Embed Size (px)
Citation preview

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
1
ImPrim Work Package 5
PHC as one pillar of regional development: Strategies to increase regional competitiveness
Report #9
Counteracting bacterial resistance within PHC in the BSR - Towards prudent prescribing of antibiotics
Editor Ingvar Ovhed3
Authors
Rolanda Valinteliene1, Ilona Bumbliene2, Kristina Leuketiene2, Ruta Radzeviciene2, E-L Strandberg3, Ingvar Ovhed3
1Institute of Hygiene, Vilnius Lithuania
2Department of Public Health, Faculty of health sciences, Klaipeda University, Lithuania
3Blekinge Centre of Competence, Karlskrona Sweden

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
2

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
3
Content
ABSTRACT .............................................................................................................................................. 5
ABBREVIATIONS .................................................................................................................................... 6
1. INTRODUCTION .................................................................................................................................. 7
2. ACHIEVEMENT – FACING ANTIMICROBIAL RESISTANCE ......................................................... 14
3. FEASIBILITY STUDY IN KLAIPEDA, LITHUANIA ........................................................................... 15
4. IMPLEMENTATION OF A REGIONAL MODEL ON CONTAINMENT OF ANTIMICROBIAL
RESISTANCE (AMR MODEL) IN KLAIPEDA ...................................................................................... 27
5. A CLINICAL AUDIT ON URINE TRACT INFECTIONS (UTI), KLAIPEDA REGION LITHUANIA .. 30
6. RESEARCH STUDY AND HAPPY AUDIT 2 ..................................................................................... 39
7. DISCUSSION AND CONCLUSIONS ................................................................................................ 41
8. REFERENCES ................................................................................................................................... 44

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
4

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
5
Abstract
The overall objective of ImPrim flagship project is to improve public health (especially in the
eastern part of the BSR). Within this wide field, the project will focus on the role of primary
health care and its benefits for the public health system as well as the regional competitiveness.
The specific objective of this PHC project piloted in the ImPrim frame work is Communicable
diseases and how to counteract the development of bacterial resistance from a primary health
care perspective. Focus for the ImPrim deliverable in the field of communicable disease was
changed.
Initially the focus was TBC and HIV,but this is not an arena where PHC will be a significant
actor. In stead was the increasing problem of bacterial resistance as a threat to future
development of health care considered to be more relevant for activities in PHC. During those
two years of the ImPrim project time when the changed focus was present, significant series of
projects have been piloted in the ImPrim frame work.
Existing professional networks like BARN (Baltic Antibiotic Resistance collaboration Networks)
have supported the implementation of highly relevant and important new policies and
organizations in the Klaipeda region in Lithuania. In clinical practice among professionals as well
as on the regional administration level have new tools and new structures been implemented.

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
6
Abbreviations
APO Audit Project Odense
BSR Baltic Sea Region
BARN Baltic Antibiotic Resistance Collaboration Networks
BCC Blekinge Centre of Competence
GP General Practitioner
IoH Institute of Hygiene
MRSA Multiple Resistant Stafylococcus Aureus
NDPHS Northern Dimension Partnership in Public Health and Social Well-
being
NDPHS EG Expert Group of the Northern Dimension Partnership in Public Health and Social Well-being
NHS The National Health Service
PC Primary Care
PHC Primary Health Care

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
7
1. Introduction
Excessive and inappropriate use of antibiotics is considered to be the most important reason for
development of bacterial resistance to antibiotics. It has been clearly documented that the
prevalence of resistant strains is correlated with the consumption of antibiotics, and studies
comparing bacterial resistance in various European countries have shown striking differences in
the consumption of antibiotics. As antibiotic resistance may spread across borders, countries with
a high prevalence of resistant strains may serve as a source of bacterial resistance for countries
with a low prevalence.
The ImPrim subprojects to counteract communicable diseases will focus on the role of Primary
Health care (PHC) in this field. A change from TBC and HIV/Aids to Respiratory Tract (RTI)
and Urinary Tract infections (UTI) has been carried out during 2011. The development of
bacterial resistance is now recognized as one of the main threats for further progress of health
care. PHC doctors play a dominating role in prescribing antibiotics for RTI as well as UTI.
ImPrim project partners have since long played an active role working for prudent prescribing of
antibiotics. Three projects partners in one of the latest transnational EU-project; “Happy Audit -
Medical Audits for Prudent Use of Antimicrobial Agents in European Primary Health Care” are
also partners of ImPrim. (2-4)
The first workshop in the BARN (Baltic Antibiotic Resistance Networks collaboration) project
was carried out in Riga during spring 2011. One out of three subprojects were dedicated to PHC
and Lithuania. This Lithuanian subproject was integrated with the ImPrim subprojects in this
field as both Blekinge Centre of Competence, Sweden (LP in ImPrim project), Institute of
Hygiene, Vilnius (PP4) and Dept of Public Health Klaipeda univ (PP14) were all active partners
in BARN networks.
A project group was formed by participants from these three ImPrim partners and their initial
idea was a project titled “Strama in Lithuania” aiming to introduce the idea of Strama in
Klaipeda region. The project idea was supported by the BARN steering committee and the
project started as a subproject of Imprim. Today two more projects are carried out under the
ImPrim umbrella and a third research project has started up coordinated from Lunds university
and funded by Sida Baltic Sea Unit to study the project process in Lithuania.
ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
8
BARN
A network of professionals in the BSR coordinated through Swedish Smittskyddsinstitutet.
Mission: BARN will bring together professionals with visions on how to counteract development
and spread of antimicrobial resistance. BARN aims to inform about old and new projects in the
Baltic Sea region, to facilitate exchange of ideas and experience. BARN will create possibilities for
informal collaboration between experts and promote projects with hands-on implications in
everyday practice. BARN will assist to identify funding opportunities. BARN is an extension of
activities initiated in the networks of BALTICCARE (The Baltic Network for Infection Control
and Containment of Antibiotic Resistance), Strama and Happy Audit.
BARN invites professionals from all fields to join to find project ideas, contribute with expertise
or just seek information.
STRAMA
In order to reduce inappropriate use of antibiotics and to counteract the increase in antimicrobial
resistance in community-acquired and nosocomial infections, a national project was initiated in
Sweden in 1994. The overall aim of Strama (The Swedish Strategic Programme Against
Antibiotic Resistance) is to preserve the effectiveness of antibiotics in humans and animals.
Strama is organised at two levels: a network of independent local multidis ciplinary groups in
each county that provide prescribers with feedback on antibiotic use and resistance and
implement guidelines; and a national executive working group funded by the government. To
gain an insight into antibiotic use, Strama has conducted several large diagnosis prescribing
surveys in primary care, in the hospital settings and in nursing homes. National antibiotic
susceptibility data for Sweden and mandatory notification show that in recent years the
proportion of Streptococcus pneumoniae with decreased sensitivity to penicillin V has stabilised
(around 6 %), but the number of notified cases of meticillin-resistant Staphylococcus aureus
(MRSA) has increased and ESBL-producing Enterobacteraceae have turned into an endemic
situation. Still, Sweden is among the countries with the lowest rates of MRSA (<1 %), S.
pneumoniae can still be treated with penicillin V and the rate of Escherichia coli-
producingESBLs is below 5 %. Strama's activities have contributed to a steady decrease in
antibiotic use from the mid 1990s until 2004(when total use slowly started to increase again)
without measurable negative consequences. Regular collaboration with national and regional
news media has been one of the key strategies.

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
9
Large diagnosis-prescribing surveys have been undertaken, and the concept of basic hygiene
precautions was introduced, together with extensive programs for early case finding. However,
surveillance has been hampered by inadequate IT systems and some difficulties in collecting
relevant data on antibiotic sales at the national level. Also, a decentralized system with 21
counties and regions has resulted in divergence of action plans and rules. The containment of
antibiotic resistance thus far may be explained by the early response in human and veterinary
medicine and close multisectorial collaboration, supported by the government, before problems
got out of hand.
On-going national projects (http://en.strama.se/dyn//,84,2,70.html )
• The Strama Point Prevelence Study 2003 and 2004 on hospital antibiotic use
• A study of hygienic routines and infections in child day care
• The Strama diagnosis-antibiotic prescribing survey 2002
• ICU-Strama Link to interactive database
• Survey of activities at the county level, 2003
• Swedish antibiotic nursing home trial (SANT)
• Self-medication with antibiotics in a Swedish general population
Weekly antibiotic prescribing and influenza activity in Sweden; a study throughout five influenza
seasons
Sweden sets national target for antibiotic use in outpatient care In December 2010 the Swedish Government announced a 500 million SEK commitment to
improving patient safety in health care during 2011 out of which 100 million SEK will be
allocated to the work with improving rational use of antibiotics. In 2010 the average use of
antibiotics in outpatient care* in Sweden was 390 prescriptions per 1000 inhabitants. There are
however, great regional differences.
The 100 million SEK to be shared between the 21 county councils in Sweden are conditional in
the way that for county councils to receive any funding they are firstly required to form a Strama
group with a clear mandate to coordinate local activities. Secondly, prescribers must increase the
adherence to treatment recommendations aiming at no more than 250 prescriptions per 1000
inhabitants per year by 2014, a national target set by the Swedish government. The funding will
be allocated yearly in relation to potential step-wise fulfillment of the mentioned criteria.

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
10
* Outpatient care refers to antibiotics prescribed in primary care and open specialist surgeries.
New organisation of Strama
From July 1st 2010, Strama (the Swedish Strategic Programme against Antibiotic Resistance) is an
advisory body with the remit to assist the Swedish Institute for Infectious Disease Control in:
1) matters regarding antibiotic use and containment of antibiotic resistance
2) facilitating an interdisciplinary and locally approved working model, ensuring involvement by
concerned authorities, counties, municipalities and non-profit organizations.
HAPPY AUDIT in Lithuania
In the transnational EU-project Happy Audit a clinical APO-audit on RTI and antibiotic
prescribing in PHC was carried out in seven countries during 2008 and 2009. In 2008, 618 GPs in
Spain, Denmark, Sweden, Lithuania, Kaliningrad region and Argentine took part and in 2009 511
GPs. They registered in all 33273 consultations in 2008 and 29390 in 2009. The goal was to lower
the prescribing of Antibiotics per se but also to change the policy towards more narrow
antibiotics. Moreover the doctors in Lithuania, Spain, Argentine and Kaliningrad region got
access to use new Point of Care (POC) tests: StrepA and C-Reactive Protein (CRP). Between the
two registration periods the participants were offered an intervention program including training
courses on appropriate use of antibiotics for RTIs, clinical recommendations for diagnosis and
treatment of RTIs, posters for waiting rooms and brochures and hand out to patients about
prudent use of antibiotics and training in use and interpretation of POC tests.
The main results was a relative reduction of 25% in the doctors’ total prescribing of antibiotics.
In Argentine the relative reduction of total antibiotic prescribing was 20%, in Denmark 9% and
in Sweden 10%. In Lithuania the antibiotic prescribing was nealy halved, while in the same time
the fraction of penicillin V markedly increased. In Kaliningrad the prescribing of antibiotics more
than halved and in Spain the doctors’ prescribing of antibiotics was reduced by approx. 1/3.
Most impressive changes of doctors prescribing were seen in Klaipeda region in Lithuania (1-4).
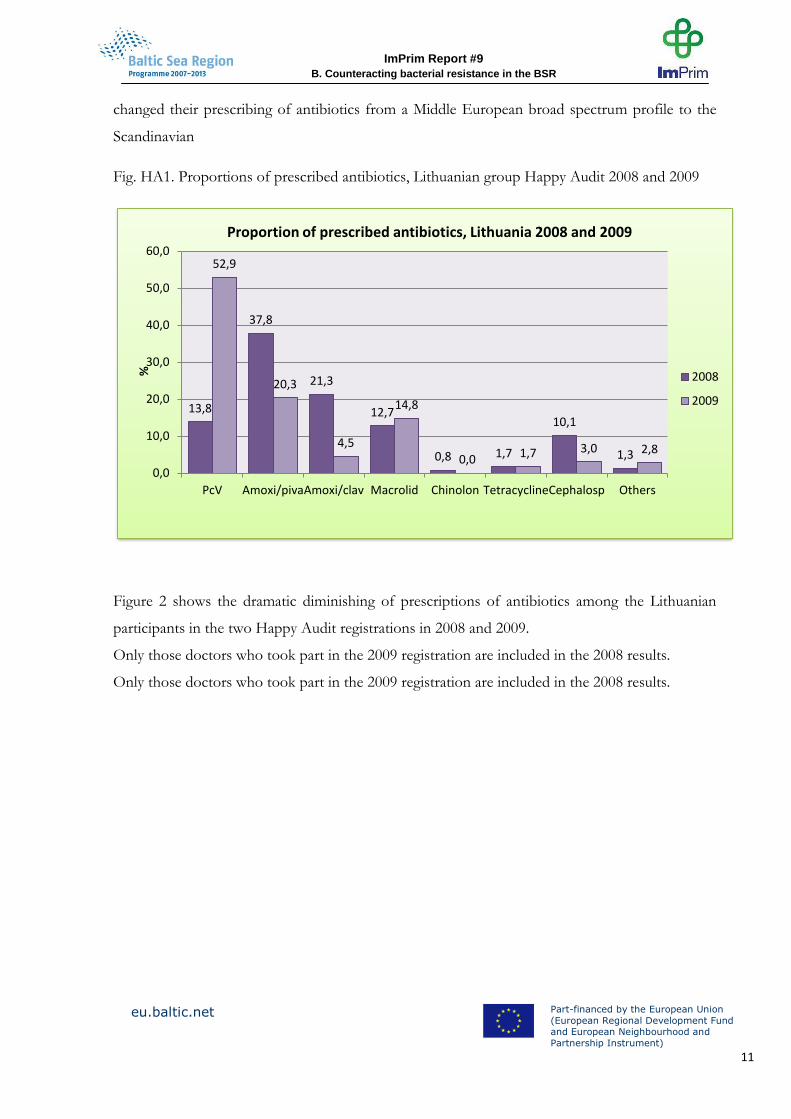
As shown in fig. 1, For Lithuanian doctors the use of the narrow penicillin, PcV had increased
from 13,8% to more than 50% between 2008 to 2009. This means that the Lithuanian group
ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
11
changed their prescribing of antibiotics from a Middle European broad spectrum profile to the
Scandinavian
Fig. HA1. Proportions of prescribed antibiotics, Lithuanian group Happy Audit 2008 and 2009
Figure 2 shows the dramatic diminishing of prescriptions of antibiotics among the Lithuanian
participants in the two Happy Audit registrations in 2008 and 2009.
Only those doctors who took part in the 2009 registration are included in the 2008 results.
Only those doctors who took part in the 2009 registration are included in the 2008 results.
13,8
37,8
21,3
12,7
0,8 1,7
10,1
1,3
52,9
20,3
4,5
14,8
0,0 1,7 3,0 2,8
0,0
10,0
20,0
30,0
40,0
50,0
60,0
PcV Amoxi/piva Amoxi/clav Macrolid Chinolon Tetracycline Cephalosp Others
%
Proportion of prescribed antibiotics, Lithuania 2008 and 2009
2008
2009

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
12
Figure HA2. Total prescription of antibiotics, Lithuanian group Happy Audit
In figures this meant that in 2008 the doctors did not prescribe antibiotics at 1395 out of total
2409 consultations. But, in 2009 the same doctors did not prescribe antibiotics in 1491 out of a
total of 1976 consultations for acute respiratory infections.
The BARN projects and ImPrim
The BARN projects carried out in connection with the ImPrim project: To create a Strama-like
group in Lithuania and carrying out first clinical audit on UTI.
The first workshop in the BARN project was carried out in Riga during spring 2011. One out of
three subprojects were dedicated to PHC and Lithuania. A project group was formed by
participants from Institute of Hygiene, Vilnius, Department of Public Health, Klaipeda university
and Blekinge Centre of Competence – all three ImPrim partners, PP4, PP14 and LP. This group
presented a project titled “Strama in Lithuania” later on “planning a regional antimicrobial
management group”aiming to introduce the idea of Strama in Klaipeda region. The project idea
was supported and the project started as a subproject of Imprim. Today two parallel projects are
carried out under the ImPrim umbrella and a third research project has started up coordinated
from Lunds university to study the PHC process in Lithuania.
2008 2009
None AB 57,9 75,5
Any AB 41,5 23,7
0
10
20
30
40
50
60
70
80
%
No or any antibiotics prescribed, Happy Audit 2008 and 2009, GPs Lithuania

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
13
Professionals from Institute of Hygiene (IoH), Vilnius have taken active part in the BARN
meetings in Riga and Vilnius during 2011. Inspired by these workshops IoH (Imprim PP4) has
started up two ImPrim subprojects on regional strategy on antibacterial resistance and
implementation of a prudent prescribing of antibiotics together with Department of Public
Health, Klaipeda university (ImPrim PP14) and Blekinge Centre of Competence (BCC ImPrim
LP).
First subproject has been a feasibility study in Klaipeda region – implemented during 2011.
An analysis of regional governmental and municipal resources of institutions as well human
resources was carried out. Moreover available data on antibiotic use as well as bacterial resistance
in Klaipeda region has been described. The following functions were described; Funding, Data
monitoring, Dissemination of information, Training of medical staff, Public education, Desicion
making. Responsible institutions would be Primary Care Centres, Municipality of the Klaipeda
District, Klaipeda City Municipality, Public health bureau and Klaipeda university, Responsible
for reporting on microbiological as well as consumption data would be Klaiepda territorial Sick
Fund, Centre of Public Health and microbiological laboratories.
A steering group of 14 persons, mostly doctors, was formed and has started to work. Their first
task will be to carry out a clinical audit on UTI in PHC as well as hospital care. An audit report
will be produced after the registration phase. The follow up meetings will give opportunity to
invite doctors in PHC as well as on hospital to educational activities. These activities will take
place mostly during year 2012, but are planned to continue in the future. This group of 14 people
will be the basis for the future Lithuanian “Strama” or antimicrobial management group. This
work will be described in detail in the following pages by Dr Rolanda Valintiene, IoH.
In Klaipeda region the project is coordinated from the Department of Public Health at the
Klaipeda university. Regional coordinators are dr Ruta Radzeviciene-Jurgute and dr Ilona
Bumbliene. When the group of professionals was formed their first project was to carry out a
clinical audit on UTI. Both doctors in PHC and in hospital care will be engaged. The first step in
an audit process will be to get consensus on the variables. UTI – Urine Tract Infections, are not
as common as respiratory tract infections in PHC. However, these infections are of significant
importance up to the issue of bacterial resistance. Patients are many times old and those patients
have a tendency to develop pyelonephritis risking sepsis or bacteriemia. These complicating
ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
14
infections are life threatening not least if they are caused by resistant bacterias. It is well known
that PHC doctors have a tendency to use broad spectrum antibiotics for the more simple UTIs.
Prescribing must be strict prudent to meet the dangerous increasing bacterial resistance. The
audit project per se will involve starting up an audit centre at the department of Public Health at
Klaipeda university, described in the ImPrim report no 3: “Quality improvement from a bottom-
up perspective - the clinical audit tool”
2. Achievement – facing antimicrobial resistance
Implementation of regional model on containment of antimicrobial resistance
Objective: To prepare and pilot regional strategy on containment of antimicrobial resistance and
implementation of rational antibiotic use.
Location: Klaipeda region, Lithuania
Time: July 2011 – December 2012
Responsible participants:
Institute of Hygiene – Project leader
Klaipeda University – Project partner
Plan of implementation:
Feasibility study in Klaipeda region – to identify main partners and investigate priority activities
(2011 July – November )
Preparation of regional strategy on containment of AMR (2011 December – 2012 February
Implementation of regional model on containment of antimicrobial resistance (AMR model) in
Klaipeda region (2012 March – December)
Expected outcomes:
Outcomes Indicators of activities
Regional strategy on containment of AMR
Presentation of the strategy to national experts
Formation of regional antimicrobial management group
Plan of activities and regular meetings
Creation of monitoring system of antibiotics prescribing
Accessibility of data
Training of regional antimicrobial management group members and other health care workers
Number of participants

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
15
Overview of activities
3. Feasibility study in Klaipeda, Lithuania
Feasibility study in Klaipeda region – To identify main partners and investigate priority activities
– Period: July – November 2011. The study consisted of three parts:
1. Analysis of health care providers in Klaipeda region.
2. Analysis of functions of health care related institutions
3. Analysis of perceptions and expectations related to AMR control of different
stakeholders
The first inventory study was performed to investigate the network of health care providers in
Klaipeda region.
Hospital care
There are nine hospitals in Klaipeda city and region – Klaipeda Republican Hospital, Klaipeda
Seamen‘s Hospital, Klaipeda University Hospital, Klaipeda Medical Nursing Hospital, Children‘s
Hospital of Klaipeda, Klaipeda district Gargzdai Hospital, Klaipeda tuberculosis hospital, Silute
Hospital, Kretinga Hospital.
Microbiological investigations and determination of sensitivity to antibiotics of isolated bacteria
are performed in three hospital laboratories – the Klaipeda Republican Hospital, Klaipeda
Seamen‘s Hospital and Klaipeda University Hospital.
Primary health
There are 47 primary health care centers in Klaipeda city and district. Microbiological
investigations are performed in different laboratories based on bilateral agreements between
Center and laboratory selected on the basis of best economical conditions.
Preparation of regional strategy on containment of AMR
Preparation of regional strategy on containment of AMR (2011 December – 2012 February
The aim of this second study was to analyze functions, regulations, human resources of
governmental and municipal health and high education institutions, to determine their current

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
16
responsibilities in AMR control and their possibilities to coordinate work of regional
antimicrobial management group (futher -Group), based on Sweden STRAMA model, in
Klaipeda region.
All public health, health care and related institutions including municipality, state health insurance
fund and Klaipeda University were selected for analysis. Regulations, functions and objectives of
institutions were analyzed through their official websites and during the meetings with specialists
from these institutions. One of the objectives of the analysis was to identify potential members of
AMR group in Klaipeda region and to identify main institution which could coordinate the group
work. Functions related with public health surveillance, health promotion, health programs,
prescription drugs, microbiological diagnosis, population health status, communicable diseases
were collected.
Main functions were collected from official institutions regulations and to identify institutions
relevant for the project following keywords were used: antimicrobial resistance management,
antimicrobial resistance, antibiotic consumption, antibiotic usage, prudent use of antibiotics,
public health surveillance, health promotion, health programs, prescription drugs, microbiological
diagnosis, population health status, communicable diseases.
None of the institutions had antimicrobial resistance management, antimicrobial resistance,
antibiotic consumption, antibiotic usage, prudent use of antibiotics mentioned in their regulations
so for further detailed analysis were selected seven institutions with other Project keywords in
their regulations:
Klaipeda Territorial Health Insurance Fund
Klaipeda City Municipality
Klaipeda District Municipality
Klaipeda Public Health Bureau
Klaipeda District Municipality Public Health Bureau
Klaipeda Public Health Centre
Klaipeda University

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
17
Klaipeda Territorial Health Insurance Fund
Klaipeda Territorial Health Insurance Fund (THIF) is a state institution, whose objective is to
guarantee the insured person‘s health care delivery and reimbursement of medicines and costs for
services and medicines issued payment.
THIF functions related with Project keywords:
Fund local health programs;
Analyze and evaluate data on the county‘s municipal population health status and demographic
structure of population trends;
Control personal health care services and medicines cost, quantity and quality.
Klaipeda City Municipality
Klaipeda City Municipality objectives related with public health are to solve city problems in
organizing programs, adoption of legal documents, coordinating activities of other responsible
institutions. Klaipeda City Municipality functions related with Project keywords (elected of
responsibilities and roles of institution specialists) are:
Prepare decisions and other regulations related with health care organization, management,
execution and control.
Organize preparation of municipality sponsored decisions and programs.
Prepare decisions and other regulations related to the primary health care.
Initiate and supervise the Lithuanian health program, implementation of public health programs
at the local level.
Prepare and/ or initiate municipal complex and targeted health programs implementation to
ensure organization of services, service performance monitoring.
Coordinate public health education issues.
Participate in the preparation of city plans for the prevention of communicable diseases, anti-
epidemic tools acts and organizes their implementation of controls.
Organize implementation of public health and long-term continuous health programs
Control implementation of communicable disease prevention measures in city plan and other
legal anti-epidemic measures

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
18
Klaipeda District Municipality
Klaipeda District Municipality objectives related with population health are to solve city
problems in organizing programs, adoption of legal documents, coordinating activities of other
responsible institutions. There is Health and Social Welfare Committee in Municipality of
Klaipeda District. Function of this Committee related with Project keywords are:
Consider and submit proposals to the protection of the health issues and control their
implementation
In addition, in 2011 one of the health priorities for action is:
Communicable diseases (tuberculosis, rabies, sexually transmitted diseases) prevention
Klaipeda Public Health Bureau
The main objectives of the Bureau activities – to improve health of the population, reduce
morbidity and mortality. Klaipeda Public Health Bureau conducts public health surveillance in
the city and Among the activities of the Bureau – organization and presentation of non-
specialized public health services to population main fo which is health promotion.
Klaipeda Public Health Bureau functions related with Project keywords are:
Develop and implement public health promotion and disease prevention programs
Carry out health education, spread knowledge about healthy lifestyles and propagate it,
Provide information about health measures and events for population
Implement mandatory health education
Klaipeda District Municipality Public Health Bureau
The main objectives of the Bureau activities – to improve health of the population, reduce
morbidity and mortality. Klaipeda District Municipality Public Health Bureau conducts public
health surveillance in the district. Klaipeda District Municipality Public Health Bureau functions
related with Project keywords are:
Development and implementation public health strengthening measures
Organization of health training for population, dissemination of knowledge about healthy
lifestyles, propagation of healthy lifestyles, to provide information about health measures and
events
Implementation of Lithuanian health program, the Government of the Republic of
Lithuania resolutions adopted by public health programs and health measures in the municipality

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
19
Implementation of measures of municipality special program for public health support and
other local health programs
Develop of community health improvement programs, to participate in projects
Klaipeda Public Health Centre
Klaipeda Public Health Centre is institution, which have three directions of action – public health
safety, public health safety control and communicable disease prevention and control.
Klaipeda Public Health Centre functions related with Project keywords:
According to Lithuanian Republic of communicable disease prevention and control
statutory powers implement communicable disease prevention and control
Implement epidemiological surveillance of communicable diseases
Carry out epidemiological investigation of diseases and their outbreaks,
management of cases and liquidation of outbreaks
Having regard to the epidemiological situation prepares / participates in the
development of targeted communicable diseases prevention and control programs for
municipalities, submit these programs proposals to the municipal administrations, submit
proposals for communicable diseases prevention plans, participate in formation of municipality
communicable diseases management plans
Klaipeda University
Klaipeda University Faculty of Health Sciences one of the main areas of research:
Complex biomedical and social research for sustainable society development by modeling aspect
Health promotion and disease prevention methodologies and health care efficiency research
Klaipeda department of National Public Health Surveillance Laboratory
One of the main functions of Laboratory is to conduct laboratory tests required for
communicable diseases diagnosis and prevention. However Klaipeda branch of laboratory not
perform this function.
After analysis of official websites, all functions of the analyzed institutions have been divided into
the following categories: control, funding, data monitoring, dissemination of information,
training of medical staff, public education, making decisions, organization, data reporting
(microbiological, consumption) (1 table). The aim was to determine which institution could be as

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
20
the main and coordinating regional AMR management group. Some functions of institutions
overlaped, but there is no institution, which is responsible for antimicrobial resistance
management in the region.
1. Control Klaipeda Territorial Health Insurance Fund
Centre of Public Health
2. Funding Klaipeda Territorial Health Insurance Fund
Municipality of the Klaipeda District
Klaipeda City Municipality
3. Data monitoring Klaipeda Territorial Health Insurance Fund
Public health bureau
Centre of Public Health
Microbiology laboratories (of hospitals etc)
4. Dissemination of information
Public health bureau
Klaipeda university
Centre of Public Health
5. Training of medical staff Klaipeda university
Primary care centre
6. Public education Public health bureau
Primary care centre
7. Making decisions Klaipeda Territorial Health Insurance Fund
Municipality of the Klaipeda District
Klaipeda City Municipality
8. Organization Municipality of the Klaipeda District
Klaipeda City Municipality
Public health bureau
Klaipeda university
Primary care centre
9. Data reporting (microbiological, consumption)
Klaipeda Territorial Health Insurance Fund
Centre of Public Health
Microbiology laboratories (of hospitals etc)
Primary care centre
1 table. Functions of health care related institutions in Klaipeda region
The third study was performed to learn perceptions and expectations related to AMR control of
primary care doctors, local health care administrators and public health officials.
The third study was performed to learn perceptions and expectations related to AMR control of
primary care doctors, local health care administrators and public health officials. Objectives of
interviews with primary care doctors, local health care administrators and public health officials
was to determine awareness about antimicrobial resistance problem and expectations about

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
21
necessary measures and actions to solve antimicrobial resistance problem. Face to face interviews
were performed. There were representatives of these institutions interviewed:
Public Health Centre
Klaipeda District Municipality Public Health Bureau
Klaipeda Public Health Bureau
Klaipeda Republican Hospital
Primary health care center
Public Health Centre
Public Health Centre
Interview with Head of Communicable Disease Division and Deputy director
Main current related activities: Public Health Centre collects information from all laboratories
and health care institutions about isolated recordable pathogens. MRSA, VRE, resistant
salmonella are among them but detailed analysis and feedback is not performed.
Possible future activities after creation of regional AMR group: Public Health Centre could
perform preventive measures (disseminate information to the public), cooperate and exchange
information with primary health care centers.
Identified problems: treatment algorithms for doctors are missing, they could be developed
during the project.
Klaipeda District Municipality Public Health Bureau
Interview with Director of Bureau and health promotion specialist
Main current related activities: Klaipeda District Municipality Public Health Bureau implements
preventive measures, which must be coordinated with municipality.
Possible future activities after creation of regional AMR group: Bureau could disseminate
information to the public, coordinate AMR group meetings.
Identified problems: what‘s missing for AMR problem solution in bureau: more knowledge on
AMR topics. Possible problems of participation in project: doubts about Klaipeda city and
Klaipeda district work compatibility, institution doesn‘t feel that could influence primary health
care specialists.
Klaipeda Public Health Bureau
Interview with Deputy director

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
22
Main current related activities: Public health bureau of Klaipeda city implements preventive
measures. Antimicrobial resistance management is one of bureau priority activities.
Possible future activities after creation of regional AMR group: Bureau could disseminate
information to the public and health care professionals.
Identified problems: what‘s missing in Bureau: more knowledge on AMR topics.
Klaipeda Republican Hospital
Interview with infection control specialist, microbiologist
Main current related activities: Klaipeda Republican Hospital collects antimicrobial resistance
data in the hospital, however data base non-computerized, data for only two years.
Possible future activities after creation of regional AMR group : Klaipeda Republican Hospital
could share experiences and hospital data.
Identified problems: what‘s missing for AMR problem solution in the hospital: computerized
program for collection and analysis of antimicrobial resistance data
Problems of participation in project implementation: too little cooperation between hospitals in
Klaipeda region, few microbiological samples from primary health care centers.
Primary health care center
Interview with Director and general practitioner
Main current related activities: Primary health care center coordinated and participated in Happy
audit study
Possible future activities after creation of regional AMR group: Center could be responsible for
clinical audit and lead the related subgroup.
Identified problems: what‘s missing for AMR problem solution in primary health care: treatment
recommendations, system where general practitioners could compare each other by prescribing
antibiotics, trainings on antimicrobial resistance and antibiotic prescribing topics.
Additional activities performed:
Visit to Sweden (4 persons) to learn about Strama work at national and local levels
Representatives from main Project partners (Institute of Hygiene, Klaipeda University) have
visited meeting in Hoor (Sweden) January 2012. During discussions with participation of the
meeting the Project implementation was reviewed and Swedish experience was learned. The
importance to involve health care administrators and policy makers was stressed out. There were

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
23
methods how to measure the effect of the program and effectiveness of STRAMA-like group
discussed.
The goal of the second phase of the Project was to prepare the regional’s strategy on
containment of antimicrobial resistance. Preparation of the proposal of strategy was implemented
in November 2011, February 2012.
Activities
Formation of regional antimicrobial management group
Preparation of working plan of regional antimicrobial management group
Formation of regional antimicrobial management group
Previous phase of the Project have identified potential stakeholders and suggested main areas of
activities for local antimicrobial management group. Meeting with STRAMA people in Sweden
have helped to set priorities and structure the proposals of AMR group composition and their
plan of action prepared by the specialist from the Institute of Hygiene.
The second phase started from Joint meeting of representatives from identified regional
stakeholders.
The main tasks for the meeting were to nominate AMR group members, set their priority
activities and discuss the working forms.
The regional meeting was organized in November 2011 inviting representatives from stakeholder
institutions: Health Sciences Faculty of Klaipeda University, JSC "My family doctor" (Primary
health center), Klaipeda Territorial Health Insurance Fund, Public Health Center, Public Health
Bureaus, doctors of Klaipeda municipality and Klaipeda district municipality and doctors
(epidemiologists, infection control specialists, microbiologists) form Klaipeda hospitals.
Participants - potential members of regional AMR management group were chosen from
institutions – stakeholders identified during the first phase of the Project whose functions were
partly related to management of antibiotic use and antimicrobial resistance. It was decided during
the meeting that in addition the regional AMR group should include different specialists from all
biggest Klaipeda region hospitals – one specialist per hospital (clinician, microbiologist or
infection control specialist). The call was sent out to all Klaipeda hospital to nominate persons.
ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
24
The specialists in the group were chosen by the areas of competence to perform the functions of
the group. The functions are: microorganisms resistant monitoring; public education; family
doctor; monitoring of antibacterial drug prescribing; funding; senior epidemiologist; public health
promotion and training;
Final composition of regional antimicrobial management group:
1. Janina Asadauskienė (Municipality doctor)
2. Ilona Bumblienė (Epidemiologist)
3. Alfridas Bumblys (Health Insurance Fund)
4. Rasa Girdžiūnienė (Infectious diseases doctor)
5. Arnoldas Jurgutis (Klaipeda University)
6. Laima Kaveckienė (Municipality doctor)
7. Rūta Markevičė (Institute of Hygiene)
8. Ineta Pačiauskaitė (Public health bureau)
9. Rūta Radzevičienė –Jurgutė (Primary health care physician)
10. Ona Sokolova (Public health centre)
11. Daiva Sriebalienė (Epidemiologist)
12. Jūratė Šuliauskaitė (Pediatrician)
13. Neringa Tarvydienė (Public health bureau)
14. Rita Vėlavičienė (Microbiologist)
There were short presentations done by representatives of some institutions to get better
understanding about currently available data, performed activities, experiences.
Main positive points :
- previous experience of Klaipeda University and family doctors in auditing antibiotic prescribing
during Happy audit project,
- some data on resistance of reportable pathogens available in Public Health Centre;
- data on consumption of reimbursed antibiotics (more relevant for children population) available
in regional health insurance fund with the availability to stratify data by doctor, clinic, patient.
Main problematic points:
- Most of the hospitals do not have computerized system in the microbiology laboratory;
- There are no tradition of collaboration between hospitals;

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
25
- Different institutions serve for the different population (e.g. – regional health insurance fund and
Public health centre – for Klaipeda region (several municipalities), public health bureau – for one
municipality, hospitals – differently)
After discussions the prioritization of activities was done and main areas of activities for Regional
AMR management group suggested were:
- Monitoring of resistance of infectious agents and creation of a data register;
- Creation of a data register of antibiotic use;
- Initiation of preparation of treatment guidelines;
- The feedback of data about antibiotic prescribing (from health insurance fund) to primary care
institutions;
Preparation of working plan of regional antimicrobial management group
The preparation of the working plan have started during the same Joint meeting. There were
short presentations done by representatives of some institutions to get better understanding
about currently available data, performed activities, experiences.
Main positive points identified :
- previous experience of Klaipeda University and family doctors in auditing antibiotic prescribing
during Happy audit project,
- some data on resistance of reportable pathogens available in Public Health Centre;
- data on consumption of reimbursed antibiotics (more relevant for children population) available
in regional health insurance fund with the availability to stratify data by doctor, clinic, patient.
Main problematic points identified:
- Most of the hospitals do not have computerized system in the microbiology laboratory;
- There are no tradition of collaboration between hospitals;
- Different institutions serve for the different population (e.g. – regional health insurance fund and
Public health centre – for Klaipeda region (several municipalities), public health bureau – for one
municipality, hospitals – differently)
After discussions the prioritization of activities was done and main areas of activities for Regional
AMR management group suggested were:
ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
26
- Monitoring of resistance of infectious agents and creation of a data register;
- Creation of a data register of antibiotic use;
- Initiation of preparation of treatment guidelines;
- The feedback of data about antibiotic prescribing (from health insurance fund) to primary care
institutions;
The final AMR management group action plan for 2012 have been finalized via electronic
communication and it includes key activities:
Coordination
- Training about antimicrobial resistant and antibiotic consumption for AMR management group
and others health care professionals (25 persons). (4. x 8 hrs. x 4 experts)
- Working group meetings (for 4 meetings per 2012)
- Working group meeting with a national group of AMR
Monitoring of antimicrobial resistance
- Creation of AMR monitoring database
- Determination of resistance of selected microorganisms (UTI study)
Monitoring of antimicrobial drugs consumption
- creation of audit system
- continuous surveillance of antibiotic consumption using regional health insurance fund data
- self medication study in Klaipeda city and district
Promotion and implementation of proper use of antibacterial agents
- dissemination of information to public
- a “simple” audit (sending information from regional health insurance fund on antibiotic
prescribing to family medicine centers)
- final conference.
The second meeting of the regional AMR group have been organized to approve the action plan
and approve the activity regulations rules.

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
27
The main functionsof the Group have been set as follow:
- disscuss and tackle arising antimicrobial resistance and antibiotic usage problems in the
Klaipeda region;
- participate in the monitoring of antimicrobial resistance and antibiotic consumption in Klaipeda
region;
- make suggestions and recommendations to local authorities, institutions and national experts to
prevent the spread of antimicrobial-resistant microorganisms and promote rational use of
antibiotics.
The group carrying out its functions is entitled to:
- get information for the Group's activities from the institutions whose representatives
participate in group activities;
- consult with other specialist (experts) not involved in the Group,
- prepare and offer the proposals and the necessary management decisions to solve the problems
of antimicrobial resistance.
4. Implementation of a regional model on containment of antimicrobial resistance (AMR model) in Klaipeda
Implementation of regional model on containment of antimicrobial resistance (AMR model) in
Klaipeda region (2012 March – December)
The implementation of key activities of AMR management group action plan for 2012:
Training on antimicrobial resistant and antibiotic consumption for regional AMR management
group and others health care professionals.
Inequalities in knowledge on AMR and related issues among representatives of all stakeholders
have been identified as one of the problems during the first Joint meeting was. So it was essential
to start the activities from the training of Group specialists.
The main topics of the training of Group were rational use of antibiotics and development,
control of resistance. The training was conducted in two session of two days (four days in total).
The target group of training was local antimicrobial resistance management group members,
general practitioners, microbiologists and other health professionals.
ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
28
National lecturers – recognized specialists in clinical microbiology and pharmacology have been
invited as lectors. The main topics were: „Antibiotics: Why is it important today to talk about
their rationale use? “, „Antimicrobial resistance: the situation in Europe and Lithuania“,
„Bacterial resistance to antimicrobials: mechanisms of resistance, detection methods and use of
results in clinical practice“, „Infection diagnosis and treatment challenges associated with multiple
resistance: ESBL-producing bacteria“, “The importance of clinical microbiology in diagnostic of
infectious diseases“, „Susceptibility to antimicrobial agents in: methods of antibiotic selection and
interpretation of the results“, “Proper use of antibiotics: appropriate principles of antimicrobial
drug use“.
The practical part of the training was spent to review and discuss in detail the activities from the
Group action plan.
Working group meetings (4 meetings per 2012)
Two group meetings were organized till July. First was organized to discuss about the analysis
and dissemination of antibiotic prescribing data from Klaipeda Territorial Health Insurance Fund
(feedback to Primary health care centers). Organization of study to evaluate the extent of self-
medication with antibiotics and knowledge about antibacterial medicines in Klaipeda region was
discussed during the second meeting.
The third meeting will take place in September to discuss the preparation of leaflets and other
information material to public informing them about the problem of antimicrobial resistance and
importance of proper use of antibiotics. The list of events dedicated to European antibiotic
awareness day (November 18) will be disussed and approved.
The fourth meeting will take place in the end of the year to review activities of 2012 and set the
palnt for 2013.
Monitoring of antimicrobial resistance
Creation of AMR monitoring database
As none of the laboratories have AMR monitoring database, the possibility to use WHONET
program in hospitals was discussed with all the laboratories ant decided to translate WHONET
program into Lithuanian language. The training to use of WHONET to specialists from
ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
29
microbiology laboratories will be carried in September 2012 followed by installation of the
program in hospitals.
Determination of resistance of selected microorganisms (UTI study)
In addition to ongoing resistance surveillance (mentioned in section 1.2.) pathogens of urinary
tract infections were selected for active antimicrobial resistance surveillance. The determination
of resistance of urinary tract infections agents is planning on October 2012, during the second
phase of UTI audit. It is planed to stimulate primary health doctors to take samples in all case of
UTI, determination of resistance of isolated bacteria will per carried out in one selected
laboratory.
Monitoring of antimicrobial drugs consumption
Creation of audit system
See - UTI audit study.
Continuous surveillance of antibiotic consumption using Klaipeda health insurance fund data.
It was decided to set the indicators and feedback to primary health centers information on
antibiotic prescribing. All the information will be treated confidentially. Health insurance fund
data have been selected as most easily accessed and well represented data source. Unfortunatelly
only information on reimbursed medicines is collected and due to national reimbursement system
(antibiotics are reimbursed for children (all diseases) and in few cases to adults (selected diseases
e.g. pneumonia) antibiotic prescribing for children (0-18 years) was selected for monitoring. The
list of indicators to monitor antibiotic consumption (prescribing) was set up during Group
meetings and training sessions. The main indicators for antibiotic monitoring have been
identified as follows:
- number of antibiotic prescriptions / 1000 children (0-18 years) in separate municipalities
of Klaipeda region 2011;
- number of antibiotic prescriptions to children / 1000 children (0-18 years) in separate
primary care centers of Klaipeda region 2011;
- percentage of phenoxymethylpenicillin prescriptions to children among all penicillin group
prescriptions to children in separate primary care centers of Klaipeda region 2011.
-
The first feedback to Primary Care Centers was send on June 2012 including data from 2011.
Another feedback is planning on September 2012, to present data of the half-year of 2012.

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
30
Self medication study in Klaipeda city and district
This study aims to evaluate extent of self-medication with antibiotics and knowledge about
antibacterial medicines among citizens of Klaipeda region. The ongoing survey which includes
interviews with 300 residents. The survey is carried out by Klaipeda city and district public health
bureau. Results of the study will be used to plan activities to rice public awareness about
resistance and prepare material for different public groups.
Promotion and implementation of proper use of antibacterial agents
A “simple” audit (sending information from regional health insurance fund on antibiotic
prescribing to primary care centers)
The first feedback to Primary Care Centers was send on June 2012 including data from 2011. All
the information is kept confidentially (not showing the names of other centers). Another
feedback is planning on September 2012, to present data of the half-year of 2012.
The report of the data was send to 41 primary care centers in all 7 municipalities of Klaipeda
region.
There were huge antibiotics prescribing differences (69 times) found between separate primary
health care centers when analyzing 2011 data. Low proportion (4,4 %) of narrow spectrum
antibiotics was discovered in most Primary care centers.
Dissemination of information to public
The main activities to dissemination project results and experience will start in the autumn of
2012: There are planed: meeting with doctors in Klaipeda hospitals, publishing of guidelines of
urinary tract infections diagnosis and treatment and final conference (November 2012). Activities
to public will be carried out as European antibiotic awareness day activities, their final list will be
approved in September.
5. A clinical audit on Urine Tract Infections (UTI), Klaipeda region Lithuania
As a part of the ImPrim project on Communicable diseases on how to counteract antibiotic
resistance an auditproject was carried out on UTI. The Audit was executed in two levels: in two
ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
31
Klaipeda hospitals and four PHC centers. Variables in hospitals and variables in primary care are
somewhat different also up numbers. Doctors in PC registered 61 variables for each patient and
in hospitals the doctors registered several more or a total of 120 variables for each patient. There
are of course both differences and similarities between patients in PHC and at hospital with UTI.
In hospital a patient with a pyelonephritis can be very severe case, while most UTI n PHC are
quite simple to handle. However, if a pyelonephritis has got a sepsis caused by a multi resistant
bacteria and the first therapy alternative will be inappropriate the outcome might be a
catastrophe.
Most patients with a pyelonephritis have had earlier more simple UTI. If they at those episodes
have got broad spectrum antibiotics the risk for coming resistant infections will be bigger. Still
there will all the time be less severe pyelonephritis who easily will be treated adequately and
effectively in PHC. So, this field has since long been complex and difficult.
Variables in the PHC UTI audit
Gender
Age
Symptoms and signs
Fever
Chills
Dysuria
Frequent urination
Suprapubic pain
Side (back) pain
General ailment
Genital symptoms
None of the listed
Duration in days
History
Urinary Tract Infection within 6 past
months
Antibiotics within 6 past months
Pregnancy
Investigations
Urine test with automatic analyzer
Urine strip test
Microscopy
CRP
Complete blood test
Urine culture
None of the listed
Urine test
Leukocytes rate < 100
Leukocytes rate 100 -250
Leukocytes rate 250 – 500
Erythrocytes rate < 10
Erythrocytes rate 10 – 20
Erythrocytes rate 20 – 30
Erythrocytes rate > 30
Nitrate positive
Nitrate negative
Urine culture
Not done
Done - no growth of bacteria

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
32
Growth of bacteria
E Coli
Other
Sensitivity
Amoxicillin
Amoxicillin with clavulanic r.
First generation cephalosporins:
cephalothin
Second generation cephalosporins:
cefuroxime
Third generation cephalosporins:
cefotaxime / ceftazidime
Trimethoprim / trimethoprim +
sulfamethoxazole
Nitrofurantoin
Ciprofloxacin
Norfloxacin
Doctor’s diagnosis
Cystitis
Pyelonephritis
Asymptomatic bacteriuria
Urinary tract infection for pregnant
women
Other urinary tract infection
Other information
The patient insisted on antibiotic
Referred to consultation of specialist /
hospitalized
None of the listed
Treatment
Waiting for culture results
Amoxicillin
Amoxicillin + clavulanic acid
Ciprofloxacin
Norfloxacin
Trimethoprim / sulfamethoxazole
Nitrofurantoin
Furadonin
First generation cephalosporins:
cephalothin
Second generation cephalosporins:
cefuroxime
Third generation cephalosporins:
cefotaxime / ceftazidime
No antibiotics prescribed
Herbal antiseptics
Duration of treatment (days)
Results
The first three figures show one obvious difference between PHC and hospital up to UTI
patients age and gender. We have a higher proportion of men in hospital mostly due to the older
patients with hypertrophic prostate. In lower ages girls and adult women are the most common
patients, mostly treated in PHC for a simple cystitis.
Figure UTI:1

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
33
Figure UTI:2
Figure UTI:3
Men Women
PHC 18,92% 79,73%
Hospital 38,18% 61,82%
0,00%
10,00%
20,00%
30,00%
40,00%
50,00%
60,00%
70,00%
80,00%
90,00%
Pe
r ce
nt
Urine Tract Infections in PHC and hospital, genders Klaipeda 2012
≤6ys 7-18ys 19-65ys ≥66ys
PHC 6,1% 6,8% 67,6% 19,6%
Hospital 0,0% 1,8% 34,5% 63,6%
0,0%
10,0%
20,0%
30,0%
40,0%
50,0%
60,0%
70,0%
80,0%
Pe
r ce
nt
Urine Tract Infections, PHC and hospital, Age groups Klaipeda 2012

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
34
Comment figure UTI.3: Interesting is that asymptomatic bacteriauria was as common on hospital as
in PHC. But also important will be that most severe infections, the pyelonephritis are as common
in PHC as the cases with asymptomatic bacteriauria.
Asymptom bact.uria
Cystitits Pyelonephritis Other
PHC 18,0% 43,0% 18,0% 32,0%
Hospital 18,0% 13,0% 55,0% 22,0%
0,0%
10,0%
20,0%
30,0%
40,0%
50,0%
60,0%
Diagnosis Urine Tract infections, Klaipeda 2012
ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
35
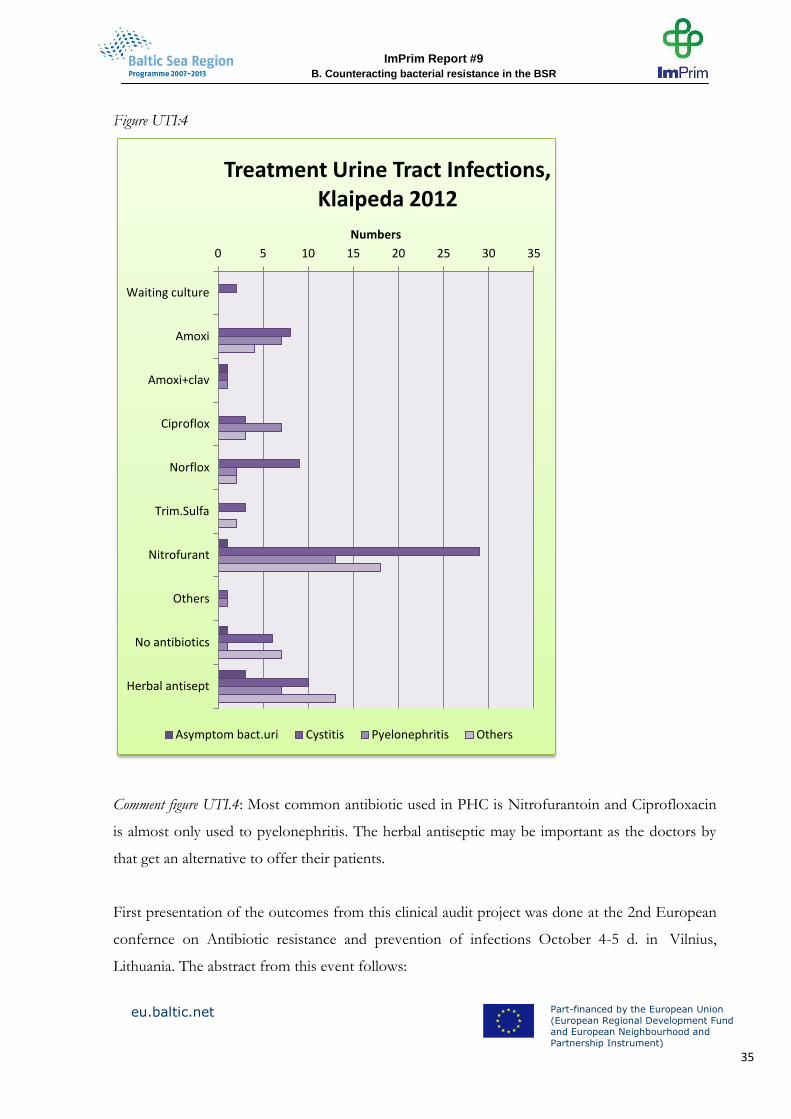
Figure UTI:4
Comment figure UTI.4: Most common antibiotic used in PHC is Nitrofurantoin and Ciprofloxacin
is almost only used to pyelonephritis. The herbal antiseptic may be important as the doctors by
that get an alternative to offer their patients.
First presentation of the outcomes from this clinical audit project was done at the 2nd European
confernce on Antibiotic resistance and prevention of infections October 4-5 d. in Vilnius,
Lithuania. The abstract from this event follows:
0 5 10 15 20 25 30 35
Waiting culture
Amoxi
Amoxi+clav
Ciproflox
Norflox
Trim.Sulfa
Nitrofurant
Others
No antibiotics
Herbal antisept
Numbers
Treatment Urine Tract Infections, Klaipeda 2012
Asymptom bact.uri Cystitis Pyelonephritis Others
ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
36
Abstract to present at at the 2nd European confernce on Antibiotic resistance and prevention of
infections October 4-5 d. in Vilnius, Lithuania.
Application of Apo Audit method for improvement of management of UTI in primary
health care and hospital care in Klaipeda
Bumbliene I.1,3, Strandberg E.L2,4, Radzeviciene R.1,5, Ovhed I.4, Jurgutis A.1, Salyga J.3,
Jukneviciute V.1.
1 Klaipedos University, 2 Lund University, 3 Klaipesda Seamens Hospital, 4 Blekinge Centre of
Competence, 5 JCC “Mano seimos gydytojas”
Clinical evidences show that inappropriate, irrational use of antibiotics is closely related to
bacterial resistance. Urine track infections are one of the most common diseases in primary
health care, as well as in inpatient care. Successful treatment of urine track infections highly
depends on identification of the microorganism that caused urine track infection, on the
prescription of appropriate antibiotic, it`s dose and the duration of treatment.
After the diagnosis of urine track infection physician usually starts the empirical antibacterial
treatment based only on the assumption about possible pathogen. However, choice of treatment
strategy depends on health care institution that the patient addresses. If the patient is treated in
inpatient care institution possibilities to identify the urine track infection agent and resistance to
antibiotics are higher. After the identification of urine track infection agent and resistance to
antimicrobial medicines, treatment with antibiotics becomes more rational.
In the end of year 2011 Klaipeda University Health Science Faculty Public Health Department
initiated urine track infections diagnostics and treatment study. The objective of the study was to
ascertain how family physicians and inpatient physicians diagnose and treat the patients with
urine track infections, applying internal quality control method (APO). The audit was
implemented in 3 levels: general practice level, outpatient care and inpatient care institutions. 23
family physicians, 17 doctors consultants of outpatient and inpatient departments’ participated in
the audit. According to the results of the study and learning objectives proposed by the doctors,
the training workshops were organised. Moreover, more appropriate conditions for diagnostic
were facilitated, and urine track infections protocols were prepared. Doctors’ participation on
voluntary bases creates more appropriate attitude towards rational use of antibiotics.

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
37
First follow-up meeting on UTI audit, Klaipeda region September 2012
The following report is direct notes from the first clinical audit on UTI registered parallel on two
both PHC and hospital level. The intense clinical discussion is demonstrated. It is the common
outcome from such a registration. The participants have a very concrete basis of data from their
own practice.
Initial group work
During the follow up meeting results of the first urinary tract infections (UTI) registration were
discussed by participating family doctors (FD) and specialist doctors (nephrologists, urologists,
rheabilitologists) in 5 small groups. Groups of 24 physicians discussed the results of the audit
approx. 50 min.
Meeting experts
After groups discussions some emerging issues were written on the sticky notes which were
placed on the flip chart board (separately GPs and specialists issues). All the doctors participated
in general discussion on the raised questions. Two experts - Jolanta Miciulevičienė - Laboratory
Medicine physician of Vilnius City Hospital Laboratory and Inga Skarupskienė – associated
professor from Kaunas Medical University Hospital Nephrology Clinic helped to answer unclear
questions. Issues that have been discussed:
• To prevent a recurrence of UTI, how much time a / b should be taken?
• Is there a need to treat asymptomatic bacteriuria ?
• Complete blood count test - is it informative for diagnostics?
• What was meant by "other urinary tract infection" when physicians marked it in the registration
chart?
• What should be duration of treatment with antibiotics?
When there are 25-75 leukocytes detected in automatic urine test - should the treatment for UTI
be given?
• Does it make sense for treatment with herbal antiseptics? How effective are they?
• How important is to perform the urinary red blood cell count?
• Where the primary health care doctors can perform a urine microscopy?
• Erythrocyte results – what do they tell?
• Is there a need for treatment with amoxicillin and clavulanic acid, why is not enough
amoxicillin?
• Microscopic or automatic analyzer urine test are better? Are they equivalent?
• Why do GPs cannot perform urine culture?
• Do re-visit means that the patient is not sufficiently cured?
• How much reasonable is to continue treatment with nitrofurantoin about 3 months 100mg
once per day?
How long in the hospital does it take to receive results of antibioticogram?
• Why in the hospital after receiving results of antibioticogram most often is given ceftriaxon?
Maybe it is according to some algorithm?

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
38
Comments and discussions
• Primary care doctors: the diagnosis of "another UTI infection" – is marked when the doctor is
not sure what diagnosis should be put, when it is not clear either it is cystitis or pyelonephritis.
Finally it was agreed that if there is fever and pain - more likely will be to diagnose pyelonephritis.
Asymptomatic bacteriuria is quite often diagnosed in primary care, but it is somehow confusing,
because there is no possibility to perform urine culture for GPs, and asymptomatic bacteriuria
can be diagnosed when 2 cultures in a row for women and one culture for men is positive. GPs
stated that they diagnosed asymptomatic bacteriuria when the patient had no symptoms, and
urine test not culture was positive.
Diagnosis of UTI depends a lot on collection of urine samples. Once again common rules and
mistakes for collecting urine sample were discussed by the participants.
Different policies
It became obvious that primary health care center and hospital opportunities to perform urine
tests vary. In the hospitals urine microscopy is always performed whenever the culture is sent. In
primary health care centers it is more difficult, because it is difficult to perform microscopy and
culture. It is not forbidden, but the state is not paying for this test, it costs 30-70 litas depending
on antibioticogram, only if the patient agrees to pay by himself, it can be performed. Suggestion
by the experts was that at least microscopic test in the laboratory should be done, if GPs find
leucocytes after performing automatic analysis of urine.
If acute severe illness is suspected GPs should do CRP, it is more valuable then to perform total
blood test, but in the case of pyelonephritis it should have some value.
Urea – is the least effective investigation to assess kidney function, although it is payed by the
state, but in acute UTI it is not valuable and is not worth doing.
Uncomplicated UTI (for young, premenopausal, non-pregnant women) is best treated without
antibiotics at all, but if necessary: first choice medication is nitrofurantoin (Nitrofurantoin
monohydrate) or sulfamethaxozol/trimetoprim (Biseptol,Septrin), second choice - quinolones,
however it is better not to start treatment with these medications.
Herbal antiseptics can be used in prevention, not treatment. There is some scientific evidence
that cranberries are effective for UTI prevention. But it should not be the one which is
prescribed for the acute infection.
The long-term nitrofurantoin treatment is accepted if UTI are happening more than 2 episodes
per half-year, or 3 - within one year. Pyelonephritis is more rare in primary care than the lower
UTI like cystitis. Nitrofurantoin is not suitable for treatment of pyelonephritis.
Gentamicin is not recommended for treatment of UTI in primary care also.
In the hospital antibioticogram results are got within few days, but in spite of other possibilities
of treatment most often was chosen ceftriaxon, because it is most cheap for the hospital to
buy!!!!!
Conclusions
Recommendations for treatment of any infection varies between countries, much depends on the
antibiotics market. Lithuania is too small a country to have its own guidelines, and must adapt to

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
39
other guidelines. However, what concerns the treatment at least American experience and
guidance should be avoided, because there is most worst situation with antibiotic resistance.
As a result of this project guidelines for primary care management of UTI should be published
with the guidance of Hygiene Institute.
The second registration will be carried out during autumn 2012. If urine culture in PHC will be
possible during that registration this project will produce totally new scientific knowledge.
6. Research study and Happy audit 2
Research study
The whole process on communicable diseases in ImPrim started up in 2011 and will be closed in
2012. However, the activities will continue far ahead. The topic is of crucial importance for
clinicians as well as for public health. Because of that, Swedish Sida now gives financial support
for a research study, aiming to evaluate scientifically the two projects – the regional “Strama” in
Lithuania and the clinical audit on UTI as well as the initiation of an audit centre in Klaipeda
region.
This research study is coordinated from Family medicine unit, Department of clinical sciences,
Malmö, Lunds university. A network of researchers from Lithuania and Sweden has been
formed. Two workshops have been carried out , in Klaipeda in sep 2011 and in Höör, Sweden
Jan 2012. During the last meeting professor Sigvard Mölstad described the strategy for the
Swedish Strama work like this: The overall objective is: “To preserve effective antibacterial
therapy for current and future generations” and Strama intend to;
Create a cross-sectorial national forum to
- share information
- formulate national strategies
- support and initiate research activities
- collaborate with media
Happy Audit 2
The two projects recommended from the BARN platform; “Strama in Lithuania” and “Klaipeda
Auditcentre” are carried out through financing from the EUS-BSR project ImPrim. During the

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
40
last BARN meeting in Vilnius was proposed that next step at the PHC level would be a clinical
audit among family doctors in Latvia, Lithuania, Poland, Sweden and Kaliningrad oblast. This
work, called “Happy Audit 2” has now started. Focus will be doctors’ diagnosis of RTI and their
prescribing of antibiotics. First registration period will be three weeks during October –
November 2012. That means a mapping of about 2000-3000 consultations from each country or
about 12-15 000 in total.
The following variables will be measured
Variables Happy Audit 2
Code doctor:
Date (day) for registration):
Patients age:
Patients gender:
1. Duration: days with symptoms
Symptoms
2. Fever (temp>38,5)
3. Cough and/or rhinorrhoea
4. Ear pain
5. Painful swalling
6. Tonsill exudat
7. Tender cerv gland
8. Dyspnoe or tachypnoe
9. Increased sputum
10. Purulent sputum
11. None
Investigation
12. StrepA positive
13. StrepA negative
14. CRP (mg/l)
15. X-ray positive
16. x-ray negative
17. None
Ethiology
18. Probably viral infection
19. Probably bacterial infection
Your diagnosis
20. Common cold
21. Acute media otitis
22. Acute sinusitis
23. Acute pharyngitis
24. Acute tonsillitis
26. Pneumonia
27. Exacerbation of COPD or chronic
bronchit
28. Influenza
29. Other acute RTI
Prescription of antibiotic
30. Penicillin V
31. Amoxi/pivampicillin
32. Amoxicillin + clavulan acid
33. macrolid
34. Chinolon
35. Tetracyclin
36. Cephalosporin
37. Other antibiotic
38. No antibiotic prescribed

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
41
Other activities/ decisions
39. Delayed prescription
40. Pc allergy
41. If possible I would have chosen PcV
tablets in this case.
42. Patient demands antibiotic therapy
43. Patient denies antibiotic therapy
43. Follow up own clinic
44. Referral to other spec/hospital
45. Neither
7. Discussion and conclusions
Several important steps have been taken during 2011 and 2012 to develop these projects on how
to counteract the development of antibiotic resistance. Even for the heavy fields Tuberculosis
and HIV- Aids have problems with increasing resistance developed. However, that will seldom
or perhaps almost never be a main problem in PHC research and therapy. Therefore the
permission to change focus for the ImPrim activities in the field communicable diseases became
very important. In stead of TBc/HIV focus was changed to antibiotic resistance among bacteria
which cause ordinary RTIs and UTIs. These infections are frequent in PHC and ordinary hospital
care. Doctors in PHC are prescribing more than 90% of all antibiotics.
Also of great importance has been the parallel establishing of the network BARN. Three out of
the ImPrim project partners took part in BARN from the beginning. Because of that, the
subprojects in ImPrim got support from authoritative specialists all around the BSR. Moreover
the project partners had thorough experiences from the earlier transnational EU project Happy
Audit. All together these prerequisites made it possible to start a series of important and
integrated parallel subprojects. The regional management group will be the start of a Strama like
national intervention in Lithuania. Register data for continuous control of resistance pattern and
antibiotic use will be of basic importance. The audit centre established at the department of
Public Health at Klaipeda university has already started up and delivered data from a clinical audit
on diagnosis and treatment of UTI in both PHC and hospital care. The follow up activities will
be an important intervention initiating clinical discussions and lectures based on the participants
own results.
The ImPrim subprojects on communicable diseases have been developed from a basis of
Evidence based medicine (EBM) in the field of Infectious diseases and antibiotic prescribing.
Transnational professional networks are important sources of inspiration. The projects illustrate
how the bottom-up perspective can be used as a support for the health care planning on the
national as well as the regional level. By this way of working, essential changes in health care may
ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
42
be most easy to initiate. Moreover, these projects, which have taken place inside the ImPrim
framework will continue in future network constellations like BARN. By that the ImPrim project
will initiate further research and development (R&D) projects in a crucial field.
STRATEGIES TO FOLLOW
According to the ambitious subprojects carried out in the ImPrim framework in this field the
strategy for a future work in PHC is quite clear. An important part in this work has been the
close collaboration with the high-level professional network; Baltic Antibiotic Resistance
collaboration Networks (BARN). Already has the ImPrim project in this field implied formation
of a regional group with a wide competence and area of responsibility. This group has started
eduction as well as carried out important clinical audit projects among doctors in both PHC and
hospital care. Moreover, has the sick fund published register data on antibiotic prescribing to
children.
Today is widely recognized that the increasing microbial resistance will be a future threat to a
continuing favourable development of public health.
The following conclusions may be drawn on what strategies to follow:
A regional and national strategy for containment of antimicrobial resistance must be formulated
Regional groups active in this field must be established, responsible for publishing guidelines as
well as continuous education activities supporting clinical audit projects in in prudent prescribing
of antibiotics.
Working with public health issues via media and direct to the population, especially families with
preschool children.
Working with more stringent demands for a optimal hygiene in hospitals
increasing public knowledge about hygiene and preventive care of different infectious diseases
Develop microbiological registers with continuous follow up of the national microbial resistance
pattern and feed-back to regional, national and international authorities.

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
43
Develop register on the continuous antibiotic consumption available for all patients.
Develop register on the continuous antibiotic consumption in veterinary medicine.
Develop a transnational strategy for collaboration in the field of antimicrobial resistance

ImPrim Report #9
B. Counteracting bacterial resistance in the BSR
eu.baltic.net
Part-financed by the European Union
(European Regional Development Fund and European Neighbourhood and
Partnership Instrument)
44
8. References
1. Håkansson A, Ovhed I, Jurgutis A, Kalda R, Ticmane G. Family medicine in the Baltic
countries. Scand J Prim Health Care. 2008;26(2):67-9.
2. Bjerrum L, Munck A, Gahrn-Hansen B, Hansen MP, Jarbol DE, Cordoba G, Llor C, Cots JM,
Hernández S, López-Valcárcel BG, Pérez A, Caballero L, von der Heyde W, Radzeviciene R,
Jurgutis A, Reutskiy A, Egorova E, Strandberg EL, Ovhed I, Mölstad S, Stichele RV, Benko R,
Vlahovic-Palcevski V, Lionis C, Rønning M.
Health Alliance for prudent antibiotic prescribing in patients with respiratory tract infections
(HAPPY AUDIT) -impact of a non-randomised multifaceted intervention programme. BMC
Fam Pract. 2011;12:52.
3. Strandberg EL. Developing General Practice: The Role of the APO-method. Thesis Lunds
university 2008.
4. Butler CC, Hood K, Kelly MJ, Goossens H, Verheij T, Little P, Melbye H, Torres A, Mölstad
S, Godycki-Cwirko M, Almirall J, Blasi F, Schaberg T, Edwards P, Rautakorpi UM, Hupkova H,
Wood J, Nuttall J, Coenen S. Treatment of acute cough/lower respiratory tract infection by
antibiotic class and associated outcomes: a 13 European country observational study in primary
care. J Antimicrob Chemother. 2010;65:2472-8. Epub 2010 Sep 18.
5. Strandberg EL, Ovhed I, Troein M, Håkansson A. Influence of self-registration on audit
participants and their non-participating colleagues. A retrospective study of medical records
concerning prescription patterns. Scand J Prim Health Care. 2005;23:42-6.













![092 2019 Dossier Ecosistema Urbano [+] Alternative Housing ... · 2000 Ecosistema Urbano, una oficina multidis-ciplinar —actualmente con sedes en Madrid y en Miami— cuyo enfoque](https://img.pdfslide.us/doc/110x75/5ec8fc90a1b3d77468652dc3/092-2019-dossier-ecosistema-urbano-alternative-housing-2000-ecosistema-urbano.jpg)











