Embed Size (px)
Citation preview

RevenueCycleStrategist
Insights and actions for successful results
hfma.org/rcs
Sponsored by
www.parallon.net
October 2013
In recent years, the Centers for Medicare& Medicaid Services (CMS) has increasedthe number of program contractors thatreview provider claims and payments(see the sidebar on page 2). The alphabetsoup of CMS contractors can be confusingbecause they all share responsibility for identifying potential overpaymentsand conducting pre- and post-paymentaudits.
A recent federal decision furtherempowers these contractors. They nowhave the authority to determine paymenterror rates that, in turn, may justifyextrapolation of alleged error rates to theuniverse of claims beyond the original
sample (Gentiva Healthcare Corp. v.Sebelius, No. 1:11-cv-00438, D.C.Cir. July 23, 2013).
ZPICs contract with CMS to perform aunique role and responsibility. Althoughaudits by other CMS contractors mayresult in a provider’s obligation torefund previous payments, a ZPIC auditmay expose a provider or supplier topotential liability for fraud. Indeed,ZPICs function as the fraud detectionarm of the Medicare AdministrativeContractors (MACs) and are tasked withidentifying instances of potential fraudthat may result in large overpaymentsand/or referral to other government
Although all CMS payment audits should be taken seriously, a ZPICaudit poses the potential threat of a federal fraud investigation.
INSIDE THIS ISSUE
Reconciling Patient Payments
Across a Multi-Site
Physician Practice 4
ICD-10 Training for the Rest of Us 6
Coding for Complex Chronic
Care Coordination Services 7
Now You Can Earn CPEs …
with Your HFMA Newsletter
Subscription 7
Satisfaction with Physician
Revenue Cycle Functions 8
MORE ONLINE
Subscribers can access back issues as well
as web extra content at hfma.org/rcs
What Hospitals Need to Know AboutZPIC Audits By Gary Keilty and Kristen McDonald

2 October 2013 Revenue Cycle Strategist
agencies, such as the Office of InspectorGeneral (OIG), for further investigation.
A document request by a ZPIC shouldtrigger immediate involvement of aprovider’s in-house counsel, outsidecounsel, and compliance department. Tounderstand the unique and serious risksassociated with a ZPIC audit, providersshould be aware of ZPIC audit triggersand paths, action steps to take in theevent of a ZPIC audit, and strategies forchallenging ZPIC findings.
ZPIC Audit Triggers and Paths
ZPIC audits are typically not random.Rather, ZPICs conduct inquiries becausethey have identified a potential fraudconcern through various triggers.
Audit triggers. ZPICs often operate some-what in “the shadows,” by using providerpayment and utilization data collected byMACs, CMS, and private provider datacollection entities to identify possibleanomalies, such as high utilization of
certain services in relation to local andnational patterns, billing trends, andlengths of stay, among others. ZPICs alsoreview referrals of potential fraud fromsources like patient complaints (whethermade through the OIG’s hotline ordirectly to the ZPIC) and referrals fromother CMS program integrity contractors(such as RACs and MACs). In addition,ZPICs often consider general fraud alertsissued by CMS or the OIG as issues ripefor provider data analysis.
Audit paths. ZPICs may initiate pre-pay-ment or post-payment audits with littleor no notice to the provider. In bothtypes of audits, the ZPIC reviews a sampleof the provider’s patient record informa-tion. Once initiated, audits usually takethe following path:>Formal request for patient recordinformation>Interviews with beneficiaries andprovider employees>Review of patient record informationand determination of potential overpayments>Use of statistical sampling to extrapolatethe amount of an alleged overpaymentbased on an error rate within the sampled claims
>Referral of an extrapolated overpay-ment amount to the provider’s MAC forprocessing of a payment demand letter
A ZPIC may refer its findings to the OIGwithout the provider’s knowledge if theZPIC’s review supports the initial allegation of potential fraud.
Action Steps in the Event of an Audit
Due to the potential serious consequencesof a ZPIC inquiry, once providers becomeaware of a ZPIC inquiry, the followingaction steps are recommended:
Designate a point person.One person withinthe organization should be designated tocoordinate all responses to the ZPIC’srequests. Ideally, this individual shouldwork closely with legal counsel on allactions responsive to the ZPIC’s requests.This will help ensure a coordinated collec-tion effort, timely submission, and earlyinvolvement of legal counsel. It will alsoafford the provider the protection of theattorney-client privilege should potentialfraud issues be identified.
Conduct an independent data analysis.A prompt, independent data analysis ofrequested patient record information
Robert Fromberg Karen ThomasEditor-in-Chief Senior Editor
Amy D. LarsenProduction
Revenue Cycle Strategist is published 10 times a year bythe Healthcare Financial Management Association, ThreeWestbrook Corporate Center, Suite 600, Westchester, IL60154-5732
Presorted nonprofit postage paid in Palatine, IL 60067.©2013 Healthcare Financial Management Association.
Volume 10, Number 9
Subscriptions are $120 for HFMA members and $165 for other individuals and organizations. Subscribe online atwww.hfma.org/rcs or call 800-252-HFMA, ext 2.To order reprints, call 800-252-HFMA, ext. 384.
To submit an article, contact Karen Thomas at [email protected].
Revenue Cycle Strategist is indexed with Hospital andHealth Administration Index and the HealthSTAR database.
Material published in Revenue Cycle Strategist is providedsolely for the information and education of its readers. HFMA does not endorse the published material or warrant or guarantee its accuracy. The statements and opinions inRevenue Cycle Strategist articles and columns are those of the authors and not those of HFMA. References tocommercialmanufacturers, vendors, products, or servicesthat may appear in such articles or columns do not constitute endorsements by HFMA.
ISSN 1549-0858
A Guide to CMS Payment Review Program Contractors
MACs.Medicare Administrative Contractors (MACs) serve as providers’ primary point of
contact for enrollment and training on Medicare coverage, billing, and claims processing.
They also conduct pre-payment audits.
MICs.Medicaid Integrity Contractors (MICs) contract with CMS to conduct audit-related
activities for state Medicaid programs.
RACs.Medicare Recovery Audit Contractors (RACs) are charged with identifying improper
Medicare fee-for-service payments—both overpayments and underpayments. RACs are paid on a
contingency fee basis, receiving a percentage of the improper payments they identify and collect.
ZPICs.Zone Program Integrity Contractors (ZPICs) function as the “fraud detection” arm of the
MACs and are tasked with identifying cases of potential fraud that may result in large overpayments
and/or referral to other government agencies, such as the OIG, for further investigation.

will help determine data/document com-monality, time periods, trends, and thetype of patient and procedure involved,thereby shedding light on the focus of theZPIC’s review and identifying potentialliability. Once again, involvement ofcounsel is critical to maintain the attor-ney-client privilege as it relates to theindependent data analysis results.
Review the requested patient records. Anindependent review of the records canhelp determine a likely error rate, ifapplicable, and project the potentialoverpayment amount that may eventuallybe calculated by the ZPIC.
Ensure availability of information.Collect andprovide all available information to sup-port the appropriateness of the requestedpatient record or claim submitted for pay-ment. Unintentionally omitting certaininformation in record requests may resultin errors that affect extrapolated overpay-ment amounts or potentially strengthenthe allegation of fraud.
Open communication channels with theZPIC. Proactive outreach to the ZPIC,with involvement of legal counsel, maypromote open communication duringthe investigation and appeal process.
Protect repayments. If applicable, ensurethat any repayments, including extrapo-lated overpayments, related to a particu-lar audited claim and/or patient areprotected from additional overpaymentrequests in the event of a subsequentRAC audit.
Strategies for Challenging ZPIC Findings
Although options are limited once a ZPICinitiates an audit, time frames and attackstrategies are key elements to considerwhen challenging the ZPIC’s findings.
Mind the time. Pay close attention todeadlines and time frames. Immediately
calculate the deadline to submit anappeal because a missed deadline translates to a lost appeal right.Calendaring a response deadline is par-ticularly important for post-paymentreviews because there is a small windowof opportunity to stay any recoupmentduring the first two phases of the appealprocess (i.e., 30 days at the redetermina-tion phase and 60 days at the reconsider-ation phase). Be aware that interestcontinues to accrue throughout theappeal process, and recoupment cannotbe stayed at third and higher levels ofappeal.
Pre-payment reviews pose differentrisks because they can drastically andnegatively affect a provider’s paymentpipeline. It is advisable to develop con-tact persons associated with the con-tracting agencies to track the status ofpending appeals, especially if the con-tractors have not issued a decision within the regulatory 60-day require-ment. Be prepared for a long appealprocess for both types of reviews; eachlevel of appeal may take months, if notlonger, to conclude.
Consider all angles of attack.When appeal-ing, consider both procedural and sub-stantive attacks. Procedural attacks, forexample, may focus on whether the ZPIC provided sufficient informationabout the grounds for its decision, incompliance with the Medicare ProgramIntegrity Manual. Substantive attacks, onthe other hand, may focus on challengingextrapolation to a universe of claimsbeyond the original audited sample,refuting the clinical findings, and/orasserting legal arguments, including
those available under the Social SecurityAct, among others.
From the financial standpoint, focusingon methods to attack an extrapolationmay limit the provider’s liability to anactual overpayment, which is often amere fraction of the extrapolated over-payment.
To attack an extrapolation, considerengaging a statistical expert to analyzethe definition of the universe, the sampleselection method, and the statisticalaccuracy of the sample, among otherevaluations. Also consider whether thestatistical expert makes a good witness,because if an appeal reaches theAdministrative Law Judge (ALJ) level,ALJs often find credible, personablestatisticians to be very useful in analyzingan otherwise complicated issue.
The Importance of Preparation
To mitigate the potential financial andlegal consequences of a ZPIC audit,providers should familiarize themselveswith ZPIC audit triggers and paths, knowthe action steps to take in the event of anaudit, and be prepared to contest ZPICfindings in a strategic way. As healthcarecosts and reimbursement continue tocome under scrutiny in the years ahead,ZPIC and other types of payment reviewsare likely to increase.
Gary Keilty is managing director, Huron Consulting
Group, Washington D.C. (gkeilty@huronconsulting
group.com).
Kristen McDonald is a healthcare partner, Jones Day,
Atlanta ([email protected]).
hfma.org/rcs October 2013 3
Pre-payment reviews pose different risks because they can drastically and negatively affect a provider’s payment pipeline.

4 October 2013 Revenue Cycle Strategist
When an internal audit suggested thatbetter controls were needed for paymentscollected by physician offices associatedwith Jefferson University Physicians(JUP), a multi-specialty physician prac-tice consisting of the full-time faculty ofthe Medical College of Thomas JeffersonUniversity, the physician business serv-ices office built an automated process fordaily and monthly reconciliation of cash,credit card, and check deposits.
Built at minimal cost, using MicrosoftExcel® spreadsheets and standard bankreporting tools, the new process hasmade daily cash reconciliation part of thephysician network’s culture, and has vir-tually eliminated deposit discrepanciesacross the network of 650 physicians and61 practices.
Identifying the Issues
When the JUP management team evalu-ated their organization’s deposit proce-dures, they identified a number of areasfor improvement. Cash payments frompatients were not clearly identified in thebank deposit process, making it hard totrack cash collections by practice loca-tion. Reconciliation of bank deposits to alist of patient encounters in the patientaccounting system was inconsistent,resulting in deposit discrepancies and adifficult month-end cash reconciliationprocess. Research for internal auditsinvolved file cabinet searches for paperdocuments.
With some help from its bank partner,JUP outlined a project that would bring
about the needed business processimprovements:>Identify over-the-counter depositsfrom all sources by JUP practice ID.>Identify deposits by type (cash, check,or credit card).>Require daily and monthly reconcilia-tion of over-the-counter deposits by allpractices.>Make the daily reconciliation processeasy for practice business office staff.>Provide a central database of depositdata by practice, for use by the physi-cian business office during month-endreconciliations, for other purposessuch as practice collection trending,and for use by the internal auditdepartment when needed.
The first step was to uniquely identifyeach bank deposit. New deposit ticketswere ordered for the physician practices.Each set was encoded with a three-partlocation identifier containing the divi-sion number, the practice location num-ber, and a deposit ticket sequencenumber. Practices were required to makeseparate daily bank deposits for cash andchecks, allowing cash deposits to be iso-lated and tracked.
Improving the Credit Card Process
Increased security surrounding patientcredit card payments and the timing ofcredit card deposits makes reconciliationof these transactions difficult. With thebank’s help, the physician businessoffice implemented a process to collectpatient account numbers at the sametime as patient credit cards are
processed. Practice registration staffwere prompted to enter the patientaccount number into the credit card terminal when the credit card wasswiped. These data then appeared on areport accessible online by the physicianbusiness office, facilitating reconcilia-tion to the patient accounting system.
In addition, all credit card terminals atphysician offices were mapped to practicelocation numbers, using a custom tableon the bank’s platform. Deposits madefrom credit card terminals appeared onbank statements and the bank’s informa-tion reporting system with a referencenumber that began with the practice loca-tion number. As part of the credit cardsystem upgrade, terminals were set tosettle automatically and transmit adeposit total to the bank after the physi-cian offices had closed, ensuring thatdeposits would be processed every day,facilitating the end-of-month reconcilia-tion. Previously, physician business officestaff had been responsible for manuallysettling the terminals and initiating thecredit card deposit transmission.
Making Daily Cash Reconciliation Easy
As part of the new process, individualpractice office managers are required toreconcile the previous day’s bankdeposits to documentation of paymentsreceived for patient encounters on thatday (deposit “batch” information). Theyalso reconcile bank deposits to JUP’spatient accounting system at month end.
Physician Revenue Cycle By Dawne Clark and Margaret Dowling
After revamping how it manages patient payments, a multi-sitePhiladelphia physician practice is now identifying deposit discrepancies within 24 hours.
Reconciling Patient Payments Across aMulti-Site Physician Practice
WEB EXTRA
Revenue Cycle Strategist subscribers: view
a sample monthly posting report, practice
deposit report, standard code table for
reporting variances, and outstanding
variance report online at hfma.org/rcs.

hfma.org/rcs October 2013 5
Two new data fields—Deposit Ticket Cashand Deposit Ticket Check—were added toJUP’s patient accounting system to create“cash control totals” and help reconcilepatient payments posted to JUP’s patientaccounting system to daily deposit ticketamounts and to the actual deposit amountsposted to the JUP bank account. Daily rec-onciliation of deposit and posting activityhelps to identify any internal theft issuesand deposit discrepancies so they can beresearched before month-end.
The new reconciliation process had to beeasy, quick, and adaptable to employeeswith different skill sets. Rather thanover-engineering the process, JUP man-agement decided to keep things simple.
The new procedure works as follows:Each day, the practice business officemanager logs onto the bank reportingsystem to access the practice’s customreport. The manager matches the deposittotals from the bank report to JUP’spatient accounting system “batch”information from the previous day.Deposit discrepancies and deposit corrections (which carry the practice IDfrom the original deposit ticket and alsoappear on the practice bank report) mustbe researched and resolved, preferablyon the same business day. Deposit cor-rections, which typically indicate mis-counted cash, an addition error on adeposit ticket, or a missing check, arerequired to be reported by practice officemanagers to the physician business officeso they can be researched and correctedin the patient record. On most days, theentire process takes less than 15 minutes.
At month end, each practice is responsiblefor completing a month-end reconciliationcomparing all JUP’s patient accountingsystem over-the-counter payments to themonth’s bank deposits for the practice.Variances are reported to the physicianbusiness office using a standard code table.
To maintain controls at the “macro”level, a physician business office staffmember downloads practice deposit datafor the entire JUP system from the bank,using a spreadsheet template written toautomate the reconciliation process.Over-the-counter payment informationfrom JUP’s patient accounting system iscompared to the bank information, andbank and patient accounting systemreports are prepared by the physicianbusiness office and distributed to practice office managers.
A “top level” physician business officereconciliation is also performed to mon-itor the accuracy of the practice level reconciliations. Standard reports used in the reconciliation process include:>Deposit correction form used to correctdeposit or posting errors detected during the reconciliation process>Monthly deposit correction summaryreport>Variance reports produced by a variancedatabase that is used to track and reportoutstanding issues that are carried fromone month to the next
Supporting the System Through Training
To support the transition to the new sys-tem, JUP offered classroom and hands-ontraining at the practices during roll-out.Training included presentations to physi-cians so they would be aware of the newprocess and would support their businessoffice managers in making the change.Presentations included a statement ofthe reasons for making the change, theadvantages to the practices, and clarityaround expectations. Training on thereconciliation system is now incorpo-rated into the orientation program fornew practice business office managers.
Achieving Results
The project has achieved all the resultsthat JUP anticipated, plus a few unexpectedbenefits:
>Daily reconciliation of physiciandeposits has become part of the JUPculture.>Deposit discrepancies are identifiedwithin 24 hours of the deposit and areclearly identified by practice.>Controls for cash deposits have beenstrengthened: Since the new reconcili-ation system was implemented, JUP has experienced no incidences of missing cash. >Deposit discrepancies carried overbetween accounting periods have virtually been eliminated.>Month-end reconciliations have beenaccelerated: Reconciliations arerequired to be completed within 10 days of report distribution. >The new reconciliation process hasreceived positive recognition from theJUP internal audit department.
One unexpected result was that creditcard receipts increased dramatically during the first year of the project. Theincrease in collections may be due to theauto-settlement of credit card terminalsand the improved reconciliation process,which make accepting credit card pay-ments easier for the physician practicestaff.
The project’s success is attributed to acombination of simple tools, commit-ment to the reconciliation process, andtraining for physician office employees.
Dawne Clark is manager of lockbox, payments, and
reconciliation for physician business services, Thomas
Jefferson University, Jefferson University Physicians,
Philadelphia ([email protected])
Margaret Dowling is senior vice president, product
management, PNC Healthcare, Philadelphia

6 October 2013 Revenue Cycle Strategist
Inpatient coders will be a hospital’s resident ICD-10 experts so they need the “soup to nuts” training, includinganatomy and terminology/physiology,ICD-10 CM, and ICD-10 PCS.
Following are suggestions for ICD-10training that is suitable for other groupsor departments in hospitals and healthsystems.
Outpatient coders. Ideally, outpatientcoders, including those coding forambulatory surgery, the emergencydepartment, and ancillary departments,would receive the same package of train-ing that inpatient coders do. However, ifthere is no intention of cross-training orif budget constraints are an issue, focuson anatomy and terminology/physiology
and ICD-10 CM training. ICD-10 PCScodes, which are the most difficult partof any ICD-10 training, will not berequired on outpatient claims.
Physicians and other documenters.Physicians, physician assistants, woundcare nurses, case managers, and otherswho document in patient records have an impact on code assignment. The solefocus of ICD-10 training for these indi-viduals should be on documentation.Whenever possible, make the trainingservice- or specialty-specific to keep itrelevant and reduce training time (andthe boredom factor). Don’t worry aboutteaching documenters how to code.Concentrate on improving their documentation skills so coders canassign codes accurately.
Patient access/registration/finance/billing.Although staff in these departmentsdon’t assign codes or document in thepatient record, they deal with codes on adaily basis. Their training should focuson the impact and code structure of ICD-10. Furthermore, they should have sometraining on the General EquivalenceMappings (or at least have a copy of theGEMs book), so they can follow a codefrom ICD-9 to ICD-10 and vice versa toget a sense of how they differ.
Administration.An overview of the impli-cations of ICD-10 will help administratorsunderstand how this new code set willhave an impact on their entire facility.
Clinical documentation improvement (CDI)staff.Organizations with very robust CDIprograms may want to give CDI staff thesame training as inpatient coders, as CDIstaff are on the front lines and havebecome very well-versed in ICD-9 codes.In other CDI departments, the training
that physicians and other documentersreceive might suffice. CDI staff are theback-up support who will ensure physi-cians are documenting what they should.They could be game-changers with ICD-10 and may help prevent the onslaught ofpost-discharge querying that is antici-pated with ICD-10 implementation.
Other departments.Find out what internal/external software systems use ICD-9 codes.GEMs training may be helpful to make themaware of how the code sets differ.
Kim Felix, RHIA, CCS, is director of education,
coding division, IOD Incorporated, Philadelphia,
and a member of HFMA’s Metropolitan Philadelphia
Chapter ([email protected]).
ICD-10
ICD-10 Training for the Rest of Us
By Kim Felix
Beyond inpatient coders, who else in a hospital or health system needs ICD-10 training? And what type of training does each department need?
Don’t worry about teachingdocumenters how to code.Concentrate on improvingtheir documentation skills so coders can assign codesaccurately.
MAP Award for HighPerformance ApplicationOpens October 30
HFMA’s MAP Award for High Performance
in Revenue Cycle recognizes healthcare
organizations that excel at meeting revenue
cycle benchmarks and implementing patient-
friendly billing practices to achieve outstanding
patient satisfaction. Winners will share
proven revenue cycle strategies at ANI 2014.
Application Opens: Oct. 30, 2013
Deadline: Feb. 28, 2014
Learn more at hfma.org/mapawards.

hfma.org/rcs October 2013 7
Q. What documentation is required for
complex chronic care coordination?
A.New CPT codes 99487-99489 for complex
chronic care coordination (CCCC) are not yet
separately reimbursable by Medicare; however,
some commercial payers do reimburse these
codes separately. If all providers capture the
codes and track payment, that would help gain
recognition and promote broader reimburse-
ment by Medicare and other payers. Codes and
their definitions are shown in the exhibit.
Documentation is key to payment. CCCC services
by the clinical staff must be captured for the
entire month. To justify the minutes reported,
all time spent should be captured, including date,
minutes spent, what was done, and who
provided the service, so that the total time
can be accurately reported.
Jennifer Swindle, RHIT, CCS-P, CPC, CPMA, CDIT,
is vice president, coding, Salud Healthcare Solutions,
LLC, Lafayette, Ind., ([email protected])
and a member of HFMA’s Indiana Pressler Memorial
Chapter.
Access the Coding Q&A archives at hfma.org/rcs.
Send your coding questions to Karen Thomas at
Coding Q&A By Jennifer Swindle
Now You Can Earn CPEs … with Your HFMA Newsletter Subscription
Coming in October: Revenue Cycle Strategist subscribers will be able to
access self-study lessons via the HFMA website to earn CPEs and certifi-
cation maintenance points. The Newsletter Self-Study Program is the per-
fect way to learn at your own pace with the flexibility to access the lessons
any time or any place. To earn a CPE, just read a CPE-eligible article,
go over the review sections, and complete a six-question final exam.
Access the First Lessons
Look for an email from HFMA in October that will link you to the following
two self-study lessons—both free to Revenue Cycle Strategist subscribers.
Developing a Charity Care Approach.Read a Revenue Cycle Strategist case
study about North Shore-Long Island Jewish Health’s multipronged
approach to charity care. You will also go over Statement 15. Developed
by HFMA’s Principles & Practices Boards, this statement gives specific
criteria and guidelines for identifying patients for charity care.
> CPE credits: 1.0
> Designed for: Revenue cycle leaders, financial counselors, and other
healthcare finance leaders interested in charity care issues
> Level: Intermediate
> Prerequisite knowledge: Basic understanding of revenue cycle billing
and operations
> NASBA field of study: Specialized knowledge and applications
Strategies for Retaining & Advancing Revenue Cycle Staff.Read a Revenue
Cycle Strategist case study about Baylor’s talent planning process, which
has reduced turnover by 4 percent over a 10-year period. You will also
read a case study about Metro Health System’s revenue cycle training
and career ladders programs, which have produced dramatic results.
> CPE credits: 1.0
> Designed for: Revenue cycle leaders and other healthcare finance
leaders interested in employee development and retention
> Level: Beginner
> NASBA Field of Study: Personnel/HR
Other newsletter self-study lessons will be posted on a quarterly basis for
Revenue Cycle Strategist subscribers to access for free—with the potential
to earn 4 CPE credits per year.
Subscribe to More Newsletters
Subscribe to all three HFMA newsletters, and you’ll be able to access up
to 12 newsletter self-study articles per year (1 CPE per article):
> Healthcare Cost Containment─Showcases provider-tested strategiesand expert advice on how to take cost control to the next level.
> Revenue Cycle Strategist─Contains expert insights and how-to actions thathelp healthcare organizations achieve and maintain peak revenue cycle.
> Strategic Financial Planning─Presents expert insights and peer-testedpractices related to planning and financing strategic, capital, and service
line projects.
Subscribe today at hfma.org/newsletters
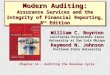
Coding for Complex Chronic CareCoordination Services Complex Chronic Care
Coordination Codes
Code Definition
99487 First hour of clinical staff time, directed by the physician, with no face-to-face encounter; per calendar month
99488 First hour of clinical staff time, directed by the physician, with one face-to-face encounter; per calendar month
99489 Each additional 30 minutes of clinical staff time, directed by the physician in a calendar month; report in addition to the initial service

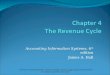
Hospital and health system CFOs and VPs of
finance report a higher level of satisfaction with
several physician group processes that report
into the hospital, compared with those that
report to the physician practice. In an HFMA
survey of 139 healthcare finance leaders,
38 percent indicated they were "completely
satisfied" with physician billing performance with
hospital/system-based oversight, while 13 percent
reported the same level of satisfaction with
practice-based oversight. Executive satisfaction
was also higher for hospital/system-based over-
sight of physician collections and physician
coding and documentation, as shown in the
exhibit. However, satisfaction with patient
registration in physician offices (which is less
likely to report to the hospital/system), was
higher for practice oversight.
Three Westbrook Corporate CenterSuite 600Westchester, IL 60154-5732
PRESORTEDNONPROFITU.S. POSTAGE
PAIDPERMIT NO. 73PALATINE, IL
To subscribe, call 800-252-HFMA,ext. 2. Or visit hfma.org/rcs
Figures at a Glance
Satisfaction with Physician Revenue Cycle Functions
Source: “Executive Survey on Hospital and Physician Affiliation Strategies, Sponsored by McKesson.” HFMA, April 2013.
Sponsored by
www.parallon.net
38%
24%
20%
13% 13% 10%
4%
20%
Physician billing Physician collections Physician coding/documentation
Physician patient registration
Hospital/ System Group Practice Oversight by: