Embed Size (px)
Citation preview


PROGRAM PENGENDALIAN RESISTENSI ANTIMIKROBA DI RUMAH
SAKITHARI PARATON. dr. SpOGK
KOMITE PENGENDALIAN RESISTENSI ANTIMIKROBA KOMITE PENGENDALIAN RESISTENSI ANTIMIKROBA

AMR & RUMAH SAKIT?
• AMR banyak di Rumah sakit (ICU, ICCU, NICU, PICU, Int. Care, Rawatinap. Infeksi)
• Antibiotik sistemik banyakdigunakan di RS
• HAI prevalensi meningkat• Staff medis RS perlu pemahaman• 50-80% Antibiotik digunakan tidak
tepat.

4
Kategori
Hasil
Sby (%)
Semg(%)
Tidak ada indikasi terapi
76 53
Tidak ada indikasi
profilaksis55 81
4AMRIN STUDY : 2002-2005
PENGGUNAAN ANTIBIOTIK DI RUMAH
SAKIT

THE PROBLEM
• Blood stream• Pneumonia• UTI• SSI
ANTIBIOTIC USE
• more difficult to treat• more procedures• high cost• ICU use• failure morbidity and mortality
AMRHAI
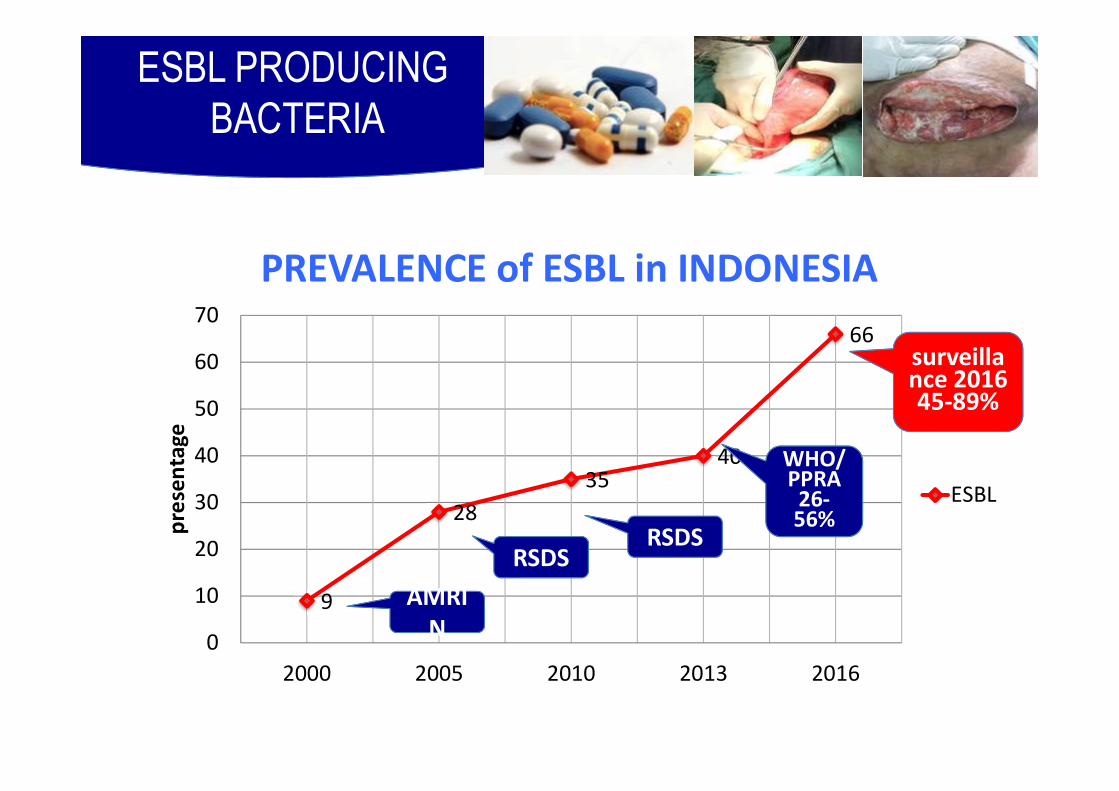
PREVALENCE of ESBL in INDONESIA
ESBL PRODUCINGBACTERIA
9
2835
40
66
0
10
20
30
40
50
60
70
2000 2005 2010 2013 2016
pres
enta
ge
ESBL
AMRIN
AMRIN
RSDSRSDS
WHO/WHO/PPRA
26-56%
surveillance 201645-89%

Table. Antibiotic susceptibility (n) pattern of ESBL producing E.coli
7
RSDS RSSA RSDM RSDK RSSD RSP TOTALCefotaxime 0.17 0.00 NA 1.57 3.31 NA 0,78Ceftriaxone 0.00 0.00 2.62 5.93 NA 0.00 1,19Ceftazidime 0.17 0.00 12.07 4.19 8.33 0.00 3,83Cefepime 0.34 42.06 26.21 9.42 25.62 0.00 12,78Ciprofloxasin 16.10 29.37 10.00 18.32 7.50 10.42 15,21Amikacin 97.95 95.24 82.99 96.34 73.33 98.96 92,4Gentamycin 61.43 69.05 62.15 10.99 56.30 63.54 55,12Fosfomycin 92.86 100.00 NA 78.57 82.89 NA 90,85Piperacillin-tazobactam
49.57 76.19 NA 76.44 65.81 66.67 60,4
Cefoperazone-sulbactam
53.85 NA 83.33 72.73 57.98 15.63 57,08
Meropenem 99.83 98.41 98.96 95.29 94.96 100.00 98,51Levofloxacin 20.14 29.37 9.00 21.48 15.38 10.42 17,66Tigecyclin 78.08 99.21 97.92 99.48 40.63 100.00 94,67
Data surveillance PPRA RSDS-Balitbangkes-WHO 2013

GLOBAL AMR
KOMITE PENGENDALIAN RESISTENSI ANTIMIKROBA KEMENTERIAN KESEHATAN

When I was asked to chair the Review on Antimicrobial Resistance (AMR), I was
told that AMR was one of the biggest health threats that mankind faces now
and in the coming decades. My initial response was to ask, ‘Why should an
economist lead this? Why not a health economist?’ The answer was that many of
the urgent problems are economic, so we need an economist, especially one versed
in macro-economic issues and the world economy, to create the solutions.
PENDAHULUAN

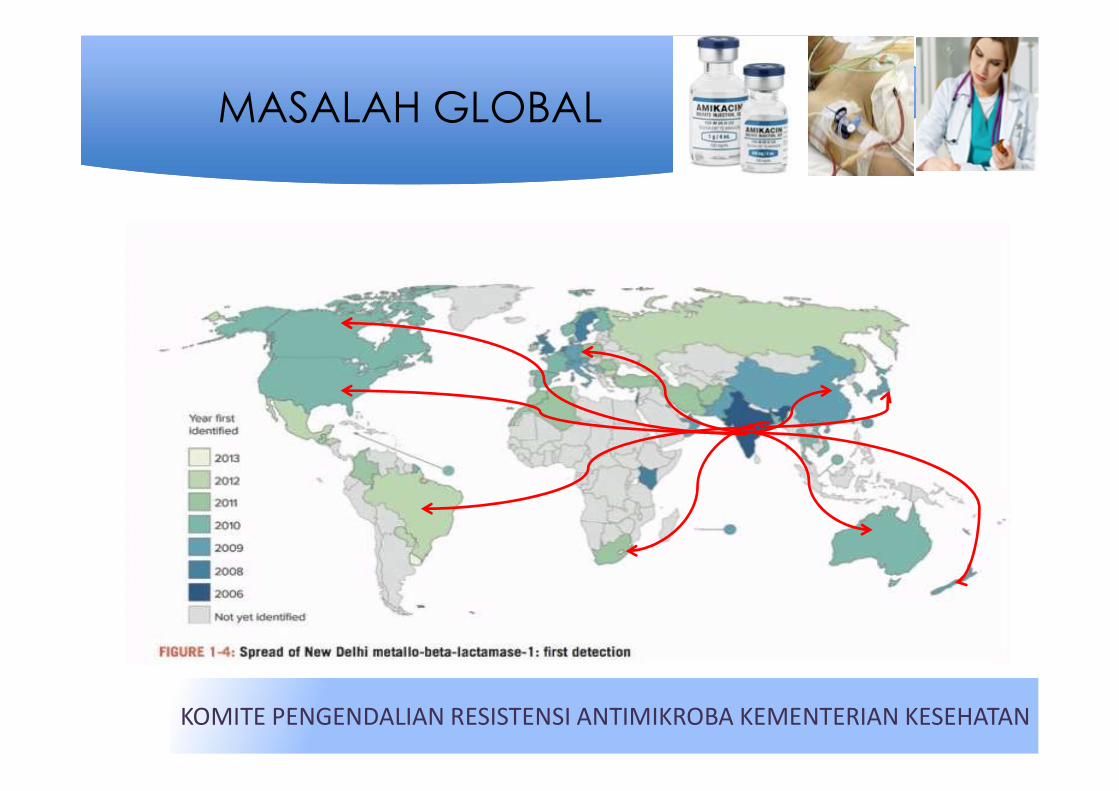
MASALAH GLOBAL
KOMITE PENGENDALIAN RESISTENSI ANTIMIKROBA KEMENTERIAN KESEHATAN

THE AMR IMPACTS

MASALAH GLOBAL
KOMITE PENGENDALIAN RESISTENSI ANTIMIKROBA KEMENTERIAN KESEHATAN
WHO 2013
700.000 / tahun
10.000.000/tahunUSD. 100 TRILLIUN
(Jim O Neill 2015)
2050
2013
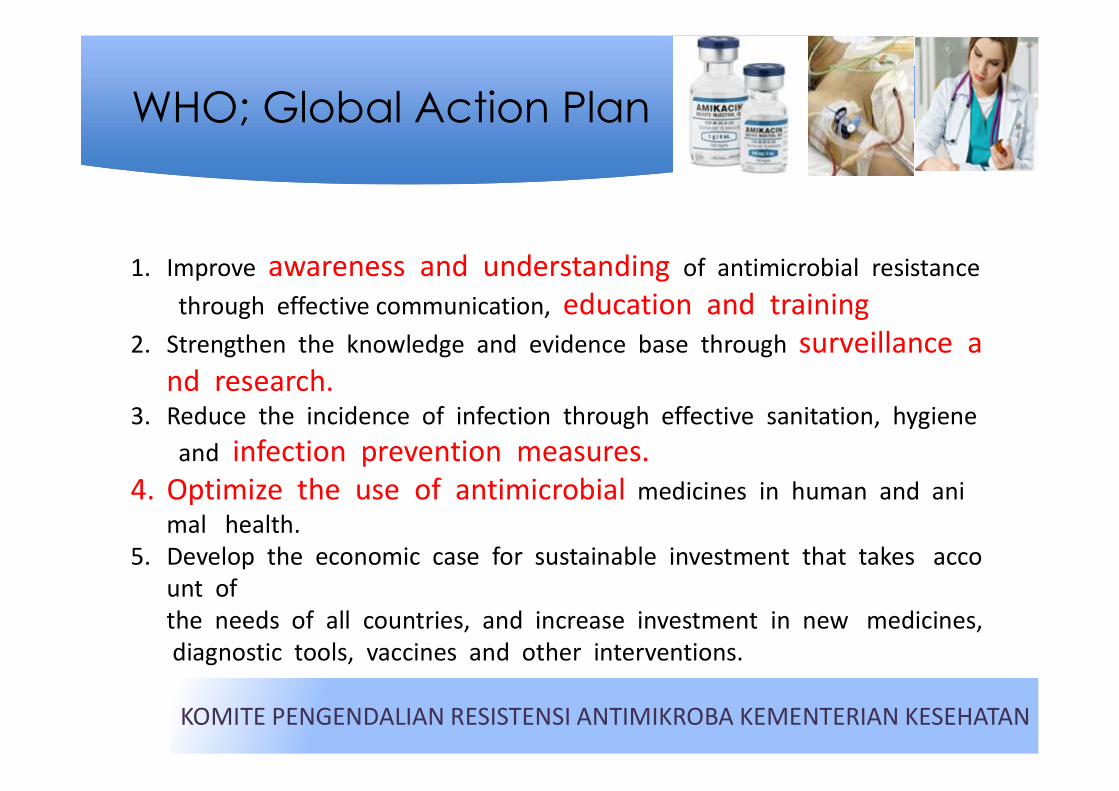
WHO; Global Action Plan
KOMITE PENGENDALIAN RESISTENSI ANTIMIKROBA KEMENTERIAN KESEHATAN
1. Improve awareness and understanding of antimicrobial resistance through effective communication, education and training
2. Strengthen the knowledge and evidence base through surveillance and research.
3. Reduce the incidence of infection through effective sanitation, hygiene and infection prevention measures.
4. Optimize the use of antimicrobial medicines in human and animal health.
5. Develop the economic case for sustainable investment that takes account of the needs of all countries, and increase investment in new medicines, diagnostic tools, vaccines and other interventions.
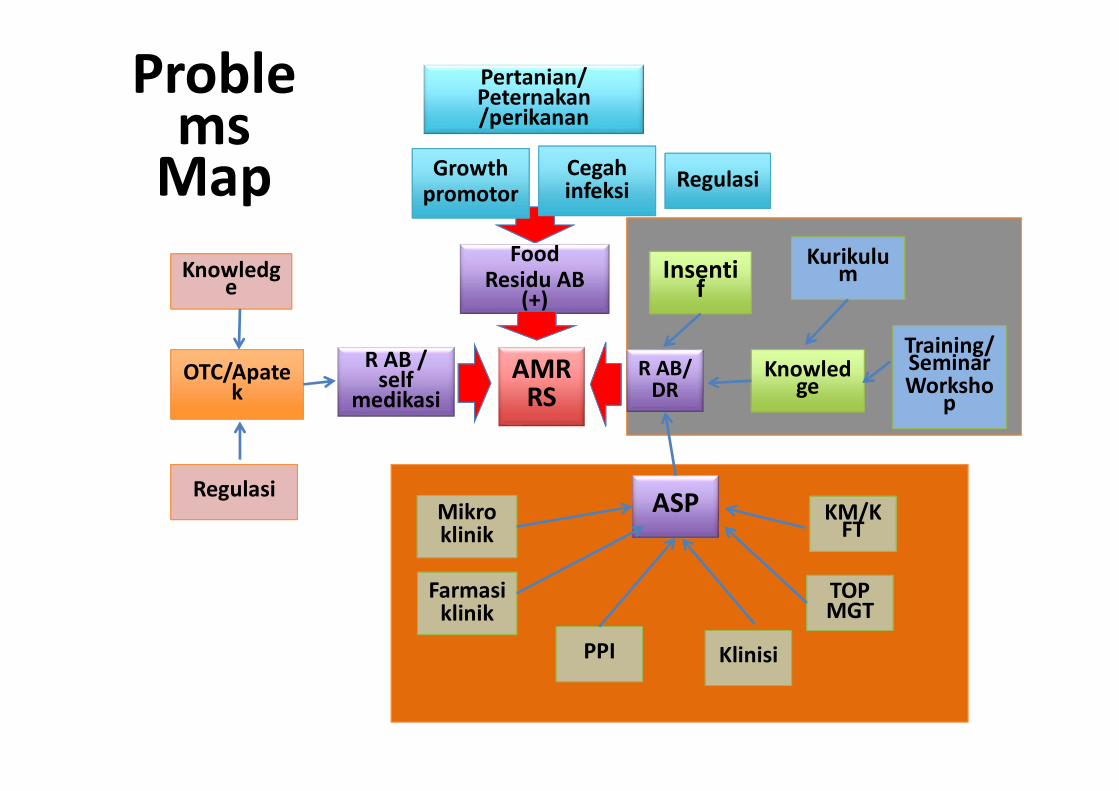
Problems
Map
AMRRS
R AB/ DR
R AB / self
medikasi
FoodResidu AB
(+)
OTC/Apatek
Growthpromotor
Pertanian/ Peternakan/perikanan
Cegahinfeksi
Insentif
Knowledge
Mikroklinik
ASP
Farmasiklinik
TOP TOP MGT
KM/KFT
Kurikulum
Training/SeminarWorksho
p
Regulasi
Knowledge
Regulasi
KlinisiPPI
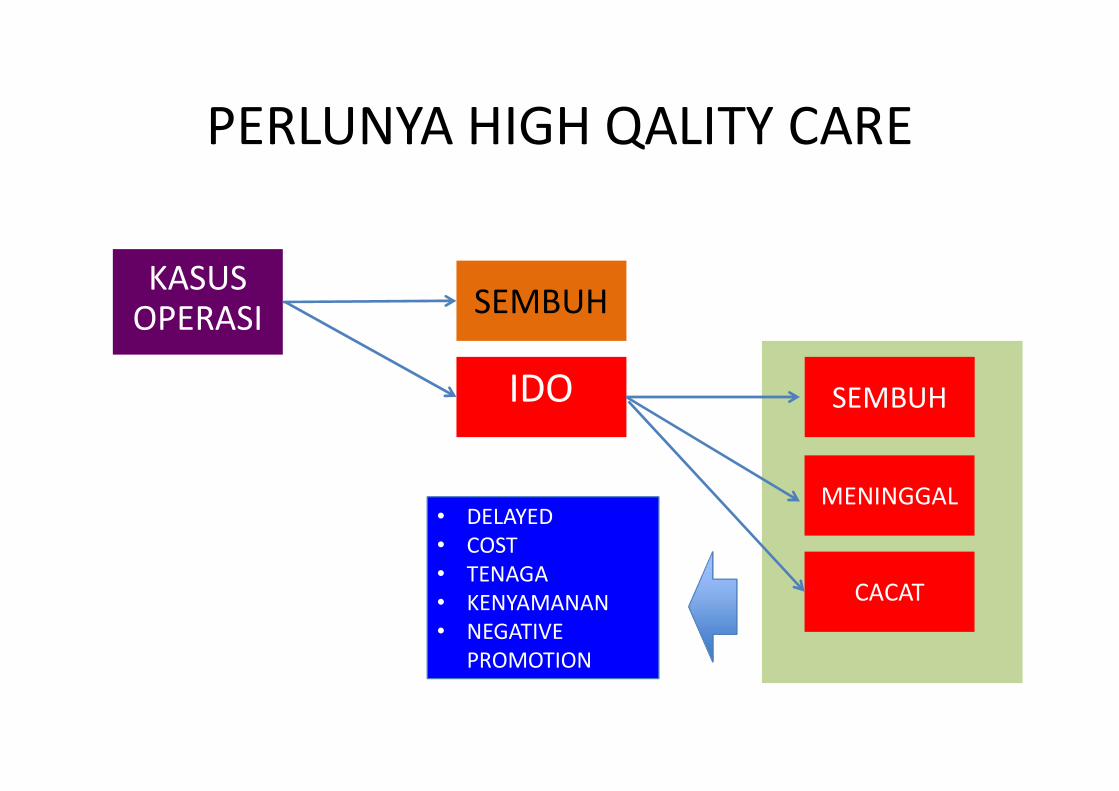
PERLUNYA HIGH QALITY CARE
KASUSOPERASI SEMBUH
IDO SEMBUH
MENINGGAL
CACAT
• DELAYED • COST • TENAGA• KENYAMANAN• NEGATIVE
PROMOTION


HEALTH RESOURCES IN INDONESIA 2016
Profesion total
Specialist 32.280
GP 116.900
Dentist 31.360
Midwife 400.000
Nurse 288.000
Pharmacist 54.900.18
Facilities total
Hospital 2.415
Health center 9.600
Drug store 24.000
Medical Faculty 73
Dentistry Faculty 27
PharmaceuticalFaculty
127
Midwife Academy 720
Nurse academy 300

REGULASI SEBAGAI LANDASAN HUKUM
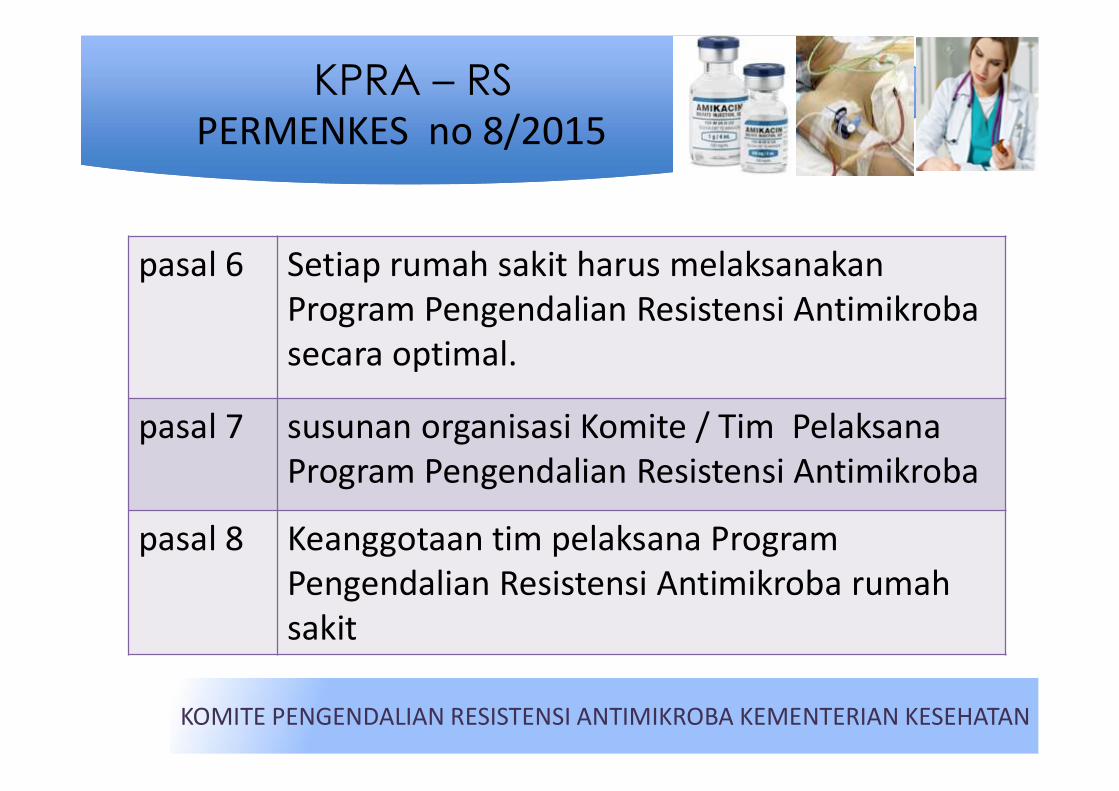
KPRA – RSPERMENKES no 8/2015
KOMITE PENGENDALIAN RESISTENSI ANTIMIKROBA KEMENTERIAN KESEHATAN
pasal 6 Setiap rumah sakit harus melaksanakanProgram Pengendalian Resistensi Antimikrobasecara optimal.
pasal 7 susunan organisasi Komite / Tim PelaksanaProgram Pengendalian Resistensi Antimikroba
pasal 8 Keanggotaan tim pelaksana Program Pengendalian Resistensi Antimikroba rumahsakit

PARADIGMA MENGATASI BAKTERI RESISTEN
CegahTransmisi
AMR
CegahTransmisi
AMR
TemukanANTIBIOTIK
baru
TemukanANTIBIOTIK
baru
Host defence
/Immunitas
Host defence
/Immunitas
Menggunakan normal
flora
Menggunakan normal
flora
CegahResistensi
CegahResistensi
AntibiotikBijak
AntibiotikBijak
ASPASP
PPI/Universal precaution
PPI/Universal precaution
Cuci TanganCuci Tangan
Lama, Cost tinggi, SulitLama, Cost tinggi, Sulit
Save Normal
Flora
Save Normal
FloraASP,
LimitasiAntiseptik
ASP, Limitasi
Antiseptik
Pro-Pre biotik
Pro-Pre biotik

ANTIBIOTIK TERAPI DAN PROFILAKSIS DALAM RANGKA PENGENDALIAN
RESISTENSI ANTIBAKTERI DI RUMAH SAKIT
HARI PARATON. dr. SpOGK
KOMITE PENGENDALIAN RESISTENSI ANTIMIKROBA
KOMITE PENGENDALIAN RESISTENSI ANTIMIKROBA

• Anak 1,4 tahun, operasi Tetralogy Fallot hari 16. • Temp/ 37-39C, PCT > 5, lekosit 23.000. • Pus luka op. Pathogen: Acinotobacter baumannii• Resistance to Cephalosphorine, Meropenem, Amikacin,
Fosfomycin.

ANTIBAKTERITERAPI
ANTIBAKTERITERAPI
25
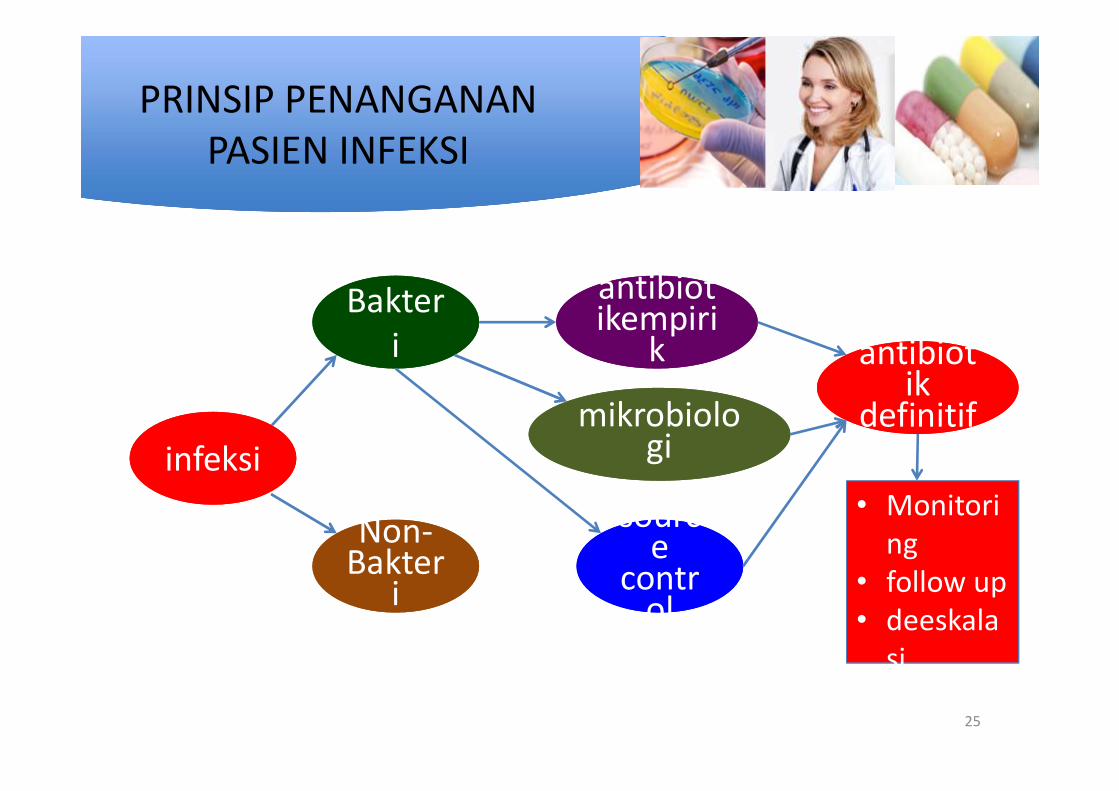
PRINSIP PENANGANAN PASIEN INFEKSI
infeksiinfeksi
Bakteri
Bakteri
Non-Bakter
i
Non-Bakter
i
antibiotikempiri
k
antibiotikempiri
k
mikrobiologi
mikrobiologi
antibiotik
definitif
antibiotik
definitif
si• stop
• Monitoring
• follow up• deeskala
si• stop
source
control
source
control

LANGKAH PERESEPAN ANTIBAKTERI
1. Apakah pasien sakit infeksi ?suhu tubuh > 38C, Nadi >90
2. Apakah infeksi bakteriLekosit>11.000, CRP(+), PCT (+)
3. Apakah ada penyebab / sumber
infeksi?kateter, drain, tampon, abces
• Demam Berdarah ?• Stroke ?• Asthma attack ?
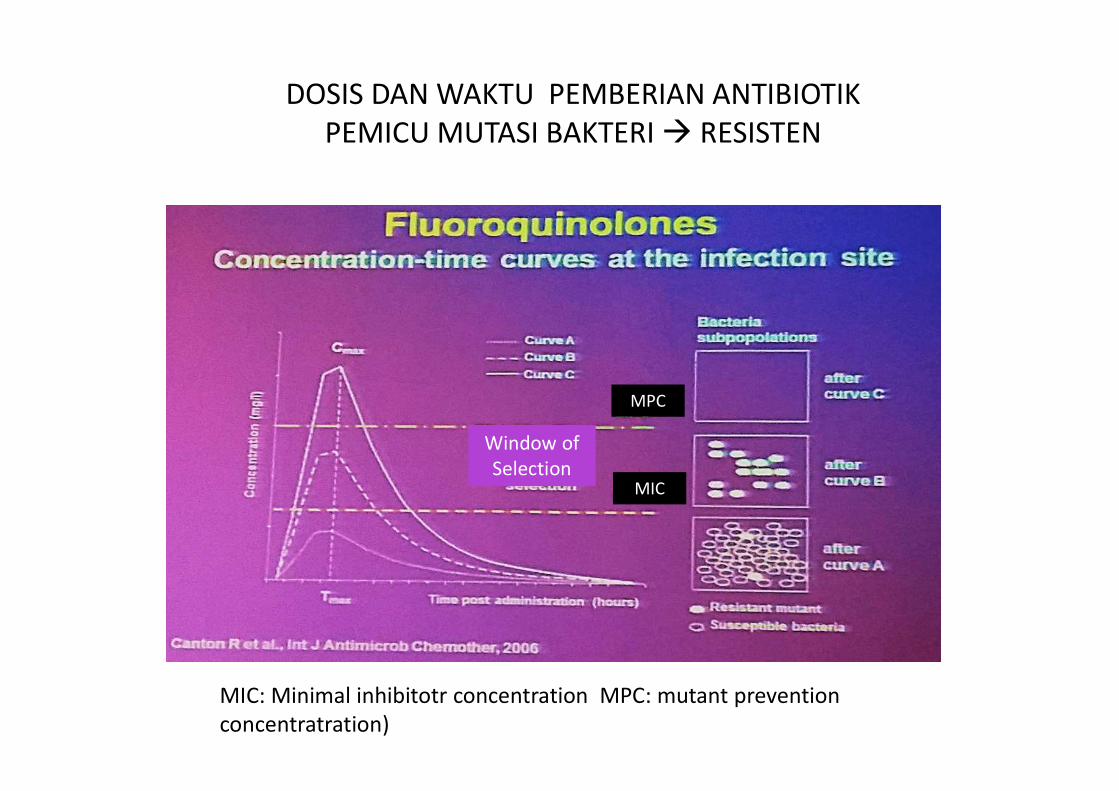
DOSIS DAN WAKTU PEMBERIAN ANTIBIOTIKPEMICU MUTASI BAKTERI RESISTEN
MIC: Minimal inhibitotr concentration MPC: mutant prevention concentratration)
MPC
MIC
Window of Selection

ANTIBAKTERITERAPI
ANTIBAKTERIPROFILAKSIS

PROFILAKSIS
1. Antibakteri, yang digunakan untuk mencegahkomplikasi infeksi padatindakan operasi.
2. diberikan sebelum operasi, ulangan saat operasi atausetelah operasi
3. batasan waktu: tidakmelebihi 24 jam

INDIKASI PROFILAKSIS
• GOLONGAN OPERASI• bersih• bersih kontaminasi• kontaminasi• kotor

Antibiotika profilaksis
kolonisasi

Profilaksis Dosis Tunggal v/s Multipel
Single-dose versus multiple-dose antibiotic prophylaxis for the surgical treatment of closed fractures .
Slobogean.et.al. Acta Orthopaedica 2010; 81 (2): 256–262
Fakta laporan
Tidak ada perbedaa
n signifikan

Results: A total of 540 patients were recruited; (females73.7% of total ). The performed surgicalprocedures were 547. The rate of wound infection was 10.9%. Multivariable logistic analysisshowed that; ASA score > 3; (p= <0.001), wound class (p= 0.001), and laparoscopic surgicaltechnique; (p= 0.002) were significantly associated with prevalence of wound infection. Surgicalprophylaxis was unnecessarily given to 311 (97.5%) of 319 patients for whom it was notrecommended. Prophylaxis was recommended for 221 patients; of them 218 (98.6 %) were givenpreoperative dose in the operating rooms. Evaluation of prescriptions for those patients showedthat; spectrum of antibiotic was adequate for 160 (73.4%) patients, 143 (65.6%) were givenaccurate doses, only 4 (1.8%) had the first preoperative dose/s in proper time window, and for186 (85.3%) of them prophylaxis was extended post-operatively. Only 36 (6.7%) prescriptionswere found to be complying with the stated criteria.
Conclusion: The rate of wound infection was high and prophylacticantibiotics were irrationally used. Multiple interventions areneeded to correct the situation.

cara pemberian AB PROFILAKSIS
• Antibakteri– Cefazolin 2 g– Cefuroxime 1,5 g
• dikamar operasi• i.v/drip dalam 100 ml NS• 30 menit sebelum insisi• dalam 15 menit• tanpa skin test• tidak perlu pemberian AB oral
pasca operasi
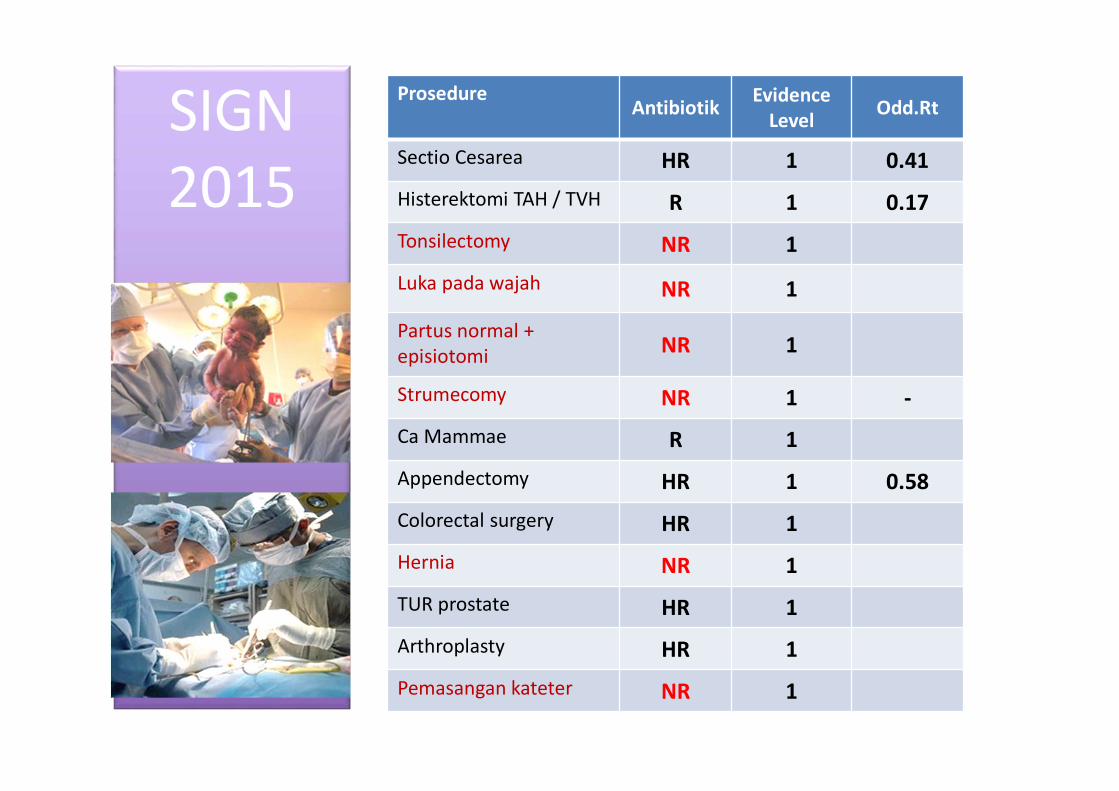
SIGN 2015
ProsedureAntibiotik Evidence
Level Odd.Rt
Sectio Cesarea HR 1 0.41
Histerektomi TAH / TVH R 1 0.17
Tonsilectomy NR 1
Luka pada wajah NR 1
Partus normal + episiotomi NR 1
Strumecomy NR 1 -
Ca Mammae R 1
Appendectomy HR 1 0.58
Colorectal surgery HR 1
Hernia NR 1
TUR prostate HR 1
Arthroplasty HR 1
Pemasangan kateter NR 1
3 - TAKE HOME MESSAGE
1. RS melaksanakan Permenkes no.8/20152. RS memiliki kebijakan, pedoman dan PPK
penggunaan antibiotik terapi dan profilaksis3. penggunaan antibiotik bijak menekan jumlah dan jenis penggunaan antibiotik menekan angka komplikasi, resistensi, kesakitan
dan kematian menekan pembeayaan pelayanan pasien
4. Perlu adanya monev dan surveillance
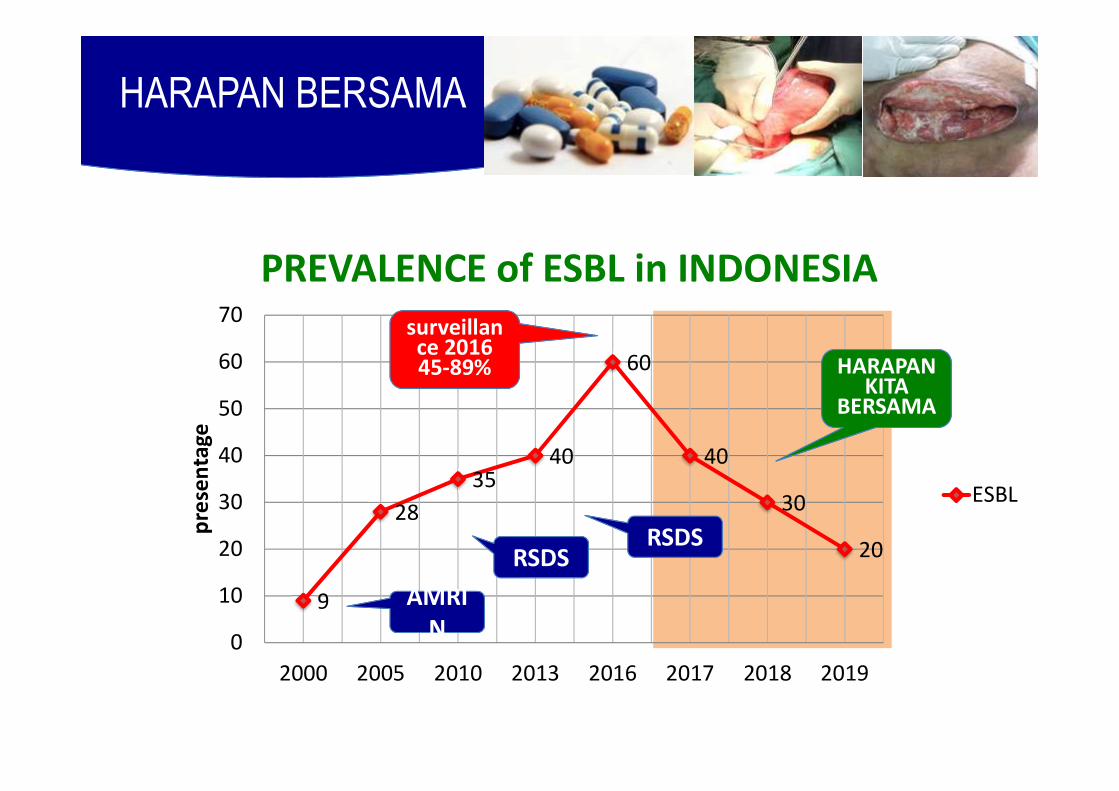
PREVALENCE of ESBL in INDONESIA
HARAPAN BERSAMA
9
2835
40
60
40
30
20
0
10
20
30
40
50
60
70
2000 2005 2010 2013 2016 2017 2018 2019
pres
enta
ge
ESBL
AMRIN
AMRIN
RSDSRSDS
surveillance 201645-89% HARAPAN
KITA BERSAMA

![Polarization-Dependent Loss: New Definition and ...groups.uni-paderborn.de/ont/publikationen/06999936_annot.pdf · displayed in a DGD profile [9, 10]. The DGD profile can be determined,](https://img.pdfslide.us/doc/110x75/606edf53244b451561181228/polarization-dependent-loss-new-definition-and-displayed-in-a-dgd-profile-9.jpg)



























![3iJLQD GH 1RWDUtD +XPEHUWR 4XH]DGD 0RUHQR $f2 0 ......2018/02/02 · 3iJLQD GH 1RWDUtD +XPEHUWR 4XH]DGD 0RUHQR,QGLFH (VFULWXUDV 3~EOLFDV $f2 0(6)HEUHUR /HWUD 'HVGH OD $ KDVWD OD =](https://img.pdfslide.us/doc/110x75/613e33a059df642846166069/3ijlqd-gh-1rwdutd-xpehuwr-4xhdgd-0ruhqr-f2-0-20180202-3ijlqd-gh.jpg)