Embed Size (px)
Citation preview

Resolution of clonal origins forendometriotic lesions using laser capturemicrodissection and the human androgenreceptor (HUMARA) assay
Yan Wu, Ph.D.,a Zainab Basir, M.D.,b Andre Kajdacsy-Balla, M.D., Ph.D.,b
Estil Strawn, M.D.,c Virgilia Macias, M.D.,b Kami Montgomery, B.S.,a andSun-Wei Guo, Ph.D.a
Medical College of Wisconsin, Milwaukee, Wisconsin
Objective: To determine the clonal origins of endometriotic lesions using laser capture microdissection andPCR-based HUMARA assay.
Design: Molecular genetic study of human tissue.
Setting: Molecular genetics laboratory in an academic setting.
Patient(s): Twenty patients with endometriosis. Forty specimens of endometriotic lesions from these patientsand one specimen of normal endometrium were analyzed.
Intervention(s): Laser capture microdissection was used to harvest epithelial cells from single and multifocalendometrial lesions from paraffin-embedded and frozen tissues, and their clonality was determined with theHUMARA assay.
Main Outcome Measure(s): Polymerase chain reaction–based HUMARA assay of clonality.
Result(s): Thirty-eight specimens were polymorphic and thus informative. Most specimens were monoclonal,as determined by the HUMARA assay. In four specimens of multifocal lesions, polyclonality was detected,but upon more refined microdissections and further analyses, we found that each focus was monoclonalindividually.
Conclusion(s): Previously reported polyclonality is very likely to be attributed to the pooling of multifocallesions or contamination of normal tissues. These results suggest that endometriotic lesions were monoclonalin origin, and in the case of multifocal lesions, each focus originates monoclonally; hence, different foci haveindependent origins. The monoclonality of endometriotic lesions suggests that they may carry neoplasticpotentials, and the apparent independent origins of multifocal lesions suggest that reconstruction of individuallesion histories may help us to understand the initiation and progression of endometriosis. (Fertil Steril� 2003;79(Suppl 1):710–7. ©2003 by American Society for Reproductive Medicine.)
Key Words: Endometriosis, clonality, laser capture microdissection, HUMARA assay, X-inactivation
Endometriosis is defined as the ectopic pres-ence of endometrial glands and stroma (1, 2). Itis a common gynecological disorder, affecting1–22% women of reproductive age, dependingon the screening procedures and populations(2, 3). The disorder is closely associated withdysmenorrhea, pelvic pain, and subfertility (4).Although it generally follows a benign course,its relationship with endometrioid and clearcell cancers of the ovary has long been sus-pected (5, 6).
Despite its high prevalence, the pathogene-sis of endometriosis still remains poorly under-
stood. Several theories regarding its etiologyhave been proposed, and these hypotheses canbe divided into three themes: in situ develop-ment (such as coelomic metaplasia or embry-onic cell rests), implantation, or a combinationof in situ development and implantation. Theimplantation theory of Sampson (7) is the mostwidely accepted, which stipulates that viableendometrial cells regurgitate through the fallo-pian tubes during menstruation to implant andgrow in peritoneum or other ectopic sites.
It has been well recognized that endometri-osis sometimes behaves as a tumor like lesion
Received May 7, 2002;revised and acceptedAugust 22, 2002.This research wassupported in part by agrant from theEndometriosis Association,Milwaukee, Wisconsin, andby a Pilot Project Grantfrom the Medical Collegeof Wisconsin.Reprint requests: Sun-WeiGuo, Ph.D., Department ofPediatrics, Medical Collegeof Wisconsin, 8701Watertown Plank Road,MS 756, Milwaukee,Wisconsin 53226-0509(FAX: 414-456-6663;E-mail: [email protected]).a Department of Pediatrics.b Department of Pathology.c Department of Obstetricsand Gynecology.
FERTILITY AND STERILITY�VOL. 79, SUPPL 1, MARCH 2003
Copyright ©2003 American Society for Reproductive MedicinePublished by Elsevier Science Inc.
Printed on acid-free paper in U.S.A.
0015-0282/03/$30.00doi:10.1016/S0015-0282(02)04821-5
710

(8) and that it displays some characteristics similar to ma-lignancy, such as invasion and metastasis. Cytogenetic stud-ies demonstrate that there are aberrant somatic genetic alter-ations, such as loss of heterozygosity (LOH) and DNAaneuploidy (6, 9–12), which are also hallmarks of cancer(13). Because it is well known that most neoplasms aremonoclonal in origin (14, 15), a better understanding ofclonal origins of endometriotic lesions should shed new lighton the initiation and progression of the disease. For example,if monoclonality of endometriotic lesions is firmly estab-lished, it may be possible to reconstruct lesion historiesthrough molecular genetic techniques. In addition, if multi-focal lesions are polyclonal yet each focus is monoclonal,that would suggest independent origins of these lesions, andthe reconstruction and comparison of lesion histories formultifocal lesions would reveal a great deal of the naturalhistory of lesions.
Several recent studies have reported that epithelial cellsfrom a single endometriotic lesion are mostly monoclonal inorigin (16–20). In about 18–40% of the cases, however,polyclonality could not be unequivocally ruled out (16–18,20). This apparent polyclonality has been attributed to pos-sible contamination of stromal cells, which are polyclonal(20), because the tissue samples used were scraped off ormanually microdissected (18, 20). It also could be presentonly at some periods of lesion development, as speculated byYano et al. (20). Although manual scraping can achievegood precision, it requires skills, patience, and manual dex-terity. As careful as one may be, manual scraping alwaysentails the risk of contamination with nonepithelial cellssuch as macrophages and fibroblasts. Hence, it is still unclearwhether the apparent polyclonality is genuine or due tocontamination. If the polyclonality in a certain percentagesof cases is proven to be genuine, then this may suggest amore complex and heterogeneous nature in the initiation andprogression of endometriosis. If the chance of contaminationcan be minimized and monoclonality of each focus is provenafter more precise tissue preparations, then reconstruction oflesion histories may be possible, and the neoplastic nature ofendometriosis is more certain.
In this study, we analyzed the largest sample size ofendometriotic lesions reported in the literature thus far usingthe HUMARA assay. The HUMARA assay allows the de-termination of clonality for cells derived from a femalesubject, based on patterns of X-chromosome in activations.In addition, we used a newly developed tissue microdissec-tion technique (21), laser capture microdissection (LCM), toharvest epithelial cells of endometriotic lesions and analyzedtheir clonality. The use of LCM allows for rapid, accurate,and reliable acquisition of cells of the desired type fromspecific microscopic regions of tissue sections under directvisualization, which in turn permits molecular genetic anal-ysis of pure populations of epithelial cells taken from lesionsamples. It greatly minimizes or even eliminates any possi-
bility of contamination. Furthermore, we examined clonalorigins of multifocal lesions.
MATERIALS AND METHODS
SpecimensThe sample collection and the use of materials for this
research were approved by the institutional review board ofthe Medical College of Wisconsin. Forty specimens of en-dometriotic lesions from 20 patients, classified as havingstage II to IV endometriosis based on the criteria establishedby the American Fertility Society, and one normal endome-trial tissue specimen were used in this study. Samples from19 patients were archival formalin-fixed, paraffin-embeddedsurgical tissues obtained from the pathology department ofthe Medical College of Wisconsin. One additional optimumcutting temperature (OCT) (Sakura Finetek, Torrance, CA)-embedded, fresh-frozen tissue specimen was obtained from apatient who underwent anterior abdominal wall surgery forremoval of symptomatic endometriotic tissue from an oldcesarean section scar. All cases were diagnosed and inde-pendently reviewed by two experienced pathologists (A.K.B.and Z.B.).
Tissue Processing and StainingFive-micrometer histological sections of formalin-fixed,
paraffin-embedded tissue were mounted on uncharged, un-coated glass slides. After drying, slides were deparaffinizedand stained immediately or stored in 70% ethanol at 4°C for�72 hours. Also, 5-�m frozen tissue sections were mountedon the uncharged, uncoated slides, immediately fixed in 70%ethanol for 60 seconds, and stained immediately.
Mayer’s Hematoxylin and eosin-Y (Fisher Healthcare,Houston, TX) were filtered before staining. The slides wererinsed in distilled water for 15 seconds, then stained asfollows: stained in Mayer’s Hematoxylin solution for 60seconds, rinsed with distilled water for 15 seconds, thenplaced in 1� automation buffer (Biomeda Corp, Foster City,CA) for 15 seconds, fixed in 70% and 95% ethanol for 30seconds each, stained with eosin-Y for 10 seconds, dehy-drated twice in 95% ethanol for 30 seconds, and dehydratedtwice in absolute ethanol for 30 seconds, followed by incu-bation twice in xylene for �5 minutes each. The slides werethen air-dried for 20 minutes and stored in a desiccator untilLCM.
Laser Capture Microdissection and DNAExtraction
Laser capture microdissection was performed with a Pix-cell II laser capture microscope (Arcturus Engineering,Mountain View, CA). Epithelial cells were captured onthermoplastic caps (Arcturus Engineering) by using a 7.5-�m-diameter laser spot and 50 mW laser power. The averagenumber of cells captured on each cap from an individualendometriotic lesion and from normal endometrium wasapproximately 200 and 1,000, respectively. After microdis-
FERTILITY & STERILITY� 711
section, the caps were placed on 0.5 �L microfuge tubeswith 40 �L of proteinase K lysis buffer ([1 mg/mL protein-ase K � 1% Tween-20 in 1� Tris-HCl/EDTA (TE), pH 8.0],Sigma, St. Louis, MO). The samples were incubated over-night at 37°C, then for 10 minutes at 95°C to inactivate theproteinase K. One microliter of linear acrylamide (Ambion,Austin, TX) and 40 �L of isopropanol were added to the celllysis and mixed well. The mixtures were incubated at �20°Cfor 2 hours. The DNA was precipitated at 16,000 � g at 4°Cfor 25 minutes, and was resuspended in 5–8 �L of 1� TEbuffer.
Restriction Enzyme HapII Digestion and PCRThe HapII digestion and PCR were performed as follows:
briefly, 4 �L of DNA extract was digested overnight at 37°Cwith or without 1 �L of HapII (10 U/�L) methylation-sensitive restriction endonuclease (Amersham PharmaciaBiotech, Piscataway, NJ) in a total volume of 10 �L. Afterdigestion, the samples were incubated at 95°C for 10 minutes
to inactivate the enzyme. Then DNA samples were amplifiedby two rounds of PCRs using primers specific for exon 1 ofthe HUMARA gene.
In round one PCR reaction, 4 �L of digested or non-digested DNA was amplified in total volume of 30 �Lcontaining: 3 �L of 10� reaction buffer (PE Biosystem,Boston, MA), 4.8 �L of dNTPs (1.25 mM each of dATP,dTTP, dCTP, and dGTP), 1.8 �L of 25 mM MgCl2, 0.15 �Lof AmpliTaq Gold polymerase (5 U/�L, PE Biosystem), and2 �L of the round-one primer pairs (22), 0.3 �M each(forward: 5�-TGTGGGGCCTCTACGATG-3�; reverse: 5�-TCCAAGACCTACCGA-3�), and 14.25 �L of DNAse/RNAse-free distilled water (Gibco, Rockville, MD). ThePCR reaction was performed in a Perkin-Elmer thermocyclerfor 28 cycles, each with 30 seconds at 95°C, 30 seconds at55°C, and 30 seconds at 72°C, with initial denaturation at95°C for 5 minutes. The round-two PCR reaction was per-formed with the same reaction mix as described above, 4 �L
F I G U R E 1
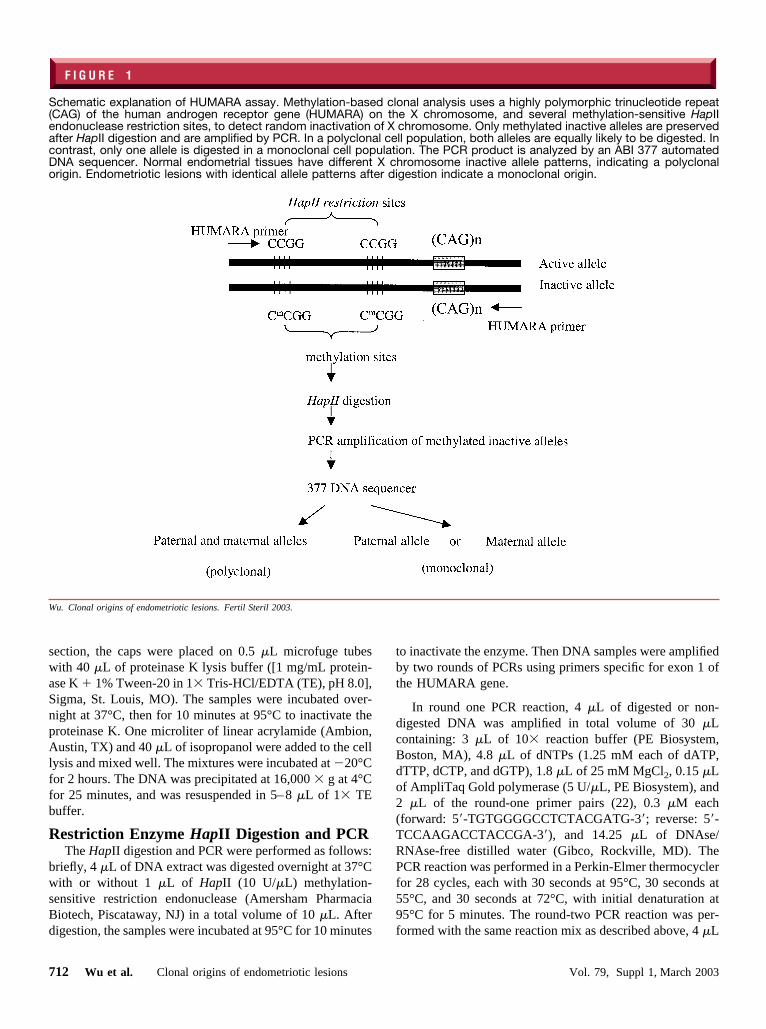
Schematic explanation of HUMARA assay. Methylation-based clonal analysis uses a highly polymorphic trinucleotide repeat(CAG) of the human androgen receptor gene (HUMARA) on the X chromosome, and several methylation-sensitive HapIIendonuclease restriction sites, to detect random inactivation of X chromosome. Only methylated inactive alleles are preservedafter HapII digestion and are amplified by PCR. In a polyclonal cell population, both alleles are equally likely to be digested. Incontrast, only one allele is digested in a monoclonal cell population. The PCR product is analyzed by an ABI 377 automatedDNA sequencer. Normal endometrial tissues have different X chromosome inactive allele patterns, indicating a polyclonalorigin. Endometriotic lesions with identical allele patterns after digestion indicate a monoclonal origin.
Wu. Clonal origins of endometriotic lesions. Fertil Steril 2003.
712 Wu et al. Clonal origins of endometriotic lesions Vol. 79, Suppl 1, March 2003
of the primary PCR product as template, and 2 �L ofround-two primer pairs (23), 0.3 �M each (forward: 5�-CCGAGGAGCTTTCCAGAATC-3�; reverse: 6-FAM la-beled 5�-TACGATGGGCTTGGGGAGAA-3�). The reac-tion was performed for 20 cycles each with 30 seconds at95°C, 30 seconds at 58°C, 30 seconds at 72°C, and an initialdenaturation at 95°C for 5 minutes. Polymerase chain reac-tion products were then stained with ethidium bromide andchecked on an 0.8% agarose gel.
Fragment AnalysisOne microliter of PCR product, 2.5 �L DI formamide (PE
Biosystem), 0.5 �L of 400HD[ROX] size standard (PE Bio-system), and 0.5 �L of loading buffer (500 mg/mL bluedextran and 25 mM ethylenediaminetetraacetic acid) weremixed and denatured at 95°C for 4 minutes, then immedi-ately cooled on ice. Of the mixture, 1.5 �L of the mixturewas loaded and separated on 10% denaturing polyacryl-amide gel on an ABI 377 automated laser-fluorescent se-quencer (PE Biosystem). Fluorescence-labeled fragmentswere automatically analyzed by GeneScan version 3.1.2 (PEBiosystem).
RESULTS
HUMARA AssayThe methylation-sensitive endonuclease enzyme HapII
recognition site is closely linked to the polymorphic CAGrepeat. If the subject is heterozygote at the HUMARA locus,then the PCR products of the HUMARA after HapII diges-tion displaying two different alleles would indicate poly-clonal origin, whereas the displaying of only one allelewould indicate monoclonality (Fig. 1). In our study, we havefound that 90% (18 of 20) of the patients have heterozygousgenotype for the HUMARA gene. This is consistent with thereported heterozygosity frequency of the HUMARA gene(24).
Epithelial Cells Isolated by LCMEpithelial cells were distinctly captured from the sections
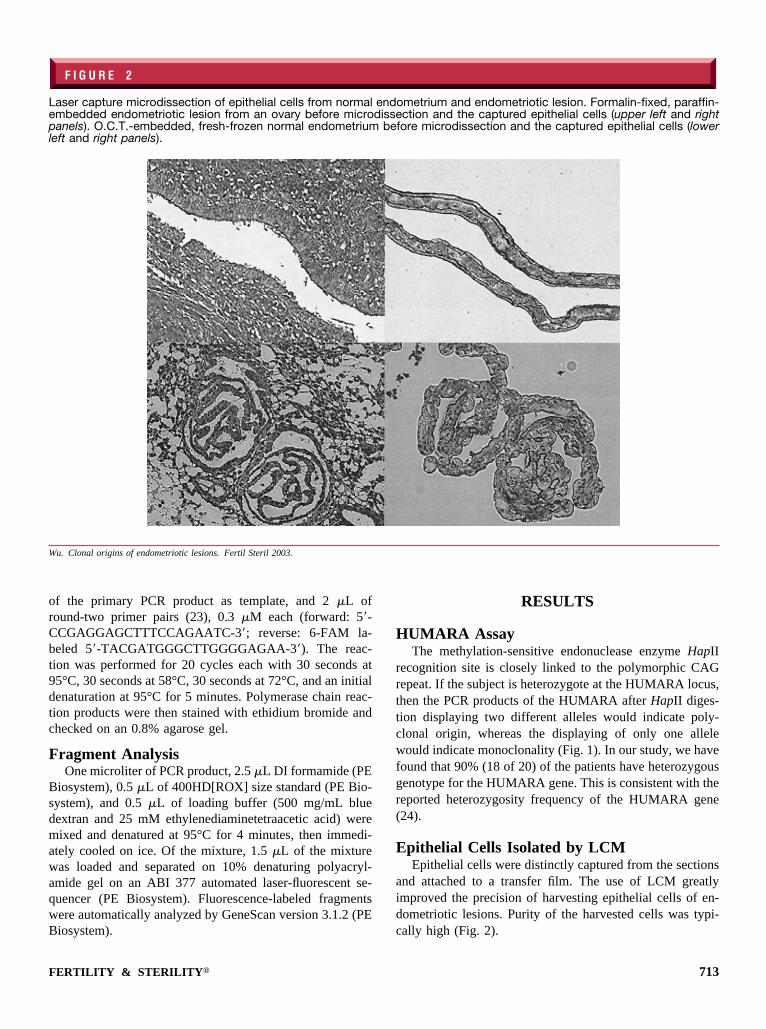
and attached to a transfer film. The use of LCM greatlyimproved the precision of harvesting epithelial cells of en-dometriotic lesions. Purity of the harvested cells was typi-cally high (Fig. 2).
F I G U R E 2
Laser capture microdissection of epithelial cells from normal endometrium and endometriotic lesion. Formalin-fixed, paraffin-embedded endometriotic lesion from an ovary before microdissection and the captured epithelial cells (upper left and rightpanels). O.C.T.-embedded, fresh-frozen normal endometrium before microdissection and the captured epithelial cells (lowerleft and right panels).
Wu. Clonal origins of endometriotic lesions. Fertil Steril 2003.
FERTILITY & STERILITY� 713

Clinical Diagnosis and Clonality AnalysisThe results are summarized in Table 1. Thirteen patients
had unilateral ovarian endometriotic lesions only, and fourpatients had bilateral ovarian lesions. The remaining of threepatients had lesions located on the peritoneal surfaces, pos-terior serosa of uterus, and adnexa, respectively (Table 1).
In two patients (cases 4 and 10), the patterns of X chro-mosome inactivation showed only one allelic peak evenbefore digestion, indicating that they were homozygous atthe HUMARA locus. Of the remaining 18 informative cases,12 (cases 1–3, 5–9, 13, 14, 16, and 18) showed randominactivation patterns of the X chromosome (Fig. 3), a featureof monoclonality. In cases 15, 17, and 20, when epithelialcells from two foci were harvested by LCM and pooled forHUMARA assay, we found that both allelic peaks werepresent after digestion (Table 1), indicating that the analyzedcell populations were polyclonal. Suspecting that the mixtureof different foci could result in polyclonality, we then mi-
crodissected each focus individually using LCM and sub-jected them to HUMARA assay separately from the otherfoci. Indeed, we found that two lesions from the same patienthad different allelic patterns (Fig. 4). These results suggestedthat although epithelial cells pooled from multiple foci arepolyclonal, each individual focus is monoclonal in origin.
Among four cases of bilateral ovarian lesions, three (cas-es 11, 12, and 20) showed an identical allelic pattern betweenlesions after digestion, whereas one (case 19) showed diver-gent allelic patterns between lesions after digestion. Becausemethylation is random, the identical allelic patterns for bi-lateral lesions gave no information regarding their clonalorigins even though one could still determine that eachindividual lesion was monoclonal. However, in one case inwhich there were different allelic patterns for bilateral le-sions (case 19), it indicated that the two lesions had mono-clonal origins, but each lesion arose from a different clone.
DISCUSSION
In this study with by far the largest number of specimens,we have demonstrated using LCM and HUMARA assay thateach and every focus of endometriotic lesions is monoclonal.Although in three cases the initial clonality analyses usingcells microdissected from multifocal lesions indicated poly-clonality, further, refined microdissection of each individualfocus and subsequent clonality analysis indicated that eachindividual focus was monoclonal. In addition, we demon-strated that in cases of bilateral ovarian lesions the lesionsare not derived from the same clone, which is consistent withfindings of Jimbo et al. (23).
Although our results further confirmed the findings byprevious investigators (16–20) that most endometriotic le-sions are monoclonal, our analysis of cases with more thanone focus demonstrated that each minute focus is monoclo-nal, although these foci are physically so close that theyappear to the naked eye to be part of the same lesion. Thisfinding suggested one alternative, and, in our view, a morelikely possibility for the apparent polyclonality in previousreports. That is, besides contamination of stromal cells, themixture of cells from neighboring lesions can also produceapparent polyclonality.
Our results strongly indicate that each focus of endometri-otic lesion originates from a single progenitor cell and that,in the case of multifocal lesions, the lesions have indepen-dent origins. Although these findings in and by themselvesdo not directly support any specific theory of endometriosisetiology, they nonetheless are consistent with the most pop-ular theory of retrograde menstruation, because from a pieceof shed endometrium, polyclonal in origin, a single cellcould implant and grow into a focus of endometriosis. Thesefindings also suggest that given the physical proximity of
T A B L E 1
Summary of results.
Caseno.
Age atexamination
(y) Location of lesion
No. ofanalyzed
fociInactivated
alleles
1 29 Left ovary 1 L2 33 Left ovary 1 L3 29 Left ovary 1 L4 28 Left ovary 2 NI5 36 Right ovary 2 S6 43 Left ovary and tube 2 L7 25 Left ovary 2 S8 40 Peritoneal implant 2 S9 46 Left adnexa 2 S
10 35 Left ovary 2 NI11 34 Right ovary 2 L
Left ovary 1 L12 28 Right ovary 1 S
Left ovary 1 S13 47 Right ovary 2 L14 23 Left ovary 1 S15 42 Uterus 2 L/S3L,S
Uterus 1 S16 32 Left ovary 2 L17 31 Right ovary 2 L/S3L,S
Right ovary 1 L18 34 Right ovary 1 S19 27 Right ovary 1 L
Left ovary 1 S20 50 Right ovary 1 L
Left ovary 1 LLeft paraovarian 1 LLeft paraovarian 1 S
Note: NI � noninformative (homozygous); S � shorter allele; L � longerallele; L/S � heterozygous (polyclonal).
Wu. Clonal origins of endometriotic lesions. Fertil Steril 2003.
714 Wu et al. Clonal origins of endometriotic lesions Vol. 79, Suppl 1, March 2003

F I G U R E 3
Representative results of clonality assays. Methylation patterns with or without HapII digestion of epithelial cells fromendometriotic lesion are shown. A significant reduction of one of the alleles is observed after HapII digestion in all represen-tative cases, indicating a monoclonal origin. Epithelial cells from normal endometrium served as control and exhibited the samemethylation pattern with or without HapII digestion, indicating a polyclonal origin.
Wu. Clonal origins of endometriotic lesions. Fertil Steril 2003.
F I G U R E 4
Laser capture microdissection of two endometriotic lesions from the left paraovary of case 20 and their clonal properties. Theepithelial cells from lesions 1 and 2 were selectively isolated and transferred to film. After HapII digestion, the shorter allele fromlesion 1 was completely deleted, whereas the longer allele from lesion 2 was significantly reduced, indicating their independentorigins.
Wu. Clonal origins of endometriotic lesions. Fertil Steril 2003.
FERTILITY & STERILITY� 715

multifocal lesions and their polyclonal origins, metastasisfrom a monoclonal endometrial lesion may be unlikely.Monoclonality does argue against the metaplasia theory,where celomic epithelium would convert into glandular ep-ithelium. Of course, this does not exclude a role for otherendometriotic cells or even stroma cells in the process ofadhesion and development of the lesion as facilitators orwith paracrine action.
In view of this, the progression of endometriosis can bethought to occur through successions of selection and clonalexpansion, as in neoplasia (15, 25). The monoclonality ofendometriotic lesions implies that because all current cells inthe lesion are descendants of a single progenitor cell, its cellgenealogy or history could be potentially reconstructed. Thishistory, once reconstructed, possibly through molecular bi-ology methods, would permit a comparison of lesion histo-ries among multiple lesions in a patient, and once correlatedwith information on lesion sites and on other clinical vari-ables such as staging, age of onset, and recurrence, wouldshed new light on how lesions initiate and progress.
Studies by Jimbo and his coworkers (23) found that if thepurity of the harvested epithelial cells was �70%, the allelicratio increased significantly, rendering clonality determina-tion difficult. Because the stromal components of an endo-metriotic lesion are polyclonal (24), the precise capture ofepithelial cells from the lesion lining becomes critical to theaccuracy of clonality analysis. LCM has been proven to be atissue microdissection procedure that allows accurate, evensingle-cell, tissue sampling from small target tissues such asendometriotic lesions (21, 26–28). Using LCM, we candirectly check the purity of the captured cells by visualizingmicroscopically (shown in Fig. 2) and accurately harvestinga single or few cells of interest from small endometrioticlesions. Therefore, our results brought more certainty thatthe majority if not all of endometriotic lesions are monoclo-nal in origin and may thus carry a neoplastic potential.Furthermore, in all three apparently polyclonal cases, fur-ther, more refined microdissection of single-lesion focus andsubsequent clonal analysis indicated that each focus ismonoclonal, but mixing multifocal lesions resulted in poly-clonality.
In summary, we have used LCM and PCR-based HU-MARA assay to determine the clonality of endometrioticlesions. We analyzed 38 informative, LCM-collected endo-metriotic lesion specimens from 18 patients and found thatthey were all monoclonal. In the case where initial HU-MARA assays indicated polyclonality, further, more refinedmicrodissection and assay of individual focus each resultedin monoclonality. Our results demonstrated that the use ofLCM can not only eliminate contamination of unwanted celltypes but also permit more refined acquisition of cells froma single focus. These individual foci turned out to be mono-
clonal individually, although collectively they can be ofpolyclonal origin.
Acknowledgments: The authors thank Soumitra Ghosh, M.D., D. Phil., forhis support of this project and Obrad Kokanovic, B.Sc., for his excellenttechnical assistance.
References1. Heaps JM, Nieberg RK, Berek JS. Malignant neoplasms arising in
endometriosis. Obstet Gynecol 1990;75:1023–8.2. Olive DL, Schwartz LB. Endometriosis. N Engl J Med 1993;328:1759–
69.3. Mahmood TA, Templeton A. Prevalence and genesis of endometriosis.
Hum Reprod 1991;6:544–9.4. Farquhar CM. Extracts from the “clinical evidence.” Endometriosis.
BMJ 2000;320:1449–52.5. Vercellini P, Parazzini F, Bolis G, Carinelli S, Dindelli M, Vendola N,
et al. Endometriosis and ovarian cancer. Am J Obstet Gynecol 1993;169:181–2.
6. Jiang X, Morland SJ, Hitchcock A, Thomas EJ, Campbell IG. Allelo-typing of endometriosis with adjacent ovarian carcinoma reveals evi-dence of a common lineage. Cancer Res 1998;58:1707–12.
7. Sampson JA. Peritoneal endometriosis due to the menstrual dissemina-tion of endometrial tissue into the peritoneal cavity. Am J ObstetGynecol 1927;14:422–69.
8. Serov SF, Scully RE, Sobin LH. Histological typing of ovarian tu-mours. International histological classification of tumours. No. 9. Ge-neva, Switzerland: World Health Organization, 1973:51–3.
9. Ballouk F, Ross JS, Wolf BC. Ovarian endometriotic cysts. An analysisof cytologic atypia and DNA ploidy patterns. Am J Clin Pathol 1994;102:415–9.
10. Dangel A, Medchill MT, Davis G, Meloni AM, Sandberg AA. Cyto-genetic studies in endometriosis tissue. Cancer Genet Cytogenet 1994;78:172–4.
11. Shin JC, Ross HL, Elias S, Nguyen DD, Mitchell-Leef D, Simpson JL,et al. Detection of chromosomal aneuploidy in endometriosis by multi-color fluorescence in situ hybridization (FISH). Hum Genet 1997;100:401–6.
12. Gogusev J, Bouquet de Joliniere J, Telvi L, Doussau M, du Manoir S,Stojkoski A, et al. Detection of DNA copy number changes in humanendometriosis by comparative genomic hybridization. Hum Genet1999;105:444–51.
13. Duesberg P, Rausch C, Rasinck D, Hehlmann R. Genetic instability ofcancer cells is proportional to their degree of aneuploidy. Proc NatlAcad Sci USA 1998;95:13692–7.
14. Fialkow PJ. Clonal origin of human tumors. Biochim Biophys Acta1976;458:283–321.
15. Nowell PC. The clonal evolution of tumor cell populations. Science1976;194:23–8.
16. Nilbert M, Pejovic T, Mandahl N, Iosif S, Willen H, Mitelman F.Monoclonal origin of endometriotic cysts. Int J Gynecol Cancer 1995;5:61–3.
17. Jiang X, Hitchcock A, Bryan EJ, Watson RH, Englefield P, Thomas EJ,et al. Microsatellite analysis of endometriosis reveals loss of heterozy-gosity at candidate ovarian tumor suppressor gene loci. Cancer Res1996;56:3534–9.
18. Jimbo H, Hitomi Y, Yoshikawa H, Yano T, Momoeda M, Sakamoto A,et al. Evidence for monoclonal expansion of epithelial cells in ovarianendometrial cysts. Am J Pathol 1997;150:1173–8.
19. Tamura M, Fukaya T, Murakami T, Uehara S, Yajima A. Analysis ofclonality in human endometriotic cysts based on evaluation of Xchromosome inactivation in archival formalin-fixed, paraffin-embeddedtissue. Lab Invest 1998;78:213–8.
20. Yano T, Jimbo H, Yoshikawa H, Tsutsumi O, Taketani Y. Molecularanalysis of clonality in ovarian endometrial cysts. Gynecol ObstetInvest 1999;47(Suppl 1):41–5.
21. Emmert-Buck MR, Bonner RF, Smith PD, Chuaqui RF, Zhuang Z,Goldstein SR, et al. Laser capture microdissection. Science 1996;274:998–1001.
22. Raihanatou D, Karl-Ludwig S, Christopher P, Nazli S, Vivian W, HorstB, et al. Monoclonality in normal epithelium and in hyperplastic andneoplastic lesions of the breast. J Pathol 2001;193:27–32.
23. Jimbo H, Hitomi Y, Yoshikawa H, Yano T, Momoeda M, Yasugi T, etal. Clonality analysis of bilateral ovarian endometrial cysts. Fertil Steril1999;72:1142–3.
24. Allen RC, Zoghbi HY, Moseley AB, Roseblatt HM, Belmont JW.Methylation of HapII and HhaI sites near the polymorphic CAG repeat
716 Wu et al. Clonal origins of endometriotic lesions Vol. 79, Suppl 1, March 2003

in the human androgen-receptor gene correlates with X chromosomeinactivation. Am J Hum Genet 1992;51:1229–39.
25. Kinzler KW, Vogelstein B. Lessons from hereditary colorectal cancer.Cell 1996;87:159–70.
26. Bonner RF, Emmer-Buck M, Cole K, Pohida T, Chuaqui R, GoldsteinS, et al. Laser capture microdissection: molecular analysis of tissue.Science 1997;278:1481–3.
27. Bernsen MR, Dijikman HB, deVries E, Figdor CG, Ruitor DJ, AdemaGJ, et al. Identification of multiple mRNA and DNA sequences fromsmall tissue samples isolated by laser-assisted microdissection. LabInvest 1998;78:1267–73.
28. Sirivatanauksorn Y, Drury R, Crnogorae-Jurcevic T, SirivatanauksornV, Lemoine NR. Laser-assisted microdissection: applications in molec-ular pathology. J Pathol 1999;189:150–4.
FERTILITY & STERILITY� 717












![Postmenopausal Vaginal Endometriotic Cyst: A …Postmenopausal Vaginal Endometriotic Cyst 3 recurrence or occurrence of de novo lesions [2]. Ovarian estro-gen secreting tumors can](https://img.pdfslide.us/doc/110x75/5f0d71af7e708231d43a62cd/postmenopausal-vaginal-endometriotic-cyst-a-postmenopausal-vaginal-endometriotic.jpg)















