Embed Size (px)
Citation preview

Rethinking the Treatment of Older Adults With Acute Myeloid Leukemia
Mark J. Levis, MD, PhD
Associate Professor of Oncology
The Sidney Kimmel Comprehensive Cancer Center
Johns Hopkins University

Disclosure of Conflicts of Interest
Mark J. Levis, MD, PhD, discloses that he has served as an advisor/consultant for Teva Pharmaceuticals and Ambit Biosciences Corp.

Unapproved Use Disclosure
The University of Cincinnati College of Medicine and i3
Health require CME faculty (speakers) to disclose to
attendees when products or procedures being discussed
are off-label, unlabeled, experimental, and/or
investigational (not FDA approved), and any limitations on
the information that is presented, such as data that are
preliminary or that represent ongoing research, interim
analyses, and/or unsupported opinion.
Dr. Levis discloses that he will discuss off-label uses of
decitabine and sorafenib.

Learning Objectives
Assess methods to classify and determine the prognosis of older adults with acute myeloid leukemia (AML)
Explain how patient characteristics and risk stratification affect treatment selection
Evaluate efficacy and safety data on existing and novel therapies for older adults with AML

• Annual US diagnoses: 7,820• Annual US deaths: 5,930
• Annual US diagnoses: 6,770• Annual US deaths: 4,440
Siegel et al, 2013.
AML is a clonal malignant proliferation of myeloid blast cells in the marrow with impaired normal hematopoiesis.
AML: Scope of the Problem
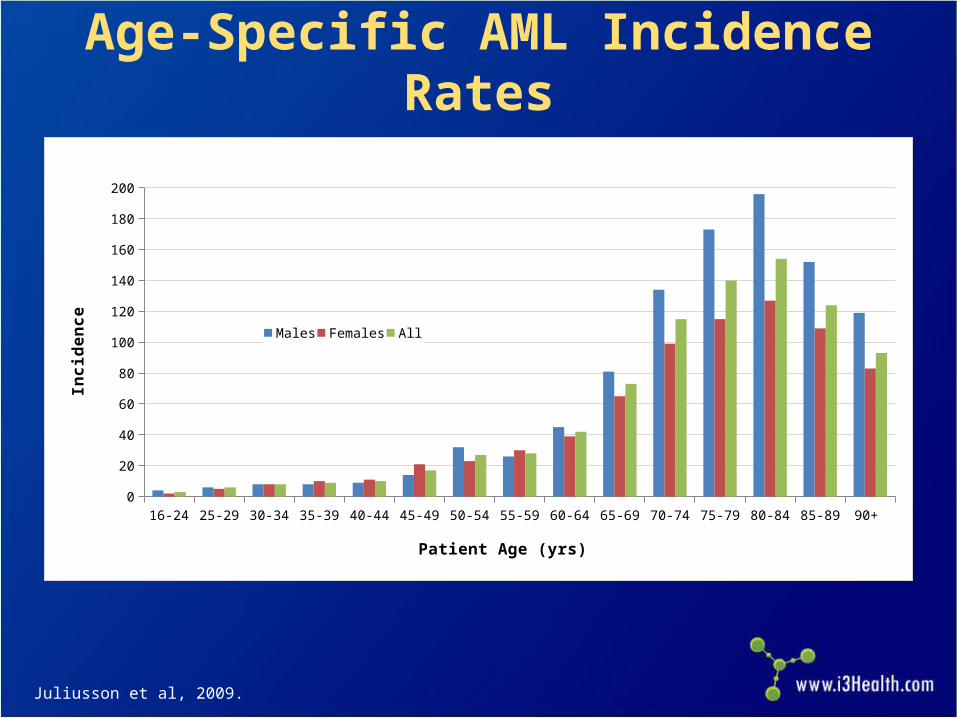
Age-Specific AML Incidence Rates
Juliusson et al, 2009.
16-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85-89 90+ 0
20
40
60
80
100
120
140
160
180
200
Males Females All
Patient Age (yrs)
Inc
ide
nc
e

MRC Trials: Younger Adults 15 to 59 Years (n=7,704)
MRC = United Kingdom Medical Research Council.Burnett, 2012.

MRC Trials: Older Adults 60+ Years (n=3,541)
Burnett, 2012.

Traditional Paradigm for the Treatment of AML
Induction therapy
Complete response
Primary refractory
Salvage therapy
Consolidation chemotherapy
Relapse?
Complete response?
Allogeneic transplant
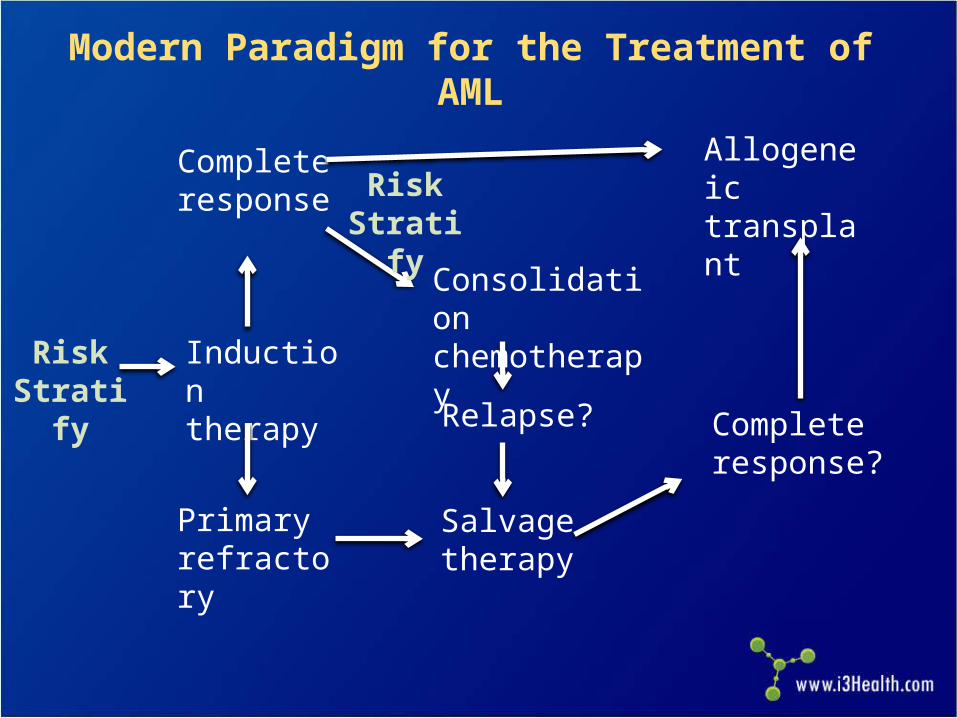
Modern Paradigm for the Treatment of AML
Complete response?
Induction therapy
Risk Stratify
Complete response
Relapse?
Primary refractory
Salvage therapy
Consolidation chemotherapy
Allogeneic transplantRisk
Stratify

Ara-C = cytarabine; ICE = idarubicin/cytarabine/etoposide; ADE = daunorubicin/cytarabine/etoposide; IA = idarubicin/cytarabine.National Comprehensive Cancer Network (NCCN), 2013.
Common Induction Regimens Used in Adult Patients With AML
Agents Doses
“7 + 3” inductionCytarabine (100–200 mg/m² infusion x 7 d) and anthracycline (daunorubicin, idarubicin, or mitoxanrone x 3 d)
Intensified induction Various combinations of Ara-C, etoposide, anthracycline (ICE, ADE, IA, etc.)
Low-dose Ara-C 20 mg bid for 10 d
Azacitidine 75 mg/m2 daily for 5–10 d
Decitabine 20 mg/m2 daily for 5 d

Hi-DAC = high-dose cytarabine; HLA = human leukocyte antigen.NCCN, 2013.
Common Consolidation Regimens Used in Adult Patients With AML
Agents Doses
“HiDAC” (4 cycles) Cytarabine (3,000 mg/m²) infused over 3 hrs bid on Days 1, 3, and 5
Allogeneic transplant Either myeloablative or nonmyeloablative, with an HLA-matched or alternative donor
Low-dose Ara-C 20 mg bid for 10 d at 4–6 wk intervals
Azacitidine 75 mg/m2/d for 5–10 d, repeated monthly
Decitabine 20 mg/m2/d for 5 d, repeated monthly

How do older patients with AML fit into this modern paradigm?

SNF = skilled nursing facility.Menzin et al, 2002.
AML Therapy in Elderly Americans
65–74 75–84 85 Total
N 1,132 1,082 443 2,657
Received chemotherapy (%) 44 24 6 30
Hospitalized (%) 89 91 83 89
Hospital/SNF days (%) 33 30 27 31
Median survival (mos) 3 2 1 2
Hospice (%) 15 19 20 17
Age group (yrs)

NA = not applicable.Menzin et al, 2006.
Survival in Elderly AML by Therapy 3,317 elderly patients aged ≥65 years with AML 1,193 (36%) received chemotherapy (younger, fewer
comorbidities) 888 patients matched in both cohorts
Survival
Median (mos) 1-Yr (%)
Overall 4.4 NA
Chemotherapy 6.1 30
No therapy 1.7 10

NCCN, 2013; Rogers, 2010; Higa et al, 1991; Jabbour et al, 2006; Harris et al, 2008.
Supportive Care Is Effective but Insufficient as a Primary Treatment
Symptom Treatment
Fungal infectionsAzole antifungals (posaconazole, voriconazole, echinacandins, amphotericin-B)
Bacterial infections Broad-spectrum antibiotics
Viral infections Acyclovir, valacyclovir
Leukocytosis Hydroxyurea
Neutropenia G-CSF (filgrastim), GM-CSF (sargramostim) during post-remission therapy
Anemia/thrombocytopeniaLeukocyte-depleted products for transfusion and irradiated blood products for patients receiving immunosuppressive therapy; screen for cytomegalovirus
Tumor lysis syndromeProphylaxis with intravenous hydration with diuresis, urinary alkalinization, allopurinol; treatment with rasburicase
Cognitive declinePatient monitoring for nystagmus, dysmetria, slurred speech, and ataxia before each dose of cytarabine
Nausea/vomiting Serotonin receptor antagonists (ondansetron)
Ocular toxicity Saline or steroid drops in both eyes during cytarabine therapy
Oral mucositis Mouthwash with viscous lidocaine, Maalox, and injectable diphenhydramine

DNR = daunorubicin; CR = complete response; SQ = subcutaneously.Lowenberg et al, 1989; Tilly et al, 1990.
“Standard” Chemotherapy vs. Nonintensive
DNR + Ara-C vs. “watch and wait” (hydroxyurea)
– CR in 58% vs. 0%
– Median survival: 21 vs. 11 weeks
– Survival at 2.5 years: 13% vs. 0% Ara-C SQ 20 mg/m2 for 21 days vs. “7 + 3”
– CR with “7 + 3”: 52% vs. 32%
– induction death with “7 + 3”: 31% vs. 10%
– Similar survival and CR duration

Pts = patients.Juliusson et al, 2006.
Intention to Induce by Age and Region (Swedish Registry)
Region
Pts
con
side
red
for
rem
issi
on in
duct
ion
ther
apy
(%)

APL = acute promyelocytic leukemia; RI = resistive index. Juliusson et al, 2006.
Survival Among Patients Ages 70–79
(region, sample size)

aData not available for all patients.ATRA = all-trans retinoic acid; MDS = myelodysplastic syndromes.Burnett et al, 2007.
Low-Dose Ara-C vs. Hydroxyurea ± ATRA in Elderly AML or High-Risk MDS
217 elderly patients aged ≥60: 155 aged ≥65 years, 58 secondary AML, 30 high-risk MDS
Ara-C 20 mg bid x 10 every 4–6 weeks vs. hydroxyurea
Ara-C Hydroxyurea P
na 102 99 NA
CR (%) 18 1 0.00006
1-Year OS (%) 27 3 0.0009
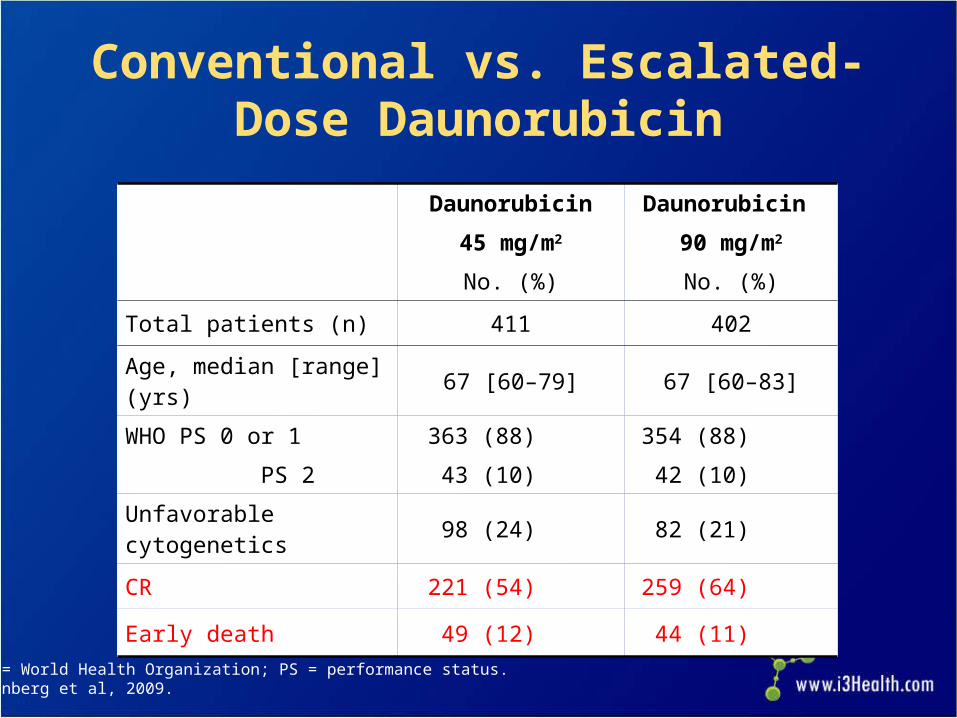
WHO = World Health Organization; PS = performance status.Lowenberg et al, 2009.
Conventional vs. Escalated-Dose Daunorubicin
Daunorubicin
45 mg/m2
No. (%)
Daunorubicin
90 mg/m2
No. (%)
Total patients (n) 411 402
Age, median [range] (yrs) 67 [60–79] 67 [60–83]
WHO PS 0 or 1
PS 2
363 (88)
43 (10)
354 (88)
42 (10)
Unfavorable cytogenetics 98 (24) 82 (21)
CR 221 (54) 259 (64)
Early death 49 (12) 44 (11)

Lowenberg et al, 2009.
Conventional vs. Escalated-Dose Daunorubicin, Survival by Age

Lowenberg et al, 2009.
Conventional vs. Escalated-Dose Daunorubicin, Survival by Age (cont.)

VPA = valproic acid; ATRA = all trans retinoic acid; CRi = complete response with incomplete hematologic recovery; PR = partial response; HI = hematologic improvement.Thépot et al, 2009.
Frontline Azacitidine
• Sample of 165 patients treated with azacitidine 75 mg/m2 ± VPA and ATRA ; 32% had 20%–29% marrow blasts
• Median age, 74 yrs (31–91); 83% 65 years; median cycles, 4; median follow-up, 16 mos
Response No. (%)
CR + CRi 19 + 3 (13)
PR 10 (6)
HI 28 (17)
• Median response duration, 6.9 months
• Median survival, 9.4 months; 1-year OS, 37%
19%

AZA = azacitidine; IC = intensive chemotherapy; LDAC = low-dose cytarabine; BSC = best supportive care; CCR = conventional care regimen; NS = not significant. Fenaux et al, 2010.
Azacitidine Prolongs Survival in WHO-Defined AML
113 older patients with 20%–29% blasts (WHO AML) Median age 70 years; poor cytogenetics 24% 55 randomly assigned to AZA, 58 to conventional care
regimens (IC 11, LDAC 20, BSC 27) Median follow-up, 20 months; median cycles, 8 (1–39)
Parameter AZA CCR P value
CR (%) 18 16 NS
Median OS 24.5 16.0 0.005
Hospitalization (pt/yr) 3.4 4.3 0.03
Infection (pt/yr) 0.58 1.14 0.003

Initial Conclusions
Modern AML treatment requires risk stratification at multiple time points
Treatment confers a survival benefit over supportive care, even in older AML patients

Risk Stratification(Questions to Consider for Each Patient)
Will the patient survive treatment?How likely is it that a patient will achieve
remission?– What type of induction therapy should be used?
If a remission is achieved, will the patient benefit from consolidation?– What type of consolidation therapy should be
used?

Appelbaum et al, 2006.
Thirty-Day Mortality of AML Induction Therapy: Effect of PS
Age (yrs) <56 56–65 66–75 >75
PS Early Death (%)
0 2 11 12 14
1 3 5 16 18
2 2 18 31 50
3 0 29 47 82

Juliusson et al, 2009.
Proportion of AML (Non-APL) Patients, PS 0 to 4 at Diagnosis
16-24 25-29 30-34 35-39 40-44 45-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85-89 90+ All0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
WHO 0
WHO I
WHO II
WHO III
WHO IV
Missing
Age (yrs)
Pts
per
WH
O p
erfo
rman
ce s
tatu
s (%
)

Kantarjian et al, 2006.
Prognostic Model: MD Anderson
Prognostic Factor CR Rate
8-Wk Mortality
1-Yr Survival
Age ≥75 yrs ■ ■ ■
Poor performance status ■ ■ ■
Unfavorable karyotype ■ ■ ■
Anemia ■
Leukocytosis ■
Antecedent hematologic disease ■ ■ ■
Creatinine >1.3 mg/dL ■ ■ ■
Elevated lactate dehydrogenase ■
Treated in laminar flow room ■ ■ ■
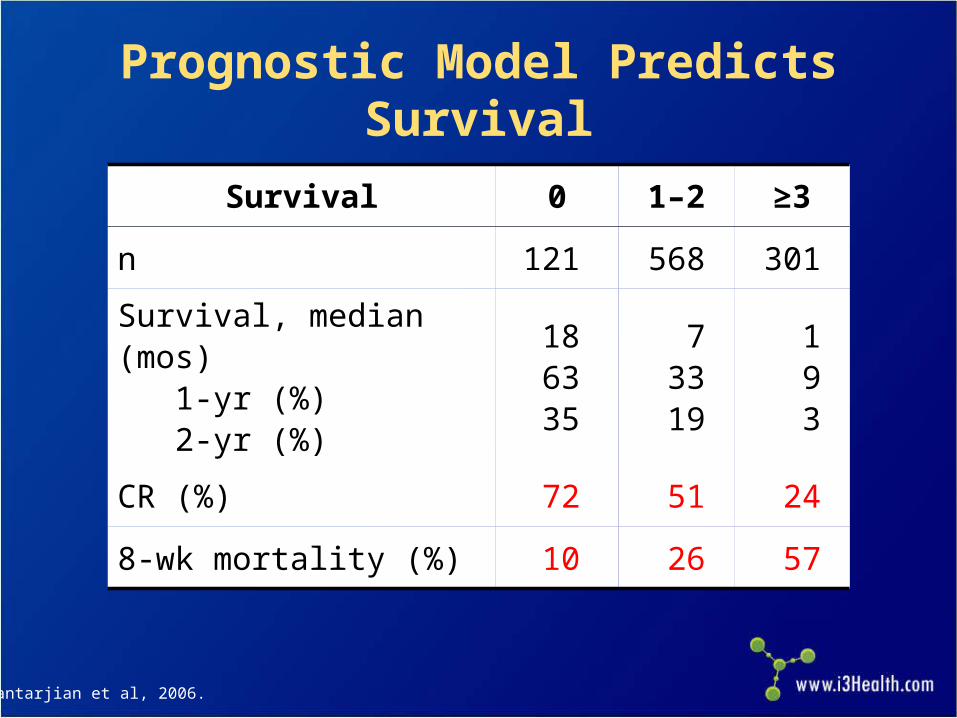
Kantarjian et al, 2006.
Prognostic Model Predicts Survival
Survival 0 1–2 ≥3
n 121 568 301
Survival, median (mos) 1-yr (%) 2-yr (%)
186335
73319
193
CR (%) 72 51 24
8-wk mortality (%) 10 26 57

1. Complex karyotype2. Monosomy karyotype3. Deletion of 5 or 74. t(6;9)5. inv(3)6. 11q23 (MLL gene)
Unfavorable1. inv(16)2. t(8;21)3. t(15;17)
Favorable
IntermediateEverything else
Cytogenetic Risk Categories
MLL = mixed lineage leukemia; inv = inversion; t = translocation. Grimwade et al, 2001; Slovak et al, 2000.

Appelbaum et al, 2006.
Unfavorable Risk Cytogenetics Increase With Age
<55 56-65 66-75 >750%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
17
6 5 4
4855 56
45
35 39 39 51
Unfavorable
Intermediate
Favorable
Age (yrs)
Inci
denc
e of
pts
with
ris
k cy
toge
netic
s

Molecular Risk CategoriesFLT3/ITD mutations = unfavorable riskNPM1 mutations = favorable risk
– In the absence of a FLT3/ITD mutation
CEBPA mutations = favorable risk– In the presence of double mutations
C-KIT mutations = unfavorable risk– In the context of core binding factor AML
FLT3 = fms-related tyrosine kinase 3; ITD = internal tandem duplication; NPM1 = nucleophosmin;CEBPA = CCAAT/enhancer binding protein, alpha; C-KIT = type III tyrosine kinase growth factor receptor.Kottaridis et al, 2001; Dohner et al, 2005; Taskesen et al, 2011; Paschka et al, 2006.

APL
CBF(inv[16], t[8;21])
CEBPA
NPM1c
Poor-risk cytogenetics
(5q-; 7q-; inv[3], complex, etc.)
FLT3/ITD
Otherint. risk
AML Categories Defined by Cytogenetic and Molecular Abnormalities in All Adults
NPM1c = mutated nucleophosmin; CBF = core-binding factor; int. = intermediate.Kottaridis et al, 2001; Dohner et al, 2005; Taskesen et al, 2011; Paschka et al, 2006.

APL
CBF(inv16, t8;21)
CEBPA
NPM1c
Poor-risk cytogenetics
(5q-; 7q-; inv[3], complex, etc)
FLT3/ITD
Otherint. risk
AML Categories Defined by Cytogenetic and Molecular Abnormalities in Older Adults
Kottaridis et al, 2001; Dohner et al, 2005; Taskesen et al, 2011; Paschka et al, 2006.

Grimwade et al, 2001.
Karyotype Significantly Impacts CR and OS in Elderly AML
CR OS (5-year)0
10
20
30
40
50
60
70
80
90
100
72
34
53
15
26
2
Favorable (7%): t(15;17), t(8;21), inv(16)
Intermediate (79%): normal, all others
Unfavorable (14%): complex (>5 abnormal)
Kar
yoty
pe In
fluen
ce o
n P
atie
nt S
urvi
val
(%)

Wt = wild type; mut = mutation.Becker et al, 2010.
DFS and OS of Patients Age ≥60 Years (A and B) and Age ≥70 Years (C and D) With Diploid AML by NPM1 Status

Overall Survival of Older AML Patients With or Without a FLT3/ITD Mutation
Patients enrolled on UK MRC AML16 trial Treated with intensive induction
Lazenby et al, 2014.

Median follow-up, 2.1 years
Nonmyeloablative Allogeneic Transplantin Patients by Decade
PFS = progression-free survival; OS = overall survival. Kasamon et al, 2013.

Sekeres et al, 2009.
Delaying Treatment Safe for Older Patients

More Conclusions
Performance status and karyotype have a major impact on the likelihood of surviving induction therapy in older AML patients
Adverse karyotypes are more common in older AML patients
Molecular and cytogenetic features influence outcomes in older AML patients the same way they do in younger AML patients
If possible, treatment of an older AML patient should be delayed until an initial risk stratification can be performed

Novel Agents in Clinical Development

Selected Novel Agents in Clinical Trials for Older Patients With AML
Class Examples
Purine analog Clofarabinea
DNA methylation inhibitor Azacitidine, decitabinea
Histone deacetylase (HDAC) inhibitor
Vorinostatb, pracinostatb
Anti-CD33 antibody conjugate Gemtuzumab ozogamicina,b
Immunomodulatory agent Lenalidomidea
FLT3 kinase inhibitor Quizartinibb, PLX3397b, ASP2215b
Polo-like kinase (PLK1) inhibitor
Volasertibb
Novel cytotoxics CPX-351b
aOff-label.bInvestigational.Slide adapted from Ravandi F, 2012.

RNR = ribonucleotide reductase.Montgomery et al, 1992.
Clofarabine
N
N N
NNH2
OHO
HO
Cl
F
Rationally designed purine analog
Resistant to deamination and phosphorolysis
Inhibition of DNA synthesis and repair
Inhibitor of RNR and DNA polymerase
Induction of apoptosis

OR = overall response; DOR = duration of response; AHD = antecedent hematologic disorder; CG = cytogenetics.Kantarjian et al, 2010.
Clofarabine Frontline Monotherapy in Elderly AML Patients
Parameter N CR (%) OR (%) DOR OS
Age 70 69 33 39 15 7.2
AHD 41 39 51 8.6+ 12
Intermediate CG 46 48 54 15 12
Unfavorable CG 62 32 42 9.5 7.2

Clofarabine for Newly-Diagnosed Older AML Patients Median age: 74 years Clofarabine 20 mg/ m2 for 5 days vs. low-dose Ara-C CR rate:
– Clofarabine: 22%– Low-dose Ara-C: 12%
Burnett et al, 2013.

Epigenetic Therapy
M M M M
DNA Methylation Histone Modification
Phosphorylation
Methylation
Acetylation
AzacitidineDecitabine
PracinostatVorinostat

PBC = absolute peripheral blood count.Cashen et al, 2010.
Frontline Decitabine in Older Patients With AML
NCR(%)
All Patients 55 24
Presenting Bone Marrow Blast (%)
<30 18 28
30 to <50 9 20
≥50 28 25
Presenting PBC
<1000 41 29
1,000 to 10,000 11 9
>10,000 3 0

Blum et al, 2010.
Ten-Day Schedule of Decitabine for Older Patients With Untreated AML
All Patients (N =
53)
Age <74 (N =
25)
Age 74+ (N =
28)
Normal Karyotype
(N = 21)
Complex Karyotype
(N = 16)
Monosomy 7 / del(7q) (N = 11)
0
20
40
60
80
100
CR Incomplete CR
Perc
ent R
espo
nse
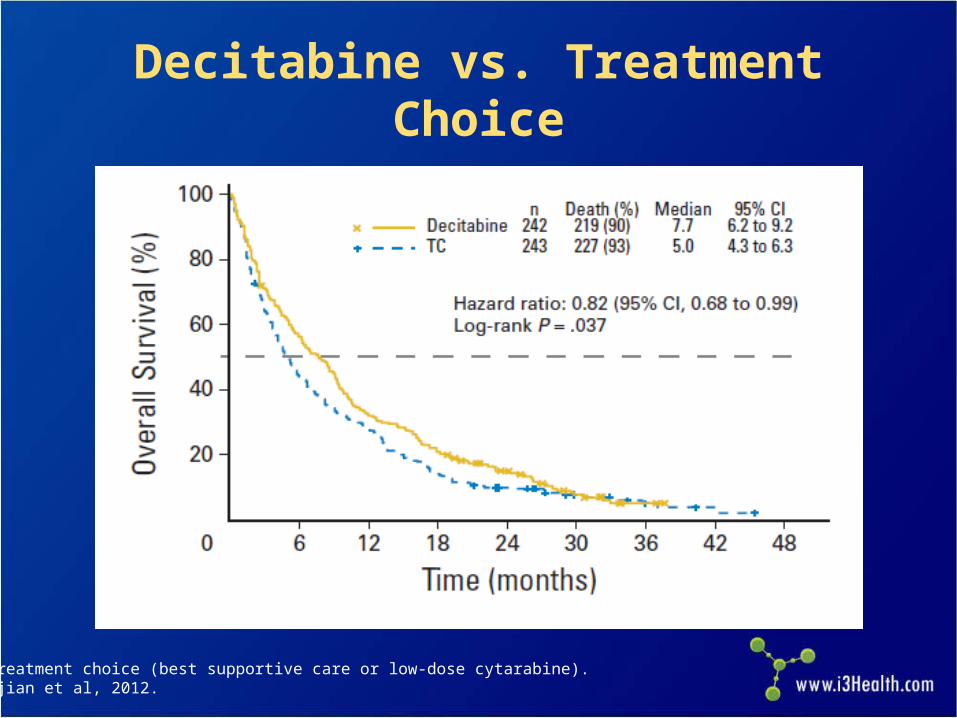
TC = treatment choice (best supportive care or low-dose cytarabine).Kantarjian et al, 2012.
Decitabine vs. Treatment Choice

Newly-diagnosed
AMLRandomize
Complete response?
“7 + 3”/HiDAC
ClofarabineDecitabine
maintenance
Allogeneic transplant
HLA-matched sibling?
FollowRandomize
E2906 Trial on Clofarabine Newly-diagnosed AML, age >60 Multicenter, cooperative group study
Eastern Cooperative Oncology Group (ECOG), 2012.

Gemtuzumab Ozogamicin
Castaigne et al, 2012.

Lenalidomide
ELN = European Leukemia Net; ORR = overall response rate; RD = resistant disease; ED = early death. Pollyea et al, 2013.
Risk Group (ELN) CR (%) CRi (%) PR (%) RD (%) ED (%)
Favorable 14 14 14 57 0
Intermediate-1 25 0 17 50 8
Intermediate-2 17 8 8 42 25
Adverse 18 18 9 27 27
• First-line azacitidine then lenalidomide• ORR 40%, including 28% CR/CRi• Common adverse events were gastrointestinal,
fatigue, and myelosuppression

16 of 110 (15%) patients remained alive for >12 months after taking quizartinib and were classified as long-term survivors
CRc 58%
7%
51%
21%
100
80
60
40
20
FLT3/ITD N=110
CR/CRp
CRi
PR
CRc = CR + CRi + CRp.Cortes et al, 2012.
Quizartinib Induces a High Response Rate in Older Patients With
Relapsed/Refractory FLT3/ITD AML
Pat
ient
s ac
hiev
ing
posi
tive
outc
omes
(%
)

Frontline Volasertib + LDAC vs. LDAC in Elderly Patients
Maertens et al, 2012.
Event-Free Survival

CPX-351: Liposomal Daunorubicin and Cytarabine
Lancet et al, 2012.
Parameter CPX-351(n=26)
“7 + 3” Regimen
(n=15)
Pts with 2 risk factors (%) 23 (88.5) 12 (80.0)
Pts with 3 risk factors (%) 3 (11.5) 3 (20.0)
CR (%) 11 (42.3) 4 (26.7)
CRi (%) 7 (26.9) 0
CR + CRi (%) 18 (69.2) 4 (26.7)
60-d mortality (%) 1 (3.8) 6 (40.0)
Median EFS (mos) 9.1 1.1
Median OS (mos) 23 (88.5) 12 (80.0)

Case Study 1: Transplantation

Case Study 1 A 67-year-old woman presents with low-grade
fever, anemia, thrombocytopenia, and leucopenia Has no comorbid conditions or antecedent
hematologic disorder; organ functions are normal Bone marrow exam reveals AML and cytogenetic
analysis reveals loss of a translocation between chromosome 9 and 11 at band q23 in 17 out of 20 metaphases
What is the recommended therapy for this patient?

Case Study 1 (cont.)
She receives induction with cytarabine, daunorubicin, and etoposide
Achieves a CR• Remission marrow shows normal karyotype• Reduced performance status, ineligible for further
therapy until Day 70 Undergoes a nonmyeloablative allogeneic
transplant with her HLA-matched sister as donor She is in ongoing remission 1 year after her
diagnosis• Normal performance status

Case Study 2: Favorable Risk

Case Study 2
A 72-year-old man presents in December 2010 with dyspnea and a white count of 149,000
No comorbid conditions or history of an antecedent hematologic disorder
Diagnosis: AML Normal karyotype; NPM1c
What treatment would you recommend?

Case Study 2 (cont.)
Receives induction therapy with cytarabine and idarubicin (“7 + 3”)
Achieves a CR Started on HiDAC consolidation therapy Relapses after 22 months Re-induced with HiDAC and achieves a second
remission Enrolled in a clinical trial for maintenance anti-
interleukin-3 receptor (CD123) antibody Remission is ongoing

Case Study 3: Progression of AML

Case Study 3 A 71-year-old man presents with fever, profound
fatigue, anemia, and circulating blasts• ECOG PS of 3• Bone marrow biopsy, 30% blasts• Complex cytogenetics, including loss of
chromosomes 5 and 7 Other past medical history:
• Chronic myelomonocytic leukemia for 1 year• Emphysema• Chronic atrial fibrillation/flutter; on anticoagulation
therapy• Stage III rectal colorectal adenocarcinoma, neo-
adjuvant radiation therapy, post-operation chemo 3 years prior
What treatment would you recommend?

Case Study 3 (cont.)
5-azacitidine 75 mg/m2 for 5 days per cycle; gets monthly treatment as outpatient
Peripheral blood cleared of blasts PS improves Bone marrow shows persistent blasts after 6 cycles Disease progression nearly a year later
• ECOG PS still 1 Referred for a clinical trial

Case Study 4: Other AML subtypes
Case Study 4
A 75-year-old woman presents in February 2010 with
bruising and petechiae Reports some bleeding when brushing her teeth WBC is 9.3 with 71% promyelocytes, Plt 12, and Hgb
8.4 Bone marrow exam is consistent with APL. You send
a specimen for cytogenetic and molecular studies
What treatment would you recommend?
WBC = white blood cell count; Plt = platelet count; Hgb = hemoglobin count.

Case Study 4 (cont.)
Receives ATRA/daunorubicin and achieves CR Consolidation with arsenic and ATRA Currently in ongoing remission

Key Takeaways Older patients can benefit from treatment in addition to
supportive care Risk stratification prior to induction is particularly
important for older AML patients Older AML patients are more likely to have unfavorable
karyotypes Cytogenetic and molecular abnormalities influence the
outcome in older AML patients the same way they do in younger AML patients
Patients should be treated in clinical trials whenever possible- Novel agents, as well as novel combinations of
established agents, are currently under investigation

ReferencesAppelbaum FR, Gundacker H, Head DR, et al (2006). Age and acute myeloid leukemia. Blood, 107(9):3481-3485.Becker H, Marcucci G, Maharry K, et al (2010). Favorable prognostic impact of NPM1 mutations in older patients with
cytogenetically normal de novo acute myeloid leukemia and associated gene- and microRNA-expression signatures: a Cancer and Leukemia Group B study. J Clin Oncol, 28(4):596-604.
Blum W, Garzon R, Klisovic RB, et al (2010). Clinical response and miR-29b predictive significance in older AML patients treated with a 10-d schedule of decitabine. Proc Natl Acad Sci USA, 107(16):7473-7478.
Burnett AK (2012). Treatment of acute myeloid leukemia: are we making progress? ASH Education Book, 1:1-6.Burnett AK, Milligan D, Prentice AG, et al (2007). A comparison of low-dose cytarabine and hydroxyurea with or without all-trans
retinoic acid for acute myeloid leukemia and high-risk myelodysplastic syndrome in patients not considered fit for intensive treatment. Cancer, 109(6):1114-1124.
Burnett AK, Russell NH, Hunter AE, et al (2013). Clofarabine doubles the response rate in older patients with acute myeloid leukemia but does not improve survival. Blood (ASH Annual Meeting Abstracts), 122(8):1384-1394.
Cashen AF, Schiller GJ, O’Donnell MR, DiPersio JF (2010). Multicenter, phase II study of decitabine for the first-line treatment of older patients with acute myeloid leukemia. J Clin Oncol, 28(4):556-661.
Castaigne S, Pautas C, Terré C, et al (2012). Effect of gemtuzumab ozogamicin on survival of adult patients with de-novo acute myeloid leukaemia (ALFA-0701): a randomised, open-label, phase 3 study. Lancet, 379(9825):1508-1516.
Cortes JE, Kantarjian H, Foran JM, et al (2013). Phase I study of quizartinin administered daily to patients with relapsed or refractory acute myleloid leukemia irrespective of FMS-like tyrosine kinase 3-internal tandem duplication status. J Clin Oncol, 3(29):3681-3687. DOI:10.1200/JCO.2013.48/8783.
Cortes JE, Perl AE, Dombret H, et al (2012). Final results of a phase 2 open-label, monotherapy efficacy and safety study of quizartinib (AC220) in patients 60 yrs of age with FLT3 ITD positive or negative relapsed/refractory acute myeloid Leukemia. Blood (ASH Annual Meeting Abstracts), 120. Abstract 48.
Dohner K, Schlenk RF, Habdank M, et al (2005). Mutant nucleophosmin (NPM1) predicts favorable prognosis in younger adults with acute myeloid leukemia and normal cytogenetics: interaction with other gene mutations. Blood (ASH Annual Meeting Abstracts), 106(12):3740-3746.
European Cooperative Oncology Group (2012). Clorafabine or daunorubicin hydrochloride and cytarabine followed by decitabine or observation in treating older patients with newly diagnosed acute myeloid leukemia. Accessed on April 18, 2014. Available at: clinicaltrials.gov/show/NCT01041703
Fenaux P, Mufti GJ, Hellström-Lindberg E, et al (2010). Azacitidine prolongs overall survival compared with conventional care regimens in elderly patients with low bone marrow blast count acute myeloid leukemia. J Clin Oncol, 28(4):562-569.

References (cont.)Grimwade D, Walker H, Harrison G, et al (2001). The predictive value of hierarchical cytogenetic classification in older adults with
acute myeloid leukemia (AML): analysis of 1065 patients entered into the United Kingdom Medical Research Council AML11 trial. Blood (ASH Annual Meeting Abstract), 98(5):1312-1320.
Harris DJ, Eilers J, Harriman A, Cashavelly BJ, Maxwell C (2008). Putting evidence into practice: Evidence-based interventions for the management of oral mucositis. Clin J Onc Nurs, 12(1):141-152.
Higa GM, Gockerman JP, Hunt AL, et al (1991). The use of prophylactic eye drops during high-dose cytosine arabinoside. Cancer, 68(8):1691-1693.
Jabbour EJ, Estey E, Kantarjian HM (2006). Adult acute myeloid leukemia. Mayo Clinic Proc, 81:247–260.Juliusson G (2011). Older patients with acute myeloid leukemia benefit from intensive chemotherapy: an update from the Swedish
Acute Leukemia Registry. Clin Lymphoma Myeloma Leuk, 11(Suppl 1):S54-S59.Juliusson G, Antunovic P, Derolf A, et al (2009). Age and acute myeloid leukemia: real world data on decision to treat and outcomes
from the Swedish Acute Leukemia Registry. Blood (ASH Annual Meeting Abstracts), 113(18):4179-4187.Juliusson G, Billström R, Gruber A, et al (2006). Attitude towards remission induction for elderly patients with acute myeloid
leukemia influences survival. Leukemia, 20(1):42-47.Kantarjian HM, Thomas XG, Dmoszynska A, et al (2012). Multicenter, randomized, open-label, phase III trial of decitabine versus
patient choice, with physician advice, of either supportive care or low-dose cytarabine for the treatment of older patients with newly diagnosed acute myeloid leukemia. J Clin Oncol, 30(21):2670-2677.
Kantarjian HM, Erba HP, Claxton D, et al (2010). Phase II study of clofarabine monotherapy in previously untreated older adults with acute myeloid leukemia and unfavorable prognostic factors. J Clin Oncol, 28(4):549-555.
Kantarjian H, O'Brien S (2010). Questions regarding frontline therapy of acute myeloid leukemia. Cancer, 116(21):4896-4901.Kantarjian H, O'Brien S, Cortes J, et al (2006). Results of intensive chemotherapy in 998 patients age 65 yrs or older with acute
myeloid leukemia or high-risk myelodysplastic syndrome: predictive prognostic models for outcome. Cancer, 106(5):1090-1098.
Kasamon YL, Prince G, Bolaños-Meade J, et al (2013). Encouraging outcomes in older patients (pts) following nonmyeloablative (NMA) haploidentical blood or marrow transplantation (haploBMT) with high-dose posttransplantation cyclophosphamide (PT/Cy). Blood (ASH Annual Meeting Abstracts), 122. Abstract 158.
Kottaridis PD, Gale RE, Frew ME, et al (2001). The presence of FLT3 internal tandem duplication in patients with acute myeloid leukemia (AML) adds important prognostic information to cytogenetic risk group and response to the first cycle of chemotherapy: analysis of 854 patients from the United Kingdom Medical Research Council AML 10 and 12 trials. Blood (ASH Annual Meeting Abstracts), 98(6):1752-1759.

References (cont.)Lancet JE, Cortes JE, Kovacsovics T, et al (2012). CPX-351 is effective in newly diagnosed older patients with AML and with
multiple risk factors. Blood (ASH Annual Meeting Abstracts), 120. Abstract 3626.Lazenby M, Gilkes AF, Marrin C, et al (2014). The prognostic relevance of flt3 and npm1 mutations on older patients treated
intensively or non-intensively: a study of 1312 patients in the UK NCRI AML16 trial. Leukemia, (Epub).Löwenberg B, Ossenkoppele GJ, van Putten W, et al (2009). High-dose daunorubicin in older patients with acute myeloid leukemia.
N Engl J Med, 361(13):1235-1248.Löwenberg B, Zittoun R, Kerkhofs H, et al (1989). On the value of intensive remission-induction chemotherapy in elderly patients of
65+ yrs with acute myeloid leukemia: a randomized phase III study of the European Organization for Research and Treatment of Cancer Leukemia Group. J Clin Oncol, 7(9):1268-1274.
Maertens J, Lübbert M, Fiedler W, et al (2012). Phase I/II study of volasertib (BI 6727), an intravenous polo-like kinase (PLK) inhibitor, in patients with acute myeloid leukemia (AML): results from the randomized phase II part for volasertib in combination with low-dose cytarabine (LDAC) versus LDAC monotherapy in patients with previously untreated AML ineligible for intensive treatment. Blood (ASH Annual Meeting Abstracts), 120. Abstract 411.
Menzin J, Boulanger L, Karsten V, et al (2006). Effects of initial treatment on survival among elderly AML patients: Findings from the SEER-Medicare database. Blood (ASH Annual Meeting Abstracts), 108(Suppl). Abstract 1973.
Menzin J, Lang K, Earle CC, et al (2002). The outcomes and costs of acute myeloid leukemia among the elderly. Arch Intern Med, 162(14):1597-1603.
Montgomery JA, Shortnacy-Fowler AT, Clayton SD, et al (1992). Synthesis and biologic activity of 2'-fluoro-2-halo derivatives of 9-beta-D-arabinofuranosyladenine. J Med Chem, 35(2):397-401.
National Comprehensive Cancer Network (2013). NCCN Clinical Practice Guidelines in Oncology. Acute myeloid leukemia. Version 2.2013. Accessed on April 27, 2014. Available at http://www.nccn.org
Paschka P, Marcucci G, Ruppert AS, et al (2006). Adverse prognostic significance of KIT mutations in adult acute myeloid leukemia with inv(16) and t(8;21): a Cancer and Leukemia Group B Study. J Clin Oncol, 24(24):3904-3911.
Pollyea DA, Zehnder J, Coutre S, et al (2013). Sequential azacitidine plus lenalidomide combination for elderly patients with untreated acute myeloid leukemia. Haematologica, 98(4):591-596.

References (cont.)
Rogers BB (2010). Advances in the management of acute myeloid leukemia in older adult patients. Oncol Nurs Forum, 37(3):E168-E179.
Sekeres MA, Elson P, Kalaycio ME, et al (2009). Time from diagnosis to treatment initiation predicts survival in younger, but not older, acute myeloid leukemia patients. Blood (ASH Annual Meeting Abstracts), 113(1):28-36.
Siegel R, Naishadham D, Jemal A (2013). Cancer statistics, 2013. CA: Cancer J Clinicians, 63:11-20.Slovak K, Kopecky J, Cassileth, PA, et al (2000). Karyotypic analysis predicts outcome of preremission and postremission therapy
in adult acute myeloid leukemia: a Southwest Oncology Group/Eastern Cooperative Oncology Group study. Blood (ASH Annual Meeting Abstracts), 96(13): 4075-4083.
Taskesen E, Bullinger L, Corbacioglu A et al. (2011). Prognostic impact, concurrent genetic mutations, and gene expression features of AML with CEBPA mutations in a cohort of 1182 cytogenetically normal AML patients: further evidence for CEBPA double mutant AML as a distinctive disease entity. Blood (ASH Annual Meeting Abstracts), 117(8):2469-2475. DOI:10.1182/blood-2010-09-307280.
Thépot S, Itzykson R, Seegers V, et al (2009). Azacytidine (AZA) as first line therapy in AML: results of the French ATU Program. Blood (ASH Annual Meeting Abstracts). Abstract 843.
Tilly H, Castaigne S, Bordessoule D, et al (1990). Low-dose cytarabine versus intensive chemotherapy in the treatment of acute nonlymphocytic leukemia in the elderly. J Clin Oncol, 8(2):272-279.