Cfo
late
(nm
ol/L
)(L
.C
asei
mic
robi
olog
ical
assa
y).
Pla
sma
fola
te(n
mol
/L)
(L.
Cas
eim
icro
biol
ogic
alas
say)
.P
lasm
ah
omoc
yste
ine
(μm
ol/L
)(H
PLC
).
<0.
05
∗T
he
Au
thor
ski
ndl
yre
ques
ted
us
toci
tebo
thth
epu
blic
atio
nin
AJC
N[1
8]an
dLa
mer
s’P
h.D
.th
esis
for
the
raw
data
[37]
.R
CB
:red
bloo
dce
ll.a Si
gnifi
can
tdi
ffer
ence
sbe
twee
nth
eba
selin
ean
dth
een
dof
the
trea
tmen
t.FA
:fol
icac
id.
MT
HF:
met
hylt
etra
hydr
ofol
ate.

Journal of Nutrition and Metabolism 7
Titles and abstracts retrieved fromelectronic, bibliographic, and expertsearches: 283
Titles and abstracts veryunlikely to be relevant: 147
Titles and abstracts appearedpotentially relevant, and collectedas full texts: 136
Full papers meeting inclusioncriteria: 15
•••
Plasma folate: 9Erythrocyte folate: 10Plasma total homocysteine: 9
Excluded studies: 121
Not RCTs (n = 46), cluster RCTs (n = 7), not adequate control group(n = 11): 64
Inadequate results for the biomarkers of interest: 15No values provided for the biomarkers of interest: 9Combined interventions where the effect could not be attributed tofolic acid/folate only: 16Review (n = 5), only abstract (n = 3): 8Other micronutrient or other population: 3
Not apparently healthy women: 6
Figure 1: Flow diagram of the articles screened, assessed, and excluded at various stages for this paper.
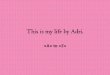
The forest plot of serum/plasma folate response to folicacid plus dietary folate supply is shown in Table 4. Theoverall pooled estimate was 0.56 (95% CI = 0.40–0.72), anda significant effect of folate on serum/plasma concentrationswas demonstrated (P < 0.00001). This means that a 2-fold higher folate intake corresponds to a 1.47-fold higherserum/plasma folate, that is, a 47% increase. The test forheterogeneity showed high heterogeneity among the studies.When subgroup analyses were carried out, heterogeneityremained high within these subgroups (Table 3). The resultsof the meta-analysis derive mainly from the trials on womenin childbearing age which represented half of all subjects.
When the effect of 5-MTHF plus dietary folate wasquantified in three studies in a total of 221 women, we foundan overall pooled estimate (95% CI) of =1.18 (0.65, 1.71);P < 0.0001 (Table 4). A doubling of 5-MTHF intake will leadto increase serum/plasma folate levels by 2.26-fold, that is,126%.
9. Red Blood Cell Folate
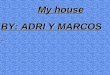
Ten trials contained eligible data regarding the effects of folicacid up to 1.0 mg/day plus dietary folate on (RBC) folate.These trials included 724 women. Supplements were takenbetween 4 and 24 weeks. These trials primarily involvedwomen of childbearing age (seven trials), whereas onlyone trial included pregnant women and two trials includedwomen during the post partum period. For further details
on the characteristics of included studies, see Table 2. Asdemonstrated in Table 5, pooling response to folic acid/folatesupplementation in one meta-analysis yielded an overallpooled Beta (95% CI) of 0.30 [0.22, 0.38]; P < 0.00001).This means that doubling the intake of folic acid leads to an23% increase of RBC folate concentrations. Primary analysiswas highly heterogeneous. Stratified analyses did not reducesubstantially the level of heterogeneity (Table 3). The resultsof the meta-analysis are highly influenced by the trials withwomen of childbearing age, because they represented themajority of subjects (486 out of 724) included in the meta-analysis.
Among the 10 studies, three also administered 5-MTHFplus dietary folate in a total of 221 women. When combinedin meta-analysis, the overall pooled estimate was 0.49 (0.20,0.77) (P = 0.0008) (Table 5).
10. Plasma tHcy
We identified nine studies that reported the effect of specifieddoses of folic acid up to 1.0 mg/day plus dietary folate onplasma tHcy. The intervention duration ranged from 4 to24 weeks. These trials were mostly conducted in womenin childbearing age (six trials), one was conducting duringpregnancy, and two studies were in women during thepostpartum period. For further details on the characteristicsof included studies, see Table 2. The primary analysis ofthe trials (Table 6) suggested that daily folic acid/folate was

8 Journal of Nutrition and Metabolism
Ta
ble
3:E
ffec
tsof
tota
lfol
ate
supp
ly(i
.e.,
folic
acid
plus
diet
ary
fola
te)1
onfo
late
inpl
asm
a/se
rum
and
inre
dbl
ood
cells
,as
wel
las
onpl
asm
ah
omoc
yste
ine
leve
lsin
wom
en,s
trat
ified
bypo
pula
tion
grou
p,du
rati
onof
supp
lem
enta
tion
,an
ddo
seof
folic
acid
supp
lem
enta
tion
.
Stra
tum
for
anal
ysis
Fola
tein
plas
ma/
seru
mFo
late
inre
dbl
ood
cells
Tota
lpla
sma
hom
ocys
tein
e
No.
ofst
udi
es(n
part
icip
ants
)
Reg
ress
ion
coeffi
cien
t[9
5%C
I]
Het
erog
enei
tyI2
(%)
No.
ofst
udi
es(n
part
icip
ants
)
Reg
ress
ion
coeffi
cien
t[9
5%C
I]
Het
erog
enei
tyI2
(%)
No.
ofst
udi
es(n
part
icip
ants
)
Reg
ress
ion
coeffi
cien
t[9
5%C
I]
Het
erog
enei
tyI2
(%)
All
stu
dies
9(6
32)
0.56
∗∗∗
[0.4
0,0.
72]
9210
(724
)0.
30∗∗∗
[0.2
2,0.
38]
829
(585
)−0
.10∗
∗
[−0.
17,−
0.04
]72
Popu
lati
ongr
oup
Wom
enin
child
bear
ing
age
4(3
43)
0.65
∗∗∗
[0.3
9,0.
92]
967
(486
)0.
33∗∗∗
[0.2
3,0.
44]
866
(470
)−0
.12∗
∗∗
[−0.
15,−
0.08
]0
Pre
gnan
tw
omen
3(2
04)
0.52
∗∗∗
[0.3
0,0.
75]
691
(153
)0.
26∗∗∗
[0.1
5,0.
37]
n.a
1(3
0)−0
.42∗
∗∗
[−0.
58,−
0.25
]n
.a
Lac
tati
ng
wom
en2
(85)
0.36
[0.0
8,0.
79]
902
(85)
0.19
∗∗∗
[0.0
9,0.
28]
02
(85)
0.03
[−0.
04,0
.11]
0
Du
rati
onof
supp
lem
enta
tion
4–12
wee
ks4
(317
)0.
51∗∗∗
[0.2
2,0.
80]
966
(415
)0.
27∗∗∗
[0.1
7,0.
37]
836
(444
)−0
.10∗
∗∗
[−0.
14,−
0.05
]31
13–2
0w
eeks
1(4
3)0.
58∗∗∗
[0.3
8,0.
77]
n.a
1(4
3)0.
26∗∗
[0.0
8,0.
44]
n.a
1(4
3)0.
03[ −
0.06
,0.1
2]n
.a
≥21
wee
ks4
(272
)0.
60∗∗∗
[0.3
8,0.
82]
843
(266
)0.
39∗∗∗
[0.2
3,0.
55]
762
(98)
−0.2
6[−
0.55
,0.0
4]90
Dos
e ≤250
μg
FA/d
ay2
(120
)0.
61∗
[0.0
5,1.
17]
822
(146
)0.
28[−
0.06
,0.6
2]70
2(1
46)
−0.1
3[−
0.28
,0.0
2]68
251–
500μ
gFA
/day
7(5
69)
0.59
∗∗∗
[0.4
1,0.
76]
939
(682
)0.
32∗∗∗
[0.2
3,0.
40]
828
(543
)−0
.12∗
∗∗
[−0.
18,−
0.06
]69
>50
0μ
gFA
/day
1(4
2)0.
13[ −
0.07
,0.3
3]n
.a1
(42)
0.16
∗∗
[0.0
4,0.
27]
n.a
1(4
2)0.
05[−
0.08
,0.1
8]n
.a
1T
he
amou
nts
offo
licac
idfr
omsu
pple
men
ts/f
orti
fied
food
sw
ere
tran
sfor
med
into
amou
nts
offo
late
bym
ult
iply
ing×
1.7
(IO
M,
2000
;[6
]).
Wh
enn
otpr
ovid
edin
the
RC
T,th
edi
etar
yfo
late
inta
keu
sed
corr
espo
nde
dto
the
mea
nva
lue
of24
7μ
g/da
y.n
.a:n
otap
plic
able
.Te
stfo
rov
eral
leff
ect
(P):∗<
0.05
,∗∗<
0.01
,∗∗∗
<0.
001.

Journal of Nutrition and Metabolism 9
Table 4: Forest plot of the effects of total folate supply (i.e., supplement plus dietary folate), with the supplement provided in form of folicacid and [6S]-5-methyltetrahydrofolate [5-MTHF] on serum or plasma folate in childbearing age, pregnant and lactating women.
Study or subgroup Beta SE Weight BetaIV, Random, 95% CI
BetaIV, Random, 95% CI
Folic acid
−2 −1 0 1 2
Brouwer et al., 1999 1 [26] 0.35741049 0.04126697 12.5% 0.36 [0.28, 0.44]
Ellison et al., 2004 [33] 0.53050104 0.09332632 11.1% 0.53 [0.35, 0.71]
Fohr et al., 2002 a [31] 0.53023607 0.04406458 12.5% 0.53 [0.44, 0.62]
Green et al., 2005 [32] 1.00981877 0.06717076 11.9% 1.01 [0.88, 1.14]
Houghton et al., 2006 f [36] 0.57853113 0.09878823 10.9% 0.53 [0.38, 0.77]
Lamers et al., 2006 c [18] 0.7384753 0.06637089 11.9% 0.74 [0.61, 0.87]
Lira et al., 1989 [34] 0.37051554 0.06476415 12.0% 0.37 [0.24, 0.50]
Mackey and Picciano, 1999 [20] 0.13206921 0.10234828 10.8% 0.13 [−0.07, 0.33]
Nogueira et al., 2003 [35] 0.94291343 0.24037313 6.3% 0.94 [0.47, 1.41]
Subtotal (95% CI) 100.0% 0.56 [0.40, 0.72]
Heterogeneity: Tau2 = 0.05; Chi2 = 102.70, df = 8 (P < 0.00001); I2 = 92%
Test for overall effect: Z = 6.68 (P < 0.00001)
5-MTHF
Fohr et al., 2002 b [31] 1.65921221 0.05130933 35.0% 1.66 [1.56, 1.76]
Houghton et al., 2006 g [36] 0.74857769 0.17130372 31.0% 0.75 [0.41, 1.03]
Lamers et al., 2006 e [18] 1.06897313 0.0904731 34.0% 1.07 [0.39, 1.25]
Subtotal (95% CI) 100.0% 1.18 [0.65, 1.71]
Heterogeneity: Tau2 = 0.21; Chi2 = 50.98, df = 2 (P < 0.00001); I2 = 96%
Test for overall effect: Z = 4.35 (P < 0.0001)∗
The Authors kindly requested us to cite both the publication in AJCN [18] and Lamers’ Ph.D. thesis for the raw data [37].RCB: red blood cell.aSignificant differences between the baseline and the end of the treatment.FA: folic acid.MTHF: methyltetrahydrofolate.
significantly inversely associated with tHcy concentrations(overall pooled Beta; Beta-random effect (95% CI) = −0.10(−0.17, −0.04); P = 0.001, n = 585). Consequently, adoubling of folate intake lowers the levels of tHcy by 7%.The heterogeneity was high and therefore subgroup analysiswas conducted (Table 3). This showed that heterogeneity waslower in the subgroup of trials in women in childbearingage and breastfeeding, as well as in the subgroup of trialswith a duration of 4–12 weeks of supplementation. Again,the majority of subjects in the meta-analysis were women ofchildbearing age.
Of the studies, three also evaluated the effect of 5-MTHFplus dietary folate in a total of 221 women. An inverse, butnot statistically significant association, was found between5-MTHF and plasma tHcy (overall pooled Beta [95% CI] =−0.08 [−0.20, 0.04]) (Table 6).
11. Discussion
The amount of nutrients needed to prevent deficiencies, tomaintain body stores, and to reduce the risk of chronicdiseases represent the basis for establishing micronutrientrecommendations. Our meta-analysis was designed to quan-tify the dose-response relationship between folate intake and
biomarkers of folate status. This information is useful todecide what dose of folate or folic acid to recommend forwomen planning a pregnancy, and subsequent lactation.Previously, only Wald et al. [21] provided a quantitativeestimate of the dose-response relation between folic acidintake, in doses of up to 1 mg/day, and risk of NTD assessed.They found that serum folate concentrations increase by 0.94μg/L (95% CI = 0.77–1.10) for every 0.1 mg/day increase infolic acid intake in women aged 20–35 years. We applied abase-e logarithmic transformation on the folate intake upto 1 mg/day and markers of folate status. The overall Betarepresents the difference in the ln-transformed predictedvalue of serum/plasma folate status per one-unit differenceon the ln-transformed scale of folate intake. Therefore,the relative change in intake to the power β represents therelative change in the biomarker concentration. For example,the overall pooled Beta of 0.56 for women means that a 1.4-fold increase of the mean intake from 250 to 350 μg/daycorresponds to a 1.21-fold increase in plasma folate, thatis, from an average of 16.0 to 19.3 nmol/L (=1.21 ∗ 16),that is, 3.3 nmol/L per 100 μg/day, which is about 1.5 timesstronger than the estimated 2.13 nmol/L per 0.1 mg/day asestimated by Wald et al. [21]. Such a difference may beexplained by considering both the characteristics of thestudies included and the methodological approach used.

10 Journal of Nutrition and Metabolism
Table 5: Forest plot of the effects of total folate supply (i.e., supplement plus dietary folate), with the supplement in form of folic acid and[6S]-5-methyltetrahydrofolate (5-MTHF) on red blood cell (RBC) folate in childbearing age, pregnant and lactating women.
Study or subgroup Beta SE Weight BetaIV, Random. 95% CI
BetaIV, Random, 95% CI
Folic acid
−1 −0.5 0 0.5 1
Brouwer et al., 1999 1 [26] 0.35741049 0.04126697 12.5% 0.36 [0.23, 0.44]
Ellison et al., 2004 [33] 0.53050104 0.09332632 11.1% 0.53 [0.35, 0.71]
Fohr et al., 2002 a [31] 0.53023607 0.04406458 12.5% 0.53 [0.44, 0.62]
Green et al., 2005 [32] 1.00981877 0.06717076 11.9% 1.01 [0.88, 1.14]
Houghton et al., 2006 f [36] 0.57853113 0.09878823 10.9% 0.58 [0.38, 0.77]
Lamers et al., 2006 c [18] 0.7384753 0.06637089 11.9% 0.74 [0.61, 0.87]
Lira et al., 1989 [34] 0.37051554 0.06476415 12.0% 0.37 [0.24, 0.50]
Mackey and Picciano, 1999 [20] 0.13206921 0.10234828 10.8% 0.13 [−0.07, 0.33]
Nogueira et al., 2003 [35] 0.94291343 0.24037313 6.3% 0.94 [0.47, 1.41]
Subtotal (95% CI) 100.0% 0.56 [0.40, 0.72]
Heterogeneity: Tau2 = 0.05; Chi2 = 102.70, df = 8 (P < 0.00001); I2 = 92%
Test for overall effect: Z = 6.68 (P < 0.00001)
5-MTHF
Fohr et al., 2002 b [31] 1.65921221 0.05130933 35.0% 1.66 [1.56, 1.76]
Houghton et al, 2006 g [36] 0.74857769 0.17130372 31.0% 0.75 [0.41, 1.08]
Lamers et al., 2006 e [18] 1.06897313 0.0904731 34.0% 1.07 [0.89, 1.25]
Subtotal (95% CI) 100.0% 1.18 [0.65, 1.71]
Heterogeneity: Tau2 = 0.21; Chi2 = 50.98, df = 2 (P < 0.00001); I2 = 96%
Test for overall effect: Z = 4.35 (P < 0.0001)∗
The Authors kindly requested us to cite both the publication in AJCN [18] and Lamers’ Ph.D. thesis for the raw data [37].RCB: red blood cell.aSignificant differences between the baseline and the end of the treatment.FA: folic acid.MTHF: methyltetrahydrofolate.
Firstly, Wald and colleagues [21] included trials with andwithout a placebo/control group in their analysis whilst weused only data from randomized controlled trials. Moreover,our review involved more updated references with respectto the papers they evaluated, and only two studies wereincluded in our as well as their meta-analysis. Finally, Waldand colleagues evaluated the effect for given doses of folicacid, not for total folate intakes (i.e., folic acid plus dietaryfolate).
The main effect found by pooling data from the selectedRCTs showed that folic acid plus dietary folate supply exerteda significant effect on all the markers of folate status, whichwas particularly strong for RBC and plasma/serum folate.Similarly, the meta-analysis by Mohamed [8] showed thatroutine folate supplementation in pregnancy resulted in asubstantial reduction in the incidence of low serum andRBC levels. However, the strength of the dose-responserelationships, we observed in pregnant women and inlactating women was weaker than that found within womenin childbearing age. During these physiological periodsmaintaining maternal biomarkers concentration at a givenlevel seems to be more difficult. This may be due to theanabolic needs of pregnancy and the loss via lactation.Based on factorial approaches, folate requirements during
pregnancy are 5- to 10-fold higher than in the nonpregnantcondition, owing to the enlargement of the uterus, thedevelopment of the placenta, the increasing red cell volumeof the mother, and the growth of the developing fetus[17]. In breast feeding, milk folate secretion is strictlyregulated to keep folate supply at a level that prevents thedevelopment of folate inadequacy in infants, but often at theexpense of maternal folate stores. Metz and colleagues [42]demonstrated that folic acid was preferentially uptaken bymilk compared to serum. Moreover, the same authors foundthat also in lactating women with severe folate deficiency,oral administration of folic acid appeared to be transferredto breast milk in preference even to the hemapoietic systems[42].
It is worthwhile to note that all the RCTs included inthe meta-analysis were studies of supplementation. Supple-mental amounts of folate are required to satisfy the increasedneeds of women planning pregnancy, during pregnancy andbreastfeeding. Since natural food folates degrade during foodprocessing, and their bioavailability is low [7], folate intakesfrom diet are found to be suboptimal from the perspective ofachieving an optimal folate status [6]. In contrast, folic acid,that is, the synthetic form of folate, is highly bioavailable andchemically stable, thus it is the most common form of folate

Journal of Nutrition and Metabolism 11
Table 6: Forest plot of the effects of total folate supply (i.e., supplement plus dietary folate), with the supplement provided in form offolic acid and [6S]-5-methyltetrahydrofolate (5-MTHF) on plasma homocysteine (tHcy) folate in childbearing age, pregnant and lactatingwomen.
Study or subgroup Beta SE WeightBeta
IV, random, 95% CIBeta
IV, random, 95% CI
Folic acid
−25−0.5 0 0.50.25
Adank et al., 2003 [24] −0.12165995 0.05185699 11.9% −0.12 [−0.22, −0.02]
Brouwer et al., 1999 2 [25] −0.12939736 0.0321808 14.7% −0.13 [−0.19, −0.07]
Daly et al., 2002 [29] −0.07160639 0.05422432 11.5% −0.07 [−0.18, 0.03]
Ellison et al., 2004 [33] −0.41748287 0.08565077 7.7% −0.42 [−0.59, −0.25]
Fohr et al., 2002 a [31] −0.12081128 0.03080075 14.9% −0.12 [−0.18, −0.06]
Green et al., 2005 [32] −0.15712523 0.16696333 3.0% −0.16 [−0.48, 0.17]
Houghton et al., 2006 f [36] 0.02653085 0.04645807 12.7% 0.03 [−0.06, 0.12]
Lamers et al., 2004 n [30] −0.11673333 0.04042075 13.5% −0.12 [−0.20, −0.04]
Mackey and Picciano, 1999 [20] 0.05149742 0.06490784 10.1% 0.05 [−0.08, 0.18]
Subtotal (95% CI) 100.0% −0.10 [−0.17, −0.04]
Heterogeneity: Tau2 = 0.01; Chi2 = 28.61, df = 8 (P = 0.0004); I2 = 72%
Test for overall effect: Z = 3.26 (P = 0.001)
5-MTHF
Fohr et al., 2002 b [31] −0.01327471 0.03959555 37.5% −0.01 [−0.09, 0.06]
Houghton et al., 2006 g [36] −0.03682917 0.06823177 28.5% −0.04 [−0.17, 0.10]
Lamers et al., 2004 p [30] −0.19316684 0.0506911 34.0% −0.19 [−0.29, −0.09]
Subtotal (95% CI) 100.0% −0.08 [−0.20, 0.04]
Heterogeneity: Tau2 = 0.01; Chi2 = 8.18, df =2 (P = 0.02); I2 = 76%
Test for overall effect: Z = 1.34 (P = 0.18)
used in supplements and fortified foods. Interestingly, bycomparing the strength of associations between total folateintake and folate status, we observed that the relationshiptended to be stronger for 5-MTHF than for folic acid. Someauthors suggested that 5-MTHF was as effective as or moreeffective than folic acid in preserving folate status [17, 18, 36]given that 5-MTHF is the predominant folate transport andstorage form within the body. Use of the naturally occurringfolate form 5-MTHF as a possible substitute for folic acid isunder consideration because it is unlikely to mask vitamin B-12 deficiency, and does not produce unmetabolized folic acidin the circulation in contrast to folic acid [43].
The main strength of this meta-analysis is the selection ofdata from randomized controlled trials. Ideally, RCTs shouldprovide reliable data about the effect of an intervention.This means that changes in folate indicators are definitelydue to folic acid/folate intervention. However, it has to betaken into account that after the Medical Research CouncilVitamin Study [16] studies designed to assess the effect offolic acid intake on measures of folate status in the pericon-ceptional period cannot be studied in controlled trials dueto ethical reasons. Folic acid supplementation is recognizedindispensable around conception in protecting against NTDsbecause the neural tube closes between 23rd and 27th day ofpregnancy. Thereby, the application of our inclusion criterialets us to exclude several studies on this topic because theywere not RCTs. Moreover, we found that there is an overalllack of research regarding the role of folate in pregnancy
outcomes different from NTDs. Further research is needed toinvestigate the role of folate supply in the latter two trimestersof pregnancy. An adequate folate intake seems in fact toplay an important role in the implantation and developmentof the placenta, and in improving endothelial function,to suggest that adequate amount of folate might also bebeneficial along the entire gestation [7]. Similarly, functionalor health outcomes of various folic acid/folate intakes havebeen rarely explored in lactating women. On the whole, infact, trials included in this review mostly recruited womenof childbearing age, while trials on women during pregnancyand lactation are scarce, suggesting that further research isneeded to explore this question. Most of the trials includedsmall size samples. Moreover, our assessment of internalvalidity showed that most of the studies had a moderateto high risk of bias as assessed by our criteria. We found agreat heterogeneity among trials probably due to differencesin methodological factors and physiological characteristicsof women studied. However, the analysis of the potentialinfluence of folic acid dose, duration of supplementation, orpopulation on the association revealed that these factors didnot significantly explain the between-study heterogeneity.
12. Conclusion
Statistically significant relationships between total folateintake and serum/plasma folate, red blood cell folate and

12 Journal of Nutrition and Metabolism
tHcy were shown. In particular, a doubling of the total folateintake significantly increased the folate concentration level inserum/plasma and RBC by 47% and 23%, respectively, andlowered the levels of plasma tHcy by 7%. This dose-responseapproach here applied may in future be applied for derivingthe intake dose necessary to achieve the optimal level of afolate biomarker for women of childbearing age, as well asfor pregnant and lactating women.
Conflict of Interest
No conflicts of interest have been declared by the authors.
Acknowledgments
The authors would like to thank Anne Molloy and YvonneLamers because they kindly provided us with some informa-tion and missing data. This research was undertaken as anactivity of the European Micronutrient RecommendationsAligned (EURRECA) Network of Excellence [22], fundedby the European Commission Contract no. FP6 036196-2(FOOD). The original conception of the systematic reviewwas undertaken by the EURRECA Network and coordinatedby partners based at Wageningen University (WU), theNetherlands and the University of East Anglia (UEA), UK.Susan Fairweather-Tait (UEA), Lisette de Groot (WU), Pietervan’t Veer (WU), Kate Ashton (UEA), Amelie Casgrain(UEA), Adrienne Cavelaars (WU), Rachel Collings (UEA),Rosalie Dhonukshe-Rutten (WU), Esmee Doets (WU),LindaHarvey (UEA), and Lee Hooper (UEA) designed anddeveloped the review protocol and search strategy.
References
[1] A. Djukic, “Folate-responsive neurologic diseases,” PediatricNeurology, vol. 37, no. 6, pp. 387–397, 2007.
[2] Homocysteine Lowering Trialists’ Collaboration, “Loweringblood homocysteine with folic acid based supplements: meta-analysis of randomised trials,” British Medical Journal, vol. 316,no. 7135, pp. 894–898, 1998.
[3] N. Milman, K. E. Byg, A. M. Hvas, T. Bergholt, and L. Eriksen,“Erythrocyte folate, plasma folate and plasma homocysteineduring normal pregnancy and postpartum: a longitudinalstudy comprising 404 Danish women,” European Journal ofHaematology, vol. 76, no. 3, pp. 200–205, 2006.
[4] C. P. Wild, C. Andersson, N. M. O’Brien, L. Wilson, and J. A.Woods, “A critical evaluation of the application of biomarkersin epidemiological studies on diet and health,” British Journalof Nutrition, vol. 86, no. 1, pp. S37–S53, 2001.
[5] World Health Organization and Food and Agriculture Orga-nization of the United Nations, “Folate and folic acid,” inVitamin and Mineral Requirements in Human Nutrition, pp.289–302, FAO/WHO Report, 2nd edition, 2004.
[6] H. Mc Nulty and J. M. Scott, “Intake and status of folateand related B-vitamins: considerations and challenges inachieving optimal status,” British Journal of Nutrition, vol. 99,supplement 3, pp. S48–S54, 2008.
[7] K. Fekete, C. Berti, I. Cetin, M. Hermoso, B. V. Koletzko, andT. Decsi, “Perinatal folate supply: relevance in health outcome
parameters,” Maternal and Child Nutrition, vol. 6, supplement2, pp. S23–S38, 2010.
[8] M. K. Folate, “Supplementation in pregnancy,” The CochraneDatabase of Systematic Reviews, no. 3, Article ID CD000183,1997.
[9] T. Tamura and M. F. Picciano, “Folate and human reproduc-tion,” American Journal of Clinical Nutrition, vol. 83, no. 5, pp.993–1016, 2006.
[10] German Nutrition Society and Austrian Nutrition Society,“Swiss Society for Nutrition Research,” Reference Values forNutrient Intake (D-A-CH), 2000.
[11] “Nutrient Reference Values for Australia and New Zealand,”National Health and Medical Research Council, 2005.
[12] O. Moreiras, A. Carbajal, L. Cabrera, and C. Cuadrado,“ıIngestas recomendadas de energiIa y nutrientes para lapoblacioIn espanfiola,” ı Tablas de composicion de alimentos,11a edicioIn revisada y ampliada, pp. 227-230, 2007.
[13] Nordic Nutrition Recommendations (NNR), Integrating Nutri-tion and Physical Activity, Nordic Council of Ministers,Copenhagen, Denmark, 4th edition, 2004.
[14] Livelli di Assunzione Raccomandati di Energia e Nutrienti perla Popolazione Italiana (LARN), Revision, Societa Italiana diNutrizione Umana (SINU), 1996.
[15] Panel on DRVs of the Committee on Medical Aspects of FoodPolicy (COMA), “Dietary reference values (DRVs) for foodenergy and nutrients for the UK,” Report on Health and SocialSubjects 41, 1991.
[16] MRC Vitamin Study Research Group, “Prevention of neuraltube defects: results of the Medical Research Council VitaminStudy,” The Lancet, vol. 338, no. 8760, pp. 131–137, 1991.
[17] C. Berti, H. K. Biesalski, R. Gartner et al., “Micronutrientsin pregnancy: current knowledge and unresolved questions,”Clinical Nutrition, vol. 30, pp. 689–701, 2011.
[18] Y. Lamers, R. Prinz-Langenohl, S. Bramswig, and K. Pietrzik,“Red blood cell folate concentrations increase more after sup-plementation with [6S]-5-methyltetrahydrofolate than withfolic acid in women of childbearing age,” The American Journalof Clinical Nutrition, vol. 84, pp. 156–161, 2006.
[19] K. Pietrzik, R. Prinz-Langenohl, Y. Lamers, E. S. Wintergerst,and S. Bramswig, “Randomized, placebo-controlled, double-blind study evaluating the effectiveness of a folic acid contain-ing multivitamin supplement in increasing erythrocyte folatelevels in young women of child-bearing age,” in Poster at the18th International Nutrition Congress, Durban, South Africa,September, 2005.
[20] A. D. Mackey and M. F. Picciano, “Maternal folate statusduring extended lactation and the effect of supplemental folicacid,” American Journal of Clinical Nutrition, vol. 69, no. 2, pp.285–292, 1999.
[21] N. J. Wald, M. R. Law, J. K. Morris, and D. S. Wald,“Quantifying the effect of folic acid,” The Lancet, vol. 358, no.9298, pp. 2069–2073, 2001.
[22] http://www.eurreca.org/everyone.[23] E. L. Doets, J. P. van Wijngaarden, A. Szczecinska et al.,
“Vitamin B12 intake and status and cognitive function inelderly people: a systematic review with meta-analyses”.
[24] C. Adank, T. J. Green, C. M. Skeaff, and B. Briars, “Weeklyhigh-dose folic acid supplementation is effective in loweringserum homocysteine concentrations in women,” Annals ofNutrition and Metabolism, vol. 47, no. 2, pp. 55–59, 2003.
[25] I. A. Brouwer, M. van Dusseldorp, M. Duran et al., “Low-dose folic acid supplementation does not influence plasmamethionine concentrations in young non-pregnant women,”British Journal of Nutrition, vol. 82, no. 2, pp. 85–89, 1999.

Journal of Nutrition and Metabolism 13
[26] I. A. Brouwer, M. van Dusseldorp, C. M. G. Thomaset al., “Low-dose folic acid supplementation decreases plasmahomocysteine concentrations: a randomized trial,” AmericanJournal of Clinical Nutrition, vol. 1, no. 69, pp. 99–104, 1999.
[27] G. J. Cuskelly, H. McNulty, and J. M. Scott, “Effect ofincreasing dietary folate on red-cell folate: implications forprevention of neural tube defects,” The Lancet, vol. 347, no.9002, pp. 657–659, 1996.
[28] S. Daly, J. L. Mills, A. M. Molloy et al., “Minimum effectivedose of folic acid for food fortification to prevent neural-tubedefects,” The Lancet, vol. 350, no. 9092, pp. 1666–1669, 1997.
[29] S. Daly, J. L. Mills, A. M. Molloy et al., “Low-dose folic acidlowers plasma homocysteine levels in women of child-bearingage,” QJM—Monthly Journal of the Association of Physicians,vol. 95, no. 11, pp. 733–740, 2002.
[30] Y. Lamers, R. Prinz-Langenohl, R. Moser, and K. Pietrzik,“Supplementation with [6S]-5-methyltetrahydrofolate or folicacid equally reduces plasma total homocysteine concen-trations in healthy women,” American Journal of ClinicalNutrition, vol. 79, no. 3, pp. 473–478, 2004.
[31] I. P. Fohr, R. Prinz-Langenohl, A. Bronstrup et al., “5,10-Methylenetetrahydrofolate reductase genotype determines theplasma homocysteine-lowering effect of supplementationwith 5-methyltetrahydrofolate or folic acid in healthy youngwomen,” American Journal of Clinical Nutrition, vol. 75, no. 2,pp. 275–282, 2002.
[32] T. J. Green, S. C. Murray, J. E. P. Rockell, and B. J. Venn,“Folic acid fortified milk increases blood folate and lowershomocysteine concentration in women of childbearing age,”Asia Pacific Journal of Clinical Nutrition, vol. 14, no. 2, pp. 173–178, 2005.
[33] J. Ellison, P. Clark, I. D. Walker, and I. A. Greer, “Effect ofsupplementation with folic acid throughout pregnancy onplasma homocysteine concentration,” Thrombosis Research,vol. 114, no. 1, pp. 25–27, 2004.
[34] P. Lira, N. Barrena, A. Foradori, G. Gormaz, and G. Grebe,“Folate deficiency in pregnancy: effect of supplemental folate,”Sangre, vol. 34, no. 1, pp. 24–27, 1989.
[35] N. N. Nogueira, J. V. Parente, and S. M. F. Cozzolino,“Mudancas na concentracao plasmatica de zinco e acido folicoem adolescentes gravidas submetidas a diferentes esquemas desuplementacao,” Cadernos de Saude Publica, vol. 19, pp. 155–160, 2003.
[36] L. A. Houghton, K. L. Sherwood, R. Pawlosky, S. Ito, andD. L. O’Connor, “[6S]-5-Methyltetrahydrofolate is at least aseffective as folic acid in preventing a decline in blood folateconcentrations during lactation,” American Journal of ClinicalNutrition, vol. 83, no. 4, pp. 842–850, 2006.
[37] Y. Lamers, (6S)-5-Methyltetrahydrofolate Compared to FolicAcid Supplementation: Effect on Risk Markers of Neural TubeDefects, Cuvillier, Goettingen, Germany, 2006.
[38] J. P. T. Higgins and S. Green, Cochrane Handbook for SystematicReviews of Interventions Version 5.0.2, 2009.
[39] Institute of Medicine, Dietary Reference Intakes for Thiamin,Riboflavin, Niacin, Vitamin B6, Folate, Vitamin B12, Pan-thothenic Acid, Biotin, and Choline, National Academy Press,Washington, DC, USA, 2000.
[40] O. W. Souverein, C. Dullemeijer, P. van’t Veer P, and H. vande Voet, “Transformations of summary statistics as input inmeta-analysis for linear dose-response models on a logarith-mic scale: a methodology developed within EURRECA,” BMCMedical Research Methodology, vol. 12, article 57, 2012.
[41] R. DerSimonian and N. Laird, “Meta-analysis in clinical trials,”Controlled Clinical Trials, vol. 7, no. 3, pp. 177–188, 1986.
[42] J. Metz, R. Zalusky, and V. Herbert, “Folic acid binding byserum and milk,” American Journal of Clinical Nutrition, vol.21, no. 4, pp. 289–297, 1968.
[43] B. J. Venn, T. J. Green, R. Moser, J. E. Mckenzie, C. M. Skeaff,and J. Mann, “Increases in blood folate indices are similarin women of childbearing age supplemented with [6S]-5-methyltetrahydrofolate and folic acid,” Journal of Nutrition,vol. 132, no. 11, pp. 3353–3355, 2002.

Submit your manuscripts athttp://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com