Embed Size (px)
Citation preview
cancercontrol.cancer.gov/brp
Resources and Support for Implementation Science and
Tobacco Control at NIH

NIH Fogarty International Center https://www.fic.nih.gov/researchtopics/pages/implementationscience.aspx
NIH Fogarty International Center https://www.fic.nih.gov/researchtopics/pages/implementationscience.aspx

NIH Office of Behavioral and Social Science Research
(OBSSR) https://obssr.od.nih.gov/scientific-initiatives/dissemination-and-implementation/
National Cancer Institute https://cancercontrol.cancer.gov/IS/

National Heart, Lung and Blood Institute https://www.nhlbi.nih.gov/about/org/ctris/

NIH Resources Dissemination and Implementation Science
• Training programs
– Training Institute for Dissemination and Implementation Research in Health
– NCI Implementation Science Team Masters Courses and Webinar Series
• Conferences
– Conference in the Science of Dissemination and Implementation in Health,
December 4-5, 2017
• Online courses and materials
– FIC Toolkit Overcoming Barriers to Implementation in Global Health
– Research to Reality online forum for cancer control researchers and
practitioners
NIH D&I Funding Opportunity
• Open to Foreign Institutions
• Three different mechanisms – R01, R21, R03
• Studies of strategies to implement health promotion, prevention, screening,
early detection, and diagnostic interventions, as well as effective
treatments, clinical procedures, or guidelines in existing care systems.

cancercontrol.cancer.gov/brp
Current Tobacco Control Funding Initiatives at NCI
10
Tobacco Control as a Global Cancer Research Priority
• November 2012 – Research leaders from 15 countries
came to NIH to discuss priorities in global cancer
research.
• With respect to modifiable lifestyle risk factors for
cancer, there is a consensus that tobacco use remains,
by far, the most important at a global level.
• Measures that can already be taken to control tobacco
use include removing tobacco products from trade
agreements, increasing taxes on tobacco products,
controlling tobacco industry marketing, and building
support among health professionals.
Source: H. Varmus, H. S. Kumar, Addressing the growing international challenge of
cancer: A multinational perspective. Sci. Transl. Med. 5, 175cm2 (2013).

11
TCRB International Research Webpage http://cancercontrol.cancer.gov/brp/tcrb/international/
12
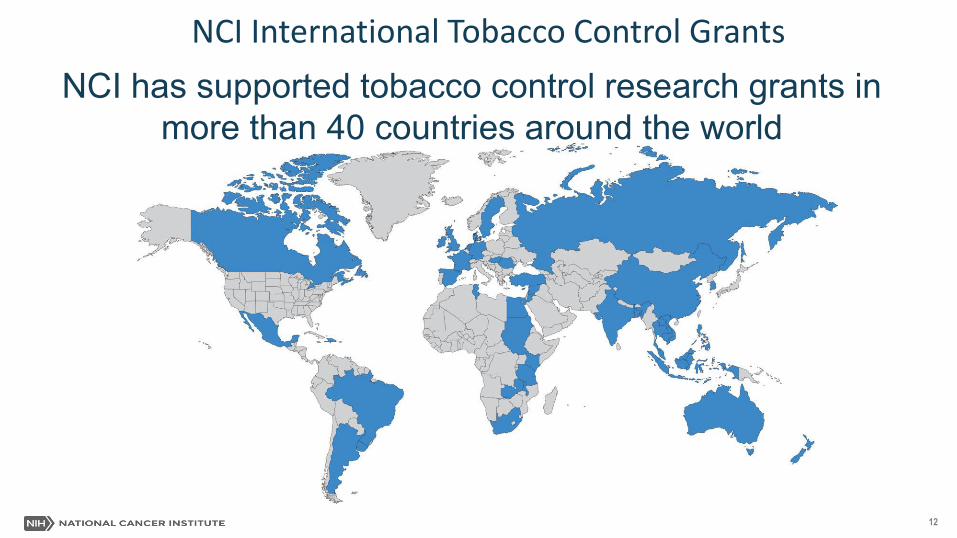
NCI International Tobacco Control Grants
NCI has supported tobacco control research grants in
more than 40 countries around the world
13
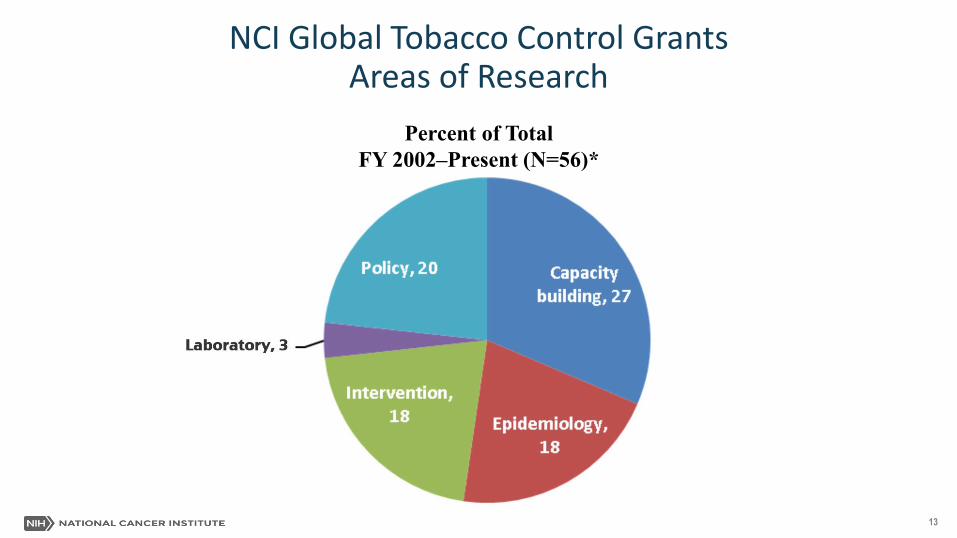
NCI Global Tobacco Control Grants Areas of Research
Percent of Total
FY 2002–Present (N=56)*
NIH International Tobacco and Health Research and
Capacity Building Program https://www.fic.nih.gov/programs/pages/tobacco.aspx
15
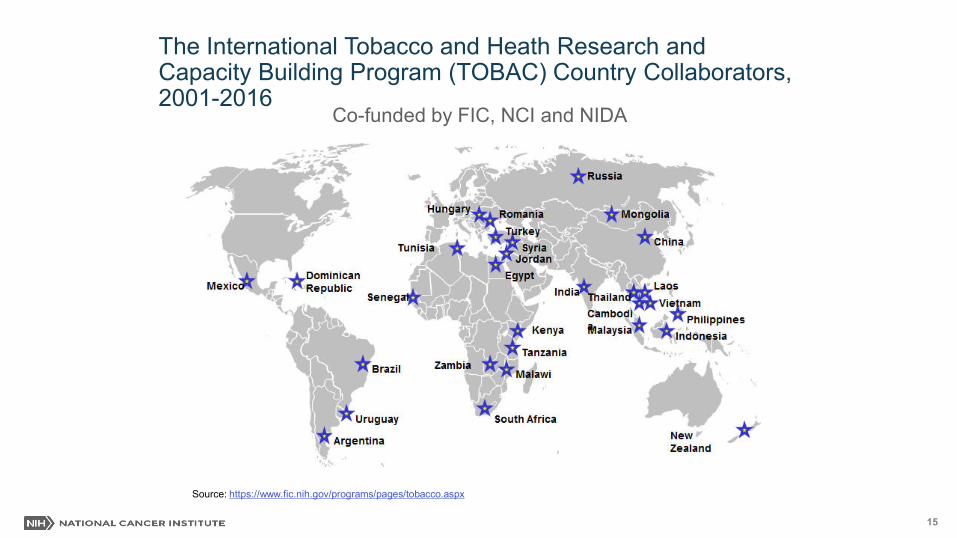
The International Tobacco and Heath Research and Capacity Building Program (TOBAC) Country Collaborators, 2001-2016
Source: https://www.fic.nih.gov/programs/pages/tobacco.aspx
Co-funded by FIC, NCI and NIDA
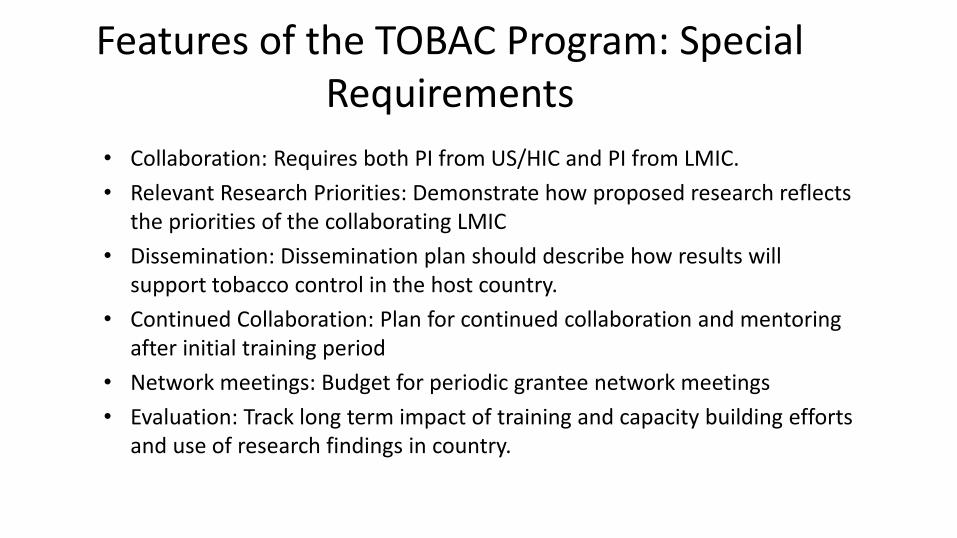
Features of the TOBAC Program: Special
Requirements
• Collaboration: Requires both PI from US/HIC and PI from LMIC.
• Relevant Research Priorities: Demonstrate how proposed research reflects
the priorities of the collaborating LMIC
• Dissemination: Dissemination plan should describe how results will
support tobacco control in the host country.
• Continued Collaboration: Plan for continued collaboration and mentoring
after initial training period
• Network meetings: Budget for periodic grantee network meetings
• Evaluation: Track long term impact of training and capacity building efforts
and use of research findings in country.
Rationale:
Growth in waterpipe smoking in Eastern Mediterranean region and other
parts of the world, especially among young adults, combined with
widespread misperceptions that waterpipe smoking is less harmful and
addictive than cigarette smoking.
Specific Aims:
• Develop health warning labels specific to waterpipe tobacco smoking
using focus groups in Lebanon and Tunisia
• Evaluate warning labels with 400+ young adults (18 – 25 years) in each
country assessing reaction, harm perception, quit intentions, and
perceived effectiveness
• Key informant interviews with government officials and NGOs to assess
capacity and possible barriers to implementation
Translating evidence and building capacity to support waterpipe
control in the Eastern Mediterranean (PI: Maziak, W.)
18
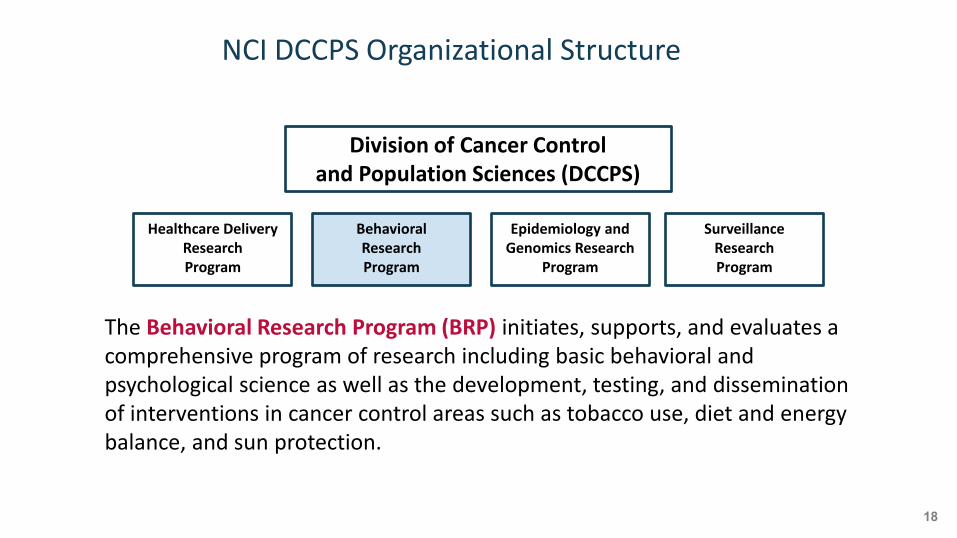
NCI DCCPS Organizational Structure
Division of Cancer Control
and Population Sciences (DCCPS)
Epidemiology and
Genomics Research
Program
Behavioral
Research
Program
Healthcare Delivery
Research
Program
Surveillance
Research
Program
The Behavioral Research Program (BRP) initiates, supports, and evaluates a
comprehensive program of research including basic behavioral and
psychological science as well as the development, testing, and dissemination
of interventions in cancer control areas such as tobacco use, diet and energy
balance, and sun protection.
cancercontrol.cancer.gov/brp/
19
How We Fund Grants
Although most of our portfolio consists of investigator-initiated (unsolicited) grants,
BRP also supports grant applications in specific areas of interest
Requests for Applications (RFA)
Identifies the specific receipt date(s), the estimated amount of funds earmarked for the initiative, the
number of awards likely to be funded, and any specific criteria for scientific peer review; applications
re ei ed in response to a parti ular RFA are re ie ed y an Institute’s S ientifi Re ie Group
Program Announcements (PA)
Most PA applications are submitted with a standing receipt date and are reviewed with all other
applications received at that time using standard peer-review processes
Program Announcement (PAR)
Program announcements with special receipt, referral, and/or review considerations
For more information: cancer.gov/grants-training/grants-process/grants-process.pdf
20
Grant Recipients
A grant provides federal financial assistance, including money, property, or both to an eligible
entity to perform approved scientific activities with little or no government involvement
Nonprofit organizations
For-profit organizations
Institutions of higher education
Hospitals
Research foundations
State, local, and tribal governments
Federal institutions
Foreign institutions and international organizations (varies by announcement)
Other organizations (e.g., school districts, faith-based, public housing)
See each FOA for scientific disciplines of interest and transdisciplinary considerations For more information: cancer.gov/grants-training/grants-process/grants-process.pdf
21
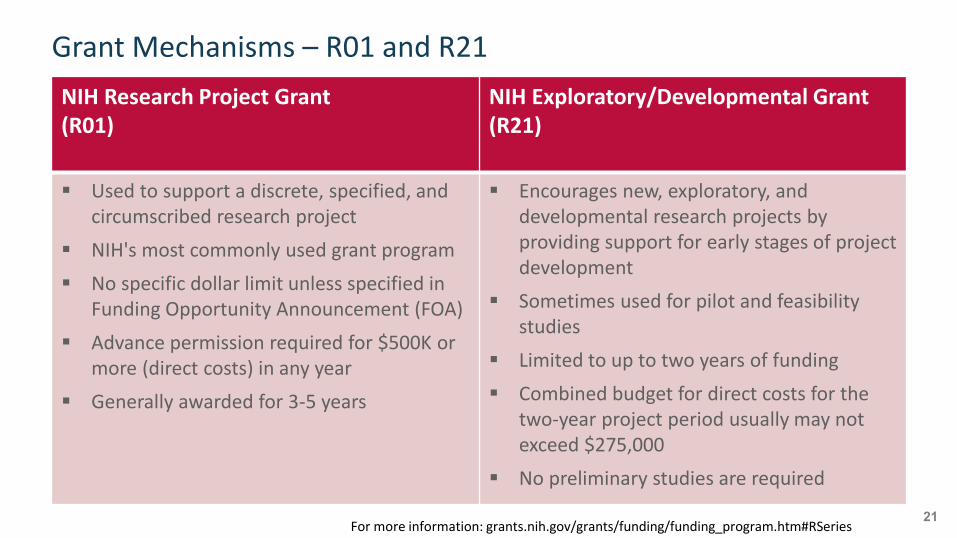
Grant Mechanisms – R01 and R21
NIH Research Project Grant
(R01)
NIH Exploratory/Developmental Grant
(R21)
Used to support a discrete, specified, and
circumscribed research project
NIH's most commonly used grant program
No specific dollar limit unless specified in
Funding Opportunity Announcement (FOA)
Advance permission required for $500K or
more (direct costs) in any year
Generally awarded for 3-5 years
Encourages new, exploratory, and
developmental research projects by
providing support for early stages of project
development
Sometimes used for pilot and feasibility
studies
Limited to up to two years of funding
Combined budget for direct costs for the
two-year project period usually may not
exceed $275,000
No preliminary studies are required
For more information: grants.nih.gov/grants/funding/funding_program.htm#RSeries
22
Tobacco Use and HIV in Low and Middle Income
Countries (LMICs)
PAR-17-087 (R01) & PAR-17-086 (R21) Contact:
Mark Parascandola
301-841-5474
Funding Announcements
Tobacco Use and HIV in Low and Middle Income Countries (LMICs)
PAR-17-087 [R01]
https://grants.nih.gov/grants/guide/pa-files/PAR-17-087.html
PAR-17-086 [R21]
https://grants.nih.gov/grants/guide/pa-files/PAR-17-086.html
National Institute on Drug Abuse (NIDA) is participating with NCI
Grants can be submitted to either NIDA or NCI, and either Institute can be named as a secondary assignment
Goals of Funding Announcement
Encourage research focused on tobacco use and HIV/AIDS in low and middle income countries (LMICs). In particular, applications are encouraged that focus on the development and evaluation of tobacco cessation interventions tailored to HIV positive populations, including those with co-morbidities such as tuberculosis (TB), in low-resource settings.
Novel, transdisciplinary nature of addressing tobacco use in context of HIV in LMICs
Bring together investigators from diverse disciplines and research foci to pool their efforts on this syndemic
Encourage sharing of research strategies and data across disciplines and geographic regions
Dedicated review group with experience in LMICs and both tobacco and HIV
PAR = no set aside funding
Background: Tobacco and HIV/AIDS
Smoking prevalence higher among PLHIV compared with general
population
PLHIV who smoke tobacco suffer greater morbidity and mortality than
non-smoking counterparts
PLHIV who smoke have higher risk of infection, greater progression from
HIV to AIDS, and weaker response to anti-retroviral therapy (ART)
Introduction of ART has led to decline in AIDS mortality and increased
life expectancy for PLHIV, increasing risk for NCDs and related behavioral
risk factors
Existing HIV and TB prevention and treatment guidelines do not include
a focus on tobacco use
Opportunities and Challenges
HIV and TB treatment context provides opportunity to intervene around tobacco use
Existing infrastructure for community interventions
Diagnosis of HIV/AIDS or TB provides teachable moment
However, smoking cessation interventions for PLHIV present additional challenges
Lower cessation rates
Complications with other substance abuse, mental illness, socio-economic status
Bulk of the evidence base for tobacco cessation comes from HICs
LMICs may have limited access to pharmacologic treatments, fewer trained health professionals, weaker tobacco control policies
Need for tailored interventions in LMIC context
Sample of Example Research Questions
What types of tobacco cessation interventions are most effective in persons with HIV,
with or without TB co-infection, to achieve improved tobacco abstinence as well as
disease treatment outcomes in low-resource environments?
What are the barriers to integrating tobacco control interventions into the existing HIV
and TB prevention and treatment context in LMICs?
What is the cost-effectiveness of integrating smoking cessation within HIV and TB
treatment? What interventions can be effectively introduced to low-resource settings in
LMICs?
How does the social and behavioral context of tobacco use in PLHIV in LMICs, including
the use and abuse of other substances, influence tobacco use behavior and cessation
outcomes?
What policy interventions could be embedded in HIV and TB control programs that
would serve to improve the outcomes of cessation or prevention efforts at both a clinical
and population level?
28
Evaluation Criteria
Standard Review Criteria:
Significance, Investigator(s), Innovation, Approach, Environment
Specific to this FOA:
Is the study or intervention appropriate for LMIC settings?
Can the intervention be scaled up and implemented in the setting in which it is being
studied?
Does the project provide a well-developed plan for dissemination of research results
to the LMIC countries where the research is taking place?
29
Other Important Information
Applications will be evaluated by reviewers with relevant expertise in HIV/AIDS,
tobacco control, and global health
R01s are 3-5 year grants, which require preliminary studies
R21s are 2-year grants, which are considered exploratory and do not require
preliminary studies
Non-domestic (non-U.S.) Entities (Foreign Institutions) are eligible to apply.
Grants ith dire t osts ≥ $500,000 in any year require Program approval for
submission
Submit materials to Program Director at least 8 weeks prior to receipt
https://grants.nih.gov/grants/guide/notice-files/NOT-CA-02-029.html
https://grants.nih.gov/grants/guide/notice-files/NOT-OD-02-004.html
30
Improving Smoking Cessation
in Socioeconomically Disadvantaged Populations
via Scalable Interventions
PAR-16-202 (R01) & PAR-16-201 (R21) Contact:
Yvonne Hunt
240-276-6975
31
Improving Smoking Cessation – R01/R21
Background – Smoking in the U.S. is increasingly concentrated among
socioeconomically disadvantaged (SED) populations, leading to marked
smoking-related health disparities
SED populations have less access to empirically validated treatments, face
more obstacles to engage in and maintain behavior change, and are less likely
to use treatments
PAR Purpose – Develop and test scalable smoking cessation interventions
with the potential to improve cessation outcomes among socioeconomically
disadvantaged populations
32
Improving Smoking Cessation – R01/R21
Emphasis:
Interventions that have the potential to be scalable, implementable, and
sustainable in real-world settings
General Research Approaches:
Test enhancements of interventions currently scaled or ready to scale
Evaluation of existing interventions which could be scaled if evidence supports
Requirements:
Justify how the intervention can be scaled and packaged for broad use
Propose a testable hypothesis related to the scalability of the intervention
33
Improving Smoking Cessation – R01/R21
Example Research Questions:
In what ways can scalable interventions be developed or modified to
increase engagement with treatment and enhance long-term behavioral
change?
What strategies might be used to systematically increase access to and
utilization of cessation services in socioeconomically disadvantaged
populations?
How might available infrastructures that provide services to
socioeconomically disadvantaged populations be utilized to also deliver
smoking cessation interventions?
34
Improving Smoking Cessation – R01/R21
Targeted Subpopulations – SED smokers (e.g., low income, low educational
attainment, un- or underemployed, un- or underinsured, racial/ethnic
groups living in low-resource communities, other disadvantaged groups such
as veterans, incarcerated)
Transdisciplinary Approach – Teams may include public health, clinical,
behavioral, and social scientists, statisticians, economists, technology
developers, researchers with expertise in dissemination and implementation
Not Intended to Support:
Observational studies describing factors that influence cessation behavior,
treatment engagement, implementation or dissemination in real-world
contexts; studies for which smoking cessation is not an end-point; studies to
test interventions for cessation of non-combustible tobacco products
35
Mobile Health: Technology and Outcomes in
Low and Middle Income Countries (R21)
PAR-16-292 (R21) Contact:
Mark Parascandola
301-841-5474
36
Mobile Health: Technology and Outcomes in Low and Middle Income Countries (R21)
Background – Enormous potential for mobile technology to transform
health care, personal health management, and basic health research.
The potential of mHealth is especially relevant to LMICs, where cell
phone ownership is rising rapidly, but access to health care and
providers is often limited. While there has been a large increase in
interventions that use mobile phones, research on these interventions
is often lacking.
Definition of mHealth – The use of mobile and wireless devices (cell
phones, tablets, etc.) to improve health outcomes, health care
services, and health research.
37
Research Objectives
This FOA encourages research projects that study the
development/adaptation of mHealth interventions for the prevention,
diagnosis, management, and treatment of specific health conditions.
Applicants are encouraged to propose research projects that have the
potential to provide an understanding of principles underlying effective
mHealth interventions or tools that are generalizable to the field.
This initiative aims to support projects that adapt or develop
technologies that are appropriate for LMIC settings. A plethora of
mHealth applications and devices have been developed in high-
income countries, however, these technologies are not necessarily
suitable for the needs of individuals in LMICs.
38
Special Requirements
All projects are required to involve partnerships between U.S. and
LMIC researchers and to develop mHealth research capacity at LMIC
institutions that can continue beyond the period of the grant.
Applicants should consider appropriate collaborations with
researchers from diverse disciplines such as behavioral science,
engineering, computer science, business, medicine, public health,
and/or other relevant fields.
In addition, applicants should consider partnering with individuals in
public or private organizations, including health system entities, which
could enable future research or implementation efforts within the
relevant LMIC.
39
Other Important Information
Non-domestic (non-U.S.) Entities (Foreign Institutions) are eligible to apply.
Participating NIH Institutes and Centers include: Fogarty International Center,
National Cancer Institute, National Institute on Deafness and Other
Communication Disorders, National Institute of Mental Health, National
Institute of Biomedical Imaging and Bioengineering
FIC Contact: Laura Povlich, Ph.D.
Fogarty International Center (FIC (http://www.fic.nih.gov))) Telephone: 301-
827-2227
Email: [email protected] (mailto:[email protected])
NCI Contact: Vidya Vedham, Ph.D.
National Cancer Institute (NCI (http://www.nci.nih.gov/)) Telephone: 240-276-
7272
Email: [email protected] (mailto:[email protected])

Questions
Tobacco and HIV in Low and Middle Income Countries (LMICs)
41
Are these funding opportunities only offered to interventions
conducted in the U.S.? Are projects conducted overseas going
to be funded? Do you have to be a U.S. citizen or have a green
card to apply for funds?
42
Can a new investigator receive special accommodation in
review?
43
Resources for New Funding Announcements
Funding Opportunities, Webinars and list of FAQs for funding announcements:
http://cancercontrol.cancer.gov/funding-foa-applicants.html
There, you can also find links to FOAs and Program Director contact information
Connect with any BRP staff member via contact information listed on:
http://staffprofiles.cancer.gov/brp/
Email questions to BRP anytime at [email protected]
Subscribe or unsubscribe from NCI/BRP email updates at
http://cancercontrol.cancer.gov/brp/e-newsletter/subscribe.html
1 - 8 0 0 - 4 - C A N C E R
U.S. Department of Health & Human Services
National Institutes of Health | National Cancer Institute
cancercontrol.cancer.gov/brp
Produced February 2017