Embed Size (px)
Citation preview

YIJOM-2790; No of Pages 8
Research Paper
Trauma
Int. J. Oral Maxillofac. Surg. 2013; xxx: xxx–xxxhttp://dx.doi.org/10.1016/j.ijom.2013.10.008, available online at http://www.sciencedirect.com
In vitro mechanical assessmentof 2.0-mm system three-dimensional miniplates inanterior mandibular fracturesK. P. de Oliveira, P. H. de Moraes, J. S. P. da Silva, W. F. de Queiroz, A. R.Germano: In vitro mechanical assessment of 2.0-mm system three-dimensionalminiplates in anterior mandibular fractures. Int. J. Oral Maxillofac. Surg. 2013; xxx:xxx–xxx. Crown Copyright # 2013 Published by Elsevier Ltd on behalf ofInternational Association of Oral and Maxillofacial Surgeons. All rights reserved.
Abstract. This study constituted a comparative assessment of the mechanicalresistance of square and rectangular 2.0-mm system three-dimensional miniplatesas compared to the standard configuration using two straight miniplates. 90polyurethane replica mandibles were used for the mechanical trials. Groups 1, 2,and 3 simulated complete symphyseal fractures characterized by linear separationof the central incisors; groups 4, 5, and 6 simulated parasymphyseal fractures withan oblique configuration. Groups 1 and 4 represented the standard method with twostraight miniplates set parallel to one another. Square miniplates were used ingroups 2 and 5, and rectangular miniplates in groups 3 and 6. A universal testingmachine set to a velocity of 10 mm/min and delivering a vertical linear load to thefirst left molar was used to test each group. Maximum load values and load valueswith pre-established dislocation of 5 mm were obtained and submitted to statisticalanalysis using a calculated reliability interval of 95%. The mechanicalperformances of the devices were similar, except in the case of rectangular platesused in the parasymphyseal fractures. The innovative fixation methods used showedsignificantly better results in the case of symphyseal fractures.
Please cite this article in press as: de KP, et al. In vitro mechanical assessment of 2.0-mm
anterior mandibular fractures, Int J Oral Maxillofac Surg (2013), http://dx.doi.org/10.101
0901-5027/000001+08 $36.00/0 Crown Copyright # 2013 Published by Elsevier Ltd on behalf of International Associati
K. P. de Oliveira, P. H. de Moraes,J. S. P. da Silva, W. F. de Queiroz,A. R. GermanoDepartment of Oral and Maxillofacial Surgery,Hospital Universitario Onofre Lopes, FederalUniversity of Rio Grande do Norte, Natal, RioGrande do Norte, Brazil
Keywords: internal fracture fixation; mandibu-lar fractures; biomaterial; biomechanics;trauma.
Accepted for publication 8 October 2013
In recent years, different methods havebeen proposed for the surgical treatmentof mandibular fractures. Rigid internalfixation (RIF) is used to achieve a stableanatomical reduction, thereby reducingthe risk of postoperative displacement offractured bone fragments, avoiding theneed for maxillomandibular fixation1,2
and favouring an early return to normalfunctioning.3,4
The mandible is subject to forces gen-erated by the chewing muscles transmittedvia the teeth and the temporomandibularjoints. During treatment, tensions anddeformations occur according to the dis-tribution of the external forces and theproperties and geometry of the materialbeing used.5 It is well known that themandible is normally subjected to tension-ing forces on its superior border and com-
pression forces on its inferior border.5–8
However, that is only true for fractures inthe body and angle of the mandible; in thecase of fractures in the symphyseal andparasymphyseal regions, the oppositesituation prevails and a single form ofbiomechanical behaviour can be expectedfor this latter region as a whole.6
Irrespective of the fixation method used,stability is a key factor for the successful
system three-dimensional miniplates in
6/j.ijom.2013.10.008
on of Oral and Maxillofacial Surgeons. All rights reserved.

2 de Oliveira et al.
YIJOM-2790; No of Pages 8
treatment of the symphyseal fracture.9,10
This can be evaluated by mechanical teststhat simulate the forces that the mandib-ular fractures will be subjected to, makingit possible to determine the resistance ofthe fixation material and the behaviour ofthe fractured region.4
The symphysis is one of the most com-mon mandibular fracture sites, withreports of prevalence varying from 9%to 57%; it is only surpassed by fracturesof the condyle or of the angle.5–9 Eachmandibular region has its own peculiari-ties, including variations in the forcesexerted by the chewing muscles, zonesof fragility, and the possible presence ofmechanical forces acting in differentdirections. These factors determine theextent of a region’s susceptibility totrauma and its propensity for a favourableresponse to treatment.5,11
Recent work done by Madsen et al.6 andby Oliveira and Passeri4 has involved thecomparative biomechanical assessment ofdifferent fixation techniques applied tosymphyseal and parasymphyseal mandib-ular fractures, but they did not make use ofthree-dimensional (3D) fixations.
Farmand11, who was the first to under-take a biomechanical investigation of 3Dplates in 1996, studied the performance ofa plate in the shape of the four sides of asquare open in the middle. In his view, thedevice, which was fixed by screws, wouldfoster stability in three dimensions, and itsbiomechanical characteristics were com-parable to those of conventional mini-plates. The open-centred squareconfiguration would be the smallest pos-sible one for a 3D plate component. In thatstudy, the clinical results and investiga-tions showed that 3D plates provided goodstability during osteosynthesis associatedwith more complicated cases of mandib-ular fracture. The author also stated thatthe 1-mm profile of the connecting arms ofthe device made its adaptation to the bonewithout distortions easier, and that theuntrammelled areas between the connect-ing arms ensured a good blood supply tothe bone.
In spite of the small number of in vitrostudies using 3D plates in fractures in theanterior region of the mandible, there aresome authors who have reported the effi-cacy of the method. In two clinical studies,Jain et al. demonstrated the effectivenessof 3D miniplates for fixation in the treat-ment of mandibular fractures in thatregion and analysed their advantagesand disadvantages over a 2-month fol-low-up period. In the configuration usedin their work, the material used proved tobe less costly and readily adaptable, as
Please cite this article in press as: de KP, e
anterior mandibular fractures, Int J Oral M
well as reducing the operation time andproviding greater stability.12,13
While there have been some investiga-tions using 3D plates as the fixationmethod, there is no scientific evidenceconcerning their use in the symphysis/parasymphysis region.4,6,14–17 Thus thepresent work was undertaken to performa laboratory evaluation of the resistanceand performance of square and rectangular2.0-mm system 3D miniplates used tostabilize fractures in the anterior regionof the mandible, as compared to the per-formance of standard pattern plates,namely two straight plates also of the2.0-mm (screw diameter) system.
Materials and methods
For the purposes of this study, two rigidpolyurethane mandible models with com-plete sets of teeth were prepared (NacionalOssos, Jau, Sao Paulo, Brazil) and twodifferent ‘fractures’ in the form of cutswere made in them using a metal disc atlow speed rotation. The ‘osteotomies’simulated symphyseal and parasymphy-seal fractures. The simulated symphysealfracture consisted of a linear cut in thecentre of the mandible, from between themedian incisors down to the basal part ofthe mandible. The parasymphyseal frac-ture was represented by an oblique cutoriginating between the median incisorsand going down in a slightly posteriordirection to the base of the mandible onthe right side. The two models were sent tothe model company, which then produced90 standardized replicas, 45 for each typeof ‘fracture’.
Four hundred and eighty titanium–alu-minium–vanadium alloy (Ti–6Al–V)screws (PROMM, Industria de MateriaisCirurgicos, Porto Alegre, Rio Grande doSul, Brazil) were used, of which 240 were6 mm long and 240 were 12 mm long, allcompatible with the 2.0-mm system. 120miniplates were used as follows: 60straight four-hole miniplates that are thestandard pattern for the 2.0-mm system, 30square four-hole miniplates, and 30 rec-tangular four-hole miniplates. The squareand rectangular miniplates were designedby the authors and made to order by thesuppliers (PROMM, Industria de Materi-ais Cirurgicos).
Sample preparation
The rigid polyurethane mandibles weredivided into six groups of 15 mandibleseach for mechanical trials in accordancewith a statistical design obtained using aprogramme for sample size determination
t al. In vitro mechanical assessment of 2.0-mm
axillofac Surg (2013), http://dx.doi.org/10.101
(Diman 1.0); the confidence intervalestablished was 95%.
The mandibular fractures in the replicasof groups 1 and 4 were stabilized usingtwo straight four-hole miniplates of the 2-mm system on each. These were fixed inparallel, one in the superior position andthe other in an inferior position, with caretaken so that the superior plates werealways lower than the level of the dentalroot apices. These two groups were con-sidered to be the standard pattern or con-trol groups. Fixation in groups 2 and 5used square miniplates, and in groups 3and 6, rectangular miniplates were used.Each square and rectangular miniplate wasstabilized with four screws (Figs. 1–3). Inall groups, the screws that were nearest tothe dental apices were 6 mm long, whilethose inserted near the inferior border ofthe mandible were 12 mm long.
The three different fixation methodswere used on both types of fracture, i.e.,on the linear fracture (symphyseal) and theoblique fracture (parasymphyseal). Thesymphyseal fracture was present in groups1, 2, and 3, and the parasymphyseal frac-ture in groups 4, 5, and 6.
To ensure uniformity in the miniplatepositioning, each one was pre-moulded tothe surface of the fractured mandible usingspecific bending tools and a standardizedtemplate, thereby diminishing the possi-bility of alterations among them that mightresult from manual preparation of thesamples.
At the time of miniplate fastening, thehemi-mandible was stabilized using dropsof prefabricated self-polymerizing resinand the miniplates positioned to makeperforation possible. The same operatorcarried out all perforations.
Mechanical testing
The equipment used for load testing wasthe Autograph AG-X 300 kN model of theShimadzu Universal Mechanical TestingMachine (Shimadzu Corporation,Chiyoda, Tokyo, Japan).
For testing purposes, a specificallydesigned clamp was constructed to stabi-lize the polyurethane mandible during theapplication of the test loads (Fig. 4). Thisclamp was perfectly adapted to tightlyhold the posterior region of the rightmandible, accommodating the border ofthe ramus from the angle to the condyle.To make testing feasible, a metal rod wasprepared and adapted to the universaltesting machine in such a way that thepoint of application of the test loads wasaligned with the central fossa of the firstleft molar (Fig. 5).
system three-dimensional miniplates in
6/j.ijom.2013.10.008

Mechanical assessment of 3D miniplates 3
YIJOM-2790; No of Pages 8
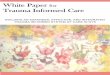
Fig. 1. (a) Group 1: symphyseal fracture, straight miniplates. (b) Group 4: parasymphyseal fracture, straight miniplates.
Fig. 2. (a) Group 2: symphyseal fracture, square miniplate. (b) Group 5: parasymphyseal fracture, square miniplate.
The velocity of the load test was cali-brated at 10 mm/min on the basis of theresults of pilot studies experimentingwith various velocities, and the testwas orientated by the protocol used byOliveira and Passeri.4 Two readings wereobtained, one at the moment that themetal rod attained a displacement of5 mm under the constant load appliedto the system at the pre-established
Please cite this article in press as: de KP, e
anterior mandibular fractures, Int J Oral M
Fig. 3. (a) Group 3: symphyseal fracture, rectan
velocity, and the other was taken whenthe maximum load that the system couldresist was attained. Values were regis-tered in Newtons (N).
Statistical analysis
After the average of the load readings at5 mm displacement of the rod and atmaximum load had been obtained for
t al. In vitro mechanical assessment of 2.0-mm
axillofac Surg (2013), http://dx.doi.org/10.101
gular miniplate. (b) Group 6: parasymphyseal f
all the study groups, the data weresubjected to statistical analysis for quan-titative and comparative purposes. Thedata were also analysed after groupingby type of simulated fracture cut. SPSSsoftware was used for the analysis(SPSS version 19 for Windows; IBMCorp., Armonk, NY, USA), and the cal-culated confidence interval was 95%(95% CI).
system three-dimensional miniplates in
6/j.ijom.2013.10.008
racture, rectangular miniplate.

4 de Oliveira et al.
YIJOM-2790; No of Pages 8
Fig. 4. (a) Device developed for the study, before sample positioning; and (b) its adaptation inthe universal testing machine.
Results
Load readings in Newtons were obtainedfor each sample in the symphyseal andparasymphyseal fracture groups at the
Please cite this article in press as: de KP, e
anterior mandibular fractures, Int J Oral M
Fig. 5. Rod in position at the beginning of the
moment that rod displacement reachedthe 5 mm mark.
For the symphyseal fractures, nostatistically significant differences wereobserved in the average values and the
t al. In vitro mechanical assessment of 2.0-mm
axillofac Surg (2013), http://dx.doi.org/10.101
load test.
standard deviations among the differenttypes of fixation used. At that predeter-mined moment of displacement, the high-est average value was obtained by group 1(straight miniplates), followed by groups 2(square miniplate) and 3 (rectangularminiplate), respectively (Table 1).
In the case of the parasymphyseal frac-tures, there was no statistically significantdifference between groups 4 (straightminiplates) and 5 (square miniplate).However the value in group 6 (rectangularminiplate) was significantly lower than ingroups 4 and 5 (Table 2).
Next, the maximum load values (N)were obtained for the moment when thesystem still supported the load, but beyondwhich its resistance started to decreaseshowing that fixation failure had occurred.
In the case of the symphyseal fractures,the average values and the standard devia-tion values for maximum load showed thatthe maximum force attained and applied tothe system was higher in group 1 (thestandard or control group) than in groups2 and 3. However, there were no statisti-cally significant differences betweengroups 2 and 3 and the control group(Table 3).
In the case of the parasymphyseal frac-tures, the highest load resistance figurewas obtained for group 4 (the controlgroup), followed by group 5 and group6. The difference between group 4 andgroup 5 was not statistically significant;however, the maximum load in group 6was significantly lower than that in group4. There was no statistically significantdifference between group 5 and group 6figures in this respect (Table 4).
When the two fracture groups (sym-physeal vs. parasymphyseal) were com-pared, the maximum registered forcesupported by the system was foundfor the symphyseal fractures. The differ-ence in maximum force measurementsbetween the symphysis and parasymphy-sis groups was statistically significant(Table 5).
Discussion
In vitro tests have been carried out todescribe the biomechanical behaviourof supporting devices in a bid to validatethe various modes of fixation.4,6,18–25
Although scientific research has been car-ried out to assess the biomechanical per-formance of the different fixation methodsused in oral and maxillofacial trauma,there has been far less attention paid tofixation of the mandibular symphysis, andthis is true even for the use of 3D fixationdevices in that region.
system three-dimensional miniplates in
6/j.ijom.2013.10.008

Mechanical assessment of 3D miniplates 5
YIJOM-2790; No of Pages 8
Table 1. Force measurements at 5 mm displacement: symphyseal fracture.
Group No. Average SD Median Min Max 95% CI
G1 15 16.22 3.54 17.17 6.05 20.60 14.26–18.18G2 15 15.32 3.20 16.50 7.68 19.79 13.54–17.09G3 15 13.85 1.18 13.45 11.92 16.16 13.20–14.51
G1, straight miniplates; G2, square miniplate; G3, rectangular miniplate; SD, standard devia-tion; CI, confidence interval.
Table 2. Force measurements at 5 mm displacement: parasymphyseal fracture.
Group No. Average SD Median Min Max 95% CI
G4 15 12.48a 2.19 12.49 7.20 16.83 11.27–13.70G5 15 12.59a 3.19 11.54 7.68 18.50 10.82–14.36G6 15 9.10b 2.09 9.30 3.62 11.54 7.94–10.25
G4, straight miniplates; G5, square miniplate; G6, rectangular miniplate; SD, standard devia-tion; CI, confidence interval.a,bDifferences between the results marked with the letters ‘a’ and ‘b’ are statistically significant.Statistical testing was based on the calculated 95% CI.
Table 3. Maximum force measurements for the groups with symphyseal fractures.
Group No. Average SD Median Min Max 95% CI
G1 15 26.88 5.42 27.13 12.02 35.38 23.88–29.89G2 15 22.24 4.09 22.89 15.35 29.04 19.97–24.51G3 15 22.86 2.26 22.79 19.17 28.32 21.61–24.11
G1, straight miniplates; G2, square miniplate; G3, rectangular miniplate; SD, standard devia-tion; CI, confidence interval.
Anatomically accurate models used astest specimens can effectively simulatephysiological conditions.23 In the caseof polyurethane, its modulus of elasticity,an important factor in choosing this typeof material, is very similar to that of bonystructures, thereby justifying its use inbiomechanical testing. It has a value forthis modulus of around 0.07 GPa, whichplaces it within the range of valuesobtained for human bone: Cordey20
reported values ranging from less than0.1 GPa in bone marrow to 2 GPa in cor-tical bone tissue.
Please cite this article in press as: de KP, e
anterior mandibular fractures, Int J Oral M
Table 4. Maximum force measurements for the
Group No. Average SD M
G4 15 19.53a 3.50 20G5 15 17.34a,b 4.80 16G6 15 15.30b 3.12 15
G4, straight miniplates; G5, square miniplate; Gtion; CI, confidence interval.a,bDifferences between the results marked with thStatistical testing was based on the calculated 9
Table 5. Maximum force measurements groupe
Group No. Average SD
Symphysis 45 23.99a 4.54
Parasymphysis 45 17.39b 4.17
SD, standard deviation; CI, confidence interval.a,bDifference is statistically significant. Statistica
The force mechanisms involved inchewing and the forces experienced bythe bones involved are highly complex.19
Axial loads are those that produce com-pression forces or tensions in a struc-ture.20,26 They act at points of contactthat may serve as a screen or friction zoneand consequently they may be influentialin inducing rotation or displacement.19 Ina clinical situation, it is important to beaware that effects of bending forces are farmore important than those of axial forces.
The third type of force involved istorque, which produces or tends to pro-
t al. In vitro mechanical assessment of 2.0-mm
axillofac Surg (2013), http://dx.doi.org/10.101
groups with parasymphyseal fractures.
edian Min Max 95% CI
.50 12.35 27.23 17.59–21.47
.59 9.35 25.27 14.68–20.00
.69 8.10 19.17 13.57–17.03
6, rectangular miniplate; SD, standard devia-
e letters ‘a’ and ‘b’ are statistically significant.5% CI.
d by the two types of fracture.
Median Min Max 95% CI
23.70 12.02 35.38 22.63–25.3617.69 8.10 27.23 16.17–18.64
l testing was based on the calculated 95% CI.
duce rotation or twisting.20 It is knownthat bone is normally subject to tensionforces on its upper border and compres-sion forces on its lower border.6,8,17,24
However, that is only true for fracturesin the body and angle of the mandible, andin the case of symphyseal and parasym-physeal fractures, the opposite situationprevails. Thus a complex form of biome-chanical behaviour can be expected for theregion as a whole.3,6
According to research conducted byTams et al.25, the symphyseal region hasone of the highest negative moments offorce (defined as being the reduction inthe distance between the fragments onthe alveolar border) as compared to othermandibular regions, and this generatesgreat tension at the inferior border andcompression at the superior border. Theseresearchers found little evidence of shearforces in this region, but found thatmoments of force are more intensely pre-sent than in other regions. The same studyreported that moments of flexure (bending)are 1.5 times greater than torque forces inthe anterior region of the mandible.
Research using 3D models has provedthat when loads are applied to chewingpoints in the posterior region of the mand-ible where the molar teeth are located, thegreatest intensity of torque forces is foundin the region of the symphysis. Further-more, studies using 3D models haveshown that the areas of tension and com-pression are not fixed but are liable toalternate with one another.6,18,26–28 Otherstudies evaluating the use of RIF haveapplied the forces to the region of thecentral incisors,29,30 which offers only avery small area of contact, making itdifficult to accommodate the testingdevice and increasing the likelihood ofits slipping from the point of contactand altering the results.19
Our study took heed of the variousrecommendations made by Tamset al.25, who determined the most effectivepositioning of the plates, and took parti-cular care in the case of the superior borderto respect the anatomical limits of thetooth root apices. However, due to theheight of the anterior region of the testspecimens and the fixed standard length ofthe vertical bars of the miniplates, it wasnot possible to insert the 3D devices ontothe bone surface as high up as possible,which would have been more favourablefor neutralizing torque. This means thatideally, to maximize efficiency, plateswith a variety of dimensions should beavailable to the surgeon in order to addressthe anatomical variations that are foundamong individuals being treated.
system three-dimensional miniplates in
6/j.ijom.2013.10.008

6 de Oliveira et al.
YIJOM-2790; No of Pages 8
Up until now there have been very fewreports published in the literature of stu-dies comparing fixations using standardminiplates of the Champy et al.31,32 typeand those using 3D miniplates in the treat-ment of mandibular fractures, to identifytheir respective advantages and disadvan-tages. Square and rectangular miniplatesdo have a disadvantage at the moment ofmoulding to the bone surface, as they haveto be bent in three dimensions, whereas thelinear plates only have to be bent in two. Itis more difficult to get a perfect adaptationwith the 3D plates than with the linearones because they are objects in the formof a plane that need to be adapted to acurved surface and not just an object in theform of a straight line.13 This was corro-borated in the present study.
The advantage of the 3D plates is thatthey provide improved mechanical stabi-lity as compared to the conventional mini-plates, although that additional stabilitymay be lost in the case of oblique frac-tures. The reason for this is that in obliquefractures it is difficult to reconcile all therecommendations for an ideal fixationusing a device that consists of horizontalbars and vertical bars parallel to the frac-ture line13. This may explain the differ-ences in resistance encountered among thefixation devices in this study according tothe type of fracture (Table 5).
The principles and utilization of 3Dminiplates in mandibular fractures havenot yet been fully established. In a recentresearch survey among 104 American andEuropean dental surgeons belonging to theAssociation for Osteosynthesis/Associa-tion for the Study of Internal Fixation(AO/ASIF), only 6% declared that theymade use of such materials for fixation.33
Furthermore, there are no case seriesreports available in the specialized litera-ture and only a small number of publishedstudies investigating their advantages ascompared to traditional plates and mini-plates for bone reconstruction.12,13
With regard to the displacement valueto be adopted, there are authors who havestandardized the use of a displacementvalue of 1 mm,34,35 3 mm,36 and10 mm,19 or the moment when the systemcollapses, if the latter should occur beforethe predetermined displacement is regis-tered.37 Madsen et al.6 used a continuousload right through to the moment ofmechanical failure of the system, or tothe limit of displacement, when evaluatingsymphysis fractures. Vieira e Oliveira andPasseri4 registered resistance values atintervals, or at the limit of predetermineddisplacement. As a simplified form forpresenting the results and to give enough
Please cite this article in press as: de KP, e
anterior mandibular fractures, Int J Oral M
information for the evaluation of multipledata, we adopted a predetermined displa-cement value of 5 mm and used the max-imum load to demonstrate the limits of theresistance each system is capable of.
With regard to the displacement velo-city, different protocols can be found inthe literature, with great variationsbetween them. In research work compar-ing different RIF techniques, Asprino38
and Brasileiro29 proposed the use of adisplacement velocity of 1 mm/min. Tri-vellato37 preferred a velocity of 2 mm/min. In biomechanical studies to evaluatefixations in the anterior region of polyur-ethane mandibles, Madsen et al.6 used avelocity of 5 mm/min to deliver load to theedge of the incisors and 1 mm/min whenapplying load to the left molar region.Oliveira and Passeri4 adopted a predeter-mined displacement velocity of 10 mm/min for the first left molar. The pilot teststhat were carried out on specimens prior tothis study showed greater accuracy whenthe predetermined displacement value of10 mm/min was adopted, hence this valuewas used as the standard in the presentresearch.
The results obtained for the symphysealfracture groups in terms of both the pre-determined 5 mm displacement valuesand the maximum force resisted (Tables1 and 3), underscore the good performanceof the square and rectangular devices usedin comparison to the control group. Theseare therefore viable options for use infractures in that particular region of themandible. With regard to the parasymphy-seal fracture groups, in terms of the 5 mmdisplacement, the results for the rectangu-lar miniplates were significantly differentto those of the control group, which actu-ally registered the highest values of allgroups. The reduced level of resistancedemonstrated by the rectangular plateswhen used in parasymphyseal fracturesmay be related to the oblique configura-tion of the cut (which tends to interferewith the equidistant positioning of theconnecting arms of the miniplates in rela-tion to the slanting trajectory of the cut), tothe lesser number of screws involved, andto the lack of a perfect adaptation of theminiplate to the polyurethane model.
While the load was being applied, theparasymphyseal fractures were those thatsuffered the greatest rotation effects due tothe configuration of the cuts, whichfavoured the axis of movement. Shearand compression forces in the basal regionare less active in oblique cuts than instraight line cuts. This means that the leftmandible side to which the force is appliedundergoes greater and more intense dis-
t al. In vitro mechanical assessment of 2.0-mm
axillofac Surg (2013), http://dx.doi.org/10.101
placement towards the opposite hemi-mandible when the cuts are oblique. Gen-erally speaking, due to such force compo-nents acting in the oblique fracture groups,the tendency to displacement is greaterand the use of fixation systems endowedwith greater rigidity should be considered.What must be remembered, however, isthat this was an in vitro trial and conse-quently subject to certain limitations–there is a need for more intense investiga-tion into the use of 3D plates, especially inthe case of rectangular miniplates.Furthermore, it has already been madeclear that the forces used in biting areconsiderably reduced after mandibularfracture treatment, so it may possiblynot be necessary to employ such very rigidsystems to stabilize fractures during thehealing period.39,40
With 3D plates, the spacing of thescrews means that the loads or forcesacting on the plate are shared by the upperand lower sections of the plate and thisenhances the resistance to rotation gener-ated by torsion forces. In the case of thesquare plates, because the configurationsituates the screws at small distances fromone another and from the geometricalcentre of the plate, the tendency for screwsto lose their hold during the application ofthe test forces is increased. In mechanicalterms, the square format and its screwpositions is less stable than the rectangularformat because its geometry provides lessstability. However, there were no detect-able statistically significant differencesamong these groups in the measurementstaken at maximum force in either of thefracture configurations. A significant dif-ference was only observed in one prede-termined displacement of 5 mm, in whichsituation the square plates were moreeffective in the oblique fractures.
It must be stressed that the greatestdisplacement registered in testing thegroups with fixation based on rectangularminiplates, for both kinds of cut, is causedby the greater deformation they suffer, andthis is especially demonstrated by the factthat in some of the tested samples thescrews did not come out but remainedin place until the limits of miniplate defor-mation had been attained, at which pointthe tip of the vertical rod slipped out of thecentral fossa of the first left molar. Theexplanation for this would be that theenergy provoking deformation stemmingfrom the force being applied and the waythat the system uses that energy in deform-ing the plate, limits the forces that mighteventually displace the screw so that itbecomes an event that takes longer tooccur. From the biomechanical point of
system three-dimensional miniplates in
6/j.ijom.2013.10.008

Mechanical assessment of 3D miniplates 7
YIJOM-2790; No of Pages 8
view, such deformations in the plates areactually beneficial, but only up to the pointwhere they reach the limits of their elas-ticity. Once that point has been passed,they no longer favour fixation stabilitybecause they are unable to go back tonormal once the force has ceased andaccordingly make the fracture reductionand fixation obtained by the treatmentunfeasible.
The fixations showed their best resultsin the symphyseal fractures with differ-ences that were statistically significant.Thus, extrapolating to the clinical situa-tion, we would observe that 3D fixationswith four screws, as tested in the study insymphyseal fractures, would probablyfunction adequately in stabilizing suchfractures, considering that they presenteda good mechanical performance. On theother hand, their loss of performance in theparasymphyseal fractures could minimizethe success of 3D fixations tested in clin-ical situations, especially when the rectan-gular plates are used. The incorporation oftwo more screws in each segment of the3D plates would probably lead to betterresults in fracture stabilization, but in thatcase they would no longer have any clin-ical advantages considering that straightplates mounted in parallel have deliveredgood results for years and they are easierto mould. Another aspect to consider is themodification of the biting force after thetrauma, because even though the rectan-gular miniplates may have obtained infer-ior results, the stabilization they achievemay be sufficient to allow for the skeletalunit to function during the repair processbecause they reduce the functionaldemand made on it during the first 4weeks. Clinical investigations could con-firm these findings and they are importantand necessary to validate this alternativeform of functionally stable internal fixa-tion in the anterior region of the mandible.
Funding
None.
Competing interests
None declared.
Ethical approval
Not required.
Acknowledgement. The authors would liketo express their gratitude to PROMM1 -Industria de Materiais Cirurgicos, PortoAlegre, Rio Grande do Sul, Brazil, for
Please cite this article in press as: de KP, e
anterior mandibular fractures, Int J Oral M
their kind support through donations ofthe titanium plates and screws used in thisresearch.
References
1. Cabrini Gabrielli MA, Real Gabrielli MF,
Marcantonio E, Hochuli-Vieira E. Fixation
of mandibular fractures with 2.0-mm mini-
plates: review of 191 cases. J Oral Maxillo-
fac Surg 2003;61:430–6.
2. Boulorian R, Stewart L, Berger J. Transoral
2.0-mm miniplate fixation of mandibular
fractures plus 2 weeks’ maxillomandibular
fixation: a prospective study. J Oral Max-
illofac Surg 2002;60:167–70.
3. Lovald S, Baack B, Gaball C, Olson G,
Hoard A. Biomechanical optimization of
bone plates used in rigid fixation of man-
dibular symphysis fractures. J Oral Maxil-
lofac Surg 2010;68:1833–41.
4. Vieira e Oliveira TR, Passeri LA. Mechan-
ical evaluation of different techniques for
symphysis fracture fixation: an in vitro poly-
urethane mandible study. J Oral Maxillofac
Surg 2011;69:e141–6.
5. Peterson LJ, Ellis III E, Hupp JR, Tucker
MR. Contemporary oral and maxillofacial
surgery. 4th ed. St. Louis: Mosby; 2005.
6. Madsen MJ, McDaniel CA, Haug RH. A
biomechanical evaluation of plating techni-
ques used for reconstructing mandibular
symphysis/parasymphysis fractures. J Oral
Maxillofac Surg 2008;66:2012–9.
7. Wong RC, Tideman H, Kin L, Merkx MA.
Biomechanics of mandibular reconstruction:
a review. Int J Oral Maxillofac Surg
2010;39:313–9.
8. Ji B, Wang C, Liu L, Long J, Tian W, Wang
H. A biomechanical analysis of titanium
miniplates used for treatment of mandibular
symphyseal fractures with the finite element
method. Oral Surg Oral Med Oral Pathol
Oral Radiol Endod 2010;109:e21–7.
9. Brasileiro BF, Passeri LA. Epidemiological
analysis of maxillofacial fractures in Brazil:
a 5-year prospective study. Oral Surg Oral
Med Oral Pathol Oral Radiol Endod
2006;102:28–34.
10. Chiodo TA, Milles M. Use of monocortical
miniplates for the intraoral treatment of
mandibular fractures. Atlas Oral Maxillofac
Surg Clin North Am 2009;17:19–25.
11. Farmand M. Experiences with the 3-D mini-
plate osteosynthesis in mandibular fractures.
Fortschr Kiefer Gesichtschir 1996;41:
85–7.
12. Jain MK, Manjunath KS, Bhagwan BK,
Shah DK. Comparison of 3-dimensional
and standard miniplate fixation in the man-
agement of mandibular fractures. J Oral
Maxillofac Surg 2010;68:1568–72.
13. Jain MK, Sankar K, Ramesh C, Bhatta R.
Management of mandibular interforaminal
fractures using 3 dimensional locking and
standard titanium miniplates—a comparative
t al. In vitro mechanical assessment of 2.0-mm
axillofac Surg (2013), http://dx.doi.org/10.101
preliminary report of 10 cases. J Craniomax-
illofac Surg 2012;40:e475–8.
14. Fernandez JR, Gallas M, Burguera JM,
Viano JM. A three-dimensional numerical
simulation of mandible fracture reduction
with screwed miniplates. J Biomech 2003;
36:329–37.
15. Zix J, Lieger O, Iizuca T. Use of straight and
curved 3-dimensional titanium miniplates
for fracture fixation at the mandibular angle.
J Oral Maxillofac Surg 2007;65:1758–63.
16. Meyer C, Serhir L, Boutemi P. Experimental
evaluation of three osteosynthesis devices
used for stabilizing. J Craniomaxillofac Surg
2006;34:173–81.
17. Prein J. Manual of internal fixation in the
cranio-facial skeleton. Berlin: Springer;
1998.
18. Rudderman RH, Mullen RL, Phillips JH.
The biophysics of mandibular fractures: an
evolution toward understanding. Plast
Reconstr Surg 2008;121:596–607.
19. Sato FR. Avaliacao mecanica e fotoelastica
de diferentes tecnicas de fixacao interna
rıgida da osteotomia sagital em avancos
mandibulares. Dissertation. Piracicaba: Uni-
camp; 2009.
20. Cordey J. Introduction: basic concepts and
definitions in mechanics. Injury 2000;
31(Suppl. 2):1–13.
21. Haug RH, Barber BS, Punjabi AP. An in
vitro comparison of the effect of number and
pattern of positional screws on load resis-
tance. J Oral Maxillofac Surg 1999;57:300–
8.
22. Bredbenner TL, Haug RH. Substitutes for
human cadaveric bone in maxillofacial rigid
fixation research. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod 2000;90:574–80.
23. Kroon FH, Mathisson M, Cordey JR, Rahn
BA. The use of miniplates in mandibular
fractures—an in vitro study. J Craniomax-
illofac Surg 1991;19:199–204.
24. Spina AM, Marciani RD. Mandibular fac-
tures. In: Fonseca RJ, editor. Oral and
maxillofacial surgery—trauma. 1st ed. Phi-
ladelphia: W.B. Saunders; 2000. p. 85–135.
25. Tams J, Loon JP, Otten E, Rozema FR, Bos
RR. A three dimensional study of bending
and torsion moments for different fracture
sites. J Oral Maxillofac Surg 1997;26:
383–8.
26. Sauerbier S, Schon R, Otten JE, Schmelzei-
sen R, Gutwald R. The development of plate
osteosynthesis for the treatment of fractures
of the mandibular body: a literature review. J
Craniomaxillofac Surg 2008;36:251–9.
27. Rudman RA, Rosenthal SC, Shen C,
Ruskin JD, Ifju PG. Photoelastic analysis
of miniplate osteosynthesis for mandibular
angle fractures. Oral Surg Oral Med Oral
Pathol Oral Radiol Endod 1997;84:
129–36.
28. Lovald ST, Wagner JD, Baack B. Biomecha-
nical optimization of bone plates used in
rigid fixation of mandibular fractures. J Oral
Maxillofac Surg 2009;67:973–85.
system three-dimensional miniplates in
6/j.ijom.2013.10.008

8 de Oliveira et al.
YIJOM-2790; No of Pages 8
29. Brasileiro BF. Avaliacao biomecanica in
vitro de tecnicas de fixacao interna rıgida
metalica para a osteotomia sagital do ramo
mandibular e movimentos de avanco e recuo.
Piracicaba: Unicamp/FOP; 2007.
30. Guimaraes-Filho R. Avaliacao in vitro da
resistencia mecanica entre parafusos meta-
licos e reabsorvıveis. Piracicaba: Unicamp/
FOP; 2003.
31. Champy M, Lodde JP, Jaeger JH, Wilk A.
Osteosyntheses mandibulaires selon la tech-
nique de Michelet, Bases biomecaniques. Rev
Stomatol Chir Maxillofac 1976;77:569–76.
32. Champy M, Lodde JP, Jaeger JH, Wilk A,
Gerber JC. Osteosyntheses mandibulaires
selon la technique de Michelet, Presentation
d’un nouveau material resultats. Rev Stoma-
tol Chir Maxillofac 1976;77:577–82.
33. Gear AJ, Apasova E, Schmitz JP, Schubert
W. Treatment modalities for mandibular
angle fractures. J Oral Maxillofac Surg
2005;63:655–63.
34. Kim HC, Essaki S, Kameyama T. Compar-
ison of screw placement patterns on the
Please cite this article in press as: de KP, e
anterior mandibular fractures, Int J Oral M
rigidity of the sagittal split ramus osteotomy:
technical note. J Craniomaxillofac Surg
1995;23:54–6.
35. Ardary WC, Tracy DJ, Brownridge GW,
Urata MM. Comparative evaluation of screw
configuration on the stability of the sagittal
split osteotomy. Oral Surg Oral Med Oral
Pathol 1989;68:125–9.
36. Foley WL, Frost DE, Paulin Jr WB, Tucker
MR. Internal screw fixation: comparison of
placement pattern and rigidity. J Oral Max-
illofac Surg 1989;47:720–3.
37. Trivellato AE. Resistencia a flexao de fix-
acao em osteotomia de costela bovina, var-
iando o numero, a localizacao e a extensao
das placas. Piracicaba: Unicamp/FOP; 2001.
38. Asprino L. Comparacao da resistencia ao
carregamento de tres tecnicas de fixacao
interna rıgida utilizada no tratamento de
fraturas condilares. Estudo in vitro em hemi-
mandıbulas de poliuretano. Piracicaba: Uni-
camp/FOP; 2005.
39. Tate GS, Ellis III E, Throckmorton G. Bite
forces in patients treated for mandibular
t al. In vitro mechanical assessment of 2.0-mm
axillofac Surg (2013), http://dx.doi.org/10.101
fractures: implications for fixation recom-
mendations. J Oral Maxillofac Surg 1994;
52:734–6.
40. Van Sickels JE, Peterson GP, Holms S, Haug
RH. An in vitro comparison of an adjustable
bone fixation system. J Oral Maxillofac Surg
2005;63:1620–5.
Address:A.R. GermanoDepartment of Oral and Maxillofacial
SurgeryHospital Universitario Onofre LopesFederal University of Rio Grande do
Norte – UFRNAv. Nilo Pecanha620 – PetropolisCEP 59012-300BrazilTel.: +55 84 3215 4130;Fax: +55 84 3215 4130E-mail: [email protected]
system three-dimensional miniplates in
6/j.ijom.2013.10.008