Embed Size (px)
Citation preview

IN CRITICAL CONDITION:
THE URGENT NEEED TO REFORM THE
INDIAN HEALTH SERVICE’S
ABERDEEN AREA
REPORT OF
CHAIRMAN BYRON L. DORGAN
TO THE
COMMITTEE ON
INDIAN AFFAIRS
ONE HUNDRED AND ELEVENTH CONGRESS
SECOND SESSION
_________________
DECEMBER 28, 2010 _____________________
PRINTED FOR THE US E OF THE COMMITTEE ON INDIAN AFFAIRS

Page 2 of 68
TABLE OF CONTENTS
Relevant Acronyms ........................................................................................................................... 3
Introduction...................................................................................................................................... 4
Background ...................................................................................................................................... 4
Findings ............................................................................................................................................ 5
Transfers, Details and Reassignments ...................................................................................... 6
Employees Placed on Lengthy Periods of Administrative Leave ................................................ 7
Increased Equal Employment Opportunity Complaints.............................................................. 9
Increased Employee Grievances and Other Filings .................................................................. 13
Missing or Stolen Narcotics and Other Controlled Substances ................................................. 15
Substantial Diverted Health Care Services.............................................................................. 19
Mismanagement of Contract Health Service Funding .............................................................. 22
At-Risk: Facility Accreditation or Certification....................................................................... 23
Expired Health Care Provider Licenses and Other Credentials ................................................. 27
Disciplinary Actions Taken Against Provider Licenses ........................................................... 29
Employee Misconduct and Poor Performance ......................................................................... 30
Hiring Excluded Employees or Those with Unsuitable Criminal Records ................................. 36
Mismanagement of Third Party Billing .................................................................................. 38
Staff Vacancies..................................................................................................................... 40
Use of Locum Tenens ........................................................................................................... 42
Agency Directives Inhibit Employee Communications with Congress...................................... 42
Initiatives to Address Aberdeen Area Deficiencies .......................................................................... 44
Indian Health Service‟s Initiatives to Address Aberdeen Area Deficiencies .............................. 44
Department of Health and Human Service‟s Initiatives to Improve Performance
in the Aberdeen Area ............................................................................................................ 46
Appendix ........................................................................................................................................ 47
Exhibit A: Submitted Testimony of the Director of Indian Health Service ................................ 47
Exhibit B: Submitted Statement for the Record of the
Laborers‟ International Union of North America..................................................................... 59
Exhibit C: Belcourt Service Unit Diversions ........................................................................... 64
Exhibit D: Employees Placed on Lengthy Administrative Leave Hours .................................... 65
Exhibit C: Providers with State Licensure Problems................................................................ 67

Page 3 of 68
RELEVANT ACRONYMS
AAOPD: Aberdeen Area Office Personnel Director ACLS: Advanced Life Support
ADR: alternative dispute resolution AO: Administrative Officer ASFR: Assistant Secretary for Financial Resources
CAP: Corrective Action Plan CCNACI: Child Care National Agency Check and Inquiries
CD: Clinical Director CDA: community development agency CEO: Chief Executive Officer
CHS: Contract Health Services CMS: Centers for Medicare and Medicaid Services
COP: conditions of participation CPR: cardiopulmonary resuscitation CSRA: Civil Service Reform Act of 1978
DEA: Drug Enforcement Administration DON: Director of Nursing
DPHN: Director of Public Health Nursing EEO: Equal Employee Opportunity EEOC: Equal Employment Opportunity Commission
EMLATA: Emergency Medical Treatment and Active Labor Act ESC: Evidence of Standards Compliance
FAD: Final Agency Decision FBI: Federal Bureau of Investigation FY: Fiscal Year
HHS: Department of Health and Human Services IHS: Indian Health Service
JC: Joint Commission LEIE: List of Excluded Individuals/Entities MIR: Management Implication Report
MSPB: Merit Systems Protection Board NPDB: National Practitioner Data Bank
NRP: Neonatal Resuscitation Program OGC: Office of General Counsel OIG: Office of Inspector General
PMAP: Performance Management Appraisal Program RMOs: responsible management officials
RPMS: Resource and Patient Management System ULP: Unfair Labor Practice

Page 4 of 68
INTRODUCTION
On June 23, 2010, Chairman Byron Dorgan initiated a formal investigation of the Indian Health Service‟s (IHS) Aberdeen Area (hereafter “the Area”) in response to years of hearing
from individual American Indians/Alaska Natives, Indian tribes and IHS employees about substandard health care services and mismanagement. Chairman Dorgan received complaints about Aberdeen Area IHS-run facilities plagued by frequent reduced or diverted services,
mismanagement, poor performing employees, lack of employee accountability, and malfeasance. These conditions negatively impact the care provided to individuals and produce a work
environment riddled with waste, fraud and abuse.
The Chairman initiated an investigation in order to identify these problems and their causes.
The investigation included: reviewing over 140,000 pages of documents submitted by IHS and the Department of Health and Human Services‟ Office of Inspector General (OIG), visiting three
IHS service units, meeting with tribes and interviewing individual IHS employees. In addition, nearly 200 individuals contacted the Committee regarding mismanagement of facilities in the Area. This report provides an overview of the Chairman‟s investigative findings.
On September 28, 2010, the Committee held a hearing on its investigative findings. During
the course of this hearing the Chairman identified deficiencies in management, employee accountability, financial integrity, and oversight of IHS' Aberdeen Area facilities. The Chairman determined that these weaknesses have contributed to reduced access and quality of health care
services available to patients served in the Area.
The Committee was scheduled to have a subsequent hearing on December 8, 2010 regarding IHS‟ initiatives to address the findings of the Chairman‟s investigation. However, due to United States Senate scheduling conflicts the hearing was canceled. As a result, provided in the
Appendix of this report as Exhibits “A” and “B,” respectively, are the testimony submitted by Dr. Yvette Roubideaux, Director of IHS, and the statement for the record submitted by the
Laborers‟ International Union of North America (LIUNA), a union that represents the majority of non-management civil service IHS employees.
BACKGROUND
The Aberdeen Area is comprised of 20 IHS and tribally-managed service units.1 The Area employs 1,955 individuals and has an annual budget of $293 million.2 The Area also has two urban programs that provide services in five locations ranging from community health to
comprehensive primary health care services.
The Area serves 18 Indian tribes in four states: South Dakota, North Dakota, Nebraska, and Iowa. The annual estimated workload for the Area includes: 3,475 inpatient admissions, 859,163 outpatient visits and 77,039 dental visits.3
1 Indian Health Serv ice, “Aberdeen Area Administrative Review,” April 2010 at 1.
2 Id at 1.
3 Ibid.

Page 5 of 68
The Majority Staff concentrated the investigation on the following nine IHS-run service units and facilities in the Aberdeen Area:
Belcourt Service Unit of North Dakota (Turtle Mountain Band of Chippewa);
Fort Totten Health Center of North Dakota (Spirit Lake Sioux Tribe);
Fort Yates Service Unit of North Dakota (Standing Rock Sioux Tribe);
Winnebago Service Unit of Nebraska (Winnebago Tribe of Nebraska);
Sisseton Service Unit of South Dakota (Sisseton-Wahpeton Oyate Tribe);
Pine Ridge Service Unit of South Dakota (Oglala Sioux Tribe);
Rapid City Service Unit of South Dakota (urban Indian health facility);
Rosebud Service Unit of South Dakota (Rosebud Sioux Tribe); and,
Aberdeen Area Office, located in Aberdeen, South Dakota.
FINDINGS
The investigation identified mismanagement, lack of employee accountability and financial
integrity, as well as insufficient oversight of IHS' Aberdeen Area facilities. These issues impact overall access and quality of health care services provided to Native American patients in the
Aberdeen Area. Many of these issues may stem from a greater lack of oversight by the Area office and IHS headquarters fostering an environment where employees and management are not held accountable for poor performance.
Provided below is a detailed summary of the findings of the investigation. In brief, the
Chairman found:
Over the course of the last ten years, IHS repeatedly used transfers, reassignments,
details, or lengthy administrative leave to deal with employees who had a record of misconduct or poor performance.
There were higher numbers of Equal Employee Opportunity (EEO) complaints in the
Aberdeen Area in comparison to the entire IHS, as well as insufficient numbers of EEO counselors and mediators.
Three service units have a history of missing or stolen narcotics and nearly all facilities failed to provide evidence of performing consistent monthly pharmaceutical audits of
narcotics and other controlled substances.
Three service units experienced substantial and recurring diversions or reduced health care services from 2007 to 2010, which negatively impacts patients and quickly diminishes limited Contract Health Service (CHS) funding.
Mismanagement of CHS program funding has resulted in some facilities having funding
surpluses and the transfer of dollars to likely non-CHS programs.
Five IHS hospitals are at risk of losing their accreditation or certification from the Centers for Medicare and Medicaid Services (CMS) or other deeming entities. Several

Page 6 of 68
Aberdeen Area facilities were cited as having providers with licensure and credentialing problems, Emergency Medical Treatment and Active Labor Act (EMTALA) violations,
emergency department deficiencies or other conditions that could place a patient‟s safety at risk.
IHS lacks an adequate system to detect instances of IHS health care providers whose
licenses have been revoked, suspended or under other disciplinary actions by licensing boards.
IHS health care providers treating patients with expired state licenses and/or other certifications on numerous occasions, which violates federal regulations and internal IHS
policies.
Particular health facilities continue to have significant backlogs in posting, billing and
collecting claims from third party insurers (i.e., Medicare, Medicaid and private insurers). One facility repeatedly transferred its third party payments to other facilities in the
Aberdeen Area.
There were lengthy periods of senior staff vacancies in the Clinical Director and Chief Executive Officer positions, resulting in inconsistent management and leadership at
Aberdeen Area facilities.
The use of contract providers (locum tenens) is costly ($17.2 million in the last three
years). While the overall cost of contract providers has decreased in comparison to last year, two facilities have increased their locum tenens expenses this year.
IHS policies and directives discourage employees from communicating with Congress.
Transfers, Details and Reassignments. There are a number of federal regulations governing the transfer, detail and reassignment of employees. Specifically, a federal agency may appoint
by transfer to a competitive service position, without a break in service of a single workday, a current career or career-conditional employee of another federal agency.4 A detail is a temporary
assignment to a different position for a specified period, with the employee returning to his or her regular duties at the end of the detail.5 A reassignment is the “change of an employee, while serving continuously within the same federal agency, from one position to another without
promotion or demotion.”6
The investigation revealed that between 2002 and August 2010 there were a total of 364 reassignments, 235 details and 31 employee transfers. Additionally, the available documentation suggests that employees who filed EEO complaints were more likely to be detailed or reassigned
4 Office of Personnel Management‟s (OPM) “Guide to Processing Personnel Action,” (Processing Guide); 5 U.S.C.
§ 3503; and, 5 CFR § 351.302. 5 5 U.S.C. § 3341; OPM Processing Guide.
6 5 CFR § 210.102(b)(12); OPM Processing Guide. Reassignment to a position with more promot ion potential than
the present position requires competition under the agency's merit staffing plan.

Page 7 of 68
compared to those that did not. The following is a list of our key findings on the transfer, detail and reassignment of employees.
Reassignments:
o Nearly 11 percent of total reassigned employees had filed an EEO complaint (formal or informal).
o Nearly 8 percent of the employees were placed on administrative leave prior to reassignment.
o About 3 percent of the employees had filed a grievance or other filing prior to their
reassignment.
Details: o About 13 percent of the total detailed employees had filed an EEO complaint (formal
or informal).
o No employees were placed on administrative leave prior to being detailed. o 6 percent of the employees had filed a grievance or other filing prior to being
detailed.
Transfers:
o 3 percent of the total transferred employees had filed an EEO complaint (formal or informal).
o 3 percent of the total transferred employees were placed on administrative leave prior to transfer.
o No employees had filed a grievance prior to transfer. Information the Chairman received only includes the employees who were transferred,
detailed or reassigned to facilities located within the Aberdeen Area; it does not provide information on individuals employed in the Area but who were transferred, detailed or
reassigned to facilities outside the Area. Furthermore, the Chairman requested that IHS submit all letters pertaining to a direct reassignment in the last 10 years. IHS only submitted 8 reassignment letters, despite IHS data indicating that it performed over 364 reassignment actions
pertaining to 306 employees in the Aberdeen Area since 2002.
Employees Placed on Lengthy Periods of Administrative Leave. Through the investigation it was determined that 176 employees were placed on paid administrative leave between 2005 and 2010 in the Aberdeen Area. Leave for any individual varied greatly, ranging from eight hours to
over eight consecutive months.
The IHS defines administrative leave as an excused absence from duty, administratively authorized, without loss of pay.7 Administrative leave is “granted at the discretion of the manager, or the official with delegated authority, for reasonable periods of time for a variety of
special situations.”8 Situations where excused absence may be authorized include, but are not limited to, voting and registration, military service registration, blood donations, and inclement
weather.
7 IHS, Orientation Handbook, August 10, 2010 at 72.
8 Ibid.

Page 8 of 68
IHS policy does not expressly cite administrative leave for the purposes of a pending personnel investigation, but as described further below, numerous instances were found of
employees being placed on administrative leave pending the performance of an investigation.
The use of administrative leave has grown significantly over the past few years. The data submitted by IHS demonstrates that in 2005 only eight employees were placed on administrative leave, due to “management election” or for training purposes. However, by 2009 that number
increased to 35 employees, during which time several employees were placed on leave multiple times. One employee was placed on administrative leave for at least 1,200 hours. This trend has
not changed in 2010. As of September 2010, 34 employees have been placed on leave with an average length of 97.4 hours.
The following chart provides the number of employees on administrative leave and the average length of leave from January 2005 to September 2010 for the facilities the investigation
focused on in the Aberdeen Area.
The most common reason for placing an employee on administrative leave is a pending
investigation of the employee or management election, meaning it was the supervisor‟s determination to place the employee on administrative leave.
Further, the frequent use of administrative leave for purposes of a pending investigation may demonstrate unreasonably lengthy investigations. Attached as “Exhibit C” in the Appendix is a
list of particular employees with the lengthiest administrative leave hours. Overall, the 11
FACILITY NUMBER OF
EMPLOYEES ON
ADMINISTRATIVE
LEAVE
AVERAGE LENGTH OF
ADMINISTRATIVE
LEAVE
1/2005 – 9/2010 1/2005 – 9/2010
Aberdeen Area Office 22 1.4 Weeks
Belcourt 22 6 Weeks
Fort Totten 5 1.8 Weeks
Fort Yates 8 1.8 Weeks
Kyle 3 1.3 Weeks
Lower Brule 4 7.8 Weeks
McLaughlin 1 1.8 Week
New Town 6 4 Days
Pine Ridge 23 2.2 Weeks
Rapid City 24 1.5 Weeks
Rosebud 26 1.4 Weeks
Sisseton 11 4 Weeks
Wagner 1 1 Week
Winnebago 13 3 Weeks
TOTAL 169 2.6 Weeks
(Average)

Page 9 of 68
employees who were placed on administrative leave due to pending investigations between 2005 and 2010 averaged over 560 hours of leave (more than 4 ½ months).
One employee at Sisseton Service Unit‟s Woodrow Wilson Keeble Memorial Health Care
Center had the lengthiest consecutive leave period, totaling over eight months in 2009 due to a pending investigation. Specifically, this particular employee was under investigation due to allegations of sexual harassment and creation of a hostile work environment.
The documents submitted by IHS demonstrate that many employees were placed on
administrative leave multiple times. For instance, a senior level employee at Belcourt Service Unit‟s Quentin N. Burdick Memorial Hospital was placed on leave during 12 pay periods in 2009 and one pay period in 2006, totaling nearly six months. IHS‟ documents indicate that the
individual was placed on leave pending an investigation involving allegations of misconduct. Another employee at the same hospital was placed on leave during the course of eight pay
periods in 2006, and 19 pay periods in 2007, totaling over one year. The investigation also revealed that the Area Director failed to remain informed of whether a
subordinate employee was on administrative leave. In this case, during the Committee‟s hearing on September 28, 2010, the Aberdeen Area Director, Charlene Red Thunder, testified that an
Aberdeen Area employee was on administrative leave for over 12 months. After reviewing additional documents that IHS submitted, the Chairman determined that this was inaccurate. It was determined that the employee was not on administrative leave for 12 months, but instead had
taken a combination of personal and sick leave and was assigned to work from home to perform “unclassified duties.” Ultimately, the employee worked from home for 28.5 days in 2009 and
149 days in 2010. However, the IHS failed to have a formal telework agreement with that employee as is commonly required before an employee can work from home for such an extensive period of time.
Increased Equal Employment Opportunity Complaints. The investigation found that the
number of Equal Employment Opportunity (EEO) complaints filed in the Aberdeen Area has increased at a faster rate than for the entire IHS. In addition, certain individuals were repeatedly the primary subject of multiple EEO infractions. Finally, the Chairman identified one instance
where IHS failed to implement its own EEO Final Agency Decision for over seven months.
Filings with the Equal Employment Opportunity Commission (EEOC) generally stem from an informal complaint filed with IHS. Such complaints include allegations involving discrimination against an employee because of the person's race, color, religion, sex (including
pregnancy), national origin, age (40 or older), disability, or genetic information.
Employees in a local facility generally file complaints with their onsite Equal Employment Opportunity (EEO) counselor. Employees are encouraged to resolve their claims through alternative dispute resolution (ADR), such as mediation. EEO mediators or contractors are
utilized during the ADR process. The EEO counselor submits the final report of the EEO complaint to the EEO manager located in the Area Office. If ADR is not effective, the employee
may file a formal complaint with the EEOC.

Page 10 of 68
In addition, IHS recommends that each facility have at least two EEO counselors or more if the facility has greater than 100 employees. Employees volunteer to become EEO counselors as
a part of their collateral duties. EEO counselors are required to receive 32 hours of training prior to assuming counseling duties, as well as eight hours of additional training each year.
Employees can also volunteer to become EEO mediators as part of their collateral duties, and they will accept a case for mediation as their primary workload permits.
The Chairman received information from IHS regarding both formal and informal EEO complaints. The data demonstrates that the Area has experienced an upward trend in EEO filings
and suffers from an inadequate level of trained EEO counselors and mediators. Further, certain employees were the subject of multiple EEO complaints, in which they were alleged to have discriminated against a colleague or subordinate.
The investigation revealed that employees in the Aberdeen Area have filed 222 formal or
informal EEOs from 2000 to July 23, 2010. Further, based upon IHS data from January 2005 to July 2010 there were 53 EEO open cases (matters that had not resolved) and 159 closed EEO cases (matters that had been resolved).
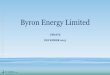
As illustrated in the graph below, IHS data demonstrates that EEOs filed for the Aberdeen
Area as of July 23, 2010 had already surpassed overall filings for the entire IHS in 2009. The Chairman identified that the number of EEOs in the Area increased from six in 2000, 25 in 2005, and 35 in 2009, to 63 as of July 23, 2010. As illustrated in the below graph, although EEO
filings decreased in 2009, filings as of July 23, 2010 nearly doubled.
At certain facilities in the Aberdeen Area, EEO complaints have increased considerably in
the past five years. By far, Belcourt has had the greatest number of EEO filings, totaling 50 over the last five years, escalating from two in 2005 to 15 as of July 23, 2010. The Area Office has
the second highest amount of EEOs as of July 23, 2010, totaling 29. Data for Pine Ridge (28),
0
10
20
30
40
50
60
70
80
90
100
2000 2002 2004 2006 2008 July-2010
EEO Complaints by Year in Aberdeen Area
Aberdeen Area EEO Formal
& Informal Complaints
IHS EEO Complaints

Page 11 of 68
Rosebud (27), and Rapid City (26) demonstrate that the total number of EEOs for these facilities did not lag far behind.
Based upon data received by IHS, the Majority Staff also found the primary reason that
employees in the Aberdeen Area filed EEO complaints was due to gender discrimination, reprisal or retaliation. EEO filings that allege reprisal or retaliation account for 44 percent of all EEO complaints in the past ten years. From 2008 to 2010, the number of EEO complaints based
on reprisal or retaliation was substantially greater than those filed years prior. For instance, in 2005 there were five filings based on reprisal/retaliation; however, by 2008 the number of filings
was 20 and from January 2010 to July 23, 2010 there have been 19. Despite the rising number of EEOs and IHS' recommendation that each facility have a
minimum of two EEO counselors, the Chairman found there was a lack of sufficient EEO counselors and mediators in the entire Area. Specifically, as of September 2010 only 13 certified
EEO counselors and three EEO mediators are employed in the Aberdeen Area. The Area also has only one EEO manager and one EEO specialist located in the Area Office as of September 2010. The Area set a goal of training 15 more EEO counselors by October 2010. However, as of
November 2010 the IHS had not met this goal.
Through the investigation one instance was identified in which the IHS failed to fully implement its Final Agency Decision regarding an EEO complaint filed by an employee at a facility in the Aberdeen Area. On September 18, 2007, an employee filed an EEO complaint
claiming an illegal suspension and ultimate denial of privileges due to their national origin. On April 6, 2009, the IHS determined that the EEO complainant had been harassed, the hospital‟s
medical by-laws were not followed, and derogatory comments were made about the employee‟s national origin. Ultimately, the Agency determined that the employee was exposed to an environment that was “unduly harsh and extreme, bordering on the hellish.”9 One individual
interviewed by the Agency described the work environment at the hospital as “toxic” and further explained that nurses had ignored the EEO complainant‟s pleas for assistance during surgical
procedures. The nurses‟ behavior was ultimately reported to their superiors but “it was ignored.”10 The April 6, 2009 Financial Agency Decision details that the EEO complainant identified three senior level employees as the management officials responsible for creating a
hostile work environment.11
In a subsequent Final Agency Decision dated March 4, 2010, the IHS determined that the EEO complainant should be reinstated to their position at the same Aberdeen Area facility or reinstated at another facility in the IHS system. However, despite several requests from the
complainant and their attorney over a period of 8 months, IHS failed to reinstate the complainant. In addition, the EEO complainant was awarded over $150,000 in equitable relief,
back pay, compensatory damages, attorney‟s fees, and other costs. In November 2010 the Agency began to adhere to its Final Agency Decision by taking proper action to reinstate the complainant.
9 Agency File No. HHS-IHS-0511-2007, April 6, 2009 at 16.
10 Id. at 14.
11 Id. at 10.

Page 12 of 68
The Chairman requested that IHS submit certain documents related to EEO filings in order to identify employees that were the subject of multiple EEO complaints. The Chairman received
documents from IHS relating to 81 of the 159 closed EEO cases from 2005 to 2010. The Chairman determined that 12 employees on two or more occasions were alleged to have
discriminated against their subordinate, colleague or other employee. These 12 employees were the subject of 31 EEO complaints, nine of which were resolved through a settlement agreement and three were adjudicated with a finding of discrimination.
The IHS confirmed to the Majority Staff that it does not have a policy for dealing with
employees who are repeatedly the prime subject of EEO cases where there is a finding of discrimination. IHS‟ policies are limited to requiring EEO office staff to share the findings of discrimination and the named responsible management officials (RMOs) with IHS leadership.
The EEO office advises the named RMOs of the findings and requests that the RMOs take corrective, curative or preventive action to ensure that violations of the law do not reoccur.
Based on the information IHS provided the following are examples of employees that were the subject of multiple EEO complaints.
Employee 1 and 2
Two senior level employees at a facility in the Aberdeen Area were each the subject of
multiple EEO complaints. In two EEO cases both employees were the primary subject of the EEO complaints. As described earlier, one EEO complainant was awarded over $150,000 in damages and other fees due to the hostile environment that was alleged to be created by these
two senior level employees and an additional former employee.12
Another provider at the same facility in the Aberdeen Area identified the same two senior level employees, among others, as the prime subject of an EEO complaint filed on May 15, 2008. On May 14, 2010, the EEO Commission found that the complainant was subjected to a hostile
work environment due to the employee‟s race and was retaliated against for prior EEO activity.13 The Commission noted that the two senior level employees failed to take proper action and
continued to support false complaints made by another employee even after the true facts were ascertained.14 The judge found that when the EEO complainant told one of the senior level employees about the harassment the individual failed to conduct an investigation into the
complainant‟s accusations, and ultimately disciplined the complainant for acts the person did not commit.15 The Commission ultimately awarded the EEO complainant $50,000 in damages.
12
IHS Agency File No. HHS-IHS-0511-2007, April 6, 2009. 13
EEOC No. 443-2010-00153X, May 14, 2010. 14
Id. at 15 – 21. 15
Ibid.

Page 13 of 68
Employee 3
A former senior level employee at a facility in the Aberdeen Area was identified in six
different EEO case files as the official alleged to have discriminated against other employees.16
The alleged misconduct occurred in each of these cases between 2006 and 2008, including during the employee‟s tenure as a senior level official. Ultimately, in five of the six EEO case
files the IHS determined that no discrimination occurred, while the sixth claim was dismissed because the complainant failed to file within the time frame required.
Employee 4
Another former senior level employee at a facility in the Aberdeen Area was the primary subject of alleged discriminatory misconduct on three occasions.17 Two of the three EEO complaints were ultimately dismissed in 2007 and 2008, respectively. The third complaint was
dismissed because the claimant entered into a settlement agreement of non-monetary value.
Employee 5
A former senior level employee at a facility in the Aberdeen Area was named the primary subject of three EEO complaints filed between 2006 and 2008.18 Of the three EEOs filed, no discriminatory act was found in two cases, while the third case was settled and the complainant
was awarded over $22,000.
Employee 6
Another former senior level employee at a facility in the Aberdeen Area was identified in two EEO case files as the official alleged to have discriminated against employees.19 The alleged misconduct occurred in 2007 and 2008, respectively. One EEO claim was dismissed due
to procedural issues, while the second complaint was settled without a monetary award.
Increased Employee Grievances and Other Filings. IHS employees, like other federal employees, may file actions as Merit Systems Protection Board (MSPB) complaints, Unfair Labor Practice (ULP) complaints, or grievances, among other options. ULP complaints include
interfering with or prohibiting union activities, failure to bargain in good faith, position description changes, and terminations. Employees may file grievances due to letters of warning,
reprimands, suspensions, hostile work environments, harassment, and leave restrictions, among others.
16
Report of Investigation, Case No. IHSC-064-06, September 4, 2007; Report of Investigation, September 18, 2007;
Report of Investigation, Case No. IHS-050-06; Report of Investigation, Case No. HHS-IHS-054-2006; Report of
Investigation, Case No. IHS-028-05, August 17, 2005; and, Final Agency Intake Decision, Case No. HHS-IHS-
0251-2007, July 30, 2007. 17
Report of Investigation, Case No. IHS-069-05, April 7, 2006; Report of Investigation, Case No. HHS-IHS-1361-
2008, June 8, 2009; and, Report of Investigation, Case No. IHS-0062-06. 18
Report of Investigation, Case No.HHS-IHS-0226-2008; Report of Investigation, Case No. HHS-IHS-0113-2007;
and, Report of Investigation, Case No. HHS-IHS-0501-2007. 19
Report of Investigation, Case No. HHS-IHS-1361-2008, June 8, 2009; and, Report of Investigation, Case No.
HHS-IHS-0223-2008, August 26, 2008.

Page 14 of 68
The MSPB is an independent, quasi-judicial agency in the executive branch that serves as the
guardian of federal merit systems. The MSPB was established in 1978 and codified by the Civil Service Reform Act of 1978 (CSRA), Public Law No. 95-454. MSPB carries out its statutory
responsibilities and authorities primarily by adjudicating individual employee appeals and by conducting merit systems studies, including hearing and deciding certain discr imination complaints, claims of whistle blowing reprisal, and negotiating and resolving ULPs.
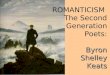
Based upon the information IHS submitted the investigation revealed that of the facilities
reviewed from January 2000 to September 2010, employees filed 354 work force grievances, ULPs and MSPBs at Aberdeen Area IHS facilities (including the Aberdeen Area Office). There were a total of 232 employee grievances, amounting to over 65 percent of all filings. The
following graph is based on data received from IHS.
Aberdeen Area
Employee Work Grievances and Other Filings by Type and Facility:
January 2000 – September 2010
As illustrated above, in comparison to all other IHS service units, the Belcourt Service Unit had the greatest number of employee grievances, ULPs and MSPBs filed (72), accounting for 20
percent of all employee filings in the Area in the last ten years. The overwhelming amount of these filings were employee grievances (38), which included challenging a reprimand, detail,
suspension or absence without leave, as well as reporting harassment. Pine Ridge Service Unit ranked second in employee grievances (39). Similar to Belcourt Service Unit, the majority of Pine Ridge Service Unit‟s filings were employee grievances.
0
10
20
30
40
50
60
70
80
MSPB
ULP
Grievances
Total

Page 15 of 68
The investigation also identified that while certain service units have experienced a higher rate of employee grievances, ULP, and MSPB filings than others, the overall Area has had a
general decrease in these filings since 2004. In 2004 there were 48 filings; by 2008 it had declined to 18; and thus far in 2010 the number has held at 18.
Missing or Stolen Narcotics and Other Controlled Substances. The Chairman found that the frequency of missing or stolen narcotics and other controlled substances varied among IHS
pharmacies. However, at certain facilities substantial levels of missing or stolen narcotics was a recurring issue, while a lack of consistent monthly audits of narcotics was a frequent issue at
others. Moreover, shortfalls in staffing and security deficiencies have contributed to greater amounts
of missing or stolen narcotics at facilities, such as Quentin N. Burdick Memorial Hospital. Without consistent oversight, proper auditing, adequate staffing and sufficient security measures
IHS will be at-risk of continued loss or theft of narcotics and other controlled substances. There is a myriad regulations pertaining to controlled substances and how they should be
handled, recorded, audited and reviewed by IHS pharmacies. There are also additional regulations provided for Schedule II drugs, such as Codeine, Morphine, Hyrdocodone, and
Oxycodone. Primarily, these regulations and guidelines are set forth by the Drug Enforcement
Administration (DEA), HHS, Joint Commission, Centers for Medicare and Medicaid Services (CMS), internal policies of IHS and the state in which the pharmacy is located. For instance, to
be a participating pharmacy, which enables a pharmacy to bill for services rendered to Medicare or Medicaid patients, there must be a current and accurate record of receipt and disposition of all scheduled drugs.20 Furthermore, any discrepancy in the count of scheduled drugs should be
reconciled promptly and abuses and/or losses of controlled substances must be reported.21 Pharmacies must also have an adequate number of personnel to ensure quality pharmaceutical
services.22 According to a 2010 internal IHS review of Aberdeen Area pharmacies an array of problems
have contributed to challenges in managing and curtailing missing or stolen narcotics. 23 In addition, the IHS review indicates that the understaffing of pharmacists, though staffing has
improved from 39 percent ideal staffing in 2006 to 61 percent in 2009, continues to be a contributing challenge.24 IHS also determined in this report that increased prescription volume and medication therapy management, coupled with funding challenges, has resulted in
insufficient accountability of controlled substances.
20
Centers for Medicare & Medicaid Serv ices‟ Condition of Part icipation: Pharmaceutical Services, 42 CFR § 482.25 (a)(d ). 21
42 CFR § 482.25 (b)(7). 22
42 C.F.R. § 482.25 (a)(2). 23
IHS, Aberdeen Area Pharmacies, 2010 (no exact date provided in document). 24
Ibid.

Page 16 of 68
According to the same internal IHS 2010 of Aberdeen Area pharmacies, the Area experienced a 27 percent increase in prescription volume from 2006 to 2008.25 The Chairman
also recently became aware of one patient at Quentin N. Burdick Memorial Hospital that allegedly was prescribed on average 360 Oxycontin tablets per month in 2006. This information
was submitted to the Federal Bureau of Investigation (FBI), which ultimately referred the matter to the DEA and later to HHS‟ OIG. The Chairman has requested additional information; however, at the time of releasing this report the information had not been made available.
The Aberdeen Area also continues to have deficiencies in consistent monthly auditing of its
pharmacies. For instance, the hospitals at Rosebud Service Unit, Fort Yates Service Unit, Rapid City Service Unit, Belcourt Service Unit and Pine Ridge Service Unit provided inconsistent evidence that they conducted routine monthly audits. According to an IHS document titled,
“Summary of Controlled Monthly Audits,” in 2008 three service unit‟s hospitals, Belcourt, Fort Yates and Rapid City, in 2009, two service unit‟s hospitals, Rapid City and Winnebago, and in
2010, three service unit‟s hospitals, Rapid City, Belcourt and Fort Yates, failed to submit certain monthly audits.26
However, after reviewing the monthly audit documents submitted by IHS the Chairman found additional deficiencies that the Agency failed to identify. For instance, in 2009 Fort Yates
also failed to submit monthly audits for three months: February, March and August. Also, two monthly audits encompassed four months, December 17, 2008 to February 13, 2009 and October 15, 2008 to December 17, 2008, respectively. Moreover, IHS did not detail that Rosebud
Service Unit‟s hospital missed six months of monthly audits in 2009, and 2 months of monthly audits in 2008.
The following are examples of particular pharmacies that have experienced significant loss or theft of narcotics and other controlled substances.
Belcourt Service Unit
The investigation revealed that Belcourt Service Unit‟s Quentin Burdick Memorial Hospital
has had a troubling history of diverted narcotics and other controlled substances. Based on information received from the OIG and IHS, the facility has experienced substantial losses or thefts of Schedule II drugs since 2003.
According to a March 2003 Management Implication Report (MIR), the OIG found that the pharmacy was not in compliance with Title 21, section 1306.12 of the CFR, which requires a
provider to write a new prescription for Schedule II drugs – not a refill.27 The OIG identified that the pharmacy had routinely refilled Schedule II drugs without a new prescription. More
troubling, the MIR states that when a senior level official was questioned about this, they
25
Ibid. 26
IHS, “Summary of Controlled Substances,” (two page summary of controlled substance monthly audits), no date
provided. 27
Office of Inspector General (OIG), Management Implication Report (MIR) No. 03 -0010, March 12, 2003.

Page 17 of 68
responded that they were “certain that Schedule II drugs could be refilled, and that [they] had „seen it done all the time.‟”28
The OIG expressed concern that the “very fact that the word „refill‟ is written on a patient
care component [a type of medical record used in the IHS medical records system] is good enough to fill the prescription for a Schedule II drug lends credence to the fact that the standards for obtaining the drugs aren't as strict in the IHS facility as they are in the private sector.”29
Further, the OIG noted that “one IHS provider admitted to testing a patient who routinely receives the Schedule II narcotic, and there was no trace of the drug in the patient's system. Yet,
because of the ease at which the Schedule II narcotic is prescribed, the patient was able to continue receiving it.”30
In a March 30, 2004 Memorandum and Order of the U.S. District Court of North Dakota Northwestern Division, the Court cited that “the apparent failure of IHS to control the dispensing
of Schedule II narcotics from its hospital facility has created, and will continue to create, ongoing controversy and strife within the hospital and the community.”31 The court also noted that “it sincerely hopes that officials from the regional and national offices of IHS will
investigate, address and correct this institutional problem. To do nothing… would be a tragedy.”32
Based on documents the Chairman received from IHS, the pharmacy‟s inadequate management of controlled substances continued. In May 2006, an Aberdeen Area program
review found that the pharmacy was not correctly handling narcotics. For instance, there was no evidence that the required random monthly audits of controlled substances were performed.
In 2010, the hospital reported missing or stolen narcotics on four separate occasions. On March 22, 2010, an internal email from a Quentin N. Burdick Memorial Hospital staff
pharmacist indicated that another employee was caught stealing narcotics.33 Nearly one month later on April 19th, an e-mail from a staff pharmacist indicated that for Hydrocodone the
inventory in the electronic system was 2,424, yet the actual count was 1,925, resulting in a total shortage of 499 tablets. 34 On June 6th, a DEA form was completed indicating over 12,000 Alprazolam, Diazepam and Propoxyphen were reported stolen due to employee theft. 35 Finally,
a July 1, 2010, document authored by an IHS pharmacy consultant indicated that a narcotics count conducted on June 21 showed over 48,000 tablets of Hydrocodone unaccounted for.36
28
Id. at 2. 29
Id. at 3. 30
Ibid. 31
Case No. A4-02-133. at 17. 32
Ibid. 33
Email authored by the Staff Pharmacist addressed to the Chief Executive Officer o f Quentin N. Burdick Memorial
Hospital, March 22, 2010. 34
Email authored by the Staff Pharmacist addressed to the Chief Executive Officer o f Quentin Burd ick Memorial
Hospital, April 19, 2010. 35
Quentin N. Burdick Memorial Hospital, “The Report of Theft or Loss of Controlled Substances,” (D rug
Enforcement Administration (DEA) Form 106), June 6, 2010. 36 Schuchardt, Jon, Aberdeen Area Pharmacy Consultant, “Belcourt Diversion short synopsis,” July 1, 2010. See
also internal document titled “BE12BC~1.DOC.”

Page 18 of 68
On June 26, 2010, an Aberdeen Area review of the pharmacy found that the pharmacy had failed to maintain accountability of controlled substances and previous recommendations for the
facility had never been implemented.37 The report also indicated that the facility‟s pharmacy was out of compliance with CMS conditions of participation, placing its DEA license at risk. 38
At the time of IHS' review of the pharmacy, the Chief Pharmacist and Staff Pharmacist positions were vacant. According to the same June 26th IHS report of the pharmacy, the Resource
Requirements Methodology (RRM) indicates that the hospital “requires 11.5 pharmacists to adequately staff the facility.”39 Since January 2010 to June 2010, the pharmacy was staffed at
between two to four pharmacists daily, resulting in “an unacceptable level of pharmacy staffing and a recipe for critical medication error, poor patient interactions, and once again, minimal oversight of controlled substances with potential for…diversions.”40
Rapid City IHS Hospital
The investigation identified that required monthly audit reporting of narcotics and controlled
substances at Rapid City IHS Hospital were not consistently performed from 2008 to 2010. According to documents submitted by IHS, monthly audits were not performed for five months in 2008. IHS failed to submit monthly audits for three months of 2009. Finally, no monthly
audit was performed in 2010 for the month of January.
In addition, based upon IHS documents the investigation also revealed various incidents of missing controlled substances. Specifically, the pharmacy issued a total of four official DEA reports of theft or missing controlled substances since 2008 that indicated various instances of
missing narcotics.41 The pharmacy submitted a report of theft or loss of controlled substances dated March 19, 2008, which indicates that 5,569 Hydrocodone tablets were missing due to
employee pilferage.42 On that same day, the pharmacy issued an amended report indicating the loss of 5,417 Hydrocodone tablets; 965 Darvocet tablets; and 187 Xanax tablets, totaling 6,569 missing controlled substances in one day.43 The report identified employee theft as the reason
for loss pills. In addition, there were two reports of theft or loss of controlled substances in March and April of 2010 detailing the loss of four tablets of Oxycodone. 44 One report indicates
employee theft as the reason for missing narcotics.45 Based upon discussions with the OIG, the Chairman found that on November 25, 2008, a
former employee for Rapid City IHS Hospital was sentenced to five years probation and was
37
Aberdeen Area IHS Pharmacy Consultant, “Belcourt Review of Narcotic Accountability and Diversion Issues,”
June 26, 2010. 38
Id. at 7. 39
Ibid. 40
Ibid. 41
Ch ief Pharmacy Service of Rapid City IHS Hospital, DEA Form 106, dates of issuance, March 16, 2010, April 2,
2010, and two were issued on March 19, 2008. 42
Ch ief Pharmacy Service of Rapid City IHS Hospital, DEA Form 106, March, 19, 2008. 43
Ch ief Pharmacy Service of Rapid City IHS Hospital, Amended DEA Form 106, March, 19, 2008. 44
Ch ief Pharmacy Service of Rapid City IHS Hospital, DEA Form 106, dates of issuance, March 16, 2010 and April
2, 2010. 45
Ch ief Pharmacy Service of Rapid City IHS Hospital, DEA Form 106, March 16, 2010.

Page 19 of 68
required to pay restitution of $5,000 for committing health care fraud, a felony, and after admitting to OIG‟s special agents that he/she had stolen controlled substances from the hospital.
Sisseton Service Unit
According to Aberdeen Area reviews from 2005 to 2007, Sisseton Service Unit‟s Woodrow
Wilson Keeble Memorial Health Care Center‟s pharmacy showed improvements. However, in 2009 the OIG performed a review of the pharmacy and found significant discrepancies in narcotics accounting and unsecure dispensation of medications. 46
On March 17, 2009, the facility‟s pharmacy filed two official reports indicating that
employees stole 14,000 Hydrocodone and an additional 6,615 Hydrocodone tablets, respectively, totaling 20,615 missing Schedule II drugs.47 According to a March 21, 2009 report issued by the Aberdeen Area Office, OIG conducted a site visit and found significant discrepancies and gaps
in overall controls and oversight.48 For instance, IHS' electronic Resource and Patient Management System (RPMS) reports indicated that the pharmacy had dispensed151,160
Hydrocodone tablets, yet 177,100 tablets were purchased. Moreover, the pharmacy failed to perform a perpetual inventory of schedule III controlled substances. During the OIG‟s site visit, two pharmacy technicians admitted that they had stolen Hydrocodone from the pharmacy. As a
result, the Area Office provided a range of recommendations, most of which were security measures.49
In April 2009, the Aberdeen Area Office conducted a review of the pharmacy and found that while it had implemented several of the recommendations previously issued, 6,615 tablets of
Hydrocodone were still unaccounted for.50 On August 30, 2010, the Aberdeen Area Pharmacy Consultant performed a review of Sisseton‟s pharmacy and found that it had made progress in
implementing many of the OIG‟s recommendations. While minor issues remained, such as the need to remove certain narcotics from the facility, the reviewer stated that it was “unlikely that diversion will be an issue for some time.”51
Substantial Diverted Health Care Services. Generally, health care services are diverted,
including service reductions, when an IHS facility determines that it will not accept patients for certain treatment or care, thereby diverting patients to another facility. However, a hospital cannot close its emergency department and is obligated under the Emergency Medical Treatment
and Active Labor Act (EMTALA) to, at a minimum, complete a medical screening exam, provide stabilization and then, if necessary, transfer the patient. Diverted health care services are due to a range of issues, including a shortage of providers, inadequate reimbursement from
public and private insurers, and lack of bed availability.
46
Aberdeen Area Office (no author), Trip Report, March 21, 2009. 47
Ch ief Pharmacy Service of Sisseton-Wahpeton Oyate Health Care Center, DEA Form 106, two forms issued,
March 17, 2009. 48
Aberdeen Area Office (no author), Trip Report, March 21, 2009. 49
Ibid. 50
Aberdeen Area IHS Pharmacy Consultant, “Sisseton Service Unit Yearly Pharmacy Review and Physical Narcotic
Audit: April 8-9, 2009,” April 13, 2009. 51
Aberdeen Area IHS Pharmacy Consultant, “Sisseton Service Unit Yearly Pharmacy Review and Physical Narcotic
Audit: August 30, 2010,” August 30, 2010.

Page 20 of 68
The investigation revealed that, of the service units reviewed, a shortage of providers was the most cited reason for service diversions. Other reasons for service diversions included: no
available inpatient beds, nonworking equipment, water outages, and high humidity.
According to IHS documents, only one hospital, Rosebud, produced a policy on diversion and three of seven hospitals in the Aberdeen Area (Ft. Yates, Eagle Butte, and Winnebago) have tracked data since 2003 on service diversions.52 This indicates the Aberdeen Area Office or IHS‟
greater failure to effectively oversee local facilities‟ management of patient care.
During the hearing on September 28, 2010, the Chairman learned that IHS has made Rosebud‟s diversion policy applicable Area-wide.53 However, the current policy lacks a clear definition of who exactly has the authority to place the health care facility on diversion status and
does not set parameters on the length of diversions.
After reviewing the data submitted by IHS on health care service diversions, the investigation revealed inconsistencies in the data submitted demonstrating its unreliability. In addition, the Chairman learned that diversions not only detracts from providing patients with consistent care
but can be extremely costly and deplete from CHS funding.
Service Diversions Data Inaccuracies
IHS submitted data in early July 2010 on diverted/reduced services at facilities in the Aberdeen Area over the past ten years. The data showed that Quentin Burdick Memorial Hospital had experienced significant diversions over the past two years. Specifically, there were
53 days of service diversions in 2008, 306 days in 2009 and seven days in 2010.
However, IHS submitted additional information on September 16, 2010 that was inconsistent with the prior data. According to the latter submission, Quentin Burdick Memorial Hospital had experienced only 79 days of diversions/reductions in the past two years – not 313 as was
originally reported. Thus, the information IHS later submitted was substantially disproportionate to its original submission.
The investigation also found inconsistencies with data submitted by IHS concerning service diversions at Rosebud and Sisseton Hospitals. Based on the data submitted to the Chairman on
September 16, 2010, Rosebud Hospital had no diversions in 2003, 2004 and 2008.54 However, according to documents submitted on July 28, 2010 specific to Rosebud hospital diverted services occurred nearly every year since 2000, such as 108 patients that were diverted in 2003.
Furthermore, the September 16, 2010 data submitted by IHS does not indicate that diverted services occurred at Sisseton Hospital.55 However, according to data submitted by the Agency
on July 28, 2010 from 2000 to 2010, Sisseton Hospital repeatedly diverted x-ray services, dental
52
United States Senate Committee on Indian Affairs, Hearing entitled, “In Critical Condition: The Urgent Need to
Reform the Indian Health Service‟s Aberdeen Area,” Question presented to Ms. Charlene Red Thunder from
Senator Tim Johnson of South Dakota at 20. 53
Ibid. 54
IHS, “Reduction in Services,” submitted September 16, 2010. 55
IHS, “Reduction in Services,” submitted September 16, 2010.

Page 21 of 68
and preoperative treatments.56 Nevertheless, IHS failed to list any service diversions at Sisseton Hospital in its September 16th data submission.
Lack of Service Diversion Policy
The Chairman also found no evidence that service units were provided with a policy that
details who has authority to make decisions on diversions, when they may occur, and the length of the diversions as of August 2010. This has resulted in the inconsistent use and lack of oversight of diversions.
For example, the Aberdeen Area completed a program review of Belcourt Service Unit‟s
Quentin Burdick Memorial Hospital‟s health care service diversions on November 7, 2008.57 The review indicated a lack of oversight and inconsistent policies for when the hospital should divert patients. In addition, a senior level official at the hospital had little, if any, control over
the decision to divert patients. Consequently, the decision to begin diverting adult patients was made by two other senior employees, but they never developed an explanation as to why they
were diverting patients or a concrete strategy for how to get out of the diversion. Finally, according to this internal report there was no evidence of a proactive effort to identify the root causes of the problem or find alternative means to ensure admission of patients.
There also appears to be a „business as usual‟ attitude when diversions occur at the hospital.
In the same November 7, 2008 Aberdeen Area program review of the hospital it indicates that one of the employees that decided to diverted health care services stated that the facility had frequently diverted inpatient admissions in the past and it was “no big deal then so, why is
everyone getting excited about it now?” This lack of concern expressed by this senior employee indicates poor leadership and an acceptance of service diversions, despite the burden placed on
patients. During the hearing on September 28, 2010, the Chairman learned that Rosebud Hospital‟s
diversion policy was adopted Area-wide. The current policy does not provide guidance on the following: 1) who is the deciding official on diverting patient care; 2) whether diversions must
have the final approval of the Area Office; and, 3) what parameters, if any, are recommended on the length of diversions.
Service Diversions Impact CHS Funding
Service diversions not only impact the consistency and level of care provided to patients, it can also be extremely costly by detracting needed funding from CHS. Attached as “Exhibit D” in the Appendix is a chart specific to the cost of diversions at Quentin Burdick Memorial
Hospital. This chart was developed from documents that IHS submitted to the Chairman. Based upon the information submitted by IHS the investigation revealed that a total of 666 patients
56
Sisseton Hospital, “Facility Operations: Diversion/Reduction in Health Care Services from 200[0] to 2008, as well
as years 2009 and 2010,” date of submission July 28, 2010. 57
June Sabatinos, BSN, RN, MBA, and Mark Jackson, MD, Clinical Director, “Program Review at Quentin N.
Burdick Memorial Health Care Facility,” November 7, 2008.

Page 22 of 68
were transferred from the hospital due to diverted services from October 2008 to June 2010. These diversions cost over $2.5 million in funding to CHS.
Mismanagement of Contract Health Service Funding. The CHS program funds health care
services for Native Americans when they must go outside the Indian health care facility system. CHS supplements the direct health care provided at Indian health facilities.
The IHS and tribes contract with private providers when the Indian health program is unable to provide care, either because there is no Indian health facility or the existing Indian health
facility is incapable of providing the service needed. CHS can include primary health care, routine and emergency ambulatory care, hospital stays, laboratory tests, pharmacy, and diagnostic imaging and screening services. Currently, the IHS and tribes contract with more than
2,000 private health care providers.
In order for CHS to pay for health care services, a patient must follow a specific approval process established by the IHS. There are essentially two tracks by which a patient seeks care through the CHS program: (1) a self- referral; or, (2) an approval from the Indian health
program‟s CHS Review Committee, in conjunction with a clinician referral where an Indian health facility is present. Each tribe or Indian health program has a CHS Review Committee that
is charged with reviewing each CHS case and must determine on a case-by-case basis whether the care should be covered.
Through the years, the Chairman has learned that CHS funding is generally rationed due to funding constraints. Many tribes have informed the Committee that Priority I cases that cover “life or limb” situations run out of needed funding by June of each year. Many tribal members
have reported extreme numbers of denials and deferrals of CHS cases due to funding shortfalls.
IHS facilities are supposed to create monthly budgets for CHS funding and allocate funds on a priority basis so that the funds last through the end of each year. However, based upon data submitted by IHS Aberdeen Area facilities often end the year with a surplus of CHS funding. For
instance, in FY2007 facilities had a total of $6.8 million in excess CHS funding, in FY2008 $2.4 million and in FY2009 $2.9 million.58
The investigation also discovered instances in which CHS funds were transferred (known as “non-recurring funds”) to other programs and facilities. Notably, Aberdeen Area facilities have
transferred $309,000 in CHS funds to tribal ambulatory programs, including a $100,000 transfer from the Fort Yates CHS program in FY2008, which ended the year with a deficit. 59 Also, in
FY2008 the Sisseton Service Unit transferred $250,000 in CHS funds to a tribal program for oral health issues, which is likely not in compliance with CHS‟ priority system. 60 Funds were also transferred twice from the Sisseton Service Unit‟s CHS program: $2,500,000 as a loan to
58
Aberdeen Area Office (no author), “Contract Health Serv ices Service Unit & Area Program Year End Balances,”
July 22, 2010. 59
Aberdeen Area Office (no author), “Contract Health Serv ices Recurring & Non -recurring Funding,” September
10, 2010. 60
Ibid.

Page 23 of 68
Rosebud (to be repaid over the next four years) in FY2010 and $800,000 in FY2008 to Fort Yates.61
Finally, IHS recommended in its April 2010 review of the Aberdeen Area that increased
routine communications with service unit CHS staff, training of its electronic reimbursement systems, and better management of the appeal process should be implemented. IHS has begun to fully implement these recommendations; however, it is unclear the extent to which it has
assisted in alleviating many of the current challenges in management of the CHS program.
At-Risk: Facility Accreditation or Certification. The investigation identified multiple instances of IHS facilities receiving poor evaluations and being placed on notice for possible loss of accreditation. According to IHS' April 2010 review of the Aberdeen Area, five facilities were
at risk of losing accreditation. IHS concluded in its April 2010 review that the “loss of accreditation would have devastating effects on these Service Unit budgets and severely restrict
program operations.” Described below, the Majority Staff identified a total of six facilities with accreditation problems and/or EMTALA violations.
Accreditation is the process through which hospitals and other health care facilities are evaluated on their quality of care, treatment and services provided, based on established
standards of performance in the health care industry. CMS or a handful of organizations, called “deeming organizations,” perform triennial surveys and inspections of IHS health care facilities and provide the accreditation or certifications that are recognized throughout the industry.
The most prominent of these groups is the Joint Commission, which has “deeming” authority
from CMS, meaning that any hospital meeting the Joint Commission‟s conditions also satisfies the CMS conditions for reimbursement. The Joint Commission typically evaluates facilities once every three years. If a facility does not meet the necessary conditions for accreditation, the
Joint Commission will place the facility on notice and typically require that improvements be made within 90 days or risk losing its accreditation.
Through the investigation the Chairman identified certain at-risk facilities given the information that IHS submitted. Specifically, the investigation revealed that IHS hospitals
located at Pine Ridge Service Unit, Rosebud Service Unit, Belcourt Service Unit, Rapid City Service Unit, Fort Yates Service Unit, and Winnebago Service Unit had substantial accreditation
and EMTALA issues. For instance, a CMS report from March 19, 2010, notes that Pine Ridge Hospital received a number of EMTALA complaints in 2009 and 2010, which centered on insufficient care in its Emergency Department. In addition, in November 2010, CMS reviewed
Rapid City IHS Hospital‟s corrective action plans in response to a May 2005 EMTALA complaint (fifth revisit) and a September 2008 EMTALA complaint (second revisit). CMS
determined that the Hospital‟s corrective action p lans were unacceptable, requiring the facility to submit more responsive plans in order to avoid jeopardizing its accreditation.
The following are examples of accreditation or certifications problems at service units that were reviewed during the course of the Chairman‟s investigation.
61
Ibid.

Page 24 of 68
Rosebud Hospital
The Rosebud Hospital is one such facility where the investigation revealed a troubling record
of repeat poor evaluations. From 2004 to 2009, the facility was routinely cited for being out of
compliance with a number of CMS requirements. In a document titled, “Meet and Greet,” it details that in May 2008 staff identified a number of serious concerns, including poor quality of
care, questionable access to care, employee complaints not being resolved, bills not being paid on time, and a lack of professionalism in the clinic. According to a CMS August 2008 report, CMS conducted an unannounced site visit on August 27, 2008, and found that the facility had
violated EMTALA, which requires that hospitals provide care to anyone presenting with an emergency condition regardless of ability to pay or legal status. The following day, CMS
conducted a separate investigation of an additional complaint. A CMS Recertification Survey Report dated July 2, 2009, detailed one troubling incident in
October 2008 involving a pregnant patient at the Emergency Room (ER). The patient arrived at the ER with contractions every five minutes and was triaged as urgent. One and a half hours
later, she was discharged from the ER. The patient proceeded to the outpatient department due to her continued contractions and was told to walk around and go to the bathroom for a urinalysis. Forty-one minutes after the patient was discharged from the ER, she delivered the
baby in the outpatient clinic bathroom.
Further, a November 2009 Administrative Review describes how, on April 7, 2009, the White River Nursing Home filed a complaint with CMS after a patient who had been discharged to them from Rosebud Hospital showed evidence of nursing neglect. CMS determined that
“conditions within Rosebud Hospital posed an immediate and serious threat to the health and safety of patients” in certain areas, and they placed the facility on “Immediate Jeopardy” status.
The hospital submitted a Corrective Action Plan on April 10, 2009, and CMS lifted the jeopardy status.
On April 24, 2009, a letter from CMS to the hospital indicated that the facility was not in compliance with all conditions of participation (COP) for hospitals. CMS found that the facility
was deficient in its governing body and nursing services. Specifically, the facility had ongoing issues with prevention of pressure ulcers and urinary catheter management, while the hospital‟s governing body had failed to provide proper oversight of nursing services to ensure these issues
were addressed. As a result, the facility was once again placed in jeopardy status as conditions at the facility continued to pose a risk for patients.
During a recertification survey in June 2009, which was in response to the April 7, 2009, complaint, CMS concluded that the hospital was not in compliance with all of the Conditions of
Participation for Hospitals, which are required for accreditation. The review identified serious problems with the quality of nursing care, an unqualified nursing supervisor, disengaged and inaccessible managers, disorganization, lack of basic supplies, and overall disrepair of the
facility. Surveyors noted a series of troubling examples of poor patient care in the past year, including the woman giving birth in the bathroom of the outpatient clinic in October 2008; a
patient being discharged with an IV catheter left in his/her arm; and, a 16 year-old patient being discharged 24 hours after delivering a baby by Cesarean section (also known as a C-section), a

Page 25 of 68
surgical procedure normally utilized to deliver one or more babies. The hospital filed a formal Corrective Action Plan (CAP), which, according to a November 18, 2009, letter from CMS, was
returned as “unacceptable.” The facility submitted revised CAP on November 25, 2009.
The Chairman did not receive any accreditation documentation for the hospital beyond November 2009. As of November 2010, the Chairman received no evidence from IHS that the facility had taken measures to correct its jeopardy status or that CMS or IHS had performed any
additional reviews.
Fort Yates Service Unit
Fort Yates Service Unit‟s Standing Rock IHS Hospital has had substantial accreditation problems since 2007. In May 2007, a Mock Joint Commission survey of the hospital performed by Care Education Group, Inc. (CEG) identified a host of issues, including failure to verify staff
credentials, providers treating patients with expired licenses, improper documentation and missing policies and procedures.
Two months later, the Joint Commission performed a survey of the hospital and found a number of areas of non-compliance and required the facility to submit an Evidence of Standards
Compliance (ESC) within 45 days. According to the July 2007 Accreditation Survey, found, in part, that the hospital failed to consistently track provider licensure information, there was no
process for reviewing medication orders after the pharmacy closed, and there were no policies on assessing the appropriateness of prescriptions.
Over a year later, in September 2009, CMS notified the hospital that it was found to be in compliance and had only minor deficiencies. However, a Mock Joint Commission survey
conducted by CEG in November 2009 found a substantial list of problems, including expired medications and supplies (some more than six years old), rusted equipment, sterilization issues, and incomplete and improper patient care documentation. More troubling, a patient was
transferred with no evidence that the physician approved the transfer and many providers had expired and/or unverified licenses.62
In February 2010, CMS performed a “substantial allegation survey” and found that the hospital was not in compliance with the Conditions of Participation for Hospitals due to unsafe
water temperatures. According to a letter from CMS on February 18, 2010, surveyors found that “conditions within PHS Indian Health Services Hospital at Fort Yates posed an immediate and serious threat to the health and safety of patients” relating to the unsafe water temperatures.63
The hospital immediately submitted a corrective action plan and the immediate jeopardy status was abated. Following the abatement, however, as the letter notes, “deficient practice continues
to create a potential for harm” and CMS continued with the facility‟s scheduled termination of October 1, 2010. In an April 29, 2010, letter, the North Dakota Medicaid Director notified the
62
Slaba, Carol, Eric D. Joseph and Nancy E. Webster. “Mock Joint Commission Survey Report by Score and
Department: Standing Rock Service Unit, Fort Yates, North Dakota,” November 2009 at 6-7, 39. 63
Chickering, Steven D. “Letter from Steven D. Chickering, CMS Western Consortium Survey & Cert ification
Officer, to Carl Ducheneaux, Interim Chief Executive Officer, PHS Indian Hospital at Fort Yates ,” Feb. 18, 2010.

Page 26 of 68
hospital that unless CMS rescinded its termination action, the state‟s Department of Human Services would also terminate its state Medicaid Provider Agreement on October 1, 2010. 64
The Joint Commission conducted a survey of the hospital in July 2010 and identified a
number of areas of non-compliance. Joint Commission found that the hospital had no process for ongoing professional practice evaluation, instances of lapsed provider privileges, no assessments of patient‟s mental, emotional and behavioral functioning, missing documentation of
written plans of care for behavior health clinic patients, and insufficient documentation of patient consent for various procedures. The hospital was already on “immediate jeopardy” status
stemming from the February allegation survey, but the projected termination date was extended by CMS from May to October 2010, and most recently to January 2011.
Belcourt Service Unit
Belcourt Service Unit‟s Quentin N. Burdick Memorial Hospital has also had a history of accreditation issues. Joint Commission reports for the hospital in 2007 and 2010 and the
hospital‟s laboratory in 2006, 2008 and 2010 required the facility to submit an ESC within 45 days from the date of the issued report describing progress made on correcting deficiencies and/or compliance issues. Failure to make sufficient progress may negatively impact
accreditation.
A Joint Commission Survey Assistance Report was completed by CEG in 2007. This report includes reviews of specific areas of Quentin Burdick Hospital, which would be included in a Joint Commission accreditation review. The summary of findings and deficiencies lists over 80
for the hospital. The findings include, but are not limited to, safety concerns related to the lack of relevant policies for certain emergencies; incorrect procedures for removing hazardous waste;
patient charts not containing correct information; and nursing staff for the emergency room have access to the entire pharmacy. The 2007 report also reveals ten significant deficiencies in licensure and credentials of providers, such as three providers with expired certifications and
others in which the hospital failed to verify a provider‟s license.
In 2006, 2008 and 2010 Joint Commission‟s reports for the hospital‟s laboratory accreditation all required ESCs to be submitted within 45 days of the report. The reports demonstrate ongoing compliance issues. For example, the 2008 report lists such concerns as the
laboratory failing to document which staff conducted tests and there were no documented comprehensive investigations and remedial actions taken for unacceptable lab results. The 2010 report indicated insufficient compliance in staff competence.
A Mock Survey of Quentin N. Burdick Memorial Hospital was conducted by CEG on
February 22, 2010, through February 25, 2010, and found varying issues within the hospital. These findings included: improper storage and monitoring of medications and medical equipment; inadequate patient records in medical files; and, lack of proper training, reviewing,
and tracking of employee qualifications in Human Resources. From July 7th through July 9th of 2010 the Joint Commission conducted an accreditation survey of the hospital and found 24
64
Anderson, Maggie D. “Letter from Maggie D. Anderson, North Dakota Medicaid Director, to Carl Ducheneaux,
Interim Chief Executive Officer, PHS Indian Hospital at Fort Yates.” Apr. 29, 2010.

Page 27 of 68
deficiencies requiring the submission of ESCs, including nine areas related to credentialing practitioners and privileges.
Expired Health Care Provider Licenses and Other Credentials. Generally, credentials are a
health practitioner‟s documentation of education, clinical training, licensure, experience, current competence, and ethical behavior. Providers are also required to have particular credentials, such as cardiopulmonary resuscitation (CPR), Drug Enforcement Administration (DEA),
Advanced Life Support (ACLS), and a Neonatal Resuscitation Program (NRP) license in order to practice various types of medicine, prescribe medicine and/or work in a health facility.
The main purpose of the credentialing and privileging process is to ensure that qualified and competent practitioners are granted medical staff membership and/or privileges. Active
credentialing of providers is an established standard of conduct and is required by law. 65 According to the “IHS Medical Staff Credentialing and Privileging Guide,” dated September
2005, the Agency requires at a “minimum primary source verification of the following: licensure, professional education, post graduate training and experience, current competence and ability to perform (health status).”66
While physicians and Physician Assistants are generally required to be credentialed and
privileged, nurses and pharmacists are not required to be privileged.67 However, their license should be verified initially and at each subsequent licensure renewal to ensure that it is unrestricted and in good standing.68
IHS is also required to retain all such records for at least ten years after the individual‟s
termination of employment or association with IHS.69 Credentialing is an essential element to gaining accreditation and certification of facilities. Also, if a provider‟s state license lapses the facility is required to reimburse Medicare, Medicaid or private insurers for services rendered to
patients during that time.
Despite these requirements, the investigation revealed various instances of lapsed provider licenses, certifications, registrations, and privileges at Belcourt Service Unit, Fort Yates Service Unit, Rapid City IHS Hospital, and Winnebago Service Unit‟s hospitals. The following are
examples of expired provider licenses and certifications problems at certain facilities reviewed.
65
Darling v. Charleston Community Memorial Hospital , 211 N.E. 2d 253 (Ill. Sup. Ct. 1965); Thompson v. Nason
Hospital, 591 A. 2d 703, 707 (Penn. Sup. Ct. 1991); Privacy Act of 1974, as amended, 5 U.S.C. § 552a(e)(4). See,
IHS Circular No. 95-16, Credentials and Privileges Review Process for the Medical Staff, December 8, 1995 and,
IHS, “Indian Health Serv ice Medical Staff Credentialing and Priv ileg ing Guide,” September 2005. 66
For instance, the Joint Commission requires that hospitals verify licensure, certification or reg istration with the
primary source at the time of hire and upon expiration of the credentials. An outside authority, such as the medical
school from which a medical degree was awarded, or the state licensing board that granted a license, will normally
be asked to provide the evidence or attest to the validity of the provider‟s credentials , licensure or reg istration. IHS,
“Indian Health Service Medical Staff Credentialing and Privileging Guide,” September 2005 at 2. 67
Id. at 7. 68
Ibid. 69
71 F.R. § 34626

Page 28 of 68
Belcourt Service Unit
As detailed in the accreditation section of this report, a 2007 Mock Joint Commission Survey performed by CEG found licensure issues at Belcourt Service Unit‟s Quentin Burdick Memorial
Hospital. Specifically, three of CEG‟s findings related to the hospital‟s failure to verify licenses and three other findings involved expired provider licenses, one in 2002 and two others in 2007.
In addition, CEG determined that for two of the providers with expired licenses, both had expired CPR certifications and one had an expired certification of ACLS and NRP. Finally, CEG found that certain employees‟ skill sets were not adequate for the relevant health care field.
In a subsequent 2010 Mock Joint Commission Survey conducted by CEG in February of
2010, a “Human Resource File Review” was conducted involving a review of 28 employee files demonstrating the persistence of licensure and certification problems. For example, CEG found that ten employees did not have the proper license or registration, eight did not receive mandated
background checks and 15 did not have verification of their education. Finally, a July 2010 Joint Commission accreditation report also found nine areas of deficiencies related to credentialing
practitioners and privileges.
Rapid City IHS Hospital
The investigation also identified significant licensing and credentialing lapses at Rapid City
IHS Hospital. IHS submitted a June 2007 Mock Joint Commission Survey of Rapid City IHS
Hospital conducted by CEG, which identified several providers that had expired licenses or certifications. For example, one physician had an expired medical license for over seven
months. In an accreditation survey conducted on August 9-10 of 2007, the Joint Commission
identified additional issues involving the hospital‟s failure to verify licenses. For instance, a nurse‟s license was due for renewal on December 20, 2006. However, license verification was
not performed until July 27, 2007 – nearly seven months later. According to Agency documents dated between May 2008 through April 2009, licensure and
certification problems at the hospital persisted. The following is a summary of the key issues identified:
o Two medical doctors with expired state licenses; o Six doctors and family nurse practitioners with expired CPR certifications;
o Eight family nurse practitioners and physicians with lapsed ACLS or Pediatric Advanced Life Support (PALS) certifications; and,
o One family nurse practitioner with an expired DEA license.
Winnebago Service Unit
A September 2009 Mock Joint Commission Survey conducted by CEG at Winnebago
Service Unit‟s Hospital highlights significant licensure and credentialing problems. The surveyors reviewed 13 credential files and found the following:

Page 29 of 68
o Failure to verify a Physician Assistant‟s education; o Four providers‟ licenses had expired, (some over nine months ago, but the facility had
not verified or checked for renewal); o Three providers had no Child Care National Agency Check and Inquiries (CNACI), a
background check required for those who provide care to persons under age 18. CNACIs include checking the individual for convictions of crimes involving children. For instance, one provider had worked at the facility since December 2005 and
another had worked at the facility since July 2004, yet no CNACIs were performed; and,
o Three providers‟ ACLS certification had expired and three providers‟ CPR certification had expired.
In a subsequent accreditation survey conducted by the Joint Commission from August 3rd through August 6th of 2010, the hospital was awarded an insufficient compliance rating for
failing to verify employee licensure/certification and exceeding two year privileging limitations. Specifically, the Joint Commission found that the hospital had no documentation of primary source licensure/certification verification for four employees, including two nurses. In addition,
two physicians‟ re-appointments exceeded two years, including one physician whose privileges had lapsed for 22 days.
It is unclear whether these facilities took corrective action and refunded Medicare, Medicaid or private insurers for services rendered by unlicensed providers. However, the investigation
revealed one instance in which a facility took corrective action to refund Medicare. An employee at Rapid City provided services to patients without a valid license from April 1, 2001,
to October 2, 2003. The facility ultimately refunded over $63,000 to Medicare.
Disciplinary Actions Taken Against Provider Licenses. Health care providers are required
by law to have an active license (from any state) in order to serve patients at IHS facilities. IHS is required to maintain records of provider licenses, including adverse actions for at least ten
years after the individual‟s termination of employment or association with IHS. 70
The Chairman requested that IHS submit information on all providers with licensure problems, including disciplinary actions, revocations and restrictions taken by state licensing
boards over the past ten years. IHS submitted the name of two physicians detailing a total of four incidences, such as state licensure revocations, restrictions and voluntary surrender.
Based upon the information received from state licensing boards, the investigation revealed more instances of health care providers with reprimands, license suspensions, encumbrances, and
revocations. Attached as “Exhibit E” in the Appendix is a description of some of the providers the Chairman discovered had disciplinary actions taken against their license, but were not identified by IHS in the data it submitted to the Committee.
The Agency‟s failure to submit information pertaining to provider licenses demonstrates a
clear lack of adequate oversight and monitoring in this critical area. Without proper monitoring
70
71 F.R. § 34626

Page 30 of 68
and a guarantee that a health provider has a medical license in good standing, patient safety and care may be jeopardized and IHS could be exposed to litigation.
In addition to Exhibit E, the following are some of the individuals the Committee identified
with licensing problems, all of whom worked for Belcourt Service Unit‟s Quentin N. Burdick Memorial Hospital at the time of the related disciplinary action.
Nurse One – A state board of nursing found the nurse had diverted controlled substances for personal use, worked in an “impaired” condition and failed to abide by the Nursing
Advocacy Program (monitors use of controlled substances) on numerous occasions from 1989 to 2003. For example, in 2000 the nurse was in such an impaired condition that
during a C-Section procedure the nurse “could not properly place and hold retractors, and hold the patient‟s skin in place for staples.”
Nurse Two – A state board of nursing determined that the nurse had failed to notify or take action against an operating room supervising nurse who worked in an impaired
condition in 1999 and 2000.
Nurse Three – A state board of nursing found that the nurse had failed to supervise an
unlicensed assistive person and falsified a patient‟s chart in 2002.
Nurse Four – A state board of nursing determined that the nurse practiced without a state license for more than 30 days in 2004.
Nurse Five – A state board of nursing found that the nurse slept in an empty patient room
while on duty in 2005.
Employee Misconduct and Poor Performance. Based on documents received from IHS, individuals that contacted the Committee and HHS‟ Office of Inspector General (OIG), the Chairman found evidence of employee misconduct, yet the Area failed to take reasonable action
or chose to transfer, detail and/or reassign the employee to another facility. Below are some of the more egregious examples.
Winnebago Service Unit
An administrative review performed by the Aberdeen Area Office in November 2009 details issues involving a senior level management employee at Winnebago Hospital. IHS' Aberdeen
Area reviewers found that:
o According to interviews with members of the Governing Body and Supervisors, the
senior employee reported to work two days a week (16 hours) on average and frequently arrives late.
o The senior employee was absent without approval/authorization for 130 work hours in 2008 and 2009. In two particular instances the senior employee was supposed to be attending meetings, one with HHS and another with the Nebraska State Medicaid

Page 31 of 68
Director. In each instance, the employee did not submit Government Travel Vouchers verifying travel.
o The senior employee misused government funding by using facility funds to purchase food for hospital employees on various occasions.
o The senior employee used a government vehicle for personal purposes. Administrative reviewers ultimately found that that this senior employee did not
“demonstrate the leadership and ethical skills necessary” and had difficulty with “interpersonal skills needed to influence people, avoid unwanted influence, develop cooperative relationships,
establish and maintain networks, understand individuals, facilitate teamwork and resolve conflicts constructively at the Winnebago facility.”71 The reviewers concluded that appropriate disciplinary action should be taken against the employee.
The senior employee was placed on administrative leave for over two months in 2009 and
three and a half months in 2010 due in large part to a pending investigation involving misuse of authority and mismanagement. Although, the Agency proposed the employee‟s removal such actions were ultimately mitigated to a „last rights agreement‟ in which the employee agreed not
to apply for another position within the Aberdeen Area for one year from the date of the execution of the agreement and agreed to voluntarily resign at the end of a 30 calendar day
period, withdraw any informal and/or formal complaints or appeals to the Merit Systems Protection Board and any other venues.
According to IHS' website, the employee still works for IHS. The Chairman also received information indicating that this employee was previously reassigned from another Aberdeen
Area facility in July 2004, prior to working at Winnebago.
Fort Totten Health Center
In September 2006, the Spirit Lake Nation passed a resolution accusing a senior level
management employee at Fort Totten Health Center of hostile work environment, retaliation against subordinates and noncompliance with IHS policy, i.e., “prohibited personnel practices.”
The tribe ultimately passed a resolution in October 2007 expelling the employee from the Spirit Lake reservation.
The OIG and IHS investigated these allegations at the request of Chairman Dorgan. IHS performed its review in March 2007, six months after Spirit Lake Nation passed two tribal resolutions regarding the employee. IHS‟ investigation found that the employee had 1) misused
authority, 2) acted in an unprofessional manner, 3) created a hostile work environment, 4) engaged in sexual harassment, 5) misused government property, 6) had not abided by time and
attendance policies, and 7) retaliated against subordinates, among other findings. The OIG performed a criminal investigation and issued a report in September of 2008.
Although the OIG did not find that criminal misconduct had occurred and the Department of Justice declined to prosecute the employee, the OIG identified that many of the alleged and
71
IHS, Administrative Review: Winnebago Hospital, November 2009.

Page 32 of 68
substantiated acts committed by the employee, and reviewed by IHS' investigation fall within prohibited personnel practices as defined by 5 U.S.C. § 2302(b), including:
o Nepotism;
o Reprisal for whistleblowing; o Failure to take personnel actions against employees; o Discrimination; and,
o Deceiving or willfully obstructing an individual from competing for employment.
IHS‟ reviewers recommended the immediate removal of the employee, in part due to the potential continued loss of money if more EEO complaints were filed and IHS lost. The OIG found that four of five EEO complaints originated prior to the employee‟s arrival at Fort Totten
Health Center; however, all of them included issues specifically involving the employee. Mainly, complainants alleged that the employee had retaliated against them for the EEO
complaints they had filed prior to the employee‟s arrival at the facility. The allegations in the EEO cases included the following, which have all been settled, costing IHS over $50,000 at the time of OIG‟s September 2008 report.
o Employee alleged discrimination based on race, national origin and reprisal.
o Employee alleged hostile work environment because of race, sex and national origin, and alleged reprisal occurred during the EEO process.
o Employee alleged discriminated based on national origin and reprisal. The employee
also alleged that management created a hostile work environment in which the employee was ultimately detailed.
o Employee alleged subjection to a hostile work environment. o Employee alleged discrimination based on disability and national origin.
Despite IHS‟ findings, the employee was ultimately suspended without pay for 14 days, from August 26 to September 8, 2007. The employee was eventually placed on direct reassignment to
another service unit in the Aberdeen Area. This individual remains employed at IHS. The Chairman learned that this employee was
recently detailed to another facility in the Aberdeen Area.
Belcourt Service Unit
As referenced in other sections of this report, Belcourt Service Unit‟s Quentin N. Burdick
Memorial Hospital has an extensive history of mismanagement, resulting in diversion of narcotics/controlled substances, extensive diverted health care services and ample complaints
filed by its employees. There have been three OIG reports specifically regarding the hospital. First, a December
2002 report on retaliation for whistleblowing, mismanagement and harassment by a senior level management employee of the hospital. Second, two follow-up reports in June 2004 and March
2003 regarding extensive diverted narcotics (discussed in a prior section). The Chairman also received from IHS two internal reviews of the hospital dated November 2008 and June 2010.

Page 33 of 68
The following are three examples of employee misconduct at the facility and the Agency‟s related corrective actions.
o Example 1: Employee A (Senior Level Management Employee)
The Committee found the following information based upon an OIG investigation:
In April of 2000 several billers discovered that large amounts of the Schedule II narcotics, Oxycodone, were being prescribed and dispensed at the hospital‟s pharmacy, Medicare
Secondary Payor forms were back dated for billing purposes and there was no purpose of visit listed in patient records. Some individuals, for whom no purpose for the visit was listed, received refills for Oxycodone and were employees at the hospital. The matter had been
reported to Employee A since 1999 but no corrective actions were taken.
In August 2000, another employee brought the drug diversion issues to the attention of the Aberdeen Area Office Personnel Director (AAOPD). In October 2000, the AAOPD filed a report with Employee A and indicated that the matter “needed to be investigated, and if true,
pursue corrective action. This may include making contact with proper authorities.” The Aberdeen Area Director, Deputy Director and Executive Officer were also copied on the review
conducted by the AAOPD. In February 23, 2001, Employee A instructed a subordinate to provide a written response to
the issues in the AAOPD‟s review. Mistakenly, this letter was ultimately circulated, which identified many existing employees at the hospital. Ultimately, three senior level employees
discovered that this subordinate employee had provided negative information about them. Ultimately, Employee A failed to inform hospital staff of the following: 1) Employee A had
ordered the subordinate employee to draft a written response to the AAOPD; 2) the document was meant to be confidential; and, 3) the subordinate employee was acting within policy to
identify illegal activity taking place at the hospital and inform IHS management as set forth in 45 CFR § 73.735-1301 and HHS‟ General Administration Manual.
According to OIG‟s report, Employee A was upset that the subordinate employee also disclosed derogatory information about Employee A. Ultimately, Employee A failed to share the
above information with staff and as retaliation for providing information regarding illegal activity at the hospital allowed several employees that were referenced in the subordinate employee‟s draft response to the AAOPD to file a Privacy Act complaint against the subordinate
employee.
According to OIG‟s report, in April 2001 an IHS Aberdeen Area Privacy Act Investigator conducted a Privacy Act investigation. The OIG report indicates that IHS' findings were inaccurate and conclusions were not supported by facts. Based upon the erroneous information
contained in IHS' investigative report, IHS management began consulting with IHS' Office of General Counsel (OGC) regarding prospective disciplinary actions against the subordinate
employee originally ordered by Employee A to draft a response to the AAOPD. Ultimately, the OGC advised IHS to take no action until OIG had completed their investigation.

Page 34 of 68
The December 2002 OIG report found that:
Medicare Secondary Payor documents were backdated and altered by hospital bille rs, which was directly instructed by a senior level employee.
Many records for Schedule II narcotics reflected no office visit and stated, “telephone call, med refill.”
Drug Enforcement Administration Diversion Agents confirmed that a high volume of Oxycodone was dispensed through the hospital‟s pharmacy.
Certain hospital employees, in 1999, 2000 and 2001, pressured physicians to prescribe drugs to patients, friends and relatives. Other hospital employees solicited physicians in
hallways at the facility to have their personal prescriptions for drugs refilled without an office visit.
Employee A allowed the hiring of a dentist who had been terminated from the U.S.
Public Health Service Commission Corps in January 2001, but had made a false statement on his official application indicating that he had never been fired from any job
over the past five years. Employee A was aware of the termination and false statement, but permitted the hiring to take place.
Employee A provided false and misleading information to the OIG.
Employee A had made derogatory racial comments.
Employee A retaliated against the employee that was ordered to provide a draft response to the AAOPD.
The OIG noted at page six of its December 2002 report that through the course of its two-year ongoing investigation, they had “documented a pattern of mismanagement, discrimination,
and retaliation with a divisive management style resulting in civil suits, grievances, and unwarranted allegations of Privacy Act violations.” The OIG further concluded that Employee A
was “the driving force behind each problem” and recommended immediate termination. Based upon documents received from IHS, the Committee found that despite OIGs
recommendation to terminate Employee A, the individual was reassigned on March 24, 2002, within the Aberdeen Area. In March 2004, according to the memorandum and order issued by
the U.S. District Court of North Dakota Northwestern Division, the court noted that Employee A was currently employed at another facility in the Aberdeen Area. Further, in 2008 the individual was detailed from that facility to another in the Aberdeen Area and received an outstanding or
equivalent Performance Management Appraisal Program (PMAP) and was awarded 24 hours paid leave. The Majority Staff found that IHS did not submit information from 2000 to 2007
regarding the individual‟s PMAP assessment. Since IHS only submitted documents for individuals placed on administrative leave from 2005 to 2010, it is unclear whether this same person was placed on administrative leave at any point during OIGs or IHS' investigation.
Ultimately, Employee A retired from the Agency in 2009.
o Example 2: Employees C, D and E (All Senior Level Employees) Based on documents received from IHS, the Aberdeen Area performed a program review of
the hospital in November 2008, which examined the diversion of adult inpatients allegedly due to inadequate provider staffing levels and lack of equipment and supplies (see “Substantial

Page 35 of 68
Diverted or Reduced Health Care Services section” for additional information about diversion levels at Quentin N. Burdick Memorial Hospital).
IHS concluded that Employee C, a senior level nurse, had created an intimidating
environment and his/her subordinates had “well founded fears of retaliation” for speaking out against any of Employee C‟s decisions or behaviors. As an example, the report notes that a state board of nursing expressed written concern to another senior level employee, Employee D, about
the number of nurses reported to the board by Employee C. According to the report, it states that after this state licensing board conducted its investigation it found that the allegations submitted
by Employee C were unfounded. Further, according to the report, the letter suggested that Employee C needed additional training and support.
IHS also found that, on at least one occasion, another employee, Employee E, a senior level physician, refused particular work schedules, despite the hospital having severe provider staff
shortages. In addition, some contracted employees refused to work at the hospital because Employee E had treated five to six of them badly and would not return. As cited in the section titled “Substantial Diverted or Reduced Health Care Services,” Employee E is the same
individual that reacted to the lengthy diversion of services provided at the hospital nonchalantly without a sense of urgency to take appropriate action to correct the diversion crisis.
As a result of these findings, in part IHS recommended that:
1. The behaviors of Employee E and Employee C should be “dealt with” and cited that no matter “how experienced the next CEO is, he or she will not be successful because these
two individuals have proven that they can effectively undermine the CEO and suffer no consequences.”
2. “Eliminating the behaviors of these two employees is paramount to support the efforts of an experienced leader to help employees achieve some degree of insight and develop
motivation for positive change that is once again patient focused.”
The investigation revealed that ultimately Employee D resigned, while Employees C and E
remain employed at the hospital. The Majority Staff also found that Employee E had previously been reassigned from another facility in the Aberdeen Area in February 2008. Employee C was
also detailed within the service unit in February 2005. Despite IHS‟ clear concerns about Employee C in 2008, this employee‟s PMAP rating was fully successful or equivalent and was awarded a significant bonus.72 In 2009, Employee C received a bonus of over 16 hours of paid
leave. As detailed in the EEO section of this report, this employee was a primary subject of multiple EEO complaints filed against IHS.
o Example 3: Employee F (Senior Level Employee)
According to documents submitted by the OIG, a reassignment letter dated October 23, 2006, from the Deputy Director of the Aberdeen Area to Employee F, of Quentin Burdick Memorial
72
Aberdeen Area Office (no author), “Performance Management Appraisal Program 2000-2009,” Received from
IHS August 24, 2010.

Page 36 of 68
Hospital. The letter indicates that Employee F is reassigned from one facility in the Aberdeen Area to another located in the Area. At the time, Employee F was already on detail from one
service unit in the Aberdeen Area to another.
The letter indicates that Employee F‟s reassignment was based upon an August 3, 2006, finding that the employee abused authority. Further, there was an adverse action taken against the employee. As a result, Employee F was placed on 30-day suspension. The letter cites that
after Employee F was informed of a forthcoming detail, the employee reported for volunteer duty with the Army National Guard, thus giving the appearance of “purposely delaying” the
pending official detail. According to the information provided in the October 23, 2006 letter, Employee F‟s
reassignment was “management‟s last effort to attempt to correct unwarranted and unacceptable workplace behaviors.” The Deputy Director of the Aberdeen Area also warned Employee F that
the next adverse action would result in a proposed removal from employment with IHS. Employee F passed away this year. However, prior to the employee‟s death, the employee
was placed on leave for alleged misconduct.
Hiring Excluded Employees or Those with Unsuitable Criminal Records. The investigation revealed several instances in which Aberdeen Area employees were hired by IHS despite being on the OIG‟s List of Excluded Individuals/Entities (LEIE). In addition, the
Chairman identified one instance in which an employee with an embezzlement conviction was hired in a temporary position.
Under section 1128A of the Social Security Act, the OIG was given the authority to exclude certain individuals and other entities from participating in all federally funded health care
programs. The basis for exclusion includes, convictions for program re lated fraud and patient abuse, licensing board disciplinary actions, and default on Health Education Assistance Loans.
The OIG maintains the LEIE, which lists all excluded persons and entities. The effect of OIG exclusion is that no Federal health care program payment may be made for
any items or services furnished by the excluded individual or entity. In addition, any items and services furnished at the medical direction or prescription of an excluded physician or other
authorized individual are not reimbursable from a third party insurer. This prohibition extends to payments for administrative and management services not directly related to patient care, but that are a necessary component of providing items and services to Federal program beneficiaries.
Federal law permits the waiver of an exclusion where the exclusion would impose a hardship
on program beneficiaries. Waivers are determined by the OIG on a case-by-case basis. Moreover, the reinstatement of excluded individuals and entities are not automatic. Generally, once an exclusion has ended, those wishing to again participate in Medicare, Medicaid and all
other Federal health care programs must apply for reinstatement and receive authorized notice from the OIG that reinstatement has been granted.

Page 37 of 68
In June 2008, the OIG issued a report indicating that IHS had two persons, one current employee and another former employee, that were employed at two Aberdeen Area facilities. At
the time of issuing this report, it is uncertain whether these employees currently work for IHS. The following are the details concerning these two cases.
Employee at Winnebago Hospital
An employee at the Winnebago Hospital was convicted of two felony counts of criminal
conspiracy related to the delivery of Diazepam, a medication commonly used to treat anxiety and
insomnia. In addition, the employee‟s license was revoked by the state licensing board from 1990 to 1993 for professional performance and competence issues.
On May 30, 1991 the OIG placed the employee on its LEIE. The employee applied for reinstatement in March 2008 and was removed from the list on April 23, 2008, at which time the
employee was granted reinstatement. However, the OIG determined that the employee was hired by IHS in 2001, over seven years prior to reinstatement. Further, OIG‟s report notes that IHS
had determined that the employee was suitable for employment at the time of hiring the employee in 2001.
Employee at an Aberdeen Area Facility
The OIG determined in its June 2008 report that an employee was convicted in 2001 of one felony count of theft or embezzlement in connection with health care services. At the time of conviction, the employee worked for an Aberdeen Area facility and the IHS was listed as the
victim in the case.
According to the same report, the OIG excluded the employee from participating in Federal health care programs until November 28, 2007. Despite the exclusion, IHS determined that the person was suitable for employment and was employed as an emergency hire twice in 2007.
The Chairman also identified another incident where a recently hired employee was not
placed on OIG‟s exclusion list, but the employee‟s criminal record may have made them unsuitable for the job in which they were hired to perform. Specifically, a federal judge convicted the employee of embezzling money from a tribe and was sentenced to a year in federal
prison. According to news reports, the individual had embezzled federal grant funding to support a gambling addiction. Despite the conviction, IHS determined that the employee was
suitable for employment and hired them temporarily at an Aberdeen Area hospital. This employee ultimately worked in the business office in a temporary position that routinely exposed them to patient‟s private information.
The investigation revealed that the OIG may have never posted the convicted employee in
its exclusion list given that their duties may not have been considered a necessary component of providing items and services to federal program beneficiaries, especially since the position was temporary. As such, it is unclear whether there is a federally operated list that IHS could have
referred to in order to learn of this employee‟s conviction, absent disclosure from the employee or a criminal background check. It is also unclear what measures IHS took to evaluate the

Page 38 of 68
employee‟s suitability for employment versus the risk posed to the illegal use of patient information.
Mismanagement of Third Party Billing. The Indian Health Care Improvement Act
authorizes IHS to collect reimbursement for services provided at IHS facilities from third party insurers, such as Medicare, Medicaid, and private health insurers. Third party billing is an essential revenue generator for facilities and, in some cases, has enabled facilities to provide
enhanced services to patients.
Based on data received from IHS most facilities suffer from backlogs in posting third party claims within the required time frame and have failed to collect on all claims billed. IHS' Aberdeen Area Administrative Review Report completed in April 2010 demonstrates the
persistence of backlogs in coding and billing, which stalls the recoupment of third party payments. For instance, certain facilities failed to bill inpatient and outpatient claims within the
required time frame of ten days and six days, respectively. In a document submitted by IHS on September 22, 2010, the following service units had the
lengthiest backlogged third party billing, where Medicare claims were not submitted until more than a month later: Belcourt Service Unit (65 days); Sisseton Service Unit (116 days); Rosebud
Service Unit (38 days); and, Fort Yates Service Unit (32 days). Other documents demonstrate a high number of uncollected bills after 120 days. According
to an IHS report received on September 9, 2010, bills to third parties over 120 days past due should amount to no more than 20 percent of the outstanding claims due. That same report listed
the following service units as having outstanding claims above IHS‟ acceptable levels: Belcourt Service Unit (39 percent), Rosebud Service Unit (30 percent) and Fort Yates Service Unit (42 percent). Finally, according to IHS' Aberdeen Area Administrative Review Report dated April
2010, the facilities are not transmitting bills over 180 days past due to the Program Support Center for collections, as required by IHS Debt Collection Policy. Below are examples of
problems identified in third party billing.
Fort Yates Service Unit
Internal monthly billing reports for fiscal years 2006 to 2010 indicate an extensive list of
unpaid amounts, some as large as $317,000 in the month of May 2010. A 2010 e-mail indicates that the unit had collected over $3.8 million, exceeding their projected goal; however, the unit still has $278,286 yet to post. A January 2010 Corrective Action Plan from Health Information
Management indicated that over 2,097 patient visits had not been billed nearly 30 days after the date of service. Further, according to the internal monthly billing reports, significant amounts in
third party billing were unpaid: in FY2010 this amount totaled over $1.0 million.
Winnebago Service Unit
According to a 2008 “Third Party Internal Controls Review,” the Winnebago Service Unit did not submit third party claims in accordance with IHS requirements. Despite the requirement
that outpatient claims must be submitted within six days from the date of service, claims lagged

Page 39 of 68
for over 43 days for Medicare, 34 days for Medicaid and 53 days for private insurance. More troubling, inpatient claims were not submitted until 118 days for Medicare, 51 days for Medicaid
and 77 days for private insurance, even though regulations require these claims be billed within ten days.
There were also backlogs in payments posted, despite a 72-hour requirement. According to the same 2008 report, Winnebago‟s posting staff did not post payments for Medicare until 15
days later, Medicaid 17 days later and six days later for private insurance. Unfortunately, the 2008 report was the only document submitted on Winnebago‟s third party internal controls.
Therefore, the Chairman is unable to determine whether the above issues persisted in 2009 and 2010 or if these problems were present in years prior to 2008.
The Chairman received no documentation regarding billing backlogs from 2009. However, in a document submitted by IHS on September 22, 2010, the Winnebago facility had decreased its
billing backlog to six days for Medicaid, seven days for Medicare, and five days for private insurers.
Based upon additional information by IHS the investigation identified $2.1 million in third
party billing payment transfers from Winnebago Service Unit‟s hospital to other facilit ies in the Aberdeen Area over the past ten years. On September 11, 2006, the Winnebago Service Unit transferred $500,000 to Wagner Service Unit. Prior to transferring these funds, Wagner Service
Unit had a combined deficit of $32,632 in mental health, Contract Health Service and facilities support programs. Eight days later, Winnebago Service Unit transferred $500,000 to Eagle Butte
Service Unit, which had a deficit of $9,786 in Contract Health Service funds. In April 2007, Winnebago Service Unit transferred $100,000 to Eagle Butte Service Unit, which at the time had a combined deficit of $58,963 in its Contract Health Service program and equipment accounts.
Finally, in April 2010, the Winnebago Service Unit transferred – for the third time – funds of $1 million to the Eagle Butte Service Unit.
To complete these transfers of funds, IHS uses an “H” form, which details the funds to be transferred and the facilities involved. The “H” forms are approved by the CEO of the facility,
the Aberdeen Area Budget Officer, the Financial Management Officer, the Executive Office(r) and the Area Director. The tribes served by the IHS facilities, however, are not necessarily
notified. The Chairman is aware of only one instance where the tribe was consulted and approved of the transfer of funds to another facility. Further, each transfer of funds did not consistently include the terms of repayment, such as accrued interest. Finally, it is unclear
whether any of the above listed facilities have begun to repay Winnebago Service Unit‟s hospital for over $2.1 million in third party payment collections transfers.
Belcourt Service Unit
The investigation found a history of improper and delayed billing and posting, which places the billing office in noncompliance with several requirements. An internal August 2006 report
by the facility‟s Acting Compliance Officer indicates that Belcourt Service Unit‟s Quentin N. Burdick Hospital was compliant with two of 24 areas for billing, demonstrating gross

Page 40 of 68
deficiencies in billing claims such as, almost 6,000 claims had not been billed within the six-day requirement for January through August 2006.
While some improvements were made in 2007, an internal IHS “Third Party Controls
Review” found numerous areas of non-compliance in coding/data entry. For example, coding is required to be entered within four days of service. However, there was a backlog spanning two weeks or more and error reports were not being printed or reviewed. The reviewer found that
errors included 247 records missing a primary provider and purpose of visit, 50 incomplete radiology visits, 115 incomplete lab visits, 146 incomplete pharmacy visits and 37 inpatient
errors. The reviewer also found that the CEO was not reviewing third party billing. A 2009 “Third Party Controls Review” indicates continued issues with billing and posting
not being conducted within the proper timeline creating a situation where the business office is out of compliance. It is unclear whether a review was performed in 2010 since the 2009 report
appears to switch between the years of 2009 and 2010. According to IHS documents submitted to the Chairman in September 2010, hospital last
reported backlog of its Medicare billing indicated a 65 day backlog as of June 23, 2010. The hospital had a 37-day backlog in its private insurance billing as of August 2, 2010. Further, the
hospital‟s most updated record of Medicaid billing was on September 14, 2010, and it indicated a six-day backlog. According to IHS the hospital is currently utilizing a contractor to assist with its billing activity.
Staff Vacancies. A significant challenge to providing consistent and quality health care to
AI/ANs is ensuring adequate staffing of IHS-run facilities. Improving the retention and recruitment of skilled personnel, particularly physicians, nurses and other health care professionals, would mean increased patient‟s access to health care services. The Indian Health
Care Improvement Act (P.L.-94-437), requires one individual be assigned in each Area office for recruitment activities.
The Chairman requested that IHS submit information on staff vacancies for Clinical
Director (CD) and Chief Executive Officer (CEO) at each facility in the Aberdeen Area over the
last five years. The Committee found lengthy vacancies for all of these positions and several employees placed in “acting” positions.
The investigation revealed that as of September 2010 in the Aberdeen Area many of the
most senior level positions, CD and CEO, had either been vacant for an extended period or were
filled by individuals in an acting capacity. At the Belcourt, Fort Yates, Winnebago, and Sisseton Service Units three of four CEO positions and two of four CD positions were vacant as of
September 2010. Further, since 2007 Belcourt Service Unit‟s Quentin N. Burdick Memorial Hospital has had at least six different CEOs in charge of the facility. At other facilities such as, the CEO position of Fort Yates Service Unit, has suffered from lengthy vacancy periods
amounting to as much as a year and a half. According to documents, received by IHS, hiring individuals to fill permanent CEO or CD positions has taken as long as 34 months to fill. As of
November 2010, IHS had made progress in filling vacant CD and CEO positions; however, preventative measures should be taken to ensure lengthy vacancies do not reoccur.

Page 41 of 68
According to a report titled, “The Indian Health Service: Status and Recommendations for Physician, Nurse and Other Healthcare Professional Recruitment and Retention,” the Agency‟s
overall vacancy rates for January 2010 are 21 percent for physicians, 17 percent for dentists, 16 percent of nurses, and 11 percent for pharmacists.73 The investigation identified that filling
provider positions in the Aberdeen Area has continued to be a challenge, which directly impacts patient care. In addition, the IHS does not monitor or track the vacancy rates for mental health professionals, such as psychologists, psychiatrists or clinical social workers. The following are
examples of provider vacancies and its impact on access to health care services.
Belcourt Service Unit
In early 2008 there were nine vacant physician positions, three vacant pharmacist positions and six vacant dentist positions at Belcourt Service Unit‟s Quentin N. Burdick Memorial Hospital. In addition, during this same time IHS had lapsed contracts with providers (i.e., locum
tenens). Further, in 2009 four health care provider positions were vacant.
The combination of vacancies in health care providers and the facility‟s inability to secure temporary providers, led to diversions in health care services. As noted in the previous section titled, “Substantial Diverted Health Care Services,” from October 2008 to June 2010 a shortage
of providers was the primary cited reason for placing the hospital on diversion status and resulted in 388 days of diverted health care services.
Fort Yates Service Unit
Over the last five years, the Standing Rock Sioux Tribe has experienced multiple tragic spikes in suicides among the Native American youth residing on or near the Reservation. The
shortage of mental health care providers has resulted in limited access to mental or behavioral health services for the youth on the Reservation. If fully staffed, the IHS Fort Yates Service Unit, which serves the tribal community, would have only two mental health provider positions,
a Mental Health Director and Staff Psychologist.
In the first half of 2009 the Standing Rock Sioux Tribe‟s health officials reported that 50 Native American youth attempted suicide. This year tribal health officials reported that another 50 suicides were attempted and 10 suicides were completed. Often both mental health provider
positions at the Fort Yates Service Unit were vacant during periods of increased suicides. In fact, at the onset of the most recent spike in suicide attempts, in August 2010, the Mental Health
Director position had been vacant for over a year and the staff psychologist position for several months. Furthermore, the investigation identified that the Mental Health Director position which was vacated in August 2009, was not posted or advertised until May 2010, nine months after the
position was originally vacated.
On August 24th the Chairman sent a letter to the Director of IHS, Dr. Roubideaux, regarding the spike in suicides and lack of mental health professionals on the Standing Rock Reservation.
73
Author Unknown, Report to the Director of Indian Health Service, “The Indian Health Service: Status and
Recommendations for Physician, Nurse and Other Healthcare Professional Recruitment and Retention. Report to the
I.H.S. Director,” 2010 at 12.

Page 42 of 68
On September 17th the Chairman received a response letter from Dr. Roubideaux stating that both mental health provider positions at Fort Yates Service Unit had been posted and the Mental
Health Director position was filled on September 7, 2010. The investigation revealed that although the position was filled, it was later vacated. As of November 2010 the Mental Health
Director position remains vacant, having not been permanently filled since August 2009.
Use of Locum Tenens. Contract providers (also termed locum tenens) are generally utilized
by IHS to fill staff vacancies, to provide for specialty care or to enhance the current services available at a health care facility. The Chairman requested IHS to submit information
concerning the use of locum tenens, particularly the number of contract providers serving in the Aberdeen Area and the cost of these contracts from 2000 to 2010. While IHS was not able to provide information on the exact number of providers, the Chairman did receive information
relating to its cost from FY2008 to FY2010.
The investigation revealed that the use of locum tenens cost the Aberdeen Area over $17.2 million over the last three fiscal years. The cost of locum tenens has decreased this year, totaling $4.4 million, in comparison to FY2009, totaling over $9.3 million. However, when the
Committee compared the FY2008 cost of locum tenens to this year, we found an increase of over $1 million.
The Chairman also found that while nearly every service unit experienced a decrease in the cost of locum tenens from FY2009 to FY2010, Sisseton Service Unit and Kyle Health Center
locum tenen expenditures increased. Specifically, the cost of locum tenens at Sisseton Service Unit increased from $946,000 in FY2009 to $1.4 million in FY2010. Kyle Health Center‟s
locum tenens in FY2009 was over $21,000; however, by FY2010 costs increased to nearly $300,000.
Agency Directives Inhibit Employee Communications with Congress. During the course of the investigation, numerous employees of the IHS expressed fears of reprimand, retribution, and
concerns about communicating with congressional staff due to emails and actions taken by the Director of IHS and local supervisory employees.
The Chairman received copies of an IHS-wide e-mail dated April 26, 2010 from Dr. Yvette Roubideaux, Director of IHS, discouraging IHS employees from communicating with Congress,
tribal governments, other agencies and groups without permission from either their direct supervisor or staff at the headquarters office located in Rockville, MD. The e-mail indicates that IHS employees should “always get approval before talking in your official capacity with
Congress, the Department [of Health and Human Services (HHS)], or the media.” It further notes that at “all times” employees are “speaking for IHS.” Numerous IHS employees were
concerned that this could be interpreted to mean that at “all times” employees are speaking in their official capacity and, therefore, at no time are they permitted to speak with Congress or other groups without prior approval.
Finally, the e-mail states that employees should “avoid making statements about the direction
of the organization or recommendations on policy matters” unless they have “approval to do so and it is consistent” with what is being said up the chain-of-command.” However, many IHS

Page 43 of 68
employees felt that they were forbidden from making statements about their own observances or experience within IHS, which may be vastly different from those “up the chain-of-command.”
Additionally, the Chairman obtained an e-mail dated July 30, 2009 stating that “all
communications to and from HHS” must go through the Chief Financial Officer and that “all communications with Congress” must go through Michael Mahsetky, Legislative Director, at the IHS headquarters office. Further, employees are prohibited from having conversations about IHS
matters without clearance from Mr. Mahsetky.
This policy was reinforced by a senior level employee in the Fort Yates Service Unit in an e-mail forwarded by a third party who was previously under disciplinary action in part for communicating with Congress and the tribe, among other issues.
The impact of these emails on employee morale and their willingness to communicate with
Congress was seen in several instances. For example, during a site visit to Quentin Burdick Memorial Hospital, an employee informed Committee staff that they could not speak with the them because there was a “gag order.” Further, after the Committee staff left the facility, certain
employees were told by a supervising employee that they must provide all information that they shared with the Committee staff to the Agency. Finally, the Laborers International Union of
North America has reported to the Committee staff that since the investigation was initiated one employee was told by their supervisor that they were not allowed to communicate with Congress.
Although the Chief of Staff to the Secretary of HHS directly informed the Chairman of the
Committee that IHS and other departmental employees are allowed to communicate with Congress, many IHS employees felt differently based on the above emails and actions by local supervisors. Federal law safeguards the “right of employees, individually or collectively, to
petition Congress or a Member of Congress, or to furnish information” to a Committee. 74 Congress has also expressly provided that no funds appropriated in any act of Congress may be
spent to pay the salary of one who prohibits or prevents an employee of an executive agency from providing information to Congress, when such information concerns relevant official matters. Congress has also enacted provisions that provide that no funds may be spent to enforce
any agency nondisclosure policy, or nondisclosure agreement with an officer or employee, without expressly providing an exemption for information provided to the Congress.
Although investigations into federal agencies are uncomfortable, and clearly supervisors
worry that employees may communicate messages to Congress that are inconsistent with the
current political agenda, communication is essential to the oversight responsibility of the Committee and should not be hampered in any manner.
74
5 U.S.C. § 7211.

Page 44 of 68
INITIATIVES TO ADDRESS INDIAN HEALTH SERVICE’S
ABERDEEN AREA DEFICIENCIES
Indian Health Service’s Initiatives in the Aberdeen Area. Under the guidance of the
Director, Dr. Roubideaux, the IHS is working to review each IHS Area, including each Area Office. The Aberdeen Area was the second Area to be reviewed. In addition, IHS has taken additional actions to resolve other outstanding issues identified in the Chairman‟s investigation.
The following paragraphs detail key actions taken by IHS to date.
Ensure that IHS does not hire or contract with excluded felons, and conducts background
checks as a condition of hiring. The Chairman‟s investigation found that IHS had hired individuals placed on the LEIE.
IHS has stated that they are now conducting background checks for all pending new hires.
Furthermore, anyone who hires someone on the OIG exclusion list will be held accountable with appropriate disciplinary action. Although IHS plans to perform a background check on all current employees, IHS has not provided the Chairman with a concrete plan on how to address
current employees who have a criminal record that may make them unsuitable for particular job responsibilities.
Limit use of administrative leave. The Chairman‟s investigation found that administrative leave has been utilized excessively and for lengthy periods of time as a tool to address problem
employees. Formerly, the decision to place employees on administrative leave was performed at the local facility.
IHS now plans to require written approval by the Director of the IHS Area Office for each
administrative leave request. In addition, IHS‟ goal is to closely monitor the status and length of
time that employees are placed on administrative leave due to a pend ing investigation. Further, IHS has often placed the same employees on long periods of administrative leave due to lengthy
internal investigations. As a result of the Chairman‟s findings, IHS is in the process of reviewing the use of administrative leave and, if necessary, will take action to ensure it is used appropriately on a case-by-case basis.
Improve security in IHS pharmacies. The Chairman‟s investigation revealed that several
facilities in the Aberdeen Area that had a recurring history of missing and stolen narcotics and inadequate pharmaceutical audits. Specifically, the Chairman‟s findings indicated that numerous facilities in the Aberdeen Area were not following the IHS policy of performing monthly audits.
As a result of these findings, IHS is performing a review of all relevant pharmacy policies,
monitoring processes and systems. However, to date IHS has not articulated a plan on how it will enforce its current auditing requirements. In addition, in the Aberdeen Area the IHS plans to establish specific rooms to store controlled substances in each facility‟s pharmacy and install
cameras and dual security systems to prevent theft. Yet, it is unclear when these security measures will be implemented. Further, IHS' corrective actions does not include initiatives to
address staff shortages, despite IHS' 2010 report on Aberdeen Area pharmacies that determined that vacancies continue to be a challenge and contribute to greater management challenges.

Page 45 of 68
Ensure health care providers have current licenses/credentialing. The Chairman‟s investigation identified that IHS failed to ensure all health care providers in the Aberdeen Area
have an active health care provider license. The investigation identified multiple instances where nurses received reprimands for misconduct by state licensing boards where IHS was unaware of
the majority of these actions. Through the investigation the Chairman also learned that IHS is required to reimburse Medicare, Medicaid and private insurers for services delivered by providers with an expired, suspended or revoked license. The Majority Staff only identified one
instance in which IHS reimbursed the third party for services rendered by a provider with a lapsed medical license. Finally, the investigation revealed that according to reports issued by the
OIG, IHS failed to routinely query or report information into the National Practitioner Data Bank (NPDB), despite the mandate that all agencies submit information on disciplinary actions against physicians, dentists, and other health care practitioners.
Dr. Roubideaux has directed all Area Directors and Chief Medical Officers to review how
each Area monitors health care providers‟ licenses. Ultimately, IHS plans to develop a process to ensure that providers with expired licenses are not allowed to practice in IHS facilities until their status is corrected. IHS also plans to ensure that all providers are queried on the NPDB and
OIG‟s exclusion list prior to their hiring. Thus far, Dr. Roubideaux has required the use of a checklist for managers to ensure all requirements are met in clearing applicants against the OIG
Exclusion List, and that fingerprints are cleared and licenses have been validated before an applicant reports for duty.
However, IHS has not presented the Chairman with a comprehensive plan for corrective action or time frame for ensuring that employees are up-to-date on provider qualifications,
training/education and licensing. Moreover, IHS has failed to demonstrate an action plan for reimbursement to Medicare, Medicaid and private insurers for services rendered by providers with revoked or expired licensure.
Although the IHS‟ policy is to check all current practitioners against the NPDB, such efforts
may be futile since IHS has failed to ensure all IHS facilities are reporting to the database. Further, given that state licensing boards provided the Majority Staff with substantial information regarding license revocations, suspensions and reprimands that IHS was not aware
of, the Chairman is concerned that performing NPDB checks alone is inadequate.
Improve business practices in the Contract Health Services Program. The Chairman‟s investigation identified several funding transfers (termed “non-recurring funds”) from the Contract Health Services (CHS) program to 638 tribal programs. The Chairman is uncertain
whether this practice violates the authority and regulations of the CHS program.
Despite this concern, IHS maintains the funding transfers are allowed under the regulations and does not plan to take corrective actions. IHS plans to discuss, with an ongoing tribal CHS workgroup, issues related to transferring CHS funds to tribal programs. However, its corrective
action plans does not include performing an evaluation of whether CHS funding transfers are within the framework of the law.

Page 46 of 68
Addressing Certification/Accreditation Problems at Five Facilities. The investigation found that six facilities in the Aberdeen Area have recurring accreditation/certification problems, which
could jeopardize patient safety and quality of care.
IHS reports having begun meetings with CMS to address accreditation/certification problems. Nevertheless, IHS has not demonstrated to the Chairman a clear plan of how to address recurring accreditation/certification problems at its facilities. IHS‟ health care facilities
are accredited by entities other than CMS. Therefore, IHS may consider holding similar meetings with other accrediting/certifying entities, such as the Joint Commission.
Department of Health and Human Service’s Initiatives to Improve Performance in the
Aberdeen Area. Under the leadership of Secretary Kathleen Sebelius, HHS has begun a “program integrity initiative,” an agency-wide improvement plan. This initiative will include a risk assessment of HHS‟s agencies, including IHS, which it will then utilize to establish a plan to
address issues and support successes within each HHS agency. The Council on Program Integrity is comprised of the heads of each agency in the Department and staff from the Office of
the Assistant Secretary for Financial Resources.
The Council on Program Integrity will work with IHS to perform a risk assessment, as well
as to examine all Government Accountability Office, OIG, tribal and Committee on Indian Affairs‟ concerns and reports. The Council on Program Integrity‟s goal is to work with IHS to
identify the Agency‟s greatest risks and then establish a permanent integrity initiative at IHS to ensure that the Agency successfully fulfills its mission. HHS officially began the review of IHS on August 9th. Thus far, the Council on Program Integrity review is focusing on the Aberdeen
Area, including human resources, finance policies and procedures.

Page 47 of 68
APPENDIX
Exhibit A: Testimony of Dr. Roubideaux
Testimony of Dr. Yvette Roubideaux, Director of Indian Health Service, submitted in preparation for a Senate Committee on Indian Affairs hearing originally scheduled on December 8th, which
was ultimately canceled.
Mr. Chairman and Members of the Committee:
Good Morning. I am Dr. Yvette Roubideaux, Director of the Indian Health
Service (IHS). I am pleased to have the opportunity to testify on the Senate
Committee on Indian Affairs’ ongoing review of the Aberdeen Area’s
programs and operations. And, I am honored to have served the IHS during
your tenure as Chairman of this Committee. Your leadership and concerns
have had a direct impact on the manner in which IHS goes about
conducting the business of delivering health care to Indian people; and, I
am personally grateful for the direction you have provided toward improving
health outcomes of American Indians.
As I noted in my testimony before this Committee in September, I am a
member of the Rosebud Sioux Tribe of South Dakota. I have a long history
with the Indian Health Service Aberdeen Area. I am aware of the
longstanding challenges facing the Area, including insufficient
accountability with respect to performance and financial management, and
the difficulties of providing care in rural, remote, and impoverished
communities with existing resources. We are determined to make

Page 48 of 68
meaningful progress toward addressing these issues by utilizing existing
resources.
In September, I testified that the Area’s management problems are not
solely attributable to limited resources, but it does play a role. We can
manage our human and financial resources more capably, and that is what
I am committed to doing.
In fact, my priorities for our agency during my time as Director are focused
on changing and improving the entire IHS system in numerous ways. Our
patients, our staff, and our Tribes are all in agreement that we need to
reform the IHS. I know the members of this Committee are committed to
the same goal, and your investigation has been helpful in identifying
additional problems and providing valuable input as we continue to work to
bring needed and lasting change to the agency. As you know all too well, a
quick fix won’t work here – and that’s why we’re focused on the
fundamental changes necessary for long-term success.
In addition, I continue to work to advance my priority goals for IHS in the
Aberdeen Area which has helped to address many of the specific concerns
raised by this Committee. I will report on these goals and then discuss both

Page 49 of 68
updates to the Aberdeen Area review since September and reviews for all
12 of the Areas.
Priorities for IHS reform
In September, I testified about the four agency priorities that will guide
fundamental reform in IHS and the work of the agency in the coming years.
Specific to my priority to reform the IHS and immediately following this
Committee’s September hearing, I implemented several actions to make
improvements. I issued a clear and specific agency-wide directive to
address the concern about individuals on the Office of Inspector General
Exclusion List being hired in the Aberdeen Area. I made it clear to all IHS
staff that hiring employees on the OIG General Exclusion List is
unacceptable. All management and appropriate Human Resource staff
were instructed to check each potential hire against the OIG Exclusion List
before they are hired, as a part of the initial routine background clearance
for all employees, and document that the Exclusion List was checked.
In addition, supervisors must also certify they have conducted reference
checks, and ensure the OIG Exclusion list was checked in each case
before making a selection or hiring. If any individuals are hired that appear
on the OIG Exclusion List, the hiring supervisor will be held accountable. I

Page 50 of 68
can testify today that no Aberdeen Area employee or contractor working in
the Area, which totals 2,114 individuals, is on the OIG Exclusion List. Since
the hearing, we checked all 15,700 IHS employees against the OIG
Exclusion List and we currently have no employees on the list.
In addition, all new hires and contractors will now undergo fingerprint
checks before they report for duty, and funds are committed to upgrade
software for finger printing for all 13 IHS sites in the Aberdeen Area. All
new Area contracts will include pre-clearance security requirements before
contractors are hired to work in our facilities.
While these actions cover the agency’s own hiring process, we also issued
a new policy on October 29 to ensure these same background clearance
requirements apply to our contractors. New contracts awarded after
October 29, 2010,must have a contract term of “security pre-clearance” for
any employees referred to IHS through the contract. The contractor will be
responsible for appropriate security clearance of the contract employee
they are providing to the Indian Health Service, before the employee
arrives on-site. Some contracts currently have this requirement. However,
if the pre-clearance requirement is not currently a term in a particular
contract, then the individuals who are sent to IHS through these contracts

Page 51 of 68
should be treated the same as employees who were hired or already on
board prior to October 29. Those employees, if they will be assigned to IHS
for an extended period of time, will be cleared after they begin working, as
they would have been prior to the October 29 policy change. Existing
contractors will be notified of this policy change.
The Committee has also previously expressed concern regarding drug
diversion and pharmacy security. I am pleased to report we are
strengthening pharmacy security in the Aberdeen Area. The Area Director,
Ms. Red Thunder, is making funding available to purchase camera/security
systems for all IHS locations. She will ensure that security measures are
strengthened, including monthly monitoring of inventories of controlled
substances; implementation of caged controlled substance work areas; and
limited access to pharmacy work areas that include a swipe card and
combination keypad lock by authorized personnel only. Seven IHS sites are
renovating pharmacy areas to heighten security measures. The number of
pharmacists will be increased to ensure sufficient monitoring of controlled
substances. I have also directed all IHS Area Directors to review security in
their pharmacies and implement security measures if not already in place.
During the September hearing before this Committee, we discussed the
problem of provider’s practicing on expired or restricted licenses. On an
Agency-wide basis, we are reforming our hiring process to address this

Page 52 of 68
issue. In the Aberdeen Area, the Director is requiring additional steps in
the hiring process to ensure healthcare providers have current licenses.
She has instructed the Human Resources office to change the application
process so that only qualified applicants who submit a copy of their current
license will be cleared for referral on a selection certification, and all
selecting officials are required to validate applicant licenses before
selection is made. A checklist is now available for managers to ensure all
requirements are met in clearing applicants against the OIG Exclusion List,
and that fingerprints are cleared and licenses have been validated before
an applicant reports for duty.
The issue of prolonged use of administrative leave was also previously
raised by the Committee. The Aberdeen Area Director has issued a
directive outlining the administrative leave policy and requiring strict
adherence to the policy. All administrative leave over eight hours must be
approved by the Area Director. All leave approving officials are required to
examine employee timecards each pay period to ensure compliance. I
have instructed all IHS Area Directors to review their use of administrative
leave and take similar actions to correct any problems they find.

Page 53 of 68
The Aberdeen Area Director has implemented other actions to increase
oversight and accountability of Area management and staff. Ethics and
Integrity training is required as part of orientation for all new staff and is
also available to all staff. Since July, at least 133 employees have
completed the training. The Area Director has required monthly conference
calls with Chief Executive Officers to ensure the Agency priorities are
communicated to staff and to provide a forum for discussing ways of
improving processes/systems and accountability. She has responded to all
requests from the HHS’s Program Integrity Task Force and submitted all
required documents on a timely basis.
In addition to the actions listed above, the Aberdeen Area has continued to
implement the recommendations made from the Area Management Review
completed in April 2010. Since September, the Area Director directed all
Chief Executive Officers at 12 IHS sites to provide education on the
Contract Health Services guidelines and regulations to the general public,
Tribal leaders, patients, and vendors, and to provide annual training for all
21 IHS and Tribal Contract Health Services programs. The training
includes a provider education manual outlining the paths for navigating the
IHS and CHS programs.

Page 54 of 68
The Area Director implemented a comprehensive agency orientation
program for all new employees, which includes a weekly video conference
for all new hires and current staff.
The Area Director closed out FY 2010 budget deficit-free and FY 2010
third-party collections surpassed FY 2009 collections by $34 million.
The Area Director requires all meetings with Tribal leadership and service
unit governing body meeting agendas be structured to reflect the Agency
priorities.
The Area Director has required annual reviews of service unit functions and
requires corrective action plans be posted on a shared internal website for
monitoring compliance with all service unit plans.
The Area Director requested and has signed a formal agreement with the
IHS Headquarters Equal Employment Opportunity (EEO) program to
provide oversight for the Aberdeen Area EEO functions, including the
development of a training plan for all supervisors, managers, and
counselors. The training will include Basic EEO, Alternative Dispute

Page 55 of 68
Resolution, and NoFear Act. She has required all 12 IHS sites to identify
counselors to attend the training. The Area Director has begun holding
quarterly meetings between Service Unit executive leadership and Area
Office staff to address budgets, human resources, and facility accreditation
issues. CEO’s are required to review productivity reports on various
services in order to monitor productivity and service delivery and ensure
appropriate action is taken when areas of deficiency are identified through
performance indicators, such as the Government Performance Results Act
measures. The Area Director has filled all but one of the Area Chief
Executive Officer positions at 12 IHS sites, and interviews are being
scheduled in consultation with tribes to fill the remaining CEO vacancy. All,
but two of the Clinical Director positions at IHS sites are filled and the Area
is actively recruiting to fill these positions. Of course, Area Director, Ms.
Red Thunder and her leadership team have not always been perfect.
Nevertheless, she has done a commendable job of making meaningful
progress in addressing management issues, at times, under extremely
challenging conditions – in an Area known for having particularly serious
problems. That’s one of the reasons why Ron His Horse is Thunder stated
during the last hearing that tribes consider Ms. Red Thunder the best
Aberdeen Area Director they have ever had.

Page 56 of 68
IHS Reform for all 12 Areas
I originally began this work last year, by initiating a series of administrative
reviews of all 12 IHS Areas to examine key administrative functions in order
to identify best practices and areas for improvement. As a result of
concerns expressed by the Committee that some of the issues identified in
the Aberdeen Area may be occurring in other Areas, we-intensified our
activities to review other Areas and develop a structure for more regular
oversight of the management of all 12 IHS Areas. The reviews were
designed to obtain an initial assessment of the administrative issues in all
the IHS Areas, and included some, but not all, of the issues raised by the
Committee's investigation. However, in response to the Committee's
concerns, I have instructed senior leadership to do the following:
a. Incorporate all the concerns raised by the Committee's investigation into
the Area reviews;
b. Accelerate the reviews so that all 12 Area reviews are completed within
a two-year time period;
c. Implement recommendations of the Aberdeen Area Program Integrity
Task Force; and,
d. Develop a timetable for reviewing all IHS-operated facilities with a focus
on identifying and reviewing the highest risk facilities first.

Page 57 of 68
In response to the Committee’s announcement of its investigation into
problems in the Aberdeen Area, the HHS Council on Program Integrity
established the Aberdeen Area Program Integrity Task Force. The Task
Force is reviewing IHS policies and standards, as well as the problems
identified by the Committee to ensure that: (1) proper policies and
procedures are in place in the Aberdeen Area; and (2) those policies and
procedures result in corrective actions that prevent problems and improve
service in the Aberdeen Area. We will use the Task Force’s
recommendations, which will be completed by early spring, to help
formulate the reviews in all 12 Areas. While these reviews are conducted
over a two year period with available resources, I plan to implement
corrective actions at the time problems are identified and will not wait until
the end of the two year period to correct problems. I am committed to
working to correct any problems as soon as they are identified and I have
already begun to address issues raised in the last hearing. We will have the
ability to incorporate into reviews an oversight function to make sure
actions I have directed Area Directors to take have been implemented. I
am also incorporating specific measurable performance indicators that
must be met by all agency senior leadership, including Area Directors and
CEOs, that will demonstrate whether improvements have actually been
made. I will hold senior leadership and Area Directors accountable for
failure to implement these corrective actions.

Page 58 of 68
I want to assure the Committee that the Administration supports my efforts
to change and improve the way the IHS does business, and the way its
employees provide health care.
The IHS is committed to cooperating fully with the Chairman’s investigation.
My staff and I have worked to be as responsive as possible to the
Committee’s requests for documents within the stated timeframes, and to
answer follow-up questions and requests for clarification expeditiously.
Providing complete and timely agency responses to all the Committee’s
information requests is and will continue to be a top priority of mine through
the completion of the Committee’s review of the Aberdeen Area operations.
Mr. Chairman, this concludes my statement. Thank you again for your
long-standing commitment to improve Indian health, both in the Aberdeen
Area and throughout IHS, and for the opportunity to testify today on the
Aberdeen Area Indian Health Service programs.
I will be happy to answer any questions you may have.

Page 59 of 68
Exhibit B: Testimony of Laborers’ International Union of North America
Statement for the Record submitted in preparation for a Senate Committee on Indian Affairs
hearing originally scheduled on December 8th, which was ultimately canceled.
On behalf of the Indian Health Service National Council of the Laborers’ International Union of North
America (LIUNA), the union thanks the Committee for holding this hearing on the widespread
mismanagement nationwide at the Indian Health Service (I.H.S.).
LIUNA proudly represents approximately 500,000 workers in the United States and Canada. While
primarily in the construction industry, the union also represents 65,000 workers in federal, healthcare,
and public employment. LIUNA has represented federal employees at the Indian Health Service since
1977. We represent 9,600 employees at I.H.S. nationwide – over 90% of all bargaining-unit eligible
workers at the Agency. The I.H.S. has one of the highest densities of union membership of any
government agency. LIUNA represents all job classifications at I.H.S., from surgeons to housekeepers to
public health educators. The vast majority of workers LIUNA represents at I.H.S. are Native American.
The employees LIUNA represents are very dedicated to I.H.S.’s mission as part of their jobs and because
of the important role the agency plays in providing health care to them and their families as enrolled
tribal members.
Earlier this year, LIUNA submitted a statement to this Committee regarding mismanagement in the
Aberdeen Area of I.H.S. Today, we appreciate the opportunity to comment on themes of
mismanagement nationwide at the Agency, and to provide some recommendations for needed reform.
The Union shares Director Roubideaux’s goals for I.H.S., which include: improving recruitment and
retention; improving health care quality and access through increased accountability and customer
service; ensuring transparency, fairness, accountability, and inclusivity. However, pervasive problems
with communications, the Agency’s systemic lack of understanding and respect for federal labor law,
including their collective bargaining obligation, have hampered the Union’s ability to work with I.H.S. to
improve the Agency.
Pervasive Mismanagement at I.H.S. Harms Workers and Patients
As the exclusive representative of over 9,000 employees nationwide at I.H.S., the Union has extensive
experience with management problems at the Agency. These problems primarily fall into two
categories – financial and supervisory mismanagement.
Financial Mismanagement
I.H.S. continues to be under-funded. However, an increase in the Agency’s budget alone will not solve
the financial mismanagement at I.H.S. Instead, Congress, HHS, and I.H.S. must all work to ensure proper
financial accountability.

Page 60 of 68
First, many I.H.S. Service Unit Directors and Area Directors do not properly budget for their facility’s
needs. In 2009 alone, shortfalls in facility operating budgets led to threats of reduction in services (or
actual diversions of services) in Belcourt, North Dakota; Kayenta, Arizona; Rosebud, South Dakota; and
Phoenix, Arizona. These diversions or threats of reductions in services harm workplace morale and also
can compromise patient health and safety. Another key budgeting issue is decentralization across I.H.S.
regions. While Areas and facilities must have some leeway in determining their specific needs, the
current decentralized system results in little accountability or oversight at Agency headquarters. In
addition to diversions or reductions in services, this lack of accountability and oversight leads to t he
following: harms in the Agency’s ability to fill vacant positions in a timely manner, resulting in
understaffing; widely divergent performance awards for employees getting the same rating in different
Areas; and different levels of the use of contract health services, wasting federal funds.
Second, I.H.S. excessively uses contract health care workers. Nurses at I.H.S. are typically paid between
$25-$35/hour. However, contract nurses filling vacant positions cost the Agency $60-$70/hour. Taking
into account the vacancy rate for nurses, the cost to I.H.S. to hire these contract workers is estimated to
be tens of millions of dollars. Physician positions are also often contracted out, at an even higher pay
rate. Contract employees cannot be in the Union’s bargaining unit, so those workers lack key workplace
rights. Reports from facilities show that contract nurses are less well-trained and less familiar with and
sensitive to the unique needs of I.H.S. and its Native population than the federal employees who work
there.
Third, several GAO reports have detailed mismanagement of property at I.H.S. Despite the GAO’s
findings, several senior I.H.S. officials responsible for this mismanagement still work at I.H.S. The failure
to take action against the responsible managers is demoralizing to the employees.
Supervisory Mismanagement
Employees at I.H.S. are consistently ranked in the top 10% of the federal workforce in the annual “Best
Places to Work” Survey. However, I.H.S. managers are consistently ranked in the worst 10%. Managers
at I.H.S. are either poorly trained, unqualified, or both. There is no mandatory training in human
relations or labor relations for supervisors. Managers typically either do not understand, or fail to
respect, federal labor law. The primary types of these legal violations are: changes in working conditions
without union notification; denials of proper leave requests by employees; abuse and harassment of
employees; overtime/Fair Labor Standards Act violations; and health and safety violations.
Some of the most egregious examples of how supervisory mismanagement harms I.H.S. employees and
patients include:
Employees being forced to work in facilities without running water (Wamblee, SD), electricity (Eagle Butte, SD), or a functioning sewer system (Wamblee, SD).
Chronic understaffing - especially of nurses.
Managers ignore reports from employees of patient safety concerns, including possible EMTALA violations.

Page 61 of 68
Chronic over-use of term and temporary employees, which violates merit system principles.
Managers violating nepotism rules and improperly hiring family members. CEOs/Area Directors detailing poor-performing supervisors to other I.H.S. facilities instead of
disciplining/removing them.
Managers putting employees on long-term administrative leave during disciplinary investigations, violating the employee’s due process rights.
Managers threatening employees for cooperating with CMS investigators. Denying workers properly requested leave, including:
o Leave to be with a child on military leave from Afghanistan (Phoenix, AZ) o Leave when a worker was trapped at home during a severe ice and snow storm (Gallup,
NM) o Leave when a worker collapsed due to a diabetic condition when her electricity went
out during a blizzard (Eagle Butte, SD) o Leave when the worker provides a note from his/her physician (multiple facilities) o Leave to care for a sick child (the supervisor told the employee she should have a family
member care for her child instead of her, a violation of FMLA) (Shiprock, NM) o Leave for a veteran suffering from PTSD (Ft. Defiance, AZ) o Leave for the death of a parent (Northern Navajo Medical Center; also widespread)
This year alone, the Union has filed hundreds of unfair labor practices and grievances over managers’
failure to adhere to federal labor law and the union’s collective bargaining agreements – however, these
filings fail to deter management misconduct. Dr. Roubideaux must set a tone at the top that this type of
violation will not be tolerated.
I.H.S. Must Partner with the Union and Employees to Reform and Revitalize the Agency
In order to carry out necessary reforms at the Agency, Dr. Roubideaux and other senior leaders at I.H.S.
must partner with the Union and its workforce.
Improved Communications
The Union supports Dr. Roubideaux’s goals to reform and revitalize I.H.S. However, in order to partner
on these efforts, I.H.S. needs to improve its communication practices with the Union and the workers
we represent.
In the past year, Dr. Roubideaux has sent out a number of memos regarding working conditions to the
I.H.S. workforce. However, the Union was never provided copies of these memos, in violation of federal
labor law. The topics of these memos are on important topics ranging from ethics to hiring practices to
reviewing and changing performance management practices to customer service. The Union has
requested that it receive these notices when the employees receive them.
Under President Obama’s Executive Order 13522, I.H.S. has an obligation to give the Union “pre-
decisional involvement in all workplace matters to the greatest extent practicable…” This can and
should include the issues included in Dr. Roubideaux’s memos. The Union and its employees have
invaluable insight from the point of view of the front-line worker, as well as Agency-wide problems and

Page 62 of 68
possible solutions. Management cannot continue to operate in a bubble; it must listen to the voice of
the worker in order to bring about real reform at the Agency.
Implementation of the New National Collective Bargaining Agreement
On October 15, 2010, after more than five years of negotiations, the new LIUNA-I.H.S. national collective
bargaining agreement (NCBA) covering over 9,600 of the Agency’s employees went into effect. The
NCBA puts all workers represented by LIUNA under one contract; previously, both management and
labor had to deal with over 30 contracts. This new NCBA will bring about a more efficient process for
both parties. The NCBA includes a host of issues that will help the workforce and management work
more effectively together, including: union presence on health and safety committees; workplace
flexibility, including flexiplace and compressed and alternative work schedules; and union participation
in new employee orientation. These joint ventures will help to increase productivity, promote
efficiency, and improve morale at the Agency.
Implementation of the Labor-Management Relations Council
President Obama issued Executive Order 13522 on December 9, 2009. This Order implements labor-
management partnerships at federal agencies, and also requires pre-decisional involvement of unions in
all workplace matters to the fullest extent without regard to whether those issues are subjects of
bargaining. In short, the Order’s goal is to ensure greater involvement by unions in the federal agency
decision-making process for issues affecting federal employees. In addition, the new LIUNA-I.H.S. NCBA
also includes a provision to establish such a partnership (known as the Labor Management Relations
Council, LMRC). The IHS LMRC must be implemented by January 15, 2011. LIUNA looks forward to
partnering with I.H.S. on a host of issues, including two in particular:
o Implementation of the Indian Health Care Improvement Act provisions in the Affordable Care Act - The IHCIA and other ACA provisions will affect I.H.S. employees. These provisions include: maintaining consistent funding for the IHS core health care facilities; providing for the release of significant capital improvement funds to build and maintain health care facilities; increasing recruitment and scholarship programs for Indian health professionals; and a host of other programs affecting Native patients at the Agency, such as diabetes, home health, and mental and substance abuse programs.
o Expanded Supervisor Training in Labor and Human Relations - Most I.H.S. supervisors receive little or no training in labor and human relations. The more supervisor training in these areas, the more supervisors will know the law and the NCBA. Training should lead therefore to fewer grievances, unfair labor practices, and discrimination cases. Fewer filings save the Agency a great deal of time and funds, and will improve employee morale.
Conclusion and Recommendations
LIUNA appreciates the work that this Committee has done to investigate and try to reform serious
management problems throughout I.H.S. The Union and the workers it represents should be seen as a

Page 63 of 68
resource willing to work with Congress and I.H.S. to remedy these problems. Ultimately, the patients
that we serve will benefit. To this end, we recommend the following:
1. Involve the union and the workforce in plans to reform I.H.S. This would not only allow for the agency to hear from the rank and file workers on the ground, but also would increase I.H.S. employees’ confidence in Dr. Roubideaux’s leadership and ability to improve morale. Set a tone from the top that the union is a partner in reform at the agency. This should be done by implementing provisions in President’s Obama’s Executive Order (13522) and the LIUNA -I.H.S. NCBA to form a Labor-Management Relations Committee.
2. Determine best practices for management at I.H.S. and work with the union and agency employees to implement those practices throughout the Aberdeen Area and nationwide. These should include: o Reporting of patient complaints o Preventing health and safety violations o Establishing a Labor-Management review body to examine and implement best practices
that improve patient care, customer service and public relations.
3. Hold poor managers accountable. Discontinue the practice of detailing poor performing managers from one facility to another. Discontinue the practice of placing poor performing managers on overly long administrative leave.
4. Include budgeting, financial planning, and accounting as part of the reform process to avoid diversion of services. These should include: o Prevention of diversions and reductions in services o Re-centralization of key budget functions at Agency headquarters
5. Determine baseline metrics for labor-management reform. Conduct an inventory of the numbers and types of grievances, unfair labor practices, EEO complaints, and MSPB disciplinary cases and work with the union to determine the cause of these problems and how to eliminate them.
6. Review why I.H.S. employees are consistently ranked in the top 10% of federal employees while I.H.S. management is ranked in the bottom 10% of agencies.
7. Commit to recruitment and retention of federal workers at the agency (rather than reliance on contract workers) to save costs, improve morale, and ensure consistency of care. Ensure that all managers receive training on labor-management issues, including performance management systems and the collective bargaining agreement with the union.
The implementation of this collaborative process brings the front-line caregivers into the reform process
with the inevitable result of achieving the joint labor-management mission of improving patient care.

Page 64 of 68
EXHIBIT C: BELCOURT DIVERSIONS
History and Cost of Diversions in Health Care Services
(2006-2010)
Dates: Type of Diversion: Length of
Diversion:
Number of Patients could have been
served at IHS (if no
diversion)
Cost to CHS
10/11/2008
to 11/5/2008
Due to the shortage of providers, no adult
patient admissions with diversion to
Trinity Hospital, Minot, ND, with approved CHS referrals. Pediatric patient
admissions were still available. OB-GYN patient admissions were available.
26 days
47 (62 total patients
transferred)
$235,000
12/4/2008
to 9/1/2009
Due to the shortage of providers, no adult
patient admissions with diversion to Trinity Hospital, Minot, ND, with
approved CHS referrals. Pediatric patient admissions were still available. OB-GYN
patient admissions were available.
271 days
375
(501 total patients transferred)
$1,900,000
9/1/2009
to 11/1/2009
Due to shortage of 4 Hospitalists providers to cover all shifts, full adult in-patient
services were not available, with partial
diversion to Trinity Hospital, Minot ND with approved CHS referrals. Pediatric
patient admissions were still available. OB-GYN patient admissions were available.
Diversion was reduced, and then was eliminated with hiring of the 4 providers.
62 days
75
(99 total patients transferred)
$375,000
12/21/2008
to
1/2/2009
Due to the shortage of providers, no Pediatric patient admissions with
diversion to Trinity Hospital, Minot, ND, with approved CHS referrals. Adult patient
admissions were still available. OB-GYN patient admissions were available.
14 days
0 (1 patient
transferred but
could not have been served at IHS )
0
3/29/2009 to
4/5/2009
Due to the shortage of providers, no
Pediatric patient admissions with diversion to Trinity Hospital, Minot, ND,
with approved CHS referrals. Adult patient
admissions were still available. OB-GYN patient admissions were available.
8 days 2
(3 total patients
transferred)
$10,000
5/30/2010 to
6/6/2010
Due to loss of provider (placed on
Administrative Leave), the extended hours Convenience Clinic was not in
operation. Contracted providers are now
in place acquired to fill in for this service.
7 days 0 0
Total number of
transferred patients:
666
Total Cost to CHS:
$2,520,000
Total number of
transferred as a result of the lack of
providers: 499
Note: CHS Patients and Cost Estimates are based on IHS documentation ($5,000 per patient).

Page 65 of 68
EXHIBIT D:
EMPLOYEES PLACED ON LENGTHY ADMINISTRATIVE LEAVE HOURS
Senior Employee in Aberdeen Area Office o 2007: 1 week
o 2008: 2 ½ months o Reason for Leave: Pending Investigation for Allegations of Misconduct
Employee in Lower Brule o 2008: Over 2 Months
o 2009: Nearly 5 months o Reason for Leave: Pending Investigation for Inability to Perform Job Duties
Employee in Pine Ridge Service Unit o 2007: Nearly 4 months
o Reason for Leave: Pending Investigation for Failure to Report to Duty
Senior Employee in Sisseton Service Unit o 2009: Over 8 Months
o Reason for Leave: Pending Investigation for Allegations of Sexual Harassment and Hostile Work Environment
Senior Employee in Winnebago Service Unit o 2009: Over 2 Months
o Reason for Leave: Pending Investigation for Allegations of Misuse of Authority and Mismanagement
Employee at Belcourt Service Unit o 2006: Over 3 ½ months
o 2007: Nearly 9 months o Reason for Leave: Pending Investigation or Settlement Agreement involving
Destroyed Medical Records
Employee at Belcourt Service Unit
o 2006: Nearly 2 weeks o 2009: Over 5 ½ months
o Reason for Leave: Pending Investigation for Allegations of Misconduct
Employee at Belcourt Service Unit o 2010: Nearly 1 Month
o Reason for Leave: Pending Disciplinary Action for Conduct Unbecoming, Inappropriate Statements and Failing to Follow Instructions

Page 66 of 68
Employee at Belcourt Service Unit
o 2010: Nearly 2 Months o Reason for Leave: Pending Investigation and BIA Criminal Investigation for
Inappropriate Touching of Patient
Employee at Fort Yates
o 2006: Nearly 2 Months o Reason for Leave: Pending Disciplinary Action for Domestic Abuse and
Disorderly Conduct
Employee at Fort Thompson
o 2010: Over 1 Month o Reason for Leave: Pending Disciplinary Action for Failure to Follow Supervisor
Instructions
Employee at Pine Ridge
o 2006: Nearly 3 Weeks o 2007: Over 1 ½ Months
o Reason for Leave: Pending Investigation for Diversion of Drugs

Page 67 of 68
EXHIBIT E:
PROVIDERS WITH STATE LICENSE SUSPENSION, REVOCATION,
TERMINATION, REPRIMAND AND OTHER ACTIONS
The following is a sample of the information the Chairman received from a state board of nursing concerning IHS providers that worked or are currently working in the Aberdeen Area.
Nurse 1
Employed at two Aberdeen Area facilities during the course of actions taken by the licensing
board.
Board Actions and Timeline:
September 2009: Letter of Reprimand and Remediation for allegations of patient neglect
while working at an Aberdeen Area hospital; licensee had to undergo courses/training.
October 2009: Nursing Board received a complaint from a senior level employee at an
Aberdeen Area hospital about patient neglect by the licensee; Board stated that the
licensee had also given false testimony during an informal meeting with the Board
January 2010: Board investigators conducted an informal meeting with the licensee at the
Board‟s office to discuss the hospital‟s complaint. At the meeting, the nurse indicated
reassignment by the IHS to outpatient care because of concerns that were raised
concerning Nurse 1‟s patient care.” According to documents submitted by the Board, the
OIG was advised of Nurse 1‟s practice issues and the licensee was ultimately removed
from federal service effective Dec. 10, 2009.
March 2010: Nurse 1‟s license was suspended.
April 2010: Nurse 1 voluntarily surrendered nursing license.
Current Employment Status: No longer employed in federal service.
Nurse 2
Employed at an Aberdeen Area facility at the time of the board‟s actions.
Board Actions and Timeline:
July 2007: Licensee contacted the Board of Nursing and admitted to diverting Vicodin
for personal use for a period of seven months; licensee was referred to the chemical
dependency program; licensee also provided an affidavit/statement to OIG admitting this
diversion.
September 2007: Arrest warrant was issued for licensee, who was to be charged with
felony health care fraud and possession of a controlled substance.
October 2007: Board suspended Nurse 2‟s license indefinitely and licensee voluntarily
surrendered license.
January 2008: Board reinstated Nurse 2‟s license after licensee requested reinstatement
for successful completion of dependency program.
Currently employed by IHS.

Page 68 of 68
Nurse 3
Employed at an Aberdeen Area facility at time of board‟s action.
Board Actions and Timeline:
August 2009: License placed on one-year probation for patient care issues (non-
adherence to standards of practice, issues of documentation, inappropriate assessments
and treatments, and lack of patient education); licensee ordered to undergo
courses/training.
Currently employed by IHS.
Nurse 4
Employed at an Aberdeen Area facility at time of board‟s actions.
Board Actions and Timeline:
July 2003: Licensee was referred to the chemical dependency program by IHS and signed
a contract to participate after admitting suffering a relapse in dependency.
November 2003: Licensee was discharged from the program for failure to comply.
January 2004: Board suspended Nurse 4‟s license after hearing; licensee failed to appear.
Nurse 5
Board Actions and Timeline:
February 2000: Licensee voluntarily surrendered his license.
November 2003: Board reinstated Nurse 5‟s license with the condition that the nurse
participates in the chemical dependency program; licensee had admitted to diverting
narcotics from his employer for his own use.
May 2005: Licensee was discharged from chemical dependency program.
June 2005: Board summarily suspended Nurse 5‟s license after contacting the nurse about
a complaint and requested that the nurse meet with the Board at an informal meeting;
licensee expressed indecision about continuing with the chemical dependency program as
well as the return to nursing and did not appear at the meeting.
September 2005: Board suspended the nurse‟s license indefinitely.
Currently employed by IHS.
Nurse 6
Board Actions and Timeline:
July 2004: Board issued Letter of Reprimand for unprofessional conduct, based on
allegations received from coworkers.
Currently employed by IHS.