Embed Size (px)
Citation preview

Revascularization in Stable Disease: Should Hierarchy of Noninvasive Tests Change?
Mt Sinai SymposiumOctober 2019
Athena Poppas, MD, FACC FASE
Vice-President, American College of Cardiology
Professor of Medicine, Brown University Medical School
Chief, Cardiology Division
Director, Lifespan Cardiovascular Institute
Rhode Island, Miriam and Newport Hospitals
Disclosures: NONE

Noninvasive Testing Options
Stress ECG
Stress echo
Stress SPECT
CT
CMR
PET

Revascularization in Stable Ischemic Heart Disease: No improvement in survival
• Large RCT, with angiographic CAD as measure:• Revascularization equivalent to optimal medical therapy
in reducing MACE or improving survival• BARI2D, NEJM 2009
• Courage trial, NEJM 2007
• Recent trials in FFR suggest better guidance for PCI vs OMT• FAME, NEJM 2009, DeBruyne FAME2. NEJM 2012.
• NIH/NHLBI ISCHEMIA, • International Study of Comparative Health Effectiveness With
Medical and Invasive Approaches

Revascularization in Stable Disease: Should Hierarchy of Noninvasive Tests change?
•Why: • atherosclerosis• test performance
•What:• Symptoms • Revascularization versus medical treatment
•How:• Current Stress Testing Algorithms• Supportive research
• Knowledge Gaps • Future directions
•Help me know what to do in the office tomorrow!

Evolution of atheroscleous
plaque

SPECT , PET/CT
MBF
PET CT
Endotelial Dysfunction
Aterosclerosis Symptoms & Prognostication
Imaging Modalities for Coronary Artery Disease

Functional versus Anatomic Testing?
•Establish the diagnosis of obstructive CAD?• Either anatomic or functional
•Revascularization decision-making?• Both anatomy and function

European Heart Journal, ehz425, https://doi.org/10.1093/eurheartj/ehz425
Initial diagnostic management of symptomatic
patients with suspected CAD

2014 ACC/AHA: SIHD Guideline Update
• A standard exercise test is the first choice to diagnose IHD for patients
with an interpretable ECG and able to exercise, especially if the
likelihood is intermediate (10-90%).
• Those who have an uninterpretable ECG and can exercise, should undergo
exercise stress test with nuclear MPI or echocardiography, particularly if
likelihood of IHD is >10%. If unable to exercise, MPI or echocardiography with
pharmacologic stress is recommended.
• Patients diagnosed with SIHD should undergo assessment of risk for
death or complications.
• Those who have an uninterpretable ECG and are able to exercise, should
undergo an exercise stress with nuclear MPI or echocardiography, while for
patients unable to exercise, nuclear MPI or echocardiography with pharmacologic
stress is recommended.
• Coronary arteriography should be considered for patients with SIHD
whose clinical characteristics and results of noninvasive testing indicate
a high likelihood of severe IHD and benefits are deemed to exceed risk

2014 ACC/AHA Algorithm for Risk
Assessment of Patients With SIHD
*Colors correspond to the ACCF/AHA Classification of Recommendations and LOE

European Heart Journal, ehz425, https://doi.org/10.1093/eurheartj/ehz425
Diagnostic pathways in symptomatic
patients with suspected CAD

Considerations in test choice
• The choice of the stress test depends on:
• Patient level of function • ECG• Local availability and expertise• Patient's body habitus • Need for concomitant assessment of hemodynamics or
valvular disease• Cost
• Radiation exposure• Patient choice• Patient’s pre-test probability

Case History
45 year old women smoker with left-sided, sharp chest pain
PE: BP 152/88 HR 80ECG: Sinus, ST flattening LABS: LDL 170, HDL 38
What is the pretest probability of CAD?a. 5%b. 20%c. 40%d. 80%

Pretest Likelihood of CAD:Low versus high risk patients
Age M W M W M W
35 3-35 1-19 8-59 2-39 30-88 10-78
45 9-47 2-22 21-70 5-43 51-92 20-79
55 23-59 4-25 45-79 10-47 80-95 38-82
65 49-69 9-29 71-86 20-51 93-97 56-84
High risk= tob, lipids, HTN w/ nml ECG Duke Database. JACC 2012;60(24)
Noncardiac CP Atypical CP Typical CP

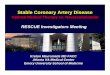
Pre-test probabilities of coronary artery disease
15 815 symptomatic patients according to age, sex, and symptoms in a pooled analysisJuarez-Orozco. Eur Heart J Cardiovasc Imaging. 2019. and ESC Guidelines

Stress Echocardiogram: Results
• Exercised 7:34 minutes on Bruce protocol
• Peak HR=158 BPM, peak BP=160/80
• Symptoms: leg fatigue, typical chest pain
• results:

Peak Stress ECG

Stress Echocardiogram


Cardiac Catheterization-80% LAD

Stress tests are good at detecting CAD in patients at intermediate likelihood
Imaging stress tests are good at guiding invasive treatment

Bayes’ Theorem: test intermediate risk
Patterson and Horowitz
J Am Coll Cardiol
1989;13:1653.

Stress testing
• Methodology
• Accuracy
• Prognosis

Functional Testing:Exercise adds incremental information
•Elicit clinical symptoms
•Functional status
•Provide prognostic information

Exercise capacity and survival
Myers et al. N Engl J Med 346: 793, 2002

Heart rate response and survival
Lauer et al. Circulation 93: 1520, 1996

Noninvasive Testing Options
Stress ECG
Stress echo
Stress SPECT
CT
CMR
PET

How Good is Stress Testing
• Methodology
• Accuracy
• Prognosis
Likelihood ratios: measure of diagnostic accuracy

Stress Tests: Methodology
From Armstrong Prog In Cardiovasc Dis 1997;39:499.

Sensitivity and Specificity
• Derived from comparison to angiography (>50% LM or 70% LAD/LCx/RCA luminal diameter occlusion)
• Sensitivity (61%-73%)
• Specificity (59-81%)
• True value of exercise ECG stress test is its specificity

Likelihood ratios: Test result changes probability that CAD exists
European Heart Journal, Volume 39, Issue 35, 14 September 2018, Pages 3322–3330

28,664 patients from 132 studiesEuropean Heart Journal, Volume 39, Issue 35, 14 September 2018, Pages 3322–3330,
Non-invasive tests to rule in/out obstructive coronary artery disease

Stress testing
• Methodology
• Accuracy
• Prognosis

Exercise Stress EchocardiographyPredictive of Prognosis
• 5798 patients • age 62 ±12 years
• History of prior PTCA/CABG/MI• Men=56% Women=22%
• MVA predictors of events:• Exercise WMSI
• Workload <6METS
• Arruda-Olsen AM. JACC 2002;39:625.
• 7236 outpatients • age 54 ±12 years
• History of CAD, 10%• Positive tests: 18%
• Normal test: annual event rate equivalent to age/sex matched populations
• Fine NM. Mayo Clin Proc 2013;88(12):1408

Cardiac SPECT: Prognostic Value
Hachamovitch Circ 1998 Medical Therapy Cath Revascularization
Increasing Ischemia

SPECT vs. PET
SPECT
• Widely available
• Exercise studies
• Tc-99m labeled tracers
• Inconsistent AC
• Long(er) study protocols
• Higher radiation exposure
• Lower resolution
• No CFR quantification
PET
• Limited access
• Only pharmacologic studies
• Cyclotron/generator produced
• AC for all studies
• Short protocols
• Lower radiation exposure
• Higher resolution
• Quantification of CFR

Tc-99m tetrofosmin Rb-82
57-yomwith exertional chest pain, hypertension, dyslipidemia, diabetes mellitus,obese
((BMI): 40.1 kg/m2)

Risk reclassification with PET CFR
Murthy et al. Circulation 124: 2215, 2011

16,029 consecutive patients with Rubidium-82 rest-stress PET MPI
PET: Prognostic Value

Case example: stress MRI
• 65 y/o woman with h/o HTN admitted for CP
• Troponin: <0.04 x 3
• ECG normal
• TTE: Normal LV size &function, LVH, no WMA’s, (+) MVP

Function

Perfusion Imaging
STR
ESS
RES
T

Stress CMR: good at diagnosing/localizing CAD
CMR & CAD: high sensitivity (>90%) and specificity (>80%)

MRI vasodilating stress perfusion study
A negative Stress CMR confers very low annualized event rate (0.6 to 1.5%)

Net Reclassification Index (NRI) of CAD Risk (N=792)
Shay RV, Heydari B, Abbasi SA, et al. Circulation. 2013 Aug 6;128(6):605-14.

What is the added value of functional testing?
vs.

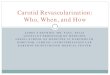
SPECT imaging predicts cardiac events
0.0
0.5
1.0
1.5
2.0
2.5
3.0
3.5
4.0
4.5
Normal Mildly abnormal Moderately abnormal
Severely abnormal
An
nu
al
even
t r
ate (
%)
Cardiac death
MI
Hachamovich et al. Circulation 1998; 97: 535

PROMISE study: Functional vs. Anatomic tests
• RCT with 10K patients enrolled in either CTA or functional testing arms• 67.3% of functional testing was nuclear stress testing
• CTA associated with lower rates of angiography overall• More angiography performed in first 90 days following CTA
• Conclusion: coronary CTA is an alternative to functional stress testing among low- to intermediate-risk patients with chest pain.

PROMISEPrimary Endpoint (death, MI, UA, MACE)
Douglas et al. N Engl J Med 372: 1291, 2015

Functional testing to rule in CADAnatomic testing to rule out
vs.

Knowledge Gaps:
• Medical versus interventional therapy?• COURAGE, BARI 2D• AHA 2019: NIH/NHLBI ISCHEMIA
• International Study of Comparative Health Effectiveness With Medical and Invasive Approaches
• Imaging Comparative Effectiveness • Limited RCT in this area
• Application and generalizability:• Local expertise• Health care costs in value-based/ACO models

Revascularization in Stable Disease: Hierarchy of Noninvasive Tests SHOULD change
•Why: • Asymmetric progression of atherosclerosis• Imaging of different disease states
•What:• Symptoms?: functional or anatomic testing• Revascularization? versus medical treatment: both
•How:• Current Algorithms:
• CCTA lower risk (R/O) and imaging higher risk (R/I)
• Knowledge Gaps • ISCHEMIA trial, comparative effectiveness/cost
• Please, just tell me what to do in the office tomorrow!

European Heart Journal, ehz425, https://doi.org/10.1093/eurheartj/ehz425
Diagnostic management of symptomatic
patients with suspected CAD

Thank you for your attention!
Brown University Cardiology Faculty and Fellows


European Heart Journal, ehz425, https://doi.org/10.1093/eurheartj/ehz425
Diagnostic pathways in symptomatic
patients with suspected CAD

Extra slides

Stress testing
• Why: symptomatic
• How: Methodology
• Which imaging modality

ROMICAT-II
• More downstream testing and higher radiation exposure with CT
• Similar cost ($4,289 [CT] vs. $4,060 [Standard])
Hoffmann et al. N Engl J Med 2012; 367: 299

Pre-operative Evaluation

Pre-operative Evaluation

Pre-operative Evaluation

Exercise Stress TestingIndications
Class I
• Diagnosis of coronary artery disease in intermediate risk patients
• Prognosis and/or assessment of functional capacity in patients with known heart disease
• Early or predischarge MI risk/therapy assessment
• Assessment of risk/therapy in CHF patients (CPT)
• Dyspnea (CPT)
• Recurrent symptoms after revascularization
• Establish pacemaker settings in patients with rate responsive pacemakers

Exercise Stress TestingIndications
Class IIA
• Diagnosis of vasospastic angina
• Post-coronary revascularization exercise therapy
• Evaluate exercise capacity if patient is unreliable (CPT)
• Evaluate exercise-induced cardiac arrhythmias

Exercise Stress TestingIndications
Class IIB
• Diagnosis of CAD in adults with low or high pretest risk
• Periodic prognostic assessment in patients with stable CAD
• Post-MI assessments in patients with catheterization
• Determine exercise training intensity

Exercise Stress TestingIndications
Class III (NO benefit, potential harm)
• Prognostic risk already established by catheterization
• Severe comorbidity limiting life expectancy
• Routine use to evaluate exercise capacity
• Screening of asymptomatic subjects
• Routine assessment of asymptomatic patients after coronary revascularization