Embed Size (px)
Citation preview

Research ArticleHigh Intensity Interval Training Favourably AffectsAngiotensinogen mRNA Expression and Markers of CardiorenalHealth in a Rat Model of Early-Stage Chronic Kidney Disease
Patrick S Tucker12 Aaron T Scanlan12 and Vincent J Dalbo12
1Clinical Biochemistry Laboratory Central Queensland University Building 81 Bruce Highway Rockhampton QLD 4702 Australia2Human Exercise and Training Laboratory Central Queensland University Building 81 Bruce HighwayRockhampton QLD 4702 Australia
Correspondence should be addressed to Vincent J Dalbo vdalbocqueduau
Received 29 January 2015 Accepted 3 April 2015
Academic Editor Macaulay Onuigbo
Copyright copy 2015 Patrick S Tucker et al This is an open access article distributed under the Creative Commons AttributionLicense which permits unrestricted use distribution and reproduction in any medium provided the original work is properlycited
The majority of CKD-related complications stem from cardiovascular pathologies such as hypertension To help reducecardiovascular complications aerobic exercise is often prescribed Emerging evidence suggests high intensity interval training(HIIT) may be more beneficial than traditional aerobic exercise However appraisals of varying forms of aerobic exercise alongwith descriptions of mechanisms responsible for health-related improvements are lacking This study examined the effects of 8weeks of HIIT (85 VO
2max) versus low intensity aerobic exercise (LIT 45ndash50 VO2max) and sedentary behaviour (SED) in an
animal model of early-stage CKD Tissue-specificmRNA expression of RAAS-related genes and CKD-related clinical markers wereexamined Compared to SED HIIT resulted in increased plasma albumin (119901 = 0001) reduced remnant kidney weight (119901 = 0028)and reduced kidney weight-body weight ratios (119901 = 0045) Compared to LIT HIIT resulted in reduced Agt mRNA expression(119901 = 0035) reduced plasma LDL (119901 = 0001) triglycerides (119901 = 0029) and total cholesterol (119901 = 0002) increased plasmaalbumin (119901 = 0047) reduced remnant kidney weight (119901 = 0005) and reduced kidney weight-body weight ratios (119901 = 0048)These results suggest HIIT is a more potent regulator of several markers that describe and influence health in CKD
1 Introduction
The Australian Bureau of Statistics estimates that 14 ofAustralians (32 million) have at least one marker of kidneydamage or dysfunction [1] putting them at an increasedrisk of developing chronic kidney disease (CKD) CKD isa progressive and irreversible condition associated with anincreased risk of developing cardiovascular disease (CVD)[2] and a decreased life expectancy [2] It is possible toslow the progression of CKD particularly while the diseaseis in its early stages allowing for the delay of health-related complications and burdensome treatments associatedwith advanced CKD However as CKD progresses CKD-related risk factors (eg hypertension) and comorbidities(eg CVD) become less manageable resulting in a lifeexpectancy that steadily decreases as a function of continual
reductions in estimated glomerular filtration rate (eGFR)[2ndash4] Considering the irreversible nature of CKD and therelationship between life expectancy and kidney function itis apparent that slowing the progression of CKD is the idealapproach to CKD treatment
As new and existing cases of CKD progress to the extentthat they require renal replacement therapy (RRT) a termthat refers to dialysis or renal transplantation the existingburden on the healthcare system will increase considerably[5] Direct financial impact will stem from increases in costlytreatments such as dialysis which is expensive compared tomanymedical treatments while indirect financial impact willstem from an increased need for infrastructure includingadditional healthcare professionals equipment and treat-ment space [5] While current rates of RRT are troubling(more than 20000 Australians in 2012) [1] it is the pace
Hindawi Publishing CorporationBioMed Research InternationalVolume 2015 Article ID 156584 11 pageshttpdxdoiorg1011552015156584
2 BioMed Research International
at which RRT rates are increasing that is most concerningStatistical analyses have indicated by the year 2020 thatRRT prevalence is expected to increase by 29 with anaccompanying 37 increase in RRT-related expenditure [5]The sharp increase in RRT is largely due to associatedincreases in risk factors including obesity [6] physical inac-tivity [6] and hypertension [7] CKD-related hypertensionis especially noteworthy as hypertension is closely associatedwith declining eGFR independent of other risk factors [8 9]This hypertension-associated decline in eGFR is one reasonprior to commencing RRT the most common CKD-relatedtreatments focus on reducing hypertension The rationalebehind this approach is threefold (1) CKD is an indepen-dent risk factor for cardiac events [10 11] (2) controllinghypertension is the best way to influence quality of life [12]and prognosis [13 14] in CKD patients (3) hypertension isthe most influential modifiable-factor associated with CKDprogression [15]
Central to the concept of hypertension is the reninangiotensin aldosterone system (RAAS) a general termapplied to the network of enzymes and hormones thatregulate blood pressure [16] RAAS is characterised by renina protein encoded by the gene Ren that cleaves a peptidebond on angiotensinogen a protein encoded by the geneAgt resulting in angiotensin I [17] Although angiotensin I isbiologically inactive on its own it is converted to angiotensinII by angiotensin-converting enzyme [17] a protein encodedby the geneAceThe resulting angiotensin II influences bloodpressure by potentially binding to angiotensin II receptortype 1 [17] a receptor encoded by the genes Agtr1a andAgtr1b on intraglomerular mesangial cells causing them tocontract along with surrounding blood vessels In additionangiotensin II regulates the expression ofCyp11b2 a gene thatencodes the enzyme aldosterone synthase the enzyme thatsynthesises aldosterone [17] Once synthesised aldosteronepromotes the reabsorption of sodiumandwater in the tubulesof the kidney leading to increased blood volume whichresults in increased blood pressure [18] Considering thisit is apparent that intervention-based research focused onmodulating the activityexpression of the aforementionedRAAS-related compounds is timely
Chronic aerobic exercise training has emerged as apromising therapy in terms of reducing or regulating hyper-tension [19ndash21] Considering that CKD progression is closelyrelated to progressive hypertension [9 22] chronic aerobicexercise training may be especially beneficial in patientswith early-stage CKD who hope to avoid or delay the needfor RRT Recently high intensity interval training (HIIT)(asymp85 VO
2max) has been the focus of many cliniciansand researchers [23] who hypothesise that HIIT may elicitgreater benefits compared to traditional aerobic exercise(LIT) (asymp50 VO
2max) [24ndash26] Reasons for this suppositioninclude improved cardiovascular [24ndash26] and metabolic [23]outcomes In addition HIIT is also safe for many high-risk populations [26] including patients with CKD [27]This paired with the fact that HIIT encourages adherenceto aerobic exercise training programs [28] makes HIITan attractive therapeutic option for clinicians who aim to
regulate bloodpressure anddelay the need forRRT in patientswith CKD
Although it has been established that aerobic exercisebeneficially affects blood pressure investigations that focuson the direct effects of HIIT on the molecular components ofRAAS especially in models of early-stage CKD are unavail-able Moreover the underlying molecular mechanisms thatallow for increased benefit in HIIT compared to traditionalaerobic exercise have yet to be describedThis is largely due tothe fact that studies conducting tissue-specific analyses of themolecular markers involved in RAAS are difficult to performinhumans necessitating the need for animalmodels As suchthe purpose of the present study is to determine the effects ofchronic HIIT (4 times per week for 8 weeks) on the mRNAexpression of several key RAAS-related genes (Ren Agt AceAgtr1a Agtr1b and Cyp11b2) as well as traditional clinicalmarkers of CKD (creatinine albumin total cholesterol high-density lipoprotein low-density lipoprotein triglyceridesblood pressure body weight kidney weight and kidneyweight-body weight ratio) in an animal model of early-stage CKD It was hypothesised that HIIT would exert amore beneficial effect on RAAS-related mRNA expressionand traditional CKD-related clinical markers compared to asedentary (SED) condition and LIT
2 Materials and Methods21 Animals and General Overview Male spontaneouslyhypertensive rats (SHR) (119899 = 39) (Animal Resource CentreCanning Vale WA Australia) were housed in a temperature-controlled room (22ndash25∘C) with a dark-light cycle of 12 12hours and provided with ad libitum access to standardlaboratory chow and water At the time of arrival ratswere 4-5 weeks old Following a 2-week habituation periodallowing for acclimatisation to their new environment allrats underwent a unilateral nephrectomy (6-7 weeks old)Following surgery rats were allowed to recover for 2 weeks(8-9 weeks old) prior to the initiation of an 8-week aerobicexercise intervention Blood pressures body weights andbody lengths were recorded at baseline (preexercise) 4weeks (mid-intervention) and 8 weeks (postintervention)Following the 8-week intervention rats were euthanised24 hours following their last bout of exercise and tissueswere collected for subsequent analysis (16-17 weeks old)All research procedures were granted prior approval by aninstitutional Animal Ethics Committee
22 Anesthetisation andEuthanasia Procedures Prior to neph-rectomy rats were anesthetised with Zoletil (25mgkg) andXylazine (10mgkg) For pain relief Meloxicam (2mgkg)was injected once daily for 2 days following nephrectomyPrior to blood pressure readings rats were anesthetised withZoletil (25mgkg) Saline was injected subcutaneously fol-lowing each anesthetisation to help avoid dehydration Priorto being euthanised rats were given a Lethabarb injection(15mgkg)
23 Disease Modelling To mimic early-stage CKD a reduc-tion in renal function was induced by performing a unilateral
BioMed Research International 3
nephrectomy Briefly a small lumbar incision was made andthe left kidney was removed from each rat In addition tonephrectomising the rats SHRs were used to mimic the ele-vated blood pressure that is common inCKD Formore infor-mation regarding the disease model used in this study as wellas rationale refer to Supplement 1 in SupplementaryMaterialavailable online at httpdxdoiorg1011552015156584
24 Exercise Protocol Rats were randomly assigned to oneof three treatment groups sedentary (SED 119899 = 12) lightintensity aerobic exercise (LIT 119899 = 13) and high intensityinterval aerobic exercise (HIIT 119899 = 14) The number ofanimals assigned to each group was dependent on the formof exercise as the possibility existed that aerobic exercise mayhave proven too strenuous resulting in the need to withdrawan animal from the experiment However there were noadverse events in any group suggesting that aerobic exercisewas well-tolerated in this disease model
At 8-9 weeks of age rats in the LIT and HIIT wereintroduced to treadmill running for 8 weeks An identical 5-minute warm-up (15mmin) was performed by both traininggroups before each exercise session The LIT group exercisedat a treadmill speed of 15mmin with an incline of 1∘ (45ndash50 VO
2max) [29] up to 33 minutes per day 4 days perweek for 8 weeks The HIIT group exercised at a treadmillspeed of up to 50mmin with an incline of up to 10∘ (asymp85VO2max) [29] 30minutes per day (2-minute stationary period
followed by 1-minute sprinttimes 10 repetitions) 4 days per weekfor 8 weeks Differing treadmill inclines were used to achievethe desired intensity To permit adequate adaptation totreadmill running thereby allowing each exercise session tobe completed in its entirety exercise training was progressiveBy the beginning of the fourth week of training all rats wereperforming exercise sessions atmaximum intensitydurationthe exercise effort remained constant for the remaining 5weeks of training In an effort to standardise variables relatedto exercise training while simultaneously allowing for thecomparison of different forms sessions between LIT andHIITwerematched based on distance travelled per boutThatis despite the difference in exercisemodality between groupsLIT and HIIT travelled the same distance (plusmn1 meter) duringeach exercise session with distances progressing in unisonfrom asymp200 meters per session in week 1 to asymp500 meters persession in week 8 (Table 1)
25 Tissue Homogenisation and mRNA Isolation Tissuesused for analyses were chosen based on tissue-specifictranscriptomic work performed in SHRs [30] Renal tissuespecifically consisted of renal cortex asmRNA is differentiallyexpressed dependent on the type of renal tissue [31] For thesake of consistency hepatic tissue specifically consisted of theouter portion of the right lateral lobe
Approximately 100mg (plusmn10mg) of renal (for analysisof Ren Ace Agtr1b and Cyp11b2 mRNA) and hepatic (foranalysis of Agt and Agtr1a mRNA) tissue was homogenisedin 1mLof TRI-reagent using theTRI-reagentmethod (SigmaAldrich St Louis MO USA) Samples were then centrifugedat 12000timesg for 10 minutes at 4∘C The resulting supernatantwas transferred to a new microtube and incubated for 5
minutes at room temperature to allow for disassociation ofthe nucleoprotein complex Following incubation 02mL ofchloroform was added before this solution was mixed andthen incubated for 3 minutes Samples were then centrifugedat 12000timesg for 15 minutes at 4∘C The resulting supernatantwas transferred to a new microtube Following this sepa-ration 500120583L of 2-propanol was added to each microtubeMicrotubes were incubated at room temperature for 10minutes and then centrifuged at 12000timesg for 10 minutes at4∘C The resulting supernatant was removed leaving behinda mRNA pellet The mRNA pellet was exposed to 2 ethanolwashes (1mL 75) Following each wash microtubes werevortexed and centrifuged at 7500timesg for 5 minutes at 4∘CThe mRNA pellets were then allowed to air dry under afume hood before being dissolved in 30 120583L of RNase-freewater A 260280 ratio was calculated to assess mRNA puritywith all ratios falling within commonly accepted parameters(260280 ratio of 19ndash21) (NanoDrop 2000c Thermo Sci-entific Wilmington DE USA) The diluted mRNA sampleswere stored at minus80∘C until later analyses
26 Total mRNA Determination and Reverse Transcrip-tion Total mRNA concentrations from each sample weredetermined using a spectrophotometer (NanoDrop 2000cThermo Scientific Wilmington DE USA) Next mRNAconcentrations were adjusted to 400 ng120583L by diluting thecrude total mRNA extracts with RNase-free water Thestandardised solutions of total cellular mRNA were reversetranscribed to synthesise complimentaryDNA (cDNA) usinga High Capacity cDNA Reverse Transcription Kit (AppliedBiosystems Foster City CA USA) Briefly 2x RT mastermix was prepared per kit instructions Next 10 120583L of RT mixwas added (and mixed via pipette trituration) to 10 120583L of thestandardised mRNA solution These samples were placed ona thermal cycler (T100Thermal Cycler Bio-Rad GladesvilleNSW Australia) set to run at 25∘C for 10 minutes 37∘Cfor 120 minutes and 85∘C for 5 minutes Following reversetranscription the resulting cDNA template concentrationswere diluted to 5 ng120583L by adding RNase-free water Thestandardised cDNA solutions were frozen at minus80∘C untilquantitative reverse transcription polymerase chain reaction(qRT-PCR) was performed
27 Quantitative Reverse Transcription Polymerase ChainReaction Analysis Forward and reverse oligonucleotideprimer pairs were developed using National Centre forBiotechnology Informationrsquos (NCBI Bethesda MD USA)Primer Designer Tool before being commercially synthesised(GeneWorks Hindmarsh SA Australia) (Table 2) Gapdhwas used as an internal reference gene for detecting relativechange in the quantity of target mRNA due to its consid-eration as a constitutively expressed housekeeping gene fol-lowing aerobic exercise training Following the examinationof primer efficiencies qRT-PCR reactions were mixed Reac-tions contained the following mixture 25120583L of preparedcDNA template 5 120583L of SYBR Select Master Mix (Life Tech-nologies Mulgrave Victoria Australia) 05 120583L of sense andantisense primers and 15 120583L RNase-free water Followingthe mixture of each reaction qRT-PCR was performed with
4 BioMed Research International
Table 1 Detailed exercise protocol
Group Variable Measure Wk 1 Wk 2 Wk 3 Wk 4 Wk 5 Wk 6 Wk 7 Wk 8SED NA NA NA NA NA NA NA NA NA NA
LIT45ndash50 VO2max
Max speed MetersMin 15 15 15 15 15 15 15 15Incline Degrees 1 1 1 1 1 1 1 1Duration Minutes 133 20 266 333 333 333 333 333Intensity Constant treadmill speed and constant treadmill inclineFrequency BoutsWk 4 4 4 4 4 4 4 4
Distance per bout Meters 1995 300 399 4995 4995 4995 4995 4995Distance per week Meters 798 1200 1596 1998 1998 1998 1998 1998
HIITasymp85 VO2max
Max speed MetersMin 20 30 40 50 50 50 50 50Incline Degrees 5 10 10 10 10 10 10 10Duration Minutes 30 30 30 30 30 30 30 30Intensity 2min stationary period followed by 1min sprint period times 10 repsFrequency BoutsWk 4 4 4 4 4 4 4 4
Distance per bout Meters 200 300 400 500 500 500 500 500Distance per week Meters 800 1200 1600 2000 2000 2000 2000 2000
Identical 5-min warm-up (15mmin) was performed by both training groups prior to each exercise bout
Table 2 Primer sequences
Target Primer sequence (51015840-31015840)Angiotensin I converting enzyme (Ace) forward CTTGACCCTGGATTGCAGCCAngiotensin I converting enzyme (Ace) reverse GTTTCGTGAGGAAGCCAGGAAngiotensin II receptor type 1a (Agtr1a) forward AGTCCTGTTCCACCCGATCAAngiotensin II receptor type 1a (Agtr1a) reverse TCCAGACAAAATGCCAGCCAAngiotensin II receptor type 1b (Agtr1b) forward ACTGCACACGGTGCATTTTAAngiotensin II receptor type 1b (Agtr1b) reverse TAATTGTGCCTGCCAGCCTTAngiotensinogen (serpin peptidase inhibitor clade A member 8) (Agt) forward CTGGAGCTAAAGGACACACAGAAngiotensinogen (serpin peptidase inhibitor clade A member 8) (Agt) reverse GTGAAGGGACCCAAGCTCTCCytochrome P450 family 11 subfamily b polypeptide 2 (Cyp11b2) forward TAACTCAGGGAGCTTTACCTCTCytochrome P450 family 11 subfamily b polypeptide 2 (Cyp11b2) reverse CTGAGACCCTTTGAAGGCCGRenin (Ren) forward CCGTGGTCCTCACCAACTACRenin (Ren) reverse CTTGGCCAGCATGAAGGGTAGlyceraldehyde-3-phosphate dehydrogenase (Gapdh) forward GTTACCAGGGCTGCCTTCTCGlyceraldehyde-3-phosphate dehydrogenase (Gapdh) reverse GATGGTGATGGGTTTCCCGT
a thermal cycler (Rotor-Gene Q Qiagen Venlo Nether-lands) The amplification sequence involved an initial 10-minute cycle at 95∘C followed by 40 cycles each composedof a denaturation step (95∘C for 15 seconds) and a primerannealingextension step (60∘C for 45 seconds) Meltingcurves were performed to ensure that sufficient PCR productwas being generated by each primer in the absence of primerdimers All assays were performed in duplicate (coefficientof variation = 001) mRNA expression data were calculatedusing the Livak method [32] and data are presented as thefold change of the gene of interest relative to that of controlanimals (SED)
28 Clinical Markers in Plasma All bloodplasma markerswere assessed using blood taken from the descending aorta
of each rat Blood was collected into EDTA tubes followinglethal injection directly after the thoracic cavity of the animalhad been opened before tissues were collected This bloodwas centrifuged for 10 minutes at 1500timesg and the resultingplasma was aliquoted to 20mL microtubes and frozen atminus80∘C until it was analysed
Plasma triglyceridesweremeasured using a commerciallyavailable assay kit (Abcam Cambridge England UnitedKingdom) Briefly standards were prepared per the kitinstructions Next 25120583L of plasma was combined with assaybuffer in the well of a 96-well plate Lipase (2120583L) was addedto each well and solutions were mixed before incubating for20 minutes at room temperature Triglyceride reaction mixwas added to each well and solutions were mixed beforeincubating for 60 minutes at room temperature Triglycerideconcentrations were measured colorimetrically
BioMed Research International 5
Plasma high-density lipoprotein (HDL) and low-densitylipoprotein (LDL) were measured using a commerciallyavailable assay kit (Abcam Cambridge England UnitedKingdom) HDL and LDL fractions of plasma sampleswere separated per the kit instructions and standards wereprepared Next 15 120583L of HDL and LDL fractions was firstcombined with cholesterol assay buffer followed by reactionmix Solutions were mixed and then allowed to incubatefor 60 minutes at 37∘C HDL and LDL concentrations weremeasured colorimetrically Total cholesterol was calculatedusing a variation of the Friedlander formula [33]
Plasma creatinine was measured using a commerciallyavailable assay kit (Abcam Cambridge England UnitedKingdom) Standards were prepared per the kit instructionsNext 25 120583L of plasma was combined with assay buffer inthe well of a 96-well plate Reaction mix was added tothis solution and samples were allowed to incubate at 37∘Cfor 60 minutes Creatinine concentrations were measuredcolorimetrically
Plasma albumin was measured using a commerciallyavailable enzyme-linked immunosorbent assay (ELISA) kit(Abcam Cambridge England United Kingdom) Standardswere prepared per the kit instructions Plasma samples wereprepared and added to sample wells Biotinylated albuminwas then added to each well and this solution was mixedgently before a 60-minute incubation period Followingseveralwashes 1x Streptavidin-Peroxidase (SP) conjugatewasadded to each well prior to a 30-minute incubation periodOnce again plates were washed and 50120583L of chromogensubstrate was added followed by a 12-minute incubationperiod Stop solution was then added to each well andalbumin concentrations were measured colorimetrically
29 Clinical and Anthropometric Measurements Blood pres-sures body weights and body lengths were recorded beforesurgery baseline (preexercise) 4 weeks (mid-intervention)and 8 weeks (postintervention) Kidney weights wererecorded after intervention Systolic blood pressure (SBP)wasmeasured using data acquisition hardware (PowerLab ADIn-stuments Bella Vista NSW Australia) coupled to a nonin-vasive blood pressure (NIBP) system (NIBP System ADIn-stuments Bella Vista NSW Australia) with a pulse trans-ducercuff (Pulse TransducerPressure Cuff for NIBP ADIn-stuments Bella Vista NSW Australia) Measurements werethen analysed using LabChart 8 (ADInstuments Bella VistaNSW Australia) Body length was measured from tip-of-nose to tip-of-tail Body weight and remnant kidney weightwere measured to the nearest thousandth of a gram Bodylength and body weight measurements were taken whileeach rat was sedated directly prior to SBP measurement
210 Statistics mRNAdata are presented asmean plusmn standarderror of themean (SEM) All other data are presented asmeanplusmn standard deviation (SD) Body length body weight bodylength-body weight ratio and SBP data were analysed using3 times 3 (group times time) repeated measures analysis of variance(RMANOVA) When applicable group effects andor timeeffects were examined using separate one-way ANOVAs withTukey post hoc comparisons Data for all other measures
(mRNA expression plasma markers kidney weight andkidney weight-body weight ratio) were analysed using one-way ANOVAs with Tukey post hoc comparisons Analyseswere performed using IBM SPSS Statistics (v200 IBMCorporation Armonk NY USA) Statistical significance wasset at 119901 lt 005
3 Results
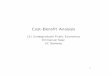
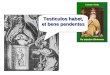
31 Quantitative Reverse Transcription Polymerase ChainReaction Analysis Results pertaining to renal expressionof RAAS-related mRNA can be seen in Figure 1 Resultspertaining to hepatic expression of RAAS-related mRNA canbe seen in Figure 2 Expression of renal Ren Ace Agtr1band Cyp11b2 mRNA and hepatic Agtr1a mRNA was notsignificantly different between groups (119901 gt 005) Expressionof hepatic Agt mRNA was significantly decreased in HIITcompared to LIT (119901 = 0035)
32 Clinical Markers in Plasma Results pertaining to clinicalmarkers in plasma can be seen in Table 3 Plasma measuresLDL (119901 = 0001) triglycerides (119901 = 0029) and totalcholesterol (119901 = 0002) were significantly lower in HIITcompared to LIT Plasma albumin was significantly higher inHIIT compared to SED (119901 = 0001) and LIT (119901 = 0047)
33 Anthropometric Measurements and Kidney WeightResults pertaining to anthropologicalmeasurements and kid-ney weight can be seen in Tables 3 and 4 Body Length bodyweight body length-body weight ratio and SBP increasedsignificantly from baseline to 4Weeks and from 4Weeks to 8Weeks (119901 lt 005) in all groups (Table 4) with no significantgroup interactions Kidney weight was significantly lower inHIIT compared to the SED (119901 = 0028) and LIT (119901 = 0005)Kidney weight-body weight ratio was significantly lower inHIIT compared to the SED (119901 = 0045) and LIT (119901 = 0048)(Table 3)
4 Discussion
The current study examined the ability of varying forms ofaerobic exercise to influence mRNA expression of severalRAAS-related genes as well as commonCKD-related clinicaland anthropometric markers in an animal model of early-stage CKD This is the first investigation to compare theefficacy of varying forms of aerobic exercise as it pertainsto the modulation of tissue-specific mRNA expression ofRAAS-related genes HIIT produced more favourable out-comes compared to SED and LIT in that HIIT resulted insignificantly reduced mRNA expression of Agt (compared toLIT) significantly improved plasma levels of LDL triglyc-erides and total cholesterol (compared to LIT) significantlyimproved plasma levels of albumin (compared to SED andLIT) and significantly reduced remnant kidney weight andkidney weight-body weight ratios (compared to SED andLIT)
Results regarding the mRNA expression of Agt are inter-esting The mRNA expression of all other genes (Ace Ren
6 BioMed Research International
200
160
120
080
040
000
200
160
120
080
040
000
200
160
120
080
040
000
SED (n = 12) LIT (n = 13) HIIT (n = 14) SED (n = 12) LIT (n = 13) HIIT (n = 14)
SED (n = 12) SED (n = 12)LIT (n = 13) HIIT (n = 14) LIT (n = 13) HIIT (n = 14)
100 053 053061 100 034
039 085
Ren-mRNA expression fold change(norm to GAPDH) (norm to GAPDH)
Ace-mRNA expression fold change
(norm to GAPDH)Agtr1b-mRNA expression fold change
(norm to GAPDH)Cyp11b2-mRNA expression fold change
086043100 100
200
160
120
080
040
000
Figure 1 Renal mRNA expression fold change
Agtr1a Agtr1b and Cyp11b2) was nonsignificantly downreg-ulated in both exercise groups compared to SED HoweverAgt mRNA expression was upregulated in LIT compared toSED (not significant) and HIIT (119901 = 0035) It is worthmentioning that our results are not the first data to suggestthat lower intensity aerobic exercise training may result inunfortunate adaptations in animal models of CKD aerobicexercise training performed at 50ndash70 of VO
2max has beenreported to result in increased resting SBP and decreasedmyocardial capillary density in an animal model of CKD[34]
Differential mRNA expression of Agt may partiallyexplain the nonsignificant (119901 = 0074) difference in SBP inHIIT during Week 8 compared to SED (119901 = 014 +528)and LIT (119901 = 074 +601) The downregulation in themRNA expression of Agt in HIIT may also explain the lackof significant differences in other RAAS genes in this studyThat is a decrease in the mRNA expression of Agt may havequenched the need for any additional significant decreases inthe expression of other RAAS genes This may explain whyeven though there was a near-significant reduction in SBPin HIIT compared to LIT (119901 = 0074) mRNA expression
BioMed Research International 7
p = 0035
118
076084
063
200
160
120
080
040
000
200
160
120
080
040
000
SED (n = 12) LIT (n = 13) HIIT (n = 14)
SED (n = 12) LIT (n = 13) HIIT (n = 14)
Agtr1a-mRNA expression fold change(norm to GAPDH)
(norm to GAPDH)Agt-mRNA expression fold change
100
100
Figure 2 Hepatic mRNA expression fold change
of several RAAS-related of genes (Ace Ren Agtr1b andCyp11b2) was slightly but not significantly increased in HIITcompared to LIT A review on hepatic angiotensinogen [35]discusses the noteworthy influence that angiotensinogen hason blood pressure Decreased levels of angiotensinogen usingangiotensinogen-antibodies in rats [36] and Agt-knockoutmice [37] exhibit lower blood pressure relative to controlsConversely angiotensinogen infusion in mice [38] and Agtoverexpression in rats [39] result in increased blood pressureEvidence suggests that angiotensinogen is a more potentinfluencer of blood pressure than previously suspected [35
Table 3 Nonrepeated clinical and anthropometric measures
Clinicalmeasure Group Mean Standard
deviationMean duplicate
CV
HDL (mgmL)SED 082 013
006LIT 088 015HIIT 093 012
LDL (mgmL)SED 127 027
003LIT 155 034HIIT 108lowast 032
TAG (mgmL)SED 565 166
004LIT 635 265HIIT 411lowast 204
CHOL(mgmL)
SED 322 047NALIT 371 061
HIIT 283lowast 073
CRE(nmol120583L)
SED 107 051004LIT 206 179
HIIT 211 126
ALB (mgmL)SED 2623 384
004LIT 2988 642HIIT 3524dagger 608
Kidney weight(g)
SED 157 009NALIT 159 012
HIIT 146dagger 008
KW-BW ratioSED 00050 00003
NALIT 00050 00003HIIT 00047dagger 00002
Significance set at 119901 le 005lowastSignificantly different from LITdaggerSignificantly different from LIT and SEDHDL high density lipoprotein LDL low density lipoprotein TAG triglyc-erides CHOL total cholesterol CRE creatinine ALB albumin KW-BWkidney weight-body weight CV coefficient of variation
39] often more influential than other components of RAAS[40] and deserves more attention as a potential targetin hypertension-related therapies [35] proposals that aresupported by our findings
Large amounts of between-animal variation in themRNAexpression of RAAS-related genes in SED may explain thelack of significant results in the current study Duplicate-duplicate variation was low (CV = 001) suggesting largeamounts of between-animal variation in SED The issueof between-animal mRNA variation has been empiricallyaddressed in the past [41ndash43] with the most commonlysuggested remedy being an increase in sample size Inter-estingly variation in between-animal mRNA expression inSED is higher across all genes (except for Agt) comparedto LIT and HIIT similar to previous work that has exam-ined RAAS-related mRNA expression in sedentary versusexercise-trained SHRs [20 44] This combined with the factthat aerobic exercise resulted in a downregulation across allgenes compared to SED (expect for Agt in LIT) suggeststhat RAAS-related mRNA expression may be poorly and
8 BioMed Research International
Table 4 Repeated clinical and anthropometric measures
Clinical measure Group Baseline 4 Weekslowast 8 Weeksdagger
(Preintervention) (Mid-Intervention) (Postintervention)
Body length (cm)SED 2848 (186) 3503 (085) 3741 (106)LIT 2932 (165) 3515 (079) 3789 (088)HIIT 2961 (225) 3546 (065) 3787 (062)
Body weight (g)SED 22442 (1782) 27605 (1831) 31353 (1662)LIT 23159 (2101) 27742 (2077) 31825 (2103)HIIT 23090 (1998) 27487 (1646) 30816 (1758)
BL-BW ratioSED 0126 (0007) 0127 (0007) 0120 (0004)LIT 0127 (0009) 0128 (0007) 0119 (0009)HIIT 0129 (0007) 0130 (0008) 0124 (0006)
Systolic blood pressure (mmHg)SED 17557 (927) 20777 (1739) 23977 (1285)LIT 17309 (945) 20925 (231) 24163 (2142)HIIT 17465 (1482) 21625 (1624) 22712 (1423)
Values presented as mean (standard deviation)Significance set at 119901 le 005lowastSignificantly different compared to baseline for all groupsdaggerSignificantly different compared to baseline and 4 weeks for all groupsBL-BW body length-body weight
indiscriminately regulated in the absence of aerobic exercisein an animal model of early-stage CKD That is aerobicexercise may help to control otherwise haphazard RAAS-related mRNA expression that occurs during the early stagesof CKD Several informative reviews have outlined theissue of unregulated blood pressure control [45] and morespecifically unregulated RAAS activity [46] in CKD but thisis the first study to suggest that one of the mechanisms bywhich aerobic exercise may prove beneficial is via tightenedcontrol of RAAS-related mRNA expression independentof statistically significant improvements to RAAS-relatedmRNA expression
In the current study the significant decreases in plasmaLDL triglycerides and total cholesterol in HIIT compared toLIT but not SED are encouraging and somewhat surprisingA recent study performed in healthy well-trained humansreported nonsignificant improvements in LDL triglyceridesand total cholesterol after 12 weeks of HIIT [47] In spe-cial andor clinical populations HIIT seems to exert moreinfluence over blood lipids Cardiac rehabilitation patientswho engaged in HIIT experienced significant improvementsin HDL relative to traditional aerobic exercise training[26] However triglyceride measurements were not differentbetween groups and LDL measurements were not reported[26] HIIT has also proven to be beneficial in obese men[48] and women [49] resulting in improved HDL [48]LDL [48] triglycerides [48 49] and total cholesterol [4849] Despite the slowly-accumulating data a recent review[50] that notes the ability of HIIT to influence blood lipidshas yet to be established especially in special populationssuggesting that this specific line of research the effects ofHIIT on blood lipids should be further examined This isespecially true in CKD as lipid-related disorders are theleading cause of complications in CVD [51 52] and CVD-related complications are the leading cause of death in CKD
patients [10 11] As such dyslipidemia should be rankedamong the primary concerns of CKD-related research [53]
Similar to blood lipids a recent review notes that theeffects of exercise training on plasma albumin in patientswith CKD are unclear [54] Moreover data describing theeffects of HIIT on plasma albumin in patients with CKD areunavailable Hypoalbuminemia is an independent predictorof renal dysfunction [55] and an independent predictor ofCVD in early-stage CKD [56] and can be used to identifyCKD patients at increased risk of developing CVD [56] Inobese individuals with metabolic syndrome two commoncharacteristics of CKD 12 weeks of aerobic exercise trainingsignificantly reduced albuminuria (urinary albumin) com-pared to a no-exercise control group [57] Aerobic exercisetraining (16 weeks at 60 of maximal aerobic velocity) hasalso proven useful at reducing albuminuria in SHRs [44]Because hypoalbuminemia is related to declining kidneyfunction [55] blood albumin andor urinary albumin areuseful markers for assessing the preservation of renal tissueIn the current study plasma albumin was significantly higherin HIIT compared to SED and LIT suggesting that renalstructure and function are better preserved by HIIT Thepreservation of renal structure and function and subsequentincrease in plasma albumin may have been due to the down-regulation of Agt mRNA expression and the accompanyingdecrease in SBP in HIIT as hypertension is directly related torenal damage [44 58]
Also considered an indicator of renal damage kid-ney weight and kidney weight-body weight ratio weresignificantly lower in HIIT compared to SED and LITHypertension-related declines in renal function are associ-ated with compensatory alterations to renal tissue such astubulointerstitial fibrosis [59 60] Often pathological thesealterations result in glomerular hypertrophy [59 60] Usinghistological and molecular applications 16 weeks of aerobic
BioMed Research International 9
exercise training (performed at 60 of maximal aerobicvelocity) has been shown to reduce renal fibrosis in SHRs[44] Although renal fibrosis and renal hypertrophy aredirectly related data that specifically describes the effectsof HIIT on renal hypertrophy are unavailable Similar tothe mechanisms that account for increased levels of plasmaalbumin in HIIT there is evidence to suggest that thesignificantly lower kidney weight and kidney weight-bodyweight ratios in HIIT compared to SED and LIT may bedue to decreased fibrosis Decreases in renal fibrosis maybe due to decreases in hypertension-mediated renal damagefollowing a downregulation of the mRNA expression of Agtand a decrease in SBP (in HIIT) [44 58]
5 Conclusions
In summary in an animal model of early-stage CKD HIITappeared to be more beneficial compared to SED and LITas HIIT was responsible for a significant downregulation inthe mRNA expression of Agt The downregulated mRNAexpression of Agt along with significant improvements toblood lipids (LDL triglycerides and total cholesterol) maypartially explain the nonsignificant decrease in SBP andsignificant improvements to plasma albumin kidney weightand kidney weight-body weight ratios in HIIT relative toSED and LIT Future work would benefit from examiningRAAS-related protein expression as well as specific measuresof renal histology and morphology Future work would alsobenefit from examining whether the positive HIIT-relatedeffects seen in the present study are apparent in differentrelated disease models (eg nonnephrectomised SHRs or 56nephrectomy SHRs)
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] AIHW Ed Australiarsquos Health 2014 Australiarsquos Health SeriesAustralian Institute of Health and Welfare (AIHW) CanberraAustralia 2014
[2] A S Go G M Chertow D Fan C E McCulloch andC-Y Hsu ldquoChronic kidney disease and the risks of deathcardiovascular events and hospitalizationrdquo The New EnglandJournal of Medicine vol 351 no 13 pp 1296ndash1370 2004
[3] U D Mathisen T Melsom O C Ingebretsen et al ldquoEstimatedGFR associates with cardiovascular risk factors independentlyof measured GFRrdquo Journal of the American Society of Nephrol-ogy vol 22 no 5 pp 927ndash937 2011
[4] DM Silverstein ldquoInflammation in chronic kidney disease rolein the progression of renal and cardiovascular diseaserdquoPediatricNephrology vol 24 no 8 pp 1445ndash1452 2009
[5] P S Tucker M I Kingsley R H Morton A T Scanlan andV J Dalbo ldquoThe increasing financial impact of chronic kidneydisease in Australiardquo International Journal of Nephrology vol2014 Article ID 120537 7 pages 2014
[6] B Stengel M E Tarver-Carr N R Powe M S Eberhardt andF L Brancati ldquoLifestyle factors obesity and the risk of chronickidney diseaserdquo Epidemiology vol 14 no 4 pp 479ndash487 2003
[7] R T Gansevoort R Correa-Rotter B R Hemmelgarn et alldquoChronic kidney disease and cardiovascular risk epidemiologymechanisms and preventionrdquoTheLancet vol 382 no 9889 pp339ndash352 2013
[8] M M H Hermans R Henry J M Dekker et al ldquoEstimatedglomerular filtration rate and urinary albumin excretion areindependently associated with greater arterial stiffness theHoorn studyrdquo Journal of the American Society of Nephrology vol18 no 6 pp 1942ndash1952 2007
[9] M L Ford L A Tomlinson T P E Chapman C Rajkumar andS G Holt ldquoAortic stiffness is independently associated with rateof renal function decline in chronic kidney disease stages 3 and4rdquo Hypertension vol 55 no 5 pp 1110ndash1115 2010
[10] D EWeiner H Tighiouart P C Stark et al ldquoKidney disease asa risk factor for recurrent cardiovascular disease andmortalityrdquoAmerican Journal of Kidney Diseases vol 44 no 2 pp 198ndash2062004
[11] D E Weiner H Tighiouart M G Amin et al ldquoChronickidney disease as a risk factor for cardiovascular disease and all-causemortality a pooled analysis of community-based studiesrdquoJournal of the American Society of Nephrology vol 15 no 5 pp1307ndash1315 2004
[12] R K Soni A C Porter J P Lash and M L Unruh ldquoHealth-related quality of life in hypertension chronic kidney diseaseand coexistent chronic health conditionsrdquo Advances in ChronicKidney Disease vol 17 no 4 pp e17ndashe26 2010
[13] J Segura C Campo P Gil et al ldquoDevelopment of chronickidney disease and cardiovascular prognosis in essential hyper-tensive patientsrdquo Journal of the American Society of Nephrologyvol 15 no 6 pp 1616ndash1622 2004
[14] J Blacher A P Guerin B Pannier S J Marchais M E Safarand G M London ldquoImpact of aortic stiffness on survival inend-stage renal diseaserdquo Circulation vol 99 no 18 pp 2434ndash2439 1999
[15] G L Bakris E Ritz and World Kidney Day Steering Commit-tee ldquoThe message for World Kidney Day 2009 hypertensionand kidney disease a marriage that should be preventedrdquo TheJournal of Clinical Hypertension (Greenwich) vol 11 no 3 pp144ndash147 2009
[16] J L Lavoie and C D Sigmund ldquoMinireview overview ofthe renin-angiotensin systemmdashan endocrine and paracrinesystemrdquo Endocrinology vol 144 no 6 pp 2179ndash2183 2003
[17] A Nguyen Dinh Cat and RM Touyz ldquoA new look at the renin-angiotensin systemmdashfocusing on the vascular systemrdquo Peptidesvol 32 no 10 pp 2141ndash2150 2011
[18] U C Brewster and M A Perazella ldquoThe renin-angiotensin-aldosterone system and the kidney effects on kidney diseaserdquoThe American Journal of Medicine vol 116 no 4 pp 263ndash2722004
[19] S Ciampone R Borges I P De Lima F F Mesquita EC Cambiucci and J A R Gontijo ldquoLong-term exerciseattenuates blood pressure responsiveness andmodulates kidneyangiotensin II signalling and urinary sodium excretion in SHRrdquoJournal of the Renin-Angiotensin-Aldosterone System vol 12 no4 pp 394ndash403 2011
[20] D Agarwal M A Welsch J N Keller and J Francis ldquoChronicexercise modulates RAS components and improves balancebetween pro- and anti-inflammatory cytokines in the brain of
10 BioMed Research International
SHRrdquo Basic Research in Cardiology vol 106 no 6 pp 1069ndash1085 2011
[21] E J Howden R G Fassett N M Isbel and J S CoombesldquoExercise training in chronic kidney disease patientsrdquo SportsMedicine vol 42 no 6 pp 473ndash488 2012
[22] S Nielsen A Schmitz M Rehling and C E Mogensen ldquoSys-tolic blood pressure relates to the rate of decline of glomerularfiltration rate in type II diabetesrdquo Diabetes Care vol 16 no 11pp 1427ndash1432 1993
[23] A E Tjoslashnna I M Leinan A T Bartnes et al ldquoLow- and high-volume of intensive endurance training significantly improvesmaximal oxygen uptake after 10-weeks of training in healthymenrdquo PLoS ONE vol 8 no 5 Article ID e65382 2013
[24] T Moholdt E Madssen Oslash Rognmo and I L Aamot ldquoThehigher the better Interval training intensity in coronary heartdiseaserdquo Journal of Science and Medicine in Sport vol 17 no 5pp 506ndash510 2014
[25] H E Molmen-Hansen T Stolen A E Tjonna et al ldquoAerobicinterval training reduces blood pressure and improves myocar-dial function in hypertensive patientsrdquo European Journal ofPreventive Cardiology vol 19 no 2 pp 151ndash160 2012
[26] T Moholdt I L Aamot I Granoslashien et al ldquoAerobic intervaltraining increases peak oxygen uptake more than usual careexercise training in myocardial infarction patients a random-ized controlled studyrdquo Clinical Rehabilitation vol 26 no 1 pp33ndash44 2012
[27] E J Howden J S Coombes H Strand B Douglas K LCampbell and N M Isbel ldquoExercise training in CKD efficacyadherence and safetyrdquoAmerican Journal of KidneyDiseases vol65 no 4 pp 583ndash591 2015
[28] A C KingW L Haskell D R Young R K Oka andM L Ste-fanick ldquoLong-term effects of varying intensities and formats ofphysical activity on participation rates fitness and lipoproteinsin men and women aged 50 to 65 yearsrdquo Circulation vol 91 no10 pp 2596ndash2604 1995
[29] G A Brooks and T P White ldquoDetermination of metabolicand heart rate responses of rats to treadmill exerciserdquo Journalof Applied Physiology Respiratory Environmental and ExercisePhysiology vol 45 no 6 pp 1009ndash1015 1978
[30] Y Yu J C Fuscoe C Zhao et al ldquoA rat RNA-Seq transcriptomicBodyMap across 11 organs and 4 developmental stagesrdquo NatureCommunications vol 5 article 3230 2014
[31] F Z Marques A E Campain M Tomaszewski et al ldquoGeneexpression profiling reveals renin mRNA overexpression inhuman hypertensive kidneys and a role formicroRNAsrdquoHyper-tension vol 58 no 6 pp 1093ndash1098 2011
[32] K J Livak and T D Schmittgen ldquoAnalysis of relative geneexpression data using real-time quantitative PCRand the 2minusΔΔ119862TmethodrdquoMethods vol 25 no 4 pp 402ndash408 2001
[33] Y Friedlander J D Kark S Eisenberg and Y Stein ldquoCalcula-tion of LDL-cholesterol from total cholesterol triglyceride andHDL-cholesterol a comparison of methods in the JerusalemLipid Research Clinic Prevalence Studyrdquo Israel Journal of Medi-cal Sciences vol 18 no 12 pp 1242ndash1252 1982
[34] K DMarcus andCM Tipton ldquoExercise training and its effectswith renal hypertensive ratsrdquo Journal of Applied Physiology vol59 no 5 pp 1410ndash1415 1985
[35] K Kitada H Kobori and A Nishiyama ldquoLiver-specificangiotensinogen suppression an old yet novel target forblood pressure control through RAS inhibitionrdquo HypertensionResearch vol 37 no 5 pp 393ndash394 2014
[36] J Gardes J Bouhnik E Clauser P Corvol and JMenard ldquoRoleof angiotensinogen in blood pressure homeostasisrdquo Hyperten-sion vol 4 no 2 pp 185ndash189 1982
[37] K Tanimoto F Sugiyama Y Goto et al ldquoAngiotensinogen-deficient mice with hypotensionrdquo The Journal of BiologicalChemistry vol 269 no 50 pp 31334ndash31337 1994
[38] S Kimura J J Mullins B Bunnemann et al ldquoHigh bloodpressure in transgenic mice carrying the rat angiotensinogengenerdquoThe EMBO Journal vol 11 no 3 pp 821ndash827 1992
[39] JMenard A-I K El Amrani F Savoie J Bouhnik K R LynchandM J Peach ldquoAngiotensinogen an attractive and underratedparticipant in hypertension and inflammationrdquo Hypertensionvol 18 no 5 pp 705ndash707 1991
[40] S Agrawal S Agarwal and S Naik ldquoGenetic contributionand associated pathophysiology in end-stage renal diseaserdquoTheApplication of Clinical Genetics vol 3 pp 65ndash84 2010
[41] W-C Cheng W-Y Shu C-Y Li et al ldquoIntra- and inter-individual variance of gene expression in clinical studiesrdquo PLoSONE vol 7 no 6 Article ID e38650 2012
[42] A Whitehead and D L Crawford ldquoVariation in tissue-specificgene expression among natural populationsrdquo Genome Biologyvol 6 no 2 article R13 2005
[43] A L Oberg B M Bot D E Grill G A Poland and TM Therneau ldquoTechnical and biological variance structure inmRNA-Seq data life in the real worldrdquo BMC Genomics vol 13no 1 article 304 2012
[44] D Agarwal C M Elks S D Reed N Mariappan D SA Majid and J Francis ldquoChronic exercise preserves renalstructure and hemodynamics in spontaneously hypertensiveratsrdquo Antioxidants amp Redox Signaling vol 16 no 2 pp 139ndash1522012
[45] P Zamboli L De Nicola R Minutolo V Bertino F Catapanoand G Conte ldquoManagement of hypertension in chronic kidneydiseaserdquoCurrentHypertensionReports vol 8 no 6 pp 497ndash5012006
[46] G Remuzzi N Perico M Macia and P Ruggenenti ldquoThe roleof renin-angiotensin-aldosterone system in the progression ofchronic kidney diseaserdquo Kidney International vol 68 no 99pp S57ndashS65 2005
[47] N Ouerghi M Feki N Kaabachi M Khammassi S Boukor-raa and A Bouassida ldquoEffects of a high-intensity intermittenttraining programon aerobic capacity and lipid profile in trainedsubjectsrdquoOpenAccess Journal of SportsMedicine vol 5 pp 243ndash248 2014
[48] A Paoli Q F Pacelli T Moro et al ldquoEffects of high-intensitycircuit training low-intensity circuit training and endurancetraining on blood pressure and lipoproteins in middle-agedoverweight menrdquo Lipids in Health and Disease vol 12 no 1article 131 2013
[49] G Racil O Ben Ounis O Hammouda et al ldquoEffects of highvs Moderate exercise intensity during interval training onlipids and adiponectin levels in obese young femalesrdquo EuropeanJournal of Applied Physiology vol 113 no 10 pp 2531ndash25402013
[50] H S Kessler S B Sisson and K R Short ldquoThe potentialfor high-intensity interval training to reduce cardiometabolicdisease riskrdquo Sports Medicine vol 42 no 6 pp 489ndash509 2012
[51] J Poss F Custodis CWernerOWeingartnerM Bohm andULaufs ldquoCardiovascular disease and dyslipidemia beyond LDLrdquoCurrent Pharmaceutical Design vol 17 no 9 pp 861ndash870 2011
BioMed Research International 11
[52] J R Burnett ldquoLipids lipoproteins atherosclerosis and cardio-vascular diseaserdquoThe Clinical Biochemist Reviews vol 25 no 1p 2 2004
[53] G Piecha M Adamczak and E Ritz ldquoDyslipidemia in chronickidney disease pathogenesis and interventionrdquo Polskie Archi-wum Medycyny Wewnetrznej vol 119 no 7-8 pp 487ndash4922009
[54] N A Smart A D Williams I Levinger et al ldquoExercise ampSports Science Australia (ESSA) position statement on exerciseand chronic kidney diseaserdquo Journal of Science and Medicine inSport vol 16 no 5 pp 406ndash411 2013
[55] S-J Pinto-Sietsma W M T Janssen H L Hillege G NavisD de Zeeuw and P E de Jong ldquoUrinary albumin excretion isassociated with renal functional abnormalities in a nondiabeticpopulationrdquo Journal of the American Society of Nephrology vol11 no 10 pp 1882ndash1888 2000
[56] N R Shah and F Dumler ldquoHypoalbuminaemiamdasha marker ofcardiovascular disease in patients with chronic kidney diseasestages II-IVrdquo International Journal ofMedical Sciences vol 5 no6 pp 366ndash370 2008
[57] N E Straznicky M T Grima E A Lambert et al ldquoExerciseaugments weight loss induced improvement in renal functionin obese metabolic syndrome individualsrdquo Journal of Hyperten-sion vol 29 no 3 pp 553ndash564 2011
[58] R D Manning Jr N Tian and S Meng ldquoOxidative stress andantioxidant treatment in hypertension and the associated renaldamagerdquoAmerican Journal of Nephrology vol 25 no 4 pp 311ndash317 2005
[59] G Keller G Zimmer GMall E Ritz andK Amann ldquoNephronnumber in patients with primary hypertensionrdquo The NewEngland Journal of Medicine vol 348 no 2 pp 101ndash108 2003
[60] J Floege M W Burns C E Alpers et al ldquoGlomerular cellproliferation and PDGF expression precede glomerulosclerosisin the remnant kidney modelrdquo Kidney International vol 41 no2 pp 297ndash309 1992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 BioMed Research International
at which RRT rates are increasing that is most concerningStatistical analyses have indicated by the year 2020 thatRRT prevalence is expected to increase by 29 with anaccompanying 37 increase in RRT-related expenditure [5]The sharp increase in RRT is largely due to associatedincreases in risk factors including obesity [6] physical inac-tivity [6] and hypertension [7] CKD-related hypertensionis especially noteworthy as hypertension is closely associatedwith declining eGFR independent of other risk factors [8 9]This hypertension-associated decline in eGFR is one reasonprior to commencing RRT the most common CKD-relatedtreatments focus on reducing hypertension The rationalebehind this approach is threefold (1) CKD is an indepen-dent risk factor for cardiac events [10 11] (2) controllinghypertension is the best way to influence quality of life [12]and prognosis [13 14] in CKD patients (3) hypertension isthe most influential modifiable-factor associated with CKDprogression [15]
Central to the concept of hypertension is the reninangiotensin aldosterone system (RAAS) a general termapplied to the network of enzymes and hormones thatregulate blood pressure [16] RAAS is characterised by renina protein encoded by the gene Ren that cleaves a peptidebond on angiotensinogen a protein encoded by the geneAgt resulting in angiotensin I [17] Although angiotensin I isbiologically inactive on its own it is converted to angiotensinII by angiotensin-converting enzyme [17] a protein encodedby the geneAceThe resulting angiotensin II influences bloodpressure by potentially binding to angiotensin II receptortype 1 [17] a receptor encoded by the genes Agtr1a andAgtr1b on intraglomerular mesangial cells causing them tocontract along with surrounding blood vessels In additionangiotensin II regulates the expression ofCyp11b2 a gene thatencodes the enzyme aldosterone synthase the enzyme thatsynthesises aldosterone [17] Once synthesised aldosteronepromotes the reabsorption of sodiumandwater in the tubulesof the kidney leading to increased blood volume whichresults in increased blood pressure [18] Considering thisit is apparent that intervention-based research focused onmodulating the activityexpression of the aforementionedRAAS-related compounds is timely
Chronic aerobic exercise training has emerged as apromising therapy in terms of reducing or regulating hyper-tension [19ndash21] Considering that CKD progression is closelyrelated to progressive hypertension [9 22] chronic aerobicexercise training may be especially beneficial in patientswith early-stage CKD who hope to avoid or delay the needfor RRT Recently high intensity interval training (HIIT)(asymp85 VO
2max) has been the focus of many cliniciansand researchers [23] who hypothesise that HIIT may elicitgreater benefits compared to traditional aerobic exercise(LIT) (asymp50 VO
2max) [24ndash26] Reasons for this suppositioninclude improved cardiovascular [24ndash26] and metabolic [23]outcomes In addition HIIT is also safe for many high-risk populations [26] including patients with CKD [27]This paired with the fact that HIIT encourages adherenceto aerobic exercise training programs [28] makes HIITan attractive therapeutic option for clinicians who aim to
regulate bloodpressure anddelay the need forRRT in patientswith CKD
Although it has been established that aerobic exercisebeneficially affects blood pressure investigations that focuson the direct effects of HIIT on the molecular components ofRAAS especially in models of early-stage CKD are unavail-able Moreover the underlying molecular mechanisms thatallow for increased benefit in HIIT compared to traditionalaerobic exercise have yet to be describedThis is largely due tothe fact that studies conducting tissue-specific analyses of themolecular markers involved in RAAS are difficult to performinhumans necessitating the need for animalmodels As suchthe purpose of the present study is to determine the effects ofchronic HIIT (4 times per week for 8 weeks) on the mRNAexpression of several key RAAS-related genes (Ren Agt AceAgtr1a Agtr1b and Cyp11b2) as well as traditional clinicalmarkers of CKD (creatinine albumin total cholesterol high-density lipoprotein low-density lipoprotein triglyceridesblood pressure body weight kidney weight and kidneyweight-body weight ratio) in an animal model of early-stage CKD It was hypothesised that HIIT would exert amore beneficial effect on RAAS-related mRNA expressionand traditional CKD-related clinical markers compared to asedentary (SED) condition and LIT
2 Materials and Methods21 Animals and General Overview Male spontaneouslyhypertensive rats (SHR) (119899 = 39) (Animal Resource CentreCanning Vale WA Australia) were housed in a temperature-controlled room (22ndash25∘C) with a dark-light cycle of 12 12hours and provided with ad libitum access to standardlaboratory chow and water At the time of arrival ratswere 4-5 weeks old Following a 2-week habituation periodallowing for acclimatisation to their new environment allrats underwent a unilateral nephrectomy (6-7 weeks old)Following surgery rats were allowed to recover for 2 weeks(8-9 weeks old) prior to the initiation of an 8-week aerobicexercise intervention Blood pressures body weights andbody lengths were recorded at baseline (preexercise) 4weeks (mid-intervention) and 8 weeks (postintervention)Following the 8-week intervention rats were euthanised24 hours following their last bout of exercise and tissueswere collected for subsequent analysis (16-17 weeks old)All research procedures were granted prior approval by aninstitutional Animal Ethics Committee
22 Anesthetisation andEuthanasia Procedures Prior to neph-rectomy rats were anesthetised with Zoletil (25mgkg) andXylazine (10mgkg) For pain relief Meloxicam (2mgkg)was injected once daily for 2 days following nephrectomyPrior to blood pressure readings rats were anesthetised withZoletil (25mgkg) Saline was injected subcutaneously fol-lowing each anesthetisation to help avoid dehydration Priorto being euthanised rats were given a Lethabarb injection(15mgkg)
23 Disease Modelling To mimic early-stage CKD a reduc-tion in renal function was induced by performing a unilateral
BioMed Research International 3
nephrectomy Briefly a small lumbar incision was made andthe left kidney was removed from each rat In addition tonephrectomising the rats SHRs were used to mimic the ele-vated blood pressure that is common inCKD Formore infor-mation regarding the disease model used in this study as wellas rationale refer to Supplement 1 in SupplementaryMaterialavailable online at httpdxdoiorg1011552015156584
24 Exercise Protocol Rats were randomly assigned to oneof three treatment groups sedentary (SED 119899 = 12) lightintensity aerobic exercise (LIT 119899 = 13) and high intensityinterval aerobic exercise (HIIT 119899 = 14) The number ofanimals assigned to each group was dependent on the formof exercise as the possibility existed that aerobic exercise mayhave proven too strenuous resulting in the need to withdrawan animal from the experiment However there were noadverse events in any group suggesting that aerobic exercisewas well-tolerated in this disease model
At 8-9 weeks of age rats in the LIT and HIIT wereintroduced to treadmill running for 8 weeks An identical 5-minute warm-up (15mmin) was performed by both traininggroups before each exercise session The LIT group exercisedat a treadmill speed of 15mmin with an incline of 1∘ (45ndash50 VO
2max) [29] up to 33 minutes per day 4 days perweek for 8 weeks The HIIT group exercised at a treadmillspeed of up to 50mmin with an incline of up to 10∘ (asymp85VO2max) [29] 30minutes per day (2-minute stationary period
followed by 1-minute sprinttimes 10 repetitions) 4 days per weekfor 8 weeks Differing treadmill inclines were used to achievethe desired intensity To permit adequate adaptation totreadmill running thereby allowing each exercise session tobe completed in its entirety exercise training was progressiveBy the beginning of the fourth week of training all rats wereperforming exercise sessions atmaximum intensitydurationthe exercise effort remained constant for the remaining 5weeks of training In an effort to standardise variables relatedto exercise training while simultaneously allowing for thecomparison of different forms sessions between LIT andHIITwerematched based on distance travelled per boutThatis despite the difference in exercisemodality between groupsLIT and HIIT travelled the same distance (plusmn1 meter) duringeach exercise session with distances progressing in unisonfrom asymp200 meters per session in week 1 to asymp500 meters persession in week 8 (Table 1)
25 Tissue Homogenisation and mRNA Isolation Tissuesused for analyses were chosen based on tissue-specifictranscriptomic work performed in SHRs [30] Renal tissuespecifically consisted of renal cortex asmRNA is differentiallyexpressed dependent on the type of renal tissue [31] For thesake of consistency hepatic tissue specifically consisted of theouter portion of the right lateral lobe
Approximately 100mg (plusmn10mg) of renal (for analysisof Ren Ace Agtr1b and Cyp11b2 mRNA) and hepatic (foranalysis of Agt and Agtr1a mRNA) tissue was homogenisedin 1mLof TRI-reagent using theTRI-reagentmethod (SigmaAldrich St Louis MO USA) Samples were then centrifugedat 12000timesg for 10 minutes at 4∘C The resulting supernatantwas transferred to a new microtube and incubated for 5
minutes at room temperature to allow for disassociation ofthe nucleoprotein complex Following incubation 02mL ofchloroform was added before this solution was mixed andthen incubated for 3 minutes Samples were then centrifugedat 12000timesg for 15 minutes at 4∘C The resulting supernatantwas transferred to a new microtube Following this sepa-ration 500120583L of 2-propanol was added to each microtubeMicrotubes were incubated at room temperature for 10minutes and then centrifuged at 12000timesg for 10 minutes at4∘C The resulting supernatant was removed leaving behinda mRNA pellet The mRNA pellet was exposed to 2 ethanolwashes (1mL 75) Following each wash microtubes werevortexed and centrifuged at 7500timesg for 5 minutes at 4∘CThe mRNA pellets were then allowed to air dry under afume hood before being dissolved in 30 120583L of RNase-freewater A 260280 ratio was calculated to assess mRNA puritywith all ratios falling within commonly accepted parameters(260280 ratio of 19ndash21) (NanoDrop 2000c Thermo Sci-entific Wilmington DE USA) The diluted mRNA sampleswere stored at minus80∘C until later analyses
26 Total mRNA Determination and Reverse Transcrip-tion Total mRNA concentrations from each sample weredetermined using a spectrophotometer (NanoDrop 2000cThermo Scientific Wilmington DE USA) Next mRNAconcentrations were adjusted to 400 ng120583L by diluting thecrude total mRNA extracts with RNase-free water Thestandardised solutions of total cellular mRNA were reversetranscribed to synthesise complimentaryDNA (cDNA) usinga High Capacity cDNA Reverse Transcription Kit (AppliedBiosystems Foster City CA USA) Briefly 2x RT mastermix was prepared per kit instructions Next 10 120583L of RT mixwas added (and mixed via pipette trituration) to 10 120583L of thestandardised mRNA solution These samples were placed ona thermal cycler (T100Thermal Cycler Bio-Rad GladesvilleNSW Australia) set to run at 25∘C for 10 minutes 37∘Cfor 120 minutes and 85∘C for 5 minutes Following reversetranscription the resulting cDNA template concentrationswere diluted to 5 ng120583L by adding RNase-free water Thestandardised cDNA solutions were frozen at minus80∘C untilquantitative reverse transcription polymerase chain reaction(qRT-PCR) was performed
27 Quantitative Reverse Transcription Polymerase ChainReaction Analysis Forward and reverse oligonucleotideprimer pairs were developed using National Centre forBiotechnology Informationrsquos (NCBI Bethesda MD USA)Primer Designer Tool before being commercially synthesised(GeneWorks Hindmarsh SA Australia) (Table 2) Gapdhwas used as an internal reference gene for detecting relativechange in the quantity of target mRNA due to its consid-eration as a constitutively expressed housekeeping gene fol-lowing aerobic exercise training Following the examinationof primer efficiencies qRT-PCR reactions were mixed Reac-tions contained the following mixture 25120583L of preparedcDNA template 5 120583L of SYBR Select Master Mix (Life Tech-nologies Mulgrave Victoria Australia) 05 120583L of sense andantisense primers and 15 120583L RNase-free water Followingthe mixture of each reaction qRT-PCR was performed with
4 BioMed Research International
Table 1 Detailed exercise protocol
Group Variable Measure Wk 1 Wk 2 Wk 3 Wk 4 Wk 5 Wk 6 Wk 7 Wk 8SED NA NA NA NA NA NA NA NA NA NA
LIT45ndash50 VO2max
Max speed MetersMin 15 15 15 15 15 15 15 15Incline Degrees 1 1 1 1 1 1 1 1Duration Minutes 133 20 266 333 333 333 333 333Intensity Constant treadmill speed and constant treadmill inclineFrequency BoutsWk 4 4 4 4 4 4 4 4
Distance per bout Meters 1995 300 399 4995 4995 4995 4995 4995Distance per week Meters 798 1200 1596 1998 1998 1998 1998 1998
HIITasymp85 VO2max
Max speed MetersMin 20 30 40 50 50 50 50 50Incline Degrees 5 10 10 10 10 10 10 10Duration Minutes 30 30 30 30 30 30 30 30Intensity 2min stationary period followed by 1min sprint period times 10 repsFrequency BoutsWk 4 4 4 4 4 4 4 4
Distance per bout Meters 200 300 400 500 500 500 500 500Distance per week Meters 800 1200 1600 2000 2000 2000 2000 2000
Identical 5-min warm-up (15mmin) was performed by both training groups prior to each exercise bout
Table 2 Primer sequences
Target Primer sequence (51015840-31015840)Angiotensin I converting enzyme (Ace) forward CTTGACCCTGGATTGCAGCCAngiotensin I converting enzyme (Ace) reverse GTTTCGTGAGGAAGCCAGGAAngiotensin II receptor type 1a (Agtr1a) forward AGTCCTGTTCCACCCGATCAAngiotensin II receptor type 1a (Agtr1a) reverse TCCAGACAAAATGCCAGCCAAngiotensin II receptor type 1b (Agtr1b) forward ACTGCACACGGTGCATTTTAAngiotensin II receptor type 1b (Agtr1b) reverse TAATTGTGCCTGCCAGCCTTAngiotensinogen (serpin peptidase inhibitor clade A member 8) (Agt) forward CTGGAGCTAAAGGACACACAGAAngiotensinogen (serpin peptidase inhibitor clade A member 8) (Agt) reverse GTGAAGGGACCCAAGCTCTCCytochrome P450 family 11 subfamily b polypeptide 2 (Cyp11b2) forward TAACTCAGGGAGCTTTACCTCTCytochrome P450 family 11 subfamily b polypeptide 2 (Cyp11b2) reverse CTGAGACCCTTTGAAGGCCGRenin (Ren) forward CCGTGGTCCTCACCAACTACRenin (Ren) reverse CTTGGCCAGCATGAAGGGTAGlyceraldehyde-3-phosphate dehydrogenase (Gapdh) forward GTTACCAGGGCTGCCTTCTCGlyceraldehyde-3-phosphate dehydrogenase (Gapdh) reverse GATGGTGATGGGTTTCCCGT
a thermal cycler (Rotor-Gene Q Qiagen Venlo Nether-lands) The amplification sequence involved an initial 10-minute cycle at 95∘C followed by 40 cycles each composedof a denaturation step (95∘C for 15 seconds) and a primerannealingextension step (60∘C for 45 seconds) Meltingcurves were performed to ensure that sufficient PCR productwas being generated by each primer in the absence of primerdimers All assays were performed in duplicate (coefficientof variation = 001) mRNA expression data were calculatedusing the Livak method [32] and data are presented as thefold change of the gene of interest relative to that of controlanimals (SED)
28 Clinical Markers in Plasma All bloodplasma markerswere assessed using blood taken from the descending aorta
of each rat Blood was collected into EDTA tubes followinglethal injection directly after the thoracic cavity of the animalhad been opened before tissues were collected This bloodwas centrifuged for 10 minutes at 1500timesg and the resultingplasma was aliquoted to 20mL microtubes and frozen atminus80∘C until it was analysed
Plasma triglyceridesweremeasured using a commerciallyavailable assay kit (Abcam Cambridge England UnitedKingdom) Briefly standards were prepared per the kitinstructions Next 25120583L of plasma was combined with assaybuffer in the well of a 96-well plate Lipase (2120583L) was addedto each well and solutions were mixed before incubating for20 minutes at room temperature Triglyceride reaction mixwas added to each well and solutions were mixed beforeincubating for 60 minutes at room temperature Triglycerideconcentrations were measured colorimetrically
BioMed Research International 5
Plasma high-density lipoprotein (HDL) and low-densitylipoprotein (LDL) were measured using a commerciallyavailable assay kit (Abcam Cambridge England UnitedKingdom) HDL and LDL fractions of plasma sampleswere separated per the kit instructions and standards wereprepared Next 15 120583L of HDL and LDL fractions was firstcombined with cholesterol assay buffer followed by reactionmix Solutions were mixed and then allowed to incubatefor 60 minutes at 37∘C HDL and LDL concentrations weremeasured colorimetrically Total cholesterol was calculatedusing a variation of the Friedlander formula [33]
Plasma creatinine was measured using a commerciallyavailable assay kit (Abcam Cambridge England UnitedKingdom) Standards were prepared per the kit instructionsNext 25 120583L of plasma was combined with assay buffer inthe well of a 96-well plate Reaction mix was added tothis solution and samples were allowed to incubate at 37∘Cfor 60 minutes Creatinine concentrations were measuredcolorimetrically
Plasma albumin was measured using a commerciallyavailable enzyme-linked immunosorbent assay (ELISA) kit(Abcam Cambridge England United Kingdom) Standardswere prepared per the kit instructions Plasma samples wereprepared and added to sample wells Biotinylated albuminwas then added to each well and this solution was mixedgently before a 60-minute incubation period Followingseveralwashes 1x Streptavidin-Peroxidase (SP) conjugatewasadded to each well prior to a 30-minute incubation periodOnce again plates were washed and 50120583L of chromogensubstrate was added followed by a 12-minute incubationperiod Stop solution was then added to each well andalbumin concentrations were measured colorimetrically
29 Clinical and Anthropometric Measurements Blood pres-sures body weights and body lengths were recorded beforesurgery baseline (preexercise) 4 weeks (mid-intervention)and 8 weeks (postintervention) Kidney weights wererecorded after intervention Systolic blood pressure (SBP)wasmeasured using data acquisition hardware (PowerLab ADIn-stuments Bella Vista NSW Australia) coupled to a nonin-vasive blood pressure (NIBP) system (NIBP System ADIn-stuments Bella Vista NSW Australia) with a pulse trans-ducercuff (Pulse TransducerPressure Cuff for NIBP ADIn-stuments Bella Vista NSW Australia) Measurements werethen analysed using LabChart 8 (ADInstuments Bella VistaNSW Australia) Body length was measured from tip-of-nose to tip-of-tail Body weight and remnant kidney weightwere measured to the nearest thousandth of a gram Bodylength and body weight measurements were taken whileeach rat was sedated directly prior to SBP measurement
210 Statistics mRNAdata are presented asmean plusmn standarderror of themean (SEM) All other data are presented asmeanplusmn standard deviation (SD) Body length body weight bodylength-body weight ratio and SBP data were analysed using3 times 3 (group times time) repeated measures analysis of variance(RMANOVA) When applicable group effects andor timeeffects were examined using separate one-way ANOVAs withTukey post hoc comparisons Data for all other measures
(mRNA expression plasma markers kidney weight andkidney weight-body weight ratio) were analysed using one-way ANOVAs with Tukey post hoc comparisons Analyseswere performed using IBM SPSS Statistics (v200 IBMCorporation Armonk NY USA) Statistical significance wasset at 119901 lt 005
3 Results
31 Quantitative Reverse Transcription Polymerase ChainReaction Analysis Results pertaining to renal expressionof RAAS-related mRNA can be seen in Figure 1 Resultspertaining to hepatic expression of RAAS-related mRNA canbe seen in Figure 2 Expression of renal Ren Ace Agtr1band Cyp11b2 mRNA and hepatic Agtr1a mRNA was notsignificantly different between groups (119901 gt 005) Expressionof hepatic Agt mRNA was significantly decreased in HIITcompared to LIT (119901 = 0035)
32 Clinical Markers in Plasma Results pertaining to clinicalmarkers in plasma can be seen in Table 3 Plasma measuresLDL (119901 = 0001) triglycerides (119901 = 0029) and totalcholesterol (119901 = 0002) were significantly lower in HIITcompared to LIT Plasma albumin was significantly higher inHIIT compared to SED (119901 = 0001) and LIT (119901 = 0047)
33 Anthropometric Measurements and Kidney WeightResults pertaining to anthropologicalmeasurements and kid-ney weight can be seen in Tables 3 and 4 Body Length bodyweight body length-body weight ratio and SBP increasedsignificantly from baseline to 4Weeks and from 4Weeks to 8Weeks (119901 lt 005) in all groups (Table 4) with no significantgroup interactions Kidney weight was significantly lower inHIIT compared to the SED (119901 = 0028) and LIT (119901 = 0005)Kidney weight-body weight ratio was significantly lower inHIIT compared to the SED (119901 = 0045) and LIT (119901 = 0048)(Table 3)
4 Discussion
The current study examined the ability of varying forms ofaerobic exercise to influence mRNA expression of severalRAAS-related genes as well as commonCKD-related clinicaland anthropometric markers in an animal model of early-stage CKD This is the first investigation to compare theefficacy of varying forms of aerobic exercise as it pertainsto the modulation of tissue-specific mRNA expression ofRAAS-related genes HIIT produced more favourable out-comes compared to SED and LIT in that HIIT resulted insignificantly reduced mRNA expression of Agt (compared toLIT) significantly improved plasma levels of LDL triglyc-erides and total cholesterol (compared to LIT) significantlyimproved plasma levels of albumin (compared to SED andLIT) and significantly reduced remnant kidney weight andkidney weight-body weight ratios (compared to SED andLIT)
Results regarding the mRNA expression of Agt are inter-esting The mRNA expression of all other genes (Ace Ren
6 BioMed Research International
200
160
120
080
040
000
200
160
120
080
040
000
200
160
120
080
040
000
SED (n = 12) LIT (n = 13) HIIT (n = 14) SED (n = 12) LIT (n = 13) HIIT (n = 14)
SED (n = 12) SED (n = 12)LIT (n = 13) HIIT (n = 14) LIT (n = 13) HIIT (n = 14)
100 053 053061 100 034
039 085
Ren-mRNA expression fold change(norm to GAPDH) (norm to GAPDH)
Ace-mRNA expression fold change
(norm to GAPDH)Agtr1b-mRNA expression fold change
(norm to GAPDH)Cyp11b2-mRNA expression fold change
086043100 100
200
160
120
080
040
000
Figure 1 Renal mRNA expression fold change
Agtr1a Agtr1b and Cyp11b2) was nonsignificantly downreg-ulated in both exercise groups compared to SED HoweverAgt mRNA expression was upregulated in LIT compared toSED (not significant) and HIIT (119901 = 0035) It is worthmentioning that our results are not the first data to suggestthat lower intensity aerobic exercise training may result inunfortunate adaptations in animal models of CKD aerobicexercise training performed at 50ndash70 of VO
2max has beenreported to result in increased resting SBP and decreasedmyocardial capillary density in an animal model of CKD[34]
Differential mRNA expression of Agt may partiallyexplain the nonsignificant (119901 = 0074) difference in SBP inHIIT during Week 8 compared to SED (119901 = 014 +528)and LIT (119901 = 074 +601) The downregulation in themRNA expression of Agt in HIIT may also explain the lackof significant differences in other RAAS genes in this studyThat is a decrease in the mRNA expression of Agt may havequenched the need for any additional significant decreases inthe expression of other RAAS genes This may explain whyeven though there was a near-significant reduction in SBPin HIIT compared to LIT (119901 = 0074) mRNA expression
BioMed Research International 7
p = 0035
118
076084
063
200
160
120
080
040
000
200
160
120
080
040
000
SED (n = 12) LIT (n = 13) HIIT (n = 14)
SED (n = 12) LIT (n = 13) HIIT (n = 14)
Agtr1a-mRNA expression fold change(norm to GAPDH)
(norm to GAPDH)Agt-mRNA expression fold change
100
100
Figure 2 Hepatic mRNA expression fold change
of several RAAS-related of genes (Ace Ren Agtr1b andCyp11b2) was slightly but not significantly increased in HIITcompared to LIT A review on hepatic angiotensinogen [35]discusses the noteworthy influence that angiotensinogen hason blood pressure Decreased levels of angiotensinogen usingangiotensinogen-antibodies in rats [36] and Agt-knockoutmice [37] exhibit lower blood pressure relative to controlsConversely angiotensinogen infusion in mice [38] and Agtoverexpression in rats [39] result in increased blood pressureEvidence suggests that angiotensinogen is a more potentinfluencer of blood pressure than previously suspected [35
Table 3 Nonrepeated clinical and anthropometric measures
Clinicalmeasure Group Mean Standard
deviationMean duplicate
CV
HDL (mgmL)SED 082 013
006LIT 088 015HIIT 093 012
LDL (mgmL)SED 127 027
003LIT 155 034HIIT 108lowast 032
TAG (mgmL)SED 565 166
004LIT 635 265HIIT 411lowast 204
CHOL(mgmL)
SED 322 047NALIT 371 061
HIIT 283lowast 073
CRE(nmol120583L)
SED 107 051004LIT 206 179
HIIT 211 126
ALB (mgmL)SED 2623 384
004LIT 2988 642HIIT 3524dagger 608
Kidney weight(g)
SED 157 009NALIT 159 012
HIIT 146dagger 008
KW-BW ratioSED 00050 00003
NALIT 00050 00003HIIT 00047dagger 00002
Significance set at 119901 le 005lowastSignificantly different from LITdaggerSignificantly different from LIT and SEDHDL high density lipoprotein LDL low density lipoprotein TAG triglyc-erides CHOL total cholesterol CRE creatinine ALB albumin KW-BWkidney weight-body weight CV coefficient of variation
39] often more influential than other components of RAAS[40] and deserves more attention as a potential targetin hypertension-related therapies [35] proposals that aresupported by our findings
Large amounts of between-animal variation in themRNAexpression of RAAS-related genes in SED may explain thelack of significant results in the current study Duplicate-duplicate variation was low (CV = 001) suggesting largeamounts of between-animal variation in SED The issueof between-animal mRNA variation has been empiricallyaddressed in the past [41ndash43] with the most commonlysuggested remedy being an increase in sample size Inter-estingly variation in between-animal mRNA expression inSED is higher across all genes (except for Agt) comparedto LIT and HIIT similar to previous work that has exam-ined RAAS-related mRNA expression in sedentary versusexercise-trained SHRs [20 44] This combined with the factthat aerobic exercise resulted in a downregulation across allgenes compared to SED (expect for Agt in LIT) suggeststhat RAAS-related mRNA expression may be poorly and
8 BioMed Research International
Table 4 Repeated clinical and anthropometric measures
Clinical measure Group Baseline 4 Weekslowast 8 Weeksdagger
(Preintervention) (Mid-Intervention) (Postintervention)
Body length (cm)SED 2848 (186) 3503 (085) 3741 (106)LIT 2932 (165) 3515 (079) 3789 (088)HIIT 2961 (225) 3546 (065) 3787 (062)
Body weight (g)SED 22442 (1782) 27605 (1831) 31353 (1662)LIT 23159 (2101) 27742 (2077) 31825 (2103)HIIT 23090 (1998) 27487 (1646) 30816 (1758)
BL-BW ratioSED 0126 (0007) 0127 (0007) 0120 (0004)LIT 0127 (0009) 0128 (0007) 0119 (0009)HIIT 0129 (0007) 0130 (0008) 0124 (0006)
Systolic blood pressure (mmHg)SED 17557 (927) 20777 (1739) 23977 (1285)LIT 17309 (945) 20925 (231) 24163 (2142)HIIT 17465 (1482) 21625 (1624) 22712 (1423)
Values presented as mean (standard deviation)Significance set at 119901 le 005lowastSignificantly different compared to baseline for all groupsdaggerSignificantly different compared to baseline and 4 weeks for all groupsBL-BW body length-body weight
indiscriminately regulated in the absence of aerobic exercisein an animal model of early-stage CKD That is aerobicexercise may help to control otherwise haphazard RAAS-related mRNA expression that occurs during the early stagesof CKD Several informative reviews have outlined theissue of unregulated blood pressure control [45] and morespecifically unregulated RAAS activity [46] in CKD but thisis the first study to suggest that one of the mechanisms bywhich aerobic exercise may prove beneficial is via tightenedcontrol of RAAS-related mRNA expression independentof statistically significant improvements to RAAS-relatedmRNA expression
In the current study the significant decreases in plasmaLDL triglycerides and total cholesterol in HIIT compared toLIT but not SED are encouraging and somewhat surprisingA recent study performed in healthy well-trained humansreported nonsignificant improvements in LDL triglyceridesand total cholesterol after 12 weeks of HIIT [47] In spe-cial andor clinical populations HIIT seems to exert moreinfluence over blood lipids Cardiac rehabilitation patientswho engaged in HIIT experienced significant improvementsin HDL relative to traditional aerobic exercise training[26] However triglyceride measurements were not differentbetween groups and LDL measurements were not reported[26] HIIT has also proven to be beneficial in obese men[48] and women [49] resulting in improved HDL [48]LDL [48] triglycerides [48 49] and total cholesterol [4849] Despite the slowly-accumulating data a recent review[50] that notes the ability of HIIT to influence blood lipidshas yet to be established especially in special populationssuggesting that this specific line of research the effects ofHIIT on blood lipids should be further examined This isespecially true in CKD as lipid-related disorders are theleading cause of complications in CVD [51 52] and CVD-related complications are the leading cause of death in CKD
patients [10 11] As such dyslipidemia should be rankedamong the primary concerns of CKD-related research [53]
Similar to blood lipids a recent review notes that theeffects of exercise training on plasma albumin in patientswith CKD are unclear [54] Moreover data describing theeffects of HIIT on plasma albumin in patients with CKD areunavailable Hypoalbuminemia is an independent predictorof renal dysfunction [55] and an independent predictor ofCVD in early-stage CKD [56] and can be used to identifyCKD patients at increased risk of developing CVD [56] Inobese individuals with metabolic syndrome two commoncharacteristics of CKD 12 weeks of aerobic exercise trainingsignificantly reduced albuminuria (urinary albumin) com-pared to a no-exercise control group [57] Aerobic exercisetraining (16 weeks at 60 of maximal aerobic velocity) hasalso proven useful at reducing albuminuria in SHRs [44]Because hypoalbuminemia is related to declining kidneyfunction [55] blood albumin andor urinary albumin areuseful markers for assessing the preservation of renal tissueIn the current study plasma albumin was significantly higherin HIIT compared to SED and LIT suggesting that renalstructure and function are better preserved by HIIT Thepreservation of renal structure and function and subsequentincrease in plasma albumin may have been due to the down-regulation of Agt mRNA expression and the accompanyingdecrease in SBP in HIIT as hypertension is directly related torenal damage [44 58]
Also considered an indicator of renal damage kid-ney weight and kidney weight-body weight ratio weresignificantly lower in HIIT compared to SED and LITHypertension-related declines in renal function are associ-ated with compensatory alterations to renal tissue such astubulointerstitial fibrosis [59 60] Often pathological thesealterations result in glomerular hypertrophy [59 60] Usinghistological and molecular applications 16 weeks of aerobic
BioMed Research International 9
exercise training (performed at 60 of maximal aerobicvelocity) has been shown to reduce renal fibrosis in SHRs[44] Although renal fibrosis and renal hypertrophy aredirectly related data that specifically describes the effectsof HIIT on renal hypertrophy are unavailable Similar tothe mechanisms that account for increased levels of plasmaalbumin in HIIT there is evidence to suggest that thesignificantly lower kidney weight and kidney weight-bodyweight ratios in HIIT compared to SED and LIT may bedue to decreased fibrosis Decreases in renal fibrosis maybe due to decreases in hypertension-mediated renal damagefollowing a downregulation of the mRNA expression of Agtand a decrease in SBP (in HIIT) [44 58]
5 Conclusions
In summary in an animal model of early-stage CKD HIITappeared to be more beneficial compared to SED and LITas HIIT was responsible for a significant downregulation inthe mRNA expression of Agt The downregulated mRNAexpression of Agt along with significant improvements toblood lipids (LDL triglycerides and total cholesterol) maypartially explain the nonsignificant decrease in SBP andsignificant improvements to plasma albumin kidney weightand kidney weight-body weight ratios in HIIT relative toSED and LIT Future work would benefit from examiningRAAS-related protein expression as well as specific measuresof renal histology and morphology Future work would alsobenefit from examining whether the positive HIIT-relatedeffects seen in the present study are apparent in differentrelated disease models (eg nonnephrectomised SHRs or 56nephrectomy SHRs)
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] AIHW Ed Australiarsquos Health 2014 Australiarsquos Health SeriesAustralian Institute of Health and Welfare (AIHW) CanberraAustralia 2014
[2] A S Go G M Chertow D Fan C E McCulloch andC-Y Hsu ldquoChronic kidney disease and the risks of deathcardiovascular events and hospitalizationrdquo The New EnglandJournal of Medicine vol 351 no 13 pp 1296ndash1370 2004
[3] U D Mathisen T Melsom O C Ingebretsen et al ldquoEstimatedGFR associates with cardiovascular risk factors independentlyof measured GFRrdquo Journal of the American Society of Nephrol-ogy vol 22 no 5 pp 927ndash937 2011
[4] DM Silverstein ldquoInflammation in chronic kidney disease rolein the progression of renal and cardiovascular diseaserdquoPediatricNephrology vol 24 no 8 pp 1445ndash1452 2009
[5] P S Tucker M I Kingsley R H Morton A T Scanlan andV J Dalbo ldquoThe increasing financial impact of chronic kidneydisease in Australiardquo International Journal of Nephrology vol2014 Article ID 120537 7 pages 2014
[6] B Stengel M E Tarver-Carr N R Powe M S Eberhardt andF L Brancati ldquoLifestyle factors obesity and the risk of chronickidney diseaserdquo Epidemiology vol 14 no 4 pp 479ndash487 2003
[7] R T Gansevoort R Correa-Rotter B R Hemmelgarn et alldquoChronic kidney disease and cardiovascular risk epidemiologymechanisms and preventionrdquoTheLancet vol 382 no 9889 pp339ndash352 2013
[8] M M H Hermans R Henry J M Dekker et al ldquoEstimatedglomerular filtration rate and urinary albumin excretion areindependently associated with greater arterial stiffness theHoorn studyrdquo Journal of the American Society of Nephrology vol18 no 6 pp 1942ndash1952 2007
[9] M L Ford L A Tomlinson T P E Chapman C Rajkumar andS G Holt ldquoAortic stiffness is independently associated with rateof renal function decline in chronic kidney disease stages 3 and4rdquo Hypertension vol 55 no 5 pp 1110ndash1115 2010
[10] D EWeiner H Tighiouart P C Stark et al ldquoKidney disease asa risk factor for recurrent cardiovascular disease andmortalityrdquoAmerican Journal of Kidney Diseases vol 44 no 2 pp 198ndash2062004
[11] D E Weiner H Tighiouart M G Amin et al ldquoChronickidney disease as a risk factor for cardiovascular disease and all-causemortality a pooled analysis of community-based studiesrdquoJournal of the American Society of Nephrology vol 15 no 5 pp1307ndash1315 2004
[12] R K Soni A C Porter J P Lash and M L Unruh ldquoHealth-related quality of life in hypertension chronic kidney diseaseand coexistent chronic health conditionsrdquo Advances in ChronicKidney Disease vol 17 no 4 pp e17ndashe26 2010
[13] J Segura C Campo P Gil et al ldquoDevelopment of chronickidney disease and cardiovascular prognosis in essential hyper-tensive patientsrdquo Journal of the American Society of Nephrologyvol 15 no 6 pp 1616ndash1622 2004
[14] J Blacher A P Guerin B Pannier S J Marchais M E Safarand G M London ldquoImpact of aortic stiffness on survival inend-stage renal diseaserdquo Circulation vol 99 no 18 pp 2434ndash2439 1999
[15] G L Bakris E Ritz and World Kidney Day Steering Commit-tee ldquoThe message for World Kidney Day 2009 hypertensionand kidney disease a marriage that should be preventedrdquo TheJournal of Clinical Hypertension (Greenwich) vol 11 no 3 pp144ndash147 2009
[16] J L Lavoie and C D Sigmund ldquoMinireview overview ofthe renin-angiotensin systemmdashan endocrine and paracrinesystemrdquo Endocrinology vol 144 no 6 pp 2179ndash2183 2003
[17] A Nguyen Dinh Cat and RM Touyz ldquoA new look at the renin-angiotensin systemmdashfocusing on the vascular systemrdquo Peptidesvol 32 no 10 pp 2141ndash2150 2011
[18] U C Brewster and M A Perazella ldquoThe renin-angiotensin-aldosterone system and the kidney effects on kidney diseaserdquoThe American Journal of Medicine vol 116 no 4 pp 263ndash2722004
[19] S Ciampone R Borges I P De Lima F F Mesquita EC Cambiucci and J A R Gontijo ldquoLong-term exerciseattenuates blood pressure responsiveness andmodulates kidneyangiotensin II signalling and urinary sodium excretion in SHRrdquoJournal of the Renin-Angiotensin-Aldosterone System vol 12 no4 pp 394ndash403 2011
[20] D Agarwal M A Welsch J N Keller and J Francis ldquoChronicexercise modulates RAS components and improves balancebetween pro- and anti-inflammatory cytokines in the brain of
10 BioMed Research International
SHRrdquo Basic Research in Cardiology vol 106 no 6 pp 1069ndash1085 2011
[21] E J Howden R G Fassett N M Isbel and J S CoombesldquoExercise training in chronic kidney disease patientsrdquo SportsMedicine vol 42 no 6 pp 473ndash488 2012
[22] S Nielsen A Schmitz M Rehling and C E Mogensen ldquoSys-tolic blood pressure relates to the rate of decline of glomerularfiltration rate in type II diabetesrdquo Diabetes Care vol 16 no 11pp 1427ndash1432 1993
[23] A E Tjoslashnna I M Leinan A T Bartnes et al ldquoLow- and high-volume of intensive endurance training significantly improvesmaximal oxygen uptake after 10-weeks of training in healthymenrdquo PLoS ONE vol 8 no 5 Article ID e65382 2013
[24] T Moholdt E Madssen Oslash Rognmo and I L Aamot ldquoThehigher the better Interval training intensity in coronary heartdiseaserdquo Journal of Science and Medicine in Sport vol 17 no 5pp 506ndash510 2014
[25] H E Molmen-Hansen T Stolen A E Tjonna et al ldquoAerobicinterval training reduces blood pressure and improves myocar-dial function in hypertensive patientsrdquo European Journal ofPreventive Cardiology vol 19 no 2 pp 151ndash160 2012
[26] T Moholdt I L Aamot I Granoslashien et al ldquoAerobic intervaltraining increases peak oxygen uptake more than usual careexercise training in myocardial infarction patients a random-ized controlled studyrdquo Clinical Rehabilitation vol 26 no 1 pp33ndash44 2012
[27] E J Howden J S Coombes H Strand B Douglas K LCampbell and N M Isbel ldquoExercise training in CKD efficacyadherence and safetyrdquoAmerican Journal of KidneyDiseases vol65 no 4 pp 583ndash591 2015
[28] A C KingW L Haskell D R Young R K Oka andM L Ste-fanick ldquoLong-term effects of varying intensities and formats ofphysical activity on participation rates fitness and lipoproteinsin men and women aged 50 to 65 yearsrdquo Circulation vol 91 no10 pp 2596ndash2604 1995
[29] G A Brooks and T P White ldquoDetermination of metabolicand heart rate responses of rats to treadmill exerciserdquo Journalof Applied Physiology Respiratory Environmental and ExercisePhysiology vol 45 no 6 pp 1009ndash1015 1978
[30] Y Yu J C Fuscoe C Zhao et al ldquoA rat RNA-Seq transcriptomicBodyMap across 11 organs and 4 developmental stagesrdquo NatureCommunications vol 5 article 3230 2014
[31] F Z Marques A E Campain M Tomaszewski et al ldquoGeneexpression profiling reveals renin mRNA overexpression inhuman hypertensive kidneys and a role formicroRNAsrdquoHyper-tension vol 58 no 6 pp 1093ndash1098 2011
[32] K J Livak and T D Schmittgen ldquoAnalysis of relative geneexpression data using real-time quantitative PCRand the 2minusΔΔ119862TmethodrdquoMethods vol 25 no 4 pp 402ndash408 2001
[33] Y Friedlander J D Kark S Eisenberg and Y Stein ldquoCalcula-tion of LDL-cholesterol from total cholesterol triglyceride andHDL-cholesterol a comparison of methods in the JerusalemLipid Research Clinic Prevalence Studyrdquo Israel Journal of Medi-cal Sciences vol 18 no 12 pp 1242ndash1252 1982
[34] K DMarcus andCM Tipton ldquoExercise training and its effectswith renal hypertensive ratsrdquo Journal of Applied Physiology vol59 no 5 pp 1410ndash1415 1985
[35] K Kitada H Kobori and A Nishiyama ldquoLiver-specificangiotensinogen suppression an old yet novel target forblood pressure control through RAS inhibitionrdquo HypertensionResearch vol 37 no 5 pp 393ndash394 2014
[36] J Gardes J Bouhnik E Clauser P Corvol and JMenard ldquoRoleof angiotensinogen in blood pressure homeostasisrdquo Hyperten-sion vol 4 no 2 pp 185ndash189 1982
[37] K Tanimoto F Sugiyama Y Goto et al ldquoAngiotensinogen-deficient mice with hypotensionrdquo The Journal of BiologicalChemistry vol 269 no 50 pp 31334ndash31337 1994
[38] S Kimura J J Mullins B Bunnemann et al ldquoHigh bloodpressure in transgenic mice carrying the rat angiotensinogengenerdquoThe EMBO Journal vol 11 no 3 pp 821ndash827 1992
[39] JMenard A-I K El Amrani F Savoie J Bouhnik K R LynchandM J Peach ldquoAngiotensinogen an attractive and underratedparticipant in hypertension and inflammationrdquo Hypertensionvol 18 no 5 pp 705ndash707 1991
[40] S Agrawal S Agarwal and S Naik ldquoGenetic contributionand associated pathophysiology in end-stage renal diseaserdquoTheApplication of Clinical Genetics vol 3 pp 65ndash84 2010
[41] W-C Cheng W-Y Shu C-Y Li et al ldquoIntra- and inter-individual variance of gene expression in clinical studiesrdquo PLoSONE vol 7 no 6 Article ID e38650 2012
[42] A Whitehead and D L Crawford ldquoVariation in tissue-specificgene expression among natural populationsrdquo Genome Biologyvol 6 no 2 article R13 2005
[43] A L Oberg B M Bot D E Grill G A Poland and TM Therneau ldquoTechnical and biological variance structure inmRNA-Seq data life in the real worldrdquo BMC Genomics vol 13no 1 article 304 2012
[44] D Agarwal C M Elks S D Reed N Mariappan D SA Majid and J Francis ldquoChronic exercise preserves renalstructure and hemodynamics in spontaneously hypertensiveratsrdquo Antioxidants amp Redox Signaling vol 16 no 2 pp 139ndash1522012
[45] P Zamboli L De Nicola R Minutolo V Bertino F Catapanoand G Conte ldquoManagement of hypertension in chronic kidneydiseaserdquoCurrentHypertensionReports vol 8 no 6 pp 497ndash5012006
[46] G Remuzzi N Perico M Macia and P Ruggenenti ldquoThe roleof renin-angiotensin-aldosterone system in the progression ofchronic kidney diseaserdquo Kidney International vol 68 no 99pp S57ndashS65 2005
[47] N Ouerghi M Feki N Kaabachi M Khammassi S Boukor-raa and A Bouassida ldquoEffects of a high-intensity intermittenttraining programon aerobic capacity and lipid profile in trainedsubjectsrdquoOpenAccess Journal of SportsMedicine vol 5 pp 243ndash248 2014
[48] A Paoli Q F Pacelli T Moro et al ldquoEffects of high-intensitycircuit training low-intensity circuit training and endurancetraining on blood pressure and lipoproteins in middle-agedoverweight menrdquo Lipids in Health and Disease vol 12 no 1article 131 2013
[49] G Racil O Ben Ounis O Hammouda et al ldquoEffects of highvs Moderate exercise intensity during interval training onlipids and adiponectin levels in obese young femalesrdquo EuropeanJournal of Applied Physiology vol 113 no 10 pp 2531ndash25402013
[50] H S Kessler S B Sisson and K R Short ldquoThe potentialfor high-intensity interval training to reduce cardiometabolicdisease riskrdquo Sports Medicine vol 42 no 6 pp 489ndash509 2012
[51] J Poss F Custodis CWernerOWeingartnerM Bohm andULaufs ldquoCardiovascular disease and dyslipidemia beyond LDLrdquoCurrent Pharmaceutical Design vol 17 no 9 pp 861ndash870 2011
BioMed Research International 11
[52] J R Burnett ldquoLipids lipoproteins atherosclerosis and cardio-vascular diseaserdquoThe Clinical Biochemist Reviews vol 25 no 1p 2 2004
[53] G Piecha M Adamczak and E Ritz ldquoDyslipidemia in chronickidney disease pathogenesis and interventionrdquo Polskie Archi-wum Medycyny Wewnetrznej vol 119 no 7-8 pp 487ndash4922009
[54] N A Smart A D Williams I Levinger et al ldquoExercise ampSports Science Australia (ESSA) position statement on exerciseand chronic kidney diseaserdquo Journal of Science and Medicine inSport vol 16 no 5 pp 406ndash411 2013
[55] S-J Pinto-Sietsma W M T Janssen H L Hillege G NavisD de Zeeuw and P E de Jong ldquoUrinary albumin excretion isassociated with renal functional abnormalities in a nondiabeticpopulationrdquo Journal of the American Society of Nephrology vol11 no 10 pp 1882ndash1888 2000
[56] N R Shah and F Dumler ldquoHypoalbuminaemiamdasha marker ofcardiovascular disease in patients with chronic kidney diseasestages II-IVrdquo International Journal ofMedical Sciences vol 5 no6 pp 366ndash370 2008
[57] N E Straznicky M T Grima E A Lambert et al ldquoExerciseaugments weight loss induced improvement in renal functionin obese metabolic syndrome individualsrdquo Journal of Hyperten-sion vol 29 no 3 pp 553ndash564 2011
[58] R D Manning Jr N Tian and S Meng ldquoOxidative stress andantioxidant treatment in hypertension and the associated renaldamagerdquoAmerican Journal of Nephrology vol 25 no 4 pp 311ndash317 2005
[59] G Keller G Zimmer GMall E Ritz andK Amann ldquoNephronnumber in patients with primary hypertensionrdquo The NewEngland Journal of Medicine vol 348 no 2 pp 101ndash108 2003
[60] J Floege M W Burns C E Alpers et al ldquoGlomerular cellproliferation and PDGF expression precede glomerulosclerosisin the remnant kidney modelrdquo Kidney International vol 41 no2 pp 297ndash309 1992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 3
nephrectomy Briefly a small lumbar incision was made andthe left kidney was removed from each rat In addition tonephrectomising the rats SHRs were used to mimic the ele-vated blood pressure that is common inCKD Formore infor-mation regarding the disease model used in this study as wellas rationale refer to Supplement 1 in SupplementaryMaterialavailable online at httpdxdoiorg1011552015156584
24 Exercise Protocol Rats were randomly assigned to oneof three treatment groups sedentary (SED 119899 = 12) lightintensity aerobic exercise (LIT 119899 = 13) and high intensityinterval aerobic exercise (HIIT 119899 = 14) The number ofanimals assigned to each group was dependent on the formof exercise as the possibility existed that aerobic exercise mayhave proven too strenuous resulting in the need to withdrawan animal from the experiment However there were noadverse events in any group suggesting that aerobic exercisewas well-tolerated in this disease model
At 8-9 weeks of age rats in the LIT and HIIT wereintroduced to treadmill running for 8 weeks An identical 5-minute warm-up (15mmin) was performed by both traininggroups before each exercise session The LIT group exercisedat a treadmill speed of 15mmin with an incline of 1∘ (45ndash50 VO
2max) [29] up to 33 minutes per day 4 days perweek for 8 weeks The HIIT group exercised at a treadmillspeed of up to 50mmin with an incline of up to 10∘ (asymp85VO2max) [29] 30minutes per day (2-minute stationary period
followed by 1-minute sprinttimes 10 repetitions) 4 days per weekfor 8 weeks Differing treadmill inclines were used to achievethe desired intensity To permit adequate adaptation totreadmill running thereby allowing each exercise session tobe completed in its entirety exercise training was progressiveBy the beginning of the fourth week of training all rats wereperforming exercise sessions atmaximum intensitydurationthe exercise effort remained constant for the remaining 5weeks of training In an effort to standardise variables relatedto exercise training while simultaneously allowing for thecomparison of different forms sessions between LIT andHIITwerematched based on distance travelled per boutThatis despite the difference in exercisemodality between groupsLIT and HIIT travelled the same distance (plusmn1 meter) duringeach exercise session with distances progressing in unisonfrom asymp200 meters per session in week 1 to asymp500 meters persession in week 8 (Table 1)
25 Tissue Homogenisation and mRNA Isolation Tissuesused for analyses were chosen based on tissue-specifictranscriptomic work performed in SHRs [30] Renal tissuespecifically consisted of renal cortex asmRNA is differentiallyexpressed dependent on the type of renal tissue [31] For thesake of consistency hepatic tissue specifically consisted of theouter portion of the right lateral lobe
Approximately 100mg (plusmn10mg) of renal (for analysisof Ren Ace Agtr1b and Cyp11b2 mRNA) and hepatic (foranalysis of Agt and Agtr1a mRNA) tissue was homogenisedin 1mLof TRI-reagent using theTRI-reagentmethod (SigmaAldrich St Louis MO USA) Samples were then centrifugedat 12000timesg for 10 minutes at 4∘C The resulting supernatantwas transferred to a new microtube and incubated for 5
minutes at room temperature to allow for disassociation ofthe nucleoprotein complex Following incubation 02mL ofchloroform was added before this solution was mixed andthen incubated for 3 minutes Samples were then centrifugedat 12000timesg for 15 minutes at 4∘C The resulting supernatantwas transferred to a new microtube Following this sepa-ration 500120583L of 2-propanol was added to each microtubeMicrotubes were incubated at room temperature for 10minutes and then centrifuged at 12000timesg for 10 minutes at4∘C The resulting supernatant was removed leaving behinda mRNA pellet The mRNA pellet was exposed to 2 ethanolwashes (1mL 75) Following each wash microtubes werevortexed and centrifuged at 7500timesg for 5 minutes at 4∘CThe mRNA pellets were then allowed to air dry under afume hood before being dissolved in 30 120583L of RNase-freewater A 260280 ratio was calculated to assess mRNA puritywith all ratios falling within commonly accepted parameters(260280 ratio of 19ndash21) (NanoDrop 2000c Thermo Sci-entific Wilmington DE USA) The diluted mRNA sampleswere stored at minus80∘C until later analyses
26 Total mRNA Determination and Reverse Transcrip-tion Total mRNA concentrations from each sample weredetermined using a spectrophotometer (NanoDrop 2000cThermo Scientific Wilmington DE USA) Next mRNAconcentrations were adjusted to 400 ng120583L by diluting thecrude total mRNA extracts with RNase-free water Thestandardised solutions of total cellular mRNA were reversetranscribed to synthesise complimentaryDNA (cDNA) usinga High Capacity cDNA Reverse Transcription Kit (AppliedBiosystems Foster City CA USA) Briefly 2x RT mastermix was prepared per kit instructions Next 10 120583L of RT mixwas added (and mixed via pipette trituration) to 10 120583L of thestandardised mRNA solution These samples were placed ona thermal cycler (T100Thermal Cycler Bio-Rad GladesvilleNSW Australia) set to run at 25∘C for 10 minutes 37∘Cfor 120 minutes and 85∘C for 5 minutes Following reversetranscription the resulting cDNA template concentrationswere diluted to 5 ng120583L by adding RNase-free water Thestandardised cDNA solutions were frozen at minus80∘C untilquantitative reverse transcription polymerase chain reaction(qRT-PCR) was performed
27 Quantitative Reverse Transcription Polymerase ChainReaction Analysis Forward and reverse oligonucleotideprimer pairs were developed using National Centre forBiotechnology Informationrsquos (NCBI Bethesda MD USA)Primer Designer Tool before being commercially synthesised(GeneWorks Hindmarsh SA Australia) (Table 2) Gapdhwas used as an internal reference gene for detecting relativechange in the quantity of target mRNA due to its consid-eration as a constitutively expressed housekeeping gene fol-lowing aerobic exercise training Following the examinationof primer efficiencies qRT-PCR reactions were mixed Reac-tions contained the following mixture 25120583L of preparedcDNA template 5 120583L of SYBR Select Master Mix (Life Tech-nologies Mulgrave Victoria Australia) 05 120583L of sense andantisense primers and 15 120583L RNase-free water Followingthe mixture of each reaction qRT-PCR was performed with
4 BioMed Research International
Table 1 Detailed exercise protocol
Group Variable Measure Wk 1 Wk 2 Wk 3 Wk 4 Wk 5 Wk 6 Wk 7 Wk 8SED NA NA NA NA NA NA NA NA NA NA
LIT45ndash50 VO2max
Max speed MetersMin 15 15 15 15 15 15 15 15Incline Degrees 1 1 1 1 1 1 1 1Duration Minutes 133 20 266 333 333 333 333 333Intensity Constant treadmill speed and constant treadmill inclineFrequency BoutsWk 4 4 4 4 4 4 4 4
Distance per bout Meters 1995 300 399 4995 4995 4995 4995 4995Distance per week Meters 798 1200 1596 1998 1998 1998 1998 1998
HIITasymp85 VO2max
Max speed MetersMin 20 30 40 50 50 50 50 50Incline Degrees 5 10 10 10 10 10 10 10Duration Minutes 30 30 30 30 30 30 30 30Intensity 2min stationary period followed by 1min sprint period times 10 repsFrequency BoutsWk 4 4 4 4 4 4 4 4
Distance per bout Meters 200 300 400 500 500 500 500 500Distance per week Meters 800 1200 1600 2000 2000 2000 2000 2000
Identical 5-min warm-up (15mmin) was performed by both training groups prior to each exercise bout
Table 2 Primer sequences
Target Primer sequence (51015840-31015840)Angiotensin I converting enzyme (Ace) forward CTTGACCCTGGATTGCAGCCAngiotensin I converting enzyme (Ace) reverse GTTTCGTGAGGAAGCCAGGAAngiotensin II receptor type 1a (Agtr1a) forward AGTCCTGTTCCACCCGATCAAngiotensin II receptor type 1a (Agtr1a) reverse TCCAGACAAAATGCCAGCCAAngiotensin II receptor type 1b (Agtr1b) forward ACTGCACACGGTGCATTTTAAngiotensin II receptor type 1b (Agtr1b) reverse TAATTGTGCCTGCCAGCCTTAngiotensinogen (serpin peptidase inhibitor clade A member 8) (Agt) forward CTGGAGCTAAAGGACACACAGAAngiotensinogen (serpin peptidase inhibitor clade A member 8) (Agt) reverse GTGAAGGGACCCAAGCTCTCCytochrome P450 family 11 subfamily b polypeptide 2 (Cyp11b2) forward TAACTCAGGGAGCTTTACCTCTCytochrome P450 family 11 subfamily b polypeptide 2 (Cyp11b2) reverse CTGAGACCCTTTGAAGGCCGRenin (Ren) forward CCGTGGTCCTCACCAACTACRenin (Ren) reverse CTTGGCCAGCATGAAGGGTAGlyceraldehyde-3-phosphate dehydrogenase (Gapdh) forward GTTACCAGGGCTGCCTTCTCGlyceraldehyde-3-phosphate dehydrogenase (Gapdh) reverse GATGGTGATGGGTTTCCCGT
a thermal cycler (Rotor-Gene Q Qiagen Venlo Nether-lands) The amplification sequence involved an initial 10-minute cycle at 95∘C followed by 40 cycles each composedof a denaturation step (95∘C for 15 seconds) and a primerannealingextension step (60∘C for 45 seconds) Meltingcurves were performed to ensure that sufficient PCR productwas being generated by each primer in the absence of primerdimers All assays were performed in duplicate (coefficientof variation = 001) mRNA expression data were calculatedusing the Livak method [32] and data are presented as thefold change of the gene of interest relative to that of controlanimals (SED)
28 Clinical Markers in Plasma All bloodplasma markerswere assessed using blood taken from the descending aorta
of each rat Blood was collected into EDTA tubes followinglethal injection directly after the thoracic cavity of the animalhad been opened before tissues were collected This bloodwas centrifuged for 10 minutes at 1500timesg and the resultingplasma was aliquoted to 20mL microtubes and frozen atminus80∘C until it was analysed
Plasma triglyceridesweremeasured using a commerciallyavailable assay kit (Abcam Cambridge England UnitedKingdom) Briefly standards were prepared per the kitinstructions Next 25120583L of plasma was combined with assaybuffer in the well of a 96-well plate Lipase (2120583L) was addedto each well and solutions were mixed before incubating for20 minutes at room temperature Triglyceride reaction mixwas added to each well and solutions were mixed beforeincubating for 60 minutes at room temperature Triglycerideconcentrations were measured colorimetrically
BioMed Research International 5
Plasma high-density lipoprotein (HDL) and low-densitylipoprotein (LDL) were measured using a commerciallyavailable assay kit (Abcam Cambridge England UnitedKingdom) HDL and LDL fractions of plasma sampleswere separated per the kit instructions and standards wereprepared Next 15 120583L of HDL and LDL fractions was firstcombined with cholesterol assay buffer followed by reactionmix Solutions were mixed and then allowed to incubatefor 60 minutes at 37∘C HDL and LDL concentrations weremeasured colorimetrically Total cholesterol was calculatedusing a variation of the Friedlander formula [33]
Plasma creatinine was measured using a commerciallyavailable assay kit (Abcam Cambridge England UnitedKingdom) Standards were prepared per the kit instructionsNext 25 120583L of plasma was combined with assay buffer inthe well of a 96-well plate Reaction mix was added tothis solution and samples were allowed to incubate at 37∘Cfor 60 minutes Creatinine concentrations were measuredcolorimetrically
Plasma albumin was measured using a commerciallyavailable enzyme-linked immunosorbent assay (ELISA) kit(Abcam Cambridge England United Kingdom) Standardswere prepared per the kit instructions Plasma samples wereprepared and added to sample wells Biotinylated albuminwas then added to each well and this solution was mixedgently before a 60-minute incubation period Followingseveralwashes 1x Streptavidin-Peroxidase (SP) conjugatewasadded to each well prior to a 30-minute incubation periodOnce again plates were washed and 50120583L of chromogensubstrate was added followed by a 12-minute incubationperiod Stop solution was then added to each well andalbumin concentrations were measured colorimetrically
29 Clinical and Anthropometric Measurements Blood pres-sures body weights and body lengths were recorded beforesurgery baseline (preexercise) 4 weeks (mid-intervention)and 8 weeks (postintervention) Kidney weights wererecorded after intervention Systolic blood pressure (SBP)wasmeasured using data acquisition hardware (PowerLab ADIn-stuments Bella Vista NSW Australia) coupled to a nonin-vasive blood pressure (NIBP) system (NIBP System ADIn-stuments Bella Vista NSW Australia) with a pulse trans-ducercuff (Pulse TransducerPressure Cuff for NIBP ADIn-stuments Bella Vista NSW Australia) Measurements werethen analysed using LabChart 8 (ADInstuments Bella VistaNSW Australia) Body length was measured from tip-of-nose to tip-of-tail Body weight and remnant kidney weightwere measured to the nearest thousandth of a gram Bodylength and body weight measurements were taken whileeach rat was sedated directly prior to SBP measurement
210 Statistics mRNAdata are presented asmean plusmn standarderror of themean (SEM) All other data are presented asmeanplusmn standard deviation (SD) Body length body weight bodylength-body weight ratio and SBP data were analysed using3 times 3 (group times time) repeated measures analysis of variance(RMANOVA) When applicable group effects andor timeeffects were examined using separate one-way ANOVAs withTukey post hoc comparisons Data for all other measures
(mRNA expression plasma markers kidney weight andkidney weight-body weight ratio) were analysed using one-way ANOVAs with Tukey post hoc comparisons Analyseswere performed using IBM SPSS Statistics (v200 IBMCorporation Armonk NY USA) Statistical significance wasset at 119901 lt 005
3 Results
31 Quantitative Reverse Transcription Polymerase ChainReaction Analysis Results pertaining to renal expressionof RAAS-related mRNA can be seen in Figure 1 Resultspertaining to hepatic expression of RAAS-related mRNA canbe seen in Figure 2 Expression of renal Ren Ace Agtr1band Cyp11b2 mRNA and hepatic Agtr1a mRNA was notsignificantly different between groups (119901 gt 005) Expressionof hepatic Agt mRNA was significantly decreased in HIITcompared to LIT (119901 = 0035)
32 Clinical Markers in Plasma Results pertaining to clinicalmarkers in plasma can be seen in Table 3 Plasma measuresLDL (119901 = 0001) triglycerides (119901 = 0029) and totalcholesterol (119901 = 0002) were significantly lower in HIITcompared to LIT Plasma albumin was significantly higher inHIIT compared to SED (119901 = 0001) and LIT (119901 = 0047)
33 Anthropometric Measurements and Kidney WeightResults pertaining to anthropologicalmeasurements and kid-ney weight can be seen in Tables 3 and 4 Body Length bodyweight body length-body weight ratio and SBP increasedsignificantly from baseline to 4Weeks and from 4Weeks to 8Weeks (119901 lt 005) in all groups (Table 4) with no significantgroup interactions Kidney weight was significantly lower inHIIT compared to the SED (119901 = 0028) and LIT (119901 = 0005)Kidney weight-body weight ratio was significantly lower inHIIT compared to the SED (119901 = 0045) and LIT (119901 = 0048)(Table 3)
4 Discussion
The current study examined the ability of varying forms ofaerobic exercise to influence mRNA expression of severalRAAS-related genes as well as commonCKD-related clinicaland anthropometric markers in an animal model of early-stage CKD This is the first investigation to compare theefficacy of varying forms of aerobic exercise as it pertainsto the modulation of tissue-specific mRNA expression ofRAAS-related genes HIIT produced more favourable out-comes compared to SED and LIT in that HIIT resulted insignificantly reduced mRNA expression of Agt (compared toLIT) significantly improved plasma levels of LDL triglyc-erides and total cholesterol (compared to LIT) significantlyimproved plasma levels of albumin (compared to SED andLIT) and significantly reduced remnant kidney weight andkidney weight-body weight ratios (compared to SED andLIT)
Results regarding the mRNA expression of Agt are inter-esting The mRNA expression of all other genes (Ace Ren
6 BioMed Research International
200
160
120
080
040
000
200
160
120
080
040
000
200
160
120
080
040
000
SED (n = 12) LIT (n = 13) HIIT (n = 14) SED (n = 12) LIT (n = 13) HIIT (n = 14)
SED (n = 12) SED (n = 12)LIT (n = 13) HIIT (n = 14) LIT (n = 13) HIIT (n = 14)
100 053 053061 100 034
039 085
Ren-mRNA expression fold change(norm to GAPDH) (norm to GAPDH)
Ace-mRNA expression fold change
(norm to GAPDH)Agtr1b-mRNA expression fold change
(norm to GAPDH)Cyp11b2-mRNA expression fold change
086043100 100
200
160
120
080
040
000
Figure 1 Renal mRNA expression fold change
Agtr1a Agtr1b and Cyp11b2) was nonsignificantly downreg-ulated in both exercise groups compared to SED HoweverAgt mRNA expression was upregulated in LIT compared toSED (not significant) and HIIT (119901 = 0035) It is worthmentioning that our results are not the first data to suggestthat lower intensity aerobic exercise training may result inunfortunate adaptations in animal models of CKD aerobicexercise training performed at 50ndash70 of VO
2max has beenreported to result in increased resting SBP and decreasedmyocardial capillary density in an animal model of CKD[34]
Differential mRNA expression of Agt may partiallyexplain the nonsignificant (119901 = 0074) difference in SBP inHIIT during Week 8 compared to SED (119901 = 014 +528)and LIT (119901 = 074 +601) The downregulation in themRNA expression of Agt in HIIT may also explain the lackof significant differences in other RAAS genes in this studyThat is a decrease in the mRNA expression of Agt may havequenched the need for any additional significant decreases inthe expression of other RAAS genes This may explain whyeven though there was a near-significant reduction in SBPin HIIT compared to LIT (119901 = 0074) mRNA expression
BioMed Research International 7
p = 0035
118
076084
063
200
160
120
080
040
000
200
160
120
080
040
000
SED (n = 12) LIT (n = 13) HIIT (n = 14)
SED (n = 12) LIT (n = 13) HIIT (n = 14)
Agtr1a-mRNA expression fold change(norm to GAPDH)
(norm to GAPDH)Agt-mRNA expression fold change
100
100
Figure 2 Hepatic mRNA expression fold change
of several RAAS-related of genes (Ace Ren Agtr1b andCyp11b2) was slightly but not significantly increased in HIITcompared to LIT A review on hepatic angiotensinogen [35]discusses the noteworthy influence that angiotensinogen hason blood pressure Decreased levels of angiotensinogen usingangiotensinogen-antibodies in rats [36] and Agt-knockoutmice [37] exhibit lower blood pressure relative to controlsConversely angiotensinogen infusion in mice [38] and Agtoverexpression in rats [39] result in increased blood pressureEvidence suggests that angiotensinogen is a more potentinfluencer of blood pressure than previously suspected [35
Table 3 Nonrepeated clinical and anthropometric measures
Clinicalmeasure Group Mean Standard
deviationMean duplicate
CV
HDL (mgmL)SED 082 013
006LIT 088 015HIIT 093 012
LDL (mgmL)SED 127 027
003LIT 155 034HIIT 108lowast 032
TAG (mgmL)SED 565 166
004LIT 635 265HIIT 411lowast 204
CHOL(mgmL)
SED 322 047NALIT 371 061
HIIT 283lowast 073
CRE(nmol120583L)
SED 107 051004LIT 206 179
HIIT 211 126
ALB (mgmL)SED 2623 384
004LIT 2988 642HIIT 3524dagger 608
Kidney weight(g)
SED 157 009NALIT 159 012
HIIT 146dagger 008
KW-BW ratioSED 00050 00003
NALIT 00050 00003HIIT 00047dagger 00002
Significance set at 119901 le 005lowastSignificantly different from LITdaggerSignificantly different from LIT and SEDHDL high density lipoprotein LDL low density lipoprotein TAG triglyc-erides CHOL total cholesterol CRE creatinine ALB albumin KW-BWkidney weight-body weight CV coefficient of variation
39] often more influential than other components of RAAS[40] and deserves more attention as a potential targetin hypertension-related therapies [35] proposals that aresupported by our findings
Large amounts of between-animal variation in themRNAexpression of RAAS-related genes in SED may explain thelack of significant results in the current study Duplicate-duplicate variation was low (CV = 001) suggesting largeamounts of between-animal variation in SED The issueof between-animal mRNA variation has been empiricallyaddressed in the past [41ndash43] with the most commonlysuggested remedy being an increase in sample size Inter-estingly variation in between-animal mRNA expression inSED is higher across all genes (except for Agt) comparedto LIT and HIIT similar to previous work that has exam-ined RAAS-related mRNA expression in sedentary versusexercise-trained SHRs [20 44] This combined with the factthat aerobic exercise resulted in a downregulation across allgenes compared to SED (expect for Agt in LIT) suggeststhat RAAS-related mRNA expression may be poorly and
8 BioMed Research International
Table 4 Repeated clinical and anthropometric measures
Clinical measure Group Baseline 4 Weekslowast 8 Weeksdagger
(Preintervention) (Mid-Intervention) (Postintervention)
Body length (cm)SED 2848 (186) 3503 (085) 3741 (106)LIT 2932 (165) 3515 (079) 3789 (088)HIIT 2961 (225) 3546 (065) 3787 (062)
Body weight (g)SED 22442 (1782) 27605 (1831) 31353 (1662)LIT 23159 (2101) 27742 (2077) 31825 (2103)HIIT 23090 (1998) 27487 (1646) 30816 (1758)
BL-BW ratioSED 0126 (0007) 0127 (0007) 0120 (0004)LIT 0127 (0009) 0128 (0007) 0119 (0009)HIIT 0129 (0007) 0130 (0008) 0124 (0006)
Systolic blood pressure (mmHg)SED 17557 (927) 20777 (1739) 23977 (1285)LIT 17309 (945) 20925 (231) 24163 (2142)HIIT 17465 (1482) 21625 (1624) 22712 (1423)
Values presented as mean (standard deviation)Significance set at 119901 le 005lowastSignificantly different compared to baseline for all groupsdaggerSignificantly different compared to baseline and 4 weeks for all groupsBL-BW body length-body weight
indiscriminately regulated in the absence of aerobic exercisein an animal model of early-stage CKD That is aerobicexercise may help to control otherwise haphazard RAAS-related mRNA expression that occurs during the early stagesof CKD Several informative reviews have outlined theissue of unregulated blood pressure control [45] and morespecifically unregulated RAAS activity [46] in CKD but thisis the first study to suggest that one of the mechanisms bywhich aerobic exercise may prove beneficial is via tightenedcontrol of RAAS-related mRNA expression independentof statistically significant improvements to RAAS-relatedmRNA expression
In the current study the significant decreases in plasmaLDL triglycerides and total cholesterol in HIIT compared toLIT but not SED are encouraging and somewhat surprisingA recent study performed in healthy well-trained humansreported nonsignificant improvements in LDL triglyceridesand total cholesterol after 12 weeks of HIIT [47] In spe-cial andor clinical populations HIIT seems to exert moreinfluence over blood lipids Cardiac rehabilitation patientswho engaged in HIIT experienced significant improvementsin HDL relative to traditional aerobic exercise training[26] However triglyceride measurements were not differentbetween groups and LDL measurements were not reported[26] HIIT has also proven to be beneficial in obese men[48] and women [49] resulting in improved HDL [48]LDL [48] triglycerides [48 49] and total cholesterol [4849] Despite the slowly-accumulating data a recent review[50] that notes the ability of HIIT to influence blood lipidshas yet to be established especially in special populationssuggesting that this specific line of research the effects ofHIIT on blood lipids should be further examined This isespecially true in CKD as lipid-related disorders are theleading cause of complications in CVD [51 52] and CVD-related complications are the leading cause of death in CKD
patients [10 11] As such dyslipidemia should be rankedamong the primary concerns of CKD-related research [53]
Similar to blood lipids a recent review notes that theeffects of exercise training on plasma albumin in patientswith CKD are unclear [54] Moreover data describing theeffects of HIIT on plasma albumin in patients with CKD areunavailable Hypoalbuminemia is an independent predictorof renal dysfunction [55] and an independent predictor ofCVD in early-stage CKD [56] and can be used to identifyCKD patients at increased risk of developing CVD [56] Inobese individuals with metabolic syndrome two commoncharacteristics of CKD 12 weeks of aerobic exercise trainingsignificantly reduced albuminuria (urinary albumin) com-pared to a no-exercise control group [57] Aerobic exercisetraining (16 weeks at 60 of maximal aerobic velocity) hasalso proven useful at reducing albuminuria in SHRs [44]Because hypoalbuminemia is related to declining kidneyfunction [55] blood albumin andor urinary albumin areuseful markers for assessing the preservation of renal tissueIn the current study plasma albumin was significantly higherin HIIT compared to SED and LIT suggesting that renalstructure and function are better preserved by HIIT Thepreservation of renal structure and function and subsequentincrease in plasma albumin may have been due to the down-regulation of Agt mRNA expression and the accompanyingdecrease in SBP in HIIT as hypertension is directly related torenal damage [44 58]
Also considered an indicator of renal damage kid-ney weight and kidney weight-body weight ratio weresignificantly lower in HIIT compared to SED and LITHypertension-related declines in renal function are associ-ated with compensatory alterations to renal tissue such astubulointerstitial fibrosis [59 60] Often pathological thesealterations result in glomerular hypertrophy [59 60] Usinghistological and molecular applications 16 weeks of aerobic
BioMed Research International 9
exercise training (performed at 60 of maximal aerobicvelocity) has been shown to reduce renal fibrosis in SHRs[44] Although renal fibrosis and renal hypertrophy aredirectly related data that specifically describes the effectsof HIIT on renal hypertrophy are unavailable Similar tothe mechanisms that account for increased levels of plasmaalbumin in HIIT there is evidence to suggest that thesignificantly lower kidney weight and kidney weight-bodyweight ratios in HIIT compared to SED and LIT may bedue to decreased fibrosis Decreases in renal fibrosis maybe due to decreases in hypertension-mediated renal damagefollowing a downregulation of the mRNA expression of Agtand a decrease in SBP (in HIIT) [44 58]
5 Conclusions
In summary in an animal model of early-stage CKD HIITappeared to be more beneficial compared to SED and LITas HIIT was responsible for a significant downregulation inthe mRNA expression of Agt The downregulated mRNAexpression of Agt along with significant improvements toblood lipids (LDL triglycerides and total cholesterol) maypartially explain the nonsignificant decrease in SBP andsignificant improvements to plasma albumin kidney weightand kidney weight-body weight ratios in HIIT relative toSED and LIT Future work would benefit from examiningRAAS-related protein expression as well as specific measuresof renal histology and morphology Future work would alsobenefit from examining whether the positive HIIT-relatedeffects seen in the present study are apparent in differentrelated disease models (eg nonnephrectomised SHRs or 56nephrectomy SHRs)
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] AIHW Ed Australiarsquos Health 2014 Australiarsquos Health SeriesAustralian Institute of Health and Welfare (AIHW) CanberraAustralia 2014
[2] A S Go G M Chertow D Fan C E McCulloch andC-Y Hsu ldquoChronic kidney disease and the risks of deathcardiovascular events and hospitalizationrdquo The New EnglandJournal of Medicine vol 351 no 13 pp 1296ndash1370 2004
[3] U D Mathisen T Melsom O C Ingebretsen et al ldquoEstimatedGFR associates with cardiovascular risk factors independentlyof measured GFRrdquo Journal of the American Society of Nephrol-ogy vol 22 no 5 pp 927ndash937 2011
[4] DM Silverstein ldquoInflammation in chronic kidney disease rolein the progression of renal and cardiovascular diseaserdquoPediatricNephrology vol 24 no 8 pp 1445ndash1452 2009
[5] P S Tucker M I Kingsley R H Morton A T Scanlan andV J Dalbo ldquoThe increasing financial impact of chronic kidneydisease in Australiardquo International Journal of Nephrology vol2014 Article ID 120537 7 pages 2014
[6] B Stengel M E Tarver-Carr N R Powe M S Eberhardt andF L Brancati ldquoLifestyle factors obesity and the risk of chronickidney diseaserdquo Epidemiology vol 14 no 4 pp 479ndash487 2003
[7] R T Gansevoort R Correa-Rotter B R Hemmelgarn et alldquoChronic kidney disease and cardiovascular risk epidemiologymechanisms and preventionrdquoTheLancet vol 382 no 9889 pp339ndash352 2013
[8] M M H Hermans R Henry J M Dekker et al ldquoEstimatedglomerular filtration rate and urinary albumin excretion areindependently associated with greater arterial stiffness theHoorn studyrdquo Journal of the American Society of Nephrology vol18 no 6 pp 1942ndash1952 2007
[9] M L Ford L A Tomlinson T P E Chapman C Rajkumar andS G Holt ldquoAortic stiffness is independently associated with rateof renal function decline in chronic kidney disease stages 3 and4rdquo Hypertension vol 55 no 5 pp 1110ndash1115 2010
[10] D EWeiner H Tighiouart P C Stark et al ldquoKidney disease asa risk factor for recurrent cardiovascular disease andmortalityrdquoAmerican Journal of Kidney Diseases vol 44 no 2 pp 198ndash2062004
[11] D E Weiner H Tighiouart M G Amin et al ldquoChronickidney disease as a risk factor for cardiovascular disease and all-causemortality a pooled analysis of community-based studiesrdquoJournal of the American Society of Nephrology vol 15 no 5 pp1307ndash1315 2004
[12] R K Soni A C Porter J P Lash and M L Unruh ldquoHealth-related quality of life in hypertension chronic kidney diseaseand coexistent chronic health conditionsrdquo Advances in ChronicKidney Disease vol 17 no 4 pp e17ndashe26 2010
[13] J Segura C Campo P Gil et al ldquoDevelopment of chronickidney disease and cardiovascular prognosis in essential hyper-tensive patientsrdquo Journal of the American Society of Nephrologyvol 15 no 6 pp 1616ndash1622 2004
[14] J Blacher A P Guerin B Pannier S J Marchais M E Safarand G M London ldquoImpact of aortic stiffness on survival inend-stage renal diseaserdquo Circulation vol 99 no 18 pp 2434ndash2439 1999
[15] G L Bakris E Ritz and World Kidney Day Steering Commit-tee ldquoThe message for World Kidney Day 2009 hypertensionand kidney disease a marriage that should be preventedrdquo TheJournal of Clinical Hypertension (Greenwich) vol 11 no 3 pp144ndash147 2009
[16] J L Lavoie and C D Sigmund ldquoMinireview overview ofthe renin-angiotensin systemmdashan endocrine and paracrinesystemrdquo Endocrinology vol 144 no 6 pp 2179ndash2183 2003
[17] A Nguyen Dinh Cat and RM Touyz ldquoA new look at the renin-angiotensin systemmdashfocusing on the vascular systemrdquo Peptidesvol 32 no 10 pp 2141ndash2150 2011
[18] U C Brewster and M A Perazella ldquoThe renin-angiotensin-aldosterone system and the kidney effects on kidney diseaserdquoThe American Journal of Medicine vol 116 no 4 pp 263ndash2722004
[19] S Ciampone R Borges I P De Lima F F Mesquita EC Cambiucci and J A R Gontijo ldquoLong-term exerciseattenuates blood pressure responsiveness andmodulates kidneyangiotensin II signalling and urinary sodium excretion in SHRrdquoJournal of the Renin-Angiotensin-Aldosterone System vol 12 no4 pp 394ndash403 2011
[20] D Agarwal M A Welsch J N Keller and J Francis ldquoChronicexercise modulates RAS components and improves balancebetween pro- and anti-inflammatory cytokines in the brain of
10 BioMed Research International
SHRrdquo Basic Research in Cardiology vol 106 no 6 pp 1069ndash1085 2011
[21] E J Howden R G Fassett N M Isbel and J S CoombesldquoExercise training in chronic kidney disease patientsrdquo SportsMedicine vol 42 no 6 pp 473ndash488 2012
[22] S Nielsen A Schmitz M Rehling and C E Mogensen ldquoSys-tolic blood pressure relates to the rate of decline of glomerularfiltration rate in type II diabetesrdquo Diabetes Care vol 16 no 11pp 1427ndash1432 1993
[23] A E Tjoslashnna I M Leinan A T Bartnes et al ldquoLow- and high-volume of intensive endurance training significantly improvesmaximal oxygen uptake after 10-weeks of training in healthymenrdquo PLoS ONE vol 8 no 5 Article ID e65382 2013
[24] T Moholdt E Madssen Oslash Rognmo and I L Aamot ldquoThehigher the better Interval training intensity in coronary heartdiseaserdquo Journal of Science and Medicine in Sport vol 17 no 5pp 506ndash510 2014
[25] H E Molmen-Hansen T Stolen A E Tjonna et al ldquoAerobicinterval training reduces blood pressure and improves myocar-dial function in hypertensive patientsrdquo European Journal ofPreventive Cardiology vol 19 no 2 pp 151ndash160 2012
[26] T Moholdt I L Aamot I Granoslashien et al ldquoAerobic intervaltraining increases peak oxygen uptake more than usual careexercise training in myocardial infarction patients a random-ized controlled studyrdquo Clinical Rehabilitation vol 26 no 1 pp33ndash44 2012
[27] E J Howden J S Coombes H Strand B Douglas K LCampbell and N M Isbel ldquoExercise training in CKD efficacyadherence and safetyrdquoAmerican Journal of KidneyDiseases vol65 no 4 pp 583ndash591 2015
[28] A C KingW L Haskell D R Young R K Oka andM L Ste-fanick ldquoLong-term effects of varying intensities and formats ofphysical activity on participation rates fitness and lipoproteinsin men and women aged 50 to 65 yearsrdquo Circulation vol 91 no10 pp 2596ndash2604 1995
[29] G A Brooks and T P White ldquoDetermination of metabolicand heart rate responses of rats to treadmill exerciserdquo Journalof Applied Physiology Respiratory Environmental and ExercisePhysiology vol 45 no 6 pp 1009ndash1015 1978
[30] Y Yu J C Fuscoe C Zhao et al ldquoA rat RNA-Seq transcriptomicBodyMap across 11 organs and 4 developmental stagesrdquo NatureCommunications vol 5 article 3230 2014
[31] F Z Marques A E Campain M Tomaszewski et al ldquoGeneexpression profiling reveals renin mRNA overexpression inhuman hypertensive kidneys and a role formicroRNAsrdquoHyper-tension vol 58 no 6 pp 1093ndash1098 2011
[32] K J Livak and T D Schmittgen ldquoAnalysis of relative geneexpression data using real-time quantitative PCRand the 2minusΔΔ119862TmethodrdquoMethods vol 25 no 4 pp 402ndash408 2001
[33] Y Friedlander J D Kark S Eisenberg and Y Stein ldquoCalcula-tion of LDL-cholesterol from total cholesterol triglyceride andHDL-cholesterol a comparison of methods in the JerusalemLipid Research Clinic Prevalence Studyrdquo Israel Journal of Medi-cal Sciences vol 18 no 12 pp 1242ndash1252 1982
[34] K DMarcus andCM Tipton ldquoExercise training and its effectswith renal hypertensive ratsrdquo Journal of Applied Physiology vol59 no 5 pp 1410ndash1415 1985
[35] K Kitada H Kobori and A Nishiyama ldquoLiver-specificangiotensinogen suppression an old yet novel target forblood pressure control through RAS inhibitionrdquo HypertensionResearch vol 37 no 5 pp 393ndash394 2014
[36] J Gardes J Bouhnik E Clauser P Corvol and JMenard ldquoRoleof angiotensinogen in blood pressure homeostasisrdquo Hyperten-sion vol 4 no 2 pp 185ndash189 1982
[37] K Tanimoto F Sugiyama Y Goto et al ldquoAngiotensinogen-deficient mice with hypotensionrdquo The Journal of BiologicalChemistry vol 269 no 50 pp 31334ndash31337 1994
[38] S Kimura J J Mullins B Bunnemann et al ldquoHigh bloodpressure in transgenic mice carrying the rat angiotensinogengenerdquoThe EMBO Journal vol 11 no 3 pp 821ndash827 1992
[39] JMenard A-I K El Amrani F Savoie J Bouhnik K R LynchandM J Peach ldquoAngiotensinogen an attractive and underratedparticipant in hypertension and inflammationrdquo Hypertensionvol 18 no 5 pp 705ndash707 1991
[40] S Agrawal S Agarwal and S Naik ldquoGenetic contributionand associated pathophysiology in end-stage renal diseaserdquoTheApplication of Clinical Genetics vol 3 pp 65ndash84 2010
[41] W-C Cheng W-Y Shu C-Y Li et al ldquoIntra- and inter-individual variance of gene expression in clinical studiesrdquo PLoSONE vol 7 no 6 Article ID e38650 2012
[42] A Whitehead and D L Crawford ldquoVariation in tissue-specificgene expression among natural populationsrdquo Genome Biologyvol 6 no 2 article R13 2005
[43] A L Oberg B M Bot D E Grill G A Poland and TM Therneau ldquoTechnical and biological variance structure inmRNA-Seq data life in the real worldrdquo BMC Genomics vol 13no 1 article 304 2012
[44] D Agarwal C M Elks S D Reed N Mariappan D SA Majid and J Francis ldquoChronic exercise preserves renalstructure and hemodynamics in spontaneously hypertensiveratsrdquo Antioxidants amp Redox Signaling vol 16 no 2 pp 139ndash1522012
[45] P Zamboli L De Nicola R Minutolo V Bertino F Catapanoand G Conte ldquoManagement of hypertension in chronic kidneydiseaserdquoCurrentHypertensionReports vol 8 no 6 pp 497ndash5012006
[46] G Remuzzi N Perico M Macia and P Ruggenenti ldquoThe roleof renin-angiotensin-aldosterone system in the progression ofchronic kidney diseaserdquo Kidney International vol 68 no 99pp S57ndashS65 2005
[47] N Ouerghi M Feki N Kaabachi M Khammassi S Boukor-raa and A Bouassida ldquoEffects of a high-intensity intermittenttraining programon aerobic capacity and lipid profile in trainedsubjectsrdquoOpenAccess Journal of SportsMedicine vol 5 pp 243ndash248 2014
[48] A Paoli Q F Pacelli T Moro et al ldquoEffects of high-intensitycircuit training low-intensity circuit training and endurancetraining on blood pressure and lipoproteins in middle-agedoverweight menrdquo Lipids in Health and Disease vol 12 no 1article 131 2013
[49] G Racil O Ben Ounis O Hammouda et al ldquoEffects of highvs Moderate exercise intensity during interval training onlipids and adiponectin levels in obese young femalesrdquo EuropeanJournal of Applied Physiology vol 113 no 10 pp 2531ndash25402013
[50] H S Kessler S B Sisson and K R Short ldquoThe potentialfor high-intensity interval training to reduce cardiometabolicdisease riskrdquo Sports Medicine vol 42 no 6 pp 489ndash509 2012
[51] J Poss F Custodis CWernerOWeingartnerM Bohm andULaufs ldquoCardiovascular disease and dyslipidemia beyond LDLrdquoCurrent Pharmaceutical Design vol 17 no 9 pp 861ndash870 2011
BioMed Research International 11
[52] J R Burnett ldquoLipids lipoproteins atherosclerosis and cardio-vascular diseaserdquoThe Clinical Biochemist Reviews vol 25 no 1p 2 2004
[53] G Piecha M Adamczak and E Ritz ldquoDyslipidemia in chronickidney disease pathogenesis and interventionrdquo Polskie Archi-wum Medycyny Wewnetrznej vol 119 no 7-8 pp 487ndash4922009
[54] N A Smart A D Williams I Levinger et al ldquoExercise ampSports Science Australia (ESSA) position statement on exerciseand chronic kidney diseaserdquo Journal of Science and Medicine inSport vol 16 no 5 pp 406ndash411 2013
[55] S-J Pinto-Sietsma W M T Janssen H L Hillege G NavisD de Zeeuw and P E de Jong ldquoUrinary albumin excretion isassociated with renal functional abnormalities in a nondiabeticpopulationrdquo Journal of the American Society of Nephrology vol11 no 10 pp 1882ndash1888 2000
[56] N R Shah and F Dumler ldquoHypoalbuminaemiamdasha marker ofcardiovascular disease in patients with chronic kidney diseasestages II-IVrdquo International Journal ofMedical Sciences vol 5 no6 pp 366ndash370 2008
[57] N E Straznicky M T Grima E A Lambert et al ldquoExerciseaugments weight loss induced improvement in renal functionin obese metabolic syndrome individualsrdquo Journal of Hyperten-sion vol 29 no 3 pp 553ndash564 2011
[58] R D Manning Jr N Tian and S Meng ldquoOxidative stress andantioxidant treatment in hypertension and the associated renaldamagerdquoAmerican Journal of Nephrology vol 25 no 4 pp 311ndash317 2005
[59] G Keller G Zimmer GMall E Ritz andK Amann ldquoNephronnumber in patients with primary hypertensionrdquo The NewEngland Journal of Medicine vol 348 no 2 pp 101ndash108 2003
[60] J Floege M W Burns C E Alpers et al ldquoGlomerular cellproliferation and PDGF expression precede glomerulosclerosisin the remnant kidney modelrdquo Kidney International vol 41 no2 pp 297ndash309 1992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 BioMed Research International
Table 1 Detailed exercise protocol
Group Variable Measure Wk 1 Wk 2 Wk 3 Wk 4 Wk 5 Wk 6 Wk 7 Wk 8SED NA NA NA NA NA NA NA NA NA NA
LIT45ndash50 VO2max
Max speed MetersMin 15 15 15 15 15 15 15 15Incline Degrees 1 1 1 1 1 1 1 1Duration Minutes 133 20 266 333 333 333 333 333Intensity Constant treadmill speed and constant treadmill inclineFrequency BoutsWk 4 4 4 4 4 4 4 4
Distance per bout Meters 1995 300 399 4995 4995 4995 4995 4995Distance per week Meters 798 1200 1596 1998 1998 1998 1998 1998
HIITasymp85 VO2max
Max speed MetersMin 20 30 40 50 50 50 50 50Incline Degrees 5 10 10 10 10 10 10 10Duration Minutes 30 30 30 30 30 30 30 30Intensity 2min stationary period followed by 1min sprint period times 10 repsFrequency BoutsWk 4 4 4 4 4 4 4 4
Distance per bout Meters 200 300 400 500 500 500 500 500Distance per week Meters 800 1200 1600 2000 2000 2000 2000 2000
Identical 5-min warm-up (15mmin) was performed by both training groups prior to each exercise bout
Table 2 Primer sequences
Target Primer sequence (51015840-31015840)Angiotensin I converting enzyme (Ace) forward CTTGACCCTGGATTGCAGCCAngiotensin I converting enzyme (Ace) reverse GTTTCGTGAGGAAGCCAGGAAngiotensin II receptor type 1a (Agtr1a) forward AGTCCTGTTCCACCCGATCAAngiotensin II receptor type 1a (Agtr1a) reverse TCCAGACAAAATGCCAGCCAAngiotensin II receptor type 1b (Agtr1b) forward ACTGCACACGGTGCATTTTAAngiotensin II receptor type 1b (Agtr1b) reverse TAATTGTGCCTGCCAGCCTTAngiotensinogen (serpin peptidase inhibitor clade A member 8) (Agt) forward CTGGAGCTAAAGGACACACAGAAngiotensinogen (serpin peptidase inhibitor clade A member 8) (Agt) reverse GTGAAGGGACCCAAGCTCTCCytochrome P450 family 11 subfamily b polypeptide 2 (Cyp11b2) forward TAACTCAGGGAGCTTTACCTCTCytochrome P450 family 11 subfamily b polypeptide 2 (Cyp11b2) reverse CTGAGACCCTTTGAAGGCCGRenin (Ren) forward CCGTGGTCCTCACCAACTACRenin (Ren) reverse CTTGGCCAGCATGAAGGGTAGlyceraldehyde-3-phosphate dehydrogenase (Gapdh) forward GTTACCAGGGCTGCCTTCTCGlyceraldehyde-3-phosphate dehydrogenase (Gapdh) reverse GATGGTGATGGGTTTCCCGT
a thermal cycler (Rotor-Gene Q Qiagen Venlo Nether-lands) The amplification sequence involved an initial 10-minute cycle at 95∘C followed by 40 cycles each composedof a denaturation step (95∘C for 15 seconds) and a primerannealingextension step (60∘C for 45 seconds) Meltingcurves were performed to ensure that sufficient PCR productwas being generated by each primer in the absence of primerdimers All assays were performed in duplicate (coefficientof variation = 001) mRNA expression data were calculatedusing the Livak method [32] and data are presented as thefold change of the gene of interest relative to that of controlanimals (SED)
28 Clinical Markers in Plasma All bloodplasma markerswere assessed using blood taken from the descending aorta
of each rat Blood was collected into EDTA tubes followinglethal injection directly after the thoracic cavity of the animalhad been opened before tissues were collected This bloodwas centrifuged for 10 minutes at 1500timesg and the resultingplasma was aliquoted to 20mL microtubes and frozen atminus80∘C until it was analysed
Plasma triglyceridesweremeasured using a commerciallyavailable assay kit (Abcam Cambridge England UnitedKingdom) Briefly standards were prepared per the kitinstructions Next 25120583L of plasma was combined with assaybuffer in the well of a 96-well plate Lipase (2120583L) was addedto each well and solutions were mixed before incubating for20 minutes at room temperature Triglyceride reaction mixwas added to each well and solutions were mixed beforeincubating for 60 minutes at room temperature Triglycerideconcentrations were measured colorimetrically
BioMed Research International 5
Plasma high-density lipoprotein (HDL) and low-densitylipoprotein (LDL) were measured using a commerciallyavailable assay kit (Abcam Cambridge England UnitedKingdom) HDL and LDL fractions of plasma sampleswere separated per the kit instructions and standards wereprepared Next 15 120583L of HDL and LDL fractions was firstcombined with cholesterol assay buffer followed by reactionmix Solutions were mixed and then allowed to incubatefor 60 minutes at 37∘C HDL and LDL concentrations weremeasured colorimetrically Total cholesterol was calculatedusing a variation of the Friedlander formula [33]
Plasma creatinine was measured using a commerciallyavailable assay kit (Abcam Cambridge England UnitedKingdom) Standards were prepared per the kit instructionsNext 25 120583L of plasma was combined with assay buffer inthe well of a 96-well plate Reaction mix was added tothis solution and samples were allowed to incubate at 37∘Cfor 60 minutes Creatinine concentrations were measuredcolorimetrically
Plasma albumin was measured using a commerciallyavailable enzyme-linked immunosorbent assay (ELISA) kit(Abcam Cambridge England United Kingdom) Standardswere prepared per the kit instructions Plasma samples wereprepared and added to sample wells Biotinylated albuminwas then added to each well and this solution was mixedgently before a 60-minute incubation period Followingseveralwashes 1x Streptavidin-Peroxidase (SP) conjugatewasadded to each well prior to a 30-minute incubation periodOnce again plates were washed and 50120583L of chromogensubstrate was added followed by a 12-minute incubationperiod Stop solution was then added to each well andalbumin concentrations were measured colorimetrically
29 Clinical and Anthropometric Measurements Blood pres-sures body weights and body lengths were recorded beforesurgery baseline (preexercise) 4 weeks (mid-intervention)and 8 weeks (postintervention) Kidney weights wererecorded after intervention Systolic blood pressure (SBP)wasmeasured using data acquisition hardware (PowerLab ADIn-stuments Bella Vista NSW Australia) coupled to a nonin-vasive blood pressure (NIBP) system (NIBP System ADIn-stuments Bella Vista NSW Australia) with a pulse trans-ducercuff (Pulse TransducerPressure Cuff for NIBP ADIn-stuments Bella Vista NSW Australia) Measurements werethen analysed using LabChart 8 (ADInstuments Bella VistaNSW Australia) Body length was measured from tip-of-nose to tip-of-tail Body weight and remnant kidney weightwere measured to the nearest thousandth of a gram Bodylength and body weight measurements were taken whileeach rat was sedated directly prior to SBP measurement
210 Statistics mRNAdata are presented asmean plusmn standarderror of themean (SEM) All other data are presented asmeanplusmn standard deviation (SD) Body length body weight bodylength-body weight ratio and SBP data were analysed using3 times 3 (group times time) repeated measures analysis of variance(RMANOVA) When applicable group effects andor timeeffects were examined using separate one-way ANOVAs withTukey post hoc comparisons Data for all other measures
(mRNA expression plasma markers kidney weight andkidney weight-body weight ratio) were analysed using one-way ANOVAs with Tukey post hoc comparisons Analyseswere performed using IBM SPSS Statistics (v200 IBMCorporation Armonk NY USA) Statistical significance wasset at 119901 lt 005
3 Results
31 Quantitative Reverse Transcription Polymerase ChainReaction Analysis Results pertaining to renal expressionof RAAS-related mRNA can be seen in Figure 1 Resultspertaining to hepatic expression of RAAS-related mRNA canbe seen in Figure 2 Expression of renal Ren Ace Agtr1band Cyp11b2 mRNA and hepatic Agtr1a mRNA was notsignificantly different between groups (119901 gt 005) Expressionof hepatic Agt mRNA was significantly decreased in HIITcompared to LIT (119901 = 0035)
32 Clinical Markers in Plasma Results pertaining to clinicalmarkers in plasma can be seen in Table 3 Plasma measuresLDL (119901 = 0001) triglycerides (119901 = 0029) and totalcholesterol (119901 = 0002) were significantly lower in HIITcompared to LIT Plasma albumin was significantly higher inHIIT compared to SED (119901 = 0001) and LIT (119901 = 0047)
33 Anthropometric Measurements and Kidney WeightResults pertaining to anthropologicalmeasurements and kid-ney weight can be seen in Tables 3 and 4 Body Length bodyweight body length-body weight ratio and SBP increasedsignificantly from baseline to 4Weeks and from 4Weeks to 8Weeks (119901 lt 005) in all groups (Table 4) with no significantgroup interactions Kidney weight was significantly lower inHIIT compared to the SED (119901 = 0028) and LIT (119901 = 0005)Kidney weight-body weight ratio was significantly lower inHIIT compared to the SED (119901 = 0045) and LIT (119901 = 0048)(Table 3)
4 Discussion
The current study examined the ability of varying forms ofaerobic exercise to influence mRNA expression of severalRAAS-related genes as well as commonCKD-related clinicaland anthropometric markers in an animal model of early-stage CKD This is the first investigation to compare theefficacy of varying forms of aerobic exercise as it pertainsto the modulation of tissue-specific mRNA expression ofRAAS-related genes HIIT produced more favourable out-comes compared to SED and LIT in that HIIT resulted insignificantly reduced mRNA expression of Agt (compared toLIT) significantly improved plasma levels of LDL triglyc-erides and total cholesterol (compared to LIT) significantlyimproved plasma levels of albumin (compared to SED andLIT) and significantly reduced remnant kidney weight andkidney weight-body weight ratios (compared to SED andLIT)
Results regarding the mRNA expression of Agt are inter-esting The mRNA expression of all other genes (Ace Ren
6 BioMed Research International
200
160
120
080
040
000
200
160
120
080
040
000
200
160
120
080
040
000
SED (n = 12) LIT (n = 13) HIIT (n = 14) SED (n = 12) LIT (n = 13) HIIT (n = 14)
SED (n = 12) SED (n = 12)LIT (n = 13) HIIT (n = 14) LIT (n = 13) HIIT (n = 14)
100 053 053061 100 034
039 085
Ren-mRNA expression fold change(norm to GAPDH) (norm to GAPDH)
Ace-mRNA expression fold change
(norm to GAPDH)Agtr1b-mRNA expression fold change
(norm to GAPDH)Cyp11b2-mRNA expression fold change
086043100 100
200
160
120
080
040
000
Figure 1 Renal mRNA expression fold change
Agtr1a Agtr1b and Cyp11b2) was nonsignificantly downreg-ulated in both exercise groups compared to SED HoweverAgt mRNA expression was upregulated in LIT compared toSED (not significant) and HIIT (119901 = 0035) It is worthmentioning that our results are not the first data to suggestthat lower intensity aerobic exercise training may result inunfortunate adaptations in animal models of CKD aerobicexercise training performed at 50ndash70 of VO
2max has beenreported to result in increased resting SBP and decreasedmyocardial capillary density in an animal model of CKD[34]
Differential mRNA expression of Agt may partiallyexplain the nonsignificant (119901 = 0074) difference in SBP inHIIT during Week 8 compared to SED (119901 = 014 +528)and LIT (119901 = 074 +601) The downregulation in themRNA expression of Agt in HIIT may also explain the lackof significant differences in other RAAS genes in this studyThat is a decrease in the mRNA expression of Agt may havequenched the need for any additional significant decreases inthe expression of other RAAS genes This may explain whyeven though there was a near-significant reduction in SBPin HIIT compared to LIT (119901 = 0074) mRNA expression
BioMed Research International 7
p = 0035
118
076084
063
200
160
120
080
040
000
200
160
120
080
040
000
SED (n = 12) LIT (n = 13) HIIT (n = 14)
SED (n = 12) LIT (n = 13) HIIT (n = 14)
Agtr1a-mRNA expression fold change(norm to GAPDH)
(norm to GAPDH)Agt-mRNA expression fold change
100
100
Figure 2 Hepatic mRNA expression fold change
of several RAAS-related of genes (Ace Ren Agtr1b andCyp11b2) was slightly but not significantly increased in HIITcompared to LIT A review on hepatic angiotensinogen [35]discusses the noteworthy influence that angiotensinogen hason blood pressure Decreased levels of angiotensinogen usingangiotensinogen-antibodies in rats [36] and Agt-knockoutmice [37] exhibit lower blood pressure relative to controlsConversely angiotensinogen infusion in mice [38] and Agtoverexpression in rats [39] result in increased blood pressureEvidence suggests that angiotensinogen is a more potentinfluencer of blood pressure than previously suspected [35
Table 3 Nonrepeated clinical and anthropometric measures
Clinicalmeasure Group Mean Standard
deviationMean duplicate
CV
HDL (mgmL)SED 082 013
006LIT 088 015HIIT 093 012
LDL (mgmL)SED 127 027
003LIT 155 034HIIT 108lowast 032
TAG (mgmL)SED 565 166
004LIT 635 265HIIT 411lowast 204
CHOL(mgmL)
SED 322 047NALIT 371 061
HIIT 283lowast 073
CRE(nmol120583L)
SED 107 051004LIT 206 179
HIIT 211 126
ALB (mgmL)SED 2623 384
004LIT 2988 642HIIT 3524dagger 608
Kidney weight(g)
SED 157 009NALIT 159 012
HIIT 146dagger 008
KW-BW ratioSED 00050 00003
NALIT 00050 00003HIIT 00047dagger 00002
Significance set at 119901 le 005lowastSignificantly different from LITdaggerSignificantly different from LIT and SEDHDL high density lipoprotein LDL low density lipoprotein TAG triglyc-erides CHOL total cholesterol CRE creatinine ALB albumin KW-BWkidney weight-body weight CV coefficient of variation
39] often more influential than other components of RAAS[40] and deserves more attention as a potential targetin hypertension-related therapies [35] proposals that aresupported by our findings
Large amounts of between-animal variation in themRNAexpression of RAAS-related genes in SED may explain thelack of significant results in the current study Duplicate-duplicate variation was low (CV = 001) suggesting largeamounts of between-animal variation in SED The issueof between-animal mRNA variation has been empiricallyaddressed in the past [41ndash43] with the most commonlysuggested remedy being an increase in sample size Inter-estingly variation in between-animal mRNA expression inSED is higher across all genes (except for Agt) comparedto LIT and HIIT similar to previous work that has exam-ined RAAS-related mRNA expression in sedentary versusexercise-trained SHRs [20 44] This combined with the factthat aerobic exercise resulted in a downregulation across allgenes compared to SED (expect for Agt in LIT) suggeststhat RAAS-related mRNA expression may be poorly and
8 BioMed Research International
Table 4 Repeated clinical and anthropometric measures
Clinical measure Group Baseline 4 Weekslowast 8 Weeksdagger
(Preintervention) (Mid-Intervention) (Postintervention)
Body length (cm)SED 2848 (186) 3503 (085) 3741 (106)LIT 2932 (165) 3515 (079) 3789 (088)HIIT 2961 (225) 3546 (065) 3787 (062)
Body weight (g)SED 22442 (1782) 27605 (1831) 31353 (1662)LIT 23159 (2101) 27742 (2077) 31825 (2103)HIIT 23090 (1998) 27487 (1646) 30816 (1758)
BL-BW ratioSED 0126 (0007) 0127 (0007) 0120 (0004)LIT 0127 (0009) 0128 (0007) 0119 (0009)HIIT 0129 (0007) 0130 (0008) 0124 (0006)
Systolic blood pressure (mmHg)SED 17557 (927) 20777 (1739) 23977 (1285)LIT 17309 (945) 20925 (231) 24163 (2142)HIIT 17465 (1482) 21625 (1624) 22712 (1423)
Values presented as mean (standard deviation)Significance set at 119901 le 005lowastSignificantly different compared to baseline for all groupsdaggerSignificantly different compared to baseline and 4 weeks for all groupsBL-BW body length-body weight
indiscriminately regulated in the absence of aerobic exercisein an animal model of early-stage CKD That is aerobicexercise may help to control otherwise haphazard RAAS-related mRNA expression that occurs during the early stagesof CKD Several informative reviews have outlined theissue of unregulated blood pressure control [45] and morespecifically unregulated RAAS activity [46] in CKD but thisis the first study to suggest that one of the mechanisms bywhich aerobic exercise may prove beneficial is via tightenedcontrol of RAAS-related mRNA expression independentof statistically significant improvements to RAAS-relatedmRNA expression
In the current study the significant decreases in plasmaLDL triglycerides and total cholesterol in HIIT compared toLIT but not SED are encouraging and somewhat surprisingA recent study performed in healthy well-trained humansreported nonsignificant improvements in LDL triglyceridesand total cholesterol after 12 weeks of HIIT [47] In spe-cial andor clinical populations HIIT seems to exert moreinfluence over blood lipids Cardiac rehabilitation patientswho engaged in HIIT experienced significant improvementsin HDL relative to traditional aerobic exercise training[26] However triglyceride measurements were not differentbetween groups and LDL measurements were not reported[26] HIIT has also proven to be beneficial in obese men[48] and women [49] resulting in improved HDL [48]LDL [48] triglycerides [48 49] and total cholesterol [4849] Despite the slowly-accumulating data a recent review[50] that notes the ability of HIIT to influence blood lipidshas yet to be established especially in special populationssuggesting that this specific line of research the effects ofHIIT on blood lipids should be further examined This isespecially true in CKD as lipid-related disorders are theleading cause of complications in CVD [51 52] and CVD-related complications are the leading cause of death in CKD
patients [10 11] As such dyslipidemia should be rankedamong the primary concerns of CKD-related research [53]
Similar to blood lipids a recent review notes that theeffects of exercise training on plasma albumin in patientswith CKD are unclear [54] Moreover data describing theeffects of HIIT on plasma albumin in patients with CKD areunavailable Hypoalbuminemia is an independent predictorof renal dysfunction [55] and an independent predictor ofCVD in early-stage CKD [56] and can be used to identifyCKD patients at increased risk of developing CVD [56] Inobese individuals with metabolic syndrome two commoncharacteristics of CKD 12 weeks of aerobic exercise trainingsignificantly reduced albuminuria (urinary albumin) com-pared to a no-exercise control group [57] Aerobic exercisetraining (16 weeks at 60 of maximal aerobic velocity) hasalso proven useful at reducing albuminuria in SHRs [44]Because hypoalbuminemia is related to declining kidneyfunction [55] blood albumin andor urinary albumin areuseful markers for assessing the preservation of renal tissueIn the current study plasma albumin was significantly higherin HIIT compared to SED and LIT suggesting that renalstructure and function are better preserved by HIIT Thepreservation of renal structure and function and subsequentincrease in plasma albumin may have been due to the down-regulation of Agt mRNA expression and the accompanyingdecrease in SBP in HIIT as hypertension is directly related torenal damage [44 58]
Also considered an indicator of renal damage kid-ney weight and kidney weight-body weight ratio weresignificantly lower in HIIT compared to SED and LITHypertension-related declines in renal function are associ-ated with compensatory alterations to renal tissue such astubulointerstitial fibrosis [59 60] Often pathological thesealterations result in glomerular hypertrophy [59 60] Usinghistological and molecular applications 16 weeks of aerobic
BioMed Research International 9
exercise training (performed at 60 of maximal aerobicvelocity) has been shown to reduce renal fibrosis in SHRs[44] Although renal fibrosis and renal hypertrophy aredirectly related data that specifically describes the effectsof HIIT on renal hypertrophy are unavailable Similar tothe mechanisms that account for increased levels of plasmaalbumin in HIIT there is evidence to suggest that thesignificantly lower kidney weight and kidney weight-bodyweight ratios in HIIT compared to SED and LIT may bedue to decreased fibrosis Decreases in renal fibrosis maybe due to decreases in hypertension-mediated renal damagefollowing a downregulation of the mRNA expression of Agtand a decrease in SBP (in HIIT) [44 58]
5 Conclusions
In summary in an animal model of early-stage CKD HIITappeared to be more beneficial compared to SED and LITas HIIT was responsible for a significant downregulation inthe mRNA expression of Agt The downregulated mRNAexpression of Agt along with significant improvements toblood lipids (LDL triglycerides and total cholesterol) maypartially explain the nonsignificant decrease in SBP andsignificant improvements to plasma albumin kidney weightand kidney weight-body weight ratios in HIIT relative toSED and LIT Future work would benefit from examiningRAAS-related protein expression as well as specific measuresof renal histology and morphology Future work would alsobenefit from examining whether the positive HIIT-relatedeffects seen in the present study are apparent in differentrelated disease models (eg nonnephrectomised SHRs or 56nephrectomy SHRs)
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] AIHW Ed Australiarsquos Health 2014 Australiarsquos Health SeriesAustralian Institute of Health and Welfare (AIHW) CanberraAustralia 2014
[2] A S Go G M Chertow D Fan C E McCulloch andC-Y Hsu ldquoChronic kidney disease and the risks of deathcardiovascular events and hospitalizationrdquo The New EnglandJournal of Medicine vol 351 no 13 pp 1296ndash1370 2004
[3] U D Mathisen T Melsom O C Ingebretsen et al ldquoEstimatedGFR associates with cardiovascular risk factors independentlyof measured GFRrdquo Journal of the American Society of Nephrol-ogy vol 22 no 5 pp 927ndash937 2011
[4] DM Silverstein ldquoInflammation in chronic kidney disease rolein the progression of renal and cardiovascular diseaserdquoPediatricNephrology vol 24 no 8 pp 1445ndash1452 2009
[5] P S Tucker M I Kingsley R H Morton A T Scanlan andV J Dalbo ldquoThe increasing financial impact of chronic kidneydisease in Australiardquo International Journal of Nephrology vol2014 Article ID 120537 7 pages 2014
[6] B Stengel M E Tarver-Carr N R Powe M S Eberhardt andF L Brancati ldquoLifestyle factors obesity and the risk of chronickidney diseaserdquo Epidemiology vol 14 no 4 pp 479ndash487 2003
[7] R T Gansevoort R Correa-Rotter B R Hemmelgarn et alldquoChronic kidney disease and cardiovascular risk epidemiologymechanisms and preventionrdquoTheLancet vol 382 no 9889 pp339ndash352 2013
[8] M M H Hermans R Henry J M Dekker et al ldquoEstimatedglomerular filtration rate and urinary albumin excretion areindependently associated with greater arterial stiffness theHoorn studyrdquo Journal of the American Society of Nephrology vol18 no 6 pp 1942ndash1952 2007
[9] M L Ford L A Tomlinson T P E Chapman C Rajkumar andS G Holt ldquoAortic stiffness is independently associated with rateof renal function decline in chronic kidney disease stages 3 and4rdquo Hypertension vol 55 no 5 pp 1110ndash1115 2010
[10] D EWeiner H Tighiouart P C Stark et al ldquoKidney disease asa risk factor for recurrent cardiovascular disease andmortalityrdquoAmerican Journal of Kidney Diseases vol 44 no 2 pp 198ndash2062004
[11] D E Weiner H Tighiouart M G Amin et al ldquoChronickidney disease as a risk factor for cardiovascular disease and all-causemortality a pooled analysis of community-based studiesrdquoJournal of the American Society of Nephrology vol 15 no 5 pp1307ndash1315 2004
[12] R K Soni A C Porter J P Lash and M L Unruh ldquoHealth-related quality of life in hypertension chronic kidney diseaseand coexistent chronic health conditionsrdquo Advances in ChronicKidney Disease vol 17 no 4 pp e17ndashe26 2010
[13] J Segura C Campo P Gil et al ldquoDevelopment of chronickidney disease and cardiovascular prognosis in essential hyper-tensive patientsrdquo Journal of the American Society of Nephrologyvol 15 no 6 pp 1616ndash1622 2004
[14] J Blacher A P Guerin B Pannier S J Marchais M E Safarand G M London ldquoImpact of aortic stiffness on survival inend-stage renal diseaserdquo Circulation vol 99 no 18 pp 2434ndash2439 1999
[15] G L Bakris E Ritz and World Kidney Day Steering Commit-tee ldquoThe message for World Kidney Day 2009 hypertensionand kidney disease a marriage that should be preventedrdquo TheJournal of Clinical Hypertension (Greenwich) vol 11 no 3 pp144ndash147 2009
[16] J L Lavoie and C D Sigmund ldquoMinireview overview ofthe renin-angiotensin systemmdashan endocrine and paracrinesystemrdquo Endocrinology vol 144 no 6 pp 2179ndash2183 2003
[17] A Nguyen Dinh Cat and RM Touyz ldquoA new look at the renin-angiotensin systemmdashfocusing on the vascular systemrdquo Peptidesvol 32 no 10 pp 2141ndash2150 2011
[18] U C Brewster and M A Perazella ldquoThe renin-angiotensin-aldosterone system and the kidney effects on kidney diseaserdquoThe American Journal of Medicine vol 116 no 4 pp 263ndash2722004
[19] S Ciampone R Borges I P De Lima F F Mesquita EC Cambiucci and J A R Gontijo ldquoLong-term exerciseattenuates blood pressure responsiveness andmodulates kidneyangiotensin II signalling and urinary sodium excretion in SHRrdquoJournal of the Renin-Angiotensin-Aldosterone System vol 12 no4 pp 394ndash403 2011
[20] D Agarwal M A Welsch J N Keller and J Francis ldquoChronicexercise modulates RAS components and improves balancebetween pro- and anti-inflammatory cytokines in the brain of
10 BioMed Research International
SHRrdquo Basic Research in Cardiology vol 106 no 6 pp 1069ndash1085 2011
[21] E J Howden R G Fassett N M Isbel and J S CoombesldquoExercise training in chronic kidney disease patientsrdquo SportsMedicine vol 42 no 6 pp 473ndash488 2012
[22] S Nielsen A Schmitz M Rehling and C E Mogensen ldquoSys-tolic blood pressure relates to the rate of decline of glomerularfiltration rate in type II diabetesrdquo Diabetes Care vol 16 no 11pp 1427ndash1432 1993
[23] A E Tjoslashnna I M Leinan A T Bartnes et al ldquoLow- and high-volume of intensive endurance training significantly improvesmaximal oxygen uptake after 10-weeks of training in healthymenrdquo PLoS ONE vol 8 no 5 Article ID e65382 2013
[24] T Moholdt E Madssen Oslash Rognmo and I L Aamot ldquoThehigher the better Interval training intensity in coronary heartdiseaserdquo Journal of Science and Medicine in Sport vol 17 no 5pp 506ndash510 2014
[25] H E Molmen-Hansen T Stolen A E Tjonna et al ldquoAerobicinterval training reduces blood pressure and improves myocar-dial function in hypertensive patientsrdquo European Journal ofPreventive Cardiology vol 19 no 2 pp 151ndash160 2012
[26] T Moholdt I L Aamot I Granoslashien et al ldquoAerobic intervaltraining increases peak oxygen uptake more than usual careexercise training in myocardial infarction patients a random-ized controlled studyrdquo Clinical Rehabilitation vol 26 no 1 pp33ndash44 2012
[27] E J Howden J S Coombes H Strand B Douglas K LCampbell and N M Isbel ldquoExercise training in CKD efficacyadherence and safetyrdquoAmerican Journal of KidneyDiseases vol65 no 4 pp 583ndash591 2015
[28] A C KingW L Haskell D R Young R K Oka andM L Ste-fanick ldquoLong-term effects of varying intensities and formats ofphysical activity on participation rates fitness and lipoproteinsin men and women aged 50 to 65 yearsrdquo Circulation vol 91 no10 pp 2596ndash2604 1995
[29] G A Brooks and T P White ldquoDetermination of metabolicand heart rate responses of rats to treadmill exerciserdquo Journalof Applied Physiology Respiratory Environmental and ExercisePhysiology vol 45 no 6 pp 1009ndash1015 1978
[30] Y Yu J C Fuscoe C Zhao et al ldquoA rat RNA-Seq transcriptomicBodyMap across 11 organs and 4 developmental stagesrdquo NatureCommunications vol 5 article 3230 2014
[31] F Z Marques A E Campain M Tomaszewski et al ldquoGeneexpression profiling reveals renin mRNA overexpression inhuman hypertensive kidneys and a role formicroRNAsrdquoHyper-tension vol 58 no 6 pp 1093ndash1098 2011
[32] K J Livak and T D Schmittgen ldquoAnalysis of relative geneexpression data using real-time quantitative PCRand the 2minusΔΔ119862TmethodrdquoMethods vol 25 no 4 pp 402ndash408 2001
[33] Y Friedlander J D Kark S Eisenberg and Y Stein ldquoCalcula-tion of LDL-cholesterol from total cholesterol triglyceride andHDL-cholesterol a comparison of methods in the JerusalemLipid Research Clinic Prevalence Studyrdquo Israel Journal of Medi-cal Sciences vol 18 no 12 pp 1242ndash1252 1982
[34] K DMarcus andCM Tipton ldquoExercise training and its effectswith renal hypertensive ratsrdquo Journal of Applied Physiology vol59 no 5 pp 1410ndash1415 1985
[35] K Kitada H Kobori and A Nishiyama ldquoLiver-specificangiotensinogen suppression an old yet novel target forblood pressure control through RAS inhibitionrdquo HypertensionResearch vol 37 no 5 pp 393ndash394 2014
[36] J Gardes J Bouhnik E Clauser P Corvol and JMenard ldquoRoleof angiotensinogen in blood pressure homeostasisrdquo Hyperten-sion vol 4 no 2 pp 185ndash189 1982
[37] K Tanimoto F Sugiyama Y Goto et al ldquoAngiotensinogen-deficient mice with hypotensionrdquo The Journal of BiologicalChemistry vol 269 no 50 pp 31334ndash31337 1994
[38] S Kimura J J Mullins B Bunnemann et al ldquoHigh bloodpressure in transgenic mice carrying the rat angiotensinogengenerdquoThe EMBO Journal vol 11 no 3 pp 821ndash827 1992
[39] JMenard A-I K El Amrani F Savoie J Bouhnik K R LynchandM J Peach ldquoAngiotensinogen an attractive and underratedparticipant in hypertension and inflammationrdquo Hypertensionvol 18 no 5 pp 705ndash707 1991
[40] S Agrawal S Agarwal and S Naik ldquoGenetic contributionand associated pathophysiology in end-stage renal diseaserdquoTheApplication of Clinical Genetics vol 3 pp 65ndash84 2010
[41] W-C Cheng W-Y Shu C-Y Li et al ldquoIntra- and inter-individual variance of gene expression in clinical studiesrdquo PLoSONE vol 7 no 6 Article ID e38650 2012
[42] A Whitehead and D L Crawford ldquoVariation in tissue-specificgene expression among natural populationsrdquo Genome Biologyvol 6 no 2 article R13 2005
[43] A L Oberg B M Bot D E Grill G A Poland and TM Therneau ldquoTechnical and biological variance structure inmRNA-Seq data life in the real worldrdquo BMC Genomics vol 13no 1 article 304 2012
[44] D Agarwal C M Elks S D Reed N Mariappan D SA Majid and J Francis ldquoChronic exercise preserves renalstructure and hemodynamics in spontaneously hypertensiveratsrdquo Antioxidants amp Redox Signaling vol 16 no 2 pp 139ndash1522012
[45] P Zamboli L De Nicola R Minutolo V Bertino F Catapanoand G Conte ldquoManagement of hypertension in chronic kidneydiseaserdquoCurrentHypertensionReports vol 8 no 6 pp 497ndash5012006
[46] G Remuzzi N Perico M Macia and P Ruggenenti ldquoThe roleof renin-angiotensin-aldosterone system in the progression ofchronic kidney diseaserdquo Kidney International vol 68 no 99pp S57ndashS65 2005
[47] N Ouerghi M Feki N Kaabachi M Khammassi S Boukor-raa and A Bouassida ldquoEffects of a high-intensity intermittenttraining programon aerobic capacity and lipid profile in trainedsubjectsrdquoOpenAccess Journal of SportsMedicine vol 5 pp 243ndash248 2014
[48] A Paoli Q F Pacelli T Moro et al ldquoEffects of high-intensitycircuit training low-intensity circuit training and endurancetraining on blood pressure and lipoproteins in middle-agedoverweight menrdquo Lipids in Health and Disease vol 12 no 1article 131 2013
[49] G Racil O Ben Ounis O Hammouda et al ldquoEffects of highvs Moderate exercise intensity during interval training onlipids and adiponectin levels in obese young femalesrdquo EuropeanJournal of Applied Physiology vol 113 no 10 pp 2531ndash25402013
[50] H S Kessler S B Sisson and K R Short ldquoThe potentialfor high-intensity interval training to reduce cardiometabolicdisease riskrdquo Sports Medicine vol 42 no 6 pp 489ndash509 2012
[51] J Poss F Custodis CWernerOWeingartnerM Bohm andULaufs ldquoCardiovascular disease and dyslipidemia beyond LDLrdquoCurrent Pharmaceutical Design vol 17 no 9 pp 861ndash870 2011
BioMed Research International 11
[52] J R Burnett ldquoLipids lipoproteins atherosclerosis and cardio-vascular diseaserdquoThe Clinical Biochemist Reviews vol 25 no 1p 2 2004
[53] G Piecha M Adamczak and E Ritz ldquoDyslipidemia in chronickidney disease pathogenesis and interventionrdquo Polskie Archi-wum Medycyny Wewnetrznej vol 119 no 7-8 pp 487ndash4922009
[54] N A Smart A D Williams I Levinger et al ldquoExercise ampSports Science Australia (ESSA) position statement on exerciseand chronic kidney diseaserdquo Journal of Science and Medicine inSport vol 16 no 5 pp 406ndash411 2013
[55] S-J Pinto-Sietsma W M T Janssen H L Hillege G NavisD de Zeeuw and P E de Jong ldquoUrinary albumin excretion isassociated with renal functional abnormalities in a nondiabeticpopulationrdquo Journal of the American Society of Nephrology vol11 no 10 pp 1882ndash1888 2000
[56] N R Shah and F Dumler ldquoHypoalbuminaemiamdasha marker ofcardiovascular disease in patients with chronic kidney diseasestages II-IVrdquo International Journal ofMedical Sciences vol 5 no6 pp 366ndash370 2008
[57] N E Straznicky M T Grima E A Lambert et al ldquoExerciseaugments weight loss induced improvement in renal functionin obese metabolic syndrome individualsrdquo Journal of Hyperten-sion vol 29 no 3 pp 553ndash564 2011
[58] R D Manning Jr N Tian and S Meng ldquoOxidative stress andantioxidant treatment in hypertension and the associated renaldamagerdquoAmerican Journal of Nephrology vol 25 no 4 pp 311ndash317 2005
[59] G Keller G Zimmer GMall E Ritz andK Amann ldquoNephronnumber in patients with primary hypertensionrdquo The NewEngland Journal of Medicine vol 348 no 2 pp 101ndash108 2003
[60] J Floege M W Burns C E Alpers et al ldquoGlomerular cellproliferation and PDGF expression precede glomerulosclerosisin the remnant kidney modelrdquo Kidney International vol 41 no2 pp 297ndash309 1992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 5
Plasma high-density lipoprotein (HDL) and low-densitylipoprotein (LDL) were measured using a commerciallyavailable assay kit (Abcam Cambridge England UnitedKingdom) HDL and LDL fractions of plasma sampleswere separated per the kit instructions and standards wereprepared Next 15 120583L of HDL and LDL fractions was firstcombined with cholesterol assay buffer followed by reactionmix Solutions were mixed and then allowed to incubatefor 60 minutes at 37∘C HDL and LDL concentrations weremeasured colorimetrically Total cholesterol was calculatedusing a variation of the Friedlander formula [33]
Plasma creatinine was measured using a commerciallyavailable assay kit (Abcam Cambridge England UnitedKingdom) Standards were prepared per the kit instructionsNext 25 120583L of plasma was combined with assay buffer inthe well of a 96-well plate Reaction mix was added tothis solution and samples were allowed to incubate at 37∘Cfor 60 minutes Creatinine concentrations were measuredcolorimetrically
Plasma albumin was measured using a commerciallyavailable enzyme-linked immunosorbent assay (ELISA) kit(Abcam Cambridge England United Kingdom) Standardswere prepared per the kit instructions Plasma samples wereprepared and added to sample wells Biotinylated albuminwas then added to each well and this solution was mixedgently before a 60-minute incubation period Followingseveralwashes 1x Streptavidin-Peroxidase (SP) conjugatewasadded to each well prior to a 30-minute incubation periodOnce again plates were washed and 50120583L of chromogensubstrate was added followed by a 12-minute incubationperiod Stop solution was then added to each well andalbumin concentrations were measured colorimetrically
29 Clinical and Anthropometric Measurements Blood pres-sures body weights and body lengths were recorded beforesurgery baseline (preexercise) 4 weeks (mid-intervention)and 8 weeks (postintervention) Kidney weights wererecorded after intervention Systolic blood pressure (SBP)wasmeasured using data acquisition hardware (PowerLab ADIn-stuments Bella Vista NSW Australia) coupled to a nonin-vasive blood pressure (NIBP) system (NIBP System ADIn-stuments Bella Vista NSW Australia) with a pulse trans-ducercuff (Pulse TransducerPressure Cuff for NIBP ADIn-stuments Bella Vista NSW Australia) Measurements werethen analysed using LabChart 8 (ADInstuments Bella VistaNSW Australia) Body length was measured from tip-of-nose to tip-of-tail Body weight and remnant kidney weightwere measured to the nearest thousandth of a gram Bodylength and body weight measurements were taken whileeach rat was sedated directly prior to SBP measurement
210 Statistics mRNAdata are presented asmean plusmn standarderror of themean (SEM) All other data are presented asmeanplusmn standard deviation (SD) Body length body weight bodylength-body weight ratio and SBP data were analysed using3 times 3 (group times time) repeated measures analysis of variance(RMANOVA) When applicable group effects andor timeeffects were examined using separate one-way ANOVAs withTukey post hoc comparisons Data for all other measures
(mRNA expression plasma markers kidney weight andkidney weight-body weight ratio) were analysed using one-way ANOVAs with Tukey post hoc comparisons Analyseswere performed using IBM SPSS Statistics (v200 IBMCorporation Armonk NY USA) Statistical significance wasset at 119901 lt 005
3 Results
31 Quantitative Reverse Transcription Polymerase ChainReaction Analysis Results pertaining to renal expressionof RAAS-related mRNA can be seen in Figure 1 Resultspertaining to hepatic expression of RAAS-related mRNA canbe seen in Figure 2 Expression of renal Ren Ace Agtr1band Cyp11b2 mRNA and hepatic Agtr1a mRNA was notsignificantly different between groups (119901 gt 005) Expressionof hepatic Agt mRNA was significantly decreased in HIITcompared to LIT (119901 = 0035)
32 Clinical Markers in Plasma Results pertaining to clinicalmarkers in plasma can be seen in Table 3 Plasma measuresLDL (119901 = 0001) triglycerides (119901 = 0029) and totalcholesterol (119901 = 0002) were significantly lower in HIITcompared to LIT Plasma albumin was significantly higher inHIIT compared to SED (119901 = 0001) and LIT (119901 = 0047)
33 Anthropometric Measurements and Kidney WeightResults pertaining to anthropologicalmeasurements and kid-ney weight can be seen in Tables 3 and 4 Body Length bodyweight body length-body weight ratio and SBP increasedsignificantly from baseline to 4Weeks and from 4Weeks to 8Weeks (119901 lt 005) in all groups (Table 4) with no significantgroup interactions Kidney weight was significantly lower inHIIT compared to the SED (119901 = 0028) and LIT (119901 = 0005)Kidney weight-body weight ratio was significantly lower inHIIT compared to the SED (119901 = 0045) and LIT (119901 = 0048)(Table 3)
4 Discussion
The current study examined the ability of varying forms ofaerobic exercise to influence mRNA expression of severalRAAS-related genes as well as commonCKD-related clinicaland anthropometric markers in an animal model of early-stage CKD This is the first investigation to compare theefficacy of varying forms of aerobic exercise as it pertainsto the modulation of tissue-specific mRNA expression ofRAAS-related genes HIIT produced more favourable out-comes compared to SED and LIT in that HIIT resulted insignificantly reduced mRNA expression of Agt (compared toLIT) significantly improved plasma levels of LDL triglyc-erides and total cholesterol (compared to LIT) significantlyimproved plasma levels of albumin (compared to SED andLIT) and significantly reduced remnant kidney weight andkidney weight-body weight ratios (compared to SED andLIT)
Results regarding the mRNA expression of Agt are inter-esting The mRNA expression of all other genes (Ace Ren
6 BioMed Research International
200
160
120
080
040
000
200
160
120
080
040
000
200
160
120
080
040
000
SED (n = 12) LIT (n = 13) HIIT (n = 14) SED (n = 12) LIT (n = 13) HIIT (n = 14)
SED (n = 12) SED (n = 12)LIT (n = 13) HIIT (n = 14) LIT (n = 13) HIIT (n = 14)
100 053 053061 100 034
039 085
Ren-mRNA expression fold change(norm to GAPDH) (norm to GAPDH)
Ace-mRNA expression fold change
(norm to GAPDH)Agtr1b-mRNA expression fold change
(norm to GAPDH)Cyp11b2-mRNA expression fold change
086043100 100
200
160
120
080
040
000
Figure 1 Renal mRNA expression fold change
Agtr1a Agtr1b and Cyp11b2) was nonsignificantly downreg-ulated in both exercise groups compared to SED HoweverAgt mRNA expression was upregulated in LIT compared toSED (not significant) and HIIT (119901 = 0035) It is worthmentioning that our results are not the first data to suggestthat lower intensity aerobic exercise training may result inunfortunate adaptations in animal models of CKD aerobicexercise training performed at 50ndash70 of VO
2max has beenreported to result in increased resting SBP and decreasedmyocardial capillary density in an animal model of CKD[34]
Differential mRNA expression of Agt may partiallyexplain the nonsignificant (119901 = 0074) difference in SBP inHIIT during Week 8 compared to SED (119901 = 014 +528)and LIT (119901 = 074 +601) The downregulation in themRNA expression of Agt in HIIT may also explain the lackof significant differences in other RAAS genes in this studyThat is a decrease in the mRNA expression of Agt may havequenched the need for any additional significant decreases inthe expression of other RAAS genes This may explain whyeven though there was a near-significant reduction in SBPin HIIT compared to LIT (119901 = 0074) mRNA expression
BioMed Research International 7
p = 0035
118
076084
063
200
160
120
080
040
000
200
160
120
080
040
000
SED (n = 12) LIT (n = 13) HIIT (n = 14)
SED (n = 12) LIT (n = 13) HIIT (n = 14)
Agtr1a-mRNA expression fold change(norm to GAPDH)
(norm to GAPDH)Agt-mRNA expression fold change
100
100
Figure 2 Hepatic mRNA expression fold change
of several RAAS-related of genes (Ace Ren Agtr1b andCyp11b2) was slightly but not significantly increased in HIITcompared to LIT A review on hepatic angiotensinogen [35]discusses the noteworthy influence that angiotensinogen hason blood pressure Decreased levels of angiotensinogen usingangiotensinogen-antibodies in rats [36] and Agt-knockoutmice [37] exhibit lower blood pressure relative to controlsConversely angiotensinogen infusion in mice [38] and Agtoverexpression in rats [39] result in increased blood pressureEvidence suggests that angiotensinogen is a more potentinfluencer of blood pressure than previously suspected [35
Table 3 Nonrepeated clinical and anthropometric measures
Clinicalmeasure Group Mean Standard
deviationMean duplicate
CV
HDL (mgmL)SED 082 013
006LIT 088 015HIIT 093 012
LDL (mgmL)SED 127 027
003LIT 155 034HIIT 108lowast 032
TAG (mgmL)SED 565 166
004LIT 635 265HIIT 411lowast 204
CHOL(mgmL)
SED 322 047NALIT 371 061
HIIT 283lowast 073
CRE(nmol120583L)
SED 107 051004LIT 206 179
HIIT 211 126
ALB (mgmL)SED 2623 384
004LIT 2988 642HIIT 3524dagger 608
Kidney weight(g)
SED 157 009NALIT 159 012
HIIT 146dagger 008
KW-BW ratioSED 00050 00003
NALIT 00050 00003HIIT 00047dagger 00002
Significance set at 119901 le 005lowastSignificantly different from LITdaggerSignificantly different from LIT and SEDHDL high density lipoprotein LDL low density lipoprotein TAG triglyc-erides CHOL total cholesterol CRE creatinine ALB albumin KW-BWkidney weight-body weight CV coefficient of variation
39] often more influential than other components of RAAS[40] and deserves more attention as a potential targetin hypertension-related therapies [35] proposals that aresupported by our findings
Large amounts of between-animal variation in themRNAexpression of RAAS-related genes in SED may explain thelack of significant results in the current study Duplicate-duplicate variation was low (CV = 001) suggesting largeamounts of between-animal variation in SED The issueof between-animal mRNA variation has been empiricallyaddressed in the past [41ndash43] with the most commonlysuggested remedy being an increase in sample size Inter-estingly variation in between-animal mRNA expression inSED is higher across all genes (except for Agt) comparedto LIT and HIIT similar to previous work that has exam-ined RAAS-related mRNA expression in sedentary versusexercise-trained SHRs [20 44] This combined with the factthat aerobic exercise resulted in a downregulation across allgenes compared to SED (expect for Agt in LIT) suggeststhat RAAS-related mRNA expression may be poorly and
8 BioMed Research International
Table 4 Repeated clinical and anthropometric measures
Clinical measure Group Baseline 4 Weekslowast 8 Weeksdagger
(Preintervention) (Mid-Intervention) (Postintervention)
Body length (cm)SED 2848 (186) 3503 (085) 3741 (106)LIT 2932 (165) 3515 (079) 3789 (088)HIIT 2961 (225) 3546 (065) 3787 (062)
Body weight (g)SED 22442 (1782) 27605 (1831) 31353 (1662)LIT 23159 (2101) 27742 (2077) 31825 (2103)HIIT 23090 (1998) 27487 (1646) 30816 (1758)
BL-BW ratioSED 0126 (0007) 0127 (0007) 0120 (0004)LIT 0127 (0009) 0128 (0007) 0119 (0009)HIIT 0129 (0007) 0130 (0008) 0124 (0006)
Systolic blood pressure (mmHg)SED 17557 (927) 20777 (1739) 23977 (1285)LIT 17309 (945) 20925 (231) 24163 (2142)HIIT 17465 (1482) 21625 (1624) 22712 (1423)
Values presented as mean (standard deviation)Significance set at 119901 le 005lowastSignificantly different compared to baseline for all groupsdaggerSignificantly different compared to baseline and 4 weeks for all groupsBL-BW body length-body weight
indiscriminately regulated in the absence of aerobic exercisein an animal model of early-stage CKD That is aerobicexercise may help to control otherwise haphazard RAAS-related mRNA expression that occurs during the early stagesof CKD Several informative reviews have outlined theissue of unregulated blood pressure control [45] and morespecifically unregulated RAAS activity [46] in CKD but thisis the first study to suggest that one of the mechanisms bywhich aerobic exercise may prove beneficial is via tightenedcontrol of RAAS-related mRNA expression independentof statistically significant improvements to RAAS-relatedmRNA expression
In the current study the significant decreases in plasmaLDL triglycerides and total cholesterol in HIIT compared toLIT but not SED are encouraging and somewhat surprisingA recent study performed in healthy well-trained humansreported nonsignificant improvements in LDL triglyceridesand total cholesterol after 12 weeks of HIIT [47] In spe-cial andor clinical populations HIIT seems to exert moreinfluence over blood lipids Cardiac rehabilitation patientswho engaged in HIIT experienced significant improvementsin HDL relative to traditional aerobic exercise training[26] However triglyceride measurements were not differentbetween groups and LDL measurements were not reported[26] HIIT has also proven to be beneficial in obese men[48] and women [49] resulting in improved HDL [48]LDL [48] triglycerides [48 49] and total cholesterol [4849] Despite the slowly-accumulating data a recent review[50] that notes the ability of HIIT to influence blood lipidshas yet to be established especially in special populationssuggesting that this specific line of research the effects ofHIIT on blood lipids should be further examined This isespecially true in CKD as lipid-related disorders are theleading cause of complications in CVD [51 52] and CVD-related complications are the leading cause of death in CKD
patients [10 11] As such dyslipidemia should be rankedamong the primary concerns of CKD-related research [53]
Similar to blood lipids a recent review notes that theeffects of exercise training on plasma albumin in patientswith CKD are unclear [54] Moreover data describing theeffects of HIIT on plasma albumin in patients with CKD areunavailable Hypoalbuminemia is an independent predictorof renal dysfunction [55] and an independent predictor ofCVD in early-stage CKD [56] and can be used to identifyCKD patients at increased risk of developing CVD [56] Inobese individuals with metabolic syndrome two commoncharacteristics of CKD 12 weeks of aerobic exercise trainingsignificantly reduced albuminuria (urinary albumin) com-pared to a no-exercise control group [57] Aerobic exercisetraining (16 weeks at 60 of maximal aerobic velocity) hasalso proven useful at reducing albuminuria in SHRs [44]Because hypoalbuminemia is related to declining kidneyfunction [55] blood albumin andor urinary albumin areuseful markers for assessing the preservation of renal tissueIn the current study plasma albumin was significantly higherin HIIT compared to SED and LIT suggesting that renalstructure and function are better preserved by HIIT Thepreservation of renal structure and function and subsequentincrease in plasma albumin may have been due to the down-regulation of Agt mRNA expression and the accompanyingdecrease in SBP in HIIT as hypertension is directly related torenal damage [44 58]
Also considered an indicator of renal damage kid-ney weight and kidney weight-body weight ratio weresignificantly lower in HIIT compared to SED and LITHypertension-related declines in renal function are associ-ated with compensatory alterations to renal tissue such astubulointerstitial fibrosis [59 60] Often pathological thesealterations result in glomerular hypertrophy [59 60] Usinghistological and molecular applications 16 weeks of aerobic
BioMed Research International 9
exercise training (performed at 60 of maximal aerobicvelocity) has been shown to reduce renal fibrosis in SHRs[44] Although renal fibrosis and renal hypertrophy aredirectly related data that specifically describes the effectsof HIIT on renal hypertrophy are unavailable Similar tothe mechanisms that account for increased levels of plasmaalbumin in HIIT there is evidence to suggest that thesignificantly lower kidney weight and kidney weight-bodyweight ratios in HIIT compared to SED and LIT may bedue to decreased fibrosis Decreases in renal fibrosis maybe due to decreases in hypertension-mediated renal damagefollowing a downregulation of the mRNA expression of Agtand a decrease in SBP (in HIIT) [44 58]
5 Conclusions
In summary in an animal model of early-stage CKD HIITappeared to be more beneficial compared to SED and LITas HIIT was responsible for a significant downregulation inthe mRNA expression of Agt The downregulated mRNAexpression of Agt along with significant improvements toblood lipids (LDL triglycerides and total cholesterol) maypartially explain the nonsignificant decrease in SBP andsignificant improvements to plasma albumin kidney weightand kidney weight-body weight ratios in HIIT relative toSED and LIT Future work would benefit from examiningRAAS-related protein expression as well as specific measuresof renal histology and morphology Future work would alsobenefit from examining whether the positive HIIT-relatedeffects seen in the present study are apparent in differentrelated disease models (eg nonnephrectomised SHRs or 56nephrectomy SHRs)
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] AIHW Ed Australiarsquos Health 2014 Australiarsquos Health SeriesAustralian Institute of Health and Welfare (AIHW) CanberraAustralia 2014
[2] A S Go G M Chertow D Fan C E McCulloch andC-Y Hsu ldquoChronic kidney disease and the risks of deathcardiovascular events and hospitalizationrdquo The New EnglandJournal of Medicine vol 351 no 13 pp 1296ndash1370 2004
[3] U D Mathisen T Melsom O C Ingebretsen et al ldquoEstimatedGFR associates with cardiovascular risk factors independentlyof measured GFRrdquo Journal of the American Society of Nephrol-ogy vol 22 no 5 pp 927ndash937 2011
[4] DM Silverstein ldquoInflammation in chronic kidney disease rolein the progression of renal and cardiovascular diseaserdquoPediatricNephrology vol 24 no 8 pp 1445ndash1452 2009
[5] P S Tucker M I Kingsley R H Morton A T Scanlan andV J Dalbo ldquoThe increasing financial impact of chronic kidneydisease in Australiardquo International Journal of Nephrology vol2014 Article ID 120537 7 pages 2014
[6] B Stengel M E Tarver-Carr N R Powe M S Eberhardt andF L Brancati ldquoLifestyle factors obesity and the risk of chronickidney diseaserdquo Epidemiology vol 14 no 4 pp 479ndash487 2003
[7] R T Gansevoort R Correa-Rotter B R Hemmelgarn et alldquoChronic kidney disease and cardiovascular risk epidemiologymechanisms and preventionrdquoTheLancet vol 382 no 9889 pp339ndash352 2013
[8] M M H Hermans R Henry J M Dekker et al ldquoEstimatedglomerular filtration rate and urinary albumin excretion areindependently associated with greater arterial stiffness theHoorn studyrdquo Journal of the American Society of Nephrology vol18 no 6 pp 1942ndash1952 2007
[9] M L Ford L A Tomlinson T P E Chapman C Rajkumar andS G Holt ldquoAortic stiffness is independently associated with rateof renal function decline in chronic kidney disease stages 3 and4rdquo Hypertension vol 55 no 5 pp 1110ndash1115 2010
[10] D EWeiner H Tighiouart P C Stark et al ldquoKidney disease asa risk factor for recurrent cardiovascular disease andmortalityrdquoAmerican Journal of Kidney Diseases vol 44 no 2 pp 198ndash2062004
[11] D E Weiner H Tighiouart M G Amin et al ldquoChronickidney disease as a risk factor for cardiovascular disease and all-causemortality a pooled analysis of community-based studiesrdquoJournal of the American Society of Nephrology vol 15 no 5 pp1307ndash1315 2004
[12] R K Soni A C Porter J P Lash and M L Unruh ldquoHealth-related quality of life in hypertension chronic kidney diseaseand coexistent chronic health conditionsrdquo Advances in ChronicKidney Disease vol 17 no 4 pp e17ndashe26 2010
[13] J Segura C Campo P Gil et al ldquoDevelopment of chronickidney disease and cardiovascular prognosis in essential hyper-tensive patientsrdquo Journal of the American Society of Nephrologyvol 15 no 6 pp 1616ndash1622 2004
[14] J Blacher A P Guerin B Pannier S J Marchais M E Safarand G M London ldquoImpact of aortic stiffness on survival inend-stage renal diseaserdquo Circulation vol 99 no 18 pp 2434ndash2439 1999
[15] G L Bakris E Ritz and World Kidney Day Steering Commit-tee ldquoThe message for World Kidney Day 2009 hypertensionand kidney disease a marriage that should be preventedrdquo TheJournal of Clinical Hypertension (Greenwich) vol 11 no 3 pp144ndash147 2009
[16] J L Lavoie and C D Sigmund ldquoMinireview overview ofthe renin-angiotensin systemmdashan endocrine and paracrinesystemrdquo Endocrinology vol 144 no 6 pp 2179ndash2183 2003
[17] A Nguyen Dinh Cat and RM Touyz ldquoA new look at the renin-angiotensin systemmdashfocusing on the vascular systemrdquo Peptidesvol 32 no 10 pp 2141ndash2150 2011
[18] U C Brewster and M A Perazella ldquoThe renin-angiotensin-aldosterone system and the kidney effects on kidney diseaserdquoThe American Journal of Medicine vol 116 no 4 pp 263ndash2722004
[19] S Ciampone R Borges I P De Lima F F Mesquita EC Cambiucci and J A R Gontijo ldquoLong-term exerciseattenuates blood pressure responsiveness andmodulates kidneyangiotensin II signalling and urinary sodium excretion in SHRrdquoJournal of the Renin-Angiotensin-Aldosterone System vol 12 no4 pp 394ndash403 2011
[20] D Agarwal M A Welsch J N Keller and J Francis ldquoChronicexercise modulates RAS components and improves balancebetween pro- and anti-inflammatory cytokines in the brain of
10 BioMed Research International
SHRrdquo Basic Research in Cardiology vol 106 no 6 pp 1069ndash1085 2011
[21] E J Howden R G Fassett N M Isbel and J S CoombesldquoExercise training in chronic kidney disease patientsrdquo SportsMedicine vol 42 no 6 pp 473ndash488 2012
[22] S Nielsen A Schmitz M Rehling and C E Mogensen ldquoSys-tolic blood pressure relates to the rate of decline of glomerularfiltration rate in type II diabetesrdquo Diabetes Care vol 16 no 11pp 1427ndash1432 1993
[23] A E Tjoslashnna I M Leinan A T Bartnes et al ldquoLow- and high-volume of intensive endurance training significantly improvesmaximal oxygen uptake after 10-weeks of training in healthymenrdquo PLoS ONE vol 8 no 5 Article ID e65382 2013
[24] T Moholdt E Madssen Oslash Rognmo and I L Aamot ldquoThehigher the better Interval training intensity in coronary heartdiseaserdquo Journal of Science and Medicine in Sport vol 17 no 5pp 506ndash510 2014
[25] H E Molmen-Hansen T Stolen A E Tjonna et al ldquoAerobicinterval training reduces blood pressure and improves myocar-dial function in hypertensive patientsrdquo European Journal ofPreventive Cardiology vol 19 no 2 pp 151ndash160 2012
[26] T Moholdt I L Aamot I Granoslashien et al ldquoAerobic intervaltraining increases peak oxygen uptake more than usual careexercise training in myocardial infarction patients a random-ized controlled studyrdquo Clinical Rehabilitation vol 26 no 1 pp33ndash44 2012
[27] E J Howden J S Coombes H Strand B Douglas K LCampbell and N M Isbel ldquoExercise training in CKD efficacyadherence and safetyrdquoAmerican Journal of KidneyDiseases vol65 no 4 pp 583ndash591 2015
[28] A C KingW L Haskell D R Young R K Oka andM L Ste-fanick ldquoLong-term effects of varying intensities and formats ofphysical activity on participation rates fitness and lipoproteinsin men and women aged 50 to 65 yearsrdquo Circulation vol 91 no10 pp 2596ndash2604 1995
[29] G A Brooks and T P White ldquoDetermination of metabolicand heart rate responses of rats to treadmill exerciserdquo Journalof Applied Physiology Respiratory Environmental and ExercisePhysiology vol 45 no 6 pp 1009ndash1015 1978
[30] Y Yu J C Fuscoe C Zhao et al ldquoA rat RNA-Seq transcriptomicBodyMap across 11 organs and 4 developmental stagesrdquo NatureCommunications vol 5 article 3230 2014
[31] F Z Marques A E Campain M Tomaszewski et al ldquoGeneexpression profiling reveals renin mRNA overexpression inhuman hypertensive kidneys and a role formicroRNAsrdquoHyper-tension vol 58 no 6 pp 1093ndash1098 2011
[32] K J Livak and T D Schmittgen ldquoAnalysis of relative geneexpression data using real-time quantitative PCRand the 2minusΔΔ119862TmethodrdquoMethods vol 25 no 4 pp 402ndash408 2001
[33] Y Friedlander J D Kark S Eisenberg and Y Stein ldquoCalcula-tion of LDL-cholesterol from total cholesterol triglyceride andHDL-cholesterol a comparison of methods in the JerusalemLipid Research Clinic Prevalence Studyrdquo Israel Journal of Medi-cal Sciences vol 18 no 12 pp 1242ndash1252 1982
[34] K DMarcus andCM Tipton ldquoExercise training and its effectswith renal hypertensive ratsrdquo Journal of Applied Physiology vol59 no 5 pp 1410ndash1415 1985
[35] K Kitada H Kobori and A Nishiyama ldquoLiver-specificangiotensinogen suppression an old yet novel target forblood pressure control through RAS inhibitionrdquo HypertensionResearch vol 37 no 5 pp 393ndash394 2014
[36] J Gardes J Bouhnik E Clauser P Corvol and JMenard ldquoRoleof angiotensinogen in blood pressure homeostasisrdquo Hyperten-sion vol 4 no 2 pp 185ndash189 1982
[37] K Tanimoto F Sugiyama Y Goto et al ldquoAngiotensinogen-deficient mice with hypotensionrdquo The Journal of BiologicalChemistry vol 269 no 50 pp 31334ndash31337 1994
[38] S Kimura J J Mullins B Bunnemann et al ldquoHigh bloodpressure in transgenic mice carrying the rat angiotensinogengenerdquoThe EMBO Journal vol 11 no 3 pp 821ndash827 1992
[39] JMenard A-I K El Amrani F Savoie J Bouhnik K R LynchandM J Peach ldquoAngiotensinogen an attractive and underratedparticipant in hypertension and inflammationrdquo Hypertensionvol 18 no 5 pp 705ndash707 1991
[40] S Agrawal S Agarwal and S Naik ldquoGenetic contributionand associated pathophysiology in end-stage renal diseaserdquoTheApplication of Clinical Genetics vol 3 pp 65ndash84 2010
[41] W-C Cheng W-Y Shu C-Y Li et al ldquoIntra- and inter-individual variance of gene expression in clinical studiesrdquo PLoSONE vol 7 no 6 Article ID e38650 2012
[42] A Whitehead and D L Crawford ldquoVariation in tissue-specificgene expression among natural populationsrdquo Genome Biologyvol 6 no 2 article R13 2005
[43] A L Oberg B M Bot D E Grill G A Poland and TM Therneau ldquoTechnical and biological variance structure inmRNA-Seq data life in the real worldrdquo BMC Genomics vol 13no 1 article 304 2012
[44] D Agarwal C M Elks S D Reed N Mariappan D SA Majid and J Francis ldquoChronic exercise preserves renalstructure and hemodynamics in spontaneously hypertensiveratsrdquo Antioxidants amp Redox Signaling vol 16 no 2 pp 139ndash1522012
[45] P Zamboli L De Nicola R Minutolo V Bertino F Catapanoand G Conte ldquoManagement of hypertension in chronic kidneydiseaserdquoCurrentHypertensionReports vol 8 no 6 pp 497ndash5012006
[46] G Remuzzi N Perico M Macia and P Ruggenenti ldquoThe roleof renin-angiotensin-aldosterone system in the progression ofchronic kidney diseaserdquo Kidney International vol 68 no 99pp S57ndashS65 2005
[47] N Ouerghi M Feki N Kaabachi M Khammassi S Boukor-raa and A Bouassida ldquoEffects of a high-intensity intermittenttraining programon aerobic capacity and lipid profile in trainedsubjectsrdquoOpenAccess Journal of SportsMedicine vol 5 pp 243ndash248 2014
[48] A Paoli Q F Pacelli T Moro et al ldquoEffects of high-intensitycircuit training low-intensity circuit training and endurancetraining on blood pressure and lipoproteins in middle-agedoverweight menrdquo Lipids in Health and Disease vol 12 no 1article 131 2013
[49] G Racil O Ben Ounis O Hammouda et al ldquoEffects of highvs Moderate exercise intensity during interval training onlipids and adiponectin levels in obese young femalesrdquo EuropeanJournal of Applied Physiology vol 113 no 10 pp 2531ndash25402013
[50] H S Kessler S B Sisson and K R Short ldquoThe potentialfor high-intensity interval training to reduce cardiometabolicdisease riskrdquo Sports Medicine vol 42 no 6 pp 489ndash509 2012
[51] J Poss F Custodis CWernerOWeingartnerM Bohm andULaufs ldquoCardiovascular disease and dyslipidemia beyond LDLrdquoCurrent Pharmaceutical Design vol 17 no 9 pp 861ndash870 2011
BioMed Research International 11
[52] J R Burnett ldquoLipids lipoproteins atherosclerosis and cardio-vascular diseaserdquoThe Clinical Biochemist Reviews vol 25 no 1p 2 2004
[53] G Piecha M Adamczak and E Ritz ldquoDyslipidemia in chronickidney disease pathogenesis and interventionrdquo Polskie Archi-wum Medycyny Wewnetrznej vol 119 no 7-8 pp 487ndash4922009
[54] N A Smart A D Williams I Levinger et al ldquoExercise ampSports Science Australia (ESSA) position statement on exerciseand chronic kidney diseaserdquo Journal of Science and Medicine inSport vol 16 no 5 pp 406ndash411 2013
[55] S-J Pinto-Sietsma W M T Janssen H L Hillege G NavisD de Zeeuw and P E de Jong ldquoUrinary albumin excretion isassociated with renal functional abnormalities in a nondiabeticpopulationrdquo Journal of the American Society of Nephrology vol11 no 10 pp 1882ndash1888 2000
[56] N R Shah and F Dumler ldquoHypoalbuminaemiamdasha marker ofcardiovascular disease in patients with chronic kidney diseasestages II-IVrdquo International Journal ofMedical Sciences vol 5 no6 pp 366ndash370 2008
[57] N E Straznicky M T Grima E A Lambert et al ldquoExerciseaugments weight loss induced improvement in renal functionin obese metabolic syndrome individualsrdquo Journal of Hyperten-sion vol 29 no 3 pp 553ndash564 2011
[58] R D Manning Jr N Tian and S Meng ldquoOxidative stress andantioxidant treatment in hypertension and the associated renaldamagerdquoAmerican Journal of Nephrology vol 25 no 4 pp 311ndash317 2005
[59] G Keller G Zimmer GMall E Ritz andK Amann ldquoNephronnumber in patients with primary hypertensionrdquo The NewEngland Journal of Medicine vol 348 no 2 pp 101ndash108 2003
[60] J Floege M W Burns C E Alpers et al ldquoGlomerular cellproliferation and PDGF expression precede glomerulosclerosisin the remnant kidney modelrdquo Kidney International vol 41 no2 pp 297ndash309 1992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

6 BioMed Research International
200
160
120
080
040
000
200
160
120
080
040
000
200
160
120
080
040
000
SED (n = 12) LIT (n = 13) HIIT (n = 14) SED (n = 12) LIT (n = 13) HIIT (n = 14)
SED (n = 12) SED (n = 12)LIT (n = 13) HIIT (n = 14) LIT (n = 13) HIIT (n = 14)
100 053 053061 100 034
039 085
Ren-mRNA expression fold change(norm to GAPDH) (norm to GAPDH)
Ace-mRNA expression fold change
(norm to GAPDH)Agtr1b-mRNA expression fold change
(norm to GAPDH)Cyp11b2-mRNA expression fold change
086043100 100
200
160
120
080
040
000
Figure 1 Renal mRNA expression fold change
Agtr1a Agtr1b and Cyp11b2) was nonsignificantly downreg-ulated in both exercise groups compared to SED HoweverAgt mRNA expression was upregulated in LIT compared toSED (not significant) and HIIT (119901 = 0035) It is worthmentioning that our results are not the first data to suggestthat lower intensity aerobic exercise training may result inunfortunate adaptations in animal models of CKD aerobicexercise training performed at 50ndash70 of VO
2max has beenreported to result in increased resting SBP and decreasedmyocardial capillary density in an animal model of CKD[34]
Differential mRNA expression of Agt may partiallyexplain the nonsignificant (119901 = 0074) difference in SBP inHIIT during Week 8 compared to SED (119901 = 014 +528)and LIT (119901 = 074 +601) The downregulation in themRNA expression of Agt in HIIT may also explain the lackof significant differences in other RAAS genes in this studyThat is a decrease in the mRNA expression of Agt may havequenched the need for any additional significant decreases inthe expression of other RAAS genes This may explain whyeven though there was a near-significant reduction in SBPin HIIT compared to LIT (119901 = 0074) mRNA expression
BioMed Research International 7
p = 0035
118
076084
063
200
160
120
080
040
000
200
160
120
080
040
000
SED (n = 12) LIT (n = 13) HIIT (n = 14)
SED (n = 12) LIT (n = 13) HIIT (n = 14)
Agtr1a-mRNA expression fold change(norm to GAPDH)
(norm to GAPDH)Agt-mRNA expression fold change
100
100
Figure 2 Hepatic mRNA expression fold change
of several RAAS-related of genes (Ace Ren Agtr1b andCyp11b2) was slightly but not significantly increased in HIITcompared to LIT A review on hepatic angiotensinogen [35]discusses the noteworthy influence that angiotensinogen hason blood pressure Decreased levels of angiotensinogen usingangiotensinogen-antibodies in rats [36] and Agt-knockoutmice [37] exhibit lower blood pressure relative to controlsConversely angiotensinogen infusion in mice [38] and Agtoverexpression in rats [39] result in increased blood pressureEvidence suggests that angiotensinogen is a more potentinfluencer of blood pressure than previously suspected [35
Table 3 Nonrepeated clinical and anthropometric measures
Clinicalmeasure Group Mean Standard
deviationMean duplicate
CV
HDL (mgmL)SED 082 013
006LIT 088 015HIIT 093 012
LDL (mgmL)SED 127 027
003LIT 155 034HIIT 108lowast 032
TAG (mgmL)SED 565 166
004LIT 635 265HIIT 411lowast 204
CHOL(mgmL)
SED 322 047NALIT 371 061
HIIT 283lowast 073
CRE(nmol120583L)
SED 107 051004LIT 206 179
HIIT 211 126
ALB (mgmL)SED 2623 384
004LIT 2988 642HIIT 3524dagger 608
Kidney weight(g)
SED 157 009NALIT 159 012
HIIT 146dagger 008
KW-BW ratioSED 00050 00003
NALIT 00050 00003HIIT 00047dagger 00002
Significance set at 119901 le 005lowastSignificantly different from LITdaggerSignificantly different from LIT and SEDHDL high density lipoprotein LDL low density lipoprotein TAG triglyc-erides CHOL total cholesterol CRE creatinine ALB albumin KW-BWkidney weight-body weight CV coefficient of variation
39] often more influential than other components of RAAS[40] and deserves more attention as a potential targetin hypertension-related therapies [35] proposals that aresupported by our findings
Large amounts of between-animal variation in themRNAexpression of RAAS-related genes in SED may explain thelack of significant results in the current study Duplicate-duplicate variation was low (CV = 001) suggesting largeamounts of between-animal variation in SED The issueof between-animal mRNA variation has been empiricallyaddressed in the past [41ndash43] with the most commonlysuggested remedy being an increase in sample size Inter-estingly variation in between-animal mRNA expression inSED is higher across all genes (except for Agt) comparedto LIT and HIIT similar to previous work that has exam-ined RAAS-related mRNA expression in sedentary versusexercise-trained SHRs [20 44] This combined with the factthat aerobic exercise resulted in a downregulation across allgenes compared to SED (expect for Agt in LIT) suggeststhat RAAS-related mRNA expression may be poorly and
8 BioMed Research International
Table 4 Repeated clinical and anthropometric measures
Clinical measure Group Baseline 4 Weekslowast 8 Weeksdagger
(Preintervention) (Mid-Intervention) (Postintervention)
Body length (cm)SED 2848 (186) 3503 (085) 3741 (106)LIT 2932 (165) 3515 (079) 3789 (088)HIIT 2961 (225) 3546 (065) 3787 (062)
Body weight (g)SED 22442 (1782) 27605 (1831) 31353 (1662)LIT 23159 (2101) 27742 (2077) 31825 (2103)HIIT 23090 (1998) 27487 (1646) 30816 (1758)
BL-BW ratioSED 0126 (0007) 0127 (0007) 0120 (0004)LIT 0127 (0009) 0128 (0007) 0119 (0009)HIIT 0129 (0007) 0130 (0008) 0124 (0006)
Systolic blood pressure (mmHg)SED 17557 (927) 20777 (1739) 23977 (1285)LIT 17309 (945) 20925 (231) 24163 (2142)HIIT 17465 (1482) 21625 (1624) 22712 (1423)
Values presented as mean (standard deviation)Significance set at 119901 le 005lowastSignificantly different compared to baseline for all groupsdaggerSignificantly different compared to baseline and 4 weeks for all groupsBL-BW body length-body weight
indiscriminately regulated in the absence of aerobic exercisein an animal model of early-stage CKD That is aerobicexercise may help to control otherwise haphazard RAAS-related mRNA expression that occurs during the early stagesof CKD Several informative reviews have outlined theissue of unregulated blood pressure control [45] and morespecifically unregulated RAAS activity [46] in CKD but thisis the first study to suggest that one of the mechanisms bywhich aerobic exercise may prove beneficial is via tightenedcontrol of RAAS-related mRNA expression independentof statistically significant improvements to RAAS-relatedmRNA expression
In the current study the significant decreases in plasmaLDL triglycerides and total cholesterol in HIIT compared toLIT but not SED are encouraging and somewhat surprisingA recent study performed in healthy well-trained humansreported nonsignificant improvements in LDL triglyceridesand total cholesterol after 12 weeks of HIIT [47] In spe-cial andor clinical populations HIIT seems to exert moreinfluence over blood lipids Cardiac rehabilitation patientswho engaged in HIIT experienced significant improvementsin HDL relative to traditional aerobic exercise training[26] However triglyceride measurements were not differentbetween groups and LDL measurements were not reported[26] HIIT has also proven to be beneficial in obese men[48] and women [49] resulting in improved HDL [48]LDL [48] triglycerides [48 49] and total cholesterol [4849] Despite the slowly-accumulating data a recent review[50] that notes the ability of HIIT to influence blood lipidshas yet to be established especially in special populationssuggesting that this specific line of research the effects ofHIIT on blood lipids should be further examined This isespecially true in CKD as lipid-related disorders are theleading cause of complications in CVD [51 52] and CVD-related complications are the leading cause of death in CKD
patients [10 11] As such dyslipidemia should be rankedamong the primary concerns of CKD-related research [53]
Similar to blood lipids a recent review notes that theeffects of exercise training on plasma albumin in patientswith CKD are unclear [54] Moreover data describing theeffects of HIIT on plasma albumin in patients with CKD areunavailable Hypoalbuminemia is an independent predictorof renal dysfunction [55] and an independent predictor ofCVD in early-stage CKD [56] and can be used to identifyCKD patients at increased risk of developing CVD [56] Inobese individuals with metabolic syndrome two commoncharacteristics of CKD 12 weeks of aerobic exercise trainingsignificantly reduced albuminuria (urinary albumin) com-pared to a no-exercise control group [57] Aerobic exercisetraining (16 weeks at 60 of maximal aerobic velocity) hasalso proven useful at reducing albuminuria in SHRs [44]Because hypoalbuminemia is related to declining kidneyfunction [55] blood albumin andor urinary albumin areuseful markers for assessing the preservation of renal tissueIn the current study plasma albumin was significantly higherin HIIT compared to SED and LIT suggesting that renalstructure and function are better preserved by HIIT Thepreservation of renal structure and function and subsequentincrease in plasma albumin may have been due to the down-regulation of Agt mRNA expression and the accompanyingdecrease in SBP in HIIT as hypertension is directly related torenal damage [44 58]
Also considered an indicator of renal damage kid-ney weight and kidney weight-body weight ratio weresignificantly lower in HIIT compared to SED and LITHypertension-related declines in renal function are associ-ated with compensatory alterations to renal tissue such astubulointerstitial fibrosis [59 60] Often pathological thesealterations result in glomerular hypertrophy [59 60] Usinghistological and molecular applications 16 weeks of aerobic
BioMed Research International 9
exercise training (performed at 60 of maximal aerobicvelocity) has been shown to reduce renal fibrosis in SHRs[44] Although renal fibrosis and renal hypertrophy aredirectly related data that specifically describes the effectsof HIIT on renal hypertrophy are unavailable Similar tothe mechanisms that account for increased levels of plasmaalbumin in HIIT there is evidence to suggest that thesignificantly lower kidney weight and kidney weight-bodyweight ratios in HIIT compared to SED and LIT may bedue to decreased fibrosis Decreases in renal fibrosis maybe due to decreases in hypertension-mediated renal damagefollowing a downregulation of the mRNA expression of Agtand a decrease in SBP (in HIIT) [44 58]
5 Conclusions
In summary in an animal model of early-stage CKD HIITappeared to be more beneficial compared to SED and LITas HIIT was responsible for a significant downregulation inthe mRNA expression of Agt The downregulated mRNAexpression of Agt along with significant improvements toblood lipids (LDL triglycerides and total cholesterol) maypartially explain the nonsignificant decrease in SBP andsignificant improvements to plasma albumin kidney weightand kidney weight-body weight ratios in HIIT relative toSED and LIT Future work would benefit from examiningRAAS-related protein expression as well as specific measuresof renal histology and morphology Future work would alsobenefit from examining whether the positive HIIT-relatedeffects seen in the present study are apparent in differentrelated disease models (eg nonnephrectomised SHRs or 56nephrectomy SHRs)
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] AIHW Ed Australiarsquos Health 2014 Australiarsquos Health SeriesAustralian Institute of Health and Welfare (AIHW) CanberraAustralia 2014
[2] A S Go G M Chertow D Fan C E McCulloch andC-Y Hsu ldquoChronic kidney disease and the risks of deathcardiovascular events and hospitalizationrdquo The New EnglandJournal of Medicine vol 351 no 13 pp 1296ndash1370 2004
[3] U D Mathisen T Melsom O C Ingebretsen et al ldquoEstimatedGFR associates with cardiovascular risk factors independentlyof measured GFRrdquo Journal of the American Society of Nephrol-ogy vol 22 no 5 pp 927ndash937 2011
[4] DM Silverstein ldquoInflammation in chronic kidney disease rolein the progression of renal and cardiovascular diseaserdquoPediatricNephrology vol 24 no 8 pp 1445ndash1452 2009
[5] P S Tucker M I Kingsley R H Morton A T Scanlan andV J Dalbo ldquoThe increasing financial impact of chronic kidneydisease in Australiardquo International Journal of Nephrology vol2014 Article ID 120537 7 pages 2014
[6] B Stengel M E Tarver-Carr N R Powe M S Eberhardt andF L Brancati ldquoLifestyle factors obesity and the risk of chronickidney diseaserdquo Epidemiology vol 14 no 4 pp 479ndash487 2003
[7] R T Gansevoort R Correa-Rotter B R Hemmelgarn et alldquoChronic kidney disease and cardiovascular risk epidemiologymechanisms and preventionrdquoTheLancet vol 382 no 9889 pp339ndash352 2013
[8] M M H Hermans R Henry J M Dekker et al ldquoEstimatedglomerular filtration rate and urinary albumin excretion areindependently associated with greater arterial stiffness theHoorn studyrdquo Journal of the American Society of Nephrology vol18 no 6 pp 1942ndash1952 2007
[9] M L Ford L A Tomlinson T P E Chapman C Rajkumar andS G Holt ldquoAortic stiffness is independently associated with rateof renal function decline in chronic kidney disease stages 3 and4rdquo Hypertension vol 55 no 5 pp 1110ndash1115 2010
[10] D EWeiner H Tighiouart P C Stark et al ldquoKidney disease asa risk factor for recurrent cardiovascular disease andmortalityrdquoAmerican Journal of Kidney Diseases vol 44 no 2 pp 198ndash2062004
[11] D E Weiner H Tighiouart M G Amin et al ldquoChronickidney disease as a risk factor for cardiovascular disease and all-causemortality a pooled analysis of community-based studiesrdquoJournal of the American Society of Nephrology vol 15 no 5 pp1307ndash1315 2004
[12] R K Soni A C Porter J P Lash and M L Unruh ldquoHealth-related quality of life in hypertension chronic kidney diseaseand coexistent chronic health conditionsrdquo Advances in ChronicKidney Disease vol 17 no 4 pp e17ndashe26 2010
[13] J Segura C Campo P Gil et al ldquoDevelopment of chronickidney disease and cardiovascular prognosis in essential hyper-tensive patientsrdquo Journal of the American Society of Nephrologyvol 15 no 6 pp 1616ndash1622 2004
[14] J Blacher A P Guerin B Pannier S J Marchais M E Safarand G M London ldquoImpact of aortic stiffness on survival inend-stage renal diseaserdquo Circulation vol 99 no 18 pp 2434ndash2439 1999
[15] G L Bakris E Ritz and World Kidney Day Steering Commit-tee ldquoThe message for World Kidney Day 2009 hypertensionand kidney disease a marriage that should be preventedrdquo TheJournal of Clinical Hypertension (Greenwich) vol 11 no 3 pp144ndash147 2009
[16] J L Lavoie and C D Sigmund ldquoMinireview overview ofthe renin-angiotensin systemmdashan endocrine and paracrinesystemrdquo Endocrinology vol 144 no 6 pp 2179ndash2183 2003
[17] A Nguyen Dinh Cat and RM Touyz ldquoA new look at the renin-angiotensin systemmdashfocusing on the vascular systemrdquo Peptidesvol 32 no 10 pp 2141ndash2150 2011
[18] U C Brewster and M A Perazella ldquoThe renin-angiotensin-aldosterone system and the kidney effects on kidney diseaserdquoThe American Journal of Medicine vol 116 no 4 pp 263ndash2722004
[19] S Ciampone R Borges I P De Lima F F Mesquita EC Cambiucci and J A R Gontijo ldquoLong-term exerciseattenuates blood pressure responsiveness andmodulates kidneyangiotensin II signalling and urinary sodium excretion in SHRrdquoJournal of the Renin-Angiotensin-Aldosterone System vol 12 no4 pp 394ndash403 2011
[20] D Agarwal M A Welsch J N Keller and J Francis ldquoChronicexercise modulates RAS components and improves balancebetween pro- and anti-inflammatory cytokines in the brain of
10 BioMed Research International
SHRrdquo Basic Research in Cardiology vol 106 no 6 pp 1069ndash1085 2011
[21] E J Howden R G Fassett N M Isbel and J S CoombesldquoExercise training in chronic kidney disease patientsrdquo SportsMedicine vol 42 no 6 pp 473ndash488 2012
[22] S Nielsen A Schmitz M Rehling and C E Mogensen ldquoSys-tolic blood pressure relates to the rate of decline of glomerularfiltration rate in type II diabetesrdquo Diabetes Care vol 16 no 11pp 1427ndash1432 1993
[23] A E Tjoslashnna I M Leinan A T Bartnes et al ldquoLow- and high-volume of intensive endurance training significantly improvesmaximal oxygen uptake after 10-weeks of training in healthymenrdquo PLoS ONE vol 8 no 5 Article ID e65382 2013
[24] T Moholdt E Madssen Oslash Rognmo and I L Aamot ldquoThehigher the better Interval training intensity in coronary heartdiseaserdquo Journal of Science and Medicine in Sport vol 17 no 5pp 506ndash510 2014
[25] H E Molmen-Hansen T Stolen A E Tjonna et al ldquoAerobicinterval training reduces blood pressure and improves myocar-dial function in hypertensive patientsrdquo European Journal ofPreventive Cardiology vol 19 no 2 pp 151ndash160 2012
[26] T Moholdt I L Aamot I Granoslashien et al ldquoAerobic intervaltraining increases peak oxygen uptake more than usual careexercise training in myocardial infarction patients a random-ized controlled studyrdquo Clinical Rehabilitation vol 26 no 1 pp33ndash44 2012
[27] E J Howden J S Coombes H Strand B Douglas K LCampbell and N M Isbel ldquoExercise training in CKD efficacyadherence and safetyrdquoAmerican Journal of KidneyDiseases vol65 no 4 pp 583ndash591 2015
[28] A C KingW L Haskell D R Young R K Oka andM L Ste-fanick ldquoLong-term effects of varying intensities and formats ofphysical activity on participation rates fitness and lipoproteinsin men and women aged 50 to 65 yearsrdquo Circulation vol 91 no10 pp 2596ndash2604 1995
[29] G A Brooks and T P White ldquoDetermination of metabolicand heart rate responses of rats to treadmill exerciserdquo Journalof Applied Physiology Respiratory Environmental and ExercisePhysiology vol 45 no 6 pp 1009ndash1015 1978
[30] Y Yu J C Fuscoe C Zhao et al ldquoA rat RNA-Seq transcriptomicBodyMap across 11 organs and 4 developmental stagesrdquo NatureCommunications vol 5 article 3230 2014
[31] F Z Marques A E Campain M Tomaszewski et al ldquoGeneexpression profiling reveals renin mRNA overexpression inhuman hypertensive kidneys and a role formicroRNAsrdquoHyper-tension vol 58 no 6 pp 1093ndash1098 2011
[32] K J Livak and T D Schmittgen ldquoAnalysis of relative geneexpression data using real-time quantitative PCRand the 2minusΔΔ119862TmethodrdquoMethods vol 25 no 4 pp 402ndash408 2001
[33] Y Friedlander J D Kark S Eisenberg and Y Stein ldquoCalcula-tion of LDL-cholesterol from total cholesterol triglyceride andHDL-cholesterol a comparison of methods in the JerusalemLipid Research Clinic Prevalence Studyrdquo Israel Journal of Medi-cal Sciences vol 18 no 12 pp 1242ndash1252 1982
[34] K DMarcus andCM Tipton ldquoExercise training and its effectswith renal hypertensive ratsrdquo Journal of Applied Physiology vol59 no 5 pp 1410ndash1415 1985
[35] K Kitada H Kobori and A Nishiyama ldquoLiver-specificangiotensinogen suppression an old yet novel target forblood pressure control through RAS inhibitionrdquo HypertensionResearch vol 37 no 5 pp 393ndash394 2014
[36] J Gardes J Bouhnik E Clauser P Corvol and JMenard ldquoRoleof angiotensinogen in blood pressure homeostasisrdquo Hyperten-sion vol 4 no 2 pp 185ndash189 1982
[37] K Tanimoto F Sugiyama Y Goto et al ldquoAngiotensinogen-deficient mice with hypotensionrdquo The Journal of BiologicalChemistry vol 269 no 50 pp 31334ndash31337 1994
[38] S Kimura J J Mullins B Bunnemann et al ldquoHigh bloodpressure in transgenic mice carrying the rat angiotensinogengenerdquoThe EMBO Journal vol 11 no 3 pp 821ndash827 1992
[39] JMenard A-I K El Amrani F Savoie J Bouhnik K R LynchandM J Peach ldquoAngiotensinogen an attractive and underratedparticipant in hypertension and inflammationrdquo Hypertensionvol 18 no 5 pp 705ndash707 1991
[40] S Agrawal S Agarwal and S Naik ldquoGenetic contributionand associated pathophysiology in end-stage renal diseaserdquoTheApplication of Clinical Genetics vol 3 pp 65ndash84 2010
[41] W-C Cheng W-Y Shu C-Y Li et al ldquoIntra- and inter-individual variance of gene expression in clinical studiesrdquo PLoSONE vol 7 no 6 Article ID e38650 2012
[42] A Whitehead and D L Crawford ldquoVariation in tissue-specificgene expression among natural populationsrdquo Genome Biologyvol 6 no 2 article R13 2005
[43] A L Oberg B M Bot D E Grill G A Poland and TM Therneau ldquoTechnical and biological variance structure inmRNA-Seq data life in the real worldrdquo BMC Genomics vol 13no 1 article 304 2012
[44] D Agarwal C M Elks S D Reed N Mariappan D SA Majid and J Francis ldquoChronic exercise preserves renalstructure and hemodynamics in spontaneously hypertensiveratsrdquo Antioxidants amp Redox Signaling vol 16 no 2 pp 139ndash1522012
[45] P Zamboli L De Nicola R Minutolo V Bertino F Catapanoand G Conte ldquoManagement of hypertension in chronic kidneydiseaserdquoCurrentHypertensionReports vol 8 no 6 pp 497ndash5012006
[46] G Remuzzi N Perico M Macia and P Ruggenenti ldquoThe roleof renin-angiotensin-aldosterone system in the progression ofchronic kidney diseaserdquo Kidney International vol 68 no 99pp S57ndashS65 2005
[47] N Ouerghi M Feki N Kaabachi M Khammassi S Boukor-raa and A Bouassida ldquoEffects of a high-intensity intermittenttraining programon aerobic capacity and lipid profile in trainedsubjectsrdquoOpenAccess Journal of SportsMedicine vol 5 pp 243ndash248 2014
[48] A Paoli Q F Pacelli T Moro et al ldquoEffects of high-intensitycircuit training low-intensity circuit training and endurancetraining on blood pressure and lipoproteins in middle-agedoverweight menrdquo Lipids in Health and Disease vol 12 no 1article 131 2013
[49] G Racil O Ben Ounis O Hammouda et al ldquoEffects of highvs Moderate exercise intensity during interval training onlipids and adiponectin levels in obese young femalesrdquo EuropeanJournal of Applied Physiology vol 113 no 10 pp 2531ndash25402013
[50] H S Kessler S B Sisson and K R Short ldquoThe potentialfor high-intensity interval training to reduce cardiometabolicdisease riskrdquo Sports Medicine vol 42 no 6 pp 489ndash509 2012
[51] J Poss F Custodis CWernerOWeingartnerM Bohm andULaufs ldquoCardiovascular disease and dyslipidemia beyond LDLrdquoCurrent Pharmaceutical Design vol 17 no 9 pp 861ndash870 2011
BioMed Research International 11
[52] J R Burnett ldquoLipids lipoproteins atherosclerosis and cardio-vascular diseaserdquoThe Clinical Biochemist Reviews vol 25 no 1p 2 2004
[53] G Piecha M Adamczak and E Ritz ldquoDyslipidemia in chronickidney disease pathogenesis and interventionrdquo Polskie Archi-wum Medycyny Wewnetrznej vol 119 no 7-8 pp 487ndash4922009
[54] N A Smart A D Williams I Levinger et al ldquoExercise ampSports Science Australia (ESSA) position statement on exerciseand chronic kidney diseaserdquo Journal of Science and Medicine inSport vol 16 no 5 pp 406ndash411 2013
[55] S-J Pinto-Sietsma W M T Janssen H L Hillege G NavisD de Zeeuw and P E de Jong ldquoUrinary albumin excretion isassociated with renal functional abnormalities in a nondiabeticpopulationrdquo Journal of the American Society of Nephrology vol11 no 10 pp 1882ndash1888 2000
[56] N R Shah and F Dumler ldquoHypoalbuminaemiamdasha marker ofcardiovascular disease in patients with chronic kidney diseasestages II-IVrdquo International Journal ofMedical Sciences vol 5 no6 pp 366ndash370 2008
[57] N E Straznicky M T Grima E A Lambert et al ldquoExerciseaugments weight loss induced improvement in renal functionin obese metabolic syndrome individualsrdquo Journal of Hyperten-sion vol 29 no 3 pp 553ndash564 2011
[58] R D Manning Jr N Tian and S Meng ldquoOxidative stress andantioxidant treatment in hypertension and the associated renaldamagerdquoAmerican Journal of Nephrology vol 25 no 4 pp 311ndash317 2005
[59] G Keller G Zimmer GMall E Ritz andK Amann ldquoNephronnumber in patients with primary hypertensionrdquo The NewEngland Journal of Medicine vol 348 no 2 pp 101ndash108 2003
[60] J Floege M W Burns C E Alpers et al ldquoGlomerular cellproliferation and PDGF expression precede glomerulosclerosisin the remnant kidney modelrdquo Kidney International vol 41 no2 pp 297ndash309 1992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 7
p = 0035
118
076084
063
200
160
120
080
040
000
200
160
120
080
040
000
SED (n = 12) LIT (n = 13) HIIT (n = 14)
SED (n = 12) LIT (n = 13) HIIT (n = 14)
Agtr1a-mRNA expression fold change(norm to GAPDH)
(norm to GAPDH)Agt-mRNA expression fold change
100
100
Figure 2 Hepatic mRNA expression fold change
of several RAAS-related of genes (Ace Ren Agtr1b andCyp11b2) was slightly but not significantly increased in HIITcompared to LIT A review on hepatic angiotensinogen [35]discusses the noteworthy influence that angiotensinogen hason blood pressure Decreased levels of angiotensinogen usingangiotensinogen-antibodies in rats [36] and Agt-knockoutmice [37] exhibit lower blood pressure relative to controlsConversely angiotensinogen infusion in mice [38] and Agtoverexpression in rats [39] result in increased blood pressureEvidence suggests that angiotensinogen is a more potentinfluencer of blood pressure than previously suspected [35
Table 3 Nonrepeated clinical and anthropometric measures
Clinicalmeasure Group Mean Standard
deviationMean duplicate
CV
HDL (mgmL)SED 082 013
006LIT 088 015HIIT 093 012
LDL (mgmL)SED 127 027
003LIT 155 034HIIT 108lowast 032
TAG (mgmL)SED 565 166
004LIT 635 265HIIT 411lowast 204
CHOL(mgmL)
SED 322 047NALIT 371 061
HIIT 283lowast 073
CRE(nmol120583L)
SED 107 051004LIT 206 179
HIIT 211 126
ALB (mgmL)SED 2623 384
004LIT 2988 642HIIT 3524dagger 608
Kidney weight(g)
SED 157 009NALIT 159 012
HIIT 146dagger 008
KW-BW ratioSED 00050 00003
NALIT 00050 00003HIIT 00047dagger 00002
Significance set at 119901 le 005lowastSignificantly different from LITdaggerSignificantly different from LIT and SEDHDL high density lipoprotein LDL low density lipoprotein TAG triglyc-erides CHOL total cholesterol CRE creatinine ALB albumin KW-BWkidney weight-body weight CV coefficient of variation
39] often more influential than other components of RAAS[40] and deserves more attention as a potential targetin hypertension-related therapies [35] proposals that aresupported by our findings
Large amounts of between-animal variation in themRNAexpression of RAAS-related genes in SED may explain thelack of significant results in the current study Duplicate-duplicate variation was low (CV = 001) suggesting largeamounts of between-animal variation in SED The issueof between-animal mRNA variation has been empiricallyaddressed in the past [41ndash43] with the most commonlysuggested remedy being an increase in sample size Inter-estingly variation in between-animal mRNA expression inSED is higher across all genes (except for Agt) comparedto LIT and HIIT similar to previous work that has exam-ined RAAS-related mRNA expression in sedentary versusexercise-trained SHRs [20 44] This combined with the factthat aerobic exercise resulted in a downregulation across allgenes compared to SED (expect for Agt in LIT) suggeststhat RAAS-related mRNA expression may be poorly and
8 BioMed Research International
Table 4 Repeated clinical and anthropometric measures
Clinical measure Group Baseline 4 Weekslowast 8 Weeksdagger
(Preintervention) (Mid-Intervention) (Postintervention)
Body length (cm)SED 2848 (186) 3503 (085) 3741 (106)LIT 2932 (165) 3515 (079) 3789 (088)HIIT 2961 (225) 3546 (065) 3787 (062)
Body weight (g)SED 22442 (1782) 27605 (1831) 31353 (1662)LIT 23159 (2101) 27742 (2077) 31825 (2103)HIIT 23090 (1998) 27487 (1646) 30816 (1758)
BL-BW ratioSED 0126 (0007) 0127 (0007) 0120 (0004)LIT 0127 (0009) 0128 (0007) 0119 (0009)HIIT 0129 (0007) 0130 (0008) 0124 (0006)
Systolic blood pressure (mmHg)SED 17557 (927) 20777 (1739) 23977 (1285)LIT 17309 (945) 20925 (231) 24163 (2142)HIIT 17465 (1482) 21625 (1624) 22712 (1423)
Values presented as mean (standard deviation)Significance set at 119901 le 005lowastSignificantly different compared to baseline for all groupsdaggerSignificantly different compared to baseline and 4 weeks for all groupsBL-BW body length-body weight
indiscriminately regulated in the absence of aerobic exercisein an animal model of early-stage CKD That is aerobicexercise may help to control otherwise haphazard RAAS-related mRNA expression that occurs during the early stagesof CKD Several informative reviews have outlined theissue of unregulated blood pressure control [45] and morespecifically unregulated RAAS activity [46] in CKD but thisis the first study to suggest that one of the mechanisms bywhich aerobic exercise may prove beneficial is via tightenedcontrol of RAAS-related mRNA expression independentof statistically significant improvements to RAAS-relatedmRNA expression
In the current study the significant decreases in plasmaLDL triglycerides and total cholesterol in HIIT compared toLIT but not SED are encouraging and somewhat surprisingA recent study performed in healthy well-trained humansreported nonsignificant improvements in LDL triglyceridesand total cholesterol after 12 weeks of HIIT [47] In spe-cial andor clinical populations HIIT seems to exert moreinfluence over blood lipids Cardiac rehabilitation patientswho engaged in HIIT experienced significant improvementsin HDL relative to traditional aerobic exercise training[26] However triglyceride measurements were not differentbetween groups and LDL measurements were not reported[26] HIIT has also proven to be beneficial in obese men[48] and women [49] resulting in improved HDL [48]LDL [48] triglycerides [48 49] and total cholesterol [4849] Despite the slowly-accumulating data a recent review[50] that notes the ability of HIIT to influence blood lipidshas yet to be established especially in special populationssuggesting that this specific line of research the effects ofHIIT on blood lipids should be further examined This isespecially true in CKD as lipid-related disorders are theleading cause of complications in CVD [51 52] and CVD-related complications are the leading cause of death in CKD
patients [10 11] As such dyslipidemia should be rankedamong the primary concerns of CKD-related research [53]
Similar to blood lipids a recent review notes that theeffects of exercise training on plasma albumin in patientswith CKD are unclear [54] Moreover data describing theeffects of HIIT on plasma albumin in patients with CKD areunavailable Hypoalbuminemia is an independent predictorof renal dysfunction [55] and an independent predictor ofCVD in early-stage CKD [56] and can be used to identifyCKD patients at increased risk of developing CVD [56] Inobese individuals with metabolic syndrome two commoncharacteristics of CKD 12 weeks of aerobic exercise trainingsignificantly reduced albuminuria (urinary albumin) com-pared to a no-exercise control group [57] Aerobic exercisetraining (16 weeks at 60 of maximal aerobic velocity) hasalso proven useful at reducing albuminuria in SHRs [44]Because hypoalbuminemia is related to declining kidneyfunction [55] blood albumin andor urinary albumin areuseful markers for assessing the preservation of renal tissueIn the current study plasma albumin was significantly higherin HIIT compared to SED and LIT suggesting that renalstructure and function are better preserved by HIIT Thepreservation of renal structure and function and subsequentincrease in plasma albumin may have been due to the down-regulation of Agt mRNA expression and the accompanyingdecrease in SBP in HIIT as hypertension is directly related torenal damage [44 58]
Also considered an indicator of renal damage kid-ney weight and kidney weight-body weight ratio weresignificantly lower in HIIT compared to SED and LITHypertension-related declines in renal function are associ-ated with compensatory alterations to renal tissue such astubulointerstitial fibrosis [59 60] Often pathological thesealterations result in glomerular hypertrophy [59 60] Usinghistological and molecular applications 16 weeks of aerobic
BioMed Research International 9
exercise training (performed at 60 of maximal aerobicvelocity) has been shown to reduce renal fibrosis in SHRs[44] Although renal fibrosis and renal hypertrophy aredirectly related data that specifically describes the effectsof HIIT on renal hypertrophy are unavailable Similar tothe mechanisms that account for increased levels of plasmaalbumin in HIIT there is evidence to suggest that thesignificantly lower kidney weight and kidney weight-bodyweight ratios in HIIT compared to SED and LIT may bedue to decreased fibrosis Decreases in renal fibrosis maybe due to decreases in hypertension-mediated renal damagefollowing a downregulation of the mRNA expression of Agtand a decrease in SBP (in HIIT) [44 58]
5 Conclusions
In summary in an animal model of early-stage CKD HIITappeared to be more beneficial compared to SED and LITas HIIT was responsible for a significant downregulation inthe mRNA expression of Agt The downregulated mRNAexpression of Agt along with significant improvements toblood lipids (LDL triglycerides and total cholesterol) maypartially explain the nonsignificant decrease in SBP andsignificant improvements to plasma albumin kidney weightand kidney weight-body weight ratios in HIIT relative toSED and LIT Future work would benefit from examiningRAAS-related protein expression as well as specific measuresof renal histology and morphology Future work would alsobenefit from examining whether the positive HIIT-relatedeffects seen in the present study are apparent in differentrelated disease models (eg nonnephrectomised SHRs or 56nephrectomy SHRs)
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] AIHW Ed Australiarsquos Health 2014 Australiarsquos Health SeriesAustralian Institute of Health and Welfare (AIHW) CanberraAustralia 2014
[2] A S Go G M Chertow D Fan C E McCulloch andC-Y Hsu ldquoChronic kidney disease and the risks of deathcardiovascular events and hospitalizationrdquo The New EnglandJournal of Medicine vol 351 no 13 pp 1296ndash1370 2004
[3] U D Mathisen T Melsom O C Ingebretsen et al ldquoEstimatedGFR associates with cardiovascular risk factors independentlyof measured GFRrdquo Journal of the American Society of Nephrol-ogy vol 22 no 5 pp 927ndash937 2011
[4] DM Silverstein ldquoInflammation in chronic kidney disease rolein the progression of renal and cardiovascular diseaserdquoPediatricNephrology vol 24 no 8 pp 1445ndash1452 2009
[5] P S Tucker M I Kingsley R H Morton A T Scanlan andV J Dalbo ldquoThe increasing financial impact of chronic kidneydisease in Australiardquo International Journal of Nephrology vol2014 Article ID 120537 7 pages 2014
[6] B Stengel M E Tarver-Carr N R Powe M S Eberhardt andF L Brancati ldquoLifestyle factors obesity and the risk of chronickidney diseaserdquo Epidemiology vol 14 no 4 pp 479ndash487 2003
[7] R T Gansevoort R Correa-Rotter B R Hemmelgarn et alldquoChronic kidney disease and cardiovascular risk epidemiologymechanisms and preventionrdquoTheLancet vol 382 no 9889 pp339ndash352 2013
[8] M M H Hermans R Henry J M Dekker et al ldquoEstimatedglomerular filtration rate and urinary albumin excretion areindependently associated with greater arterial stiffness theHoorn studyrdquo Journal of the American Society of Nephrology vol18 no 6 pp 1942ndash1952 2007
[9] M L Ford L A Tomlinson T P E Chapman C Rajkumar andS G Holt ldquoAortic stiffness is independently associated with rateof renal function decline in chronic kidney disease stages 3 and4rdquo Hypertension vol 55 no 5 pp 1110ndash1115 2010
[10] D EWeiner H Tighiouart P C Stark et al ldquoKidney disease asa risk factor for recurrent cardiovascular disease andmortalityrdquoAmerican Journal of Kidney Diseases vol 44 no 2 pp 198ndash2062004
[11] D E Weiner H Tighiouart M G Amin et al ldquoChronickidney disease as a risk factor for cardiovascular disease and all-causemortality a pooled analysis of community-based studiesrdquoJournal of the American Society of Nephrology vol 15 no 5 pp1307ndash1315 2004
[12] R K Soni A C Porter J P Lash and M L Unruh ldquoHealth-related quality of life in hypertension chronic kidney diseaseand coexistent chronic health conditionsrdquo Advances in ChronicKidney Disease vol 17 no 4 pp e17ndashe26 2010
[13] J Segura C Campo P Gil et al ldquoDevelopment of chronickidney disease and cardiovascular prognosis in essential hyper-tensive patientsrdquo Journal of the American Society of Nephrologyvol 15 no 6 pp 1616ndash1622 2004
[14] J Blacher A P Guerin B Pannier S J Marchais M E Safarand G M London ldquoImpact of aortic stiffness on survival inend-stage renal diseaserdquo Circulation vol 99 no 18 pp 2434ndash2439 1999
[15] G L Bakris E Ritz and World Kidney Day Steering Commit-tee ldquoThe message for World Kidney Day 2009 hypertensionand kidney disease a marriage that should be preventedrdquo TheJournal of Clinical Hypertension (Greenwich) vol 11 no 3 pp144ndash147 2009
[16] J L Lavoie and C D Sigmund ldquoMinireview overview ofthe renin-angiotensin systemmdashan endocrine and paracrinesystemrdquo Endocrinology vol 144 no 6 pp 2179ndash2183 2003
[17] A Nguyen Dinh Cat and RM Touyz ldquoA new look at the renin-angiotensin systemmdashfocusing on the vascular systemrdquo Peptidesvol 32 no 10 pp 2141ndash2150 2011
[18] U C Brewster and M A Perazella ldquoThe renin-angiotensin-aldosterone system and the kidney effects on kidney diseaserdquoThe American Journal of Medicine vol 116 no 4 pp 263ndash2722004
[19] S Ciampone R Borges I P De Lima F F Mesquita EC Cambiucci and J A R Gontijo ldquoLong-term exerciseattenuates blood pressure responsiveness andmodulates kidneyangiotensin II signalling and urinary sodium excretion in SHRrdquoJournal of the Renin-Angiotensin-Aldosterone System vol 12 no4 pp 394ndash403 2011
[20] D Agarwal M A Welsch J N Keller and J Francis ldquoChronicexercise modulates RAS components and improves balancebetween pro- and anti-inflammatory cytokines in the brain of
10 BioMed Research International
SHRrdquo Basic Research in Cardiology vol 106 no 6 pp 1069ndash1085 2011
[21] E J Howden R G Fassett N M Isbel and J S CoombesldquoExercise training in chronic kidney disease patientsrdquo SportsMedicine vol 42 no 6 pp 473ndash488 2012
[22] S Nielsen A Schmitz M Rehling and C E Mogensen ldquoSys-tolic blood pressure relates to the rate of decline of glomerularfiltration rate in type II diabetesrdquo Diabetes Care vol 16 no 11pp 1427ndash1432 1993
[23] A E Tjoslashnna I M Leinan A T Bartnes et al ldquoLow- and high-volume of intensive endurance training significantly improvesmaximal oxygen uptake after 10-weeks of training in healthymenrdquo PLoS ONE vol 8 no 5 Article ID e65382 2013
[24] T Moholdt E Madssen Oslash Rognmo and I L Aamot ldquoThehigher the better Interval training intensity in coronary heartdiseaserdquo Journal of Science and Medicine in Sport vol 17 no 5pp 506ndash510 2014
[25] H E Molmen-Hansen T Stolen A E Tjonna et al ldquoAerobicinterval training reduces blood pressure and improves myocar-dial function in hypertensive patientsrdquo European Journal ofPreventive Cardiology vol 19 no 2 pp 151ndash160 2012
[26] T Moholdt I L Aamot I Granoslashien et al ldquoAerobic intervaltraining increases peak oxygen uptake more than usual careexercise training in myocardial infarction patients a random-ized controlled studyrdquo Clinical Rehabilitation vol 26 no 1 pp33ndash44 2012
[27] E J Howden J S Coombes H Strand B Douglas K LCampbell and N M Isbel ldquoExercise training in CKD efficacyadherence and safetyrdquoAmerican Journal of KidneyDiseases vol65 no 4 pp 583ndash591 2015
[28] A C KingW L Haskell D R Young R K Oka andM L Ste-fanick ldquoLong-term effects of varying intensities and formats ofphysical activity on participation rates fitness and lipoproteinsin men and women aged 50 to 65 yearsrdquo Circulation vol 91 no10 pp 2596ndash2604 1995
[29] G A Brooks and T P White ldquoDetermination of metabolicand heart rate responses of rats to treadmill exerciserdquo Journalof Applied Physiology Respiratory Environmental and ExercisePhysiology vol 45 no 6 pp 1009ndash1015 1978
[30] Y Yu J C Fuscoe C Zhao et al ldquoA rat RNA-Seq transcriptomicBodyMap across 11 organs and 4 developmental stagesrdquo NatureCommunications vol 5 article 3230 2014
[31] F Z Marques A E Campain M Tomaszewski et al ldquoGeneexpression profiling reveals renin mRNA overexpression inhuman hypertensive kidneys and a role formicroRNAsrdquoHyper-tension vol 58 no 6 pp 1093ndash1098 2011
[32] K J Livak and T D Schmittgen ldquoAnalysis of relative geneexpression data using real-time quantitative PCRand the 2minusΔΔ119862TmethodrdquoMethods vol 25 no 4 pp 402ndash408 2001
[33] Y Friedlander J D Kark S Eisenberg and Y Stein ldquoCalcula-tion of LDL-cholesterol from total cholesterol triglyceride andHDL-cholesterol a comparison of methods in the JerusalemLipid Research Clinic Prevalence Studyrdquo Israel Journal of Medi-cal Sciences vol 18 no 12 pp 1242ndash1252 1982
[34] K DMarcus andCM Tipton ldquoExercise training and its effectswith renal hypertensive ratsrdquo Journal of Applied Physiology vol59 no 5 pp 1410ndash1415 1985
[35] K Kitada H Kobori and A Nishiyama ldquoLiver-specificangiotensinogen suppression an old yet novel target forblood pressure control through RAS inhibitionrdquo HypertensionResearch vol 37 no 5 pp 393ndash394 2014
[36] J Gardes J Bouhnik E Clauser P Corvol and JMenard ldquoRoleof angiotensinogen in blood pressure homeostasisrdquo Hyperten-sion vol 4 no 2 pp 185ndash189 1982
[37] K Tanimoto F Sugiyama Y Goto et al ldquoAngiotensinogen-deficient mice with hypotensionrdquo The Journal of BiologicalChemistry vol 269 no 50 pp 31334ndash31337 1994
[38] S Kimura J J Mullins B Bunnemann et al ldquoHigh bloodpressure in transgenic mice carrying the rat angiotensinogengenerdquoThe EMBO Journal vol 11 no 3 pp 821ndash827 1992
[39] JMenard A-I K El Amrani F Savoie J Bouhnik K R LynchandM J Peach ldquoAngiotensinogen an attractive and underratedparticipant in hypertension and inflammationrdquo Hypertensionvol 18 no 5 pp 705ndash707 1991
[40] S Agrawal S Agarwal and S Naik ldquoGenetic contributionand associated pathophysiology in end-stage renal diseaserdquoTheApplication of Clinical Genetics vol 3 pp 65ndash84 2010
[41] W-C Cheng W-Y Shu C-Y Li et al ldquoIntra- and inter-individual variance of gene expression in clinical studiesrdquo PLoSONE vol 7 no 6 Article ID e38650 2012
[42] A Whitehead and D L Crawford ldquoVariation in tissue-specificgene expression among natural populationsrdquo Genome Biologyvol 6 no 2 article R13 2005
[43] A L Oberg B M Bot D E Grill G A Poland and TM Therneau ldquoTechnical and biological variance structure inmRNA-Seq data life in the real worldrdquo BMC Genomics vol 13no 1 article 304 2012
[44] D Agarwal C M Elks S D Reed N Mariappan D SA Majid and J Francis ldquoChronic exercise preserves renalstructure and hemodynamics in spontaneously hypertensiveratsrdquo Antioxidants amp Redox Signaling vol 16 no 2 pp 139ndash1522012
[45] P Zamboli L De Nicola R Minutolo V Bertino F Catapanoand G Conte ldquoManagement of hypertension in chronic kidneydiseaserdquoCurrentHypertensionReports vol 8 no 6 pp 497ndash5012006
[46] G Remuzzi N Perico M Macia and P Ruggenenti ldquoThe roleof renin-angiotensin-aldosterone system in the progression ofchronic kidney diseaserdquo Kidney International vol 68 no 99pp S57ndashS65 2005
[47] N Ouerghi M Feki N Kaabachi M Khammassi S Boukor-raa and A Bouassida ldquoEffects of a high-intensity intermittenttraining programon aerobic capacity and lipid profile in trainedsubjectsrdquoOpenAccess Journal of SportsMedicine vol 5 pp 243ndash248 2014
[48] A Paoli Q F Pacelli T Moro et al ldquoEffects of high-intensitycircuit training low-intensity circuit training and endurancetraining on blood pressure and lipoproteins in middle-agedoverweight menrdquo Lipids in Health and Disease vol 12 no 1article 131 2013
[49] G Racil O Ben Ounis O Hammouda et al ldquoEffects of highvs Moderate exercise intensity during interval training onlipids and adiponectin levels in obese young femalesrdquo EuropeanJournal of Applied Physiology vol 113 no 10 pp 2531ndash25402013
[50] H S Kessler S B Sisson and K R Short ldquoThe potentialfor high-intensity interval training to reduce cardiometabolicdisease riskrdquo Sports Medicine vol 42 no 6 pp 489ndash509 2012
[51] J Poss F Custodis CWernerOWeingartnerM Bohm andULaufs ldquoCardiovascular disease and dyslipidemia beyond LDLrdquoCurrent Pharmaceutical Design vol 17 no 9 pp 861ndash870 2011
BioMed Research International 11
[52] J R Burnett ldquoLipids lipoproteins atherosclerosis and cardio-vascular diseaserdquoThe Clinical Biochemist Reviews vol 25 no 1p 2 2004
[53] G Piecha M Adamczak and E Ritz ldquoDyslipidemia in chronickidney disease pathogenesis and interventionrdquo Polskie Archi-wum Medycyny Wewnetrznej vol 119 no 7-8 pp 487ndash4922009
[54] N A Smart A D Williams I Levinger et al ldquoExercise ampSports Science Australia (ESSA) position statement on exerciseand chronic kidney diseaserdquo Journal of Science and Medicine inSport vol 16 no 5 pp 406ndash411 2013
[55] S-J Pinto-Sietsma W M T Janssen H L Hillege G NavisD de Zeeuw and P E de Jong ldquoUrinary albumin excretion isassociated with renal functional abnormalities in a nondiabeticpopulationrdquo Journal of the American Society of Nephrology vol11 no 10 pp 1882ndash1888 2000
[56] N R Shah and F Dumler ldquoHypoalbuminaemiamdasha marker ofcardiovascular disease in patients with chronic kidney diseasestages II-IVrdquo International Journal ofMedical Sciences vol 5 no6 pp 366ndash370 2008
[57] N E Straznicky M T Grima E A Lambert et al ldquoExerciseaugments weight loss induced improvement in renal functionin obese metabolic syndrome individualsrdquo Journal of Hyperten-sion vol 29 no 3 pp 553ndash564 2011
[58] R D Manning Jr N Tian and S Meng ldquoOxidative stress andantioxidant treatment in hypertension and the associated renaldamagerdquoAmerican Journal of Nephrology vol 25 no 4 pp 311ndash317 2005
[59] G Keller G Zimmer GMall E Ritz andK Amann ldquoNephronnumber in patients with primary hypertensionrdquo The NewEngland Journal of Medicine vol 348 no 2 pp 101ndash108 2003
[60] J Floege M W Burns C E Alpers et al ldquoGlomerular cellproliferation and PDGF expression precede glomerulosclerosisin the remnant kidney modelrdquo Kidney International vol 41 no2 pp 297ndash309 1992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

8 BioMed Research International
Table 4 Repeated clinical and anthropometric measures
Clinical measure Group Baseline 4 Weekslowast 8 Weeksdagger
(Preintervention) (Mid-Intervention) (Postintervention)
Body length (cm)SED 2848 (186) 3503 (085) 3741 (106)LIT 2932 (165) 3515 (079) 3789 (088)HIIT 2961 (225) 3546 (065) 3787 (062)
Body weight (g)SED 22442 (1782) 27605 (1831) 31353 (1662)LIT 23159 (2101) 27742 (2077) 31825 (2103)HIIT 23090 (1998) 27487 (1646) 30816 (1758)
BL-BW ratioSED 0126 (0007) 0127 (0007) 0120 (0004)LIT 0127 (0009) 0128 (0007) 0119 (0009)HIIT 0129 (0007) 0130 (0008) 0124 (0006)
Systolic blood pressure (mmHg)SED 17557 (927) 20777 (1739) 23977 (1285)LIT 17309 (945) 20925 (231) 24163 (2142)HIIT 17465 (1482) 21625 (1624) 22712 (1423)
Values presented as mean (standard deviation)Significance set at 119901 le 005lowastSignificantly different compared to baseline for all groupsdaggerSignificantly different compared to baseline and 4 weeks for all groupsBL-BW body length-body weight
indiscriminately regulated in the absence of aerobic exercisein an animal model of early-stage CKD That is aerobicexercise may help to control otherwise haphazard RAAS-related mRNA expression that occurs during the early stagesof CKD Several informative reviews have outlined theissue of unregulated blood pressure control [45] and morespecifically unregulated RAAS activity [46] in CKD but thisis the first study to suggest that one of the mechanisms bywhich aerobic exercise may prove beneficial is via tightenedcontrol of RAAS-related mRNA expression independentof statistically significant improvements to RAAS-relatedmRNA expression
In the current study the significant decreases in plasmaLDL triglycerides and total cholesterol in HIIT compared toLIT but not SED are encouraging and somewhat surprisingA recent study performed in healthy well-trained humansreported nonsignificant improvements in LDL triglyceridesand total cholesterol after 12 weeks of HIIT [47] In spe-cial andor clinical populations HIIT seems to exert moreinfluence over blood lipids Cardiac rehabilitation patientswho engaged in HIIT experienced significant improvementsin HDL relative to traditional aerobic exercise training[26] However triglyceride measurements were not differentbetween groups and LDL measurements were not reported[26] HIIT has also proven to be beneficial in obese men[48] and women [49] resulting in improved HDL [48]LDL [48] triglycerides [48 49] and total cholesterol [4849] Despite the slowly-accumulating data a recent review[50] that notes the ability of HIIT to influence blood lipidshas yet to be established especially in special populationssuggesting that this specific line of research the effects ofHIIT on blood lipids should be further examined This isespecially true in CKD as lipid-related disorders are theleading cause of complications in CVD [51 52] and CVD-related complications are the leading cause of death in CKD
patients [10 11] As such dyslipidemia should be rankedamong the primary concerns of CKD-related research [53]
Similar to blood lipids a recent review notes that theeffects of exercise training on plasma albumin in patientswith CKD are unclear [54] Moreover data describing theeffects of HIIT on plasma albumin in patients with CKD areunavailable Hypoalbuminemia is an independent predictorof renal dysfunction [55] and an independent predictor ofCVD in early-stage CKD [56] and can be used to identifyCKD patients at increased risk of developing CVD [56] Inobese individuals with metabolic syndrome two commoncharacteristics of CKD 12 weeks of aerobic exercise trainingsignificantly reduced albuminuria (urinary albumin) com-pared to a no-exercise control group [57] Aerobic exercisetraining (16 weeks at 60 of maximal aerobic velocity) hasalso proven useful at reducing albuminuria in SHRs [44]Because hypoalbuminemia is related to declining kidneyfunction [55] blood albumin andor urinary albumin areuseful markers for assessing the preservation of renal tissueIn the current study plasma albumin was significantly higherin HIIT compared to SED and LIT suggesting that renalstructure and function are better preserved by HIIT Thepreservation of renal structure and function and subsequentincrease in plasma albumin may have been due to the down-regulation of Agt mRNA expression and the accompanyingdecrease in SBP in HIIT as hypertension is directly related torenal damage [44 58]
Also considered an indicator of renal damage kid-ney weight and kidney weight-body weight ratio weresignificantly lower in HIIT compared to SED and LITHypertension-related declines in renal function are associ-ated with compensatory alterations to renal tissue such astubulointerstitial fibrosis [59 60] Often pathological thesealterations result in glomerular hypertrophy [59 60] Usinghistological and molecular applications 16 weeks of aerobic
BioMed Research International 9
exercise training (performed at 60 of maximal aerobicvelocity) has been shown to reduce renal fibrosis in SHRs[44] Although renal fibrosis and renal hypertrophy aredirectly related data that specifically describes the effectsof HIIT on renal hypertrophy are unavailable Similar tothe mechanisms that account for increased levels of plasmaalbumin in HIIT there is evidence to suggest that thesignificantly lower kidney weight and kidney weight-bodyweight ratios in HIIT compared to SED and LIT may bedue to decreased fibrosis Decreases in renal fibrosis maybe due to decreases in hypertension-mediated renal damagefollowing a downregulation of the mRNA expression of Agtand a decrease in SBP (in HIIT) [44 58]
5 Conclusions
In summary in an animal model of early-stage CKD HIITappeared to be more beneficial compared to SED and LITas HIIT was responsible for a significant downregulation inthe mRNA expression of Agt The downregulated mRNAexpression of Agt along with significant improvements toblood lipids (LDL triglycerides and total cholesterol) maypartially explain the nonsignificant decrease in SBP andsignificant improvements to plasma albumin kidney weightand kidney weight-body weight ratios in HIIT relative toSED and LIT Future work would benefit from examiningRAAS-related protein expression as well as specific measuresof renal histology and morphology Future work would alsobenefit from examining whether the positive HIIT-relatedeffects seen in the present study are apparent in differentrelated disease models (eg nonnephrectomised SHRs or 56nephrectomy SHRs)
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] AIHW Ed Australiarsquos Health 2014 Australiarsquos Health SeriesAustralian Institute of Health and Welfare (AIHW) CanberraAustralia 2014
[2] A S Go G M Chertow D Fan C E McCulloch andC-Y Hsu ldquoChronic kidney disease and the risks of deathcardiovascular events and hospitalizationrdquo The New EnglandJournal of Medicine vol 351 no 13 pp 1296ndash1370 2004
[3] U D Mathisen T Melsom O C Ingebretsen et al ldquoEstimatedGFR associates with cardiovascular risk factors independentlyof measured GFRrdquo Journal of the American Society of Nephrol-ogy vol 22 no 5 pp 927ndash937 2011
[4] DM Silverstein ldquoInflammation in chronic kidney disease rolein the progression of renal and cardiovascular diseaserdquoPediatricNephrology vol 24 no 8 pp 1445ndash1452 2009
[5] P S Tucker M I Kingsley R H Morton A T Scanlan andV J Dalbo ldquoThe increasing financial impact of chronic kidneydisease in Australiardquo International Journal of Nephrology vol2014 Article ID 120537 7 pages 2014
[6] B Stengel M E Tarver-Carr N R Powe M S Eberhardt andF L Brancati ldquoLifestyle factors obesity and the risk of chronickidney diseaserdquo Epidemiology vol 14 no 4 pp 479ndash487 2003
[7] R T Gansevoort R Correa-Rotter B R Hemmelgarn et alldquoChronic kidney disease and cardiovascular risk epidemiologymechanisms and preventionrdquoTheLancet vol 382 no 9889 pp339ndash352 2013
[8] M M H Hermans R Henry J M Dekker et al ldquoEstimatedglomerular filtration rate and urinary albumin excretion areindependently associated with greater arterial stiffness theHoorn studyrdquo Journal of the American Society of Nephrology vol18 no 6 pp 1942ndash1952 2007
[9] M L Ford L A Tomlinson T P E Chapman C Rajkumar andS G Holt ldquoAortic stiffness is independently associated with rateof renal function decline in chronic kidney disease stages 3 and4rdquo Hypertension vol 55 no 5 pp 1110ndash1115 2010
[10] D EWeiner H Tighiouart P C Stark et al ldquoKidney disease asa risk factor for recurrent cardiovascular disease andmortalityrdquoAmerican Journal of Kidney Diseases vol 44 no 2 pp 198ndash2062004
[11] D E Weiner H Tighiouart M G Amin et al ldquoChronickidney disease as a risk factor for cardiovascular disease and all-causemortality a pooled analysis of community-based studiesrdquoJournal of the American Society of Nephrology vol 15 no 5 pp1307ndash1315 2004
[12] R K Soni A C Porter J P Lash and M L Unruh ldquoHealth-related quality of life in hypertension chronic kidney diseaseand coexistent chronic health conditionsrdquo Advances in ChronicKidney Disease vol 17 no 4 pp e17ndashe26 2010
[13] J Segura C Campo P Gil et al ldquoDevelopment of chronickidney disease and cardiovascular prognosis in essential hyper-tensive patientsrdquo Journal of the American Society of Nephrologyvol 15 no 6 pp 1616ndash1622 2004
[14] J Blacher A P Guerin B Pannier S J Marchais M E Safarand G M London ldquoImpact of aortic stiffness on survival inend-stage renal diseaserdquo Circulation vol 99 no 18 pp 2434ndash2439 1999
[15] G L Bakris E Ritz and World Kidney Day Steering Commit-tee ldquoThe message for World Kidney Day 2009 hypertensionand kidney disease a marriage that should be preventedrdquo TheJournal of Clinical Hypertension (Greenwich) vol 11 no 3 pp144ndash147 2009
[16] J L Lavoie and C D Sigmund ldquoMinireview overview ofthe renin-angiotensin systemmdashan endocrine and paracrinesystemrdquo Endocrinology vol 144 no 6 pp 2179ndash2183 2003
[17] A Nguyen Dinh Cat and RM Touyz ldquoA new look at the renin-angiotensin systemmdashfocusing on the vascular systemrdquo Peptidesvol 32 no 10 pp 2141ndash2150 2011
[18] U C Brewster and M A Perazella ldquoThe renin-angiotensin-aldosterone system and the kidney effects on kidney diseaserdquoThe American Journal of Medicine vol 116 no 4 pp 263ndash2722004
[19] S Ciampone R Borges I P De Lima F F Mesquita EC Cambiucci and J A R Gontijo ldquoLong-term exerciseattenuates blood pressure responsiveness andmodulates kidneyangiotensin II signalling and urinary sodium excretion in SHRrdquoJournal of the Renin-Angiotensin-Aldosterone System vol 12 no4 pp 394ndash403 2011
[20] D Agarwal M A Welsch J N Keller and J Francis ldquoChronicexercise modulates RAS components and improves balancebetween pro- and anti-inflammatory cytokines in the brain of
10 BioMed Research International
SHRrdquo Basic Research in Cardiology vol 106 no 6 pp 1069ndash1085 2011
[21] E J Howden R G Fassett N M Isbel and J S CoombesldquoExercise training in chronic kidney disease patientsrdquo SportsMedicine vol 42 no 6 pp 473ndash488 2012
[22] S Nielsen A Schmitz M Rehling and C E Mogensen ldquoSys-tolic blood pressure relates to the rate of decline of glomerularfiltration rate in type II diabetesrdquo Diabetes Care vol 16 no 11pp 1427ndash1432 1993
[23] A E Tjoslashnna I M Leinan A T Bartnes et al ldquoLow- and high-volume of intensive endurance training significantly improvesmaximal oxygen uptake after 10-weeks of training in healthymenrdquo PLoS ONE vol 8 no 5 Article ID e65382 2013
[24] T Moholdt E Madssen Oslash Rognmo and I L Aamot ldquoThehigher the better Interval training intensity in coronary heartdiseaserdquo Journal of Science and Medicine in Sport vol 17 no 5pp 506ndash510 2014
[25] H E Molmen-Hansen T Stolen A E Tjonna et al ldquoAerobicinterval training reduces blood pressure and improves myocar-dial function in hypertensive patientsrdquo European Journal ofPreventive Cardiology vol 19 no 2 pp 151ndash160 2012
[26] T Moholdt I L Aamot I Granoslashien et al ldquoAerobic intervaltraining increases peak oxygen uptake more than usual careexercise training in myocardial infarction patients a random-ized controlled studyrdquo Clinical Rehabilitation vol 26 no 1 pp33ndash44 2012
[27] E J Howden J S Coombes H Strand B Douglas K LCampbell and N M Isbel ldquoExercise training in CKD efficacyadherence and safetyrdquoAmerican Journal of KidneyDiseases vol65 no 4 pp 583ndash591 2015
[28] A C KingW L Haskell D R Young R K Oka andM L Ste-fanick ldquoLong-term effects of varying intensities and formats ofphysical activity on participation rates fitness and lipoproteinsin men and women aged 50 to 65 yearsrdquo Circulation vol 91 no10 pp 2596ndash2604 1995
[29] G A Brooks and T P White ldquoDetermination of metabolicand heart rate responses of rats to treadmill exerciserdquo Journalof Applied Physiology Respiratory Environmental and ExercisePhysiology vol 45 no 6 pp 1009ndash1015 1978
[30] Y Yu J C Fuscoe C Zhao et al ldquoA rat RNA-Seq transcriptomicBodyMap across 11 organs and 4 developmental stagesrdquo NatureCommunications vol 5 article 3230 2014
[31] F Z Marques A E Campain M Tomaszewski et al ldquoGeneexpression profiling reveals renin mRNA overexpression inhuman hypertensive kidneys and a role formicroRNAsrdquoHyper-tension vol 58 no 6 pp 1093ndash1098 2011
[32] K J Livak and T D Schmittgen ldquoAnalysis of relative geneexpression data using real-time quantitative PCRand the 2minusΔΔ119862TmethodrdquoMethods vol 25 no 4 pp 402ndash408 2001
[33] Y Friedlander J D Kark S Eisenberg and Y Stein ldquoCalcula-tion of LDL-cholesterol from total cholesterol triglyceride andHDL-cholesterol a comparison of methods in the JerusalemLipid Research Clinic Prevalence Studyrdquo Israel Journal of Medi-cal Sciences vol 18 no 12 pp 1242ndash1252 1982
[34] K DMarcus andCM Tipton ldquoExercise training and its effectswith renal hypertensive ratsrdquo Journal of Applied Physiology vol59 no 5 pp 1410ndash1415 1985
[35] K Kitada H Kobori and A Nishiyama ldquoLiver-specificangiotensinogen suppression an old yet novel target forblood pressure control through RAS inhibitionrdquo HypertensionResearch vol 37 no 5 pp 393ndash394 2014
[36] J Gardes J Bouhnik E Clauser P Corvol and JMenard ldquoRoleof angiotensinogen in blood pressure homeostasisrdquo Hyperten-sion vol 4 no 2 pp 185ndash189 1982
[37] K Tanimoto F Sugiyama Y Goto et al ldquoAngiotensinogen-deficient mice with hypotensionrdquo The Journal of BiologicalChemistry vol 269 no 50 pp 31334ndash31337 1994
[38] S Kimura J J Mullins B Bunnemann et al ldquoHigh bloodpressure in transgenic mice carrying the rat angiotensinogengenerdquoThe EMBO Journal vol 11 no 3 pp 821ndash827 1992
[39] JMenard A-I K El Amrani F Savoie J Bouhnik K R LynchandM J Peach ldquoAngiotensinogen an attractive and underratedparticipant in hypertension and inflammationrdquo Hypertensionvol 18 no 5 pp 705ndash707 1991
[40] S Agrawal S Agarwal and S Naik ldquoGenetic contributionand associated pathophysiology in end-stage renal diseaserdquoTheApplication of Clinical Genetics vol 3 pp 65ndash84 2010
[41] W-C Cheng W-Y Shu C-Y Li et al ldquoIntra- and inter-individual variance of gene expression in clinical studiesrdquo PLoSONE vol 7 no 6 Article ID e38650 2012
[42] A Whitehead and D L Crawford ldquoVariation in tissue-specificgene expression among natural populationsrdquo Genome Biologyvol 6 no 2 article R13 2005
[43] A L Oberg B M Bot D E Grill G A Poland and TM Therneau ldquoTechnical and biological variance structure inmRNA-Seq data life in the real worldrdquo BMC Genomics vol 13no 1 article 304 2012
[44] D Agarwal C M Elks S D Reed N Mariappan D SA Majid and J Francis ldquoChronic exercise preserves renalstructure and hemodynamics in spontaneously hypertensiveratsrdquo Antioxidants amp Redox Signaling vol 16 no 2 pp 139ndash1522012
[45] P Zamboli L De Nicola R Minutolo V Bertino F Catapanoand G Conte ldquoManagement of hypertension in chronic kidneydiseaserdquoCurrentHypertensionReports vol 8 no 6 pp 497ndash5012006
[46] G Remuzzi N Perico M Macia and P Ruggenenti ldquoThe roleof renin-angiotensin-aldosterone system in the progression ofchronic kidney diseaserdquo Kidney International vol 68 no 99pp S57ndashS65 2005
[47] N Ouerghi M Feki N Kaabachi M Khammassi S Boukor-raa and A Bouassida ldquoEffects of a high-intensity intermittenttraining programon aerobic capacity and lipid profile in trainedsubjectsrdquoOpenAccess Journal of SportsMedicine vol 5 pp 243ndash248 2014
[48] A Paoli Q F Pacelli T Moro et al ldquoEffects of high-intensitycircuit training low-intensity circuit training and endurancetraining on blood pressure and lipoproteins in middle-agedoverweight menrdquo Lipids in Health and Disease vol 12 no 1article 131 2013
[49] G Racil O Ben Ounis O Hammouda et al ldquoEffects of highvs Moderate exercise intensity during interval training onlipids and adiponectin levels in obese young femalesrdquo EuropeanJournal of Applied Physiology vol 113 no 10 pp 2531ndash25402013
[50] H S Kessler S B Sisson and K R Short ldquoThe potentialfor high-intensity interval training to reduce cardiometabolicdisease riskrdquo Sports Medicine vol 42 no 6 pp 489ndash509 2012
[51] J Poss F Custodis CWernerOWeingartnerM Bohm andULaufs ldquoCardiovascular disease and dyslipidemia beyond LDLrdquoCurrent Pharmaceutical Design vol 17 no 9 pp 861ndash870 2011
BioMed Research International 11
[52] J R Burnett ldquoLipids lipoproteins atherosclerosis and cardio-vascular diseaserdquoThe Clinical Biochemist Reviews vol 25 no 1p 2 2004
[53] G Piecha M Adamczak and E Ritz ldquoDyslipidemia in chronickidney disease pathogenesis and interventionrdquo Polskie Archi-wum Medycyny Wewnetrznej vol 119 no 7-8 pp 487ndash4922009
[54] N A Smart A D Williams I Levinger et al ldquoExercise ampSports Science Australia (ESSA) position statement on exerciseand chronic kidney diseaserdquo Journal of Science and Medicine inSport vol 16 no 5 pp 406ndash411 2013
[55] S-J Pinto-Sietsma W M T Janssen H L Hillege G NavisD de Zeeuw and P E de Jong ldquoUrinary albumin excretion isassociated with renal functional abnormalities in a nondiabeticpopulationrdquo Journal of the American Society of Nephrology vol11 no 10 pp 1882ndash1888 2000
[56] N R Shah and F Dumler ldquoHypoalbuminaemiamdasha marker ofcardiovascular disease in patients with chronic kidney diseasestages II-IVrdquo International Journal ofMedical Sciences vol 5 no6 pp 366ndash370 2008
[57] N E Straznicky M T Grima E A Lambert et al ldquoExerciseaugments weight loss induced improvement in renal functionin obese metabolic syndrome individualsrdquo Journal of Hyperten-sion vol 29 no 3 pp 553ndash564 2011
[58] R D Manning Jr N Tian and S Meng ldquoOxidative stress andantioxidant treatment in hypertension and the associated renaldamagerdquoAmerican Journal of Nephrology vol 25 no 4 pp 311ndash317 2005
[59] G Keller G Zimmer GMall E Ritz andK Amann ldquoNephronnumber in patients with primary hypertensionrdquo The NewEngland Journal of Medicine vol 348 no 2 pp 101ndash108 2003
[60] J Floege M W Burns C E Alpers et al ldquoGlomerular cellproliferation and PDGF expression precede glomerulosclerosisin the remnant kidney modelrdquo Kidney International vol 41 no2 pp 297ndash309 1992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 9
exercise training (performed at 60 of maximal aerobicvelocity) has been shown to reduce renal fibrosis in SHRs[44] Although renal fibrosis and renal hypertrophy aredirectly related data that specifically describes the effectsof HIIT on renal hypertrophy are unavailable Similar tothe mechanisms that account for increased levels of plasmaalbumin in HIIT there is evidence to suggest that thesignificantly lower kidney weight and kidney weight-bodyweight ratios in HIIT compared to SED and LIT may bedue to decreased fibrosis Decreases in renal fibrosis maybe due to decreases in hypertension-mediated renal damagefollowing a downregulation of the mRNA expression of Agtand a decrease in SBP (in HIIT) [44 58]
5 Conclusions
In summary in an animal model of early-stage CKD HIITappeared to be more beneficial compared to SED and LITas HIIT was responsible for a significant downregulation inthe mRNA expression of Agt The downregulated mRNAexpression of Agt along with significant improvements toblood lipids (LDL triglycerides and total cholesterol) maypartially explain the nonsignificant decrease in SBP andsignificant improvements to plasma albumin kidney weightand kidney weight-body weight ratios in HIIT relative toSED and LIT Future work would benefit from examiningRAAS-related protein expression as well as specific measuresof renal histology and morphology Future work would alsobenefit from examining whether the positive HIIT-relatedeffects seen in the present study are apparent in differentrelated disease models (eg nonnephrectomised SHRs or 56nephrectomy SHRs)
Conflict of Interests
The authors declare that there is no conflict of interestsregarding the publication of this paper
References
[1] AIHW Ed Australiarsquos Health 2014 Australiarsquos Health SeriesAustralian Institute of Health and Welfare (AIHW) CanberraAustralia 2014
[2] A S Go G M Chertow D Fan C E McCulloch andC-Y Hsu ldquoChronic kidney disease and the risks of deathcardiovascular events and hospitalizationrdquo The New EnglandJournal of Medicine vol 351 no 13 pp 1296ndash1370 2004
[3] U D Mathisen T Melsom O C Ingebretsen et al ldquoEstimatedGFR associates with cardiovascular risk factors independentlyof measured GFRrdquo Journal of the American Society of Nephrol-ogy vol 22 no 5 pp 927ndash937 2011
[4] DM Silverstein ldquoInflammation in chronic kidney disease rolein the progression of renal and cardiovascular diseaserdquoPediatricNephrology vol 24 no 8 pp 1445ndash1452 2009
[5] P S Tucker M I Kingsley R H Morton A T Scanlan andV J Dalbo ldquoThe increasing financial impact of chronic kidneydisease in Australiardquo International Journal of Nephrology vol2014 Article ID 120537 7 pages 2014
[6] B Stengel M E Tarver-Carr N R Powe M S Eberhardt andF L Brancati ldquoLifestyle factors obesity and the risk of chronickidney diseaserdquo Epidemiology vol 14 no 4 pp 479ndash487 2003
[7] R T Gansevoort R Correa-Rotter B R Hemmelgarn et alldquoChronic kidney disease and cardiovascular risk epidemiologymechanisms and preventionrdquoTheLancet vol 382 no 9889 pp339ndash352 2013
[8] M M H Hermans R Henry J M Dekker et al ldquoEstimatedglomerular filtration rate and urinary albumin excretion areindependently associated with greater arterial stiffness theHoorn studyrdquo Journal of the American Society of Nephrology vol18 no 6 pp 1942ndash1952 2007
[9] M L Ford L A Tomlinson T P E Chapman C Rajkumar andS G Holt ldquoAortic stiffness is independently associated with rateof renal function decline in chronic kidney disease stages 3 and4rdquo Hypertension vol 55 no 5 pp 1110ndash1115 2010
[10] D EWeiner H Tighiouart P C Stark et al ldquoKidney disease asa risk factor for recurrent cardiovascular disease andmortalityrdquoAmerican Journal of Kidney Diseases vol 44 no 2 pp 198ndash2062004
[11] D E Weiner H Tighiouart M G Amin et al ldquoChronickidney disease as a risk factor for cardiovascular disease and all-causemortality a pooled analysis of community-based studiesrdquoJournal of the American Society of Nephrology vol 15 no 5 pp1307ndash1315 2004
[12] R K Soni A C Porter J P Lash and M L Unruh ldquoHealth-related quality of life in hypertension chronic kidney diseaseand coexistent chronic health conditionsrdquo Advances in ChronicKidney Disease vol 17 no 4 pp e17ndashe26 2010
[13] J Segura C Campo P Gil et al ldquoDevelopment of chronickidney disease and cardiovascular prognosis in essential hyper-tensive patientsrdquo Journal of the American Society of Nephrologyvol 15 no 6 pp 1616ndash1622 2004
[14] J Blacher A P Guerin B Pannier S J Marchais M E Safarand G M London ldquoImpact of aortic stiffness on survival inend-stage renal diseaserdquo Circulation vol 99 no 18 pp 2434ndash2439 1999
[15] G L Bakris E Ritz and World Kidney Day Steering Commit-tee ldquoThe message for World Kidney Day 2009 hypertensionand kidney disease a marriage that should be preventedrdquo TheJournal of Clinical Hypertension (Greenwich) vol 11 no 3 pp144ndash147 2009
[16] J L Lavoie and C D Sigmund ldquoMinireview overview ofthe renin-angiotensin systemmdashan endocrine and paracrinesystemrdquo Endocrinology vol 144 no 6 pp 2179ndash2183 2003
[17] A Nguyen Dinh Cat and RM Touyz ldquoA new look at the renin-angiotensin systemmdashfocusing on the vascular systemrdquo Peptidesvol 32 no 10 pp 2141ndash2150 2011
[18] U C Brewster and M A Perazella ldquoThe renin-angiotensin-aldosterone system and the kidney effects on kidney diseaserdquoThe American Journal of Medicine vol 116 no 4 pp 263ndash2722004
[19] S Ciampone R Borges I P De Lima F F Mesquita EC Cambiucci and J A R Gontijo ldquoLong-term exerciseattenuates blood pressure responsiveness andmodulates kidneyangiotensin II signalling and urinary sodium excretion in SHRrdquoJournal of the Renin-Angiotensin-Aldosterone System vol 12 no4 pp 394ndash403 2011
[20] D Agarwal M A Welsch J N Keller and J Francis ldquoChronicexercise modulates RAS components and improves balancebetween pro- and anti-inflammatory cytokines in the brain of
10 BioMed Research International
SHRrdquo Basic Research in Cardiology vol 106 no 6 pp 1069ndash1085 2011
[21] E J Howden R G Fassett N M Isbel and J S CoombesldquoExercise training in chronic kidney disease patientsrdquo SportsMedicine vol 42 no 6 pp 473ndash488 2012
[22] S Nielsen A Schmitz M Rehling and C E Mogensen ldquoSys-tolic blood pressure relates to the rate of decline of glomerularfiltration rate in type II diabetesrdquo Diabetes Care vol 16 no 11pp 1427ndash1432 1993
[23] A E Tjoslashnna I M Leinan A T Bartnes et al ldquoLow- and high-volume of intensive endurance training significantly improvesmaximal oxygen uptake after 10-weeks of training in healthymenrdquo PLoS ONE vol 8 no 5 Article ID e65382 2013
[24] T Moholdt E Madssen Oslash Rognmo and I L Aamot ldquoThehigher the better Interval training intensity in coronary heartdiseaserdquo Journal of Science and Medicine in Sport vol 17 no 5pp 506ndash510 2014
[25] H E Molmen-Hansen T Stolen A E Tjonna et al ldquoAerobicinterval training reduces blood pressure and improves myocar-dial function in hypertensive patientsrdquo European Journal ofPreventive Cardiology vol 19 no 2 pp 151ndash160 2012
[26] T Moholdt I L Aamot I Granoslashien et al ldquoAerobic intervaltraining increases peak oxygen uptake more than usual careexercise training in myocardial infarction patients a random-ized controlled studyrdquo Clinical Rehabilitation vol 26 no 1 pp33ndash44 2012
[27] E J Howden J S Coombes H Strand B Douglas K LCampbell and N M Isbel ldquoExercise training in CKD efficacyadherence and safetyrdquoAmerican Journal of KidneyDiseases vol65 no 4 pp 583ndash591 2015
[28] A C KingW L Haskell D R Young R K Oka andM L Ste-fanick ldquoLong-term effects of varying intensities and formats ofphysical activity on participation rates fitness and lipoproteinsin men and women aged 50 to 65 yearsrdquo Circulation vol 91 no10 pp 2596ndash2604 1995
[29] G A Brooks and T P White ldquoDetermination of metabolicand heart rate responses of rats to treadmill exerciserdquo Journalof Applied Physiology Respiratory Environmental and ExercisePhysiology vol 45 no 6 pp 1009ndash1015 1978
[30] Y Yu J C Fuscoe C Zhao et al ldquoA rat RNA-Seq transcriptomicBodyMap across 11 organs and 4 developmental stagesrdquo NatureCommunications vol 5 article 3230 2014
[31] F Z Marques A E Campain M Tomaszewski et al ldquoGeneexpression profiling reveals renin mRNA overexpression inhuman hypertensive kidneys and a role formicroRNAsrdquoHyper-tension vol 58 no 6 pp 1093ndash1098 2011
[32] K J Livak and T D Schmittgen ldquoAnalysis of relative geneexpression data using real-time quantitative PCRand the 2minusΔΔ119862TmethodrdquoMethods vol 25 no 4 pp 402ndash408 2001
[33] Y Friedlander J D Kark S Eisenberg and Y Stein ldquoCalcula-tion of LDL-cholesterol from total cholesterol triglyceride andHDL-cholesterol a comparison of methods in the JerusalemLipid Research Clinic Prevalence Studyrdquo Israel Journal of Medi-cal Sciences vol 18 no 12 pp 1242ndash1252 1982
[34] K DMarcus andCM Tipton ldquoExercise training and its effectswith renal hypertensive ratsrdquo Journal of Applied Physiology vol59 no 5 pp 1410ndash1415 1985
[35] K Kitada H Kobori and A Nishiyama ldquoLiver-specificangiotensinogen suppression an old yet novel target forblood pressure control through RAS inhibitionrdquo HypertensionResearch vol 37 no 5 pp 393ndash394 2014
[36] J Gardes J Bouhnik E Clauser P Corvol and JMenard ldquoRoleof angiotensinogen in blood pressure homeostasisrdquo Hyperten-sion vol 4 no 2 pp 185ndash189 1982
[37] K Tanimoto F Sugiyama Y Goto et al ldquoAngiotensinogen-deficient mice with hypotensionrdquo The Journal of BiologicalChemistry vol 269 no 50 pp 31334ndash31337 1994
[38] S Kimura J J Mullins B Bunnemann et al ldquoHigh bloodpressure in transgenic mice carrying the rat angiotensinogengenerdquoThe EMBO Journal vol 11 no 3 pp 821ndash827 1992
[39] JMenard A-I K El Amrani F Savoie J Bouhnik K R LynchandM J Peach ldquoAngiotensinogen an attractive and underratedparticipant in hypertension and inflammationrdquo Hypertensionvol 18 no 5 pp 705ndash707 1991
[40] S Agrawal S Agarwal and S Naik ldquoGenetic contributionand associated pathophysiology in end-stage renal diseaserdquoTheApplication of Clinical Genetics vol 3 pp 65ndash84 2010
[41] W-C Cheng W-Y Shu C-Y Li et al ldquoIntra- and inter-individual variance of gene expression in clinical studiesrdquo PLoSONE vol 7 no 6 Article ID e38650 2012
[42] A Whitehead and D L Crawford ldquoVariation in tissue-specificgene expression among natural populationsrdquo Genome Biologyvol 6 no 2 article R13 2005
[43] A L Oberg B M Bot D E Grill G A Poland and TM Therneau ldquoTechnical and biological variance structure inmRNA-Seq data life in the real worldrdquo BMC Genomics vol 13no 1 article 304 2012
[44] D Agarwal C M Elks S D Reed N Mariappan D SA Majid and J Francis ldquoChronic exercise preserves renalstructure and hemodynamics in spontaneously hypertensiveratsrdquo Antioxidants amp Redox Signaling vol 16 no 2 pp 139ndash1522012
[45] P Zamboli L De Nicola R Minutolo V Bertino F Catapanoand G Conte ldquoManagement of hypertension in chronic kidneydiseaserdquoCurrentHypertensionReports vol 8 no 6 pp 497ndash5012006
[46] G Remuzzi N Perico M Macia and P Ruggenenti ldquoThe roleof renin-angiotensin-aldosterone system in the progression ofchronic kidney diseaserdquo Kidney International vol 68 no 99pp S57ndashS65 2005
[47] N Ouerghi M Feki N Kaabachi M Khammassi S Boukor-raa and A Bouassida ldquoEffects of a high-intensity intermittenttraining programon aerobic capacity and lipid profile in trainedsubjectsrdquoOpenAccess Journal of SportsMedicine vol 5 pp 243ndash248 2014
[48] A Paoli Q F Pacelli T Moro et al ldquoEffects of high-intensitycircuit training low-intensity circuit training and endurancetraining on blood pressure and lipoproteins in middle-agedoverweight menrdquo Lipids in Health and Disease vol 12 no 1article 131 2013
[49] G Racil O Ben Ounis O Hammouda et al ldquoEffects of highvs Moderate exercise intensity during interval training onlipids and adiponectin levels in obese young femalesrdquo EuropeanJournal of Applied Physiology vol 113 no 10 pp 2531ndash25402013
[50] H S Kessler S B Sisson and K R Short ldquoThe potentialfor high-intensity interval training to reduce cardiometabolicdisease riskrdquo Sports Medicine vol 42 no 6 pp 489ndash509 2012
[51] J Poss F Custodis CWernerOWeingartnerM Bohm andULaufs ldquoCardiovascular disease and dyslipidemia beyond LDLrdquoCurrent Pharmaceutical Design vol 17 no 9 pp 861ndash870 2011
BioMed Research International 11
[52] J R Burnett ldquoLipids lipoproteins atherosclerosis and cardio-vascular diseaserdquoThe Clinical Biochemist Reviews vol 25 no 1p 2 2004
[53] G Piecha M Adamczak and E Ritz ldquoDyslipidemia in chronickidney disease pathogenesis and interventionrdquo Polskie Archi-wum Medycyny Wewnetrznej vol 119 no 7-8 pp 487ndash4922009
[54] N A Smart A D Williams I Levinger et al ldquoExercise ampSports Science Australia (ESSA) position statement on exerciseand chronic kidney diseaserdquo Journal of Science and Medicine inSport vol 16 no 5 pp 406ndash411 2013
[55] S-J Pinto-Sietsma W M T Janssen H L Hillege G NavisD de Zeeuw and P E de Jong ldquoUrinary albumin excretion isassociated with renal functional abnormalities in a nondiabeticpopulationrdquo Journal of the American Society of Nephrology vol11 no 10 pp 1882ndash1888 2000
[56] N R Shah and F Dumler ldquoHypoalbuminaemiamdasha marker ofcardiovascular disease in patients with chronic kidney diseasestages II-IVrdquo International Journal ofMedical Sciences vol 5 no6 pp 366ndash370 2008
[57] N E Straznicky M T Grima E A Lambert et al ldquoExerciseaugments weight loss induced improvement in renal functionin obese metabolic syndrome individualsrdquo Journal of Hyperten-sion vol 29 no 3 pp 553ndash564 2011
[58] R D Manning Jr N Tian and S Meng ldquoOxidative stress andantioxidant treatment in hypertension and the associated renaldamagerdquoAmerican Journal of Nephrology vol 25 no 4 pp 311ndash317 2005
[59] G Keller G Zimmer GMall E Ritz andK Amann ldquoNephronnumber in patients with primary hypertensionrdquo The NewEngland Journal of Medicine vol 348 no 2 pp 101ndash108 2003
[60] J Floege M W Burns C E Alpers et al ldquoGlomerular cellproliferation and PDGF expression precede glomerulosclerosisin the remnant kidney modelrdquo Kidney International vol 41 no2 pp 297ndash309 1992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

10 BioMed Research International
SHRrdquo Basic Research in Cardiology vol 106 no 6 pp 1069ndash1085 2011
[21] E J Howden R G Fassett N M Isbel and J S CoombesldquoExercise training in chronic kidney disease patientsrdquo SportsMedicine vol 42 no 6 pp 473ndash488 2012
[22] S Nielsen A Schmitz M Rehling and C E Mogensen ldquoSys-tolic blood pressure relates to the rate of decline of glomerularfiltration rate in type II diabetesrdquo Diabetes Care vol 16 no 11pp 1427ndash1432 1993
[23] A E Tjoslashnna I M Leinan A T Bartnes et al ldquoLow- and high-volume of intensive endurance training significantly improvesmaximal oxygen uptake after 10-weeks of training in healthymenrdquo PLoS ONE vol 8 no 5 Article ID e65382 2013
[24] T Moholdt E Madssen Oslash Rognmo and I L Aamot ldquoThehigher the better Interval training intensity in coronary heartdiseaserdquo Journal of Science and Medicine in Sport vol 17 no 5pp 506ndash510 2014
[25] H E Molmen-Hansen T Stolen A E Tjonna et al ldquoAerobicinterval training reduces blood pressure and improves myocar-dial function in hypertensive patientsrdquo European Journal ofPreventive Cardiology vol 19 no 2 pp 151ndash160 2012
[26] T Moholdt I L Aamot I Granoslashien et al ldquoAerobic intervaltraining increases peak oxygen uptake more than usual careexercise training in myocardial infarction patients a random-ized controlled studyrdquo Clinical Rehabilitation vol 26 no 1 pp33ndash44 2012
[27] E J Howden J S Coombes H Strand B Douglas K LCampbell and N M Isbel ldquoExercise training in CKD efficacyadherence and safetyrdquoAmerican Journal of KidneyDiseases vol65 no 4 pp 583ndash591 2015
[28] A C KingW L Haskell D R Young R K Oka andM L Ste-fanick ldquoLong-term effects of varying intensities and formats ofphysical activity on participation rates fitness and lipoproteinsin men and women aged 50 to 65 yearsrdquo Circulation vol 91 no10 pp 2596ndash2604 1995
[29] G A Brooks and T P White ldquoDetermination of metabolicand heart rate responses of rats to treadmill exerciserdquo Journalof Applied Physiology Respiratory Environmental and ExercisePhysiology vol 45 no 6 pp 1009ndash1015 1978
[30] Y Yu J C Fuscoe C Zhao et al ldquoA rat RNA-Seq transcriptomicBodyMap across 11 organs and 4 developmental stagesrdquo NatureCommunications vol 5 article 3230 2014
[31] F Z Marques A E Campain M Tomaszewski et al ldquoGeneexpression profiling reveals renin mRNA overexpression inhuman hypertensive kidneys and a role formicroRNAsrdquoHyper-tension vol 58 no 6 pp 1093ndash1098 2011
[32] K J Livak and T D Schmittgen ldquoAnalysis of relative geneexpression data using real-time quantitative PCRand the 2minusΔΔ119862TmethodrdquoMethods vol 25 no 4 pp 402ndash408 2001
[33] Y Friedlander J D Kark S Eisenberg and Y Stein ldquoCalcula-tion of LDL-cholesterol from total cholesterol triglyceride andHDL-cholesterol a comparison of methods in the JerusalemLipid Research Clinic Prevalence Studyrdquo Israel Journal of Medi-cal Sciences vol 18 no 12 pp 1242ndash1252 1982
[34] K DMarcus andCM Tipton ldquoExercise training and its effectswith renal hypertensive ratsrdquo Journal of Applied Physiology vol59 no 5 pp 1410ndash1415 1985
[35] K Kitada H Kobori and A Nishiyama ldquoLiver-specificangiotensinogen suppression an old yet novel target forblood pressure control through RAS inhibitionrdquo HypertensionResearch vol 37 no 5 pp 393ndash394 2014
[36] J Gardes J Bouhnik E Clauser P Corvol and JMenard ldquoRoleof angiotensinogen in blood pressure homeostasisrdquo Hyperten-sion vol 4 no 2 pp 185ndash189 1982
[37] K Tanimoto F Sugiyama Y Goto et al ldquoAngiotensinogen-deficient mice with hypotensionrdquo The Journal of BiologicalChemistry vol 269 no 50 pp 31334ndash31337 1994
[38] S Kimura J J Mullins B Bunnemann et al ldquoHigh bloodpressure in transgenic mice carrying the rat angiotensinogengenerdquoThe EMBO Journal vol 11 no 3 pp 821ndash827 1992
[39] JMenard A-I K El Amrani F Savoie J Bouhnik K R LynchandM J Peach ldquoAngiotensinogen an attractive and underratedparticipant in hypertension and inflammationrdquo Hypertensionvol 18 no 5 pp 705ndash707 1991
[40] S Agrawal S Agarwal and S Naik ldquoGenetic contributionand associated pathophysiology in end-stage renal diseaserdquoTheApplication of Clinical Genetics vol 3 pp 65ndash84 2010
[41] W-C Cheng W-Y Shu C-Y Li et al ldquoIntra- and inter-individual variance of gene expression in clinical studiesrdquo PLoSONE vol 7 no 6 Article ID e38650 2012
[42] A Whitehead and D L Crawford ldquoVariation in tissue-specificgene expression among natural populationsrdquo Genome Biologyvol 6 no 2 article R13 2005
[43] A L Oberg B M Bot D E Grill G A Poland and TM Therneau ldquoTechnical and biological variance structure inmRNA-Seq data life in the real worldrdquo BMC Genomics vol 13no 1 article 304 2012
[44] D Agarwal C M Elks S D Reed N Mariappan D SA Majid and J Francis ldquoChronic exercise preserves renalstructure and hemodynamics in spontaneously hypertensiveratsrdquo Antioxidants amp Redox Signaling vol 16 no 2 pp 139ndash1522012
[45] P Zamboli L De Nicola R Minutolo V Bertino F Catapanoand G Conte ldquoManagement of hypertension in chronic kidneydiseaserdquoCurrentHypertensionReports vol 8 no 6 pp 497ndash5012006
[46] G Remuzzi N Perico M Macia and P Ruggenenti ldquoThe roleof renin-angiotensin-aldosterone system in the progression ofchronic kidney diseaserdquo Kidney International vol 68 no 99pp S57ndashS65 2005
[47] N Ouerghi M Feki N Kaabachi M Khammassi S Boukor-raa and A Bouassida ldquoEffects of a high-intensity intermittenttraining programon aerobic capacity and lipid profile in trainedsubjectsrdquoOpenAccess Journal of SportsMedicine vol 5 pp 243ndash248 2014
[48] A Paoli Q F Pacelli T Moro et al ldquoEffects of high-intensitycircuit training low-intensity circuit training and endurancetraining on blood pressure and lipoproteins in middle-agedoverweight menrdquo Lipids in Health and Disease vol 12 no 1article 131 2013
[49] G Racil O Ben Ounis O Hammouda et al ldquoEffects of highvs Moderate exercise intensity during interval training onlipids and adiponectin levels in obese young femalesrdquo EuropeanJournal of Applied Physiology vol 113 no 10 pp 2531ndash25402013
[50] H S Kessler S B Sisson and K R Short ldquoThe potentialfor high-intensity interval training to reduce cardiometabolicdisease riskrdquo Sports Medicine vol 42 no 6 pp 489ndash509 2012
[51] J Poss F Custodis CWernerOWeingartnerM Bohm andULaufs ldquoCardiovascular disease and dyslipidemia beyond LDLrdquoCurrent Pharmaceutical Design vol 17 no 9 pp 861ndash870 2011
BioMed Research International 11
[52] J R Burnett ldquoLipids lipoproteins atherosclerosis and cardio-vascular diseaserdquoThe Clinical Biochemist Reviews vol 25 no 1p 2 2004
[53] G Piecha M Adamczak and E Ritz ldquoDyslipidemia in chronickidney disease pathogenesis and interventionrdquo Polskie Archi-wum Medycyny Wewnetrznej vol 119 no 7-8 pp 487ndash4922009
[54] N A Smart A D Williams I Levinger et al ldquoExercise ampSports Science Australia (ESSA) position statement on exerciseand chronic kidney diseaserdquo Journal of Science and Medicine inSport vol 16 no 5 pp 406ndash411 2013
[55] S-J Pinto-Sietsma W M T Janssen H L Hillege G NavisD de Zeeuw and P E de Jong ldquoUrinary albumin excretion isassociated with renal functional abnormalities in a nondiabeticpopulationrdquo Journal of the American Society of Nephrology vol11 no 10 pp 1882ndash1888 2000
[56] N R Shah and F Dumler ldquoHypoalbuminaemiamdasha marker ofcardiovascular disease in patients with chronic kidney diseasestages II-IVrdquo International Journal ofMedical Sciences vol 5 no6 pp 366ndash370 2008
[57] N E Straznicky M T Grima E A Lambert et al ldquoExerciseaugments weight loss induced improvement in renal functionin obese metabolic syndrome individualsrdquo Journal of Hyperten-sion vol 29 no 3 pp 553ndash564 2011
[58] R D Manning Jr N Tian and S Meng ldquoOxidative stress andantioxidant treatment in hypertension and the associated renaldamagerdquoAmerican Journal of Nephrology vol 25 no 4 pp 311ndash317 2005
[59] G Keller G Zimmer GMall E Ritz andK Amann ldquoNephronnumber in patients with primary hypertensionrdquo The NewEngland Journal of Medicine vol 348 no 2 pp 101ndash108 2003
[60] J Floege M W Burns C E Alpers et al ldquoGlomerular cellproliferation and PDGF expression precede glomerulosclerosisin the remnant kidney modelrdquo Kidney International vol 41 no2 pp 297ndash309 1992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 11
[52] J R Burnett ldquoLipids lipoproteins atherosclerosis and cardio-vascular diseaserdquoThe Clinical Biochemist Reviews vol 25 no 1p 2 2004
[53] G Piecha M Adamczak and E Ritz ldquoDyslipidemia in chronickidney disease pathogenesis and interventionrdquo Polskie Archi-wum Medycyny Wewnetrznej vol 119 no 7-8 pp 487ndash4922009
[54] N A Smart A D Williams I Levinger et al ldquoExercise ampSports Science Australia (ESSA) position statement on exerciseand chronic kidney diseaserdquo Journal of Science and Medicine inSport vol 16 no 5 pp 406ndash411 2013
[55] S-J Pinto-Sietsma W M T Janssen H L Hillege G NavisD de Zeeuw and P E de Jong ldquoUrinary albumin excretion isassociated with renal functional abnormalities in a nondiabeticpopulationrdquo Journal of the American Society of Nephrology vol11 no 10 pp 1882ndash1888 2000
[56] N R Shah and F Dumler ldquoHypoalbuminaemiamdasha marker ofcardiovascular disease in patients with chronic kidney diseasestages II-IVrdquo International Journal ofMedical Sciences vol 5 no6 pp 366ndash370 2008
[57] N E Straznicky M T Grima E A Lambert et al ldquoExerciseaugments weight loss induced improvement in renal functionin obese metabolic syndrome individualsrdquo Journal of Hyperten-sion vol 29 no 3 pp 553ndash564 2011
[58] R D Manning Jr N Tian and S Meng ldquoOxidative stress andantioxidant treatment in hypertension and the associated renaldamagerdquoAmerican Journal of Nephrology vol 25 no 4 pp 311ndash317 2005
[59] G Keller G Zimmer GMall E Ritz andK Amann ldquoNephronnumber in patients with primary hypertensionrdquo The NewEngland Journal of Medicine vol 348 no 2 pp 101ndash108 2003
[60] J Floege M W Burns C E Alpers et al ldquoGlomerular cellproliferation and PDGF expression precede glomerulosclerosisin the remnant kidney modelrdquo Kidney International vol 41 no2 pp 297ndash309 1992
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom