Embed Size (px)
Citation preview
HSEHealth & Safety
Executive
Genetic variation in susceptibility to chronic effects of organophosphate
exposure
Prepared by the University of Manchester and Manchester Royal Infirmary
for the Health and Safety Executive 2005
RESEARCH REPORT 408
HSEHealth & Safety
Executive
Genetic variation in susceptibility to chronic effects of organophosphate
exposure
NM Cherry*, PN Durrington+, B Mackness+
MI Mackness+, AE Smith*, M Dippnall* & AC Povey*
*Centre for Occupational and Environmental Health Division of Epidemiology and Health Sciences
University of Manchester Oxford Road
Manchester M13 9PL
+University Department of Medicine Manchester Royal Infirmary
Oxford Road Manchester M13 9WL
A case-referent study was carried out to investigate whether the ability to metabolise and detoxify organophosphates differed between sheep dippers with self-reported chronic ill-health (cases) and healthy dippers (referents) of similar age and with a similar dipping history. Cases and referents were interviewed by a study nurse and information on their current health and occupational history obtained. A blood sample was also taken, DNA extracted and polymorphisms in genes associated with organophosphate metabolism determined.
This report and the work it describes were funded by the Health and Safety Executive (HSE). Its contents, including any opinions and/or conclusions expressed, are those of the authors alone and do not necessarily reflect HSE policy.
HSE BOOKS

© Crown copyright 2005
First published 2005
All rights reserved. No part of this publication may bereproduced, stored in a retrieval system, or transmitted inany form or by any means (electronic, mechanical,photocopying, recording or otherwise) without the priorwritten permission of the copyright owner.
Applications for reproduction should be made in writing to: Licensing Division, Her Majesty's Stationery Office, St Clements House, 2-16 Colegate, Norwich NR3 1BQ or by e-mail to [email protected]
ii
ACKNOWLEDGEMENTS
The study was funded by the UK Health and Safety Executive (3837/R79.002). The authors would like to thank Stuart Thomson, Janet Schofield, Elizabeth Smallshaw, and Caroline Fitzgerald for interviewing participants, Priscilla Appelbe for coordinating the field work and Stephanie Middleton for expert technical assistance
iii

iv
CONTENTS
SECTION Page
List of Tables vi List of Figures vii List of Appendices viiiExecutive Summary ix
1.0 INTRODUCTION 1 1.1 AIMS AND OBJECTIVES OF THE CURRENT STUDY 2
2.0 MATERIALS AND METHODS 4 2.1 STUDY DESIGN 4 2.2 FIELD METHODS 4 2.3 ANALYSIS OF PON1 PHENOTYPE AND GENOTYPE 5 2.4 ANALYSIS OF GST AND CYP GENOTYPES 5 2.5 CLASSIFICATION OF EXPOSURE TO SHEEP DIPS 5 2.6 ANALYSIS 7 2.7 SAMPLE SIZE 8
3.0 RESULTS 9 3.1 FULL ANALYSIS 9
3.1.1 Study population 9 3.1.2 PON1 genotyping 10 3.1.3 PON1 phenotyping 11 3.1.4 GST and CYP genotyping 12
3.2 Staged analysis 16 3.2.1 Study population 16 3.2.2 PON1 Genotyping 20 3.2.3 GST and CYP genotyping 22
4.0 DISCUSSION 25
REFERENCES 27
v
LIST OF TABLES
No Title Page 1. Comparison of cases and referents 9 2. Distribution of the PON 1 polymorphisms in the cases and referents 10 3. Odds ratios for case status for polymorphisms at positions 192 and 10 55 of PON14. Hydrolysis of PON1 substrates in cases and referents 11 5. Hydrolysis of PON1 substrates in cases and referents divided by 13
PON1-192 genotype 6. Hydrolysis of PON1 substrates in cases and referents divided by 13
PON1-55 genotype 7. PON1 activity towards diazoxon and paraoxon according to 14
PON1-55 and PON1-192 genotype 8. Distribution of GSTM1, GSTT1 and GSTP1 genotypes in cases 15
and referents 9. Distribution of CYP2D6, CYP3A4 and CYP3A5 genotypes in 15 cases and referents10. Symptoms for which the proportion of cases above the median 19
symptom score was twice that of referents 11. Associations between PON1-192 genotype and case status 21 12. Associations between PON1-55 genotype and case status 21 13. Associations between GSTM1 genotype and case status 22 14. Associations between GSTT1 genotype and case status 22 15. Associations between combined GSTM1 and GSTT1 genotype 23
and case status 16. Associations between GSTP1 genotype and case status 23 17. Associations between CYP2D6 genotype and case status 23 18. Associations between CYP3A4 genotype and case status 24 19. Associations between CYP3A5 genotype and case status 24
vi
LIST OF FIGURES
No Title Page 1. Odds ratio of being a case according to quintile of diazoxon 11
hydrolysis 2. Histogram of responses to question “Now thinking overall about 16
your health during the past month, how much have you been troubled by ill-health” 3. Histogram of responses to question “How much do you feel your 17
health now has been affected by using sheep dip” 4. Proportion of cases and referents with symptom scores greater 18
than the median symptom score
vii
LIST OF APPENDICES No Title Page
1 Advertisement used to publicise study 312 Initial letter to subjects who wrote in following the publicity 32 3 Information sheet 33 4 Initial questionnaire to enquirers 35 5 Follow up letter to cases 36 6 Initial letter to potential referents 37 7 Consent form 38 8 Work and lifestyle questionnaire 39 9 Health questionnaire 48 10 Code for symptom questionnaires 58 11 Nurse questionnaire 61 12 Sheep dipping history questionnaire 74 13 Letter to GP of participant 85 14 GP questionnaire 86 15 Primary exposure variables 87 16 Pesticide Codes 88 17 Subject group 1 89 18 Subject group 2 90 19 Discriminant Analysis excluding subject group 1 91 20 Discriminant Analysis excluding subject groups 1 and 2 92 21 Frequencies of self-reported ill-health in cases and referents 93 22 First published paper (Lancet 2002; 359: 763-64.) 9623 Second published paper (Pharmacogenetics 2003;13:81-88) 100
viii
EXECUTIVE SUMMARY
A substantial number of sheep farmers complain of chronic ill health which they attribute to repeated exposure to organophosphates (OPs). Symptoms appear to occur only in a small proportion of dippers whose characteristics are poorly understood but individuals with specific defects in the metabolic pathway for organophosphates, however, would be expected to be at greater risk of damage following exposure. OPs are hydrolysed by human serum paraoxonase (PON1) thus limiting toxicity. The PON1 coding region has two polymorphisms involving the amino acids at position 55 (leucine [L] → methionine [M]) and 192 (glutamine [Q]→ arginine [R]), giving rise to isoenzymes which differ in their catalytic rate for the hydrolysis of OPs. Other enzyme systems have also been reported to be involved in the activation (e.g. CYP) and detoxification (GST) of OPs and may also determine sensitivity to OP exposure. The principal objective of the study was to determine whether sheep farmers with self-reported disabling chronic symptoms contain a greater proportion of individuals with dysfunctional polymorphisms at positions 192 and 55 of human serum paraoxonase than sheep farmers without these symptoms.
A case-referent study was carried out in which cases (n=175) were sheep dippers with self-reported chronic ill-health which they attributed to sheep dip. Cases nominated sheep dippers of similar age (not blood relatives) who they believed to be of good health and who had had a similar dipping history (n=234). Cases and referents were very similar except that cases had spent less total time dipping than referents (19.4 vs 22.0 years p<0.001). A similar proportion of cases and referents had used diazinon based sheep dips. Cases were more likely than referents to have at least 1 R allele (OR=1.93: 95% CI 1.24-3.01) at position 192, both alleles of type LL (OR=1.70: 95% CI 1.07-2.68) at position 55 and to have diazoxonase activity below the median (OR=1.77: 95% CI 1.18-2.67). There were no differences in the frequency of GSTM1*1 and *2 and GSTT1*1 and *2 polymorphisms in cases and referents: 9% of cases but only 5.8 % of referents were double null homozygotes (odds ratio 1.61, 95%CI 0.74-3.48). There was evidence of a small increased risk associated with having a GSTP1*B or *C allele (OR 1.33, 95% CI 0.87-2.01) and with the CYP2D6 WT genotype (OR 1.47; 95% CI 0.83-2.60). There was no risk associated with the CYP3A4 or CYP3A5 genotypes.
Certain subjects were then excluded on clinical grounds or after discriminant analysis in a staged analysis. Risk associated with the PON1 192 and 55 genotypes altered little with these changes in the population. There was no risk associated with the GSTM1*2 (null) or GSTT1*2 (null) genotype after exclusion of subject groups. Cases however were more likely to be both GSTM1*2 (null) and GSTT1*2 (null) than referents with 12.0% of cases being double null negative but only 5.7% of referents: the odds ratio (95%CI) was 2.26 (0.89-5.75). There was no risk associated with GSTP1, CYP2D6, CYP3A4 or CYP3A5 genotype after exclusion of subject groups. These findings are consistent with the hypothesis that organophosphates contribute to the self-reported ill health of sheep dippers.
ix

x
1.0 INTRODUCTION
Health problems associated with acute OP toxicity are well defined but, ill-health induced by chronic exposures to OPs is poorly defined and remains controversial1. A substantial number of sheep farmers complain of chronic ill health which they attribute to repeated exposure to organophosphates (OPs). Those complaining of ill-health that they attribute to repeated OP exposure report a wide range of symptoms, often severe, which can include headache, limb pains, fatiguability, sleep disturbance, poor concentration , mood changes and suicidal thoughts2. A recent study reported an association between psychiatric disorders (particularly depression) and musculoskeletal disorders (particularly myalgia) and short-term and long-term exposure to Ops3. However, there are no widely accepted diagnostic criteria for chronic ill health associated with OP exposure. Careful epidemiological investigation of current workers shows, at most, slight changes in cognitive function following repeated exposure4. Although acute poisoning might result in significant neuropsychological abnormalities5, the symptoms (neurobehavioural and cognitive complaints, affective disturbances, chronic fatigue and neurological complaints) 2 reported by sheep farmers do not correspond closely to the type of subclinical effect that has been documented following frank poisoning or repeated exposure1. Moreover, symptoms appear to occur only in a small proportion of dippers whose characteristics are poorly understood. If organophosphates were associated with chronic ill health then individuals with specific defects in the metabolic pathway for organophosphates might be expected to be at greater risk of ill-health following exposure. Full investigation of the relation of exposure to ill health would require knowledge of the type, intensity and duration of exposure.
man
The hydrolysis of OP pesticides by serum paraoxonase (aryldialkylphosphatase, E.C.3.1.8.1) is a major factor determining their toxicity to vertebrates including
6-10. Human serum paraoxonase (PON1) located on high-density lipoprotein has an amino acid polymorphism at position-19211,12 which results in two alloenzymes (R form with arginine at 192 and Q with glutamine ), which differ in their hydrolytic activity towards paraoxon. Paraoxon is hydrolysed at a higher rate by the R than the Q alloenzyme 6,8,11,12. These alloenzymes have similar hydrolytic activity towards certain other substrates, such as phenylacetate. The historical view that the R alloenzyme of PON1 was the most protective because of its higher activity towards paraoxon has been challenged by findings showing the Q alloenzyme hydrolysed diazoxon and the nerve gases sarin and soman faster than the R form in vitro13. Whether all organophosphate pesticides are metabolised in a similar fashion to diazoxon is at present unclear but potentially the effects of these polymorphisms will be exposure dependent.
A second PON1 polymorphism at position 55 involving a leucine (L)- methionine (M) substitution was not previously believed to affect PON1 activity11-14. However, a study of the 192 and 55 polymorphisms in 279 healthy people, indicated that
1
both have an independent effect on serum PON1 activity, but not concentration15. MM homozygotes have the lowest PON1 activity regardless of their 192 genotype. The effects of L/M polymorphism on the hydrolysis of organophosphate pesticides are largely unknown but it may also make an important contribution to genetic susceptibility to OP poisoning. These results suggest that genotyping for both polymorphisms may be necessary for identifying those individuals at most risk of OP poisoning 15,16.
PON1 also hydrolyses a wide range of other substrates including lactones, thiolactones, cyclic carbonate esters and phosphatidylcholine oxidation products 17,18. PON1 provides protection against the oxidation of low-density lipoprotein (LDL) presumably via the hydrolysis of oxidised LDL phospholipids 8,18 and is thus believed to provide protection against cardiovascular diseases such as atherosclerosis. Low serum PON1 activity has been associated with increased risk of atherosclerosis but the genetic association studies between PON1 polymorphisms and disease risk are less consistent possibly because PON1 polymorphisms may alter risk in specific subgroups19. Low serum PON1 activity has also been associated with Persian Gulf War Veterans self-reporting Gulf War syndrome20 and the PON1 Q alloenzyme associated with neurologic symptom complexes in Gulf War Veterans21.
Other enzyme systems are involved in the activation and detoxification of OPs22
and may also determine sensitivity to OP exposure23. Cytochrome p450 mediated reactions can result in the activation of diazinon into diazoxon (and other metabolites) and the detoxification of diazoxon and chlorfenvinphos. CYP3A4 has recently been implicated as the principal enzyme that metabolises diazinon in the human liver, though CYP 2D6 also appears to have some activity24,25. Both enzymes show large inter-individual variation in activity26,27. Variation in CYP2D6 activity is largely genetically determined and polymorphisms in the CYP2D6 gene have been associated with, for example, Parkinson’s disease28. Variation in CYP3A4 activity may also be genetically determined as polymorphisms in the CYP3A4 gene have been reported29 but it is unclear whether these polymorphisms have any functional significance30,31. Glutathione S-transferases have also been reported to play a role in the metabolism of organophosphates32 but whether this occurs in vivo has been doubted33. GSTM1, GSTT1, and GSTP1 are also polymorphic genes and interindividual variation in the expression or functional activity of these enzymes may be important in determining susceptibility to human disease34. Deletions in both the GSTM1 and GSTT1 genes result in the total absence of enzyme activity whereas polymorphisms in the GSTP1 gene have been reported to affect the activity of the enzyme for at least some substrates 34.35. Susceptibility to OP poisoning may thus potentially result from the balance between activation and detoxification systems and this balance may be different for different exposures 36.
1.1 AIMS AND OBJECTIVES OF THE CURRENT STUDY
The overall aim was to examine whether differences in the ability to metabolise and detoxify organophosphates were associated with self-reported chronic ill
2

health amongst sheep dippers. The specific objectives were to determine whether there were any differences between sheep farmers with self-reported chronic ill-health and healthy sheep farmers in 1. the proportion of individuals with dysfunctional polymorphisms at positions 192
and 55 of the PON1 gene 2. the ability to metabolise diazoxon, paraoxon and phenylacetate 3. the prevalence of other possible susceptibility CYP and GST genotypes An additional objective was to examine whether 4. The strength of these associations differs with the OP product habitually used
3
2.0 MATERIALS AND METHODS
2.1 STUDY DESIGN The design was that of a case-referent study, in which the odds ratio for dysfunctional polymorphisms were computed. Cases were sheep dippers who believed that their chronic ill health was a result of exposure to sheep dip . Referents were nominated by the cases: referents were then reported to have had a similar pattern of sheep dipping, were in good general health and of similar age (±10 years), lived in the same locality and were not blood relatives of the case who nominated them.
2.2 FIELD METHODS Following radio and newspaper advertisements (Appendix 1), people who reported themselves ill as a result of exposure to sheep dip were identified. Each eligible subject (case) then received a letter describing the study in greater detail (Appendix 2), an information sheet (Appendix 3) and a brief questionnaire (Appendix 4) asking them to provide details of their ill-health, when they were last involved in dipping and whether they could identify three people from the same age group who were not blood relatives, did not suffer from ill-health and who carried out a similar regime of sheep dipping (Appendix 4). These potential referents were then contacted by telephone to confirm their eligibility.
Cases and referents were then further contacted by letter (Appendices 5 and 6) and telephone, if necessary, to arrange an interview time. They also received a consent form (Appendix 7) and a work and lifestyle questionnaire (Appendix 8). Subjects were asked in detail (using a detailed symptom questionnaire based upon that used for the Gulf War study 37 carried out in Manchester; Appendix 9), about their health during the previous month, indicating on an adjacent visual analogue scale ranging from “not at all” to “very seriously”, how much they had been troubled by each of the 95 symptoms (Appendix 9). The abbreviated code for each symptom on the questionnaire is shown in Appendix 10. The participants were asked to complete these questionnaires prior to the arrival of the research nurse. At the interview, the research nurse verified that the questionnaires were completed and obtained further detailed information on lifestyle factors, lifetime medical history and any recent symptoms (Appendix 11). Additionally, a separate, detailed, nine page questionnaire was completed for every job in which the subject had ever been involved in sheep dipping including both OP and non-OP dips (Appendix 12). This questionnaire covered various activities and particulars of interest, aimed at quantifying the nature and extent of potential exposure to sheep dip pesticides and was based on a questionnaire developed at the Institute of Occupational Medicine38.
Information was also collected on other potential occupational exposures to pesticides from activities such as fumigations, veterinary treatments of other farm animals, other crop protection measures, other occupations involving use
4
of pesticides (Appendix 12) and other potential confounding exposures such as lead and other heavy metals, vibration, and solvents (Appendix 11).
Consent to approach the general practitioner was sought from each respondent (Appendix 7). If given, general practitioners were approached by mail (Appendix 13), with telephone follow-up, and asked to confirm the diagnosis reported for any neurological or psychological illness (Appendix 14).
At the end of the interview a venous blood sample was taken for subsequent analysis: samples were split into two and one was sent by post directly for PON1 genotyping and phenotyping whilst the other was immediately frozen and stored frozen until subsequent analysis of CYP and GST genotyping.
2.3 ANALYSIS OF PON1 PHENOTYPE AND GENOTYPE Serum and EDTA-plasma were separated by low-speed centrifugation. Serum and lymphocytes from the EDTA-plasma were stored at -20°C for no more than 3 months prior to analysis. The lithium-heparin plasma was used immediately for liver function tests. PON1 activity assays and liver function tests could not be performed in 12 cases and 18 controls due to gross haemolysis of the samples.
Asparate transaminase, alanine transaminase, alkaline phosphatase, bilirubin and γ-glutamyltransferase were measured using a Hitachi 727 analyser in the Department of Biochemistry, Manchester Royal Infirmary, UK so as to determine that there was no adverse effect of abnormal hepatic function on PON1 secretion which in man is entirely from the liver.
Serum PON1 activity towards paraoxon, phenyl-acetate and diazoxon were analysed spectrophotometrically as described previously13,15,39. PON1 concentration was determined by ELISA with rabbit antihuman PON1 monospecific antisera40. DNA was extracted from lymphocytes and the PON1-55 and PON1-192 genotypes determined by PCR amplification and restriction enzyme digestion as described 12.
2.4 ANALYSIS OF GST AND CYP GENOTYPES. Genotyping for polymorphisms in the CYP2D6, CYP3A4, GSTM1 and GSTT1genes was carried out using PCR based procedures 29,31,41-43.
2.5 CLASSIFICATION OF EXPOSURE TO SHEEP DIPS Sheep dipping activities were classified in two stages; an initial assessment of the most important descriptives, together with a subsequent and a more detailed analysis of related occupational exposures and other confounders. For each study participant , a series of 54 primary variables (Appendix 15) was extracted from the questionnaires. These variables were then coded for every year covered by the period 1970 to present, decades that covered the period of active organophosphate sheep dip use.
5
Every pesticide reported to have been used, by each farmer, for each of the 30 years was also classified. All 1500 reported 'pesticides' were decoded, as far as was reasonably practicable, into their trade names. Each of these proper names was given a unique code number, and there were some 580 codes at the end of this work. Every farmer therefore had a list of pesticides code numbers reported for each year. The code numbers were banded into easilyidentifiable categories (Appendix 16) to enable quick reclassification as and when more information regarding the pesticide comes to light. Furthermore, we delineated between responses where the farmer was certain of his answer, and where the information was "possible" or "probable".
Farmers were found to commonly use several types of sheep dip in any given year. Typically, they used different chemicals for control of scab and fly pests, generally at two or more dipping sessions throughout a year. To account for the multiple sheep dip use , exposures to different classes of chemicals were ranked and for each of the 30 years, the farmers' pesticide usage was scored on a hierarchical basis (Rank A>B>C>D>E>F) as to whether the farmer reported : probable use of diazinon (rank A), possible use of diazinon (rankB), probable use of non-diazinon OP (rank C), possible use of other non-diazinon OP (rank D), use of only non-OP's (rank E) and use of unknown pesticide/product (rank F). For example, if a farmer had used both Diazinon (an OP) and Chlorfenvinphos (an OP), in a given year, then that year would be classified as being a year where he used Diazinon. Similarly, if the farmer had used Chlorfenvinphos and Flumethrin (a non-OP), then that year would be classified as a year where he had used an OP. The exception to this was if a year was categorised as being a non-OP year, then for that year, all otherpesticides used in that year must have been positively identified as being non-OP. If the farmer had used a non-OP and an 'unknown', then that year would be graded as being an unknown pesticide year, as the unknown pesticide could possibly have been OP in nature.
For each year with the same pesticide year rank, the following summarymeasures were calculated: Total years dipping: a count of the number of years the farmer had been
involved in sheep dipping, using this pesticide type. Number of dipping days per year: a count of the number of days in any given
year where the farmer had been involved in sheep dipping . Frequency of concentrate handling: the multiple of number of days the
farmer had dipped sheep in that year, by an estimate of how many times per day the farmer had handled the sheep dip concentrate ( e.g. to replenish the dip bath). Gross numbers of sheep dipped: the multiple of 'number of dipping days per
year' by an estimate of the number of sheep or lambs the farmer normally dipped per day that year. Number of years as a Paddler / Plunger / Dipper: this variable was used to
estimate the number of years the farmer had been employed in the activity, where exposure to splashes from the dip bath, was likely to have been highest.
6
Additionally, the first and last years dipped using that type of sheep dip, were coded. This method enabled the groups of chemicals to be analysed either independently or grouped together.
2.6 ANALYSIS Univariate comparison of cases and referents was carried out using either parametric or non-parametric techniques depending upon whether the variable had a gaussian distribution or not. The chi squared test was used to determine the significance of differences in allele frequency. ANOVA was used to test for differences in parameters between genotypes. Independent effects of the PON1-55 and PON1-192 polymorphisms on diazoxon hydrolysis were sought by multiple regression analysis. Cases and controls were analysed separately. Risk associated with specific genotypes was examined using odds ratios (and 95% confidence intervals) unadjusted and after adjustment for age, sex, region and date of first dipping.
Health questionnaire responses on each 10cm visual analogue scale were allocated as a symptom score to 1-20 equally spaced segments. Subjects who provided usable answers to at least 90 of the 95 symptoms were included in the main analysis. The subject’s mean response to all other symptoms was assigned where five or less symptoms had been missed 37.
Mean severity scores were skewed and transformation of the raw data did not result in a normal or quasi normal distribution. As such the median score of each symptom was calculated and the proportion of cases and referents above the median determined.
The initial analyses previously published included all cases and referents recruited for the study44,45. Additional analyses were then carried out after the exclusion of subjects with more than 5 missing symptoms and those who, on increasingly strict assumptions, may have contributed no information to the comparison of cases and referents. Subjects were excluded on the basis of clinical grounds (see below) or a result of discriminant analysis.
Excluded subjects then consisted of the following 4 groups: Group 1 comprised cases and referents with a chronic condition attributed by their general practitioner to a clearly defined event (e.g. trauma, stroke), causal agent (e.g. paralytic poliovirus) or congenital condition (e.g. cerebral palsy (Appendix 17). Subjects were identified by a clinician blind to the status of the subject using answers provided on the GP questionnaire (Appendix 14).
Group 2 comprised cases and referents with established neurological disease (e.g. multiple sclerosis, Parkinson's disease, Guillain-Barré syndrome, Alzheimer's disease) for which there are objective diagnostic criteria but uncertain aetiology (Appendix 18). Subjects were identified by a clinician blind to the status of the subject using answers provided on the GP questionnaire (Appendix 14).
7

Group 3 comprised subjects identified by discriminant analysis (Appendix 19) excluding Group 1 as being atypical of their classification (cases/referents).
Group 4 comprised subjects identified by discriminant analysis (Appendix 20) excluding Groups 1 and 2 as being atypical of their classification (cases/referents).
The associations between case status and PON1-192, PON1-55 , GSTM1, GSTT1, GSTP1, CYP2D6, CYP3A4 and CYP3A5 polymorphisms were initially calculated for the whole population (“full analysis”) and then also for subpopulations defined by excluding groups defined as above in a series of analyses as follows : Stage 1 analysis: all subjects excluding those with more than 5 unusable responses to the symptom question 37
Stage 2 analysis: all subjects except subject group 1 Stage 3 analysis: all subjects except subject groups 1 and 2 Stage 4 analysis: all subjects except subject groups 1 and 3 Stage 5 analysis: all subjects except subject groups 1, 2 and 4
2.7 SAMPLE SIZE Previous work had indicated that polymorphisms for Q and R at position 192 are distributed 74%:26% in a UK population15. To detect an odds ratio of 1.6 for the R polymorphism with α = 0.05 and β = 0.20 a sample size of 120 cases with 2 referents would be needed. In order to allow for ineligibility among referents, the number chosen for each case was increased to 3.
8

3.0 RESULTS
3.1 FULL ANALYSIS 3.1.1 Study population A total of 197 individuals, who believed they were unwell as a result of sheep dipping, contacted the study team as a result of the initial publicity . Of these, the first 9 were used to pilot the questionnaire and procedures; these subjects are not included in this report. Of the remaining 188, 175 were interviewed, 4 refused or could not be contacted, 6 had not dipped sheep and 3 died before the interview. Of the cases, 102 identified one or more controls who were eligible (had dipped sheep, were not blood relatives, were within 10 years of age of the subject, and lived in the same part of the country). Those unable to identify controls said that this was because they were no longer in farming, were too unwell to see other people or did not know any sheep farmer who was unaffected by the dip. There were 309 controls nominated. Of these 234 were included in the analysis, 11 were ineligible because they had not dipped sheep, 39 did not match any case (because of age, location or relatedness) and were not approached and 25 were approached, but refused. Blood samples for PON1 activity analysis were obtained from 163 cases and 216 controls.
156 (89%) cases and 210 (90%) referents were men (Table 1). The majority of cases and referents, 112 (64%) and 155 (66%) respectively, lived in England and there was no difference in their geographical distribution. The mean age of first dipping was 21·7 (SD 10·0) and 19·9 years (8·1), respectively. Cases were born around 2 years before referents, but the time they had spent dipping (19·4±7.5 years) was significantly less (p=0.0004) than that of referents (22·0±7·2 years). Only 25% (43) of cases but 51% (120) of referents had dipped sheep since 1997. Two-thirds of all participants reported that they had, at some time, used dips containing diazinon (115 (66%) cases, 152 (65%) referents). 88 (22%) participants had not used diazinon but had used some organophosphate, and 54 (13%) could not give sufficient detail for classification.
Table 1 Comparison of cases and referents Variable
Gender % male Scotland/NI
Wales N/NW England E/SE England
Region (%)
SW England Age at interview Mean ± SD Year first dipped Mean ± SD
Total years dipping Mean ± SD
Overall (n=409)
Cases (n=175)
Referents (n=234) p
89.5 89.1 89.7 0.48 12.7 13.7 12.0 22.0 22.3 21.8 13.2 15.4 11.5 23.7 26.3 21.8 28.4 22.3 32.9
0.18
52.7±11.0 53.9±10.4 51.8±11.5 0.05 1967.6±12.3 1967.4±12.3 1967.8±12.6 0.77
20.9±7.5 19.4±7.5 22.0±7.2 <0.001
9
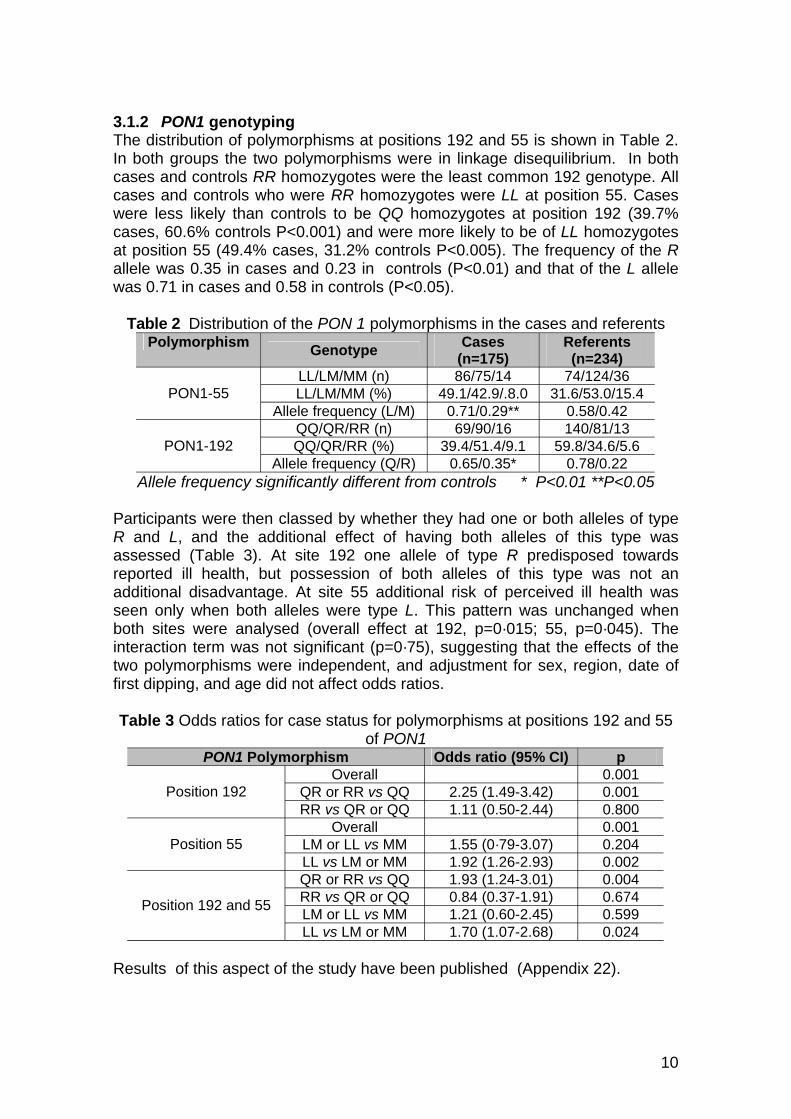
3.1.2 PON1 genotyping The distribution of polymorphisms at positions 192 and 55 is shown in Table 2. In both groups the two polymorphisms were in linkage disequilibrium. In both cases and controls RR homozygotes were the least common 192 genotype. All cases and controls who were RR homozygotes were LL at position 55. Cases were less likely than controls to be QQ homozygotes at position 192 (39.7% cases, 60.6% controls P<0.001) and were more likely to be of LL homozygotes at position 55 (49.4% cases, 31.2% controls P<0.005). The frequency of the R allele was 0.35 in cases and 0.23 in controls (P<0.01) and that of the L allele was 0.71 in cases and 0.58 in controls (P<0.05).
Table 2 Distribution of the PON 1 polymorphisms in the cases and referents Polymorphism
PON1-55
PON1-192
Genotype
LL/LM/MM (n) LL/LM/MM (%)
Allele frequency (L/M) QQ/QR/RR (n) QQ/QR/RR (%)
Allele frequency (Q/R)
Cases (n=175) 86/75/14
49.1/42.9/.8.0 0.71/0.29** 69/90/16
39.4/51.4/9.1 0.65/0.35*
Referents (n=234)
74/124/36 31.6/53.0/15.4
0.58/0.42 140/81/13
59.8/34.6/5.6 0.78/0.22
Allele frequency significantly different from controls * P<0.01 **P<0.05
Participants were then classed by whether they had one or both alleles of type R and L, and the additional effect of having both alleles of this type was assessed (Table 3). At site 192 one allele of type R predisposed towards reported ill health, but possession of both alleles of this type was not an additional disadvantage. At site 55 additional risk of perceived ill health was seen only when both alleles were type L. This pattern was unchanged when both sites were analysed (overall effect at 192, p=0·015; 55, p=0·045). The interaction term was not significant (p=0·75), suggesting that the effects of the two polymorphisms were independent, and adjustment for sex, region, date of first dipping, and age did not affect odds ratios.
Table 3 Odds ratios for case status for polymorphisms at positions 192 and 55 of PON1
PON1 Polymorphism Overall
QR or RR vs QQPosition 192 RR vs QR or QQ
Overall LM or LL vs MMPosition 55 LL vs LM or MM QR or RR vs QQ RR vs QR or QQ LM or LL vs MMPosition 192 and 55
LL vs LM or MM
Odds ratio (95% CI)
2.25 (1.49-3.42) 1.11 (0.50-2.44)
1.55 (0·79-3.07) 1.92 (1.26-2.93) 1.93 (1.24-3.01) 0.84 (0.37-1.91) 1.21 (0.60-2.45) 1.70 (1.07-2.68)
p 0.001 0.001 0.800 0.001 0.204 0.002 0.004 0.674 0.599 0.024
Results of this aspect of the study have been published (Appendix 22).
10
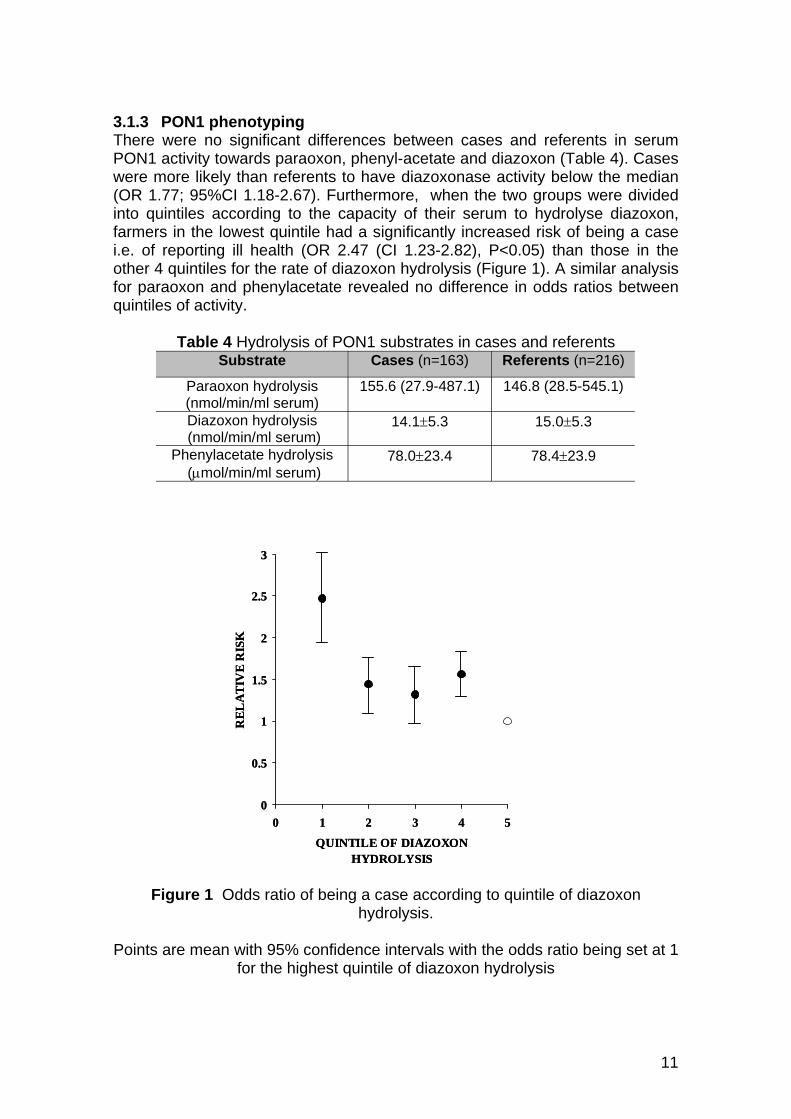
3.1.3 PON1 phenotyping There were no significant differences between cases and referents in serum PON1 activity towards paraoxon, phenyl-acetate and diazoxon (Table 4). Cases were more likely than referents to have diazoxonase activity below the median (OR 1.77; 95%CI 1.18-2.67). Furthermore, when the two groups were divided into quintiles according to the capacity of their serum to hydrolyse diazoxon, farmers in the lowest quintile had a significantly increased risk of being a case i.e. of reporting ill health (OR 2.47 (CI 1.23-2.82), P<0.05) than those in the other 4 quintiles for the rate of diazoxon hydrolysis (Figure 1). A similar analysis for paraoxon and phenylacetate revealed no difference in odds ratios between quintiles of activity.
Table 4 Hydrolysis of PON1 substrates in cases and referents Substrate Cases (n=163) Referents (n=216)
Paraoxon hydrolysis (nmol/min/ml serum)
155.6 (27.9-487.1) 146.8 (28.5-545.1)
Diazoxon hydrolysis (nmol/min/ml serum)
14.1±5.3 15.0±5.3
Phenylacetate hydrolysis (µmol/min/ml serum)
78.0±23.4 78.4±23.9
REL
ATI
VE
RIS
KR
ELA
TIV
E R
ISK
33
2.52.5
22
1.51.5
11
0.50.5
000 1 2 3 4 50 1 2 3 4 5
QUINTILE OF DIAZOXONQUINTILE OF DIAZOXONHYDROLYSISHYDROLYSIS
Figure 1 Odds ratio of being a case according to quintile of diazoxon hydrolysis.
Points are mean with 95% confidence intervals with the odds ratio being set at 1 for the highest quintile of diazoxon hydrolysis
11
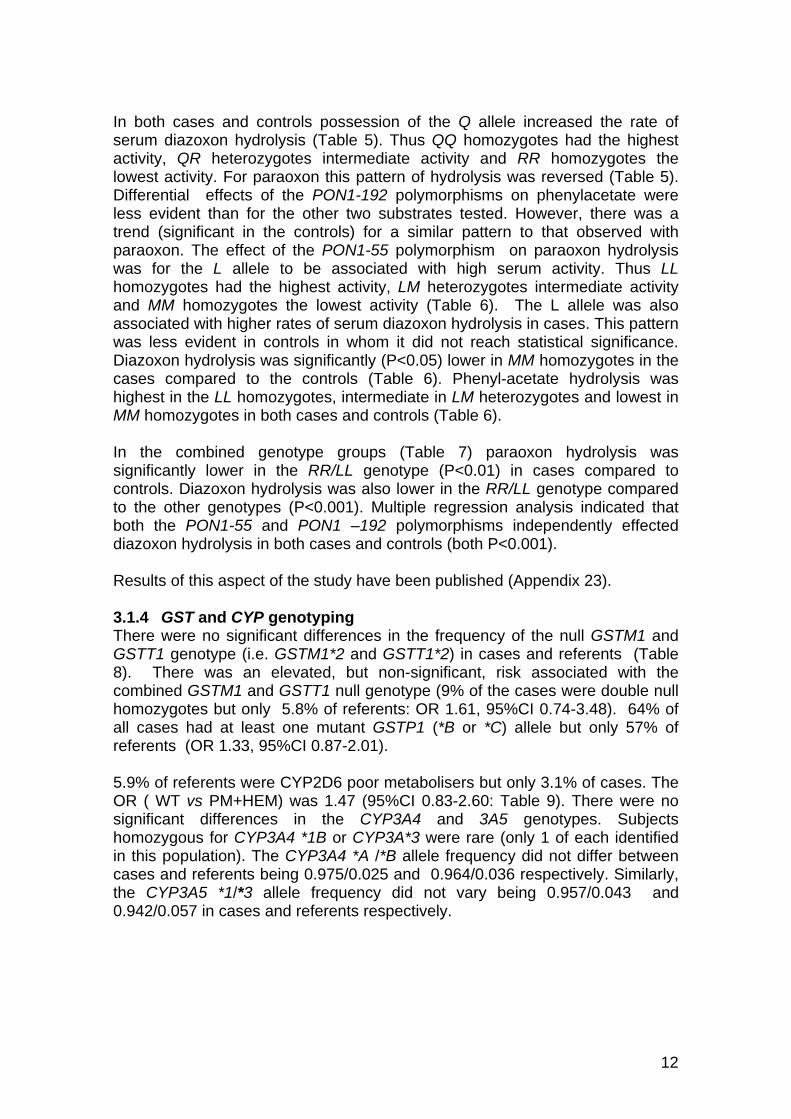
In both cases and controls possession of the Q allele increased the rate of serum diazoxon hydrolysis (Table 5). Thus QQ homozygotes had the highest activity, QR heterozygotes intermediate activity and RR homozygotes the lowest activity. For paraoxon this pattern of hydrolysis was reversed (Table 5). Differential effects of the PON1-192 polymorphisms on phenylacetate were less evident than for the other two substrates tested. However, there was a trend (significant in the controls) for a similar pattern to that observed with paraoxon. The effect of the PON1-55 polymorphism on paraoxon hydrolysis was for the L allele to be associated with high serum activity. Thus LL homozygotes had the highest activity, LM heterozygotes intermediate activity and MM homozygotes the lowest activity (Table 6). The L allele was also associated with higher rates of serum diazoxon hydrolysis in cases. This pattern was less evident in controls in whom it did not reach statistical significance. Diazoxon hydrolysis was significantly (P<0.05) lower in MM homozygotes in the cases compared to the controls (Table 6). Phenyl-acetate hydrolysis was highest in the LL homozygotes, intermediate in LM heterozygotes and lowest in MM homozygotes in both cases and controls (Table 6).
In the combined genotype groups (Table 7) paraoxon hydrolysis was significantly lower in the RR/LL genotype (P<0.01) in cases compared to controls. Diazoxon hydrolysis was also lower in the RR/LL genotype compared to the other genotypes (P<0.001). Multiple regression analysis indicated that both the PON1-55 and PON1 –192 polymorphisms independently effected diazoxon hydrolysis in both cases and controls (both P<0.001).
Results of this aspect of the study have been published (Appendix 23).
3.1.4 GST and CYP genotyping There were no significant differences in the frequency of the null GSTM1 and GSTT1 genotype (i.e. GSTM1*2 and GSTT1*2) in cases and referents (Table 8). There was an elevated, but non-significant, risk associated with the combined GSTM1 and GSTT1 null genotype (9% of the cases were double null homozygotes but only 5.8% of referents: OR 1.61, 95%CI 0.74-3.48). 64% of all cases had at least one mutant GSTP1 (*B or *C) allele but only 57% of referents (OR 1.33, 95%CI 0.87-2.01).
5.9% of referents were CYP2D6 poor metabolisers but only 3.1% of cases. The OR ( WT vs PM+HEM) was 1.47 (95%CI 0.83-2.60: Table 9). There were no significant differences in the CYP3A4 and 3A5 genotypes. Subjects homozygous for CYP3A4 *1B or CYP3A*3 were rare (only 1 of each identified in this population). The CYP3A4 *A /*B allele frequency did not differ between cases and referents being 0.975/0.025 and 0.964/0.036 respectively. Similarly, the CYP3A5 *1/*3 allele frequency did not vary being 0.957/0.043 and 0.942/0.057 in cases and referents respectively.
12
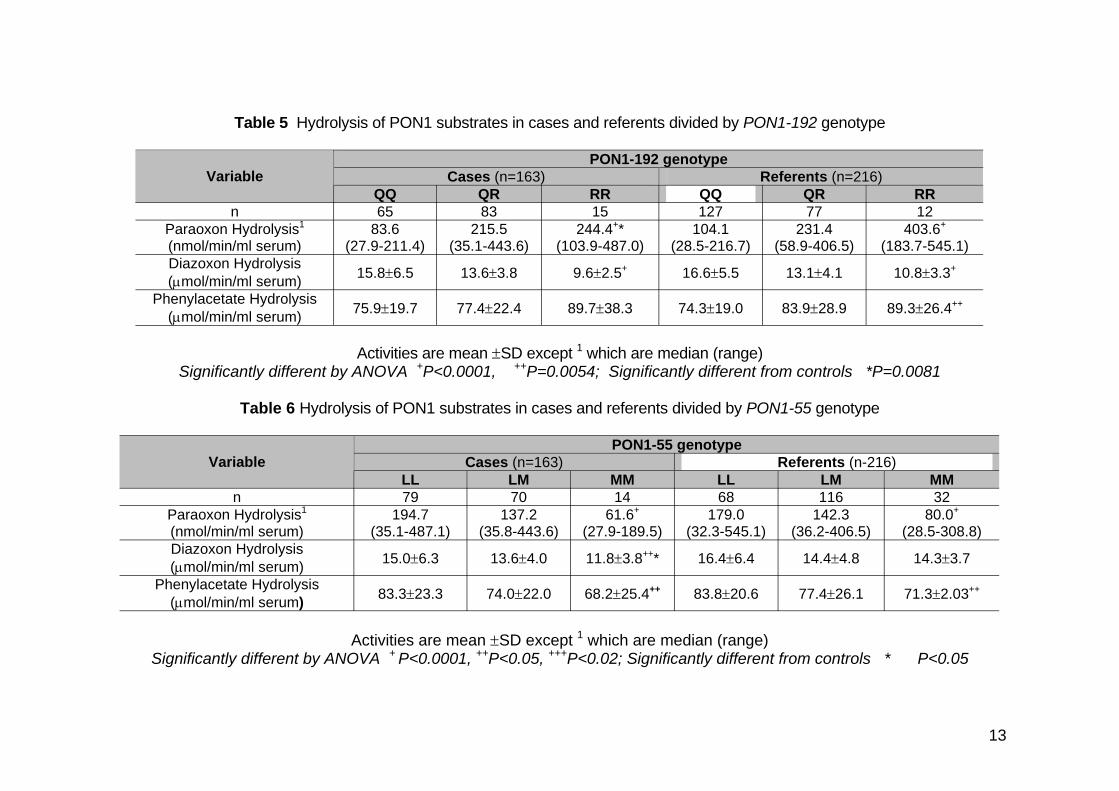
Table 5 Hydrolysis of PON1 substrates in cases and referents divided by PON1-192 genotype
Paraoxon Hydrolysis1
(nmol/min/ml serum)
Variable
n 83.6
(27.9-211.4)
QQ 65
215.5 (35.1-443.6)
Cases (n=163) QR 83
244.4+* (103.9-487.0)
104.1 (28.5-216.7)
PON1-192 genotype
RR QQ 15 127
231.4 (58.9-406.5)
Referents (n=216) QR 77
403.6+
(183.7-545.1)
RR 12
Diazoxon Hydrolysis (µmol/min/ml serum) 15.8±6.5 13.6±3.8 9.6±2.5+ 16.6±5.5 13.1±4.1 10.8±3.3+
Phenylacetate Hydrolysis (µmol/min/ml serum) 75.9±19.7 77.4±22.4 89.7±38.3 74.3±19.0 83.9±28.9 89.3±26.4++
Activities are mean ±SD except 1 which are median (range) Significantly different by ANOVA +P<0.0001, ++P=0.0054; Significantly different from controls *P=0.0081
Table 6 Hydrolysis of PON1 substrates in cases and referents divided by PON1-55 genotype
Paraoxon Hydrolysis1
(nmol/min/ml serum)
Variable
n 194.7
(35.1-487.1)
LL 79
137.2 (35.8-443.6)
Cases (n=163) LM 70
61.6+
(27.9-189.5) 179.0
(32.3-545.1)
PON1-55 genotype
MM LL 14 68
142.3 (36.2-406.5)
Referents (n-216) LM 116
80.0+
(28.5-308.8)
MM 32
Diazoxon Hydrolysis (µmol/min/ml serum) 15.0±6.3 13.6±4.0 11.8±3.8++* 16.4±6.4 14.4±4.8 14.3±3.7
Phenylacetate Hydrolysis (µmol/min/ml serum) 83.3±23.3 74.0±22.0 68.2±25.4++ 83.8±20.6 77.4±26.1 71.3±2.03++
Activities are mean ±SD except 1 which are median (range) Significantly different by ANOVA + P<0.0001, ++P<0.05, +++P<0.02; Significantly different from controls * P<0.05
13
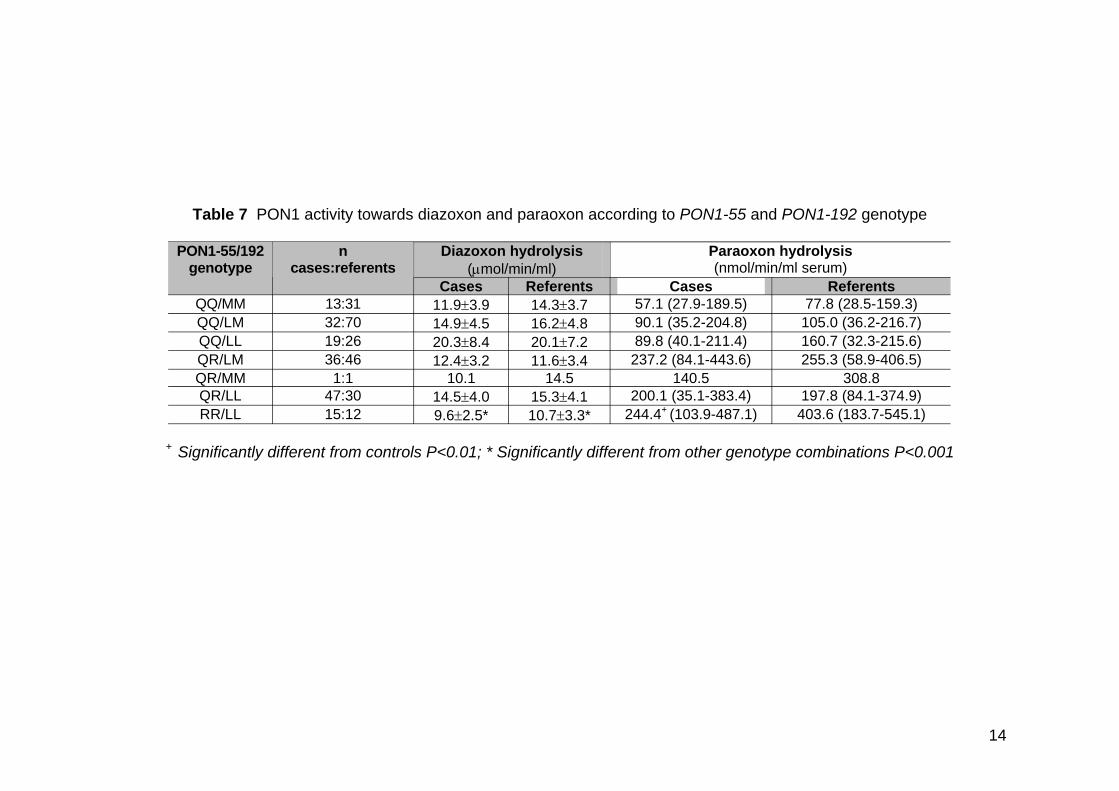
Table 7 PON1 activity towards diazoxon and paraoxon according to PON1-55 and PON1-192 genotype
PON1-55/192 genotype
n cases:referents
Diazoxon hydrolysis (µmol/min/ml)
Paraoxon hydrolysis (nmol/min/ml serum)
Cases Referents Cases Referents QQ/MM 13:31 11.9±3.9 14.3±3.7 57.1 (27.9-189.5) 77.8 (28.5-159.3) QQ/LM 32:70 14.9±4.5 16.2±4.8 90.1 (35.2-204.8) 105.0 (36.2-216.7) QQ/LL 19:26 20.3±8.4 20.1±7.2 89.8 (40.1-211.4) 160.7 (32.3-215.6) QR/LM 36:46 12.4±3.2 11.6±3.4 237.2 (84.1-443.6) 255.3 (58.9-406.5) QR/MM 1:1 10.1 14.5 140.5 308.8 QR/LL 47:30 14.5±4.0 15.3±4.1 200.1 (35.1-383.4) 197.8 (84.1-374.9) RR/LL 15:12 9.6±2.5* 10.7±3.3* 244.4+ (103.9-487.1) 403.6 (183.7-545.1)
+ Significantly different from controls P<0.01; * Significantly different from other genotype combinations P<0.001
14
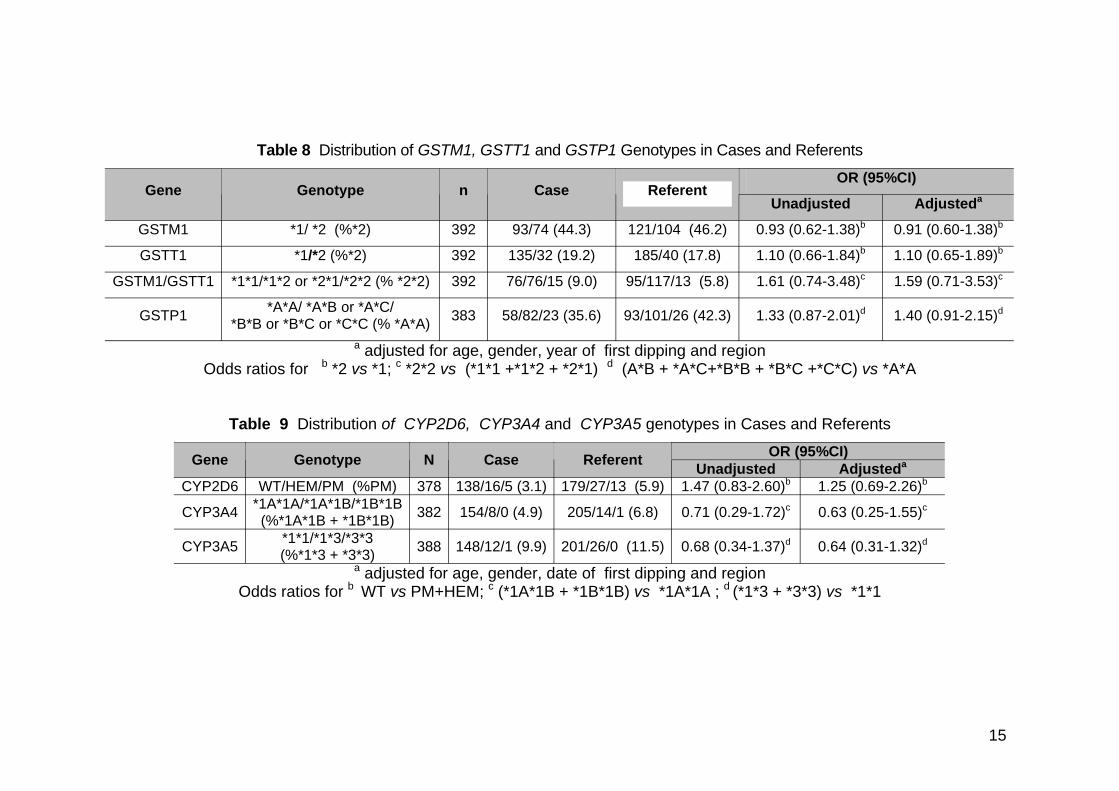
Table 8 Distribution of GSTM1, GSTT1 and GSTP1 Genotypes in Cases and Referents
Gene Genotype n Case Referent OR (95%CI)
Unadjusted Adjusteda
GSTM1 *1/ *2 (%*2) 392 93/74 (44.3) 121/104 (46.2) 0.93 (0.62-1.38)b 0.91 (0.60-1.38)b
GSTT1 *1/*2 (%*2) 392 135/32 (19.2) 185/40 (17.8) 1.10 (0.66-1.84)b 1.10 (0.65-1.89)b
GSTM1/GSTT1 *1*1/*1*2 or *2*1/*2*2 (% *2*2) 392 76/76/15 (9.0) 95/117/13 (5.8) 1.61 (0.74-3.48)c 1.59 (0.71-3.53)c
GSTP1 *A*A/ *A*B or *A*C/ *B*B or *B*C or *C*C (% *A*A) 383 58/82/23 (35.6) 93/101/26 (42.3) 1.33 (0.87-2.01)d 1.40 (0.91-2.15)d
a adjusted for age, gender, year of first dipping and regiondOdds ratios for b *2 vs *1; c *2*2 vs (*1*1 +*1*2 + *2*1) (A*B + *A*C+*B*B + *B*C +*C*C) vs *A*A
Table 9 Distribution of CYP2D6, CYP3A4 and CYP3A5 genotypes in Cases and Referents
Gene
CYP2D6
CYP3A4
CYP3A5
Genotype
WT/HEM/PM (%PM) *1A*1A/*1A*1B/*1B*1B (%*1A*1B + *1B*1B)
*1*1/*1*3/*3*3 (%*1*3 + *3*3)
N
378
382
388
Case
138/16/5 (3.1)
154/8/0 (4.9)
148/12/1 (9.9)
Referent
179/27/13 (5.9)
205/14/1 (6.8)
201/26/0 (11.5)
OR (95%CI) Unadjusted Adjusteda
1.47 (0.83-2.60)b 1.25 (0.69-2.26)b
0.71 (0.29-1.72)c 0.63 (0.25-1.55)c
0.68 (0.34-1.37)d 0.64 (0.31-1.32)d
a adjusted for age, gender, date of first dipping and region Odds ratios for b WT vs PM+HEM; c (*1A*1B + *1B*1B) vs *1A*1A ; d (*1*3 + *3*3) vs *1*1
15
3.2 STAGED ANALYSIS
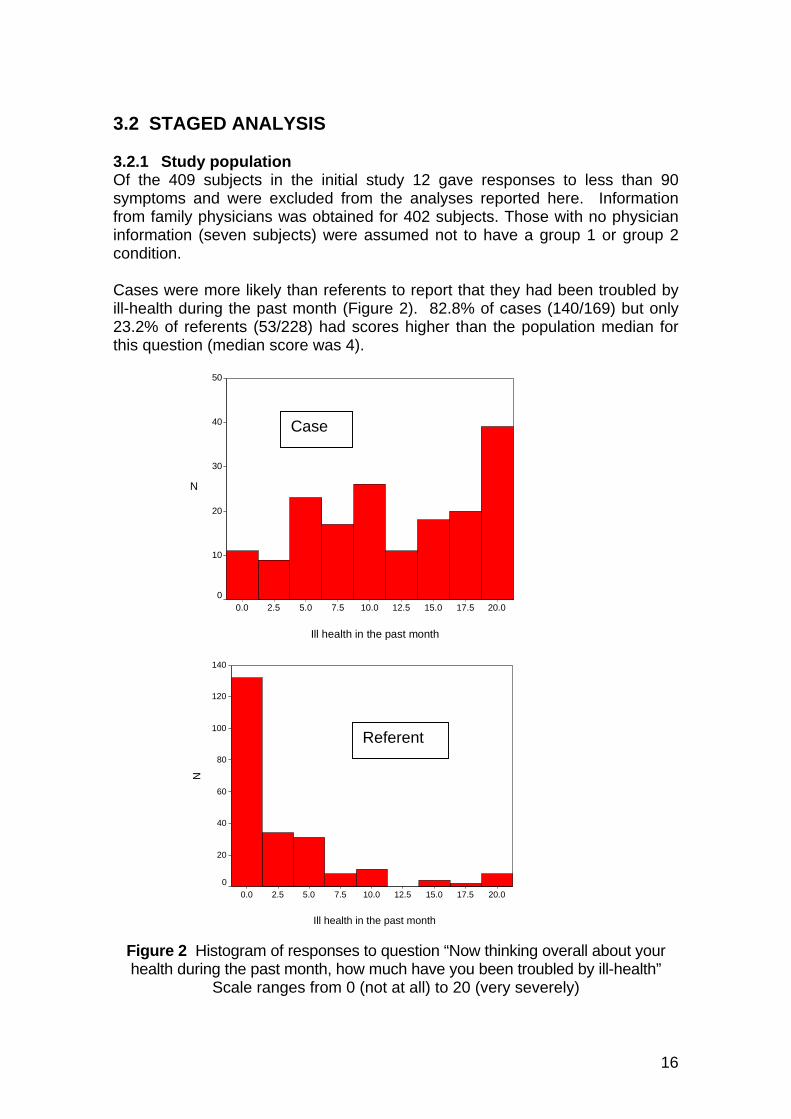
3.2.1 Study population Of the 409 subjects in the initial study 12 gave responses to less than 90 symptoms and were excluded from the analyses reported here. Information from family physicians was obtained for 402 subjects. Those with no physician information (seven subjects) were assumed not to have a group 1 or group 2 condition.
Cases were more likely than referents to report that they had been troubled by ill-health during the past month (Figure 2). 82.8% of cases (140/169) but only 23.2% of referents (53/228) had scores higher than the population median for this question (median score was 4).
Ill i
N
50
40
30
20
10
0
Case
health n the past month
20.0 17.5 15.0 12.5 10.0 7.5 5.0 2.5 0.0
N
140
120
100
80
60
40
20
0
Referent
0.0 2.5 5.0 7.5 10.0 12.5 15.0 17.5 20.0
Ill health in the past month
Figure 2 Histogram of responses to question “Now thinking overall about your health during the past month, how much have you been troubled by ill-health”
Scale ranges from 0 (not at all) to 20 (very severely)
16
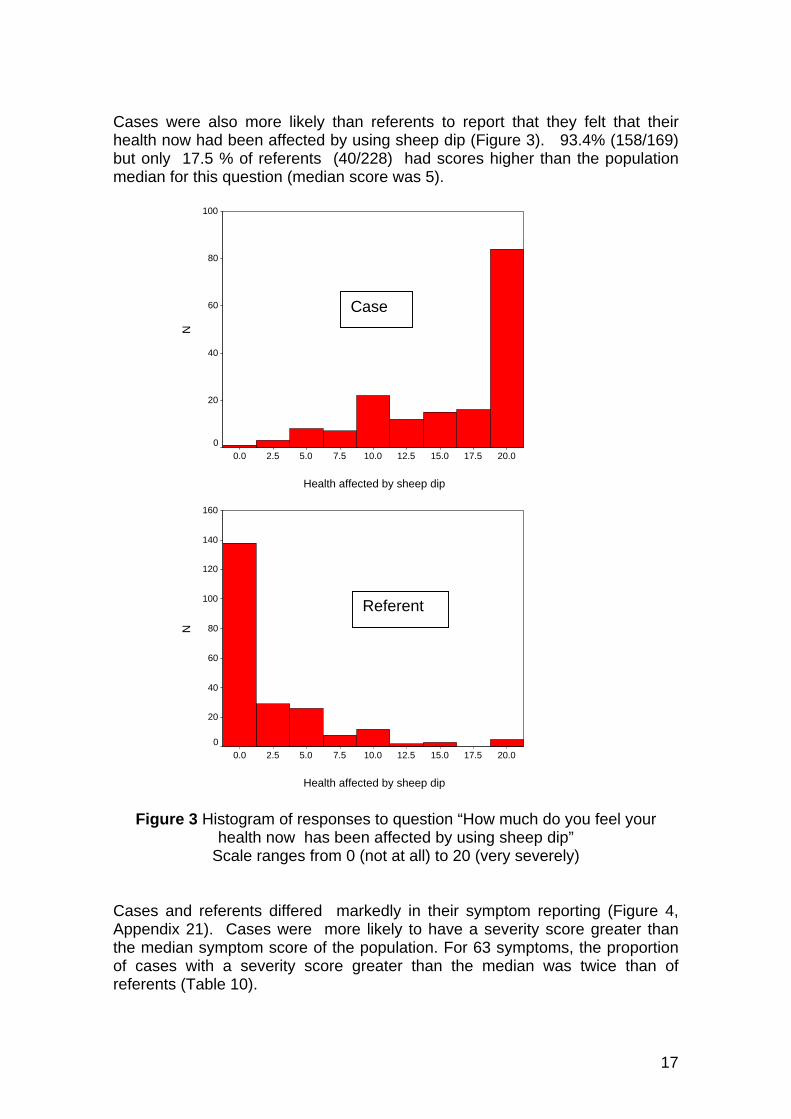
Cases were also more likely than referents to report that they felt that their health now had been affected by using sheep dip (Figure 3). 93.4% (158/169) but only 17.5 % of referents (40/228) had scores higher than the population median for this question (median score was 5).
NN
100
80
60
40
20
0 0.0 2.5 5.0 7.5 10.0 12.5 15.0 17.5 20.0
Case
Health affected by sheep dip
160
140
120
100
80
60
40
20
0 0.0 2.5 5.0 7.5 10.0 12.5 15.0 17.5 20.0
Referent
Health affected by sheep dip
Figure 3 Histogram of responses to question “How much do you feel your health now has been affected by using sheep dip”
Scale ranges from 0 (not at all) to 20 (very severely)
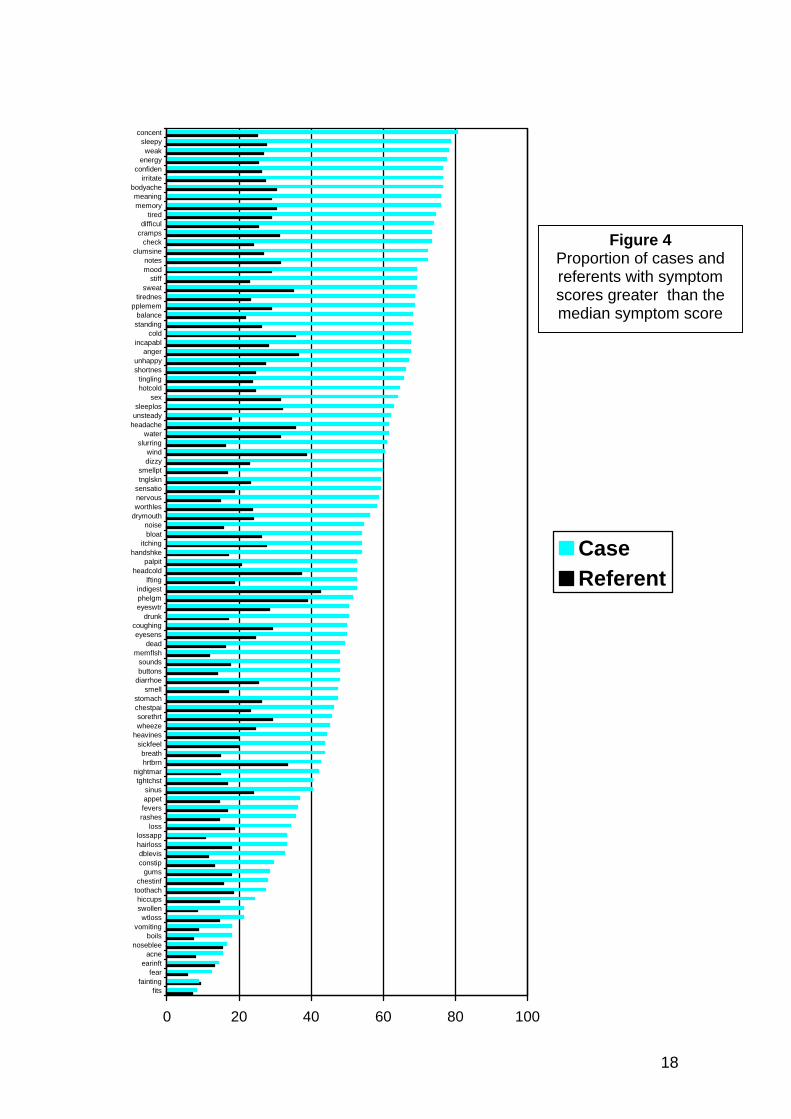
Cases and referents differed markedly in their symptom reporting (Figure 4, Appendix 21). Cases were more likely to have a severity score greater than the median symptom score of the population. For 63 symptoms, the proportion of cases with a severity score greater than the median was twice than of referents (Table 10).
17
concent sleepy weak
energy confiden
irritate bodyache meaning memory
tired difficul
cramps check
clumsine notes mood
stiff sweat
tirednes pplemem
balance standing
cold incapabl
anger unhappy shortnes
tingling hotcold
sex sleeplos
unsteady headache
water slurring
wind dizzy
smellpt tnglskn
sensatio nervous worthles
drymouth noise bloat
itching handshke
palpit headcold
lfting indigest phelgm eyeswtr
drunk coughing eyesens
dead memflsh
sounds buttons
diarrhoe smell
stomach chestpai sorethrt wheeze
heavines sickfeel breath hrtbrn
nightmar tghtchst
sinus appet fevers rashes
loss lossapp hairloss dblevis constip
gums chestinf
toothach hiccups swollen wtloss
vomiting boils
noseblee acne
earinft fear
fainting fits
Figure 4 Proportion of cases and referents with symptom scores greater than the median symptom score
Case Referent
0 20 40 60 80 100
18
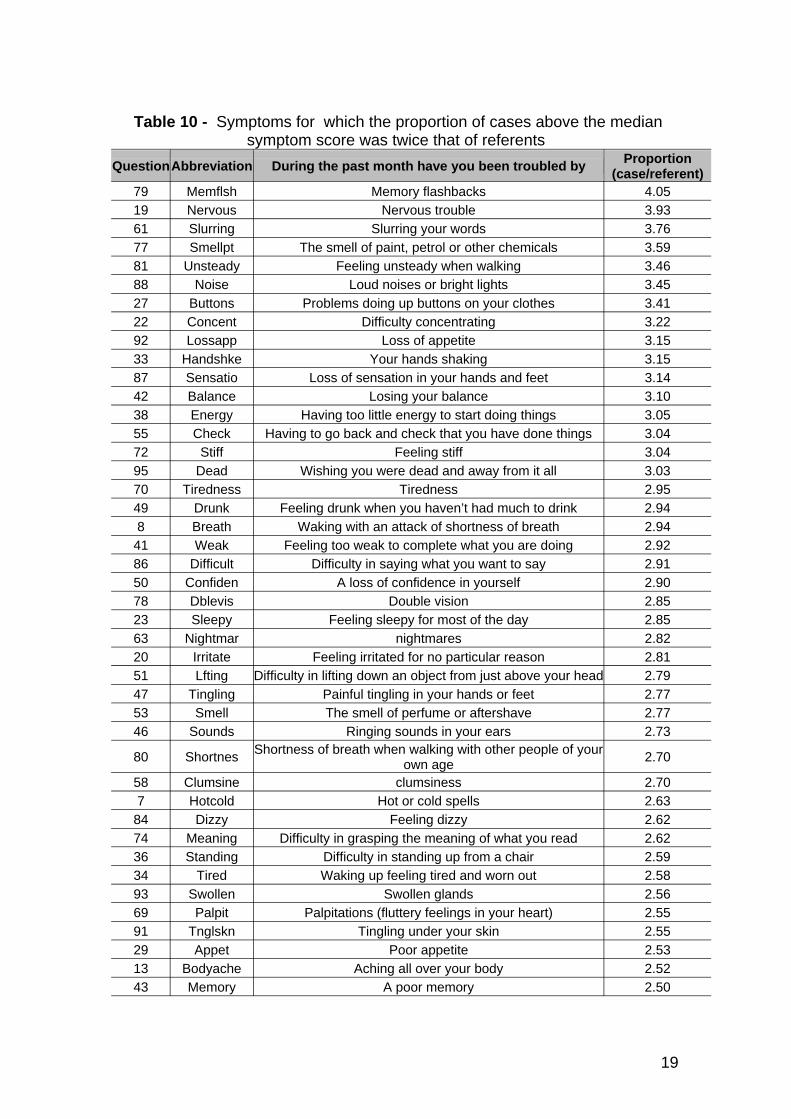
Table 10 - Symptoms for which the proportion of cases above the median symptom score was twice that of referents
Question Abbreviation
79 Memflsh 19 Nervous 61 Slurring 77 Smellpt 81 Unsteady 88 Noise 27 Buttons 22 Concent 92 Lossapp 33 Handshke 87 Sensatio 42 Balance 38 Energy 55 Check 72 Stiff 95 Dead 70 Tiredness 49 Drunk 8 Breath
41 Weak 86 Difficult 50 Confiden 78 Dblevis 23 Sleepy 63 Nightmar 20 Irritate 51 Lfting 47 Tingling 53 Smell 46 Sounds
80 Shortnes
58 Clumsine 7 Hotcold
84 Dizzy 74 Meaning 36 Standing 34 Tired 93 Swollen 69 Palpit 91 Tnglskn 29 Appet 13 Bodyache 43 Memory
During the past month have you been troubled by
Memory flashbacks Nervous trouble
Slurring your words The smell of paint, petrol or other chemicals
Feeling unsteady when walking Loud noises or bright lights
Problems doing up buttons on your clothes Difficulty concentrating
Loss of appetite Your hands shaking
Loss of sensation in your hands and feet Losing your balance
Having too little energy to start doing things Having to go back and check that you have done things
Feeling stiff Wishing you were dead and away from it all
Tiredness Feeling drunk when you haven’t had much to drink
Waking with an attack of shortness of breath Feeling too weak to complete what you are doing
Difficulty in saying what you want to say A loss of confidence in yourself
Double vision Feeling sleepy for most of the day
nightmares Feeling irritated for no particular reason
Difficulty in lifting down an object from just above your head Painful tingling in your hands or feet The smell of perfume or aftershave
Ringing sounds in your ears Shortness of breath when walking with other people of your
own age clumsiness
Hot or cold spells Feeling dizzy
Difficulty in grasping the meaning of what you read Difficulty in standing up from a chair Waking up feeling tired and worn out
Swollen glands Palpitations (fluttery feelings in your heart)
Tingling under your skin Poor appetite
Aching all over your body A poor memory
Proportion (case/referent)
4.05 3.93 3.76 3.59 3.46 3.45 3.41 3.22 3.15 3.15 3.14 3.10 3.05 3.04 3.04 3.03 2.95 2.94 2.94 2.92 2.91 2.90 2.85 2.85 2.82 2.81 2.79 2.77 2.77 2.73
2.70
2.70 2.63 2.62 2.62 2.59 2.58 2.56 2.55 2.55 2.53 2.52 2.50
19
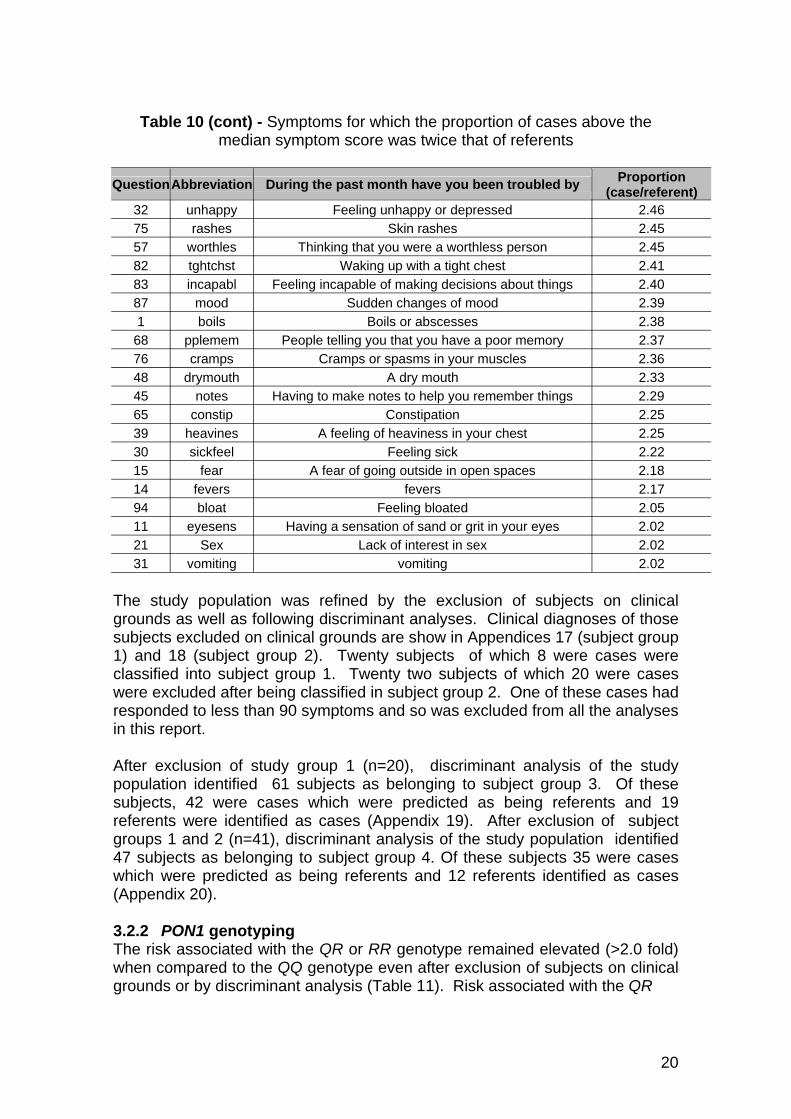
Table 10 (cont) - Symptoms for which the proportion of cases above the median symptom score was twice that of referents
Question Abbreviation During the past month have you been troubled by
32 unhappy Feeling unhappy or depressed 75 rashes Skin rashes 57 worthles Thinking that you were a worthless person 82 tghtchst Waking up with a tight chest 83 incapabl Feeling incapable of making decisions about things 87 mood Sudden changes of mood 1 boils Boils or abscesses
68 pplemem People telling you that you have a poor memory 76 cramps Cramps or spasms in your muscles 48 drymouth A dry mouth 45 notes Having to make notes to help you remember things 65 constip Constipation 39 heavines A feeling of heaviness in your chest 30 sickfeel Feeling sick 15 fear A fear of going outside in open spaces 14 fevers fevers 94 bloat Feeling bloated 11 eyesens Having a sensation of sand or grit in your eyes 21 Sex Lack of interest in sex 31 vomiting vomiting
Proportion (case/referent)
2.46 2.45 2.45 2.41 2.40 2.39 2.38 2.37 2.36 2.33 2.29 2.25 2.25 2.22 2.18 2.17 2.05 2.02 2.02 2.02
The study population was refined by the exclusion of subjects on clinical grounds as well as following discriminant analyses. Clinical diagnoses of those subjects excluded on clinical grounds are show in Appendices 17 (subject group 1) and 18 (subject group 2). Twenty subjects of which 8 were cases were classified into subject group 1. Twenty two subjects of which 20 were cases were excluded after being classified in subject group 2. One of these cases had responded to less than 90 symptoms and so was excluded from all the analyses in this report.
After exclusion of study group 1 (n=20), discriminant analysis of the study population identified 61 subjects as belonging to subject group 3. Of these subjects, 42 were cases which were predicted as being referents and 19 referents were identified as cases (Appendix 19). After exclusion of subject groups 1 and 2 (n=41), discriminant analysis of the study population identified 47 subjects as belonging to subject group 4. Of these subjects 35 were cases which were predicted as being referents and 12 referents identified as cases (Appendix 20).
3.2.2 PON1 genotyping The risk associated with the QR or RR genotype remained elevated (>2.0 fold) when compared to the QQ genotype even after exclusion of subjects on clinical grounds or by discriminant analysis (Table 11). Risk associated with the QR
20
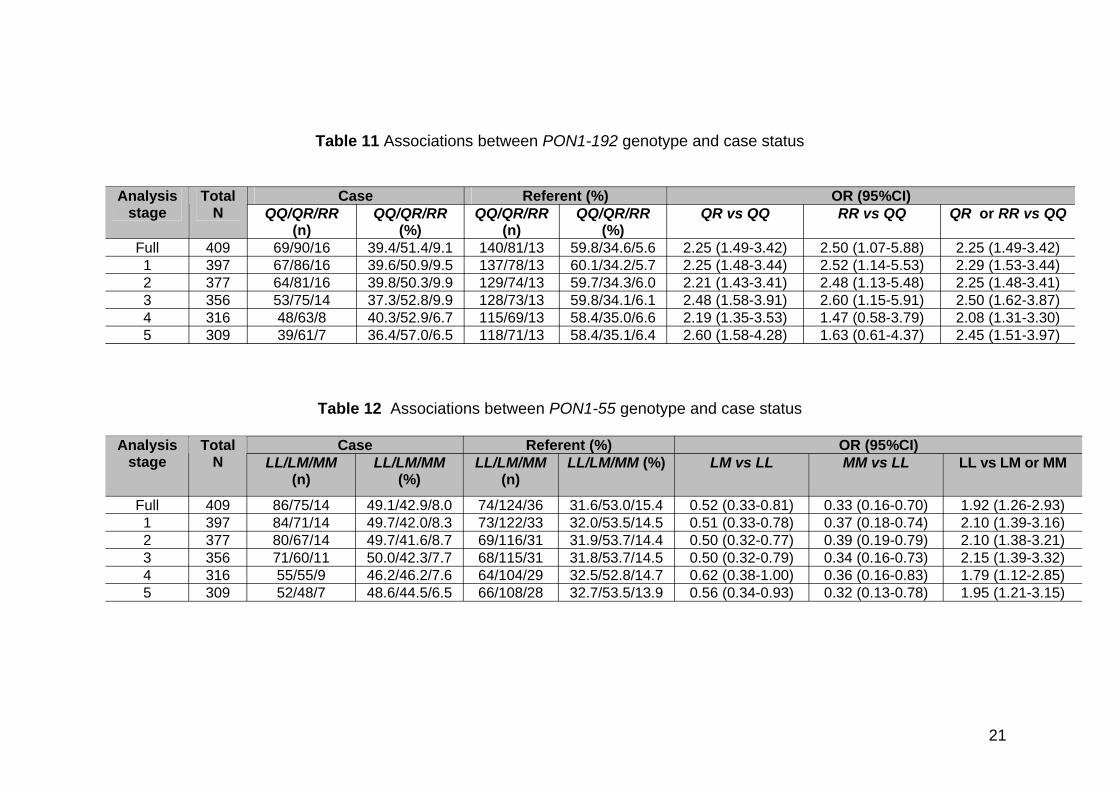
Table 11 Associations between PON1-192 genotype and case status
Analysis stage
Total N
Case Referent (%) OR (95%CI) QQ/QR/RR
(n) QQ/QR/RR
(%) QQ/QR/RR
(n) QQ/QR/RR
(%) QR vs QQ RR vs QQ QR or RR vs QQ
Full 409 69/90/16 39.4/51.4/9.1 140/81/13 59.8/34.6/5.6 2.25 (1.49-3.42) 2.50 (1.07-5.88) 2.25 (1.49-3.42) 1 397 67/86/16 39.6/50.9/9.5 137/78/13 60.1/34.2/5.7 2.25 (1.48-3.44) 2.52 (1.14-5.53) 2.29 (1.53-3.44) 2 377 64/81/16 39.8/50.3/9.9 129/74/13 59.7/34.3/6.0 2.21 (1.43-3.41) 2.48 (1.13-5.48) 2.25 (1.48-3.41) 3 356 53/75/14 37.3/52.8/9.9 128/73/13 59.8/34.1/6.1 2.48 (1.58-3.91) 2.60 (1.15-5.91) 2.50 (1.62-3.87) 4 316 48/63/8 40.3/52.9/6.7 115/69/13 58.4/35.0/6.6 2.19 (1.35-3.53) 1.47 (0.58-3.79) 2.08 (1.31-3.30) 5 309 39/61/7 36.4/57.0/6.5 118/71/13 58.4/35.1/6.4 2.60 (1.58-4.28) 1.63 (0.61-4.37) 2.45 (1.51-3.97)
Table 12 Associations between PON1-55 genotype and case status
Analysis stage
Total N
Case Referent (%) OR (95%CI) LL/LM/MM
(n) LL/LM/MM
(%) LL/LM/MM
(n) LL/LM/MM (%) LM vs LL MM vs LL LL vs LM or MM
Full 409 86/75/14 49.1/42.9/8.0 74/124/36 31.6/53.0/15.4 0.52 (0.33-0.81) 0.33 (0.16-0.70) 1.92 (1.26-2.93) 1 397 84/71/14 49.7/42.0/8.3 73/122/33 32.0/53.5/14.5 0.51 (0.33-0.78) 0.37 (0.18-0.74) 2.10 (1.39-3.16) 2 377 80/67/14 49.7/41.6/8.7 69/116/31 31.9/53.7/14.4 0.50 (0.32-0.77) 0.39 (0.19-0.79) 2.10 (1.38-3.21) 3 356 71/60/11 50.0/42.3/7.7 68/115/31 31.8/53.7/14.5 0.50 (0.32-0.79) 0.34 (0.16-0.73) 2.15 (1.39-3.32) 4 316 55/55/9 46.2/46.2/7.6 64/104/29 32.5/52.8/14.7 0.62 (0.38-1.00) 0.36 (0.16-0.83) 1.79 (1.12-2.85) 5 309 52/48/7 48.6/44.5/6.5 66/108/28 32.7/53.5/13.9 0.56 (0.34-0.93) 0.32 (0.13-0.78) 1.95 (1.21-3.15)
21
genotype (vs QQ) remained similar but that of the RR genotype (vs QQ) was reduced when subjects were excluded by discriminant analysis. The risk associated with the LL genotype remained elevated when compared to the LM or MM genotype even after subject exclusion (Table 12). The decreased risk associated with the MM genotype was lower than that of the LM genotype.
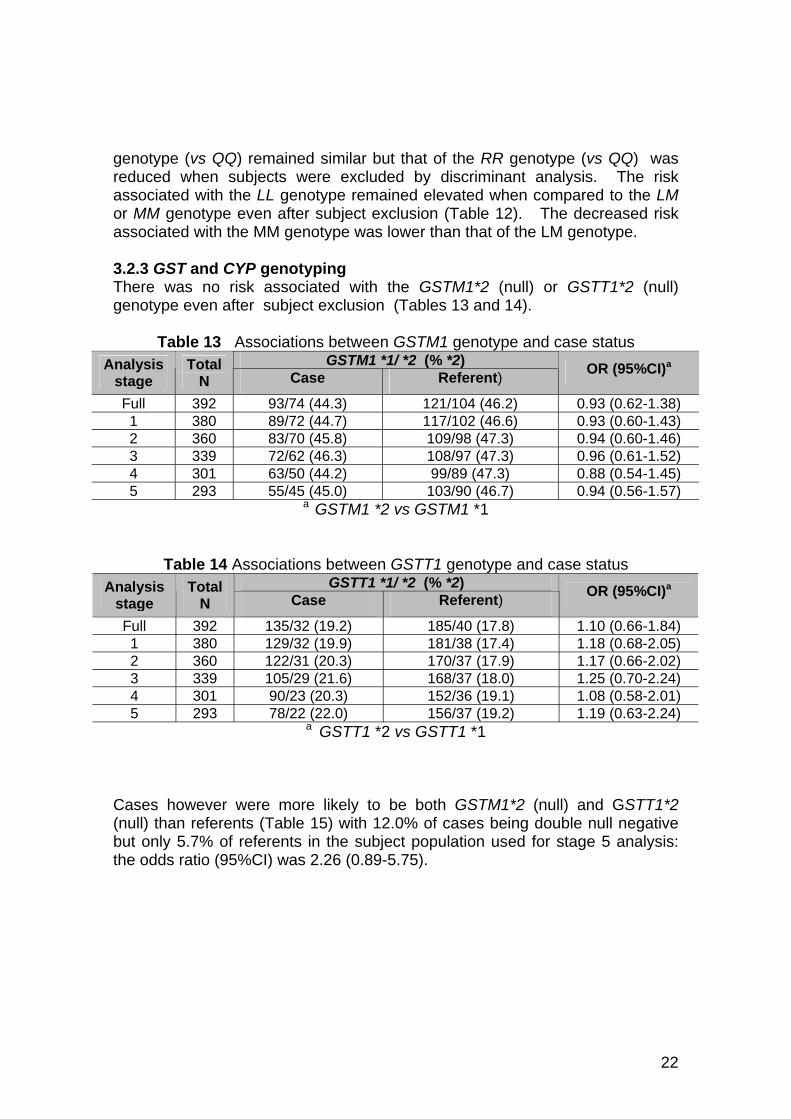
3.2.3 GST and CYP genotyping There was no risk associated with the GSTM1*2 (null) or GSTT1*2 (null) genotype even after subject exclusion (Tables 13 and 14).
Table 13 Associations between GSTM1 genotype and case status (% *2)
stage Total
N Case Referent) )a
Full 392 93/74 (44.3) 121/104 (46.2) 0.93 (0.62-1.38) 1 380 89/72 (44.7) 117/102 (46.6) 0.93 (0.60-1.43) 2 360 83/70 (45.8) 109/98 (47.3) 0.94 (0.60-1.46) 3 339 72/62 (46.3) 108/97 (47.3) 0.96 (0.61-1.52) 4 301 63/50 (44.2) 99/89 (47.3) 0.88 (0.54-1.45) 5 293 55/45 (45.0) 103/90 (46.7) 0.94 (0.56-1.57)
GSTM1 *1/ *2Analysis OR (95%CI
a GSTM1 *2 vs GSTM1 *1
Table 14 GSTT1 genotype and case status GSTT1 *1/ *2 (% *2)
stage Total
N Case Referent) )a
Full 392 135/32 (19.2) 185/40 (17.8) 1.10 (0.66-1.84) 1 380 129/32 (19.9) 181/38 (17.4) 1.18 (0.68-2.05) 2 360 122/31 (20.3) 170/37 (17.9) 1.17 (0.66-2.02) 3 339 105/29 (21.6) 168/37 (18.0) 1.25 (0.70-2.24) 4 301 90/23 (20.3) 152/36 (19.1) 1.08 (0.58-2.01) 5 293 78/22 (22.0) 156/37 (19.2) 1.19 (0.63-2.24)
Associations between Analysis OR (95%CI
a GSTT1 *2 vs GSTT1 *1
Cases however were more likely to be both GSTM1*2 (null) and GSTT1*2 (null) than referents (Table 15) with 12.0% of cases being double null negative but only 5.7% of referents in the subject population used for stage 5 analysis: the odds ratio (95%CI) was 2.26 (0.89-5.75).
22
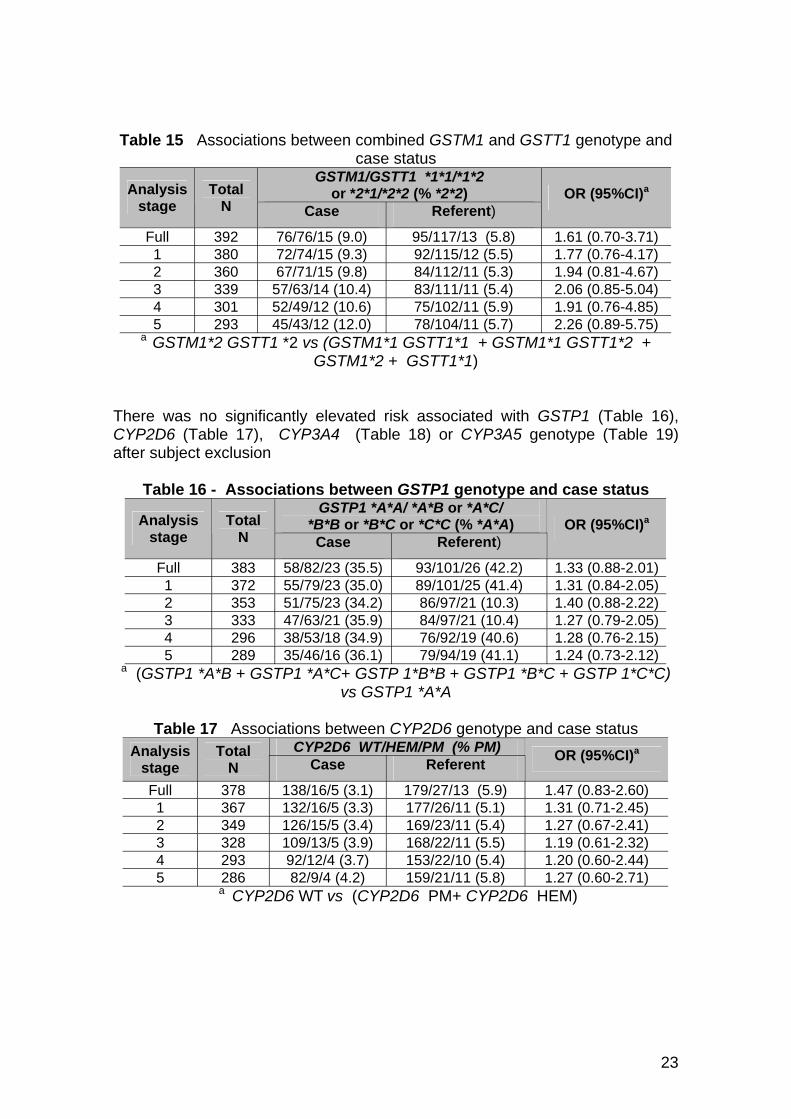
Table 15 Associations between combined GSTM1 and GSTT1 genotype and case status
or *2*1/*2*2 (% )stage
Total N Case Referent)
)a
Full 392 ) 95/117/13 ( 1.61 (0.70-3.71) 1 380 ) 92/115/12 (5.5) 1.77 (0.76-4.17) 2 360 ) 84/112/11 (5.3) 1.94 (0.81-4.67) 3 339 57/63/14 (10.4) 83/111/11 (5.4) 2.06 (0.85-5.04) 4 301 52/49/12 (10.6) 75/102/11 (5.9) 1.91 (0.76-4.85) 5 293 45/43/12 (12.0) 78/104/11 (5.7) 2.26 (0.89-5.75)
GSTM1/GSTT1 *1*1/*1*2 *2*2Analysis OR (95%CI
76/76/15 (9.0 5.8) 72/74/15 (9.367/71/15 (9.8
a GSTM1*2 GSTT1 *2 vs (GSTM1*1 GSTT1*1 + GSTM1*1 GSTT1*2 + GSTM1*2 + GSTT1*1)
There was no significantly elevated risk associated with GSTP1 (Table 16), CYP2D6 (Table 17), CYP3A4 (Table 18) or CYP3A5 genotype (Table 19) after subject exclusion
Table 16 - GSTP1 or /
*B*B or or (% )stage
Total N Case Referent)
)a
Full 383 58/82/23 (35.5) 93/101/26 (42.2) 1.33 (0.88-2.01) 1 372 55/79/23 (35.0) 89/101/25 (41.4) 1.31 (0.84-2.05) 2 353 51/75/23 (34.2) 86/97/21 (10.3) 1.40 (0.88-2.22) 3 333 47/63/21 (35.9) 84/97/21 (10.4) 1.27 (0.79-2.05) 4 296 38/53/18 (34.9) 76/92/19 (40.6) 1.28 (0.76-2.15) 5 289 35/46/16 (36.1) 79/94/19 (41.1) 1.24 (0.73-2.12)
Associations between genotype and case status GSTP1 *A*A/ *A*B *A*C
*B*C *C*C *A*AAnalysis OR (95%CI
a (GSTP1 *A*B + GSTP1 *A*C+ GSTP 1*B*B + GSTP1 *B*C + GSTP 1*C*C) vs GSTP1 *A*A
Table 17 Associations between genotype and case status CYP2D6 / ( )
stage Total
N Case Referent )a
Full 378 ) 179/27/13 ( 1.47 (0.83-2.60) 1 367 ) 177/26/11 (5.1) 1.31 (0.71-2.45) 2 349 ) 169/23/11 (5.4) 1.27 (0.67-2.41) 3 328 ) 168/22/11 (5.5) 1.19 (0.61-2.32) 4 293 92/12/4 (3.7) 153/22/10 (5.4) 1.20 (0.60-2.44) 5 286 82/9/4 (4.2) 159/21/11 (5.8) 1.27 (0.60-2.71)
CYP2D6WT/HEM PM % PMAnalysis OR (95%CI
138/16/5 (3.1 5.9) 132/16/5 (3.3126/15/5 (3.4109/13/5 (3.9
a CYP2D6 WT vs (CYP2D6 PM+ CYP2D6 HEM)
23
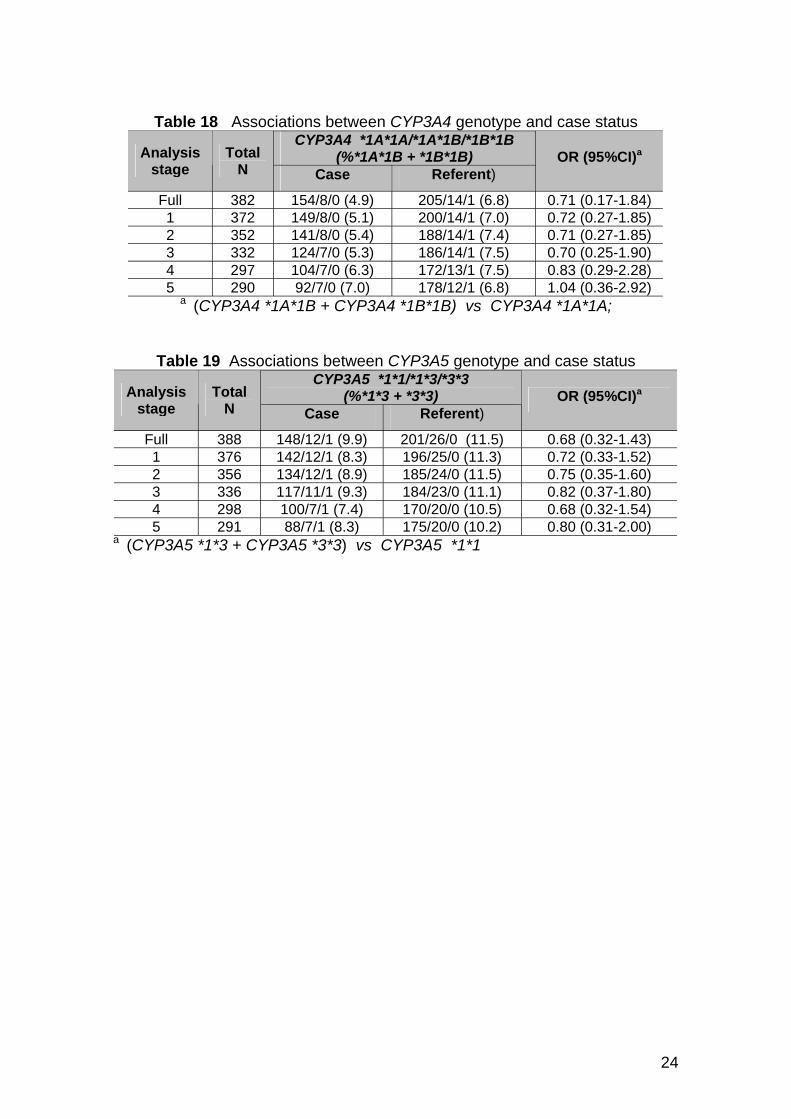
Table 18 Associations between genotype and case status CYP3A4
stage Total
N Case Referent) )a
Full 382 154/8/0 (4.9) ) 0.71 (0.17-1.84) 1 372 149/8/0 (5.1) ) 0.72 (0.27-1.85) 2 352 141/8/0 (5.4) ) 0.71 (0.27-1.85) 3 332 124/7/0 (5.3) ) 0.70 (0.25-1.90) 4 297 104/7/0 (6.3) ) 0.83 (0.29-2.28) 5 290 92/7/0 (7.0) ) 1.04 (0.36-2.92)
CYP3A4*1A*1A/*1A*1B/*1B*1B
(%*1A*1B + *1B*1B) Analysis OR (95%CI
205/14/1 (6.8200/14/1 (7.0188/14/1 (7.4186/14/1 (7.5172/13/1 (7.5178/12/1 (6.8
a (CYP3A4 *1A*1B + CYP3A4 *1B*1B) vs CYP3A4 *1A*1A;
Table 19 Associations between genotype and case status CYP3A5
stage Total
N Case Referent) )a
Full 388 ) 201/26/0 0.68 (0.32-1.43) 1 376 ) 196/25/0 (11.3) 0.72 (0.33-1.52) 2 356 ) 185/24/0 (11.5) 0.75 (0.35-1.60) 3 336 ) 184/23/0 (11.1) 0.82 (0.37-1.80) 4 298 100/7/1 (7.4) 170/20/0 (10.5) 0.68 (0.32-1.54) 5 291 88/7/1 (8.3) 175/20/0 (10.2) 0.80 (0.31-2.00)
CYP3A5*1*1/*1*3/*3*3
(%*1*3 + *3*3) Analysis OR (95%CI
148/12/1 (9.9 (11.5) 142/12/1 (8.3134/12/1 (8.9117/11/1 (9.3
a (CYP3A5 *1*3 + CYP3A5 *3*3) vs CYP3A5 *1*1
24
4.0 DISCUSSION
Experiments in animals have shown that PON1 is important in protecting against OP toxicity46 and that PON1-192 genotype is a major determinant of the rate of hydrolysis of OPs in vitro 13 but not necessarily in vivo47 . The PON1-55 polymorphism also affects the capacity of PON1 to hydrolyse OPs in vitro15. Results from this study indicating that there were differences in the case and referent population in not only the PON1 genotype but also diazoxonase activity are thus consistent with the study hypothesis that OPs contribute to the reported ill health of people who dip sheep.
PON1 metabolises a range of different substrates17,18 and it is conceivable that the reported associations in this study may result from exposure to another substrate, but at the current time there would appear to be no other plausible candidate agent. Physiological substrates for PON1 include lipid peroxidation products18 and accordingly associations between heart disease and PON1 genotype/phenotype have been described but not consistently 19 . Selection bias may thus result from only selecting referents in good health. However, it should be noted that firstly, exclusion of those patients with known heart disease did not alter the risk estimates (see Appendix 22). Furthermore, selection bias did not appear to be a problem as the genotype distribution in the referent group in this study population was consistent with previously published UK datasets 15,48 .
Cases and referents in the SCOPE study differed in their self-report of the severity of many individual symptoms and in the frequency of reporting of these symptoms. This is not surprising as the cases were self-selected as being in poor health and the referents chosen were in ‘good general health’. In the absence of clear diagnostic criteria for chronic ill health associated with OP exposure, cases in this study will have a range of different conditions, some of which may not be caused by OP exposure. In addition, some referents may be symptomatic without invoking OP exposure as a cause. Both would tend to bias the study towards a null result. With further refinement of case and control definition, risk estimates may increase. The method of recruiting subjects will not introduce bias as the recruited population would not know their PON1 genotype or phenotype. An alternative approach of using existing clinical records to reduce heterogeneity by exclusion may however do so; those who believe their condition to be due to OP exposure may be much more likely to have sought medical investigation and to have received a diagnosis than the referents.
To further evaluate the associations between PON1, GST and CYP genotypes and self-reported chronic ill-health in this population, further analysis was carried out after the exclusion of subjects on both clinical grounds and after discriminant analysis. Subjects were excluded so as to provide a more homogenous case and referent population. This refinement made very little difference to the risk associated with PON1 genotype or the lack of risk associated with the other examined genotypes indicating that the original analysis was robust; the missing symptom data on 12 subjects and physician
25
information on seven subjects is unlikely to influence this conclusion. There was some suggestion of increased risk in those subjects who were both GSTM1 null and GSTT1 null but the role of GSTM1 and GSTT1 in the metabolism of OPs is unclear; although it has been reported that glutathione S-transferases can degrade diazinon the importance of such reactions in vivo has been doubted 14-16.
In summary, results from the study are consistent with the a priori hypothesis that organophosphates contribute to the reported ill health of people who dip sheep.
26
REFERENCES
1 Committee on Toxicity of Chemicals in Food, Consumer Products and the Environment. (1999) Organophosphates. Department of Health.
2 Royal College of Physicians and Royal College of Psychiatrists (1998) Organophosphate sheep dip: clinical aspects of long-term low-dose exposure. Report of a joint working party. London: Royal College of Physicians and Royal College of Psychiatrists.
3 Dunn G (2002) Report on an analytical study of OP sheep dips. Veterinary Medicines Directorate, Surrey.
4 Stephens R, Spurgeon A, Calvert IA, Beach J, Levy LS, Berry H, et al. (1995) Neuropsychological effects of long-term exposure to organophosphates in sheep dip. Lancet, 345, 1135-1139.
5 Steenland K, Jenkins B, Ames RG, O'Malley M, Chrislip D, Russo J. (1994) Chronic Neurological Sequelae to Organophosphate Pesticide Poisoning. Am. J. Public Health, 84, No 5; 731-736
6 La Du BN (1996) Structural and functional diversity of paraoxonase. Nature Medicine 2: 1186-1187.
7 Mackness MI, Thompson HM, Hardy AR, Walker CH (1987) Distinction between 'A'-esterases and arylesterases - implications for esterase classification. Biochem. J. 245: 293-296.
8 Mackness MI, Mackness B, Durrington PN, Connelly PW, Hegele RF (1996) Paraoxonase: biochemistry, genetics and relationship to plasma lipids and lipoproteins. Curr. Opinion Lipidol., 7, 69-76.
9 Mackness MI (1989) 'A'-Esterases - Enzymes looking for a role? Biochem. Pharmacol 38 385-390.
10 Walker CH, Mackness MI (1983) Commentary "Esterases: Problems of identification and classification". Biochem. Pharmacol. 32, (22): 3265-3269
11 Adkins S, Gan KN, Mody M, La Du BN, (1993) Molecular basis for the polymorphic forms of human serum paraoxonase/arylesterase: Glutamine or Arginine at position 191, for the respective A or B alloenzymes. Am. J. Hum. Genet. 52:598-608.
12 Humbert R, Adler DA, Disteche CM, Hassett C, Omiecinski CJ, Furlong CE (1993) The molecular basis for the human serum paraoxonase activity polymorphism. Nature Genetics 3: 73-76.
13 Davies HG, Richter RJ, Keifer M, Broomfield CA, Sowalla J, Furlong CE (1996) The effect of the human serum paraoxonase polymorphism is reversed with diazoxon, soman and sarin. Nature Genetics 14: 334-336.
14 La Du BN (1992) Human serum paraoxonase/arylesterase. In Pharmacogenetics of Drug Metabolism. W. Karlow editor. Pergamon Press, New York. pp51-91.
15 Mackness B, Mackness MI, Arrol S, Tarkie W, Durrington PF (1997) Effect of the molecular polymorphisms of human paraoxonase on the rate of hydrolysis of paraoxon. Brit. J. Pharmacol. 112: 265-268.
16 Costa LG, Manzo L (1995) Biochemical markers of neurotoxicity: research strategies and epidemiological applications. Toxicol. Letts. 77: 137-144.
27
17 Billecke S, Draganov D, Counsell R, Stetson P, Watson C, Hsu C. La Du BN (2000) Human serum paraoxonase (PON1) isozymes Q and R hydrolyse lactones and cyclic carbonate esters. Drug. Metab. Dispos. 28: 1335-1342.
18 Ahmed Z, Ravandi A, Maguire GF, Emili A, Draganov D, La Du BN, Kuksis A, Connelly PW (2002) Multiple substrates for Paraoxonase-1 during oxidation of phosphatidylcholine by peroxynitrite. Biochem. Biophys. Res. Comm.. 290: 391-396.
19 Senti M, Tomas M, Elosua R, Marrugat J. (2000) Interrelationship of serum paraoxonase activity and paraoxonase genetic variants on atherosclerosis risk Contributions to Science , 1: 323-329.
20 Mackness B, Durrington PN, Mackness MI. (2000) Low paraoxonase in Persian Gulf War veterans self-reporting gulf war syndrome. Biochem. Biophys. Res. Commun. 276: 729-733.
21 Haley RW, Billecke S, La Du BN. (1999) Association of low PON1 Type Q (Type A) arylesterase activity with neurologic symptom complexes in Gulf War Veterans. Toxicol. Appl. Pharmacol. 157: 227-233.
22 Dillon HH, Ho MH (1987) Biological monitoring of exposure to organophosphorus pesticides in Ho MH, Dillon HH (eds) Biological Monitoring of exposure to chemicals. Organic Compounds, New York; John Wiley & Sons 227-287.
23 Soreq H, Zakut H (1993) Human cholinesterases and anticholinesterases. Academic Press, California.
24 Butler AM, Murray M (1997) Biotransformation of parathion in human liver: participation of CYP3A4 and its inactivation during microsomal parathion oxidation. J. Pharmacol. Exp. Ther., 280: 966-973,
25 Sams C, Mason HJ, Rawbone R (2000) Evidence for the activation of organophosphate pesticides by cytochromes P450 3A4 and 2D6 in human liver microsomes. Toxicol Lett., 116:217-221.
26 May DG, Porter J, Wilkinson GR, Branch RA (1994) Frequency distribution of dapsone N-hydroxylase, a putative probe for p4503A4 activity in a white population. Clin. Pharmacol. Ther., 55: 492-500.
27 Daly AK (1995) Molecular basis of polymorphic drug metabolism J. Mol. Med., 73: 539-553.
28 Smith CAD, Gough AC, Leigh PN, Summers BA, Harding AE, Maranganore DM, Sturman SG, Schapira AHV, Williams AC, Spurr NK, Wolf C R (1992) Debrisoquine hydroxylase gene polymorphism and susceptibility to Parkinson's disease. Lancet, 339: 1375-1377.
29 Rebbeck TR, Jaffe JM, Walker AH, Wein AJ, Malkowicz SB (1998) Modification of clinical presentation of prostate tumors by a novel genetic variant in CYP3A4. J. Natl. Cancer Inst., 90: 1225-1229
30 Westlind A, Lofberg L, Tindber N, Andersson TB, Ingelman-Sundberg M (1999) Interindividual differences in hepatic expression of CYP3A4: relationship to genetic polymorphism in the 5'-upstream regulatory region. Biochem. Biophys. Res. Comm., 259: 201-205.
31 Sata F, Sapone A, Elizondo G, Stocker P, Miller VP, Zheng W, Raunio H, Crespi CL, Gonzalez FJ (2000) CYP3A4 allelic variants with amino acid substitutions in exons 7 and 12: evidence for an allelic variant with altered catalytic activity. Clin. Pharmacol. Ther., 67: 48-56.
28
32 Motoyama N (1980) Glutathione S-transferases: their role in the metabolism of organophosphorus insecticides. Rev. Biochem. Toxicol., 2: 49-69.
33 Sultatos LG (1992) Role of glutathione in the mammalian detoxication of organophosphorus insecticides. In Chambers JE and Levi PE (Eds) Organophosphates : Chemistry, Fate, and Effects. Academic Press, NY, pp 155-168
34 Rebbeck TR. (1997) Molecular epidemiology of the human glutathione s-transferase genotypes GSTM1 and GSTT1 in cancer susceptibility. Cancer Epidemiol. Biomarkers & Prevent., 6: 733-743
35 Ali-Osman F, Akande O, Antoun G, Mao JX, Buolamwini J. (1997) Molecular cloning, characterisation, and expression in Escherichia coli of full-length cDNAs of three human glutathione S-transferase Pi gene variants. Evidence for differential catalyic activity of the encoded proteins. J. Biol. Chem., 272: 10004-10012.
36 Omenn GS (1987) The role of genetic differences in human susceptibility to pesticides in Costa LG et al (Eds) Toxicology of pesticides: experimental, clinical and regulatory aspects, Springer-Verlag, Berlin, pp 93-106.
37 Cherry N, Creed F, Silman A, Dunn G, Baxter D, Smedley J, Taylor S, Macfarlane GJ (2001) Health and exposures of United Kingdom Gulf War Veterans. Part I: the pattern and extent of ill health. Occup. Environ. Med., 58: 291-298.
38 Niven KJM, Scott AJ, Hagen S, Waclawski ER, Lovett M, Cherrie B, Bodsworth PL, Robertson A, Elder A, Cocker J, Nutley B, Roff M (1993) Occupational Hygiene Assessment of Sheep Dipping Practices and Processes. IOM Report TM/93/03. IOM Edinburgh.
39 La Du BN, Eckerson HW (1984) The polymorphic paraoxonase/arylesterase isozymes of human serum. Fed. Proc., 43: 23382341.
40 Abbott CA, Mackness MI, Kumar S. Boulton AJM, Durrington PN (1995) Serum paraoxonase activity, concentration and phenotype distribution in diabetes mellitus. Arterioscler. Thromb. Vasc. Biol., 15, 1812-1818.
41 Lewis SJ, Cherry NM, McLNiven R, Barber PV, Povey AC. (2001) Polymorphisms in the NAD(P)H: Quinone oxidoreductase gene and small cell lung cancer risk in a UK population. Lung Cancer, 34: 177-183
42 Lewis SJ, Cherry NM, McLNiven R, Barber PV, Povey AC. (2002) GSTM1, GSTT1 and GSTP1 polymorphisms and lung cancer risk. Cancer Letters, 180: 165-171.
43 Povey AC, Guppy MJ, Hall CN, Jackson PE, Badawi AF, Cooper DP, O'Connor PJ, Margison GP. (2001) Host determinants of DNA alkylation and DNA repair activity in human colorectal tissue: O6-methylguanine levels are associated with GST-T1 genotype and O6-alkylguanine-DNA alkyltransferase activity with CYP2D6 genotype. Mutat. Res., 495: 103115.
44 Cherry NM, Mackness M, Durrington P, Povey AC, Dippnall WM, Smith AE, Mackness B. (2002) Paraoxonase (PON1) polymorphisms in farmers attributing ill-health to sheep dip. Lancet , 359: 763-764
29
45 Mackness B, Durrington P, Povey AC, Thomson S, Middleton S, Dippnall M, Mackness M, Smith AR, Cherry NM. (2003) Paraoxonase and susceptibility to organophosphorus poisoning in farmers dipping sheep. Pharmacogenetics, 13: 81-88.
46 Shih DM, Gu L, Xia Y-R, Navab M, Li W-F, Hama S, Castellani LW, Furlong CE, Costa LG, Fogelman AM, Lusis AJ. (1998) Mice lacking serume paroxonase are susceptible to organophosphate toxicity and atherosclerosis. Nature, 394: 284-287.
47 Li W-F, Costa LG, Richter RJ, Hagen T, Shih DM, Tward A, Lusis AJ, Furlong CE. (2000) Catalytic efficiency determines the in vivo efficacy of PON1 for detoxifying organophosphorous compounds. Pharmacogenetics, 10: 767-779.
48 Mackness B, Durrington PN, Boulton AJM, Hine D, Mackness MI. (2002) Serum paraoxonase activity in patients with type 1 diabetes compared to healthy controls. Eur. J. Clin. Invest., 32: 259-264.
30
Appendix 1 Advertisement used to publicise study
31
Appendix 2 Initial letter to subjects who wrote in following the publicity
«Salutation» «First name» «Surname» «Address_1» «Address_2» «Address_3» «Address_4» «Address_5» «Address_6» «Address_7»
August 1999
Dear «Salutation» «Surname»
Thank you for contacting us about the SCOPE study. I enclose an information sheet that should answer some of your questions about who we are and what we are doing. If you feel you might be willing to take part we would like you to fill in the brief formenclosed with this letter and send it back in the envelope provided. We will then contact you to let you know when we plan to be in your area.
If you do take part in the study the nurse will visit you at home, at a time agreed with you in advance. She will ask you about your health and your work since leaving school. She will also take a blood sample. One of the doctors may later need to speak to your general practitioner about your health in the past.
All the information you give to the study will be completely confidential. We will give you the result of your own tests but these will not be passed to anyone else without your permission.
I do hope you will consider taking part and send back the form straight away.
Yours sincerely
Professor Nicola Cherry, MD, PhD, FFOM Principal investigator, SCOPE Study
32
Appendix 3 Information sheet
S C O P E
Susceptibility to Chronic OrganoPhosphate Exposure
Information Sheet
Background
A substantial number of sheep farmers from various parts of the country complain of chronic ill health which they relate to the use of organophosphate sheep dip.
Epidemiological studies conducted so far have not determined why some people are at particular risk of ill health following exposure.
Why another study?
SCOPE will investigate whether some people have genetic factors that make them more susceptible to chronic effects of organophosphates. No systematic study of sheep dipping has investigated this possibility.
How will the study be conducted?
People who have developed illness will be asked to volunteer. Each will be asked to nominate three people who they know have had similar exposure over the years to themselves but have not developed an illness.
What information is needed?
Everyone in the study will be visited at home by an experienced nurse and asked to complete questionnaires on current health, medical history and work exposure. They will be asked to give consent for us to seek information about them from their doctor. In addition, blood samples will be taken for laboratory analysis.
What tests will be done on the blood samples?
Each blood sample will be tested to see if it contains more or less of certain proteins (called enzymes) which help breakdown chemicals in sheep dip. From your blood sample we will be able to tell how well you can breakdown such chemicals. We may also look for other occupational chemicals, such as lead, that might affect your health.
What can this tell us?
33
If people with ill health have less of the specific enzyme, this will suggest that the illness may come from sheep dip.
Why should I participate?
Your participation in this study is entirely voluntary. As in many medical research studies, there may not be a direct benefit to you at this stage. This research is carried out with the aim of helping to prevent this problem in future. The people who take part may therefore play an important part in future prevention.
Confidentiality
All information will be treated in the strictest confidence. No-one will be identifiable in any report on the study and no-one except your own medical practitioner will be asked for information about you. Only the research team will have access to study information; each member of the team will sign an undertaking to respect confidentiality.
Ethics
This study has been carefully scrutinised and approved by the Ethics Committee of the University of Manchester.
Who is organising the study?
SCOPE is being carried out by doctors and other medical researchers in the Medical School of The University of Manchester.
Who is paying for SCOPE?
The study is funded through the Health and Safety Executive.
WE HOPE THAT YOU WILL HELP US WITH THIS RESEARCH
YOUR INPUT IS VERY IMPORTANT TO US
For information or advice call the free SCOPE Helpline on 0800 028 1941. Our address is SCOPE, Centre for Occupational Health, University of Manchester,
Stopford Building, Oxford Road, Manchester, M13 9PT
34
Appendix 4 Initial questionnaire to enquirers
SCOPE If you are happy for our nurse to contact you please check that we have written your name and address correctly and amend or complete the details if necessary.
Name «Salutation» «First_name» «Surname» Mr/Mrs/Ms First name Surname
Postal address (including postcode) «Address_1» «Address_2» «Address_3» «Address_4» «Address_5» «Address_6»
Please write here telephone numbers where we may contact you.
Day ....................................................... Area code number
Evening ............. .......................................... Area code number
What is your date of birth? ....... day ........ month ........ year
What sort of illness do you have now?
Please write below the three symptoms that trouble you most
1) ...............................................................................................
2) ....................................................................................................
3) ......................................................................................................
When were you last involved in dipping sheep?
........ month ........ year
As part of the study we will ask you to give us the name and address of three people of about your age who are not related to you and who have been dipping sheep but have not developed ill health.
Do you think you will be able to think of a number of people who would fit this? Yes No Many thanks for completing this form. Please send it back in the envelope provided. We will be in touch during the next few days.
35

Appendix 5 Follow up letter to cases
Date
[pt name and address]
Dear [pt name]
Following our recent telephone conversation, please find enclosed two questionnaires which form part of the SCOPE project. The questionnaire in blue is concerned with general health in the last month and the questionnaire in yellow is concerned with exposure to sheep dip, lifestyle factors and health. If you have any difficulties in filling out the questionnaires please contact me on 0800 028 1941.
I will phone you in about a week to arrange a convenient time to visit (within 2 weeks if possible). I would be grateful if you could complete the questionnaire before my visit. Please do not send them back as I will collect the forms when I come to interview you and also collect the blood sample.
We would like to thank you for agreeing to participate in this important phase of the SCOPE project.
Please let me reassure you that confidentiality will be maintained and should you have any questions please telephone me on 0800 028 1941.
Yours sincerely
Research Nurse
Appendix 6 Initial letter to potential referents
36

Date
[pt name and address]
Dear [pt name]
Following our recent telephone conversation, please find enclosed two questionnaires which form part of the SCOPE project. The questionnaire in blue is concerned with general health in the last month and the questionnaire in yellow is concerned with exposure to sheep dip, lifestyle factors and health. If you have any difficulties in filling out the questionnaires please contact me on 0800 028 1941.
I will phone you in about a week to arrange a convenient time to visit (within 2 weeks if possible). I would be grateful if you could complete the questionnaire before my visit. Please do not send them back as I will collect the forms when I come to interview you and also collect the blood sample.
We would like to thank you for agreeing to participate in this important phase of the SCOPE project. I enclose a copy of the information sheet in case you have not seen one.
Please let me reassure you that confidentiality will be maintained and should you have any questions please telephone me on 0800 028 1941.
Yours sincerely
Research Nurse
37
I
Appendix 7 Consent form
SCOPE
CONSENT TO TAKE PART IN A RESEARCH STUDY
of
confirm that I:
• have read and understood the information leaflet.
• agree to take part in the study.
• understand that I can stop participating in the study at any time; this action will not affect my future care.
• give permission for SCOPE to ask my medical practitioner to provide information about me for the purposes of the study.
• give permission for samples to be stored for later chemical analysis.
Signature
Date
38
Appendix 8 – Work and Lifestyle questionnaire
SCOPE Susceptibility to Chronic OrganoPhosphate Exposure
WORK AND LIFESTYLE QUESTIONNAIRE
This study, funded by the Health and Safety Executive, has been set up to investigate whether some people are more susceptible than others to chronic effects of organophosphates. Everyone helping with this study is being asked to fill in a questionnaire like this one. Please work through the questionnaire filling in each question that applies to you. The study nurse will help with any queries, or you can telephone the freephone on 0800 028 1941 if you need help.
All the information you give will be completely confidential to the study team. It will not be passed on to your GP unless you ask us to do so. You will not be identified in any publication about the study and your name and address will not be entered on the study's data base.
Name: .............................................................................................................................
Address: ..............................................................................................................
........................................................................................................................
........................................................................................................................
Postcode: .............................................................................................................................
1. What is your date of birth?
................... day ........................ month ........................... year Now please turn over and complete the questions about your work and your health.
39
Now we would like to ask about your work 2. Please write below the type of work you have done in every job you have held for more than one month since leaving school or college, starting with the first job you did. Please number the jobs in the left hand column (i.e. the first job is 1). Continue on a separate sheet if necessary.
40
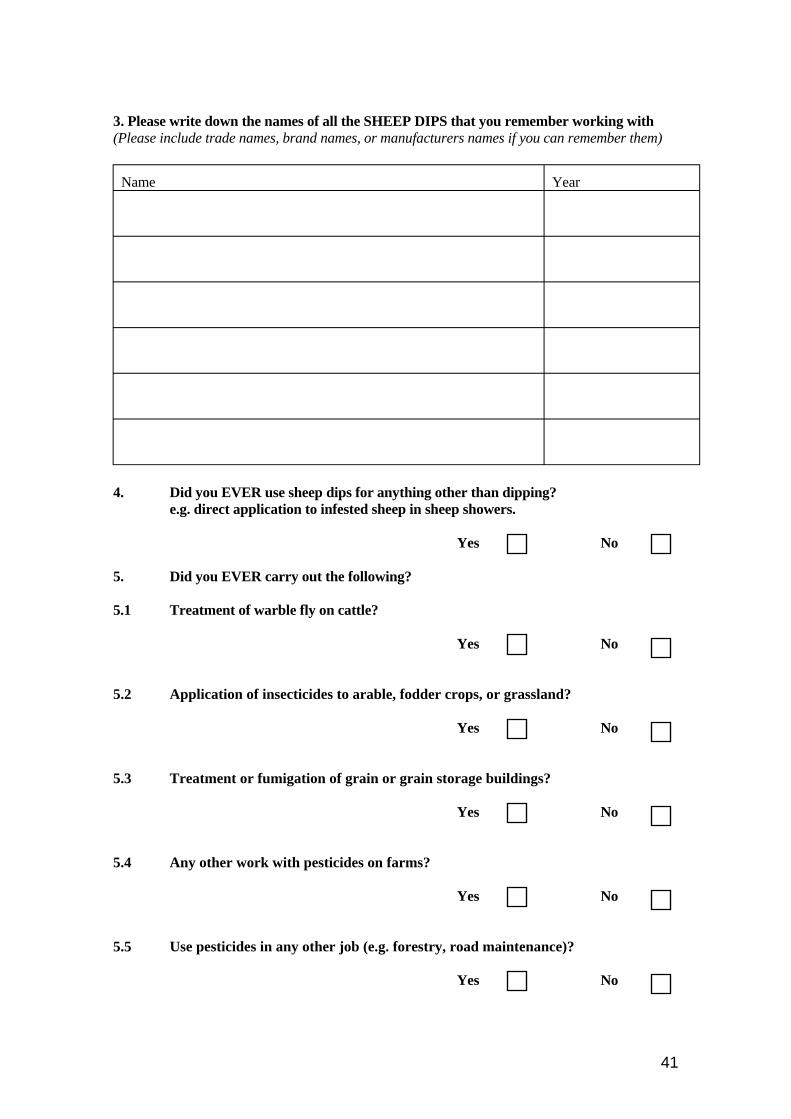
3. Please write down the names of all the SHEEP DIPS that you remember working with (Please include trade names, brand names, or manufacturers names if you can remember them)
Name Year
4. Did you EVER use sheep dips for anything other than dipping? e.g. direct application to infested sheep in sheep showers.
Yes No
5. Did you EVER carry out the following?
5.1 Treatment of warble fly on cattle?
Yes No
5.2 Application of insecticides to arable, fodder crops, or grassland?
Yes No
5.3 Treatment or fumigation of grain or grain storage buildings?
Yes No
5.4 Any other work with pesticides on farms?
Yes No
5.5 Use pesticides in any other job (e.g. forestry, road maintenance)?
Yes No
41
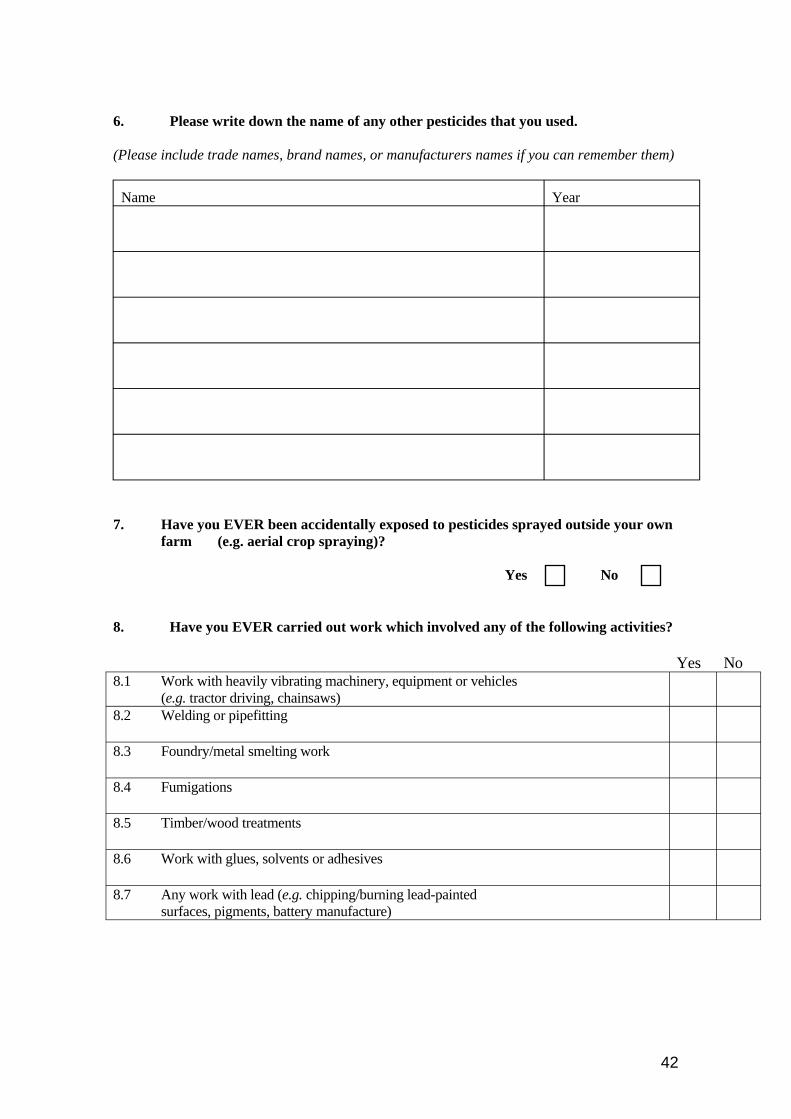
6. Please write down the name of any other pesticides that you used.
(Please include trade names, brand names, or manufacturers names if you can remember them)
Name Year
7. Have you EVER been accidentally exposed to pesticides sprayed outside your own farm (e.g. aerial crop spraying)?
Yes No
8. Have you EVER carried out work which involved any of the following activities?
Yes No 8.1 Work with heavily vibrating machinery, equipment or vehicles
(e.g. tractor driving, chainsaws) 8.2 Welding or pipefitting
8.3 Foundry/metal smelting work
8.4 Fumigations
8.5 Timber/wood treatments
8.6 Work with glues, solvents or adhesives
8.7 Any work with lead (e.g. chipping/burning lead-painted surfaces, pigments, battery manufacture)
42
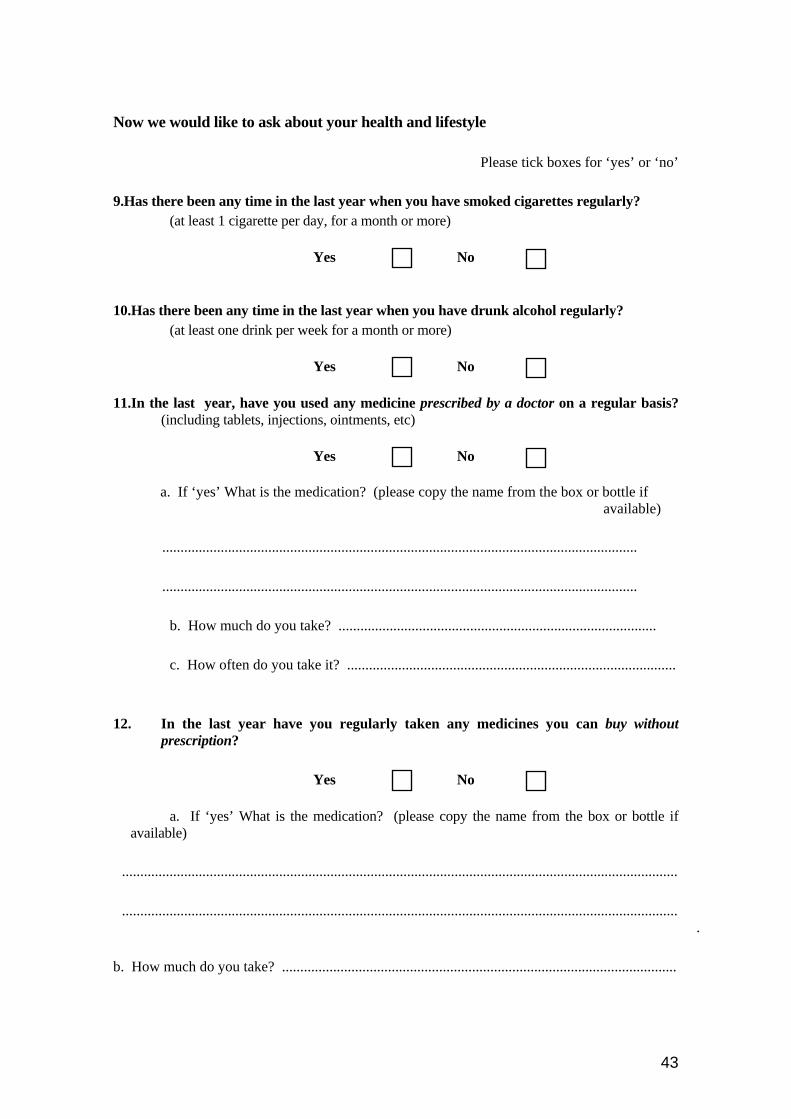
Now we would like to ask about your health and lifestyle
Please tick boxes for ‘yes’ or ‘no’
9.Has there been any time in the last year when you have smoked cigarettes regularly? (at least 1 cigarette per day, for a month or more)
Yes No
10.Has there been any time in the last year when you have drunk alcohol regularly? (at least one drink per week for a month or more)
Yes No
11.In the last year, have you used any medicine prescribed by a doctor on a regular basis? (including tablets, injections, ointments, etc)
Yes No
a. If ‘yes’ What is the medication? (please copy the name from the box or bottle if available)
..................................................................................................................................
..................................................................................................................................
b. How much do you take? .......................................................................................
c. How often do you take it? ..........................................................................................
12. In the last year have you regularly taken any medicines you can buy without prescription?
Yes No
a. If ‘yes’ What is the medication? (please copy the name from the box or bottle if available)
........................................................................................................................................................
........................................................................................................................................................ .
b. How much do you take? ............................................................................................................
43
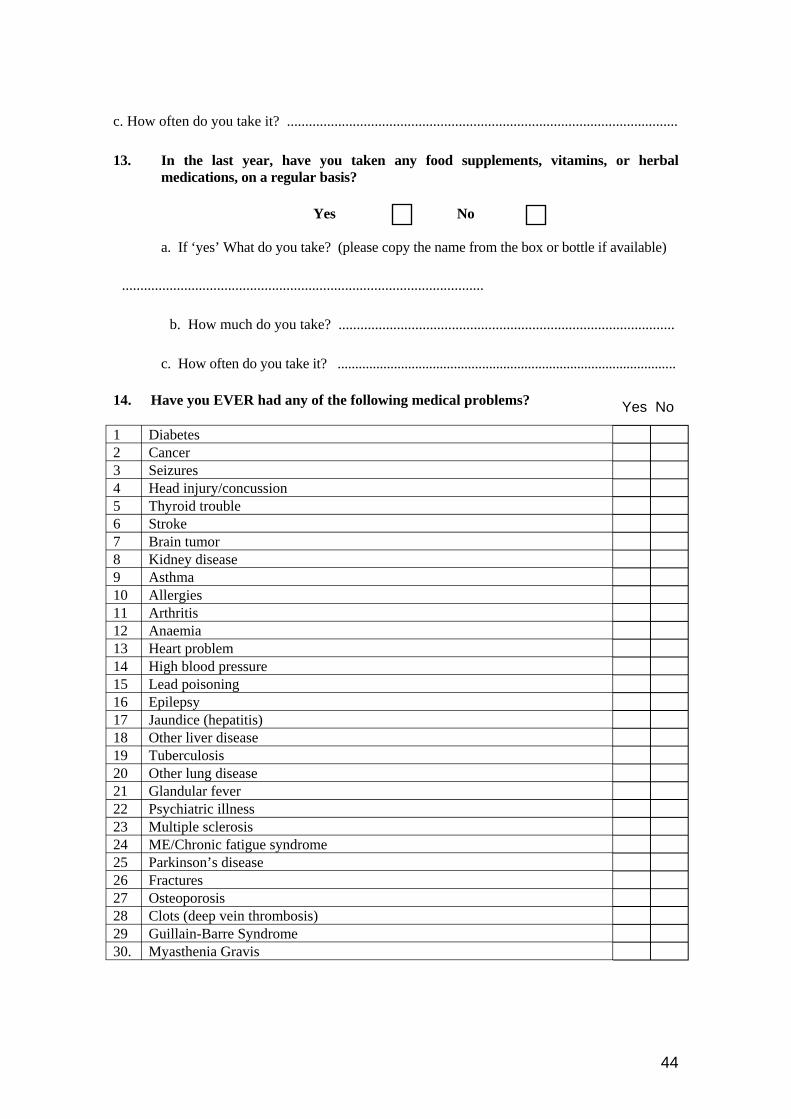
c. How often do you take it? ...........................................................................................................
13. In the last year, have you taken any food supplements, vitamins, or herbal medications, on a regular basis?
Yes No
a. If ‘yes’ What do you take? (please copy the name from the box or bottle if available)
...................................................................................................
b. How much do you take? ............................................................................................
c. How often do you take it? ................................................................................................
14. Have you EVER had any of the following medical problems? Yes No
1 Diabetes 2 Cancer 3 Seizures 4 Head injury/concussion 5 Thyroid trouble 6 Stroke 7 Brain tumor 8 Kidney disease 9 Asthma 10 Allergies 11 Arthritis 12 Anaemia 13 Heart problem 14 High blood pressure 15 Lead poisoning 16 Epilepsy 17 Jaundice (hepatitis) 18 Other liver disease 19 Tuberculosis 20 Other lung disease 21 Glandular fever 22 Psychiatric illness 23 Multiple sclerosis 24 ME/Chronic fatigue syndrome 25 Parkinson’s disease 26 Fractures 27 Osteoporosis 28 Clots (deep vein thrombosis) 29 Guillain-Barre Syndrome 30. Myasthenia Gravis
44
15. Have you EVER been admitted to hospital?
Yes No
If yes, please write below your age, why you were admitted and, if possible, the name of the hospital.
Age (or date) Town/City
Why were you admitted? Name of the hospital
16. Have you EVER been sent to see a hospital specialist as an outpatient?
Yes No
If yes, please write below your age, why you were sent to see the specialist and the name of the hospital or clinic
Age (or date) (i.e. what was wrong with you?) Town/City Why did you go? Name of the hospital or clinic
45
17. Do you now have, or have you had in the past, any condition that has caused you to visit your general practitioners repeatedly over a period of months or years?
Yes No
If yes, please write below the age at which you first consulted your GP, for this condition, how long this lasted, and what was thought to be wrong.
Age at which you first consulted? problem?
How long did this on? (months/years)
What was thought to be the
18. Have you EVER taken medication for longer than one month at a stretch?
Yes No
If yes, please write below the type of medication, what you took it for, and who prescribed it.
Type of medication (name if possible)
What condition did you take if for?
How old were you when you started taking it?
How long did you take it for?
Who prescribed it? (GP, specialist?)
46
_____________________________________________________________________________
____________________________________________________________________________
_____________________________________________________________________________
19. Have you EVER suffered from “dipper’s flu”?
Yes No
20. Do you think you have EVER had an infectious illness that you caught through your work with animals?
Yes No
If yes, please write below what the infection was?
Many thanks for filling in this questionnaire. The research nurse will collect it and answer any of your questions. Please put it in the envelope provided and keep it in a safe place until he calls.
47
i
SCOPE
N DOB No.
Appendix 9 Health Quest onnaire
Susceptibility to Chronic OrganoPhosphate Exposure
ame
HEALTH QUESTIONNAIRE
This questionnaire asks about your health in the last month. We need to find out the pattern of health of everyone taking part in SCOPE, to see which symptoms are part of the general wear and tear of farming life and which may be due to sheep dips. Please fill the questionnaire in carefully, following the example below, and putting a cross on every line.
On the next 9 pages you will find a list of symptoms that people of your age complain about from time to time. We want you to think about your health in the PAST MONTH and tell us if you have been troubled or not by each of these symptoms. To make it easy for you to reply, all we ask is that you put a cross through each line between or against the markers (I), to show how much you have been troubled by the symptom.
EXAMPLE
Loss of appetite
Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
Gain in weight
Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
In this example, the person has been seriously troubled by loss of appetite but, as you might expect, not at all by gain in weight.
Please put a cross through each of the lines that follow to indicate how troubled you have been by the symptom during the past month.
REMEMBER - you can put a cross anywhere along the line. Please don’t miss any questions out but put a cross through every line. If you haven’t been troubled, put a cross against ‘Not at all’ as in the “Gain in Weight” example
48
1. During the PAST MONTH have you been troubled by 1 Boils or abscesses ? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
2 Sweating ? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
3 Having wind ? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
4 Getting up at night to pass water ? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
5 Stomach pain ? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
6 Indigestion ? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
7 Hot or cold spells ? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
8 Waking with an attack of shortness of breath ? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
9 Diarrhoea ? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
10 A loss in weight ? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
11 Having a sensation of sand or grit in your eyes? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
12 Bleeding gums? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
13 Aching all over your body ? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
14 Fevers? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
49
1. During the PAST MONTH have you been troubled by 15 A fear of going outside in open spaces? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
16 Toothache? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
17 Nosebleeds ? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
18 Fits or convulsions? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
19 Nervous trouble? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
20 Feeling irritated for no particular reason? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
21 Lack of interest in sex? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
22 Difficulty concentrating? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
23 Feeling sleepy for most of the day? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
24 Sinus problems? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
25 Wheezing or whistling in your chest? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
26 Headaches? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
27 Problems doing up buttons on your clothes ? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
28 Pain in your chest? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
50
1. During the PAST MONTH have you been troubled by 29 Poor appetite? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
30 Feeling sick? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
31 Vomiting? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
32 Feeling unhappy and depressed? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
33 Your hands shaking? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
34 Waking up feeling tired and worn out? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
35 Losing sleep due to worry? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
36 Difficulty in standing up from a chair? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
37 Coughing? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
38 Having too little energy to start doing things? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
39 A feeling of heaviness in your chest? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
40 Fainting? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
41 Feeling too weak to complete what you Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely are doing? 42 Losing your balance? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
51
1. During the PAST MONTH have you been troubled by 43 A poor memory? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
44 Itching skin? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
45 Having to make notes to help you Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely remember things?
46 Ringing sounds in your ears? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
47 Painful tingling in your hands or feet? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
48 A dry mouth? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
49 Feeling drunk when you haven’t had Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely much to drink?
50 Loss of sensation in your hands and feet Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
51 Difficulty in lifting down an object from Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely just above your head?
52 A loss of confidence in yourself? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
53 The smell of perfume or aftershave? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
54 Head colds? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
52
1. During the PAST MONTH have you been troubled by 55 Having to go back and check that you have Not at all
done things?
56 Feelings of anger which are difficult to control? Not at all
57 Thinking that you were a worthless person? Not at all
58 Clumsiness? Not at all
59 A sore throat? Not at all
60 Hair loss? Not at all
61 Slurring your words? Not at all
62 Loss of sense of smell? Not at all
63 Nightmares Not at all
64 Ear infections? Not at all
65 Constipation? Not at all
66 Hiccups? Not at all
67 Phlegm or sputum (spit from the chest)? Not at all 68 People telling you that you have a poor memory? Not at all
I--------.------.------.------.------.------.------.------.------.--------I Very Severely
I--------.------.------.------.------.------.------.------.------.--------I Very Severely
I--------.------.------.------.------.------.------.------.------.--------I Very Severely
I--------.------.------.------.------.------.------.------.------.--------I Very Severely
I--------.------.------.------.------.------.------.------.------.--------I Very Severely
I--------.------.------.------.------.------.------.------.------.--------I Very Severely
I--------.------.------.------.------.------.------.------.------.--------I Very Severely
I--------.------.------.------.------.------.------.------.------.--------I Very Severely
I--------.------.------.------.------.------.------.------.------.--------I Very Severely
I--------.------.------.------.------.------.------.------.------.--------I Very Severely
I--------.------.------.------.------.------.------.------.------.--------I Very Severely
I--------.------.------.------.------.------.------.------.------.--------I Very Severely
I--------.------.------.------.------.------.------.------.------.--------I Very Severely I--------.------.------.------.------.------.------.------.------.--------I Very Severely
53
1. During the PAST MONTH have you been troubled by 69 Palpitations (fluttery feelings in the heart)? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
70 Tiredness? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
71 A flare-up of acne? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
72 Feeling stiff? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
73 Chest infections? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
74 Difficulty in grasping the meaning of Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely what you read?
75 Skin rashes? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
76 Cramps or spasms in your muscles? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
77 The smell of paint, petrol or other Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely chemicals?
78 Double vision? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
79 Memory flashbacks? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
80 Shortness of breath when walking with other Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely people of your own age?
81 Feeling unsteady when walking? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
54
1. During the PAST MONTH have you been troubled by 82 Waking up with a tight chest? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
83 Feeling incapable of making decisions about Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely things?
84 Feeling dizzy? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
85 Heartburn? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
86 Difficulty in saying what you want to say? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
87 Sudden changes of mood? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
88 Loud noises or bright lights? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
89 Your eyes watering? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
90 Cold hands or feet? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
91 Tingling under your skin? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
92 Loss of appetite? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
93 Swollen glands? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
94 Feeling bloated? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely 95 Wishing you were dead and away from it all? Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
55
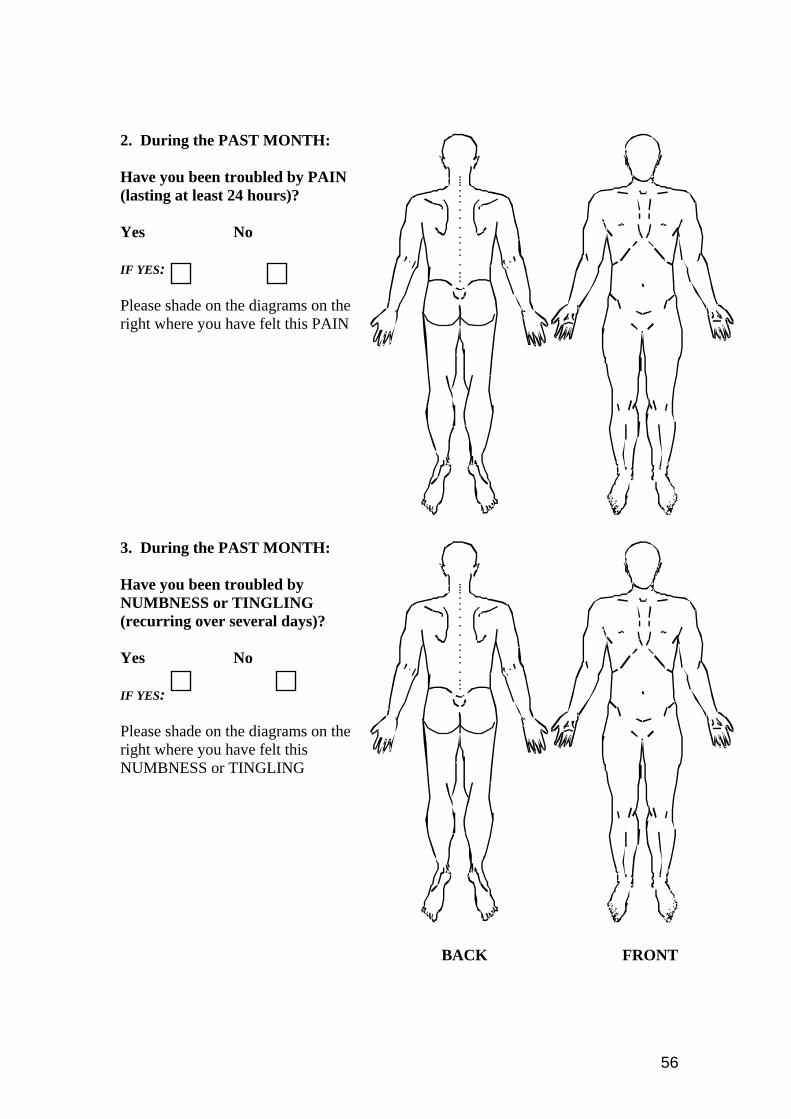
2. During the PAST MONTH:
Have you been troubled by PAIN (lasting at least 24 hours)?
Yes No
IF YES:
Please shade on the diagrams on the right where you have felt this PAIN
3. During the PAST MONTH:
Have you been troubled by NUMBNESS or TINGLING (recurring over several days)?
Yes No
IF YES:
Please shade on the diagrams on the right where you have felt this NUMBNESS or TINGLING
BACK FRONT
56
4. Now THINKING OVERALL about your health during the past month, how much have you been troubled by ill-health?
Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
5. How much do you feel your health now has been affected by using sheep dip?
Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
6. a) During the PAST MONTH have you been bothered by any other health problems?
Not at all I--------.------.------.------.------.------.------.------.------.--------I Very Severely
b) What are these other health problems?
____________________________________________________________________
____________________________________________________________________
____________________________________________________________________
Many thanks for filling in this questionnaire. The research nurse will collect it and answer any of your questions. Please put it in the envelope provided and keep it in a safe place until he calls.
57
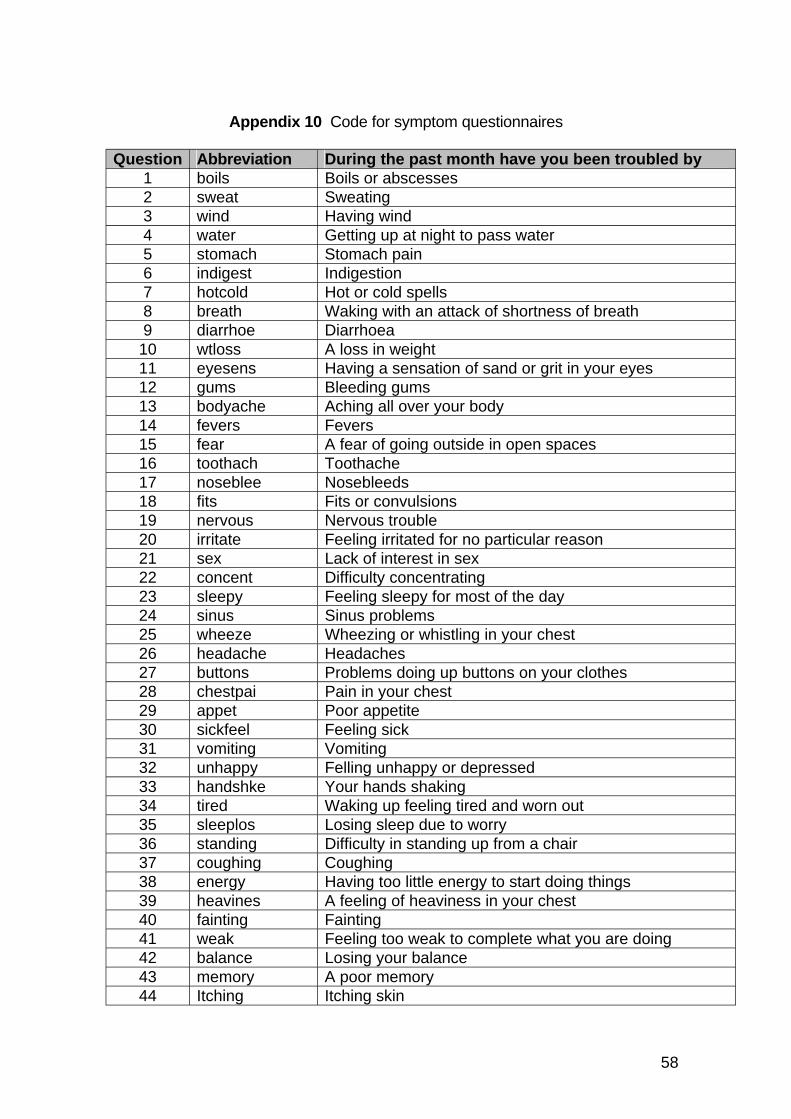
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 34 35 36 37 38 39 40 41 42 43 44
Appendix 10 Code for symptom questionnaires
Question Abbreviation boils sweat wind water stomach indigest hotcold breath diarrhoe wtloss eyesens gums bodyache fevers fear toothach noseblee fits nervous irritate sex concent sleepy sinus wheeze headache buttons chestpai appet sickfeel vomiting unhappy handshke tired sleeplos standing coughing energy heavines fainting weak balance memory Itching
During the past month have you been troubled by Boils or abscesses Sweating Having wind Getting up at night to pass water Stomach pain Indigestion Hot or cold spells Waking with an attack of shortness of breath Diarrhoea A loss in weight Having a sensation of sand or grit in your eyes Bleeding gums Aching all over your body Fevers A fear of going outside in open spaces Toothache Nosebleeds Fits or convulsions Nervous trouble Feeling irritated for no particular reason Lack of interest in sex Difficulty concentrating Feeling sleepy for most of the day Sinus problems Wheezing or whistling in your chest Headaches Problems doing up buttons on your clothes Pain in your chest Poor appetite Feeling sick Vomiting Felling unhappy or depressed Your hands shaking Waking up feeling tired and worn out Losing sleep due to worry Difficulty in standing up from a chair Coughing Having too little energy to start doing things A feeling of heaviness in your chest Fainting Feeling too weak to complete what you are doing Losing your balance A poor memory Itching skin
58
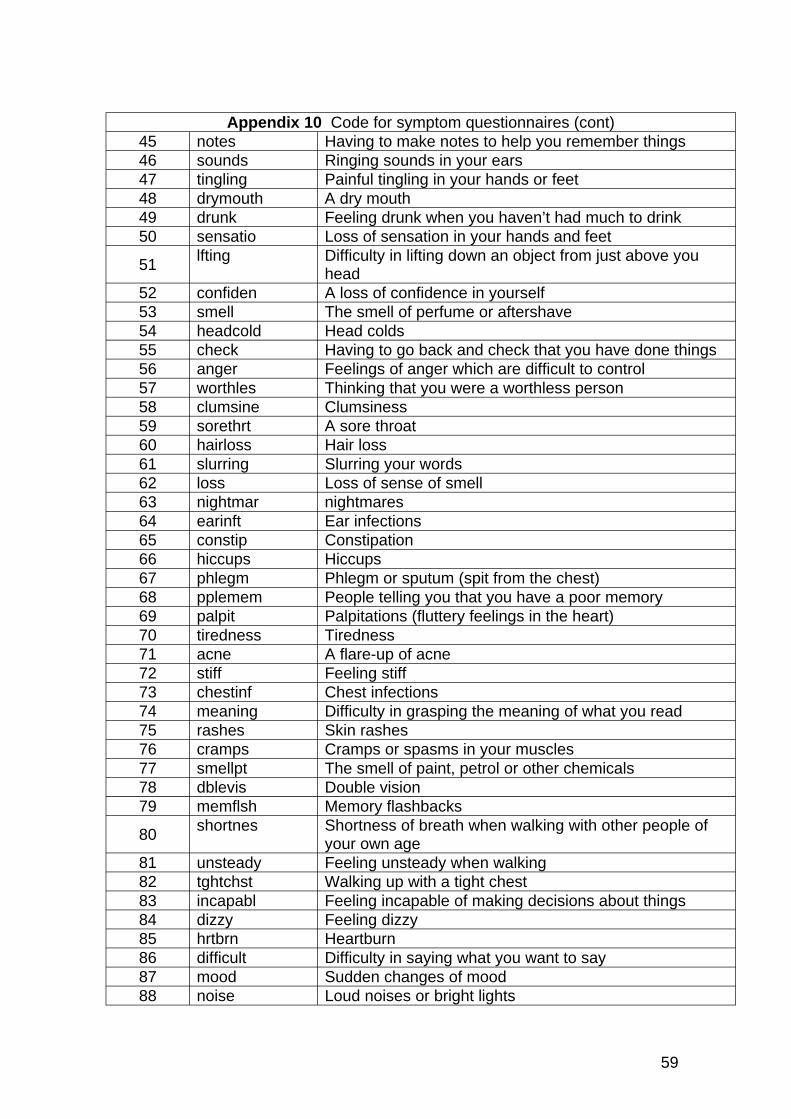
Appendix 10 Code for symptom questionnaires (cont) 45 notes Having to make notes to help you remember things 46 sounds Ringing sounds in your ears 47 tingling Painful tingling in your hands or feet 48 drymouth A dry mouth 49 drunk Feeling drunk when you haven’t had much to drink 50 sensatio Loss of sensation in your hands and feet
51 lfting Difficulty in lifting down an object from just above you head
52 confiden A loss of confidence in yourself 53 smell The smell of perfume or aftershave 54 headcold Head colds 55 check Having to go back and check that you have done things 56 anger Feelings of anger which are difficult to control 57 worthles Thinking that you were a worthless person 58 clumsine Clumsiness 59 sorethrt A sore throat 60 hairloss Hair loss 61 slurring Slurring your words 62 loss Loss of sense of smell 63 nightmar nightmares 64 earinft Ear infections 65 constip Constipation 66 hiccups Hiccups 67 phlegm Phlegm or sputum (spit from the chest) 68 pplemem People telling you that you have a poor memory 69 palpit Palpitations (fluttery feelings in the heart) 70 tiredness Tiredness 71 acne A flare-up of acne 72 stiff Feeling stiff 73 chestinf Chest infections 74 meaning Difficulty in grasping the meaning of what you read 75 rashes Skin rashes 76 cramps Cramps or spasms in your muscles 77 smellpt The smell of paint, petrol or other chemicals 78 dblevis Double vision 79 memflsh Memory flashbacks
80 shortnes Shortness of breath when walking with other people of your own age
81 unsteady Feeling unsteady when walking 82 tghtchst Walking up with a tight chest 83 incapabl Feeling incapable of making decisions about things 84 dizzy Feeling dizzy 85 hrtbrn Heartburn 86 difficult Difficulty in saying what you want to say 87 mood Sudden changes of mood 88 noise Loud noises or bright lights
59
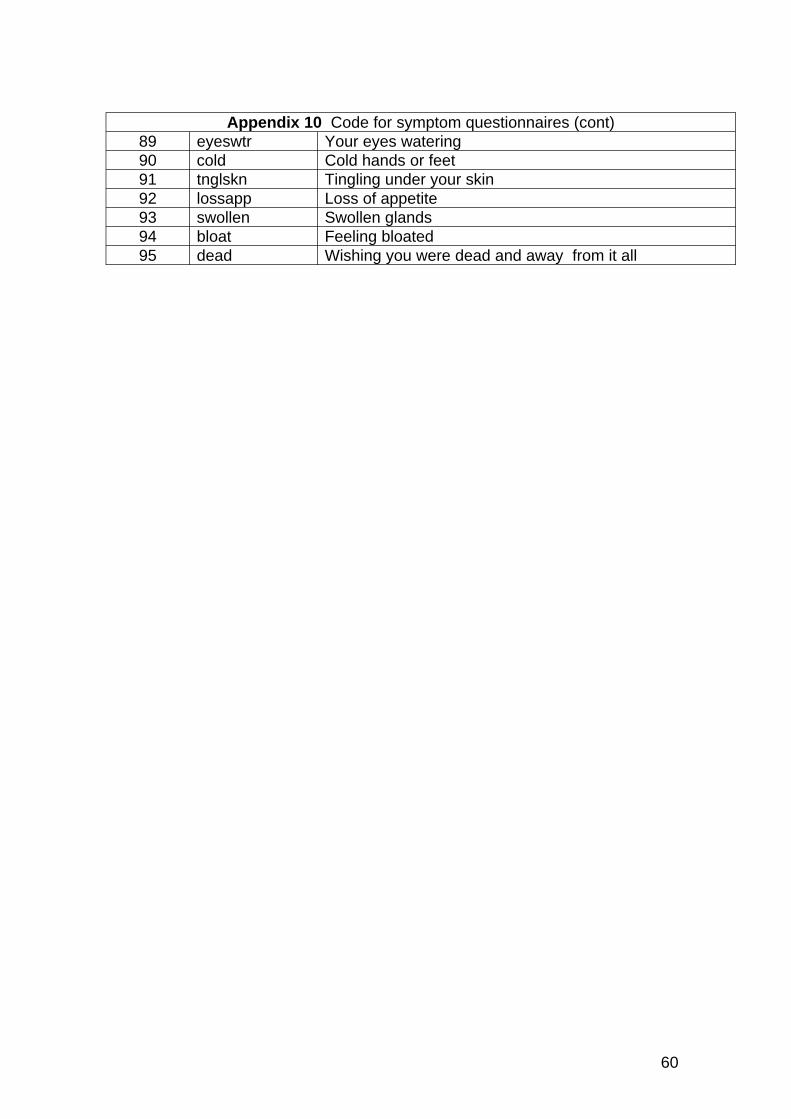
Appendix 10 Code for symptom questionnaires (cont) 89 eyeswtr Your eyes watering 90 cold Cold hands or feet 91 tnglskn Tingling under your skin 92 lossapp Loss of appetite 93 swollen Swollen glands 94 bloat Feeling bloated 95 dead Wishing you were dead and away from it all
60
SCOPE
Name DOB No.
Date Time
Appendix 11- Nurse questionnaire
Susceptibility to Chronic OrganoPhosphate Exposure
NURSE QUESTIONNAIRE
READ INTRODUCTION TO SUBJECT
Complete this questionnaire while checking through both the exposure and medical questionnaires that were sent to the subject .
OBTAIN CONSENT
Name and address of GP ................................................................................................
..................................................................................................................................
..................................................................................................................................
PUT LABEL ON QUESTIONNAIRE
Check name/address on Work and Lifestyle Questionnaire.
Q1 Check fully completed .
Q2.1 Check that all jobs are numbered in date order starting with the first job.
Q2.2 Check that the record is continuous. Ask about gaps greater than 1 month and write in the activity (e.g. armed forces, student,
unemployed, prison, hospital).
Q2.3 Has he/she done any part-time work? Yes No If yes, please write on grid.
Q2.4 Has he/she used sheep dip as a contractor? Yes No If yes, please write in the grid.
Now ask exposure history questionnaire for each job in turn when dipping has occurred starting with the most recent.
Having finished the exposure history questionnaire please go to question 4 on the work and lifestyle questionnaire.
61
Q4 Yes No
If yes, ask If no, go to Q5.1
(A) Please describe in your own words what you did
.....................................................................................................................
.....................................................................................................................
(B) When did you use it? (years) ............................................................
(C) How often did you do this? ...............................................................
(D) What did you use? ............................................................................
Q5.1 Yes No
If yes, ask If no, go to Q5.2
(A) When did you use it? (years) ............................................................
(B) How often did you do this? ...............................................................
(C) What did you use? ............................................................................
(D) Please describe in your own words what you did
.....................................................................................................................
.....................................................................................................................
Q5.2 Yes No
If yes, ask If no go to Q5.3
(A) When did you use it? (years) ...........................................................
(B) How often did you do this? ...............................................................
(C) What did you use? ...........................................................................
(D) Please describe in your own words what you did .....................................................................................................................
.....................................................................................................................
62
Q5.3 Yes No
If yes, ask If no, go to Q5.4
(A) When did you use it? (years) ............................................................
(B) How often did you do this? ..............................................................
(C) What did you use? ............................................................................
(D) Please describe in your own words what you did
.....................................................................................................................
.....................................................................................................................
Q5.4 Yes No
If yes, ask If no, go to Q5.5
(A) When did you use it? (years) ............................................................
(B) How often did you do this? ...............................................................
(C) What did you use? ..........................................................………….
(D) Please describe in your own words what you did
.....................................................................................................................
.....................................................................................................................
Q5.5 Yes No
If yes, ask If no, go to Q6
(A) When did you use it? (years) ............................................................
(B) How often did you do this? ...............................................................
(C) What did you use? ...........................................................................
(D) Please describe in your own words what you did
.....................................................................................................................
.....................................................................................................................
63
Q6 If any names are mentioned, ask If none, re-ask the question and if still no go to Q7
(A) When did you use it? (years) ............................................................
(B) How often did you use it? ................................................................
(C) Please describe in your own words what you did
.....................................................................................................................
.....................................................................................................................
Q7 Yes No
If yes, ask If no, go to Q8
(A) When did this happen? .....................................................................
(B) How often did this happen? ..............................................................
(C) Please describe in your own words what happened
.....................................................................................................................
.....................................................................................................................
.....................................................................................................................
64
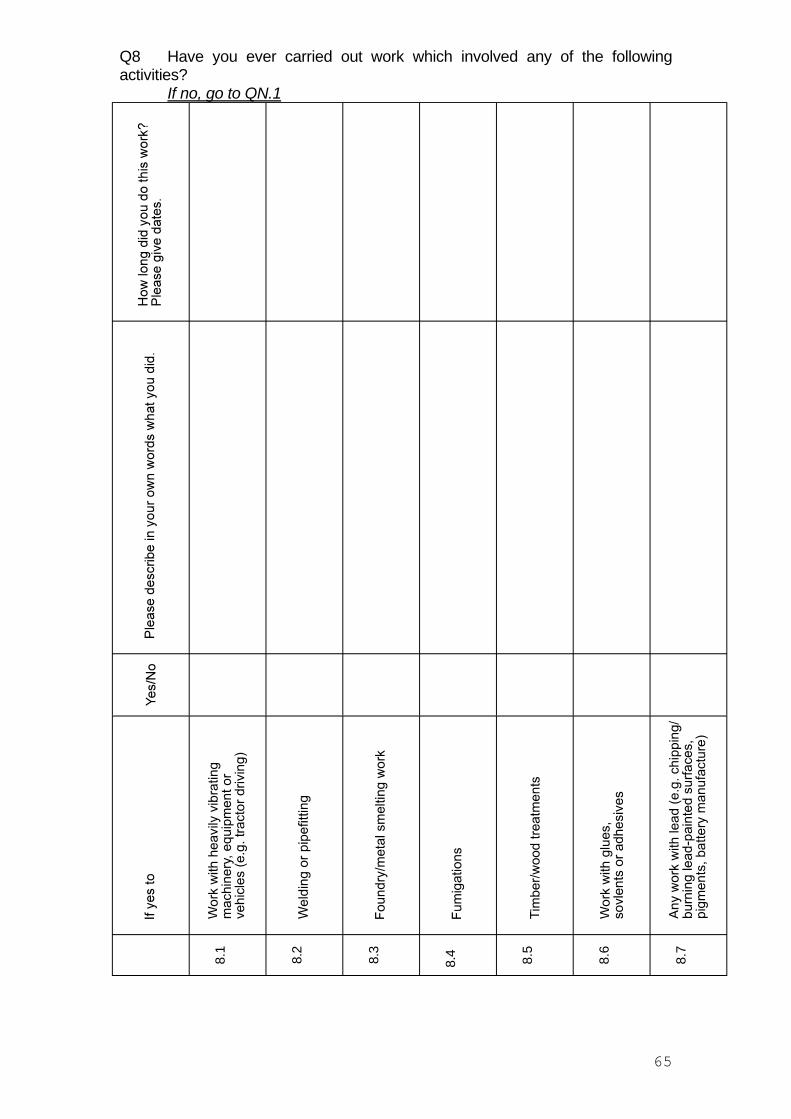
Q8 Have you ever carried out work which involved any of the following activities?
If no, go to QN.1
8.1
8.2
8.3
8.4 8.5
8.6
8.7
65
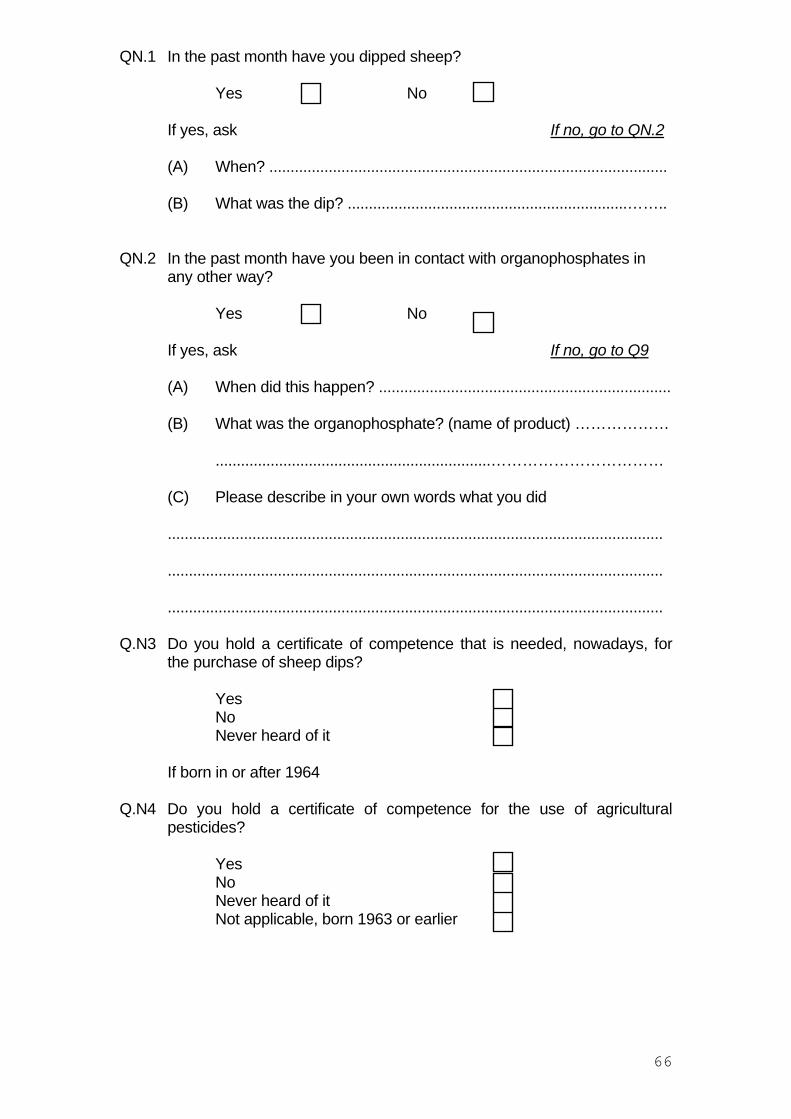
QN.1 In the past month have you dipped sheep?
Yes No
If yes, ask If no, go to QN.2
(A) When? ..............................................................................................
(B) What was the dip? ..................................................................……..
QN.2 In the past month have you been in contact with organophosphates in any other way?
Yes No
If yes, ask If no, go to Q9
(A) When did this happen? .....................................................................
(B) What was the organophosphate? (name of product) ………………
.................................................................……………………………
(C) Please describe in your own words what you did
.....................................................................................................................
.....................................................................................................................
.....................................................................................................................
Q.N3 Do you hold a certificate of competence that is needed, nowadays, for the purchase of sheep dips?
Yes No
Never heard of it
If born in or after 1964
Q.N4 Do you hold a certificate of competence for the use of agricultural pesticides?
Yes No
Never heard of it Not applicable, born 1963 or earlier
66
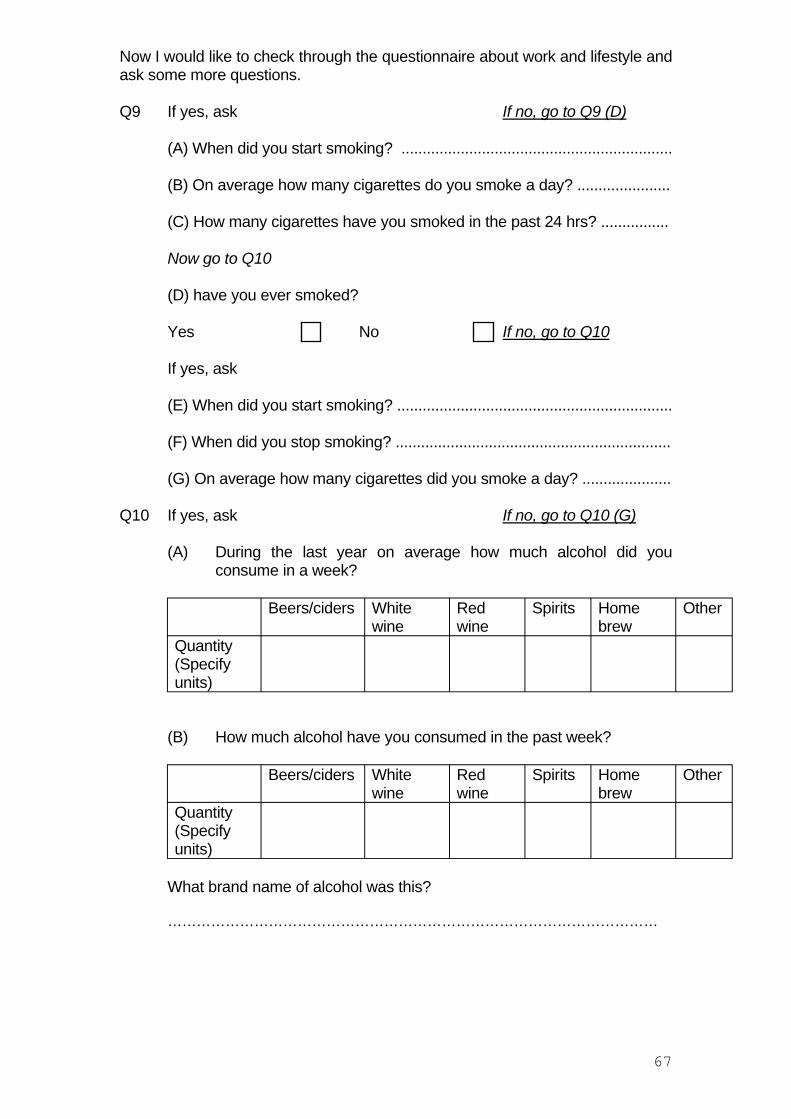
Now I would like to check through the questionnaire about work and lifestyle and ask some more questions.
Q9 If yes, ask If no, go to Q9 (D)
(A) When did you start smoking? ................................................................
(B) On average how many cigarettes do you smoke a day? ......................
(C) How many cigarettes have you smoked in the past 24 hrs? ................
Now go to Q10
(D) have you ever smoked?
Yes No If no, go to Q10
If yes, ask
(E) When did you start smoking? .................................................................
(F) When did you stop smoking? .................................................................
(G) On average how many cigarettes did you smoke a day? .....................
Q10 If yes, ask If no, go to Q10 (G)
(A) During the last year on average how much alcohol did you consume in a week?
Beers/ciders White wine
Red wine
Spirits Home brew
Other
Quantity (Specify units)
(B) How much alcohol have you consumed in the past week?
Beers/ciders White wine
Red wine
Spirits Home brew
Other
Quantity (Specify units)
What brand name of alcohol was this?
…………………………………………………………………………………………
67
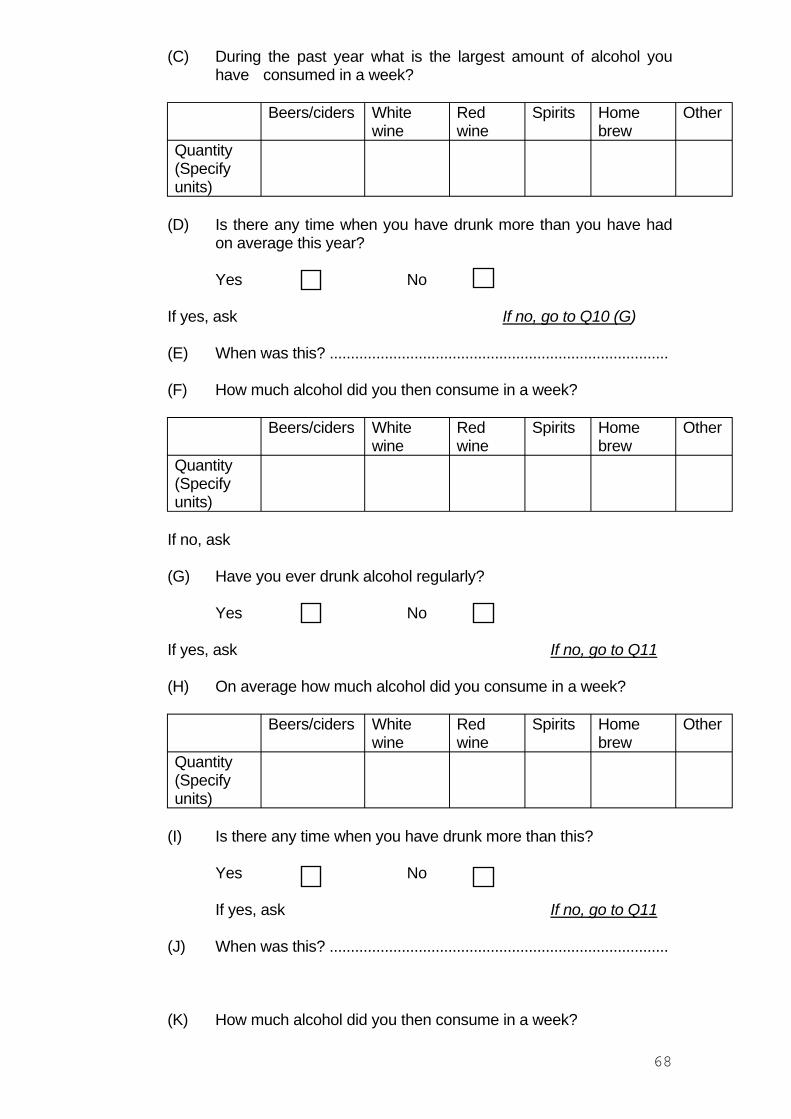
(C) During the past year what is the largest amount of alcohol you have consumed in a week?
Beers/ciders White wine
Red wine
Spirits Home brew
Other
Quantity (Specify units)
(D) Is there any time when you have drunk more than you have had on average this year?
Yes No
If yes, ask If no, go to Q10 (G)
(E) When was this? ................................................................................
(F) How much alcohol did you then consume in a week?
Beers/ciders White wine
Red wine
Spirits Home brew
Other
Quantity (Specify units)
If no, ask
(G) Have you ever drunk alcohol regularly?
Yes No
If yes, ask If no, go to Q11
(H) On average how much alcohol did you consume in a week?
Beers/ciders White wine
Red wine
Spirits Home brew
Other
Quantity (Specify units)
(I) Is there any time when you have drunk more than this?
Yes No
If yes, ask If no, go to Q11
(J) When was this? ................................................................................
(K) How much alcohol did you then consume in a week?
68
Beers/ciders White wine
Red wine
Spirits Home brew
Other
Quantity (Specify units)
Q11 If yes, check that the name of the medication is given, with amounts and frequency.
Ask
(A). What did you take it for? ..................................................................
(B) When did you start taking it? ............................................................
(C) When did you last take it? ................................................................
Q12 If yes, check that the name of the medication is given, with amounts and frequency.
Ask
(A). What did you take it for? ...................................................................
(B) When did you start taking it? ...........................................................
(C) When did you last take it? ...............................................................
Q13 If yes, check that the name of the medication is given, with amounts and frequency.
Ask
(A). What did you take it for? ..................................................................
(B) When did you start taking it? ............................................................
(C) When did you last take it? ...............................................................
69
Now lets talk about your health. I would first like to go through the symptom questionnaire just to ensure that it is fully completed. [Nurse - check for completeness and for ambiguous information].
Q14 You said in your questionnaire you’ve had a problem with ........Can I ask more?
Medical problem Yes/No If yes, was this diagnosed by a doctor? Yes/No
If yes, when was this diagnosed?
Please describe what type of illness you had
1 Diabetes
2 Cancer
3 Seizure
4 Head injury/concussion
5 Thyroid trouble
6 Stroke
7 Brain tumour
8 Kidney disease
9 Asthma
10 Allergies
11 Arthritis
12 Anaemia
13 Heart problem
14 High blood pressure
15 Lead poisoning
16 Epilepsy
17 Jaundice (hepatitis)
18 Other liver disease
19 Tuberculosis
20 Other lung problems
21 Glandular fever
22 Psychiatric illness
23 Multiple sclerosis
24 ME/Chronic fatigue syndrome
25 Parkinson’s disease
26 Fractures
27 Osteoporosis
28 Clots (deep vein thrombosis)
29 Guillain-Barre syndrome
30 Myasthenia Gravis
Q15 Check complete
70
Q16 Check complete
Q17 Check complete
Q18 Check complete
Q19 If yes, ask
(A) In which years did you get dipper’s flu? ...........................................
(B) Had you been handling concentrate on the day (or the day before) you got the symptoms?
.....................................................................................................................
(C) In your own words can you describe the symptoms
.....................................................................................................................
....................................................................................................................
.....................................................................................................................
(D) Did you have fever at this time? Yes No
(E) Was this measured by a thermometer? Yes No
Q20 If yes, ask
(A) When did you have this illness? ......................................................
(B) In your own words can you describe the symptoms
.....................................................................................................................
.....................................................................................................................
71
Now I would like to take your blood sample.
Interviewer: please check whether initial refusers are now able to produce contacts.
Yes No
If yes, please provide details of contacts (name address, phone number)
1. .......................................................................................................................
.......................................................................................................................
.......................................................................................................................
2. ......................................................................................................................
.......................................................................................................................
.......................................................................................................................
3. .......................................................................................................................
.......................................................................................................................
.......................................................................................................................
If no, why?
Interviewer: please check one or more columns - do not read out answers
Yes No
(1) You do not want people to know you are ill?
(2) You no longer have contact with sheep farmers?
(3) Everyone you know who uses sheep dip is ill?
(4) Other reason? (please state)
.....................................................................................................................
72
Finally,
Contact number: ...............................................................................................................
(A) If one of the research scientists needs to ask more about your exposures at work can they contact you directly
Yes No
(B) If necessary for the research can we see you again?
Yes No
(C) Do you have any sheep dip still on site?
Yes No
(D) If yes, can we take a photograph of the container?
Yes No
(E) If one of our researchers would like to take a sample of it would it be possible to come back?
Yes No
(F) Have you taken part in any other similar study?
Yes No
If yes, which study was this?
.....................................................................................................................
(G) Are you a member of an OP Support Group?
Yes No
If yes, which group is this?
.....................................................................................................................
The results of the study will be published in due course. Would you like to receive a summary of the results?
Yes No
Thank you very much for your time and patience.
Date Time
73
Appendix 12 Sheep dipping history questionnaire
Individual’s name and code number…......
2.1 JOB QUESTIONNAIRE Job Sequence number…........
2.1a For each year of this job, please answer the following questions:-
Year
…...
..in
this
yea
r…...
......
.
How
man
y sh
eep
and
la
mbs
did
yo
uno
rmal
ly
dip
in a
ny o
ne
day?
Wha
t was
the
grea
test
num
ber
of s
heep
and
la
mbs
that
you
di
pped
in
any
one
day?
How
man
y da
ys d
id
you
dip
shee
p (o
r la
mbs
)du
ring
the
year
?
Wha
t was
the
grea
test
num
ber o
f da
ys in
a ro
w
that
you
di
pped
she
ep
(or l
ambs
)?
AD
id y
ou
suffe
r fro
m
‘Dip
pers
Fl
u’ ?
YES
/ NO
BD
id y
ou fe
el a
ny
othe
r ill
heal
th
effe
cts
follo
win
g sh
eep
dipp
ing
YES
/ NO
If YE
S to
eith
er A
or B
, w
hat
wer
e yo
ur s
ympt
oms?
74
INTERVIEWER : Please confirm the details of all the sheep dip chemicals the subject remembers using
(Please include trade names, brand names, or manufacturers names if he can remember them) ( use Work and Lifestyle Questionnaire Q3 as a starting point of years covered by this job)
Name given by subject Year(s) used
If subject cannot remember the name(s) of the pesticide s/he used...
USE SHOW CARD #1, ASK...
2.1b Do you think it was one of these common dips?
No Yes Don't know
If 'yes', write in above the name and years when used. If 'don't know', ASK...
2.1c Do you think it was it an O-P dip? No Yes Don't know
If 'yes', ASK...
2.1d Do you think it was based on "Diazinon" , or was it some other type of pesticide?
Diazinon Other Don't know
If subject still cannot remember the pesticide(s) used, ASK...
75
______________________________________________________________________
______________________________________________________________________
2.2e Is there anybody else we could contact who might remember the pesticide? ( e.g. farm manager, farm labourer, VET, supplier, relative etc.- include contact details if applicable)
2.2 SHEEP DIPPING AREA
The next set of questions are about where you carried out sheep dipping in this job.
2.2a Which type(s) of dipping bath did you use?
Yes / No Years when used 1 Straight swim 2 Circular 3 Other (specify)
........................................................................................................................................................
........................................................................................................................................................
2.2b Where were the dipping bath(s) located? Yes / No Years when used
1 Outside (in the open air) 2 Within a building 3 Within a mobile trailer 4 Covered area (roofed but open sides) 5 Other (specify)
........................................................................................................................................................
........................................................................................................................................................
2.2c How did the sheep enter the dip?
Yes / No 1 Sheep walked in 2 Sheep dropped in (tilt / slide mechanism) 3 Manually thrown in (by hand)
Years when applicable (angled ramp / slope)
2.2d How many sheep were normally in the dip bath at the same time?
Yes / No 1 ime
Years when applicable One sheep at a t
76
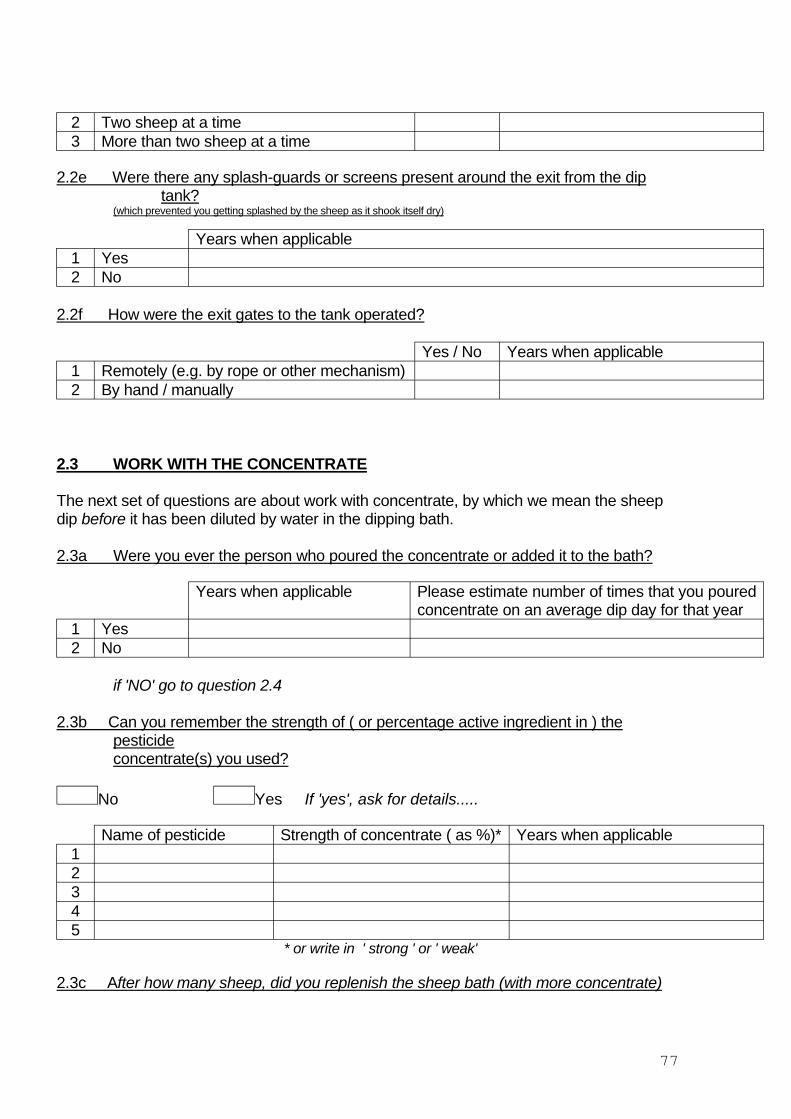
2 Two sheep at a time 3 More than two sheep at a time
2.2e Were there any splash-guards or screens present around the exit from the dip tank?
(which prevented you getting splashed by the sheep as it shook itself dry)
Years when applicable 1 Yes 2 No
2.2f How were the exit gates to the tank operated?
Yes / No 1 2 By hand / manually
Years when applicable Remotely (e.g. by rope or other mechanism)
2.3 WORK WITH THE CONCENTRATE
The next set of questions are about work with concentrate, by which we mean the sheep dip before it has been diluted by water in the dipping bath.
2.3a Were you ever the person who poured the concentrate or added it to the bath?
Years when applicable Please estimate number of times that you poured concentrate on an average dip day for that year
1 Yes 2 No
if 'NO' go to question 2.4
2.3b Can you remember the strength of ( or percentage active ingredient in ) the pesticide concentrate(s) you used?
No Yes If 'yes', ask for details.....
Name of pesticide Strength of concentrate ( as %)* Years when applicable 1 2 3 4 5
* or write in ' strong ' or ' weak'
2.3c After how many sheep, did you replenish the sheep bath (with more concentrate)
77
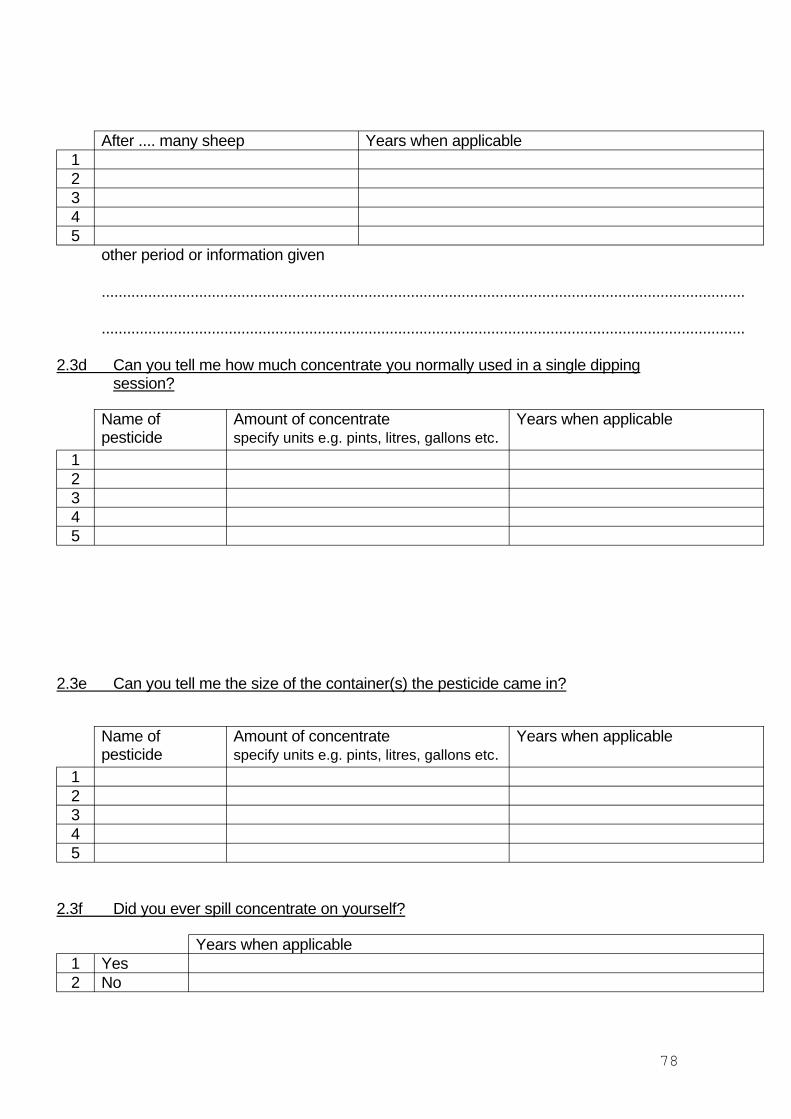
After .... many sheep Years when applicable 1 2 3 4 5
other period or information given
........................................................................................................................................................
........................................................................................................................................................
2.3d Can you tell me how much concentrate you normally used in a single dipping session?
Name of Amount of concentrate Years when applicable pesticide specify units e.g. pints, litres, gallons etc.
1 2 3 4 5
2.3e Can you tell me the size of the container(s) the pesticide came in?
Name of Amount of concentrate Years when applicable pesticide specify units e.g. pints, litres, gallons etc.
1 2 3 4 5
2.3f Did you ever spill concentrate on yourself?
Years when applicable 1 Yes 2 No
78
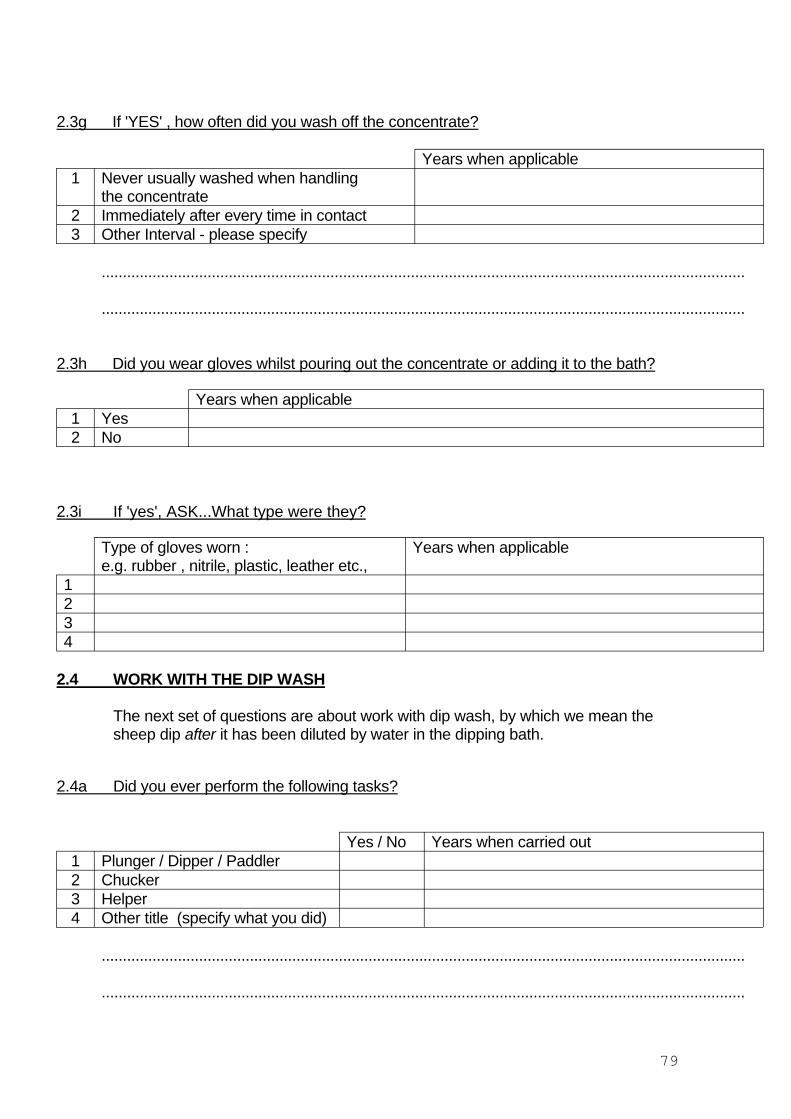
2.3g If 'YES' , how often did you wash off the concentrate?
Years when applicable 1 Never usually washed when handling
the concentrate 2 Immediately after every time in contact 3 Other Interval - please specify
........................................................................................................................................................
........................................................................................................................................................
2.3h Did you wear gloves whilst pouring out the concentrate or adding it to the bath?
Years when applicable 1 Yes 2 No
2.3i If 'yes', ASK...What type were they?
1
Type of gloves worn : e.g. rubber , nitrile, plastic, leather etc.,
Years when applicable
2 3 4
2.4 WORK WITH THE DIP WASH
The next set of questions are about work with dip wash, by which we mean the sheep dip after it has been diluted by water in the dipping bath.
2.4a Did you ever perform the following tasks?
Yes / No Years when carried out 1 Plunger / Dipper / Paddler 2 Chucker 3 Helper 4 Other title (specify what you did)
........................................................................................................................................................
........................................................................................................................................................
79
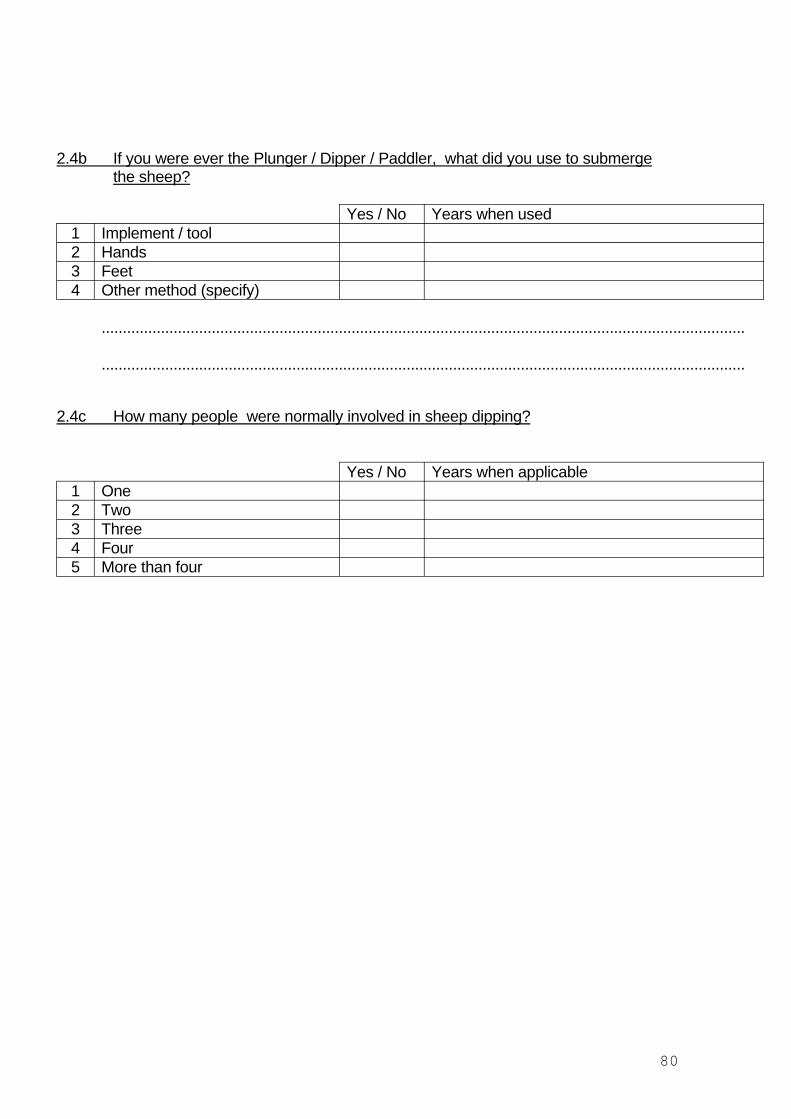
2.4b If you were ever the Plunger / Dipper / Paddler, what did you use to submerge the sheep?
Yes / No 1 Implement / tool 2 Hands 3 Feet 4 Other method (specify)
Years when used
........................................................................................................................................................
........................................................................................................................................................
2.4c How many people were normally involved in sheep dipping?
Yes / No Years when applicable 1 One 2 Two 3 Three 4 Four 5 More than four
80
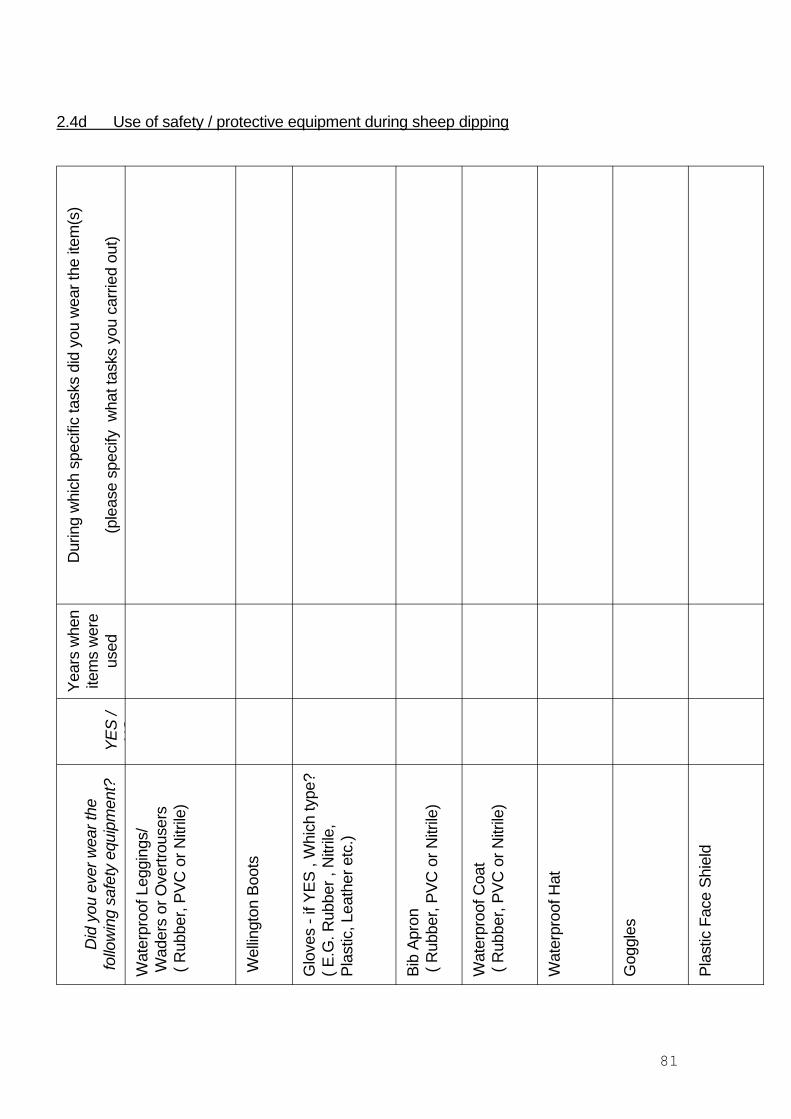
2.4d Use of safety / protective equipment during sheep dipping
Did
you
eve
r wea
r the
fo
llow
ing
safe
ty e
quip
men
t?YE
S /
NO
Year
s w
hen
item
s w
ere
used
Dur
ing
whi
ch s
peci
fic ta
sks
did
you
wea
r the
item
(s)
(ple
ase
spec
ify w
hat t
asks
you
car
ried
out)
Wat
erpr
oof L
eggi
ngs/
Wad
ers
or O
vertr
ouse
rs( R
ubbe
r, PV
C o
r Nitr
ile)
Wel
lingt
on B
oots
Glo
ves
- if Y
ES ,
Whi
ch ty
pe?
( E.G
. Rub
ber ,
Nitr
ile,
Plas
tic, L
eath
er e
tc.)
Bib
Apro
n ( R
ubbe
r, PV
C o
r Nitr
ile)
Wat
erpr
oof C
oat
( Rub
ber,
PVC
or N
itrile
)
Wat
erpr
oof H
at
Gog
gles
Plas
tic F
ace
Shie
ld
81
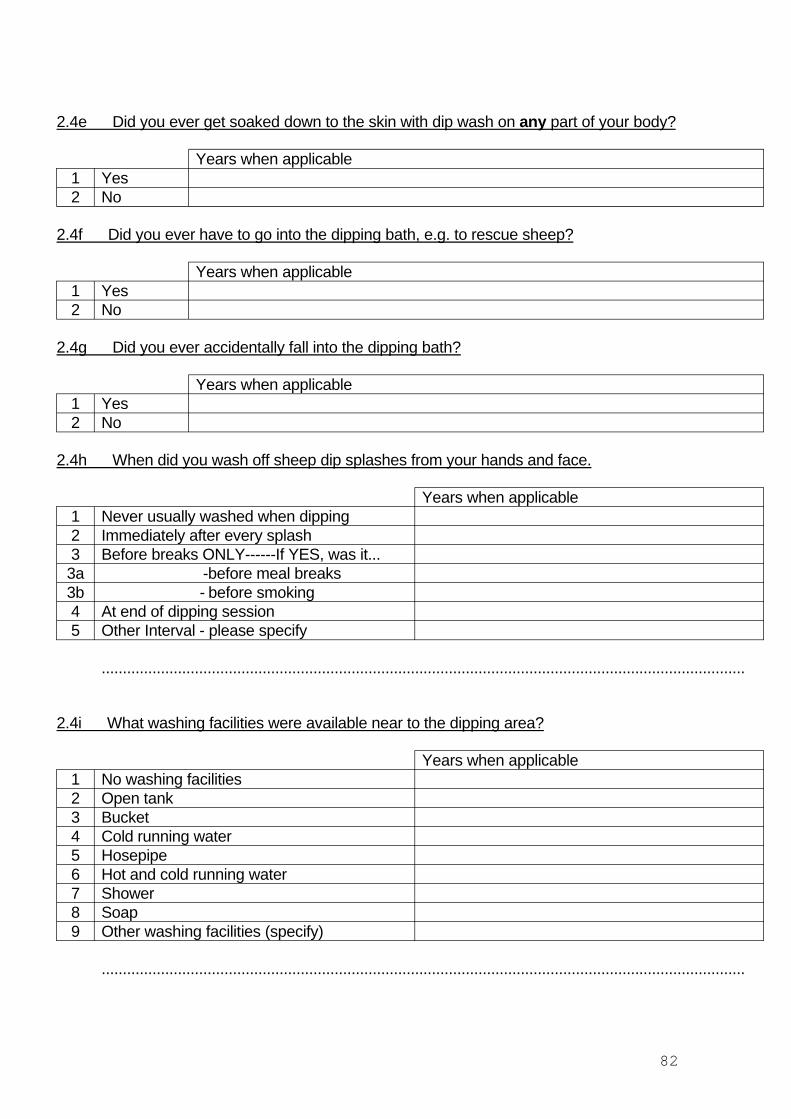
2.4e Did you ever get soaked down to the skin with dip wash on any part of your body?
Years when applicable 1 Yes 2 No
2.4f Did you ever have to go into the dipping bath, e.g. to rescue sheep?
Years when applicable 1 Yes 2 No
2.4g Did you ever accidentally fall into the dipping bath?
Years when applicable 1 Yes 2 No
2.4h When did you wash off sheep dip splashes from your hands and face.
Years when applicable 1 Never usually washed when dipping 2 Immediately after every splash 3 Before breaks ONLY------If YES, was it... 3a -before meal breaks 3b - before smoking 4 At end of dipping session 5 Other Interval - please specify
........................................................................................................................................................
2.4i What washing facilities were available near to the dipping area?
Years when applicable 1 No washing facilities 2 Open tank 3 Bucket 4 Cold running water 5 Hosepipe 6 Hot and cold running water 7 Shower 8 Soap 9 Other washing facilities (specify)
........................................................................................................................................................
82
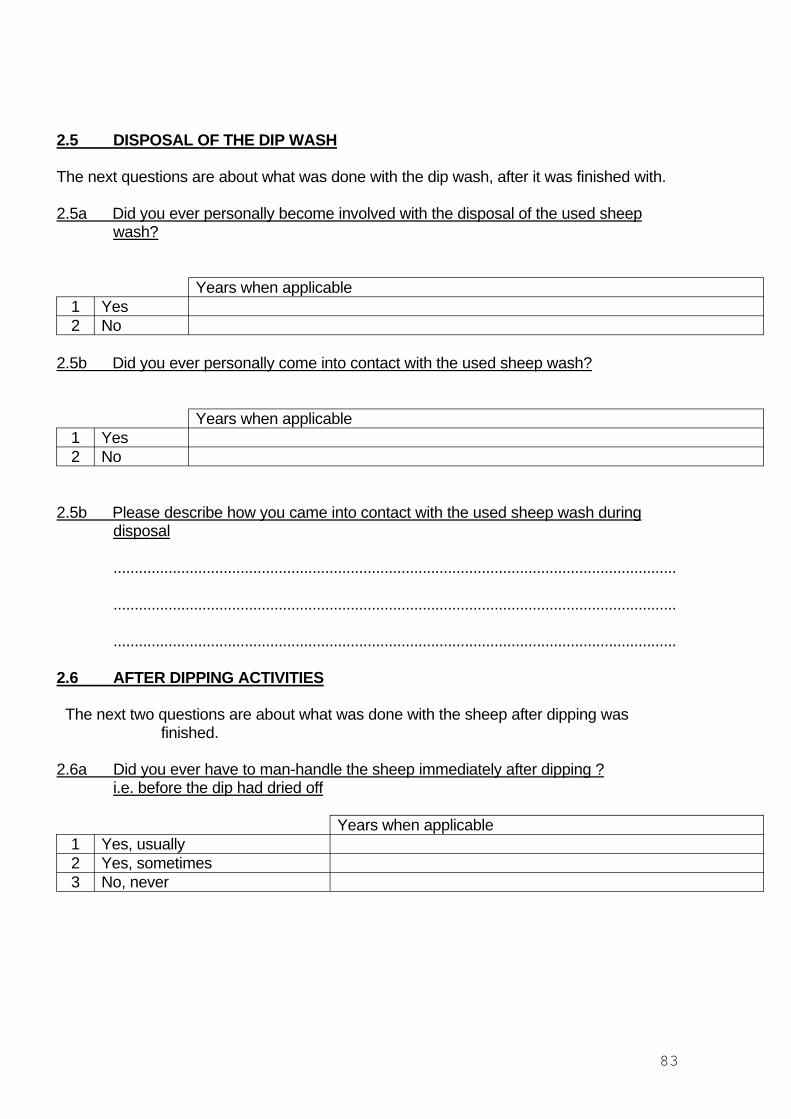
2.5 DISPOSAL OF THE DIP WASH
The next questions are about what was done with the dip wash, after it was finished with.
2.5a Did you ever personally become involved with the disposal of the used sheep wash?
Years when applicable 1 Yes 2 No
2.5b Did you ever personally come into contact with the used sheep wash?
Years when applicable 1 Yes 2 No
2.5b Please describe how you came into contact with the used sheep wash during disposal
.....................................................................................................................................
.....................................................................................................................................
.....................................................................................................................................
2.6 AFTER DIPPING ACTIVITIES
The next two questions are about what was done with the sheep after dipping was finished.
2.6a Did you ever have to man-handle the sheep immediately after dipping ? i.e. before the dip had dried off
Years when applicable 1 Yes, usually 2 Yes, sometimes 3 No, never
83
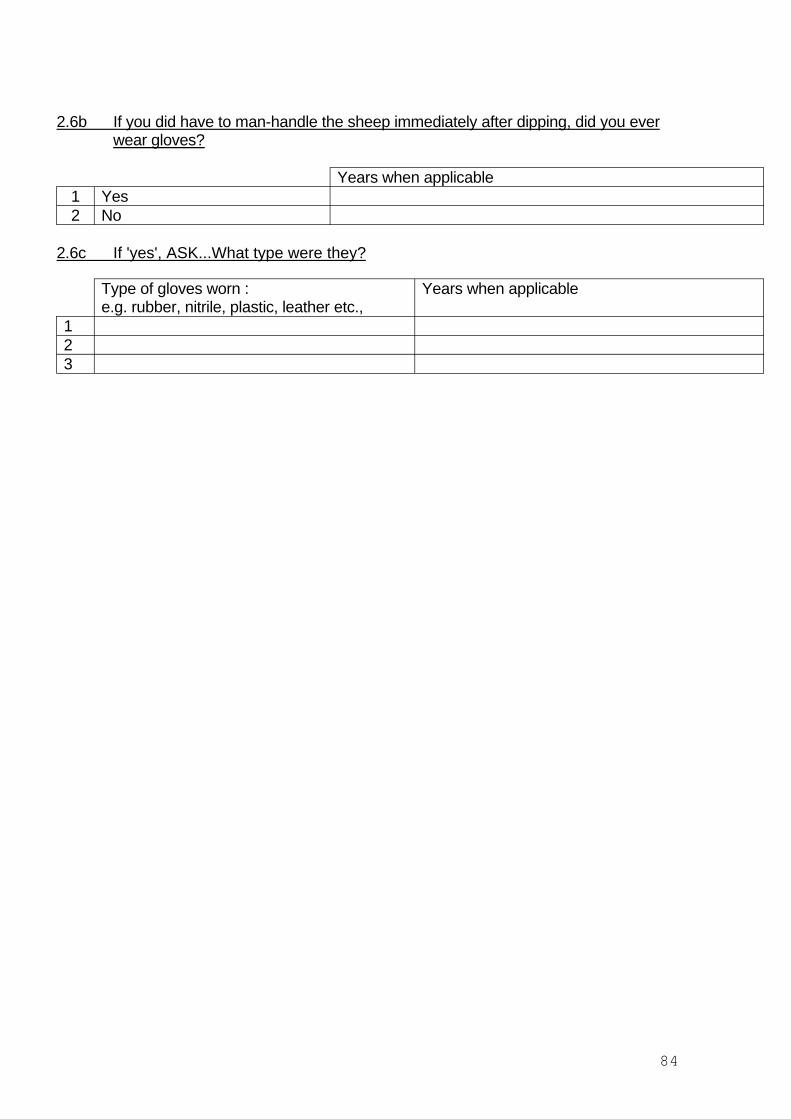
2.6b If you did have to man-handle the sheep immediately after dipping, did you ever wear gloves?
Years when applicable 1 Yes 2 No
2.6c If 'yes', ASK...What type were they?
1
Type of gloves worn : e.g. rubber, nitrile, plastic, leather etc.,
Years when applicable
2 3
84
Appendix 13 Letter to GP
Dear Dr [dr name]address] [date]
RE: [pt name, address and Date of Birth]
I am writing to you about your patient who is taking part in SCOPE, a study of the effects of sheep dip. This study, funded by the Health and Safety Executive, is to determine whether sheep farmers with a variant allele in the paraoxonase enzyme that metabolises some organophosphates are more at risk of ill health attributable to dipping. Your patient has agreed to take part in the study and I enclose a copy of the signed consent form.
In order to answer this question we have to enrol sheep dippers who believe that they have not been affected by dip as well as those who are unwell. In both groups we need to know if there is any history of neurological disease that might give rise to symptoms that could be confused with the effects of organophosphate poisoning. I should be very grateful if you would give us this information about your patient on the brief form attached.
Thank you for your help. If you have any questions please do not hesitate to telephone me or my colleague ……. who is co-ordinating this part of the study.
Kind regards Yours sincerely
Nicola Cherry Professor of Occupational and Environmental Medicine
85
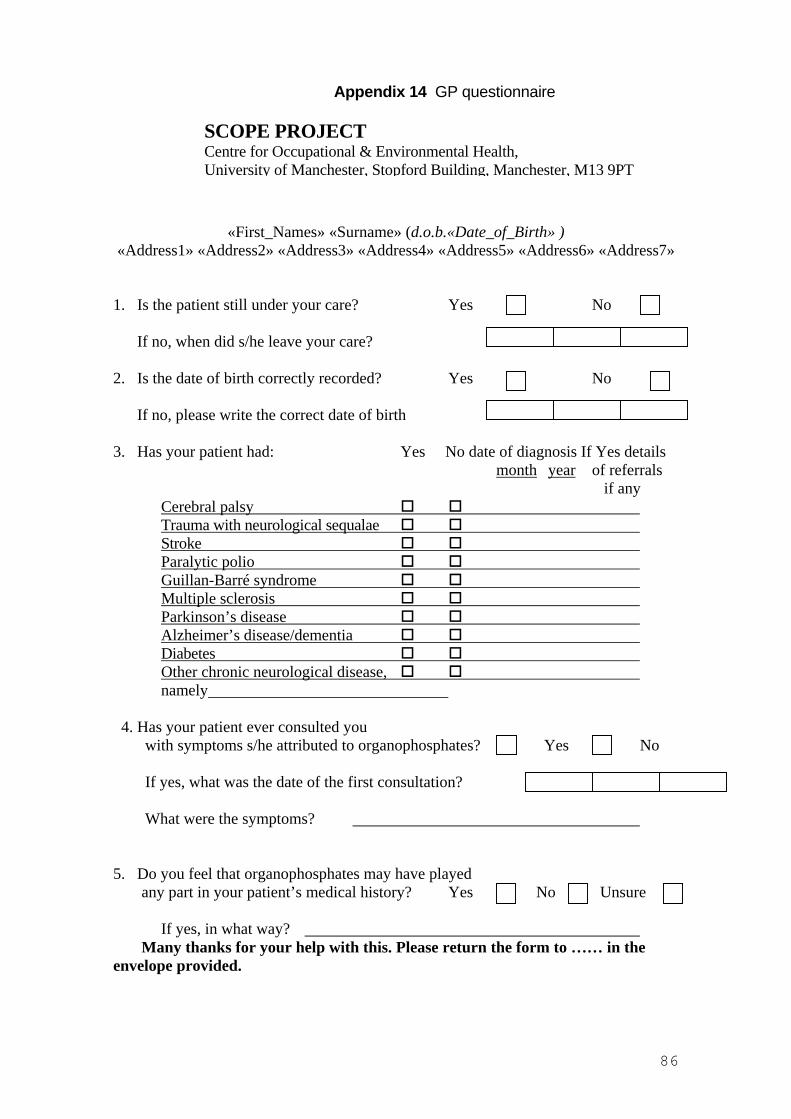
Appendix 14 GP questionnaire
SCOPE PROJECT Centre for Occupational & Environmental Health, University of Manchester, Stopford Building, Manchester, M13 9PT
«First_Names» «Surname» (d.o.b.«Date_of_Birth» )«Address1» «Address2» «Address3» «Address4» «Address5» «Address6» «Address7»
1. Is the patient still under your care? Yes No
If no, when did s/he leave your care?
2. Is the date of birth correctly recorded? Yes No
If no, please write the correct date of birth
3. Has your patient had: Yes No date of diagnosis If Yes details month year of referrals
if any Cerebral palsy Trauma with neurological sequalae
Stroke Paralytic polio Guillan-Barré syndrome Multiple sclerosis Parkinson’s disease Alzheimer’s disease/dementia
Diabetes Other chronic neurological disease,
namely
4. Has your patient ever consulted you with symptoms s/he attributed to organophosphates? Yes No
If yes, what was the date of the first consultation?
What were the symptoms?
5. Do you feel that organophosphates may have played any part in your patient’s medical history? Yes No Unsure
If yes, in what way? Many thanks for your help with this. Please return the form to …… in the
envelope provided.
86
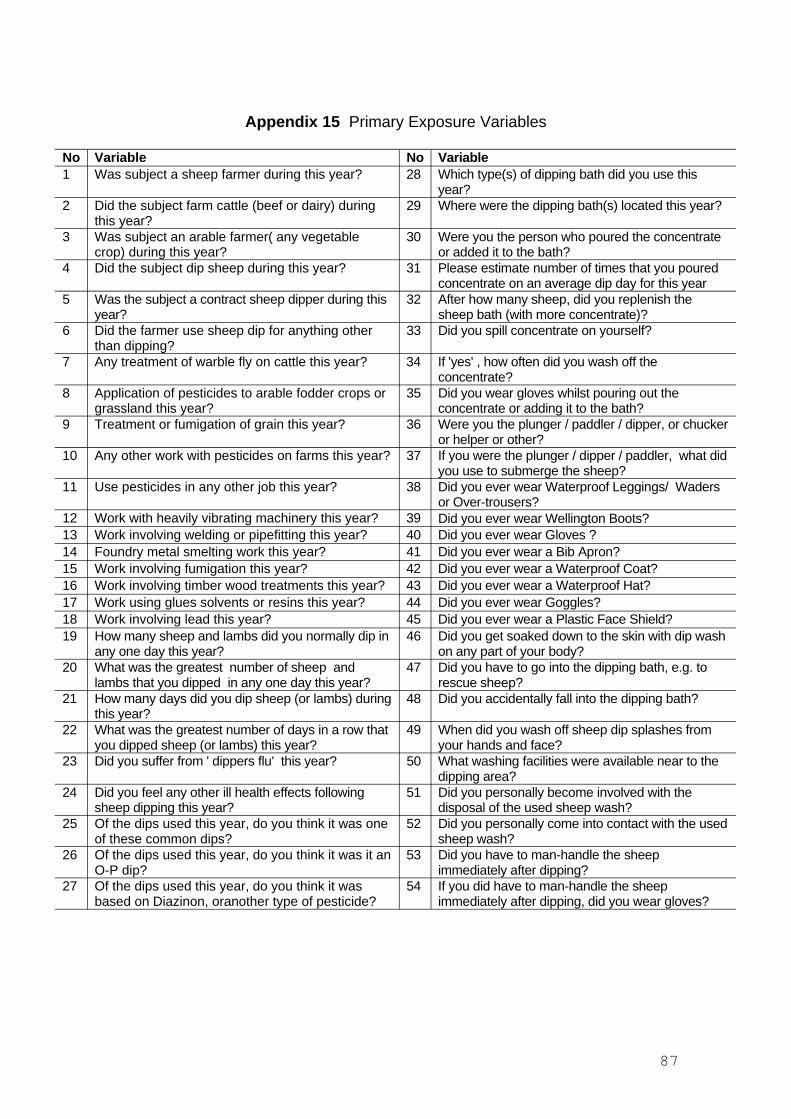
Appendix 15 Primary Exposure Variables
No Variable No Variable 1 Was subject a sheep farmer during this year? 28 Which type(s) of dipping bath did you use this
year? 2 Did the subject farm cattle (beef or dairy) during
this year? 29 Where were the dipping bath(s) located this year?
3 Was subject an arable farmer( any vegetable crop) during this year?
30 Were you the person who poured the concentrate or added it to the bath?
4 Did the subject dip sheep during this year? 31 Please estimate number of times that you poured concentrate on an average dip day for this year
5 Was the subject a contract sheep dipper during this year?
32 After how many sheep, did you replenish the sheep bath (with more concentrate)?
6 Did the farmer use sheep dip for anything other than dipping?
33 Did you spill concentrate on yourself?
7 Any treatment of warble fly on cattle this year? 34 If 'yes' , how often did you wash off the concentrate?
8 Application of pesticides to arable fodder crops or grassland this year?
35 Did you wear gloves whilst pouring out the concentrate or adding it to the bath?
9 Treatment or fumigation of grain this year? 36 Were you the plunger / paddler / dipper, or chucker or helper or other?
10 Any other work with pesticides on farms this year? 37 If you were the plunger / dipper / paddler, what did you use to submerge the sheep?
11 Use pesticides in any other job this year? 38 Did you ever wear Waterproof Leggings/ Waders or Over-trousers?
12 Work with heavily vibrating machinery this year? 39 Did you ever wear Wellington Boots? 13 Work involving welding or pipefitting this year? 40 Did you ever wear Gloves ? 14 Foundry metal smelting work this year? 41 Did you ever wear a Bib Apron? 15 Work involving fumigation this year? 42 Did you ever wear a Waterproof Coat? 16 Work involving timber wood treatments this year? 43 Did you ever wear a Waterproof Hat? 17 Work using glues solvents or resins this year? 44 Did you ever wear Goggles? 18 Work involving lead this year? 45 Did you ever wear a Plastic Face Shield? 19 How many sheep and lambs did you normally dip in
any one day this year? 46 Did you get soaked down to the skin with dip wash
on any part of your body? 20 What was the greatest number of sheep and
lambs that you dipped in any one day this year? 47 Did you have to go into the dipping bath, e.g. to
rescue sheep? 21 How many days did you dip sheep (or lambs) during
this year? 48 Did you accidentally fall into the dipping bath?
22 What was the greatest number of days in a row that you dipped sheep (or lambs) this year?
49 When did you wash off sheep dip splashes from your hands and face?
23 Did you suffer from ' dippers flu' this year? 50 What washing facilities were available near to the dipping area?
24 Did you feel any other ill health effects following sheep dipping this year?
51 Did you personally become involved with the disposal of the used sheep wash?
25 Of the dips used this year, do you think it was one of these common dips?
52 Did you personally come into contact with the used sheep wash?
26 Of the dips used this year, do you think it was it an O-P dip?
53 Did you have to man-handle the sheep immediately after dipping?
27 Of the dips used this year, do you think it was based on Diazinon, oranother type of pesticide?
54 If you did have to man-handle the sheep immediately after dipping, did you wear gloves?
87
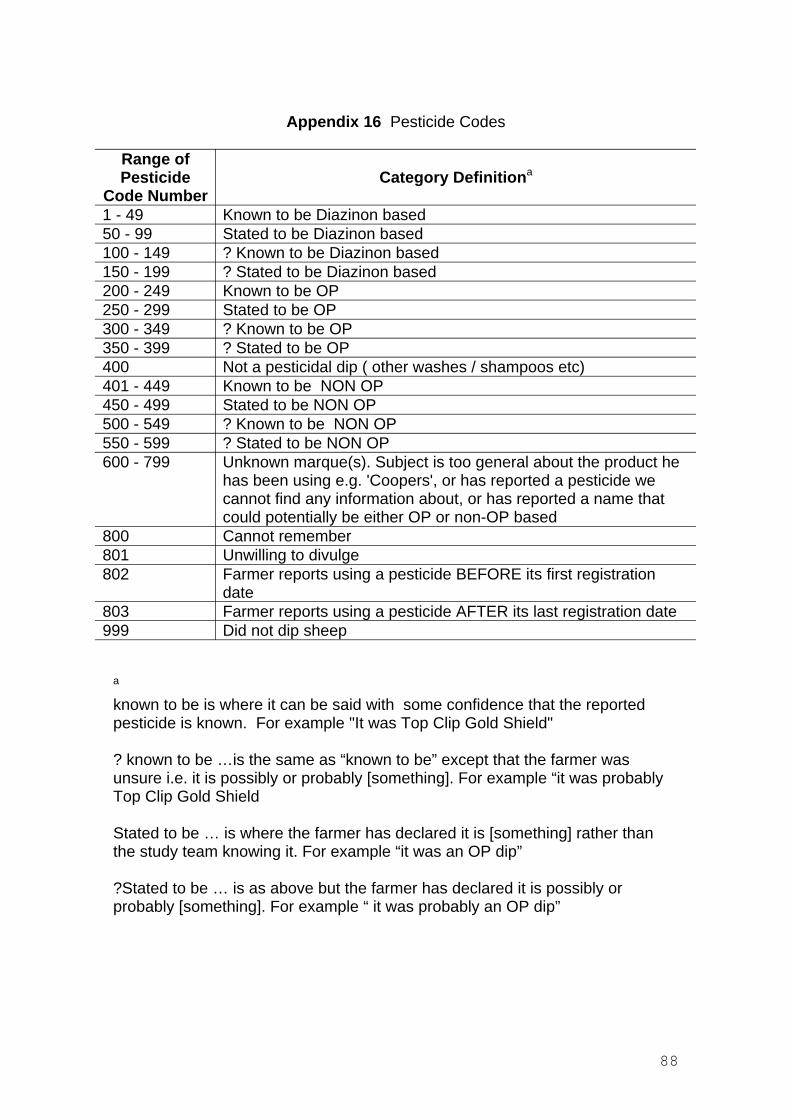
400
800 801 802
803 999
Appendix 16 Pesticide Codes
Range of Pesticide
Code Number 1 - 49 50 - 99 100 - 149 150 - 199 200 - 249 250 - 299 300 - 349 350 - 399
401 - 449 450 - 499 500 - 549 550 - 599 600 - 799
a
Category Definitiona
Known to be Diazinon based Stated to be Diazinon based ? Known to be Diazinon based ? Stated to be Diazinon based Known to be OP Stated to be OP ? Known to be OP ? Stated to be OP Not a pesticidal dip ( other washes / shampoos etc) Known to be NON OP Stated to be NON OP ? Known to be NON OP ? Stated to be NON OP Unknown marque(s). Subject is too general about the product he has been using e.g. 'Coopers', or has reported a pesticide we cannot find any information about, or has reported a name that could potentially be either OP or non-OP based Cannot remember Unwilling to divulge Farmer reports using a pesticide BEFORE its first registration date Farmer reports using a pesticide AFTER its last registration date Did not dip sheep
known to be is where it can be said with some confidence that the reported pesticide is known. For example "It was Top Clip Gold Shield"
? known to be …is the same as “known to be” except that the farmer was unsure i.e. it is possibly or probably [something]. For example “it was probably Top Clip Gold Shield
Stated to be … is where the farmer has declared it is [something] rather than the study team knowing it. For example “it was an OP dip”
?Stated to be … is as above but the farmer has declared it is possibly or probably [something]. For example “ it was probably an OP dip”
88
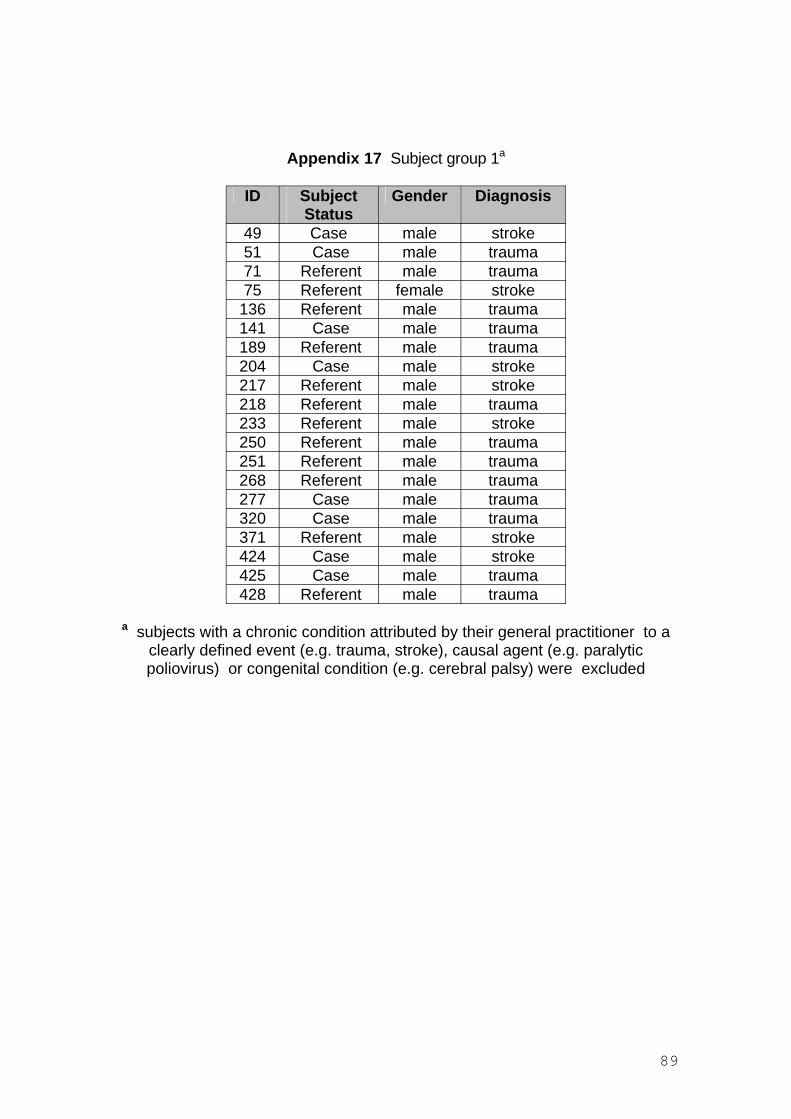
Appendix 17 Subject group 1a
ID Subject Status
Gender Diagnosis
49 Case male stroke 51 Case male trauma 71 Referent male trauma 75 Referent female stroke
136 Referent male trauma 141 Case male trauma 189 Referent male trauma 204 Case male stroke 217 Referent male stroke 218 Referent male trauma 233 Referent male stroke 250 Referent male trauma 251 Referent male trauma 268 Referent male trauma 277 Case male trauma 320 Case male trauma 371 Referent male stroke 424 Case male stroke 425 Case male trauma 428 Referent male trauma
a subjects with a chronic condition attributed by their general practitioner to a clearly defined event (e.g. trauma, stroke), causal agent (e.g. paralytic poliovirus) or congenital condition (e.g. cerebral palsy) were excluded
89
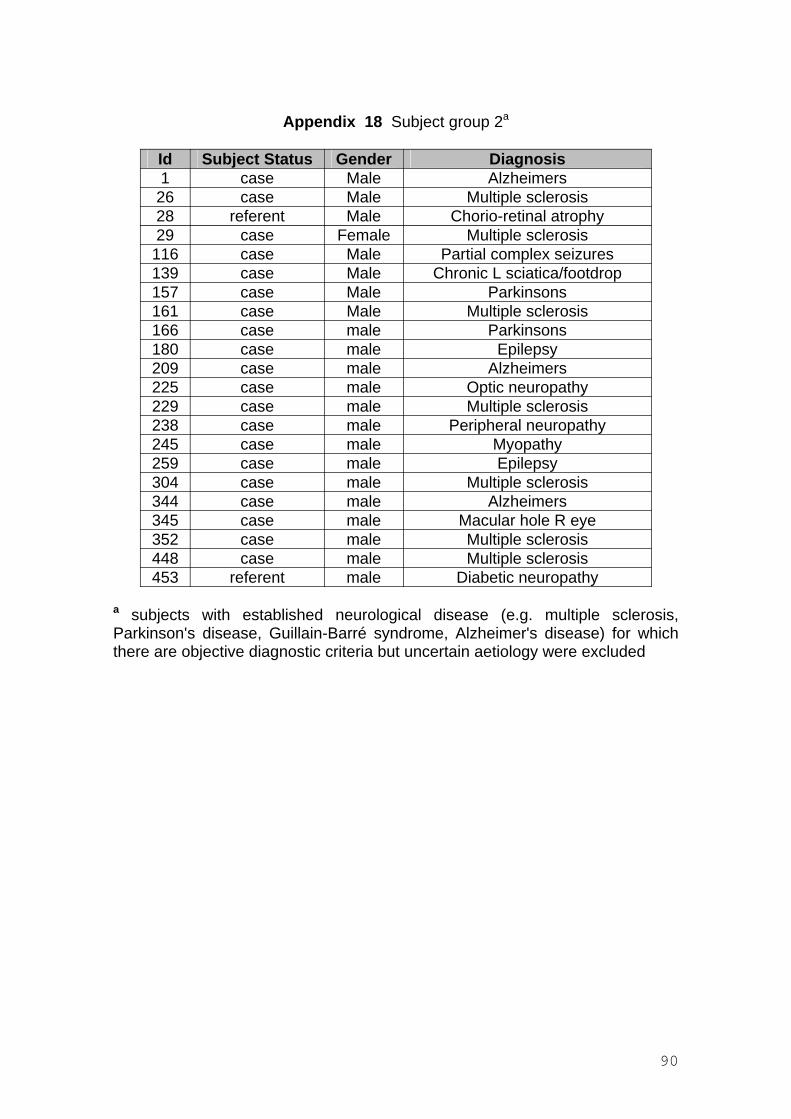
Appendix 18 Subject group 2a
Id Subject Status Gender Diagnosis 1 case Male Alzheimers
26 case Male Multiple sclerosis 28 referent Male Chorio-retinal atrophy 29 case Female Multiple sclerosis 116 case Male Partial complex seizures 139 case Male Chronic L sciatica/footdrop 157 case Male Parkinsons 161 case Male Multiple sclerosis 166 case male Parkinsons 180 case male Epilepsy 209 case male Alzheimers 225 case male Optic neuropathy 229 case male Multiple sclerosis 238 case male Peripheral neuropathy 245 case male Myopathy 259 case male Epilepsy 304 case male Multiple sclerosis 344 case male Alzheimers 345 case male Macular hole R eye 352 case male Multiple sclerosis 448 case male Multiple sclerosis 453 referent male Diabetic neuropathy
a subjects with established neurological disease (e.g. multiple sclerosis, Parkinson's disease, Guillain-Barré syndrome, Alzheimer's disease) for which there are objective diagnostic criteria but uncertain aetiology were excluded
90
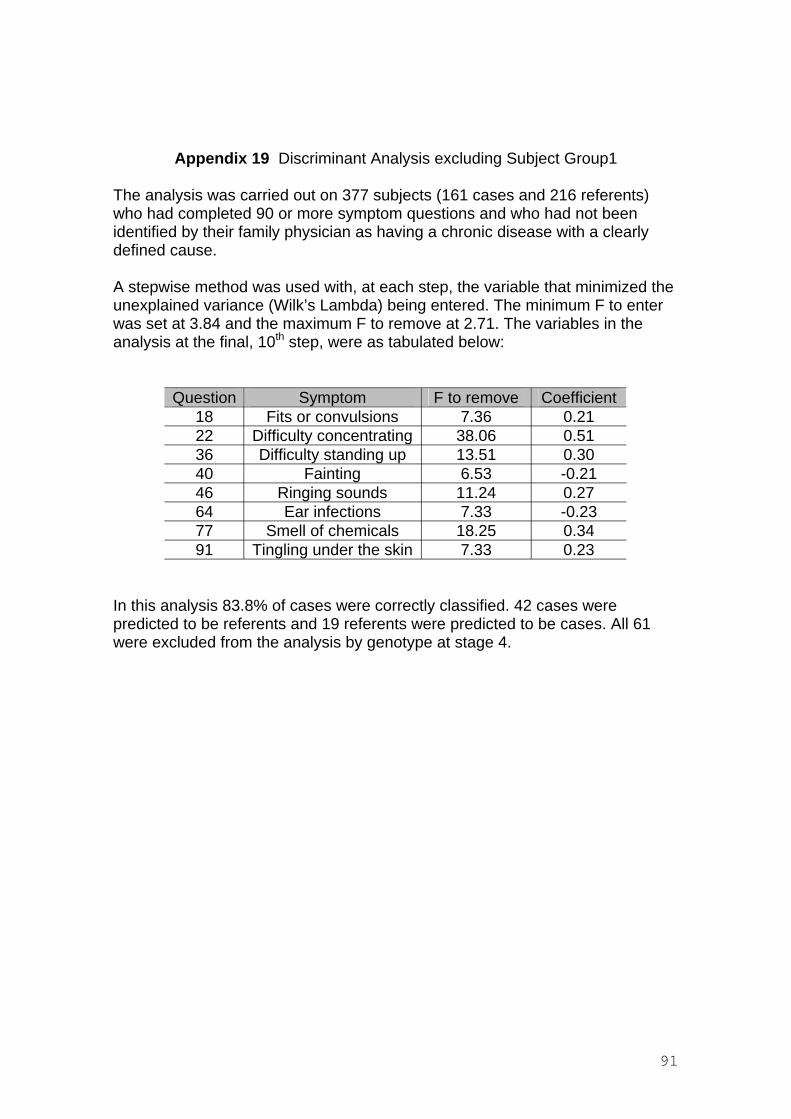
Appendix 19 Discriminant Analysis excluding Subject Group1
The analysis was carried out on 377 subjects (161 cases and 216 referents) who had completed 90 or more symptom questions and who had not been identified by their family physician as having a chronic disease with a clearly defined cause.
A stepwise method was used with, at each step, the variable that minimized the unexplained variance (Wilk’s Lambda) being entered. The minimum F to enter was set at 3.84 and the maximum F to remove at 2.71. The variables in the analysis at the final, 10th step, were as tabulated below:
Question Symptom F to remove Coefficient 18 Fits or convulsions 7.36 0.21 22 Difficulty concentrating 38.06 0.51 36 Difficulty standing up 13.51 0.30 40 Fainting 6.53 -0.21 46 Ringing sounds 11.24 0.27 64 Ear infections 7.33 -0.23 77 Smell of chemicals 18.25 0.34 91 Tingling under the skin 7.33 0.23
In this analysis 83.8% of cases were correctly classified. 42 cases were predicted to be referents and 19 referents were predicted to be cases. All 61 were excluded from the analysis by genotype at stage 4.
91
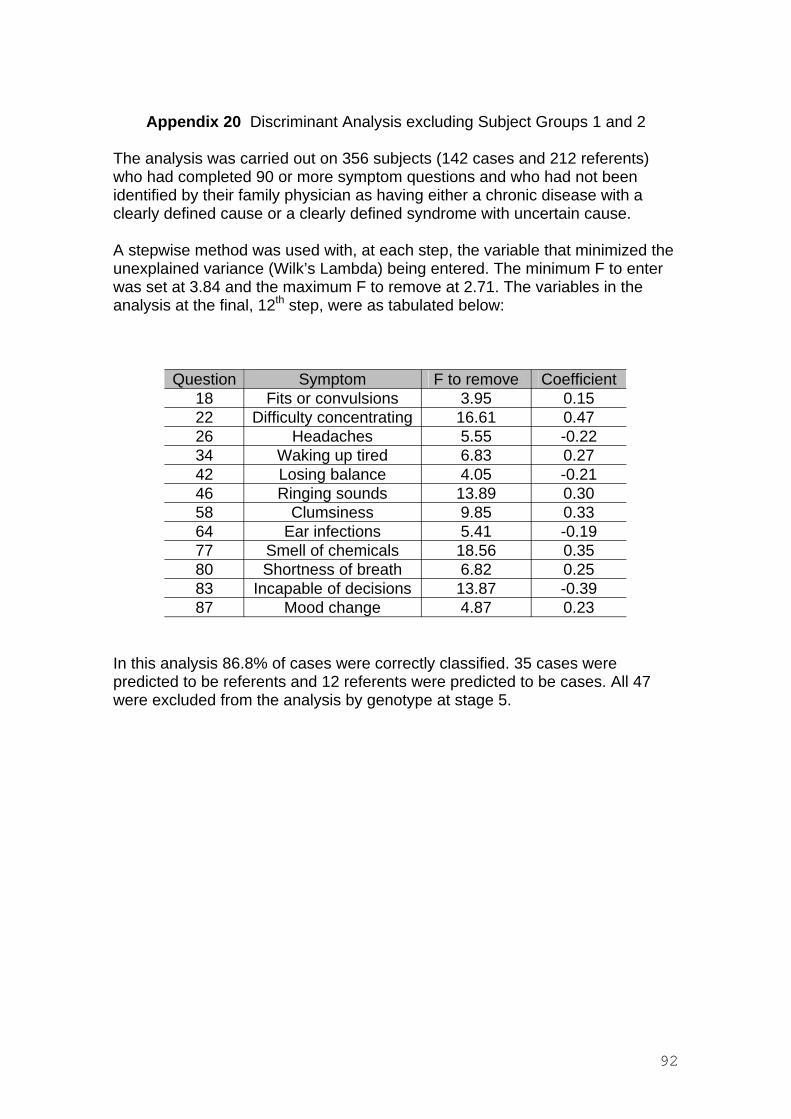
Appendix 20 Discriminant Analysis excluding Subject Groups 1 and 2
The analysis was carried out on 356 subjects (142 cases and 212 referents) who had completed 90 or more symptom questions and who had not been identified by their family physician as having either a chronic disease with a clearly defined cause or a clearly defined syndrome with uncertain cause.
A stepwise method was used with, at each step, the variable that minimized the unexplained variance (Wilk’s Lambda) being entered. The minimum F to enter was set at 3.84 and the maximum F to remove at 2.71. The variables in the analysis at the final, 12th step, were as tabulated below:
Question Symptom F to remove Coefficient 18 Fits or convulsions 3.95 0.15 22 Difficulty concentrating 16.61 0.47 26 Headaches 5.55 -0.22 34 Waking up tired 6.83 0.27 42 Losing balance 4.05 -0.21 46 Ringing sounds 13.89 0.30 58 Clumsiness 9.85 0.33 64 Ear infections 5.41 -0.19 77 Smell of chemicals 18.56 0.35 80 Shortness of breath 6.82 0.25 83 Incapable of decisions 13.87 -0.39 87 Mood change 4.87 0.23
In this analysis 86.8% of cases were correctly classified. 35 cases were predicted to be referents and 12 referents were predicted to be cases. All 47 were excluded from the analysis by genotype at stage 5.
92
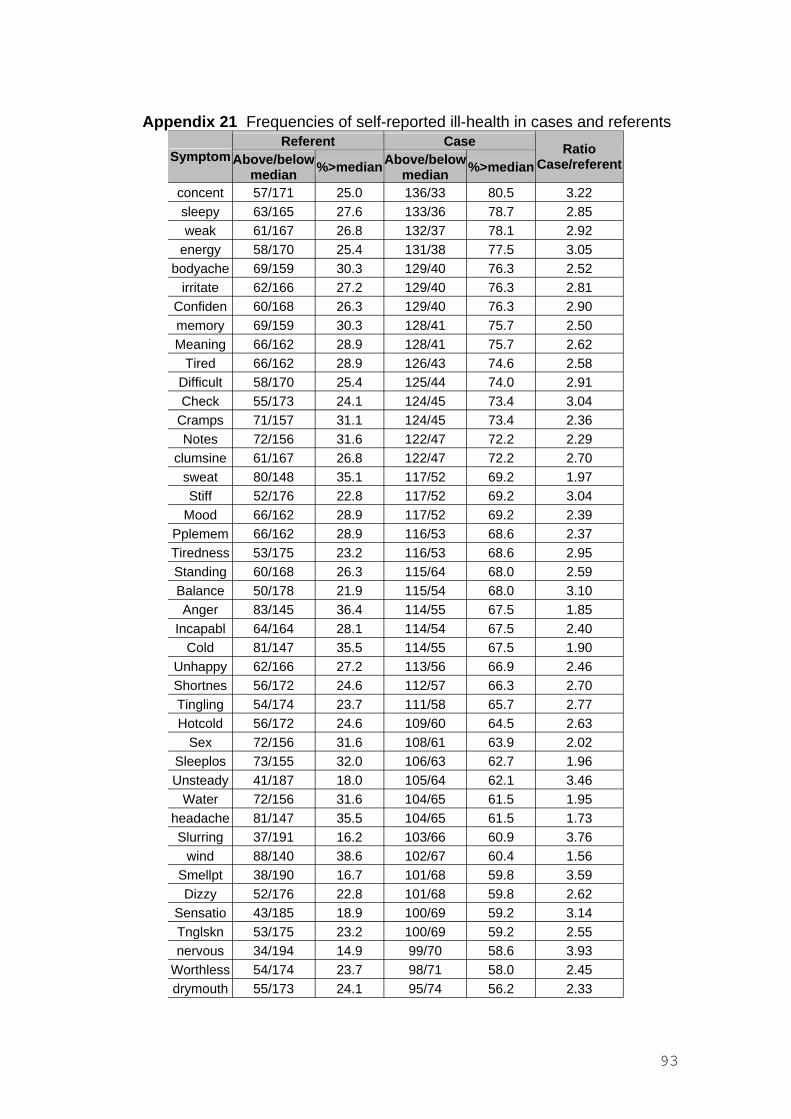
Appendix 21 Frequencies of self-reported ill-health in cases and referents Referent Case RatioSymptom Above/below %>medianAbove/below Case/referent %>median median median
concent 57/171 25.0 136/33 80.5 3.22 sleepy 63/165 27.6 133/36 78.7 2.85 weak 61/167 26.8 132/37 78.1 2.92
energy 58/170 25.4 131/38 77.5 3.05 bodyache 69/159 30.3 129/40 76.3 2.52
irritate 62/166 27.2 129/40 76.3 2.81 Confiden 60/168 26.3 129/40 76.3 2.90 memory 69/159 30.3 128/41 75.7 2.50 Meaning 66/162 28.9 128/41 75.7 2.62
Tired 66/162 28.9 126/43 74.6 2.58 Difficult 58/170 25.4 125/44 74.0 2.91 Check 55/173 24.1 124/45 73.4 3.04
Cramps 71/157 31.1 124/45 73.4 2.36 Notes 72/156 31.6 122/47 72.2 2.29
clumsine 61/167 26.8 122/47 72.2 2.70 sweat 80/148 35.1 117/52 69.2 1.97 Stiff 52/176 22.8 117/52 69.2 3.04
Mood 66/162 28.9 117/52 69.2 2.39 Pplemem 66/162 28.9 116/53 68.6 2.37 Tiredness 53/175 23.2 116/53 68.6 2.95 Standing 60/168 26.3 115/64 68.0 2.59 Balance 50/178 21.9 115/54 68.0 3.10 Anger 83/145 36.4 114/55 67.5 1.85
Incapabl 64/164 28.1 114/54 67.5 2.40 Cold 81/147 35.5 114/55 67.5 1.90
Unhappy 62/166 27.2 113/56 66.9 2.46 Shortnes 56/172 24.6 112/57 66.3 2.70 Tingling 54/174 23.7 111/58 65.7 2.77 Hotcold 56/172 24.6 109/60 64.5 2.63
Sex 72/156 31.6 108/61 63.9 2.02 Sleeplos 73/155 32.0 106/63 62.7 1.96 Unsteady 41/187 18.0 105/64 62.1 3.46
Water 72/156 31.6 104/65 61.5 1.95 headache 81/147 35.5 104/65 61.5 1.73 Slurring 37/191 16.2 103/66 60.9 3.76
wind 88/140 38.6 102/67 60.4 1.56 Smellpt 38/190 16.7 101/68 59.8 3.59 Dizzy 52/176 22.8 101/68 59.8 2.62
Sensatio 43/185 18.9 100/69 59.2 3.14 Tnglskn 53/175 23.2 100/69 59.2 2.55 nervous 34/194 14.9 99/70 58.6 3.93
Worthless 54/174 23.7 98/71 58.0 2.45 drymouth 55/173 24.1 95/74 56.2 2.33
93
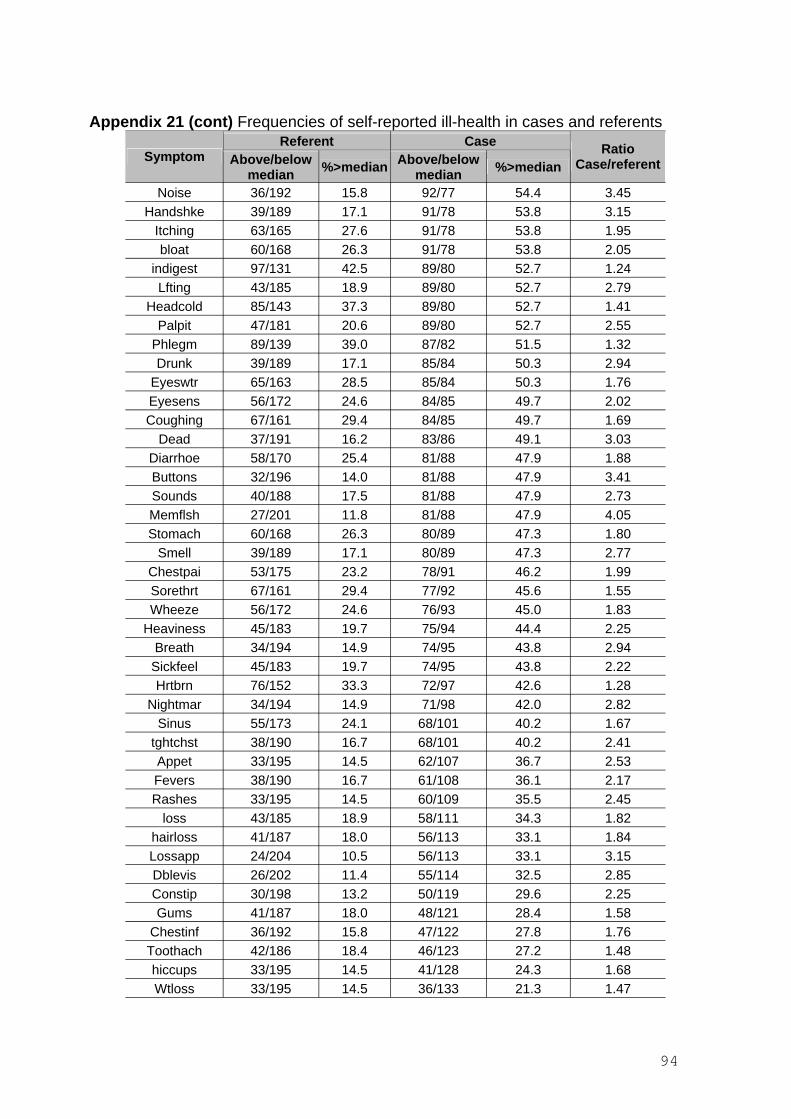
Appendix 21 (cont) Frequencies of self-reported ill-health in cases and referents
Symptom Referent Case
Above/below median %>median Above/below
median %>median Ratio
Case/referent
Noise 36/192 15.8 92/77 54.4 3.45 Handshke 39/189 17.1 91/78 53.8 3.15
Itching 63/165 27.6 91/78 53.8 1.95 bloat 60/168 26.3 91/78 53.8 2.05
indigest 97/131 42.5 89/80 52.7 1.24 Lfting 43/185 18.9 89/80 52.7 2.79
Headcold 85/143 37.3 89/80 52.7 1.41 Palpit 47/181 20.6 89/80 52.7 2.55
Phlegm 89/139 39.0 87/82 51.5 1.32 Drunk 39/189 17.1 85/84 50.3 2.94
Eyeswtr 65/163 28.5 85/84 50.3 1.76 Eyesens 56/172 24.6 84/85 49.7 2.02 Coughing 67/161 29.4 84/85 49.7 1.69
Dead 37/191 16.2 83/86 49.1 3.03 Diarrhoe 58/170 25.4 81/88 47.9 1.88 Buttons 32/196 14.0 81/88 47.9 3.41 Sounds 40/188 17.5 81/88 47.9 2.73 Memflsh 27/201 11.8 81/88 47.9 4.05 Stomach 60/168 26.3 80/89 47.3 1.80
Smell 39/189 17.1 80/89 47.3 2.77 Chestpai 53/175 23.2 78/91 46.2 1.99 Sorethrt 67/161 29.4 77/92 45.6 1.55 Wheeze 56/172 24.6 76/93 45.0 1.83
Heaviness 45/183 19.7 75/94 44.4 2.25 Breath 34/194 14.9 74/95 43.8 2.94 Sickfeel 45/183 19.7 74/95 43.8 2.22 Hrtbrn 76/152 33.3 72/97 42.6 1.28
Nightmar 34/194 14.9 71/98 42.0 2.82 Sinus 55/173 24.1 68/101 40.2 1.67
tghtchst 38/190 16.7 68/101 40.2 2.41 Appet 33/195 14.5 62/107 36.7 2.53 Fevers 38/190 16.7 61/108 36.1 2.17 Rashes 33/195 14.5 60/109 35.5 2.45
loss 43/185 18.9 58/111 34.3 1.82 hairloss 41/187 18.0 56/113 33.1 1.84 Lossapp 24/204 10.5 56/113 33.1 3.15 Dblevis 26/202 11.4 55/114 32.5 2.85 Constip 30/198 13.2 50/119 29.6 2.25 Gums 41/187 18.0 48/121 28.4 1.58
Chestinf 36/192 15.8 47/122 27.8 1.76 Toothach 42/186 18.4 46/123 27.2 1.48 hiccups 33/195 14.5 41/128 24.3 1.68 Wtloss 33/195 14.5 36/133 21.3 1.47
94
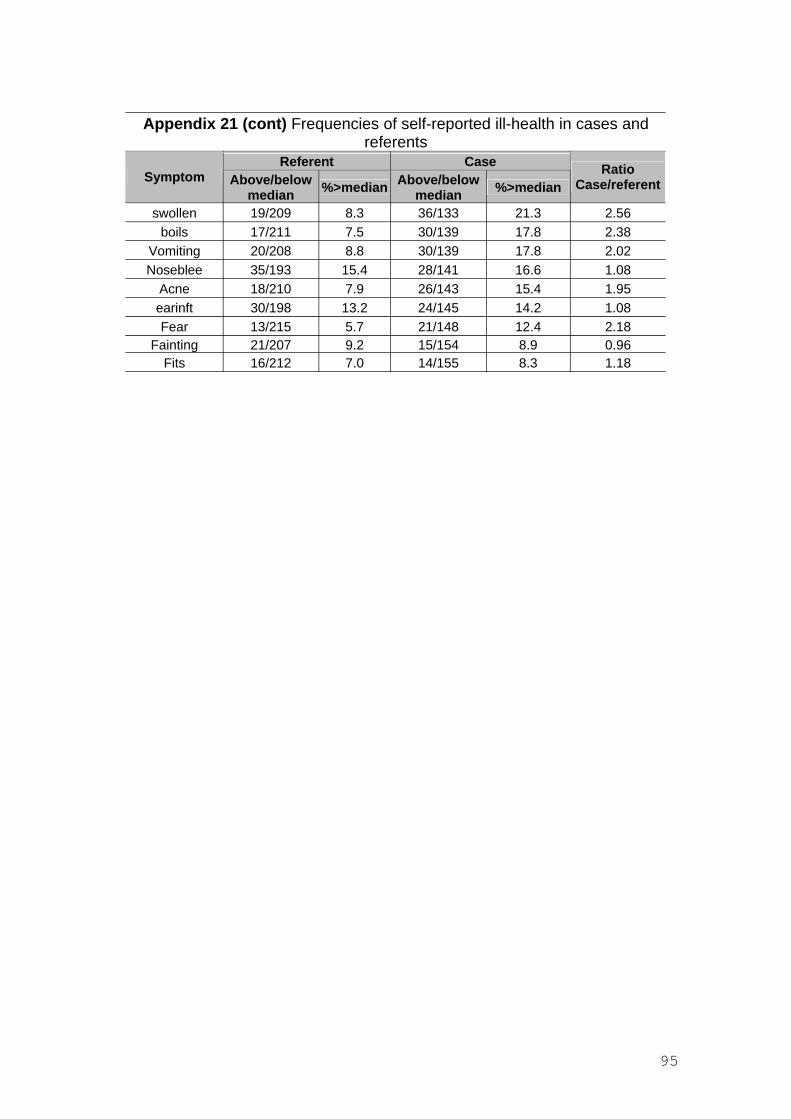
Appendix 21 (cont) Frequencies of self-reported ill-health in cases and referents
Referent Case RatioSymptom Above/below %>median Above/below %>median Case/referent median median
swollen 19/209 8.3 36/133 21.3 2.56 boils 17/211 7.5 30/139 17.8 2.38
Vomiting 20/208 8.8 30/139 17.8 2.02 Noseblee 35/193 15.4 28/141 16.6 1.08
Acne 18/210 7.9 26/143 15.4 1.95 earinft 30/198 13.2 24/145 14.2 1.08 Fear 13/215 5.7 21/148 12.4 2.18
Fainting 21/207 9.2 15/154 8.9 0.96 Fits 16/212 7.0 14/155 8.3 1.18
95
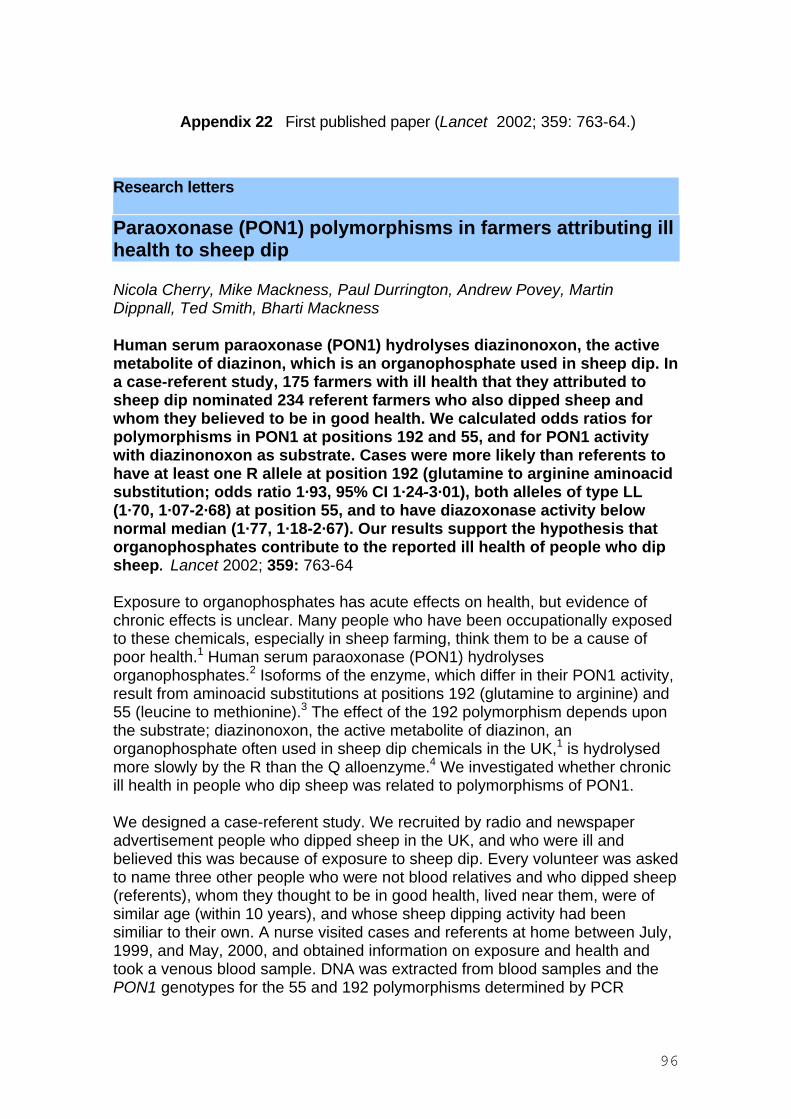
Appendix 22 First published paper (Lancet 2002; 359: 763-64.)
Research letters
Paraoxonase (PON1) polymorphisms in farmers attributing ill health to sheep dip
Nicola Cherry, Mike Mackness, Paul Durrington, Andrew Povey, Martin Dippnall, Ted Smith, Bharti Mackness
Human serum paraoxonase (PON1) hydrolyses diazinonoxon, the active metabolite of diazinon, which is an organophosphate used in sheep dip. In a case-referent study, 175 farmers with ill health that they attributed to sheep dip nominated 234 referent farmers who also dipped sheep and whom they believed to be in good health. We calculated odds ratios for polymorphisms in PON1 at positions 192 and 55, and for PON1 activity with diazinonoxon as substrate. Cases were more likely than referents to have at least one R allele at position 192 (glutamine to arginine aminoacid substitution; odds ratio 1·93, 95% CI 1·24-3·01), both alleles of type LL (1·70, 1·07-2·68) at position 55, and to have diazoxonase activity below normal median (1·77, 1·18-2·67). Our results support the hypothesis that organophosphates contribute to the reported ill health of people who dip sheep. Lancet 2002; 359: 763-64
Exposure to organophosphates has acute effects on health, but evidence of chronic effects is unclear. Many people who have been occupationally exposed to these chemicals, especially in sheep farming, think them to be a cause of poor health.1 Human serum paraoxonase (PON1) hydrolyses organophosphates.2 Isoforms of the enzyme, which differ in their PON1 activity, result from aminoacid substitutions at positions 192 (glutamine to arginine) and 55 (leucine to methionine).3 The effect of the 192 polymorphism depends upon the substrate; diazinonoxon, the active metabolite of diazinon, an organophosphate often used in sheep dip chemicals in the UK,1 is hydrolysed more slowly by the R than the Q alloenzyme.4 We investigated whether chronic ill health in people who dip sheep was related to polymorphisms of PON1.
We designed a case-referent study. We recruited by radio and newspaper advertisement people who dipped sheep in the UK, and who were ill and believed this was because of exposure to sheep dip. Every volunteer was asked to name three other people who were not blood relatives and who dipped sheep (referents), whom they thought to be in good health, lived near them, were of similar age (within 10 years), and whose sheep dipping activity had been similiar to their own. A nurse visited cases and referents at home between July, 1999, and May, 2000, and obtained information on exposure and health and took a venous blood sample. DNA was extracted from blood samples and the PON1 genotypes for the 55 and 192 polymorphisms determined by PCR
96
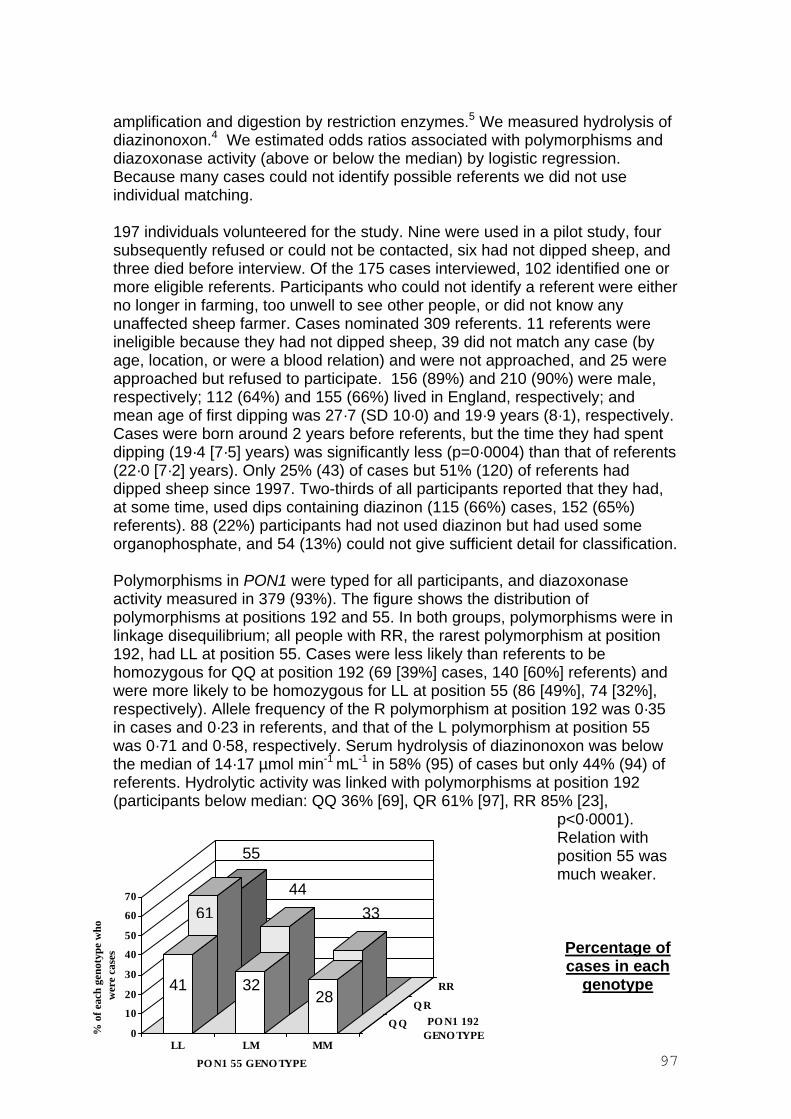
amplification and digestion by restriction enzymes.5 We measured hydrolysis of diazinonoxon.4 We estimated odds ratios associated with polymorphisms and diazoxonase activity (above or below the median) by logistic regression. Because many cases could not identify possible referents we did not use individual matching.
197 individuals volunteered for the study. Nine were used in a pilot study, four subsequently refused or could not be contacted, six had not dipped sheep, and three died before interview. Of the 175 cases interviewed, 102 identified one or more eligible referents. Participants who could not identify a referent were either no longer in farming, too unwell to see other people, or did not know any unaffected sheep farmer. Cases nominated 309 referents. 11 referents were ineligible because they had not dipped sheep, 39 did not match any case (by age, location, or were a blood relation) and were not approached, and 25 were approached but refused to participate. 156 (89%) and 210 (90%) were male, respectively; 112 (64%) and 155 (66%) lived in England, respectively; and mean age of first dipping was 27·7 (SD 10·0) and 19·9 years (8·1), respectively. Cases were born around 2 years before referents, but the time they had spent dipping (19·4 [7·5] years) was significantly less (p=0·0004) than that of referents (22·0 [7·2] years). Only 25% (43) of cases but 51% (120) of referents had dipped sheep since 1997. Two-thirds of all participants reported that they had, at some time, used dips containing diazinon (115 (66%) cases, 152 (65%) referents). 88 (22%) participants had not used diazinon but had used some organophosphate, and 54 (13%) could not give sufficient detail for classification.
Polymorphisms in PON1 were typed for all participants, and diazoxonase activity measured in 379 (93%). The figure shows the distribution of polymorphisms at positions 192 and 55. In both groups, polymorphisms were in linkage disequilibrium; all people with RR, the rarest polymorphism at position 192, had LL at position 55. Cases were less likely than referents to be homozygous for QQ at position 192 (69 [39%] cases, 140 [60%] referents) and were more likely to be homozygous for LL at position 55 (86 [49%], 74 [32%], respectively). Allele frequency of the R polymorphism at position 192 was 0·35 in cases and 0·23 in referents, and that of the L polymorphism at position 55 was 0·71 and 0·58, respectively. Serum hydrolysis of diazinonoxon was below the median of 14·17 µmol min-1 mL-1 in 58% (95) of cases but only 44% (94) of referents. Hydrolytic activity was linked with polymorphisms at position 192 (participants below median: QQ 36% [69], QR 61% [97], RR 85% [23],
p<0·0001). Relation with position 55 was much weaker.
0
10
20
30
40
50
60
70
% o
f eac
h ge
noty
pe w
how
ere
case
s
Q Q
Q R
41
61
55
32
44
28
33
PO N1 192 GENO TYPE
Percentage of cases in each
RR genotype
LL LM MM
PO N1 55 GENO TYPE 97
Number of people in each genotype: QQ/LL n=49 (20 cases, 29 referents), QQ/LM n=113 (36,77) QQ/MM n=47 (13, 34) QR/LL n=82 (50, 32) QR/LM n=86 (39,47) QR/MM n=3 (1,2), RR/LL n=29 (16, 13). No participant had LM/RR or MM/RR genotype
We initially classed participants by whether they had one or both alleles of type R and L, and then assessed the additional effect of having both alleles of this type (table). At site 192 one allele of type R predisposed towards reported ill health, but possession of both alleles of this type was not an additional disadvantage. At site 55 additional risk of perceived ill health was seen only when both alleles were type L. This pattern was unchanged when both sites were analysed (overall effect at 192, p=0·015; 55, p=0·045). The interaction term was not significant (p=0·75), suggesting that the effects of the two polymorphisms were independent, and adjustment for sex, region, date of first dipping, and age did not affect odds ratios. The frequency of self-reported heart disease was related to polymorphisms at position 192 but, in 137 cases and 214 referents reporting no heart disease, the odds ratio for reported ill health remained raised (odds ratio at 192=1·79, 95% CI 1·13-2·84; at 55=1·93, 1·21-3·08).
Odds ratios for case status for polymorphisms at positions 192 and 55 of PON1
Position 192QR or RR vs QQ RR vs QR or QQ Position 55LM or LL vs MM LL vs LM or MM Positions 192 and 55 QR or RR vs QQ RR vs QR or QQ LM or LL vs MM LL vs LM or MM
Odds ratio (95% CI) p 0·001
2·25 (1·49-3·42) 0·001 1·11 (0·50-2·44) 0·800
0·001 1·55 (0·79-3·07) 0·204 1·92 (1·26-2·93) 0·002
1·93 (1·24-3·01) 0·004 0·84 (0·37-1·91) 0·674 1·21 (0·60-2·45) 0·599 1·70 (1·07-2·68) 0·024
The unadjusted odds ratio for diazinonoxon activity below median was 1·77 (1·12-2·67). The adjusted odds ratios, including both polymorphisms and activity, were 1·49 (position 192, 0·94-2·37) and 1·90 (55, 1·19-3·03), and for activity was 1·76 (1·12-2·76).
The PON1 192 polymorphism associated with a diminished ability to hydrolyse diazinonoxon was more frequent in people reporting ill health, as was the LL polymorphism at position 55. Cases were more likely than referents to have low
98
serum hydrolytic activity for diazinonoxon. These results suggest that organophosphates contribute to the reported ill health of people who dip sheep.
References 1. Committee on Toxicity of Chemicals in Food, Consumer Products and the
Environment: organophosphates. London: Department of Health, 1999. 2. Costa LG, Li WF, Richter RJ, Shih DM, Lusis A, Furlong CE. The role of
paraoxonase (PON1) in the detoxication of organophosphates and its human polymorphism. Chem Biol Interact 1999; 119: 429-38.
3. Mackness B, Mackness MI, Arrol S, Turkie W, Durrington PN. Effect of the molecular polymorphisms of human paraoxonase (PON1) on the rate of hydrolysis of paraoxon. Br J Pharmacol 1997; 122: 265-68.
4. Davies HG, Richter RJ, Keifer M, Broomfield CA, Sowalla J, Furlong CE. The effect of the human serum paraoxonase polymorphism is reversed with diazoxon, soman and sarin. Nat Genet 1996; 14: 334-36.
5. Humbert R, Adler DA, Disteche CM, Hassett C, Omiecinski CJ, Furlong CE. The molecular basis for the human serum paraoxonase activity polymorphism. Nat Genet 1993; 3: 73-76.
Contributors N Cherry, A Povey, M Mackness, P Durrington and B Mackness designed the study. M and B Mackness directed laboratory work, N Cherry and A Povey did statistical analysis. All authors helped to write the report.
Conflict of interest statement None declared.
Acknowledgments We thank Stuart Thomson, Janet Schofield, Elizabeth Smallshaw, and Caroline Fitzgerald for interviewing participants, and Priscilla Appelbe for coordinating interviews. The study was funded by the UK Health and Safety Executive (3837/R79.002). The study sponsor had no role in design, data collection, data analysis, data interpretation, or in writing of the report.
Centre for Occupational and Environmental Health, University of Manchester, Manchester M13 9PL, UK (Prof N Cherry MD, A Povey PhD, M Dippnall BSc, T Smith MB); and Department of Medicine, Manchester Royal Infirmary, Manchester (M Mackness PhD, Prof P Durrington MD, B Mackness PhD)
Correspondence to: Prof Nicola Cherry (e-mail:[email protected])
99
Appendix 23 Second published paper (Pharmacogenetics 2003;13:81-88)
PARAOXONASE AND SUSCEPTIBILITY TO ORGANOPHOSPHORUS POISONING IN FARMERS DIPPING SHEEP
Bharti Mackness PhD1,3, Paul Durrington FMedSci1, Andrew Povey PhD2, Stuart Thomson Dip HSW2, Martin Dippnall BSc2, Mike Mackness PhD1, Ted Smith
MB2 and Nicola Cherry MD2,
1 University Department of Medicine Manchester Royal Infirmary Oxford RoadManchester M13 9WL UK
2 Centre for Occupational and Environmental Health University of Manchester Manchester M13 9PT UK
3 Corresponding author Tel: +44 161 276 8633and reprint requests to:- Fax: +44 161 274 4833
Email: [email protected]
KEY-WORDS: Paraoxonase, Polymorphisms, Diazoxon, Organophosphate, Exposure
The study was funded by the UK Health and Safety Executive (2827/R79.002).
100

ABSTRACT
Objectives Human serum paraoxonase (PON1) hydrolyses organophosphate pesticides (OPs) entering the blood circulation and tissue fluid thus limiting toxicity. The PON1 coding region has two polymorphisms involving the amino acids at position 55 (L→M) and 192 (Q→R), giving rise to isoenzymes which differ in their catalytic rate for the hydrolysis of OPs. We therefore hypothesised that individuals inheriting low activity isoforms of PON1 would be more liable to report symptoms of OP toxicity.
Methods We have therefore investigated the relationship between PON1 genetic polymorphisms and PON1 activity in farmers reporting chronic ill-health which they attributed to OP exposure whilst sheep dipping (cases) and farmers who carried out similar activities, but remained well (controls). Diazoxon, paraoxon and phenylacetate were used as substrates for PON1. Diazoxon is the active metabolite of diazinon, the sheep dip most commonly used in the UK.
Results Cases were found to be more likely to have the R192 allele (P<0.01) and to have the L55 allele (P<0.05) than the controls. This combination of R and L genotypes was associated with lower PON1 activity towards diazoxon in both cases and controls. Farmers in the lowest quintile for the rate of serum diazoxon hydrolysis had a greater risk of being a case i.e. of reporting ill-health (odds ratio 2.47 (95% CI 1.35-2.82), than the other four quintiles of diazoxon hydrolysis. The rate of serum hydrolysis of paraoxon was greatest in cases and controls with the R/L haplotype (both P<0.001).
Conclusions The farmers reporting chronic ill-health due to organophosphate exposure have a higher proportion of the PON1-192R polymorphism associated with lower rates of diazoxon hydrolysis and lower rates of diazoxon hydrolysis than the controls and that their ill-health may be explained by a lower ability to detoxify diazoxon.
101
INTRODUCTION
Organophosphorus compounds are widely used as agricultural pesticides [1]. The acute effects of exposure to organophosphates (OPs) include miosis, bradycardia, bronchoconstriction, hypoventilation and paralysis. OP poisoning results in many thousands of deaths each year [2]. However, the contribution to the development of chronic ill health of persistent exposure to quantities of OP insufficient to cause acute toxicity has been controversial. A recent report for the UK Department of Health concluded that the evidence for chronic ill-health due to the effects of repeated low level exposure was inconclusive [3]. None the less workers, who have been occupationally exposed to OPs, particularly in sheep dipping, and have subsequently developed chronic illness firmly believe that OPs have caused their condition. Previous studies of sheep dippers have involved workers still actively farming and excluded those no longer able to farm, and thus have not addressed directly whether OP exposure is a cause of chronic disease [4-6].
If serious ill health does occur in some sheep farmers exposed to OPs this might be because of repeated exceptionally high exposure (for example, work practices that did not protect from exposure) or from some particular susceptibility (for example, a reduced ability to detoxify organophosphates) or a combination of both.
Serum paraoxonase (E.C. 3.1.8.1, PON1) hydrolyses a wide variety of substrates including OPs, arylesters, lipid hydroperoxides and lactones and appears to have a role in the development of such diverse diseases as atherosclerosis and perhaps microvascular disease in diabetes mellitus and Parkinson’s disease as well as in acute OP toxicity [7].
The hydrolysis of OP pesticides by PON1 is a major determinant of their toxicity to vertebrates, including man [8-13]. In PON1 knock-out mice, the absence of the PON1 gene results in rapid death on exposure to OPs in doses sublethal to wild-type mice [14]. In the human there is considerable individual variation in the serum activity of PON1 and this is partly genetically determined [8,11-13]. Two genetic polymorphisms due to amino-acid substitutions at positions 55 (L→M) and 192 (Q→R) result in PON1 isoenzymes, which differ greatly in their activity towards various substrates [13,15-17]. The effect of the 192 polymorphism on OP hydrolysis depends upon the nature of the OP substrate [18]. Diazoxon, the toxic metabolite of diazinon, an OP widely used in sheep dip in the UK, is metabolised more slowly by the R alloenzyme, whereas other OPs, such as paraoxon, are metabolised more slowly by the Q alloenzyme [16]. While such differences in OP hydrolysis, which might lead to differential susceptibility to OP toxicity, have been suggested as a reason for ill health in those presumed to have been exposed to OPs, for example in the Gulf War [19], information from systematic studies of people with verified exposure has until now been lacking.
A preliminary report of the present study revealed that the PON1 R and L alleles were associated with self-reported ill-health in sheep farmers [20]. The present investigation extends the observation by demonstrating the effect of the PON1 polymorphisms both on self-reported ill health and on serum PON1 activity towards three representative substrates; phenylacetate and paraoxon, which are well-known PON1 substrates (paraoxonase is so called because of its ability to hydrolyse paraoxon) and diazoxon, the active metabolite of the most frequently used OP in sheep dipping in the UK, diazinon. PON1 192 polymorphic isoenzymes have
102
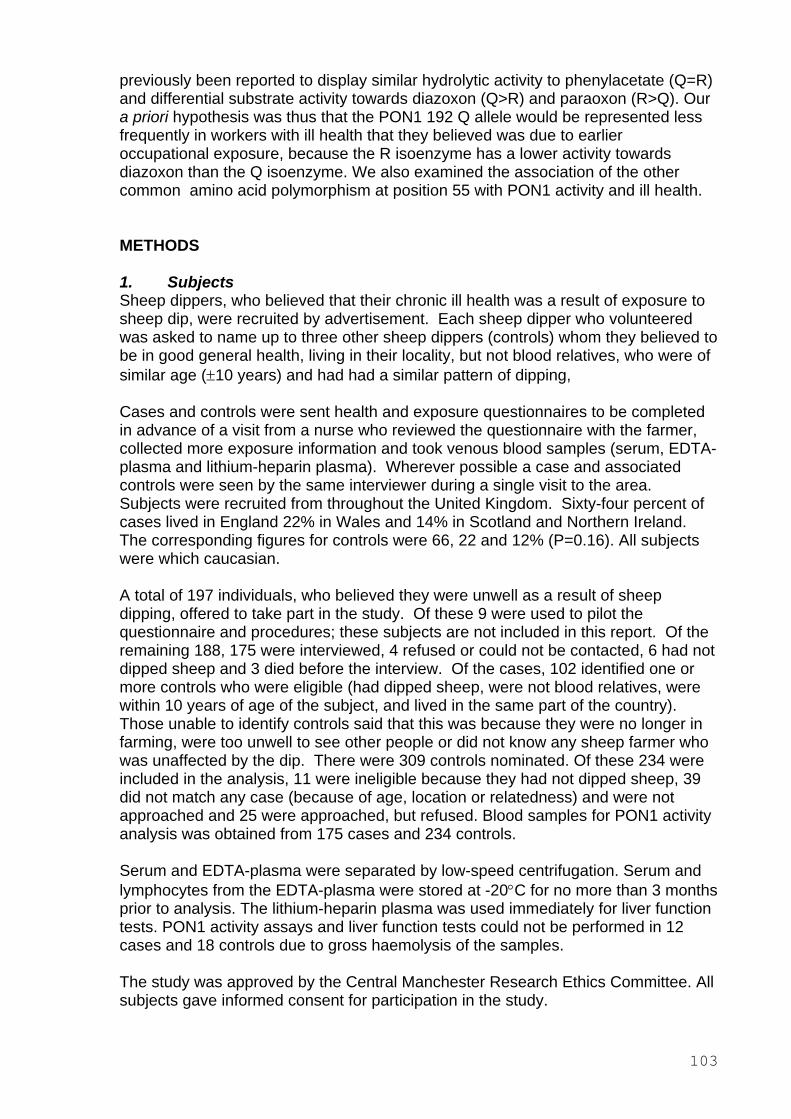
previously been reported to display similar hydrolytic activity to phenylacetate (Q=R) and differential substrate activity towards diazoxon (Q>R) and paraoxon (R>Q). Our a priori hypothesis was thus that the PON1 192 Q allele would be represented less frequently in workers with ill health that they believed was due to earlier occupational exposure, because the R isoenzyme has a lower activity towards diazoxon than the Q isoenzyme. We also examined the association of the other common amino acid polymorphism at position 55 with PON1 activity and ill health.
METHODS
1. Subjects Sheep dippers, who believed that their chronic ill health was a result of exposure to sheep dip, were recruited by advertisement. Each sheep dipper who volunteered was asked to name up to three other sheep dippers (controls) whom they believed to be in good general health, living in their locality, but not blood relatives, who were of similar age (±10 years) and had had a similar pattern of dipping,
Cases and controls were sent health and exposure questionnaires to be completed in advance of a visit from a nurse who reviewed the questionnaire with the farmer, collected more exposure information and took venous blood samples (serum, EDTA-plasma and lithium-heparin plasma). Wherever possible a case and associated controls were seen by the same interviewer during a single visit to the area. Subjects were recruited from throughout the United Kingdom. Sixty-four percent of cases lived in England 22% in Wales and 14% in Scotland and Northern Ireland. The corresponding figures for controls were 66, 22 and 12% (P=0.16). All subjects were which caucasian.
A total of 197 individuals, who believed they were unwell as a result of sheep dipping, offered to take part in the study. Of these 9 were used to pilot the questionnaire and procedures; these subjects are not included in this report. Of the remaining 188, 175 were interviewed, 4 refused or could not be contacted, 6 had not dipped sheep and 3 died before the interview. Of the cases, 102 identified one or more controls who were eligible (had dipped sheep, were not blood relatives, were within 10 years of age of the subject, and lived in the same part of the country). Those unable to identify controls said that this was because they were no longer in farming, were too unwell to see other people or did not know any sheep farmer who was unaffected by the dip. There were 309 controls nominated. Of these 234 were included in the analysis, 11 were ineligible because they had not dipped sheep, 39 did not match any case (because of age, location or relatedness) and were not approached and 25 were approached, but refused. Blood samples for PON1 activity analysis was obtained from 175 cases and 234 controls.
Serum and EDTA-plasma were separated by low-speed centrifugation. Serum and lymphocytes from the EDTA-plasma were stored at -20°C for no more than 3 months prior to analysis. The lithium-heparin plasma was used immediately for liver function tests. PON1 activity assays and liver function tests could not be performed in 12 cases and 18 controls due to gross haemolysis of the samples.
The study was approved by the Central Manchester Research Ethics Committee. All subjects gave informed consent for participation in the study.
103
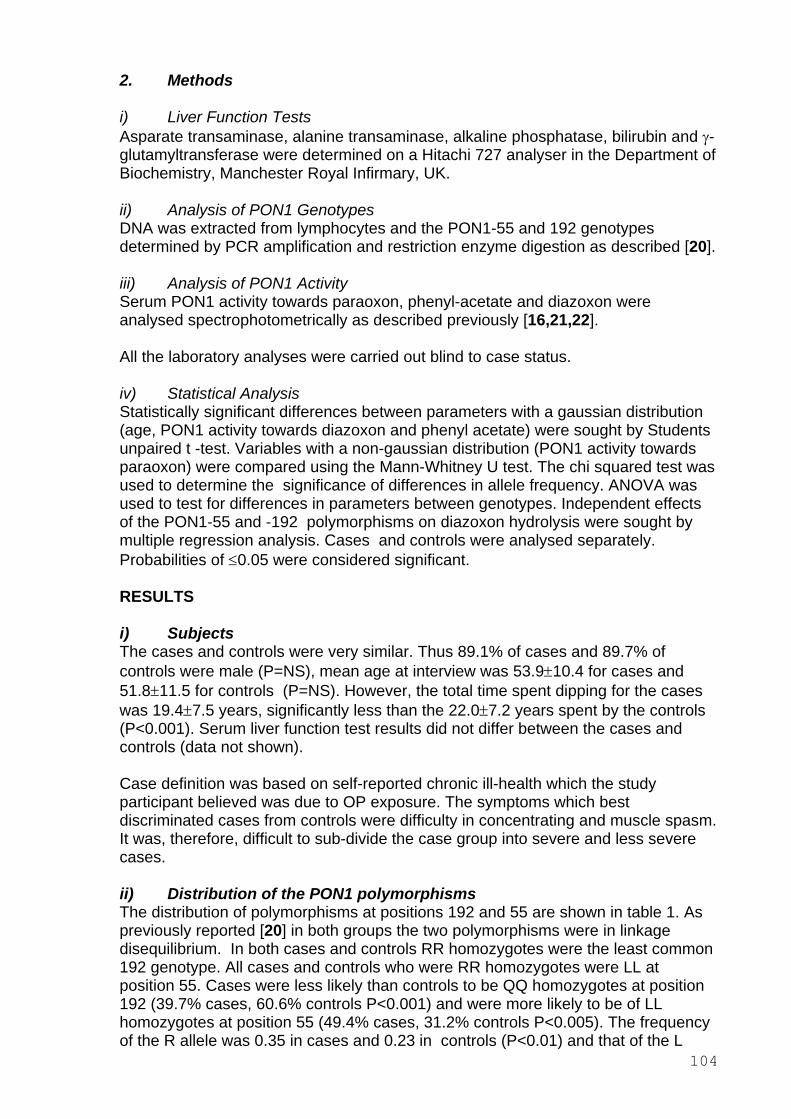
2. Methods
i) Liver Function Tests Asparate transaminase, alanine transaminase, alkaline phosphatase, bilirubin and γ-glutamyltransferase were determined on a Hitachi 727 analyser in the Department of Biochemistry, Manchester Royal Infirmary, UK.
ii) Analysis of PON1 Genotypes DNA was extracted from lymphocytes and the PON1-55 and 192 genotypes determined by PCR amplification and restriction enzyme digestion as described [20].
iii) Analysis of PON1 Activity Serum PON1 activity towards paraoxon, phenyl-acetate and diazoxon were analysed spectrophotometrically as described previously [16,21,22].
All the laboratory analyses were carried out blind to case status.
iv) Statistical Analysis Statistically significant differences between parameters with a gaussian distribution (age, PON1 activity towards diazoxon and phenyl acetate) were sought by Students unpaired t -test. Variables with a non-gaussian distribution (PON1 activity towards paraoxon) were compared using the Mann-Whitney U test. The chi squared test was used to determine the significance of differences in allele frequency. ANOVA was used to test for differences in parameters between genotypes. Independent effects of the PON1-55 and -192 polymorphisms on diazoxon hydrolysis were sought by multiple regression analysis. Cases and controls were analysed separately. Probabilities of ≤0.05 were considered significant.
RESULTS
i) Subjects The cases and controls were very similar. Thus 89.1% of cases and 89.7% of controls were male (P=NS), mean age at interview was 53.9±10.4 for cases and 51.8±11.5 for controls (P=NS). However, the total time spent dipping for the cases was 19.4±7.5 years, significantly less than the 22.0±7.2 years spent by the controls (P<0.001). Serum liver function test results did not differ between the cases and controls (data not shown).
Case definition was based on self-reported chronic ill-health which the study participant believed was due to OP exposure. The symptoms which best discriminated cases from controls were difficulty in concentrating and muscle spasm. It was, therefore, difficult to sub-divide the case group into severe and less severe cases.
ii) Distribution of the PON1 polymorphisms The distribution of polymorphisms at positions 192 and 55 are shown in table 1. As previously reported [20] in both groups the two polymorphisms were in linkage disequilibrium. In both cases and controls RR homozygotes were the least common 192 genotype. All cases and controls who were RR homozygotes were LL at position 55. Cases were less likely than controls to be QQ homozygotes at position 192 (39.7% cases, 60.6% controls P<0.001) and were more likely to be of LL homozygotes at position 55 (49.4% cases, 31.2% controls P<0.005). The frequency of the R allele was 0.35 in cases and 0.23 in controls (P<0.01) and that of the L
104
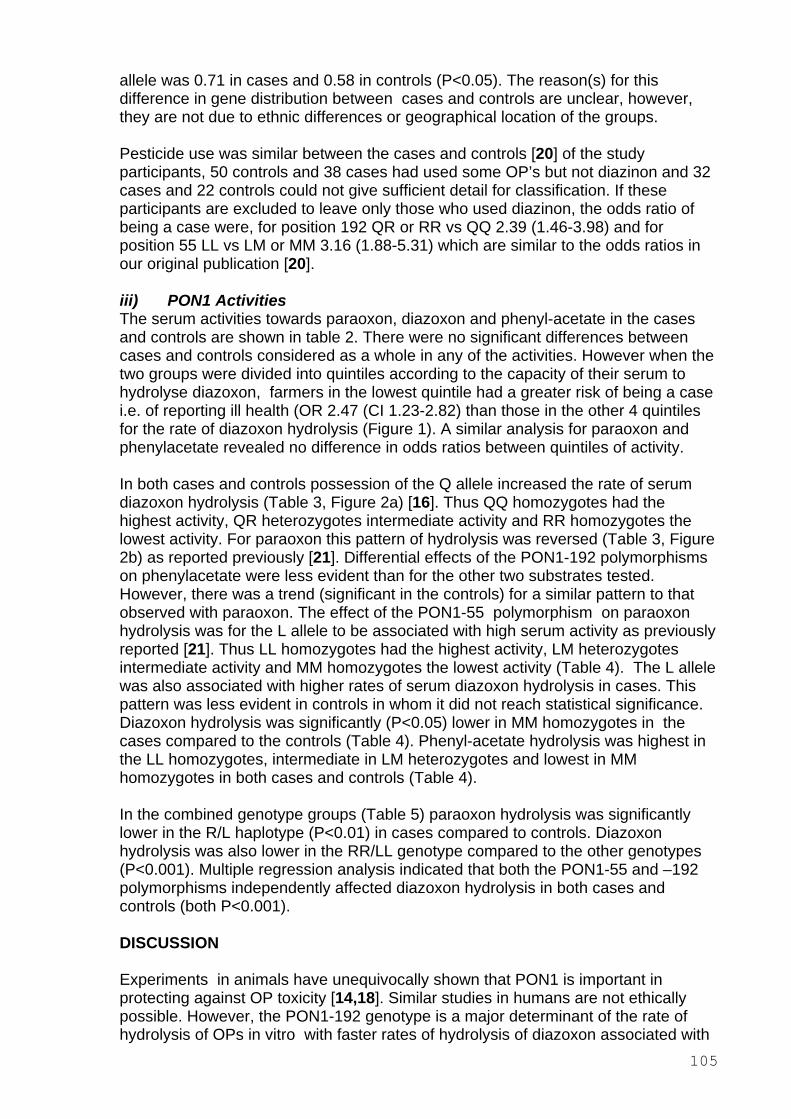
allele was 0.71 in cases and 0.58 in controls (P<0.05). The reason(s) for this difference in gene distribution between cases and controls are unclear, however, they are not due to ethnic differences or geographical location of the groups.
Pesticide use was similar between the cases and controls [20] of the study participants, 50 controls and 38 cases had used some OP’s but not diazinon and 32 cases and 22 controls could not give sufficient detail for classification. If these participants are excluded to leave only those who used diazinon, the odds ratio of being a case were, for position 192 QR or RR vs QQ 2.39 (1.46-3.98) and for position 55 LL vs LM or MM 3.16 (1.88-5.31) which are similar to the odds ratios in our original publication [20].
iii) PON1 Activities The serum activities towards paraoxon, diazoxon and phenyl-acetate in the cases and controls are shown in table 2. There were no significant differences between cases and controls considered as a whole in any of the activities. However when the two groups were divided into quintiles according to the capacity of their serum to hydrolyse diazoxon, farmers in the lowest quintile had a greater risk of being a case i.e. of reporting ill health (OR 2.47 (CI 1.23-2.82) than those in the other 4 quintiles for the rate of diazoxon hydrolysis (Figure 1). A similar analysis for paraoxon and phenylacetate revealed no difference in odds ratios between quintiles of activity.
In both cases and controls possession of the Q allele increased the rate of serum diazoxon hydrolysis (Table 3, Figure 2a) [16]. Thus QQ homozygotes had the highest activity, QR heterozygotes intermediate activity and RR homozygotes the lowest activity. For paraoxon this pattern of hydrolysis was reversed (Table 3, Figure 2b) as reported previously [21]. Differential effects of the PON1-192 polymorphisms on phenylacetate were less evident than for the other two substrates tested. However, there was a trend (significant in the controls) for a similar pattern to that observed with paraoxon. The effect of the PON1-55 polymorphism on paraoxon hydrolysis was for the L allele to be associated with high serum activity as previously reported [21]. Thus LL homozygotes had the highest activity, LM heterozygotes intermediate activity and MM homozygotes the lowest activity (Table 4). The L allele was also associated with higher rates of serum diazoxon hydrolysis in cases. This pattern was less evident in controls in whom it did not reach statistical significance. Diazoxon hydrolysis was significantly (P<0.05) lower in MM homozygotes in the cases compared to the controls (Table 4). Phenyl-acetate hydrolysis was highest in the LL homozygotes, intermediate in LM heterozygotes and lowest in MM homozygotes in both cases and controls (Table 4).
In the combined genotype groups (Table 5) paraoxon hydrolysis was significantly lower in the R/L haplotype (P<0.01) in cases compared to controls. Diazoxon hydrolysis was also lower in the RR/LL genotype compared to the other genotypes (P<0.001). Multiple regression analysis indicated that both the PON1-55 and –192 polymorphisms independently affected diazoxon hydrolysis in both cases and controls (both P<0.001).
DISCUSSION
Experiments in animals have unequivocally shown that PON1 is important in protecting against OP toxicity [14,18]. Similar studies in humans are not ethically possible. However, the PON1-192 genotype is a major determinant of the rate of hydrolysis of OPs in vitro with faster rates of hydrolysis of diazoxon associated with
105
the Q allele [13,15-17] and this has led to speculation that the PON1-192 genotype might be related to the likelihood of OP toxicity in humans [13,15-17]. The PON1-55 polymorphism also affects the capacity of PON1 to hydrolyse OPs in vitro [21]. Those farmers in the lowest quintile of diazoxon hydrolysis were 2.5 times (P<0.05) more likely to report ill health which they attributed to sheep dipping than were those in the highest quintile of diazoxon hydrolysis. Furthermore this susceptibility appeared to be genetic in origin, because farmers reporting chronic ill-health due to sheep dipping also more commonly had R or L PON1 alleles than similarly employed controls who believed themselves to be healthy. Kinetic analysis of the human PON1 isoforms defined by the PON1-192 polymorphism have indicated that the catalytic efficiency (Vmax/km) is the determination of the in vivo efficacy of diazonon detoxication [23].
In our previous preliminary report, those with the genotype combination LL and QR or RR were at greatest risk of reporting ill health [20]. In the present study diazoxon hydrolysis was lower when the R/L haplotype present than with any other genotype combination. Cases with these genotypes had lower activity than controls, but this was not statistically significant. Although the lower PON1 activities in this group could be expected from the relationship between low diazoxon hydrolysis and the risk of having ill health, it could also be argued that they have been further decreased as the result of exposure to OPs. We have recently studied agricultural workers attempting deliberate self-harm by directly ingesting OPs (results unpublished). Whilst their acute OP intoxication resulted in a decrease in PON1 activity, it recovered to normal levels within 6 weeks of acute intoxication. Thus the most conservative interpretation of our finding of a link between genetic susceptibility to diazoxon toxicity and chronic ill health is that exposure to this agent in quantities encountered in its routine use is harmful. Subacute or chronic OP exposure is a plausible explanation for chronic ill health amongst sheep dip workers.
The occurrence of PON1 polymorphisms in the human population is likely to contribute to the survival potential of the species against a wider range of toxic substances than would otherwise be possible. Thus the substrate dependent polymorphism of PON1 may mean that genotypes most likely to confer resistance to diazoxon toxicity may simultaneously confer greater susceptibility to other OPs e.g. individuals carrying the Q and M alleles will be more susceptible to methyl-parathion and fenitrothion toxicity than individuals carrying the R and L alleles.
There are no other studies of similar design to the present one amongst agricultural workers. It has been suggested that Gulf War syndrome could be the result of subacute OP exposure, although the existence of a specific syndrome is controversial and potential explanations legion. None the less in one study UK veterans of the Persian Gulf War who believed they had Gulf War Illness had low PON1 activity to paraoxon [24]. In that study the decrease in PON1 activity was unrelated to either the PON1-55 or -192 genotypes, whereas in another similar study Haley and co-workers reported a preponderance of individuals carrying the Q allele in US veterans with Gulf War Syndrome [25].
In conclusion our results suggest that the PON1 genotype which determines the rate of hydrolysis of diazoxon (and other OPs) is related to illness in farmers reporting chronic ill-health due to the occupational use of OPs.
106

ACKNOWLEDGEMENTS The authors would like to thank Stephanie Middleton for expert technical assistance, Janet Schofield, Elizabeth Smallshaw and Caroline Fitzgerald for interviewing the study participants and Priscilla Appelbe for field work co-ordination.
107
REFERENCES
1. World Health Organisation. Public health impact of pesticides used in agriculture Geneva: WHO 1990.
2. World Health Organisation. Informal consultation on planning strategy for the prevention of pesticide poisoning. Geneva, 25-29 November 1985. WHO/VBC/86.926 Geneva: WHO 1986.
3. Committee on toxicity of chemicals in food, consumer products and the environment. Organophosphates. Department of Health: London 1999.
4. Stephens, R., Spurgeon, A., Calvert, I.A. et al. Neuropsychological effects of long-term exposure to organophosphates in sheep dip. Lancet 1995; 345: 11351139.
5. Rees, H. Exposure to sheep dip and the incidence of acute symptoms in a group of Welsh sheep farmers. Occup. Env. Med. 1996; 53: 258-263.
6. Pilkington, A., Buchanan, D., Jamal, G.A. et al. An epidemiological study of the relationship between exposure to organophosphate pesticides and indices of chronic peripheral neuropathy, and neuropsychological abnormalities in sheep farmers and dippers. Occupational and Environmental Medicine. 2001; 58: 702710.
7. Durrington, P.N., Mackness, B., Mackness, M.I., Paraoxonase and Atherosclerosis. Arterioscler. Thromb. Vasc. Biol. 2001; 21: 473-480.
8. Costa, L.G., Li, W.F., Richter, R.J., Shih, D.M., Lusis, A., Furlong, C.E. The role of paraoxonase (PON1) in detoxication of organophosphates and its human polymorphism. Chem. Biol. Interact. 1999; 119/120: 429-38.
9. Akgür, S.A., Ozturk, P., Sozmen, E.Y., Delen, Y., Tanyalein, T., Eye, B. Paraoxonase and acetylcholinesterase activities in humans exposed to organophosphorus compounds. J. Toxicol. Environ. Health. Part A. 1999; 58: 469-74.
10. Li, W-F., Costa, L.G., Furlong C.E. Serum paraoxonase status: a major factor in determining resistance to organophosphates. J. Toxicol. Environ. Health. 1993; 40: 337-346.
11. La Du, B.N. Human serum paraoxonase/arylesterase. In Pharmacogenetics of Drug Metabolism. W. Kalow, editor. Pergamon Press, New York. 1992; 51-91.
12. La Du, B.N., Billecke, S., Hsu, C., Haley, R.W., Broomfield, C.A. Serum paraoxonase (PON1) isozymes: The quantitative analysis of isozymes effecting individual sensitivity to environmental chemicals. Drug. Metab. Disp. 2001; 29: 566-569.
13. Mackness, B., Durrington, P.N., Mackness, M.I. Human serum paraoxonase. Gen. Pharmac. 1998; 31: 329-336
108
14. Shih, D.M., Gu, L., Xia, Y-R. et al Mice lacking serum paraoxonase are susceptible to organophosphate toxicity and atherosclerosis. Nature. 1998; 394: 284-287.
15. Blatter-Garin, M-C., James, R.W., Dussoix, P. et al. Paraoxonase Polymorphism Met-Leu 54 is associated with modified serum concentrations of the enzyme. J. Clin. Invest. 1997; 99: 62-66
16. Davies, H.G., Richter, R.J., Keifer, M., Broomfield, C.A., Sowalla, J., Furlong, C.E. The effect of the human serum paraoxonase polymorphism is reversed with diazoxon, soman and sarin. Nature Genetics 1996; 14: 334-336.
17. Mackness, M.I., Mackness, B., Durrington, P.N., Connelly, P.W., Hegele, R.A. Paraoxonase: biochemistry, genetics and relationship to plasma lipoproteins. Curr. Opin. Lipidol. 1996; 7: 69-76.
18. Furlong, C.E., Li, W-F., Richter, R.J. et al. Genetic and temporal determinants of pesticide sensitivity: Role of paraoxonase (PON1). Neurotoxicology 2000; 21: 91-100.
19. Haley, R.W., Kurt, T.L. Self-reported exposure to neurotoxic chemical combinations in the Gulf War. A cross-section epidemiologic study. JAMA 1997; 277: 231-237
20. Cherry, N., Mackness, M.I., Durrington, P.N. et al Paraoxonase (PON1) polymorphisms in farmers attributing ill health to sheep dip. Lancet. 2002; 359: 763-764.
21. Mackness, B., Mackness, M.I., Arrol, S., Turkie, W., Durrington, P.N. Effect of the molecular polymorphisms of human paraoxonase (PON1) on the rate of hydrolysis of paraoxon. Br. J. Pharmacol. 1997; 112: 265-268.
22. La Du, B.N., Eckerson, H.W. The polymorphic paraoxonase/arylesterase isozymes of human serum. Fed. Proc. 1984; 43: 2338-2341.
23. Li, W.F., Costa, L.G., Richter, R.J., et al Catalytic efficiency determines the in vivo efficacy of PON1 for detoxifying organophosphorus compounds. Pharmacogenetics. 2000; 10: 767-779.
24. Mackness, B., Durrington, P.N., Mackness, M.I. Low paraoxonase in Persian Gulf War Veterans self-reporting Gulf War Syndrome. Biochem. Biophys. Res. Comms. 2000; 276: 729-733.
25. Haley, R.W., Billecke, S., La Du, B.N. Association of low PON1 type Q (type A) Arylesterase activity with neurologic symptom complexes in Gulf War Veterans. Toxicol. Appl. Pharmacol. 1999; 157: 227-233.
109
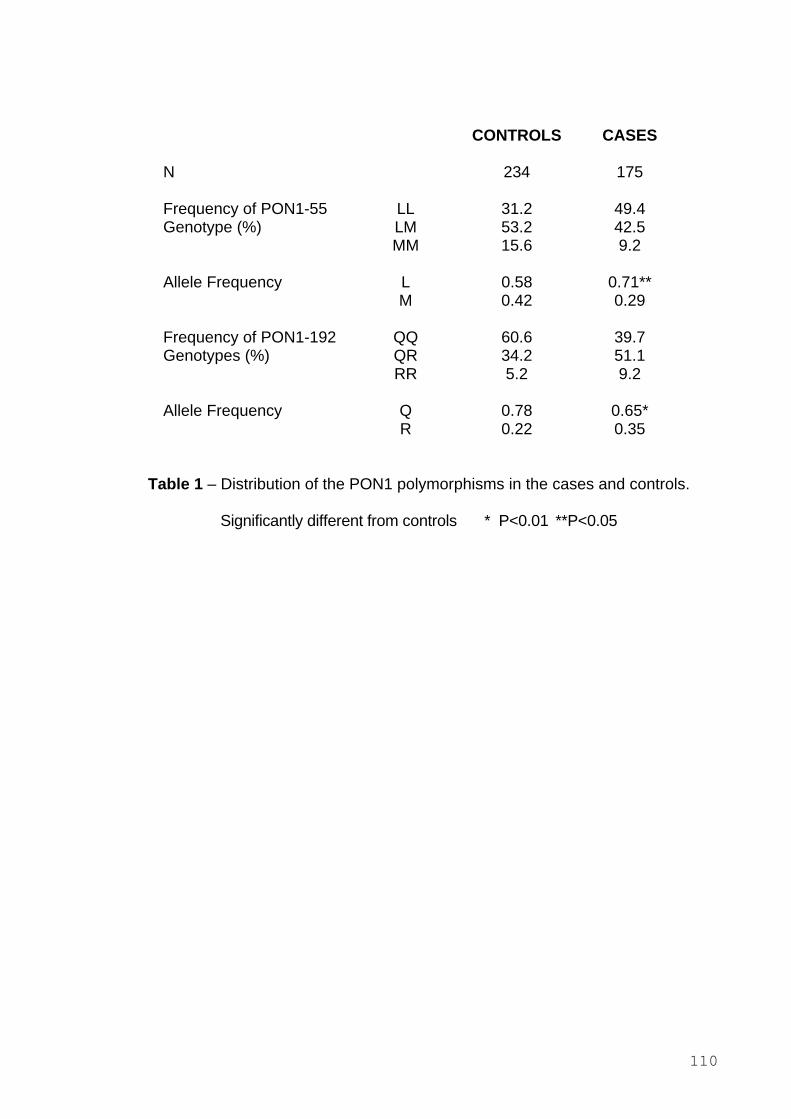
CONTROLS CASES
N 234 175
Frequency of PON1-55 LL 31.2 49.4 Genotype (%) LM 53.2 42.5
MM 15.6 9.2
Allele Frequency L 0.58 0.71** M 0.42 0.29
Frequency of PON1-192 QQ 60.6 39.7 Genotypes (%) QR 34.2 51.1
RR 5.2 9.2
Allele Frequency Q 0.78 0.65* R 0.22 0.35
Table 1 – Distribution of the PON1 polymorphisms in the cases and controls.
Significantly different from controls * P<0.01 **P<0.05
110
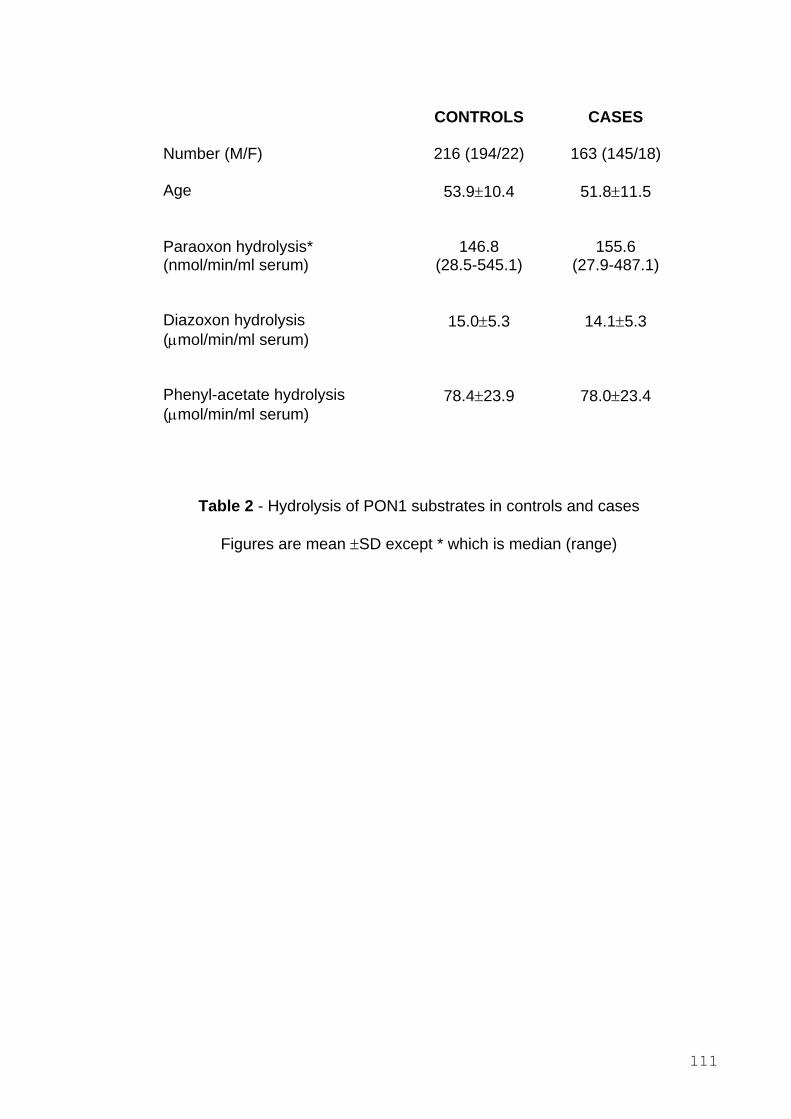
CONTROLS CASES
Number (M/F)
Age
Paraoxon hydrolysis* (nmol/min/ml serum)
Diazoxon hydrolysis (µmol/min/ml serum)
Phenyl-acetate hydrolysis (µmol/min/ml serum)
216 (194/22) 163 (145/18)
53.9±10.4 51.8±11.5
146.8 155.6 (28.5-545.1) (27.9-487.1)
15.0±5.3 14.1±5.3
78.4±23.9 78.0±23.4
Table 2 - Hydrolysis of PON1 substrates in controls and cases
Figures are mean ±SD except * which is median (range)
111
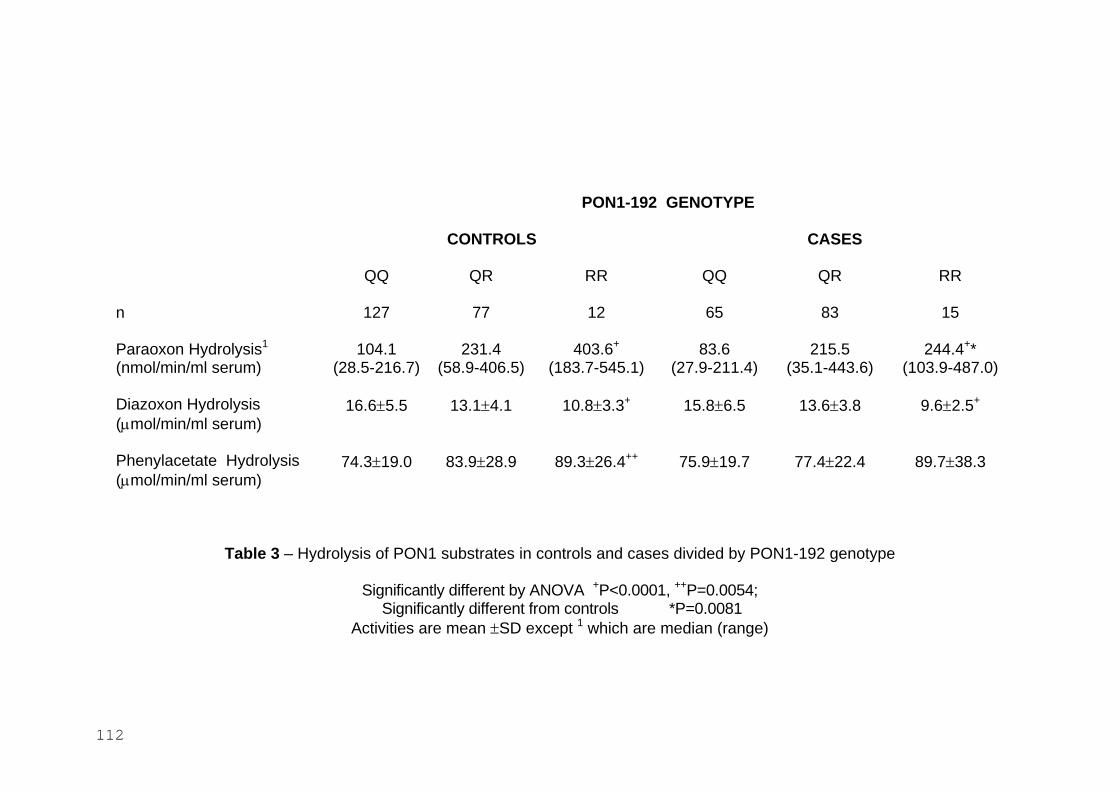
PON1-192 GENOTYPE
CONTROLS CASES
QQ QR RR QQ QR RR
n 127 77 12 65 83 15
Paraoxon Hydrolysis1 104.1 231.4 403.6+ 83.6 215.5 244.4+* (nmol/min/ml serum) (28.5-216.7) (58.9-406.5) (183.7-545.1) (27.9-211.4) (35.1-443.6) (103.9-487.0)
Diazoxon Hydrolysis 16.6±5.5 13.1±4.1 10.8±3.3+ 15.8±6.5 13.6±3.8 9.6±2.5+
(µmol/min/ml serum)
Phenylacetate Hydrolysis 74.3±19.0 83.9±28.9 89.3±26.4++ 75.9±19.7 77.4±22.4 89.7±38.3 (µmol/min/ml serum)
Table 3 – Hydrolysis of PON1 substrates in controls and cases divided by PON1-192 genotype
Significantly different by ANOVA +P<0.0001, ++P=0.0054; Significantly different from controls *P=0.0081
Activities are mean ±SD except 1 which are median (range)
112
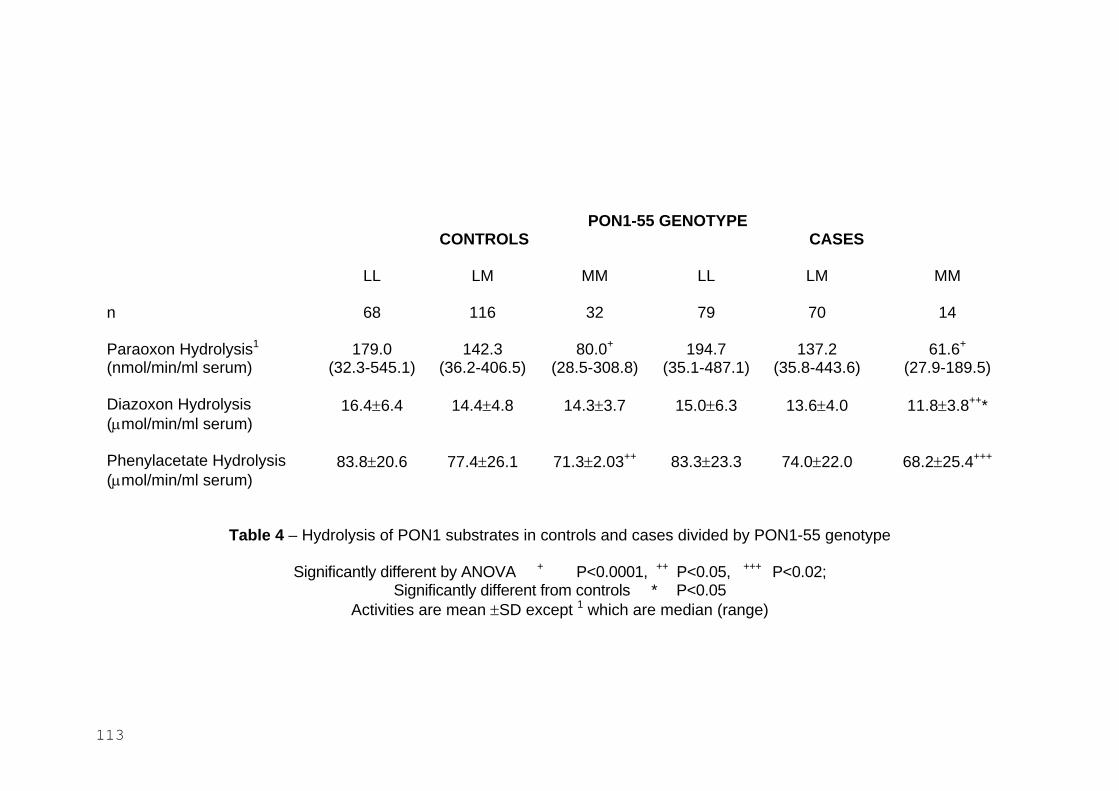
PON1-55 GENOTYPE CONTROLS CASES
LL LM MM LL LM MM
n 68 116 32 79 70
Paraoxon Hydrolysis1 179.0 142.3 80.0+ 194.7 137.2 61.6+
(nmol/min/ml serum) (32.3-545.1) (36.2-406.5) (28.5-308.8) (35.1-487.1) (35.8-443.6) (27.9-189.5)
Diazoxon Hydrolysis 16.4±6.4 14.4±4.8 14.3±3.7 15.0±6.3 13.6±4.0 11.8±3.8++* (µmol/min/ml serum)
Phenylacetate Hydrolysis 83.8±20.6 77.4±26.1 71.3±2.03++ 83.3±23.3 74.0±22.0 68.2±25.4+++
(µmol/min/ml serum)
Table 4 – Hydrolysis of PON1 substrates in controls and cases divided by PON1-55 genotype
+++ Significantly different by ANOVA + P<0.0001, ++ P<0.05, P<0.02; Significantly different from controls * P<0.05
Activities are mean ±SD except 1 which are median (range)
113
14
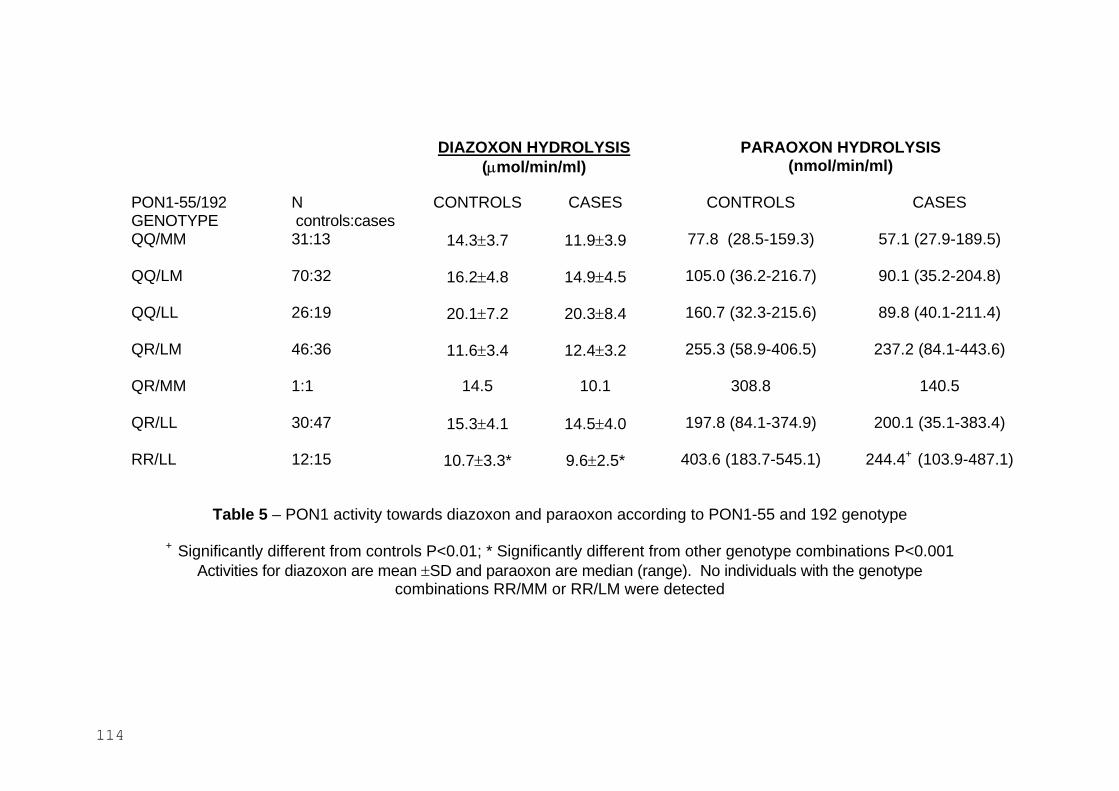
DIAZOXON HYDROLYSIS PARAOXON HYDROLYSIS (µmol/min/ml) (nmol/min/ml)
PON1-55/192 N CONTROLS CASES CONTROLS CASES GENOTYPE controls:cases QQ/MM 31:13 14.3±3.7 11.9±3.9 77.8 (28.5-159.3) 57.1 (27.9-189.5)
QQ/LM 70:32 16.2±4.8 14.9±4.5 105.0 (36.2-216.7) 90.1 (35.2-204.8)
QQ/LL 26:19 20.1±7.2 20.3±8.4 160.7 (32.3-215.6) 89.8 (40.1-211.4)
QR/LM 46:36 11.6±3.4 12.4±3.2 255.3 (58.9-406.5) 237.2 (84.1-443.6)
QR/MM 1:1 14.5 10.1 308.8 140.5
QR/LL 30:47 15.3±4.1 14.5±4.0 197.8 (84.1-374.9) 200.1 (35.1-383.4)
RR/LL 12:15 10.7±3.3* 9.6±2.5* 403.6 (183.7-545.1) 244.4+ (103.9-487.1)
Table 5 – PON1 activity towards diazoxon and paraoxon according to PON1-55 and 192 genotype
+ Significantly different from controls P<0.01; * Significantly different from other genotype combinations P<0.001 Activities for diazoxon are mean ±SD and paraoxon are median (range). No individuals with the genotype
combinations RR/MM or RR/LM were detected
114
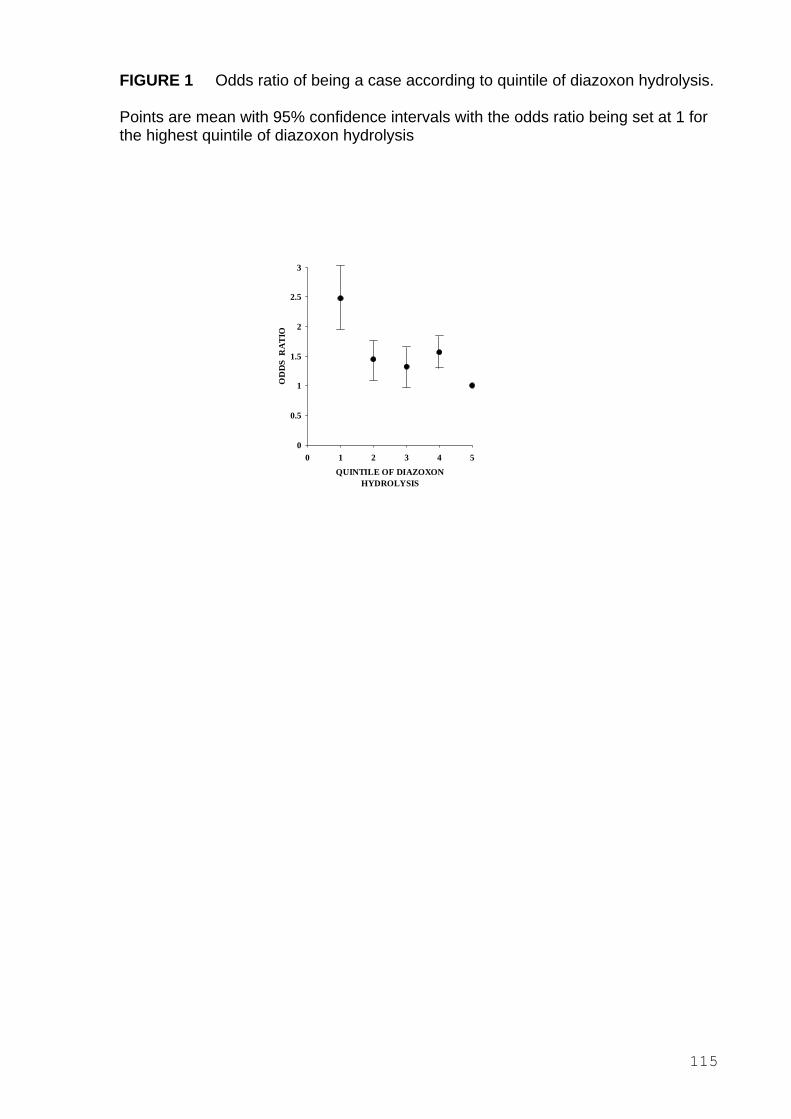
FIGURE 1 Odds ratio of being a case according to quintile of diazoxon hydrolysis.
Points are mean with 95% confidence intervals with the odds ratio being set at 1 for the highest quintile of diazoxon hydrolysis
OD
DS
RA
TIO
3
2.5
2
1.5
1
0.5
0 0 1 2 3 4 5
QUINTILE OF DIAZOXON HYDROLYSIS
115
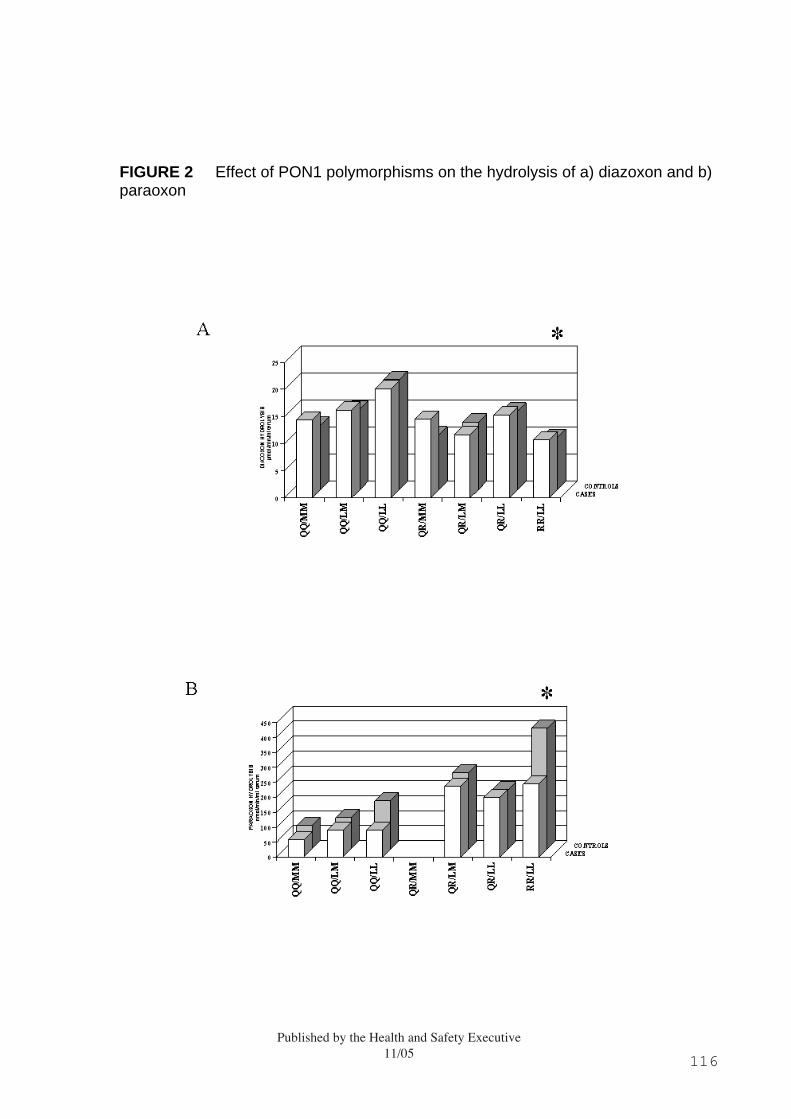
FIGURE 2 Effect of PON1 polymorphisms on the hydrolysis of a) diazoxon and b) paraoxon
Published by the Health and Safety Executive11/05 116
RR 408