Embed Size (px)
Citation preview
Hindawi Publishing CorporationBioMed Research InternationalVolume 2013 Article ID 451349 9 pageshttpdxdoiorg1011552013451349
Research ArticleCX3CR1 Receptor Polymorphisms Th1 Cell Recruitment andAcute Myocardial Infarction Outcome Looking for a Link
S Pucci P Mazzarelli M J Zonetti T Fisco E Bonanno L G Spagnoli and A Mauriello
Department of Biomedicine and Prevention University of Rome ldquoTor Vergatardquo Via Montpellier 1 00133 Rome Italy
Correspondence should be addressed to S Pucci sabinapucyahooit
Received 30 April 2013 Revised 6 September 2013 Accepted 12 September 2013
Academic Editor Nishath Altaf
Copyright copy 2013 S Pucci et al This is an open access article distributed under the Creative Commons Attribution License whichpermits unrestricted use distribution and reproduction in any medium provided the original work is properly cited
Fractalkine is a proinflammatory chemokine that participates in atherosclerotic process mediating the interactions of vascular cellsand leukocytes and selective recruitment ofTh1 lymphocytes through interaction with CX3CR1 receptorThe polymorphism of thefractalkine receptor 280M-containing haplotype which codifies for a receptor with minor expression and with a reduced bindingcapability represents a novel protective factor of atherosclerotic disease We investigated the association among CX3CR1 genotypethe inflammatory infiltrate subpopulations recruited in the plaque and the in situ expression of fractalkine and its receptor inpatients who died of myocardial infarction (AMI) compared with subjects who died of noncardiac causes Patients with nonlethalAMI (AMI survivors) were also investigated to correlate the CX3CR1 polymorphisms and the incidence of lethal AMI A strongT cells infiltrate was found in infarct related artery (IRA) plaques of AMI patients presenting the V
249T280
haplotype (84)Conversely a decreased T cell recruitment was associated with I
249T280
haplotype in the controls (64) The significant higherpresence of the variant allele I249 in homo- and heterozygosis found in controls (91) and in AMI survivors (94) with respect tothe patients who died of AMI (48) showed the relevance of this polymorphism both in the onset and outcome of acutemyocardialinfarctionThe presence of CX3CR1 polymorphisms could influence the incidence and the outcome of acute myocardial infarctionaltering the inflammation of the whole coronary tree by the impaired recruitment of Th1 polarized subpopulation in the coronaryplaque
1 Introduction
Genetic factor appears to be important determinant of car-diovascular disease In particular specific genetic polymor-phisms that modulate blood pressure coagulation and lipidmetabolism have been identified to be associated with risk ofcoronary artery disease However none of these associationshas identified the precise molecular basis of pathologicalaccumulation of leukocytes in vessel wall that characterizedthe onset of acute myocardial infarction
Acute myocardial infarction (AMI) in fact is related to adiffuse active inflammation of the coronary tree associatedwith rupture of one of the multiple vulnerable plaques
Unlike stable plaques characterized by a chronic infiltrateof macrophages vulnerable plaques display an inflamma-tory infiltrate composed by T cells activated towards a Th1pathway and whose recruitment is regulated by chemokinescytokines and their receptors [1 2]
In particular chemokines are part of effector and ampli-fication mechanisms of polarized Th1 or Th2 mediatedimmune responses therefore their receptors may serve asTh1 versusTh2marker and lead to the selectivemodulation ofT cell dependent immunity Hence the receptor expressionand the chemokines release are closely linked to T cellpolarization and activation
Fractalkine (CX3CL1) is a proinflammatory chemokinethat induces chemotaxis of circulating monocytes and selec-tive recruitment ofTh1 lymphocytes through interactionwithits ligand the CX3CR1 receptor that is highly expressedon Th1 activated T cells [3ndash11] It has been observed thatthe expressions of fractalkine and its receptor CX3CR1 areupregulated in atherosclerosis lesions and the severity ofatherosclerosis is greatly improved by inhibiting their expres-sions indicating that the fractalkineCX3CR1 pair is closelyrelated to atherosclerosis
2 BioMed Research International
Studies on CX3CR1 receptor knock out animal modelsand on human coronaries with native atherosclerosis pointout the important role of fractalkine in atherogenesis andplaque progression [12 13]
Recent data demonstrated the enhanced expression ofCXCL1 and its receptor (CX3CR1) in coronary artery diseasethat could be downmodulated by statin therapy [14] Thesedata suggest a role of CXCL1 and CXCR1 as therapeutic tar-gets in the care of CADpatients including those with unstabledisease
Epidemiological studies have proved the existence of twocommon nonsynonymous single-nucleotide polymorphismsof CX3CR1 receptor gene (V249I and T280M)The polymor-phisms of the fractalkine receptor that codify for a moleculewithminor expression and with a reduced binding capabilityhave been proposed as a novel protectivemarker for coronarydisease In particular the CX3CR1 I249 allele in homo- andheterozygote conditions has been associated with a markedreduction in risk of acute coronary events [15ndash17] In additionpopulation studies on CX3CR1 polymorphism have firmlyconfirmed that 280M-containing haplotype is associatedwith reduced risk of atherosclerotic disease As shown byexperimental studies the presence of the I
249M280
haplotypecodifies for a chemokine receptor variant that has impairedadhesive function low binding activity and low recruitmentefficiency of T cells within the plaque On the contrary theCX3CR1 V
249T280
haplotype characterized by high expres-sion and binding efficiency is associated with high riskof CAD and could be related to plaque vulnerability andrupture
All these data suggest that the CX3CR1 V249 and T280polymorphisms could amplify the Th1 response trigger-ing plaque vulnerability and rupture Moreover the higherexpression and binding activity of this receptor could influ-ence the atherogenesis in patients with artery disease and theincidence and the outcome of the myocardial infarction
Little information is available regarding the risk factorspredicting the subsequent lethal cardiac events after acutemyocardial infarction (AMI) In fact despite the use ofadvanced medical and invasive procedures the risk adjusted90-day mortality rates in patients with myocardial infarctionare up to 20ndash24 Recent data pointed out the relevant roleof diffuse inflammatory process We have recently demon-strated in patients who died of a first AMI the presence ofa strongly activated T cell infiltrate in the entire coronary treeand in the peri-infarctual and in the remote unaffectedmyocardial regions underlying both coronary and myocar-dial vulnerability [18 19] In view of that the object ofthis investigation was to determine if the CX3CR1 polymor-phisms genetic factors previously described to be involvedin atherogenesis play a role in the pathobiology of acutemyocardial infarction
Therefore we evaluated the inflammatory burden and thein situ expression of fractalkine and its receptor in coronaryplaques of patients died of myocardial infarction (AMI) ascompared to subjects died of noncardiac causes in order tofocus if the presence of I249M280 haplotype correlates withan impairedTh1 cell recruitment in the plaque
We further evaluate if the CX3CR1 polymorphisms couldinfluence the outcome of acute myocardial infarction Atthis purpose we examined the of CX3CR1 polymorphismspresence in individuals who died of noncardiac causes in acohort of patients that survived at acutemyocardial infarction(AMI survivors) compared with patients died of AMI
2 Methods
21 Case Selection We observed 25 patients (17 males8females mean age 705 plusmn 18 years) died of acute myocardialinfarction (AMI group) and 22 age-matched patients (15males7 females mean age 737 plusmn 28) died of noncardiaccauses andwithout clinical cardiac history (NCCgroup) Fur-ther 16 patients (mean age 65 plusmn 99 yr 13males) who survivedat a previous myocardial infarction (MI) suitable for surgicalventricular restoration have been analyzed (SVR group)Clinical angiographic and surgical characteristics are listedin Table 1 In the AMI group the time from symptom onsetto death was within 72 hours for all cases Clinical historyand standard electrocardiographic findings defined acutemyocardial infarction Histopathological examination of themyocardium confirmed AMI as cause of death The infarctwas transmural and from a single coronary artery distribu-tion in all cases Myocardium from NCC patients died ofbronchopneumonia pulmonary embolism and intestinalhemorrhage did not show either infarct or necrosis in allcases
Themain indications for surgery of patients of SVR groupwere symptoms of heart failure angina andor a combinationof the two Four patients of this group (25) had associatedmitral valve repair for a grade 3+4+ of mitral regurgitationThe surgical technique has been previously described [1]Mitral valve (MV) is repaired when needed through theventricle
Patients with chronic inflammatory diseases or tumorswere excluded from the study to avoid bias due to immuno-logical changes All autopsies were performed within 12ndash24hours of death
22 Tissue Handling and Processing At the autopsy in AMIand NCC the 4 major epicardial coronary arteries (leftmain left anterior descending left circumflex and right)were dissected from each heart 10 buffered formalin fixedcut transversely at 5mm intervals decalcified if necessaryparaffin embedded and serially sectioned for morphologicaland immunohistochemical studiesThe hearts were transver-sally cut at 1 cm intervals from the apex to the base Themyocardium was examined for the presence and extent ofinfarctionThe location ofmyocardial infarctionwas detectedby immersion of a cross-section of the heart in a solutionof triphenyltetrazolium chloride (for the autoptic demon-stration of myocardial infarction) In addition in all casesanother cross-section of the heart was processed for histolog-ical examination and the infarction was confirmed by lightmicroscopy
In SVR patients LVmyocardial samples were obtained atthe time of surgical operation The tissue was taken from thetransition zone between MI and the remote normal region
BioMed Research International 3
Table 1 Clinical and surgical data of patients
AMIlowast group (25 pts) NCClowast group (22 pts) SVRlowast group (16 pts)Clinical data
Age (yr plusmn SE) 705 plusmn 18 737 plusmn 28 65 plusmn 27
Male 17 (68) 15 (68) 13 (81)Hypertension 18 (72) 14 (64) 11 (69)Diabetes 13 (52) 10 (45) 7 (44)Previous smoking 13 (52) 11 (50) 7 (44)Hyperlipidemia 14 (56) 10 (45) 8 (50)Previous MI () 0 0 16 (100)Previous PTCA 0 0 5 (31)
Autoptic data causes of deathAcute MI 25 (100) 0
Anterior wall 13 (52) 0Posterolateral wall 7 (28) 0Posterior wall 5 (20) 0
Bronchopneumonia 0 14 (64)Pulmonary embolism 0 5 (23)Intestinal hemorrhage 0 3 (14)
Surgical dataMean time fromMI to Op (mo plusmn SE) 51 plusmn 9
EF (plusmn SE) 30 plusmn 25
LVEDV (mL plusmn SE) 183 plusmn 102
LVESV (mL plusmn SE) 129 plusmn 101
CABG 15 (94)LIMA grafts 15 (94)No of total anastomosis (plusmnSE) 29 plusmn 03
lowastAMI acute myocardial infarction patients NCC subjects dead for noncardiac causes SVR patients survived to a first AMIData are absolute numbers (percentage)Abbreviations CABG coronary artery bypass graft EF ejection fraction LIMA left internal mammary artery LVEDV left ventricle end-diastolic volumeLVESV left ventricle end-systolic volume MI myocardial infarction PTCA percutaneous transluminal coronary angioplasty SE standard error
All tissues were fixed in 10 formalin and embedded inparaffin
23 Morphological Studies Coronary sections from the twogroups HampE and pentachrome stained were examined bylight microscopy Culprit plaques were defined as lesionsshowing either plaque rupture or erosion with superimposedthrombusThe coronary artery showing the culprit lesionwasdefined as infarct-related artery (IRA) In AMI were exam-ined the culprit segment in the IRA including the throm-botic lesion 15 cm long a segment 15 cm long in whichmaximum of stenosis was present in the non-IRA coronaryIn NCC a segment of 15 cm long in which maximum ofstenosis was present was selected All coronary segmentswere cut transversely at 5mm intervals A total of 216 arterialsegments were paraffin embedded and serially sectioned 150from the AMI group (75 from IRA and 75 from non-IRAcoronaries) and 66 from NCC group respectively
24 Immunohistochemical Studies (IHC) Serial 3 120583m thicksections were cut from paraffin blocks and mounted onSuperFrost Plus slides (Menzel-Glaser Germany) 120572-smoothactin CD68 CD3 (Dakopatts Denmark) fractalkine (RampD
System Minneapolis MN) and CX3CR1 (GmbH Gottin-gen D) primary monoclonal antibodies were used CD68(alkaline phosphataseanti-alkaline phosphatase) and CD3(DAB detected) IHC was used to quantify the inflammatoryinfiltrate For each antibody positive cells as a mean of 10randomly selected fields per section were counted at amagnification of 40X in the plaque shoulder region and inthe cap itself
25 Confocal Microscopy Immunofluorescence In order tocharacterize the cell subpopulations that express CX3CR1 weperformed a triple immunostaining for confocal microscopyParaffin sections of coronary plaques were first incubatedwith anti-CD3 MoAb (1 20 1 h at RT) rinsed and thenincubated with biotinylated mouse IgG Fluorescence wasobtained by incubating the sections with a streptavidin-coumarin fluorochrome A second reaction with primaryantibodies to CX3CR1 (dilution 1 50 1 h at RT in the dark)was performed Fluorescence was obtained with a conjugatestreptavidin-fluorescein conjugate (FITC) A third immunos-taining was performed by incubating the sections withanti-IFN gamma monoclonal antibody (dilution 1 25 1 hat RT in the dark) Sections were incubated with tyramide
4 BioMed Research International
signal amplification biotin system (NEN Life Science Prod-ucts Boston MA USA) Fluorescence was obtained with astreptavidin-Texas Red fluorescent conjugate Control sec-tions were incubated with amixture of irrelevantmonoclonalreagents having a similar isotype Images were acquired bymeans of Noran confocal microscope at 60X14 NA immer-sion oil lens Three D stacks were acquired at a resolution of01 micron in119883- 119884- and 119885-axis
26 DNA Extraction DNA was extracted from formalinfixed and paraffin embedded heart of the subjects describedabove Paraffin was removed with xylene for 5min at roomtemperature Samples were centrifuged at full speed for 5minat RT Supernatant was removed and 12mL of 100 ethanolwas added to remove residual xyleneTheDNAwas extractedwith the QIAamp DNA kit (Qiagen GmbH Germany) andresuspended in 50 120583L of Buffer AE
27 Screening for Polymorphisms The DNA quality wascontrolled by a genomic polymerase reaction assay (PCR)using the primer set for BAK gene The following two poly-morphisms have been analyzed I249 a guanidine to adeninesubstitution at nucleotide 745 of the open reading framechanging valine at position 249 to isoleucine and M280 acytosine to thymidine substitution at nucleotide 839 changinga threonine at position 280The PCR product was analyzed in2 agarose gel stained with ethidium bromide CX3CR1 geneT280M and V249I mutations were identified after amplifica-tion of 311 base pairs (bp) (primers forward 51015840 AGA ATCATC CAG ACG CTG TTT TCC 31015840 reverse 51015840 CAG AGGACAGCCAGGCATTTCC31015840)TheT280MandV429Iweredetected on the same amplified fragment Amplification reac-tions were performed using 35 cycles of 95∘C 69∘C and 72∘Cfor 30 seconds each preceded by a single cycle of 95∘C for 3minutes and followed by a single cycle of 72∘C for 10 minutesIn order to type the alleles at codons 249 and 280 5 120583L ofPCR reactionwas digested respectively with Acl I (NewEng-land Biolabs BeverlyMA) or BsbmB1 (New England BiolabsBeverlyMA) in 20 120583L of reaction as previously described [11]In order to evaluate the efficiency of endonucleases enzymescontrol DNA with Acl I and Bst 4CI restriction sites wasused and DNA was loaded at different times on agarose gelThe genotypes were analysed and determined by analyticalelectrophoresis of each digestion on a 2 agarose gel
28 Statistical Analysis Statistical analysis of the data wasperformed with SPSS for Windows (version 110 SPSSChicago IL) Unpaired 119905-test was utilized to assess intergroupdifferences for continuous variables The 1198832 test was used toestablish differences in the distribution between categoricalvariables The statistical significance of different polymor-phisms present in the single groups was identified by Fisherrsquosexact test A 119875 value of lt005 was considered statisticallysignificant
Using logistic regression analysis (SPSS 130) the associ-ation of each polymorphism with the cardiovascular events(fatal AMI survivors and control group) was adjusted forage gender smoking cigarette hypertension diabetes mel-litus and hyperlipidemia
0 10 20 30 40
AMI
CTRL
T cellsMacrophages
(a)
0 20 40 60 80 100
AMI
CTRL
CX3CR1
(b)
Figure 1 Inflammatory cells characterization (a) shows the per-centages of inflammatory cells T lymphocytes (dotted bar) andmacrophages (dashed bar) in AMI and control group (b) Shows thepercentages of T cells CX3CR1 positive in AMI and control group
3 Results
31 Coronary Plaques Inflammation The examination of thewhole coronary tree of the AMI group demonstrated thepresence ofmultiple complicated atherosclerotic plaqueswitha thin fibrous cap and a high inflammatory infiltrate more-over in the coronary branch supplying the infarct area (IRA)we found a disruptedthrombotic plaque (culprit plaque)Conversely the coronary trees of the control group (NCC)showed atherosclerotic lesions with a thick fibrous cap and ascanty inflammatory infiltrate No plaque disruption or ero-sion or thrombosis has been observed Clinical autoptic andsurgical patient characteristics are showed in Table 1
Cell subpopulations were characterized by immunohis-tochemical studies using specific antibodies for lymphocytes(CD3 T cells) macrophages (CD68) and smooth musclecells (120572-actin) A quantitative analysis demonstrated a signif-icant (119875 lt 001) increase in the inflammatory cells per area(CD3 and CD68 positive) in AMI plaques (514 plusmn 25) ascompared with the plaques of the NCC group (224 plusmn 19)T lymphocytes represented the 185plusmn23 of the plaque cellsin AMI and the 64 plusmn 18 of cells in the NCC whereasmacrophages were 329 plusmn 32 in the AMI and 160 plusmn 18 intheNCC (Figure 1(a))Moreover the expression of IFN-120574wasassessed in culprit lesions by immunofluorescence staining(coronary artery fromAMI group) with confocal microscopy(Figure 3)
BioMed Research International 5
32 Fractalkine and CX3CR1 Expression The Fractalkineexpression was evaluated by immunohistochemistry in orderto compare T cell population recruitment and chemokinerelease
Figure 2(b) shows the expression of CD3 fractalkinereceptor CX3CR1 Figure 2(c) in T cells infiltrating the culpritlesion In AMI plaques immunostaining for fractalkine wasstrongly positive (Figure 2(d)) The immunofluorescence inFigure 3 demonstrated the coexpression of these three pro-teins in the same cells of AMI culprit plaque confirming theexistence of a T cell chronic active inflammation Moreoverthese data demonstrated theTh1 mediated immune response(IFN-120574 production) involved in plaque inflammation anddestabilization correlated with the presence of Th1 polarizedT cells (CXCR1 expressing cells) recruited in the plaque by theinteraction of fractalkine and the CX3CR1 receptor on the Tcell membrane
The immunohistochemical studies demonstrated thatendothelial cells in plaques of AMI patients gave rise to adiffuse positive reaction for fractalkine Smooth muscle cellswere focally positive while lymphocytes and macrophageswere not Conversely in the plaques of NCC group all thecell types were almost negative for fractalkine (Figure 2)
The fractalkine receptor (CX3CR1) was strongly anddiffusely expressed in the cell membrane in T lympho-cytes of AMI plaques (Figure 2(c)) as compared to controlMacrophages and smoothmuscle cells gave rise to a weak andscattered positive reaction The reaction was almost negativein the plaques of NCC group only a weak positive stainingwas present in smooth muscle cells and macrophages in theplaque (Figure 2(g))
The quantitative study revealed that 83 of T cells in theAMI plaques were CX3CR1 positive (Figure 1(b)) indicating aTh1 subset polarized subpopulation Furthermore a confocalobservation of IFN-120574 expression confirmed that T lympho-cytes expressed IFN-120574 (Figure 3)
In the coronary plaques from control group T lympho-cytes showed a lower level of CX3CR1 positivity (18 of Tlymphocytes were positive) (Figure 1(b)) in this group thereaction for IFN-120574 was completely negative (not shown)
33 CX3CR1 Genotype Correlates with the Th1 Cells Recruit-ment It has been previously demonstrated that CX3CR1genotypes influence the fractalkine receptor binding affinityand therefore Th1 lymphocytes recruitment In order tocorrelate the presence of activated Th1 lymphocytes withCX3CR1 genotype patientswere genotyped for theV249I andT280Mpolymorphisms of CXCR1 gene DNA extracted frommyocardial formalin fixed and paraffin embedded sectionswas analyzed by polymerase chain reaction The genotypewas determined on the amplicon of 311 bp after digestionwithendonucleases specific for each polymorphism The analysisof CX3CR1 V249I and T280M polymorphisms demonstratedthat 13 out of 25 patients who died of infarction (52) werehomozygous for the V249 allele and 21 out of 25 (84) werehomozygous for the T280 allele (Table 2) Moreover the 40ofAMI patients (1025) were heterozygous for theV249 allelebut all of these were homozygous for T280 allele as shown inTable 2 On the other hand only 8 (225) of AMI patients
displayed I249 allele in homozygosis and T280 in homo-(84) or heterozygosis (16) Notably the two AMI patientswho presented the variant haplotypes 249II and 280TMhad reduced T infiltrate and low IFN-120574 production in theplaque but a large number of B cells In Table 2 the correlationbetween the genotype and the inflammatory infiltrate burdenis reported The higher presence of 249VV (52) in AMIgroup as compared to controls is correlated with the presenceof a consistent T cell infiltrate expressing CX3CR1 (119875 lt 001)confirming the Th1 polarized subpopulation recruitment inthe plaque
4 Correlation among AMI AMI Survivorsand NCC Genotype
The genotype analysis has been extended to a cohort ofindividuals survived at a first myocardial infarction (119899 = 16)in order to compare the presence of the allele variant with theoccurrence and the outcome of the acute event
We found that the 52 of AMI patients (1325) displayedthe V249 allele in homozygosis as compared with the 6of the AMI survivors (116) and the 9 of controls (222)(Table 3)
The multivariate analysis of each V249I polymorphismadjusted for clinical data in the three study groups showedthat the VV249 haplotype was significantly associated onlywith the fatal AMI (119875 = 0001) but not with all the major riskfactors
On the other hand the I249 variant allele was expressedin homozygosis only in the 8 of the AMI patients (225)(Table 3) as compared with the 36 of controls (822) andthe 31 of AMI survivors (516)
The analysis of T280Mpolymorphism displayed the pres-ence of the M280 variant allele in homozygosis in the 4 ofcontrols (122) as comparedwithAMI and survivors patientswhich showed no presence of this allele in homozygosis Thepresence ofM280 allele in homozygosiswas always associatedwith the I249 allele
In summary the significant higher presence of the variantallele I249 in homo- and heterozygosis found in controls(91) and in AMI survivors (94) with respect to thepatients died of AMI (48) showed the relevance of thispolymorphism both in the onset and outcome of acutemyocardial infarction confirming the correlation betweenCX3CR1 genotype and prognosis of the acute event
5 Discussion
Epidemiological and clinical studies have shown that theCX3CR1 receptor polymorphisms are linked with the risk ofcoronary artery diseases [14 15]
In particular the presence of CX3CR1 V249 and T280single nucleotide polymorphisms codify for a fractalkinereceptor that is overexpressed by activated inflammatory cellsand with higher binding affinity for fractalkine its naturalligand [16 20]
The genotyping analysis of the subjects enrolled in thepresent study demonstrated for the first time a direct corre-lation between CX3CR1 V249I and T280M polymorphisms
6 BioMed Research International
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
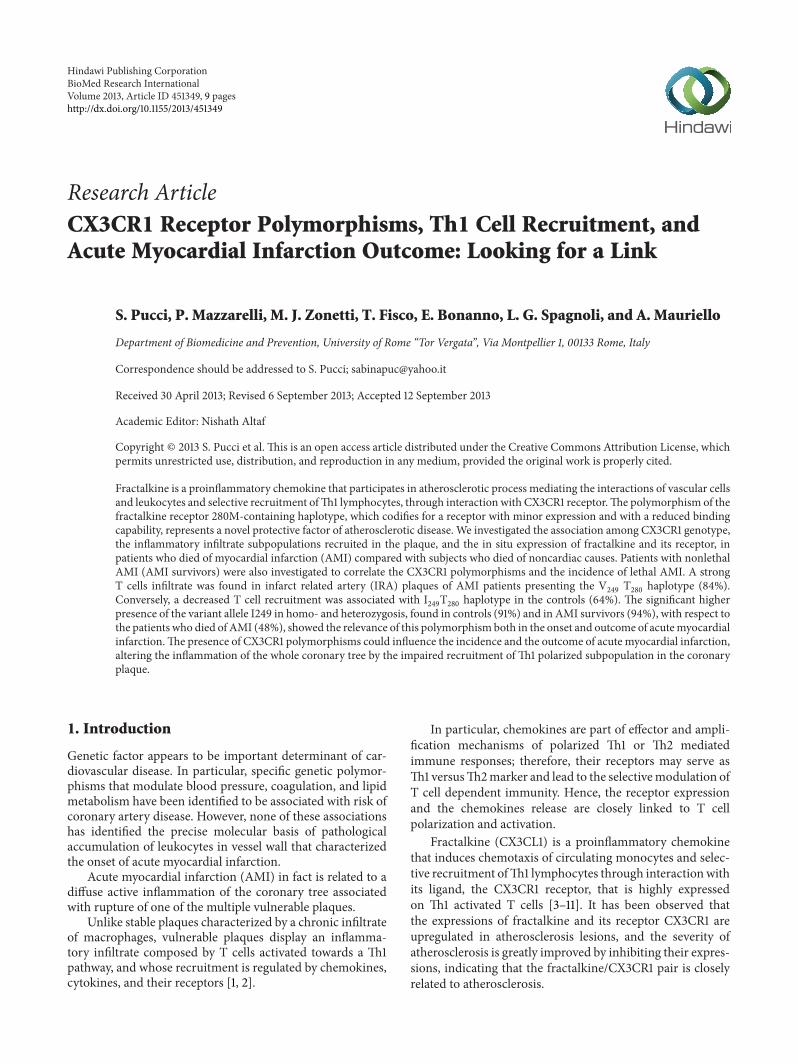
Figure 2 Coronary plaques morphology and inflammatory infiltrate characterization in AMI group (a)ndash(d) and control group (e)ndash(h) (a)shows an haematoxylin eosin stain of a plaque from AMI group showing a complicated plaque with a large necrotic core a thin cap and ahigh inflammatory infiltrate with a high percentage of lymphocytes ((b) macrophages CD68 positive revealed by alkaline phosphataseanti-alkaline phosphatase red reaction and T lymphocytes CD3 positive DAB detected streptavidinbiotin immunoperoxidase brown reaction)(c) shows the immunostaining against the fractalkine receptor CX3CR1 that gave rise to a strong diffuse positive reaction in the T cells of AMIgroup (d) (in the insert a particular corresponding to the area indicated by the arrow magnification 40x) demonstrate a positive reaction forfractalkine in the endothelial cells (e) shows an haematoxylin eosin of a coronary from a patient died by bronchopneumonia without clinicalcardiac historyThe plaque shows a thick fibrotic cap and the inflammatory infiltrate is scanty and predominantly constituted bymacrophages((f) macrophages CD68 positive revealed by alkaline phosphataseanti-alkaline phosphatase red reaction and T lymphocytes CD3 positiveDAB dectected streptavidinbiotin immunoperoxidase brown reaction) The immunostaining for the fractalkine receptor CX3CR1 gave riseto a weak positive reaction in the smooth muscle cells and macrophages ((g) 10x magnification) The reaction for fractalkine was negative inthe control group (h) (in the insert a particular corresponding to the area indicated by the arrow magnification 40x)
BioMed Research International 7
(b)
(c)
(d)(a)
Figure 3 Confocal microscopy examination of triple stain in a culprit lesion (coronary artery from AMI group) (a) (magnification 2000x)shows a 2D reconstruction triple stain for T cells CD3 (blue) fractalkine receptor CX3CR1 (green) and IFN-gamma (red) yellow lightblue and white areas were due to multiple positivity (b) CD3 immunostaining revealed by coumarin conjugated streptavidin (c) CX3CR1immunostaining revealed by FITC conjugated streptavidin (d) IFN-gamma immunostaining revealed by Texas Red conjugated streptavidin
Table 2 Correlation between inflammatory infiltrate and CX3CR1 polymorphismsect
AMI NCCVV249
1325 (52)lowastVI249
1025 (40)II249225 (8)
VV249222 (9)
VI2491222 (55)
II249822 (36)
CD3Negweak 0 0 1 1 7 7Pos moderate 0 1 1 1 5 0Strong 13 9 0 0 0 0
CD20Negweak 12 9 0 2 12 7Pos moderate 1 1 0 0 0 0Strong 0 0 2 0 0 0
CXCL1Negweak 0 0 0 1 12 7Pos moderate 1 1 2 1 0 0Strong 12 9 0 0 0 0
CXCR1Negweak 0 0 1 1 7 7Pos moderate 0 1 1 0 5 0Strong 13 9 0 1 0 0
sectThe table shows the IHC results in the coronary plaque of AMI and control patients (NCC) correlated to the presence of CX3CR1 V249I polymorphism inthe same groups lowastIn parentheses the percentage of patients was reported
and the occurrence of acute fatal myocardial infarction Astriking link between genotype and prognosis of the acuteevent was suggested by the observation of AMI survivorsgenotypes Notably the in situ CX3CR1 high expression in
AMI patients correlates with the presence of V249 polymor-phism in homo- or heterozygosis Conversely the genotypeanalysis of controls (with no CVD history) demonstrated thepresence of I249 polymorphism in homozygosis
8 BioMed Research International
Table 3 Analysis of CX3CR1 polymorphisms in patients andcontrol groups
AMI(119899 = 25)
SVR(119899 = 16)
NCC(119899 = 22)
V249IVV 13 (52) 1 (6) 2 (9)VI 10 (40) 10 (63) 12 (55)II 2 (8) 5 (31) 8 (36)
119875 = 0003 119875 = 0003 119875 = 0006
T280MTT 21 (84) 9 (56) 14 (64)TM 4 (16) 7 (44) 7 (32)MM 0 0 1 (4)
119875 = 0001 119875 = 0002 119875 = 0001
Data are absolute numbers (percentage)Abbreviations AMI acute myocardial infarction SVR patients survived toa first AMI NCC subjects dead for noncardiac causesThe statistical significance of different polymorphisms present in the singlegroups was identified by Fisherrsquos exact test
Indeed CX3CR1 V249T280 polymorphisms in homozy-gosis or heterozygosis have been demonstrated in 92 of theAMI patients analyzed (mean age 70 years old) In particular52 of the AMI patients examined were homozygous forCX3CR1 V249 whereas the analysis of the genotype of thecontrol subjects (mean age 737 years old) demonstrated thepresence of CX3CR1 V249 polymorphism in homozygosisonly in the 9 of cases The findings of the high percentageof II249 (36) and MM280 (4) in subjects died of nocardiac causes suggest a possible link between CX3CR1 poly-morphism T cell recruitment and acute eventMoreover thegenotype observations on survivors group suggest that thepresence of I249 allele is relevant not only for the occurrencebut also in the outcome of the acute event
There is evidence of the influence of CX3CR1 variableexpression and function on T cells recruitment efficiency[14 21 22]
Studies on CX3CR1 null mice crossed into apoE minusminusbackground [12] demonstrated that although CX3CL1 wasstrongly expressed in smooth muscle cells in the lesion thelack of the CX3CR1 receptor was related to a significantreduction in macrophages and T cells recruitment within thevessel wall associated with a reduction of atherosclerosis
In present work we also show a close association betweenCX3CR1 genotypes and coronary plaques T cell inflam-mation that is a relevant character of vulnerable plaquesaccording to data previously published [1 2]
Indeed coronary plaques of patients with CX3CR1 I249allele displayed a weaker T cell inflammation as compared toindividuals homozygous for the CX3CR1 V249 allele
In particular we show that CX3CR1 is highly expressedby the majority of T cells infiltrating IRA plaques of 22 out of25 AMI patients
It is worth noting that the two patients showing a lowexpression of CX3CR1 were CX3CR1 I249 homozygou andtheir plaques were infiltrated by B lymphocytes suggestinga different pathogenesis for AMI
Conversely immunostaining for CX3CR1 was negative orfaint positive in plaques of controls where the T lymphocytesinfiltrate was lower as compared with AMI patients
Therefore it can be assumed that the high expression ofCX3CR1 together with the in situ expression of fractalkine(CX3CL1) correlates with the increased recruitment of Tlymphocytes deeply infiltrating in the plaques of the AMIpatients
The special feature of fractalkine among other mem-bers of the chemokine family is due to the fact that it isexpressed both as soluble and membrane-bound form onthe surface of inflamed endothelium Interestingly whereassoluble fractalkine (CX3CL1) was reported to recruit lym-phocytes andmonocytes immobilized forms ofCX3CL1 havebeen shown to directly mediate the rapid capture and firmadhesion of leukocytes expressing its receptor CX3CR1 underphysiological flow conditions [23] The direct binding of thechemokine to CX3CR1 does not require the upregulationand activation of integrins suggesting that fractalkine andCX3CR1 mediate a novel pathway for leukocytes traffick-ing [24] In addition to the intrinsic adhesive functionof fractalkine this chemokine can also transduce signalsthrough G proteins that enhance the avidity of integrinbinding to its ligands for leukocytes recruitment [25 26]
The coexpression of CD3 IFN-gamma and CX3CR1 onT cell population found inAMI plaques compared to controlsdemonstrates the in situ activation of inflammatory cellspointing out the probable involvement of a recent immuneTh1 response in plaque destabilization and ruptureMoreoverthe data obtained suggest that the susceptibility to vascularinflammation is correlated with the amplified recruitment ofTh1 polarized cells expressing the high or low affinity CX3CR1receptor The findings revealing CX3CR1 expression by 80of T cell population along with the presence of fractalkinein IRA plaques suggest that these two events are both likelyto play a major role in determining plaque vulnerability byorchestratingTh1 cells recruitment
In agreement with previous clinical and epidemiologicalstudies our data demonstrate a close association betweenV249I and T280M polymorphisms coronary plaque vul-nerability and AMI confirming that the subjects with I249allele display a low level of T cell inflammation and areduced risk of developing vulnerable plaques and they have adecreased incidence of acute events (probably due to a lowerCX3CR1 binding affinity) [27] The comparative analysis ofthe different CXCR3 polymorphisms and the inflammatoryinfiltrate shows a significant difference between fatal AMIand NCC A study limitation is the lacking in the compar-ative analysis of the coronary surgical samples from AMIsurvivors These patients in fact underwent a ventricularrestoration for a previous nonfatal AMI event Despite theabove limitations our study provides lines of evidence thatthe I249 allele could be strongly involved in the protectionfrom fatal AMI with these association being independent ofthe major ldquoconventionalrdquo cardiovascular risk factors Furtherstudies will be addressed with a prospective massive scalepopulation study to validate this assumption
In conclusion CX3CR1 genotype could be considered as anew marker to stratify the population according to fatal AMI
BioMed Research International 9
risk Moreover CX3CR1 is likely to amplify the Th1 immuneresponse directly related to plaque vulnerability irrespec-tively of the causal agents (ie ox-LDL or Chlamydia) thusstanding out as a potential target in fatal AMI prevention
References
[1] A I Gotlieb ldquoAtherosclerosis and acute coronary syndromesrdquoCardiovascular Pathology vol 14 no 4 pp 181ndash184 2005
[2] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[3] P Fraticelli M Sironi G Bianchi et al ldquoFractalkine (CX3CL1)as an amplification circuit of polarized Th1 responsesrdquo Journalof Clinical Investigation vol 107 no 9 pp 1173ndash1181 2001
[4] R Bonecchi G Bianchi P P Bordignon et al ldquoDifferentialexpression of chemokine receptors and chemotactic respon-siveness of type 1 T helper cells (Th1s) and Th2srdquo Journal ofExperimental Medicine vol 187 no 1 pp 129ndash134 1998
[5] J F Bazan K B Bacon G Hardiman et al ldquoA new class ofmembrane-bound chemokine with a CX3C motifrdquo Nature vol385 no 6617 pp 640ndash642 1997
[6] C Murdoch and A Finn ldquoChemokine receptors and their rolein vascular biologyrdquo Journal of Vascular Research vol 37 no 1pp 1ndash7 2000
[7] C Murdoch and A Finn ldquoChemokine receptors and their rolein inflammation and infectious diseasesrdquo Blood vol 95 no 10pp 3032ndash3043 2000
[8] C Combadiere K Salzwedel E D Smith H L Tiffany E ABerger and PMMurphy ldquoIdentification of CX3CR1 A chemo-tactic receptor for the human CX3C chemokine fractalkineand a fusion coreceptor for HIV-1rdquo The Journal of BiologicalChemistry vol 273 no 37 pp 23799ndash23804 1998
[9] G A Chapman K E Moores J Gohil et al ldquoThe role offractalkine in the recruitment of monocytes to the endothe-liumrdquo European Journal of Pharmacology vol 392 no 3 pp189ndash195 2000
[10] T Kasama K Wakabayashi M Sato R Takahashi and TIsozaki ldquoRelevance of the CX3CL1fractalkine-CX3CR1 path-way in vasculitis and vasculopathyrdquo Translational Research vol155 no 1 pp 20ndash26 2010
[11] M Garcıa-Alvarez J Berenguer M Guzman-Fulgencio et alldquoHigh plasma fractalkine (CX3CL1) levels are associated withsevere liver disease inHIVHCVco-infected patients withHCVgenotype 1rdquo Cytokine vol 54 no 3 pp 244ndash248 2011
[12] P Lesnik C A Haskell and I F Charo ldquoDecreased atheroscle-rosis in CX3CR1-- mice reveals a role for fractalkine inatherogenesisrdquo Journal of Clinical Investigation vol 111 no 3pp 333ndash340 2003
[13] M Stolla J Pelisek M-L von Bruhl A Schafer V Barockeand P Heider ldquoFractalkine is expressed in early and advancedatherosclerotic lesions and supports monocyte recruitment viaCX3CR1rdquo PLoS ONE vol 7 no 8 Article ID e43572 2012
[14] J K Damas A Boullier T Waelighre et al ldquoExpression offractalkine (CX3CL1) and its receptor CX3CR1 is elevated incoronary artery disease and is reduced during statin therapyrdquoArteriosclerosis Thrombosis and Vascular Biology vol 25 no12 pp 2567ndash2572 2005
[15] A M Fong L A Robinson D A Steeber et al ldquoFractalkineand CX3CR1 mediate a novel mechanism of leukocyte capturefirm adhesion and activation under physiologic flowrdquo Journalof Experimental Medicine vol 188 no 8 pp 1413ndash1419 1998
[16] D Moatti S Faure F Fumeron et al ldquoPolymorphism in thefractalkine receptor CX3CR1 as a genetic risk factor for coro-nary artery diseaserdquo Blood vol 97 no 7 pp 1925ndash1928 2001
[17] N Singh N Sinha S Kumar C M Pandey and S AgrawalldquoPolymorphism in chemokine receptor genes and risk of acutemyocardial infarction in North Indian populationrdquo MolecularBiology Reports vol 39 no 3 pp 2753ndash2759 2012
[18] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[19] G K Hansson and A Hermansson ldquoThe immune system inatherosclerosisrdquoNature Immunology vol 12 no 3 pp 204ndash2122011
[20] H Umehara E Bloom T Okazaki N Domae and T ImaildquoFractalkine and vascular injuryrdquoTrends in Immunology vol 22no 11 pp 602ndash607 2001
[21] H Umehara S Goda T Imai et al ldquoFractalkine a CX3C-chemokine functions predominantly as an adhesion moleculeinmonocytic cell line THP-1rdquo Immunology andCell Biology vol79 no 3 pp 298ndash302 2001
[22] L Lasagni M Francalanci F Annunziato et al ldquoAn alter-natively spliced variant of CXCR3 mediates the inhibition ofendothelial cell growth induced by IP-10 Mig and I-TACand acts as functional receptor for platelet factor 4rdquo Journal ofExperimental Medicine vol 197 no 11 pp 1537ndash1549 2003
[23] S Jung J Aliberti P Graemmel et al ldquoAnalysis of fractalkinereceptor CX3CR1 function by targeted deletion and greenfluorescent protein reporter gene insertionrdquo Molecular andCellular Biology vol 20 no 11 pp 4106ndash4114 2000
[24] D H McDermott J P J Halcox W H Schenke et alldquoAssociation between polymorphism in the chemokine receptorCX3CR1 and coronary vascular endothelial dysfunction andatherosclerosisrdquoCirculation Research vol 89 no 5 pp 401ndash4072001
[25] H Umehara and T Imai ldquoRole of fractalkine in leukocyteadhesion and migration and in vascular injuryrdquoDrug News andPerspectives vol 14 no 8 pp 460ndash464 2001
[26] H Fujimoto Y Tanaka Z-J Liu et al ldquoDown-regulation of 1205726integrin an anti-oncogene product by functional cooperationof H-Ras and c-Mycrdquo Genes to Cells vol 6 no 4 pp 337ndash3432001
[27] M Kimoli S Miyakis P Georgakopoulos E Noefytou A DAchimastos and D A Spandidos ldquoPolymorphisms of frac-talkine receptorCX3CR1 gene in patientswith symptomatic andasymptomatic carotid artery stenosisrdquo Journal of Atherosclerosisand Thrombosis vol 16 no 5 pp 604ndash610 2009
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

2 BioMed Research International
Studies on CX3CR1 receptor knock out animal modelsand on human coronaries with native atherosclerosis pointout the important role of fractalkine in atherogenesis andplaque progression [12 13]
Recent data demonstrated the enhanced expression ofCXCL1 and its receptor (CX3CR1) in coronary artery diseasethat could be downmodulated by statin therapy [14] Thesedata suggest a role of CXCL1 and CXCR1 as therapeutic tar-gets in the care of CADpatients including those with unstabledisease
Epidemiological studies have proved the existence of twocommon nonsynonymous single-nucleotide polymorphismsof CX3CR1 receptor gene (V249I and T280M)The polymor-phisms of the fractalkine receptor that codify for a moleculewithminor expression and with a reduced binding capabilityhave been proposed as a novel protectivemarker for coronarydisease In particular the CX3CR1 I249 allele in homo- andheterozygote conditions has been associated with a markedreduction in risk of acute coronary events [15ndash17] In additionpopulation studies on CX3CR1 polymorphism have firmlyconfirmed that 280M-containing haplotype is associatedwith reduced risk of atherosclerotic disease As shown byexperimental studies the presence of the I
249M280
haplotypecodifies for a chemokine receptor variant that has impairedadhesive function low binding activity and low recruitmentefficiency of T cells within the plaque On the contrary theCX3CR1 V
249T280
haplotype characterized by high expres-sion and binding efficiency is associated with high riskof CAD and could be related to plaque vulnerability andrupture
All these data suggest that the CX3CR1 V249 and T280polymorphisms could amplify the Th1 response trigger-ing plaque vulnerability and rupture Moreover the higherexpression and binding activity of this receptor could influ-ence the atherogenesis in patients with artery disease and theincidence and the outcome of the myocardial infarction
Little information is available regarding the risk factorspredicting the subsequent lethal cardiac events after acutemyocardial infarction (AMI) In fact despite the use ofadvanced medical and invasive procedures the risk adjusted90-day mortality rates in patients with myocardial infarctionare up to 20ndash24 Recent data pointed out the relevant roleof diffuse inflammatory process We have recently demon-strated in patients who died of a first AMI the presence ofa strongly activated T cell infiltrate in the entire coronary treeand in the peri-infarctual and in the remote unaffectedmyocardial regions underlying both coronary and myocar-dial vulnerability [18 19] In view of that the object ofthis investigation was to determine if the CX3CR1 polymor-phisms genetic factors previously described to be involvedin atherogenesis play a role in the pathobiology of acutemyocardial infarction
Therefore we evaluated the inflammatory burden and thein situ expression of fractalkine and its receptor in coronaryplaques of patients died of myocardial infarction (AMI) ascompared to subjects died of noncardiac causes in order tofocus if the presence of I249M280 haplotype correlates withan impairedTh1 cell recruitment in the plaque
We further evaluate if the CX3CR1 polymorphisms couldinfluence the outcome of acute myocardial infarction Atthis purpose we examined the of CX3CR1 polymorphismspresence in individuals who died of noncardiac causes in acohort of patients that survived at acutemyocardial infarction(AMI survivors) compared with patients died of AMI
2 Methods
21 Case Selection We observed 25 patients (17 males8females mean age 705 plusmn 18 years) died of acute myocardialinfarction (AMI group) and 22 age-matched patients (15males7 females mean age 737 plusmn 28) died of noncardiaccauses andwithout clinical cardiac history (NCCgroup) Fur-ther 16 patients (mean age 65 plusmn 99 yr 13males) who survivedat a previous myocardial infarction (MI) suitable for surgicalventricular restoration have been analyzed (SVR group)Clinical angiographic and surgical characteristics are listedin Table 1 In the AMI group the time from symptom onsetto death was within 72 hours for all cases Clinical historyand standard electrocardiographic findings defined acutemyocardial infarction Histopathological examination of themyocardium confirmed AMI as cause of death The infarctwas transmural and from a single coronary artery distribu-tion in all cases Myocardium from NCC patients died ofbronchopneumonia pulmonary embolism and intestinalhemorrhage did not show either infarct or necrosis in allcases
Themain indications for surgery of patients of SVR groupwere symptoms of heart failure angina andor a combinationof the two Four patients of this group (25) had associatedmitral valve repair for a grade 3+4+ of mitral regurgitationThe surgical technique has been previously described [1]Mitral valve (MV) is repaired when needed through theventricle
Patients with chronic inflammatory diseases or tumorswere excluded from the study to avoid bias due to immuno-logical changes All autopsies were performed within 12ndash24hours of death
22 Tissue Handling and Processing At the autopsy in AMIand NCC the 4 major epicardial coronary arteries (leftmain left anterior descending left circumflex and right)were dissected from each heart 10 buffered formalin fixedcut transversely at 5mm intervals decalcified if necessaryparaffin embedded and serially sectioned for morphologicaland immunohistochemical studiesThe hearts were transver-sally cut at 1 cm intervals from the apex to the base Themyocardium was examined for the presence and extent ofinfarctionThe location ofmyocardial infarctionwas detectedby immersion of a cross-section of the heart in a solutionof triphenyltetrazolium chloride (for the autoptic demon-stration of myocardial infarction) In addition in all casesanother cross-section of the heart was processed for histolog-ical examination and the infarction was confirmed by lightmicroscopy
In SVR patients LVmyocardial samples were obtained atthe time of surgical operation The tissue was taken from thetransition zone between MI and the remote normal region
BioMed Research International 3
Table 1 Clinical and surgical data of patients
AMIlowast group (25 pts) NCClowast group (22 pts) SVRlowast group (16 pts)Clinical data
Age (yr plusmn SE) 705 plusmn 18 737 plusmn 28 65 plusmn 27
Male 17 (68) 15 (68) 13 (81)Hypertension 18 (72) 14 (64) 11 (69)Diabetes 13 (52) 10 (45) 7 (44)Previous smoking 13 (52) 11 (50) 7 (44)Hyperlipidemia 14 (56) 10 (45) 8 (50)Previous MI () 0 0 16 (100)Previous PTCA 0 0 5 (31)
Autoptic data causes of deathAcute MI 25 (100) 0
Anterior wall 13 (52) 0Posterolateral wall 7 (28) 0Posterior wall 5 (20) 0
Bronchopneumonia 0 14 (64)Pulmonary embolism 0 5 (23)Intestinal hemorrhage 0 3 (14)
Surgical dataMean time fromMI to Op (mo plusmn SE) 51 plusmn 9
EF (plusmn SE) 30 plusmn 25
LVEDV (mL plusmn SE) 183 plusmn 102
LVESV (mL plusmn SE) 129 plusmn 101
CABG 15 (94)LIMA grafts 15 (94)No of total anastomosis (plusmnSE) 29 plusmn 03
lowastAMI acute myocardial infarction patients NCC subjects dead for noncardiac causes SVR patients survived to a first AMIData are absolute numbers (percentage)Abbreviations CABG coronary artery bypass graft EF ejection fraction LIMA left internal mammary artery LVEDV left ventricle end-diastolic volumeLVESV left ventricle end-systolic volume MI myocardial infarction PTCA percutaneous transluminal coronary angioplasty SE standard error
All tissues were fixed in 10 formalin and embedded inparaffin
23 Morphological Studies Coronary sections from the twogroups HampE and pentachrome stained were examined bylight microscopy Culprit plaques were defined as lesionsshowing either plaque rupture or erosion with superimposedthrombusThe coronary artery showing the culprit lesionwasdefined as infarct-related artery (IRA) In AMI were exam-ined the culprit segment in the IRA including the throm-botic lesion 15 cm long a segment 15 cm long in whichmaximum of stenosis was present in the non-IRA coronaryIn NCC a segment of 15 cm long in which maximum ofstenosis was present was selected All coronary segmentswere cut transversely at 5mm intervals A total of 216 arterialsegments were paraffin embedded and serially sectioned 150from the AMI group (75 from IRA and 75 from non-IRAcoronaries) and 66 from NCC group respectively
24 Immunohistochemical Studies (IHC) Serial 3 120583m thicksections were cut from paraffin blocks and mounted onSuperFrost Plus slides (Menzel-Glaser Germany) 120572-smoothactin CD68 CD3 (Dakopatts Denmark) fractalkine (RampD
System Minneapolis MN) and CX3CR1 (GmbH Gottin-gen D) primary monoclonal antibodies were used CD68(alkaline phosphataseanti-alkaline phosphatase) and CD3(DAB detected) IHC was used to quantify the inflammatoryinfiltrate For each antibody positive cells as a mean of 10randomly selected fields per section were counted at amagnification of 40X in the plaque shoulder region and inthe cap itself
25 Confocal Microscopy Immunofluorescence In order tocharacterize the cell subpopulations that express CX3CR1 weperformed a triple immunostaining for confocal microscopyParaffin sections of coronary plaques were first incubatedwith anti-CD3 MoAb (1 20 1 h at RT) rinsed and thenincubated with biotinylated mouse IgG Fluorescence wasobtained by incubating the sections with a streptavidin-coumarin fluorochrome A second reaction with primaryantibodies to CX3CR1 (dilution 1 50 1 h at RT in the dark)was performed Fluorescence was obtained with a conjugatestreptavidin-fluorescein conjugate (FITC) A third immunos-taining was performed by incubating the sections withanti-IFN gamma monoclonal antibody (dilution 1 25 1 hat RT in the dark) Sections were incubated with tyramide
4 BioMed Research International
signal amplification biotin system (NEN Life Science Prod-ucts Boston MA USA) Fluorescence was obtained with astreptavidin-Texas Red fluorescent conjugate Control sec-tions were incubated with amixture of irrelevantmonoclonalreagents having a similar isotype Images were acquired bymeans of Noran confocal microscope at 60X14 NA immer-sion oil lens Three D stacks were acquired at a resolution of01 micron in119883- 119884- and 119885-axis
26 DNA Extraction DNA was extracted from formalinfixed and paraffin embedded heart of the subjects describedabove Paraffin was removed with xylene for 5min at roomtemperature Samples were centrifuged at full speed for 5minat RT Supernatant was removed and 12mL of 100 ethanolwas added to remove residual xyleneTheDNAwas extractedwith the QIAamp DNA kit (Qiagen GmbH Germany) andresuspended in 50 120583L of Buffer AE
27 Screening for Polymorphisms The DNA quality wascontrolled by a genomic polymerase reaction assay (PCR)using the primer set for BAK gene The following two poly-morphisms have been analyzed I249 a guanidine to adeninesubstitution at nucleotide 745 of the open reading framechanging valine at position 249 to isoleucine and M280 acytosine to thymidine substitution at nucleotide 839 changinga threonine at position 280The PCR product was analyzed in2 agarose gel stained with ethidium bromide CX3CR1 geneT280M and V249I mutations were identified after amplifica-tion of 311 base pairs (bp) (primers forward 51015840 AGA ATCATC CAG ACG CTG TTT TCC 31015840 reverse 51015840 CAG AGGACAGCCAGGCATTTCC31015840)TheT280MandV429Iweredetected on the same amplified fragment Amplification reac-tions were performed using 35 cycles of 95∘C 69∘C and 72∘Cfor 30 seconds each preceded by a single cycle of 95∘C for 3minutes and followed by a single cycle of 72∘C for 10 minutesIn order to type the alleles at codons 249 and 280 5 120583L ofPCR reactionwas digested respectively with Acl I (NewEng-land Biolabs BeverlyMA) or BsbmB1 (New England BiolabsBeverlyMA) in 20 120583L of reaction as previously described [11]In order to evaluate the efficiency of endonucleases enzymescontrol DNA with Acl I and Bst 4CI restriction sites wasused and DNA was loaded at different times on agarose gelThe genotypes were analysed and determined by analyticalelectrophoresis of each digestion on a 2 agarose gel
28 Statistical Analysis Statistical analysis of the data wasperformed with SPSS for Windows (version 110 SPSSChicago IL) Unpaired 119905-test was utilized to assess intergroupdifferences for continuous variables The 1198832 test was used toestablish differences in the distribution between categoricalvariables The statistical significance of different polymor-phisms present in the single groups was identified by Fisherrsquosexact test A 119875 value of lt005 was considered statisticallysignificant
Using logistic regression analysis (SPSS 130) the associ-ation of each polymorphism with the cardiovascular events(fatal AMI survivors and control group) was adjusted forage gender smoking cigarette hypertension diabetes mel-litus and hyperlipidemia
0 10 20 30 40
AMI
CTRL
T cellsMacrophages
(a)
0 20 40 60 80 100
AMI
CTRL
CX3CR1
(b)
Figure 1 Inflammatory cells characterization (a) shows the per-centages of inflammatory cells T lymphocytes (dotted bar) andmacrophages (dashed bar) in AMI and control group (b) Shows thepercentages of T cells CX3CR1 positive in AMI and control group
3 Results
31 Coronary Plaques Inflammation The examination of thewhole coronary tree of the AMI group demonstrated thepresence ofmultiple complicated atherosclerotic plaqueswitha thin fibrous cap and a high inflammatory infiltrate more-over in the coronary branch supplying the infarct area (IRA)we found a disruptedthrombotic plaque (culprit plaque)Conversely the coronary trees of the control group (NCC)showed atherosclerotic lesions with a thick fibrous cap and ascanty inflammatory infiltrate No plaque disruption or ero-sion or thrombosis has been observed Clinical autoptic andsurgical patient characteristics are showed in Table 1
Cell subpopulations were characterized by immunohis-tochemical studies using specific antibodies for lymphocytes(CD3 T cells) macrophages (CD68) and smooth musclecells (120572-actin) A quantitative analysis demonstrated a signif-icant (119875 lt 001) increase in the inflammatory cells per area(CD3 and CD68 positive) in AMI plaques (514 plusmn 25) ascompared with the plaques of the NCC group (224 plusmn 19)T lymphocytes represented the 185plusmn23 of the plaque cellsin AMI and the 64 plusmn 18 of cells in the NCC whereasmacrophages were 329 plusmn 32 in the AMI and 160 plusmn 18 intheNCC (Figure 1(a))Moreover the expression of IFN-120574wasassessed in culprit lesions by immunofluorescence staining(coronary artery fromAMI group) with confocal microscopy(Figure 3)
BioMed Research International 5
32 Fractalkine and CX3CR1 Expression The Fractalkineexpression was evaluated by immunohistochemistry in orderto compare T cell population recruitment and chemokinerelease
Figure 2(b) shows the expression of CD3 fractalkinereceptor CX3CR1 Figure 2(c) in T cells infiltrating the culpritlesion In AMI plaques immunostaining for fractalkine wasstrongly positive (Figure 2(d)) The immunofluorescence inFigure 3 demonstrated the coexpression of these three pro-teins in the same cells of AMI culprit plaque confirming theexistence of a T cell chronic active inflammation Moreoverthese data demonstrated theTh1 mediated immune response(IFN-120574 production) involved in plaque inflammation anddestabilization correlated with the presence of Th1 polarizedT cells (CXCR1 expressing cells) recruited in the plaque by theinteraction of fractalkine and the CX3CR1 receptor on the Tcell membrane
The immunohistochemical studies demonstrated thatendothelial cells in plaques of AMI patients gave rise to adiffuse positive reaction for fractalkine Smooth muscle cellswere focally positive while lymphocytes and macrophageswere not Conversely in the plaques of NCC group all thecell types were almost negative for fractalkine (Figure 2)
The fractalkine receptor (CX3CR1) was strongly anddiffusely expressed in the cell membrane in T lympho-cytes of AMI plaques (Figure 2(c)) as compared to controlMacrophages and smoothmuscle cells gave rise to a weak andscattered positive reaction The reaction was almost negativein the plaques of NCC group only a weak positive stainingwas present in smooth muscle cells and macrophages in theplaque (Figure 2(g))
The quantitative study revealed that 83 of T cells in theAMI plaques were CX3CR1 positive (Figure 1(b)) indicating aTh1 subset polarized subpopulation Furthermore a confocalobservation of IFN-120574 expression confirmed that T lympho-cytes expressed IFN-120574 (Figure 3)
In the coronary plaques from control group T lympho-cytes showed a lower level of CX3CR1 positivity (18 of Tlymphocytes were positive) (Figure 1(b)) in this group thereaction for IFN-120574 was completely negative (not shown)
33 CX3CR1 Genotype Correlates with the Th1 Cells Recruit-ment It has been previously demonstrated that CX3CR1genotypes influence the fractalkine receptor binding affinityand therefore Th1 lymphocytes recruitment In order tocorrelate the presence of activated Th1 lymphocytes withCX3CR1 genotype patientswere genotyped for theV249I andT280Mpolymorphisms of CXCR1 gene DNA extracted frommyocardial formalin fixed and paraffin embedded sectionswas analyzed by polymerase chain reaction The genotypewas determined on the amplicon of 311 bp after digestionwithendonucleases specific for each polymorphism The analysisof CX3CR1 V249I and T280M polymorphisms demonstratedthat 13 out of 25 patients who died of infarction (52) werehomozygous for the V249 allele and 21 out of 25 (84) werehomozygous for the T280 allele (Table 2) Moreover the 40ofAMI patients (1025) were heterozygous for theV249 allelebut all of these were homozygous for T280 allele as shown inTable 2 On the other hand only 8 (225) of AMI patients
displayed I249 allele in homozygosis and T280 in homo-(84) or heterozygosis (16) Notably the two AMI patientswho presented the variant haplotypes 249II and 280TMhad reduced T infiltrate and low IFN-120574 production in theplaque but a large number of B cells In Table 2 the correlationbetween the genotype and the inflammatory infiltrate burdenis reported The higher presence of 249VV (52) in AMIgroup as compared to controls is correlated with the presenceof a consistent T cell infiltrate expressing CX3CR1 (119875 lt 001)confirming the Th1 polarized subpopulation recruitment inthe plaque
4 Correlation among AMI AMI Survivorsand NCC Genotype
The genotype analysis has been extended to a cohort ofindividuals survived at a first myocardial infarction (119899 = 16)in order to compare the presence of the allele variant with theoccurrence and the outcome of the acute event
We found that the 52 of AMI patients (1325) displayedthe V249 allele in homozygosis as compared with the 6of the AMI survivors (116) and the 9 of controls (222)(Table 3)
The multivariate analysis of each V249I polymorphismadjusted for clinical data in the three study groups showedthat the VV249 haplotype was significantly associated onlywith the fatal AMI (119875 = 0001) but not with all the major riskfactors
On the other hand the I249 variant allele was expressedin homozygosis only in the 8 of the AMI patients (225)(Table 3) as compared with the 36 of controls (822) andthe 31 of AMI survivors (516)
The analysis of T280Mpolymorphism displayed the pres-ence of the M280 variant allele in homozygosis in the 4 ofcontrols (122) as comparedwithAMI and survivors patientswhich showed no presence of this allele in homozygosis Thepresence ofM280 allele in homozygosiswas always associatedwith the I249 allele
In summary the significant higher presence of the variantallele I249 in homo- and heterozygosis found in controls(91) and in AMI survivors (94) with respect to thepatients died of AMI (48) showed the relevance of thispolymorphism both in the onset and outcome of acutemyocardial infarction confirming the correlation betweenCX3CR1 genotype and prognosis of the acute event
5 Discussion
Epidemiological and clinical studies have shown that theCX3CR1 receptor polymorphisms are linked with the risk ofcoronary artery diseases [14 15]
In particular the presence of CX3CR1 V249 and T280single nucleotide polymorphisms codify for a fractalkinereceptor that is overexpressed by activated inflammatory cellsand with higher binding affinity for fractalkine its naturalligand [16 20]
The genotyping analysis of the subjects enrolled in thepresent study demonstrated for the first time a direct corre-lation between CX3CR1 V249I and T280M polymorphisms
6 BioMed Research International
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
Figure 2 Coronary plaques morphology and inflammatory infiltrate characterization in AMI group (a)ndash(d) and control group (e)ndash(h) (a)shows an haematoxylin eosin stain of a plaque from AMI group showing a complicated plaque with a large necrotic core a thin cap and ahigh inflammatory infiltrate with a high percentage of lymphocytes ((b) macrophages CD68 positive revealed by alkaline phosphataseanti-alkaline phosphatase red reaction and T lymphocytes CD3 positive DAB detected streptavidinbiotin immunoperoxidase brown reaction)(c) shows the immunostaining against the fractalkine receptor CX3CR1 that gave rise to a strong diffuse positive reaction in the T cells of AMIgroup (d) (in the insert a particular corresponding to the area indicated by the arrow magnification 40x) demonstrate a positive reaction forfractalkine in the endothelial cells (e) shows an haematoxylin eosin of a coronary from a patient died by bronchopneumonia without clinicalcardiac historyThe plaque shows a thick fibrotic cap and the inflammatory infiltrate is scanty and predominantly constituted bymacrophages((f) macrophages CD68 positive revealed by alkaline phosphataseanti-alkaline phosphatase red reaction and T lymphocytes CD3 positiveDAB dectected streptavidinbiotin immunoperoxidase brown reaction) The immunostaining for the fractalkine receptor CX3CR1 gave riseto a weak positive reaction in the smooth muscle cells and macrophages ((g) 10x magnification) The reaction for fractalkine was negative inthe control group (h) (in the insert a particular corresponding to the area indicated by the arrow magnification 40x)
BioMed Research International 7
(b)
(c)
(d)(a)
Figure 3 Confocal microscopy examination of triple stain in a culprit lesion (coronary artery from AMI group) (a) (magnification 2000x)shows a 2D reconstruction triple stain for T cells CD3 (blue) fractalkine receptor CX3CR1 (green) and IFN-gamma (red) yellow lightblue and white areas were due to multiple positivity (b) CD3 immunostaining revealed by coumarin conjugated streptavidin (c) CX3CR1immunostaining revealed by FITC conjugated streptavidin (d) IFN-gamma immunostaining revealed by Texas Red conjugated streptavidin
Table 2 Correlation between inflammatory infiltrate and CX3CR1 polymorphismsect
AMI NCCVV249
1325 (52)lowastVI249
1025 (40)II249225 (8)
VV249222 (9)
VI2491222 (55)
II249822 (36)
CD3Negweak 0 0 1 1 7 7Pos moderate 0 1 1 1 5 0Strong 13 9 0 0 0 0
CD20Negweak 12 9 0 2 12 7Pos moderate 1 1 0 0 0 0Strong 0 0 2 0 0 0
CXCL1Negweak 0 0 0 1 12 7Pos moderate 1 1 2 1 0 0Strong 12 9 0 0 0 0
CXCR1Negweak 0 0 1 1 7 7Pos moderate 0 1 1 0 5 0Strong 13 9 0 1 0 0
sectThe table shows the IHC results in the coronary plaque of AMI and control patients (NCC) correlated to the presence of CX3CR1 V249I polymorphism inthe same groups lowastIn parentheses the percentage of patients was reported
and the occurrence of acute fatal myocardial infarction Astriking link between genotype and prognosis of the acuteevent was suggested by the observation of AMI survivorsgenotypes Notably the in situ CX3CR1 high expression in
AMI patients correlates with the presence of V249 polymor-phism in homo- or heterozygosis Conversely the genotypeanalysis of controls (with no CVD history) demonstrated thepresence of I249 polymorphism in homozygosis
8 BioMed Research International
Table 3 Analysis of CX3CR1 polymorphisms in patients andcontrol groups
AMI(119899 = 25)
SVR(119899 = 16)
NCC(119899 = 22)
V249IVV 13 (52) 1 (6) 2 (9)VI 10 (40) 10 (63) 12 (55)II 2 (8) 5 (31) 8 (36)
119875 = 0003 119875 = 0003 119875 = 0006
T280MTT 21 (84) 9 (56) 14 (64)TM 4 (16) 7 (44) 7 (32)MM 0 0 1 (4)
119875 = 0001 119875 = 0002 119875 = 0001
Data are absolute numbers (percentage)Abbreviations AMI acute myocardial infarction SVR patients survived toa first AMI NCC subjects dead for noncardiac causesThe statistical significance of different polymorphisms present in the singlegroups was identified by Fisherrsquos exact test
Indeed CX3CR1 V249T280 polymorphisms in homozy-gosis or heterozygosis have been demonstrated in 92 of theAMI patients analyzed (mean age 70 years old) In particular52 of the AMI patients examined were homozygous forCX3CR1 V249 whereas the analysis of the genotype of thecontrol subjects (mean age 737 years old) demonstrated thepresence of CX3CR1 V249 polymorphism in homozygosisonly in the 9 of cases The findings of the high percentageof II249 (36) and MM280 (4) in subjects died of nocardiac causes suggest a possible link between CX3CR1 poly-morphism T cell recruitment and acute eventMoreover thegenotype observations on survivors group suggest that thepresence of I249 allele is relevant not only for the occurrencebut also in the outcome of the acute event
There is evidence of the influence of CX3CR1 variableexpression and function on T cells recruitment efficiency[14 21 22]
Studies on CX3CR1 null mice crossed into apoE minusminusbackground [12] demonstrated that although CX3CL1 wasstrongly expressed in smooth muscle cells in the lesion thelack of the CX3CR1 receptor was related to a significantreduction in macrophages and T cells recruitment within thevessel wall associated with a reduction of atherosclerosis
In present work we also show a close association betweenCX3CR1 genotypes and coronary plaques T cell inflam-mation that is a relevant character of vulnerable plaquesaccording to data previously published [1 2]
Indeed coronary plaques of patients with CX3CR1 I249allele displayed a weaker T cell inflammation as compared toindividuals homozygous for the CX3CR1 V249 allele
In particular we show that CX3CR1 is highly expressedby the majority of T cells infiltrating IRA plaques of 22 out of25 AMI patients
It is worth noting that the two patients showing a lowexpression of CX3CR1 were CX3CR1 I249 homozygou andtheir plaques were infiltrated by B lymphocytes suggestinga different pathogenesis for AMI
Conversely immunostaining for CX3CR1 was negative orfaint positive in plaques of controls where the T lymphocytesinfiltrate was lower as compared with AMI patients
Therefore it can be assumed that the high expression ofCX3CR1 together with the in situ expression of fractalkine(CX3CL1) correlates with the increased recruitment of Tlymphocytes deeply infiltrating in the plaques of the AMIpatients
The special feature of fractalkine among other mem-bers of the chemokine family is due to the fact that it isexpressed both as soluble and membrane-bound form onthe surface of inflamed endothelium Interestingly whereassoluble fractalkine (CX3CL1) was reported to recruit lym-phocytes andmonocytes immobilized forms ofCX3CL1 havebeen shown to directly mediate the rapid capture and firmadhesion of leukocytes expressing its receptor CX3CR1 underphysiological flow conditions [23] The direct binding of thechemokine to CX3CR1 does not require the upregulationand activation of integrins suggesting that fractalkine andCX3CR1 mediate a novel pathway for leukocytes traffick-ing [24] In addition to the intrinsic adhesive functionof fractalkine this chemokine can also transduce signalsthrough G proteins that enhance the avidity of integrinbinding to its ligands for leukocytes recruitment [25 26]
The coexpression of CD3 IFN-gamma and CX3CR1 onT cell population found inAMI plaques compared to controlsdemonstrates the in situ activation of inflammatory cellspointing out the probable involvement of a recent immuneTh1 response in plaque destabilization and ruptureMoreoverthe data obtained suggest that the susceptibility to vascularinflammation is correlated with the amplified recruitment ofTh1 polarized cells expressing the high or low affinity CX3CR1receptor The findings revealing CX3CR1 expression by 80of T cell population along with the presence of fractalkinein IRA plaques suggest that these two events are both likelyto play a major role in determining plaque vulnerability byorchestratingTh1 cells recruitment
In agreement with previous clinical and epidemiologicalstudies our data demonstrate a close association betweenV249I and T280M polymorphisms coronary plaque vul-nerability and AMI confirming that the subjects with I249allele display a low level of T cell inflammation and areduced risk of developing vulnerable plaques and they have adecreased incidence of acute events (probably due to a lowerCX3CR1 binding affinity) [27] The comparative analysis ofthe different CXCR3 polymorphisms and the inflammatoryinfiltrate shows a significant difference between fatal AMIand NCC A study limitation is the lacking in the compar-ative analysis of the coronary surgical samples from AMIsurvivors These patients in fact underwent a ventricularrestoration for a previous nonfatal AMI event Despite theabove limitations our study provides lines of evidence thatthe I249 allele could be strongly involved in the protectionfrom fatal AMI with these association being independent ofthe major ldquoconventionalrdquo cardiovascular risk factors Furtherstudies will be addressed with a prospective massive scalepopulation study to validate this assumption
In conclusion CX3CR1 genotype could be considered as anew marker to stratify the population according to fatal AMI
BioMed Research International 9
risk Moreover CX3CR1 is likely to amplify the Th1 immuneresponse directly related to plaque vulnerability irrespec-tively of the causal agents (ie ox-LDL or Chlamydia) thusstanding out as a potential target in fatal AMI prevention
References
[1] A I Gotlieb ldquoAtherosclerosis and acute coronary syndromesrdquoCardiovascular Pathology vol 14 no 4 pp 181ndash184 2005
[2] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[3] P Fraticelli M Sironi G Bianchi et al ldquoFractalkine (CX3CL1)as an amplification circuit of polarized Th1 responsesrdquo Journalof Clinical Investigation vol 107 no 9 pp 1173ndash1181 2001
[4] R Bonecchi G Bianchi P P Bordignon et al ldquoDifferentialexpression of chemokine receptors and chemotactic respon-siveness of type 1 T helper cells (Th1s) and Th2srdquo Journal ofExperimental Medicine vol 187 no 1 pp 129ndash134 1998
[5] J F Bazan K B Bacon G Hardiman et al ldquoA new class ofmembrane-bound chemokine with a CX3C motifrdquo Nature vol385 no 6617 pp 640ndash642 1997
[6] C Murdoch and A Finn ldquoChemokine receptors and their rolein vascular biologyrdquo Journal of Vascular Research vol 37 no 1pp 1ndash7 2000
[7] C Murdoch and A Finn ldquoChemokine receptors and their rolein inflammation and infectious diseasesrdquo Blood vol 95 no 10pp 3032ndash3043 2000
[8] C Combadiere K Salzwedel E D Smith H L Tiffany E ABerger and PMMurphy ldquoIdentification of CX3CR1 A chemo-tactic receptor for the human CX3C chemokine fractalkineand a fusion coreceptor for HIV-1rdquo The Journal of BiologicalChemistry vol 273 no 37 pp 23799ndash23804 1998
[9] G A Chapman K E Moores J Gohil et al ldquoThe role offractalkine in the recruitment of monocytes to the endothe-liumrdquo European Journal of Pharmacology vol 392 no 3 pp189ndash195 2000
[10] T Kasama K Wakabayashi M Sato R Takahashi and TIsozaki ldquoRelevance of the CX3CL1fractalkine-CX3CR1 path-way in vasculitis and vasculopathyrdquo Translational Research vol155 no 1 pp 20ndash26 2010
[11] M Garcıa-Alvarez J Berenguer M Guzman-Fulgencio et alldquoHigh plasma fractalkine (CX3CL1) levels are associated withsevere liver disease inHIVHCVco-infected patients withHCVgenotype 1rdquo Cytokine vol 54 no 3 pp 244ndash248 2011
[12] P Lesnik C A Haskell and I F Charo ldquoDecreased atheroscle-rosis in CX3CR1-- mice reveals a role for fractalkine inatherogenesisrdquo Journal of Clinical Investigation vol 111 no 3pp 333ndash340 2003
[13] M Stolla J Pelisek M-L von Bruhl A Schafer V Barockeand P Heider ldquoFractalkine is expressed in early and advancedatherosclerotic lesions and supports monocyte recruitment viaCX3CR1rdquo PLoS ONE vol 7 no 8 Article ID e43572 2012
[14] J K Damas A Boullier T Waelighre et al ldquoExpression offractalkine (CX3CL1) and its receptor CX3CR1 is elevated incoronary artery disease and is reduced during statin therapyrdquoArteriosclerosis Thrombosis and Vascular Biology vol 25 no12 pp 2567ndash2572 2005
[15] A M Fong L A Robinson D A Steeber et al ldquoFractalkineand CX3CR1 mediate a novel mechanism of leukocyte capturefirm adhesion and activation under physiologic flowrdquo Journalof Experimental Medicine vol 188 no 8 pp 1413ndash1419 1998
[16] D Moatti S Faure F Fumeron et al ldquoPolymorphism in thefractalkine receptor CX3CR1 as a genetic risk factor for coro-nary artery diseaserdquo Blood vol 97 no 7 pp 1925ndash1928 2001
[17] N Singh N Sinha S Kumar C M Pandey and S AgrawalldquoPolymorphism in chemokine receptor genes and risk of acutemyocardial infarction in North Indian populationrdquo MolecularBiology Reports vol 39 no 3 pp 2753ndash2759 2012
[18] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[19] G K Hansson and A Hermansson ldquoThe immune system inatherosclerosisrdquoNature Immunology vol 12 no 3 pp 204ndash2122011
[20] H Umehara E Bloom T Okazaki N Domae and T ImaildquoFractalkine and vascular injuryrdquoTrends in Immunology vol 22no 11 pp 602ndash607 2001
[21] H Umehara S Goda T Imai et al ldquoFractalkine a CX3C-chemokine functions predominantly as an adhesion moleculeinmonocytic cell line THP-1rdquo Immunology andCell Biology vol79 no 3 pp 298ndash302 2001
[22] L Lasagni M Francalanci F Annunziato et al ldquoAn alter-natively spliced variant of CXCR3 mediates the inhibition ofendothelial cell growth induced by IP-10 Mig and I-TACand acts as functional receptor for platelet factor 4rdquo Journal ofExperimental Medicine vol 197 no 11 pp 1537ndash1549 2003
[23] S Jung J Aliberti P Graemmel et al ldquoAnalysis of fractalkinereceptor CX3CR1 function by targeted deletion and greenfluorescent protein reporter gene insertionrdquo Molecular andCellular Biology vol 20 no 11 pp 4106ndash4114 2000
[24] D H McDermott J P J Halcox W H Schenke et alldquoAssociation between polymorphism in the chemokine receptorCX3CR1 and coronary vascular endothelial dysfunction andatherosclerosisrdquoCirculation Research vol 89 no 5 pp 401ndash4072001
[25] H Umehara and T Imai ldquoRole of fractalkine in leukocyteadhesion and migration and in vascular injuryrdquoDrug News andPerspectives vol 14 no 8 pp 460ndash464 2001
[26] H Fujimoto Y Tanaka Z-J Liu et al ldquoDown-regulation of 1205726integrin an anti-oncogene product by functional cooperationof H-Ras and c-Mycrdquo Genes to Cells vol 6 no 4 pp 337ndash3432001
[27] M Kimoli S Miyakis P Georgakopoulos E Noefytou A DAchimastos and D A Spandidos ldquoPolymorphisms of frac-talkine receptorCX3CR1 gene in patientswith symptomatic andasymptomatic carotid artery stenosisrdquo Journal of Atherosclerosisand Thrombosis vol 16 no 5 pp 604ndash610 2009
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 3
Table 1 Clinical and surgical data of patients
AMIlowast group (25 pts) NCClowast group (22 pts) SVRlowast group (16 pts)Clinical data
Age (yr plusmn SE) 705 plusmn 18 737 plusmn 28 65 plusmn 27
Male 17 (68) 15 (68) 13 (81)Hypertension 18 (72) 14 (64) 11 (69)Diabetes 13 (52) 10 (45) 7 (44)Previous smoking 13 (52) 11 (50) 7 (44)Hyperlipidemia 14 (56) 10 (45) 8 (50)Previous MI () 0 0 16 (100)Previous PTCA 0 0 5 (31)
Autoptic data causes of deathAcute MI 25 (100) 0
Anterior wall 13 (52) 0Posterolateral wall 7 (28) 0Posterior wall 5 (20) 0
Bronchopneumonia 0 14 (64)Pulmonary embolism 0 5 (23)Intestinal hemorrhage 0 3 (14)
Surgical dataMean time fromMI to Op (mo plusmn SE) 51 plusmn 9
EF (plusmn SE) 30 plusmn 25
LVEDV (mL plusmn SE) 183 plusmn 102
LVESV (mL plusmn SE) 129 plusmn 101
CABG 15 (94)LIMA grafts 15 (94)No of total anastomosis (plusmnSE) 29 plusmn 03
lowastAMI acute myocardial infarction patients NCC subjects dead for noncardiac causes SVR patients survived to a first AMIData are absolute numbers (percentage)Abbreviations CABG coronary artery bypass graft EF ejection fraction LIMA left internal mammary artery LVEDV left ventricle end-diastolic volumeLVESV left ventricle end-systolic volume MI myocardial infarction PTCA percutaneous transluminal coronary angioplasty SE standard error
All tissues were fixed in 10 formalin and embedded inparaffin
23 Morphological Studies Coronary sections from the twogroups HampE and pentachrome stained were examined bylight microscopy Culprit plaques were defined as lesionsshowing either plaque rupture or erosion with superimposedthrombusThe coronary artery showing the culprit lesionwasdefined as infarct-related artery (IRA) In AMI were exam-ined the culprit segment in the IRA including the throm-botic lesion 15 cm long a segment 15 cm long in whichmaximum of stenosis was present in the non-IRA coronaryIn NCC a segment of 15 cm long in which maximum ofstenosis was present was selected All coronary segmentswere cut transversely at 5mm intervals A total of 216 arterialsegments were paraffin embedded and serially sectioned 150from the AMI group (75 from IRA and 75 from non-IRAcoronaries) and 66 from NCC group respectively
24 Immunohistochemical Studies (IHC) Serial 3 120583m thicksections were cut from paraffin blocks and mounted onSuperFrost Plus slides (Menzel-Glaser Germany) 120572-smoothactin CD68 CD3 (Dakopatts Denmark) fractalkine (RampD
System Minneapolis MN) and CX3CR1 (GmbH Gottin-gen D) primary monoclonal antibodies were used CD68(alkaline phosphataseanti-alkaline phosphatase) and CD3(DAB detected) IHC was used to quantify the inflammatoryinfiltrate For each antibody positive cells as a mean of 10randomly selected fields per section were counted at amagnification of 40X in the plaque shoulder region and inthe cap itself
25 Confocal Microscopy Immunofluorescence In order tocharacterize the cell subpopulations that express CX3CR1 weperformed a triple immunostaining for confocal microscopyParaffin sections of coronary plaques were first incubatedwith anti-CD3 MoAb (1 20 1 h at RT) rinsed and thenincubated with biotinylated mouse IgG Fluorescence wasobtained by incubating the sections with a streptavidin-coumarin fluorochrome A second reaction with primaryantibodies to CX3CR1 (dilution 1 50 1 h at RT in the dark)was performed Fluorescence was obtained with a conjugatestreptavidin-fluorescein conjugate (FITC) A third immunos-taining was performed by incubating the sections withanti-IFN gamma monoclonal antibody (dilution 1 25 1 hat RT in the dark) Sections were incubated with tyramide
4 BioMed Research International
signal amplification biotin system (NEN Life Science Prod-ucts Boston MA USA) Fluorescence was obtained with astreptavidin-Texas Red fluorescent conjugate Control sec-tions were incubated with amixture of irrelevantmonoclonalreagents having a similar isotype Images were acquired bymeans of Noran confocal microscope at 60X14 NA immer-sion oil lens Three D stacks were acquired at a resolution of01 micron in119883- 119884- and 119885-axis
26 DNA Extraction DNA was extracted from formalinfixed and paraffin embedded heart of the subjects describedabove Paraffin was removed with xylene for 5min at roomtemperature Samples were centrifuged at full speed for 5minat RT Supernatant was removed and 12mL of 100 ethanolwas added to remove residual xyleneTheDNAwas extractedwith the QIAamp DNA kit (Qiagen GmbH Germany) andresuspended in 50 120583L of Buffer AE
27 Screening for Polymorphisms The DNA quality wascontrolled by a genomic polymerase reaction assay (PCR)using the primer set for BAK gene The following two poly-morphisms have been analyzed I249 a guanidine to adeninesubstitution at nucleotide 745 of the open reading framechanging valine at position 249 to isoleucine and M280 acytosine to thymidine substitution at nucleotide 839 changinga threonine at position 280The PCR product was analyzed in2 agarose gel stained with ethidium bromide CX3CR1 geneT280M and V249I mutations were identified after amplifica-tion of 311 base pairs (bp) (primers forward 51015840 AGA ATCATC CAG ACG CTG TTT TCC 31015840 reverse 51015840 CAG AGGACAGCCAGGCATTTCC31015840)TheT280MandV429Iweredetected on the same amplified fragment Amplification reac-tions were performed using 35 cycles of 95∘C 69∘C and 72∘Cfor 30 seconds each preceded by a single cycle of 95∘C for 3minutes and followed by a single cycle of 72∘C for 10 minutesIn order to type the alleles at codons 249 and 280 5 120583L ofPCR reactionwas digested respectively with Acl I (NewEng-land Biolabs BeverlyMA) or BsbmB1 (New England BiolabsBeverlyMA) in 20 120583L of reaction as previously described [11]In order to evaluate the efficiency of endonucleases enzymescontrol DNA with Acl I and Bst 4CI restriction sites wasused and DNA was loaded at different times on agarose gelThe genotypes were analysed and determined by analyticalelectrophoresis of each digestion on a 2 agarose gel
28 Statistical Analysis Statistical analysis of the data wasperformed with SPSS for Windows (version 110 SPSSChicago IL) Unpaired 119905-test was utilized to assess intergroupdifferences for continuous variables The 1198832 test was used toestablish differences in the distribution between categoricalvariables The statistical significance of different polymor-phisms present in the single groups was identified by Fisherrsquosexact test A 119875 value of lt005 was considered statisticallysignificant
Using logistic regression analysis (SPSS 130) the associ-ation of each polymorphism with the cardiovascular events(fatal AMI survivors and control group) was adjusted forage gender smoking cigarette hypertension diabetes mel-litus and hyperlipidemia
0 10 20 30 40
AMI
CTRL
T cellsMacrophages
(a)
0 20 40 60 80 100
AMI
CTRL
CX3CR1
(b)
Figure 1 Inflammatory cells characterization (a) shows the per-centages of inflammatory cells T lymphocytes (dotted bar) andmacrophages (dashed bar) in AMI and control group (b) Shows thepercentages of T cells CX3CR1 positive in AMI and control group
3 Results
31 Coronary Plaques Inflammation The examination of thewhole coronary tree of the AMI group demonstrated thepresence ofmultiple complicated atherosclerotic plaqueswitha thin fibrous cap and a high inflammatory infiltrate more-over in the coronary branch supplying the infarct area (IRA)we found a disruptedthrombotic plaque (culprit plaque)Conversely the coronary trees of the control group (NCC)showed atherosclerotic lesions with a thick fibrous cap and ascanty inflammatory infiltrate No plaque disruption or ero-sion or thrombosis has been observed Clinical autoptic andsurgical patient characteristics are showed in Table 1
Cell subpopulations were characterized by immunohis-tochemical studies using specific antibodies for lymphocytes(CD3 T cells) macrophages (CD68) and smooth musclecells (120572-actin) A quantitative analysis demonstrated a signif-icant (119875 lt 001) increase in the inflammatory cells per area(CD3 and CD68 positive) in AMI plaques (514 plusmn 25) ascompared with the plaques of the NCC group (224 plusmn 19)T lymphocytes represented the 185plusmn23 of the plaque cellsin AMI and the 64 plusmn 18 of cells in the NCC whereasmacrophages were 329 plusmn 32 in the AMI and 160 plusmn 18 intheNCC (Figure 1(a))Moreover the expression of IFN-120574wasassessed in culprit lesions by immunofluorescence staining(coronary artery fromAMI group) with confocal microscopy(Figure 3)
BioMed Research International 5
32 Fractalkine and CX3CR1 Expression The Fractalkineexpression was evaluated by immunohistochemistry in orderto compare T cell population recruitment and chemokinerelease
Figure 2(b) shows the expression of CD3 fractalkinereceptor CX3CR1 Figure 2(c) in T cells infiltrating the culpritlesion In AMI plaques immunostaining for fractalkine wasstrongly positive (Figure 2(d)) The immunofluorescence inFigure 3 demonstrated the coexpression of these three pro-teins in the same cells of AMI culprit plaque confirming theexistence of a T cell chronic active inflammation Moreoverthese data demonstrated theTh1 mediated immune response(IFN-120574 production) involved in plaque inflammation anddestabilization correlated with the presence of Th1 polarizedT cells (CXCR1 expressing cells) recruited in the plaque by theinteraction of fractalkine and the CX3CR1 receptor on the Tcell membrane
The immunohistochemical studies demonstrated thatendothelial cells in plaques of AMI patients gave rise to adiffuse positive reaction for fractalkine Smooth muscle cellswere focally positive while lymphocytes and macrophageswere not Conversely in the plaques of NCC group all thecell types were almost negative for fractalkine (Figure 2)
The fractalkine receptor (CX3CR1) was strongly anddiffusely expressed in the cell membrane in T lympho-cytes of AMI plaques (Figure 2(c)) as compared to controlMacrophages and smoothmuscle cells gave rise to a weak andscattered positive reaction The reaction was almost negativein the plaques of NCC group only a weak positive stainingwas present in smooth muscle cells and macrophages in theplaque (Figure 2(g))
The quantitative study revealed that 83 of T cells in theAMI plaques were CX3CR1 positive (Figure 1(b)) indicating aTh1 subset polarized subpopulation Furthermore a confocalobservation of IFN-120574 expression confirmed that T lympho-cytes expressed IFN-120574 (Figure 3)
In the coronary plaques from control group T lympho-cytes showed a lower level of CX3CR1 positivity (18 of Tlymphocytes were positive) (Figure 1(b)) in this group thereaction for IFN-120574 was completely negative (not shown)
33 CX3CR1 Genotype Correlates with the Th1 Cells Recruit-ment It has been previously demonstrated that CX3CR1genotypes influence the fractalkine receptor binding affinityand therefore Th1 lymphocytes recruitment In order tocorrelate the presence of activated Th1 lymphocytes withCX3CR1 genotype patientswere genotyped for theV249I andT280Mpolymorphisms of CXCR1 gene DNA extracted frommyocardial formalin fixed and paraffin embedded sectionswas analyzed by polymerase chain reaction The genotypewas determined on the amplicon of 311 bp after digestionwithendonucleases specific for each polymorphism The analysisof CX3CR1 V249I and T280M polymorphisms demonstratedthat 13 out of 25 patients who died of infarction (52) werehomozygous for the V249 allele and 21 out of 25 (84) werehomozygous for the T280 allele (Table 2) Moreover the 40ofAMI patients (1025) were heterozygous for theV249 allelebut all of these were homozygous for T280 allele as shown inTable 2 On the other hand only 8 (225) of AMI patients
displayed I249 allele in homozygosis and T280 in homo-(84) or heterozygosis (16) Notably the two AMI patientswho presented the variant haplotypes 249II and 280TMhad reduced T infiltrate and low IFN-120574 production in theplaque but a large number of B cells In Table 2 the correlationbetween the genotype and the inflammatory infiltrate burdenis reported The higher presence of 249VV (52) in AMIgroup as compared to controls is correlated with the presenceof a consistent T cell infiltrate expressing CX3CR1 (119875 lt 001)confirming the Th1 polarized subpopulation recruitment inthe plaque
4 Correlation among AMI AMI Survivorsand NCC Genotype
The genotype analysis has been extended to a cohort ofindividuals survived at a first myocardial infarction (119899 = 16)in order to compare the presence of the allele variant with theoccurrence and the outcome of the acute event
We found that the 52 of AMI patients (1325) displayedthe V249 allele in homozygosis as compared with the 6of the AMI survivors (116) and the 9 of controls (222)(Table 3)
The multivariate analysis of each V249I polymorphismadjusted for clinical data in the three study groups showedthat the VV249 haplotype was significantly associated onlywith the fatal AMI (119875 = 0001) but not with all the major riskfactors
On the other hand the I249 variant allele was expressedin homozygosis only in the 8 of the AMI patients (225)(Table 3) as compared with the 36 of controls (822) andthe 31 of AMI survivors (516)
The analysis of T280Mpolymorphism displayed the pres-ence of the M280 variant allele in homozygosis in the 4 ofcontrols (122) as comparedwithAMI and survivors patientswhich showed no presence of this allele in homozygosis Thepresence ofM280 allele in homozygosiswas always associatedwith the I249 allele
In summary the significant higher presence of the variantallele I249 in homo- and heterozygosis found in controls(91) and in AMI survivors (94) with respect to thepatients died of AMI (48) showed the relevance of thispolymorphism both in the onset and outcome of acutemyocardial infarction confirming the correlation betweenCX3CR1 genotype and prognosis of the acute event
5 Discussion
Epidemiological and clinical studies have shown that theCX3CR1 receptor polymorphisms are linked with the risk ofcoronary artery diseases [14 15]
In particular the presence of CX3CR1 V249 and T280single nucleotide polymorphisms codify for a fractalkinereceptor that is overexpressed by activated inflammatory cellsand with higher binding affinity for fractalkine its naturalligand [16 20]
The genotyping analysis of the subjects enrolled in thepresent study demonstrated for the first time a direct corre-lation between CX3CR1 V249I and T280M polymorphisms
6 BioMed Research International
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
Figure 2 Coronary plaques morphology and inflammatory infiltrate characterization in AMI group (a)ndash(d) and control group (e)ndash(h) (a)shows an haematoxylin eosin stain of a plaque from AMI group showing a complicated plaque with a large necrotic core a thin cap and ahigh inflammatory infiltrate with a high percentage of lymphocytes ((b) macrophages CD68 positive revealed by alkaline phosphataseanti-alkaline phosphatase red reaction and T lymphocytes CD3 positive DAB detected streptavidinbiotin immunoperoxidase brown reaction)(c) shows the immunostaining against the fractalkine receptor CX3CR1 that gave rise to a strong diffuse positive reaction in the T cells of AMIgroup (d) (in the insert a particular corresponding to the area indicated by the arrow magnification 40x) demonstrate a positive reaction forfractalkine in the endothelial cells (e) shows an haematoxylin eosin of a coronary from a patient died by bronchopneumonia without clinicalcardiac historyThe plaque shows a thick fibrotic cap and the inflammatory infiltrate is scanty and predominantly constituted bymacrophages((f) macrophages CD68 positive revealed by alkaline phosphataseanti-alkaline phosphatase red reaction and T lymphocytes CD3 positiveDAB dectected streptavidinbiotin immunoperoxidase brown reaction) The immunostaining for the fractalkine receptor CX3CR1 gave riseto a weak positive reaction in the smooth muscle cells and macrophages ((g) 10x magnification) The reaction for fractalkine was negative inthe control group (h) (in the insert a particular corresponding to the area indicated by the arrow magnification 40x)
BioMed Research International 7
(b)
(c)
(d)(a)
Figure 3 Confocal microscopy examination of triple stain in a culprit lesion (coronary artery from AMI group) (a) (magnification 2000x)shows a 2D reconstruction triple stain for T cells CD3 (blue) fractalkine receptor CX3CR1 (green) and IFN-gamma (red) yellow lightblue and white areas were due to multiple positivity (b) CD3 immunostaining revealed by coumarin conjugated streptavidin (c) CX3CR1immunostaining revealed by FITC conjugated streptavidin (d) IFN-gamma immunostaining revealed by Texas Red conjugated streptavidin
Table 2 Correlation between inflammatory infiltrate and CX3CR1 polymorphismsect
AMI NCCVV249
1325 (52)lowastVI249
1025 (40)II249225 (8)
VV249222 (9)
VI2491222 (55)
II249822 (36)
CD3Negweak 0 0 1 1 7 7Pos moderate 0 1 1 1 5 0Strong 13 9 0 0 0 0
CD20Negweak 12 9 0 2 12 7Pos moderate 1 1 0 0 0 0Strong 0 0 2 0 0 0
CXCL1Negweak 0 0 0 1 12 7Pos moderate 1 1 2 1 0 0Strong 12 9 0 0 0 0
CXCR1Negweak 0 0 1 1 7 7Pos moderate 0 1 1 0 5 0Strong 13 9 0 1 0 0
sectThe table shows the IHC results in the coronary plaque of AMI and control patients (NCC) correlated to the presence of CX3CR1 V249I polymorphism inthe same groups lowastIn parentheses the percentage of patients was reported
and the occurrence of acute fatal myocardial infarction Astriking link between genotype and prognosis of the acuteevent was suggested by the observation of AMI survivorsgenotypes Notably the in situ CX3CR1 high expression in
AMI patients correlates with the presence of V249 polymor-phism in homo- or heterozygosis Conversely the genotypeanalysis of controls (with no CVD history) demonstrated thepresence of I249 polymorphism in homozygosis
8 BioMed Research International
Table 3 Analysis of CX3CR1 polymorphisms in patients andcontrol groups
AMI(119899 = 25)
SVR(119899 = 16)
NCC(119899 = 22)
V249IVV 13 (52) 1 (6) 2 (9)VI 10 (40) 10 (63) 12 (55)II 2 (8) 5 (31) 8 (36)
119875 = 0003 119875 = 0003 119875 = 0006
T280MTT 21 (84) 9 (56) 14 (64)TM 4 (16) 7 (44) 7 (32)MM 0 0 1 (4)
119875 = 0001 119875 = 0002 119875 = 0001
Data are absolute numbers (percentage)Abbreviations AMI acute myocardial infarction SVR patients survived toa first AMI NCC subjects dead for noncardiac causesThe statistical significance of different polymorphisms present in the singlegroups was identified by Fisherrsquos exact test
Indeed CX3CR1 V249T280 polymorphisms in homozy-gosis or heterozygosis have been demonstrated in 92 of theAMI patients analyzed (mean age 70 years old) In particular52 of the AMI patients examined were homozygous forCX3CR1 V249 whereas the analysis of the genotype of thecontrol subjects (mean age 737 years old) demonstrated thepresence of CX3CR1 V249 polymorphism in homozygosisonly in the 9 of cases The findings of the high percentageof II249 (36) and MM280 (4) in subjects died of nocardiac causes suggest a possible link between CX3CR1 poly-morphism T cell recruitment and acute eventMoreover thegenotype observations on survivors group suggest that thepresence of I249 allele is relevant not only for the occurrencebut also in the outcome of the acute event
There is evidence of the influence of CX3CR1 variableexpression and function on T cells recruitment efficiency[14 21 22]
Studies on CX3CR1 null mice crossed into apoE minusminusbackground [12] demonstrated that although CX3CL1 wasstrongly expressed in smooth muscle cells in the lesion thelack of the CX3CR1 receptor was related to a significantreduction in macrophages and T cells recruitment within thevessel wall associated with a reduction of atherosclerosis
In present work we also show a close association betweenCX3CR1 genotypes and coronary plaques T cell inflam-mation that is a relevant character of vulnerable plaquesaccording to data previously published [1 2]
Indeed coronary plaques of patients with CX3CR1 I249allele displayed a weaker T cell inflammation as compared toindividuals homozygous for the CX3CR1 V249 allele
In particular we show that CX3CR1 is highly expressedby the majority of T cells infiltrating IRA plaques of 22 out of25 AMI patients
It is worth noting that the two patients showing a lowexpression of CX3CR1 were CX3CR1 I249 homozygou andtheir plaques were infiltrated by B lymphocytes suggestinga different pathogenesis for AMI
Conversely immunostaining for CX3CR1 was negative orfaint positive in plaques of controls where the T lymphocytesinfiltrate was lower as compared with AMI patients
Therefore it can be assumed that the high expression ofCX3CR1 together with the in situ expression of fractalkine(CX3CL1) correlates with the increased recruitment of Tlymphocytes deeply infiltrating in the plaques of the AMIpatients
The special feature of fractalkine among other mem-bers of the chemokine family is due to the fact that it isexpressed both as soluble and membrane-bound form onthe surface of inflamed endothelium Interestingly whereassoluble fractalkine (CX3CL1) was reported to recruit lym-phocytes andmonocytes immobilized forms ofCX3CL1 havebeen shown to directly mediate the rapid capture and firmadhesion of leukocytes expressing its receptor CX3CR1 underphysiological flow conditions [23] The direct binding of thechemokine to CX3CR1 does not require the upregulationand activation of integrins suggesting that fractalkine andCX3CR1 mediate a novel pathway for leukocytes traffick-ing [24] In addition to the intrinsic adhesive functionof fractalkine this chemokine can also transduce signalsthrough G proteins that enhance the avidity of integrinbinding to its ligands for leukocytes recruitment [25 26]
The coexpression of CD3 IFN-gamma and CX3CR1 onT cell population found inAMI plaques compared to controlsdemonstrates the in situ activation of inflammatory cellspointing out the probable involvement of a recent immuneTh1 response in plaque destabilization and ruptureMoreoverthe data obtained suggest that the susceptibility to vascularinflammation is correlated with the amplified recruitment ofTh1 polarized cells expressing the high or low affinity CX3CR1receptor The findings revealing CX3CR1 expression by 80of T cell population along with the presence of fractalkinein IRA plaques suggest that these two events are both likelyto play a major role in determining plaque vulnerability byorchestratingTh1 cells recruitment
In agreement with previous clinical and epidemiologicalstudies our data demonstrate a close association betweenV249I and T280M polymorphisms coronary plaque vul-nerability and AMI confirming that the subjects with I249allele display a low level of T cell inflammation and areduced risk of developing vulnerable plaques and they have adecreased incidence of acute events (probably due to a lowerCX3CR1 binding affinity) [27] The comparative analysis ofthe different CXCR3 polymorphisms and the inflammatoryinfiltrate shows a significant difference between fatal AMIand NCC A study limitation is the lacking in the compar-ative analysis of the coronary surgical samples from AMIsurvivors These patients in fact underwent a ventricularrestoration for a previous nonfatal AMI event Despite theabove limitations our study provides lines of evidence thatthe I249 allele could be strongly involved in the protectionfrom fatal AMI with these association being independent ofthe major ldquoconventionalrdquo cardiovascular risk factors Furtherstudies will be addressed with a prospective massive scalepopulation study to validate this assumption
In conclusion CX3CR1 genotype could be considered as anew marker to stratify the population according to fatal AMI
BioMed Research International 9
risk Moreover CX3CR1 is likely to amplify the Th1 immuneresponse directly related to plaque vulnerability irrespec-tively of the causal agents (ie ox-LDL or Chlamydia) thusstanding out as a potential target in fatal AMI prevention
References
[1] A I Gotlieb ldquoAtherosclerosis and acute coronary syndromesrdquoCardiovascular Pathology vol 14 no 4 pp 181ndash184 2005
[2] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[3] P Fraticelli M Sironi G Bianchi et al ldquoFractalkine (CX3CL1)as an amplification circuit of polarized Th1 responsesrdquo Journalof Clinical Investigation vol 107 no 9 pp 1173ndash1181 2001
[4] R Bonecchi G Bianchi P P Bordignon et al ldquoDifferentialexpression of chemokine receptors and chemotactic respon-siveness of type 1 T helper cells (Th1s) and Th2srdquo Journal ofExperimental Medicine vol 187 no 1 pp 129ndash134 1998
[5] J F Bazan K B Bacon G Hardiman et al ldquoA new class ofmembrane-bound chemokine with a CX3C motifrdquo Nature vol385 no 6617 pp 640ndash642 1997
[6] C Murdoch and A Finn ldquoChemokine receptors and their rolein vascular biologyrdquo Journal of Vascular Research vol 37 no 1pp 1ndash7 2000
[7] C Murdoch and A Finn ldquoChemokine receptors and their rolein inflammation and infectious diseasesrdquo Blood vol 95 no 10pp 3032ndash3043 2000
[8] C Combadiere K Salzwedel E D Smith H L Tiffany E ABerger and PMMurphy ldquoIdentification of CX3CR1 A chemo-tactic receptor for the human CX3C chemokine fractalkineand a fusion coreceptor for HIV-1rdquo The Journal of BiologicalChemistry vol 273 no 37 pp 23799ndash23804 1998
[9] G A Chapman K E Moores J Gohil et al ldquoThe role offractalkine in the recruitment of monocytes to the endothe-liumrdquo European Journal of Pharmacology vol 392 no 3 pp189ndash195 2000
[10] T Kasama K Wakabayashi M Sato R Takahashi and TIsozaki ldquoRelevance of the CX3CL1fractalkine-CX3CR1 path-way in vasculitis and vasculopathyrdquo Translational Research vol155 no 1 pp 20ndash26 2010
[11] M Garcıa-Alvarez J Berenguer M Guzman-Fulgencio et alldquoHigh plasma fractalkine (CX3CL1) levels are associated withsevere liver disease inHIVHCVco-infected patients withHCVgenotype 1rdquo Cytokine vol 54 no 3 pp 244ndash248 2011
[12] P Lesnik C A Haskell and I F Charo ldquoDecreased atheroscle-rosis in CX3CR1-- mice reveals a role for fractalkine inatherogenesisrdquo Journal of Clinical Investigation vol 111 no 3pp 333ndash340 2003
[13] M Stolla J Pelisek M-L von Bruhl A Schafer V Barockeand P Heider ldquoFractalkine is expressed in early and advancedatherosclerotic lesions and supports monocyte recruitment viaCX3CR1rdquo PLoS ONE vol 7 no 8 Article ID e43572 2012
[14] J K Damas A Boullier T Waelighre et al ldquoExpression offractalkine (CX3CL1) and its receptor CX3CR1 is elevated incoronary artery disease and is reduced during statin therapyrdquoArteriosclerosis Thrombosis and Vascular Biology vol 25 no12 pp 2567ndash2572 2005
[15] A M Fong L A Robinson D A Steeber et al ldquoFractalkineand CX3CR1 mediate a novel mechanism of leukocyte capturefirm adhesion and activation under physiologic flowrdquo Journalof Experimental Medicine vol 188 no 8 pp 1413ndash1419 1998
[16] D Moatti S Faure F Fumeron et al ldquoPolymorphism in thefractalkine receptor CX3CR1 as a genetic risk factor for coro-nary artery diseaserdquo Blood vol 97 no 7 pp 1925ndash1928 2001
[17] N Singh N Sinha S Kumar C M Pandey and S AgrawalldquoPolymorphism in chemokine receptor genes and risk of acutemyocardial infarction in North Indian populationrdquo MolecularBiology Reports vol 39 no 3 pp 2753ndash2759 2012
[18] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[19] G K Hansson and A Hermansson ldquoThe immune system inatherosclerosisrdquoNature Immunology vol 12 no 3 pp 204ndash2122011
[20] H Umehara E Bloom T Okazaki N Domae and T ImaildquoFractalkine and vascular injuryrdquoTrends in Immunology vol 22no 11 pp 602ndash607 2001
[21] H Umehara S Goda T Imai et al ldquoFractalkine a CX3C-chemokine functions predominantly as an adhesion moleculeinmonocytic cell line THP-1rdquo Immunology andCell Biology vol79 no 3 pp 298ndash302 2001
[22] L Lasagni M Francalanci F Annunziato et al ldquoAn alter-natively spliced variant of CXCR3 mediates the inhibition ofendothelial cell growth induced by IP-10 Mig and I-TACand acts as functional receptor for platelet factor 4rdquo Journal ofExperimental Medicine vol 197 no 11 pp 1537ndash1549 2003
[23] S Jung J Aliberti P Graemmel et al ldquoAnalysis of fractalkinereceptor CX3CR1 function by targeted deletion and greenfluorescent protein reporter gene insertionrdquo Molecular andCellular Biology vol 20 no 11 pp 4106ndash4114 2000
[24] D H McDermott J P J Halcox W H Schenke et alldquoAssociation between polymorphism in the chemokine receptorCX3CR1 and coronary vascular endothelial dysfunction andatherosclerosisrdquoCirculation Research vol 89 no 5 pp 401ndash4072001
[25] H Umehara and T Imai ldquoRole of fractalkine in leukocyteadhesion and migration and in vascular injuryrdquoDrug News andPerspectives vol 14 no 8 pp 460ndash464 2001
[26] H Fujimoto Y Tanaka Z-J Liu et al ldquoDown-regulation of 1205726integrin an anti-oncogene product by functional cooperationof H-Ras and c-Mycrdquo Genes to Cells vol 6 no 4 pp 337ndash3432001
[27] M Kimoli S Miyakis P Georgakopoulos E Noefytou A DAchimastos and D A Spandidos ldquoPolymorphisms of frac-talkine receptorCX3CR1 gene in patientswith symptomatic andasymptomatic carotid artery stenosisrdquo Journal of Atherosclerosisand Thrombosis vol 16 no 5 pp 604ndash610 2009
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

4 BioMed Research International
signal amplification biotin system (NEN Life Science Prod-ucts Boston MA USA) Fluorescence was obtained with astreptavidin-Texas Red fluorescent conjugate Control sec-tions were incubated with amixture of irrelevantmonoclonalreagents having a similar isotype Images were acquired bymeans of Noran confocal microscope at 60X14 NA immer-sion oil lens Three D stacks were acquired at a resolution of01 micron in119883- 119884- and 119885-axis
26 DNA Extraction DNA was extracted from formalinfixed and paraffin embedded heart of the subjects describedabove Paraffin was removed with xylene for 5min at roomtemperature Samples were centrifuged at full speed for 5minat RT Supernatant was removed and 12mL of 100 ethanolwas added to remove residual xyleneTheDNAwas extractedwith the QIAamp DNA kit (Qiagen GmbH Germany) andresuspended in 50 120583L of Buffer AE
27 Screening for Polymorphisms The DNA quality wascontrolled by a genomic polymerase reaction assay (PCR)using the primer set for BAK gene The following two poly-morphisms have been analyzed I249 a guanidine to adeninesubstitution at nucleotide 745 of the open reading framechanging valine at position 249 to isoleucine and M280 acytosine to thymidine substitution at nucleotide 839 changinga threonine at position 280The PCR product was analyzed in2 agarose gel stained with ethidium bromide CX3CR1 geneT280M and V249I mutations were identified after amplifica-tion of 311 base pairs (bp) (primers forward 51015840 AGA ATCATC CAG ACG CTG TTT TCC 31015840 reverse 51015840 CAG AGGACAGCCAGGCATTTCC31015840)TheT280MandV429Iweredetected on the same amplified fragment Amplification reac-tions were performed using 35 cycles of 95∘C 69∘C and 72∘Cfor 30 seconds each preceded by a single cycle of 95∘C for 3minutes and followed by a single cycle of 72∘C for 10 minutesIn order to type the alleles at codons 249 and 280 5 120583L ofPCR reactionwas digested respectively with Acl I (NewEng-land Biolabs BeverlyMA) or BsbmB1 (New England BiolabsBeverlyMA) in 20 120583L of reaction as previously described [11]In order to evaluate the efficiency of endonucleases enzymescontrol DNA with Acl I and Bst 4CI restriction sites wasused and DNA was loaded at different times on agarose gelThe genotypes were analysed and determined by analyticalelectrophoresis of each digestion on a 2 agarose gel
28 Statistical Analysis Statistical analysis of the data wasperformed with SPSS for Windows (version 110 SPSSChicago IL) Unpaired 119905-test was utilized to assess intergroupdifferences for continuous variables The 1198832 test was used toestablish differences in the distribution between categoricalvariables The statistical significance of different polymor-phisms present in the single groups was identified by Fisherrsquosexact test A 119875 value of lt005 was considered statisticallysignificant
Using logistic regression analysis (SPSS 130) the associ-ation of each polymorphism with the cardiovascular events(fatal AMI survivors and control group) was adjusted forage gender smoking cigarette hypertension diabetes mel-litus and hyperlipidemia
0 10 20 30 40
AMI
CTRL
T cellsMacrophages
(a)
0 20 40 60 80 100
AMI
CTRL
CX3CR1
(b)
Figure 1 Inflammatory cells characterization (a) shows the per-centages of inflammatory cells T lymphocytes (dotted bar) andmacrophages (dashed bar) in AMI and control group (b) Shows thepercentages of T cells CX3CR1 positive in AMI and control group
3 Results
31 Coronary Plaques Inflammation The examination of thewhole coronary tree of the AMI group demonstrated thepresence ofmultiple complicated atherosclerotic plaqueswitha thin fibrous cap and a high inflammatory infiltrate more-over in the coronary branch supplying the infarct area (IRA)we found a disruptedthrombotic plaque (culprit plaque)Conversely the coronary trees of the control group (NCC)showed atherosclerotic lesions with a thick fibrous cap and ascanty inflammatory infiltrate No plaque disruption or ero-sion or thrombosis has been observed Clinical autoptic andsurgical patient characteristics are showed in Table 1
Cell subpopulations were characterized by immunohis-tochemical studies using specific antibodies for lymphocytes(CD3 T cells) macrophages (CD68) and smooth musclecells (120572-actin) A quantitative analysis demonstrated a signif-icant (119875 lt 001) increase in the inflammatory cells per area(CD3 and CD68 positive) in AMI plaques (514 plusmn 25) ascompared with the plaques of the NCC group (224 plusmn 19)T lymphocytes represented the 185plusmn23 of the plaque cellsin AMI and the 64 plusmn 18 of cells in the NCC whereasmacrophages were 329 plusmn 32 in the AMI and 160 plusmn 18 intheNCC (Figure 1(a))Moreover the expression of IFN-120574wasassessed in culprit lesions by immunofluorescence staining(coronary artery fromAMI group) with confocal microscopy(Figure 3)
BioMed Research International 5
32 Fractalkine and CX3CR1 Expression The Fractalkineexpression was evaluated by immunohistochemistry in orderto compare T cell population recruitment and chemokinerelease
Figure 2(b) shows the expression of CD3 fractalkinereceptor CX3CR1 Figure 2(c) in T cells infiltrating the culpritlesion In AMI plaques immunostaining for fractalkine wasstrongly positive (Figure 2(d)) The immunofluorescence inFigure 3 demonstrated the coexpression of these three pro-teins in the same cells of AMI culprit plaque confirming theexistence of a T cell chronic active inflammation Moreoverthese data demonstrated theTh1 mediated immune response(IFN-120574 production) involved in plaque inflammation anddestabilization correlated with the presence of Th1 polarizedT cells (CXCR1 expressing cells) recruited in the plaque by theinteraction of fractalkine and the CX3CR1 receptor on the Tcell membrane
The immunohistochemical studies demonstrated thatendothelial cells in plaques of AMI patients gave rise to adiffuse positive reaction for fractalkine Smooth muscle cellswere focally positive while lymphocytes and macrophageswere not Conversely in the plaques of NCC group all thecell types were almost negative for fractalkine (Figure 2)
The fractalkine receptor (CX3CR1) was strongly anddiffusely expressed in the cell membrane in T lympho-cytes of AMI plaques (Figure 2(c)) as compared to controlMacrophages and smoothmuscle cells gave rise to a weak andscattered positive reaction The reaction was almost negativein the plaques of NCC group only a weak positive stainingwas present in smooth muscle cells and macrophages in theplaque (Figure 2(g))
The quantitative study revealed that 83 of T cells in theAMI plaques were CX3CR1 positive (Figure 1(b)) indicating aTh1 subset polarized subpopulation Furthermore a confocalobservation of IFN-120574 expression confirmed that T lympho-cytes expressed IFN-120574 (Figure 3)
In the coronary plaques from control group T lympho-cytes showed a lower level of CX3CR1 positivity (18 of Tlymphocytes were positive) (Figure 1(b)) in this group thereaction for IFN-120574 was completely negative (not shown)
33 CX3CR1 Genotype Correlates with the Th1 Cells Recruit-ment It has been previously demonstrated that CX3CR1genotypes influence the fractalkine receptor binding affinityand therefore Th1 lymphocytes recruitment In order tocorrelate the presence of activated Th1 lymphocytes withCX3CR1 genotype patientswere genotyped for theV249I andT280Mpolymorphisms of CXCR1 gene DNA extracted frommyocardial formalin fixed and paraffin embedded sectionswas analyzed by polymerase chain reaction The genotypewas determined on the amplicon of 311 bp after digestionwithendonucleases specific for each polymorphism The analysisof CX3CR1 V249I and T280M polymorphisms demonstratedthat 13 out of 25 patients who died of infarction (52) werehomozygous for the V249 allele and 21 out of 25 (84) werehomozygous for the T280 allele (Table 2) Moreover the 40ofAMI patients (1025) were heterozygous for theV249 allelebut all of these were homozygous for T280 allele as shown inTable 2 On the other hand only 8 (225) of AMI patients
displayed I249 allele in homozygosis and T280 in homo-(84) or heterozygosis (16) Notably the two AMI patientswho presented the variant haplotypes 249II and 280TMhad reduced T infiltrate and low IFN-120574 production in theplaque but a large number of B cells In Table 2 the correlationbetween the genotype and the inflammatory infiltrate burdenis reported The higher presence of 249VV (52) in AMIgroup as compared to controls is correlated with the presenceof a consistent T cell infiltrate expressing CX3CR1 (119875 lt 001)confirming the Th1 polarized subpopulation recruitment inthe plaque
4 Correlation among AMI AMI Survivorsand NCC Genotype
The genotype analysis has been extended to a cohort ofindividuals survived at a first myocardial infarction (119899 = 16)in order to compare the presence of the allele variant with theoccurrence and the outcome of the acute event
We found that the 52 of AMI patients (1325) displayedthe V249 allele in homozygosis as compared with the 6of the AMI survivors (116) and the 9 of controls (222)(Table 3)
The multivariate analysis of each V249I polymorphismadjusted for clinical data in the three study groups showedthat the VV249 haplotype was significantly associated onlywith the fatal AMI (119875 = 0001) but not with all the major riskfactors
On the other hand the I249 variant allele was expressedin homozygosis only in the 8 of the AMI patients (225)(Table 3) as compared with the 36 of controls (822) andthe 31 of AMI survivors (516)
The analysis of T280Mpolymorphism displayed the pres-ence of the M280 variant allele in homozygosis in the 4 ofcontrols (122) as comparedwithAMI and survivors patientswhich showed no presence of this allele in homozygosis Thepresence ofM280 allele in homozygosiswas always associatedwith the I249 allele
In summary the significant higher presence of the variantallele I249 in homo- and heterozygosis found in controls(91) and in AMI survivors (94) with respect to thepatients died of AMI (48) showed the relevance of thispolymorphism both in the onset and outcome of acutemyocardial infarction confirming the correlation betweenCX3CR1 genotype and prognosis of the acute event
5 Discussion
Epidemiological and clinical studies have shown that theCX3CR1 receptor polymorphisms are linked with the risk ofcoronary artery diseases [14 15]
In particular the presence of CX3CR1 V249 and T280single nucleotide polymorphisms codify for a fractalkinereceptor that is overexpressed by activated inflammatory cellsand with higher binding affinity for fractalkine its naturalligand [16 20]
The genotyping analysis of the subjects enrolled in thepresent study demonstrated for the first time a direct corre-lation between CX3CR1 V249I and T280M polymorphisms
6 BioMed Research International
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
Figure 2 Coronary plaques morphology and inflammatory infiltrate characterization in AMI group (a)ndash(d) and control group (e)ndash(h) (a)shows an haematoxylin eosin stain of a plaque from AMI group showing a complicated plaque with a large necrotic core a thin cap and ahigh inflammatory infiltrate with a high percentage of lymphocytes ((b) macrophages CD68 positive revealed by alkaline phosphataseanti-alkaline phosphatase red reaction and T lymphocytes CD3 positive DAB detected streptavidinbiotin immunoperoxidase brown reaction)(c) shows the immunostaining against the fractalkine receptor CX3CR1 that gave rise to a strong diffuse positive reaction in the T cells of AMIgroup (d) (in the insert a particular corresponding to the area indicated by the arrow magnification 40x) demonstrate a positive reaction forfractalkine in the endothelial cells (e) shows an haematoxylin eosin of a coronary from a patient died by bronchopneumonia without clinicalcardiac historyThe plaque shows a thick fibrotic cap and the inflammatory infiltrate is scanty and predominantly constituted bymacrophages((f) macrophages CD68 positive revealed by alkaline phosphataseanti-alkaline phosphatase red reaction and T lymphocytes CD3 positiveDAB dectected streptavidinbiotin immunoperoxidase brown reaction) The immunostaining for the fractalkine receptor CX3CR1 gave riseto a weak positive reaction in the smooth muscle cells and macrophages ((g) 10x magnification) The reaction for fractalkine was negative inthe control group (h) (in the insert a particular corresponding to the area indicated by the arrow magnification 40x)
BioMed Research International 7
(b)
(c)
(d)(a)
Figure 3 Confocal microscopy examination of triple stain in a culprit lesion (coronary artery from AMI group) (a) (magnification 2000x)shows a 2D reconstruction triple stain for T cells CD3 (blue) fractalkine receptor CX3CR1 (green) and IFN-gamma (red) yellow lightblue and white areas were due to multiple positivity (b) CD3 immunostaining revealed by coumarin conjugated streptavidin (c) CX3CR1immunostaining revealed by FITC conjugated streptavidin (d) IFN-gamma immunostaining revealed by Texas Red conjugated streptavidin
Table 2 Correlation between inflammatory infiltrate and CX3CR1 polymorphismsect
AMI NCCVV249
1325 (52)lowastVI249
1025 (40)II249225 (8)
VV249222 (9)
VI2491222 (55)
II249822 (36)
CD3Negweak 0 0 1 1 7 7Pos moderate 0 1 1 1 5 0Strong 13 9 0 0 0 0
CD20Negweak 12 9 0 2 12 7Pos moderate 1 1 0 0 0 0Strong 0 0 2 0 0 0
CXCL1Negweak 0 0 0 1 12 7Pos moderate 1 1 2 1 0 0Strong 12 9 0 0 0 0
CXCR1Negweak 0 0 1 1 7 7Pos moderate 0 1 1 0 5 0Strong 13 9 0 1 0 0
sectThe table shows the IHC results in the coronary plaque of AMI and control patients (NCC) correlated to the presence of CX3CR1 V249I polymorphism inthe same groups lowastIn parentheses the percentage of patients was reported
and the occurrence of acute fatal myocardial infarction Astriking link between genotype and prognosis of the acuteevent was suggested by the observation of AMI survivorsgenotypes Notably the in situ CX3CR1 high expression in
AMI patients correlates with the presence of V249 polymor-phism in homo- or heterozygosis Conversely the genotypeanalysis of controls (with no CVD history) demonstrated thepresence of I249 polymorphism in homozygosis
8 BioMed Research International
Table 3 Analysis of CX3CR1 polymorphisms in patients andcontrol groups
AMI(119899 = 25)
SVR(119899 = 16)
NCC(119899 = 22)
V249IVV 13 (52) 1 (6) 2 (9)VI 10 (40) 10 (63) 12 (55)II 2 (8) 5 (31) 8 (36)
119875 = 0003 119875 = 0003 119875 = 0006
T280MTT 21 (84) 9 (56) 14 (64)TM 4 (16) 7 (44) 7 (32)MM 0 0 1 (4)
119875 = 0001 119875 = 0002 119875 = 0001
Data are absolute numbers (percentage)Abbreviations AMI acute myocardial infarction SVR patients survived toa first AMI NCC subjects dead for noncardiac causesThe statistical significance of different polymorphisms present in the singlegroups was identified by Fisherrsquos exact test
Indeed CX3CR1 V249T280 polymorphisms in homozy-gosis or heterozygosis have been demonstrated in 92 of theAMI patients analyzed (mean age 70 years old) In particular52 of the AMI patients examined were homozygous forCX3CR1 V249 whereas the analysis of the genotype of thecontrol subjects (mean age 737 years old) demonstrated thepresence of CX3CR1 V249 polymorphism in homozygosisonly in the 9 of cases The findings of the high percentageof II249 (36) and MM280 (4) in subjects died of nocardiac causes suggest a possible link between CX3CR1 poly-morphism T cell recruitment and acute eventMoreover thegenotype observations on survivors group suggest that thepresence of I249 allele is relevant not only for the occurrencebut also in the outcome of the acute event
There is evidence of the influence of CX3CR1 variableexpression and function on T cells recruitment efficiency[14 21 22]
Studies on CX3CR1 null mice crossed into apoE minusminusbackground [12] demonstrated that although CX3CL1 wasstrongly expressed in smooth muscle cells in the lesion thelack of the CX3CR1 receptor was related to a significantreduction in macrophages and T cells recruitment within thevessel wall associated with a reduction of atherosclerosis
In present work we also show a close association betweenCX3CR1 genotypes and coronary plaques T cell inflam-mation that is a relevant character of vulnerable plaquesaccording to data previously published [1 2]
Indeed coronary plaques of patients with CX3CR1 I249allele displayed a weaker T cell inflammation as compared toindividuals homozygous for the CX3CR1 V249 allele
In particular we show that CX3CR1 is highly expressedby the majority of T cells infiltrating IRA plaques of 22 out of25 AMI patients
It is worth noting that the two patients showing a lowexpression of CX3CR1 were CX3CR1 I249 homozygou andtheir plaques were infiltrated by B lymphocytes suggestinga different pathogenesis for AMI
Conversely immunostaining for CX3CR1 was negative orfaint positive in plaques of controls where the T lymphocytesinfiltrate was lower as compared with AMI patients
Therefore it can be assumed that the high expression ofCX3CR1 together with the in situ expression of fractalkine(CX3CL1) correlates with the increased recruitment of Tlymphocytes deeply infiltrating in the plaques of the AMIpatients
The special feature of fractalkine among other mem-bers of the chemokine family is due to the fact that it isexpressed both as soluble and membrane-bound form onthe surface of inflamed endothelium Interestingly whereassoluble fractalkine (CX3CL1) was reported to recruit lym-phocytes andmonocytes immobilized forms ofCX3CL1 havebeen shown to directly mediate the rapid capture and firmadhesion of leukocytes expressing its receptor CX3CR1 underphysiological flow conditions [23] The direct binding of thechemokine to CX3CR1 does not require the upregulationand activation of integrins suggesting that fractalkine andCX3CR1 mediate a novel pathway for leukocytes traffick-ing [24] In addition to the intrinsic adhesive functionof fractalkine this chemokine can also transduce signalsthrough G proteins that enhance the avidity of integrinbinding to its ligands for leukocytes recruitment [25 26]
The coexpression of CD3 IFN-gamma and CX3CR1 onT cell population found inAMI plaques compared to controlsdemonstrates the in situ activation of inflammatory cellspointing out the probable involvement of a recent immuneTh1 response in plaque destabilization and ruptureMoreoverthe data obtained suggest that the susceptibility to vascularinflammation is correlated with the amplified recruitment ofTh1 polarized cells expressing the high or low affinity CX3CR1receptor The findings revealing CX3CR1 expression by 80of T cell population along with the presence of fractalkinein IRA plaques suggest that these two events are both likelyto play a major role in determining plaque vulnerability byorchestratingTh1 cells recruitment
In agreement with previous clinical and epidemiologicalstudies our data demonstrate a close association betweenV249I and T280M polymorphisms coronary plaque vul-nerability and AMI confirming that the subjects with I249allele display a low level of T cell inflammation and areduced risk of developing vulnerable plaques and they have adecreased incidence of acute events (probably due to a lowerCX3CR1 binding affinity) [27] The comparative analysis ofthe different CXCR3 polymorphisms and the inflammatoryinfiltrate shows a significant difference between fatal AMIand NCC A study limitation is the lacking in the compar-ative analysis of the coronary surgical samples from AMIsurvivors These patients in fact underwent a ventricularrestoration for a previous nonfatal AMI event Despite theabove limitations our study provides lines of evidence thatthe I249 allele could be strongly involved in the protectionfrom fatal AMI with these association being independent ofthe major ldquoconventionalrdquo cardiovascular risk factors Furtherstudies will be addressed with a prospective massive scalepopulation study to validate this assumption
In conclusion CX3CR1 genotype could be considered as anew marker to stratify the population according to fatal AMI
BioMed Research International 9
risk Moreover CX3CR1 is likely to amplify the Th1 immuneresponse directly related to plaque vulnerability irrespec-tively of the causal agents (ie ox-LDL or Chlamydia) thusstanding out as a potential target in fatal AMI prevention
References
[1] A I Gotlieb ldquoAtherosclerosis and acute coronary syndromesrdquoCardiovascular Pathology vol 14 no 4 pp 181ndash184 2005
[2] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[3] P Fraticelli M Sironi G Bianchi et al ldquoFractalkine (CX3CL1)as an amplification circuit of polarized Th1 responsesrdquo Journalof Clinical Investigation vol 107 no 9 pp 1173ndash1181 2001
[4] R Bonecchi G Bianchi P P Bordignon et al ldquoDifferentialexpression of chemokine receptors and chemotactic respon-siveness of type 1 T helper cells (Th1s) and Th2srdquo Journal ofExperimental Medicine vol 187 no 1 pp 129ndash134 1998
[5] J F Bazan K B Bacon G Hardiman et al ldquoA new class ofmembrane-bound chemokine with a CX3C motifrdquo Nature vol385 no 6617 pp 640ndash642 1997
[6] C Murdoch and A Finn ldquoChemokine receptors and their rolein vascular biologyrdquo Journal of Vascular Research vol 37 no 1pp 1ndash7 2000
[7] C Murdoch and A Finn ldquoChemokine receptors and their rolein inflammation and infectious diseasesrdquo Blood vol 95 no 10pp 3032ndash3043 2000
[8] C Combadiere K Salzwedel E D Smith H L Tiffany E ABerger and PMMurphy ldquoIdentification of CX3CR1 A chemo-tactic receptor for the human CX3C chemokine fractalkineand a fusion coreceptor for HIV-1rdquo The Journal of BiologicalChemistry vol 273 no 37 pp 23799ndash23804 1998
[9] G A Chapman K E Moores J Gohil et al ldquoThe role offractalkine in the recruitment of monocytes to the endothe-liumrdquo European Journal of Pharmacology vol 392 no 3 pp189ndash195 2000
[10] T Kasama K Wakabayashi M Sato R Takahashi and TIsozaki ldquoRelevance of the CX3CL1fractalkine-CX3CR1 path-way in vasculitis and vasculopathyrdquo Translational Research vol155 no 1 pp 20ndash26 2010
[11] M Garcıa-Alvarez J Berenguer M Guzman-Fulgencio et alldquoHigh plasma fractalkine (CX3CL1) levels are associated withsevere liver disease inHIVHCVco-infected patients withHCVgenotype 1rdquo Cytokine vol 54 no 3 pp 244ndash248 2011
[12] P Lesnik C A Haskell and I F Charo ldquoDecreased atheroscle-rosis in CX3CR1-- mice reveals a role for fractalkine inatherogenesisrdquo Journal of Clinical Investigation vol 111 no 3pp 333ndash340 2003
[13] M Stolla J Pelisek M-L von Bruhl A Schafer V Barockeand P Heider ldquoFractalkine is expressed in early and advancedatherosclerotic lesions and supports monocyte recruitment viaCX3CR1rdquo PLoS ONE vol 7 no 8 Article ID e43572 2012
[14] J K Damas A Boullier T Waelighre et al ldquoExpression offractalkine (CX3CL1) and its receptor CX3CR1 is elevated incoronary artery disease and is reduced during statin therapyrdquoArteriosclerosis Thrombosis and Vascular Biology vol 25 no12 pp 2567ndash2572 2005
[15] A M Fong L A Robinson D A Steeber et al ldquoFractalkineand CX3CR1 mediate a novel mechanism of leukocyte capturefirm adhesion and activation under physiologic flowrdquo Journalof Experimental Medicine vol 188 no 8 pp 1413ndash1419 1998
[16] D Moatti S Faure F Fumeron et al ldquoPolymorphism in thefractalkine receptor CX3CR1 as a genetic risk factor for coro-nary artery diseaserdquo Blood vol 97 no 7 pp 1925ndash1928 2001
[17] N Singh N Sinha S Kumar C M Pandey and S AgrawalldquoPolymorphism in chemokine receptor genes and risk of acutemyocardial infarction in North Indian populationrdquo MolecularBiology Reports vol 39 no 3 pp 2753ndash2759 2012
[18] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[19] G K Hansson and A Hermansson ldquoThe immune system inatherosclerosisrdquoNature Immunology vol 12 no 3 pp 204ndash2122011
[20] H Umehara E Bloom T Okazaki N Domae and T ImaildquoFractalkine and vascular injuryrdquoTrends in Immunology vol 22no 11 pp 602ndash607 2001
[21] H Umehara S Goda T Imai et al ldquoFractalkine a CX3C-chemokine functions predominantly as an adhesion moleculeinmonocytic cell line THP-1rdquo Immunology andCell Biology vol79 no 3 pp 298ndash302 2001
[22] L Lasagni M Francalanci F Annunziato et al ldquoAn alter-natively spliced variant of CXCR3 mediates the inhibition ofendothelial cell growth induced by IP-10 Mig and I-TACand acts as functional receptor for platelet factor 4rdquo Journal ofExperimental Medicine vol 197 no 11 pp 1537ndash1549 2003
[23] S Jung J Aliberti P Graemmel et al ldquoAnalysis of fractalkinereceptor CX3CR1 function by targeted deletion and greenfluorescent protein reporter gene insertionrdquo Molecular andCellular Biology vol 20 no 11 pp 4106ndash4114 2000
[24] D H McDermott J P J Halcox W H Schenke et alldquoAssociation between polymorphism in the chemokine receptorCX3CR1 and coronary vascular endothelial dysfunction andatherosclerosisrdquoCirculation Research vol 89 no 5 pp 401ndash4072001
[25] H Umehara and T Imai ldquoRole of fractalkine in leukocyteadhesion and migration and in vascular injuryrdquoDrug News andPerspectives vol 14 no 8 pp 460ndash464 2001
[26] H Fujimoto Y Tanaka Z-J Liu et al ldquoDown-regulation of 1205726integrin an anti-oncogene product by functional cooperationof H-Ras and c-Mycrdquo Genes to Cells vol 6 no 4 pp 337ndash3432001
[27] M Kimoli S Miyakis P Georgakopoulos E Noefytou A DAchimastos and D A Spandidos ldquoPolymorphisms of frac-talkine receptorCX3CR1 gene in patientswith symptomatic andasymptomatic carotid artery stenosisrdquo Journal of Atherosclerosisand Thrombosis vol 16 no 5 pp 604ndash610 2009
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 5
32 Fractalkine and CX3CR1 Expression The Fractalkineexpression was evaluated by immunohistochemistry in orderto compare T cell population recruitment and chemokinerelease
Figure 2(b) shows the expression of CD3 fractalkinereceptor CX3CR1 Figure 2(c) in T cells infiltrating the culpritlesion In AMI plaques immunostaining for fractalkine wasstrongly positive (Figure 2(d)) The immunofluorescence inFigure 3 demonstrated the coexpression of these three pro-teins in the same cells of AMI culprit plaque confirming theexistence of a T cell chronic active inflammation Moreoverthese data demonstrated theTh1 mediated immune response(IFN-120574 production) involved in plaque inflammation anddestabilization correlated with the presence of Th1 polarizedT cells (CXCR1 expressing cells) recruited in the plaque by theinteraction of fractalkine and the CX3CR1 receptor on the Tcell membrane
The immunohistochemical studies demonstrated thatendothelial cells in plaques of AMI patients gave rise to adiffuse positive reaction for fractalkine Smooth muscle cellswere focally positive while lymphocytes and macrophageswere not Conversely in the plaques of NCC group all thecell types were almost negative for fractalkine (Figure 2)
The fractalkine receptor (CX3CR1) was strongly anddiffusely expressed in the cell membrane in T lympho-cytes of AMI plaques (Figure 2(c)) as compared to controlMacrophages and smoothmuscle cells gave rise to a weak andscattered positive reaction The reaction was almost negativein the plaques of NCC group only a weak positive stainingwas present in smooth muscle cells and macrophages in theplaque (Figure 2(g))
The quantitative study revealed that 83 of T cells in theAMI plaques were CX3CR1 positive (Figure 1(b)) indicating aTh1 subset polarized subpopulation Furthermore a confocalobservation of IFN-120574 expression confirmed that T lympho-cytes expressed IFN-120574 (Figure 3)
In the coronary plaques from control group T lympho-cytes showed a lower level of CX3CR1 positivity (18 of Tlymphocytes were positive) (Figure 1(b)) in this group thereaction for IFN-120574 was completely negative (not shown)
33 CX3CR1 Genotype Correlates with the Th1 Cells Recruit-ment It has been previously demonstrated that CX3CR1genotypes influence the fractalkine receptor binding affinityand therefore Th1 lymphocytes recruitment In order tocorrelate the presence of activated Th1 lymphocytes withCX3CR1 genotype patientswere genotyped for theV249I andT280Mpolymorphisms of CXCR1 gene DNA extracted frommyocardial formalin fixed and paraffin embedded sectionswas analyzed by polymerase chain reaction The genotypewas determined on the amplicon of 311 bp after digestionwithendonucleases specific for each polymorphism The analysisof CX3CR1 V249I and T280M polymorphisms demonstratedthat 13 out of 25 patients who died of infarction (52) werehomozygous for the V249 allele and 21 out of 25 (84) werehomozygous for the T280 allele (Table 2) Moreover the 40ofAMI patients (1025) were heterozygous for theV249 allelebut all of these were homozygous for T280 allele as shown inTable 2 On the other hand only 8 (225) of AMI patients
displayed I249 allele in homozygosis and T280 in homo-(84) or heterozygosis (16) Notably the two AMI patientswho presented the variant haplotypes 249II and 280TMhad reduced T infiltrate and low IFN-120574 production in theplaque but a large number of B cells In Table 2 the correlationbetween the genotype and the inflammatory infiltrate burdenis reported The higher presence of 249VV (52) in AMIgroup as compared to controls is correlated with the presenceof a consistent T cell infiltrate expressing CX3CR1 (119875 lt 001)confirming the Th1 polarized subpopulation recruitment inthe plaque
4 Correlation among AMI AMI Survivorsand NCC Genotype
The genotype analysis has been extended to a cohort ofindividuals survived at a first myocardial infarction (119899 = 16)in order to compare the presence of the allele variant with theoccurrence and the outcome of the acute event
We found that the 52 of AMI patients (1325) displayedthe V249 allele in homozygosis as compared with the 6of the AMI survivors (116) and the 9 of controls (222)(Table 3)
The multivariate analysis of each V249I polymorphismadjusted for clinical data in the three study groups showedthat the VV249 haplotype was significantly associated onlywith the fatal AMI (119875 = 0001) but not with all the major riskfactors
On the other hand the I249 variant allele was expressedin homozygosis only in the 8 of the AMI patients (225)(Table 3) as compared with the 36 of controls (822) andthe 31 of AMI survivors (516)
The analysis of T280Mpolymorphism displayed the pres-ence of the M280 variant allele in homozygosis in the 4 ofcontrols (122) as comparedwithAMI and survivors patientswhich showed no presence of this allele in homozygosis Thepresence ofM280 allele in homozygosiswas always associatedwith the I249 allele
In summary the significant higher presence of the variantallele I249 in homo- and heterozygosis found in controls(91) and in AMI survivors (94) with respect to thepatients died of AMI (48) showed the relevance of thispolymorphism both in the onset and outcome of acutemyocardial infarction confirming the correlation betweenCX3CR1 genotype and prognosis of the acute event
5 Discussion
Epidemiological and clinical studies have shown that theCX3CR1 receptor polymorphisms are linked with the risk ofcoronary artery diseases [14 15]
In particular the presence of CX3CR1 V249 and T280single nucleotide polymorphisms codify for a fractalkinereceptor that is overexpressed by activated inflammatory cellsand with higher binding affinity for fractalkine its naturalligand [16 20]
The genotyping analysis of the subjects enrolled in thepresent study demonstrated for the first time a direct corre-lation between CX3CR1 V249I and T280M polymorphisms
6 BioMed Research International
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
Figure 2 Coronary plaques morphology and inflammatory infiltrate characterization in AMI group (a)ndash(d) and control group (e)ndash(h) (a)shows an haematoxylin eosin stain of a plaque from AMI group showing a complicated plaque with a large necrotic core a thin cap and ahigh inflammatory infiltrate with a high percentage of lymphocytes ((b) macrophages CD68 positive revealed by alkaline phosphataseanti-alkaline phosphatase red reaction and T lymphocytes CD3 positive DAB detected streptavidinbiotin immunoperoxidase brown reaction)(c) shows the immunostaining against the fractalkine receptor CX3CR1 that gave rise to a strong diffuse positive reaction in the T cells of AMIgroup (d) (in the insert a particular corresponding to the area indicated by the arrow magnification 40x) demonstrate a positive reaction forfractalkine in the endothelial cells (e) shows an haematoxylin eosin of a coronary from a patient died by bronchopneumonia without clinicalcardiac historyThe plaque shows a thick fibrotic cap and the inflammatory infiltrate is scanty and predominantly constituted bymacrophages((f) macrophages CD68 positive revealed by alkaline phosphataseanti-alkaline phosphatase red reaction and T lymphocytes CD3 positiveDAB dectected streptavidinbiotin immunoperoxidase brown reaction) The immunostaining for the fractalkine receptor CX3CR1 gave riseto a weak positive reaction in the smooth muscle cells and macrophages ((g) 10x magnification) The reaction for fractalkine was negative inthe control group (h) (in the insert a particular corresponding to the area indicated by the arrow magnification 40x)
BioMed Research International 7
(b)
(c)
(d)(a)
Figure 3 Confocal microscopy examination of triple stain in a culprit lesion (coronary artery from AMI group) (a) (magnification 2000x)shows a 2D reconstruction triple stain for T cells CD3 (blue) fractalkine receptor CX3CR1 (green) and IFN-gamma (red) yellow lightblue and white areas were due to multiple positivity (b) CD3 immunostaining revealed by coumarin conjugated streptavidin (c) CX3CR1immunostaining revealed by FITC conjugated streptavidin (d) IFN-gamma immunostaining revealed by Texas Red conjugated streptavidin
Table 2 Correlation between inflammatory infiltrate and CX3CR1 polymorphismsect
AMI NCCVV249
1325 (52)lowastVI249
1025 (40)II249225 (8)
VV249222 (9)
VI2491222 (55)
II249822 (36)
CD3Negweak 0 0 1 1 7 7Pos moderate 0 1 1 1 5 0Strong 13 9 0 0 0 0
CD20Negweak 12 9 0 2 12 7Pos moderate 1 1 0 0 0 0Strong 0 0 2 0 0 0
CXCL1Negweak 0 0 0 1 12 7Pos moderate 1 1 2 1 0 0Strong 12 9 0 0 0 0
CXCR1Negweak 0 0 1 1 7 7Pos moderate 0 1 1 0 5 0Strong 13 9 0 1 0 0
sectThe table shows the IHC results in the coronary plaque of AMI and control patients (NCC) correlated to the presence of CX3CR1 V249I polymorphism inthe same groups lowastIn parentheses the percentage of patients was reported
and the occurrence of acute fatal myocardial infarction Astriking link between genotype and prognosis of the acuteevent was suggested by the observation of AMI survivorsgenotypes Notably the in situ CX3CR1 high expression in
AMI patients correlates with the presence of V249 polymor-phism in homo- or heterozygosis Conversely the genotypeanalysis of controls (with no CVD history) demonstrated thepresence of I249 polymorphism in homozygosis
8 BioMed Research International
Table 3 Analysis of CX3CR1 polymorphisms in patients andcontrol groups
AMI(119899 = 25)
SVR(119899 = 16)
NCC(119899 = 22)
V249IVV 13 (52) 1 (6) 2 (9)VI 10 (40) 10 (63) 12 (55)II 2 (8) 5 (31) 8 (36)
119875 = 0003 119875 = 0003 119875 = 0006
T280MTT 21 (84) 9 (56) 14 (64)TM 4 (16) 7 (44) 7 (32)MM 0 0 1 (4)
119875 = 0001 119875 = 0002 119875 = 0001
Data are absolute numbers (percentage)Abbreviations AMI acute myocardial infarction SVR patients survived toa first AMI NCC subjects dead for noncardiac causesThe statistical significance of different polymorphisms present in the singlegroups was identified by Fisherrsquos exact test
Indeed CX3CR1 V249T280 polymorphisms in homozy-gosis or heterozygosis have been demonstrated in 92 of theAMI patients analyzed (mean age 70 years old) In particular52 of the AMI patients examined were homozygous forCX3CR1 V249 whereas the analysis of the genotype of thecontrol subjects (mean age 737 years old) demonstrated thepresence of CX3CR1 V249 polymorphism in homozygosisonly in the 9 of cases The findings of the high percentageof II249 (36) and MM280 (4) in subjects died of nocardiac causes suggest a possible link between CX3CR1 poly-morphism T cell recruitment and acute eventMoreover thegenotype observations on survivors group suggest that thepresence of I249 allele is relevant not only for the occurrencebut also in the outcome of the acute event
There is evidence of the influence of CX3CR1 variableexpression and function on T cells recruitment efficiency[14 21 22]
Studies on CX3CR1 null mice crossed into apoE minusminusbackground [12] demonstrated that although CX3CL1 wasstrongly expressed in smooth muscle cells in the lesion thelack of the CX3CR1 receptor was related to a significantreduction in macrophages and T cells recruitment within thevessel wall associated with a reduction of atherosclerosis
In present work we also show a close association betweenCX3CR1 genotypes and coronary plaques T cell inflam-mation that is a relevant character of vulnerable plaquesaccording to data previously published [1 2]
Indeed coronary plaques of patients with CX3CR1 I249allele displayed a weaker T cell inflammation as compared toindividuals homozygous for the CX3CR1 V249 allele
In particular we show that CX3CR1 is highly expressedby the majority of T cells infiltrating IRA plaques of 22 out of25 AMI patients
It is worth noting that the two patients showing a lowexpression of CX3CR1 were CX3CR1 I249 homozygou andtheir plaques were infiltrated by B lymphocytes suggestinga different pathogenesis for AMI
Conversely immunostaining for CX3CR1 was negative orfaint positive in plaques of controls where the T lymphocytesinfiltrate was lower as compared with AMI patients
Therefore it can be assumed that the high expression ofCX3CR1 together with the in situ expression of fractalkine(CX3CL1) correlates with the increased recruitment of Tlymphocytes deeply infiltrating in the plaques of the AMIpatients
The special feature of fractalkine among other mem-bers of the chemokine family is due to the fact that it isexpressed both as soluble and membrane-bound form onthe surface of inflamed endothelium Interestingly whereassoluble fractalkine (CX3CL1) was reported to recruit lym-phocytes andmonocytes immobilized forms ofCX3CL1 havebeen shown to directly mediate the rapid capture and firmadhesion of leukocytes expressing its receptor CX3CR1 underphysiological flow conditions [23] The direct binding of thechemokine to CX3CR1 does not require the upregulationand activation of integrins suggesting that fractalkine andCX3CR1 mediate a novel pathway for leukocytes traffick-ing [24] In addition to the intrinsic adhesive functionof fractalkine this chemokine can also transduce signalsthrough G proteins that enhance the avidity of integrinbinding to its ligands for leukocytes recruitment [25 26]
The coexpression of CD3 IFN-gamma and CX3CR1 onT cell population found inAMI plaques compared to controlsdemonstrates the in situ activation of inflammatory cellspointing out the probable involvement of a recent immuneTh1 response in plaque destabilization and ruptureMoreoverthe data obtained suggest that the susceptibility to vascularinflammation is correlated with the amplified recruitment ofTh1 polarized cells expressing the high or low affinity CX3CR1receptor The findings revealing CX3CR1 expression by 80of T cell population along with the presence of fractalkinein IRA plaques suggest that these two events are both likelyto play a major role in determining plaque vulnerability byorchestratingTh1 cells recruitment
In agreement with previous clinical and epidemiologicalstudies our data demonstrate a close association betweenV249I and T280M polymorphisms coronary plaque vul-nerability and AMI confirming that the subjects with I249allele display a low level of T cell inflammation and areduced risk of developing vulnerable plaques and they have adecreased incidence of acute events (probably due to a lowerCX3CR1 binding affinity) [27] The comparative analysis ofthe different CXCR3 polymorphisms and the inflammatoryinfiltrate shows a significant difference between fatal AMIand NCC A study limitation is the lacking in the compar-ative analysis of the coronary surgical samples from AMIsurvivors These patients in fact underwent a ventricularrestoration for a previous nonfatal AMI event Despite theabove limitations our study provides lines of evidence thatthe I249 allele could be strongly involved in the protectionfrom fatal AMI with these association being independent ofthe major ldquoconventionalrdquo cardiovascular risk factors Furtherstudies will be addressed with a prospective massive scalepopulation study to validate this assumption
In conclusion CX3CR1 genotype could be considered as anew marker to stratify the population according to fatal AMI
BioMed Research International 9
risk Moreover CX3CR1 is likely to amplify the Th1 immuneresponse directly related to plaque vulnerability irrespec-tively of the causal agents (ie ox-LDL or Chlamydia) thusstanding out as a potential target in fatal AMI prevention
References
[1] A I Gotlieb ldquoAtherosclerosis and acute coronary syndromesrdquoCardiovascular Pathology vol 14 no 4 pp 181ndash184 2005
[2] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[3] P Fraticelli M Sironi G Bianchi et al ldquoFractalkine (CX3CL1)as an amplification circuit of polarized Th1 responsesrdquo Journalof Clinical Investigation vol 107 no 9 pp 1173ndash1181 2001
[4] R Bonecchi G Bianchi P P Bordignon et al ldquoDifferentialexpression of chemokine receptors and chemotactic respon-siveness of type 1 T helper cells (Th1s) and Th2srdquo Journal ofExperimental Medicine vol 187 no 1 pp 129ndash134 1998
[5] J F Bazan K B Bacon G Hardiman et al ldquoA new class ofmembrane-bound chemokine with a CX3C motifrdquo Nature vol385 no 6617 pp 640ndash642 1997
[6] C Murdoch and A Finn ldquoChemokine receptors and their rolein vascular biologyrdquo Journal of Vascular Research vol 37 no 1pp 1ndash7 2000
[7] C Murdoch and A Finn ldquoChemokine receptors and their rolein inflammation and infectious diseasesrdquo Blood vol 95 no 10pp 3032ndash3043 2000
[8] C Combadiere K Salzwedel E D Smith H L Tiffany E ABerger and PMMurphy ldquoIdentification of CX3CR1 A chemo-tactic receptor for the human CX3C chemokine fractalkineand a fusion coreceptor for HIV-1rdquo The Journal of BiologicalChemistry vol 273 no 37 pp 23799ndash23804 1998
[9] G A Chapman K E Moores J Gohil et al ldquoThe role offractalkine in the recruitment of monocytes to the endothe-liumrdquo European Journal of Pharmacology vol 392 no 3 pp189ndash195 2000
[10] T Kasama K Wakabayashi M Sato R Takahashi and TIsozaki ldquoRelevance of the CX3CL1fractalkine-CX3CR1 path-way in vasculitis and vasculopathyrdquo Translational Research vol155 no 1 pp 20ndash26 2010
[11] M Garcıa-Alvarez J Berenguer M Guzman-Fulgencio et alldquoHigh plasma fractalkine (CX3CL1) levels are associated withsevere liver disease inHIVHCVco-infected patients withHCVgenotype 1rdquo Cytokine vol 54 no 3 pp 244ndash248 2011
[12] P Lesnik C A Haskell and I F Charo ldquoDecreased atheroscle-rosis in CX3CR1-- mice reveals a role for fractalkine inatherogenesisrdquo Journal of Clinical Investigation vol 111 no 3pp 333ndash340 2003
[13] M Stolla J Pelisek M-L von Bruhl A Schafer V Barockeand P Heider ldquoFractalkine is expressed in early and advancedatherosclerotic lesions and supports monocyte recruitment viaCX3CR1rdquo PLoS ONE vol 7 no 8 Article ID e43572 2012
[14] J K Damas A Boullier T Waelighre et al ldquoExpression offractalkine (CX3CL1) and its receptor CX3CR1 is elevated incoronary artery disease and is reduced during statin therapyrdquoArteriosclerosis Thrombosis and Vascular Biology vol 25 no12 pp 2567ndash2572 2005
[15] A M Fong L A Robinson D A Steeber et al ldquoFractalkineand CX3CR1 mediate a novel mechanism of leukocyte capturefirm adhesion and activation under physiologic flowrdquo Journalof Experimental Medicine vol 188 no 8 pp 1413ndash1419 1998
[16] D Moatti S Faure F Fumeron et al ldquoPolymorphism in thefractalkine receptor CX3CR1 as a genetic risk factor for coro-nary artery diseaserdquo Blood vol 97 no 7 pp 1925ndash1928 2001
[17] N Singh N Sinha S Kumar C M Pandey and S AgrawalldquoPolymorphism in chemokine receptor genes and risk of acutemyocardial infarction in North Indian populationrdquo MolecularBiology Reports vol 39 no 3 pp 2753ndash2759 2012
[18] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[19] G K Hansson and A Hermansson ldquoThe immune system inatherosclerosisrdquoNature Immunology vol 12 no 3 pp 204ndash2122011
[20] H Umehara E Bloom T Okazaki N Domae and T ImaildquoFractalkine and vascular injuryrdquoTrends in Immunology vol 22no 11 pp 602ndash607 2001
[21] H Umehara S Goda T Imai et al ldquoFractalkine a CX3C-chemokine functions predominantly as an adhesion moleculeinmonocytic cell line THP-1rdquo Immunology andCell Biology vol79 no 3 pp 298ndash302 2001
[22] L Lasagni M Francalanci F Annunziato et al ldquoAn alter-natively spliced variant of CXCR3 mediates the inhibition ofendothelial cell growth induced by IP-10 Mig and I-TACand acts as functional receptor for platelet factor 4rdquo Journal ofExperimental Medicine vol 197 no 11 pp 1537ndash1549 2003
[23] S Jung J Aliberti P Graemmel et al ldquoAnalysis of fractalkinereceptor CX3CR1 function by targeted deletion and greenfluorescent protein reporter gene insertionrdquo Molecular andCellular Biology vol 20 no 11 pp 4106ndash4114 2000
[24] D H McDermott J P J Halcox W H Schenke et alldquoAssociation between polymorphism in the chemokine receptorCX3CR1 and coronary vascular endothelial dysfunction andatherosclerosisrdquoCirculation Research vol 89 no 5 pp 401ndash4072001
[25] H Umehara and T Imai ldquoRole of fractalkine in leukocyteadhesion and migration and in vascular injuryrdquoDrug News andPerspectives vol 14 no 8 pp 460ndash464 2001
[26] H Fujimoto Y Tanaka Z-J Liu et al ldquoDown-regulation of 1205726integrin an anti-oncogene product by functional cooperationof H-Ras and c-Mycrdquo Genes to Cells vol 6 no 4 pp 337ndash3432001
[27] M Kimoli S Miyakis P Georgakopoulos E Noefytou A DAchimastos and D A Spandidos ldquoPolymorphisms of frac-talkine receptorCX3CR1 gene in patientswith symptomatic andasymptomatic carotid artery stenosisrdquo Journal of Atherosclerosisand Thrombosis vol 16 no 5 pp 604ndash610 2009
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
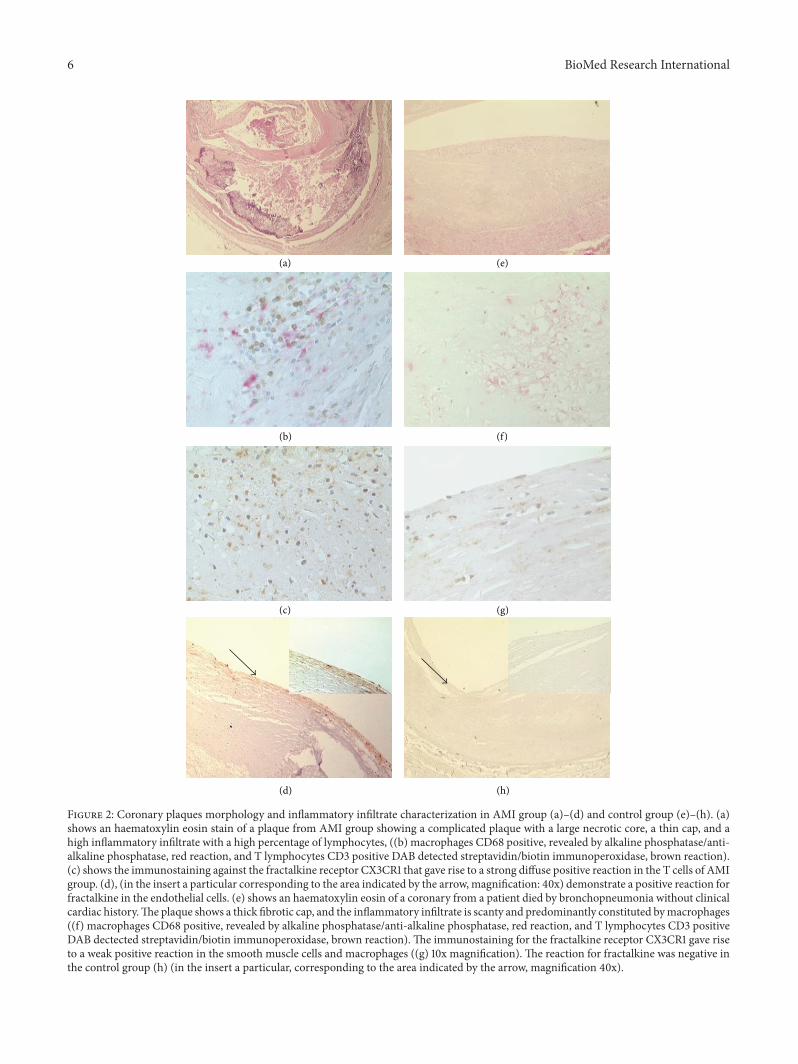
6 BioMed Research International
(a)
(b)
(c)
(d)
(e)
(f)
(g)
(h)
Figure 2 Coronary plaques morphology and inflammatory infiltrate characterization in AMI group (a)ndash(d) and control group (e)ndash(h) (a)shows an haematoxylin eosin stain of a plaque from AMI group showing a complicated plaque with a large necrotic core a thin cap and ahigh inflammatory infiltrate with a high percentage of lymphocytes ((b) macrophages CD68 positive revealed by alkaline phosphataseanti-alkaline phosphatase red reaction and T lymphocytes CD3 positive DAB detected streptavidinbiotin immunoperoxidase brown reaction)(c) shows the immunostaining against the fractalkine receptor CX3CR1 that gave rise to a strong diffuse positive reaction in the T cells of AMIgroup (d) (in the insert a particular corresponding to the area indicated by the arrow magnification 40x) demonstrate a positive reaction forfractalkine in the endothelial cells (e) shows an haematoxylin eosin of a coronary from a patient died by bronchopneumonia without clinicalcardiac historyThe plaque shows a thick fibrotic cap and the inflammatory infiltrate is scanty and predominantly constituted bymacrophages((f) macrophages CD68 positive revealed by alkaline phosphataseanti-alkaline phosphatase red reaction and T lymphocytes CD3 positiveDAB dectected streptavidinbiotin immunoperoxidase brown reaction) The immunostaining for the fractalkine receptor CX3CR1 gave riseto a weak positive reaction in the smooth muscle cells and macrophages ((g) 10x magnification) The reaction for fractalkine was negative inthe control group (h) (in the insert a particular corresponding to the area indicated by the arrow magnification 40x)
BioMed Research International 7
(b)
(c)
(d)(a)
Figure 3 Confocal microscopy examination of triple stain in a culprit lesion (coronary artery from AMI group) (a) (magnification 2000x)shows a 2D reconstruction triple stain for T cells CD3 (blue) fractalkine receptor CX3CR1 (green) and IFN-gamma (red) yellow lightblue and white areas were due to multiple positivity (b) CD3 immunostaining revealed by coumarin conjugated streptavidin (c) CX3CR1immunostaining revealed by FITC conjugated streptavidin (d) IFN-gamma immunostaining revealed by Texas Red conjugated streptavidin
Table 2 Correlation between inflammatory infiltrate and CX3CR1 polymorphismsect
AMI NCCVV249
1325 (52)lowastVI249
1025 (40)II249225 (8)
VV249222 (9)
VI2491222 (55)
II249822 (36)
CD3Negweak 0 0 1 1 7 7Pos moderate 0 1 1 1 5 0Strong 13 9 0 0 0 0
CD20Negweak 12 9 0 2 12 7Pos moderate 1 1 0 0 0 0Strong 0 0 2 0 0 0
CXCL1Negweak 0 0 0 1 12 7Pos moderate 1 1 2 1 0 0Strong 12 9 0 0 0 0
CXCR1Negweak 0 0 1 1 7 7Pos moderate 0 1 1 0 5 0Strong 13 9 0 1 0 0
sectThe table shows the IHC results in the coronary plaque of AMI and control patients (NCC) correlated to the presence of CX3CR1 V249I polymorphism inthe same groups lowastIn parentheses the percentage of patients was reported
and the occurrence of acute fatal myocardial infarction Astriking link between genotype and prognosis of the acuteevent was suggested by the observation of AMI survivorsgenotypes Notably the in situ CX3CR1 high expression in
AMI patients correlates with the presence of V249 polymor-phism in homo- or heterozygosis Conversely the genotypeanalysis of controls (with no CVD history) demonstrated thepresence of I249 polymorphism in homozygosis
8 BioMed Research International
Table 3 Analysis of CX3CR1 polymorphisms in patients andcontrol groups
AMI(119899 = 25)
SVR(119899 = 16)
NCC(119899 = 22)
V249IVV 13 (52) 1 (6) 2 (9)VI 10 (40) 10 (63) 12 (55)II 2 (8) 5 (31) 8 (36)
119875 = 0003 119875 = 0003 119875 = 0006
T280MTT 21 (84) 9 (56) 14 (64)TM 4 (16) 7 (44) 7 (32)MM 0 0 1 (4)
119875 = 0001 119875 = 0002 119875 = 0001
Data are absolute numbers (percentage)Abbreviations AMI acute myocardial infarction SVR patients survived toa first AMI NCC subjects dead for noncardiac causesThe statistical significance of different polymorphisms present in the singlegroups was identified by Fisherrsquos exact test
Indeed CX3CR1 V249T280 polymorphisms in homozy-gosis or heterozygosis have been demonstrated in 92 of theAMI patients analyzed (mean age 70 years old) In particular52 of the AMI patients examined were homozygous forCX3CR1 V249 whereas the analysis of the genotype of thecontrol subjects (mean age 737 years old) demonstrated thepresence of CX3CR1 V249 polymorphism in homozygosisonly in the 9 of cases The findings of the high percentageof II249 (36) and MM280 (4) in subjects died of nocardiac causes suggest a possible link between CX3CR1 poly-morphism T cell recruitment and acute eventMoreover thegenotype observations on survivors group suggest that thepresence of I249 allele is relevant not only for the occurrencebut also in the outcome of the acute event
There is evidence of the influence of CX3CR1 variableexpression and function on T cells recruitment efficiency[14 21 22]
Studies on CX3CR1 null mice crossed into apoE minusminusbackground [12] demonstrated that although CX3CL1 wasstrongly expressed in smooth muscle cells in the lesion thelack of the CX3CR1 receptor was related to a significantreduction in macrophages and T cells recruitment within thevessel wall associated with a reduction of atherosclerosis
In present work we also show a close association betweenCX3CR1 genotypes and coronary plaques T cell inflam-mation that is a relevant character of vulnerable plaquesaccording to data previously published [1 2]
Indeed coronary plaques of patients with CX3CR1 I249allele displayed a weaker T cell inflammation as compared toindividuals homozygous for the CX3CR1 V249 allele
In particular we show that CX3CR1 is highly expressedby the majority of T cells infiltrating IRA plaques of 22 out of25 AMI patients
It is worth noting that the two patients showing a lowexpression of CX3CR1 were CX3CR1 I249 homozygou andtheir plaques were infiltrated by B lymphocytes suggestinga different pathogenesis for AMI
Conversely immunostaining for CX3CR1 was negative orfaint positive in plaques of controls where the T lymphocytesinfiltrate was lower as compared with AMI patients
Therefore it can be assumed that the high expression ofCX3CR1 together with the in situ expression of fractalkine(CX3CL1) correlates with the increased recruitment of Tlymphocytes deeply infiltrating in the plaques of the AMIpatients
The special feature of fractalkine among other mem-bers of the chemokine family is due to the fact that it isexpressed both as soluble and membrane-bound form onthe surface of inflamed endothelium Interestingly whereassoluble fractalkine (CX3CL1) was reported to recruit lym-phocytes andmonocytes immobilized forms ofCX3CL1 havebeen shown to directly mediate the rapid capture and firmadhesion of leukocytes expressing its receptor CX3CR1 underphysiological flow conditions [23] The direct binding of thechemokine to CX3CR1 does not require the upregulationand activation of integrins suggesting that fractalkine andCX3CR1 mediate a novel pathway for leukocytes traffick-ing [24] In addition to the intrinsic adhesive functionof fractalkine this chemokine can also transduce signalsthrough G proteins that enhance the avidity of integrinbinding to its ligands for leukocytes recruitment [25 26]
The coexpression of CD3 IFN-gamma and CX3CR1 onT cell population found inAMI plaques compared to controlsdemonstrates the in situ activation of inflammatory cellspointing out the probable involvement of a recent immuneTh1 response in plaque destabilization and ruptureMoreoverthe data obtained suggest that the susceptibility to vascularinflammation is correlated with the amplified recruitment ofTh1 polarized cells expressing the high or low affinity CX3CR1receptor The findings revealing CX3CR1 expression by 80of T cell population along with the presence of fractalkinein IRA plaques suggest that these two events are both likelyto play a major role in determining plaque vulnerability byorchestratingTh1 cells recruitment
In agreement with previous clinical and epidemiologicalstudies our data demonstrate a close association betweenV249I and T280M polymorphisms coronary plaque vul-nerability and AMI confirming that the subjects with I249allele display a low level of T cell inflammation and areduced risk of developing vulnerable plaques and they have adecreased incidence of acute events (probably due to a lowerCX3CR1 binding affinity) [27] The comparative analysis ofthe different CXCR3 polymorphisms and the inflammatoryinfiltrate shows a significant difference between fatal AMIand NCC A study limitation is the lacking in the compar-ative analysis of the coronary surgical samples from AMIsurvivors These patients in fact underwent a ventricularrestoration for a previous nonfatal AMI event Despite theabove limitations our study provides lines of evidence thatthe I249 allele could be strongly involved in the protectionfrom fatal AMI with these association being independent ofthe major ldquoconventionalrdquo cardiovascular risk factors Furtherstudies will be addressed with a prospective massive scalepopulation study to validate this assumption
In conclusion CX3CR1 genotype could be considered as anew marker to stratify the population according to fatal AMI
BioMed Research International 9
risk Moreover CX3CR1 is likely to amplify the Th1 immuneresponse directly related to plaque vulnerability irrespec-tively of the causal agents (ie ox-LDL or Chlamydia) thusstanding out as a potential target in fatal AMI prevention
References
[1] A I Gotlieb ldquoAtherosclerosis and acute coronary syndromesrdquoCardiovascular Pathology vol 14 no 4 pp 181ndash184 2005
[2] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[3] P Fraticelli M Sironi G Bianchi et al ldquoFractalkine (CX3CL1)as an amplification circuit of polarized Th1 responsesrdquo Journalof Clinical Investigation vol 107 no 9 pp 1173ndash1181 2001
[4] R Bonecchi G Bianchi P P Bordignon et al ldquoDifferentialexpression of chemokine receptors and chemotactic respon-siveness of type 1 T helper cells (Th1s) and Th2srdquo Journal ofExperimental Medicine vol 187 no 1 pp 129ndash134 1998
[5] J F Bazan K B Bacon G Hardiman et al ldquoA new class ofmembrane-bound chemokine with a CX3C motifrdquo Nature vol385 no 6617 pp 640ndash642 1997
[6] C Murdoch and A Finn ldquoChemokine receptors and their rolein vascular biologyrdquo Journal of Vascular Research vol 37 no 1pp 1ndash7 2000
[7] C Murdoch and A Finn ldquoChemokine receptors and their rolein inflammation and infectious diseasesrdquo Blood vol 95 no 10pp 3032ndash3043 2000
[8] C Combadiere K Salzwedel E D Smith H L Tiffany E ABerger and PMMurphy ldquoIdentification of CX3CR1 A chemo-tactic receptor for the human CX3C chemokine fractalkineand a fusion coreceptor for HIV-1rdquo The Journal of BiologicalChemistry vol 273 no 37 pp 23799ndash23804 1998
[9] G A Chapman K E Moores J Gohil et al ldquoThe role offractalkine in the recruitment of monocytes to the endothe-liumrdquo European Journal of Pharmacology vol 392 no 3 pp189ndash195 2000
[10] T Kasama K Wakabayashi M Sato R Takahashi and TIsozaki ldquoRelevance of the CX3CL1fractalkine-CX3CR1 path-way in vasculitis and vasculopathyrdquo Translational Research vol155 no 1 pp 20ndash26 2010
[11] M Garcıa-Alvarez J Berenguer M Guzman-Fulgencio et alldquoHigh plasma fractalkine (CX3CL1) levels are associated withsevere liver disease inHIVHCVco-infected patients withHCVgenotype 1rdquo Cytokine vol 54 no 3 pp 244ndash248 2011
[12] P Lesnik C A Haskell and I F Charo ldquoDecreased atheroscle-rosis in CX3CR1-- mice reveals a role for fractalkine inatherogenesisrdquo Journal of Clinical Investigation vol 111 no 3pp 333ndash340 2003
[13] M Stolla J Pelisek M-L von Bruhl A Schafer V Barockeand P Heider ldquoFractalkine is expressed in early and advancedatherosclerotic lesions and supports monocyte recruitment viaCX3CR1rdquo PLoS ONE vol 7 no 8 Article ID e43572 2012
[14] J K Damas A Boullier T Waelighre et al ldquoExpression offractalkine (CX3CL1) and its receptor CX3CR1 is elevated incoronary artery disease and is reduced during statin therapyrdquoArteriosclerosis Thrombosis and Vascular Biology vol 25 no12 pp 2567ndash2572 2005
[15] A M Fong L A Robinson D A Steeber et al ldquoFractalkineand CX3CR1 mediate a novel mechanism of leukocyte capturefirm adhesion and activation under physiologic flowrdquo Journalof Experimental Medicine vol 188 no 8 pp 1413ndash1419 1998
[16] D Moatti S Faure F Fumeron et al ldquoPolymorphism in thefractalkine receptor CX3CR1 as a genetic risk factor for coro-nary artery diseaserdquo Blood vol 97 no 7 pp 1925ndash1928 2001
[17] N Singh N Sinha S Kumar C M Pandey and S AgrawalldquoPolymorphism in chemokine receptor genes and risk of acutemyocardial infarction in North Indian populationrdquo MolecularBiology Reports vol 39 no 3 pp 2753ndash2759 2012
[18] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[19] G K Hansson and A Hermansson ldquoThe immune system inatherosclerosisrdquoNature Immunology vol 12 no 3 pp 204ndash2122011
[20] H Umehara E Bloom T Okazaki N Domae and T ImaildquoFractalkine and vascular injuryrdquoTrends in Immunology vol 22no 11 pp 602ndash607 2001
[21] H Umehara S Goda T Imai et al ldquoFractalkine a CX3C-chemokine functions predominantly as an adhesion moleculeinmonocytic cell line THP-1rdquo Immunology andCell Biology vol79 no 3 pp 298ndash302 2001
[22] L Lasagni M Francalanci F Annunziato et al ldquoAn alter-natively spliced variant of CXCR3 mediates the inhibition ofendothelial cell growth induced by IP-10 Mig and I-TACand acts as functional receptor for platelet factor 4rdquo Journal ofExperimental Medicine vol 197 no 11 pp 1537ndash1549 2003
[23] S Jung J Aliberti P Graemmel et al ldquoAnalysis of fractalkinereceptor CX3CR1 function by targeted deletion and greenfluorescent protein reporter gene insertionrdquo Molecular andCellular Biology vol 20 no 11 pp 4106ndash4114 2000
[24] D H McDermott J P J Halcox W H Schenke et alldquoAssociation between polymorphism in the chemokine receptorCX3CR1 and coronary vascular endothelial dysfunction andatherosclerosisrdquoCirculation Research vol 89 no 5 pp 401ndash4072001
[25] H Umehara and T Imai ldquoRole of fractalkine in leukocyteadhesion and migration and in vascular injuryrdquoDrug News andPerspectives vol 14 no 8 pp 460ndash464 2001
[26] H Fujimoto Y Tanaka Z-J Liu et al ldquoDown-regulation of 1205726integrin an anti-oncogene product by functional cooperationof H-Ras and c-Mycrdquo Genes to Cells vol 6 no 4 pp 337ndash3432001
[27] M Kimoli S Miyakis P Georgakopoulos E Noefytou A DAchimastos and D A Spandidos ldquoPolymorphisms of frac-talkine receptorCX3CR1 gene in patientswith symptomatic andasymptomatic carotid artery stenosisrdquo Journal of Atherosclerosisand Thrombosis vol 16 no 5 pp 604ndash610 2009
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
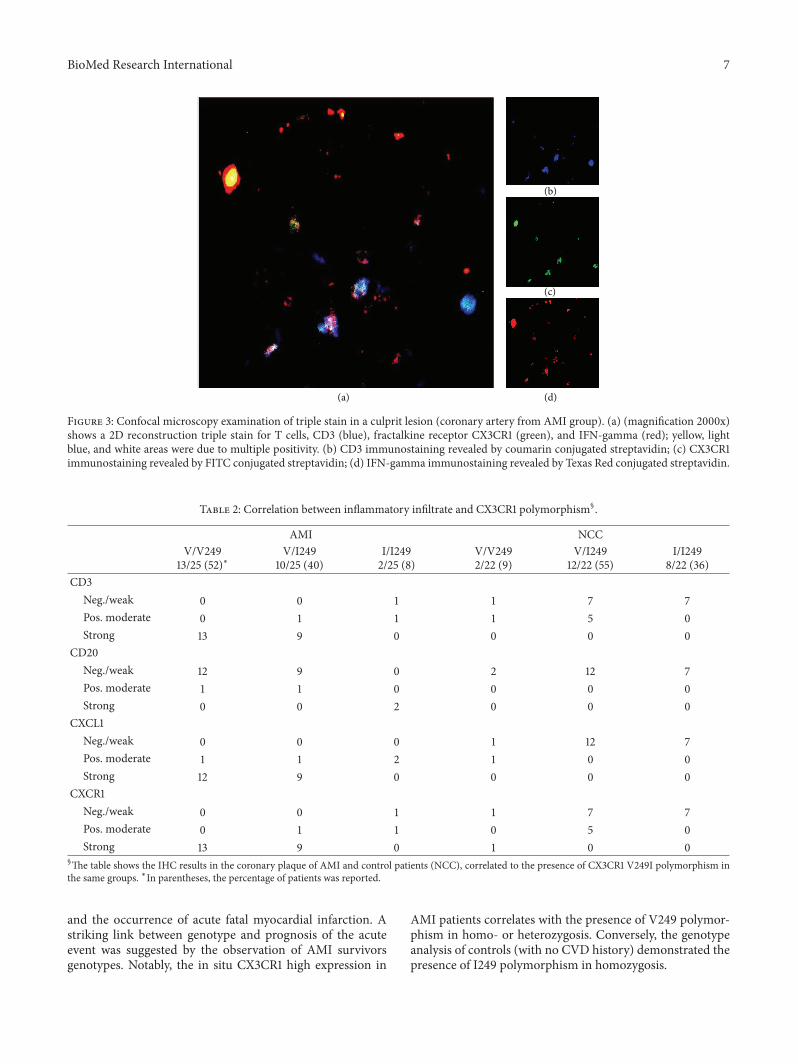
BioMed Research International 7
(b)
(c)
(d)(a)
Figure 3 Confocal microscopy examination of triple stain in a culprit lesion (coronary artery from AMI group) (a) (magnification 2000x)shows a 2D reconstruction triple stain for T cells CD3 (blue) fractalkine receptor CX3CR1 (green) and IFN-gamma (red) yellow lightblue and white areas were due to multiple positivity (b) CD3 immunostaining revealed by coumarin conjugated streptavidin (c) CX3CR1immunostaining revealed by FITC conjugated streptavidin (d) IFN-gamma immunostaining revealed by Texas Red conjugated streptavidin
Table 2 Correlation between inflammatory infiltrate and CX3CR1 polymorphismsect
AMI NCCVV249
1325 (52)lowastVI249
1025 (40)II249225 (8)
VV249222 (9)
VI2491222 (55)
II249822 (36)
CD3Negweak 0 0 1 1 7 7Pos moderate 0 1 1 1 5 0Strong 13 9 0 0 0 0
CD20Negweak 12 9 0 2 12 7Pos moderate 1 1 0 0 0 0Strong 0 0 2 0 0 0
CXCL1Negweak 0 0 0 1 12 7Pos moderate 1 1 2 1 0 0Strong 12 9 0 0 0 0
CXCR1Negweak 0 0 1 1 7 7Pos moderate 0 1 1 0 5 0Strong 13 9 0 1 0 0
sectThe table shows the IHC results in the coronary plaque of AMI and control patients (NCC) correlated to the presence of CX3CR1 V249I polymorphism inthe same groups lowastIn parentheses the percentage of patients was reported
and the occurrence of acute fatal myocardial infarction Astriking link between genotype and prognosis of the acuteevent was suggested by the observation of AMI survivorsgenotypes Notably the in situ CX3CR1 high expression in
AMI patients correlates with the presence of V249 polymor-phism in homo- or heterozygosis Conversely the genotypeanalysis of controls (with no CVD history) demonstrated thepresence of I249 polymorphism in homozygosis
8 BioMed Research International
Table 3 Analysis of CX3CR1 polymorphisms in patients andcontrol groups
AMI(119899 = 25)
SVR(119899 = 16)
NCC(119899 = 22)
V249IVV 13 (52) 1 (6) 2 (9)VI 10 (40) 10 (63) 12 (55)II 2 (8) 5 (31) 8 (36)
119875 = 0003 119875 = 0003 119875 = 0006
T280MTT 21 (84) 9 (56) 14 (64)TM 4 (16) 7 (44) 7 (32)MM 0 0 1 (4)
119875 = 0001 119875 = 0002 119875 = 0001
Data are absolute numbers (percentage)Abbreviations AMI acute myocardial infarction SVR patients survived toa first AMI NCC subjects dead for noncardiac causesThe statistical significance of different polymorphisms present in the singlegroups was identified by Fisherrsquos exact test
Indeed CX3CR1 V249T280 polymorphisms in homozy-gosis or heterozygosis have been demonstrated in 92 of theAMI patients analyzed (mean age 70 years old) In particular52 of the AMI patients examined were homozygous forCX3CR1 V249 whereas the analysis of the genotype of thecontrol subjects (mean age 737 years old) demonstrated thepresence of CX3CR1 V249 polymorphism in homozygosisonly in the 9 of cases The findings of the high percentageof II249 (36) and MM280 (4) in subjects died of nocardiac causes suggest a possible link between CX3CR1 poly-morphism T cell recruitment and acute eventMoreover thegenotype observations on survivors group suggest that thepresence of I249 allele is relevant not only for the occurrencebut also in the outcome of the acute event
There is evidence of the influence of CX3CR1 variableexpression and function on T cells recruitment efficiency[14 21 22]
Studies on CX3CR1 null mice crossed into apoE minusminusbackground [12] demonstrated that although CX3CL1 wasstrongly expressed in smooth muscle cells in the lesion thelack of the CX3CR1 receptor was related to a significantreduction in macrophages and T cells recruitment within thevessel wall associated with a reduction of atherosclerosis
In present work we also show a close association betweenCX3CR1 genotypes and coronary plaques T cell inflam-mation that is a relevant character of vulnerable plaquesaccording to data previously published [1 2]
Indeed coronary plaques of patients with CX3CR1 I249allele displayed a weaker T cell inflammation as compared toindividuals homozygous for the CX3CR1 V249 allele
In particular we show that CX3CR1 is highly expressedby the majority of T cells infiltrating IRA plaques of 22 out of25 AMI patients
It is worth noting that the two patients showing a lowexpression of CX3CR1 were CX3CR1 I249 homozygou andtheir plaques were infiltrated by B lymphocytes suggestinga different pathogenesis for AMI
Conversely immunostaining for CX3CR1 was negative orfaint positive in plaques of controls where the T lymphocytesinfiltrate was lower as compared with AMI patients
Therefore it can be assumed that the high expression ofCX3CR1 together with the in situ expression of fractalkine(CX3CL1) correlates with the increased recruitment of Tlymphocytes deeply infiltrating in the plaques of the AMIpatients
The special feature of fractalkine among other mem-bers of the chemokine family is due to the fact that it isexpressed both as soluble and membrane-bound form onthe surface of inflamed endothelium Interestingly whereassoluble fractalkine (CX3CL1) was reported to recruit lym-phocytes andmonocytes immobilized forms ofCX3CL1 havebeen shown to directly mediate the rapid capture and firmadhesion of leukocytes expressing its receptor CX3CR1 underphysiological flow conditions [23] The direct binding of thechemokine to CX3CR1 does not require the upregulationand activation of integrins suggesting that fractalkine andCX3CR1 mediate a novel pathway for leukocytes traffick-ing [24] In addition to the intrinsic adhesive functionof fractalkine this chemokine can also transduce signalsthrough G proteins that enhance the avidity of integrinbinding to its ligands for leukocytes recruitment [25 26]
The coexpression of CD3 IFN-gamma and CX3CR1 onT cell population found inAMI plaques compared to controlsdemonstrates the in situ activation of inflammatory cellspointing out the probable involvement of a recent immuneTh1 response in plaque destabilization and ruptureMoreoverthe data obtained suggest that the susceptibility to vascularinflammation is correlated with the amplified recruitment ofTh1 polarized cells expressing the high or low affinity CX3CR1receptor The findings revealing CX3CR1 expression by 80of T cell population along with the presence of fractalkinein IRA plaques suggest that these two events are both likelyto play a major role in determining plaque vulnerability byorchestratingTh1 cells recruitment
In agreement with previous clinical and epidemiologicalstudies our data demonstrate a close association betweenV249I and T280M polymorphisms coronary plaque vul-nerability and AMI confirming that the subjects with I249allele display a low level of T cell inflammation and areduced risk of developing vulnerable plaques and they have adecreased incidence of acute events (probably due to a lowerCX3CR1 binding affinity) [27] The comparative analysis ofthe different CXCR3 polymorphisms and the inflammatoryinfiltrate shows a significant difference between fatal AMIand NCC A study limitation is the lacking in the compar-ative analysis of the coronary surgical samples from AMIsurvivors These patients in fact underwent a ventricularrestoration for a previous nonfatal AMI event Despite theabove limitations our study provides lines of evidence thatthe I249 allele could be strongly involved in the protectionfrom fatal AMI with these association being independent ofthe major ldquoconventionalrdquo cardiovascular risk factors Furtherstudies will be addressed with a prospective massive scalepopulation study to validate this assumption
In conclusion CX3CR1 genotype could be considered as anew marker to stratify the population according to fatal AMI
BioMed Research International 9
risk Moreover CX3CR1 is likely to amplify the Th1 immuneresponse directly related to plaque vulnerability irrespec-tively of the causal agents (ie ox-LDL or Chlamydia) thusstanding out as a potential target in fatal AMI prevention
References
[1] A I Gotlieb ldquoAtherosclerosis and acute coronary syndromesrdquoCardiovascular Pathology vol 14 no 4 pp 181ndash184 2005
[2] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[3] P Fraticelli M Sironi G Bianchi et al ldquoFractalkine (CX3CL1)as an amplification circuit of polarized Th1 responsesrdquo Journalof Clinical Investigation vol 107 no 9 pp 1173ndash1181 2001
[4] R Bonecchi G Bianchi P P Bordignon et al ldquoDifferentialexpression of chemokine receptors and chemotactic respon-siveness of type 1 T helper cells (Th1s) and Th2srdquo Journal ofExperimental Medicine vol 187 no 1 pp 129ndash134 1998
[5] J F Bazan K B Bacon G Hardiman et al ldquoA new class ofmembrane-bound chemokine with a CX3C motifrdquo Nature vol385 no 6617 pp 640ndash642 1997
[6] C Murdoch and A Finn ldquoChemokine receptors and their rolein vascular biologyrdquo Journal of Vascular Research vol 37 no 1pp 1ndash7 2000
[7] C Murdoch and A Finn ldquoChemokine receptors and their rolein inflammation and infectious diseasesrdquo Blood vol 95 no 10pp 3032ndash3043 2000
[8] C Combadiere K Salzwedel E D Smith H L Tiffany E ABerger and PMMurphy ldquoIdentification of CX3CR1 A chemo-tactic receptor for the human CX3C chemokine fractalkineand a fusion coreceptor for HIV-1rdquo The Journal of BiologicalChemistry vol 273 no 37 pp 23799ndash23804 1998
[9] G A Chapman K E Moores J Gohil et al ldquoThe role offractalkine in the recruitment of monocytes to the endothe-liumrdquo European Journal of Pharmacology vol 392 no 3 pp189ndash195 2000
[10] T Kasama K Wakabayashi M Sato R Takahashi and TIsozaki ldquoRelevance of the CX3CL1fractalkine-CX3CR1 path-way in vasculitis and vasculopathyrdquo Translational Research vol155 no 1 pp 20ndash26 2010
[11] M Garcıa-Alvarez J Berenguer M Guzman-Fulgencio et alldquoHigh plasma fractalkine (CX3CL1) levels are associated withsevere liver disease inHIVHCVco-infected patients withHCVgenotype 1rdquo Cytokine vol 54 no 3 pp 244ndash248 2011
[12] P Lesnik C A Haskell and I F Charo ldquoDecreased atheroscle-rosis in CX3CR1-- mice reveals a role for fractalkine inatherogenesisrdquo Journal of Clinical Investigation vol 111 no 3pp 333ndash340 2003
[13] M Stolla J Pelisek M-L von Bruhl A Schafer V Barockeand P Heider ldquoFractalkine is expressed in early and advancedatherosclerotic lesions and supports monocyte recruitment viaCX3CR1rdquo PLoS ONE vol 7 no 8 Article ID e43572 2012
[14] J K Damas A Boullier T Waelighre et al ldquoExpression offractalkine (CX3CL1) and its receptor CX3CR1 is elevated incoronary artery disease and is reduced during statin therapyrdquoArteriosclerosis Thrombosis and Vascular Biology vol 25 no12 pp 2567ndash2572 2005
[15] A M Fong L A Robinson D A Steeber et al ldquoFractalkineand CX3CR1 mediate a novel mechanism of leukocyte capturefirm adhesion and activation under physiologic flowrdquo Journalof Experimental Medicine vol 188 no 8 pp 1413ndash1419 1998
[16] D Moatti S Faure F Fumeron et al ldquoPolymorphism in thefractalkine receptor CX3CR1 as a genetic risk factor for coro-nary artery diseaserdquo Blood vol 97 no 7 pp 1925ndash1928 2001
[17] N Singh N Sinha S Kumar C M Pandey and S AgrawalldquoPolymorphism in chemokine receptor genes and risk of acutemyocardial infarction in North Indian populationrdquo MolecularBiology Reports vol 39 no 3 pp 2753ndash2759 2012
[18] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[19] G K Hansson and A Hermansson ldquoThe immune system inatherosclerosisrdquoNature Immunology vol 12 no 3 pp 204ndash2122011
[20] H Umehara E Bloom T Okazaki N Domae and T ImaildquoFractalkine and vascular injuryrdquoTrends in Immunology vol 22no 11 pp 602ndash607 2001
[21] H Umehara S Goda T Imai et al ldquoFractalkine a CX3C-chemokine functions predominantly as an adhesion moleculeinmonocytic cell line THP-1rdquo Immunology andCell Biology vol79 no 3 pp 298ndash302 2001
[22] L Lasagni M Francalanci F Annunziato et al ldquoAn alter-natively spliced variant of CXCR3 mediates the inhibition ofendothelial cell growth induced by IP-10 Mig and I-TACand acts as functional receptor for platelet factor 4rdquo Journal ofExperimental Medicine vol 197 no 11 pp 1537ndash1549 2003
[23] S Jung J Aliberti P Graemmel et al ldquoAnalysis of fractalkinereceptor CX3CR1 function by targeted deletion and greenfluorescent protein reporter gene insertionrdquo Molecular andCellular Biology vol 20 no 11 pp 4106ndash4114 2000
[24] D H McDermott J P J Halcox W H Schenke et alldquoAssociation between polymorphism in the chemokine receptorCX3CR1 and coronary vascular endothelial dysfunction andatherosclerosisrdquoCirculation Research vol 89 no 5 pp 401ndash4072001
[25] H Umehara and T Imai ldquoRole of fractalkine in leukocyteadhesion and migration and in vascular injuryrdquoDrug News andPerspectives vol 14 no 8 pp 460ndash464 2001
[26] H Fujimoto Y Tanaka Z-J Liu et al ldquoDown-regulation of 1205726integrin an anti-oncogene product by functional cooperationof H-Ras and c-Mycrdquo Genes to Cells vol 6 no 4 pp 337ndash3432001
[27] M Kimoli S Miyakis P Georgakopoulos E Noefytou A DAchimastos and D A Spandidos ldquoPolymorphisms of frac-talkine receptorCX3CR1 gene in patientswith symptomatic andasymptomatic carotid artery stenosisrdquo Journal of Atherosclerosisand Thrombosis vol 16 no 5 pp 604ndash610 2009
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom
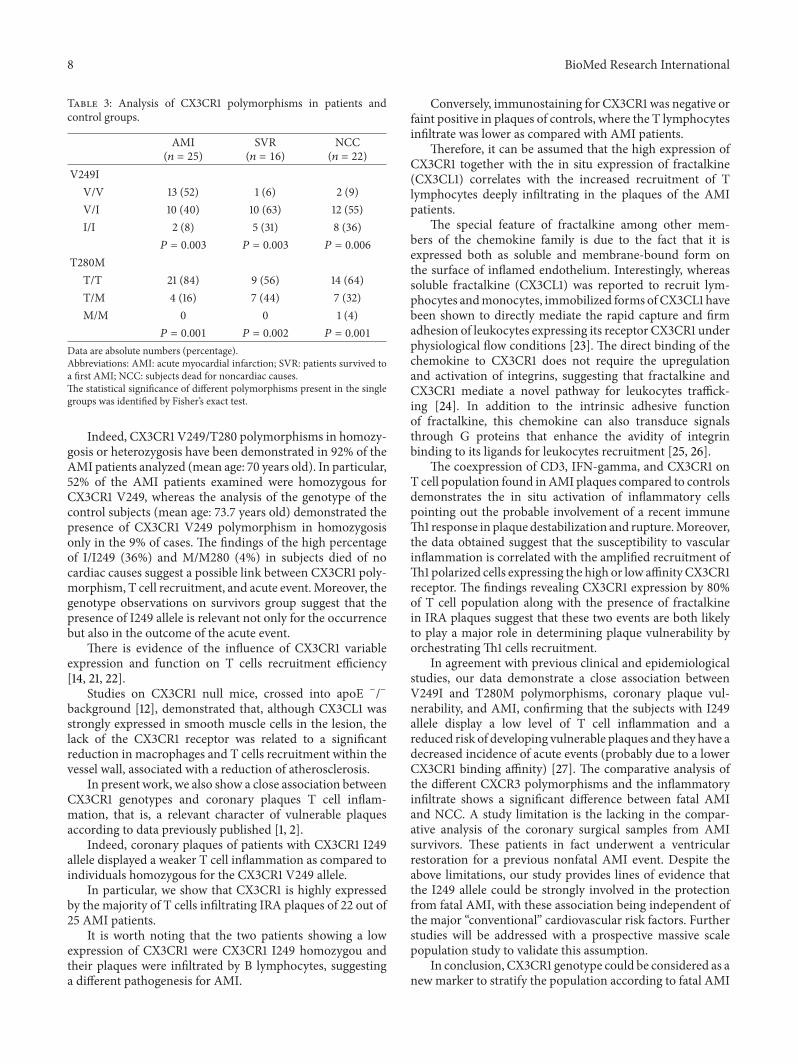
8 BioMed Research International
Table 3 Analysis of CX3CR1 polymorphisms in patients andcontrol groups
AMI(119899 = 25)
SVR(119899 = 16)
NCC(119899 = 22)
V249IVV 13 (52) 1 (6) 2 (9)VI 10 (40) 10 (63) 12 (55)II 2 (8) 5 (31) 8 (36)
119875 = 0003 119875 = 0003 119875 = 0006
T280MTT 21 (84) 9 (56) 14 (64)TM 4 (16) 7 (44) 7 (32)MM 0 0 1 (4)
119875 = 0001 119875 = 0002 119875 = 0001
Data are absolute numbers (percentage)Abbreviations AMI acute myocardial infarction SVR patients survived toa first AMI NCC subjects dead for noncardiac causesThe statistical significance of different polymorphisms present in the singlegroups was identified by Fisherrsquos exact test
Indeed CX3CR1 V249T280 polymorphisms in homozy-gosis or heterozygosis have been demonstrated in 92 of theAMI patients analyzed (mean age 70 years old) In particular52 of the AMI patients examined were homozygous forCX3CR1 V249 whereas the analysis of the genotype of thecontrol subjects (mean age 737 years old) demonstrated thepresence of CX3CR1 V249 polymorphism in homozygosisonly in the 9 of cases The findings of the high percentageof II249 (36) and MM280 (4) in subjects died of nocardiac causes suggest a possible link between CX3CR1 poly-morphism T cell recruitment and acute eventMoreover thegenotype observations on survivors group suggest that thepresence of I249 allele is relevant not only for the occurrencebut also in the outcome of the acute event
There is evidence of the influence of CX3CR1 variableexpression and function on T cells recruitment efficiency[14 21 22]
Studies on CX3CR1 null mice crossed into apoE minusminusbackground [12] demonstrated that although CX3CL1 wasstrongly expressed in smooth muscle cells in the lesion thelack of the CX3CR1 receptor was related to a significantreduction in macrophages and T cells recruitment within thevessel wall associated with a reduction of atherosclerosis
In present work we also show a close association betweenCX3CR1 genotypes and coronary plaques T cell inflam-mation that is a relevant character of vulnerable plaquesaccording to data previously published [1 2]
Indeed coronary plaques of patients with CX3CR1 I249allele displayed a weaker T cell inflammation as compared toindividuals homozygous for the CX3CR1 V249 allele
In particular we show that CX3CR1 is highly expressedby the majority of T cells infiltrating IRA plaques of 22 out of25 AMI patients
It is worth noting that the two patients showing a lowexpression of CX3CR1 were CX3CR1 I249 homozygou andtheir plaques were infiltrated by B lymphocytes suggestinga different pathogenesis for AMI
Conversely immunostaining for CX3CR1 was negative orfaint positive in plaques of controls where the T lymphocytesinfiltrate was lower as compared with AMI patients
Therefore it can be assumed that the high expression ofCX3CR1 together with the in situ expression of fractalkine(CX3CL1) correlates with the increased recruitment of Tlymphocytes deeply infiltrating in the plaques of the AMIpatients
The special feature of fractalkine among other mem-bers of the chemokine family is due to the fact that it isexpressed both as soluble and membrane-bound form onthe surface of inflamed endothelium Interestingly whereassoluble fractalkine (CX3CL1) was reported to recruit lym-phocytes andmonocytes immobilized forms ofCX3CL1 havebeen shown to directly mediate the rapid capture and firmadhesion of leukocytes expressing its receptor CX3CR1 underphysiological flow conditions [23] The direct binding of thechemokine to CX3CR1 does not require the upregulationand activation of integrins suggesting that fractalkine andCX3CR1 mediate a novel pathway for leukocytes traffick-ing [24] In addition to the intrinsic adhesive functionof fractalkine this chemokine can also transduce signalsthrough G proteins that enhance the avidity of integrinbinding to its ligands for leukocytes recruitment [25 26]
The coexpression of CD3 IFN-gamma and CX3CR1 onT cell population found inAMI plaques compared to controlsdemonstrates the in situ activation of inflammatory cellspointing out the probable involvement of a recent immuneTh1 response in plaque destabilization and ruptureMoreoverthe data obtained suggest that the susceptibility to vascularinflammation is correlated with the amplified recruitment ofTh1 polarized cells expressing the high or low affinity CX3CR1receptor The findings revealing CX3CR1 expression by 80of T cell population along with the presence of fractalkinein IRA plaques suggest that these two events are both likelyto play a major role in determining plaque vulnerability byorchestratingTh1 cells recruitment
In agreement with previous clinical and epidemiologicalstudies our data demonstrate a close association betweenV249I and T280M polymorphisms coronary plaque vul-nerability and AMI confirming that the subjects with I249allele display a low level of T cell inflammation and areduced risk of developing vulnerable plaques and they have adecreased incidence of acute events (probably due to a lowerCX3CR1 binding affinity) [27] The comparative analysis ofthe different CXCR3 polymorphisms and the inflammatoryinfiltrate shows a significant difference between fatal AMIand NCC A study limitation is the lacking in the compar-ative analysis of the coronary surgical samples from AMIsurvivors These patients in fact underwent a ventricularrestoration for a previous nonfatal AMI event Despite theabove limitations our study provides lines of evidence thatthe I249 allele could be strongly involved in the protectionfrom fatal AMI with these association being independent ofthe major ldquoconventionalrdquo cardiovascular risk factors Furtherstudies will be addressed with a prospective massive scalepopulation study to validate this assumption
In conclusion CX3CR1 genotype could be considered as anew marker to stratify the population according to fatal AMI
BioMed Research International 9
risk Moreover CX3CR1 is likely to amplify the Th1 immuneresponse directly related to plaque vulnerability irrespec-tively of the causal agents (ie ox-LDL or Chlamydia) thusstanding out as a potential target in fatal AMI prevention
References
[1] A I Gotlieb ldquoAtherosclerosis and acute coronary syndromesrdquoCardiovascular Pathology vol 14 no 4 pp 181ndash184 2005
[2] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[3] P Fraticelli M Sironi G Bianchi et al ldquoFractalkine (CX3CL1)as an amplification circuit of polarized Th1 responsesrdquo Journalof Clinical Investigation vol 107 no 9 pp 1173ndash1181 2001
[4] R Bonecchi G Bianchi P P Bordignon et al ldquoDifferentialexpression of chemokine receptors and chemotactic respon-siveness of type 1 T helper cells (Th1s) and Th2srdquo Journal ofExperimental Medicine vol 187 no 1 pp 129ndash134 1998
[5] J F Bazan K B Bacon G Hardiman et al ldquoA new class ofmembrane-bound chemokine with a CX3C motifrdquo Nature vol385 no 6617 pp 640ndash642 1997
[6] C Murdoch and A Finn ldquoChemokine receptors and their rolein vascular biologyrdquo Journal of Vascular Research vol 37 no 1pp 1ndash7 2000
[7] C Murdoch and A Finn ldquoChemokine receptors and their rolein inflammation and infectious diseasesrdquo Blood vol 95 no 10pp 3032ndash3043 2000
[8] C Combadiere K Salzwedel E D Smith H L Tiffany E ABerger and PMMurphy ldquoIdentification of CX3CR1 A chemo-tactic receptor for the human CX3C chemokine fractalkineand a fusion coreceptor for HIV-1rdquo The Journal of BiologicalChemistry vol 273 no 37 pp 23799ndash23804 1998
[9] G A Chapman K E Moores J Gohil et al ldquoThe role offractalkine in the recruitment of monocytes to the endothe-liumrdquo European Journal of Pharmacology vol 392 no 3 pp189ndash195 2000
[10] T Kasama K Wakabayashi M Sato R Takahashi and TIsozaki ldquoRelevance of the CX3CL1fractalkine-CX3CR1 path-way in vasculitis and vasculopathyrdquo Translational Research vol155 no 1 pp 20ndash26 2010
[11] M Garcıa-Alvarez J Berenguer M Guzman-Fulgencio et alldquoHigh plasma fractalkine (CX3CL1) levels are associated withsevere liver disease inHIVHCVco-infected patients withHCVgenotype 1rdquo Cytokine vol 54 no 3 pp 244ndash248 2011
[12] P Lesnik C A Haskell and I F Charo ldquoDecreased atheroscle-rosis in CX3CR1-- mice reveals a role for fractalkine inatherogenesisrdquo Journal of Clinical Investigation vol 111 no 3pp 333ndash340 2003
[13] M Stolla J Pelisek M-L von Bruhl A Schafer V Barockeand P Heider ldquoFractalkine is expressed in early and advancedatherosclerotic lesions and supports monocyte recruitment viaCX3CR1rdquo PLoS ONE vol 7 no 8 Article ID e43572 2012
[14] J K Damas A Boullier T Waelighre et al ldquoExpression offractalkine (CX3CL1) and its receptor CX3CR1 is elevated incoronary artery disease and is reduced during statin therapyrdquoArteriosclerosis Thrombosis and Vascular Biology vol 25 no12 pp 2567ndash2572 2005
[15] A M Fong L A Robinson D A Steeber et al ldquoFractalkineand CX3CR1 mediate a novel mechanism of leukocyte capturefirm adhesion and activation under physiologic flowrdquo Journalof Experimental Medicine vol 188 no 8 pp 1413ndash1419 1998
[16] D Moatti S Faure F Fumeron et al ldquoPolymorphism in thefractalkine receptor CX3CR1 as a genetic risk factor for coro-nary artery diseaserdquo Blood vol 97 no 7 pp 1925ndash1928 2001
[17] N Singh N Sinha S Kumar C M Pandey and S AgrawalldquoPolymorphism in chemokine receptor genes and risk of acutemyocardial infarction in North Indian populationrdquo MolecularBiology Reports vol 39 no 3 pp 2753ndash2759 2012
[18] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[19] G K Hansson and A Hermansson ldquoThe immune system inatherosclerosisrdquoNature Immunology vol 12 no 3 pp 204ndash2122011
[20] H Umehara E Bloom T Okazaki N Domae and T ImaildquoFractalkine and vascular injuryrdquoTrends in Immunology vol 22no 11 pp 602ndash607 2001
[21] H Umehara S Goda T Imai et al ldquoFractalkine a CX3C-chemokine functions predominantly as an adhesion moleculeinmonocytic cell line THP-1rdquo Immunology andCell Biology vol79 no 3 pp 298ndash302 2001
[22] L Lasagni M Francalanci F Annunziato et al ldquoAn alter-natively spliced variant of CXCR3 mediates the inhibition ofendothelial cell growth induced by IP-10 Mig and I-TACand acts as functional receptor for platelet factor 4rdquo Journal ofExperimental Medicine vol 197 no 11 pp 1537ndash1549 2003
[23] S Jung J Aliberti P Graemmel et al ldquoAnalysis of fractalkinereceptor CX3CR1 function by targeted deletion and greenfluorescent protein reporter gene insertionrdquo Molecular andCellular Biology vol 20 no 11 pp 4106ndash4114 2000
[24] D H McDermott J P J Halcox W H Schenke et alldquoAssociation between polymorphism in the chemokine receptorCX3CR1 and coronary vascular endothelial dysfunction andatherosclerosisrdquoCirculation Research vol 89 no 5 pp 401ndash4072001
[25] H Umehara and T Imai ldquoRole of fractalkine in leukocyteadhesion and migration and in vascular injuryrdquoDrug News andPerspectives vol 14 no 8 pp 460ndash464 2001
[26] H Fujimoto Y Tanaka Z-J Liu et al ldquoDown-regulation of 1205726integrin an anti-oncogene product by functional cooperationof H-Ras and c-Mycrdquo Genes to Cells vol 6 no 4 pp 337ndash3432001
[27] M Kimoli S Miyakis P Georgakopoulos E Noefytou A DAchimastos and D A Spandidos ldquoPolymorphisms of frac-talkine receptorCX3CR1 gene in patientswith symptomatic andasymptomatic carotid artery stenosisrdquo Journal of Atherosclerosisand Thrombosis vol 16 no 5 pp 604ndash610 2009
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

BioMed Research International 9
risk Moreover CX3CR1 is likely to amplify the Th1 immuneresponse directly related to plaque vulnerability irrespec-tively of the causal agents (ie ox-LDL or Chlamydia) thusstanding out as a potential target in fatal AMI prevention
References
[1] A I Gotlieb ldquoAtherosclerosis and acute coronary syndromesrdquoCardiovascular Pathology vol 14 no 4 pp 181ndash184 2005
[2] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[3] P Fraticelli M Sironi G Bianchi et al ldquoFractalkine (CX3CL1)as an amplification circuit of polarized Th1 responsesrdquo Journalof Clinical Investigation vol 107 no 9 pp 1173ndash1181 2001
[4] R Bonecchi G Bianchi P P Bordignon et al ldquoDifferentialexpression of chemokine receptors and chemotactic respon-siveness of type 1 T helper cells (Th1s) and Th2srdquo Journal ofExperimental Medicine vol 187 no 1 pp 129ndash134 1998
[5] J F Bazan K B Bacon G Hardiman et al ldquoA new class ofmembrane-bound chemokine with a CX3C motifrdquo Nature vol385 no 6617 pp 640ndash642 1997
[6] C Murdoch and A Finn ldquoChemokine receptors and their rolein vascular biologyrdquo Journal of Vascular Research vol 37 no 1pp 1ndash7 2000
[7] C Murdoch and A Finn ldquoChemokine receptors and their rolein inflammation and infectious diseasesrdquo Blood vol 95 no 10pp 3032ndash3043 2000
[8] C Combadiere K Salzwedel E D Smith H L Tiffany E ABerger and PMMurphy ldquoIdentification of CX3CR1 A chemo-tactic receptor for the human CX3C chemokine fractalkineand a fusion coreceptor for HIV-1rdquo The Journal of BiologicalChemistry vol 273 no 37 pp 23799ndash23804 1998
[9] G A Chapman K E Moores J Gohil et al ldquoThe role offractalkine in the recruitment of monocytes to the endothe-liumrdquo European Journal of Pharmacology vol 392 no 3 pp189ndash195 2000
[10] T Kasama K Wakabayashi M Sato R Takahashi and TIsozaki ldquoRelevance of the CX3CL1fractalkine-CX3CR1 path-way in vasculitis and vasculopathyrdquo Translational Research vol155 no 1 pp 20ndash26 2010
[11] M Garcıa-Alvarez J Berenguer M Guzman-Fulgencio et alldquoHigh plasma fractalkine (CX3CL1) levels are associated withsevere liver disease inHIVHCVco-infected patients withHCVgenotype 1rdquo Cytokine vol 54 no 3 pp 244ndash248 2011
[12] P Lesnik C A Haskell and I F Charo ldquoDecreased atheroscle-rosis in CX3CR1-- mice reveals a role for fractalkine inatherogenesisrdquo Journal of Clinical Investigation vol 111 no 3pp 333ndash340 2003
[13] M Stolla J Pelisek M-L von Bruhl A Schafer V Barockeand P Heider ldquoFractalkine is expressed in early and advancedatherosclerotic lesions and supports monocyte recruitment viaCX3CR1rdquo PLoS ONE vol 7 no 8 Article ID e43572 2012
[14] J K Damas A Boullier T Waelighre et al ldquoExpression offractalkine (CX3CL1) and its receptor CX3CR1 is elevated incoronary artery disease and is reduced during statin therapyrdquoArteriosclerosis Thrombosis and Vascular Biology vol 25 no12 pp 2567ndash2572 2005
[15] A M Fong L A Robinson D A Steeber et al ldquoFractalkineand CX3CR1 mediate a novel mechanism of leukocyte capturefirm adhesion and activation under physiologic flowrdquo Journalof Experimental Medicine vol 188 no 8 pp 1413ndash1419 1998
[16] D Moatti S Faure F Fumeron et al ldquoPolymorphism in thefractalkine receptor CX3CR1 as a genetic risk factor for coro-nary artery diseaserdquo Blood vol 97 no 7 pp 1925ndash1928 2001
[17] N Singh N Sinha S Kumar C M Pandey and S AgrawalldquoPolymorphism in chemokine receptor genes and risk of acutemyocardial infarction in North Indian populationrdquo MolecularBiology Reports vol 39 no 3 pp 2753ndash2759 2012
[18] A Mauriello G Sangiorgi S Fratoni et al ldquoDiffuse and activeinflammation occurs in both vulnerable and stable plaques ofthe entire coronary tree a histopathologic study of patientsdying of acute myocardial infarctionrdquo Journal of the AmericanCollege of Cardiology vol 45 no 10 pp 1585ndash1593 2005
[19] G K Hansson and A Hermansson ldquoThe immune system inatherosclerosisrdquoNature Immunology vol 12 no 3 pp 204ndash2122011
[20] H Umehara E Bloom T Okazaki N Domae and T ImaildquoFractalkine and vascular injuryrdquoTrends in Immunology vol 22no 11 pp 602ndash607 2001
[21] H Umehara S Goda T Imai et al ldquoFractalkine a CX3C-chemokine functions predominantly as an adhesion moleculeinmonocytic cell line THP-1rdquo Immunology andCell Biology vol79 no 3 pp 298ndash302 2001
[22] L Lasagni M Francalanci F Annunziato et al ldquoAn alter-natively spliced variant of CXCR3 mediates the inhibition ofendothelial cell growth induced by IP-10 Mig and I-TACand acts as functional receptor for platelet factor 4rdquo Journal ofExperimental Medicine vol 197 no 11 pp 1537ndash1549 2003
[23] S Jung J Aliberti P Graemmel et al ldquoAnalysis of fractalkinereceptor CX3CR1 function by targeted deletion and greenfluorescent protein reporter gene insertionrdquo Molecular andCellular Biology vol 20 no 11 pp 4106ndash4114 2000
[24] D H McDermott J P J Halcox W H Schenke et alldquoAssociation between polymorphism in the chemokine receptorCX3CR1 and coronary vascular endothelial dysfunction andatherosclerosisrdquoCirculation Research vol 89 no 5 pp 401ndash4072001
[25] H Umehara and T Imai ldquoRole of fractalkine in leukocyteadhesion and migration and in vascular injuryrdquoDrug News andPerspectives vol 14 no 8 pp 460ndash464 2001
[26] H Fujimoto Y Tanaka Z-J Liu et al ldquoDown-regulation of 1205726integrin an anti-oncogene product by functional cooperationof H-Ras and c-Mycrdquo Genes to Cells vol 6 no 4 pp 337ndash3432001
[27] M Kimoli S Miyakis P Georgakopoulos E Noefytou A DAchimastos and D A Spandidos ldquoPolymorphisms of frac-talkine receptorCX3CR1 gene in patientswith symptomatic andasymptomatic carotid artery stenosisrdquo Journal of Atherosclerosisand Thrombosis vol 16 no 5 pp 604ndash610 2009
Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom

Submit your manuscripts athttpwwwhindawicom
Stem CellsInternational
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Disease Markers
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation httpwwwhindawicom Volume 2014
Immunology ResearchHindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttpwwwhindawicom Volume 2014
Parkinsonrsquos Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttpwwwhindawicom





























