Embed Size (px)
Citation preview

Respiratory Respiratory Disease In Disease In ChildhoodChildhood
Nick ConnollyNick ConnollyPaediatric SpRPaediatric SpR
NHS TaysideNHS Tayside

Respiratory problems in Respiratory problems in childrenchildren
Neonatal respiratory problems Respiratory problems in older children
Chronic Acute

Scenario Scenario
An infant born at 30 weeks gestation develops respiratory distress at age 2 hours



Respiratory Distress Syndrome
Relative Surfactant deficiency1% all birthsPredominantly in preterm – inverse
relationship with gestation

Surfactant
PhospholipidApoproteinsSecreted at 30-32/40 Lack of surfactant results in atelectasis and
impairment of gas exchangeProduction stimulated by steroids

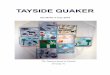
Incidence of RDS relative to gestational age
0
10
20
30
40
50
60
70
80
90
100
26 28 30 32 34 36 38 40Gestational Age
% with clinical RDS

Further problems
VentilatedSudden deterioration requiring increased
oxygenNo breath sounds on the right side of chest


Pneumothorax
Air in pleural spaceIncreased incidence with IPPV, CPAP and
ventilation Other risk factors – RDS (stiff lungs)Spontaneous - occurs in around 1% vaginal
deliveries, 1.5% caesarean sections


Chronic Lung Disease
Oxygen requirement beyond 36 weeks corrected gestation plus evidence of pulmonary parenchymal disease on CXR
Generally follows RDSBarotrauma, volume trauma, high inspired oxygenHealing stage associated with continued lung
growth over 2-3 years – often wheezy

ScenarioScenario
New born full-term infant with severe breathing difficulty after birth
?Dextrocardia


Diaphragmatic HerniaDiaphragmatic Hernia
Incidence:1/2400Associated pulmonary hypoplasiaCommonest- Posterolateral (Bochdalek),
left-sidedAvoid bag-mask IPPV?Respiratory supportSurgical


Older Children

Examination
Weight(length/height)..plotted!?clubbingChest shapeAuscultation

Breathing testsBreathing tests


Chronic problems

Cystic fibrosisCystic fibrosis
A 1 year-old child presenting with a prolonged history of cough, loose stools and failure to thrive
A newborn infant with a raised immuno-reactive trypsin level on neonatal screening who is also found to be homozygous for the ΔF508 deletion

Cystic Fibrosis
Autosomal recessiveCarrier incidence roughly 1 in 25 peopleMutations in the CFTR geneMultisystem disorderRespiratory infections are prominent


Differential diagnosisDifferential diagnosis
Immune deficiencyCiliary dyskinesiaAsthmaKartagener’s/ immotile cilia syndrome- rare

ScenarioScenario
NM is a 7 month old infant with cystic fibrosis who was admitted with 2 chest infections. He grew Staphylococcus aureus on his respiratory secretions


Cystic Fibrosis TeamCystic Fibrosis Team
ClinicianSpecialist nurseClinical psychologistSocial workerPhysiotherapistDietician

A 7-year child presents to your A 7-year child presents to your clinic with a 3-month history of clinic with a 3-month history of cough worse at night or during cough worse at night or during
active playactive play
Diagnosis: ASTHMA

Asthma – Diagnosis in ChildrenSIGN Guideline May 2008
Clinical Features that increase probability:
One or more : wheeze, cough, chest tightness, difficulty breathing
Atopy(personal or family history)Widespread wheeze on auscultationResponse to Rx

Asthma – Diagnosis in Children
SIGN Guideline May 2008
High Probability – diagnosis of asthma likely(trial of Rx – further Ix if poor response)
Low Probability – consider Ix & ? Referral
Intermediate Probability: ?watchful waiting ?spirometry(response) ? Rx & evaluate

Asthma – Diagnosis in Children

ManagementManagement
Stage 1: Treat with inhaled beta-agonists when needed
Stage 2: Treat with regular inhaled steroidsStage 3A: Regular inhaled steroids + Long
acting beta agonistsStage 3B: Stage 3A + Leukotriene
antagonists


Passive Smoking
Reduces birthweight by 250g4500 pregnancy losses p.a.30% increase in Perinatal MortalityTeratogenic : airways, cleft lip/palateGlue ear Carcinogenic4 million children live with smoking
parentIncrease likelihood of asthma attack

Acute problems

Acute asthmaAcute asthma
Cough and wheeze worsening over hours or days


TreatmentTreatment
OxygenNebulised bronchodilatorOral prednisoloneIV salbutamolIV aminophyllineIV magnesiumVentilatory support


Scenario
6 week old presented with increased work of breathing and possible apnoes
URTI symptoms over last 2 days

Bronchiolitis
Viral infection – RSVUsually under 18 months oldMore severe in younger babies, ex prem,
family of smokersTachypnoea, poor feeding, irritating coughApnoea in small babiesTreatment is supportiveIncreased incidence of wheezing episodes in
the next ?10 years

Scenario Scenario
10 year old girl with cough, high fever and sputum production Previously very well Clinical examination: Dullness on percussion Vocal fremitus and resonance Bronchial breathing


PneumoniaPneumonia
Neonates: GBS, E.coli, Klebsiella, Staph aureus
Infants: Strep pneumoniae, ChlamydiaSchool age: Strep pneumoniae, Staph
aureus, Gr A strep, Bordetella, Mycoplasma, Legionella

ScenarioScenario
A 2-year old child presenting with barking cough and difficulty in breathing of sudden onset

Differential DiagnosisDifferential Diagnosis
Inhaled foreign bodyLaryngomalaciaEpiglottitis and bacterial tracheitisAllergyCroup



Croup
Viral laryngotracheobronchitisStridor, barking coughTreatment is oral steroid to reduce
inflammation

Scenario Scenario
9 month old infant from developing country with irritability, neck rigidity, afebrile


Pulmonary TuberculosisPulmonary TuberculosisMycobacterium tuberculosisNotifiable disease1/3 of World Population!Droplet infectionPrevention(of severity): BCGDrug treatment: 2 mths- Isoniazid, Rifampicin, Pyrazinamide 4 mths- Isoniazid, Rifampicin

Common respiratory Common respiratory problems in childrenproblems in children
Infant respiratory distress syndromeCLDCongenital diaphragmatic herniaCystic fibrosis AsthmaBronchiolitisChildhood pneumoniasCroupTuberculosis

FINISHED