Embed Size (px)
Citation preview

Research ArticleImprovement in Depressive Symptoms Is Associated withReduced Oxidative Damage and Inflammatory Response in Type2 Diabetic Patients with Subsyndromal Depression The Resultsof a Randomized Controlled Trial Comparing PsychoeducationPhysical Exercise and Enhanced Treatment as Usual
Marijana VuIiT LovrenIiT1 Mirjana Pibernik-OkanoviT2 Mario Šekerija3 Manja Prašek2
Dea AjdukoviT2 Jadranka Kos2 and Norbert Hermanns4
1Department of Laboratory Medicine Merkur University Hospital Zajceva 19 10000 Zagreb Croatia2Vuk Vrhovac University Clinic for Diabetes Merkur University Hospital Zajceva 19 10000 Zagreb Croatia3Croatian Institute of Public Health Rockefellerova 7 10000 Zagreb Croatia4Forschungsinstitut Diabetes-Akademie Bad Mergentheim (FIDAM GmbH) Theodor Klotzbucher Strasse 1297980 Bad Mergentheim Germany
Correspondence should be addressed to Marijana Vucic Lovrencic vucicidbhr
Received 22 April 2015 Revised 29 June 2015 Accepted 13 July 2015
Academic Editor Francois Pouwer
Copyright copy 2015 Marijana Vucic Lovrencic et al This is an open access article distributed under the Creative CommonsAttribution License which permits unrestricted use distribution and reproduction in any medium provided the original work isproperly cited
Aims To examine one-year changes in oxidative damage and inflammation level in type 2 diabetic patients undergoing behavioraltreatment for subsyndromal depression Materials and Methods A randomized controlled comparison of psychoeducation (A)physical exercise (B) and enhanced treatment as usual (C) was performed in 209 eligible subjects in a tertiary diabetes care settingDepressive symptoms (primary outcome) and selected biomarkers of oxidative damage and inflammation (secondary outcomes)were assessed at baseline and six- and twelve-month follow-up Results Out of the 74 67 and 68 patients randomised into groupsA B and C respectively 201 completed the interventions and 179 were analysed Participants in all three groups equally improvedin depressive symptoms from baseline to one-year follow-up (repeated measures ANOVA 119865 = 1251 119901 lt 00001 1205782 = 007)Urinary 8-oxo-deoxyguanosine (u-8-oxodG) decreased (119865 = 1066 119901 lt 00001 1205782 = 006) as did sialic acid and leukocytes(119865 = 8457 1205782 = 032 and 119865 = 1261 1205782 = 007 resp 119901 lt 00001) while uric acid increased (119865 = 1253 119901 lt 00001 1205782 = 007) inall subjects during one year Improvement of depressive symptoms at 6 months significantly predicted one-year reduction in u-8-oxodG (120573 = 015 119901 = 0044) Conclusion Simple behavioral interventions are capable not only of alleviating depressive symptomsbut also of reducing the intensity of damaging oxidativeinflammatory processes in type 2 diabetic patients with subsyndromaldepression This trial is registered with ISRCTN05673017
1 Introduction
Increased prevalence of elevated depressive symptoms inpatients suffering from diabetes is well documented [1] as aretheir association with suboptimal metabolic control diabetescomplications and mortality [2ndash6] An increased incidenceof adverse health outcomes was observed not only in patientswith the established diagnosis of depression but also in those
suffering subthreshold depressive symptoms [7] indicatingthat even mild depression is clinically relevant Feasible andeffective interventions that might provide benefits to bothphysical andmental health are appraised in order to optimizehealth outcomes in this vulnerable patient group [8 9]
Recently research in this area has been focused onbiochemical markers reflecting common pathophysiologicalprocesses of insulin resistance inflammation and oxidative
Hindawi Publishing CorporationInternational Journal of EndocrinologyVolume 2015 Article ID 210406 11 pageshttpdxdoiorg1011552015210406
2 International Journal of Endocrinology
damage assumed to be intertwined in both diabetes anddepression Psychosocial stressors inappropriate diet seden-tary lifestyle obesity and increased intestinal permeabilityhave been proposed as worthwhile intervention targets fortreatment or prevention of both diseases [10ndash12] Inflam-mation was found to be associated with a combination oftype 2 diabetes and depressive symptoms compared withdepression alone and diabetes without depression [13] Fur-ther investigation in these associations was stressed necessaryfor better understanding of biological pathways underly-ing both diabetes and depressive symptoms Hypothesizingthat depressive symptom scores in newly diagnosed type2 diabetes patients are associated with higher concentra-tions of inflammatory markers Laake et al explored alarge cohort of newly diagnosed type 2 diabetic patientsTheir findings indicated that increased inflammation maybe involved in the pathogenesis of depressive symptoms intype 2 diabetes thus contributing to the increased risk ofcomplications and mortality in this group [14] Transientincreases in systematic inflammation have been observed inresponse to acute psychosocial stress with larger responsesamong individuals reporting adverse psychosocial states orconditions such as depression and low self-esteem [15]Also a hypothesis on the involvement of inflammatory aswell as oxidative and nitrosative stress pathways in thepathogenesis of depression has received much attention [16]Association between depression and oxidative damage due toboth increased reactive oxygen species (ROS) production anddecreased antioxidant capacity has been clearly evidenced ina recent meta-analysis suggesting that oxidative stress mightprovide a plausible biochemical link between depression andunfavorable health outcomes [17] The most likely generatorof oxidative stress in depression is considered to be a chroniclow-grade inflammation resulting from activation of cellularimmunity able to induce an immune-mediated damage to thecells Diabetic patients are particularly vulnerable to thesedetrimental effects since hyperglycemia per se promotesexcessive production of ROS and depletion of antioxidantdefence capacity resulting in oxidative damage that is at leastin part presumably responsible for development of micro-and macrovascular diabetic complications [18]
In spite of the growing evidence that inflammation isassociated with type 2 diabetes and depressive symptomsresearch on the interventions focusing on the interactionbetween depressive symptoms and inflammatory responseis still rare Findings obtained in general population haveshown that inflammatory markers were higher in patientssuffering major depressive disorders than in those withoutdepression and that they are significantly reduced dur-ing cognitive-behavioral therapy [19] Whether improvingdepressive symptoms may lead to reduction in increasedinflammation and oxidative damage in individuals sufferingfrom diabetes has been insufficiently studied Although arecent report has not observed significant influence of effec-tive cognitive-behavioral intervention on some inflammatoryvariables in type 2 diabetic patients with poor glucoregulationand subclinical depression [20] the relationships betweendiabetes oxidative stress low-grade inflammation and dif-ferent levels of depressive symptoms remain unclear
In this study being a part of a broader RCT comparingthe effects of treating subsyndromal depression we aimedto examine one-year changes in selected biomarkers ofoxidative stress and inflammation in type 2 diabetic patientstreated for elevated depressive symptoms that do not reachcriteria for clinical depression Depressive symptoms wereprimary while biomarkers of inflammation (leukocytes hs-CRP adiponectin and sialic acid) oxidative damage (urinary8-oxo-deoxyguanosine) and endogenous antioxidant capac-ity (uric acid) were secondary study outcomes
2 Methods
A postal screening for depressive symptoms relying on theshort form Patient Health Questionnaire-Depression (PHQ-2) [21] was used to recruit potential study participants Theinvited patients (119899 = 4858) were identified in the patientregistry based on inclusion criteria of having type 2 diabetesfor at least one year living in Zagreb and attending at leastone medical check-up during the previous year Out of 1740responders (36) 763 did not report depressive symptomsand 205 expressed no need for receiving professional help inreported mood-related difficulties After excluding patientswith clinical depression andor psychiatric treatment (119899 =134) those with severe physical limitations (119899 = 94) andthose with both physical and psychiatric limitationsillnesses(119899 = 55) or other obstacles for participation (119899 =124) 365 patients were found to be eligible Eligibility wasdetermined in a phone interview inquiring about personaldisease-related and sociodemographic data A presence orabsence of clinical depression was determined by phone-administered structured clinical interview for the DSM-IVAxis I disorders Out of the 365 eligible patients 265 agreed toparticipate among the remaining 100 58 refused to join thegroups and 42 were unreachable after the first contact Twohundred and nine patients who gave their informed consentwere randomised to study groups and completed baselineassessments A computer-generated algorithm stratified bygender was used to allocate patients to the groups and toharmonise the number of female and male participants ineach group [22] Research assistants were responsible forrunning computer-generated assignments of the participantsto the study arms and conducting the enrolment No devi-ations from computer-generated assignments occurred withexception of one patient who did not accept the proposedgroup when coming to the baseline assessment This patientwas not included in the study but suggested to choosebetween other sources of professional help
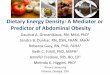
Patientsrsquo flow is shown in Figure 1Primary study outcomes were depressive symptoms
and secondary outcomes were endogenous pro- and anti-inflammatory markers (leukocytes hs-CRP sialic acid andadiponectin) serum uric acid as an indicator of antioxidantcapacity and an overall measure of oxidative damage to DNA(urinary 8-oxo-deoxyguanosine) Sample size calculationwasbased on the absolute change in depressive symptoms asmeasured by the CES-D questionnaire An improvement of05 standard deviations was considered clinically relevant[23] With alpha = 005 samples of 119873 = 59 per group were
International Journal of Endocrinology 3
Received psychoeducational
Enro
lmen
tA
lloca
tion
Lost at 6-month assessment Lost at 6-month assessment Lost at 6-month assessment
6-m
onth
assessments) assessments) assessments)
Ana
lysis
Lost at 12-month assessment Lost at 12-month
Lost at 12-month assessment
12-m
onth
fo
llow
-up
follo
w-u
p
Uneligible = 968
Did not report depressive symptoms = 763
Expressed no need for receiving professionalhelp = 205
Did not enter the study = 156
Refused to join the groups = 58
Unreachable after initial contact = 42
Randomised no show at baseline = 56
Excluded = 407
Clinical depressionpsychiatrictreatment = 134
Severe physical limitation = 94
Both physicalpsychiatric limitations = 55
Other obstacles for participation = 124
Randomized completed baseline assessment = 209
Received diabetes reeducation
Psychoeducation (n = 74)
intervention (n = 71)
withdrew (n = 3)
Physical exercise (n = 66)
intervention (n = 64)
withdrew (n = 2)
Diabetes reeducation (n = 69)
Did not receive intervention- Did not receive intervention-
Received physical exercise
(n = 68)
withdrew (n = 1)Did not receive education-
(n = 2)
(n = 5) (n = 3)
Withdrew (n = 1) missed (n = 1)(n = 6) (n = 8)
Withdrew (n = 3) missed (n = 3) Withdrew (n = 3) missed (n = 5)
Withdrew (n = 2) excluded Withdrew (n = 2) excludedassessment (n = 0)
from analysis (n = 1)from analysis (n = 3)
Analysed n = 58 (with all three Analysed n = 57 (with all threeAnalysed n = 64 (with all three
Assessed for eligibility (n = 1740)
Figure 1 Patientsrsquo flow diagram
shown to be needed to have 80 power in demonstratingstatistically significant differences in depressive symptoms Amore detailed study procedure was described elsewhere [24]
The study was carried out at the Vuk Vrhovac UniversityClinic for DiabetesmdashReference Centre for Diabetes Mellitusin Zagreb Croatia Laboratory analyses were performed atthe Department of Laboratory Medicine Merkur UniversityHospital accredited according to the ISO 151892012 ldquomedi-cal laboratoriesmdashrequirements for quality and competencerdquostandard
21 The Intervention Arms Psychoeducation Physical Exer-cise and Enhanced Treatment as Usual Two interven-tion programsmdashpsychoeducation and physical exercisemdashandenhanced treatment as usual consisting of brief diabetes reed-ucation were offered to patients reporting elevated depressivesymptoms and a need for receiving professional help inmood-related difficulties The intervention programs weredelivered in small groups attending six 90-minute weekly ses-sions One 90-minute intervention sessionmdashenhanced treat-ment as usualmdashwas offered to the control study participants
4 International Journal of Endocrinology
Table 1 Programsrsquo objectives methods of delivery and specific features
Study arm Objectives Methods of delivery Specific features
Psychoeducation
(i) Recognizing and understanding feelings(ii) Becoming aware of dysfunctionalthinking patterns(iii) Improving mood by pleasant activities(iv) Improving mood by solving problems(v) Managing automatic negative thoughts(vi) Communicating assertively providingsupport
(i) Six weekly group sessions lastingfor 90 minutes(ii) Interactive learning in smallgroups (5ndash8 participants)(iii) Self-help manual(iv) Workbook with practicalexercises
Learning and discussions supportedby a structured PowerPointpresentationTopics focused on diabetes-relatedissues and concerns
Physical exercise
(i) Acquiring warm-up flexibilitystretching and strengthening exercises(ii) Learning about physical activity andglycaemic control cardiovascular healthenergy expenditure peripheral nervesmood diabetes self-management
(i) Six weekly group sessions lastingfor 90 minutes(ii) Practicing exercises andexchanging experiences in smallgroups(iii) Written material reminding ofpracticed exercises
Learning and discussions supportedby a structured PowerPointpresentationExercise intensity measured by aheart rate monitor maintained in alight-to-medium intensity rangeBlood glucose and blood pressuremeasured before and after sessions
Enhancedtreatment asusual
(i) Discussing recent laboratory findings(ii) Addressing diabetes-related concerns
(i) One group session lasting for 90minutes(ii) Patient-centered counselling inthe group
Written self-help instructions tocope with mood difficulties
because leaving these patients without any treatment wasconsidered ethically unacceptable
The interventions were considered to have a very lowpotential for causing harm Nevertheless patient informa-tion being a part of the written consent clearly stated thatthe participants can discontinue intervention at any timeparticularly if they would perceive that their symptoms havebeen worsened Qualified professionals involved in treatmentcarefully monitored patientrsquos condition and routine labora-tory results in order to provide a timely referral to physicianrsquoscare if needed In addition patients allocated to physicalexercise underwent ECG and if indicated an ergometrictest before the study Exercise intensity was measured bya heart rate monitor and maintained in a light-to-mediumintensity range whereas blood glucose and blood pressurewere measured before and after each session
A summary of the programsrsquo objectives methods ofdelivery and specific features are presented in Table 1
22 Assessments Patient demographic variables includedage sex education family status employment and economicstatus Diabetes-related variables included years of diabetesduration and diabetes treatment with or without insulin
Screening for mood difficulties was carried out using theadapted Patient Health Questionnaire-2 [21] An additionalquestion inquiring into the patientsrsquo need for help withthese difficulties was added as it has proven to improve theinstrumentrsquos validity [25]
The presence or absence of clinical depression was deter-mined by phone-administered structured clinical interviewfor the DSM-IV Axis 1 disorders as this method has beenshown to be comparable to face-to-face interview [26]
Depressive symptoms were measured by the Center forEpidemiological Studies Depression (CES-D) Scale a 20-itemself-report instrument [27]The total score of the scale ranges
from 0 to 60 points with higher scores indicating higherdepressive symptoms The reliability of the scale at baselinewas Cronbach alpha = 083
221 Laboratory Assessments HbA1c was measured by anNGSP-certified automated immunoturbidimetric method(Tina-quant HbA1c Roche Diagnostics USA) with a totalimprecision (expressed as CV) lt15 and dual reportingof the results (NGSPDCCT aligned and IFCC-alignedmmolmol)
Leukocyte count was determined in K3EDTA-wholeblood samples with ADVIA120 blood cell counter (SiemensDiagnostic Solutions USA)
Serum uric acid and hs-CRP concentrations were mea-sured by the automated enzymatic and immunoturbidimetricassays respectively (AU680 Beckman Coulter USA)
Total serum sialic acid (TSA) was determined by acolorimetric procedure as described previously [28] Serumadiponectin was measured by a commercially available sand-wich ELISA procedure (Adiponectin Human ELISA highsensitive Biovendor CZ) with declared detection limit of047 120583gL
Urinary 8-oxo-deoxyguanosine (u-8-oxodG) was mea-sured by the competitive ELISA method (New 8-OHdGCheck Japan Institute for the Control of Ageing JaiCAShizuoka Japan) with declared assay-range of 05ndash200120583gLand improved specificity [29] On the day of analysis frozenurine samples were thawed in a water-bath (37∘C) vortexedcentrifuged (10min 3000 rpm) and u-8-oxodG assayedimmediately according to the manufacturerrsquos instructionsUrinary creatinine was measured in the same samples witha compensated colorimetric Jaffe procedure (AU680 Anal-yser Beckman Coulter Brea USA) Results were normal-ized to the creatinine concentration by the formula u-8-oxodGcreatinine (120583gmmol)
International Journal of Endocrinology 5
Variables indicating a level of depressive symptoms andbiomarkers of oxidative damage and inflammation weremeasured at baseline and after six- and twelve-month follow-up periods HbA1c leukocytes serum hs-CRP and uric acidwere assayed in fresh samples obtained in the morning afteran overnight fast Samples for sialic acid adiponectin and u-8-oxodG measurements were frozen (minus70∘C) until analyzedThe samples from each patient were analyzed with ELISAs atthe samemicroplate in order to avoid possible between-seriesvariability
23 Statistical Methods Data are presented as means (SD)unless otherwise indicated Due to the nonparametric dis-tribution hs-CRP results were log-transformed prior to theanalysis One-way ANOVA and chi squares were used todetermine baseline differences across the three treatmentarms and examine differences between continuing partici-pants and dropouts
Data were analyzed per protocol after exclusion of par-ticipants who withdrew did not attend all three follow-up meetings initiated psychopharmacological treatment ordied during the study period these results are presentedthroughout the paper Intention-to-treat (ITT) analysis wasperformed to validate these results all participants whowere randomized were analyzed despite deviations from theprotocol To perform ITT missing data were imputed usingthe baseline observation carried forward approach
Repeated measures ANOVA was used to test for changesin outcome variables across time and between the groupsCohenrsquos 1205782 coefficients ranging from 001 to 005 wereregarded as small from006 to 012moderate andge013 large
Regression analysis was employed to test directionalrelations between depressive symptoms and reduction ininflammation and oxidative stress
A 119901 value of lt005 was considered significant in allanalyses
Statistical analyses were performed by using the SPSS 17(SPSS Inc Chicago IL USA)
24 Ethical Aspects The study was approved by the VukVrhovac University Clinic for Diabetes Ethics Committee onJune 30 2010 A written informed consent was obtained fromall the participants
3 Results
Among the 1740 patients assessed for eligibility 365 wereconsidered eligible and 265 agreed to participate in the inter-ventions (72) Of these 209 completed baseline laboratoryand psychological assessments (79) with 74 randomizedto psychoeducational intervention 66 to physical exerciseand 69 to diabetes reeducation Attrition rate was 3 duringthe interventions (6 of 209 patients) 3 from baseline tosix months (7 of 203 patients) and 2 from 6-month to 12-month follow-up period (4 of 196 patients) Of the sevendropouts who completed the intervention but missed bothfollow-up assessments two missed the follow-up appoint-ments due to health problems four were unwilling to comeand one patient died No harmful incidents were recorded
throughout the interventions Four patients were excludedfromper-protocol analyses due to the initiation of pharmaco-logical therapy No differences between the participants anddropouts across the three study groups were observed
Table 2 presents demographic and diabetes-related char-acteristics of patients randomized to one of the three groupsand a baseline level of depressive symptoms as self-assessedby the CES-D questionnaire No between-group differencesregarding demographic diabetes-related and psychologicalvariables were found
The effects of interventions on depressive symptoms andbiomarkers of oxidative damage and inflammation as wellas glucoregulation (HbA1c) and BMI based on repeatedmeasures ANOVA are given in Table 3 ITT analyses showeda comparable pattern of results of all analyses in terms ofstatistical significance and effect size and are not presentedin the text
31 Changes in Depressive Symptoms No significant be-tween-group differences over time were obtained with res-pect to depressive symptoms (119865 = 061 119901 = 0656) indi-cating comparable efficacy of psychoeducation physical exer-cise and enhanced treatment as usual on the primary studyoutcome
Significant reductions in depressive symptoms occurredacross all three study groups from baseline to 12 months(119865 = 1251 119901 lt 0001 1205782 = 07) The size of the time effectindicated a moderate effect of the three treatments on self-assessed depressive symptoms
32 Changes in Biomarkers of Oxidative Damage and Inflam-mation Total leukocytes significantly decreased in all threegroups (119865 = 1261 119901 lt 00001 1205782 = 007) as did u-8-oxodG (119865 = 1066 119901 lt 00001 1205782 = 006) and sialic acid(119865 = 8457 119901 lt 00001 1205782 = 032) The latter showed smallbut statistically significant time 119909 group effect (119865 = 340119901 = 001 1205782 = 004) However after adjusting the results formultiple comparisons by Bonferroni test it did not remainsignificant Uric acid increased significantly over one year inall three groups (119865 = 1339 119901 lt 00001 1205782 = 007) Theeffects of the interventions on sialic acid can be regarded aslarge (032) and on leukocytes u-8-oxodG and uric acid asmoderate (007 006 and 007 resp)
No significant changes were registered with respect toadiponectin and hs-CRP
NeitherHbA1c nor BMIwere significantly changed in anyof the study groups from baseline to 12 months
No between-group effects were obtained with respectto one-year changes in biomarkers of inflammation andoxidative damage (all 119901 gt 005)
33 Testing for Mediation The results obtained by usingregression analyses indicated that improvement in depressivesymptoms at six months predicted reductions in u-8-oxodGat twelve-month follow-up (120573 = 015 119901 = 0044) whilethe results for sialic and uric acid were close to statisticalsignificance (119901 = 0069 and 119901 = 0070 resp) (results notshown in tables)
6 International Journal of Endocrinology
Table 2 Baseline characteristics of participants by the intervention groups (119899 = 209)
Psychoeducation Physical exercise Enhanced treatment as usual Siglowast
119873 74 66 69Age (yrs) 577 (62) 585 (48) 582 (56) 0648Female (119899) 40 37 36 0867Education (yrs) 126 (24) 124 (23) 122 (25) 0623Professional status ( employed) 30 27 30 0502Economic status ( poor) 13 12 13 0317Family status ( marriedcohabitating) 76 72 76 0488Insulin use () 32 29 32 0695OHA use () 56 57 53 0664Insulin + OHA use () 12 14 15 0632Statin use () 68 71 71 0786HbA1c () 74 (12) 72 (11) 72 (11) 0384HbA1c (mmolmol) 58 (13) 56 (13) 55 (11) 0442Body mass index kgm2 3064 (454) 2944 (467) 2996 (439) 0297Depressive symptoms (CES-D score) 197 (91) 205 (86) 197 (87) 0813Data are means (SD) or percentageslowastSig significancelowast One-way ANOVA or 1205942 as appropriateOHA = oral hypoglycemic agents
4 Discussion
This randomized interventional study attempted to evaluatethe effect of two behavioral interventions psychoeducationand physical exercise as compared to enhanced treatmentas usual on depressive symptoms and the intensity ofoxidativeinflammatory processes in diabetic patients suf-fering from subsyndromal depression The results indicateprotracted favorable effects of either intervention on loweringdepressive symptoms while reducing overall oxidative dam-age and cellular inflammatory response as well as improvingantioxidant capacity
In all three study arms a comparable and clinically mean-ingful improvement in depressive symptoms was obtainedThe intervention-independent results regarding depression-related outcomes confirm our preliminary report indicatingthat treatment as usual was equally effective as psychoe-ducation in reducing depressive symptoms and improvingmetabolic control in type 2 diabetic patients with subsyndro-mal depression [30] Also no between-groupdifferenceswerefound within a randomized controlled comparison of psy-choeducation physical exercise and control arm consistingof brief diabetes reeducation [31]The absence of a significanttreatment effect suggested that patterns of change might besimilar in all treatment groups Hypothetically addressingpatientsrsquo emotional needs and their diabetes-related distresswhich were common in all three approaches may indicate apossible pathway of change Similar findings were obtained ina study by Fisher et al [32] which demonstrated that clinicallyreasonable improvements in emotional symptoms may bestimulated by even minimal behavioral interventions
In this study a significant decrease in overall oxidativedamage was observed from basal to one-year posttreatmentfollow-up by measuring a recognized biomarker of oxidativedamage to DNAmdashurinary 8-oxodG Urinary excretion of
8-oxodG reflects the average rate of nucleic acid guanineoxidation and can be regarded as a reliable marker of generalintracellular oxidative stress [33] Research on the u-8-oxodGin diabetes revealed its significant association with severehyperglycemia poor diabetes control and severity of dia-betic complications as well as predictive value for diabetes-associated morbidity [34] The relationship between u-8-oxodG and depression has been modestly investigated andprovided controversial results from an increase to no changedepending on the study-specific depression phenotype [35ndash37] To our knowledge this is the first study investigating u-8-oxodG in patients with diabetes and elevated depressivesymptoms While the results in our exercise group are inaccord with previously reported reduction in u-8-oxodGelicited bymoderate-intensity exercise in type 2 diabetes over12 months [38] significant decrease in u-8-oxodG levels inpsychoeducation and diabetes reeducation group is a novelfinding indicating that cognitive-behavioral approach mighthave beneficial effects on oxidative damage reduction indiabetic patients with subsyndromal depression Additionalsupport for this finding was a significant increase in serumuric acid level at follow-up
Uric acid is an end-product of purine metabolism withcomplex and multifarious roles in human physiology Apartfrom causing gout hyperuricemia has been identified as arisk factor for metabolic syndrome type 2 diabetes andcardiovascular diseases [39] Recently proposed intriguinghypothesis linking hyperuricemia derived by an increasedconsumption of dietary fructose with an epidemic of car-diometabolic diseases attracted a lot of attention and createda paradigm of uric acid as being an exclusively harmfulmetabolite [40] By contrast uric acid has long been recog-nized as one of the most powerful endogenous antioxidants[41] and an efficient mediator of neuroprotection cognitivefunction and intellectual performance [42] as well as the
International Journal of Endocrinology 7
Table 3 One-year changes of depressive symptoms inflammatory- and prooxidative biomarkers
Group scores BaselineM (SD)
12-month follow-upM (SD) Effects 119865 Overall 119875lowast 119875
0 to 12molowastlowast 1205782
Depressive symptomsA (119899 = 64) 197 (91) 167 (79) Time 1251 lt0001 0003 007B (119899 = 58) 198 (82) 181 (98) Time times group 061 0656 0007C (119899 = 57) 190 (86) 174 (94)
Leukocytes (times109L)A (119899 = 63) 75 (17) 73 (17) Time 1261 lt0001 lt0001 007B (119899 = 58) 75 (16) 71 (15) Time times group 132 0265 0001C (119899 = 57) 78 (22) 71 (20)
CRP (mgL)
A (119899 = 64) 028 (049) 025 (044) Time 238 009 100 001B (119899 = 57) 034 (046) 032 (041) Time times group 087 048 001C (119899 = 57) 035 (041) 024 (039)
Sialic acid (mmolL)A (119899 = 64) 21 (031) 19 (029) Time 8457 lt0001 lt0001 032B (119899 = 58) 21 (031) 18 (022) Time times group 340 001 004C (119899 = 57) 21 (028) 18 (024)
u-8-OxodG (120583gmmol)A (119899 = 64) 11 (05) 09 (04) Time 1066 lt0001 lt0001 006B (119899 = 57) 14 (08) 11 (06) Time times group 109 036 001C (119899 = 57) 12 (07) 10 (04)
Uric acid (120583molL)A (119899 = 64) 2917 (852) 3103 (775) Time 1339 lt0001 lt0001 007B (119899 = 58) 3034 (919) 3232 (931) Time times group 025 091 0003C (119899 = 57) 2904 (779) 3145 (834)
HbA1c ()A (119899 = 64) 74 (13) 72 (09) Time 270 007 008 002B (119899 = 58) 72 (10) 72 (10) Time times group 092 045 001C (119899 = 57) 71 (10) 70 (10)
HbA1c (mmolL)A (119899 = 64) 578 (136) 559 (102) Time 331 005 100 002B (119899 = 58) 548 (114) 557 (107) Time times group 090 045 001C (119899 = 57) 548 (107) 539 (100)
Adiponectin (mgL)A (119899 = 63) 75 (23) 71 (38) Time 073 044 100 0004B (119899 = 58) 91 (61) 90 (67) Time times group 055 065 0006C (119899 = 57) 80 (50) 81 (53)
Body mass index (kgm2)A (119899 = 54) 306 (47) 306 (50) Time 172 019 011 001B (119899 = 53) 292 (45) 290 (46) Time times group 131 027 001C (119899 = 52) 301 (41) 294 (40)
lowastTwo-sided significance of differences across time and between the groups (repeated measures ANOVA)lowastlowastTwo-sided significance of differences between baseline and 12-month assessmentsLog-transformed data
8 International Journal of Endocrinology
most pronounced determinant of total plasma antioxidantcapacity in diabetic patients [43] Thus maintaining uricacid levels within physiological range appears to be morefavorable than radical lowering in prevention of variousmor-bidities Based on recent epidemiological evidence includingcardiometabolic risk assessment a new gender-independentupper limit of reference range for uric acid has been proposedat the level of 360 120583molL [44] The present study revealsa significant increase in uric acid levels at follow-up butwell below proposed cut-off above which negative effectsof hyperuricemia might be expected On the contrary theobserved uric acid increase in our study is rather suggestiveof an improved antioxidant capacity elicited by behavioralinterventions in type 2 diabetic patients with subsyndromaldepression
Beneficial effect of cognitive-behavioral interventionin reducing oxidative stress and inflammatory responsehas been reported in hemodialysis patients suffering frominsomnia [45] but rather sparse depression-related studiesmainly focused on the assessment of low-grade inflammationbiomarkers In a very recent randomized trial evaluating anewly developed cognitive-behavioral program (DIAMOS)in diabetic patients with subsyndromal depression a set ofpro- and anti-inflammatory biomarkers was analyzed at basaland one-year follow-up [20] No change in hs-CRP IL-1 andadiponectin was observed whereas a significant decrease ininterleukin-1 receptor antagonist (IL-1RA) was interpreted asan indirect index of alleviated IL-1-related damaging mech-anisms presumably involved in the pathogenesis of micro-and macrovascular complications of diabetes Likewise ourstudy could not demonstrate any influence of the behavioralinterventions on hs-CRP and adiponectin but we foundother inflammatory markers that is leukocyte count andtotal serum sialic acid (TSA) significantly reduced with thelatter being largely affected (1205782 = 032) by the interventionsperformed
Sialic acids comprise a family of heterogenous monosac-charides abundantly present on the cell membranes withcomplex and multiple biological roles in cellular signalingand immunity [46] TSA is a validated inflammatory andatherogenic marker that has been proposed as a novelbiomarker of cardiovascular disease [47] Elevated levels ofTSA in newly diagnosed type 2 diabetic patients have beenlinked to the risk for later development of macrovascularcomplications [28] Interestingly TSA has been identified asa superior predictive biomarker of metabolic syndrome overthe abundantly used hs-CRP [48] Nevertheless despite theobvious advantages TSA has been largely underutilized inthe research on combined inflammatory-metabolic patholo-gies and it has not been studied in depression until this studyOur results identify TSA as a sensitive biomarker of inflam-mation degree in subsyndromally depressed diabetic patientswhereas neither of the established biomarkers of low-gradeinflammation hs-CRP and adiponectin was able to reflectthe anti-inflammatory effect of the performed interventionsSignificant decrease in leukocyte count however clearlyconfirmed postintervention attenuation of the cell-mediatedinflammation response in our patients with an importantnotice that the presence of acute infection at the assessments
was excluded by total leukocyte count lt 100 times 109L or hs-CRP lt 50 gL
The ability of psychological intervention to reduceboth depressive symptoms and inflammation has been evi-denced in depressed breast-cancer patients [49] Further-more due to the insightful study-design Thornton et alwere able to demonstrate a bidirectional mechanistic rela-tionship between depressive symptoms and inflammationThe paradigmatic view of the low-grade inflammation asthe inflicting mechanism for depression has been at leastcomplemented if not refuted by their finding on the mecha-nistic role of depressive symptoms lowering in the reductionof inflammatory response [49] This explanatory mecha-nism might also be translated to our results particularlyconsidering a lack of any effect of interventions towardshyperglycemia and obesity in our study
It is well known that the intensity of oxidative damage andinflammation in diabetes is remarkably and positively asso-ciated with the severity of hyperglycemia [18] Howeverthe observed reduction in oxidative damage and low-gradeinflammation in our study could not be attributed to thismechanism since no significant changes from baseline tofollow-up were found in HbA1c clinically considered toreflect a fair glucoregulation (Table 3) Obesity-derived low-grade inflammation is another recognized harmful compo-nent in the pathogenesis of type 2 diabetes and its compli-cations [50] Obesity induces a disbalance between pro- andanti-inflammatory cytokinesadipokines resulting in low-grade inflammation and related adverse health outcomesranging from metabolic syndrome and diabetes to cardio-vascular diseases and cancer as well as depression [49ndash51]Reduction in bodyweight is accompanied by beneficialmeta-bolic and hormonal profiles and a reduced inflammation [52]with increased production of anti-inflammatory adipokineadiponectin suggested to be among themost relevant features[53] Since our subjects classified as overweightobese [54]retained their BMI at follow-up and revealed no changes inadiponectin levels it is likely that the observed effects ofinterventions on the reduction in depressive symptoms andoxidativeinflammatory biomarkers in this study dependedon another mechanism(s)
Chronic stress with deregulation of stress-response adap-tive mechanisms is considered to be a common feature ofboth diabetes and depression [55] There is a growing bodyof evidence suggesting that metabolic inflammation asso-ciated with obesity and diabetes inflicts neuroinflammationwhich causes serious disturbances of the hypothalamic-pituitary-adrenal (HPA) axis function and consequentlyleads to impairment of adaptive stress-response [56] More-over chronic stress exposure has recently been demonstratedas a promoting factor for accelerated oxidative damagewhereby a sustained activation of HPA-axis emerged again asthe key mediator [57] Neuroendocrine effects of behavioraltreatment for depression have not been extensively studiedbut the evidence so far suggests a hypothetical pathway thatconnects the nurturing effects derived from the patient-ther-apist ldquobondrdquo with reestablishment of neuroendocrine home-ostasis [58] Moreover positive effects of physical exercise onpreventing potentially harmful stress-related metabolic and
International Journal of Endocrinology 9
psychological consequences have been presumably mediatedby the same neuroendocrine mechanisms [59] Consideringunchanged metabolic profile of our subjects and remark-able improvements in depressive symptoms and oxida-tiveinflammatory biomarkers following either behavioralintervention it is tempting if not plausible to speculate onthe involvement of neuroendocrine mechanism(s) in achiev-ing this beneficial response It should be noted that a lackof between-group differences in changes observed in ourstudy might not be explained by a phenomenon known asldquoregression toward the meanrdquo or just a natural course ofparameters Previous findings on persistence of depressivesymptoms in people with type 2 diabetes indicate thatdepression is not only persistent [60 61] but also associatedwith an increased risk of aggravating over time [62] On theother hand oxidative damage toDNA is increasing in healthysubjects throughout time as a result of ageing process [33]while inflammatory response and ageing-associated damageto biomolecules are even more pronounced in diabetes dueto a long-term exposure to hyperglycemia and advanced-glycated end-products [34 50]
The strengths of this study are in examining a highlyprevalent population of type 2 patients with depressive symp-toms but no clinical depression using a randomized com-parative design employing structured behavioral interven-tions and analyzing clinically relevant changes of simple-to-measure oxidativeinflammatory biomarkers Its limitation isthe lack of treatment as usual control intervention precludingthe possibility to investigate the course and outcomes ofsubclinical depression without any treatment Also the studywas carried out in only one centermdasha tertiary diabetesclinicmdashwhich does not allow concluding about its feasibilityin other clinical settings Per-protocol analyses are presentedin the study results which were confirmed by the intention totreat analysis based on baseline-observation-carried-forwardapproach A lack of estimation derived frommultiple predic-tors may be considered a limitation of the study
5 Conclusions
This study has demonstrated that improvement in depressivesymptoms is accompanied with reduced oxidative dam-age and inflammatory response in type 2 diabetic patientswith subsyndromal depression Testing mediating effectshas indicated that medium-term improvement in depres-sive symptoms predicts long-term-reduction in oxidativedamage while mediating factors for observed reductionin inflammatory response should be further investigatedClinical benefits of treating subsyndromal depression wereshown to be comparable in all three treatment arms
Regardless of the mechanisms involved our study clearlyindicates that enhanced treatment as usual defined as briefpatient-centred diabetes reeducation is not inferior to psy-choeducation and exercise in providing beneficial outcomesin subsyndromally depressed type 2 diabetic patients Simplebehavioral interventions are capable not only of alleviatingdepressive symptoms but also of reducing the intensity ofdamaging oxidativeinflammatory processes thereby miti-gating the risk of development of diabetic complications
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The study was funded by the European Foundation forthe Study of Diabetes (EFSD)mdashNew Horizons CollaborativeResearch Initiative 2010 The authors would like to thankLovorka Perkovic Croatian Institute of Public Health forediting the paper
References
[1] S S Ali M A Stone J L Peters M J Davies and K KhuntildquoThe prevalence of co-morbid depression in adults with Type2 diabetes a systematic review and meta-analysisrdquo DiabeticMedicine vol 23 no 11 pp 1165ndash1173 2006
[2] P J Lustman R J Anderson K E Freedland M de Groot RM Carney and R E Clouse ldquoDepression and poor glycemiccontrol a meta-analytic review of the literaturerdquo Diabetes Carevol 23 no 7 pp 934ndash942 2000
[3] L K Richardson L E Egede M Mueller C L Echols and MGebregziabher ldquoLongitudinal effects of depression on glycemiccontrol in veterans with Type 2 diabetesrdquo General HospitalPsychiatry vol 30 no 6 pp 509ndash514 2008
[4] M de Groot R Anderson K E Freedland R E Clouse andP J Lustman ldquoAssociation of depression and diabetes com-plications ameta-analysisrdquo PsychosomaticMedicine vol 63 no4 pp 619ndash630 2001
[5] K Ismail KWinkley D Stahl T Chalder andM Edmonds ldquoAcohort study of people with diabetes and their first foot ulcerthe role of depression on mortalityrdquo Diabetes Care vol 30 no6 pp 1473ndash1479 2007
[6] X Zhang S L Norris E W Gregg Y J Cheng G Becklesand H S Kahn ldquoDepressive symptoms and mortality amongpersons with and without diabetesrdquo American Journal of Epi-demiology vol 161 no 7 pp 652ndash660 2005
[7] S A Black K S Markides and L A Ray ldquoDepression pre-dicts increased incidence of adverse health outcomes in olderMexican Americans with type 2 diabetesrdquo Diabetes Care vol26 no 10 pp 2822ndash2828 2003
[8] H Baumeister N Hutter and J Bengel ldquoPsychological andpharmacological interventions for depression in patients withdiabetesmellitus and depressionrdquoCochraneDatabase of System-atic Reviews vol 12 Article ID CD008381 2012
[9] E Harkness W Macdonald J Valderas P Coventry L Gaskand P Bower ldquoIdentifying psychosocial interventions thatimprove both physical and mental health in patients with dia-betes a systematic review and meta-analysisrdquo Diabetes Carevol 33 no 4 pp 926ndash930 2010
[10] M Berk L J Williams F N Jacka et al ldquoSo depression is aninflammatory disease but where does the inflammation comefromrdquo BMCMedicine vol 11 article 200 2013
[11] S de Kort D Keszthelyi and A A M Masclee ldquoLeaky gut anddiabetes mellitus what is the linkrdquoObesity Reviews vol 12 no6 pp 449ndash458 2011
[12] E T de Lemos J Oliveira J P Pinheiro and F Reis ldquoRegularphysical exercise as a strategy to improve antioxidant andanti-inflammatory status benefits in type 2 diabetes mellitusrdquo
10 International Journal of Endocrinology
Oxidative Medicine and Cellular Longevity vol 2012 Article ID741545 15 pages 2012
[13] T A Doyle M de Groot T Harris et al ldquoDiabetes depressivesymptoms and inflammation in older adults results fromthe Health Aging and Body Composition Studyrdquo Journal ofPsychosomatic Research vol 75 no 5 pp 419ndash424 2013
[14] J-P S Laake D Stahl S A Amiel et al ldquoThe associationbetween depressive symptoms and systemic inflammation inpeople with type 2 diabetes findings from the South Londondiabetes studyrdquoDiabetes Care vol 37 no 8 pp 2186ndash2192 2014
[15] N Rohleder ldquoStimulation of systemic low-grade inflammationby psychosocial stressrdquo Psychosomatic Medicine vol 76 no 3pp 181ndash189 2014
[16] M Maes ldquoAn intriguing and hitherto unexplained co-occur-rence depression and chronic fatigue syndrome are mani-festations of shared inflammatory oxidative and nitrosative(IOampNS) pathwaysrdquo Progress in Neuro-Psychopharmacologyand Biological Psychiatry vol 35 no 3 pp 784ndash794 2011
[17] P Palta L J Samuel E RMiller and S L Szanton ldquoDepressionand oxidative stress results from a meta-analysis of observa-tional studiesrdquo Psychosomatic Medicine vol 76 no 1 pp 12ndash192014
[18] L Rochette M Zeller Y Cottin and C Vergely ldquoDiabetes oxi-dative stress and therapeutic strategiesrdquo Biochimica et Biophys-ica Acta vol 1840 no 9 pp 2709ndash2729 2014
[19] S Keri C Szabo and O Kelemen ldquoExpression of Toll-LikeReceptors in peripheral blood mononuclear cells and responseto cognitive-behavioral therapy in major depressive disorderrdquoBrain Behavior and Immunity vol 40 pp 235ndash243 2014
[20] N Hermanns A Schmitt A Gahr et al ldquoThe effect ofa Diabetes-Specific Cognitive Behavioral Treatment Program(DIAMOS) for patients with diabetes and subclinical depres-sion results of a randomized controlled trialrdquo Diabetes Carevol 38 no 4 pp 551ndash560 2015
[21] K Kroenke R L Spitzer and J B W Williams ldquoThe patienthealth questionnaire-2 validity of a two-item depressionscreenerrdquoMedical Care vol 41 no 11 pp 1284ndash1292 2003
[22] J H Abramson ldquoWINPEPI updated computer programs forepidemiologists and their teaching potentialrdquo EpidemiologicPerspectives amp Innovations vol 8 no 1 article 1 2011
[23] J Cohen ldquoA power primerrdquo Psychological Bulletin vol 112 no1 pp 155ndash159 1992
[24] M Pibernik-Okanovic D Ajdukovic M V Lovrencic andN Hermanns ldquoDoes treatment of subsyndromal depressionimprove depression and diabetes related outcomes protocolfor a randomised controlled comparison of psycho-educationphysical exercise and treatment as usualrdquo Trials vol 12 article17 2011
[25] BArroll FGoodyear-SmithNKerse T Fishman and JGunnldquoEffect of the addition of a lsquohelprsquo question to two screeningquestions on specificity for diagnosis of depression in generalpractice diagnostic validity studyrdquo British Medical Journal vol331 no 7521 article 884 2005
[26] P Rohde P M Lewinsohn and J R Seeley ldquoComparability oftelephone and face-to-face interviews in assessing axis I and IIdisordersrdquo American Journal of Psychiatry vol 154 no 11 pp1593ndash1598 1997
[27] L S Radloff ldquoTheCES-D scalerdquoApplied Psychological Measure-ment vol 1 pp 385ndash401 1977
[28] M Gavella V Lipovac A Car M Vucic L Sokolic and RRakos ldquoSerum sialic acid in subjects with impaired glucose
tolerance and in newly diagnosed type 2 diabetic patientsrdquoActaDiabetologica vol 40 no 2 pp 95ndash100 2003
[29] M D Evans R Singh V Mistry K Sandhu P B Farmer andM S Cooke ldquoAnalysis of urinary 8-oxo-78-dihydro-purine-21015840- deoxyribonucleosides by LC-MSMS and improved ELISArdquoFree Radical Research vol 42 no 10 pp 831ndash840 2008
[30] M Pibernik-Okanovic D Begic D Ajdukovic N Andrijasevicand Z Metelko ldquoPsychoeducation versus treatment as usualin diabetic patients with subthreshold depression preliminaryresults of a randomized controlled trialrdquo Trials vol 10 article78 2009
[31] M Pibernik-Okanovic M Vucic Lovrencic D AjdukovicM Sekerija and N Hermanns ldquoPsychological behavioraland biological changes following treatments of subsyndromaldepression in people with type 2 diabetesrdquoDiabetologia vol 56supplement 1 p S465 2013
[32] L Fisher D Hessler R E Glasgow et al ldquoREDEEM a prag-matic trial to reduce diabetes distressrdquo Diabetes Care vol 36no 9 pp 2551ndash2558 2013
[33] H E Poulsen L L Nadal K Broedbaek P E Nielsen andA Weimann ldquoDetection and interpretation of 8-oxodG and 8-oxoGua in urine plasma and cerebrospinal fluidrdquo Biochimica etBiophysica ActamdashGeneral Subjects vol 1840 no 2 pp 801ndash8082014
[34] K Broedbaek A Weimann E S Stovgaard and H E PoulsenldquoUrinary 8-oxo-78-dihydro-21015840-deoxyguanosine as a biomarkerin type 2 diabetesrdquo Free Radical Biology and Medicine vol 51no 8 pp 1473ndash1479 2011
[35] M J Forlenza and G E Miller ldquoIncreased serum levels of 8-hydroxy-21015840-deoxyguanosine in clinical depressionrdquo Psychoso-matic Medicine vol 68 no 1 pp 1ndash7 2006
[36] A Jorgensen J Krogh K Miskowiak et al ldquoSystemic oxida-tively generatedDNARNAdamage in clinical depression asso-ciations to symptom severity and response to electroconvulsivetherapyrdquo Journal of Affective Disorders vol 149 no 1ndash3 pp 355ndash362 2013
[37] S Yi ANanri YMatsushitaHKasai K Kawai andTMizoueldquoDepressive symptoms and oxidative DNA damage in Japanesemunicipal employeesrdquo Psychiatry Research vol 200 no 2-3 pp318ndash322 2012
[38] H Nojima H Watanabe K Yamane et al ldquoEffect of aerobicexercise training on oxidative stress in patients with type 2diabetes mellitusrdquo Metabolism Clinical and Experimental vol57 no 2 pp 170ndash176 2008
[39] S Bonakdaran and B Kharaqani ldquoAssociation of serum uricacid and metabolic syndrome in type 2 diabetesrdquo CurrentDiabetes Reviews vol 10 no 2 pp 113ndash117 2014
[40] R J Johnson T Nakagawa L G Sanchez-Lozada et al ldquoSugaruric acid and the etiology of diabetes and obesityrdquoDiabetes vol62 no 10 pp 3307ndash3315 2013
[41] M L Wahlqvist ldquoAntioxidant relevance to human healthrdquo AsiaPacific Journal of Clinical Nutrition vol 22 no 2 pp 171ndash1762013
[42] A De Giorgi F Fabbian M Pala et al ldquoUric acid friend orfoe Uric acid and cognitive function lsquogout kills more wise menthan simplersquordquo European Review forMedical and PharmacologicalSciences vol 19 no 4 pp 640ndash646 2015
[43] M Vucic B Rocic V Bozikov and S J H Ashcroft ldquoPlasmauric acid and total antioxidant status in patients with diabetesmellitusrdquo Hormone and Metabolic Research vol 29 no 7 pp355ndash357 1997
International Journal of Endocrinology 11
[44] G Desideri G Castaldo A Lombardi et al ldquoIs it time to revisethe normal range of serum uric acid levelsrdquo European Reviewfor Medical and Pharmacological Sciences vol 18 no 9 pp1295ndash1306 2014
[45] H-Y Chen I-C Cheng Y-J Pan et al ldquoCognitive-behavioraltherapy for sleep disturbance decreases inflammatory cytokinesand oxidative stress in hemodialysis patientsrdquo Kidney Interna-tional vol 80 no 4 pp 415ndash422 2011
[46] A Varki and P Gagneux ldquoMultifarious roles of sialic acids inimmunityrdquo Annals of the New York Academy of Sciences vol1253 no 1 pp 16ndash36 2012
[47] K P Gopaul and M A Crook ldquoSialic acid a novel marker ofcardiovascular diseaserdquo Clinical Biochemistry vol 39 no 7 pp667ndash681 2006
[48] L M Browning S A Jebb G D Mishra et al ldquoElevated sialicacid but not CRP predicts features of the metabolic syndromeindependently of BMI in womenrdquo International Journal ofObesity vol 28 no 8 pp 1004ndash1010 2004
[49] LMThornton B L Andersen T A Schuler andW E CarsonldquoA psychological intervention reduces inflammatory markersby alleviating depressive symptoms secondary analysis of arandomized controlled trialrdquo Psychosomatic Medicine vol 71no 7 pp 715ndash724 2009
[50] N Esser S Legrand-Poels J Piette A J Scheen and N PaquotldquoInflammation as a link between obesity metabolic syndromeand type 2 diabetesrdquoDiabetes Research andClinical Practice vol105 no 2 pp 141ndash150 2014
[51] R Hutcheson and P Rocic ldquoThe metabolic syndrome oxida-tive stress environment and cardiovascular disease the greatexplorationrdquo Experimental Diabetes Research vol 2012 ArticleID 271028 13 pages 2012
[52] L Fontana and F B Hu ldquoOptimal body weight for health andlongevity bridging basic clinical and population researchrdquoAging Cell vol 13 no 3 pp 391ndash400 2014
[53] A T Turer and P E Scherer ldquoAdiponectin mechanistic insightsand clinical implicationsrdquo Diabetologia vol 55 no 9 pp 2319ndash2326 2012
[54] WHO ldquoObesity and overweightrdquo Fact sheet No 311 2015[55] P W Gold ldquoThe organization of the stress system and its
dysregulation in depressive illnessrdquo Molecular Psychiatry vol20 no 1 pp 32ndash47 2015
[56] S Purkayastha and D Cai ldquoNeuroinflammatory basis ofmetabolic syndromerdquo Molecular Metabolism vol 2 no 4 pp356ndash363 2013
[57] K Aschbacher A OrsquoDonovan O MWolkowitz F S DhabharY Su and E Epel ldquoGood stress bad stress and oxidative stressinsights from anticipatory cortisol reactivityrdquo Psychoneuroen-docrinology vol 38 no 9 pp 1698ndash1708 2013
[58] C F Sharpley ldquoA review of the neurobiological effects of psy-chotherapy for depressionrdquo Psychotherapy vol 47 no 4 pp603ndash615 2010
[59] M N Silverman and P A Deuster ldquoBiological mechanismsunderlying the role of physical fitness in health and resiliencerdquoInterface Focus vol 4 no 5 Article ID 20140040 2014
[60] G Nefs F Pouwer J Denollet and V Pop ldquoThe course ofdepressive symptoms in primary care patients with type 2 dia-betes results from theDiabetes Depression TypeDPersonalityZuidoost-Brabant (DiaDDZoB) Studyrdquo Diabetologia vol 55no 3 pp 608ndash616 2012
[61] M Pibernik-Okanovic D Begic K Peros S Szabo andZ Metelko ldquoPsychosocial factors contributing to persistent
depressive symptoms in type 2 diabetic patients a Croatiansurvey from the European Depression in Diabetes ResearchConsortiumrdquo Journal of Diabetes and Its Complications vol 22no 4 pp 246ndash253 2008
[62] M Bot F Pouwer J Ormel J P J Slaets and P de Jonge ldquoPre-dictors of incidentmajor depression in diabetic outpatients withsubthreshold depressionrdquo Diabetic Medicine vol 27 no 11 pp1295ndash1301 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 International Journal of Endocrinology
damage assumed to be intertwined in both diabetes anddepression Psychosocial stressors inappropriate diet seden-tary lifestyle obesity and increased intestinal permeabilityhave been proposed as worthwhile intervention targets fortreatment or prevention of both diseases [10ndash12] Inflam-mation was found to be associated with a combination oftype 2 diabetes and depressive symptoms compared withdepression alone and diabetes without depression [13] Fur-ther investigation in these associations was stressed necessaryfor better understanding of biological pathways underly-ing both diabetes and depressive symptoms Hypothesizingthat depressive symptom scores in newly diagnosed type2 diabetes patients are associated with higher concentra-tions of inflammatory markers Laake et al explored alarge cohort of newly diagnosed type 2 diabetic patientsTheir findings indicated that increased inflammation maybe involved in the pathogenesis of depressive symptoms intype 2 diabetes thus contributing to the increased risk ofcomplications and mortality in this group [14] Transientincreases in systematic inflammation have been observed inresponse to acute psychosocial stress with larger responsesamong individuals reporting adverse psychosocial states orconditions such as depression and low self-esteem [15]Also a hypothesis on the involvement of inflammatory aswell as oxidative and nitrosative stress pathways in thepathogenesis of depression has received much attention [16]Association between depression and oxidative damage due toboth increased reactive oxygen species (ROS) production anddecreased antioxidant capacity has been clearly evidenced ina recent meta-analysis suggesting that oxidative stress mightprovide a plausible biochemical link between depression andunfavorable health outcomes [17] The most likely generatorof oxidative stress in depression is considered to be a chroniclow-grade inflammation resulting from activation of cellularimmunity able to induce an immune-mediated damage to thecells Diabetic patients are particularly vulnerable to thesedetrimental effects since hyperglycemia per se promotesexcessive production of ROS and depletion of antioxidantdefence capacity resulting in oxidative damage that is at leastin part presumably responsible for development of micro-and macrovascular diabetic complications [18]
In spite of the growing evidence that inflammation isassociated with type 2 diabetes and depressive symptomsresearch on the interventions focusing on the interactionbetween depressive symptoms and inflammatory responseis still rare Findings obtained in general population haveshown that inflammatory markers were higher in patientssuffering major depressive disorders than in those withoutdepression and that they are significantly reduced dur-ing cognitive-behavioral therapy [19] Whether improvingdepressive symptoms may lead to reduction in increasedinflammation and oxidative damage in individuals sufferingfrom diabetes has been insufficiently studied Although arecent report has not observed significant influence of effec-tive cognitive-behavioral intervention on some inflammatoryvariables in type 2 diabetic patients with poor glucoregulationand subclinical depression [20] the relationships betweendiabetes oxidative stress low-grade inflammation and dif-ferent levels of depressive symptoms remain unclear
In this study being a part of a broader RCT comparingthe effects of treating subsyndromal depression we aimedto examine one-year changes in selected biomarkers ofoxidative stress and inflammation in type 2 diabetic patientstreated for elevated depressive symptoms that do not reachcriteria for clinical depression Depressive symptoms wereprimary while biomarkers of inflammation (leukocytes hs-CRP adiponectin and sialic acid) oxidative damage (urinary8-oxo-deoxyguanosine) and endogenous antioxidant capac-ity (uric acid) were secondary study outcomes
2 Methods
A postal screening for depressive symptoms relying on theshort form Patient Health Questionnaire-Depression (PHQ-2) [21] was used to recruit potential study participants Theinvited patients (119899 = 4858) were identified in the patientregistry based on inclusion criteria of having type 2 diabetesfor at least one year living in Zagreb and attending at leastone medical check-up during the previous year Out of 1740responders (36) 763 did not report depressive symptomsand 205 expressed no need for receiving professional help inreported mood-related difficulties After excluding patientswith clinical depression andor psychiatric treatment (119899 =134) those with severe physical limitations (119899 = 94) andthose with both physical and psychiatric limitationsillnesses(119899 = 55) or other obstacles for participation (119899 =124) 365 patients were found to be eligible Eligibility wasdetermined in a phone interview inquiring about personaldisease-related and sociodemographic data A presence orabsence of clinical depression was determined by phone-administered structured clinical interview for the DSM-IVAxis I disorders Out of the 365 eligible patients 265 agreed toparticipate among the remaining 100 58 refused to join thegroups and 42 were unreachable after the first contact Twohundred and nine patients who gave their informed consentwere randomised to study groups and completed baselineassessments A computer-generated algorithm stratified bygender was used to allocate patients to the groups and toharmonise the number of female and male participants ineach group [22] Research assistants were responsible forrunning computer-generated assignments of the participantsto the study arms and conducting the enrolment No devi-ations from computer-generated assignments occurred withexception of one patient who did not accept the proposedgroup when coming to the baseline assessment This patientwas not included in the study but suggested to choosebetween other sources of professional help
Patientsrsquo flow is shown in Figure 1Primary study outcomes were depressive symptoms
and secondary outcomes were endogenous pro- and anti-inflammatory markers (leukocytes hs-CRP sialic acid andadiponectin) serum uric acid as an indicator of antioxidantcapacity and an overall measure of oxidative damage to DNA(urinary 8-oxo-deoxyguanosine) Sample size calculationwasbased on the absolute change in depressive symptoms asmeasured by the CES-D questionnaire An improvement of05 standard deviations was considered clinically relevant[23] With alpha = 005 samples of 119873 = 59 per group were
International Journal of Endocrinology 3
Received psychoeducational
Enro
lmen
tA
lloca
tion
Lost at 6-month assessment Lost at 6-month assessment Lost at 6-month assessment
6-m
onth
assessments) assessments) assessments)
Ana
lysis
Lost at 12-month assessment Lost at 12-month
Lost at 12-month assessment
12-m
onth
fo
llow
-up
follo
w-u
p
Uneligible = 968
Did not report depressive symptoms = 763
Expressed no need for receiving professionalhelp = 205
Did not enter the study = 156
Refused to join the groups = 58
Unreachable after initial contact = 42
Randomised no show at baseline = 56
Excluded = 407
Clinical depressionpsychiatrictreatment = 134
Severe physical limitation = 94
Both physicalpsychiatric limitations = 55
Other obstacles for participation = 124
Randomized completed baseline assessment = 209
Received diabetes reeducation
Psychoeducation (n = 74)
intervention (n = 71)
withdrew (n = 3)
Physical exercise (n = 66)
intervention (n = 64)
withdrew (n = 2)
Diabetes reeducation (n = 69)
Did not receive intervention- Did not receive intervention-
Received physical exercise
(n = 68)
withdrew (n = 1)Did not receive education-
(n = 2)
(n = 5) (n = 3)
Withdrew (n = 1) missed (n = 1)(n = 6) (n = 8)
Withdrew (n = 3) missed (n = 3) Withdrew (n = 3) missed (n = 5)
Withdrew (n = 2) excluded Withdrew (n = 2) excludedassessment (n = 0)
from analysis (n = 1)from analysis (n = 3)
Analysed n = 58 (with all three Analysed n = 57 (with all threeAnalysed n = 64 (with all three
Assessed for eligibility (n = 1740)
Figure 1 Patientsrsquo flow diagram
shown to be needed to have 80 power in demonstratingstatistically significant differences in depressive symptoms Amore detailed study procedure was described elsewhere [24]
The study was carried out at the Vuk Vrhovac UniversityClinic for DiabetesmdashReference Centre for Diabetes Mellitusin Zagreb Croatia Laboratory analyses were performed atthe Department of Laboratory Medicine Merkur UniversityHospital accredited according to the ISO 151892012 ldquomedi-cal laboratoriesmdashrequirements for quality and competencerdquostandard
21 The Intervention Arms Psychoeducation Physical Exer-cise and Enhanced Treatment as Usual Two interven-tion programsmdashpsychoeducation and physical exercisemdashandenhanced treatment as usual consisting of brief diabetes reed-ucation were offered to patients reporting elevated depressivesymptoms and a need for receiving professional help inmood-related difficulties The intervention programs weredelivered in small groups attending six 90-minute weekly ses-sions One 90-minute intervention sessionmdashenhanced treat-ment as usualmdashwas offered to the control study participants
4 International Journal of Endocrinology
Table 1 Programsrsquo objectives methods of delivery and specific features
Study arm Objectives Methods of delivery Specific features
Psychoeducation
(i) Recognizing and understanding feelings(ii) Becoming aware of dysfunctionalthinking patterns(iii) Improving mood by pleasant activities(iv) Improving mood by solving problems(v) Managing automatic negative thoughts(vi) Communicating assertively providingsupport
(i) Six weekly group sessions lastingfor 90 minutes(ii) Interactive learning in smallgroups (5ndash8 participants)(iii) Self-help manual(iv) Workbook with practicalexercises
Learning and discussions supportedby a structured PowerPointpresentationTopics focused on diabetes-relatedissues and concerns
Physical exercise
(i) Acquiring warm-up flexibilitystretching and strengthening exercises(ii) Learning about physical activity andglycaemic control cardiovascular healthenergy expenditure peripheral nervesmood diabetes self-management
(i) Six weekly group sessions lastingfor 90 minutes(ii) Practicing exercises andexchanging experiences in smallgroups(iii) Written material reminding ofpracticed exercises
Learning and discussions supportedby a structured PowerPointpresentationExercise intensity measured by aheart rate monitor maintained in alight-to-medium intensity rangeBlood glucose and blood pressuremeasured before and after sessions
Enhancedtreatment asusual
(i) Discussing recent laboratory findings(ii) Addressing diabetes-related concerns
(i) One group session lasting for 90minutes(ii) Patient-centered counselling inthe group
Written self-help instructions tocope with mood difficulties
because leaving these patients without any treatment wasconsidered ethically unacceptable
The interventions were considered to have a very lowpotential for causing harm Nevertheless patient informa-tion being a part of the written consent clearly stated thatthe participants can discontinue intervention at any timeparticularly if they would perceive that their symptoms havebeen worsened Qualified professionals involved in treatmentcarefully monitored patientrsquos condition and routine labora-tory results in order to provide a timely referral to physicianrsquoscare if needed In addition patients allocated to physicalexercise underwent ECG and if indicated an ergometrictest before the study Exercise intensity was measured bya heart rate monitor and maintained in a light-to-mediumintensity range whereas blood glucose and blood pressurewere measured before and after each session
A summary of the programsrsquo objectives methods ofdelivery and specific features are presented in Table 1
22 Assessments Patient demographic variables includedage sex education family status employment and economicstatus Diabetes-related variables included years of diabetesduration and diabetes treatment with or without insulin
Screening for mood difficulties was carried out using theadapted Patient Health Questionnaire-2 [21] An additionalquestion inquiring into the patientsrsquo need for help withthese difficulties was added as it has proven to improve theinstrumentrsquos validity [25]
The presence or absence of clinical depression was deter-mined by phone-administered structured clinical interviewfor the DSM-IV Axis 1 disorders as this method has beenshown to be comparable to face-to-face interview [26]
Depressive symptoms were measured by the Center forEpidemiological Studies Depression (CES-D) Scale a 20-itemself-report instrument [27]The total score of the scale ranges
from 0 to 60 points with higher scores indicating higherdepressive symptoms The reliability of the scale at baselinewas Cronbach alpha = 083
221 Laboratory Assessments HbA1c was measured by anNGSP-certified automated immunoturbidimetric method(Tina-quant HbA1c Roche Diagnostics USA) with a totalimprecision (expressed as CV) lt15 and dual reportingof the results (NGSPDCCT aligned and IFCC-alignedmmolmol)
Leukocyte count was determined in K3EDTA-wholeblood samples with ADVIA120 blood cell counter (SiemensDiagnostic Solutions USA)
Serum uric acid and hs-CRP concentrations were mea-sured by the automated enzymatic and immunoturbidimetricassays respectively (AU680 Beckman Coulter USA)
Total serum sialic acid (TSA) was determined by acolorimetric procedure as described previously [28] Serumadiponectin was measured by a commercially available sand-wich ELISA procedure (Adiponectin Human ELISA highsensitive Biovendor CZ) with declared detection limit of047 120583gL
Urinary 8-oxo-deoxyguanosine (u-8-oxodG) was mea-sured by the competitive ELISA method (New 8-OHdGCheck Japan Institute for the Control of Ageing JaiCAShizuoka Japan) with declared assay-range of 05ndash200120583gLand improved specificity [29] On the day of analysis frozenurine samples were thawed in a water-bath (37∘C) vortexedcentrifuged (10min 3000 rpm) and u-8-oxodG assayedimmediately according to the manufacturerrsquos instructionsUrinary creatinine was measured in the same samples witha compensated colorimetric Jaffe procedure (AU680 Anal-yser Beckman Coulter Brea USA) Results were normal-ized to the creatinine concentration by the formula u-8-oxodGcreatinine (120583gmmol)
International Journal of Endocrinology 5
Variables indicating a level of depressive symptoms andbiomarkers of oxidative damage and inflammation weremeasured at baseline and after six- and twelve-month follow-up periods HbA1c leukocytes serum hs-CRP and uric acidwere assayed in fresh samples obtained in the morning afteran overnight fast Samples for sialic acid adiponectin and u-8-oxodG measurements were frozen (minus70∘C) until analyzedThe samples from each patient were analyzed with ELISAs atthe samemicroplate in order to avoid possible between-seriesvariability
23 Statistical Methods Data are presented as means (SD)unless otherwise indicated Due to the nonparametric dis-tribution hs-CRP results were log-transformed prior to theanalysis One-way ANOVA and chi squares were used todetermine baseline differences across the three treatmentarms and examine differences between continuing partici-pants and dropouts
Data were analyzed per protocol after exclusion of par-ticipants who withdrew did not attend all three follow-up meetings initiated psychopharmacological treatment ordied during the study period these results are presentedthroughout the paper Intention-to-treat (ITT) analysis wasperformed to validate these results all participants whowere randomized were analyzed despite deviations from theprotocol To perform ITT missing data were imputed usingthe baseline observation carried forward approach
Repeated measures ANOVA was used to test for changesin outcome variables across time and between the groupsCohenrsquos 1205782 coefficients ranging from 001 to 005 wereregarded as small from006 to 012moderate andge013 large
Regression analysis was employed to test directionalrelations between depressive symptoms and reduction ininflammation and oxidative stress
A 119901 value of lt005 was considered significant in allanalyses
Statistical analyses were performed by using the SPSS 17(SPSS Inc Chicago IL USA)
24 Ethical Aspects The study was approved by the VukVrhovac University Clinic for Diabetes Ethics Committee onJune 30 2010 A written informed consent was obtained fromall the participants
3 Results
Among the 1740 patients assessed for eligibility 365 wereconsidered eligible and 265 agreed to participate in the inter-ventions (72) Of these 209 completed baseline laboratoryand psychological assessments (79) with 74 randomizedto psychoeducational intervention 66 to physical exerciseand 69 to diabetes reeducation Attrition rate was 3 duringthe interventions (6 of 209 patients) 3 from baseline tosix months (7 of 203 patients) and 2 from 6-month to 12-month follow-up period (4 of 196 patients) Of the sevendropouts who completed the intervention but missed bothfollow-up assessments two missed the follow-up appoint-ments due to health problems four were unwilling to comeand one patient died No harmful incidents were recorded
throughout the interventions Four patients were excludedfromper-protocol analyses due to the initiation of pharmaco-logical therapy No differences between the participants anddropouts across the three study groups were observed
Table 2 presents demographic and diabetes-related char-acteristics of patients randomized to one of the three groupsand a baseline level of depressive symptoms as self-assessedby the CES-D questionnaire No between-group differencesregarding demographic diabetes-related and psychologicalvariables were found
The effects of interventions on depressive symptoms andbiomarkers of oxidative damage and inflammation as wellas glucoregulation (HbA1c) and BMI based on repeatedmeasures ANOVA are given in Table 3 ITT analyses showeda comparable pattern of results of all analyses in terms ofstatistical significance and effect size and are not presentedin the text
31 Changes in Depressive Symptoms No significant be-tween-group differences over time were obtained with res-pect to depressive symptoms (119865 = 061 119901 = 0656) indi-cating comparable efficacy of psychoeducation physical exer-cise and enhanced treatment as usual on the primary studyoutcome
Significant reductions in depressive symptoms occurredacross all three study groups from baseline to 12 months(119865 = 1251 119901 lt 0001 1205782 = 07) The size of the time effectindicated a moderate effect of the three treatments on self-assessed depressive symptoms
32 Changes in Biomarkers of Oxidative Damage and Inflam-mation Total leukocytes significantly decreased in all threegroups (119865 = 1261 119901 lt 00001 1205782 = 007) as did u-8-oxodG (119865 = 1066 119901 lt 00001 1205782 = 006) and sialic acid(119865 = 8457 119901 lt 00001 1205782 = 032) The latter showed smallbut statistically significant time 119909 group effect (119865 = 340119901 = 001 1205782 = 004) However after adjusting the results formultiple comparisons by Bonferroni test it did not remainsignificant Uric acid increased significantly over one year inall three groups (119865 = 1339 119901 lt 00001 1205782 = 007) Theeffects of the interventions on sialic acid can be regarded aslarge (032) and on leukocytes u-8-oxodG and uric acid asmoderate (007 006 and 007 resp)
No significant changes were registered with respect toadiponectin and hs-CRP
NeitherHbA1c nor BMIwere significantly changed in anyof the study groups from baseline to 12 months
No between-group effects were obtained with respectto one-year changes in biomarkers of inflammation andoxidative damage (all 119901 gt 005)
33 Testing for Mediation The results obtained by usingregression analyses indicated that improvement in depressivesymptoms at six months predicted reductions in u-8-oxodGat twelve-month follow-up (120573 = 015 119901 = 0044) whilethe results for sialic and uric acid were close to statisticalsignificance (119901 = 0069 and 119901 = 0070 resp) (results notshown in tables)
6 International Journal of Endocrinology
Table 2 Baseline characteristics of participants by the intervention groups (119899 = 209)
Psychoeducation Physical exercise Enhanced treatment as usual Siglowast
119873 74 66 69Age (yrs) 577 (62) 585 (48) 582 (56) 0648Female (119899) 40 37 36 0867Education (yrs) 126 (24) 124 (23) 122 (25) 0623Professional status ( employed) 30 27 30 0502Economic status ( poor) 13 12 13 0317Family status ( marriedcohabitating) 76 72 76 0488Insulin use () 32 29 32 0695OHA use () 56 57 53 0664Insulin + OHA use () 12 14 15 0632Statin use () 68 71 71 0786HbA1c () 74 (12) 72 (11) 72 (11) 0384HbA1c (mmolmol) 58 (13) 56 (13) 55 (11) 0442Body mass index kgm2 3064 (454) 2944 (467) 2996 (439) 0297Depressive symptoms (CES-D score) 197 (91) 205 (86) 197 (87) 0813Data are means (SD) or percentageslowastSig significancelowast One-way ANOVA or 1205942 as appropriateOHA = oral hypoglycemic agents
4 Discussion
This randomized interventional study attempted to evaluatethe effect of two behavioral interventions psychoeducationand physical exercise as compared to enhanced treatmentas usual on depressive symptoms and the intensity ofoxidativeinflammatory processes in diabetic patients suf-fering from subsyndromal depression The results indicateprotracted favorable effects of either intervention on loweringdepressive symptoms while reducing overall oxidative dam-age and cellular inflammatory response as well as improvingantioxidant capacity
In all three study arms a comparable and clinically mean-ingful improvement in depressive symptoms was obtainedThe intervention-independent results regarding depression-related outcomes confirm our preliminary report indicatingthat treatment as usual was equally effective as psychoe-ducation in reducing depressive symptoms and improvingmetabolic control in type 2 diabetic patients with subsyndro-mal depression [30] Also no between-groupdifferenceswerefound within a randomized controlled comparison of psy-choeducation physical exercise and control arm consistingof brief diabetes reeducation [31]The absence of a significanttreatment effect suggested that patterns of change might besimilar in all treatment groups Hypothetically addressingpatientsrsquo emotional needs and their diabetes-related distresswhich were common in all three approaches may indicate apossible pathway of change Similar findings were obtained ina study by Fisher et al [32] which demonstrated that clinicallyreasonable improvements in emotional symptoms may bestimulated by even minimal behavioral interventions
In this study a significant decrease in overall oxidativedamage was observed from basal to one-year posttreatmentfollow-up by measuring a recognized biomarker of oxidativedamage to DNAmdashurinary 8-oxodG Urinary excretion of
8-oxodG reflects the average rate of nucleic acid guanineoxidation and can be regarded as a reliable marker of generalintracellular oxidative stress [33] Research on the u-8-oxodGin diabetes revealed its significant association with severehyperglycemia poor diabetes control and severity of dia-betic complications as well as predictive value for diabetes-associated morbidity [34] The relationship between u-8-oxodG and depression has been modestly investigated andprovided controversial results from an increase to no changedepending on the study-specific depression phenotype [35ndash37] To our knowledge this is the first study investigating u-8-oxodG in patients with diabetes and elevated depressivesymptoms While the results in our exercise group are inaccord with previously reported reduction in u-8-oxodGelicited bymoderate-intensity exercise in type 2 diabetes over12 months [38] significant decrease in u-8-oxodG levels inpsychoeducation and diabetes reeducation group is a novelfinding indicating that cognitive-behavioral approach mighthave beneficial effects on oxidative damage reduction indiabetic patients with subsyndromal depression Additionalsupport for this finding was a significant increase in serumuric acid level at follow-up
Uric acid is an end-product of purine metabolism withcomplex and multifarious roles in human physiology Apartfrom causing gout hyperuricemia has been identified as arisk factor for metabolic syndrome type 2 diabetes andcardiovascular diseases [39] Recently proposed intriguinghypothesis linking hyperuricemia derived by an increasedconsumption of dietary fructose with an epidemic of car-diometabolic diseases attracted a lot of attention and createda paradigm of uric acid as being an exclusively harmfulmetabolite [40] By contrast uric acid has long been recog-nized as one of the most powerful endogenous antioxidants[41] and an efficient mediator of neuroprotection cognitivefunction and intellectual performance [42] as well as the
International Journal of Endocrinology 7
Table 3 One-year changes of depressive symptoms inflammatory- and prooxidative biomarkers
Group scores BaselineM (SD)
12-month follow-upM (SD) Effects 119865 Overall 119875lowast 119875
0 to 12molowastlowast 1205782
Depressive symptomsA (119899 = 64) 197 (91) 167 (79) Time 1251 lt0001 0003 007B (119899 = 58) 198 (82) 181 (98) Time times group 061 0656 0007C (119899 = 57) 190 (86) 174 (94)
Leukocytes (times109L)A (119899 = 63) 75 (17) 73 (17) Time 1261 lt0001 lt0001 007B (119899 = 58) 75 (16) 71 (15) Time times group 132 0265 0001C (119899 = 57) 78 (22) 71 (20)
CRP (mgL)
A (119899 = 64) 028 (049) 025 (044) Time 238 009 100 001B (119899 = 57) 034 (046) 032 (041) Time times group 087 048 001C (119899 = 57) 035 (041) 024 (039)
Sialic acid (mmolL)A (119899 = 64) 21 (031) 19 (029) Time 8457 lt0001 lt0001 032B (119899 = 58) 21 (031) 18 (022) Time times group 340 001 004C (119899 = 57) 21 (028) 18 (024)
u-8-OxodG (120583gmmol)A (119899 = 64) 11 (05) 09 (04) Time 1066 lt0001 lt0001 006B (119899 = 57) 14 (08) 11 (06) Time times group 109 036 001C (119899 = 57) 12 (07) 10 (04)
Uric acid (120583molL)A (119899 = 64) 2917 (852) 3103 (775) Time 1339 lt0001 lt0001 007B (119899 = 58) 3034 (919) 3232 (931) Time times group 025 091 0003C (119899 = 57) 2904 (779) 3145 (834)
HbA1c ()A (119899 = 64) 74 (13) 72 (09) Time 270 007 008 002B (119899 = 58) 72 (10) 72 (10) Time times group 092 045 001C (119899 = 57) 71 (10) 70 (10)
HbA1c (mmolL)A (119899 = 64) 578 (136) 559 (102) Time 331 005 100 002B (119899 = 58) 548 (114) 557 (107) Time times group 090 045 001C (119899 = 57) 548 (107) 539 (100)
Adiponectin (mgL)A (119899 = 63) 75 (23) 71 (38) Time 073 044 100 0004B (119899 = 58) 91 (61) 90 (67) Time times group 055 065 0006C (119899 = 57) 80 (50) 81 (53)
Body mass index (kgm2)A (119899 = 54) 306 (47) 306 (50) Time 172 019 011 001B (119899 = 53) 292 (45) 290 (46) Time times group 131 027 001C (119899 = 52) 301 (41) 294 (40)
lowastTwo-sided significance of differences across time and between the groups (repeated measures ANOVA)lowastlowastTwo-sided significance of differences between baseline and 12-month assessmentsLog-transformed data
8 International Journal of Endocrinology
most pronounced determinant of total plasma antioxidantcapacity in diabetic patients [43] Thus maintaining uricacid levels within physiological range appears to be morefavorable than radical lowering in prevention of variousmor-bidities Based on recent epidemiological evidence includingcardiometabolic risk assessment a new gender-independentupper limit of reference range for uric acid has been proposedat the level of 360 120583molL [44] The present study revealsa significant increase in uric acid levels at follow-up butwell below proposed cut-off above which negative effectsof hyperuricemia might be expected On the contrary theobserved uric acid increase in our study is rather suggestiveof an improved antioxidant capacity elicited by behavioralinterventions in type 2 diabetic patients with subsyndromaldepression
Beneficial effect of cognitive-behavioral interventionin reducing oxidative stress and inflammatory responsehas been reported in hemodialysis patients suffering frominsomnia [45] but rather sparse depression-related studiesmainly focused on the assessment of low-grade inflammationbiomarkers In a very recent randomized trial evaluating anewly developed cognitive-behavioral program (DIAMOS)in diabetic patients with subsyndromal depression a set ofpro- and anti-inflammatory biomarkers was analyzed at basaland one-year follow-up [20] No change in hs-CRP IL-1 andadiponectin was observed whereas a significant decrease ininterleukin-1 receptor antagonist (IL-1RA) was interpreted asan indirect index of alleviated IL-1-related damaging mech-anisms presumably involved in the pathogenesis of micro-and macrovascular complications of diabetes Likewise ourstudy could not demonstrate any influence of the behavioralinterventions on hs-CRP and adiponectin but we foundother inflammatory markers that is leukocyte count andtotal serum sialic acid (TSA) significantly reduced with thelatter being largely affected (1205782 = 032) by the interventionsperformed
Sialic acids comprise a family of heterogenous monosac-charides abundantly present on the cell membranes withcomplex and multiple biological roles in cellular signalingand immunity [46] TSA is a validated inflammatory andatherogenic marker that has been proposed as a novelbiomarker of cardiovascular disease [47] Elevated levels ofTSA in newly diagnosed type 2 diabetic patients have beenlinked to the risk for later development of macrovascularcomplications [28] Interestingly TSA has been identified asa superior predictive biomarker of metabolic syndrome overthe abundantly used hs-CRP [48] Nevertheless despite theobvious advantages TSA has been largely underutilized inthe research on combined inflammatory-metabolic patholo-gies and it has not been studied in depression until this studyOur results identify TSA as a sensitive biomarker of inflam-mation degree in subsyndromally depressed diabetic patientswhereas neither of the established biomarkers of low-gradeinflammation hs-CRP and adiponectin was able to reflectthe anti-inflammatory effect of the performed interventionsSignificant decrease in leukocyte count however clearlyconfirmed postintervention attenuation of the cell-mediatedinflammation response in our patients with an importantnotice that the presence of acute infection at the assessments
was excluded by total leukocyte count lt 100 times 109L or hs-CRP lt 50 gL
The ability of psychological intervention to reduceboth depressive symptoms and inflammation has been evi-denced in depressed breast-cancer patients [49] Further-more due to the insightful study-design Thornton et alwere able to demonstrate a bidirectional mechanistic rela-tionship between depressive symptoms and inflammationThe paradigmatic view of the low-grade inflammation asthe inflicting mechanism for depression has been at leastcomplemented if not refuted by their finding on the mecha-nistic role of depressive symptoms lowering in the reductionof inflammatory response [49] This explanatory mecha-nism might also be translated to our results particularlyconsidering a lack of any effect of interventions towardshyperglycemia and obesity in our study
It is well known that the intensity of oxidative damage andinflammation in diabetes is remarkably and positively asso-ciated with the severity of hyperglycemia [18] Howeverthe observed reduction in oxidative damage and low-gradeinflammation in our study could not be attributed to thismechanism since no significant changes from baseline tofollow-up were found in HbA1c clinically considered toreflect a fair glucoregulation (Table 3) Obesity-derived low-grade inflammation is another recognized harmful compo-nent in the pathogenesis of type 2 diabetes and its compli-cations [50] Obesity induces a disbalance between pro- andanti-inflammatory cytokinesadipokines resulting in low-grade inflammation and related adverse health outcomesranging from metabolic syndrome and diabetes to cardio-vascular diseases and cancer as well as depression [49ndash51]Reduction in bodyweight is accompanied by beneficialmeta-bolic and hormonal profiles and a reduced inflammation [52]with increased production of anti-inflammatory adipokineadiponectin suggested to be among themost relevant features[53] Since our subjects classified as overweightobese [54]retained their BMI at follow-up and revealed no changes inadiponectin levels it is likely that the observed effects ofinterventions on the reduction in depressive symptoms andoxidativeinflammatory biomarkers in this study dependedon another mechanism(s)
Chronic stress with deregulation of stress-response adap-tive mechanisms is considered to be a common feature ofboth diabetes and depression [55] There is a growing bodyof evidence suggesting that metabolic inflammation asso-ciated with obesity and diabetes inflicts neuroinflammationwhich causes serious disturbances of the hypothalamic-pituitary-adrenal (HPA) axis function and consequentlyleads to impairment of adaptive stress-response [56] More-over chronic stress exposure has recently been demonstratedas a promoting factor for accelerated oxidative damagewhereby a sustained activation of HPA-axis emerged again asthe key mediator [57] Neuroendocrine effects of behavioraltreatment for depression have not been extensively studiedbut the evidence so far suggests a hypothetical pathway thatconnects the nurturing effects derived from the patient-ther-apist ldquobondrdquo with reestablishment of neuroendocrine home-ostasis [58] Moreover positive effects of physical exercise onpreventing potentially harmful stress-related metabolic and
International Journal of Endocrinology 9
psychological consequences have been presumably mediatedby the same neuroendocrine mechanisms [59] Consideringunchanged metabolic profile of our subjects and remark-able improvements in depressive symptoms and oxida-tiveinflammatory biomarkers following either behavioralintervention it is tempting if not plausible to speculate onthe involvement of neuroendocrine mechanism(s) in achiev-ing this beneficial response It should be noted that a lackof between-group differences in changes observed in ourstudy might not be explained by a phenomenon known asldquoregression toward the meanrdquo or just a natural course ofparameters Previous findings on persistence of depressivesymptoms in people with type 2 diabetes indicate thatdepression is not only persistent [60 61] but also associatedwith an increased risk of aggravating over time [62] On theother hand oxidative damage toDNA is increasing in healthysubjects throughout time as a result of ageing process [33]while inflammatory response and ageing-associated damageto biomolecules are even more pronounced in diabetes dueto a long-term exposure to hyperglycemia and advanced-glycated end-products [34 50]
The strengths of this study are in examining a highlyprevalent population of type 2 patients with depressive symp-toms but no clinical depression using a randomized com-parative design employing structured behavioral interven-tions and analyzing clinically relevant changes of simple-to-measure oxidativeinflammatory biomarkers Its limitation isthe lack of treatment as usual control intervention precludingthe possibility to investigate the course and outcomes ofsubclinical depression without any treatment Also the studywas carried out in only one centermdasha tertiary diabetesclinicmdashwhich does not allow concluding about its feasibilityin other clinical settings Per-protocol analyses are presentedin the study results which were confirmed by the intention totreat analysis based on baseline-observation-carried-forwardapproach A lack of estimation derived frommultiple predic-tors may be considered a limitation of the study
5 Conclusions
This study has demonstrated that improvement in depressivesymptoms is accompanied with reduced oxidative dam-age and inflammatory response in type 2 diabetic patientswith subsyndromal depression Testing mediating effectshas indicated that medium-term improvement in depres-sive symptoms predicts long-term-reduction in oxidativedamage while mediating factors for observed reductionin inflammatory response should be further investigatedClinical benefits of treating subsyndromal depression wereshown to be comparable in all three treatment arms
Regardless of the mechanisms involved our study clearlyindicates that enhanced treatment as usual defined as briefpatient-centred diabetes reeducation is not inferior to psy-choeducation and exercise in providing beneficial outcomesin subsyndromally depressed type 2 diabetic patients Simplebehavioral interventions are capable not only of alleviatingdepressive symptoms but also of reducing the intensity ofdamaging oxidativeinflammatory processes thereby miti-gating the risk of development of diabetic complications
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The study was funded by the European Foundation forthe Study of Diabetes (EFSD)mdashNew Horizons CollaborativeResearch Initiative 2010 The authors would like to thankLovorka Perkovic Croatian Institute of Public Health forediting the paper
References
[1] S S Ali M A Stone J L Peters M J Davies and K KhuntildquoThe prevalence of co-morbid depression in adults with Type2 diabetes a systematic review and meta-analysisrdquo DiabeticMedicine vol 23 no 11 pp 1165ndash1173 2006
[2] P J Lustman R J Anderson K E Freedland M de Groot RM Carney and R E Clouse ldquoDepression and poor glycemiccontrol a meta-analytic review of the literaturerdquo Diabetes Carevol 23 no 7 pp 934ndash942 2000
[3] L K Richardson L E Egede M Mueller C L Echols and MGebregziabher ldquoLongitudinal effects of depression on glycemiccontrol in veterans with Type 2 diabetesrdquo General HospitalPsychiatry vol 30 no 6 pp 509ndash514 2008
[4] M de Groot R Anderson K E Freedland R E Clouse andP J Lustman ldquoAssociation of depression and diabetes com-plications ameta-analysisrdquo PsychosomaticMedicine vol 63 no4 pp 619ndash630 2001
[5] K Ismail KWinkley D Stahl T Chalder andM Edmonds ldquoAcohort study of people with diabetes and their first foot ulcerthe role of depression on mortalityrdquo Diabetes Care vol 30 no6 pp 1473ndash1479 2007
[6] X Zhang S L Norris E W Gregg Y J Cheng G Becklesand H S Kahn ldquoDepressive symptoms and mortality amongpersons with and without diabetesrdquo American Journal of Epi-demiology vol 161 no 7 pp 652ndash660 2005
[7] S A Black K S Markides and L A Ray ldquoDepression pre-dicts increased incidence of adverse health outcomes in olderMexican Americans with type 2 diabetesrdquo Diabetes Care vol26 no 10 pp 2822ndash2828 2003
[8] H Baumeister N Hutter and J Bengel ldquoPsychological andpharmacological interventions for depression in patients withdiabetesmellitus and depressionrdquoCochraneDatabase of System-atic Reviews vol 12 Article ID CD008381 2012
[9] E Harkness W Macdonald J Valderas P Coventry L Gaskand P Bower ldquoIdentifying psychosocial interventions thatimprove both physical and mental health in patients with dia-betes a systematic review and meta-analysisrdquo Diabetes Carevol 33 no 4 pp 926ndash930 2010
[10] M Berk L J Williams F N Jacka et al ldquoSo depression is aninflammatory disease but where does the inflammation comefromrdquo BMCMedicine vol 11 article 200 2013
[11] S de Kort D Keszthelyi and A A M Masclee ldquoLeaky gut anddiabetes mellitus what is the linkrdquoObesity Reviews vol 12 no6 pp 449ndash458 2011
[12] E T de Lemos J Oliveira J P Pinheiro and F Reis ldquoRegularphysical exercise as a strategy to improve antioxidant andanti-inflammatory status benefits in type 2 diabetes mellitusrdquo
10 International Journal of Endocrinology
Oxidative Medicine and Cellular Longevity vol 2012 Article ID741545 15 pages 2012
[13] T A Doyle M de Groot T Harris et al ldquoDiabetes depressivesymptoms and inflammation in older adults results fromthe Health Aging and Body Composition Studyrdquo Journal ofPsychosomatic Research vol 75 no 5 pp 419ndash424 2013
[14] J-P S Laake D Stahl S A Amiel et al ldquoThe associationbetween depressive symptoms and systemic inflammation inpeople with type 2 diabetes findings from the South Londondiabetes studyrdquoDiabetes Care vol 37 no 8 pp 2186ndash2192 2014
[15] N Rohleder ldquoStimulation of systemic low-grade inflammationby psychosocial stressrdquo Psychosomatic Medicine vol 76 no 3pp 181ndash189 2014
[16] M Maes ldquoAn intriguing and hitherto unexplained co-occur-rence depression and chronic fatigue syndrome are mani-festations of shared inflammatory oxidative and nitrosative(IOampNS) pathwaysrdquo Progress in Neuro-Psychopharmacologyand Biological Psychiatry vol 35 no 3 pp 784ndash794 2011
[17] P Palta L J Samuel E RMiller and S L Szanton ldquoDepressionand oxidative stress results from a meta-analysis of observa-tional studiesrdquo Psychosomatic Medicine vol 76 no 1 pp 12ndash192014
[18] L Rochette M Zeller Y Cottin and C Vergely ldquoDiabetes oxi-dative stress and therapeutic strategiesrdquo Biochimica et Biophys-ica Acta vol 1840 no 9 pp 2709ndash2729 2014
[19] S Keri C Szabo and O Kelemen ldquoExpression of Toll-LikeReceptors in peripheral blood mononuclear cells and responseto cognitive-behavioral therapy in major depressive disorderrdquoBrain Behavior and Immunity vol 40 pp 235ndash243 2014
[20] N Hermanns A Schmitt A Gahr et al ldquoThe effect ofa Diabetes-Specific Cognitive Behavioral Treatment Program(DIAMOS) for patients with diabetes and subclinical depres-sion results of a randomized controlled trialrdquo Diabetes Carevol 38 no 4 pp 551ndash560 2015
[21] K Kroenke R L Spitzer and J B W Williams ldquoThe patienthealth questionnaire-2 validity of a two-item depressionscreenerrdquoMedical Care vol 41 no 11 pp 1284ndash1292 2003
[22] J H Abramson ldquoWINPEPI updated computer programs forepidemiologists and their teaching potentialrdquo EpidemiologicPerspectives amp Innovations vol 8 no 1 article 1 2011
[23] J Cohen ldquoA power primerrdquo Psychological Bulletin vol 112 no1 pp 155ndash159 1992
[24] M Pibernik-Okanovic D Ajdukovic M V Lovrencic andN Hermanns ldquoDoes treatment of subsyndromal depressionimprove depression and diabetes related outcomes protocolfor a randomised controlled comparison of psycho-educationphysical exercise and treatment as usualrdquo Trials vol 12 article17 2011
[25] BArroll FGoodyear-SmithNKerse T Fishman and JGunnldquoEffect of the addition of a lsquohelprsquo question to two screeningquestions on specificity for diagnosis of depression in generalpractice diagnostic validity studyrdquo British Medical Journal vol331 no 7521 article 884 2005
[26] P Rohde P M Lewinsohn and J R Seeley ldquoComparability oftelephone and face-to-face interviews in assessing axis I and IIdisordersrdquo American Journal of Psychiatry vol 154 no 11 pp1593ndash1598 1997
[27] L S Radloff ldquoTheCES-D scalerdquoApplied Psychological Measure-ment vol 1 pp 385ndash401 1977
[28] M Gavella V Lipovac A Car M Vucic L Sokolic and RRakos ldquoSerum sialic acid in subjects with impaired glucose
tolerance and in newly diagnosed type 2 diabetic patientsrdquoActaDiabetologica vol 40 no 2 pp 95ndash100 2003
[29] M D Evans R Singh V Mistry K Sandhu P B Farmer andM S Cooke ldquoAnalysis of urinary 8-oxo-78-dihydro-purine-21015840- deoxyribonucleosides by LC-MSMS and improved ELISArdquoFree Radical Research vol 42 no 10 pp 831ndash840 2008
[30] M Pibernik-Okanovic D Begic D Ajdukovic N Andrijasevicand Z Metelko ldquoPsychoeducation versus treatment as usualin diabetic patients with subthreshold depression preliminaryresults of a randomized controlled trialrdquo Trials vol 10 article78 2009
[31] M Pibernik-Okanovic M Vucic Lovrencic D AjdukovicM Sekerija and N Hermanns ldquoPsychological behavioraland biological changes following treatments of subsyndromaldepression in people with type 2 diabetesrdquoDiabetologia vol 56supplement 1 p S465 2013
[32] L Fisher D Hessler R E Glasgow et al ldquoREDEEM a prag-matic trial to reduce diabetes distressrdquo Diabetes Care vol 36no 9 pp 2551ndash2558 2013
[33] H E Poulsen L L Nadal K Broedbaek P E Nielsen andA Weimann ldquoDetection and interpretation of 8-oxodG and 8-oxoGua in urine plasma and cerebrospinal fluidrdquo Biochimica etBiophysica ActamdashGeneral Subjects vol 1840 no 2 pp 801ndash8082014
[34] K Broedbaek A Weimann E S Stovgaard and H E PoulsenldquoUrinary 8-oxo-78-dihydro-21015840-deoxyguanosine as a biomarkerin type 2 diabetesrdquo Free Radical Biology and Medicine vol 51no 8 pp 1473ndash1479 2011
[35] M J Forlenza and G E Miller ldquoIncreased serum levels of 8-hydroxy-21015840-deoxyguanosine in clinical depressionrdquo Psychoso-matic Medicine vol 68 no 1 pp 1ndash7 2006
[36] A Jorgensen J Krogh K Miskowiak et al ldquoSystemic oxida-tively generatedDNARNAdamage in clinical depression asso-ciations to symptom severity and response to electroconvulsivetherapyrdquo Journal of Affective Disorders vol 149 no 1ndash3 pp 355ndash362 2013
[37] S Yi ANanri YMatsushitaHKasai K Kawai andTMizoueldquoDepressive symptoms and oxidative DNA damage in Japanesemunicipal employeesrdquo Psychiatry Research vol 200 no 2-3 pp318ndash322 2012
[38] H Nojima H Watanabe K Yamane et al ldquoEffect of aerobicexercise training on oxidative stress in patients with type 2diabetes mellitusrdquo Metabolism Clinical and Experimental vol57 no 2 pp 170ndash176 2008
[39] S Bonakdaran and B Kharaqani ldquoAssociation of serum uricacid and metabolic syndrome in type 2 diabetesrdquo CurrentDiabetes Reviews vol 10 no 2 pp 113ndash117 2014
[40] R J Johnson T Nakagawa L G Sanchez-Lozada et al ldquoSugaruric acid and the etiology of diabetes and obesityrdquoDiabetes vol62 no 10 pp 3307ndash3315 2013
[41] M L Wahlqvist ldquoAntioxidant relevance to human healthrdquo AsiaPacific Journal of Clinical Nutrition vol 22 no 2 pp 171ndash1762013
[42] A De Giorgi F Fabbian M Pala et al ldquoUric acid friend orfoe Uric acid and cognitive function lsquogout kills more wise menthan simplersquordquo European Review forMedical and PharmacologicalSciences vol 19 no 4 pp 640ndash646 2015
[43] M Vucic B Rocic V Bozikov and S J H Ashcroft ldquoPlasmauric acid and total antioxidant status in patients with diabetesmellitusrdquo Hormone and Metabolic Research vol 29 no 7 pp355ndash357 1997
International Journal of Endocrinology 11
[44] G Desideri G Castaldo A Lombardi et al ldquoIs it time to revisethe normal range of serum uric acid levelsrdquo European Reviewfor Medical and Pharmacological Sciences vol 18 no 9 pp1295ndash1306 2014
[45] H-Y Chen I-C Cheng Y-J Pan et al ldquoCognitive-behavioraltherapy for sleep disturbance decreases inflammatory cytokinesand oxidative stress in hemodialysis patientsrdquo Kidney Interna-tional vol 80 no 4 pp 415ndash422 2011
[46] A Varki and P Gagneux ldquoMultifarious roles of sialic acids inimmunityrdquo Annals of the New York Academy of Sciences vol1253 no 1 pp 16ndash36 2012
[47] K P Gopaul and M A Crook ldquoSialic acid a novel marker ofcardiovascular diseaserdquo Clinical Biochemistry vol 39 no 7 pp667ndash681 2006
[48] L M Browning S A Jebb G D Mishra et al ldquoElevated sialicacid but not CRP predicts features of the metabolic syndromeindependently of BMI in womenrdquo International Journal ofObesity vol 28 no 8 pp 1004ndash1010 2004
[49] LMThornton B L Andersen T A Schuler andW E CarsonldquoA psychological intervention reduces inflammatory markersby alleviating depressive symptoms secondary analysis of arandomized controlled trialrdquo Psychosomatic Medicine vol 71no 7 pp 715ndash724 2009
[50] N Esser S Legrand-Poels J Piette A J Scheen and N PaquotldquoInflammation as a link between obesity metabolic syndromeand type 2 diabetesrdquoDiabetes Research andClinical Practice vol105 no 2 pp 141ndash150 2014
[51] R Hutcheson and P Rocic ldquoThe metabolic syndrome oxida-tive stress environment and cardiovascular disease the greatexplorationrdquo Experimental Diabetes Research vol 2012 ArticleID 271028 13 pages 2012
[52] L Fontana and F B Hu ldquoOptimal body weight for health andlongevity bridging basic clinical and population researchrdquoAging Cell vol 13 no 3 pp 391ndash400 2014
[53] A T Turer and P E Scherer ldquoAdiponectin mechanistic insightsand clinical implicationsrdquo Diabetologia vol 55 no 9 pp 2319ndash2326 2012
[54] WHO ldquoObesity and overweightrdquo Fact sheet No 311 2015[55] P W Gold ldquoThe organization of the stress system and its
dysregulation in depressive illnessrdquo Molecular Psychiatry vol20 no 1 pp 32ndash47 2015
[56] S Purkayastha and D Cai ldquoNeuroinflammatory basis ofmetabolic syndromerdquo Molecular Metabolism vol 2 no 4 pp356ndash363 2013
[57] K Aschbacher A OrsquoDonovan O MWolkowitz F S DhabharY Su and E Epel ldquoGood stress bad stress and oxidative stressinsights from anticipatory cortisol reactivityrdquo Psychoneuroen-docrinology vol 38 no 9 pp 1698ndash1708 2013
[58] C F Sharpley ldquoA review of the neurobiological effects of psy-chotherapy for depressionrdquo Psychotherapy vol 47 no 4 pp603ndash615 2010
[59] M N Silverman and P A Deuster ldquoBiological mechanismsunderlying the role of physical fitness in health and resiliencerdquoInterface Focus vol 4 no 5 Article ID 20140040 2014
[60] G Nefs F Pouwer J Denollet and V Pop ldquoThe course ofdepressive symptoms in primary care patients with type 2 dia-betes results from theDiabetes Depression TypeDPersonalityZuidoost-Brabant (DiaDDZoB) Studyrdquo Diabetologia vol 55no 3 pp 608ndash616 2012
[61] M Pibernik-Okanovic D Begic K Peros S Szabo andZ Metelko ldquoPsychosocial factors contributing to persistent
depressive symptoms in type 2 diabetic patients a Croatiansurvey from the European Depression in Diabetes ResearchConsortiumrdquo Journal of Diabetes and Its Complications vol 22no 4 pp 246ndash253 2008
[62] M Bot F Pouwer J Ormel J P J Slaets and P de Jonge ldquoPre-dictors of incidentmajor depression in diabetic outpatients withsubthreshold depressionrdquo Diabetic Medicine vol 27 no 11 pp1295ndash1301 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

International Journal of Endocrinology 3
Received psychoeducational
Enro
lmen
tA
lloca
tion
Lost at 6-month assessment Lost at 6-month assessment Lost at 6-month assessment
6-m
onth
assessments) assessments) assessments)
Ana
lysis
Lost at 12-month assessment Lost at 12-month
Lost at 12-month assessment
12-m
onth
fo
llow
-up
follo
w-u
p
Uneligible = 968
Did not report depressive symptoms = 763
Expressed no need for receiving professionalhelp = 205
Did not enter the study = 156
Refused to join the groups = 58
Unreachable after initial contact = 42
Randomised no show at baseline = 56
Excluded = 407
Clinical depressionpsychiatrictreatment = 134
Severe physical limitation = 94
Both physicalpsychiatric limitations = 55
Other obstacles for participation = 124
Randomized completed baseline assessment = 209
Received diabetes reeducation
Psychoeducation (n = 74)
intervention (n = 71)
withdrew (n = 3)
Physical exercise (n = 66)
intervention (n = 64)
withdrew (n = 2)
Diabetes reeducation (n = 69)
Did not receive intervention- Did not receive intervention-
Received physical exercise
(n = 68)
withdrew (n = 1)Did not receive education-
(n = 2)
(n = 5) (n = 3)
Withdrew (n = 1) missed (n = 1)(n = 6) (n = 8)
Withdrew (n = 3) missed (n = 3) Withdrew (n = 3) missed (n = 5)
Withdrew (n = 2) excluded Withdrew (n = 2) excludedassessment (n = 0)
from analysis (n = 1)from analysis (n = 3)
Analysed n = 58 (with all three Analysed n = 57 (with all threeAnalysed n = 64 (with all three
Assessed for eligibility (n = 1740)
Figure 1 Patientsrsquo flow diagram
shown to be needed to have 80 power in demonstratingstatistically significant differences in depressive symptoms Amore detailed study procedure was described elsewhere [24]
The study was carried out at the Vuk Vrhovac UniversityClinic for DiabetesmdashReference Centre for Diabetes Mellitusin Zagreb Croatia Laboratory analyses were performed atthe Department of Laboratory Medicine Merkur UniversityHospital accredited according to the ISO 151892012 ldquomedi-cal laboratoriesmdashrequirements for quality and competencerdquostandard
21 The Intervention Arms Psychoeducation Physical Exer-cise and Enhanced Treatment as Usual Two interven-tion programsmdashpsychoeducation and physical exercisemdashandenhanced treatment as usual consisting of brief diabetes reed-ucation were offered to patients reporting elevated depressivesymptoms and a need for receiving professional help inmood-related difficulties The intervention programs weredelivered in small groups attending six 90-minute weekly ses-sions One 90-minute intervention sessionmdashenhanced treat-ment as usualmdashwas offered to the control study participants
4 International Journal of Endocrinology
Table 1 Programsrsquo objectives methods of delivery and specific features
Study arm Objectives Methods of delivery Specific features
Psychoeducation
(i) Recognizing and understanding feelings(ii) Becoming aware of dysfunctionalthinking patterns(iii) Improving mood by pleasant activities(iv) Improving mood by solving problems(v) Managing automatic negative thoughts(vi) Communicating assertively providingsupport
(i) Six weekly group sessions lastingfor 90 minutes(ii) Interactive learning in smallgroups (5ndash8 participants)(iii) Self-help manual(iv) Workbook with practicalexercises
Learning and discussions supportedby a structured PowerPointpresentationTopics focused on diabetes-relatedissues and concerns
Physical exercise
(i) Acquiring warm-up flexibilitystretching and strengthening exercises(ii) Learning about physical activity andglycaemic control cardiovascular healthenergy expenditure peripheral nervesmood diabetes self-management
(i) Six weekly group sessions lastingfor 90 minutes(ii) Practicing exercises andexchanging experiences in smallgroups(iii) Written material reminding ofpracticed exercises
Learning and discussions supportedby a structured PowerPointpresentationExercise intensity measured by aheart rate monitor maintained in alight-to-medium intensity rangeBlood glucose and blood pressuremeasured before and after sessions
Enhancedtreatment asusual
(i) Discussing recent laboratory findings(ii) Addressing diabetes-related concerns
(i) One group session lasting for 90minutes(ii) Patient-centered counselling inthe group
Written self-help instructions tocope with mood difficulties
because leaving these patients without any treatment wasconsidered ethically unacceptable
The interventions were considered to have a very lowpotential for causing harm Nevertheless patient informa-tion being a part of the written consent clearly stated thatthe participants can discontinue intervention at any timeparticularly if they would perceive that their symptoms havebeen worsened Qualified professionals involved in treatmentcarefully monitored patientrsquos condition and routine labora-tory results in order to provide a timely referral to physicianrsquoscare if needed In addition patients allocated to physicalexercise underwent ECG and if indicated an ergometrictest before the study Exercise intensity was measured bya heart rate monitor and maintained in a light-to-mediumintensity range whereas blood glucose and blood pressurewere measured before and after each session
A summary of the programsrsquo objectives methods ofdelivery and specific features are presented in Table 1
22 Assessments Patient demographic variables includedage sex education family status employment and economicstatus Diabetes-related variables included years of diabetesduration and diabetes treatment with or without insulin
Screening for mood difficulties was carried out using theadapted Patient Health Questionnaire-2 [21] An additionalquestion inquiring into the patientsrsquo need for help withthese difficulties was added as it has proven to improve theinstrumentrsquos validity [25]
The presence or absence of clinical depression was deter-mined by phone-administered structured clinical interviewfor the DSM-IV Axis 1 disorders as this method has beenshown to be comparable to face-to-face interview [26]
Depressive symptoms were measured by the Center forEpidemiological Studies Depression (CES-D) Scale a 20-itemself-report instrument [27]The total score of the scale ranges
from 0 to 60 points with higher scores indicating higherdepressive symptoms The reliability of the scale at baselinewas Cronbach alpha = 083
221 Laboratory Assessments HbA1c was measured by anNGSP-certified automated immunoturbidimetric method(Tina-quant HbA1c Roche Diagnostics USA) with a totalimprecision (expressed as CV) lt15 and dual reportingof the results (NGSPDCCT aligned and IFCC-alignedmmolmol)
Leukocyte count was determined in K3EDTA-wholeblood samples with ADVIA120 blood cell counter (SiemensDiagnostic Solutions USA)
Serum uric acid and hs-CRP concentrations were mea-sured by the automated enzymatic and immunoturbidimetricassays respectively (AU680 Beckman Coulter USA)
Total serum sialic acid (TSA) was determined by acolorimetric procedure as described previously [28] Serumadiponectin was measured by a commercially available sand-wich ELISA procedure (Adiponectin Human ELISA highsensitive Biovendor CZ) with declared detection limit of047 120583gL
Urinary 8-oxo-deoxyguanosine (u-8-oxodG) was mea-sured by the competitive ELISA method (New 8-OHdGCheck Japan Institute for the Control of Ageing JaiCAShizuoka Japan) with declared assay-range of 05ndash200120583gLand improved specificity [29] On the day of analysis frozenurine samples were thawed in a water-bath (37∘C) vortexedcentrifuged (10min 3000 rpm) and u-8-oxodG assayedimmediately according to the manufacturerrsquos instructionsUrinary creatinine was measured in the same samples witha compensated colorimetric Jaffe procedure (AU680 Anal-yser Beckman Coulter Brea USA) Results were normal-ized to the creatinine concentration by the formula u-8-oxodGcreatinine (120583gmmol)
International Journal of Endocrinology 5
Variables indicating a level of depressive symptoms andbiomarkers of oxidative damage and inflammation weremeasured at baseline and after six- and twelve-month follow-up periods HbA1c leukocytes serum hs-CRP and uric acidwere assayed in fresh samples obtained in the morning afteran overnight fast Samples for sialic acid adiponectin and u-8-oxodG measurements were frozen (minus70∘C) until analyzedThe samples from each patient were analyzed with ELISAs atthe samemicroplate in order to avoid possible between-seriesvariability
23 Statistical Methods Data are presented as means (SD)unless otherwise indicated Due to the nonparametric dis-tribution hs-CRP results were log-transformed prior to theanalysis One-way ANOVA and chi squares were used todetermine baseline differences across the three treatmentarms and examine differences between continuing partici-pants and dropouts
Data were analyzed per protocol after exclusion of par-ticipants who withdrew did not attend all three follow-up meetings initiated psychopharmacological treatment ordied during the study period these results are presentedthroughout the paper Intention-to-treat (ITT) analysis wasperformed to validate these results all participants whowere randomized were analyzed despite deviations from theprotocol To perform ITT missing data were imputed usingthe baseline observation carried forward approach
Repeated measures ANOVA was used to test for changesin outcome variables across time and between the groupsCohenrsquos 1205782 coefficients ranging from 001 to 005 wereregarded as small from006 to 012moderate andge013 large
Regression analysis was employed to test directionalrelations between depressive symptoms and reduction ininflammation and oxidative stress
A 119901 value of lt005 was considered significant in allanalyses
Statistical analyses were performed by using the SPSS 17(SPSS Inc Chicago IL USA)
24 Ethical Aspects The study was approved by the VukVrhovac University Clinic for Diabetes Ethics Committee onJune 30 2010 A written informed consent was obtained fromall the participants
3 Results
Among the 1740 patients assessed for eligibility 365 wereconsidered eligible and 265 agreed to participate in the inter-ventions (72) Of these 209 completed baseline laboratoryand psychological assessments (79) with 74 randomizedto psychoeducational intervention 66 to physical exerciseand 69 to diabetes reeducation Attrition rate was 3 duringthe interventions (6 of 209 patients) 3 from baseline tosix months (7 of 203 patients) and 2 from 6-month to 12-month follow-up period (4 of 196 patients) Of the sevendropouts who completed the intervention but missed bothfollow-up assessments two missed the follow-up appoint-ments due to health problems four were unwilling to comeand one patient died No harmful incidents were recorded
throughout the interventions Four patients were excludedfromper-protocol analyses due to the initiation of pharmaco-logical therapy No differences between the participants anddropouts across the three study groups were observed
Table 2 presents demographic and diabetes-related char-acteristics of patients randomized to one of the three groupsand a baseline level of depressive symptoms as self-assessedby the CES-D questionnaire No between-group differencesregarding demographic diabetes-related and psychologicalvariables were found
The effects of interventions on depressive symptoms andbiomarkers of oxidative damage and inflammation as wellas glucoregulation (HbA1c) and BMI based on repeatedmeasures ANOVA are given in Table 3 ITT analyses showeda comparable pattern of results of all analyses in terms ofstatistical significance and effect size and are not presentedin the text
31 Changes in Depressive Symptoms No significant be-tween-group differences over time were obtained with res-pect to depressive symptoms (119865 = 061 119901 = 0656) indi-cating comparable efficacy of psychoeducation physical exer-cise and enhanced treatment as usual on the primary studyoutcome
Significant reductions in depressive symptoms occurredacross all three study groups from baseline to 12 months(119865 = 1251 119901 lt 0001 1205782 = 07) The size of the time effectindicated a moderate effect of the three treatments on self-assessed depressive symptoms
32 Changes in Biomarkers of Oxidative Damage and Inflam-mation Total leukocytes significantly decreased in all threegroups (119865 = 1261 119901 lt 00001 1205782 = 007) as did u-8-oxodG (119865 = 1066 119901 lt 00001 1205782 = 006) and sialic acid(119865 = 8457 119901 lt 00001 1205782 = 032) The latter showed smallbut statistically significant time 119909 group effect (119865 = 340119901 = 001 1205782 = 004) However after adjusting the results formultiple comparisons by Bonferroni test it did not remainsignificant Uric acid increased significantly over one year inall three groups (119865 = 1339 119901 lt 00001 1205782 = 007) Theeffects of the interventions on sialic acid can be regarded aslarge (032) and on leukocytes u-8-oxodG and uric acid asmoderate (007 006 and 007 resp)
No significant changes were registered with respect toadiponectin and hs-CRP
NeitherHbA1c nor BMIwere significantly changed in anyof the study groups from baseline to 12 months
No between-group effects were obtained with respectto one-year changes in biomarkers of inflammation andoxidative damage (all 119901 gt 005)
33 Testing for Mediation The results obtained by usingregression analyses indicated that improvement in depressivesymptoms at six months predicted reductions in u-8-oxodGat twelve-month follow-up (120573 = 015 119901 = 0044) whilethe results for sialic and uric acid were close to statisticalsignificance (119901 = 0069 and 119901 = 0070 resp) (results notshown in tables)
6 International Journal of Endocrinology
Table 2 Baseline characteristics of participants by the intervention groups (119899 = 209)
Psychoeducation Physical exercise Enhanced treatment as usual Siglowast
119873 74 66 69Age (yrs) 577 (62) 585 (48) 582 (56) 0648Female (119899) 40 37 36 0867Education (yrs) 126 (24) 124 (23) 122 (25) 0623Professional status ( employed) 30 27 30 0502Economic status ( poor) 13 12 13 0317Family status ( marriedcohabitating) 76 72 76 0488Insulin use () 32 29 32 0695OHA use () 56 57 53 0664Insulin + OHA use () 12 14 15 0632Statin use () 68 71 71 0786HbA1c () 74 (12) 72 (11) 72 (11) 0384HbA1c (mmolmol) 58 (13) 56 (13) 55 (11) 0442Body mass index kgm2 3064 (454) 2944 (467) 2996 (439) 0297Depressive symptoms (CES-D score) 197 (91) 205 (86) 197 (87) 0813Data are means (SD) or percentageslowastSig significancelowast One-way ANOVA or 1205942 as appropriateOHA = oral hypoglycemic agents
4 Discussion
This randomized interventional study attempted to evaluatethe effect of two behavioral interventions psychoeducationand physical exercise as compared to enhanced treatmentas usual on depressive symptoms and the intensity ofoxidativeinflammatory processes in diabetic patients suf-fering from subsyndromal depression The results indicateprotracted favorable effects of either intervention on loweringdepressive symptoms while reducing overall oxidative dam-age and cellular inflammatory response as well as improvingantioxidant capacity
In all three study arms a comparable and clinically mean-ingful improvement in depressive symptoms was obtainedThe intervention-independent results regarding depression-related outcomes confirm our preliminary report indicatingthat treatment as usual was equally effective as psychoe-ducation in reducing depressive symptoms and improvingmetabolic control in type 2 diabetic patients with subsyndro-mal depression [30] Also no between-groupdifferenceswerefound within a randomized controlled comparison of psy-choeducation physical exercise and control arm consistingof brief diabetes reeducation [31]The absence of a significanttreatment effect suggested that patterns of change might besimilar in all treatment groups Hypothetically addressingpatientsrsquo emotional needs and their diabetes-related distresswhich were common in all three approaches may indicate apossible pathway of change Similar findings were obtained ina study by Fisher et al [32] which demonstrated that clinicallyreasonable improvements in emotional symptoms may bestimulated by even minimal behavioral interventions
In this study a significant decrease in overall oxidativedamage was observed from basal to one-year posttreatmentfollow-up by measuring a recognized biomarker of oxidativedamage to DNAmdashurinary 8-oxodG Urinary excretion of
8-oxodG reflects the average rate of nucleic acid guanineoxidation and can be regarded as a reliable marker of generalintracellular oxidative stress [33] Research on the u-8-oxodGin diabetes revealed its significant association with severehyperglycemia poor diabetes control and severity of dia-betic complications as well as predictive value for diabetes-associated morbidity [34] The relationship between u-8-oxodG and depression has been modestly investigated andprovided controversial results from an increase to no changedepending on the study-specific depression phenotype [35ndash37] To our knowledge this is the first study investigating u-8-oxodG in patients with diabetes and elevated depressivesymptoms While the results in our exercise group are inaccord with previously reported reduction in u-8-oxodGelicited bymoderate-intensity exercise in type 2 diabetes over12 months [38] significant decrease in u-8-oxodG levels inpsychoeducation and diabetes reeducation group is a novelfinding indicating that cognitive-behavioral approach mighthave beneficial effects on oxidative damage reduction indiabetic patients with subsyndromal depression Additionalsupport for this finding was a significant increase in serumuric acid level at follow-up
Uric acid is an end-product of purine metabolism withcomplex and multifarious roles in human physiology Apartfrom causing gout hyperuricemia has been identified as arisk factor for metabolic syndrome type 2 diabetes andcardiovascular diseases [39] Recently proposed intriguinghypothesis linking hyperuricemia derived by an increasedconsumption of dietary fructose with an epidemic of car-diometabolic diseases attracted a lot of attention and createda paradigm of uric acid as being an exclusively harmfulmetabolite [40] By contrast uric acid has long been recog-nized as one of the most powerful endogenous antioxidants[41] and an efficient mediator of neuroprotection cognitivefunction and intellectual performance [42] as well as the
International Journal of Endocrinology 7
Table 3 One-year changes of depressive symptoms inflammatory- and prooxidative biomarkers
Group scores BaselineM (SD)
12-month follow-upM (SD) Effects 119865 Overall 119875lowast 119875
0 to 12molowastlowast 1205782
Depressive symptomsA (119899 = 64) 197 (91) 167 (79) Time 1251 lt0001 0003 007B (119899 = 58) 198 (82) 181 (98) Time times group 061 0656 0007C (119899 = 57) 190 (86) 174 (94)
Leukocytes (times109L)A (119899 = 63) 75 (17) 73 (17) Time 1261 lt0001 lt0001 007B (119899 = 58) 75 (16) 71 (15) Time times group 132 0265 0001C (119899 = 57) 78 (22) 71 (20)
CRP (mgL)
A (119899 = 64) 028 (049) 025 (044) Time 238 009 100 001B (119899 = 57) 034 (046) 032 (041) Time times group 087 048 001C (119899 = 57) 035 (041) 024 (039)
Sialic acid (mmolL)A (119899 = 64) 21 (031) 19 (029) Time 8457 lt0001 lt0001 032B (119899 = 58) 21 (031) 18 (022) Time times group 340 001 004C (119899 = 57) 21 (028) 18 (024)
u-8-OxodG (120583gmmol)A (119899 = 64) 11 (05) 09 (04) Time 1066 lt0001 lt0001 006B (119899 = 57) 14 (08) 11 (06) Time times group 109 036 001C (119899 = 57) 12 (07) 10 (04)
Uric acid (120583molL)A (119899 = 64) 2917 (852) 3103 (775) Time 1339 lt0001 lt0001 007B (119899 = 58) 3034 (919) 3232 (931) Time times group 025 091 0003C (119899 = 57) 2904 (779) 3145 (834)
HbA1c ()A (119899 = 64) 74 (13) 72 (09) Time 270 007 008 002B (119899 = 58) 72 (10) 72 (10) Time times group 092 045 001C (119899 = 57) 71 (10) 70 (10)
HbA1c (mmolL)A (119899 = 64) 578 (136) 559 (102) Time 331 005 100 002B (119899 = 58) 548 (114) 557 (107) Time times group 090 045 001C (119899 = 57) 548 (107) 539 (100)
Adiponectin (mgL)A (119899 = 63) 75 (23) 71 (38) Time 073 044 100 0004B (119899 = 58) 91 (61) 90 (67) Time times group 055 065 0006C (119899 = 57) 80 (50) 81 (53)
Body mass index (kgm2)A (119899 = 54) 306 (47) 306 (50) Time 172 019 011 001B (119899 = 53) 292 (45) 290 (46) Time times group 131 027 001C (119899 = 52) 301 (41) 294 (40)
lowastTwo-sided significance of differences across time and between the groups (repeated measures ANOVA)lowastlowastTwo-sided significance of differences between baseline and 12-month assessmentsLog-transformed data
8 International Journal of Endocrinology
most pronounced determinant of total plasma antioxidantcapacity in diabetic patients [43] Thus maintaining uricacid levels within physiological range appears to be morefavorable than radical lowering in prevention of variousmor-bidities Based on recent epidemiological evidence includingcardiometabolic risk assessment a new gender-independentupper limit of reference range for uric acid has been proposedat the level of 360 120583molL [44] The present study revealsa significant increase in uric acid levels at follow-up butwell below proposed cut-off above which negative effectsof hyperuricemia might be expected On the contrary theobserved uric acid increase in our study is rather suggestiveof an improved antioxidant capacity elicited by behavioralinterventions in type 2 diabetic patients with subsyndromaldepression
Beneficial effect of cognitive-behavioral interventionin reducing oxidative stress and inflammatory responsehas been reported in hemodialysis patients suffering frominsomnia [45] but rather sparse depression-related studiesmainly focused on the assessment of low-grade inflammationbiomarkers In a very recent randomized trial evaluating anewly developed cognitive-behavioral program (DIAMOS)in diabetic patients with subsyndromal depression a set ofpro- and anti-inflammatory biomarkers was analyzed at basaland one-year follow-up [20] No change in hs-CRP IL-1 andadiponectin was observed whereas a significant decrease ininterleukin-1 receptor antagonist (IL-1RA) was interpreted asan indirect index of alleviated IL-1-related damaging mech-anisms presumably involved in the pathogenesis of micro-and macrovascular complications of diabetes Likewise ourstudy could not demonstrate any influence of the behavioralinterventions on hs-CRP and adiponectin but we foundother inflammatory markers that is leukocyte count andtotal serum sialic acid (TSA) significantly reduced with thelatter being largely affected (1205782 = 032) by the interventionsperformed
Sialic acids comprise a family of heterogenous monosac-charides abundantly present on the cell membranes withcomplex and multiple biological roles in cellular signalingand immunity [46] TSA is a validated inflammatory andatherogenic marker that has been proposed as a novelbiomarker of cardiovascular disease [47] Elevated levels ofTSA in newly diagnosed type 2 diabetic patients have beenlinked to the risk for later development of macrovascularcomplications [28] Interestingly TSA has been identified asa superior predictive biomarker of metabolic syndrome overthe abundantly used hs-CRP [48] Nevertheless despite theobvious advantages TSA has been largely underutilized inthe research on combined inflammatory-metabolic patholo-gies and it has not been studied in depression until this studyOur results identify TSA as a sensitive biomarker of inflam-mation degree in subsyndromally depressed diabetic patientswhereas neither of the established biomarkers of low-gradeinflammation hs-CRP and adiponectin was able to reflectthe anti-inflammatory effect of the performed interventionsSignificant decrease in leukocyte count however clearlyconfirmed postintervention attenuation of the cell-mediatedinflammation response in our patients with an importantnotice that the presence of acute infection at the assessments
was excluded by total leukocyte count lt 100 times 109L or hs-CRP lt 50 gL
The ability of psychological intervention to reduceboth depressive symptoms and inflammation has been evi-denced in depressed breast-cancer patients [49] Further-more due to the insightful study-design Thornton et alwere able to demonstrate a bidirectional mechanistic rela-tionship between depressive symptoms and inflammationThe paradigmatic view of the low-grade inflammation asthe inflicting mechanism for depression has been at leastcomplemented if not refuted by their finding on the mecha-nistic role of depressive symptoms lowering in the reductionof inflammatory response [49] This explanatory mecha-nism might also be translated to our results particularlyconsidering a lack of any effect of interventions towardshyperglycemia and obesity in our study
It is well known that the intensity of oxidative damage andinflammation in diabetes is remarkably and positively asso-ciated with the severity of hyperglycemia [18] Howeverthe observed reduction in oxidative damage and low-gradeinflammation in our study could not be attributed to thismechanism since no significant changes from baseline tofollow-up were found in HbA1c clinically considered toreflect a fair glucoregulation (Table 3) Obesity-derived low-grade inflammation is another recognized harmful compo-nent in the pathogenesis of type 2 diabetes and its compli-cations [50] Obesity induces a disbalance between pro- andanti-inflammatory cytokinesadipokines resulting in low-grade inflammation and related adverse health outcomesranging from metabolic syndrome and diabetes to cardio-vascular diseases and cancer as well as depression [49ndash51]Reduction in bodyweight is accompanied by beneficialmeta-bolic and hormonal profiles and a reduced inflammation [52]with increased production of anti-inflammatory adipokineadiponectin suggested to be among themost relevant features[53] Since our subjects classified as overweightobese [54]retained their BMI at follow-up and revealed no changes inadiponectin levels it is likely that the observed effects ofinterventions on the reduction in depressive symptoms andoxidativeinflammatory biomarkers in this study dependedon another mechanism(s)
Chronic stress with deregulation of stress-response adap-tive mechanisms is considered to be a common feature ofboth diabetes and depression [55] There is a growing bodyof evidence suggesting that metabolic inflammation asso-ciated with obesity and diabetes inflicts neuroinflammationwhich causes serious disturbances of the hypothalamic-pituitary-adrenal (HPA) axis function and consequentlyleads to impairment of adaptive stress-response [56] More-over chronic stress exposure has recently been demonstratedas a promoting factor for accelerated oxidative damagewhereby a sustained activation of HPA-axis emerged again asthe key mediator [57] Neuroendocrine effects of behavioraltreatment for depression have not been extensively studiedbut the evidence so far suggests a hypothetical pathway thatconnects the nurturing effects derived from the patient-ther-apist ldquobondrdquo with reestablishment of neuroendocrine home-ostasis [58] Moreover positive effects of physical exercise onpreventing potentially harmful stress-related metabolic and
International Journal of Endocrinology 9
psychological consequences have been presumably mediatedby the same neuroendocrine mechanisms [59] Consideringunchanged metabolic profile of our subjects and remark-able improvements in depressive symptoms and oxida-tiveinflammatory biomarkers following either behavioralintervention it is tempting if not plausible to speculate onthe involvement of neuroendocrine mechanism(s) in achiev-ing this beneficial response It should be noted that a lackof between-group differences in changes observed in ourstudy might not be explained by a phenomenon known asldquoregression toward the meanrdquo or just a natural course ofparameters Previous findings on persistence of depressivesymptoms in people with type 2 diabetes indicate thatdepression is not only persistent [60 61] but also associatedwith an increased risk of aggravating over time [62] On theother hand oxidative damage toDNA is increasing in healthysubjects throughout time as a result of ageing process [33]while inflammatory response and ageing-associated damageto biomolecules are even more pronounced in diabetes dueto a long-term exposure to hyperglycemia and advanced-glycated end-products [34 50]
The strengths of this study are in examining a highlyprevalent population of type 2 patients with depressive symp-toms but no clinical depression using a randomized com-parative design employing structured behavioral interven-tions and analyzing clinically relevant changes of simple-to-measure oxidativeinflammatory biomarkers Its limitation isthe lack of treatment as usual control intervention precludingthe possibility to investigate the course and outcomes ofsubclinical depression without any treatment Also the studywas carried out in only one centermdasha tertiary diabetesclinicmdashwhich does not allow concluding about its feasibilityin other clinical settings Per-protocol analyses are presentedin the study results which were confirmed by the intention totreat analysis based on baseline-observation-carried-forwardapproach A lack of estimation derived frommultiple predic-tors may be considered a limitation of the study
5 Conclusions
This study has demonstrated that improvement in depressivesymptoms is accompanied with reduced oxidative dam-age and inflammatory response in type 2 diabetic patientswith subsyndromal depression Testing mediating effectshas indicated that medium-term improvement in depres-sive symptoms predicts long-term-reduction in oxidativedamage while mediating factors for observed reductionin inflammatory response should be further investigatedClinical benefits of treating subsyndromal depression wereshown to be comparable in all three treatment arms
Regardless of the mechanisms involved our study clearlyindicates that enhanced treatment as usual defined as briefpatient-centred diabetes reeducation is not inferior to psy-choeducation and exercise in providing beneficial outcomesin subsyndromally depressed type 2 diabetic patients Simplebehavioral interventions are capable not only of alleviatingdepressive symptoms but also of reducing the intensity ofdamaging oxidativeinflammatory processes thereby miti-gating the risk of development of diabetic complications
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The study was funded by the European Foundation forthe Study of Diabetes (EFSD)mdashNew Horizons CollaborativeResearch Initiative 2010 The authors would like to thankLovorka Perkovic Croatian Institute of Public Health forediting the paper
References
[1] S S Ali M A Stone J L Peters M J Davies and K KhuntildquoThe prevalence of co-morbid depression in adults with Type2 diabetes a systematic review and meta-analysisrdquo DiabeticMedicine vol 23 no 11 pp 1165ndash1173 2006
[2] P J Lustman R J Anderson K E Freedland M de Groot RM Carney and R E Clouse ldquoDepression and poor glycemiccontrol a meta-analytic review of the literaturerdquo Diabetes Carevol 23 no 7 pp 934ndash942 2000
[3] L K Richardson L E Egede M Mueller C L Echols and MGebregziabher ldquoLongitudinal effects of depression on glycemiccontrol in veterans with Type 2 diabetesrdquo General HospitalPsychiatry vol 30 no 6 pp 509ndash514 2008
[4] M de Groot R Anderson K E Freedland R E Clouse andP J Lustman ldquoAssociation of depression and diabetes com-plications ameta-analysisrdquo PsychosomaticMedicine vol 63 no4 pp 619ndash630 2001
[5] K Ismail KWinkley D Stahl T Chalder andM Edmonds ldquoAcohort study of people with diabetes and their first foot ulcerthe role of depression on mortalityrdquo Diabetes Care vol 30 no6 pp 1473ndash1479 2007
[6] X Zhang S L Norris E W Gregg Y J Cheng G Becklesand H S Kahn ldquoDepressive symptoms and mortality amongpersons with and without diabetesrdquo American Journal of Epi-demiology vol 161 no 7 pp 652ndash660 2005
[7] S A Black K S Markides and L A Ray ldquoDepression pre-dicts increased incidence of adverse health outcomes in olderMexican Americans with type 2 diabetesrdquo Diabetes Care vol26 no 10 pp 2822ndash2828 2003
[8] H Baumeister N Hutter and J Bengel ldquoPsychological andpharmacological interventions for depression in patients withdiabetesmellitus and depressionrdquoCochraneDatabase of System-atic Reviews vol 12 Article ID CD008381 2012
[9] E Harkness W Macdonald J Valderas P Coventry L Gaskand P Bower ldquoIdentifying psychosocial interventions thatimprove both physical and mental health in patients with dia-betes a systematic review and meta-analysisrdquo Diabetes Carevol 33 no 4 pp 926ndash930 2010
[10] M Berk L J Williams F N Jacka et al ldquoSo depression is aninflammatory disease but where does the inflammation comefromrdquo BMCMedicine vol 11 article 200 2013
[11] S de Kort D Keszthelyi and A A M Masclee ldquoLeaky gut anddiabetes mellitus what is the linkrdquoObesity Reviews vol 12 no6 pp 449ndash458 2011
[12] E T de Lemos J Oliveira J P Pinheiro and F Reis ldquoRegularphysical exercise as a strategy to improve antioxidant andanti-inflammatory status benefits in type 2 diabetes mellitusrdquo
10 International Journal of Endocrinology
Oxidative Medicine and Cellular Longevity vol 2012 Article ID741545 15 pages 2012
[13] T A Doyle M de Groot T Harris et al ldquoDiabetes depressivesymptoms and inflammation in older adults results fromthe Health Aging and Body Composition Studyrdquo Journal ofPsychosomatic Research vol 75 no 5 pp 419ndash424 2013
[14] J-P S Laake D Stahl S A Amiel et al ldquoThe associationbetween depressive symptoms and systemic inflammation inpeople with type 2 diabetes findings from the South Londondiabetes studyrdquoDiabetes Care vol 37 no 8 pp 2186ndash2192 2014
[15] N Rohleder ldquoStimulation of systemic low-grade inflammationby psychosocial stressrdquo Psychosomatic Medicine vol 76 no 3pp 181ndash189 2014
[16] M Maes ldquoAn intriguing and hitherto unexplained co-occur-rence depression and chronic fatigue syndrome are mani-festations of shared inflammatory oxidative and nitrosative(IOampNS) pathwaysrdquo Progress in Neuro-Psychopharmacologyand Biological Psychiatry vol 35 no 3 pp 784ndash794 2011
[17] P Palta L J Samuel E RMiller and S L Szanton ldquoDepressionand oxidative stress results from a meta-analysis of observa-tional studiesrdquo Psychosomatic Medicine vol 76 no 1 pp 12ndash192014
[18] L Rochette M Zeller Y Cottin and C Vergely ldquoDiabetes oxi-dative stress and therapeutic strategiesrdquo Biochimica et Biophys-ica Acta vol 1840 no 9 pp 2709ndash2729 2014
[19] S Keri C Szabo and O Kelemen ldquoExpression of Toll-LikeReceptors in peripheral blood mononuclear cells and responseto cognitive-behavioral therapy in major depressive disorderrdquoBrain Behavior and Immunity vol 40 pp 235ndash243 2014
[20] N Hermanns A Schmitt A Gahr et al ldquoThe effect ofa Diabetes-Specific Cognitive Behavioral Treatment Program(DIAMOS) for patients with diabetes and subclinical depres-sion results of a randomized controlled trialrdquo Diabetes Carevol 38 no 4 pp 551ndash560 2015
[21] K Kroenke R L Spitzer and J B W Williams ldquoThe patienthealth questionnaire-2 validity of a two-item depressionscreenerrdquoMedical Care vol 41 no 11 pp 1284ndash1292 2003
[22] J H Abramson ldquoWINPEPI updated computer programs forepidemiologists and their teaching potentialrdquo EpidemiologicPerspectives amp Innovations vol 8 no 1 article 1 2011
[23] J Cohen ldquoA power primerrdquo Psychological Bulletin vol 112 no1 pp 155ndash159 1992
[24] M Pibernik-Okanovic D Ajdukovic M V Lovrencic andN Hermanns ldquoDoes treatment of subsyndromal depressionimprove depression and diabetes related outcomes protocolfor a randomised controlled comparison of psycho-educationphysical exercise and treatment as usualrdquo Trials vol 12 article17 2011
[25] BArroll FGoodyear-SmithNKerse T Fishman and JGunnldquoEffect of the addition of a lsquohelprsquo question to two screeningquestions on specificity for diagnosis of depression in generalpractice diagnostic validity studyrdquo British Medical Journal vol331 no 7521 article 884 2005
[26] P Rohde P M Lewinsohn and J R Seeley ldquoComparability oftelephone and face-to-face interviews in assessing axis I and IIdisordersrdquo American Journal of Psychiatry vol 154 no 11 pp1593ndash1598 1997
[27] L S Radloff ldquoTheCES-D scalerdquoApplied Psychological Measure-ment vol 1 pp 385ndash401 1977
[28] M Gavella V Lipovac A Car M Vucic L Sokolic and RRakos ldquoSerum sialic acid in subjects with impaired glucose
tolerance and in newly diagnosed type 2 diabetic patientsrdquoActaDiabetologica vol 40 no 2 pp 95ndash100 2003
[29] M D Evans R Singh V Mistry K Sandhu P B Farmer andM S Cooke ldquoAnalysis of urinary 8-oxo-78-dihydro-purine-21015840- deoxyribonucleosides by LC-MSMS and improved ELISArdquoFree Radical Research vol 42 no 10 pp 831ndash840 2008
[30] M Pibernik-Okanovic D Begic D Ajdukovic N Andrijasevicand Z Metelko ldquoPsychoeducation versus treatment as usualin diabetic patients with subthreshold depression preliminaryresults of a randomized controlled trialrdquo Trials vol 10 article78 2009
[31] M Pibernik-Okanovic M Vucic Lovrencic D AjdukovicM Sekerija and N Hermanns ldquoPsychological behavioraland biological changes following treatments of subsyndromaldepression in people with type 2 diabetesrdquoDiabetologia vol 56supplement 1 p S465 2013
[32] L Fisher D Hessler R E Glasgow et al ldquoREDEEM a prag-matic trial to reduce diabetes distressrdquo Diabetes Care vol 36no 9 pp 2551ndash2558 2013
[33] H E Poulsen L L Nadal K Broedbaek P E Nielsen andA Weimann ldquoDetection and interpretation of 8-oxodG and 8-oxoGua in urine plasma and cerebrospinal fluidrdquo Biochimica etBiophysica ActamdashGeneral Subjects vol 1840 no 2 pp 801ndash8082014
[34] K Broedbaek A Weimann E S Stovgaard and H E PoulsenldquoUrinary 8-oxo-78-dihydro-21015840-deoxyguanosine as a biomarkerin type 2 diabetesrdquo Free Radical Biology and Medicine vol 51no 8 pp 1473ndash1479 2011
[35] M J Forlenza and G E Miller ldquoIncreased serum levels of 8-hydroxy-21015840-deoxyguanosine in clinical depressionrdquo Psychoso-matic Medicine vol 68 no 1 pp 1ndash7 2006
[36] A Jorgensen J Krogh K Miskowiak et al ldquoSystemic oxida-tively generatedDNARNAdamage in clinical depression asso-ciations to symptom severity and response to electroconvulsivetherapyrdquo Journal of Affective Disorders vol 149 no 1ndash3 pp 355ndash362 2013
[37] S Yi ANanri YMatsushitaHKasai K Kawai andTMizoueldquoDepressive symptoms and oxidative DNA damage in Japanesemunicipal employeesrdquo Psychiatry Research vol 200 no 2-3 pp318ndash322 2012
[38] H Nojima H Watanabe K Yamane et al ldquoEffect of aerobicexercise training on oxidative stress in patients with type 2diabetes mellitusrdquo Metabolism Clinical and Experimental vol57 no 2 pp 170ndash176 2008
[39] S Bonakdaran and B Kharaqani ldquoAssociation of serum uricacid and metabolic syndrome in type 2 diabetesrdquo CurrentDiabetes Reviews vol 10 no 2 pp 113ndash117 2014
[40] R J Johnson T Nakagawa L G Sanchez-Lozada et al ldquoSugaruric acid and the etiology of diabetes and obesityrdquoDiabetes vol62 no 10 pp 3307ndash3315 2013
[41] M L Wahlqvist ldquoAntioxidant relevance to human healthrdquo AsiaPacific Journal of Clinical Nutrition vol 22 no 2 pp 171ndash1762013
[42] A De Giorgi F Fabbian M Pala et al ldquoUric acid friend orfoe Uric acid and cognitive function lsquogout kills more wise menthan simplersquordquo European Review forMedical and PharmacologicalSciences vol 19 no 4 pp 640ndash646 2015
[43] M Vucic B Rocic V Bozikov and S J H Ashcroft ldquoPlasmauric acid and total antioxidant status in patients with diabetesmellitusrdquo Hormone and Metabolic Research vol 29 no 7 pp355ndash357 1997
International Journal of Endocrinology 11
[44] G Desideri G Castaldo A Lombardi et al ldquoIs it time to revisethe normal range of serum uric acid levelsrdquo European Reviewfor Medical and Pharmacological Sciences vol 18 no 9 pp1295ndash1306 2014
[45] H-Y Chen I-C Cheng Y-J Pan et al ldquoCognitive-behavioraltherapy for sleep disturbance decreases inflammatory cytokinesand oxidative stress in hemodialysis patientsrdquo Kidney Interna-tional vol 80 no 4 pp 415ndash422 2011
[46] A Varki and P Gagneux ldquoMultifarious roles of sialic acids inimmunityrdquo Annals of the New York Academy of Sciences vol1253 no 1 pp 16ndash36 2012
[47] K P Gopaul and M A Crook ldquoSialic acid a novel marker ofcardiovascular diseaserdquo Clinical Biochemistry vol 39 no 7 pp667ndash681 2006
[48] L M Browning S A Jebb G D Mishra et al ldquoElevated sialicacid but not CRP predicts features of the metabolic syndromeindependently of BMI in womenrdquo International Journal ofObesity vol 28 no 8 pp 1004ndash1010 2004
[49] LMThornton B L Andersen T A Schuler andW E CarsonldquoA psychological intervention reduces inflammatory markersby alleviating depressive symptoms secondary analysis of arandomized controlled trialrdquo Psychosomatic Medicine vol 71no 7 pp 715ndash724 2009
[50] N Esser S Legrand-Poels J Piette A J Scheen and N PaquotldquoInflammation as a link between obesity metabolic syndromeand type 2 diabetesrdquoDiabetes Research andClinical Practice vol105 no 2 pp 141ndash150 2014
[51] R Hutcheson and P Rocic ldquoThe metabolic syndrome oxida-tive stress environment and cardiovascular disease the greatexplorationrdquo Experimental Diabetes Research vol 2012 ArticleID 271028 13 pages 2012
[52] L Fontana and F B Hu ldquoOptimal body weight for health andlongevity bridging basic clinical and population researchrdquoAging Cell vol 13 no 3 pp 391ndash400 2014
[53] A T Turer and P E Scherer ldquoAdiponectin mechanistic insightsand clinical implicationsrdquo Diabetologia vol 55 no 9 pp 2319ndash2326 2012
[54] WHO ldquoObesity and overweightrdquo Fact sheet No 311 2015[55] P W Gold ldquoThe organization of the stress system and its
dysregulation in depressive illnessrdquo Molecular Psychiatry vol20 no 1 pp 32ndash47 2015
[56] S Purkayastha and D Cai ldquoNeuroinflammatory basis ofmetabolic syndromerdquo Molecular Metabolism vol 2 no 4 pp356ndash363 2013
[57] K Aschbacher A OrsquoDonovan O MWolkowitz F S DhabharY Su and E Epel ldquoGood stress bad stress and oxidative stressinsights from anticipatory cortisol reactivityrdquo Psychoneuroen-docrinology vol 38 no 9 pp 1698ndash1708 2013
[58] C F Sharpley ldquoA review of the neurobiological effects of psy-chotherapy for depressionrdquo Psychotherapy vol 47 no 4 pp603ndash615 2010
[59] M N Silverman and P A Deuster ldquoBiological mechanismsunderlying the role of physical fitness in health and resiliencerdquoInterface Focus vol 4 no 5 Article ID 20140040 2014
[60] G Nefs F Pouwer J Denollet and V Pop ldquoThe course ofdepressive symptoms in primary care patients with type 2 dia-betes results from theDiabetes Depression TypeDPersonalityZuidoost-Brabant (DiaDDZoB) Studyrdquo Diabetologia vol 55no 3 pp 608ndash616 2012
[61] M Pibernik-Okanovic D Begic K Peros S Szabo andZ Metelko ldquoPsychosocial factors contributing to persistent
depressive symptoms in type 2 diabetic patients a Croatiansurvey from the European Depression in Diabetes ResearchConsortiumrdquo Journal of Diabetes and Its Complications vol 22no 4 pp 246ndash253 2008
[62] M Bot F Pouwer J Ormel J P J Slaets and P de Jonge ldquoPre-dictors of incidentmajor depression in diabetic outpatients withsubthreshold depressionrdquo Diabetic Medicine vol 27 no 11 pp1295ndash1301 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 International Journal of Endocrinology
Table 1 Programsrsquo objectives methods of delivery and specific features
Study arm Objectives Methods of delivery Specific features
Psychoeducation
(i) Recognizing and understanding feelings(ii) Becoming aware of dysfunctionalthinking patterns(iii) Improving mood by pleasant activities(iv) Improving mood by solving problems(v) Managing automatic negative thoughts(vi) Communicating assertively providingsupport
(i) Six weekly group sessions lastingfor 90 minutes(ii) Interactive learning in smallgroups (5ndash8 participants)(iii) Self-help manual(iv) Workbook with practicalexercises
Learning and discussions supportedby a structured PowerPointpresentationTopics focused on diabetes-relatedissues and concerns
Physical exercise
(i) Acquiring warm-up flexibilitystretching and strengthening exercises(ii) Learning about physical activity andglycaemic control cardiovascular healthenergy expenditure peripheral nervesmood diabetes self-management
(i) Six weekly group sessions lastingfor 90 minutes(ii) Practicing exercises andexchanging experiences in smallgroups(iii) Written material reminding ofpracticed exercises
Learning and discussions supportedby a structured PowerPointpresentationExercise intensity measured by aheart rate monitor maintained in alight-to-medium intensity rangeBlood glucose and blood pressuremeasured before and after sessions
Enhancedtreatment asusual
(i) Discussing recent laboratory findings(ii) Addressing diabetes-related concerns
(i) One group session lasting for 90minutes(ii) Patient-centered counselling inthe group
Written self-help instructions tocope with mood difficulties
because leaving these patients without any treatment wasconsidered ethically unacceptable
The interventions were considered to have a very lowpotential for causing harm Nevertheless patient informa-tion being a part of the written consent clearly stated thatthe participants can discontinue intervention at any timeparticularly if they would perceive that their symptoms havebeen worsened Qualified professionals involved in treatmentcarefully monitored patientrsquos condition and routine labora-tory results in order to provide a timely referral to physicianrsquoscare if needed In addition patients allocated to physicalexercise underwent ECG and if indicated an ergometrictest before the study Exercise intensity was measured bya heart rate monitor and maintained in a light-to-mediumintensity range whereas blood glucose and blood pressurewere measured before and after each session
A summary of the programsrsquo objectives methods ofdelivery and specific features are presented in Table 1
22 Assessments Patient demographic variables includedage sex education family status employment and economicstatus Diabetes-related variables included years of diabetesduration and diabetes treatment with or without insulin
Screening for mood difficulties was carried out using theadapted Patient Health Questionnaire-2 [21] An additionalquestion inquiring into the patientsrsquo need for help withthese difficulties was added as it has proven to improve theinstrumentrsquos validity [25]
The presence or absence of clinical depression was deter-mined by phone-administered structured clinical interviewfor the DSM-IV Axis 1 disorders as this method has beenshown to be comparable to face-to-face interview [26]
Depressive symptoms were measured by the Center forEpidemiological Studies Depression (CES-D) Scale a 20-itemself-report instrument [27]The total score of the scale ranges
from 0 to 60 points with higher scores indicating higherdepressive symptoms The reliability of the scale at baselinewas Cronbach alpha = 083
221 Laboratory Assessments HbA1c was measured by anNGSP-certified automated immunoturbidimetric method(Tina-quant HbA1c Roche Diagnostics USA) with a totalimprecision (expressed as CV) lt15 and dual reportingof the results (NGSPDCCT aligned and IFCC-alignedmmolmol)
Leukocyte count was determined in K3EDTA-wholeblood samples with ADVIA120 blood cell counter (SiemensDiagnostic Solutions USA)
Serum uric acid and hs-CRP concentrations were mea-sured by the automated enzymatic and immunoturbidimetricassays respectively (AU680 Beckman Coulter USA)
Total serum sialic acid (TSA) was determined by acolorimetric procedure as described previously [28] Serumadiponectin was measured by a commercially available sand-wich ELISA procedure (Adiponectin Human ELISA highsensitive Biovendor CZ) with declared detection limit of047 120583gL
Urinary 8-oxo-deoxyguanosine (u-8-oxodG) was mea-sured by the competitive ELISA method (New 8-OHdGCheck Japan Institute for the Control of Ageing JaiCAShizuoka Japan) with declared assay-range of 05ndash200120583gLand improved specificity [29] On the day of analysis frozenurine samples were thawed in a water-bath (37∘C) vortexedcentrifuged (10min 3000 rpm) and u-8-oxodG assayedimmediately according to the manufacturerrsquos instructionsUrinary creatinine was measured in the same samples witha compensated colorimetric Jaffe procedure (AU680 Anal-yser Beckman Coulter Brea USA) Results were normal-ized to the creatinine concentration by the formula u-8-oxodGcreatinine (120583gmmol)
International Journal of Endocrinology 5
Variables indicating a level of depressive symptoms andbiomarkers of oxidative damage and inflammation weremeasured at baseline and after six- and twelve-month follow-up periods HbA1c leukocytes serum hs-CRP and uric acidwere assayed in fresh samples obtained in the morning afteran overnight fast Samples for sialic acid adiponectin and u-8-oxodG measurements were frozen (minus70∘C) until analyzedThe samples from each patient were analyzed with ELISAs atthe samemicroplate in order to avoid possible between-seriesvariability
23 Statistical Methods Data are presented as means (SD)unless otherwise indicated Due to the nonparametric dis-tribution hs-CRP results were log-transformed prior to theanalysis One-way ANOVA and chi squares were used todetermine baseline differences across the three treatmentarms and examine differences between continuing partici-pants and dropouts
Data were analyzed per protocol after exclusion of par-ticipants who withdrew did not attend all three follow-up meetings initiated psychopharmacological treatment ordied during the study period these results are presentedthroughout the paper Intention-to-treat (ITT) analysis wasperformed to validate these results all participants whowere randomized were analyzed despite deviations from theprotocol To perform ITT missing data were imputed usingthe baseline observation carried forward approach
Repeated measures ANOVA was used to test for changesin outcome variables across time and between the groupsCohenrsquos 1205782 coefficients ranging from 001 to 005 wereregarded as small from006 to 012moderate andge013 large
Regression analysis was employed to test directionalrelations between depressive symptoms and reduction ininflammation and oxidative stress
A 119901 value of lt005 was considered significant in allanalyses
Statistical analyses were performed by using the SPSS 17(SPSS Inc Chicago IL USA)
24 Ethical Aspects The study was approved by the VukVrhovac University Clinic for Diabetes Ethics Committee onJune 30 2010 A written informed consent was obtained fromall the participants
3 Results
Among the 1740 patients assessed for eligibility 365 wereconsidered eligible and 265 agreed to participate in the inter-ventions (72) Of these 209 completed baseline laboratoryand psychological assessments (79) with 74 randomizedto psychoeducational intervention 66 to physical exerciseand 69 to diabetes reeducation Attrition rate was 3 duringthe interventions (6 of 209 patients) 3 from baseline tosix months (7 of 203 patients) and 2 from 6-month to 12-month follow-up period (4 of 196 patients) Of the sevendropouts who completed the intervention but missed bothfollow-up assessments two missed the follow-up appoint-ments due to health problems four were unwilling to comeand one patient died No harmful incidents were recorded
throughout the interventions Four patients were excludedfromper-protocol analyses due to the initiation of pharmaco-logical therapy No differences between the participants anddropouts across the three study groups were observed
Table 2 presents demographic and diabetes-related char-acteristics of patients randomized to one of the three groupsand a baseline level of depressive symptoms as self-assessedby the CES-D questionnaire No between-group differencesregarding demographic diabetes-related and psychologicalvariables were found
The effects of interventions on depressive symptoms andbiomarkers of oxidative damage and inflammation as wellas glucoregulation (HbA1c) and BMI based on repeatedmeasures ANOVA are given in Table 3 ITT analyses showeda comparable pattern of results of all analyses in terms ofstatistical significance and effect size and are not presentedin the text
31 Changes in Depressive Symptoms No significant be-tween-group differences over time were obtained with res-pect to depressive symptoms (119865 = 061 119901 = 0656) indi-cating comparable efficacy of psychoeducation physical exer-cise and enhanced treatment as usual on the primary studyoutcome
Significant reductions in depressive symptoms occurredacross all three study groups from baseline to 12 months(119865 = 1251 119901 lt 0001 1205782 = 07) The size of the time effectindicated a moderate effect of the three treatments on self-assessed depressive symptoms
32 Changes in Biomarkers of Oxidative Damage and Inflam-mation Total leukocytes significantly decreased in all threegroups (119865 = 1261 119901 lt 00001 1205782 = 007) as did u-8-oxodG (119865 = 1066 119901 lt 00001 1205782 = 006) and sialic acid(119865 = 8457 119901 lt 00001 1205782 = 032) The latter showed smallbut statistically significant time 119909 group effect (119865 = 340119901 = 001 1205782 = 004) However after adjusting the results formultiple comparisons by Bonferroni test it did not remainsignificant Uric acid increased significantly over one year inall three groups (119865 = 1339 119901 lt 00001 1205782 = 007) Theeffects of the interventions on sialic acid can be regarded aslarge (032) and on leukocytes u-8-oxodG and uric acid asmoderate (007 006 and 007 resp)
No significant changes were registered with respect toadiponectin and hs-CRP
NeitherHbA1c nor BMIwere significantly changed in anyof the study groups from baseline to 12 months
No between-group effects were obtained with respectto one-year changes in biomarkers of inflammation andoxidative damage (all 119901 gt 005)
33 Testing for Mediation The results obtained by usingregression analyses indicated that improvement in depressivesymptoms at six months predicted reductions in u-8-oxodGat twelve-month follow-up (120573 = 015 119901 = 0044) whilethe results for sialic and uric acid were close to statisticalsignificance (119901 = 0069 and 119901 = 0070 resp) (results notshown in tables)
6 International Journal of Endocrinology
Table 2 Baseline characteristics of participants by the intervention groups (119899 = 209)
Psychoeducation Physical exercise Enhanced treatment as usual Siglowast
119873 74 66 69Age (yrs) 577 (62) 585 (48) 582 (56) 0648Female (119899) 40 37 36 0867Education (yrs) 126 (24) 124 (23) 122 (25) 0623Professional status ( employed) 30 27 30 0502Economic status ( poor) 13 12 13 0317Family status ( marriedcohabitating) 76 72 76 0488Insulin use () 32 29 32 0695OHA use () 56 57 53 0664Insulin + OHA use () 12 14 15 0632Statin use () 68 71 71 0786HbA1c () 74 (12) 72 (11) 72 (11) 0384HbA1c (mmolmol) 58 (13) 56 (13) 55 (11) 0442Body mass index kgm2 3064 (454) 2944 (467) 2996 (439) 0297Depressive symptoms (CES-D score) 197 (91) 205 (86) 197 (87) 0813Data are means (SD) or percentageslowastSig significancelowast One-way ANOVA or 1205942 as appropriateOHA = oral hypoglycemic agents
4 Discussion
This randomized interventional study attempted to evaluatethe effect of two behavioral interventions psychoeducationand physical exercise as compared to enhanced treatmentas usual on depressive symptoms and the intensity ofoxidativeinflammatory processes in diabetic patients suf-fering from subsyndromal depression The results indicateprotracted favorable effects of either intervention on loweringdepressive symptoms while reducing overall oxidative dam-age and cellular inflammatory response as well as improvingantioxidant capacity
In all three study arms a comparable and clinically mean-ingful improvement in depressive symptoms was obtainedThe intervention-independent results regarding depression-related outcomes confirm our preliminary report indicatingthat treatment as usual was equally effective as psychoe-ducation in reducing depressive symptoms and improvingmetabolic control in type 2 diabetic patients with subsyndro-mal depression [30] Also no between-groupdifferenceswerefound within a randomized controlled comparison of psy-choeducation physical exercise and control arm consistingof brief diabetes reeducation [31]The absence of a significanttreatment effect suggested that patterns of change might besimilar in all treatment groups Hypothetically addressingpatientsrsquo emotional needs and their diabetes-related distresswhich were common in all three approaches may indicate apossible pathway of change Similar findings were obtained ina study by Fisher et al [32] which demonstrated that clinicallyreasonable improvements in emotional symptoms may bestimulated by even minimal behavioral interventions
In this study a significant decrease in overall oxidativedamage was observed from basal to one-year posttreatmentfollow-up by measuring a recognized biomarker of oxidativedamage to DNAmdashurinary 8-oxodG Urinary excretion of
8-oxodG reflects the average rate of nucleic acid guanineoxidation and can be regarded as a reliable marker of generalintracellular oxidative stress [33] Research on the u-8-oxodGin diabetes revealed its significant association with severehyperglycemia poor diabetes control and severity of dia-betic complications as well as predictive value for diabetes-associated morbidity [34] The relationship between u-8-oxodG and depression has been modestly investigated andprovided controversial results from an increase to no changedepending on the study-specific depression phenotype [35ndash37] To our knowledge this is the first study investigating u-8-oxodG in patients with diabetes and elevated depressivesymptoms While the results in our exercise group are inaccord with previously reported reduction in u-8-oxodGelicited bymoderate-intensity exercise in type 2 diabetes over12 months [38] significant decrease in u-8-oxodG levels inpsychoeducation and diabetes reeducation group is a novelfinding indicating that cognitive-behavioral approach mighthave beneficial effects on oxidative damage reduction indiabetic patients with subsyndromal depression Additionalsupport for this finding was a significant increase in serumuric acid level at follow-up
Uric acid is an end-product of purine metabolism withcomplex and multifarious roles in human physiology Apartfrom causing gout hyperuricemia has been identified as arisk factor for metabolic syndrome type 2 diabetes andcardiovascular diseases [39] Recently proposed intriguinghypothesis linking hyperuricemia derived by an increasedconsumption of dietary fructose with an epidemic of car-diometabolic diseases attracted a lot of attention and createda paradigm of uric acid as being an exclusively harmfulmetabolite [40] By contrast uric acid has long been recog-nized as one of the most powerful endogenous antioxidants[41] and an efficient mediator of neuroprotection cognitivefunction and intellectual performance [42] as well as the
International Journal of Endocrinology 7
Table 3 One-year changes of depressive symptoms inflammatory- and prooxidative biomarkers
Group scores BaselineM (SD)
12-month follow-upM (SD) Effects 119865 Overall 119875lowast 119875
0 to 12molowastlowast 1205782
Depressive symptomsA (119899 = 64) 197 (91) 167 (79) Time 1251 lt0001 0003 007B (119899 = 58) 198 (82) 181 (98) Time times group 061 0656 0007C (119899 = 57) 190 (86) 174 (94)
Leukocytes (times109L)A (119899 = 63) 75 (17) 73 (17) Time 1261 lt0001 lt0001 007B (119899 = 58) 75 (16) 71 (15) Time times group 132 0265 0001C (119899 = 57) 78 (22) 71 (20)
CRP (mgL)
A (119899 = 64) 028 (049) 025 (044) Time 238 009 100 001B (119899 = 57) 034 (046) 032 (041) Time times group 087 048 001C (119899 = 57) 035 (041) 024 (039)
Sialic acid (mmolL)A (119899 = 64) 21 (031) 19 (029) Time 8457 lt0001 lt0001 032B (119899 = 58) 21 (031) 18 (022) Time times group 340 001 004C (119899 = 57) 21 (028) 18 (024)
u-8-OxodG (120583gmmol)A (119899 = 64) 11 (05) 09 (04) Time 1066 lt0001 lt0001 006B (119899 = 57) 14 (08) 11 (06) Time times group 109 036 001C (119899 = 57) 12 (07) 10 (04)
Uric acid (120583molL)A (119899 = 64) 2917 (852) 3103 (775) Time 1339 lt0001 lt0001 007B (119899 = 58) 3034 (919) 3232 (931) Time times group 025 091 0003C (119899 = 57) 2904 (779) 3145 (834)
HbA1c ()A (119899 = 64) 74 (13) 72 (09) Time 270 007 008 002B (119899 = 58) 72 (10) 72 (10) Time times group 092 045 001C (119899 = 57) 71 (10) 70 (10)
HbA1c (mmolL)A (119899 = 64) 578 (136) 559 (102) Time 331 005 100 002B (119899 = 58) 548 (114) 557 (107) Time times group 090 045 001C (119899 = 57) 548 (107) 539 (100)
Adiponectin (mgL)A (119899 = 63) 75 (23) 71 (38) Time 073 044 100 0004B (119899 = 58) 91 (61) 90 (67) Time times group 055 065 0006C (119899 = 57) 80 (50) 81 (53)
Body mass index (kgm2)A (119899 = 54) 306 (47) 306 (50) Time 172 019 011 001B (119899 = 53) 292 (45) 290 (46) Time times group 131 027 001C (119899 = 52) 301 (41) 294 (40)
lowastTwo-sided significance of differences across time and between the groups (repeated measures ANOVA)lowastlowastTwo-sided significance of differences between baseline and 12-month assessmentsLog-transformed data
8 International Journal of Endocrinology
most pronounced determinant of total plasma antioxidantcapacity in diabetic patients [43] Thus maintaining uricacid levels within physiological range appears to be morefavorable than radical lowering in prevention of variousmor-bidities Based on recent epidemiological evidence includingcardiometabolic risk assessment a new gender-independentupper limit of reference range for uric acid has been proposedat the level of 360 120583molL [44] The present study revealsa significant increase in uric acid levels at follow-up butwell below proposed cut-off above which negative effectsof hyperuricemia might be expected On the contrary theobserved uric acid increase in our study is rather suggestiveof an improved antioxidant capacity elicited by behavioralinterventions in type 2 diabetic patients with subsyndromaldepression
Beneficial effect of cognitive-behavioral interventionin reducing oxidative stress and inflammatory responsehas been reported in hemodialysis patients suffering frominsomnia [45] but rather sparse depression-related studiesmainly focused on the assessment of low-grade inflammationbiomarkers In a very recent randomized trial evaluating anewly developed cognitive-behavioral program (DIAMOS)in diabetic patients with subsyndromal depression a set ofpro- and anti-inflammatory biomarkers was analyzed at basaland one-year follow-up [20] No change in hs-CRP IL-1 andadiponectin was observed whereas a significant decrease ininterleukin-1 receptor antagonist (IL-1RA) was interpreted asan indirect index of alleviated IL-1-related damaging mech-anisms presumably involved in the pathogenesis of micro-and macrovascular complications of diabetes Likewise ourstudy could not demonstrate any influence of the behavioralinterventions on hs-CRP and adiponectin but we foundother inflammatory markers that is leukocyte count andtotal serum sialic acid (TSA) significantly reduced with thelatter being largely affected (1205782 = 032) by the interventionsperformed
Sialic acids comprise a family of heterogenous monosac-charides abundantly present on the cell membranes withcomplex and multiple biological roles in cellular signalingand immunity [46] TSA is a validated inflammatory andatherogenic marker that has been proposed as a novelbiomarker of cardiovascular disease [47] Elevated levels ofTSA in newly diagnosed type 2 diabetic patients have beenlinked to the risk for later development of macrovascularcomplications [28] Interestingly TSA has been identified asa superior predictive biomarker of metabolic syndrome overthe abundantly used hs-CRP [48] Nevertheless despite theobvious advantages TSA has been largely underutilized inthe research on combined inflammatory-metabolic patholo-gies and it has not been studied in depression until this studyOur results identify TSA as a sensitive biomarker of inflam-mation degree in subsyndromally depressed diabetic patientswhereas neither of the established biomarkers of low-gradeinflammation hs-CRP and adiponectin was able to reflectthe anti-inflammatory effect of the performed interventionsSignificant decrease in leukocyte count however clearlyconfirmed postintervention attenuation of the cell-mediatedinflammation response in our patients with an importantnotice that the presence of acute infection at the assessments
was excluded by total leukocyte count lt 100 times 109L or hs-CRP lt 50 gL
The ability of psychological intervention to reduceboth depressive symptoms and inflammation has been evi-denced in depressed breast-cancer patients [49] Further-more due to the insightful study-design Thornton et alwere able to demonstrate a bidirectional mechanistic rela-tionship between depressive symptoms and inflammationThe paradigmatic view of the low-grade inflammation asthe inflicting mechanism for depression has been at leastcomplemented if not refuted by their finding on the mecha-nistic role of depressive symptoms lowering in the reductionof inflammatory response [49] This explanatory mecha-nism might also be translated to our results particularlyconsidering a lack of any effect of interventions towardshyperglycemia and obesity in our study
It is well known that the intensity of oxidative damage andinflammation in diabetes is remarkably and positively asso-ciated with the severity of hyperglycemia [18] Howeverthe observed reduction in oxidative damage and low-gradeinflammation in our study could not be attributed to thismechanism since no significant changes from baseline tofollow-up were found in HbA1c clinically considered toreflect a fair glucoregulation (Table 3) Obesity-derived low-grade inflammation is another recognized harmful compo-nent in the pathogenesis of type 2 diabetes and its compli-cations [50] Obesity induces a disbalance between pro- andanti-inflammatory cytokinesadipokines resulting in low-grade inflammation and related adverse health outcomesranging from metabolic syndrome and diabetes to cardio-vascular diseases and cancer as well as depression [49ndash51]Reduction in bodyweight is accompanied by beneficialmeta-bolic and hormonal profiles and a reduced inflammation [52]with increased production of anti-inflammatory adipokineadiponectin suggested to be among themost relevant features[53] Since our subjects classified as overweightobese [54]retained their BMI at follow-up and revealed no changes inadiponectin levels it is likely that the observed effects ofinterventions on the reduction in depressive symptoms andoxidativeinflammatory biomarkers in this study dependedon another mechanism(s)
Chronic stress with deregulation of stress-response adap-tive mechanisms is considered to be a common feature ofboth diabetes and depression [55] There is a growing bodyof evidence suggesting that metabolic inflammation asso-ciated with obesity and diabetes inflicts neuroinflammationwhich causes serious disturbances of the hypothalamic-pituitary-adrenal (HPA) axis function and consequentlyleads to impairment of adaptive stress-response [56] More-over chronic stress exposure has recently been demonstratedas a promoting factor for accelerated oxidative damagewhereby a sustained activation of HPA-axis emerged again asthe key mediator [57] Neuroendocrine effects of behavioraltreatment for depression have not been extensively studiedbut the evidence so far suggests a hypothetical pathway thatconnects the nurturing effects derived from the patient-ther-apist ldquobondrdquo with reestablishment of neuroendocrine home-ostasis [58] Moreover positive effects of physical exercise onpreventing potentially harmful stress-related metabolic and
International Journal of Endocrinology 9
psychological consequences have been presumably mediatedby the same neuroendocrine mechanisms [59] Consideringunchanged metabolic profile of our subjects and remark-able improvements in depressive symptoms and oxida-tiveinflammatory biomarkers following either behavioralintervention it is tempting if not plausible to speculate onthe involvement of neuroendocrine mechanism(s) in achiev-ing this beneficial response It should be noted that a lackof between-group differences in changes observed in ourstudy might not be explained by a phenomenon known asldquoregression toward the meanrdquo or just a natural course ofparameters Previous findings on persistence of depressivesymptoms in people with type 2 diabetes indicate thatdepression is not only persistent [60 61] but also associatedwith an increased risk of aggravating over time [62] On theother hand oxidative damage toDNA is increasing in healthysubjects throughout time as a result of ageing process [33]while inflammatory response and ageing-associated damageto biomolecules are even more pronounced in diabetes dueto a long-term exposure to hyperglycemia and advanced-glycated end-products [34 50]
The strengths of this study are in examining a highlyprevalent population of type 2 patients with depressive symp-toms but no clinical depression using a randomized com-parative design employing structured behavioral interven-tions and analyzing clinically relevant changes of simple-to-measure oxidativeinflammatory biomarkers Its limitation isthe lack of treatment as usual control intervention precludingthe possibility to investigate the course and outcomes ofsubclinical depression without any treatment Also the studywas carried out in only one centermdasha tertiary diabetesclinicmdashwhich does not allow concluding about its feasibilityin other clinical settings Per-protocol analyses are presentedin the study results which were confirmed by the intention totreat analysis based on baseline-observation-carried-forwardapproach A lack of estimation derived frommultiple predic-tors may be considered a limitation of the study
5 Conclusions
This study has demonstrated that improvement in depressivesymptoms is accompanied with reduced oxidative dam-age and inflammatory response in type 2 diabetic patientswith subsyndromal depression Testing mediating effectshas indicated that medium-term improvement in depres-sive symptoms predicts long-term-reduction in oxidativedamage while mediating factors for observed reductionin inflammatory response should be further investigatedClinical benefits of treating subsyndromal depression wereshown to be comparable in all three treatment arms
Regardless of the mechanisms involved our study clearlyindicates that enhanced treatment as usual defined as briefpatient-centred diabetes reeducation is not inferior to psy-choeducation and exercise in providing beneficial outcomesin subsyndromally depressed type 2 diabetic patients Simplebehavioral interventions are capable not only of alleviatingdepressive symptoms but also of reducing the intensity ofdamaging oxidativeinflammatory processes thereby miti-gating the risk of development of diabetic complications
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The study was funded by the European Foundation forthe Study of Diabetes (EFSD)mdashNew Horizons CollaborativeResearch Initiative 2010 The authors would like to thankLovorka Perkovic Croatian Institute of Public Health forediting the paper
References
[1] S S Ali M A Stone J L Peters M J Davies and K KhuntildquoThe prevalence of co-morbid depression in adults with Type2 diabetes a systematic review and meta-analysisrdquo DiabeticMedicine vol 23 no 11 pp 1165ndash1173 2006
[2] P J Lustman R J Anderson K E Freedland M de Groot RM Carney and R E Clouse ldquoDepression and poor glycemiccontrol a meta-analytic review of the literaturerdquo Diabetes Carevol 23 no 7 pp 934ndash942 2000
[3] L K Richardson L E Egede M Mueller C L Echols and MGebregziabher ldquoLongitudinal effects of depression on glycemiccontrol in veterans with Type 2 diabetesrdquo General HospitalPsychiatry vol 30 no 6 pp 509ndash514 2008
[4] M de Groot R Anderson K E Freedland R E Clouse andP J Lustman ldquoAssociation of depression and diabetes com-plications ameta-analysisrdquo PsychosomaticMedicine vol 63 no4 pp 619ndash630 2001
[5] K Ismail KWinkley D Stahl T Chalder andM Edmonds ldquoAcohort study of people with diabetes and their first foot ulcerthe role of depression on mortalityrdquo Diabetes Care vol 30 no6 pp 1473ndash1479 2007
[6] X Zhang S L Norris E W Gregg Y J Cheng G Becklesand H S Kahn ldquoDepressive symptoms and mortality amongpersons with and without diabetesrdquo American Journal of Epi-demiology vol 161 no 7 pp 652ndash660 2005
[7] S A Black K S Markides and L A Ray ldquoDepression pre-dicts increased incidence of adverse health outcomes in olderMexican Americans with type 2 diabetesrdquo Diabetes Care vol26 no 10 pp 2822ndash2828 2003
[8] H Baumeister N Hutter and J Bengel ldquoPsychological andpharmacological interventions for depression in patients withdiabetesmellitus and depressionrdquoCochraneDatabase of System-atic Reviews vol 12 Article ID CD008381 2012
[9] E Harkness W Macdonald J Valderas P Coventry L Gaskand P Bower ldquoIdentifying psychosocial interventions thatimprove both physical and mental health in patients with dia-betes a systematic review and meta-analysisrdquo Diabetes Carevol 33 no 4 pp 926ndash930 2010
[10] M Berk L J Williams F N Jacka et al ldquoSo depression is aninflammatory disease but where does the inflammation comefromrdquo BMCMedicine vol 11 article 200 2013
[11] S de Kort D Keszthelyi and A A M Masclee ldquoLeaky gut anddiabetes mellitus what is the linkrdquoObesity Reviews vol 12 no6 pp 449ndash458 2011
[12] E T de Lemos J Oliveira J P Pinheiro and F Reis ldquoRegularphysical exercise as a strategy to improve antioxidant andanti-inflammatory status benefits in type 2 diabetes mellitusrdquo
10 International Journal of Endocrinology
Oxidative Medicine and Cellular Longevity vol 2012 Article ID741545 15 pages 2012
[13] T A Doyle M de Groot T Harris et al ldquoDiabetes depressivesymptoms and inflammation in older adults results fromthe Health Aging and Body Composition Studyrdquo Journal ofPsychosomatic Research vol 75 no 5 pp 419ndash424 2013
[14] J-P S Laake D Stahl S A Amiel et al ldquoThe associationbetween depressive symptoms and systemic inflammation inpeople with type 2 diabetes findings from the South Londondiabetes studyrdquoDiabetes Care vol 37 no 8 pp 2186ndash2192 2014
[15] N Rohleder ldquoStimulation of systemic low-grade inflammationby psychosocial stressrdquo Psychosomatic Medicine vol 76 no 3pp 181ndash189 2014
[16] M Maes ldquoAn intriguing and hitherto unexplained co-occur-rence depression and chronic fatigue syndrome are mani-festations of shared inflammatory oxidative and nitrosative(IOampNS) pathwaysrdquo Progress in Neuro-Psychopharmacologyand Biological Psychiatry vol 35 no 3 pp 784ndash794 2011
[17] P Palta L J Samuel E RMiller and S L Szanton ldquoDepressionand oxidative stress results from a meta-analysis of observa-tional studiesrdquo Psychosomatic Medicine vol 76 no 1 pp 12ndash192014
[18] L Rochette M Zeller Y Cottin and C Vergely ldquoDiabetes oxi-dative stress and therapeutic strategiesrdquo Biochimica et Biophys-ica Acta vol 1840 no 9 pp 2709ndash2729 2014
[19] S Keri C Szabo and O Kelemen ldquoExpression of Toll-LikeReceptors in peripheral blood mononuclear cells and responseto cognitive-behavioral therapy in major depressive disorderrdquoBrain Behavior and Immunity vol 40 pp 235ndash243 2014
[20] N Hermanns A Schmitt A Gahr et al ldquoThe effect ofa Diabetes-Specific Cognitive Behavioral Treatment Program(DIAMOS) for patients with diabetes and subclinical depres-sion results of a randomized controlled trialrdquo Diabetes Carevol 38 no 4 pp 551ndash560 2015
[21] K Kroenke R L Spitzer and J B W Williams ldquoThe patienthealth questionnaire-2 validity of a two-item depressionscreenerrdquoMedical Care vol 41 no 11 pp 1284ndash1292 2003
[22] J H Abramson ldquoWINPEPI updated computer programs forepidemiologists and their teaching potentialrdquo EpidemiologicPerspectives amp Innovations vol 8 no 1 article 1 2011
[23] J Cohen ldquoA power primerrdquo Psychological Bulletin vol 112 no1 pp 155ndash159 1992
[24] M Pibernik-Okanovic D Ajdukovic M V Lovrencic andN Hermanns ldquoDoes treatment of subsyndromal depressionimprove depression and diabetes related outcomes protocolfor a randomised controlled comparison of psycho-educationphysical exercise and treatment as usualrdquo Trials vol 12 article17 2011
[25] BArroll FGoodyear-SmithNKerse T Fishman and JGunnldquoEffect of the addition of a lsquohelprsquo question to two screeningquestions on specificity for diagnosis of depression in generalpractice diagnostic validity studyrdquo British Medical Journal vol331 no 7521 article 884 2005
[26] P Rohde P M Lewinsohn and J R Seeley ldquoComparability oftelephone and face-to-face interviews in assessing axis I and IIdisordersrdquo American Journal of Psychiatry vol 154 no 11 pp1593ndash1598 1997
[27] L S Radloff ldquoTheCES-D scalerdquoApplied Psychological Measure-ment vol 1 pp 385ndash401 1977
[28] M Gavella V Lipovac A Car M Vucic L Sokolic and RRakos ldquoSerum sialic acid in subjects with impaired glucose
tolerance and in newly diagnosed type 2 diabetic patientsrdquoActaDiabetologica vol 40 no 2 pp 95ndash100 2003
[29] M D Evans R Singh V Mistry K Sandhu P B Farmer andM S Cooke ldquoAnalysis of urinary 8-oxo-78-dihydro-purine-21015840- deoxyribonucleosides by LC-MSMS and improved ELISArdquoFree Radical Research vol 42 no 10 pp 831ndash840 2008
[30] M Pibernik-Okanovic D Begic D Ajdukovic N Andrijasevicand Z Metelko ldquoPsychoeducation versus treatment as usualin diabetic patients with subthreshold depression preliminaryresults of a randomized controlled trialrdquo Trials vol 10 article78 2009
[31] M Pibernik-Okanovic M Vucic Lovrencic D AjdukovicM Sekerija and N Hermanns ldquoPsychological behavioraland biological changes following treatments of subsyndromaldepression in people with type 2 diabetesrdquoDiabetologia vol 56supplement 1 p S465 2013
[32] L Fisher D Hessler R E Glasgow et al ldquoREDEEM a prag-matic trial to reduce diabetes distressrdquo Diabetes Care vol 36no 9 pp 2551ndash2558 2013
[33] H E Poulsen L L Nadal K Broedbaek P E Nielsen andA Weimann ldquoDetection and interpretation of 8-oxodG and 8-oxoGua in urine plasma and cerebrospinal fluidrdquo Biochimica etBiophysica ActamdashGeneral Subjects vol 1840 no 2 pp 801ndash8082014
[34] K Broedbaek A Weimann E S Stovgaard and H E PoulsenldquoUrinary 8-oxo-78-dihydro-21015840-deoxyguanosine as a biomarkerin type 2 diabetesrdquo Free Radical Biology and Medicine vol 51no 8 pp 1473ndash1479 2011
[35] M J Forlenza and G E Miller ldquoIncreased serum levels of 8-hydroxy-21015840-deoxyguanosine in clinical depressionrdquo Psychoso-matic Medicine vol 68 no 1 pp 1ndash7 2006
[36] A Jorgensen J Krogh K Miskowiak et al ldquoSystemic oxida-tively generatedDNARNAdamage in clinical depression asso-ciations to symptom severity and response to electroconvulsivetherapyrdquo Journal of Affective Disorders vol 149 no 1ndash3 pp 355ndash362 2013
[37] S Yi ANanri YMatsushitaHKasai K Kawai andTMizoueldquoDepressive symptoms and oxidative DNA damage in Japanesemunicipal employeesrdquo Psychiatry Research vol 200 no 2-3 pp318ndash322 2012
[38] H Nojima H Watanabe K Yamane et al ldquoEffect of aerobicexercise training on oxidative stress in patients with type 2diabetes mellitusrdquo Metabolism Clinical and Experimental vol57 no 2 pp 170ndash176 2008
[39] S Bonakdaran and B Kharaqani ldquoAssociation of serum uricacid and metabolic syndrome in type 2 diabetesrdquo CurrentDiabetes Reviews vol 10 no 2 pp 113ndash117 2014
[40] R J Johnson T Nakagawa L G Sanchez-Lozada et al ldquoSugaruric acid and the etiology of diabetes and obesityrdquoDiabetes vol62 no 10 pp 3307ndash3315 2013
[41] M L Wahlqvist ldquoAntioxidant relevance to human healthrdquo AsiaPacific Journal of Clinical Nutrition vol 22 no 2 pp 171ndash1762013
[42] A De Giorgi F Fabbian M Pala et al ldquoUric acid friend orfoe Uric acid and cognitive function lsquogout kills more wise menthan simplersquordquo European Review forMedical and PharmacologicalSciences vol 19 no 4 pp 640ndash646 2015
[43] M Vucic B Rocic V Bozikov and S J H Ashcroft ldquoPlasmauric acid and total antioxidant status in patients with diabetesmellitusrdquo Hormone and Metabolic Research vol 29 no 7 pp355ndash357 1997
International Journal of Endocrinology 11
[44] G Desideri G Castaldo A Lombardi et al ldquoIs it time to revisethe normal range of serum uric acid levelsrdquo European Reviewfor Medical and Pharmacological Sciences vol 18 no 9 pp1295ndash1306 2014
[45] H-Y Chen I-C Cheng Y-J Pan et al ldquoCognitive-behavioraltherapy for sleep disturbance decreases inflammatory cytokinesand oxidative stress in hemodialysis patientsrdquo Kidney Interna-tional vol 80 no 4 pp 415ndash422 2011
[46] A Varki and P Gagneux ldquoMultifarious roles of sialic acids inimmunityrdquo Annals of the New York Academy of Sciences vol1253 no 1 pp 16ndash36 2012
[47] K P Gopaul and M A Crook ldquoSialic acid a novel marker ofcardiovascular diseaserdquo Clinical Biochemistry vol 39 no 7 pp667ndash681 2006
[48] L M Browning S A Jebb G D Mishra et al ldquoElevated sialicacid but not CRP predicts features of the metabolic syndromeindependently of BMI in womenrdquo International Journal ofObesity vol 28 no 8 pp 1004ndash1010 2004
[49] LMThornton B L Andersen T A Schuler andW E CarsonldquoA psychological intervention reduces inflammatory markersby alleviating depressive symptoms secondary analysis of arandomized controlled trialrdquo Psychosomatic Medicine vol 71no 7 pp 715ndash724 2009
[50] N Esser S Legrand-Poels J Piette A J Scheen and N PaquotldquoInflammation as a link between obesity metabolic syndromeand type 2 diabetesrdquoDiabetes Research andClinical Practice vol105 no 2 pp 141ndash150 2014
[51] R Hutcheson and P Rocic ldquoThe metabolic syndrome oxida-tive stress environment and cardiovascular disease the greatexplorationrdquo Experimental Diabetes Research vol 2012 ArticleID 271028 13 pages 2012
[52] L Fontana and F B Hu ldquoOptimal body weight for health andlongevity bridging basic clinical and population researchrdquoAging Cell vol 13 no 3 pp 391ndash400 2014
[53] A T Turer and P E Scherer ldquoAdiponectin mechanistic insightsand clinical implicationsrdquo Diabetologia vol 55 no 9 pp 2319ndash2326 2012
[54] WHO ldquoObesity and overweightrdquo Fact sheet No 311 2015[55] P W Gold ldquoThe organization of the stress system and its
dysregulation in depressive illnessrdquo Molecular Psychiatry vol20 no 1 pp 32ndash47 2015
[56] S Purkayastha and D Cai ldquoNeuroinflammatory basis ofmetabolic syndromerdquo Molecular Metabolism vol 2 no 4 pp356ndash363 2013
[57] K Aschbacher A OrsquoDonovan O MWolkowitz F S DhabharY Su and E Epel ldquoGood stress bad stress and oxidative stressinsights from anticipatory cortisol reactivityrdquo Psychoneuroen-docrinology vol 38 no 9 pp 1698ndash1708 2013
[58] C F Sharpley ldquoA review of the neurobiological effects of psy-chotherapy for depressionrdquo Psychotherapy vol 47 no 4 pp603ndash615 2010
[59] M N Silverman and P A Deuster ldquoBiological mechanismsunderlying the role of physical fitness in health and resiliencerdquoInterface Focus vol 4 no 5 Article ID 20140040 2014
[60] G Nefs F Pouwer J Denollet and V Pop ldquoThe course ofdepressive symptoms in primary care patients with type 2 dia-betes results from theDiabetes Depression TypeDPersonalityZuidoost-Brabant (DiaDDZoB) Studyrdquo Diabetologia vol 55no 3 pp 608ndash616 2012
[61] M Pibernik-Okanovic D Begic K Peros S Szabo andZ Metelko ldquoPsychosocial factors contributing to persistent
depressive symptoms in type 2 diabetic patients a Croatiansurvey from the European Depression in Diabetes ResearchConsortiumrdquo Journal of Diabetes and Its Complications vol 22no 4 pp 246ndash253 2008
[62] M Bot F Pouwer J Ormel J P J Slaets and P de Jonge ldquoPre-dictors of incidentmajor depression in diabetic outpatients withsubthreshold depressionrdquo Diabetic Medicine vol 27 no 11 pp1295ndash1301 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

International Journal of Endocrinology 5
Variables indicating a level of depressive symptoms andbiomarkers of oxidative damage and inflammation weremeasured at baseline and after six- and twelve-month follow-up periods HbA1c leukocytes serum hs-CRP and uric acidwere assayed in fresh samples obtained in the morning afteran overnight fast Samples for sialic acid adiponectin and u-8-oxodG measurements were frozen (minus70∘C) until analyzedThe samples from each patient were analyzed with ELISAs atthe samemicroplate in order to avoid possible between-seriesvariability
23 Statistical Methods Data are presented as means (SD)unless otherwise indicated Due to the nonparametric dis-tribution hs-CRP results were log-transformed prior to theanalysis One-way ANOVA and chi squares were used todetermine baseline differences across the three treatmentarms and examine differences between continuing partici-pants and dropouts
Data were analyzed per protocol after exclusion of par-ticipants who withdrew did not attend all three follow-up meetings initiated psychopharmacological treatment ordied during the study period these results are presentedthroughout the paper Intention-to-treat (ITT) analysis wasperformed to validate these results all participants whowere randomized were analyzed despite deviations from theprotocol To perform ITT missing data were imputed usingthe baseline observation carried forward approach
Repeated measures ANOVA was used to test for changesin outcome variables across time and between the groupsCohenrsquos 1205782 coefficients ranging from 001 to 005 wereregarded as small from006 to 012moderate andge013 large
Regression analysis was employed to test directionalrelations between depressive symptoms and reduction ininflammation and oxidative stress
A 119901 value of lt005 was considered significant in allanalyses
Statistical analyses were performed by using the SPSS 17(SPSS Inc Chicago IL USA)
24 Ethical Aspects The study was approved by the VukVrhovac University Clinic for Diabetes Ethics Committee onJune 30 2010 A written informed consent was obtained fromall the participants
3 Results
Among the 1740 patients assessed for eligibility 365 wereconsidered eligible and 265 agreed to participate in the inter-ventions (72) Of these 209 completed baseline laboratoryand psychological assessments (79) with 74 randomizedto psychoeducational intervention 66 to physical exerciseand 69 to diabetes reeducation Attrition rate was 3 duringthe interventions (6 of 209 patients) 3 from baseline tosix months (7 of 203 patients) and 2 from 6-month to 12-month follow-up period (4 of 196 patients) Of the sevendropouts who completed the intervention but missed bothfollow-up assessments two missed the follow-up appoint-ments due to health problems four were unwilling to comeand one patient died No harmful incidents were recorded
throughout the interventions Four patients were excludedfromper-protocol analyses due to the initiation of pharmaco-logical therapy No differences between the participants anddropouts across the three study groups were observed
Table 2 presents demographic and diabetes-related char-acteristics of patients randomized to one of the three groupsand a baseline level of depressive symptoms as self-assessedby the CES-D questionnaire No between-group differencesregarding demographic diabetes-related and psychologicalvariables were found
The effects of interventions on depressive symptoms andbiomarkers of oxidative damage and inflammation as wellas glucoregulation (HbA1c) and BMI based on repeatedmeasures ANOVA are given in Table 3 ITT analyses showeda comparable pattern of results of all analyses in terms ofstatistical significance and effect size and are not presentedin the text
31 Changes in Depressive Symptoms No significant be-tween-group differences over time were obtained with res-pect to depressive symptoms (119865 = 061 119901 = 0656) indi-cating comparable efficacy of psychoeducation physical exer-cise and enhanced treatment as usual on the primary studyoutcome
Significant reductions in depressive symptoms occurredacross all three study groups from baseline to 12 months(119865 = 1251 119901 lt 0001 1205782 = 07) The size of the time effectindicated a moderate effect of the three treatments on self-assessed depressive symptoms
32 Changes in Biomarkers of Oxidative Damage and Inflam-mation Total leukocytes significantly decreased in all threegroups (119865 = 1261 119901 lt 00001 1205782 = 007) as did u-8-oxodG (119865 = 1066 119901 lt 00001 1205782 = 006) and sialic acid(119865 = 8457 119901 lt 00001 1205782 = 032) The latter showed smallbut statistically significant time 119909 group effect (119865 = 340119901 = 001 1205782 = 004) However after adjusting the results formultiple comparisons by Bonferroni test it did not remainsignificant Uric acid increased significantly over one year inall three groups (119865 = 1339 119901 lt 00001 1205782 = 007) Theeffects of the interventions on sialic acid can be regarded aslarge (032) and on leukocytes u-8-oxodG and uric acid asmoderate (007 006 and 007 resp)
No significant changes were registered with respect toadiponectin and hs-CRP
NeitherHbA1c nor BMIwere significantly changed in anyof the study groups from baseline to 12 months
No between-group effects were obtained with respectto one-year changes in biomarkers of inflammation andoxidative damage (all 119901 gt 005)
33 Testing for Mediation The results obtained by usingregression analyses indicated that improvement in depressivesymptoms at six months predicted reductions in u-8-oxodGat twelve-month follow-up (120573 = 015 119901 = 0044) whilethe results for sialic and uric acid were close to statisticalsignificance (119901 = 0069 and 119901 = 0070 resp) (results notshown in tables)
6 International Journal of Endocrinology
Table 2 Baseline characteristics of participants by the intervention groups (119899 = 209)
Psychoeducation Physical exercise Enhanced treatment as usual Siglowast
119873 74 66 69Age (yrs) 577 (62) 585 (48) 582 (56) 0648Female (119899) 40 37 36 0867Education (yrs) 126 (24) 124 (23) 122 (25) 0623Professional status ( employed) 30 27 30 0502Economic status ( poor) 13 12 13 0317Family status ( marriedcohabitating) 76 72 76 0488Insulin use () 32 29 32 0695OHA use () 56 57 53 0664Insulin + OHA use () 12 14 15 0632Statin use () 68 71 71 0786HbA1c () 74 (12) 72 (11) 72 (11) 0384HbA1c (mmolmol) 58 (13) 56 (13) 55 (11) 0442Body mass index kgm2 3064 (454) 2944 (467) 2996 (439) 0297Depressive symptoms (CES-D score) 197 (91) 205 (86) 197 (87) 0813Data are means (SD) or percentageslowastSig significancelowast One-way ANOVA or 1205942 as appropriateOHA = oral hypoglycemic agents
4 Discussion
This randomized interventional study attempted to evaluatethe effect of two behavioral interventions psychoeducationand physical exercise as compared to enhanced treatmentas usual on depressive symptoms and the intensity ofoxidativeinflammatory processes in diabetic patients suf-fering from subsyndromal depression The results indicateprotracted favorable effects of either intervention on loweringdepressive symptoms while reducing overall oxidative dam-age and cellular inflammatory response as well as improvingantioxidant capacity
In all three study arms a comparable and clinically mean-ingful improvement in depressive symptoms was obtainedThe intervention-independent results regarding depression-related outcomes confirm our preliminary report indicatingthat treatment as usual was equally effective as psychoe-ducation in reducing depressive symptoms and improvingmetabolic control in type 2 diabetic patients with subsyndro-mal depression [30] Also no between-groupdifferenceswerefound within a randomized controlled comparison of psy-choeducation physical exercise and control arm consistingof brief diabetes reeducation [31]The absence of a significanttreatment effect suggested that patterns of change might besimilar in all treatment groups Hypothetically addressingpatientsrsquo emotional needs and their diabetes-related distresswhich were common in all three approaches may indicate apossible pathway of change Similar findings were obtained ina study by Fisher et al [32] which demonstrated that clinicallyreasonable improvements in emotional symptoms may bestimulated by even minimal behavioral interventions
In this study a significant decrease in overall oxidativedamage was observed from basal to one-year posttreatmentfollow-up by measuring a recognized biomarker of oxidativedamage to DNAmdashurinary 8-oxodG Urinary excretion of
8-oxodG reflects the average rate of nucleic acid guanineoxidation and can be regarded as a reliable marker of generalintracellular oxidative stress [33] Research on the u-8-oxodGin diabetes revealed its significant association with severehyperglycemia poor diabetes control and severity of dia-betic complications as well as predictive value for diabetes-associated morbidity [34] The relationship between u-8-oxodG and depression has been modestly investigated andprovided controversial results from an increase to no changedepending on the study-specific depression phenotype [35ndash37] To our knowledge this is the first study investigating u-8-oxodG in patients with diabetes and elevated depressivesymptoms While the results in our exercise group are inaccord with previously reported reduction in u-8-oxodGelicited bymoderate-intensity exercise in type 2 diabetes over12 months [38] significant decrease in u-8-oxodG levels inpsychoeducation and diabetes reeducation group is a novelfinding indicating that cognitive-behavioral approach mighthave beneficial effects on oxidative damage reduction indiabetic patients with subsyndromal depression Additionalsupport for this finding was a significant increase in serumuric acid level at follow-up
Uric acid is an end-product of purine metabolism withcomplex and multifarious roles in human physiology Apartfrom causing gout hyperuricemia has been identified as arisk factor for metabolic syndrome type 2 diabetes andcardiovascular diseases [39] Recently proposed intriguinghypothesis linking hyperuricemia derived by an increasedconsumption of dietary fructose with an epidemic of car-diometabolic diseases attracted a lot of attention and createda paradigm of uric acid as being an exclusively harmfulmetabolite [40] By contrast uric acid has long been recog-nized as one of the most powerful endogenous antioxidants[41] and an efficient mediator of neuroprotection cognitivefunction and intellectual performance [42] as well as the
International Journal of Endocrinology 7
Table 3 One-year changes of depressive symptoms inflammatory- and prooxidative biomarkers
Group scores BaselineM (SD)
12-month follow-upM (SD) Effects 119865 Overall 119875lowast 119875
0 to 12molowastlowast 1205782
Depressive symptomsA (119899 = 64) 197 (91) 167 (79) Time 1251 lt0001 0003 007B (119899 = 58) 198 (82) 181 (98) Time times group 061 0656 0007C (119899 = 57) 190 (86) 174 (94)
Leukocytes (times109L)A (119899 = 63) 75 (17) 73 (17) Time 1261 lt0001 lt0001 007B (119899 = 58) 75 (16) 71 (15) Time times group 132 0265 0001C (119899 = 57) 78 (22) 71 (20)
CRP (mgL)
A (119899 = 64) 028 (049) 025 (044) Time 238 009 100 001B (119899 = 57) 034 (046) 032 (041) Time times group 087 048 001C (119899 = 57) 035 (041) 024 (039)
Sialic acid (mmolL)A (119899 = 64) 21 (031) 19 (029) Time 8457 lt0001 lt0001 032B (119899 = 58) 21 (031) 18 (022) Time times group 340 001 004C (119899 = 57) 21 (028) 18 (024)
u-8-OxodG (120583gmmol)A (119899 = 64) 11 (05) 09 (04) Time 1066 lt0001 lt0001 006B (119899 = 57) 14 (08) 11 (06) Time times group 109 036 001C (119899 = 57) 12 (07) 10 (04)
Uric acid (120583molL)A (119899 = 64) 2917 (852) 3103 (775) Time 1339 lt0001 lt0001 007B (119899 = 58) 3034 (919) 3232 (931) Time times group 025 091 0003C (119899 = 57) 2904 (779) 3145 (834)
HbA1c ()A (119899 = 64) 74 (13) 72 (09) Time 270 007 008 002B (119899 = 58) 72 (10) 72 (10) Time times group 092 045 001C (119899 = 57) 71 (10) 70 (10)
HbA1c (mmolL)A (119899 = 64) 578 (136) 559 (102) Time 331 005 100 002B (119899 = 58) 548 (114) 557 (107) Time times group 090 045 001C (119899 = 57) 548 (107) 539 (100)
Adiponectin (mgL)A (119899 = 63) 75 (23) 71 (38) Time 073 044 100 0004B (119899 = 58) 91 (61) 90 (67) Time times group 055 065 0006C (119899 = 57) 80 (50) 81 (53)
Body mass index (kgm2)A (119899 = 54) 306 (47) 306 (50) Time 172 019 011 001B (119899 = 53) 292 (45) 290 (46) Time times group 131 027 001C (119899 = 52) 301 (41) 294 (40)
lowastTwo-sided significance of differences across time and between the groups (repeated measures ANOVA)lowastlowastTwo-sided significance of differences between baseline and 12-month assessmentsLog-transformed data
8 International Journal of Endocrinology
most pronounced determinant of total plasma antioxidantcapacity in diabetic patients [43] Thus maintaining uricacid levels within physiological range appears to be morefavorable than radical lowering in prevention of variousmor-bidities Based on recent epidemiological evidence includingcardiometabolic risk assessment a new gender-independentupper limit of reference range for uric acid has been proposedat the level of 360 120583molL [44] The present study revealsa significant increase in uric acid levels at follow-up butwell below proposed cut-off above which negative effectsof hyperuricemia might be expected On the contrary theobserved uric acid increase in our study is rather suggestiveof an improved antioxidant capacity elicited by behavioralinterventions in type 2 diabetic patients with subsyndromaldepression
Beneficial effect of cognitive-behavioral interventionin reducing oxidative stress and inflammatory responsehas been reported in hemodialysis patients suffering frominsomnia [45] but rather sparse depression-related studiesmainly focused on the assessment of low-grade inflammationbiomarkers In a very recent randomized trial evaluating anewly developed cognitive-behavioral program (DIAMOS)in diabetic patients with subsyndromal depression a set ofpro- and anti-inflammatory biomarkers was analyzed at basaland one-year follow-up [20] No change in hs-CRP IL-1 andadiponectin was observed whereas a significant decrease ininterleukin-1 receptor antagonist (IL-1RA) was interpreted asan indirect index of alleviated IL-1-related damaging mech-anisms presumably involved in the pathogenesis of micro-and macrovascular complications of diabetes Likewise ourstudy could not demonstrate any influence of the behavioralinterventions on hs-CRP and adiponectin but we foundother inflammatory markers that is leukocyte count andtotal serum sialic acid (TSA) significantly reduced with thelatter being largely affected (1205782 = 032) by the interventionsperformed
Sialic acids comprise a family of heterogenous monosac-charides abundantly present on the cell membranes withcomplex and multiple biological roles in cellular signalingand immunity [46] TSA is a validated inflammatory andatherogenic marker that has been proposed as a novelbiomarker of cardiovascular disease [47] Elevated levels ofTSA in newly diagnosed type 2 diabetic patients have beenlinked to the risk for later development of macrovascularcomplications [28] Interestingly TSA has been identified asa superior predictive biomarker of metabolic syndrome overthe abundantly used hs-CRP [48] Nevertheless despite theobvious advantages TSA has been largely underutilized inthe research on combined inflammatory-metabolic patholo-gies and it has not been studied in depression until this studyOur results identify TSA as a sensitive biomarker of inflam-mation degree in subsyndromally depressed diabetic patientswhereas neither of the established biomarkers of low-gradeinflammation hs-CRP and adiponectin was able to reflectthe anti-inflammatory effect of the performed interventionsSignificant decrease in leukocyte count however clearlyconfirmed postintervention attenuation of the cell-mediatedinflammation response in our patients with an importantnotice that the presence of acute infection at the assessments
was excluded by total leukocyte count lt 100 times 109L or hs-CRP lt 50 gL
The ability of psychological intervention to reduceboth depressive symptoms and inflammation has been evi-denced in depressed breast-cancer patients [49] Further-more due to the insightful study-design Thornton et alwere able to demonstrate a bidirectional mechanistic rela-tionship between depressive symptoms and inflammationThe paradigmatic view of the low-grade inflammation asthe inflicting mechanism for depression has been at leastcomplemented if not refuted by their finding on the mecha-nistic role of depressive symptoms lowering in the reductionof inflammatory response [49] This explanatory mecha-nism might also be translated to our results particularlyconsidering a lack of any effect of interventions towardshyperglycemia and obesity in our study
It is well known that the intensity of oxidative damage andinflammation in diabetes is remarkably and positively asso-ciated with the severity of hyperglycemia [18] Howeverthe observed reduction in oxidative damage and low-gradeinflammation in our study could not be attributed to thismechanism since no significant changes from baseline tofollow-up were found in HbA1c clinically considered toreflect a fair glucoregulation (Table 3) Obesity-derived low-grade inflammation is another recognized harmful compo-nent in the pathogenesis of type 2 diabetes and its compli-cations [50] Obesity induces a disbalance between pro- andanti-inflammatory cytokinesadipokines resulting in low-grade inflammation and related adverse health outcomesranging from metabolic syndrome and diabetes to cardio-vascular diseases and cancer as well as depression [49ndash51]Reduction in bodyweight is accompanied by beneficialmeta-bolic and hormonal profiles and a reduced inflammation [52]with increased production of anti-inflammatory adipokineadiponectin suggested to be among themost relevant features[53] Since our subjects classified as overweightobese [54]retained their BMI at follow-up and revealed no changes inadiponectin levels it is likely that the observed effects ofinterventions on the reduction in depressive symptoms andoxidativeinflammatory biomarkers in this study dependedon another mechanism(s)
Chronic stress with deregulation of stress-response adap-tive mechanisms is considered to be a common feature ofboth diabetes and depression [55] There is a growing bodyof evidence suggesting that metabolic inflammation asso-ciated with obesity and diabetes inflicts neuroinflammationwhich causes serious disturbances of the hypothalamic-pituitary-adrenal (HPA) axis function and consequentlyleads to impairment of adaptive stress-response [56] More-over chronic stress exposure has recently been demonstratedas a promoting factor for accelerated oxidative damagewhereby a sustained activation of HPA-axis emerged again asthe key mediator [57] Neuroendocrine effects of behavioraltreatment for depression have not been extensively studiedbut the evidence so far suggests a hypothetical pathway thatconnects the nurturing effects derived from the patient-ther-apist ldquobondrdquo with reestablishment of neuroendocrine home-ostasis [58] Moreover positive effects of physical exercise onpreventing potentially harmful stress-related metabolic and
International Journal of Endocrinology 9
psychological consequences have been presumably mediatedby the same neuroendocrine mechanisms [59] Consideringunchanged metabolic profile of our subjects and remark-able improvements in depressive symptoms and oxida-tiveinflammatory biomarkers following either behavioralintervention it is tempting if not plausible to speculate onthe involvement of neuroendocrine mechanism(s) in achiev-ing this beneficial response It should be noted that a lackof between-group differences in changes observed in ourstudy might not be explained by a phenomenon known asldquoregression toward the meanrdquo or just a natural course ofparameters Previous findings on persistence of depressivesymptoms in people with type 2 diabetes indicate thatdepression is not only persistent [60 61] but also associatedwith an increased risk of aggravating over time [62] On theother hand oxidative damage toDNA is increasing in healthysubjects throughout time as a result of ageing process [33]while inflammatory response and ageing-associated damageto biomolecules are even more pronounced in diabetes dueto a long-term exposure to hyperglycemia and advanced-glycated end-products [34 50]
The strengths of this study are in examining a highlyprevalent population of type 2 patients with depressive symp-toms but no clinical depression using a randomized com-parative design employing structured behavioral interven-tions and analyzing clinically relevant changes of simple-to-measure oxidativeinflammatory biomarkers Its limitation isthe lack of treatment as usual control intervention precludingthe possibility to investigate the course and outcomes ofsubclinical depression without any treatment Also the studywas carried out in only one centermdasha tertiary diabetesclinicmdashwhich does not allow concluding about its feasibilityin other clinical settings Per-protocol analyses are presentedin the study results which were confirmed by the intention totreat analysis based on baseline-observation-carried-forwardapproach A lack of estimation derived frommultiple predic-tors may be considered a limitation of the study
5 Conclusions
This study has demonstrated that improvement in depressivesymptoms is accompanied with reduced oxidative dam-age and inflammatory response in type 2 diabetic patientswith subsyndromal depression Testing mediating effectshas indicated that medium-term improvement in depres-sive symptoms predicts long-term-reduction in oxidativedamage while mediating factors for observed reductionin inflammatory response should be further investigatedClinical benefits of treating subsyndromal depression wereshown to be comparable in all three treatment arms
Regardless of the mechanisms involved our study clearlyindicates that enhanced treatment as usual defined as briefpatient-centred diabetes reeducation is not inferior to psy-choeducation and exercise in providing beneficial outcomesin subsyndromally depressed type 2 diabetic patients Simplebehavioral interventions are capable not only of alleviatingdepressive symptoms but also of reducing the intensity ofdamaging oxidativeinflammatory processes thereby miti-gating the risk of development of diabetic complications
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The study was funded by the European Foundation forthe Study of Diabetes (EFSD)mdashNew Horizons CollaborativeResearch Initiative 2010 The authors would like to thankLovorka Perkovic Croatian Institute of Public Health forediting the paper
References
[1] S S Ali M A Stone J L Peters M J Davies and K KhuntildquoThe prevalence of co-morbid depression in adults with Type2 diabetes a systematic review and meta-analysisrdquo DiabeticMedicine vol 23 no 11 pp 1165ndash1173 2006
[2] P J Lustman R J Anderson K E Freedland M de Groot RM Carney and R E Clouse ldquoDepression and poor glycemiccontrol a meta-analytic review of the literaturerdquo Diabetes Carevol 23 no 7 pp 934ndash942 2000
[3] L K Richardson L E Egede M Mueller C L Echols and MGebregziabher ldquoLongitudinal effects of depression on glycemiccontrol in veterans with Type 2 diabetesrdquo General HospitalPsychiatry vol 30 no 6 pp 509ndash514 2008
[4] M de Groot R Anderson K E Freedland R E Clouse andP J Lustman ldquoAssociation of depression and diabetes com-plications ameta-analysisrdquo PsychosomaticMedicine vol 63 no4 pp 619ndash630 2001
[5] K Ismail KWinkley D Stahl T Chalder andM Edmonds ldquoAcohort study of people with diabetes and their first foot ulcerthe role of depression on mortalityrdquo Diabetes Care vol 30 no6 pp 1473ndash1479 2007
[6] X Zhang S L Norris E W Gregg Y J Cheng G Becklesand H S Kahn ldquoDepressive symptoms and mortality amongpersons with and without diabetesrdquo American Journal of Epi-demiology vol 161 no 7 pp 652ndash660 2005
[7] S A Black K S Markides and L A Ray ldquoDepression pre-dicts increased incidence of adverse health outcomes in olderMexican Americans with type 2 diabetesrdquo Diabetes Care vol26 no 10 pp 2822ndash2828 2003
[8] H Baumeister N Hutter and J Bengel ldquoPsychological andpharmacological interventions for depression in patients withdiabetesmellitus and depressionrdquoCochraneDatabase of System-atic Reviews vol 12 Article ID CD008381 2012
[9] E Harkness W Macdonald J Valderas P Coventry L Gaskand P Bower ldquoIdentifying psychosocial interventions thatimprove both physical and mental health in patients with dia-betes a systematic review and meta-analysisrdquo Diabetes Carevol 33 no 4 pp 926ndash930 2010
[10] M Berk L J Williams F N Jacka et al ldquoSo depression is aninflammatory disease but where does the inflammation comefromrdquo BMCMedicine vol 11 article 200 2013
[11] S de Kort D Keszthelyi and A A M Masclee ldquoLeaky gut anddiabetes mellitus what is the linkrdquoObesity Reviews vol 12 no6 pp 449ndash458 2011
[12] E T de Lemos J Oliveira J P Pinheiro and F Reis ldquoRegularphysical exercise as a strategy to improve antioxidant andanti-inflammatory status benefits in type 2 diabetes mellitusrdquo
10 International Journal of Endocrinology
Oxidative Medicine and Cellular Longevity vol 2012 Article ID741545 15 pages 2012
[13] T A Doyle M de Groot T Harris et al ldquoDiabetes depressivesymptoms and inflammation in older adults results fromthe Health Aging and Body Composition Studyrdquo Journal ofPsychosomatic Research vol 75 no 5 pp 419ndash424 2013
[14] J-P S Laake D Stahl S A Amiel et al ldquoThe associationbetween depressive symptoms and systemic inflammation inpeople with type 2 diabetes findings from the South Londondiabetes studyrdquoDiabetes Care vol 37 no 8 pp 2186ndash2192 2014
[15] N Rohleder ldquoStimulation of systemic low-grade inflammationby psychosocial stressrdquo Psychosomatic Medicine vol 76 no 3pp 181ndash189 2014
[16] M Maes ldquoAn intriguing and hitherto unexplained co-occur-rence depression and chronic fatigue syndrome are mani-festations of shared inflammatory oxidative and nitrosative(IOampNS) pathwaysrdquo Progress in Neuro-Psychopharmacologyand Biological Psychiatry vol 35 no 3 pp 784ndash794 2011
[17] P Palta L J Samuel E RMiller and S L Szanton ldquoDepressionand oxidative stress results from a meta-analysis of observa-tional studiesrdquo Psychosomatic Medicine vol 76 no 1 pp 12ndash192014
[18] L Rochette M Zeller Y Cottin and C Vergely ldquoDiabetes oxi-dative stress and therapeutic strategiesrdquo Biochimica et Biophys-ica Acta vol 1840 no 9 pp 2709ndash2729 2014
[19] S Keri C Szabo and O Kelemen ldquoExpression of Toll-LikeReceptors in peripheral blood mononuclear cells and responseto cognitive-behavioral therapy in major depressive disorderrdquoBrain Behavior and Immunity vol 40 pp 235ndash243 2014
[20] N Hermanns A Schmitt A Gahr et al ldquoThe effect ofa Diabetes-Specific Cognitive Behavioral Treatment Program(DIAMOS) for patients with diabetes and subclinical depres-sion results of a randomized controlled trialrdquo Diabetes Carevol 38 no 4 pp 551ndash560 2015
[21] K Kroenke R L Spitzer and J B W Williams ldquoThe patienthealth questionnaire-2 validity of a two-item depressionscreenerrdquoMedical Care vol 41 no 11 pp 1284ndash1292 2003
[22] J H Abramson ldquoWINPEPI updated computer programs forepidemiologists and their teaching potentialrdquo EpidemiologicPerspectives amp Innovations vol 8 no 1 article 1 2011
[23] J Cohen ldquoA power primerrdquo Psychological Bulletin vol 112 no1 pp 155ndash159 1992
[24] M Pibernik-Okanovic D Ajdukovic M V Lovrencic andN Hermanns ldquoDoes treatment of subsyndromal depressionimprove depression and diabetes related outcomes protocolfor a randomised controlled comparison of psycho-educationphysical exercise and treatment as usualrdquo Trials vol 12 article17 2011
[25] BArroll FGoodyear-SmithNKerse T Fishman and JGunnldquoEffect of the addition of a lsquohelprsquo question to two screeningquestions on specificity for diagnosis of depression in generalpractice diagnostic validity studyrdquo British Medical Journal vol331 no 7521 article 884 2005
[26] P Rohde P M Lewinsohn and J R Seeley ldquoComparability oftelephone and face-to-face interviews in assessing axis I and IIdisordersrdquo American Journal of Psychiatry vol 154 no 11 pp1593ndash1598 1997
[27] L S Radloff ldquoTheCES-D scalerdquoApplied Psychological Measure-ment vol 1 pp 385ndash401 1977
[28] M Gavella V Lipovac A Car M Vucic L Sokolic and RRakos ldquoSerum sialic acid in subjects with impaired glucose
tolerance and in newly diagnosed type 2 diabetic patientsrdquoActaDiabetologica vol 40 no 2 pp 95ndash100 2003
[29] M D Evans R Singh V Mistry K Sandhu P B Farmer andM S Cooke ldquoAnalysis of urinary 8-oxo-78-dihydro-purine-21015840- deoxyribonucleosides by LC-MSMS and improved ELISArdquoFree Radical Research vol 42 no 10 pp 831ndash840 2008
[30] M Pibernik-Okanovic D Begic D Ajdukovic N Andrijasevicand Z Metelko ldquoPsychoeducation versus treatment as usualin diabetic patients with subthreshold depression preliminaryresults of a randomized controlled trialrdquo Trials vol 10 article78 2009
[31] M Pibernik-Okanovic M Vucic Lovrencic D AjdukovicM Sekerija and N Hermanns ldquoPsychological behavioraland biological changes following treatments of subsyndromaldepression in people with type 2 diabetesrdquoDiabetologia vol 56supplement 1 p S465 2013
[32] L Fisher D Hessler R E Glasgow et al ldquoREDEEM a prag-matic trial to reduce diabetes distressrdquo Diabetes Care vol 36no 9 pp 2551ndash2558 2013
[33] H E Poulsen L L Nadal K Broedbaek P E Nielsen andA Weimann ldquoDetection and interpretation of 8-oxodG and 8-oxoGua in urine plasma and cerebrospinal fluidrdquo Biochimica etBiophysica ActamdashGeneral Subjects vol 1840 no 2 pp 801ndash8082014
[34] K Broedbaek A Weimann E S Stovgaard and H E PoulsenldquoUrinary 8-oxo-78-dihydro-21015840-deoxyguanosine as a biomarkerin type 2 diabetesrdquo Free Radical Biology and Medicine vol 51no 8 pp 1473ndash1479 2011
[35] M J Forlenza and G E Miller ldquoIncreased serum levels of 8-hydroxy-21015840-deoxyguanosine in clinical depressionrdquo Psychoso-matic Medicine vol 68 no 1 pp 1ndash7 2006
[36] A Jorgensen J Krogh K Miskowiak et al ldquoSystemic oxida-tively generatedDNARNAdamage in clinical depression asso-ciations to symptom severity and response to electroconvulsivetherapyrdquo Journal of Affective Disorders vol 149 no 1ndash3 pp 355ndash362 2013
[37] S Yi ANanri YMatsushitaHKasai K Kawai andTMizoueldquoDepressive symptoms and oxidative DNA damage in Japanesemunicipal employeesrdquo Psychiatry Research vol 200 no 2-3 pp318ndash322 2012
[38] H Nojima H Watanabe K Yamane et al ldquoEffect of aerobicexercise training on oxidative stress in patients with type 2diabetes mellitusrdquo Metabolism Clinical and Experimental vol57 no 2 pp 170ndash176 2008
[39] S Bonakdaran and B Kharaqani ldquoAssociation of serum uricacid and metabolic syndrome in type 2 diabetesrdquo CurrentDiabetes Reviews vol 10 no 2 pp 113ndash117 2014
[40] R J Johnson T Nakagawa L G Sanchez-Lozada et al ldquoSugaruric acid and the etiology of diabetes and obesityrdquoDiabetes vol62 no 10 pp 3307ndash3315 2013
[41] M L Wahlqvist ldquoAntioxidant relevance to human healthrdquo AsiaPacific Journal of Clinical Nutrition vol 22 no 2 pp 171ndash1762013
[42] A De Giorgi F Fabbian M Pala et al ldquoUric acid friend orfoe Uric acid and cognitive function lsquogout kills more wise menthan simplersquordquo European Review forMedical and PharmacologicalSciences vol 19 no 4 pp 640ndash646 2015
[43] M Vucic B Rocic V Bozikov and S J H Ashcroft ldquoPlasmauric acid and total antioxidant status in patients with diabetesmellitusrdquo Hormone and Metabolic Research vol 29 no 7 pp355ndash357 1997
International Journal of Endocrinology 11
[44] G Desideri G Castaldo A Lombardi et al ldquoIs it time to revisethe normal range of serum uric acid levelsrdquo European Reviewfor Medical and Pharmacological Sciences vol 18 no 9 pp1295ndash1306 2014
[45] H-Y Chen I-C Cheng Y-J Pan et al ldquoCognitive-behavioraltherapy for sleep disturbance decreases inflammatory cytokinesand oxidative stress in hemodialysis patientsrdquo Kidney Interna-tional vol 80 no 4 pp 415ndash422 2011
[46] A Varki and P Gagneux ldquoMultifarious roles of sialic acids inimmunityrdquo Annals of the New York Academy of Sciences vol1253 no 1 pp 16ndash36 2012
[47] K P Gopaul and M A Crook ldquoSialic acid a novel marker ofcardiovascular diseaserdquo Clinical Biochemistry vol 39 no 7 pp667ndash681 2006
[48] L M Browning S A Jebb G D Mishra et al ldquoElevated sialicacid but not CRP predicts features of the metabolic syndromeindependently of BMI in womenrdquo International Journal ofObesity vol 28 no 8 pp 1004ndash1010 2004
[49] LMThornton B L Andersen T A Schuler andW E CarsonldquoA psychological intervention reduces inflammatory markersby alleviating depressive symptoms secondary analysis of arandomized controlled trialrdquo Psychosomatic Medicine vol 71no 7 pp 715ndash724 2009
[50] N Esser S Legrand-Poels J Piette A J Scheen and N PaquotldquoInflammation as a link between obesity metabolic syndromeand type 2 diabetesrdquoDiabetes Research andClinical Practice vol105 no 2 pp 141ndash150 2014
[51] R Hutcheson and P Rocic ldquoThe metabolic syndrome oxida-tive stress environment and cardiovascular disease the greatexplorationrdquo Experimental Diabetes Research vol 2012 ArticleID 271028 13 pages 2012
[52] L Fontana and F B Hu ldquoOptimal body weight for health andlongevity bridging basic clinical and population researchrdquoAging Cell vol 13 no 3 pp 391ndash400 2014
[53] A T Turer and P E Scherer ldquoAdiponectin mechanistic insightsand clinical implicationsrdquo Diabetologia vol 55 no 9 pp 2319ndash2326 2012
[54] WHO ldquoObesity and overweightrdquo Fact sheet No 311 2015[55] P W Gold ldquoThe organization of the stress system and its
dysregulation in depressive illnessrdquo Molecular Psychiatry vol20 no 1 pp 32ndash47 2015
[56] S Purkayastha and D Cai ldquoNeuroinflammatory basis ofmetabolic syndromerdquo Molecular Metabolism vol 2 no 4 pp356ndash363 2013
[57] K Aschbacher A OrsquoDonovan O MWolkowitz F S DhabharY Su and E Epel ldquoGood stress bad stress and oxidative stressinsights from anticipatory cortisol reactivityrdquo Psychoneuroen-docrinology vol 38 no 9 pp 1698ndash1708 2013
[58] C F Sharpley ldquoA review of the neurobiological effects of psy-chotherapy for depressionrdquo Psychotherapy vol 47 no 4 pp603ndash615 2010
[59] M N Silverman and P A Deuster ldquoBiological mechanismsunderlying the role of physical fitness in health and resiliencerdquoInterface Focus vol 4 no 5 Article ID 20140040 2014
[60] G Nefs F Pouwer J Denollet and V Pop ldquoThe course ofdepressive symptoms in primary care patients with type 2 dia-betes results from theDiabetes Depression TypeDPersonalityZuidoost-Brabant (DiaDDZoB) Studyrdquo Diabetologia vol 55no 3 pp 608ndash616 2012
[61] M Pibernik-Okanovic D Begic K Peros S Szabo andZ Metelko ldquoPsychosocial factors contributing to persistent
depressive symptoms in type 2 diabetic patients a Croatiansurvey from the European Depression in Diabetes ResearchConsortiumrdquo Journal of Diabetes and Its Complications vol 22no 4 pp 246ndash253 2008
[62] M Bot F Pouwer J Ormel J P J Slaets and P de Jonge ldquoPre-dictors of incidentmajor depression in diabetic outpatients withsubthreshold depressionrdquo Diabetic Medicine vol 27 no 11 pp1295ndash1301 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 International Journal of Endocrinology
Table 2 Baseline characteristics of participants by the intervention groups (119899 = 209)
Psychoeducation Physical exercise Enhanced treatment as usual Siglowast
119873 74 66 69Age (yrs) 577 (62) 585 (48) 582 (56) 0648Female (119899) 40 37 36 0867Education (yrs) 126 (24) 124 (23) 122 (25) 0623Professional status ( employed) 30 27 30 0502Economic status ( poor) 13 12 13 0317Family status ( marriedcohabitating) 76 72 76 0488Insulin use () 32 29 32 0695OHA use () 56 57 53 0664Insulin + OHA use () 12 14 15 0632Statin use () 68 71 71 0786HbA1c () 74 (12) 72 (11) 72 (11) 0384HbA1c (mmolmol) 58 (13) 56 (13) 55 (11) 0442Body mass index kgm2 3064 (454) 2944 (467) 2996 (439) 0297Depressive symptoms (CES-D score) 197 (91) 205 (86) 197 (87) 0813Data are means (SD) or percentageslowastSig significancelowast One-way ANOVA or 1205942 as appropriateOHA = oral hypoglycemic agents
4 Discussion
This randomized interventional study attempted to evaluatethe effect of two behavioral interventions psychoeducationand physical exercise as compared to enhanced treatmentas usual on depressive symptoms and the intensity ofoxidativeinflammatory processes in diabetic patients suf-fering from subsyndromal depression The results indicateprotracted favorable effects of either intervention on loweringdepressive symptoms while reducing overall oxidative dam-age and cellular inflammatory response as well as improvingantioxidant capacity
In all three study arms a comparable and clinically mean-ingful improvement in depressive symptoms was obtainedThe intervention-independent results regarding depression-related outcomes confirm our preliminary report indicatingthat treatment as usual was equally effective as psychoe-ducation in reducing depressive symptoms and improvingmetabolic control in type 2 diabetic patients with subsyndro-mal depression [30] Also no between-groupdifferenceswerefound within a randomized controlled comparison of psy-choeducation physical exercise and control arm consistingof brief diabetes reeducation [31]The absence of a significanttreatment effect suggested that patterns of change might besimilar in all treatment groups Hypothetically addressingpatientsrsquo emotional needs and their diabetes-related distresswhich were common in all three approaches may indicate apossible pathway of change Similar findings were obtained ina study by Fisher et al [32] which demonstrated that clinicallyreasonable improvements in emotional symptoms may bestimulated by even minimal behavioral interventions
In this study a significant decrease in overall oxidativedamage was observed from basal to one-year posttreatmentfollow-up by measuring a recognized biomarker of oxidativedamage to DNAmdashurinary 8-oxodG Urinary excretion of
8-oxodG reflects the average rate of nucleic acid guanineoxidation and can be regarded as a reliable marker of generalintracellular oxidative stress [33] Research on the u-8-oxodGin diabetes revealed its significant association with severehyperglycemia poor diabetes control and severity of dia-betic complications as well as predictive value for diabetes-associated morbidity [34] The relationship between u-8-oxodG and depression has been modestly investigated andprovided controversial results from an increase to no changedepending on the study-specific depression phenotype [35ndash37] To our knowledge this is the first study investigating u-8-oxodG in patients with diabetes and elevated depressivesymptoms While the results in our exercise group are inaccord with previously reported reduction in u-8-oxodGelicited bymoderate-intensity exercise in type 2 diabetes over12 months [38] significant decrease in u-8-oxodG levels inpsychoeducation and diabetes reeducation group is a novelfinding indicating that cognitive-behavioral approach mighthave beneficial effects on oxidative damage reduction indiabetic patients with subsyndromal depression Additionalsupport for this finding was a significant increase in serumuric acid level at follow-up
Uric acid is an end-product of purine metabolism withcomplex and multifarious roles in human physiology Apartfrom causing gout hyperuricemia has been identified as arisk factor for metabolic syndrome type 2 diabetes andcardiovascular diseases [39] Recently proposed intriguinghypothesis linking hyperuricemia derived by an increasedconsumption of dietary fructose with an epidemic of car-diometabolic diseases attracted a lot of attention and createda paradigm of uric acid as being an exclusively harmfulmetabolite [40] By contrast uric acid has long been recog-nized as one of the most powerful endogenous antioxidants[41] and an efficient mediator of neuroprotection cognitivefunction and intellectual performance [42] as well as the
International Journal of Endocrinology 7
Table 3 One-year changes of depressive symptoms inflammatory- and prooxidative biomarkers
Group scores BaselineM (SD)
12-month follow-upM (SD) Effects 119865 Overall 119875lowast 119875
0 to 12molowastlowast 1205782
Depressive symptomsA (119899 = 64) 197 (91) 167 (79) Time 1251 lt0001 0003 007B (119899 = 58) 198 (82) 181 (98) Time times group 061 0656 0007C (119899 = 57) 190 (86) 174 (94)
Leukocytes (times109L)A (119899 = 63) 75 (17) 73 (17) Time 1261 lt0001 lt0001 007B (119899 = 58) 75 (16) 71 (15) Time times group 132 0265 0001C (119899 = 57) 78 (22) 71 (20)
CRP (mgL)
A (119899 = 64) 028 (049) 025 (044) Time 238 009 100 001B (119899 = 57) 034 (046) 032 (041) Time times group 087 048 001C (119899 = 57) 035 (041) 024 (039)
Sialic acid (mmolL)A (119899 = 64) 21 (031) 19 (029) Time 8457 lt0001 lt0001 032B (119899 = 58) 21 (031) 18 (022) Time times group 340 001 004C (119899 = 57) 21 (028) 18 (024)
u-8-OxodG (120583gmmol)A (119899 = 64) 11 (05) 09 (04) Time 1066 lt0001 lt0001 006B (119899 = 57) 14 (08) 11 (06) Time times group 109 036 001C (119899 = 57) 12 (07) 10 (04)
Uric acid (120583molL)A (119899 = 64) 2917 (852) 3103 (775) Time 1339 lt0001 lt0001 007B (119899 = 58) 3034 (919) 3232 (931) Time times group 025 091 0003C (119899 = 57) 2904 (779) 3145 (834)
HbA1c ()A (119899 = 64) 74 (13) 72 (09) Time 270 007 008 002B (119899 = 58) 72 (10) 72 (10) Time times group 092 045 001C (119899 = 57) 71 (10) 70 (10)
HbA1c (mmolL)A (119899 = 64) 578 (136) 559 (102) Time 331 005 100 002B (119899 = 58) 548 (114) 557 (107) Time times group 090 045 001C (119899 = 57) 548 (107) 539 (100)
Adiponectin (mgL)A (119899 = 63) 75 (23) 71 (38) Time 073 044 100 0004B (119899 = 58) 91 (61) 90 (67) Time times group 055 065 0006C (119899 = 57) 80 (50) 81 (53)
Body mass index (kgm2)A (119899 = 54) 306 (47) 306 (50) Time 172 019 011 001B (119899 = 53) 292 (45) 290 (46) Time times group 131 027 001C (119899 = 52) 301 (41) 294 (40)
lowastTwo-sided significance of differences across time and between the groups (repeated measures ANOVA)lowastlowastTwo-sided significance of differences between baseline and 12-month assessmentsLog-transformed data
8 International Journal of Endocrinology
most pronounced determinant of total plasma antioxidantcapacity in diabetic patients [43] Thus maintaining uricacid levels within physiological range appears to be morefavorable than radical lowering in prevention of variousmor-bidities Based on recent epidemiological evidence includingcardiometabolic risk assessment a new gender-independentupper limit of reference range for uric acid has been proposedat the level of 360 120583molL [44] The present study revealsa significant increase in uric acid levels at follow-up butwell below proposed cut-off above which negative effectsof hyperuricemia might be expected On the contrary theobserved uric acid increase in our study is rather suggestiveof an improved antioxidant capacity elicited by behavioralinterventions in type 2 diabetic patients with subsyndromaldepression
Beneficial effect of cognitive-behavioral interventionin reducing oxidative stress and inflammatory responsehas been reported in hemodialysis patients suffering frominsomnia [45] but rather sparse depression-related studiesmainly focused on the assessment of low-grade inflammationbiomarkers In a very recent randomized trial evaluating anewly developed cognitive-behavioral program (DIAMOS)in diabetic patients with subsyndromal depression a set ofpro- and anti-inflammatory biomarkers was analyzed at basaland one-year follow-up [20] No change in hs-CRP IL-1 andadiponectin was observed whereas a significant decrease ininterleukin-1 receptor antagonist (IL-1RA) was interpreted asan indirect index of alleviated IL-1-related damaging mech-anisms presumably involved in the pathogenesis of micro-and macrovascular complications of diabetes Likewise ourstudy could not demonstrate any influence of the behavioralinterventions on hs-CRP and adiponectin but we foundother inflammatory markers that is leukocyte count andtotal serum sialic acid (TSA) significantly reduced with thelatter being largely affected (1205782 = 032) by the interventionsperformed
Sialic acids comprise a family of heterogenous monosac-charides abundantly present on the cell membranes withcomplex and multiple biological roles in cellular signalingand immunity [46] TSA is a validated inflammatory andatherogenic marker that has been proposed as a novelbiomarker of cardiovascular disease [47] Elevated levels ofTSA in newly diagnosed type 2 diabetic patients have beenlinked to the risk for later development of macrovascularcomplications [28] Interestingly TSA has been identified asa superior predictive biomarker of metabolic syndrome overthe abundantly used hs-CRP [48] Nevertheless despite theobvious advantages TSA has been largely underutilized inthe research on combined inflammatory-metabolic patholo-gies and it has not been studied in depression until this studyOur results identify TSA as a sensitive biomarker of inflam-mation degree in subsyndromally depressed diabetic patientswhereas neither of the established biomarkers of low-gradeinflammation hs-CRP and adiponectin was able to reflectthe anti-inflammatory effect of the performed interventionsSignificant decrease in leukocyte count however clearlyconfirmed postintervention attenuation of the cell-mediatedinflammation response in our patients with an importantnotice that the presence of acute infection at the assessments
was excluded by total leukocyte count lt 100 times 109L or hs-CRP lt 50 gL
The ability of psychological intervention to reduceboth depressive symptoms and inflammation has been evi-denced in depressed breast-cancer patients [49] Further-more due to the insightful study-design Thornton et alwere able to demonstrate a bidirectional mechanistic rela-tionship between depressive symptoms and inflammationThe paradigmatic view of the low-grade inflammation asthe inflicting mechanism for depression has been at leastcomplemented if not refuted by their finding on the mecha-nistic role of depressive symptoms lowering in the reductionof inflammatory response [49] This explanatory mecha-nism might also be translated to our results particularlyconsidering a lack of any effect of interventions towardshyperglycemia and obesity in our study
It is well known that the intensity of oxidative damage andinflammation in diabetes is remarkably and positively asso-ciated with the severity of hyperglycemia [18] Howeverthe observed reduction in oxidative damage and low-gradeinflammation in our study could not be attributed to thismechanism since no significant changes from baseline tofollow-up were found in HbA1c clinically considered toreflect a fair glucoregulation (Table 3) Obesity-derived low-grade inflammation is another recognized harmful compo-nent in the pathogenesis of type 2 diabetes and its compli-cations [50] Obesity induces a disbalance between pro- andanti-inflammatory cytokinesadipokines resulting in low-grade inflammation and related adverse health outcomesranging from metabolic syndrome and diabetes to cardio-vascular diseases and cancer as well as depression [49ndash51]Reduction in bodyweight is accompanied by beneficialmeta-bolic and hormonal profiles and a reduced inflammation [52]with increased production of anti-inflammatory adipokineadiponectin suggested to be among themost relevant features[53] Since our subjects classified as overweightobese [54]retained their BMI at follow-up and revealed no changes inadiponectin levels it is likely that the observed effects ofinterventions on the reduction in depressive symptoms andoxidativeinflammatory biomarkers in this study dependedon another mechanism(s)
Chronic stress with deregulation of stress-response adap-tive mechanisms is considered to be a common feature ofboth diabetes and depression [55] There is a growing bodyof evidence suggesting that metabolic inflammation asso-ciated with obesity and diabetes inflicts neuroinflammationwhich causes serious disturbances of the hypothalamic-pituitary-adrenal (HPA) axis function and consequentlyleads to impairment of adaptive stress-response [56] More-over chronic stress exposure has recently been demonstratedas a promoting factor for accelerated oxidative damagewhereby a sustained activation of HPA-axis emerged again asthe key mediator [57] Neuroendocrine effects of behavioraltreatment for depression have not been extensively studiedbut the evidence so far suggests a hypothetical pathway thatconnects the nurturing effects derived from the patient-ther-apist ldquobondrdquo with reestablishment of neuroendocrine home-ostasis [58] Moreover positive effects of physical exercise onpreventing potentially harmful stress-related metabolic and
International Journal of Endocrinology 9
psychological consequences have been presumably mediatedby the same neuroendocrine mechanisms [59] Consideringunchanged metabolic profile of our subjects and remark-able improvements in depressive symptoms and oxida-tiveinflammatory biomarkers following either behavioralintervention it is tempting if not plausible to speculate onthe involvement of neuroendocrine mechanism(s) in achiev-ing this beneficial response It should be noted that a lackof between-group differences in changes observed in ourstudy might not be explained by a phenomenon known asldquoregression toward the meanrdquo or just a natural course ofparameters Previous findings on persistence of depressivesymptoms in people with type 2 diabetes indicate thatdepression is not only persistent [60 61] but also associatedwith an increased risk of aggravating over time [62] On theother hand oxidative damage toDNA is increasing in healthysubjects throughout time as a result of ageing process [33]while inflammatory response and ageing-associated damageto biomolecules are even more pronounced in diabetes dueto a long-term exposure to hyperglycemia and advanced-glycated end-products [34 50]
The strengths of this study are in examining a highlyprevalent population of type 2 patients with depressive symp-toms but no clinical depression using a randomized com-parative design employing structured behavioral interven-tions and analyzing clinically relevant changes of simple-to-measure oxidativeinflammatory biomarkers Its limitation isthe lack of treatment as usual control intervention precludingthe possibility to investigate the course and outcomes ofsubclinical depression without any treatment Also the studywas carried out in only one centermdasha tertiary diabetesclinicmdashwhich does not allow concluding about its feasibilityin other clinical settings Per-protocol analyses are presentedin the study results which were confirmed by the intention totreat analysis based on baseline-observation-carried-forwardapproach A lack of estimation derived frommultiple predic-tors may be considered a limitation of the study
5 Conclusions
This study has demonstrated that improvement in depressivesymptoms is accompanied with reduced oxidative dam-age and inflammatory response in type 2 diabetic patientswith subsyndromal depression Testing mediating effectshas indicated that medium-term improvement in depres-sive symptoms predicts long-term-reduction in oxidativedamage while mediating factors for observed reductionin inflammatory response should be further investigatedClinical benefits of treating subsyndromal depression wereshown to be comparable in all three treatment arms
Regardless of the mechanisms involved our study clearlyindicates that enhanced treatment as usual defined as briefpatient-centred diabetes reeducation is not inferior to psy-choeducation and exercise in providing beneficial outcomesin subsyndromally depressed type 2 diabetic patients Simplebehavioral interventions are capable not only of alleviatingdepressive symptoms but also of reducing the intensity ofdamaging oxidativeinflammatory processes thereby miti-gating the risk of development of diabetic complications
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The study was funded by the European Foundation forthe Study of Diabetes (EFSD)mdashNew Horizons CollaborativeResearch Initiative 2010 The authors would like to thankLovorka Perkovic Croatian Institute of Public Health forediting the paper
References
[1] S S Ali M A Stone J L Peters M J Davies and K KhuntildquoThe prevalence of co-morbid depression in adults with Type2 diabetes a systematic review and meta-analysisrdquo DiabeticMedicine vol 23 no 11 pp 1165ndash1173 2006
[2] P J Lustman R J Anderson K E Freedland M de Groot RM Carney and R E Clouse ldquoDepression and poor glycemiccontrol a meta-analytic review of the literaturerdquo Diabetes Carevol 23 no 7 pp 934ndash942 2000
[3] L K Richardson L E Egede M Mueller C L Echols and MGebregziabher ldquoLongitudinal effects of depression on glycemiccontrol in veterans with Type 2 diabetesrdquo General HospitalPsychiatry vol 30 no 6 pp 509ndash514 2008
[4] M de Groot R Anderson K E Freedland R E Clouse andP J Lustman ldquoAssociation of depression and diabetes com-plications ameta-analysisrdquo PsychosomaticMedicine vol 63 no4 pp 619ndash630 2001
[5] K Ismail KWinkley D Stahl T Chalder andM Edmonds ldquoAcohort study of people with diabetes and their first foot ulcerthe role of depression on mortalityrdquo Diabetes Care vol 30 no6 pp 1473ndash1479 2007
[6] X Zhang S L Norris E W Gregg Y J Cheng G Becklesand H S Kahn ldquoDepressive symptoms and mortality amongpersons with and without diabetesrdquo American Journal of Epi-demiology vol 161 no 7 pp 652ndash660 2005
[7] S A Black K S Markides and L A Ray ldquoDepression pre-dicts increased incidence of adverse health outcomes in olderMexican Americans with type 2 diabetesrdquo Diabetes Care vol26 no 10 pp 2822ndash2828 2003
[8] H Baumeister N Hutter and J Bengel ldquoPsychological andpharmacological interventions for depression in patients withdiabetesmellitus and depressionrdquoCochraneDatabase of System-atic Reviews vol 12 Article ID CD008381 2012
[9] E Harkness W Macdonald J Valderas P Coventry L Gaskand P Bower ldquoIdentifying psychosocial interventions thatimprove both physical and mental health in patients with dia-betes a systematic review and meta-analysisrdquo Diabetes Carevol 33 no 4 pp 926ndash930 2010
[10] M Berk L J Williams F N Jacka et al ldquoSo depression is aninflammatory disease but where does the inflammation comefromrdquo BMCMedicine vol 11 article 200 2013
[11] S de Kort D Keszthelyi and A A M Masclee ldquoLeaky gut anddiabetes mellitus what is the linkrdquoObesity Reviews vol 12 no6 pp 449ndash458 2011
[12] E T de Lemos J Oliveira J P Pinheiro and F Reis ldquoRegularphysical exercise as a strategy to improve antioxidant andanti-inflammatory status benefits in type 2 diabetes mellitusrdquo
10 International Journal of Endocrinology
Oxidative Medicine and Cellular Longevity vol 2012 Article ID741545 15 pages 2012
[13] T A Doyle M de Groot T Harris et al ldquoDiabetes depressivesymptoms and inflammation in older adults results fromthe Health Aging and Body Composition Studyrdquo Journal ofPsychosomatic Research vol 75 no 5 pp 419ndash424 2013
[14] J-P S Laake D Stahl S A Amiel et al ldquoThe associationbetween depressive symptoms and systemic inflammation inpeople with type 2 diabetes findings from the South Londondiabetes studyrdquoDiabetes Care vol 37 no 8 pp 2186ndash2192 2014
[15] N Rohleder ldquoStimulation of systemic low-grade inflammationby psychosocial stressrdquo Psychosomatic Medicine vol 76 no 3pp 181ndash189 2014
[16] M Maes ldquoAn intriguing and hitherto unexplained co-occur-rence depression and chronic fatigue syndrome are mani-festations of shared inflammatory oxidative and nitrosative(IOampNS) pathwaysrdquo Progress in Neuro-Psychopharmacologyand Biological Psychiatry vol 35 no 3 pp 784ndash794 2011
[17] P Palta L J Samuel E RMiller and S L Szanton ldquoDepressionand oxidative stress results from a meta-analysis of observa-tional studiesrdquo Psychosomatic Medicine vol 76 no 1 pp 12ndash192014
[18] L Rochette M Zeller Y Cottin and C Vergely ldquoDiabetes oxi-dative stress and therapeutic strategiesrdquo Biochimica et Biophys-ica Acta vol 1840 no 9 pp 2709ndash2729 2014
[19] S Keri C Szabo and O Kelemen ldquoExpression of Toll-LikeReceptors in peripheral blood mononuclear cells and responseto cognitive-behavioral therapy in major depressive disorderrdquoBrain Behavior and Immunity vol 40 pp 235ndash243 2014
[20] N Hermanns A Schmitt A Gahr et al ldquoThe effect ofa Diabetes-Specific Cognitive Behavioral Treatment Program(DIAMOS) for patients with diabetes and subclinical depres-sion results of a randomized controlled trialrdquo Diabetes Carevol 38 no 4 pp 551ndash560 2015
[21] K Kroenke R L Spitzer and J B W Williams ldquoThe patienthealth questionnaire-2 validity of a two-item depressionscreenerrdquoMedical Care vol 41 no 11 pp 1284ndash1292 2003
[22] J H Abramson ldquoWINPEPI updated computer programs forepidemiologists and their teaching potentialrdquo EpidemiologicPerspectives amp Innovations vol 8 no 1 article 1 2011
[23] J Cohen ldquoA power primerrdquo Psychological Bulletin vol 112 no1 pp 155ndash159 1992
[24] M Pibernik-Okanovic D Ajdukovic M V Lovrencic andN Hermanns ldquoDoes treatment of subsyndromal depressionimprove depression and diabetes related outcomes protocolfor a randomised controlled comparison of psycho-educationphysical exercise and treatment as usualrdquo Trials vol 12 article17 2011
[25] BArroll FGoodyear-SmithNKerse T Fishman and JGunnldquoEffect of the addition of a lsquohelprsquo question to two screeningquestions on specificity for diagnosis of depression in generalpractice diagnostic validity studyrdquo British Medical Journal vol331 no 7521 article 884 2005
[26] P Rohde P M Lewinsohn and J R Seeley ldquoComparability oftelephone and face-to-face interviews in assessing axis I and IIdisordersrdquo American Journal of Psychiatry vol 154 no 11 pp1593ndash1598 1997
[27] L S Radloff ldquoTheCES-D scalerdquoApplied Psychological Measure-ment vol 1 pp 385ndash401 1977
[28] M Gavella V Lipovac A Car M Vucic L Sokolic and RRakos ldquoSerum sialic acid in subjects with impaired glucose
tolerance and in newly diagnosed type 2 diabetic patientsrdquoActaDiabetologica vol 40 no 2 pp 95ndash100 2003
[29] M D Evans R Singh V Mistry K Sandhu P B Farmer andM S Cooke ldquoAnalysis of urinary 8-oxo-78-dihydro-purine-21015840- deoxyribonucleosides by LC-MSMS and improved ELISArdquoFree Radical Research vol 42 no 10 pp 831ndash840 2008
[30] M Pibernik-Okanovic D Begic D Ajdukovic N Andrijasevicand Z Metelko ldquoPsychoeducation versus treatment as usualin diabetic patients with subthreshold depression preliminaryresults of a randomized controlled trialrdquo Trials vol 10 article78 2009
[31] M Pibernik-Okanovic M Vucic Lovrencic D AjdukovicM Sekerija and N Hermanns ldquoPsychological behavioraland biological changes following treatments of subsyndromaldepression in people with type 2 diabetesrdquoDiabetologia vol 56supplement 1 p S465 2013
[32] L Fisher D Hessler R E Glasgow et al ldquoREDEEM a prag-matic trial to reduce diabetes distressrdquo Diabetes Care vol 36no 9 pp 2551ndash2558 2013
[33] H E Poulsen L L Nadal K Broedbaek P E Nielsen andA Weimann ldquoDetection and interpretation of 8-oxodG and 8-oxoGua in urine plasma and cerebrospinal fluidrdquo Biochimica etBiophysica ActamdashGeneral Subjects vol 1840 no 2 pp 801ndash8082014
[34] K Broedbaek A Weimann E S Stovgaard and H E PoulsenldquoUrinary 8-oxo-78-dihydro-21015840-deoxyguanosine as a biomarkerin type 2 diabetesrdquo Free Radical Biology and Medicine vol 51no 8 pp 1473ndash1479 2011
[35] M J Forlenza and G E Miller ldquoIncreased serum levels of 8-hydroxy-21015840-deoxyguanosine in clinical depressionrdquo Psychoso-matic Medicine vol 68 no 1 pp 1ndash7 2006
[36] A Jorgensen J Krogh K Miskowiak et al ldquoSystemic oxida-tively generatedDNARNAdamage in clinical depression asso-ciations to symptom severity and response to electroconvulsivetherapyrdquo Journal of Affective Disorders vol 149 no 1ndash3 pp 355ndash362 2013
[37] S Yi ANanri YMatsushitaHKasai K Kawai andTMizoueldquoDepressive symptoms and oxidative DNA damage in Japanesemunicipal employeesrdquo Psychiatry Research vol 200 no 2-3 pp318ndash322 2012
[38] H Nojima H Watanabe K Yamane et al ldquoEffect of aerobicexercise training on oxidative stress in patients with type 2diabetes mellitusrdquo Metabolism Clinical and Experimental vol57 no 2 pp 170ndash176 2008
[39] S Bonakdaran and B Kharaqani ldquoAssociation of serum uricacid and metabolic syndrome in type 2 diabetesrdquo CurrentDiabetes Reviews vol 10 no 2 pp 113ndash117 2014
[40] R J Johnson T Nakagawa L G Sanchez-Lozada et al ldquoSugaruric acid and the etiology of diabetes and obesityrdquoDiabetes vol62 no 10 pp 3307ndash3315 2013
[41] M L Wahlqvist ldquoAntioxidant relevance to human healthrdquo AsiaPacific Journal of Clinical Nutrition vol 22 no 2 pp 171ndash1762013
[42] A De Giorgi F Fabbian M Pala et al ldquoUric acid friend orfoe Uric acid and cognitive function lsquogout kills more wise menthan simplersquordquo European Review forMedical and PharmacologicalSciences vol 19 no 4 pp 640ndash646 2015
[43] M Vucic B Rocic V Bozikov and S J H Ashcroft ldquoPlasmauric acid and total antioxidant status in patients with diabetesmellitusrdquo Hormone and Metabolic Research vol 29 no 7 pp355ndash357 1997
International Journal of Endocrinology 11
[44] G Desideri G Castaldo A Lombardi et al ldquoIs it time to revisethe normal range of serum uric acid levelsrdquo European Reviewfor Medical and Pharmacological Sciences vol 18 no 9 pp1295ndash1306 2014
[45] H-Y Chen I-C Cheng Y-J Pan et al ldquoCognitive-behavioraltherapy for sleep disturbance decreases inflammatory cytokinesand oxidative stress in hemodialysis patientsrdquo Kidney Interna-tional vol 80 no 4 pp 415ndash422 2011
[46] A Varki and P Gagneux ldquoMultifarious roles of sialic acids inimmunityrdquo Annals of the New York Academy of Sciences vol1253 no 1 pp 16ndash36 2012
[47] K P Gopaul and M A Crook ldquoSialic acid a novel marker ofcardiovascular diseaserdquo Clinical Biochemistry vol 39 no 7 pp667ndash681 2006
[48] L M Browning S A Jebb G D Mishra et al ldquoElevated sialicacid but not CRP predicts features of the metabolic syndromeindependently of BMI in womenrdquo International Journal ofObesity vol 28 no 8 pp 1004ndash1010 2004
[49] LMThornton B L Andersen T A Schuler andW E CarsonldquoA psychological intervention reduces inflammatory markersby alleviating depressive symptoms secondary analysis of arandomized controlled trialrdquo Psychosomatic Medicine vol 71no 7 pp 715ndash724 2009
[50] N Esser S Legrand-Poels J Piette A J Scheen and N PaquotldquoInflammation as a link between obesity metabolic syndromeand type 2 diabetesrdquoDiabetes Research andClinical Practice vol105 no 2 pp 141ndash150 2014
[51] R Hutcheson and P Rocic ldquoThe metabolic syndrome oxida-tive stress environment and cardiovascular disease the greatexplorationrdquo Experimental Diabetes Research vol 2012 ArticleID 271028 13 pages 2012
[52] L Fontana and F B Hu ldquoOptimal body weight for health andlongevity bridging basic clinical and population researchrdquoAging Cell vol 13 no 3 pp 391ndash400 2014
[53] A T Turer and P E Scherer ldquoAdiponectin mechanistic insightsand clinical implicationsrdquo Diabetologia vol 55 no 9 pp 2319ndash2326 2012
[54] WHO ldquoObesity and overweightrdquo Fact sheet No 311 2015[55] P W Gold ldquoThe organization of the stress system and its
dysregulation in depressive illnessrdquo Molecular Psychiatry vol20 no 1 pp 32ndash47 2015
[56] S Purkayastha and D Cai ldquoNeuroinflammatory basis ofmetabolic syndromerdquo Molecular Metabolism vol 2 no 4 pp356ndash363 2013
[57] K Aschbacher A OrsquoDonovan O MWolkowitz F S DhabharY Su and E Epel ldquoGood stress bad stress and oxidative stressinsights from anticipatory cortisol reactivityrdquo Psychoneuroen-docrinology vol 38 no 9 pp 1698ndash1708 2013
[58] C F Sharpley ldquoA review of the neurobiological effects of psy-chotherapy for depressionrdquo Psychotherapy vol 47 no 4 pp603ndash615 2010
[59] M N Silverman and P A Deuster ldquoBiological mechanismsunderlying the role of physical fitness in health and resiliencerdquoInterface Focus vol 4 no 5 Article ID 20140040 2014
[60] G Nefs F Pouwer J Denollet and V Pop ldquoThe course ofdepressive symptoms in primary care patients with type 2 dia-betes results from theDiabetes Depression TypeDPersonalityZuidoost-Brabant (DiaDDZoB) Studyrdquo Diabetologia vol 55no 3 pp 608ndash616 2012
[61] M Pibernik-Okanovic D Begic K Peros S Szabo andZ Metelko ldquoPsychosocial factors contributing to persistent
depressive symptoms in type 2 diabetic patients a Croatiansurvey from the European Depression in Diabetes ResearchConsortiumrdquo Journal of Diabetes and Its Complications vol 22no 4 pp 246ndash253 2008
[62] M Bot F Pouwer J Ormel J P J Slaets and P de Jonge ldquoPre-dictors of incidentmajor depression in diabetic outpatients withsubthreshold depressionrdquo Diabetic Medicine vol 27 no 11 pp1295ndash1301 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

International Journal of Endocrinology 7
Table 3 One-year changes of depressive symptoms inflammatory- and prooxidative biomarkers
Group scores BaselineM (SD)
12-month follow-upM (SD) Effects 119865 Overall 119875lowast 119875
0 to 12molowastlowast 1205782
Depressive symptomsA (119899 = 64) 197 (91) 167 (79) Time 1251 lt0001 0003 007B (119899 = 58) 198 (82) 181 (98) Time times group 061 0656 0007C (119899 = 57) 190 (86) 174 (94)
Leukocytes (times109L)A (119899 = 63) 75 (17) 73 (17) Time 1261 lt0001 lt0001 007B (119899 = 58) 75 (16) 71 (15) Time times group 132 0265 0001C (119899 = 57) 78 (22) 71 (20)
CRP (mgL)
A (119899 = 64) 028 (049) 025 (044) Time 238 009 100 001B (119899 = 57) 034 (046) 032 (041) Time times group 087 048 001C (119899 = 57) 035 (041) 024 (039)
Sialic acid (mmolL)A (119899 = 64) 21 (031) 19 (029) Time 8457 lt0001 lt0001 032B (119899 = 58) 21 (031) 18 (022) Time times group 340 001 004C (119899 = 57) 21 (028) 18 (024)
u-8-OxodG (120583gmmol)A (119899 = 64) 11 (05) 09 (04) Time 1066 lt0001 lt0001 006B (119899 = 57) 14 (08) 11 (06) Time times group 109 036 001C (119899 = 57) 12 (07) 10 (04)
Uric acid (120583molL)A (119899 = 64) 2917 (852) 3103 (775) Time 1339 lt0001 lt0001 007B (119899 = 58) 3034 (919) 3232 (931) Time times group 025 091 0003C (119899 = 57) 2904 (779) 3145 (834)
HbA1c ()A (119899 = 64) 74 (13) 72 (09) Time 270 007 008 002B (119899 = 58) 72 (10) 72 (10) Time times group 092 045 001C (119899 = 57) 71 (10) 70 (10)
HbA1c (mmolL)A (119899 = 64) 578 (136) 559 (102) Time 331 005 100 002B (119899 = 58) 548 (114) 557 (107) Time times group 090 045 001C (119899 = 57) 548 (107) 539 (100)
Adiponectin (mgL)A (119899 = 63) 75 (23) 71 (38) Time 073 044 100 0004B (119899 = 58) 91 (61) 90 (67) Time times group 055 065 0006C (119899 = 57) 80 (50) 81 (53)
Body mass index (kgm2)A (119899 = 54) 306 (47) 306 (50) Time 172 019 011 001B (119899 = 53) 292 (45) 290 (46) Time times group 131 027 001C (119899 = 52) 301 (41) 294 (40)
lowastTwo-sided significance of differences across time and between the groups (repeated measures ANOVA)lowastlowastTwo-sided significance of differences between baseline and 12-month assessmentsLog-transformed data
8 International Journal of Endocrinology
most pronounced determinant of total plasma antioxidantcapacity in diabetic patients [43] Thus maintaining uricacid levels within physiological range appears to be morefavorable than radical lowering in prevention of variousmor-bidities Based on recent epidemiological evidence includingcardiometabolic risk assessment a new gender-independentupper limit of reference range for uric acid has been proposedat the level of 360 120583molL [44] The present study revealsa significant increase in uric acid levels at follow-up butwell below proposed cut-off above which negative effectsof hyperuricemia might be expected On the contrary theobserved uric acid increase in our study is rather suggestiveof an improved antioxidant capacity elicited by behavioralinterventions in type 2 diabetic patients with subsyndromaldepression
Beneficial effect of cognitive-behavioral interventionin reducing oxidative stress and inflammatory responsehas been reported in hemodialysis patients suffering frominsomnia [45] but rather sparse depression-related studiesmainly focused on the assessment of low-grade inflammationbiomarkers In a very recent randomized trial evaluating anewly developed cognitive-behavioral program (DIAMOS)in diabetic patients with subsyndromal depression a set ofpro- and anti-inflammatory biomarkers was analyzed at basaland one-year follow-up [20] No change in hs-CRP IL-1 andadiponectin was observed whereas a significant decrease ininterleukin-1 receptor antagonist (IL-1RA) was interpreted asan indirect index of alleviated IL-1-related damaging mech-anisms presumably involved in the pathogenesis of micro-and macrovascular complications of diabetes Likewise ourstudy could not demonstrate any influence of the behavioralinterventions on hs-CRP and adiponectin but we foundother inflammatory markers that is leukocyte count andtotal serum sialic acid (TSA) significantly reduced with thelatter being largely affected (1205782 = 032) by the interventionsperformed
Sialic acids comprise a family of heterogenous monosac-charides abundantly present on the cell membranes withcomplex and multiple biological roles in cellular signalingand immunity [46] TSA is a validated inflammatory andatherogenic marker that has been proposed as a novelbiomarker of cardiovascular disease [47] Elevated levels ofTSA in newly diagnosed type 2 diabetic patients have beenlinked to the risk for later development of macrovascularcomplications [28] Interestingly TSA has been identified asa superior predictive biomarker of metabolic syndrome overthe abundantly used hs-CRP [48] Nevertheless despite theobvious advantages TSA has been largely underutilized inthe research on combined inflammatory-metabolic patholo-gies and it has not been studied in depression until this studyOur results identify TSA as a sensitive biomarker of inflam-mation degree in subsyndromally depressed diabetic patientswhereas neither of the established biomarkers of low-gradeinflammation hs-CRP and adiponectin was able to reflectthe anti-inflammatory effect of the performed interventionsSignificant decrease in leukocyte count however clearlyconfirmed postintervention attenuation of the cell-mediatedinflammation response in our patients with an importantnotice that the presence of acute infection at the assessments
was excluded by total leukocyte count lt 100 times 109L or hs-CRP lt 50 gL
The ability of psychological intervention to reduceboth depressive symptoms and inflammation has been evi-denced in depressed breast-cancer patients [49] Further-more due to the insightful study-design Thornton et alwere able to demonstrate a bidirectional mechanistic rela-tionship between depressive symptoms and inflammationThe paradigmatic view of the low-grade inflammation asthe inflicting mechanism for depression has been at leastcomplemented if not refuted by their finding on the mecha-nistic role of depressive symptoms lowering in the reductionof inflammatory response [49] This explanatory mecha-nism might also be translated to our results particularlyconsidering a lack of any effect of interventions towardshyperglycemia and obesity in our study
It is well known that the intensity of oxidative damage andinflammation in diabetes is remarkably and positively asso-ciated with the severity of hyperglycemia [18] Howeverthe observed reduction in oxidative damage and low-gradeinflammation in our study could not be attributed to thismechanism since no significant changes from baseline tofollow-up were found in HbA1c clinically considered toreflect a fair glucoregulation (Table 3) Obesity-derived low-grade inflammation is another recognized harmful compo-nent in the pathogenesis of type 2 diabetes and its compli-cations [50] Obesity induces a disbalance between pro- andanti-inflammatory cytokinesadipokines resulting in low-grade inflammation and related adverse health outcomesranging from metabolic syndrome and diabetes to cardio-vascular diseases and cancer as well as depression [49ndash51]Reduction in bodyweight is accompanied by beneficialmeta-bolic and hormonal profiles and a reduced inflammation [52]with increased production of anti-inflammatory adipokineadiponectin suggested to be among themost relevant features[53] Since our subjects classified as overweightobese [54]retained their BMI at follow-up and revealed no changes inadiponectin levels it is likely that the observed effects ofinterventions on the reduction in depressive symptoms andoxidativeinflammatory biomarkers in this study dependedon another mechanism(s)
Chronic stress with deregulation of stress-response adap-tive mechanisms is considered to be a common feature ofboth diabetes and depression [55] There is a growing bodyof evidence suggesting that metabolic inflammation asso-ciated with obesity and diabetes inflicts neuroinflammationwhich causes serious disturbances of the hypothalamic-pituitary-adrenal (HPA) axis function and consequentlyleads to impairment of adaptive stress-response [56] More-over chronic stress exposure has recently been demonstratedas a promoting factor for accelerated oxidative damagewhereby a sustained activation of HPA-axis emerged again asthe key mediator [57] Neuroendocrine effects of behavioraltreatment for depression have not been extensively studiedbut the evidence so far suggests a hypothetical pathway thatconnects the nurturing effects derived from the patient-ther-apist ldquobondrdquo with reestablishment of neuroendocrine home-ostasis [58] Moreover positive effects of physical exercise onpreventing potentially harmful stress-related metabolic and
International Journal of Endocrinology 9
psychological consequences have been presumably mediatedby the same neuroendocrine mechanisms [59] Consideringunchanged metabolic profile of our subjects and remark-able improvements in depressive symptoms and oxida-tiveinflammatory biomarkers following either behavioralintervention it is tempting if not plausible to speculate onthe involvement of neuroendocrine mechanism(s) in achiev-ing this beneficial response It should be noted that a lackof between-group differences in changes observed in ourstudy might not be explained by a phenomenon known asldquoregression toward the meanrdquo or just a natural course ofparameters Previous findings on persistence of depressivesymptoms in people with type 2 diabetes indicate thatdepression is not only persistent [60 61] but also associatedwith an increased risk of aggravating over time [62] On theother hand oxidative damage toDNA is increasing in healthysubjects throughout time as a result of ageing process [33]while inflammatory response and ageing-associated damageto biomolecules are even more pronounced in diabetes dueto a long-term exposure to hyperglycemia and advanced-glycated end-products [34 50]
The strengths of this study are in examining a highlyprevalent population of type 2 patients with depressive symp-toms but no clinical depression using a randomized com-parative design employing structured behavioral interven-tions and analyzing clinically relevant changes of simple-to-measure oxidativeinflammatory biomarkers Its limitation isthe lack of treatment as usual control intervention precludingthe possibility to investigate the course and outcomes ofsubclinical depression without any treatment Also the studywas carried out in only one centermdasha tertiary diabetesclinicmdashwhich does not allow concluding about its feasibilityin other clinical settings Per-protocol analyses are presentedin the study results which were confirmed by the intention totreat analysis based on baseline-observation-carried-forwardapproach A lack of estimation derived frommultiple predic-tors may be considered a limitation of the study
5 Conclusions
This study has demonstrated that improvement in depressivesymptoms is accompanied with reduced oxidative dam-age and inflammatory response in type 2 diabetic patientswith subsyndromal depression Testing mediating effectshas indicated that medium-term improvement in depres-sive symptoms predicts long-term-reduction in oxidativedamage while mediating factors for observed reductionin inflammatory response should be further investigatedClinical benefits of treating subsyndromal depression wereshown to be comparable in all three treatment arms
Regardless of the mechanisms involved our study clearlyindicates that enhanced treatment as usual defined as briefpatient-centred diabetes reeducation is not inferior to psy-choeducation and exercise in providing beneficial outcomesin subsyndromally depressed type 2 diabetic patients Simplebehavioral interventions are capable not only of alleviatingdepressive symptoms but also of reducing the intensity ofdamaging oxidativeinflammatory processes thereby miti-gating the risk of development of diabetic complications
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The study was funded by the European Foundation forthe Study of Diabetes (EFSD)mdashNew Horizons CollaborativeResearch Initiative 2010 The authors would like to thankLovorka Perkovic Croatian Institute of Public Health forediting the paper
References
[1] S S Ali M A Stone J L Peters M J Davies and K KhuntildquoThe prevalence of co-morbid depression in adults with Type2 diabetes a systematic review and meta-analysisrdquo DiabeticMedicine vol 23 no 11 pp 1165ndash1173 2006
[2] P J Lustman R J Anderson K E Freedland M de Groot RM Carney and R E Clouse ldquoDepression and poor glycemiccontrol a meta-analytic review of the literaturerdquo Diabetes Carevol 23 no 7 pp 934ndash942 2000
[3] L K Richardson L E Egede M Mueller C L Echols and MGebregziabher ldquoLongitudinal effects of depression on glycemiccontrol in veterans with Type 2 diabetesrdquo General HospitalPsychiatry vol 30 no 6 pp 509ndash514 2008
[4] M de Groot R Anderson K E Freedland R E Clouse andP J Lustman ldquoAssociation of depression and diabetes com-plications ameta-analysisrdquo PsychosomaticMedicine vol 63 no4 pp 619ndash630 2001
[5] K Ismail KWinkley D Stahl T Chalder andM Edmonds ldquoAcohort study of people with diabetes and their first foot ulcerthe role of depression on mortalityrdquo Diabetes Care vol 30 no6 pp 1473ndash1479 2007
[6] X Zhang S L Norris E W Gregg Y J Cheng G Becklesand H S Kahn ldquoDepressive symptoms and mortality amongpersons with and without diabetesrdquo American Journal of Epi-demiology vol 161 no 7 pp 652ndash660 2005
[7] S A Black K S Markides and L A Ray ldquoDepression pre-dicts increased incidence of adverse health outcomes in olderMexican Americans with type 2 diabetesrdquo Diabetes Care vol26 no 10 pp 2822ndash2828 2003
[8] H Baumeister N Hutter and J Bengel ldquoPsychological andpharmacological interventions for depression in patients withdiabetesmellitus and depressionrdquoCochraneDatabase of System-atic Reviews vol 12 Article ID CD008381 2012
[9] E Harkness W Macdonald J Valderas P Coventry L Gaskand P Bower ldquoIdentifying psychosocial interventions thatimprove both physical and mental health in patients with dia-betes a systematic review and meta-analysisrdquo Diabetes Carevol 33 no 4 pp 926ndash930 2010
[10] M Berk L J Williams F N Jacka et al ldquoSo depression is aninflammatory disease but where does the inflammation comefromrdquo BMCMedicine vol 11 article 200 2013
[11] S de Kort D Keszthelyi and A A M Masclee ldquoLeaky gut anddiabetes mellitus what is the linkrdquoObesity Reviews vol 12 no6 pp 449ndash458 2011
[12] E T de Lemos J Oliveira J P Pinheiro and F Reis ldquoRegularphysical exercise as a strategy to improve antioxidant andanti-inflammatory status benefits in type 2 diabetes mellitusrdquo
10 International Journal of Endocrinology
Oxidative Medicine and Cellular Longevity vol 2012 Article ID741545 15 pages 2012
[13] T A Doyle M de Groot T Harris et al ldquoDiabetes depressivesymptoms and inflammation in older adults results fromthe Health Aging and Body Composition Studyrdquo Journal ofPsychosomatic Research vol 75 no 5 pp 419ndash424 2013
[14] J-P S Laake D Stahl S A Amiel et al ldquoThe associationbetween depressive symptoms and systemic inflammation inpeople with type 2 diabetes findings from the South Londondiabetes studyrdquoDiabetes Care vol 37 no 8 pp 2186ndash2192 2014
[15] N Rohleder ldquoStimulation of systemic low-grade inflammationby psychosocial stressrdquo Psychosomatic Medicine vol 76 no 3pp 181ndash189 2014
[16] M Maes ldquoAn intriguing and hitherto unexplained co-occur-rence depression and chronic fatigue syndrome are mani-festations of shared inflammatory oxidative and nitrosative(IOampNS) pathwaysrdquo Progress in Neuro-Psychopharmacologyand Biological Psychiatry vol 35 no 3 pp 784ndash794 2011
[17] P Palta L J Samuel E RMiller and S L Szanton ldquoDepressionand oxidative stress results from a meta-analysis of observa-tional studiesrdquo Psychosomatic Medicine vol 76 no 1 pp 12ndash192014
[18] L Rochette M Zeller Y Cottin and C Vergely ldquoDiabetes oxi-dative stress and therapeutic strategiesrdquo Biochimica et Biophys-ica Acta vol 1840 no 9 pp 2709ndash2729 2014
[19] S Keri C Szabo and O Kelemen ldquoExpression of Toll-LikeReceptors in peripheral blood mononuclear cells and responseto cognitive-behavioral therapy in major depressive disorderrdquoBrain Behavior and Immunity vol 40 pp 235ndash243 2014
[20] N Hermanns A Schmitt A Gahr et al ldquoThe effect ofa Diabetes-Specific Cognitive Behavioral Treatment Program(DIAMOS) for patients with diabetes and subclinical depres-sion results of a randomized controlled trialrdquo Diabetes Carevol 38 no 4 pp 551ndash560 2015
[21] K Kroenke R L Spitzer and J B W Williams ldquoThe patienthealth questionnaire-2 validity of a two-item depressionscreenerrdquoMedical Care vol 41 no 11 pp 1284ndash1292 2003
[22] J H Abramson ldquoWINPEPI updated computer programs forepidemiologists and their teaching potentialrdquo EpidemiologicPerspectives amp Innovations vol 8 no 1 article 1 2011
[23] J Cohen ldquoA power primerrdquo Psychological Bulletin vol 112 no1 pp 155ndash159 1992
[24] M Pibernik-Okanovic D Ajdukovic M V Lovrencic andN Hermanns ldquoDoes treatment of subsyndromal depressionimprove depression and diabetes related outcomes protocolfor a randomised controlled comparison of psycho-educationphysical exercise and treatment as usualrdquo Trials vol 12 article17 2011
[25] BArroll FGoodyear-SmithNKerse T Fishman and JGunnldquoEffect of the addition of a lsquohelprsquo question to two screeningquestions on specificity for diagnosis of depression in generalpractice diagnostic validity studyrdquo British Medical Journal vol331 no 7521 article 884 2005
[26] P Rohde P M Lewinsohn and J R Seeley ldquoComparability oftelephone and face-to-face interviews in assessing axis I and IIdisordersrdquo American Journal of Psychiatry vol 154 no 11 pp1593ndash1598 1997
[27] L S Radloff ldquoTheCES-D scalerdquoApplied Psychological Measure-ment vol 1 pp 385ndash401 1977
[28] M Gavella V Lipovac A Car M Vucic L Sokolic and RRakos ldquoSerum sialic acid in subjects with impaired glucose
tolerance and in newly diagnosed type 2 diabetic patientsrdquoActaDiabetologica vol 40 no 2 pp 95ndash100 2003
[29] M D Evans R Singh V Mistry K Sandhu P B Farmer andM S Cooke ldquoAnalysis of urinary 8-oxo-78-dihydro-purine-21015840- deoxyribonucleosides by LC-MSMS and improved ELISArdquoFree Radical Research vol 42 no 10 pp 831ndash840 2008
[30] M Pibernik-Okanovic D Begic D Ajdukovic N Andrijasevicand Z Metelko ldquoPsychoeducation versus treatment as usualin diabetic patients with subthreshold depression preliminaryresults of a randomized controlled trialrdquo Trials vol 10 article78 2009
[31] M Pibernik-Okanovic M Vucic Lovrencic D AjdukovicM Sekerija and N Hermanns ldquoPsychological behavioraland biological changes following treatments of subsyndromaldepression in people with type 2 diabetesrdquoDiabetologia vol 56supplement 1 p S465 2013
[32] L Fisher D Hessler R E Glasgow et al ldquoREDEEM a prag-matic trial to reduce diabetes distressrdquo Diabetes Care vol 36no 9 pp 2551ndash2558 2013
[33] H E Poulsen L L Nadal K Broedbaek P E Nielsen andA Weimann ldquoDetection and interpretation of 8-oxodG and 8-oxoGua in urine plasma and cerebrospinal fluidrdquo Biochimica etBiophysica ActamdashGeneral Subjects vol 1840 no 2 pp 801ndash8082014
[34] K Broedbaek A Weimann E S Stovgaard and H E PoulsenldquoUrinary 8-oxo-78-dihydro-21015840-deoxyguanosine as a biomarkerin type 2 diabetesrdquo Free Radical Biology and Medicine vol 51no 8 pp 1473ndash1479 2011
[35] M J Forlenza and G E Miller ldquoIncreased serum levels of 8-hydroxy-21015840-deoxyguanosine in clinical depressionrdquo Psychoso-matic Medicine vol 68 no 1 pp 1ndash7 2006
[36] A Jorgensen J Krogh K Miskowiak et al ldquoSystemic oxida-tively generatedDNARNAdamage in clinical depression asso-ciations to symptom severity and response to electroconvulsivetherapyrdquo Journal of Affective Disorders vol 149 no 1ndash3 pp 355ndash362 2013
[37] S Yi ANanri YMatsushitaHKasai K Kawai andTMizoueldquoDepressive symptoms and oxidative DNA damage in Japanesemunicipal employeesrdquo Psychiatry Research vol 200 no 2-3 pp318ndash322 2012
[38] H Nojima H Watanabe K Yamane et al ldquoEffect of aerobicexercise training on oxidative stress in patients with type 2diabetes mellitusrdquo Metabolism Clinical and Experimental vol57 no 2 pp 170ndash176 2008
[39] S Bonakdaran and B Kharaqani ldquoAssociation of serum uricacid and metabolic syndrome in type 2 diabetesrdquo CurrentDiabetes Reviews vol 10 no 2 pp 113ndash117 2014
[40] R J Johnson T Nakagawa L G Sanchez-Lozada et al ldquoSugaruric acid and the etiology of diabetes and obesityrdquoDiabetes vol62 no 10 pp 3307ndash3315 2013
[41] M L Wahlqvist ldquoAntioxidant relevance to human healthrdquo AsiaPacific Journal of Clinical Nutrition vol 22 no 2 pp 171ndash1762013
[42] A De Giorgi F Fabbian M Pala et al ldquoUric acid friend orfoe Uric acid and cognitive function lsquogout kills more wise menthan simplersquordquo European Review forMedical and PharmacologicalSciences vol 19 no 4 pp 640ndash646 2015
[43] M Vucic B Rocic V Bozikov and S J H Ashcroft ldquoPlasmauric acid and total antioxidant status in patients with diabetesmellitusrdquo Hormone and Metabolic Research vol 29 no 7 pp355ndash357 1997
International Journal of Endocrinology 11
[44] G Desideri G Castaldo A Lombardi et al ldquoIs it time to revisethe normal range of serum uric acid levelsrdquo European Reviewfor Medical and Pharmacological Sciences vol 18 no 9 pp1295ndash1306 2014
[45] H-Y Chen I-C Cheng Y-J Pan et al ldquoCognitive-behavioraltherapy for sleep disturbance decreases inflammatory cytokinesand oxidative stress in hemodialysis patientsrdquo Kidney Interna-tional vol 80 no 4 pp 415ndash422 2011
[46] A Varki and P Gagneux ldquoMultifarious roles of sialic acids inimmunityrdquo Annals of the New York Academy of Sciences vol1253 no 1 pp 16ndash36 2012
[47] K P Gopaul and M A Crook ldquoSialic acid a novel marker ofcardiovascular diseaserdquo Clinical Biochemistry vol 39 no 7 pp667ndash681 2006
[48] L M Browning S A Jebb G D Mishra et al ldquoElevated sialicacid but not CRP predicts features of the metabolic syndromeindependently of BMI in womenrdquo International Journal ofObesity vol 28 no 8 pp 1004ndash1010 2004
[49] LMThornton B L Andersen T A Schuler andW E CarsonldquoA psychological intervention reduces inflammatory markersby alleviating depressive symptoms secondary analysis of arandomized controlled trialrdquo Psychosomatic Medicine vol 71no 7 pp 715ndash724 2009
[50] N Esser S Legrand-Poels J Piette A J Scheen and N PaquotldquoInflammation as a link between obesity metabolic syndromeand type 2 diabetesrdquoDiabetes Research andClinical Practice vol105 no 2 pp 141ndash150 2014
[51] R Hutcheson and P Rocic ldquoThe metabolic syndrome oxida-tive stress environment and cardiovascular disease the greatexplorationrdquo Experimental Diabetes Research vol 2012 ArticleID 271028 13 pages 2012
[52] L Fontana and F B Hu ldquoOptimal body weight for health andlongevity bridging basic clinical and population researchrdquoAging Cell vol 13 no 3 pp 391ndash400 2014
[53] A T Turer and P E Scherer ldquoAdiponectin mechanistic insightsand clinical implicationsrdquo Diabetologia vol 55 no 9 pp 2319ndash2326 2012
[54] WHO ldquoObesity and overweightrdquo Fact sheet No 311 2015[55] P W Gold ldquoThe organization of the stress system and its
dysregulation in depressive illnessrdquo Molecular Psychiatry vol20 no 1 pp 32ndash47 2015
[56] S Purkayastha and D Cai ldquoNeuroinflammatory basis ofmetabolic syndromerdquo Molecular Metabolism vol 2 no 4 pp356ndash363 2013
[57] K Aschbacher A OrsquoDonovan O MWolkowitz F S DhabharY Su and E Epel ldquoGood stress bad stress and oxidative stressinsights from anticipatory cortisol reactivityrdquo Psychoneuroen-docrinology vol 38 no 9 pp 1698ndash1708 2013
[58] C F Sharpley ldquoA review of the neurobiological effects of psy-chotherapy for depressionrdquo Psychotherapy vol 47 no 4 pp603ndash615 2010
[59] M N Silverman and P A Deuster ldquoBiological mechanismsunderlying the role of physical fitness in health and resiliencerdquoInterface Focus vol 4 no 5 Article ID 20140040 2014
[60] G Nefs F Pouwer J Denollet and V Pop ldquoThe course ofdepressive symptoms in primary care patients with type 2 dia-betes results from theDiabetes Depression TypeDPersonalityZuidoost-Brabant (DiaDDZoB) Studyrdquo Diabetologia vol 55no 3 pp 608ndash616 2012
[61] M Pibernik-Okanovic D Begic K Peros S Szabo andZ Metelko ldquoPsychosocial factors contributing to persistent
depressive symptoms in type 2 diabetic patients a Croatiansurvey from the European Depression in Diabetes ResearchConsortiumrdquo Journal of Diabetes and Its Complications vol 22no 4 pp 246ndash253 2008
[62] M Bot F Pouwer J Ormel J P J Slaets and P de Jonge ldquoPre-dictors of incidentmajor depression in diabetic outpatients withsubthreshold depressionrdquo Diabetic Medicine vol 27 no 11 pp1295ndash1301 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

8 International Journal of Endocrinology
most pronounced determinant of total plasma antioxidantcapacity in diabetic patients [43] Thus maintaining uricacid levels within physiological range appears to be morefavorable than radical lowering in prevention of variousmor-bidities Based on recent epidemiological evidence includingcardiometabolic risk assessment a new gender-independentupper limit of reference range for uric acid has been proposedat the level of 360 120583molL [44] The present study revealsa significant increase in uric acid levels at follow-up butwell below proposed cut-off above which negative effectsof hyperuricemia might be expected On the contrary theobserved uric acid increase in our study is rather suggestiveof an improved antioxidant capacity elicited by behavioralinterventions in type 2 diabetic patients with subsyndromaldepression
Beneficial effect of cognitive-behavioral interventionin reducing oxidative stress and inflammatory responsehas been reported in hemodialysis patients suffering frominsomnia [45] but rather sparse depression-related studiesmainly focused on the assessment of low-grade inflammationbiomarkers In a very recent randomized trial evaluating anewly developed cognitive-behavioral program (DIAMOS)in diabetic patients with subsyndromal depression a set ofpro- and anti-inflammatory biomarkers was analyzed at basaland one-year follow-up [20] No change in hs-CRP IL-1 andadiponectin was observed whereas a significant decrease ininterleukin-1 receptor antagonist (IL-1RA) was interpreted asan indirect index of alleviated IL-1-related damaging mech-anisms presumably involved in the pathogenesis of micro-and macrovascular complications of diabetes Likewise ourstudy could not demonstrate any influence of the behavioralinterventions on hs-CRP and adiponectin but we foundother inflammatory markers that is leukocyte count andtotal serum sialic acid (TSA) significantly reduced with thelatter being largely affected (1205782 = 032) by the interventionsperformed
Sialic acids comprise a family of heterogenous monosac-charides abundantly present on the cell membranes withcomplex and multiple biological roles in cellular signalingand immunity [46] TSA is a validated inflammatory andatherogenic marker that has been proposed as a novelbiomarker of cardiovascular disease [47] Elevated levels ofTSA in newly diagnosed type 2 diabetic patients have beenlinked to the risk for later development of macrovascularcomplications [28] Interestingly TSA has been identified asa superior predictive biomarker of metabolic syndrome overthe abundantly used hs-CRP [48] Nevertheless despite theobvious advantages TSA has been largely underutilized inthe research on combined inflammatory-metabolic patholo-gies and it has not been studied in depression until this studyOur results identify TSA as a sensitive biomarker of inflam-mation degree in subsyndromally depressed diabetic patientswhereas neither of the established biomarkers of low-gradeinflammation hs-CRP and adiponectin was able to reflectthe anti-inflammatory effect of the performed interventionsSignificant decrease in leukocyte count however clearlyconfirmed postintervention attenuation of the cell-mediatedinflammation response in our patients with an importantnotice that the presence of acute infection at the assessments
was excluded by total leukocyte count lt 100 times 109L or hs-CRP lt 50 gL
The ability of psychological intervention to reduceboth depressive symptoms and inflammation has been evi-denced in depressed breast-cancer patients [49] Further-more due to the insightful study-design Thornton et alwere able to demonstrate a bidirectional mechanistic rela-tionship between depressive symptoms and inflammationThe paradigmatic view of the low-grade inflammation asthe inflicting mechanism for depression has been at leastcomplemented if not refuted by their finding on the mecha-nistic role of depressive symptoms lowering in the reductionof inflammatory response [49] This explanatory mecha-nism might also be translated to our results particularlyconsidering a lack of any effect of interventions towardshyperglycemia and obesity in our study
It is well known that the intensity of oxidative damage andinflammation in diabetes is remarkably and positively asso-ciated with the severity of hyperglycemia [18] Howeverthe observed reduction in oxidative damage and low-gradeinflammation in our study could not be attributed to thismechanism since no significant changes from baseline tofollow-up were found in HbA1c clinically considered toreflect a fair glucoregulation (Table 3) Obesity-derived low-grade inflammation is another recognized harmful compo-nent in the pathogenesis of type 2 diabetes and its compli-cations [50] Obesity induces a disbalance between pro- andanti-inflammatory cytokinesadipokines resulting in low-grade inflammation and related adverse health outcomesranging from metabolic syndrome and diabetes to cardio-vascular diseases and cancer as well as depression [49ndash51]Reduction in bodyweight is accompanied by beneficialmeta-bolic and hormonal profiles and a reduced inflammation [52]with increased production of anti-inflammatory adipokineadiponectin suggested to be among themost relevant features[53] Since our subjects classified as overweightobese [54]retained their BMI at follow-up and revealed no changes inadiponectin levels it is likely that the observed effects ofinterventions on the reduction in depressive symptoms andoxidativeinflammatory biomarkers in this study dependedon another mechanism(s)
Chronic stress with deregulation of stress-response adap-tive mechanisms is considered to be a common feature ofboth diabetes and depression [55] There is a growing bodyof evidence suggesting that metabolic inflammation asso-ciated with obesity and diabetes inflicts neuroinflammationwhich causes serious disturbances of the hypothalamic-pituitary-adrenal (HPA) axis function and consequentlyleads to impairment of adaptive stress-response [56] More-over chronic stress exposure has recently been demonstratedas a promoting factor for accelerated oxidative damagewhereby a sustained activation of HPA-axis emerged again asthe key mediator [57] Neuroendocrine effects of behavioraltreatment for depression have not been extensively studiedbut the evidence so far suggests a hypothetical pathway thatconnects the nurturing effects derived from the patient-ther-apist ldquobondrdquo with reestablishment of neuroendocrine home-ostasis [58] Moreover positive effects of physical exercise onpreventing potentially harmful stress-related metabolic and
International Journal of Endocrinology 9
psychological consequences have been presumably mediatedby the same neuroendocrine mechanisms [59] Consideringunchanged metabolic profile of our subjects and remark-able improvements in depressive symptoms and oxida-tiveinflammatory biomarkers following either behavioralintervention it is tempting if not plausible to speculate onthe involvement of neuroendocrine mechanism(s) in achiev-ing this beneficial response It should be noted that a lackof between-group differences in changes observed in ourstudy might not be explained by a phenomenon known asldquoregression toward the meanrdquo or just a natural course ofparameters Previous findings on persistence of depressivesymptoms in people with type 2 diabetes indicate thatdepression is not only persistent [60 61] but also associatedwith an increased risk of aggravating over time [62] On theother hand oxidative damage toDNA is increasing in healthysubjects throughout time as a result of ageing process [33]while inflammatory response and ageing-associated damageto biomolecules are even more pronounced in diabetes dueto a long-term exposure to hyperglycemia and advanced-glycated end-products [34 50]
The strengths of this study are in examining a highlyprevalent population of type 2 patients with depressive symp-toms but no clinical depression using a randomized com-parative design employing structured behavioral interven-tions and analyzing clinically relevant changes of simple-to-measure oxidativeinflammatory biomarkers Its limitation isthe lack of treatment as usual control intervention precludingthe possibility to investigate the course and outcomes ofsubclinical depression without any treatment Also the studywas carried out in only one centermdasha tertiary diabetesclinicmdashwhich does not allow concluding about its feasibilityin other clinical settings Per-protocol analyses are presentedin the study results which were confirmed by the intention totreat analysis based on baseline-observation-carried-forwardapproach A lack of estimation derived frommultiple predic-tors may be considered a limitation of the study
5 Conclusions
This study has demonstrated that improvement in depressivesymptoms is accompanied with reduced oxidative dam-age and inflammatory response in type 2 diabetic patientswith subsyndromal depression Testing mediating effectshas indicated that medium-term improvement in depres-sive symptoms predicts long-term-reduction in oxidativedamage while mediating factors for observed reductionin inflammatory response should be further investigatedClinical benefits of treating subsyndromal depression wereshown to be comparable in all three treatment arms
Regardless of the mechanisms involved our study clearlyindicates that enhanced treatment as usual defined as briefpatient-centred diabetes reeducation is not inferior to psy-choeducation and exercise in providing beneficial outcomesin subsyndromally depressed type 2 diabetic patients Simplebehavioral interventions are capable not only of alleviatingdepressive symptoms but also of reducing the intensity ofdamaging oxidativeinflammatory processes thereby miti-gating the risk of development of diabetic complications
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The study was funded by the European Foundation forthe Study of Diabetes (EFSD)mdashNew Horizons CollaborativeResearch Initiative 2010 The authors would like to thankLovorka Perkovic Croatian Institute of Public Health forediting the paper
References
[1] S S Ali M A Stone J L Peters M J Davies and K KhuntildquoThe prevalence of co-morbid depression in adults with Type2 diabetes a systematic review and meta-analysisrdquo DiabeticMedicine vol 23 no 11 pp 1165ndash1173 2006
[2] P J Lustman R J Anderson K E Freedland M de Groot RM Carney and R E Clouse ldquoDepression and poor glycemiccontrol a meta-analytic review of the literaturerdquo Diabetes Carevol 23 no 7 pp 934ndash942 2000
[3] L K Richardson L E Egede M Mueller C L Echols and MGebregziabher ldquoLongitudinal effects of depression on glycemiccontrol in veterans with Type 2 diabetesrdquo General HospitalPsychiatry vol 30 no 6 pp 509ndash514 2008
[4] M de Groot R Anderson K E Freedland R E Clouse andP J Lustman ldquoAssociation of depression and diabetes com-plications ameta-analysisrdquo PsychosomaticMedicine vol 63 no4 pp 619ndash630 2001
[5] K Ismail KWinkley D Stahl T Chalder andM Edmonds ldquoAcohort study of people with diabetes and their first foot ulcerthe role of depression on mortalityrdquo Diabetes Care vol 30 no6 pp 1473ndash1479 2007
[6] X Zhang S L Norris E W Gregg Y J Cheng G Becklesand H S Kahn ldquoDepressive symptoms and mortality amongpersons with and without diabetesrdquo American Journal of Epi-demiology vol 161 no 7 pp 652ndash660 2005
[7] S A Black K S Markides and L A Ray ldquoDepression pre-dicts increased incidence of adverse health outcomes in olderMexican Americans with type 2 diabetesrdquo Diabetes Care vol26 no 10 pp 2822ndash2828 2003
[8] H Baumeister N Hutter and J Bengel ldquoPsychological andpharmacological interventions for depression in patients withdiabetesmellitus and depressionrdquoCochraneDatabase of System-atic Reviews vol 12 Article ID CD008381 2012
[9] E Harkness W Macdonald J Valderas P Coventry L Gaskand P Bower ldquoIdentifying psychosocial interventions thatimprove both physical and mental health in patients with dia-betes a systematic review and meta-analysisrdquo Diabetes Carevol 33 no 4 pp 926ndash930 2010
[10] M Berk L J Williams F N Jacka et al ldquoSo depression is aninflammatory disease but where does the inflammation comefromrdquo BMCMedicine vol 11 article 200 2013
[11] S de Kort D Keszthelyi and A A M Masclee ldquoLeaky gut anddiabetes mellitus what is the linkrdquoObesity Reviews vol 12 no6 pp 449ndash458 2011
[12] E T de Lemos J Oliveira J P Pinheiro and F Reis ldquoRegularphysical exercise as a strategy to improve antioxidant andanti-inflammatory status benefits in type 2 diabetes mellitusrdquo
10 International Journal of Endocrinology
Oxidative Medicine and Cellular Longevity vol 2012 Article ID741545 15 pages 2012
[13] T A Doyle M de Groot T Harris et al ldquoDiabetes depressivesymptoms and inflammation in older adults results fromthe Health Aging and Body Composition Studyrdquo Journal ofPsychosomatic Research vol 75 no 5 pp 419ndash424 2013
[14] J-P S Laake D Stahl S A Amiel et al ldquoThe associationbetween depressive symptoms and systemic inflammation inpeople with type 2 diabetes findings from the South Londondiabetes studyrdquoDiabetes Care vol 37 no 8 pp 2186ndash2192 2014
[15] N Rohleder ldquoStimulation of systemic low-grade inflammationby psychosocial stressrdquo Psychosomatic Medicine vol 76 no 3pp 181ndash189 2014
[16] M Maes ldquoAn intriguing and hitherto unexplained co-occur-rence depression and chronic fatigue syndrome are mani-festations of shared inflammatory oxidative and nitrosative(IOampNS) pathwaysrdquo Progress in Neuro-Psychopharmacologyand Biological Psychiatry vol 35 no 3 pp 784ndash794 2011
[17] P Palta L J Samuel E RMiller and S L Szanton ldquoDepressionand oxidative stress results from a meta-analysis of observa-tional studiesrdquo Psychosomatic Medicine vol 76 no 1 pp 12ndash192014
[18] L Rochette M Zeller Y Cottin and C Vergely ldquoDiabetes oxi-dative stress and therapeutic strategiesrdquo Biochimica et Biophys-ica Acta vol 1840 no 9 pp 2709ndash2729 2014
[19] S Keri C Szabo and O Kelemen ldquoExpression of Toll-LikeReceptors in peripheral blood mononuclear cells and responseto cognitive-behavioral therapy in major depressive disorderrdquoBrain Behavior and Immunity vol 40 pp 235ndash243 2014
[20] N Hermanns A Schmitt A Gahr et al ldquoThe effect ofa Diabetes-Specific Cognitive Behavioral Treatment Program(DIAMOS) for patients with diabetes and subclinical depres-sion results of a randomized controlled trialrdquo Diabetes Carevol 38 no 4 pp 551ndash560 2015
[21] K Kroenke R L Spitzer and J B W Williams ldquoThe patienthealth questionnaire-2 validity of a two-item depressionscreenerrdquoMedical Care vol 41 no 11 pp 1284ndash1292 2003
[22] J H Abramson ldquoWINPEPI updated computer programs forepidemiologists and their teaching potentialrdquo EpidemiologicPerspectives amp Innovations vol 8 no 1 article 1 2011
[23] J Cohen ldquoA power primerrdquo Psychological Bulletin vol 112 no1 pp 155ndash159 1992
[24] M Pibernik-Okanovic D Ajdukovic M V Lovrencic andN Hermanns ldquoDoes treatment of subsyndromal depressionimprove depression and diabetes related outcomes protocolfor a randomised controlled comparison of psycho-educationphysical exercise and treatment as usualrdquo Trials vol 12 article17 2011
[25] BArroll FGoodyear-SmithNKerse T Fishman and JGunnldquoEffect of the addition of a lsquohelprsquo question to two screeningquestions on specificity for diagnosis of depression in generalpractice diagnostic validity studyrdquo British Medical Journal vol331 no 7521 article 884 2005
[26] P Rohde P M Lewinsohn and J R Seeley ldquoComparability oftelephone and face-to-face interviews in assessing axis I and IIdisordersrdquo American Journal of Psychiatry vol 154 no 11 pp1593ndash1598 1997
[27] L S Radloff ldquoTheCES-D scalerdquoApplied Psychological Measure-ment vol 1 pp 385ndash401 1977
[28] M Gavella V Lipovac A Car M Vucic L Sokolic and RRakos ldquoSerum sialic acid in subjects with impaired glucose
tolerance and in newly diagnosed type 2 diabetic patientsrdquoActaDiabetologica vol 40 no 2 pp 95ndash100 2003
[29] M D Evans R Singh V Mistry K Sandhu P B Farmer andM S Cooke ldquoAnalysis of urinary 8-oxo-78-dihydro-purine-21015840- deoxyribonucleosides by LC-MSMS and improved ELISArdquoFree Radical Research vol 42 no 10 pp 831ndash840 2008
[30] M Pibernik-Okanovic D Begic D Ajdukovic N Andrijasevicand Z Metelko ldquoPsychoeducation versus treatment as usualin diabetic patients with subthreshold depression preliminaryresults of a randomized controlled trialrdquo Trials vol 10 article78 2009
[31] M Pibernik-Okanovic M Vucic Lovrencic D AjdukovicM Sekerija and N Hermanns ldquoPsychological behavioraland biological changes following treatments of subsyndromaldepression in people with type 2 diabetesrdquoDiabetologia vol 56supplement 1 p S465 2013
[32] L Fisher D Hessler R E Glasgow et al ldquoREDEEM a prag-matic trial to reduce diabetes distressrdquo Diabetes Care vol 36no 9 pp 2551ndash2558 2013
[33] H E Poulsen L L Nadal K Broedbaek P E Nielsen andA Weimann ldquoDetection and interpretation of 8-oxodG and 8-oxoGua in urine plasma and cerebrospinal fluidrdquo Biochimica etBiophysica ActamdashGeneral Subjects vol 1840 no 2 pp 801ndash8082014
[34] K Broedbaek A Weimann E S Stovgaard and H E PoulsenldquoUrinary 8-oxo-78-dihydro-21015840-deoxyguanosine as a biomarkerin type 2 diabetesrdquo Free Radical Biology and Medicine vol 51no 8 pp 1473ndash1479 2011
[35] M J Forlenza and G E Miller ldquoIncreased serum levels of 8-hydroxy-21015840-deoxyguanosine in clinical depressionrdquo Psychoso-matic Medicine vol 68 no 1 pp 1ndash7 2006
[36] A Jorgensen J Krogh K Miskowiak et al ldquoSystemic oxida-tively generatedDNARNAdamage in clinical depression asso-ciations to symptom severity and response to electroconvulsivetherapyrdquo Journal of Affective Disorders vol 149 no 1ndash3 pp 355ndash362 2013
[37] S Yi ANanri YMatsushitaHKasai K Kawai andTMizoueldquoDepressive symptoms and oxidative DNA damage in Japanesemunicipal employeesrdquo Psychiatry Research vol 200 no 2-3 pp318ndash322 2012
[38] H Nojima H Watanabe K Yamane et al ldquoEffect of aerobicexercise training on oxidative stress in patients with type 2diabetes mellitusrdquo Metabolism Clinical and Experimental vol57 no 2 pp 170ndash176 2008
[39] S Bonakdaran and B Kharaqani ldquoAssociation of serum uricacid and metabolic syndrome in type 2 diabetesrdquo CurrentDiabetes Reviews vol 10 no 2 pp 113ndash117 2014
[40] R J Johnson T Nakagawa L G Sanchez-Lozada et al ldquoSugaruric acid and the etiology of diabetes and obesityrdquoDiabetes vol62 no 10 pp 3307ndash3315 2013
[41] M L Wahlqvist ldquoAntioxidant relevance to human healthrdquo AsiaPacific Journal of Clinical Nutrition vol 22 no 2 pp 171ndash1762013
[42] A De Giorgi F Fabbian M Pala et al ldquoUric acid friend orfoe Uric acid and cognitive function lsquogout kills more wise menthan simplersquordquo European Review forMedical and PharmacologicalSciences vol 19 no 4 pp 640ndash646 2015
[43] M Vucic B Rocic V Bozikov and S J H Ashcroft ldquoPlasmauric acid and total antioxidant status in patients with diabetesmellitusrdquo Hormone and Metabolic Research vol 29 no 7 pp355ndash357 1997
International Journal of Endocrinology 11
[44] G Desideri G Castaldo A Lombardi et al ldquoIs it time to revisethe normal range of serum uric acid levelsrdquo European Reviewfor Medical and Pharmacological Sciences vol 18 no 9 pp1295ndash1306 2014
[45] H-Y Chen I-C Cheng Y-J Pan et al ldquoCognitive-behavioraltherapy for sleep disturbance decreases inflammatory cytokinesand oxidative stress in hemodialysis patientsrdquo Kidney Interna-tional vol 80 no 4 pp 415ndash422 2011
[46] A Varki and P Gagneux ldquoMultifarious roles of sialic acids inimmunityrdquo Annals of the New York Academy of Sciences vol1253 no 1 pp 16ndash36 2012
[47] K P Gopaul and M A Crook ldquoSialic acid a novel marker ofcardiovascular diseaserdquo Clinical Biochemistry vol 39 no 7 pp667ndash681 2006
[48] L M Browning S A Jebb G D Mishra et al ldquoElevated sialicacid but not CRP predicts features of the metabolic syndromeindependently of BMI in womenrdquo International Journal ofObesity vol 28 no 8 pp 1004ndash1010 2004
[49] LMThornton B L Andersen T A Schuler andW E CarsonldquoA psychological intervention reduces inflammatory markersby alleviating depressive symptoms secondary analysis of arandomized controlled trialrdquo Psychosomatic Medicine vol 71no 7 pp 715ndash724 2009
[50] N Esser S Legrand-Poels J Piette A J Scheen and N PaquotldquoInflammation as a link between obesity metabolic syndromeand type 2 diabetesrdquoDiabetes Research andClinical Practice vol105 no 2 pp 141ndash150 2014
[51] R Hutcheson and P Rocic ldquoThe metabolic syndrome oxida-tive stress environment and cardiovascular disease the greatexplorationrdquo Experimental Diabetes Research vol 2012 ArticleID 271028 13 pages 2012
[52] L Fontana and F B Hu ldquoOptimal body weight for health andlongevity bridging basic clinical and population researchrdquoAging Cell vol 13 no 3 pp 391ndash400 2014
[53] A T Turer and P E Scherer ldquoAdiponectin mechanistic insightsand clinical implicationsrdquo Diabetologia vol 55 no 9 pp 2319ndash2326 2012
[54] WHO ldquoObesity and overweightrdquo Fact sheet No 311 2015[55] P W Gold ldquoThe organization of the stress system and its
dysregulation in depressive illnessrdquo Molecular Psychiatry vol20 no 1 pp 32ndash47 2015
[56] S Purkayastha and D Cai ldquoNeuroinflammatory basis ofmetabolic syndromerdquo Molecular Metabolism vol 2 no 4 pp356ndash363 2013
[57] K Aschbacher A OrsquoDonovan O MWolkowitz F S DhabharY Su and E Epel ldquoGood stress bad stress and oxidative stressinsights from anticipatory cortisol reactivityrdquo Psychoneuroen-docrinology vol 38 no 9 pp 1698ndash1708 2013
[58] C F Sharpley ldquoA review of the neurobiological effects of psy-chotherapy for depressionrdquo Psychotherapy vol 47 no 4 pp603ndash615 2010
[59] M N Silverman and P A Deuster ldquoBiological mechanismsunderlying the role of physical fitness in health and resiliencerdquoInterface Focus vol 4 no 5 Article ID 20140040 2014
[60] G Nefs F Pouwer J Denollet and V Pop ldquoThe course ofdepressive symptoms in primary care patients with type 2 dia-betes results from theDiabetes Depression TypeDPersonalityZuidoost-Brabant (DiaDDZoB) Studyrdquo Diabetologia vol 55no 3 pp 608ndash616 2012
[61] M Pibernik-Okanovic D Begic K Peros S Szabo andZ Metelko ldquoPsychosocial factors contributing to persistent
depressive symptoms in type 2 diabetic patients a Croatiansurvey from the European Depression in Diabetes ResearchConsortiumrdquo Journal of Diabetes and Its Complications vol 22no 4 pp 246ndash253 2008
[62] M Bot F Pouwer J Ormel J P J Slaets and P de Jonge ldquoPre-dictors of incidentmajor depression in diabetic outpatients withsubthreshold depressionrdquo Diabetic Medicine vol 27 no 11 pp1295ndash1301 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

International Journal of Endocrinology 9
psychological consequences have been presumably mediatedby the same neuroendocrine mechanisms [59] Consideringunchanged metabolic profile of our subjects and remark-able improvements in depressive symptoms and oxida-tiveinflammatory biomarkers following either behavioralintervention it is tempting if not plausible to speculate onthe involvement of neuroendocrine mechanism(s) in achiev-ing this beneficial response It should be noted that a lackof between-group differences in changes observed in ourstudy might not be explained by a phenomenon known asldquoregression toward the meanrdquo or just a natural course ofparameters Previous findings on persistence of depressivesymptoms in people with type 2 diabetes indicate thatdepression is not only persistent [60 61] but also associatedwith an increased risk of aggravating over time [62] On theother hand oxidative damage toDNA is increasing in healthysubjects throughout time as a result of ageing process [33]while inflammatory response and ageing-associated damageto biomolecules are even more pronounced in diabetes dueto a long-term exposure to hyperglycemia and advanced-glycated end-products [34 50]
The strengths of this study are in examining a highlyprevalent population of type 2 patients with depressive symp-toms but no clinical depression using a randomized com-parative design employing structured behavioral interven-tions and analyzing clinically relevant changes of simple-to-measure oxidativeinflammatory biomarkers Its limitation isthe lack of treatment as usual control intervention precludingthe possibility to investigate the course and outcomes ofsubclinical depression without any treatment Also the studywas carried out in only one centermdasha tertiary diabetesclinicmdashwhich does not allow concluding about its feasibilityin other clinical settings Per-protocol analyses are presentedin the study results which were confirmed by the intention totreat analysis based on baseline-observation-carried-forwardapproach A lack of estimation derived frommultiple predic-tors may be considered a limitation of the study
5 Conclusions
This study has demonstrated that improvement in depressivesymptoms is accompanied with reduced oxidative dam-age and inflammatory response in type 2 diabetic patientswith subsyndromal depression Testing mediating effectshas indicated that medium-term improvement in depres-sive symptoms predicts long-term-reduction in oxidativedamage while mediating factors for observed reductionin inflammatory response should be further investigatedClinical benefits of treating subsyndromal depression wereshown to be comparable in all three treatment arms
Regardless of the mechanisms involved our study clearlyindicates that enhanced treatment as usual defined as briefpatient-centred diabetes reeducation is not inferior to psy-choeducation and exercise in providing beneficial outcomesin subsyndromally depressed type 2 diabetic patients Simplebehavioral interventions are capable not only of alleviatingdepressive symptoms but also of reducing the intensity ofdamaging oxidativeinflammatory processes thereby miti-gating the risk of development of diabetic complications
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
Acknowledgments
The study was funded by the European Foundation forthe Study of Diabetes (EFSD)mdashNew Horizons CollaborativeResearch Initiative 2010 The authors would like to thankLovorka Perkovic Croatian Institute of Public Health forediting the paper
References
[1] S S Ali M A Stone J L Peters M J Davies and K KhuntildquoThe prevalence of co-morbid depression in adults with Type2 diabetes a systematic review and meta-analysisrdquo DiabeticMedicine vol 23 no 11 pp 1165ndash1173 2006
[2] P J Lustman R J Anderson K E Freedland M de Groot RM Carney and R E Clouse ldquoDepression and poor glycemiccontrol a meta-analytic review of the literaturerdquo Diabetes Carevol 23 no 7 pp 934ndash942 2000
[3] L K Richardson L E Egede M Mueller C L Echols and MGebregziabher ldquoLongitudinal effects of depression on glycemiccontrol in veterans with Type 2 diabetesrdquo General HospitalPsychiatry vol 30 no 6 pp 509ndash514 2008
[4] M de Groot R Anderson K E Freedland R E Clouse andP J Lustman ldquoAssociation of depression and diabetes com-plications ameta-analysisrdquo PsychosomaticMedicine vol 63 no4 pp 619ndash630 2001
[5] K Ismail KWinkley D Stahl T Chalder andM Edmonds ldquoAcohort study of people with diabetes and their first foot ulcerthe role of depression on mortalityrdquo Diabetes Care vol 30 no6 pp 1473ndash1479 2007
[6] X Zhang S L Norris E W Gregg Y J Cheng G Becklesand H S Kahn ldquoDepressive symptoms and mortality amongpersons with and without diabetesrdquo American Journal of Epi-demiology vol 161 no 7 pp 652ndash660 2005
[7] S A Black K S Markides and L A Ray ldquoDepression pre-dicts increased incidence of adverse health outcomes in olderMexican Americans with type 2 diabetesrdquo Diabetes Care vol26 no 10 pp 2822ndash2828 2003
[8] H Baumeister N Hutter and J Bengel ldquoPsychological andpharmacological interventions for depression in patients withdiabetesmellitus and depressionrdquoCochraneDatabase of System-atic Reviews vol 12 Article ID CD008381 2012
[9] E Harkness W Macdonald J Valderas P Coventry L Gaskand P Bower ldquoIdentifying psychosocial interventions thatimprove both physical and mental health in patients with dia-betes a systematic review and meta-analysisrdquo Diabetes Carevol 33 no 4 pp 926ndash930 2010
[10] M Berk L J Williams F N Jacka et al ldquoSo depression is aninflammatory disease but where does the inflammation comefromrdquo BMCMedicine vol 11 article 200 2013
[11] S de Kort D Keszthelyi and A A M Masclee ldquoLeaky gut anddiabetes mellitus what is the linkrdquoObesity Reviews vol 12 no6 pp 449ndash458 2011
[12] E T de Lemos J Oliveira J P Pinheiro and F Reis ldquoRegularphysical exercise as a strategy to improve antioxidant andanti-inflammatory status benefits in type 2 diabetes mellitusrdquo
10 International Journal of Endocrinology
Oxidative Medicine and Cellular Longevity vol 2012 Article ID741545 15 pages 2012
[13] T A Doyle M de Groot T Harris et al ldquoDiabetes depressivesymptoms and inflammation in older adults results fromthe Health Aging and Body Composition Studyrdquo Journal ofPsychosomatic Research vol 75 no 5 pp 419ndash424 2013
[14] J-P S Laake D Stahl S A Amiel et al ldquoThe associationbetween depressive symptoms and systemic inflammation inpeople with type 2 diabetes findings from the South Londondiabetes studyrdquoDiabetes Care vol 37 no 8 pp 2186ndash2192 2014
[15] N Rohleder ldquoStimulation of systemic low-grade inflammationby psychosocial stressrdquo Psychosomatic Medicine vol 76 no 3pp 181ndash189 2014
[16] M Maes ldquoAn intriguing and hitherto unexplained co-occur-rence depression and chronic fatigue syndrome are mani-festations of shared inflammatory oxidative and nitrosative(IOampNS) pathwaysrdquo Progress in Neuro-Psychopharmacologyand Biological Psychiatry vol 35 no 3 pp 784ndash794 2011
[17] P Palta L J Samuel E RMiller and S L Szanton ldquoDepressionand oxidative stress results from a meta-analysis of observa-tional studiesrdquo Psychosomatic Medicine vol 76 no 1 pp 12ndash192014
[18] L Rochette M Zeller Y Cottin and C Vergely ldquoDiabetes oxi-dative stress and therapeutic strategiesrdquo Biochimica et Biophys-ica Acta vol 1840 no 9 pp 2709ndash2729 2014
[19] S Keri C Szabo and O Kelemen ldquoExpression of Toll-LikeReceptors in peripheral blood mononuclear cells and responseto cognitive-behavioral therapy in major depressive disorderrdquoBrain Behavior and Immunity vol 40 pp 235ndash243 2014
[20] N Hermanns A Schmitt A Gahr et al ldquoThe effect ofa Diabetes-Specific Cognitive Behavioral Treatment Program(DIAMOS) for patients with diabetes and subclinical depres-sion results of a randomized controlled trialrdquo Diabetes Carevol 38 no 4 pp 551ndash560 2015
[21] K Kroenke R L Spitzer and J B W Williams ldquoThe patienthealth questionnaire-2 validity of a two-item depressionscreenerrdquoMedical Care vol 41 no 11 pp 1284ndash1292 2003
[22] J H Abramson ldquoWINPEPI updated computer programs forepidemiologists and their teaching potentialrdquo EpidemiologicPerspectives amp Innovations vol 8 no 1 article 1 2011
[23] J Cohen ldquoA power primerrdquo Psychological Bulletin vol 112 no1 pp 155ndash159 1992
[24] M Pibernik-Okanovic D Ajdukovic M V Lovrencic andN Hermanns ldquoDoes treatment of subsyndromal depressionimprove depression and diabetes related outcomes protocolfor a randomised controlled comparison of psycho-educationphysical exercise and treatment as usualrdquo Trials vol 12 article17 2011
[25] BArroll FGoodyear-SmithNKerse T Fishman and JGunnldquoEffect of the addition of a lsquohelprsquo question to two screeningquestions on specificity for diagnosis of depression in generalpractice diagnostic validity studyrdquo British Medical Journal vol331 no 7521 article 884 2005
[26] P Rohde P M Lewinsohn and J R Seeley ldquoComparability oftelephone and face-to-face interviews in assessing axis I and IIdisordersrdquo American Journal of Psychiatry vol 154 no 11 pp1593ndash1598 1997
[27] L S Radloff ldquoTheCES-D scalerdquoApplied Psychological Measure-ment vol 1 pp 385ndash401 1977
[28] M Gavella V Lipovac A Car M Vucic L Sokolic and RRakos ldquoSerum sialic acid in subjects with impaired glucose
tolerance and in newly diagnosed type 2 diabetic patientsrdquoActaDiabetologica vol 40 no 2 pp 95ndash100 2003
[29] M D Evans R Singh V Mistry K Sandhu P B Farmer andM S Cooke ldquoAnalysis of urinary 8-oxo-78-dihydro-purine-21015840- deoxyribonucleosides by LC-MSMS and improved ELISArdquoFree Radical Research vol 42 no 10 pp 831ndash840 2008
[30] M Pibernik-Okanovic D Begic D Ajdukovic N Andrijasevicand Z Metelko ldquoPsychoeducation versus treatment as usualin diabetic patients with subthreshold depression preliminaryresults of a randomized controlled trialrdquo Trials vol 10 article78 2009
[31] M Pibernik-Okanovic M Vucic Lovrencic D AjdukovicM Sekerija and N Hermanns ldquoPsychological behavioraland biological changes following treatments of subsyndromaldepression in people with type 2 diabetesrdquoDiabetologia vol 56supplement 1 p S465 2013
[32] L Fisher D Hessler R E Glasgow et al ldquoREDEEM a prag-matic trial to reduce diabetes distressrdquo Diabetes Care vol 36no 9 pp 2551ndash2558 2013
[33] H E Poulsen L L Nadal K Broedbaek P E Nielsen andA Weimann ldquoDetection and interpretation of 8-oxodG and 8-oxoGua in urine plasma and cerebrospinal fluidrdquo Biochimica etBiophysica ActamdashGeneral Subjects vol 1840 no 2 pp 801ndash8082014
[34] K Broedbaek A Weimann E S Stovgaard and H E PoulsenldquoUrinary 8-oxo-78-dihydro-21015840-deoxyguanosine as a biomarkerin type 2 diabetesrdquo Free Radical Biology and Medicine vol 51no 8 pp 1473ndash1479 2011
[35] M J Forlenza and G E Miller ldquoIncreased serum levels of 8-hydroxy-21015840-deoxyguanosine in clinical depressionrdquo Psychoso-matic Medicine vol 68 no 1 pp 1ndash7 2006
[36] A Jorgensen J Krogh K Miskowiak et al ldquoSystemic oxida-tively generatedDNARNAdamage in clinical depression asso-ciations to symptom severity and response to electroconvulsivetherapyrdquo Journal of Affective Disorders vol 149 no 1ndash3 pp 355ndash362 2013
[37] S Yi ANanri YMatsushitaHKasai K Kawai andTMizoueldquoDepressive symptoms and oxidative DNA damage in Japanesemunicipal employeesrdquo Psychiatry Research vol 200 no 2-3 pp318ndash322 2012
[38] H Nojima H Watanabe K Yamane et al ldquoEffect of aerobicexercise training on oxidative stress in patients with type 2diabetes mellitusrdquo Metabolism Clinical and Experimental vol57 no 2 pp 170ndash176 2008
[39] S Bonakdaran and B Kharaqani ldquoAssociation of serum uricacid and metabolic syndrome in type 2 diabetesrdquo CurrentDiabetes Reviews vol 10 no 2 pp 113ndash117 2014
[40] R J Johnson T Nakagawa L G Sanchez-Lozada et al ldquoSugaruric acid and the etiology of diabetes and obesityrdquoDiabetes vol62 no 10 pp 3307ndash3315 2013
[41] M L Wahlqvist ldquoAntioxidant relevance to human healthrdquo AsiaPacific Journal of Clinical Nutrition vol 22 no 2 pp 171ndash1762013
[42] A De Giorgi F Fabbian M Pala et al ldquoUric acid friend orfoe Uric acid and cognitive function lsquogout kills more wise menthan simplersquordquo European Review forMedical and PharmacologicalSciences vol 19 no 4 pp 640ndash646 2015
[43] M Vucic B Rocic V Bozikov and S J H Ashcroft ldquoPlasmauric acid and total antioxidant status in patients with diabetesmellitusrdquo Hormone and Metabolic Research vol 29 no 7 pp355ndash357 1997
International Journal of Endocrinology 11
[44] G Desideri G Castaldo A Lombardi et al ldquoIs it time to revisethe normal range of serum uric acid levelsrdquo European Reviewfor Medical and Pharmacological Sciences vol 18 no 9 pp1295ndash1306 2014
[45] H-Y Chen I-C Cheng Y-J Pan et al ldquoCognitive-behavioraltherapy for sleep disturbance decreases inflammatory cytokinesand oxidative stress in hemodialysis patientsrdquo Kidney Interna-tional vol 80 no 4 pp 415ndash422 2011
[46] A Varki and P Gagneux ldquoMultifarious roles of sialic acids inimmunityrdquo Annals of the New York Academy of Sciences vol1253 no 1 pp 16ndash36 2012
[47] K P Gopaul and M A Crook ldquoSialic acid a novel marker ofcardiovascular diseaserdquo Clinical Biochemistry vol 39 no 7 pp667ndash681 2006
[48] L M Browning S A Jebb G D Mishra et al ldquoElevated sialicacid but not CRP predicts features of the metabolic syndromeindependently of BMI in womenrdquo International Journal ofObesity vol 28 no 8 pp 1004ndash1010 2004
[49] LMThornton B L Andersen T A Schuler andW E CarsonldquoA psychological intervention reduces inflammatory markersby alleviating depressive symptoms secondary analysis of arandomized controlled trialrdquo Psychosomatic Medicine vol 71no 7 pp 715ndash724 2009
[50] N Esser S Legrand-Poels J Piette A J Scheen and N PaquotldquoInflammation as a link between obesity metabolic syndromeand type 2 diabetesrdquoDiabetes Research andClinical Practice vol105 no 2 pp 141ndash150 2014
[51] R Hutcheson and P Rocic ldquoThe metabolic syndrome oxida-tive stress environment and cardiovascular disease the greatexplorationrdquo Experimental Diabetes Research vol 2012 ArticleID 271028 13 pages 2012
[52] L Fontana and F B Hu ldquoOptimal body weight for health andlongevity bridging basic clinical and population researchrdquoAging Cell vol 13 no 3 pp 391ndash400 2014
[53] A T Turer and P E Scherer ldquoAdiponectin mechanistic insightsand clinical implicationsrdquo Diabetologia vol 55 no 9 pp 2319ndash2326 2012
[54] WHO ldquoObesity and overweightrdquo Fact sheet No 311 2015[55] P W Gold ldquoThe organization of the stress system and its
dysregulation in depressive illnessrdquo Molecular Psychiatry vol20 no 1 pp 32ndash47 2015
[56] S Purkayastha and D Cai ldquoNeuroinflammatory basis ofmetabolic syndromerdquo Molecular Metabolism vol 2 no 4 pp356ndash363 2013
[57] K Aschbacher A OrsquoDonovan O MWolkowitz F S DhabharY Su and E Epel ldquoGood stress bad stress and oxidative stressinsights from anticipatory cortisol reactivityrdquo Psychoneuroen-docrinology vol 38 no 9 pp 1698ndash1708 2013
[58] C F Sharpley ldquoA review of the neurobiological effects of psy-chotherapy for depressionrdquo Psychotherapy vol 47 no 4 pp603ndash615 2010
[59] M N Silverman and P A Deuster ldquoBiological mechanismsunderlying the role of physical fitness in health and resiliencerdquoInterface Focus vol 4 no 5 Article ID 20140040 2014
[60] G Nefs F Pouwer J Denollet and V Pop ldquoThe course ofdepressive symptoms in primary care patients with type 2 dia-betes results from theDiabetes Depression TypeDPersonalityZuidoost-Brabant (DiaDDZoB) Studyrdquo Diabetologia vol 55no 3 pp 608ndash616 2012
[61] M Pibernik-Okanovic D Begic K Peros S Szabo andZ Metelko ldquoPsychosocial factors contributing to persistent
depressive symptoms in type 2 diabetic patients a Croatiansurvey from the European Depression in Diabetes ResearchConsortiumrdquo Journal of Diabetes and Its Complications vol 22no 4 pp 246ndash253 2008
[62] M Bot F Pouwer J Ormel J P J Slaets and P de Jonge ldquoPre-dictors of incidentmajor depression in diabetic outpatients withsubthreshold depressionrdquo Diabetic Medicine vol 27 no 11 pp1295ndash1301 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

10 International Journal of Endocrinology
Oxidative Medicine and Cellular Longevity vol 2012 Article ID741545 15 pages 2012
[13] T A Doyle M de Groot T Harris et al ldquoDiabetes depressivesymptoms and inflammation in older adults results fromthe Health Aging and Body Composition Studyrdquo Journal ofPsychosomatic Research vol 75 no 5 pp 419ndash424 2013
[14] J-P S Laake D Stahl S A Amiel et al ldquoThe associationbetween depressive symptoms and systemic inflammation inpeople with type 2 diabetes findings from the South Londondiabetes studyrdquoDiabetes Care vol 37 no 8 pp 2186ndash2192 2014
[15] N Rohleder ldquoStimulation of systemic low-grade inflammationby psychosocial stressrdquo Psychosomatic Medicine vol 76 no 3pp 181ndash189 2014
[16] M Maes ldquoAn intriguing and hitherto unexplained co-occur-rence depression and chronic fatigue syndrome are mani-festations of shared inflammatory oxidative and nitrosative(IOampNS) pathwaysrdquo Progress in Neuro-Psychopharmacologyand Biological Psychiatry vol 35 no 3 pp 784ndash794 2011
[17] P Palta L J Samuel E RMiller and S L Szanton ldquoDepressionand oxidative stress results from a meta-analysis of observa-tional studiesrdquo Psychosomatic Medicine vol 76 no 1 pp 12ndash192014
[18] L Rochette M Zeller Y Cottin and C Vergely ldquoDiabetes oxi-dative stress and therapeutic strategiesrdquo Biochimica et Biophys-ica Acta vol 1840 no 9 pp 2709ndash2729 2014
[19] S Keri C Szabo and O Kelemen ldquoExpression of Toll-LikeReceptors in peripheral blood mononuclear cells and responseto cognitive-behavioral therapy in major depressive disorderrdquoBrain Behavior and Immunity vol 40 pp 235ndash243 2014
[20] N Hermanns A Schmitt A Gahr et al ldquoThe effect ofa Diabetes-Specific Cognitive Behavioral Treatment Program(DIAMOS) for patients with diabetes and subclinical depres-sion results of a randomized controlled trialrdquo Diabetes Carevol 38 no 4 pp 551ndash560 2015
[21] K Kroenke R L Spitzer and J B W Williams ldquoThe patienthealth questionnaire-2 validity of a two-item depressionscreenerrdquoMedical Care vol 41 no 11 pp 1284ndash1292 2003
[22] J H Abramson ldquoWINPEPI updated computer programs forepidemiologists and their teaching potentialrdquo EpidemiologicPerspectives amp Innovations vol 8 no 1 article 1 2011
[23] J Cohen ldquoA power primerrdquo Psychological Bulletin vol 112 no1 pp 155ndash159 1992
[24] M Pibernik-Okanovic D Ajdukovic M V Lovrencic andN Hermanns ldquoDoes treatment of subsyndromal depressionimprove depression and diabetes related outcomes protocolfor a randomised controlled comparison of psycho-educationphysical exercise and treatment as usualrdquo Trials vol 12 article17 2011
[25] BArroll FGoodyear-SmithNKerse T Fishman and JGunnldquoEffect of the addition of a lsquohelprsquo question to two screeningquestions on specificity for diagnosis of depression in generalpractice diagnostic validity studyrdquo British Medical Journal vol331 no 7521 article 884 2005
[26] P Rohde P M Lewinsohn and J R Seeley ldquoComparability oftelephone and face-to-face interviews in assessing axis I and IIdisordersrdquo American Journal of Psychiatry vol 154 no 11 pp1593ndash1598 1997
[27] L S Radloff ldquoTheCES-D scalerdquoApplied Psychological Measure-ment vol 1 pp 385ndash401 1977
[28] M Gavella V Lipovac A Car M Vucic L Sokolic and RRakos ldquoSerum sialic acid in subjects with impaired glucose
tolerance and in newly diagnosed type 2 diabetic patientsrdquoActaDiabetologica vol 40 no 2 pp 95ndash100 2003
[29] M D Evans R Singh V Mistry K Sandhu P B Farmer andM S Cooke ldquoAnalysis of urinary 8-oxo-78-dihydro-purine-21015840- deoxyribonucleosides by LC-MSMS and improved ELISArdquoFree Radical Research vol 42 no 10 pp 831ndash840 2008
[30] M Pibernik-Okanovic D Begic D Ajdukovic N Andrijasevicand Z Metelko ldquoPsychoeducation versus treatment as usualin diabetic patients with subthreshold depression preliminaryresults of a randomized controlled trialrdquo Trials vol 10 article78 2009
[31] M Pibernik-Okanovic M Vucic Lovrencic D AjdukovicM Sekerija and N Hermanns ldquoPsychological behavioraland biological changes following treatments of subsyndromaldepression in people with type 2 diabetesrdquoDiabetologia vol 56supplement 1 p S465 2013
[32] L Fisher D Hessler R E Glasgow et al ldquoREDEEM a prag-matic trial to reduce diabetes distressrdquo Diabetes Care vol 36no 9 pp 2551ndash2558 2013
[33] H E Poulsen L L Nadal K Broedbaek P E Nielsen andA Weimann ldquoDetection and interpretation of 8-oxodG and 8-oxoGua in urine plasma and cerebrospinal fluidrdquo Biochimica etBiophysica ActamdashGeneral Subjects vol 1840 no 2 pp 801ndash8082014
[34] K Broedbaek A Weimann E S Stovgaard and H E PoulsenldquoUrinary 8-oxo-78-dihydro-21015840-deoxyguanosine as a biomarkerin type 2 diabetesrdquo Free Radical Biology and Medicine vol 51no 8 pp 1473ndash1479 2011
[35] M J Forlenza and G E Miller ldquoIncreased serum levels of 8-hydroxy-21015840-deoxyguanosine in clinical depressionrdquo Psychoso-matic Medicine vol 68 no 1 pp 1ndash7 2006
[36] A Jorgensen J Krogh K Miskowiak et al ldquoSystemic oxida-tively generatedDNARNAdamage in clinical depression asso-ciations to symptom severity and response to electroconvulsivetherapyrdquo Journal of Affective Disorders vol 149 no 1ndash3 pp 355ndash362 2013
[37] S Yi ANanri YMatsushitaHKasai K Kawai andTMizoueldquoDepressive symptoms and oxidative DNA damage in Japanesemunicipal employeesrdquo Psychiatry Research vol 200 no 2-3 pp318ndash322 2012
[38] H Nojima H Watanabe K Yamane et al ldquoEffect of aerobicexercise training on oxidative stress in patients with type 2diabetes mellitusrdquo Metabolism Clinical and Experimental vol57 no 2 pp 170ndash176 2008
[39] S Bonakdaran and B Kharaqani ldquoAssociation of serum uricacid and metabolic syndrome in type 2 diabetesrdquo CurrentDiabetes Reviews vol 10 no 2 pp 113ndash117 2014
[40] R J Johnson T Nakagawa L G Sanchez-Lozada et al ldquoSugaruric acid and the etiology of diabetes and obesityrdquoDiabetes vol62 no 10 pp 3307ndash3315 2013
[41] M L Wahlqvist ldquoAntioxidant relevance to human healthrdquo AsiaPacific Journal of Clinical Nutrition vol 22 no 2 pp 171ndash1762013
[42] A De Giorgi F Fabbian M Pala et al ldquoUric acid friend orfoe Uric acid and cognitive function lsquogout kills more wise menthan simplersquordquo European Review forMedical and PharmacologicalSciences vol 19 no 4 pp 640ndash646 2015
[43] M Vucic B Rocic V Bozikov and S J H Ashcroft ldquoPlasmauric acid and total antioxidant status in patients with diabetesmellitusrdquo Hormone and Metabolic Research vol 29 no 7 pp355ndash357 1997
International Journal of Endocrinology 11
[44] G Desideri G Castaldo A Lombardi et al ldquoIs it time to revisethe normal range of serum uric acid levelsrdquo European Reviewfor Medical and Pharmacological Sciences vol 18 no 9 pp1295ndash1306 2014
[45] H-Y Chen I-C Cheng Y-J Pan et al ldquoCognitive-behavioraltherapy for sleep disturbance decreases inflammatory cytokinesand oxidative stress in hemodialysis patientsrdquo Kidney Interna-tional vol 80 no 4 pp 415ndash422 2011
[46] A Varki and P Gagneux ldquoMultifarious roles of sialic acids inimmunityrdquo Annals of the New York Academy of Sciences vol1253 no 1 pp 16ndash36 2012
[47] K P Gopaul and M A Crook ldquoSialic acid a novel marker ofcardiovascular diseaserdquo Clinical Biochemistry vol 39 no 7 pp667ndash681 2006
[48] L M Browning S A Jebb G D Mishra et al ldquoElevated sialicacid but not CRP predicts features of the metabolic syndromeindependently of BMI in womenrdquo International Journal ofObesity vol 28 no 8 pp 1004ndash1010 2004
[49] LMThornton B L Andersen T A Schuler andW E CarsonldquoA psychological intervention reduces inflammatory markersby alleviating depressive symptoms secondary analysis of arandomized controlled trialrdquo Psychosomatic Medicine vol 71no 7 pp 715ndash724 2009
[50] N Esser S Legrand-Poels J Piette A J Scheen and N PaquotldquoInflammation as a link between obesity metabolic syndromeand type 2 diabetesrdquoDiabetes Research andClinical Practice vol105 no 2 pp 141ndash150 2014
[51] R Hutcheson and P Rocic ldquoThe metabolic syndrome oxida-tive stress environment and cardiovascular disease the greatexplorationrdquo Experimental Diabetes Research vol 2012 ArticleID 271028 13 pages 2012
[52] L Fontana and F B Hu ldquoOptimal body weight for health andlongevity bridging basic clinical and population researchrdquoAging Cell vol 13 no 3 pp 391ndash400 2014
[53] A T Turer and P E Scherer ldquoAdiponectin mechanistic insightsand clinical implicationsrdquo Diabetologia vol 55 no 9 pp 2319ndash2326 2012
[54] WHO ldquoObesity and overweightrdquo Fact sheet No 311 2015[55] P W Gold ldquoThe organization of the stress system and its
dysregulation in depressive illnessrdquo Molecular Psychiatry vol20 no 1 pp 32ndash47 2015
[56] S Purkayastha and D Cai ldquoNeuroinflammatory basis ofmetabolic syndromerdquo Molecular Metabolism vol 2 no 4 pp356ndash363 2013
[57] K Aschbacher A OrsquoDonovan O MWolkowitz F S DhabharY Su and E Epel ldquoGood stress bad stress and oxidative stressinsights from anticipatory cortisol reactivityrdquo Psychoneuroen-docrinology vol 38 no 9 pp 1698ndash1708 2013
[58] C F Sharpley ldquoA review of the neurobiological effects of psy-chotherapy for depressionrdquo Psychotherapy vol 47 no 4 pp603ndash615 2010
[59] M N Silverman and P A Deuster ldquoBiological mechanismsunderlying the role of physical fitness in health and resiliencerdquoInterface Focus vol 4 no 5 Article ID 20140040 2014
[60] G Nefs F Pouwer J Denollet and V Pop ldquoThe course ofdepressive symptoms in primary care patients with type 2 dia-betes results from theDiabetes Depression TypeDPersonalityZuidoost-Brabant (DiaDDZoB) Studyrdquo Diabetologia vol 55no 3 pp 608ndash616 2012
[61] M Pibernik-Okanovic D Begic K Peros S Szabo andZ Metelko ldquoPsychosocial factors contributing to persistent
depressive symptoms in type 2 diabetic patients a Croatiansurvey from the European Depression in Diabetes ResearchConsortiumrdquo Journal of Diabetes and Its Complications vol 22no 4 pp 246ndash253 2008
[62] M Bot F Pouwer J Ormel J P J Slaets and P de Jonge ldquoPre-dictors of incidentmajor depression in diabetic outpatients withsubthreshold depressionrdquo Diabetic Medicine vol 27 no 11 pp1295ndash1301 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

International Journal of Endocrinology 11
[44] G Desideri G Castaldo A Lombardi et al ldquoIs it time to revisethe normal range of serum uric acid levelsrdquo European Reviewfor Medical and Pharmacological Sciences vol 18 no 9 pp1295ndash1306 2014
[45] H-Y Chen I-C Cheng Y-J Pan et al ldquoCognitive-behavioraltherapy for sleep disturbance decreases inflammatory cytokinesand oxidative stress in hemodialysis patientsrdquo Kidney Interna-tional vol 80 no 4 pp 415ndash422 2011
[46] A Varki and P Gagneux ldquoMultifarious roles of sialic acids inimmunityrdquo Annals of the New York Academy of Sciences vol1253 no 1 pp 16ndash36 2012
[47] K P Gopaul and M A Crook ldquoSialic acid a novel marker ofcardiovascular diseaserdquo Clinical Biochemistry vol 39 no 7 pp667ndash681 2006
[48] L M Browning S A Jebb G D Mishra et al ldquoElevated sialicacid but not CRP predicts features of the metabolic syndromeindependently of BMI in womenrdquo International Journal ofObesity vol 28 no 8 pp 1004ndash1010 2004
[49] LMThornton B L Andersen T A Schuler andW E CarsonldquoA psychological intervention reduces inflammatory markersby alleviating depressive symptoms secondary analysis of arandomized controlled trialrdquo Psychosomatic Medicine vol 71no 7 pp 715ndash724 2009
[50] N Esser S Legrand-Poels J Piette A J Scheen and N PaquotldquoInflammation as a link between obesity metabolic syndromeand type 2 diabetesrdquoDiabetes Research andClinical Practice vol105 no 2 pp 141ndash150 2014
[51] R Hutcheson and P Rocic ldquoThe metabolic syndrome oxida-tive stress environment and cardiovascular disease the greatexplorationrdquo Experimental Diabetes Research vol 2012 ArticleID 271028 13 pages 2012
[52] L Fontana and F B Hu ldquoOptimal body weight for health andlongevity bridging basic clinical and population researchrdquoAging Cell vol 13 no 3 pp 391ndash400 2014
[53] A T Turer and P E Scherer ldquoAdiponectin mechanistic insightsand clinical implicationsrdquo Diabetologia vol 55 no 9 pp 2319ndash2326 2012
[54] WHO ldquoObesity and overweightrdquo Fact sheet No 311 2015[55] P W Gold ldquoThe organization of the stress system and its
dysregulation in depressive illnessrdquo Molecular Psychiatry vol20 no 1 pp 32ndash47 2015
[56] S Purkayastha and D Cai ldquoNeuroinflammatory basis ofmetabolic syndromerdquo Molecular Metabolism vol 2 no 4 pp356ndash363 2013
[57] K Aschbacher A OrsquoDonovan O MWolkowitz F S DhabharY Su and E Epel ldquoGood stress bad stress and oxidative stressinsights from anticipatory cortisol reactivityrdquo Psychoneuroen-docrinology vol 38 no 9 pp 1698ndash1708 2013
[58] C F Sharpley ldquoA review of the neurobiological effects of psy-chotherapy for depressionrdquo Psychotherapy vol 47 no 4 pp603ndash615 2010
[59] M N Silverman and P A Deuster ldquoBiological mechanismsunderlying the role of physical fitness in health and resiliencerdquoInterface Focus vol 4 no 5 Article ID 20140040 2014
[60] G Nefs F Pouwer J Denollet and V Pop ldquoThe course ofdepressive symptoms in primary care patients with type 2 dia-betes results from theDiabetes Depression TypeDPersonalityZuidoost-Brabant (DiaDDZoB) Studyrdquo Diabetologia vol 55no 3 pp 608ndash616 2012
[61] M Pibernik-Okanovic D Begic K Peros S Szabo andZ Metelko ldquoPsychosocial factors contributing to persistent
depressive symptoms in type 2 diabetic patients a Croatiansurvey from the European Depression in Diabetes ResearchConsortiumrdquo Journal of Diabetes and Its Complications vol 22no 4 pp 246ndash253 2008
[62] M Bot F Pouwer J Ormel J P J Slaets and P de Jonge ldquoPre-dictors of incidentmajor depression in diabetic outpatients withsubthreshold depressionrdquo Diabetic Medicine vol 27 no 11 pp1295ndash1301 2010
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom