Embed Size (px)
DESCRIPTION
A compilation of outcomes for the respy module
Citation preview

Respiratory Disease
Disease in General
1. Recognize the main presenting signs and symptoms associated with respiratory diseases
Disease Aetiology SymptomsAsthma Generally idiopathic but attacks can be
brought on by Allergens Emotional stress and fatigue Endocrine changes Temperatures and humidity changes Exercise Some drugs and chemicals
Coughing/wheezing Dyspnea Chest tightness Rapid breathing Difficulty in speaking Cyanosis Breathing difficulty Persistent cough
COPD Smoking Recurrent or chronic respiratory
infections Exposure to pollutants and
occupational chemicals Allergens Inherited factors
Breathing difficulty Wheezing Shortness of breath Breathlessness after
exercise Cyanosis Barrel-chestedness Clubbing
Influenza Influenza type A or type B. Usually type A. Headache Febrile Chills Rhinorrhea Sore throat Joint and muscle pain Loss of appetite Fatigue Malaise
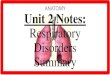
Emphysema Smoking COPD Chronic bronchitis Inherited factors – Lack of α-1
antitrypsin Pneumoconiosis
Breathing difficulty Wheezing Dyspnea Exertion dyspnea Cyanosis Barrel-chestedness Clubbing
Lung cancer Smoking Metastases seeded onto the lung
(common occurance) Exposure to carcinogenic industrial
and/or air pollutants
Chronic coughing, worsening
Haemoptysis Chronic chest pain Fever Dyspnea Wheezing Hoarseness Chest pain
Loss of appetite Weight loss Malaise Fatigue
Pneumoconiosis Inhalation of toxic minerals: Coal dust Abestos Silicon Tin/barium/iron oxide
Asymptomatic, or: Lung fibrosis Dyspnea Cough Chest pain Cyanosis Increased chance of
LRTIsCystic fibrosis Due to an autosomal recessive disease
resulting from mutations in a gene located on chromosome 7, which encodes for the CF-CL ion channel. This changes the ion balance in fluids which results in very much increased viscosity of bronchial mucous.
Chronic productive cough with thick mucous
Recurrent lung infections
Bronchiectasis Associated non-
respiratory diseases
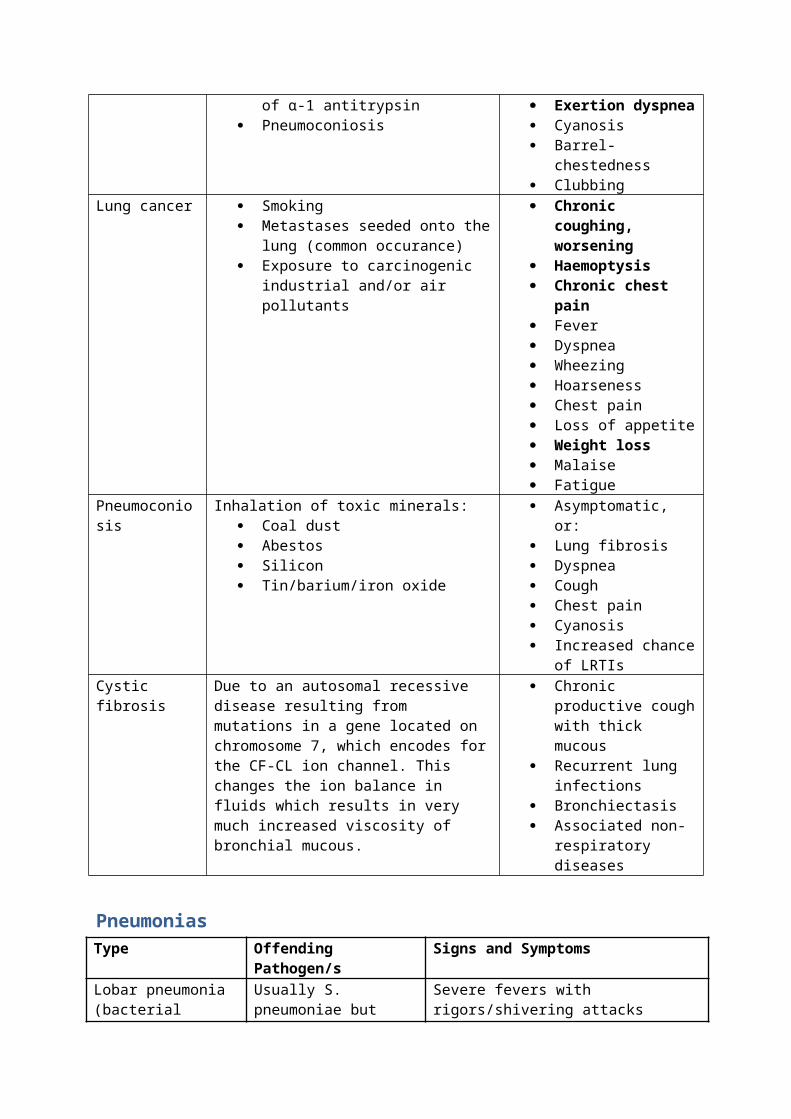
PneumoniasType Offending Pathogen/s Signs and Symptoms Lobar pneumonia (bacterial pneumonia usually split into lobar and broncho)
Usually S. pneumoniae but plenty of others
Severe fevers with rigors/shivering attacks Cough with rusty blood-stained sputum during red hepatisation stage Difficulty in breathingPossible pleurisy, sharp pain on coughing or on deep inspiration and pleural friction rub 7-10 days duration without antibiotics Antibiotic therapy – rapid cure
Bronchopneumonia Wider variety of bugs Staph /Strep Pneumococci H. influenzae P. aeruginosa Coliform bacteria
Seen in very young and very old Often accompanies other illnesses Septicaemic and toxic Green sputum High temperature Crackles at affected areas of lung
Atypical Virus – influenza most common. Others include measles, CMV, VZV
Mycoplasma Legionella Chlamydophila
Often follows URTI Sore throat, dry cough, fever, malaise, Pleuritic chest pain – sharp or stabbing Loss of appetite, anorexia, weight loss nausea, vomiting and abdominal pain
Aspiration Stroke Myasthenia Bulbar palsies ↓ consciousness Oesophageal disease
Similar to bronchopneumonia
Poor oral hygiene
2. Describe and demonstrate the process of taking a respiratory history and conducting a respiratory examination
Respiratory History Taking
1. Presenting symptoms Cough: acute or chronic; any medication is taken that may cause coughing; times when they are coughing; amount and type of sputum produced.
Dyspnoea: when it occurs; the amount of exertion required to trigger dyspnoea; duration and variability
Chest pain: SOCRATES
2. Past history Previous respiratory illnesses and past respiratory investigations, such as bronchoscopy or spirometry.
3. Occupational history A practitioner should investigate the patient’s past and present occupation, exposure to animals including birds, mouldy hay, humidifiers or air conditioners. What the patient does at work, the duration of any exposure, use of protective devices and whether other workers have become ill should also be investigated.
4. Social history Smoking history should be routine with the practitioner asking the quantity of cigarettes smoked and how long the patient’s have been smoking for. Cigarette packets should be specified in regards to a packet of 20 cigarettes.
5. Family History A medical doctor should ask about a family history of asthma, cystic fibrosis, emphysema as well as family history of infection with tuberculosis.
Respiratory Examination
1. Positioning the patient The patient should be sitting upright on a chair or on a bed undressed down to the waist.
2. General Appearance Signs that should be looked for before a thorough investigation include:
Dyspnoea Cyanosis Character of the cough Sputum Stridor Hoarseness Whether accessory muscles of respiration and/or abdominal muscles are used Respiratory rate should be determined whilst counting the patient’s pulse
Breathing pattern should also be noted3. The Hand
Clubbing of the fingers Tar stains Wasting and weakness of the small muscles of the hand by asking the patient to abduct
and adduct their fingers against force. Pulse rate Flapping tremor can be observed by asking the patient to stretch their arms forward
and dorsiflex their hands and look for tremors of the hands in this position.4. The face
Inspect the eyes for constricted pupils, partial ptosis and loss of sweating (Horner’s Syndrome)
Inspect the inside of the nose Check for central cyanosis of the tongue and lips Check the mouth for upper respiratory tract infection by inspecting the tonsils and the
pharynx Palpate sinuses
5. The trachea Check that the trachea is midline by pushing the forefinger up and backwards from the
sternal notch until the trachea is felt. Must be gentle.6. The chest
Inspect the shape and symmetry of the chest anteriorly, posteriorly and laterally. Lesions and scars should also be inspected for Assess symmetry of chest wall movement anteriorly and posteriorly. Expansion of the
upper lobes is achieved by inspection from behind the patient, looking down at the clavicles.
7. Palpation Chest expansion assessment is achieved by placing the hands firmly on the chest wall
with the fingers extending around the sides of the chest. The thumbs should almost meet in the middle line and should be slightly off the chest for free movement.
When the patient is lying down establish the position of the apex beat. Vocal fremitus can be determined by placing each palm of the hand on each side of the
chest and asking the patient to say ‘ninety nine’ Gently compress the chest wall anteroposterioly and laterally Supraclavicular and cervical lymph nodes should also be palpated for any adenopathies.
8. Percussion Percuss each lobe of the lung comparing each side of the chest. This is done both
posteriorly and anteriorly. Do not forget to percuss under the axilla to assess the middle lobe.
9. Auscultation Listen to breath sounds over the respective lobes of the lung and compare each side. Observe the breathing sounds taking note of quality, intensity and if there are added
sounds Vocal resonance should be assessed during auscultation by asking the patient to say
‘ninety nine’10. The heart
JVP and the pulmonary component of S2 should be assessed
3. Describe the differential diagnosis for a person presenting with shortness of breath and/or cough.
When creating differential diagnosis it is essential to consider the most common diagnoses first.
The table below is formatted using the acronym ‘I VINDICATE AIDS’.
Inflammatory
Vascular/cardiac InfectiousNeoplastic Degenerative Idiopathic Congenital AutoimmuneTrauma Endocrine/metabolic
Allergic IatrogenicDrugs/toxins/poison Social/other
I have divided the differential diagnosis for a cough into acute cough and chronic cough sections. A chronic cough is defined in Taber’s Cyclopedic Medical Dictionary 20/e as “a cough that occurs daily for at least three weeks”.
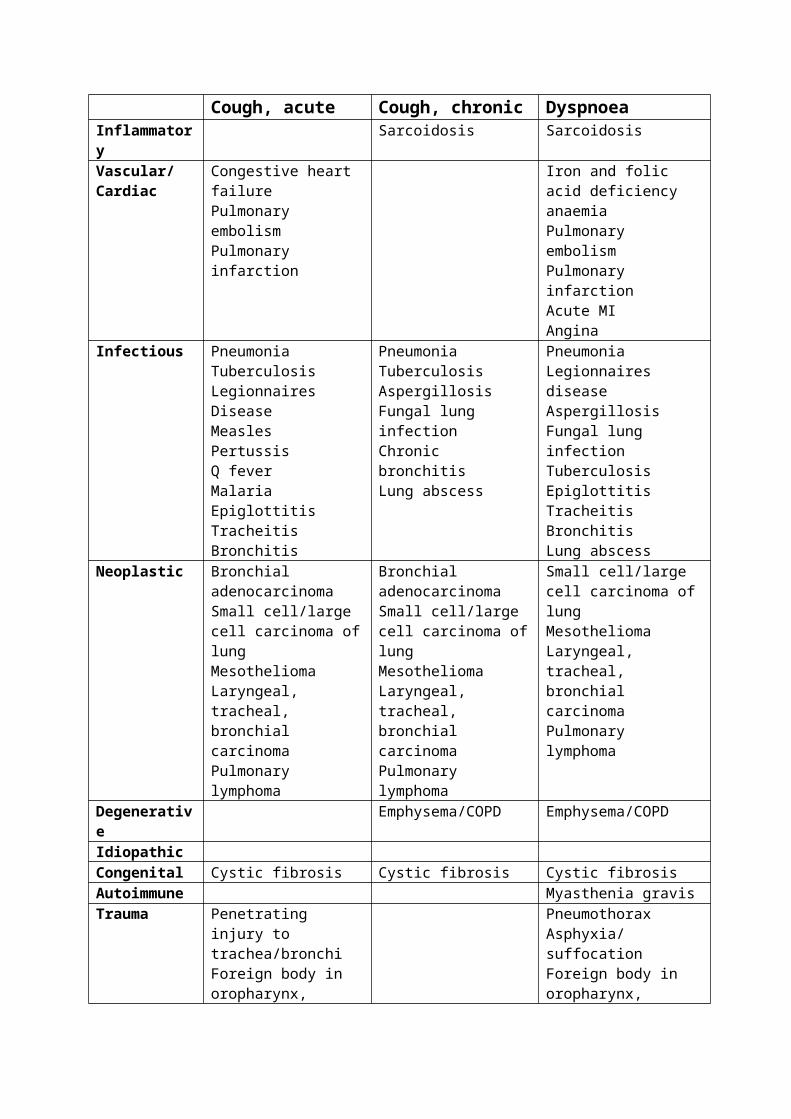
Cough, acute Cough, chronic DyspnoeaInflammatory Sarcoidosis Sarcoidosis Vascular/Cardiac
Congestive heart failurePulmonary embolismPulmonary infarction
Iron and folic acid deficiency anaemiaPulmonary embolismPulmonary infarctionAcute MIAngina
Infectious PneumoniaTuberculosisLegionnaires DiseaseMeaslesPertussisQ feverMalariaEpiglottitisTracheitisBronchitis
PneumoniaTuberculosisAspergillosisFungal lung infectionChronic bronchitisLung abscess
PneumoniaLegionnaires diseaseAspergillosisFungal lung infectionTuberculosisEpiglottitisTracheitisBronchitisLung abscess
Neoplastic Bronchial adenocarcinomaSmall cell/large cell carcinoma of lung
Bronchial adenocarcinomaSmall cell/large cell carcinoma of lung
Small cell/large cell carcinoma of lungMesotheliomaLaryngeal, tracheal,
Mesothelioma Laryngeal, tracheal, bronchial carcinomaPulmonary lymphoma
Mesothelioma Laryngeal, tracheal, bronchial carcinomaPulmonary lymphoma
bronchial carcinomaPulmonary lymphoma
Degenerative Emphysema/COPD Emphysema/COPDIdiopathicCongenital Cystic fibrosis Cystic fibrosis Cystic fibrosisAutoimmune Myasthenia gravisTrauma Penetrating injury to
trachea/bronchiForeign body in oropharynx, trachea, bronchi
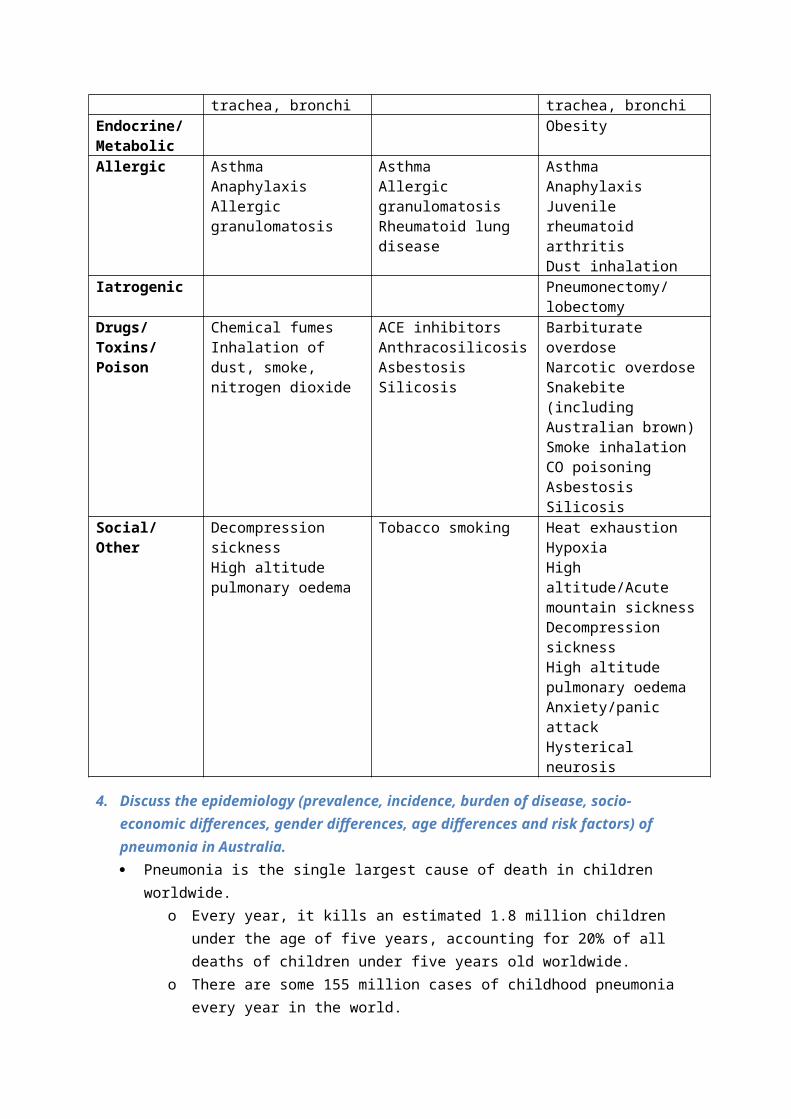
PneumothoraxAsphyxia/suffocationForeign body in oropharynx, trachea, bronchi
Endocrine/Metabolic
Obesity
Allergic AsthmaAnaphylaxisAllergic granulomatosis
AsthmaAllergic granulomatosisRheumatoid lung disease
AsthmaAnaphylaxisJuvenile rheumatoid arthritisDust inhalation
Iatrogenic Pneumonectomy/lobectomy
Drugs/Toxins/Poison
Chemical fumesInhalation of dust, smoke, nitrogen dioxide
ACE inhibitorsAnthracosilicosisAsbestosisSilicosis
Barbiturate overdoseNarcotic overdoseSnakebite (including Australian brown)Smoke inhalationCO poisoningAsbestosisSilicosis
Social/Other Decompression sicknessHigh altitude pulmonary oedema
Tobacco smoking Heat exhaustionHypoxiaHigh altitude/Acute mountain sicknessDecompression sicknessHigh altitude pulmonary oedemaAnxiety/panic attackHysterical neurosis
4. Discuss the epidemiology (prevalence, incidence, burden of disease, socio-economic differences, gender differences, age differences and risk factors) of pneumonia in Australia. Pneumonia is the single largest cause of death in children worldwide.
o Every year, it kills an estimated 1.8 million children under the age of five years, accounting for 20% of all deaths of children under five years old worldwide.
o There are some 155 million cases of childhood pneumonia every year in the world. o Pneumonia affects children and families everywhere, but is most prevalent in South
Asia and sub-Saharan Africa.
In the 2 years between July 2002 and June 2004 there were 47 870 hospitalisations for pneumonia in QLD, WA, SA and the NT combined.
o 14% of these were of ATSI people. o Of the total hospitalisations for ATSI people, 2.2% was for pneumonia. o Indigenous males and females had higher hospitalisation rates than non-indigenous
Australians across all age groups. o Hospitalisation is highest in all Australians among those aged 0-4 years and 65+
years. o Of the Indigenous Australians hospitalised for pneumonia:
Male rate/1000 = 17.0 Female rate/1000 = 14.5 Total rate/1000 = 15.7
o For non-indigenous Australians, hospitalisation for pneumonia: Male rate/1000 = 3.2 Female rate/1000 = 2.6 Total rate/1000 = 2.9
o Overall, the indigenous rates of hospitalisation are decreasing and non-indigenous rates have remained the same over the past 6 years up until 2004.
Pneumonia accounted for 2,550 registered deaths, or 1.8% of all registered deaths in 2007. o More females died from Pneumonia than males, with 1,415 female deaths
compared with 1,133 male deaths. o The median age at death for males was lower than for females, 84.6 years compared
with 89.0 years for females.
Risk Factors:
For Adults:
Age >65 years Alcoholism Cerebrovascular occlusions or neurologic impairment CHF Cirrhosis or chronic liver disease Dementia Diabetes mellitus Gastric acid suppression therapy (H2-antagonists and proton pump inhibitors) Immunocompromised state
Bone marrow transplantation Chronic lymphocytic leukemia Complement deficiency (especially C3 and C4 deficiency) Immunologic deficiency
Humoral (IgG or IgA) Cellular (eg, HIV/AIDS)
Multiple myeloma Splenic dysfunction or asplenia
Institutionalization and/or homelessness IV drug use Malignancy (especially lung tumors)
Nephrotic syndrome Recent antibiotic use or history of drug-resistant bacteria Respiratory conditions
Asthma Bronchiectasis Chronic obstructive pulmonary disease, including chronic bronchitis and/or emphysema Conditions associated with aspiration (eg, seizures, anesthesia, cerebrovascular disease) Cystic fibrosis Restrictive disease (eg, pulmonary fibrosis, neuromuscular conditions affecting the muscles of
respiration or deglutination) Tracheostomy
Smoking Viral illness (especially influenza)
For Children:
Anatomic defects such as cleft palate and tracheoesophageal fistula Asthma and allergic disorders Attendance at daycare centers Exposure to certain pathogens (eg, Legionella species, Mycobacterium tuberculosis) Frail children with chronic disease and repeated hospitalizations Gastroesophageal reflux (increases risk for aspiration pneumonia) General anesthesia History of transplantation or splenectomy Large family size Low socioeconomic status Malnutrition Passive exposure to cigarette smoke Prematurity, especially with respiratory distress syndrome Recurrent respiratory tract infection within the preceding 12 months Residence in urban or industrial communities (risk for RSV infection) Seasonal endemic infections Underlying disease, especially:
cancer cardiorespiratory (congenital heart disease, cystic fibrosis) chronic renal disease immune (HIV/AIDS) neuromuscular disorders.
Trauma
5. Describe the main characteristics of pneumonia Pneumonia = inflammation of the lung, usually caused by infection. Inflammatory exudate can spread through the lung unobstructed (due to spongy nature of
lungs), filling the alveoli with fluid and leading to consolidation.1 This can be seen on a chest X-ray.
Types of PneumoniaSeveral ways of classifying pneumonia, such as based on aetiology, anatomical location or by predisposing factors. There are over 30 causes of pneumonia, and knowing the cause is important as it dictates treatment.

Bacterial pneumonia.o Infection most commonly caused by streptococcus pneumonia in Aus. o Also can be caused by Klebsiella pneumoniae, Mycoplasma pneumoniae, Chlamydia
pneumonia, Haemophilus influenza, Legionella. Viral pneumonia.
o Infection caused by respiratory viruses. o Respiratory viruses normally cause URTI’s, but can cause pneumonia particularly in
children. o Viral pneumonia caused by the influenza virus can be severe and fatal.
Community Acquired Pneumonia (CAP). o Infection of the lungs that develops in a patient who “has not resided in a hospital or
healthcare facility in the previous 14 days”. o Most commonly caused by Streptococcus pneumoniae.
Hospital Acquired Pneumonia. o Infection that develops in a hospitalised patient, usually within the first 48 hours. o More common in those patients in an ICU, on a mechanical ventilator or who are
immunocompromised. Atypical pneumonia
o Several possible causes of atypical pneumonia: Mycoplasma
A mycoplasma is not a bacteria or virus, but has traits of both.2
Chlamydophila Legionella
Known as Legionnaire’s Disease. Caused by Legionella pneumophila (thrives in moist environments). Transmitted by inhaling water droplets with airborne organisms. Symptoms will also include diarrhoea, high fever, hyponatremia.
Lobar pneumonia o Infection of an entire lung lobe. o Caused by pathogenic bacteria.
Bronchopneumonia o Infection of one or more lobules (part of a lobe) adjacent to the bronchi. o Caused by pathogenic bacteria.
Postoperative pneumonia. o Infection that develops in a post-surgical patient who is unable to cough or breathe
deeply because of pain. o Leads to poor ventilation and the retention of secretions, leading to infection. o A subtype of hospital-acquired pneumonia.
Aspiration pneumonia. o Infection after food, vomit or a foreign object is inhaled into the lung. o Can be a result of excess alcohol intake, when the patient becomes unconscious and
vomits, and the vomit is aspirated into the lungs. Obstructive pneumonia.
o Infection in part of the lung distal to a narrowed or obstructed bronchus. o Bronchus may be blocked by tumour or foreign object. o Results in poor ventilation and the retention of secretions, leading to infection.
Signs and Symptoms Those of any systemic infection
Fever.
Tachypnoea. Shortness of breath. Cough. Purulent sputum. Chest pain. Shaking chills. Fatigue. If the pleura become inflamed, then pleuritic pain. Crackles or bronchial breath sounds on auscultation.
6. Discuss the relationship between cognitive impairment and physical illness including reference to delirium and dementia.
Cognitive impairment is described as a wide variety of impaired brain function relating to the ability of a person to think, concentrate, react to emotions, formulate ideas, solve problems, reason and remember.
Taking our first tutorial as an example, a relationship between cognitive impairment and physical illness can be observed. Our patient, Ivan, was diagnosed with pneumonia but during his recovery period, was suspected to have delirium and later, dementia. This describes a causative relationship between physical illness and cognitive impairment (i.e. physical illness cognitive impairment). Furthermore, Ivan had a history of a stroke which is also a major risk factor for various cognitive impairments.
However, cognitive impairment has also been reported to contribute to physical illness. For example, delirium is known to be a sign of problems ranging from electrolyte derangement or adverse drug effects to occult infection or less commonly disorder of the brain itself. Therefore, care should be taken in determining if delirium is a sign of an underlying physical illness.
Thus, the relationship between cognitive impairment and physical illness is not causative. Rather, it dictates what the biopsychosocial factors that proposes about a person’s wellbeing.
7. Discuss strategies aimed at reducing the impact of respiratory illness for at risk populations (focusing on children, the elderly and Indigenous populations).
Children
Whooping cough vaccine
Pertussis is a serious, contagious respiratory infection caused by the bacterium Bordetella pertussis. Whooping cough is particularly dangerous for babies aged less than six months. They are affected more seriously by the disease than older children or adults and are more likely to develop complications. One in every 200 babies who contract whooping cough will die. Immunisation is the best way to prevent whooping cough. A combined vaccine against whooping cough and other diseases is available under the National Immunisation Schedule. The vaccine should be given at:
Two, four and six months of age (diphtheria, tetanus, pertussis, hepatitis B, polio and haemophilus influenzae type b vaccine)
Four years of age (diphtheria, tetanus, pertussis and polio vaccine)
In Year 10 at secondary school – adolescents receive a booster dose of diphtheria, tetanus and pertussis vaccine.
Childhood flu vaccine campaign
In the Perth metropolitan area children aged from 6 months to 4 years of age will be eligible for free influenza vaccine this year. Children born after 1 April 2003 are eligible. This vaccine will be available from April 2008 from GPs. For those children not eligible for funded vaccine, vaccine can be purchased on script.
Elderly
Pneumonia vaccine
Pneumonia is a common condition in the elderly and can be quite serious if left untreated. The most affective form of prevention of pneumonia is immunisation. The NH&MRC Australian Immunisation Handbook recommends the influenza and pneumococcus vaccines for residents of aged care facilities to reduce the prevalence of this infection. The Victorian State Government, Department of Human Services provides pneumococcal vaccine free for people over 65 years and Aboriginal & Torres Strait Islander people over 50 years.
COPDX Guidelines
The Australian Lung Foundation has created a set of COPDX guidelines for practitioners that aim to shift the reliance of management of COPD from pharmaceuticals to a range of interventions which include patient education, self-management of exacerbations and pulmonary rehabilitation.
C: Confirm diagnosis and assess severity
O: Optimise function
P: Prevent deterioration
D: Develop support network and self-management plan
X: Manage eXacerbations
The guideline’s long term goals of the guidelines include:
primary prevention of smoking; improving rates of smoking cessation; early detection of airflow limitation in smokers before disablement; and improved management of stable disease and prevention of exacerbations.
Aboriginal
National Indigenous Pneumococcal and Influenza Immunisation Program
Pneumococcal and Influenza immunisations are given free for Aboriginal and Torres Straight Islanders over 50 or anybody under 50 who are/have:
Heavy drinkers

Kidney, heart or lung disease Severe asthmatic Diabetic Low immunity , eg HIV
Avian influenza
Posters with accompanying scripts have been implemented in Aboriginal and Torres Strait Islander communities on the human health risks of avian influenza in wild birds in Australia. They have been used by local health workers to educate the community about how to cook birds or handle dead birds to prevent the spread of avian influenza.
Closing the gap; talking chronic disease
Targeting smoking: A national network of regional campaign coordinators to help communities develop
local smoking reduction strategies and to coordinate initiatives across all levels of government, as well as health, education and other services. This will be achieved in a staged approach with coordinators recruited to cover 20 sites in 2009-10; followed by recruitment for a further 20 sites in 2010-11 and 17 sites in 2011-12.
Training for 1000 existing health and community development workers in relevant interventions to reduce smoking. Up to 200 workers will be trained in 2010-11; 400 in 2011-12 and a further 400 in 2012-13.
Access to Quit smoking services for some 13,500 Indigenous Australians, including individual, family and community-based programs over the four years.
Funding to promote health issues and services to indigenous Australians, including funding to promote smoking reduction and healthy lifestyle choices. Education and development kits will be developed by June 2010. Social marketing campaign programs will commence in 2010-11.
Funding and training of up to 105 healthy lifestyle workers to assist Indigenous individuals and families throughout Australia who are at risk of developing a chronic disease to reduce their risk of chronic disease through the adoption of healthy lifestyle choices. 42 healthy lifestyle workers will be funded and trained by June 2011, another 30 by 2012 and a further 33 by 2013.
Funding to enhance Quitline services to ensure appropriate interventions.
Taking a Breather: Asthma Management for Indigenous Australians
Emphasises role of asthma action plans in patient self-management, appropriate medications, and use of and access to devices
early detection of asthma trigger and risk factor management, particularly smoking increase access to medical devices culturally appropriate
8. Describe pharmacological and non-pharmacological methods of treatment and management for pneumonia in primary health care
Guidelines used to Assess Hospitalisation
Pneumonia Severity Index
- Determines whether patient is hospitalized based on their score from numerous tests- Done in class
Infectious Diseases Society of America
- ICU admission ifo Septic Shocko Complete respiratory failureo 3 or more criteria concerning blood/urine/gas results are met
Pharmacological Treatment
Different forms of antibiotics are prescribed. Relatively new evidence shows shorter courses of antibiotic can be just as effective as longer courses. Improvement can usually be seen in ~72 hours
Is recommended for
- Otherwise healthy peopleo Macrolideso Doxycycline
- Patients with co-morbidities- Patients with high risk of Streptococcus Pneumoniae- Antibiotic use in last 3 months
o Respiratory fluroquinoloneo ACE inhibitors
- Patients with severe Pneumoniaeo Hydrocortisone
- Paediatric Patientso Amoxicillin commonly used
Non-Pharmacological Treatment
In conjunction with pharmacological treatment
- Early mobilisation (for patients unable to move, body parts can be moved for them with beneficiary effects)
In replacement of antibiotics
- Humidified oxygen (increase oxygen absorption, reduce damage)- Hydrate- Nutritional support- Vaccination
9. Define HIV/AID.The Human Immunodeficiency Virus (HIV) attacks the immune system, which is the body’s defence against disease. This condition progressively reduces the effectiveness of the immune system and leaves individuals more susceptible to infections and tumours.
If a person’s immune system is severely damaged by the virus, they will develop the Acquired Immunodeficiency Syndrome (AIDS). This means they are vulnerable to infections and illnesses that their body could normally fight off.
HIV can live in the body for years without causing obvious damage, although the virus is constantly replicating. Many people with HIV continue to look and feel well. They may not even know they have HIV.
Transmission and at-risk groups
The virus can enter the body via contact with the bloodstream or by passing through delicate mucous membranes, such as inside the vagina, rectum or urethra.
The most common ways that people become infected with HIV are:
having sexual intercourse with an infected partner. injecting drugs using a needle or syringe that has been used by someone who is infected. as a baby of an infected mother, during pregnancy, labour or delivery, or through
breastfeeding.
As a sexually transmitted infection, HIV particularly affects adolescents and young adults.
Certain types of behaviour carry a higher risk of HIV transmission. People particularly vulnerable to HIV include injecting drug users, sex workers and men who have sex with men. Yet the vast majority of HIV infections are transmitted through sex between men and women. Nearly half of all adults living with HIV are female.
10. Discuss the diagnosis and notification process of HIV/AIDSDiagnosis: Blood tests are the most common way to diagnose HIV. These tests look for antibodies to the virus that the body creates in an attempt to fight off the virus. Early testing is crucial to prolong quality and span of life post infection. The steps towards HIV/AIDS diagnosis are as follows:
1. Universal screening is now recommended by the Centre for Disease Control for all patients aged 13-64 years with annual testing recommended for high risk populations.
o Screening tests remain voluntary, but the patient has the option to decline screening test (opt-out screening).
2. If suspicion of HIV infection is raised by history, clinical presentation, or presence of complications, counsel the patient on potential implications of testing.
o Note. There is a 12 week period after infection during which antibodies develop for which HIV testing will not be able to detect the presence of the disease.
3. Perform HIV antibody testing in the first instance using an enzyme-linked immunosorbent assay (ELISA) which detects the presence of antibodies in the blood sample.
o A positive result will warrant a second test. A second positive test will then be followed up by a western blot which tests for HIV proteins.
If initial HIV antibody test is negative or is reactive, but follow-up Western blot test is negative or indeterminate, arrange other confirmatory tests such as HIV RNA assay or p24 antigen assay.
o Combining the two tests ensures accurate diagnosis as the possibility of a false-positive can be generated through the presence of non-HIV antibodies.
4. All patients with positive HIV antibody should undergo immediate diagnostic tests . o Obtain quantitative measure of viral replication with measurement of viral
RNA. 5. Consider optional diagnostic tests including:
o Other STI’s such as Chlamydia and gonorrhoea o baseline assessments of fasting glucose and lipids if considered at risk for
cardiovascular disease or prior to ART
Notification/counselling: the notification of HIV cases to the Department of Health is predominately through by laboratories, medical practitioners and hospitals. Australia’s HIV/AIDS surveillance is among the best in the world with notification of AIDS in all states since 1982 and of HIV since 1989. Most countries do not collect public health data on all HIV diagnoses relying on other sources, such as sentinel sites, population surveys and AIDS notifications. However, because of the success of combination therapies and the reduction in AIDS incidence, there is new emphasis internationally on implementing HIV notification.
The notification process: People newly diagnosed with HIV infection are notifiable by laboratories that carry
out confirmatory HIV testing Following confirmation of diagnosis, the reference laboratory sends a notification
form to the requesting doctor to collect information including the demographics, risk exposure, previous tests and clinical status of the patient. To protect patient confidentiality, a name code is used (first two letters of the surname and given name) instead of the patient’s full name. By law, medical practitioners must complete the notification form and return it to the laboratory.
The information is then entered on the HIV database, forwarded to the National Centre in HIV Epidemiology and Clinical Research (NCHECR) for inclusion on the National HIV database, and to the World Health Organisation.
Public health units follow up notifications that report risk exposures other than male to male sexual contact or mother to child transmission.
A core element of treating patients diagnosed with HIV/AIDS is counselling. In a holistic model of health care patients receive treatment for both the physical and psychological aspects of their illness. The general aims of counselling are to:
Prevent transmission of HIV Support those affected both directly and indirectly
Counselling can be both pre and post-testing. Pre-test counselling should accompany the offer of HIV antibody testing to ensure the principle of informed consent is understood and to assist the patient in understanding the implication of a positive test result. This process should provide accurate
information regarding transmission and prevention of HIV as well as the “window period” associated with detection of the disease. Patient sexual/and or drug injecting history is also necessary to ask.
Post-test counselling should be given simply and in person. A HIV negative patient can learn about risk reduction and precautions against possible infection. The window period should be checked again and a decision to pursue further testing be made. HIV positive patients should be given time to adjust. Direct questions should be answered but the focus is on coping with the next few days. Avoid overloading the patient with information regarding HIV. Counselling should be available to the patient over the next few months. The patient should also be made away of the treatment options available and the importance of adherence.
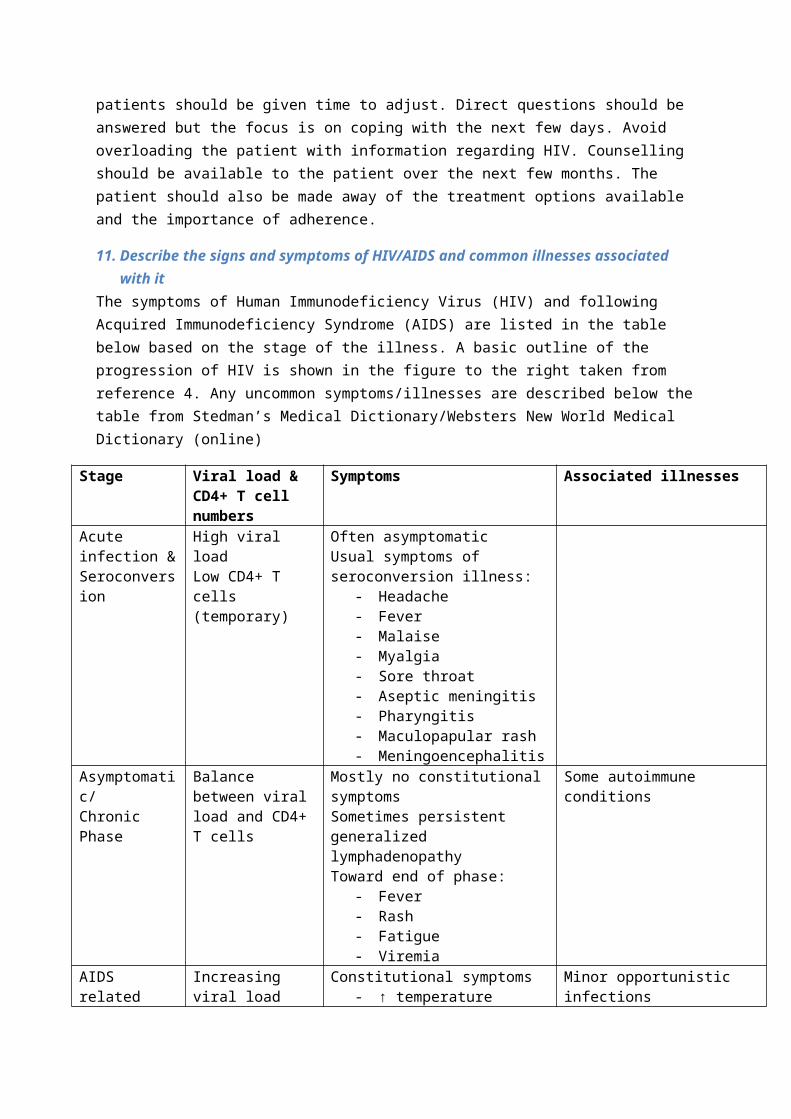
11. Describe the signs and symptoms of HIV/AIDS and common illnesses associated with itThe symptoms of Human Immunodeficiency Virus (HIV) and following Acquired Immunodeficiency Syndrome (AIDS) are listed in the table below based on the stage of the illness. A basic outline of the progression of HIV is shown in the figure to the right taken from reference 4. Any uncommon symptoms/illnesses are described below the table from Stedman’s Medical Dictionary/Websters New World Medical Dictionary (online)
Stage Viral load & CD4+ T cell numbers
Symptoms Associated illnesses
Acute infection & Seroconversion
High viral loadLow CD4+ T cells (temporary)
Often asymptomatic Usual symptoms of seroconversion illness:

- Headache- Fever- Malaise- Myalgia- Sore throat- Aseptic meningitis- Pharyngitis- Maculopapular rash- Meningoencephalitis
Asymptomatic/Chronic Phase
Balance between viral load and CD4+ T cells
Mostly no constitutional symptomsSometimes persistent generalized lymphadenopathyToward end of phase:
- Fever- Rash- Fatigue- Viremia
Some autoimmune conditions
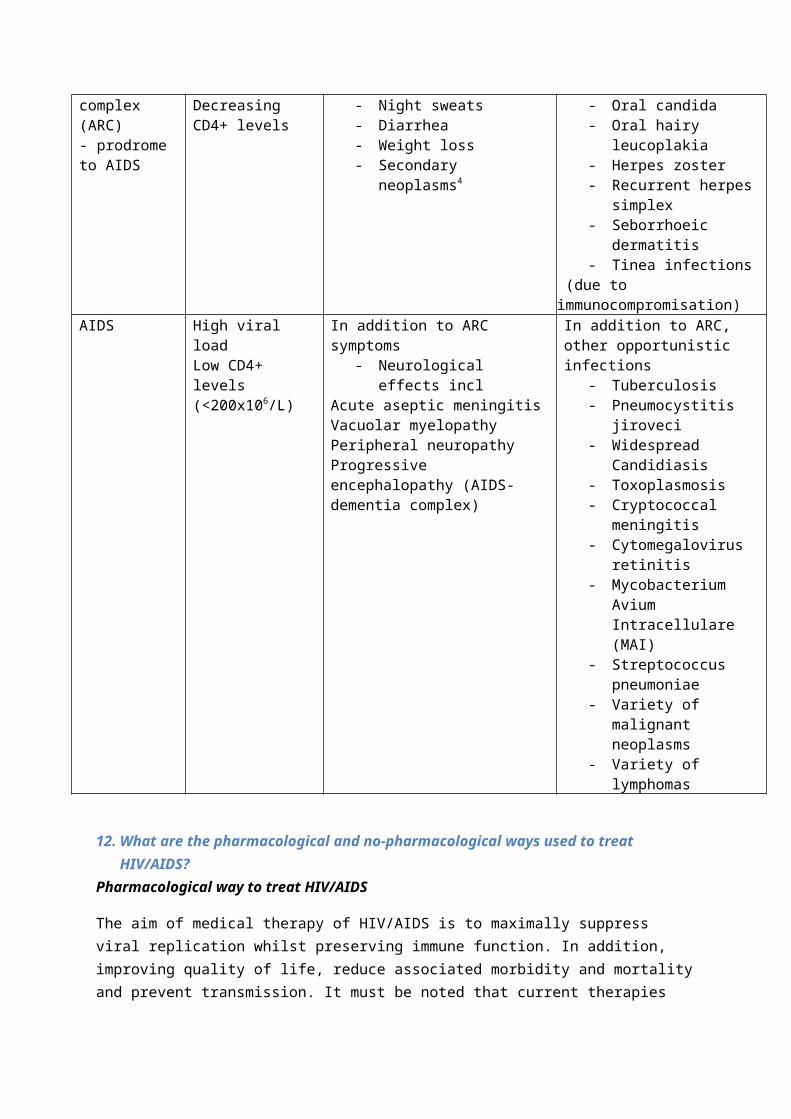
AIDS related complex (ARC)- prodrome to AIDS
Increasing viral loadDecreasing CD4+ levels
Constitutional symptoms- ↑ temperature- Night sweats- Diarrhea- Weight loss- Secondary neoplasms4
Minor opportunistic infections- Oral candida- Oral hairy leucoplakia- Herpes zoster- Recurrent herpes
simplex- Seborrhoeic dermatitis- Tinea infections
(due to immunocompromisation) AIDS High viral load
Low CD4+ levels (<200x106/L)
In addition to ARC symptoms- Neurological effects incl
Acute aseptic meningitisVacuolar myelopathyPeripheral neuropathyProgressive encephalopathy (AIDS-dementia complex)
In addition to ARC, other opportunistic infections
- Tuberculosis- Pneumocystitis jiroveci - Widespread Candidiasis- Toxoplasmosis- Cryptococcal meningitis- Cytomegalovirus
retinitis- Mycobacterium Avium
Intracellulare (MAI) - Streptococcus
pneumoniae- Variety of malignant
neoplasms- Variety of lymphomas
12. What are the pharmacological and no-pharmacological ways used to treat HIV/AIDS?Pharmacological way to treat HIV/AIDS
The aim of medical therapy of HIV/AIDS is to maximally suppress viral replication whilst preserving immune function. In addition, improving quality of life, reduce associated morbidity and mortality and prevent transmission. It must be noted that current therapies are unlikely to eliminate the virus completely, but may result in clinical improvement.
For acute exposure to HIV, chemoprophylaxis should be given and counseling to minimize transmission should be provided.
Primary prevention and screening for anyone aged 13-64 years should be undertaken in the general population and those at risk.
For patients diagnosed, counseling about secondary prevention should be provided to help prevent further transmission.
There are 4 interventions that have been shown effective in increasing survival of HIV/AIDS sufferers including;
Antiretroviral therapy (ART) – 6 drug classes usedTriple combination antiretroviral therapyDrug resistance testingImproving patient compliance
Treatment guidelines are the same for women and men.
Medical therapy should involve at least 3 antiretroviral drugs as highly active antiretroviral therapy has show to produce better outcomes with regards to mortality and opportunistic infections. Normally, medical therapy involves the use of 2 nucleoside/nucleotide reverse transcriptase inhibitors (NRTI) and either a protease inhibitor (PI) or non-nucleoside reverse transcriptase inhibitor (NNRTI). These treatment regimes have show to have greater efficacy compares to regimes without a PI or NNRTU. If there is drug failure or drug toxicity, modifying therapy should be considered. Monotherapy is not recommended. Additionally prophylactic treatments for Pneumocystis jiroveci and Mycobacterium avium, and provide vaccination against opportunistic infections that may have more serious outcomes in HIV/AIDS sufferers.
Pregnancy
Therapy should continue in pregnant women as well as therapy aimed at preventing mother to child transmission. In the first trimester, Efavirenz should be avoided. Throughout all of pregnancy etravirine and neviapine and NNRTIs should be avoided. Doses may need to be altered throughout
pregnancy due to physiological changes that occur during pregnancy. Risk of perinatial transmission and ART effects on the fetus should be analyzed.
Children
Not all antiretroviral drugs that have been approved for use in adults have been approved for use in children. There are certain antiretroviral regimens that should not be offered to children. These must be taken into consideration before prescribing an ART regime for a child with HIV/AIDS. Short-term effects are reversible. Long-term effects on children are still unknown, however increase malignancies have been found in children treated with zidovudine.
In addition to medical therapy, close monitoring of the child’s growth and development is very important and consideration with drug regimes and so forth should be taken for the care giver.
Non-Pharmacological ways to treat HIV/AIDS
Psychosocial supportive therapies are of utmost importance in HIV/AIDS patients and are offered depending on the symptoms, stage of disease and treatments. Symptom management may be difficult in advanced AIDS patients and palliative care and hospice referral may need to be considered.
HIV counseling is one of the integral therapies provided and aims to prevent transmission of HIV and to provide support for HIV patients, family and friends. It involves pretest counseling, posttest counseling, counseling during ART and counseling patients and partners together. Many psychological issues can be addressed in these counseling sessions including shock, guilt, depression, fear, anxiety, anger and frustration.
Palliative care is for relieving suffering and controlling symptoms of a chronic disease. It can include symptom control and management, education and counseling, psychosocial and spiritual support and hospice referral if needed.
With children, subjects such as palliative care and hospice referral should be discussed with the parents of a child with advanced AIDS.
Cystic Fibrosis & Child Development
13. Describe the main reasons infants present with failure to thrive and outline an approach to assessment of infants presenting with failure to thrive.
Failure to thrive is a clinical label used to describe infants and young children, generally 3 years of age and younger, who fail to grow as expected based on established growth standards for age and gender. It is categorised as either organic, non-organic failure to thrive or mixed failure to thrive based on the causative factor. However, mixed failures are commonly seen.
Causes
Psychosocial causes:
1. Parent’s emotional and material resources are diverted or not available from for the care of the child. This may be due to:

Poverty Parental depression Maladaptive parenting practices Family discord Chronically ill family member Substance abuse Losses
2. Pre-existing minor developmental deficits may develop feeding problems that lead to nutritional failure to thrive.
3. When not eating serves other purposes e.g. expression of anger or to gain attention.4. Children living in poverty due to lack of food, homelessness, or overcrowding.
Medical causes:
1. Infectious agents e.g. HIV, chronic sinusitis2. Mechanical e.g. adenoid hypertrophy, dental lesions3. Toxic/metabolic e.g. Lead toxicity, Iron deficiency4. Neurologic e.g. oral motor dysfunction (gagging, tactile hypersensitivity)5. Allergic – food allergies6. Gastrointestinal e.g. celiac disease, malabsorption
Perinatal risk factors such as prematurity and intrauterine growth retardation.
Assessment of an infant presenting with failure to thrive
1. Note whether the signs and symptoms are present. They include: Weight less than 5th or 3rd percentile Failure to maintain previously established growth trajectory, particularly after 18
months of age Decreased rate of daily weight gain for age Depressed weight for height, which always reflects inadequate nutritional intake
for the child’s metabolic requirements2. History taking:
Scrutinise the growth chart to determine onset of failure to thrive: ‘What were the changes in your family’s or child’s life around the time
child’s growth slowed?’ ‘What, when, where, why, and by whom is your child fed?’ Ascertain 24-
hour dietary recall and child’s behaviour and affect during mealtimes. ‘How much low calorie liquid does your child drink each day?’ ‘Does your child have any difficulty or is difficult when being fed?’ ‘What are your child’s bowel movements like?’ ‘Do you ever run out of food?’ ‘Does your child snore, even when there is no cold?’ Determines whether the
child is suffering from adenoid hypertrophy. ‘Is your child allergic to any foods or not allowed to out of religious or other
reasons?’ ‘Are there any significant stresses in the house?’
3. Behavioural observations of when the child is eating and quality of nonfeeding interactions.4. Physical examinations to rule out medical causes of failure to thrive.5. Tests ordered should include:
Lead CBC with differential FEP Urinalysis Urine culture
Electrolytes Purified protein derivative HIV screening Sweat tests IgA measurements Anti transglutaminase antibody Enteric pathogen screening Bone age
14. Outline the advantages and disadvantages of the various tools to assess children’s developmentResults must always be interpreted in context ie ongoing surveillance, take into account patient history.
Benefits of screening is that it aids in determining whether a child requires additional evaluation, close monitoring/surveillance or just normal ongoing monitoring.
Challenges with screening
There is a lack of evidence that informal checklists of developmental skills can predict developmental status, and a lack of criteria regarding when referral is appropriate.
A parent’s concerns are brought forward informally, and may lack understanding of development and what it means and involves. Even clinical judgement detects less than 30% of children with developmental disabilities.
Developmental screening tools can enhance surveillance and increase detection of any developmental abnormalities. There are two main types of tools; parent completed and directly administrated. These can range from general domain to domain or disorder specific.
A good screening tool with be standardised on a national level, have good reliability and good validity (consistent and sensitive/specific). It’s important to know that sensitivity and specificity of 70-80% is considered acceptable with regards to developmental screening tests.
Commonly used general screening tools;
Ages and Stages Questionnaire Battelle Developmental Inventory (BDI) Screening Test Bayley Infant Neurodevelopmental Screener (BINS) Brigance Screens-II Infant Development Inventory Child Development Review Child Development Inventory (CDI) Denver-II Developmental Screening Test Parents' Evaluation of Developmental Status (PEDS)
Advantages and disadvantages of:
- Parent completed tools -
Advantages: More cost effective
More accurate because parent knows childParent involvementFlexibility in application and implementationSimple and straightforwardTests correct for parents either under or over reportingParent report has been show to increase screening tool accuracy
Disadvantages:Parent is not educated in child development so may not interpret things correctly.Relies on commitment and abilities of the parentsNot all age intervals are covered (after 36 months the intervals are every 6 months)
- General tools -
Advantages: Early detection can lead to effective treatment before it is too lateResults can give an indication as to whether a child is school ready or not.Tests state their norms specifically
Disadvantages:Need to consider the appropriateness of any one tool to the individual patient.Don’t necessarily cover all age ranges that it may need toSome don’t take into account that development is continuous, and looks at development in stages. Don’t provide a diagnosis or detailed information about an area of developmentPeriodic screening is necessary to get a continuous full picture of a childs developmentLimited ability to predict future functioningTake time and effect to administer and interpret so may not necessarily be used as much as they should be
15. Describe cystic fibrosis including the cause of cystic fibrosis (pattern inheritance), the effect on the affected cells, the mechanism whereby the faulty gene causes the production of thick mucus and the resulting clinical features.
What is cystic fibrosis?Cystic fibrosis (also known as mucoviscidosis) is the most common life-threatening autosomal recessive condition affecting Caucasians of European descent. As of 2007, it has an incidence rate of 1 in 3200 live births in the US however it is uncommon in Asian and African American populations. It affects epithelial ion transport resulting in abnormal fluid secretion of exocrine glands and in respiratory, gastrointestinal and reproductive mucosa. There are many different mutations of the gene causing highly variable symptoms most commonly pancreatic insufficiency, persistent pulmonary infections, liver disease and infertility due to absence of the vas deferens. Cystic fibrosis is usually diagnosed in childhood and though there is no cure, treatment of associated diseases has resulted in an average prognosis of over 30 years.
Cause of cystic fibrosisCystic fibrosis is caused by a mutation in the cystic fibrosis transmembrane conductance regulatory (CFTR) gene on chromosome 7. This affects a transmembrane protein in the epithelial cells of the respiratory, GIT and reproductive systems. There are many different mutations of this gene which
cause CF however the most common and severe mutation is a 3 nucleotide deletion coding for phenylalanine at position 508, called the delta F508 mutation. Those who are homozygous for this mutation have the most severe ‘classic CF’ symptoms, however individuals can have one copy or no copies of this particular mutation and still be diagnosed with cystic fibrosis.
Mechanism of viscous mucus production & the effect on cells and the bodyThe CFTR gene codes for epithelial chloride channels in the GIT and respiratory tract responsible for secretion and reabsorption of chloride, controlling the salt and fluid balance of secretions by the mucosa. A mutation to the CFTR gene causes a defective CFTR channel which has different effects depending on the system involved.
In the respiratory system:CFTR protein is responsible for active luminal secretion of chloride. Defective CFTR proteins results in loss or reduction of chloride secretion and an increase in active luminal sodium absorption, causing passive water reabsorption from the lumen and therefore a lower water content of the surface fluid layer coating the mucosal cells. This fluid is described as a thick viscid mucus and thus giving rise to the name mucoviscidosis. This causes defective mucociliary action and therefore an accumulation of mucus which obstructs air passages predisposing cystic fibrosis sufferers to recurrent pulmonary infections and lung disease.
In the gastrointestinal system:The CFTR protein has a very similar purpose in the gastrointestinal system and a defective protein causes accumulation of hyperconcentrated viscid secretions which obstructs ductal outflow from secretory organs. This can cause problems in the pancreas as it prevents the release of enzymes necessary for food digestion and therefore cystic fibrosis patients often suffer from malnutrition and associated illnesses.
In sweat glands: The CFTR protein is responsible for luminal reabsorption of chloride ions, a loss of function results in decreased reabsorption of sodium chloride and production of hypertonic sweat.
Clinical features of Cystic fibrosisSigns and symptoms commonly associated with cystic fibrosis
Respiratory system Gastrointestinal System (Respiratory) Infections
Other
Chronic pulmonary infections
Pancreatic insufficiency Staph. aureus Male infertility (absence of vas deferens)
Bronchiectasis Distal intestinal obstruction syndrome
Haemophilus influenza
Osteoporosis
Pulmonary fibrosis Gallstones Pseudomonas aeruginosa
Arthritis
Pneumothorax Hepatic cirrhosis VasculitisPulmonary abscesses Vitaminosis Nasal polypsRespiratory failure Meconium ileus (intestinal
obstruction)Hypertrophic pulmonary osteoarthropathy

Obstructive pulmonary disease
Progressive duct dilation and metaplasia of salivary glands
Sinusitis
Cough, wheeze, haemoptysis, cyanosis, clubbing, bilateral coarse crackles
Diabetes mellitusMalabsorption presenting as large foul smelling stools, abdominal distention and poor weight gain
These are just some of the signs and symptoms as cystic fibrosis is highly variable, refer to Pathologic Basis of Disease Textbook for extended list.
16. Describe the procedure for diagnostic testing and screening (three screening levels newborn, prenatal, carrier) that can be carried out for cystic fibrosis
Diagnosis Gold standard diagnostic test = sweat electrolyte test. Those with CF have higher concentrations of sodium and chloride than normal.
o Diagnostic level = >60mmol/L. (normal level = <40mmol/L).
Can be completed at any age, although a newborn must be able to produce enough sweat (this usually happens at 2 weeks of age).
A sweat test would be completed on a newborn if they returned a positive screening. The test involves application of a chemical and an electrode to an area of skin, to cause
sweating.2 Sweat from the area is then collected and analysed by a lab.
ScreeningNEWBORN
In Aus, all newborns are screened for cystic fibrosis. A blood test is completed 3 days after birth, and a screen is completed for several disorders,
such as CF. Firstly the blood is analysed to determine the level of IRT (immunoreactive trypsin) protein
in the blood. If a high level is found, the sample is then tested for common CFTR gene mutations. Babies who return a positive result will then complete a sweat test.
PRENATAL Carrier testing can be completed for all pregnant women and their partners. If both are found to be carriers, then there is a 25% chance their baby will have CF. Further testing can be completed, such as:
o Chorionic villus sampling. Performed after 9 weeks of pregnancy. A piece of placenta is removed and the cells are analysed for the abnormal
CF gene. o Amniocentesis
Performed at 15-20 weeks of pregnancy. A sample of amniotic fluid is taken (via needle). This fluid contains cells from the baby, and so can be analysed for the
abnormal CF gene. If a couple are interested in using IVF, testing can be completed on the fertilized egg to
determine if an abnormal CF gene is present – this is preimplantation genetic diagnosis. Prenatal testing is highly accurate, but cannot indicate the level of severity of the disease.
CARRIER Carriers = those who have one copy of a mutation on the CF gene. Genetic testing can be completed on those who do not have CF, but would like to determine
if they are a carrier. A positive result indicates that the person has a mutation on a CF gene. There are over 1000 different mutations on the CF gene, and some are not identified by the
genetic test, and so a negative result does not exclude these rare mutations. Patients usually complete genetic testing for such reasons as:
o They want to have children but a partner is a carrier. o They have a blood relative with CF.
17. Describe Cystic Fibrosis management including treatment for children with the disease (physiotherapy, diet, medications). What is the purpose for each of the individual treatments?
Physiotherapy
These are airway clearance techniques designed to mobilise mucous build up in the airways.
a) Chest Percussion
Aids in the clearance of secretions up and out of the lungs to prevent the sticky lung secretions from blocking the airways.
o Reduction of infection and prevention of lung damage. The chest is clapped firmly with a cupped hand Treatment sessions vary in length from 10-15 minutes to 45-60 minutes, according to the
amount of secretions needing to be cleared. There can be between 1 and 4 treatment sessions per day, which is also dependant on the need
b) Vibrations
A gentle shaking or vibrating of the chest whilst breathing out to create mini bursts of airflow which dislodge the secretions. Usually followed by a cough to clear the secretions from the lungs.
c) Breathing Techniques
Use controlled deep and shallow breathing to move mucous up through the airways, and also to re-inflate the lungs in the case of deflation due to mucous blockage
c) Flutter Therapy
Breathing out against an alternating resistance to create back pressure to expand the small airways so they remain open for longer. The mini bursts of airflow also help to dislodge the secretions.
d) Positive Expiration Pressure (PEP)
Breathing out through a mask to create back pressure within the lungs, which opens small airways and opens side channels (collateral ventilation) to get behind secretions and dislodge them towards the exterior.
e) Autogenic Drainage
Controlled method of breathing, involving training to breathe at 3 different lung volumes:
o Low lung volume to unstick mucouso Mid lung volume to collect mucouso High lung volume manouvers to expel mucous.
Medication
a) Lungs
Medication can be taken by inhalation using nebulisers, taken orally or taken intravenously. These drugs treat the lungs in the following ways:
Bronchodilator drugs open the airways by relaxing the smooth muscle, relieving tightness and shortness of breath
Antibiotics help to control and treat infectionso Oral – eg. Cephalexen, Cephaclor.o IV
Steroids reduce airway inflammation
b) Digestive System
CF affects the pancreas so enzyme replacement capsules must be taken to enable people to properly digest and gain more energy from the food they eat. Without this medication, pancreatic enzyme insufficiency prevents digestion and absorption of nutrients.
Dosage is decided upon by a dietician.
Examples of enzymes available in Australia include CREON® and PANZYTRAT.
c) Other
Bisphosphonates are beneficial to prevent osteoporosis, which is an illness associated with lack of mineral absorption in CF.
Research is being carried out to determine the benefits of high doses of calcium and vitamin D.
Diet and Exercise
Nutrition plays a very important role in the management of someone suffering CF. Research has shown there is a link between weight gain and survival. People with CF are required to consume between 120-150% of the daily amount of food recommended for a person of the same age and size that does not have CF. This is needed to ensure they:
o Increase their chance of absorbing the nutrients needed for normal and healthy growth (in children) and general sustained health
Increase their body weight in order to fight off infections
The diet for a person with CF is high in calories, high in fat, high in salt, and high in sugar. Having a good body weight helps sufferers when they are ill as appetite is often reduced and they can lose weight. A healthy body weight also assists in fighting infection. Good nutrition and a diet rich in fruits, vegetables, proteins and fats is important for people with CF to maintain good health.
Supplements:
Fat Soluble Vitamins A, D, E, K

Electrolyte drinks, salt tablets and maintain water intake to prevent dehydration (sweat is five times saltier therefore putting sufferers at risk of dehydration).
Exercise:
There is a clear link between exercise, weight gain, body mass, lung function and survival in CF.
Exercise is a part of the daily treatment routine for people with CF because it assists with airway clearance and builds muscle mass and strength.
People are encouraged to drink plenty of water during and after exercise to avoid dehydration.
Children as a special group:
Children with CF need to eat extra calories and protein for 2 reasons: o To compensate for loss of fat and protein in the stools due to lack of pancreatic
enzymeso To help children become well-nourished so they can withstand chest infections
better. It may be necessary to take supplements if the child’s weight or appetite is poor. These
include calorie powders, enzyme supplements and shakes. It also may be necessary to use tube feeding (nasogastric or gastronomic) to allow the child
to gain adequate weight by increasing the calories and nutrients consumed. It is important to take regular supplements of vitamins A,D and E and pancreatic enzymes.
Transplantation
Lung transplantation is an option for people with advanced lung disease resulting from CF. Transplanted lungs are however susceptible to infection, rejection and other complications. In Australia there is an average wait of 9-12 months due to a donor shortage. 85% of people in Australia undergoing bilateral lung transplant survive at least 1 year and
60% at least 5 years.
18. Discuss the psychological burden on the person with the disease and the family (focus on parents and adjustment disorder).
1. Loneliness
When you can’t do the same things that your friends are, go to the same places, and you have overprotective parents, it can take a toll on somebody. Many parents, in an attempt to protect their children from the outside world, keep their children inside the house and in their direct supervision at all times. While doing this is understandable and the parents are just trying to keep their kids healthy, it can make the cystic fibrosis sufferer feel alone. Parents should make sure that their children have fun but safe activities to do with their friends. You can’t keep them locked up forever.
2. Growth
– Children that have cystic fibrosis are not going to grow as fast as their peers, and that can make them feel inadequate. While everybody else begins to grow in height during puberty, for a CF patient the growth spurt can come several years later, if at all. Many children will feel embarrassed about this, and the other kids at school are not going to make things any
easier. Classmates that are unaware that somebody has this disease can often be cruel, and teasing and bullying may occur.
3. Hospital
– Cystic fibrosis can often force children to spend several weeks in the hospital if complications occur. When this happens, the patient will be missing a good portion of schoolwork and time with their friends. Luckily, sometimes there are teachers that go to hospitals to teach those that are missing time from school, but that does not always happen. Not being able to live a normal life can cause cystic fibrosis patients to worry about their futures and wonder how they are going to be able to hold down a job.
Family
~ families were not deprived of the essentials of living, but they were not able to maintain their usual pattern of family relationships.
1. No sharing of knowledge among family members
When the mother/father is taking care of a CF child, he or she will be the only one going up and down to the physician’s office learning how to take care of the child. When he or she gets frequently fatigued by this and fails to explain to the family on how to participate in the care of the child, tension and stress develops.
This situation can easily lead to misunderstanding and tension within the family. To avoid this, both parents could be encouraged, at some point, to come together to the physician's office for discussion. Such discussions could lead to more consideration and appreciation
being given to each other. It might lessen the tendency for each to blame the other for the child's illness.
Besides that, the CF child is frequently aware of the demands he makes on the family. If these demands are not discussed freely, then everyone is caught in a "web of silence" revolving around his own feelings of frustration. This creates a burden for everyone, including the CF child, and if not discussed it can impair the psychological functioning of all members.
2. Participation of the CF child in the care
The CF child needs to be encouraged to participate in his own care program and to assume some responsibilities for him. He should not reach the age of seven being unable to tie his own shoes or dress himself. It would seem feasible, therefore, that the CF child should have an awareness of what is wrong with him, and what his abilities and limitations are.
3. Diversion of Family love and attention
The other siblings should also be given as much explanation as possible because they, too, are part of the family and attention and care is being diverted from them. This explanation could make for more understanding on the sibling's part. While it would still be difficult for him to accept some of the decisions made, he would know that it was the situation that was causing the decrease in attention and care rather than rejection of him by the parents.

4. Outsourcing some responsibilities
` In order to give these families as much assistance as possible, the community's resources should be utilized. Frequently, the parents are unaware of these or need encouragement to avail themselves of services. The homemaker service or visiting nurse service could free the
family from constant care; the local youth program could be helpful to the siblings in the family, and Family Service Agencies could be used for counselling on family problems.
19. Discuss the assistance a clinical geneticist can offer patients and their families with cystic fibrosis.
What is a clinical geneticist?
A medical doctor who has undertaken specialist training in genetics on completion of general professional training usually in internal medicine or paediatrics.
A clinical geneticist may work primarily as a researcher in a laboratory, or with patients and their families.
Patients may be referred to a clinical geneticist for diagnosis, management, genetic testing, and/or genetic counseling in relation to hereditary disorders.
What does a clinical geneticist do?
Clinical geneticists have a variety of roles. They may be involved in:
Genetic testing and diagnosing genetic disorder Prenatal screening of certain genetic disorders eg. cystic fibrosis Assess the risk of an individual inheriting or having inherited a genetic disorder(s) (genetic
risk assessment) and informing them of their risk Counsel individuals/families directly or direct individuals/families to a genetic counselor Informing the individual and their family about their specific genetic disorder such as the
diseases natural history, and features, as well as implications for family members Discussing treatment options Discussing ways in which the disorder might be prevented or outcome improved Directing families to other sources of high quality information Communicate with laboratories regarding genetic testing Act as a resource for doctors-providing information on the availability of genetic testing,
how to access such resources, and what to do with the results