-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
1/67
AETIOLOGY AND MECHANISM OF INJURY OF MIDFACIAL FRACTURES: A
PROSPECTIVE STUDY OF THE JOHANNESBURG REGION.
YusufFaroukSuleman
AresearchreportsubmittedtotheFacultyofHealthSciences,Universityofthe
Witwatersrand,Johannesburg,inpartialfulfillmentoftherequirementsforthedegree
ofMasterofDentistryinMaxillofacialandOralSurgery.
Johannesburg2008
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
2/67
2
Candidatesdeclaration
I,YusufFaroukSuleman,declarethatthisresearchreportismyownwork.Itisbeing
submittedforthedegreeofMasterofDentistryinthebranchofMaxillofacialandOral
Surgery,intheUniversityoftheWitwatersrand,Johannesburg.Ithasnotbeen
submittedbeforeforanydegreeorexaminationatthisoranyotheruniversity.
______________dayof_____________________200__.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
3/67
3
Dedication
Bismillahhirrahmaanirraheem
Tomyparentswhonurturedandguidedme
Tomybeautifulwife,Yasmeen,forherundyinglove,dedicationandsupport.
Tomy
children
from
whom
Idraw
strength
and
happiness.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
4/67
4
ABSTRACT
Objective:
Todeterminetheaetiology,biomechanicsanddemographicsofpatients
withfractures
of
the
midface.
MaterialsandMethods:
Patientswithmidfacefractures(whoconsentedtoparticipate
inthestudy)whopresentedtotheDivisionofMaxillofacialandOralSurgeryovera12
monthperiodfromDecember2005toDecember2006wereincludedinthestudy.Data
wasrecordedonage,race,gender,dateandcauseofinjury,associatedinjuriesanduse
ofalcoholatthetimeofinjury.ThefracturesweregroupedintoLeFort,zygomatico
maxillary,dentoalveolarandpanfacialfractures.
Results:
Thesamplecomprised94patients;78(82.98%)malesand16(17.02%)females
withanagerangeof3to67years.
Blacksaccountedfor77.66%ofthetotalsample,
followedbyWhites(12.77%),Coloureds(6.38%)andAsians(3.19%).
Blunttraumadue
tointerpersonalviolence,motorvehicleaccidents,gunshotwoundsandfalls
contributedto40.5%,26.6%,13.8%and5.3%ofthefracturesrespectively.LeFort
fractureswere
lesscommonlyobservedthanzygomaticomaxillarycomplexmidface
fractures.
Conclusion:Arelationshipexistsbetweenfacialtrauma,povertyandalcohol
consumption.Blunttraumaduetointerpersonalviolenceisthemostcommoncauseof
midfaceinjuries.Majorityofinjuriesaresustainedduringweekends.
Zygomaticomaxillarycomplexfracturesarethemostcommonmidfacefractures.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
5/67
5
ACKNOWLEDGEMENTS
Iwishtoexpressmysinceregratitudetothefollowingpersons:
ProfessorJ.Lownie
BDS,MDENT(MFOS),FCMFOS(SA),PhD,DrE.RikhotsoBDS,MDENT(MFOS),FCMFOS(SA)andDr.N.DayaBDS,FCMFOS(SA)fortheirsupervision.
ProfessorP.E.CleatonJonesBDS(WITS),MBCHB,DA(SA),PhD,DTM&H,DPH,DSC.forhisexpertise,enthusiasmandstatisticalanalyses.
DrE.Rikhotsoforallhisencouragement,patience,wisdomandguidance.
Dr.E.Muthrayforhissupportandassistance.
Tomyfellowregistrarswithoutwhomthisresearchwouldnotbepossible.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
6/67
6
TABLEOFCONTENTS
TITLEPAGE 1
DECLARATION 2
DEDICATION 3
ABSTRACT 4
ACKNOWLEDGEMENTS 5
TABLEOFCONTENTS 6
LISTOFFIGURES 9
LISTOFTABLES 10
NOMENCLATURE 11
CHAPTER1:INTRODUCTION 12
1.1Applied
anatomy
12
1.1.1Zygoma 13
1.1.2Maxilla 14
1.1.3Nasalbones 15
1.1.4LacrimalBones 15
1.2
History
of
midfacial
fractures
and
their
management
16
1.3Classification 18
1.3.1Zygomaticfractures 18
1.3.2Maxillaryfractures 20
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
7/67
7
1.3.3Nasoorbitoethmoid(NOE)fractures 22
1.4SignsandSymptoms 25
1.4.1NOE 25
1.4.2Maxilla 26
1.4.3Zygoma 26
1.5LiteratureReview 27
1.6AimsandObjectives 31
CHAPTER2:MATERIALSANDMETHODS 32
2.1Ethicalclearance 32
2.2InclusionCriteria 32
2.3ExclusionCriteria 32
2.4ClinicalStudy 33
2.5DataAnalysis 36
CHAPTER3:
RESULTS
37
3.1Age,genderandracedistribution 37
3.2Natureofinjuryandsocialhabits 39
3.3SpecialInvestigations 42
3.4Typeoffracturessustained 43
3.5
Analyses
44
3.6Hardwarecosts 50
CHAPTER4:DISCUSSION 51
CHAPTER5:CONCLUSION 57
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
8/67
8
REFERENCES 58
APPENDIX 63
AppendixA EthicalClearance 63
AppendixB Patientinformationsheetandconsent 64
AppendixC Participationinformationdatasheet 66
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
9/67
9
LISTOFFIGURES
Figure1.1A&Bfacialbuttressofthemidfaceandarchitecturalmodelrespectively.
13
Figure1.2
Le
fort
I,II
&
III
fracture
lines
frontal
&
three
quarter
view
21
Figure1.3NOEtypeIfractureunilateralandbilateral 23
Figure1.4NOEtypeIIfractureunilateralandbilateral 23
Figure1.5NOEtypeIIIfractureunilateralandbilateral 24
Figure2.1Occipitomentalviewindicatingmultiplefacialfractures
34
Figure2.2SMVusedtoassessfracturesofthezygomaticarch. 34
Figure2.3ThreedimensionalCTscanindicatingmultiplefacialfractures.
35
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
10/67
10
LISTOFTABLES
Table3.1Frequencydistributionbyageindecades 37
Table3.2
Frequency
distribution
by
gender
38
Table3.3Frequencydistributionbyrace 38
Table3.4Frequencydistributionbynatureofinjury 39
Table3.5Frequencydistributionbyalcoholconsumption 40
Table3.6Frequencydistributionbylossofconsciousness 40
Table3.7Frequencydistributionbyassociatedinjuries 41
Table3.8Frequencydistributionbydayoftheweek 42
Table3.9Frequencydistributionbyradiographicinvestigations 43
Table3.10Frequencydistributionbyfracturespattern 44
Table3.11Analysisofalcoholconsumptionbymechanismofinjury 45
Table3.12Analysisofalcoholconsumptionbygender 45
Table3.13Analysisofgenderbymechanismofinjury 46
Table3.14Analysisofdecadebygenderandalcoholconsumption 47
Table3.15Analysisoffracturetypebyalcoholconsumption&mechanismofinjury
48
Table3.16Analysisoffracturetypebytreatment 49
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
11/67
11
NOMENCLATURE
ComputerTomography =CT Dentoalveolar =DA
HumanImmunodeficiencyvirus =HIV Nasoorbitoethmoid =NOE
Occipitomental =OM Orthopantomograph =OPG
OpenReductionInternalFixation =ORIF Submentovertex =SMV
Zygomaticomaxillarycomplex =ZMC
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
12/67
12
Chapter1Introduction
1.1AppliedAnatomyofthemidfacialbones
Themidfaceiscomposedofthenasal,zygoma,maxilla,ethmoidanditsconchae,
palatine,inferiorconchaandvomerwhicharecollectivelyreferredtoasthemiddle
thirdofthefacialskeleton.Thesefacialbonesinisolationarecomparativelyfragilebut
gainstrength
and
support
as
they
articulate
with
each
other.
1,
2
Itisthisstrengthgainedfromeachotherthathasoftenbeendescribedasthefacial
buttresseswhichManson3alludedtowhendescribingtheverticalandhorizontalstruts
thatsupportthefacialskeleton(Figure1.1).Thehorizontalpillarsareformedbythe
frontalbar(composedofthesupraorbitalrimsandnasalprocessofthefrontalbone),
thezygomaticarch,infraorbitalrims,andthenasalbridgeandfinallythealveolar
processofthemaxilla.
Theverticalpillarsareformedfirstlymediallybythepiriformrimswhichcontinue
superiorlyasthefrontalprocessofthemaxilla.Secondlythezygomaticbuttresseswhich
continuesuperiorlywiththelateralorbitalrimsformthelateralpillarsandfinallythe
mostcaudalpillarsarethepterygoidplates.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
13/67
13
Figure1.1A&Bindicatingfacialbuttressofthemidfaceandarchitecturalmodel
respectively.4
1.1.1
ZygomaThenamezygomaisderivedfromthewordmeaningayoke(i.e.astructurethat
connectsvariouspartstogether),whereitarticulateswiththetemporal,maxillary,
frontalandsphenoidbones.Itisoftendescribedasadiamondorpyramidalshaped
boneofwhichthelateralsurfaceisconvexformingtheprominenceofthecheek.The
posteriorsurface
contributes
to
the
temporal
fossa.
Projectingsuperiorlyisthefrontalprocesswhicharticulateswiththezygomaticprocess
ofthefrontalboneinfrontandgreaterwingofsphenoidbehindtoformthelateralwall
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
14/67
14
andrimoftheorbit.Posterolaterallythetemporalprocessarticulateswiththe
zygomaticprocessofthetemporalbonetoformthezygomaticarch.Inferiorlyand
mediallyitbroadlyarticulateswiththemaxillatoformtheinferiororbitalrimand
contributestotheorbitalflooraswellasthezygomaticomaxillarybuttresswhichforms
oneofthestrutsmentionedabove.5
1.1.2Maxilla
Themaxillaconsistsofacentralbodyandfourprocessesnamelythefrontal,zygomatic,
alveolarandpalatineprocess.Thebodyishollowedoutandcontainsthemaxillary
sinus.Itispyramidalshapedwiththebasebeingthemedialsurfacefacingthenasal
cavityandtheapexbeingelongatedintothezygomaticprocess.Ithasanorbitalor
superiorsurfacewhichformsthefloorandrimoftheorbit,amalaroranterolateral
surfacewhichformspartofthecheekandaposterolateralorinfratemporalsurface
whichcontributes
to
the
infratemporal
fossa.
The
base
is
rimmed
inferiorly
by
the
alveolarprocess.
Thealveolarprocesshousesthedentalarchwiththesocketsvaryinginsizeaccordingto
theteeth.Thepalatineprocessisahorizontalprocessfromthebodytothealveolar
processandmediallyarticulateswiththepalatineprocessoftheoppositemaxillawhilst
posteriorlyitarticulateswiththehorizontalplateofthepalatinebone.Thezygomatic
processisanextensionoftheanterolateralsurfaceofthebodywhichcontributestothe
zygomaticomaxillarysuture.5
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
15/67
15
Thefrontalprocessprojectsupwardtoarticulatewiththemaxillaryprocessofthe
frontalboneaswellasthenasalboneanteriorlyandthelacrimalboneposteriorly.Itis
thissegmentofbonethatincludesthelacrimalcrestintowhichthemedialcanthus
attachesthatMarkowitzcalledthecentralfragmentindefiningnasoorbitethmoid
(NOE)fractures.6
1.1.3Nasalbones
Thepairedquadrilateralbonesformtheupperpartofthebridgeofthenoseand
articulatewiththefrontalprocessofthemaxillalaterallyandwitheachotherinthe
midline.Superiorlytheyarticulatewiththefrontalbone.
1.1.4Lacrimalbones
Eachlacrimalboneisirregularlyrectangularformingpartofthemedialwalloftheorbit.
Theyarticulate
posteriorly
with
the
paper
thin
(lamina
papyracea)
part
of
the
ethmoid,
superiorlywiththefrontalboneandinferiorlywiththebodyofthemaxilla.Thesharp
orbitalverticallacrimalcrestcontinuesinferiorlytoformthelacrimalhamulus,withits
concaveportionhousingthelacrimalsac.Thelargeranteriorlimbofthemedialcanthus
attachestotheanteriorlacrimalcrestandadjacentfrontalprocessofmaxilla.5
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
16/67
16
1.2 Historyofmidfacialfracturesandtheirmanagement
TheearliestknownwritingsofmaxillofacialfractureswererecordedintheEdwinSmith
Papyrusin1650BCwhichwerepurchasedbySmithin1862andtranslatedby
Breasted.7,8Traditionally,healingandreligionwerecloselyintertwinedasillustratedin
theHellenicperiodatthetemplesofAsklepios,whereassistantstothepriestsprovided
medicalcare.Tooneoftheseassistantsasonwasbornin460BCnamedHippocrates.
Hippocrateswhoisoftenportrayedasthefatherofmedicinedescribedamyriadof
facialinjuriesinaround400BCandhisinsightprovidedthebasisforbandagesand
singlejawinterdentalwiringasmethodsoffixationandstabilisationoffacialfractures.9
Overthe
subsequent
centuries
following
Hippocrates
there
appeared
many
techniques
whichinessencewerevariationsofhismethods.InthenineteenthcenturyCharles
FredrickReiche8
providedthefirstdetailedtreatiseofmaxillaryfractures.Carlvan
Graefe8reportedontheuseofanelastictubeplacedintothenosetomaintainpatency
oftheairwayandalsodescribedtheuseofaheadframetotreatamaxillaryfracture.It
wasalsointhesamecenturythatGarretsonandBlair8advocatedmandibularmaxillary
fixationwiththeaidofsplintstoprimarilytreatmaxillaryfractures.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
17/67
17
In1901aFrenchsurgeon,RenLeFort,10
publishedhisclassicalpaperonmidfacial
fracturepatterns.Heinflictedbluntfacialtraumaon35cadaversthensubsequently
removedthesofttissueandexaminedfracturepatternsofthefacialskeleton.Thisstudy
haseversincebeenthebasisforthedescriptionofmaxillaryfractures.
FracturesofthezygomawerenotadequatelymentionedsincethetimeofHippocrates,
howeverin1906Lothrop11
wasthefirsttodescribetheuseofanantrostomyapproach
toreduceamediallyandinferiorlydisplacedzygoma.In1909Keen11
describedan
intraoralapproachtothezygomaticarch.In1927Gillies11
describedatechniqueto
reduceazygomaticarchaswellasmanipulateafracturedzygoma.
In1942Adam12
utiliseddirectwiringtoobtainbetterstabilityofzygomaticfractures.
Foryearshisprotocolappearedtobethemainstayoftreatmentatmanyinstitutions.In
the1970sosteosynthesisbecamearealityforfacialfractureswiththeSwiss
Arbeitsgemeinschaftfr
Osteosynthesefragen
(Association
for
the
Study
of
Internal
FixationorAO)developingminiplatefixation.Todaytheuseofminiplatesprovidesthe
principalmodalityoftreatmentforreductionandfixationofdisplacedmidfacial
fractures.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
18/67
18
1.3 Classification
Thereisnouniversalconsensusontheclassificationofmidfacefractures.Several
classificationshave
been
proposed
for
midface
fractures
due
to
amyriad
of
fracture
patternsobtainedwhichreflectthecomplexnatureofconstructionofthesebones.The
objectivesoftheseclassificationsweretohelpformulateclinicalguidelinesforpatient
management.
1.3.1Zygomaticfractures
TheearliestclassificationofzygomaticfractureswasproposedbySchjelderup13
who
classifiedzygomafracturesdependantonwhichregionitwasstillattachedtoe.g.Type
IIIfractureoccurredwhenthezygomawashingedatthefrontalbone.
In1961KnightandNorth13
classifiedzygomafracturepatternsintothefollowing6
typesaccording
to
the
level
of
displacement
noted
radiographically:
TypeI :undisplacedfracture TypeII :isolatedarchfractures TypeIII
:posteriorlydisplaced TypeIV :mediallyrotated TypeV
:laterallyrotatedatthebuttress TypeVI
:multipleorcomminutedfractureincludingthebody
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
19/67
19
In1968RoweandKilley13utilisedtheprincipleofverticalandhorizontalaxialrotations
andenblocdisplacementtoclassifyzygomaticfractures.Theyutilisedthe
frontozygomatictofirstmolarplaneastheverticalaxisandtheinfraorbitalforamento
zygomaticarchplaneasthehorizontalaxis.Theauthorsclassifiedthefracturepatterns
into8groupsandsuggestedwhichonesrequiredfixation.
LarsenandThomsen13
attemptedtoclassifyzygomaticfracturesaccordingtotheir
treatmentguidelines.TheysuggestedgroupAwhichincludednoorminimallydisplaced
fractures,groupBwhichencompassedfracturesthatrequiredreductionandfixation
(thisgroupincludedcomminutedanddisplacedfractures)andgroupCwhichincluded
allotherfracturesthatrequiredreductionbutnofixation.
Withtheadventofcomputertomographyandrigidfixationsomeauthorsclassified
zygomaticfracturesbasedontheamountofkineticenergyorseverityoftheblowtothe
bone.Amongst
these
were
Manson
and
Markowitz
14who
in
1990
classified
fractures
as
low,middleandhighenergyfracturesandwhoadvocatedwhichgrouphadaroleto
playinopenreductionandfixation.Lowenergyinjuriesarecharacterisedbynoor
minimaldisplacementincludingincompleteseparationwhichareeasilyreducedand
tendtostayinpositionwithnoorminimalstabilisation.Thesefracturesaccountfor18%
of
injuries.
Middle
energy
injuries
account
for
the
bulk
of
injuries
sustained
(77%)
with
displacementrangingfrommildtomarkedwithcompleteseparationatallfoursutures.
Theyrequirevariableamountofrigidfixationdependingonthedegreeofdisplacement.
Highenergyinjuriesareassociatedwithcomminution,significantdisplacementand
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
20/67
20
telescoping.Duetotheinherentinstabilityofthesefractureswideexposurefor
adequatereductionandrigidfixationisrequired.Onoccasiongraftingmayberequired
toaddressthebuttressesduetoextensivebonydefects.
1.3.2Maxillaryfractures
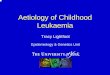
ThemostwidelyquotedclassificationofmaxillaryfracturesistheLeFortsystemof
classification.8,16HeclassifiedfracturepatternsintoLeFortI,IIandIII(Figure1.2).
TheLeFortIorlowlevelsupraapicalfractureextendshorizontallyfromthepiriform
rimlaterallyalongthealveolarprocessabovetheapicesoftheteethcontinuingbelow
thezygomaticbuttresstoinvolvethelowerthirdofthepterygoidplates.Thisresultsin
disarticulationoftheocclusalunitfromthemidface.
TheLeFortIIorpyramidalfractureextendsfromthenasalbonestoinvolvethemedial
andinfraorbitalrim,theanteriorwallofthemaxilla,thezygomaticbuttressand
pterygoidplates.Thisfractureresultsincentralmobilityofthemidfacefromthecranial
basewiththeconsequenceoflengtheningoftheface.
TheLeFortIIIorsuprazygomaticfractureextendsfromthefrontonasalregioninthe
midline,involvingthemedial,floorandlateralwallsoftheorbit,thefrontozygomatic
suture,maxillaandcontinuestotheupperthirdofthepterygoidplates.
Thisresultsin
disarticulationofthefacialbonesfromthecranialbase.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
21/67
21
Today,howeverfracturepatternsarerecognisedasfarmorecomplexthanthose
producedinLeFortslaboratory.Injuriescausedbypenetratingtraumaaswellashigh
velocityblunttraumaintroduceaspectrumoffracturesnotdescribedbyLeForts
classification.LeFortdidhoweverstatethatcomminutioncanoccurinconjunctionwith
theabovelistedfractures.Healludedtotheconceptofthesuperiorfractureasthelevel
ofclassificationandthatcomminutionoccursbelowitaccordingtothelinesof
weaknessinherentinthemidface.17
Todaytheintroductionofthemidpalatalsplitas
wellasexpansionoftheoriginalLeFortclassificationasproposedbyMarciani18
isoften
theclassificationquoted.
Figure1.2LeFortI,II&IIIfracturelinesfrontal&threequarterview.4
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
22/67
22
1.3.3Nasoorbitoethmoid(NOE)fractures
Thesefracturesareamongstthemostcomplexfracturesbothdiagnosticallyand
therapeuticallydue
to
the
intricate
anatomy
and
difficulty
in
fracture
fixation.
Gruss
19
statedthatduetothecomplexnatureofNOEfracturesnumerousclassificationswere
proposed.TheyclassifiedNOEfracturesintoisolatedorassociatedwithothermidfacial
fractures.Furthersubdivisionsweremadeintounilateralorbilateralfractures.
Theaboveclassificationshoweverfailedtoidentifythemedialcanthalattachmentand
itsrelationshiptothefracturepatterns.Aclassificationandtreatmentprotocol
proposedbyMarkowitzetal6hasbeenadoptedasthemostrelevantclassificationof
NOEfractures(Figures1.3,1.4and1.5).
Theydefinedtheareaofattachmentofthemedialcanthustotheboneasthecentral
fragmentwhichiscriticalforthediagnosisandtreatmentofNOEfractures.TypeI
fracturesproducesasinglesegmentfractureofthecentralfragment.TypeIIinjuryhasa
comminutedcentralfragmentwiththefracturesremainingexternaltothemedial
canthalinsertionandfinallytypeIIIhasacomminutedcentralfragmentwith
involvementofthecanthalinsertion.Theyalsodefinedthefracturesasunilateralor
bilateralaswellasisolatedorextendedintotheadjacentstructures.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
23/67
23
Figure1.3NOEtypeIfractureunilateralandbilateral.6
Figure1.4NOEtypeIIfractureunilateralandbilateral.6
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
24/67
24
Figure1.5NOEtypeIIIfractureunilateralandbilateral.6
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
25/67
25
1.4Signsandsymptoms
AllpatientswhosustainmidfacialfracturesareinitiallyattendedtointheAccidentand
Emergencyunitsattherelevanthospitalsandaremanagedaccordingtotheadvanced
traumaandlifesupport(ATLS)protocolasadvocatedbytheAmericanCollegeof
Surgeons.Oncethepatientisstabilisedthesecondarysurveyincludesadetailed
maxillofacialexamination.Thisexaminationwouldincludeinspectionandpalpationof
thefractures.Numerousfunctionalandaestheticdisordersaccompanymidfacial
fracturesandthefollowingaresomeofthepresentingsignsandsymptomsthatmay
occurinthedifferentfracturetypes.
1.4.1NOE
Uponinspectionanylacerations,abrasions,ecchymosis,facialoedemaandperiorbital
ecchymosismayindicateaNOEfracture.Ocularchangessuchastelecanthus,mongoloid
slantofthemedialcanthus,epicanthalfold,shorteningofthepalpebralfissure,
decreaseocularmobility,andenopthalmusarestronglysuggestiveofaNOEfracture.A
depressednasalbridge,epistaxis,binoculardiplopiaandepiphoraarefurthersignsofa
NOEfracture.6Clinicalevaluationinvolvingabowstring,Furnesstestandbimanual
palpationofthecentralfragmentaswellasanystepsinthatregioncanalsoalertthe
cliniciantothisfracture.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
26/67
26
1.4.2Maxilla
Extraoralevaluationmayrevealadishfaceappearance,elongatedface,depressed
nasalbridge,neurologicalfalloutinthedistributionoftheinfraorbitalnervesaswellas
stepdeformityatthebuttressand
infraorbitalrim.MobilityofthemaxillaattheLeFort
I,IIorIIIlevelcouldalsobenoted.Intraorallymalocclusion(inparticularananterior
openbite),mobilityofdentoalveolar(DA)segmentsortheentiremaxillacanbeelicited
aswellasstepsinthebuttressmaybepalpated.Otherintraoralsignsarestepsin
occlusion,malocclusion,diastemaformationaswellasecchymosisalongthebuttress
andthepalate.
1.4.3Zygoma
Periorbitaloedema
and
ecchymosis
is
acommon
sign
of
orbitozygomatic
complex
fractures.Othersignsincludesubconjunctivalhaemorrhagewithorwithoutlaterallimit
inallplanes,depressionofthemalareminence(lossofprojection)andneurological
falloutindistributionofinfraorbitalnerves.Dystopia,decreasedocularmovement,
binoculardiplopia,
enophthalmus,antimongoloidslantoflateralcanthusaswellas
palpablestepsaroundtheorbitalrimandbuttressarefurtherindicationofzygomatic
fractures.Limitedmouthopeningmaybepresentwhenthearchisfracturedimpeding
onthecoronoidprocessorasaresultofmuscleinjury.14
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
27/67
27
1.5LiteratureReview
Facialtraumaisoftenassociatedwithseveremorbiditywithrespecttolossoffunction
anddisfigurementaswellastheimpactofincreasedfinancialcoststoboththestate
andtheaffectedindividual.Ofthe1500facialfracturesanalysedbyRoweandKilley2
629(41.9%)involvedfracturesofthemiddlethird.KellyandHarrigan2analysed4317
facialfracturesofwhich594(13.76%)involvedthemiddlethirdofthefacialskeleton.
Ananalysisoftheassociationbetweentheepidemiologyandassociatedinjuriesisthus
importantinordertoimprovetreatmentandprevention.Beaumontetal20
undertooka
studyof389patientswithfacialfracturesinthreepopulationgroups.Theyfoundthat
themaletofemaleratiowasabout4:1.Inallethnicgroupsthepeakprevalenceof
fractureswasinthethirdandfourthdecades.Themeanageforblacks,asiansand
whiteswerenotedasbeing32,30and27yearsrespectively.Blacksweremainlyvictims
ofinterpersonalviolence,whilstinthewhitegroupmidfacialfractureswere
predominantlycausedbymotorvehicleaccidents.Inallthegroupsthemandiblewas
mostcommonlyfracturedfollowedbythemidfaceandthencombinedfracturesof
mandibleandmidface.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
28/67
28
TheaboveresultsweresimilartothefindingsbySnijman21
andDuvenage22
,published
in1963
and
1979
respectively,
whose
studies
were
conducted
in
the
Tshwane
district
of
theGautengprovince.Theyalsofoundthatathirddecadepeakwasnotedwithasimilar
malepredominance.Snijmanalsonotedthatassaultwasthemostcommoncauseof
facialfracturesamongstblacks.Hesimilarlynotedthatmotorvehiclesaccidents
accountedforahigherpercentageoffacialfracturesamongstthewhitegroup.
Mandibularfractureswerealsothemostcommonlyrecordedfacialfracturebyboth
authorsinagreementwithBeaumont.
Theseresultsareincontrasttothosepublishedinotherregions.Bataineh23
undertook
aretrospectivestudyoftheincidenceofmaxillofacialfracturesin
Jordanandnotedthat
ofthe563patientsthatpresentedfortreatmentovera5yearperiod,themandiblewas
mostfrequentlyfractured(74.4%)followedbythemaxilla,zygomaticarchandfinally
thedentoalveolarprocess.Themostcommoncausewasroadtrafficaccidents(55.2%)
followedbyaccidentalfalls(19.7%)andassault(16.9%).Amaletofemaleratioof3:1
wasnotedandthemeandecadeforinjurywasthethirddecade.Asimilar
epidemiologicalpatternwasnotedintheUnitedArabEmirates.24
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
29/67
29
Balakrishnan25
reviewed313casesinTrivandrum,Indiaintheearly1980sandfounda
markedmalepreponderance(93.3%).Thereasongivenwasthatwomenwerehardly
everinvolvedinroadtrafficaccidents.Theydonothoweversubstantiateorclarify
theirremarkwhethertherewerefewerwomenoccupantsanddrivers
inmotorvehicle
accidentsorwhetherwomenwerebetterdrivers.Onceagaintheinjurieswere
sustainedmostcommonlybyindividualsinthethirddecade.Heretrafficaccidents
followedbyassaultwerenotedtobethemostcommoncausesofmaxillofacial
fractures.InterestinglytwodecadeslaterinanotherdistrictinIndiathemaletofemale
ratiodecreasedto3.7:1.26
IntheNetherlandsvanBeek27
foundastrikingreductioninroadtrafficaccidentsand
anincreasinginfluenceofviolenceandsportresultinginachangingpatternof
maxillofacialfractures.TheseresultswereinstarkcontrasttoinjuriesinAustriaas
reportedbyGassner28
whofoundthatactivityofdailylifeandplayaccidentswasthe
maincausefollowedbysport,interpersonalviolenceandtrafficaccidents.Gassneralso
notedanincreaseinfemalepatientswithanoverallmaletofemaleratioof2.1:1.
Greene29
notedthatthedistributionofthemidfacefracturesinvolvingthe
zygomaticomaxillarycomplexwasthehighestfollowedbyorbitalblowout,nasal,
zygomatic
arch,
Le
Fort
and
finally
NOE
fractures.
The
distribution
in
Greece
was
somewhatdifferentwithzygomafracturespredominatingfollowedbyLeFortII,NOE,Le
FortIII,nasal,LeFortI,palatalsplitandfinallydentoalveolarfractures.30
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
30/67
30
AlKhateeb31
analysedcraniofacialfracturesinUnitedArabEmirates.Healsofound
thatamongmidfacialinjuriestheincidencewerehighestforzygomaticcomplex
fracturesfollowedbyNOE,isolatedorbitalfloorandLeFortfracturesrespectively.
Beaumont20
alsonotedthatthezygomaticomaxillarycomplexhadthehighest
distribution.
Ferreiraetal32
undertookastudytodeterminethedistributionofmidfacialfracturesin
childrenandadolescence.Theyfoundthatthedistributionsinprevalenceaccordingto
siteswere:zygoma,alveolar,Lefort,orbitalfloorandfinallyhardpalate.
Kontio33
interestinglyfoundinhisepidemiologicalstudyinFinlandthatthespectrumof
maxillofacialinjurieschangedsomewhat.Thedecademostaffectedwithfracturesin
1981wasthefourthwhilstin1997itwasthefifthdecade.Healsonotedadecreasein
motorvehicleincidentswithanincreaseininterpersonalviolencewhichhadbecome
moresevere
in
nature.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
31/67
31
1.6AimsandObjectives
Althoughtherearenumerousstudiesofmaxillofacialinjuriesintheliterature,onlya
fewhavecontainedmeaningfulinformationrelatingtolocaldemographicfactors.In
ordertoimproveservicedeliveryinthetreatmentofmidfacialfracturesitisparamount
toanalysecurrentdataonitsbiomechanicsandincidence.Thisstudyintendsto:
1.
Providecurrentlocaldataontheaetiology,biomechanicsanddemographicsofpatientspresentingfortreatmentoffracturesofthemidface.
2.
Toassesstheassociation,ifany,betweenfracturepatternsandmechanismofinjury,thusprovidinginsightintolocalbehaviouralpatterns.
3.
Tosupplydataofthefinancialresourcesprovidedbythedepartmentofhealthrequired
to
meet
patient
needs.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
32/67
32
Chapter2Materialsandmethods2.1Ethicalclearance
AnapplicationforethicsclearancewassoughtwiththeCommitteeforResearchon
HumanSubjects(Medical)oftheUniversityoftheWitwatersrand.TheClearance
certificate,protocolnumberM050812wasgranted(AppendixA).Verbalandwritten
explanationsofthestudyweregiventopatientswhofulfilledtheinclusioncriteriaof
thestudyandawrittenconsentwasobtainedfromeverysubject.(AppendixB)
2.2InclusionCriteria
PatientswhopresentedtotheMaxillofacialandOralSurgeryDepartmentofthe
UniversityofWitwatersrandwithmidfacialfracturesandwhogaveconsentwere
admittedtothestudy.Midfacialfracturesweredefinedasfracturesinanareaboundby
thefrontozygomatic
and
frontonasal
sutures
superiorly,
the
occlusal
plane
inferiorly,
posteriorlytothepterygoidplatesandlaterallytilltherootofthezygomaticarchas
describedbyFrost1.
2.3ExclusionCriteria
Anypatient
who
did
not
present
with
midfacial
fractures,
declined
to
give
consent
or
withdrewfromthestudy.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
33/67
33
2.4ClinicalStudy
ThiswasaprospectiveauditundertakenintheDivisionofMaxillofacialandOral
Surgery,Department
of
Surgery,
University
of
the
Witwatersrand
at
the
Chris
Hani
BaragwanathHospitalandtheJohannesburgAcademicHospitalunits.
Atotalof94patientsrecordswerecollectedbymaxillofacialregistrarsatbothunits
overa12monthperiodfrom(December2005toDecember2006).Allpatientswere
consultedonanoutpatientbasisoradmittedtotheabovehospitals.
Thedatarecorded(AppendixC)reflectedadetailedclinicalexaminationwhichincluded
ademographicprofile,medicalhistory,pastsurgicalhistory,aetiologyofthefracture
andassociatedinjuries.Ageneralevaluationfollowedbyamorespecificmaxillofacial
examinationwasundertaken.Themaxillofacialexaminationincludedsofttissue,
skeletalandaneurologicalexamination.Anintraoralexaminationfollowedwhich
assessedocclusion,dentition,alveolus,oralmucosa,palate,tongueandfloorofthe
mouth.
Specialinvestigationsinparticularradiographicexaminationswereundertakento
complimentclinicalexaminationandarriveatafinaldiagnosis.Theradiographs
routinelyutilizedincludedOccipitomental(OM)viewstakenat0o,15o,30
o,
Submentovertex(SMV),Orthopantomograph(OPG),andComputertomography(CT)
scans.Figures2.1to2.3illustratesomeexamplesoftheseradiographs.Interpretations
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
34/67
34
oftheOccipitomentalviewsweredonefollowingtheprinciplesof
McGrigorand
Campbell.34
Figure2.1Occipitomentalviewindicatingmultiplefacialfractures.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
35/67
35
Figure2.2SMVusedtoassessfracturesofthezygomaticarch.
Figure2.3ThreedimensionalCTscanindicatingmultiplefacialfractures.
Thetreatmentofferedwasnotedincludinganyplatingsystemandotheralloplastic
materialsusedforopenreductionandinternalfixation(ORIF)sothatacostingofthe
hardwarecouldbeobtained.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
36/67
36
2.5DataAnalysis
DatawasanalysedwithSASforWindows(Version9.1,SASInstituteInc.USA)
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
37/67
37
Chapter3ResultsRecordswereobtainedfromatotalof94patientswhosustainedmidfacialfractures.
3.1Age,genderandracedistribution
Thepatientsagesrangedfromthreeto67yearsold.Theagesweredefinedperdecade
foreaseofuseandforcomparativestudiesaslistedinTable3.1below.Gender
distributionrevealedamalepredominanceinaratioof4:1(Table3.2).
Table3.1Frequencydistributionbyageindecades(N=94)
Decade Agerange Numberofpatients
(N)
Percentage(%)
1
09
1
1.1
2 1019 2 2.1
3 2029 37 39.4
4 3039 25 26.6
5 4049 20 21.3
6
5059
6
6.3
7 6069 3 3.2
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
38/67
38
Table3.2Frequencydistributionbygender(N=94)
Gender N %
Male 78 82.98
Female 16 17.02
Blackpatientsaccountedforthelargestracialgroup(77.66%)followedbywhites,
colouredsandasiansrespectively(Table3.3).
Table3.3
Frequency
distribution
by
race
(N=94)
Race N %
Black 73 77.66
Coloured 6 6.38
Asian 3 3.19
White 12 12.77
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
39/67
39
3.2 Natureofinjuryandsocialhabits
ThedistributionofthecausesofthefracturesisshowninTable3.4.Themostcommon
causeof
midfacial
fractures
was
blunt
trauma
due
to
interpersonal
violence
(40.5%),
followedbymotorvehicleaccidents(26.6%),gunshotwounds(13.8%)andfalls(5.3%).
13.8%ofpatientscouldnotrecollecthowtheywereinjuredasindicatedintable3.4.Of
thosepersonsinjuredwithaweapononly2werestabwoundswiththeremaining18
injuredwithbricksorrod/pipe.
Table3.4Frequencydistributionbynatureofinjury(N=94)
Mechanismofinjury N %
Injurywithweapon(otherthan
firearm)
20 21.3
Fist/s 18 19.2
Gunshotwound/s 13 13.8
Fall 5 5.3
Motorvehicleaccident 25 26.6
Unknown
13
13.8
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
40/67
40
Ifoneconsidersallocatingthenatureofinjuryashighvelocity(gunshotandmotor
vehicleaccidents)andlowvelocityinjuries(theremainingcausesofmidfacialfractures)
thenthepercentagesare46.91%and53.09%respectively.Thisexcludesthe13patients
whocouldnotprovideinformationaboutthemechanismofinjury.
Socialhabitsinvolvingalcoholconsumptionwasalsonotedin58.51%ofthepatients
(Table3.5).Approximatelytwothirdsofpatientshadreportedsomedegreeoflossof
consciousnessasillustratedinTable3.6.
Table3.5Frequencydistributionbyalcoholconsumption(N=94)
Alcoholconsumption N %
No 39 41.49
Yes
55
58.51
Table3.6Frequencydistributionbylossofconsciousness(N=94)
Lossofconsciousness N %
No 31 32.98
Yes 63 67.02
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
41/67
41
Thecharacteristicsoftheinjuriessustainedindicatedthesiteofimpactasroughlyequal
interms
of
left
and
midline
(26.6
%
right,
30.9%
left,
31.9
%
midline
and
10.6%
unknown).Themostcommonlyassociatedinjurysustainedwithmidfacialfractureswas
afracturedmandible(32.9%)followedbychesttrauma(5.3%)asindicatedinTable3.7.
Sundayappearedtobethedayonwhichmostoftheinjuriesoccurredasillustratedin
Table3.8.
Table3.7Frequencydistributionbyassociatedinjuries(N=94)
Associatedinjury N %
None 49 52.2
Mandible 31 32.9
Chest 5 5.3
other 9 9.6
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
42/67
42
Table3.8Frequencydistributionbydayoftheweek(N=94)
Day N %
Monday*
8
8.5
Tuesday 7 7.4
Wednesday 8 8.5
Thursday 13 13.9
Friday 16 17
Saturday 15 16
Sunday 24 25.5
Unknown 3 3.2
*TwopatientswereinjuredonaMondaywhichcoincidedwithapublicholiday.
3.3SpecialInvestigations
Fromthisstudy(asshowninTable3.9)themostprevalentradiographicinvestigations
formidfacialfracturesweretheOM&SMVviews(61.7%).ThesewerefollowedbyCT
scans,
OPG
and
other
views.
It
should
also
be
noted
that
certain
radiographs
were
also
takenincombinationinclinicallyindicatedsituations.(e.g.takingofanOPGwithOM
viewsfordentoalveolarfracturewithzygomaticbonefracture).
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
43/67
43
Table3.9Frequencydistributionbyradiographicinvestigations(N=94)
Radiology N %
Occipitomental&SMV 58 61.7
CTscans 32 34
OPG 3 3.2
Other 1 1.1
3.4Typeoffracturessustained
Thefracturessustainedvariedconsiderablyfromisolatedorbitalfloorblowoutfracture
ornasalbonefracturetomultiplefracturesinvolvingacombinationofmidfacialbones.
Inordertoavoidgreaterthan5%ofcellsinacontingencybeingemptyacombinationof
fracturetypesweremade.ThefracturesweregroupedintoLeForttypefractures(I,II
orIII),dentoalveolar(DA)fractures,zygomaticomaxillarycomplex(ZMC)fractures,
panfacialfractures(involvingmultiplebones)andother(suchasNOEandBlowout
fractures).ThesearelistedinTable3.10below.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
44/67
44
Table3.10Frequencydistributionbyfracturepattern(N=94)
Typeoffracture N %
Dentoalveolar 16 17.02
Lefort (I,II,III) 13 13.83
Panfacial 16 17.02
Zygomaticcomplex 43 45.74
Other 6 6.38
3.5Analyses
Inordertogaininsightintobehaviouralpatterns,analysisofthecircumstancesofthe
injurywasdone.Ananalysisofalcoholconsumptiontothemechanismofinjurywas
alsodonetodetermineifanystatisticalsignificancecouldbeelicited.Othercriteria
werealsoassessedasreflectedinTable3.11toTable3.16below.Itwasalsorecorded
thattheaverageperiodfromthetimeofinjurytomanagementwas13.9dayswitha
rangeof1to151dayspriortotreatment.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
45/67
45
Table3.11Analysisofalcoholconsumptionbymechanismofinjury(N=81)
Alcoholconsumption Mechanismofinjury Total
HighVelocity
Low
Velocity
No(N) 27 11 38
% 33.33 13.58 46.91
Yes(N) 11 32 43
% 13.58 39.51 53.09
Total(N)
38
43
81
% 46.91 53.09 100.00
TheChisquaretestindicatedaPvalue
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
46/67
46
Table3.13Analysisofgenderbymechanismofinjury(N=81)
Gender Mechanismofinjury Total
HighVelocity LowVelocity
Female(N) 11 4 15
% 13.58 4.94 18.52
Male(N) 27 39 66
% 33.33 48.15 81.48
Total(N) 38 43 81
%
46.91
53.09
100.00
TheChisquareindicatesaPvalueof.0231
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
47/67
47
Table3.14Analysisofdecadebygenderandalcoholconsumption(N=93).
Decade Alcoholconsumption Total Gender Total
No Yes Female Male
1&2(N) 1 2 3 2 1 3
% 1.08 2.15 3.23 2.15 1.08 3.3
3(N) 17 20 37 6 31 37
% 18.28 21.51 39.78 6.45 33.33 39.78
4(N)
10
15
25
2
23
25
% 10.75 16.13 26.88 2.15 24.73 26.88
5(N) 9 11 20 4 16 20
% 9.68 11.83 21.51 4.3 17.20 21.51
6(N) 1 7 8 2 6 8
%
1.08
7.53
8.60
2.15
6.45
8.6
Total(N) 38 55 93 16 77 93
% 40.86 59.14 100 17.20 82.8 100
ChisquareindicatesaPvalueof0.5123
ChisquareindicatesaPvalueof0.1299
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
48/67
48
Table3.15Analysisoffracturetypebyalcoholconsumptionandmechanismofinjury.
Fracture Alcohol
consumption
Total Mechanismofinjury Total
No Yes Highvelocity LowVelocity
DA(N) 11 5 16 11 3 14
% 11.7 5.32 17.02 13.58 3.7 17.28
LeFort(N) 5 8 13 5 5 10
% 5.32 8.51 13.83 6.17 6.17 12.35
Other(N) 3 3 6 1 4 5
% 3.19 13.83 17.02 1.23 4.94 6.17
Panfacial(N) 3 13 16 7 8 15
% 3.19 13.83 17.02 8.64 9.88 18.52
Zygoma(N) 17 26 43 14 23 37
% 18.09 27.66 45.74 17.28 28.40 45.68
Total(N) 39 55 94 38 43 81
% 41.49 58.51 100.00 46.91 53.09 100.00
ChisquareindicatesaPvalueof0.0719
ChisquareindicatesaPvalueof0.0796
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
49/67
49
Table3.16Analysisoffracturetypebytreatment.
Fracture C ED N O X Total(N)
DA(N) 9 6 1 0 0 16
% 9.57 6.38 1.06 0.00 0.00 17.02
LeFort(N) 2 1 1 8 1 13
% 2.13 1.06 1.06 8.51 1.06 13.83
Other(N) 1 1 1 0 3 6
% 1.06 1.06 1.06 0.00 3.19 6.38
Panfacial(N) 0 0 0 16 0 16
% 0.00 0.00 0.00 17.02 0.00 17.02
Zygoma(N) 5 0 8 30 0 43
% 5.32 0.00 8.51 31.91 0.00 45.74
Total(N) 12 8 11 54 9 94
% 18.08 8.51 11.70 57.45 4.25 100.00
ChisquareindicatesaPvalueof
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
50/67
50
3.6Hardwarecosts
Atotalofthreecompaniesprovidedtheplatingsystemsforinternalfixation.The
averageprice
for
ascrew
from
these
companies
was
R
182.45
and
the
average
price
for
aminiplatewasR509.63.
Anaverageoftwominiplateswitheight1.5mmor1.3mm(dependingonwhich
companysystemwasused)screwswasusedforplatingafracturedzygoma.The
averagecostperpatientforanORIFofafracturedzygomawasR2479.12(2x509.63+8x182.45).Forpanfacialfracturesanaverageof6miniplatesand32screwswereutilizedperpatient.ThusacostofR7438.69(6x509.63+24x182.54)perpatientforORIFofpanfacialfractureswasnoted.LeFortfracturesonaveragerequired4mini
platesand16screws,resultinginacostofR4959.16(4x509.63+16x182.54)perpatientforORIFLeFortfracture.
CollatingtheabovedatawiththatofTable3.16forthenumberofORIFforeachofthe
fracturetypes,atotalofR287090.28wasobtainedastheaveragecostofhardware
utilizedinthisreport.ThisequatestoUS$35886.29perannumforthisstudy(rateof
R8.00=US$1).
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
51/67
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
52/67
52
injuriesovera27yearperiod.Falls(5.3%)weretheleastcontributorstomidfacial
fracturesinthisstudy.Onceagainsimilarepidemiologicdatawerenotedinprevious
SouthAfricanstudies.21,22,35
Fromthisstudyitwasnotedthatthemaletofemaleratiois4:1.Thismarkedmale
predominanceissimilartothoseepidemiologicalstudiesconductedinIrbid,Jordan23
andNjimegen,Netherlands.27
Thisalsocomparefavourablywithpreviousstudies
conductedinSouthAfrica.20,21,22,35
Thesefindingsarehoweverincontrasttothose
foundinInnsbruck,Austria27
andinChennai,India26
wheretheauthorsreportahigher
femaleincidencebutstillamalepredominance.
77.6%ofpatientswhosoughttreatmentinourhospitalswereblack,followedbywhites,
colouredsandasiansindescendingorderoffrequency.Possibleexplanationsforthis
trendincludethefactthatblacksconstitutethehighestpopulationinSouthAfrica.36
Secondlythe
highest
unemployment
rate
in
our
county
is
amongst
blacks.36
These
indigentpatientswithoutanyformofmedicalinsurancewouldthereforetendtoseek
treatmentinpublicinstitutionslikeours.Thesmallerpopulationgroups,withfewer
ratesofunemployment,tendtoseekmedicaltreatmentintheprivatesector.Previous
studiesinourcountrycorroboratethistrend.20,21,22,35
Ifoneconsiderstheagerangeitwasnotedthat67.0%ofindividualsthatsustained
midfacialinjurieswerereportedtobeinthethirdandfourthdecadewiththehighest
incidencenotedinthethirddecade(39.4%).Desai35
describedthisgroupas
representingtheunskilledlabourforcethatareusuallypaidweeklyandtraditionally
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
53/67
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
54/67
54
Ifoneanalysesthedataastatisticallysignificant(ChisquaretestindicatedaPvalue
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
55/67
55
Intermsoftreatment,the16patientswithpanfacialfractures,30(31.9%)ZMCand8
(8.5%)LeFortfracturesweretreatedwithopenreductionandinternalfixationwhich
allowedforimprovedrigidityoftheseunstablefractures.Inthisstudy5(11.63%)of
ZMCfracturesweretreatedbyclosedreduction.8(8.5%)patientswithundisplaced
zygomafracturesweretreatedconservatively(i.e.observationonly)asisadvocatedin
theliterature.13
TheChisquareresultsreflectedinTable3.16indicatesaPvalueof
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
56/67
56
(2)Patientoverload:Thehighprevalenceofinterpersonalviolenceinourcountryoften
resultsintraumaoverload.Combinedwithabroaderlackofresourcessuchasalackof
theatretimeitinevitablyresultsinlongerwaitingperiods.
Bythetimethesepatientsgettotheatreinappropriatehealing(intheformoffibrous
union,malunionandsepsishastakenplace)thusoftennecessitatingosteotomisingthe
fractureswithsubsequentprolongationoftheatretimeandincreasingcosts.Also
treatmentoftheolderfracturesoftenyieldssuboptimalclinicaloutcomes.
Fromthisstudyitisnotedthatonaveragethehardwarecostsforapatientwitha
ZMCfractureequatestoR2479.12whilstthatofapanfacialwasR7438.69.
InterestinglythecostsprovidedbyDuvenage22
in1979reportedatotalhospitalcost
formaxillofacialinjuries(inclusiveofanaesthetic,wardandhardwarecosts)ofR295.75
forORIFingeneral.
Desai35
in2006reportedatotalcostforhardwareonlyforORIFoffractured
mandibletothestateperannumofR158305.Thisstudyrevealsthetotalhardware
costformidfacialfracturestobeR287090.28perannum.Thesecostsdonotinclude
ward,anaestheticandtheatrefees.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
57/67
57
Chapter5ConclusionThisstudyhasshownthatthemajorityofpatientspresentingwithmidfacialfractures
werethose
of
lower
socio
economic
status
(i.e.
blacks).
The
majority
of
these
patients
wereinjuredoverweekendsandwereinebriatedatthetimeofinjury.Blunttraumadue
tointerpersonalviolencewasthemostcommoncauseoffacialfractures.Thezygomatic
complexfracturewasthemostcommonlyobservedmidfacefracture.Thisstudy
suggeststhatarelationshipexistsbetweenfacialtrauma,povertyandalcohol
consumption.It
is
also
noted
that
facial
trauma
(mainly
due
to
interpersonal
violence
in
ourcountry)placesenormousfinancialburdenonthestate.
Futurestudiesshouldseektounderstandtheepidemiologicalfactorsinfluencingfacial
traumainanefforttoimprovepreventionandmanagementoftheseinjuries.
Inadditionitisclearthattrendsareobservedwhenanalysingthedatacollated,
howeverthelimitednumbersofpatientsdonotreflectstatisticalsignificance.Again,
furtherresearchisrequiredtoencompassalargersamplesizewithadequatefollowup
ofclinicaloutcomesastoobtainmoremeaningfuldatawithothercriteriasuchas
complicationrates,sepsisratesandtotalhospitalisationcostsbeingincorporated.This
wouldenhanceabetterunderstandingofinfluencingpatternsonfacialtraumawitha
viewtoprovidinganeffectiveresponsetothisepidemic.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
58/67
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
59/67
59
8.
CunninghamLL,HaugRH.Managementofmaxillaryfractures.In:MiloroM.,GhaliGE,LarsonP,WaiteP,editors.PetersonsPrinciplesofOraland
MaxillofacialSurgery.BCDeckerInc.Canada.2004:chapter23.1:434438.
9. Mukerji R, Mukerji
M,McGurkM.Mandibularfractures:historicalperspective.BrJOralMaxillofacSurg2006;44:222228.
10.BagheriSC,
HolmgrenE,KademaniD,HommerL,BryanBellR,PotterB,etal.ComparisonoftheseverityofbilateralLeFortinjuriesinisolatedmidface
trauma.JOralMaxillofacSurg2005;63:11231129.
11.GilliesHD,KilnerTP,StoneD.Fracturesofthemalarzygomaticcompound:withadescriptionofanewxrayposition.BrJSurg1927;14:651656.
12.MansonP.Transcutaneousreductionandexternalfixationforthetreatmentofnoncomminutedzygomafractures.
J OralMaxillofacSurg1998;56,13871389.
13.EllisEIII.Fracturesofthezygomaticcomplexandarch.In:FonsecaRJ,WalkerRV,
editors.
Oral
and
Maxillofacial
Trauma.
W
B
Saunders
Company.
Philadelphia.1991:chapter18:440460.
14.BaileyJS,GoldwasserMS.Managementofzygomaticcomplexfractures.In:MiloroM.,GhaliGE,LarsonP,WaiteP,editors.PetersonsPrinciplesofOraland
MaxillofacialSurgery.BCDeckerInc.Canada.2004:chapter23.2:445455.
15.Zingg
M,
Laedrach
K,
Chen
J,
et
al.
Classification
and
treatment
of
zygomatic
fractures:areviewof1025cases.JOralMaxillofacSurg1992;50:778.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
60/67
60
16.LewD,SinnD.Diagnosisandtreatmentofmidfacefractures.In:FonsecaRJ,WalkerRV,editors.OralandMaxillofacialTrauma.WBSaundersCompany.
Philadelphia.1991:chapter19:515544.
17.MansonP.SomethoughtsontheclassificationandtreatmentofLeFortfractures.AnnPlastSurg1986;17:356363.
18.MarcianiRD.Managementofmidfacefractures:Fiftyyearslater.JOralMaxillofacSurg1993;51:960968.
19.GrussJS.Complexnasoethmoidorbitalandmidfacialfractures:roleofcraniofacialsurgicaltechniquesandimmediatebonegrafting.AnnPlastSurg
1986;17:377390.
20.BeaumontER.
FracturesofthefacialskeletoninthreeethnicgroupsinthegreaterJohannesburg.UniversityoftheWitwatersrand.Johannesburg.1981:24
47.
21.SnijmanPC.Fracturesofthebantufacialskeleton.JournalofDentAssocofSAfr1963;18:570575.
22.Duvenage.EpidemiologyofmaxillofacialandoraltraumainSouthAfrica.JournalofDentAssocofSAfr1979;33:691693.
23.BatainehA.EtiologyandincidenceofmaxillofacialfracturesinnorthofJordan.Oral
Surg
Oral
Med
Oral
Pathol
Oral
Radio
Endod
1988;
86:31
35.
24.KlenkGandKovacsA.EtiologyandpatternsoffacialfracturesintheUnitedArabEmirates.JCraniofacSurg2003;14:7884.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
61/67
61
25.BalakrishnanNandPaulG.IncidenceandaetiologyoffractureofthefaciomaxillaryskeletoninTrivanadrum:aretrospectivestudy.BrJOralMaxillofac
Surg1986;24:4043.
26.SubhashrajK,NandakumarN,RavindranC.ReviewofmaxillofacialinjuriesinChennai,India:Astudyof2748cases.BrJOralMaxillofacSurg2007;45:637639.
27.VanBeek.MerckxCA.Changesinthepatternoffracturesofthemaxillofacialskeleton.IntJOralMaxillofacSurg1999;28:424428.
28.GassnerR,TuliT,HachlO,RudischAandUlmerH.Craniomaxillofacialtrauma:a10yearreviewof9543caseswith21067injuries.JCranioMaxillofacialSurg
2003;31:5161.
29.GreeneD,RavenR,CarvalhoGandMaasCS.Epidemiologyoffacialinjuryinbluntassault.ArchOtolaryngolHeadNeckSurg1997;123:923928.
30.ZachariadesN.Papavassiliou.ThePatternandaetiologyofmaxillofacialinjuriesin
Greece.
JCranio
Maxillofacial
Surg
1990;
18:251
254.
31.AlKhateebT,AbdullahFM.CraniomaxillofacialinjuriesintheUnitedArabEmirates:aretrospectivestudy.JOralMaxillofacSurg2007;65:10941101.
32.FerreiraP,MarisaM,PhinoC,RodriguesJ,ReisJ,ArmanteJ.Midfacialfracturesinchildrenandadolescents:areviewof492cases.BrJOralMaxillofacSurg
2004;
42:501
505.
33.KontioR,SuuronenR,PonkkonenH,LindqvistC.,LaineP.Havethecausesofmaxillofacialfractureschangedoverthelast16yearsinFinland?An
epidemiologicalstudyof725fractures.DentalTraumatology2005;21:1419.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
62/67
62
34.WhaitesE.Essentialsofdentalradiographyandradiology.ChurchillLivingstone.Edinburgh2002:402406.
35.DesaiJ.MandibularfracturepatternsasrelatedtomechanismofinjuryaprospectiveauditofJohannesburgpatients.UniversityoftheWitwatersrand.
Johannesburg.2006:24.
36.LehohlaP.Censusinbrief.StatisticsSouthAfrica.1998.http://www.statsa.gov.za/censu01/Census98/HTML/default.htm(accessed25th
March2008).
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
63/67
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
64/67
64
AppendixBPARTICIPANT INFORMATIONSHEETANDCONSENT.Dearpatient
MynameisDr.YusufFSulemanandIamaregistrarintheDivisionofMaxillofacial&Oral
Surgery.Aspartofmytraining,Iamconductingastudyaboutmidfacialfractures(brokenbones
ofthefacefromtheeyebrow,nose,thebonesaroundthecheekandupperjawincludingupper
teethbutnotincludingthelowerjaw).
Asyourinjuriesareconsistentwiththosedescribedabove,Irequireyourhelpbyallowingmeto
useyourclinicalrecords;thesewouldincludeaphysicalexaminationofyourselfaswellas
analysisofyourxraysforthepurposesofthisstudy.Itishopedthatthisstudywillhelpour
departmentbetterunderstandthisinjury,andimproveonourservicetoallofourpatients.
Your
participation
in
this
study
is
purely
voluntary
if
you
so
wish
at
any
time
and
that
whether
youparticipateornotwillnotaffecttheoutcomeofyourtreatmentandsuchyoumaychoosewhetheryouwouldliketoparticipateinthisstudyornot.Ifyouopttoparticipateafew
questionswillbeaskedaboutthecircumstancessurroundinghowyougotinjuredaswellasan
examinationoftheextentofyourinjuries.Acopyoftheinformationsheetisattachedforyour
perusal.
Pleasenotethatitisyourrighttowithdrawfromthisstudyifyouwishatanytimeandthat
whetheryouparticipateornotwillnotaffecttheoutcomeofyourtreatment.
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
65/67
65
Youwillnoticethatthedatainformationsheetdoesnotreflectyournameandassuchyouwill
remainanonymousandallinformationgatheredisstrictlyconfidentialandwillbeusedforresearchpurposesonly.
Ifyouhaveanyquestionsrelatingtothisstudyorfeelthatyoumayrequiremoreinformation
aboutthestudy,youmaycontactmeon0119338107(ChrisHaniBaragwanathHospital,Ward
H4).
THEDOCTORHASEXPLAINEDHISINTENTIONSTOMEANDIAGREETOPARTICIPATEINTHIS
STUDY.IDOSOFREELYANDUNDERSTANDTHATIMAYWITHDRAWATANYTIME,WITHOUT
COMPROMISINGANYTREATMENTDUETOME.
PATIENTSIGNATURE DATE..
OR
PARENT/LEGALGUARDIAN..
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
66/67
66
AppendixCMIDFACE FRACTURE PATTERNS PATICIPANT INFORMATION DATA
SHEET.
DateofBirth: Gender: M/F
Race: DateofInjury:DateofConsultation: DateofAdmission:
Intoxicatedatthetime:
Lossofconsciousness: Y/N Hospitalno.:
Airway : patent/compromised/obstructed
Neurologicalstatus:GCSscore /15 /10
Relevantmedicalhistory:
Relevantsurgicalhistory:
Mechanismof
injury
(Tickappropriate)
Motor vehicle accident Assault
Occupant Fist
Pedestrian Foot
Motorcyclist Pipe
Cyclist Brick
Bottle
Firearm
Sport Industrial
IncludingBat/Stick
Other
Fall Miscellaneous
BluntTrauma highvelocity:(mva/other)
lowvelocity:(fists/fall)
PenetratingTrauma highvelocity:(bullet/blastshrapnel/other)
lowvelocity:(knife/other)
stateentranceandexitwound(ifapplicable)
Site
of
impact
:
left/right/midline
Softtissue : lacerations/abrasions/avulsive
Associated/Otherinjuries :
SpecialInvestigations:
-
7/28/2019 Research Report Final- Aetiology & Mechanism of
Midfacial Fractures
67/67