-
8/2/2019 Reporting Incidents
1/6
-
8/2/2019 Reporting Incidents
2/6
adverse event rqork, these proba-bly represem only a fmction of
thesedo us ad verse even& e nco unteredby provide rs A recent
review articleI121 found that between 3% and11% of hospita l ad
missions c ould beathibuted Io a dve rse drug reac tions.only ab
out 1% of serious events arerepotted to the FDA, ac co rding toone
study 113).There are probab ly several rea-sons why same selious
events arenot reported to e ither the FDA or themenufechne r.
FitsI, when co nkontedwith an unexpec ted outcom e o ftrea
tmen& physt&ns ma y not con-sider drug-tnduced or
device-in-duc ed d&ease. but rather c onsiderthe event to be
related to the c ourse0fIhedfsease.Unforhmately, thts may be duo
IOthe limited Im ining med ica l studentsreceive n dnical
pharmacokgy andtherapeutics A 1985 survey of U.S.med ica schools
found tha t only 14%of them ha d requlwd ca uses in co re&Us
end prindples of therape uticde-cl&n maldng and c linfcal
phatma-co logy. Of the rema inder. 87%taught only a few houn of
&&alpharmac ology, and most of theteaching cxc uned in the
early yearsof medtcalba lning (14).Another factor Inhibiting p
hysicffn
~hk otti& w preped by Dr . Da&dKe.%!er of he FDA for he
workingGroup.Leaders4 the WorkingGm,,,lncll&dehe fouo
urirw:Shemn
repotting is hat it is not an ingrainedprac tice-- it is not in
the cultxe ofU.S. medic ine to notify the FDAabout adverse events
or productprob lems. In other co untries such esthe United Kingd om
, adverse dntgreporting is more frequent 115). Apa tchwo rk of
repoting forms andsystem s ma y ma ke it d ifficult to filerepo rts
in the United States and m aydisc ourage even the most c
ons&n-tious professionals. Finally, physi-cians may be unclear
as to what a d-verse reac tions should be reported tothe FM.
Mindful of these problems, theFDA has co mp leted an overhaul
ofthe adverse event reporting systemWe are anno unc ing our new
systemcalled MEDWatc h: The FDA Med ialProducts Reporting Program.
(Ad-vase OV~IMSaswci&d v.& vac cineswill continue to be
repx ted throughthe Vac cineAdverse Event ReportingSystem . a joint
p rog ram of the FDAend the Centers for Disease Controlend
Prevention (9).)
This new system enc ourag eshealth care professionals to
regardrepa ting as a fundamental profes-sional and public heeith
reqmnsibil-ity. It was deve loped with the enthu-siastic SuwxI of
the med ica l co m-munity, and its succ ess till dependon close
coop.mtion amongheFDA, the med ical co mmunih). andindushy to
identify and rep&t ed-verse events and p roblems with med-ica
tions and devic es.
The FDA rec c@zes tha t the c on-fidentlalky of the identities
of bathprovide rs who repat ad verse even&and pa tients is an
impo rtant co nce rnof hea lth professiona ls. To enc our-ag e
reporting. the FDA ca refully pro-teck the identities of pm vide rS
whoreport and p&ants co ntained n FDArecords and w ill no t
release suc h in-formation to the public. UnforIu-nately. doting
the c ourse of lit&at&ma nufac turers have increasinglybeen
asked to reveal Ihe identities ofthose reporting adve rse events
end ,in some c ases. even the identitla ofpa ttents. The FDA b
elieves that
ma intaining Ibe c onfidentiality ofthese indiv iduals is
extreme ly irop or-ten< and t hm participa ted n a nomher of co
urt - vigorously opp os-ing release of the na mes of those in-volve
d in a dverse event reports. Todate, we have been successful inma
intaining he c onfidentiality of &iiinforma tion in all the ca
ses n whic hwp have been involved. Neverthe-less, we a r e
considering whether ad-diiorlal ac tions may be ap propriateto
further strag then our ab ility tosafeg uard the co nfidentiality
of thisinformation.
Our goa l in introduc ing MED-Watch is to underscore the
rerpons-bility of p roviders to identify and re-po rt ad verse
events that m ay be re-lated to FDA-reg ulate d prod uc ts. Tothat
end . we want to 1) maket easierfor p roviders to repo rt s0riou.s
events,21 make it c lear to physicians andothers what tvpes of rep
orts the FDAwants to receive. 3) mo re widely d ls-semlna te
informa tion o n the meactionshathave esultedromd-verse event and
product p roblem re-po ting. and 41 increase physicianunderstanding
and awareness ofdrug- and de&e-induc ed disease.
How TO REFaRTUnder the MEDWatc h p- m. thesepa rate o rms
previously used to re-port adverse dmg reactions, drugquality
product problems, devicequality product problems, and ad-verse reac
tions to medic al devic eshew bee n co ns&lad into a
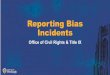
single,one-pa ge reporting form for healthpro fessionals IPIgure
1). This formca n alzo be used to rqm;: pmb lemswtth other
FDA-requlated pmducs.such as d ietary supp lements, cosmet-ics,
medic al ood s. and infen! fonnu-las (Tab le 1).
In a ddition to ma ktng reportingeasier for providets. using one
formfor both device and dtus mob lemsshould help the health ca~ecom
mu-nitv Io detec t and the FDA Io inves-@me, ad verse events.
One exam ple of how this form
&weal d Nurse- w . Vd. 39, No. 6. Novemb aKkce mber 1994
-
8/2/2019 Reporting Incidents
3/6
FIGURE 1.The MEDWatchunifiedreporting orm
404
-
8/2/2019 Reporting Incidents
4/6
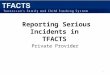
TABLE 1Advice ab out Voluntary Repo rting*
pmlbngedl
Reporteven f:. Youre not certain he productcaused he event. You
dcnt have all the detir
How to report:. Just P in the s&ions that ap ply oyour
repcrt. use sec tion c for all produc tsexceMmedical evices
Confidentiality: The pabents idenhty isheld in strict confidence
by FDA andprotected to the fullest extent of thelaw. The reponerr
idenhty may beshared wit,, the manufacturer unlessrequested
othenvise However, FDA tillnot disclose he reporters dentity
ii,response o a rquen ham the public.purwant to the Freedom of
InformaSar,*_.
. Repon either 1 FDA or themanufacnirer (or both)lmpatant
numbers.. I-800.FDA-0178 to FAX rep+,,. I-800.FDA-7737 to report
bymodem. I-800.FDA~l088 for more
. 1-800-822-7967 or a AERSformfor vaccinesIf your repoit wolves
a seriousadverreevent with a dewce and it occuned in afacility
outside a doctois office, thatfacility may be legally required to
reportto FDA antior the manufacturer Pleasenotify the person in
that facihtywhowould handle such repotting.
might facilitate investiga tion wa s theFDAs diswvey that the
latex-c uffedba rium enema tips used to pa formma ny ba rium
&ma p&edureswxmk ed life-threatenins affemk re-&INS in
som e pa ti& (41. Whenthe problem was first
recognized.pracliticmers typically believed thatp&-a nts - reac
ting to the ba riumsulfate or to o ther med ica tions usedin the
prccedwe. and therefore ad-vase incide nts were inllially repa
teda3 ba dlm l sulfate reac tions to theCenter for Drugs The new
one-pag efour asks reporters to indic ate co n-co mitant devic es
as well a s the suepec t drug a nd other d rugs used in
theprocedures. Using the new formmight have decreasedhe
f&w-up
time required by FDA officia ls, thetime needed to id entify
latex as theproblem. and the time until the med -ical com munity wa
s alerted.
The unified reporting form will beava ilable n several publica
tions, in-cluding the Physicians Desk Refer-ence, the FDA Medical
Bulletin. andAMA Drug Eoaluotions. A 24_hour-a-d ay, 7.da y-a- wek
toll-free nun-her. (800) FDA-1088, is also nowava ilable for p
roviders who want torequest forms or obtain the new FDADesk Guide
to Adverse Event andPmduct Problem Reporting.
Providers till no long er be a-peaed to send different reports
fordevic es and med ica tions 10 differentaddresses at the FDA;
there will now
be a single ma iling add ress for thesereports In add ition, hea
lth profes-sionals will be ab le to report elec tron-ically by com
puter by c alling (800)FDA-7737 and responding to thequestions that
ap pearcm he screen.Reports can be also sent to the FDAby fax.
1800) FDA-0178, a by regular mail using the self-mailer in-dude d
in the form.
In addition to reporting adverseevents to the FDA repo ;ts can
besent to ma nufac turers, whic h a re re-quired by law to fotward
reports tothe FDA l10.111. If the event has oc -curred n a health
ca re zxilihl. ravxtsof problems with med ical de&esshould also
be filed with that fac ility,which legally must report
deviceproblems to the FDA and/or themanufacturer Ill).
The Joint Commission cmAcaed-Nation of Hea lthcare
Organizationsalso has standards for monitoringand reporting adverse
medicationand deviceevenis (161. Individua l n-stih~tians may have
their own pnxe-dures and guide lines for monitoringand rep&ing
ad verse ever& w ithinthe in&it&lo& physicians ca n
ob tainthat information from the pharmac yand therapeutia com
mittee for theinstitutional dsk m ana ge r at their
in-stihdion.
WHAT TO RKORTPhystciansshould report when thereis a suspicion
that a drug or devicemay be related to a smious adverseeffect they
are not expected to es-tablish the connec6on oreven to waitun6l
evidence seem compelling. Re-ports should be alert of possible
as-sociations. Combined with other re-wrts. follow-un. and
resultsof wide-miolbgic s&es or new &diesundertaken. the
FDA can evaluatethese initial suspicions.
On the other hand, the FDA doesnot went pwidezs to report
everyadverse reaction observed; thiswould Dot be prac tica l or the
pract-tioner or useful to the FDA. TheFDAS gall is to increase
reporting
-
8/2/2019 Reporting Incidents
5/6
of serious events, not all adverseevents Whet should be reported
arethose cases in which the Physiciansospeck hat e FDA-regulated
prod-uct was assakted with a seriousout-come-death, a
life-threatening con-dition, initial or prolonged
hospital-k&ion, disability, or congenitalanomaly, or when
intervention wasrequired to prevent permanent im-pamwnt or
damage.Although traditionally problemswith devices are associated
withproduck that are defective or mal-fontion, adverse evenk can
occurwith e device eve when no malfunc-tion or defect k recognized,
for ex-ample, hypersensitivity o latex (4) ordtalyzer germicides
(17).
Especially important to report areadverse effeck from
medlcattons ordevices hat have been on the marketfor a relatively
short time-about 3years or &-because that is whenthe most
critical problems are dkcov-ered. Because most sertous adversewenk
are obsenred in the hospitalsetting (18), pi-actitioners should
beespecially diligent about reportingthese events.The FDA should
also be informedpromptly of product quality problemssuch as
defective devices, inaccumteor unreadable product labeling,packwpng
or product mix-up, con-Laminationor stebilitv rrroblem4.
andparticulateatter n-i;jeaable prod-ucts. In 1990, a total of 38
drug re-calls resulted from reporting of suchproblems (19).
Althoush vhammciskbr isk managersare oiien the ones ina position to
obsewe these problems,physicians who become aware ofsuch problems
should bring them tothe FDAs attention by calling (800)FDA-lo%3 and
submittlnq a report.One recent example 0% he impor-knee of thtt
type of report is the pas-sible link reported between hyper-kelemk
observed in two patients in amedica! center intensive care unitand
two enteral feeding products.The universitys laboratory
analysisdemonstrated that the pmduck hada potassium content about
twice that
specified on the t&l. The FDA fol-low-up of this report
revealed that ellproduct lines of the maufxtorercontained
potasstumvalues of 150%to 250% oftheeclared mnout Be-cause these
pmduck are frequentlyused as a sole sorw of nutrition,and sometimes
in patients with cam-promked renal function, the FDA ini-tiated a
recall of the product
PROVfDE PHYSICLANrn~oubworvMEDWatch k aimed et facilitating
re-porting by providers. but we alsowant to better inform providers
aboutregulatory actions taken by the FDAI rosponso to reports. we
believethis information will not only be use-ful to physicians ad
others, but thatit wtll eke encourage serious adverseevent
reporting by demonstreting thevalue of the information. The FDAwill
therefore take a more aggressivestance n reporting back to
providers.
ENHANCE PHYSICfANUNDERSTANDINGAs part of MEDWatch, the FDAhopes
to heighten physlctan aware-nessof drug- and device-fnduced
dk.ease. Our educational effork wfll tn-crude a focus on issues
such as theimportance of the problem, mecha-nkms of adverse drug
and device re-actions, and how to evaluate possibleadverse events.
As part of that effortwe plan to hold a conference forhealth care
professionals and FDAofftdals to help poise practitioners
torecognize drug- and device-inducedproblems when they occur,
andthereby Increase participation in theMEDWatch program.MEDWatch
is a m~pvrtent pro-gram that we hope will slgntftcantlyimprove ox
ability to monitor thesafety of products we regulate and tot&e
neceeeay actions suirtly and ef-fectively. Perhaps m,st
important,we hope MEDWatch will encouragean increased sense of
responsibilityamog physicians and other health
cae providers about reporting ad-verse evenk and product
problems.We are eager to work closely with themedical community to
ensure theprogmls scce..%.
REFERENCES1. Peck CC. Temple R, CoihnsJM.Understanding oNeqUeceQ
f COcuI-rent therapies.JAMA 1993;26931550-52.2. Honig PK, Wortham
DC, LmantK. Conner DP. MutltnJC.
CantilanaULTerfenadine-ketoconazole nteraction:pharmacohie;:i: 2-d
etrtrocardto-~~~iwquences. JAM4 lS93:2w3. Rossi AC, Bosco L, Fatch
GA,Tanner A, TemPteR. The importaxe ofadverse paction qorLin9 by
Physktrmr
swrofen and the tlank pain syndrome.JAMA 1988259:1~.4. Stehltn
D. When rubber rubs thewrong way. FDA Gasumer. 199226:17-21.5. Gelb
LN. ed. Denoea of ACE to-htbiton dudng &od &I third
tttmes.krr of preqeancy.FDA Mod ButI 1992:222.b. Rh&stetn PH.
Rep&kg of ad--eWlb:ekqrtoportmaacoangdrugwfety. Am Fern Phys.
1992;46:873-7.5.7. Rerr RI. PeeblesCf_ Rum@ \;Ckhs RL, Ten EM.
Antinudoareutoaott.baiks In women with &one breast m-Ptenb
Lancet 1992$?&134&7.8.DennRW.HaUPN,Rhc0CTKUreart imptent
matertats: sense andsafe&t.Br J PtastSwg 1992:4&31%.21.9.
Nightin& SL. New sqtem o,reporttng of vaccine adverse
evenk.JAM4 1%xXx4:2863.
10. JohnsonJM. Bamh D. A reviewof pastmarketingadveme drug
ewxrt.
11. Medkal Devkes;Me&al Dwke.User Fe&y. mbutor, and
Menukc-turersRe~orKg,CetiftcaUon,and Rss_istmtion.Ro&viUe,
t.fd: Dept ot Healthand Human Sewices. Fmd and DmaAdmkiskatio:
lY91:Mx)2Moa39.2iCFR parts SO3 and SO7 (docket No.YlN-0295).
12. Beard K Adwax reactiwa as a
-
8/2/2019 Reporting Incidents
6/6
causeof hospital admissions n tbe aged. 15. Neirenberg DCU
Clinical pharma- dialyzer germicides. FDA Med Bull.Drugs Agag.
1992:2%5&67. C0lOg.j ,nEtNCbo lrrr all medxal stw 1993.23:7.13.
Scott HD. Rasenbaum SE. waters denb Gun Pharm Ther. :986.40. %?%W
et al Rhcde Island plwiciws recog- 87. 18. Kennedy DL. Johnsan JM.
Night-nition and reporting of adverse drug re- ingale SS.
Monitollng of adverse d;ug&ions. R IMed J 1987;70.311-16. 16.
Accredltabo Manuai. 1993 Oak- events in hospitals. JAMA
1991:2x%brook Tenace. 111 oint Comm~~on on 2878.14. Gdfffn JP,
Weber JCP Voluntatysystems of adverse reaction repoting.
Accreditation of Healthcare Organiza-tions: 1993. 19. Eca&r G.
Goeecb R ?.ionitoangpar, I,. Adv Drug React Ac Pas Rev drug product
quality. Am Pharm1986;1:w5. 17. Gelb LN. Precautions needed far
1992.NS32:47-50
Dater to RememberAnnual Meedngsd theAmerican College of
Nurse-Midunves
15% June l&20Palm Spring. California
1998 May 22-28San Francis.% California