Embed Size (px)
Citation preview

British Journul ,qf Phric Surgery ( 1997), 50, 135-l 38 0 1997 The Bntlsh Association of Plastic Surgeons
Replantation of part of an ear as an open fan composite graft
S.-C. Lin, H.-Y. Chiu, J.-C. Yu and J.-W. Lee
Section of Plastic Surgery, Department of Surgery, National Cheng-Kung University Hospital, Tuinan, Tuilvan
SUMMA R Y. A total amputation of the superior part of an ear with associated avulsion of adjacent scalp was treated successfully with a ‘fan’ technique, in which we unfolded the posterior skin envelope from the amputated ear segment and spread it onto part of the scalp defect of the temporal region. This resulted in a large area of contact between the composite graft and its recipient bed, with the added bonus of covering up some of the scalp defect. The remaining defect of the scalp was grafted with part of the avulsed scalp.
Various techniques for the reconstruction of a detached ear have been reported, yet the results have not been always satisfactory. Microsurgical replantation, if feasible, offers the best aesthetic result but the chances of completely successful replantation are scarce, owing to the extremely tiny vessels of the ear and the soft tissue damage which often occurs with the amputation.
Few options for reconstruction remain available if replantation is not practicable. The essential principle is to conserve as much of the original tissue as possible and to nourish it with the greatest amount of viable tissue to ensure its survival. The ‘fan’ technique described here is another application of this principle. In certain cases this procedure is a reasonable alterna- tive for salvage of an amputated ear.
Case report
A 25year-old-male worker sustained a complete ampu- tation of the superior part of his right ear together with avulsion of part of the scalp, when a piece of glass fell down onto his head (Fig. 1). He was sent to our hospital 2 hours after the accident and remained alert and in good general health. The severed part was brought by his family in a plastic bag cooled with ice. The amputated part had a contused, jagged and torn skin edge, contaminated with dirt.
13.5
The patient was brought to the operating room where microscopic examination showed no vessels available for microvascular anastomosis. Since there was a large defect in the skin above the ear, it occurred to us that we could fillet the posterior skin envelope of the ear to cover this defect. Therefore we elevated the posterior skin off the perichondrium and then fanned out the skin in an “open book” fashion as illustrated in Figure 2. The composite graft was inset into the ear and part of the scalp defect, using 510 Dexon for the cartilage and 6/O nylon for the skin. The residual defect in the temporal region was grafted with the retrieved piece of scalp after it had been defatted. A light bulky dressing was applied and systemic antibiotics were given both pre- and postoperatively. The wound was left undisturbed for one week. No vasodilator nor antico- agulant was prescribed. Seven days later, the dressing was removed, revealing a virtually complete graft “take”. There
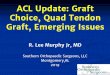
was a small area of epidermal breakdown (5 x 2 mm) over the helical rim, which ultimately necrosed and was allowed to heal by secondary intention (Fig. 3). Three weeks after the first operation, a second procedure was carried out to recreate the cephalo-auricular sulcus and the lateral projec- tion of the pinna. We elevated the replant from the mastoid region and covered the resulting postauricular defect with a full thickness skin graft taken from the right groin.
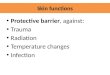
Six months later. the replanted segment of ear had a
Fig. 1
Figure l-Defects of right ear and scalp.

136 British Journal of Plastic Surgery
Fig. 2
Figure 2-Illustration of injured ear, with amputated part opened out like a fan.
good contour and normal texture with only a minor deficit in the helical rim (Fig. 4).
Discussion
Microsurgical replantation of the auricle following traumatic amputation remains the best reconstructive option.le4 However, in many situations, this alterna- tive may not be technically practicable. Various other techniques have been proposed, which involve in situ replacement of the cartilage alone or the whole auricle as a composite graft. The earliest report in the literature appeared in The Lancet in 1898.’ A lCyear- old boy had almost the whole of his right ear and an attached flap of postauricular scalp bitten off by a horse. The tissue was sutured back. The whole “graft” took, except for a small part of the rim above the lobule. The case was discussed by Gibson6 who pointed out that the key factor for free graft survival was a large area of surface contact. The same principle was applied successfully in the reconstruction of 6 noses and repair of 4 ears by Avelar et a1.,7 who in
one case used a composite skin graft of 30 cm2, without perforating its cartilage framework. Avelar et al. also briefly reviewed the history of composite skin/cartilage grafts.
A large area of contact between graft and recipient site is the mainstay of nonmicrosurgical approaches to salvage of an amputated ear. Various modifi- cations of the technique have been described. In 1971, Mladick et al* described the “pocket prin- ciple”, in which the skin over the amputated part is dermabraded and buried into a postauricular pocket for a blood supply. In 1972, Baudet et al.’ intro- duced the cartilage fenestration procedure. Destro and Speranzini” advocated preservation of part of the anterior skin envelope. Jenkins and Finucan” suggested sandwiching temporoparietal fascia between the filleted cartilage framework and the full- thickness auricular skin envelope. Ariyan and Chicarilli” replanted an ear with a platysma musculocutaneous “sandwich” flap. All of the above procedures share the common principle of “enrolling as much original auricular material as possible and bringing in the largest amount of vascularized tissue
Ear renlantation
Fig. 3
Figure 3-Early result after inset of composite graft.
available as to support the survival of the com- posite graft”.
With this basic concept in mind, we elected to broaden the effective contact surface by bivalving the auricular tissue and then spreading the two conjoined elements across the mastoid region and part of the temporal scalp defect. This design not only enhanced the chance of graft survival but also covered part of the adjacent scalp defect without creating another donor defect.
When presented with such an infrequent injury, the choice of surgical procedure depends upon various factors such as the time elapsed after the event, the size and location of the amputated part and the condition of the amputated segment and nearby skin. The “pocket-principle” may sometimes be difficult to apply in the presence of extensive destruction of peri- auricular skin. A distant or local flap such as the temporoparietal flap or platysma flap may have excessive bulk, resulting in a less than optimal result because of the poorly defined contours of the ear. Replacing anterior ear skin with skin from the mas- toid region is not ideal because the two types of skin are different. Therefore, using the amputated ear as a whole would be the most desirable approach. However, the chance of the amputated part surviving as a composite graft is the greatest concern. Following the basic principle proposed by Gibson6 Avelar et al.’ and others we employed a procedure which is quite similar to, yet still different in design from other pre-
Fig. 4
Figure 4-Final postoperative result
existing techniques. The final result indicates that the increased area of surface contact may well have been important for survival of this composite graft.
References
1. Mutimer KL, Banis JC, Upton J. Microsurgical reattachment of totally amputated ears. Plast Reconstr Surg 1987; 79: 535541.
2. Juri J, Irigaray A, Juri C, Grilli D, Blanc0 CM. Ear replantation. Plast Reconstr Surg 1987; 80: 431-5.
3. Tanaka Y, Tajima S. Completely successful replantation of an amputated ear by microvascular anastomosis. Plast Reconstr Surg 1989; 84: 66558.
4. Jeng SF, Wei FC, Noordhoff MS. Replantation of amputated facial tissues with microvascular anastomosis. Microsurgery 1994; 15: 327-33.
5. Brown WJ. Lancet 1898; i: 1533 (cited by Gibson). 6. Gibson T. Early free grafting: the restitution of parts com-
pletely separated from the body. Br J Plast Surg 1965; 18: l-11.
7. Avelar JM, Psillakis JM, Viterbo F. Use of large composite grafts in the reconstruction of deformities of the nose and ear. Br J Plast Surg 1984; 37: 55-60.
8. Mladick RA, Horton CE, Adamson JE, Cohen BI. The pocket principle: a new technique for the reattachment of a severed ear part. Plast Reconstr Surg 1971; 48: 219923.
9. Baudet J, Tramond P, Goumain A. A propos d’un pro&de original de reimplantation d’un pavilon de l’oreille totale- ment separe. Ann Chir Plast 1972; 17: 67772.
10. Destro MW, Speranzini MB. Total reconstruction of the auricle after traumatic amputation, Plast Reconstr Surg 1994; 94: 859964.

138
11. Jenkins AM, Finucan T. Primary nonmicrosurgical reconstruc- tion following ear avulsion using the temporoparietal fascial island flap. Plast Reconstr Surg 1989; 83: 148-52.
12. Ariyan S, Chicarilli ZN. Replantation of a totally amputated ear by means of a platysma musculocutaneous “sandwich” flap. Plast Reconstr Surg 1986; 78: 385-9.
The Authors
Sheng-Che Lin MD, Staff Plastic Surgeon Haw-Yen Chiu MD, Professor and Chief
British Journal of Plastic Surgery
Jui-Chin Yu MD, Chief Resident of Plastic Surgeon Jing-Wei Lee MD, Lecturer Section of Plastic Surgery, Department of Surgery, National
Cheng-Kung University Hospital, 138 Sheng-Li Road, Tainan 70428, Taiwan.
Correspondence to Jing-Wei Lee MD.
Paper received 7 August 1996. Accepted 22 October 1996, after revision.