Embed Size (px)
Citation preview

Page 1/23
Clinical Characteristics and Predictors of In-hospitalMortality in Patients with Cardiogenic Shock:Results from the RESCUE RegistryJeong Hoon Yang
Samsung Medical Center https://orcid.org/0000-0001-8138-1367Ki Hong Choi
Samsung Medical CenterYoung-Guk Ko
Severance Cardiovascular HospitalChul-Min Ahn
Severance Cardiovascular HospitalCheol Woong Yu
Korea University Anam HospitalWoo Jung Chun
Samsung Changwon HospitalWoo Jin Jang
Ewha Woman's University Seoul HospitalHyun-Joong Kim
Konkuk University Medical CenterBum Sung Kim
Konkuk University Medical CenterJang-Whan Bae
Chungbuk National University College of MedicineSang Yeub Lee
Chungbuk National University College of MedicineSung Uk Kwon
Inje University Ilsan Paik HospitalHyun-Jong Lee
Sejong General HospitalWang Soo Lee
Chung-Ang University HospitalJin-Ok Jeong
Chungnam National University HospitalSang-Don Park

Page 2/23
Inha University HospitalSeong-Hoon Lim
Dankook University HospitalSungsoo Cho
Dankook University HospitalTaek Kyu Park
Samsung Medical CenterJoo Myung Lee
Samsung Medical CenterYoung Bin Song
Samsung Medical CenterJoo-Yong Hahn
Samsung Medical CenterSeung-Hyuk Choi
Samsung Medical CenterHyeon-Cheol Gwon ( [email protected] )
Sungkyunkwan University School of Medicine
Research
Keywords: Cardiogenic shock, vasopressor, mechanical circulatory support
Posted Date: November 12th, 2020
DOI: https://doi.org/10.21203/rs.3.rs-102981/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License. Read Full License
Version of Record: A version of this preprint was published at Circulation: Heart Failure on June 1st, 2021.See the published version at https://doi.org/10.1161/CIRCHEARTFAILURE.120.008141.

Page 3/23
AbstractBackground: In the current era of mechanical circulatory support, limited data are available on prognosisof cardiogenic shock (CS) caused by various diseases. We investigated the characteristics and predictorsof in-hospital mortality in Korean CS patients.
Methods: The RESCUE study is a multi-center, retrospective and prospective registry of patients thatpresented with CS. Between January 2014 and December 2018, 1,247 patients with CS were enrolledfrom 12 major centers in Korea. The primary outcome was in-hospital mortality.
Results: In-hospital mortality rate was 33.6%. The main causes of shock were ischemic heart disease(80.7%), dilated cardiomyopathy (6.1%), myocarditis (3.2%), and non-ischemic ventricular arrhythmia(2.5%). Vasopressors were used in 1081 patients (86.7%). The most frequently used vasopressor wasdopamine (63.4%) followed by norepinephrine (57.3%). An intra-aortic balloon pump was used in 314patients (25.2%) and extracorporeal membrane oxygenator in 496 patients (39.8%). In multi-variableanalysis, age ≥70 years, cardiac arrest at presentation, vasoactive-inotrope score >80, continuous renalreplacement therapy, and mechanical ventilator were independent predictors for in-hospital mortality.
Conclusions: The in-hospital mortality of CS patients remains high despite the high utilization ofmechanical circulatory support. Age, cardiac arrest at presentation, amount of vasopressor, andadvanced organ failure were poor prognostic factors for in-hospital mortality.
Trial registration: RESCUE registry, Clinicaltrials.gov, NCT02985008, Registered 01 January 2014 -Retrospectively and Prospectively registered
https://clinicaltrials.gov/ct2/show/NCT02985008.
IntroductionCardiogenic shock (CS) is a circulatory failure related to insu�cient supply of oxygen to tissues mainlydriven by low cardiac output. Acute myocardial infarction (AMI) was reported to be the most commoncause. In-hospital mortality of CS patients has decreased in recent years but remains high.(1) Inparticular, refractory CS, which refers to persistent shock despite appropriate volume resuscitation or useof inotropes or vasopressors, is lethal in more than half of hospitalized patients.(2) Recent advances oftemporary mechanical hemodynamic support for patients with CS refractory to conventional medicaltherapy are expected to improve patient survival. However, a large-scale, randomized controlled trialshowed that routine use of intra-aortic balloon pump (IABP) as the most popular mechanical circulatorysupport (MCS) did not improve survival in CS patients with complicating AMI.(3) However, advanced MCSdevices such as Impella and extracorporeal membrane oxygenator (ECMO) showed favorable outcomesin several registries.(4, 5) Although several randomized controlled trials showed the bene�t of earlycoronary intervention and some medication strategies,(6, 7) current therapeutic strategies remainempirical and not evidence-based in CS patients.(8) Therefore, we conducted the RESCUE registry to

Page 4/23
investigate overall characteristics and predictors of clinical outcomes regarding e�cacy and safety ofcontemporary practices in CS patients.
Methods
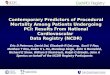
Study PopulationThe RESCUE (REtrospective and prospective observational Study to investigate Clinical oUtcomes andE�cacy of left ventricular assist device for Korean patients with cardiogenic shock, NCT02985008 atwww.clinicaltrials.gov) study is a multi-center registry of patients with CS aged over 19 years. A total of1,247 patients from 12 tertiary centers between January 2014 and December 2018 was enrolled (Fig. 1).More detailed information regarding prospective and retrospective enrollments of each institute is shownin Supplementary Table 1. The inclusion criteria were as follows: 1) systolic blood pressure < 90 mmHgfor 30 minutes or need for inotrope or vasopressor support to achieve a systolic blood pressure > 90 mmHg and 2) presence of pulmonary congestion and signs of impaired organ perfusion (alteredmental status, cold periphery, oliguria < 0.5 mL/kg/h for the previous 6 h, or blood lactate > 2 mmol/L).Exclusion criteria were (1) out-of-hospital cardiac arrest and (2) evidence of septic or hypovolemic shock.
Data Collection and OutcomesData were collected using a web-based case record form. Additional information was obtained frommedical records or by telephone contact, if necessary. The primary outcome was in-hospital mortality.The secondary outcome was altered neurological status upon discharge from the hospital, as assessedby the Glasgow-Pittsburgh Cerebral Performance Categories (CPC) scale (scores range from 1 to 5) (9).CPC scores of 1 and 2 were classi�ed as favorable neurological outcomes, while CPC scores of 3, 4, and5 were considered poor neurological outcomes. All-cause mortality was de�ned as death from any cause.The institutional review board of each hospital approved the study protocol and waived the requirementfor written informed consent for patients enrolled in the retrospective registry. We obtained informedconsent from the patients enrolled for prospective registry.
Statistical AnalysisCategorical variables were tested using the Chi-square test or Fisher’s exact test, as appropriate, andpresented as number and relative frequency. Continuous variables were compared the using Student’s t-test and presented as mean ± standard deviation or median (25th – 75th percentile). A multi-variable Coxregression analysis was used to identify the predictors of in-hospital mortality in CS patients. Forpractical purpose, continuous variables were transformed into categorical variables, which were assessedby normal range or cut-off value as determined in previous studies. The covariates considered clinicallyrelevant or that showed a univariate relationship with outcome (p ≤ 0.2) were entered into a multi-variableregression model. Clinically inter-correlated variables were excluded from the model. Statistical analyseswere performed using R Statistical Software (version 3.2.5; R Foundation for Statistical Computing,Vienna, Austria) with p < 0.05 considered statistically signi�cant.

Page 5/23
Results
Baseline CharacteristicsAmong the 1,293 patients enrolled in this study, 46 were excluded because of out-of-hospital cardiacarrest (n = 44) or withdrawal of consent (n = 2). Finally, 1,247 patients were analyzed for this study. Ofthem, 954 were enrolled retrospectively and 293 prospectively. A total of 419 patients (33.6%) died duringindex hospitalization. The characteristics of these patients are compared with those of other registries inTable 1.

Page 6/23
Table 1Clinical characteristics of patients hospitalized with cardiogenic shock in Korea compared with other
registriesVariables RESCUE SHOCK Trial CardShock Cardiovascular
Shock
Sample size 1,247 1,190 219 979
Region Korea USA Europe Japan
Time period January 2014-December 2018
April 1993 -August 1997
October 2010-December 2012
May 2012-June2014
Demographics
Age (years) 65.6 ± 13.8 68.7 ± 11.8 68 ± 11 70.3 ± 14.2
Male (%) 860 (69.0) 710 (59.7) 162 (74.0) 645 (65.9)
Body mass index(kg/m2)
23.4 ± 3.6 – 26.5 (24.2–29.0) –
Vital sign
Systolic bloodpressure (mmHg)
73.5 ± 29.1 87.7 ± 22.3 78 ± 14 78.2 ± 15.7
Diastolic bloodpressure (mmHg)
46.6 ± 19.9 52.3 ± 17.0 47 ± 10 –
Heart rate (beats/min) 82.8 ± 34.2 95.7 ± 26.2 90 ± 28 73.0 ± 48.7
Cardiac arrest aspresentation
268 (21.5) – 62 (28.3) –
Comorbidities
Diabetes mellitus 443 (35.5) 388 (32.6) 62 (28.3) 252 (25.7)
Hypertension 660 (52.9) 632 (53.1) 132 (60.3) 545 (55.7)
Dyslipidemia 330 (26.5) 497 (41.8) – 274 (28.0)
Current smoker 356 (28.5) 596 (50.1) 87 (39.7) 278 (28.4)
Chronic kidneydisease
123 (9.9) 130 (10.9) 25 (11.4) –
Peripheral arterialocclusive disease
52 (4.2) 213 (17.9) – –
Prior myocardialinfarction
160 (12.8) 445 (37.4) 54 (24.7) –
Prior cerebrovascularaccident
119 (9.5) – 20 (9.1) –

Page 7/23
Variables RESCUE SHOCK Trial CardShock CardiovascularShock
Acute coronarysyndrome
894 (75.1) 1190 (100) 177 (80.8) 499 (51.0)
Left ventricularejection fraction, %
35.9 ± 16.3 32.6 ± 13.8 33 ± 14 45.0 (30.0–60.0)
Laboratory
Hemoglobin (g/dL) 12.7 ± 2.6 12.9 ± 2.5 12.8 ± 2.2 –
Serum creatinine(mg/dL)
1.6 ± 1.4 1.4 ± 1.4 1.0 (0.8–1.4) –
Glucose (mg/dL) 223 ± 119 208 ± 105 250 ± 139 –
Lactate (mmol/L) 6.5 ± 4.7 5.4 ± 3.9 2.8 (1.7–5.8) –
Managements
Vasopressor 1,081 (86.7) – – –
Mechanical ventilator 709 (56.9) – – –
Continuous renalreplacement therapy
285 (22.9) – – –
Intra-aortic balloonpump
314 (25.2) – – –
Extracorporealmembrane oxygenator
496 (39.8) – – –
In-hospital mortality, % 419 (33.6) 731 (61.4) 80 (36.5)
30-day mortality, % 336 (34.3)
The main causes of shock were ischemic heart disease (80.7%), dilated cardiomyopathy (6.1%),myocarditis (3.2%), and non-ischemic ventricular arrhythmia (2.5%). Baseline characteristics are shown inTable 2. Compared with survivors, non-survivors were older and had lower body mass index, systolicblood pressure, diastolic blood pressure, left ventricular ejection fraction, and hemoglobin but higheraspartate transaminase, serum creatinine, glucose, and lactate levels. Furthermore, non-survivors had ahigher incidence of comorbidities such as diabetes mellitus, hypertension, chronic kidney disease, andprior MI and were more often female, showed cardiac arrest at presentation, and had an ischemic cause.

Page 8/23
Table 2Baseline patient characteristics
Variables Overall
(n = 1247)
Survivors
(n = 828)
Non-survivors
(n = 419)
p-value
Age (years) 65.6 ± 13.8 64.0 ± 13.7 68.8 ± 13.6 < 0.001
Male 860 (69.0) 588 (71.0) 272 (64.9) 0.028
Body mass index (kg/m2) 23.4 ± 3.6 23.6 ± 3.6 23.1 ± 3.4 0.038
Systolic blood pressure (mmHg) 73.5 ± 29.1 76.6 ± 27.2 67.1 ± 31.7 < 0.001
Diastolic blood pressure (mmHg) 46.6 ± 19.9 48.6 ± 19.0 42.6 ± 21.1 < 0.001
Heart rate (beats/min) 82.8 ± 34.2 82.8 ± 32.0 82.8 ± 38.3 0.992
Cardiac arrest as presentation 268 (21.5) 102 (12.3) 166 (39.6) < 0.001
Clinical presentation
Ischemic cause 1006 (80.7) 666 (80.4) 340 (81.1) 0.764
ST-segment elevation MI 355 (42.9) 355 (42.9) 202 (48.2) 0.073
Comorbidities
Diabetes mellitus 443 (35.5) 270 (32.6) 173 (41.3) 0.002
Hypertension 660 (52.9) 419 (50.6) 241 (57.5) 0.021
Dyslipidemia 330 (26.5) 227 (27.4) 103 (24.6) 0.284
Current smoker 356 (28.5) 262 (31.6) 94 (22.4) 0.001
Chronic kidney disease 123 (9.9) 58 (7.0) 65 (15.5) < 0.001
Peripheral arterial occlusive disease 52 (4.2) 30 (3.6) 22 (5.3) 0.174
Prior MI 160 (12.8) 95 (11.5) 65 (15.5) 0.044
Prior cerebrovascular accident 119 (9.5) 70 (8.5) 49 (11.7) 0.066
Left ventricular ejection fraction, % 35.9 ± 16.3 39.2 ± 15.8 28.3 ± 14.8 < 0.001
Laboratory
Hemoglobin (g/dL) 12.7 ± 2.6 12.9 ± 2.5 12.2 ± 2.7 < 0.001
Platelets (x10³/µL) 211.0 ± 81.5 217.6 ± 80.4 197.9 ± 82.2 < 0.001
Values are mean ± standard deviation or n (%).
MI, myocardial infarction; NT-proBNP, N-terminal pro b-type natriuretic peptide

Page 9/23
Variables Overall
(n = 1247)
Survivors
(n = 828)
Non-survivors
(n = 419)
p-value
Total bilirubin (mg/dL) 1.0 ± 1.8 1.0 ± 1.9 1.1 ± 1.6 0.501
Aspartate transaminase (U/L) 257 ± 990 210 ± 891 348 ± 1154 0.022
Alanine transaminase (U/L) 144 ± 462 128 ± 464 177 ± 456 0.080
Serum creatinine (mg/dL) 1.6 ± 1.4 1.4 ± 1.4 1.8 ± 1.4 < 0.001
Glucose (mg/dL) 223 ± 119 208 ± 105 250 ± 139 < 0.001
Lactate (mmol/L) 6.5 ± 4.7 5.4 ± 3.9 8.4 ± 5.2 < 0.001
Values are mean ± standard deviation or n (%).
MI, myocardial infarction; NT-proBNP, N-terminal pro b-type natriuretic peptide
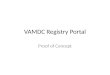
In-hospital Management and OutcomesIn-hospital management procedures are shown in Table 3. Vasopressors were used in 1081 patients(86.7%). The most frequently used vasopressor was dopamine (63.4%) followed by norepinephrine(57.3%). MCS was used in 745 patients (59.7%), while IABP was used in 314 patients (25.2%) and ECMOin 496 patients (39.8%). Combined implementation of IABP and ECMO was performed in 29 patients(2.3%). Compared with survivors, non-survivors received more extracorporeal CPR and had higher of useof dopamine, epinephrine, norepinephrine, mechanical ventilator, continuous renal replacement therapy,IABP, and ECMO. Vasoactive-inotropic score was also higher in non-survivors. Kaplan-Meier curvesshowed favorable survival in non-arrest patients (vs. arrest patients) and those with vasoactive inotropescore < 80 (vs. ≥ 80), BMI < 25 kg/m2 (vs. ≥ 25 kg/m2), and lactate < 8 mmol/L (vs. ≥ 8 mmol/L) (Fig. 2).

Page 10/23
Table 3In-hospital management methods
Variables Overall
(n = 1247)
Survivors
(n = 828)
Non-survivors
(n = 419)
p-value
Dopamine 790 (63.4) 496 (59.9) 294 (70.2) < 0.001
Epinephrine 86 (6.9) 30 (3.6) 56 (13.4) < 0.001
Norepinephrine 715 (57.3) 405 (48.9) 310 (74.0) < 0.001
Vasoactive-Inotropic Score 73.4 ± 136.5
46.0 ± 124.3
127.5 ± 143.4
< 0.001
Mechanical ventilator 709 (56.9) 347 (41.9) 362 (86.4) < 0.001
Continuous renal replacement therapy 285 (22.9) 89 (10.7) 196 (46.8) < 0.001
Intra-aortic balloon pump 314 (25.2) 193 (23.3) 121 (28.9) 0.032
Extracorporeal membrane oxygenator 496 (39.8) 239 (28.9) 257 (61.3) < 0.001
Extracorporeal cardiopulmonaryresuscitation
240 (19.2) 81 (9.8) 159 (37.9) < 0.001
ICU stay, days 11.6 ± 23.7 11.7 ± 22.3 11.2 ± 26.2 0.683
Hospital stay, days 19.2 ± 29.5 21.9 ± 29.4 13.8 ± 29.0 < 0.001
Values are mean ± standard deviation or n (%).
ICU, intensive care unit
Among 496 patients treated with ECMO, 406 received a percutaneous approach (81.9%), a distalperfusion catheter was inserted in 187 (37.7%), and left heart decompression was present in 26 (5.2%). Inaddition, 240 patients (48.4%) received extracorporeal cardiopulmonary resuscitation, and the medianCPR to pump-on time was 31 minutes (interquartile range; 15–49), while the shock to ECMO time was 86minutes (42–261). Successful weaning was achieved in 266 patients (53.6%), and those who survived todischarge numbered 239 (48.2%).
Of survivors, poor neurologic outcome was noted in 39 (4.7%), 10 with CPC 4 (1.2%) and 29 with CPC 3(3.5%). Good neurologic outcome was noted in 58 patients with CPC 2 (7.0%) and 731 with CPC 1(88.3%).

Page 11/23
Predictors of In-hospital MortalityIn multi-variable analysis, age ≥ 70 years, cardiac arrest at presentation, vasoactive-inotrope score > 80,continuous renal replacement therapy, and mechanical ventilator were independent predictors for in-hospital mortality (Table 4).

Page 12/23
Table 4Predictors for in-hospital mortality
Multi-variable analysis
Adjusted HR 95% CI p-value
Age ≥ 70 years 1.71 1.33–2.20 < 0.001
Sex, male 0.82 0.64–1.03 0.091
Body mass index, kg/m2 1.00 0.97–1.03 0.833
Cardiac arrest at presentation 1.51 1.17–1.95 0.002
Ischemic etiology 1.25 0.94–1.66 0.134
Hypertension 1.06 0.84–1.35 0.617
Diabetes mellitus 0.99 0.78–1.27 0.955
Current smoking 0.90 0.68–1.19 0.451
Prior history of chronic kidney disease 1.02 0.75–1.39 0.910
Prior history of myocardial infarction 0.96 0.72–1.29 0.789
Hemoglobin, g/dL 1.04 0.99–1.09 0.077
Serum glucose, g/dL 1.00 1.00–1.00 0.083
Transaminase > 1000 U/L 1.45 0.93–2.25 0.098
Vasoactive-inotrope score > 80 2.11 1.70–2.61 < 0.001
Continuous renal replacement therapy 1.54 1.23–1.93 < 0.001
Mechanical ventilator 2.32 1.66–3.23 < 0.001
Intra-aortic balloon pump 1.27 0.99–1.63 0.055
Extracorporeal membrane oxygenator 1.22 0.92–1.61 0.167
CI, con�dence interval; HR, hazard ratio
Adjusted variables are age ≥ 70 years, sex, body mass index, cardiac arrest at presentation, ischemicetiology, hypertension, diabetes mellitus, current smoking, prior history of chronic kidney disease andmyocardial infarction, hemoglobin, glucose level, transaminase > 1000 U/L, vasoactive-inotrope score > 80, continuous renal replacement therapy, mechanical ventilator, intra-aortic balloon pump, andextracorporeal membrane oxygenator.
DiscussionWe investigated clinical characteristics and predictors of clinical outcomes in CS patients treated withcontemporary management from a large-scale, multi-center registry. This study demonstrated the actual

Page 13/23
state of CS in Korea. The major �ndings of this study were: (1) in-hospital mortality of CS patientsremains high, (2) dopamine and norepinephrine were used as �rst-line vasopressors, (3) more than half ofthe patients required MCS devices, and (4) old age, cardiac arrest, high-dose vasopressor, and organfailure were independent predictors of in-hospital mortality.
Cardiogenic shock is a critical illness with a very high rate of fatality. However, most treatment modalitieshave been tested only empirically with no solid supporting evidence because randomized controlled trialsare very di�cult to perform in this vulnerable patient subset. For example, over 20 years, there have beenonly three major randomized controlled trials, mostly in the AMI patients. The Should We EmergentlyRevascularize Occluded Coronaries for Cardiogenic Shock (SHOCK) trial established the role of earlycoronary revascularization in AMI patients complicated by CS (10). The Intra-aortic Balloon Pump inCardiogenic Shock II (IABP-SHOCK II) trial showed that routine IABP did not reduce patient mortality. TheCulprit Lesion Only PCI versus Multivessel PCI in Cardiogenic Shock (CULPRIT-SHOCK) trial showed thatmulti-vessel PCI did improve clinical outcome.(11, 12)
On the contrary, the registry studies cover a variety of causes of CS. However, those previous studies wererelatively small in sample size or were associated with a lower rate of MCS device use, which does notre�ect current practice. The CardShock study, a European, multi-center registry, was conducted between2010 and 2012 but included only 219 patients, 13 of whom were treated with ventricular assist device orECMO. (13–15) The Japanese Circulation Society Cardiovascular Shock registry conducted between2012 and 2014 was the largest registry of CS, enrolling 979 patients, (16) but that study did not collectinformation on vasopressor or MCS usage. The RESCUE study is the largest multi-center, real-worldregistry of CS patients with a broad spectrum of etiologies. More than half of enrolled patients havereceived either IABP or ECMO, representing contemporary management of more severe forms of CS. Still,in this study, a total of 419 patients (33.6%) died at index hospitalization, which is consistent with the30–40% mortality reported in other studies performed in the early 2010s. These �ndings suggest that themortality rate of AMI patients complicated by CS may plateau over time despite introduction of newdevices and techniques improving coronary artery revascularization. Further, bene�cial hemodynamicsupport may be masked by MCS-related complications such as limb ischemia, systemic embolization,and fatal bleeding in CS patients treated with MCS.
The prognostic factors found in this study were consistent with those reported in previous studies.Indices of organ failure such as acute kidney injury requiring continuous renal replacement therapy andrespiratory failure requiring mechanical ventilator were signi�cant prognostic factors for in-hospitalmortality.(15, 16) Cardiac arrest was also a prognostic factor for in-hospital mortality. Our group showedthat extracorporeal cardiopulmonary resuscitation had a survival bene�t over the conventional approachused in a previous study.(17) Future research regarding optimal strategy of extracorporealcardiopulmonary resuscitation is needed to improve the mortality rate seen with this RESCUE registry.High vasoactive-inotrope score was a powerful indicator of in-hospital mortality in this study. Recently,our group showed that a high level of vasoactive inotropic support during the �rst 48 hours wassigni�cantly associated with increased in-hospital mortality in adult CS patients.(18) Basically, inotropes

Page 14/23
or vasopressors can improve hemodynamics in the acute stage through increased myocardialcontractility or modi�cation of vascular tone. However, these agents can also be related to adversecardiovascular events such as hypertension/hypotension, arrhythmias, peripheral, and cardiac ischemia,which may be fatal.(19) Accordingly, the decision whether to increase vasopressor dosage or applyadvanced MCS in patients who have already received high-dose vasopressor should be carefully weighedafter considering a risk-bene�t analysis.
LimitationsOur study has several limitations. First, most patients presented with an ischemic etiology, and patientswith non-ischemic cause were heterogeneous and of limited sample size. Second, this registry did notinclude all mechanical circulatory support because Impella is not currently available in Korea. Third,treatment of CS such as type and amount of �uids and vasopressor/inotropes administered and type andtiming of MCS were left to the physician’s discretion, although coronary intervention was based on theguidelines of the Korean Circulation Society.
ConclusionsThe in-hospital mortality of CS patients remains high despite high utilization of MCS. Age, cardiac arrestat presentation, amount of vasopressor, and advanced organ failure were poor prognostic factors for in-hospital mortality.
AbbreviationsAMI = Acute myocardial infarction
BMI = Body mass index
CI = Con�dence interval
CPC = Cerebral performance categories
CS = Cardiogenic shock
ECMO = Extracorporeal membrane oxygenator
IABP = Intra-aortic balloon pump
DeclarationsEthical Approval and Consent to participate

Page 15/23
The institutional review board of each hospital approved the study protocol and waived the requirementfor written informed consent for patients enrolled in the retrospective registry. We obtained informedconsent from the patients enrolled for prospective registry.
Availability of supporting data
The data that support the �ndings of this study are available from [Hyeon-Cheol Gwon] but restrictionsapply to the availability of these data, which were used under license for the current study, and so are notpublicly available. Data are however available from the authors upon reasonable request and withpermission of [Hyeon-Cheol Gwon].
Competing interests
The authors declare that they have no competing interests.
Funding: None
Authors' contributions
JHY collected data, conceived of the study, and contributed to interpretation of the data as well as todrafting the manuscript. KHC performed analysis and interpretation of the data and drafted themanuscript. Y-GK collected data and made critical revision of the manuscript for key intellectual content.C-MA collected data and made critical revision of the manuscript for key intellectual content. CWYcollected data and made critical revision of the manuscript for key intellectual content. WJC collecteddata and made critical revision of the manuscript for key intellectual content. WJJ collected data andmade critical revision of the manuscript for key intellectual content. H-JK collected data and made criticalrevision of the manuscript for key intellectual content. BSK collected data and made critical revision ofthe manuscript for key intellectual content. J-WB collected data and made critical revision of themanuscript for key intellectual content. SYL collected data and made critical revision of the manuscriptfor key intellectual content. SUK collected data and made critical revision of the manuscript for keyintellectual content. H-JL collected data and made critical revision of the manuscript for key intellectualcontent. WSL collected data and made critical revision of the manuscript for key intellectual content. J-OJcollected data and made critical revision of the manuscript for key intellectual content. S-DP collecteddata and made critical revision of the manuscript for key intellectual content. S-HL collected data andmade critical revision of the manuscript for key intellectual content. SC collected data and made criticalrevision of the manuscript for key intellectual content. TKP collected data and contributed tointerpretation of the data as well as to drafting the manuscript. JML collected data and contributed tointerpretation of the data as well as to drafting the manuscript. YBS collected data and contributed tointerpretation of the data as well as to drafting the manuscript. J-YH collected data and contributed tointerpretation of the data as well as to drafting the manuscript. H-CG collected data and supervised theinterpretation of the data as well as the drafting of the manuscript.
Acknowledgements: None

Page 16/23
Consent for Publication
The Author hereby grants the Publisher permission to publish the work.
References1. Kolte D, Khera S, Aronow WS, et al: Trends in incidence, management, and outcomes of cardiogenic
shock complicating ST-elevation myocardial infarction in the United States. J Am Heart Assoc 2014;3:e000590
2. Takayama H, Truby L, Koekort M, et al: Clinical outcome of mechanical circulatory support forrefractory cardiogenic shock in the current era. J Heart Lung Transplant 2013; 32:106-111
3. Thiele H, Zeymer U, Neumann FJ, et al: Intra-aortic balloon counterpulsation in acute myocardialinfarction complicated by cardiogenic shock (IABP-SHOCK II): �nal 12 month results of arandomised, open-label trial. Lancet 2013; 382:1638-1645
4. Kormos RL, Cowger J, Pagani FD, et al: The Society of Thoracic Surgeons Intermacs databaseannual report: Evolving indications, outcomes, and scienti�c partnerships. J Heart Lung Transplant2019; 38:114-126
5. Shin TG, Choi JH, Jo IJ, et al: Extracorporeal cardiopulmonary resuscitation in patients withinhospital cardiac arrest: A comparison with conventional cardiopulmonary resuscitation. Crit CareMed 2011; 39:1-7
�. Hochman JS, Sleeper LA, Webb JG, et al: Early revascularization in acute myocardial infarctioncomplicated by cardiogenic shock. SHOCK Investigators. Should We Emergently RevascularizeOccluded Coronaries for Cardiogenic Shock. N Engl J Med 1999; 341:625-634
7. De Backer D, Biston P, Devriendt J, et al: Comparison of dopamine and norepinephrine in thetreatment of shock. N Engl J Med 2010; 362:779-789
�. van Diepen S, Katz JN, Albert NM, et al: Contemporary Management of Cardiogenic Shock: AScienti�c Statement From the American Heart Association. Circulation 2017; 136:e232-e268
9. Cummins RO, Chamberlain DA, Abramson NS, et al: Recommended guidelines for uniform reportingof data from out-of-hospital cardiac arrest: the Utstein Style. A statement for health professionalsfrom a task force of the American Heart Association, the European Resuscitation Council, the Heartand Stroke Foundation of Canada, and the Australian Resuscitation Council. Circulation 1991;84:960-975
10. Hochman JS, Buller CE, Sleeper LA, et al: Cardiogenic shock complicating acute myocardialinfarction--etiologies, management and outcome: a report from the SHOCK Trial Registry. SHould weemergently revascularize Occluded Coronaries for cardiogenic shocK? J Am Coll Cardiol 2000;36:1063-1070
11. Thiele H, Zeymer U, Neumann FJ, et al: Intraaortic balloon support for myocardial infarction withcardiogenic shock. N Engl J Med 2012; 367:1287-1296

Page 17/23
12. Thiele H, Akin I, Sandri M, et al: PCI Strategies in Patients with Acute Myocardial Infarction andCardiogenic Shock. N Engl J Med 2017; 377:2419-2432
13. Kataja A, Tarvasmaki T, Lassus J, et al: Altered mental status predicts mortality in cardiogenic shock- results from the CardShock study. Eur Heart J Acute Cardiovasc Care 2018; 7:38-44
14. Kataja A, Tarvasmaki T, Lassus J, et al: The association of admission blood glucose level with theclinical picture and prognosis in cardiogenic shock - Results from the CardShock Study. Int J Cardiol2017; 226:48-52
15. Harjola VP, Lassus J, Sionis A, et al: Clinical picture and risk prediction of short-term mortality incardiogenic shock. Eur J Heart Fail 2015; 17:501-509
1�. Ueki Y, Mohri M, Matoba T, et al: Characteristics and Predictors of Mortality in Patients WithCardiovascular Shock in Japan- Results From the Japanese Circulation Society CardiovascularShock Registry. Circ J 2016; 80:852-859
17. Shin TG, Jo IJ, Sim MS, et al: Two-year survival and neurological outcome of in-hospital cardiacarrest patients rescued by extracorporeal cardiopulmonary resuscitation. Int J Cardiol 2013;168:3424-3430
1�. Na SJ, Chung CR, Cho YH, et al: Vasoactive Inotropic Score as a Predictor of Mortality in AdultPatients With Cardiogenic Shock: Medical Therapy Versus ECMO. Rev Esp Cardiol (Engl Ed) 2019;72:40-47
19. Overgaard CB, Dzavik V: Inotropes and vasopressors: review of physiology and clinical use incardiovascular disease. Circulation 2008; 118:1047-1056
Figures

Page 18/23
Figure 1
A �ow diagram showing selection of study patients.

Page 19/23
Figure 1
A �ow diagram showing selection of study patients.

Page 20/23
Figure 1
A �ow diagram showing selection of study patients.

Page 21/23
Figure 2
Kaplan-Meier curves for all causes of death during the 90-day follow-up. (A) Cardiac arrest (blue line)versus non-arrest (red line). (B) VIS ≥ 80 (blue line) versus < 80 (red line). (C) BMI ≥ 25 kg/m2 (blue line)versus < 25 kg/m2 (red line). (D) Lactate ≥ 8 mmol/L (blue line) versus < 8 mmol/L (red line).

Page 22/23
Figure 2
Kaplan-Meier curves for all causes of death during the 90-day follow-up. (A) Cardiac arrest (blue line)versus non-arrest (red line). (B) VIS ≥ 80 (blue line) versus < 80 (red line). (C) BMI ≥ 25 kg/m2 (blue line)versus < 25 kg/m2 (red line). (D) Lactate ≥ 8 mmol/L (blue line) versus < 8 mmol/L (red line).

Page 23/23
Figure 2
Kaplan-Meier curves for all causes of death during the 90-day follow-up. (A) Cardiac arrest (blue line)versus non-arrest (red line). (B) VIS ≥ 80 (blue line) versus < 80 (red line). (C) BMI ≥ 25 kg/m2 (blue line)versus < 25 kg/m2 (red line). (D) Lactate ≥ 8 mmol/L (blue line) versus < 8 mmol/L (red line).
Supplementary Files
This is a list of supplementary �les associated with this preprint. Click to download.
Additional�le1.docx
Additional�le1.docx
Additional�le1.docx