Embed Size (px)
Citation preview

1392 http://www.journal-imab-bg.org / J of IMAB. 2016, vol. 22, issue 4/
DENTAL CARE FOR CHILDREN AFTERREPLANTATION OF AVULSED PERMANENTINCISORS
Rossitza Kabaktchieva1, Natalia Gateva1, Angela Gusiyska2, Pavel Stanimirov3, NinaMilcheva4
1) Department of pediatric dentistry, Faculty of Dental medicine, MedicalUniversity- Sofia, Bulgaria2) Department of Conservative Dentistry, Faculty of Dental medicine, MedicalUniversity- Sofia, Bulgaria3) Department of Oral and Maxillo-Facial Surgery, Faculty of Dental medicine,Medical University- Sofia, Bulgaria4) Department of pediatric dentistry, Faculty of Dental medicine, MedicalUniversity-Varna, Bulgaria
Journal of IMAB - Annual Proceeding (Scientific Papers) 2016, vol. 22, issue 4Journal of IMABISSN: 1312-773Xhttp://www.journal-imab-bg.org
SUMMARY:The diagnosis avulsion of permanent tooth/teeth is
an emergency situation which has special requirements inrespect of proper storage of the avulsed tooth, the need ofurgent medical/dental care, time past till replantation andsplinting, the need for endodontic treatment and long termfollow up period. Those clinical actions depend on threegroups: parents/people who are with the child in the mo-ment when trauma happens and give the first aid; dentalspecialist- surgeon who replants the tooth/teeth; dentalspecialist- endodontist who takes care of the endodontictreatment and the long period after treatment for follow upand observation of the replanted teeth.
The aim of the paper is to present the dental post-operative care in a couple of cases of children with traumaand replanted avulsed permanent incisors.
Material and methods: We present four clinicalcases of children who get 6 permanent upper incisors re-planted. Replantation is made by the oral surgeon. Treat-ment and observation after replantation are made by den-tal specialists of pediatric dentistry and conservative den-tistry. All 4 cases get 3 years follow up period.
Results: After replantation of 2 central incisors withcomplete root development (first clinical case) the left onehas developed a resorption of the root but the right one isin a stable condition. Replantation of 3 teeth with incom-plete root development (second and third clinical cases)where the patients refer to specialized surgical care lessthan 60 minutes after injury and store the teeth in differ-ent ways lead to different clinical results. In the case ofavulsed upper right incisor (second case), it is stored inmilk and we observe revascularization followed by partialroot canal obliteration. The tooth is scheduled for endo-dontic treatment. In the case of upper central incisors, bothkept dry till replantation in the alveolus filled up with sub-stitute bone, we observe fast root resorption which goingto lead to early tooth loss. After replantation of the firstupper incisor with open apex, stored in physiological so-lution for 5 hours and with delayed endodontic treatment
(forth case) healing process is stable and the prognosis isgood. Follow up period for all the replanted teeth has con-tinued.
Conclusion: The presented clinical cases show thatthere is a lack of dental teams for complex treatment of chil-dren with avulsed teeth in Bulgaria. Dental specialists haveno good information about recommended by IADTprotocols (www.iadt-dentaltrauma.org), for the treatment ofteeth undergoes avulsion during childhood. Parents of thesechildren have no proper information about how to store theteeth which are avulsed and found immediately aftertrauma.
Keywords: dental trauma, dental avulsion, replan-tation, permanent teeth,
Àvulsion is one of the most serious dental injuries [1-6]. Prognosis for the replanted permanent teeth in childrenis hard and the åxtraoral storage of the avulsed tooth [7],time past from the moment of trauma till that of replanta-tion of the avulsed tooth [8], the stage of root development[9, 10]and protocol for replantation [2, 3] are important forit. The aim of replantation is to restore the aesthetics, func-tion and to maintain the alveolar bone contour [1, 2, 11-13]. Prognosis for replantation of permanent teeth which stayout of the mouth less than 60 minutes after an accident isgood and expected ankylosis lead to slow root resorptionafter a couple of years [2, 3, 14, 15]. Revascularization ofthe replanted teeth with immature root development is a re-markable outcome [9, 16]. Replantation after more than 60minutes after the accident (delayed replantation) has a poorlong-term prognosis. The periodontal ligament will benecrotic and not expected to heal. The goal in delayed re-plantation is, in addition, to restoring the tooth for esthetic,functional and psychological reasons and to maintain alveo-lar bone contour [2, 3, 17, 18]. However, the expected out-come is ankylosis, root resorption, and eventual tooth loss[2, 3, 19, 20]. In the last few years, dental practitioners re-port for coronal removal of replanted teeth and successful
https://doi.org/10.5272/jimab.2016224.1392
/ J of IMAB. 2016, vol. 22, issue 4/ http://www.journal-imab-bg.org 1393
preservation of the alveolar contour [21, 22, 23]. All effortsabout the long term complicated treatment are made for thepreservation of the alveolar bone [1, 2, 3].
There are three important aspects in a discussionabout traumatic injuries like avulsion: information for firstaid and proper storage of the avulsed tooth [24 - 30], mod-ernization of the replantation protocol [12, 31-34]and theprofessional medical and dental care for the replantedtooth[12, 35- 40].
The aim of the article is to present dental postop-erative care for children with replanted avulsed permanentincisors.
MATERIAL AND METHODS:We present four clinical cases of children with re-
planted six permanent upper incisors. Protocols for replan-tation are performed by oral surgeons. Pediatric dentists andendodontists take the postoperative dental care and con-trol the follow up period. Presented clinical cases are fol-
lowed up for 3 years. The method of case‘s presentation isdescriptive, illustrated with pictures and X-rays, which givea short information about the treatment in the emergencysituation and later in the period of postoperative care.
First clinical caseA. I., 11 years old girl. She had syncope and hit her
face on the floor and as a result avulsed her upper incisors.She was taken to the hospital and after EEG and detailedmedical check - up she was scheduled for replantation ofthe avulsed teeth under general anesthesia. The teethstayed out of the mouth for about 1 hour and were storeddry. The injured teeth were with completed root develop-ment. There was no information about the protocol of re-plantation of the incisors in the hospital. The teeth wereimmobilized by a rigid metal splint (fig. 1-A, B). Tooth 11was replanted in infra occlusion compared to tooth 21 ac-cording to an old radiograph (fig. 1-C). Antibiotics wereprescribed to the patients.
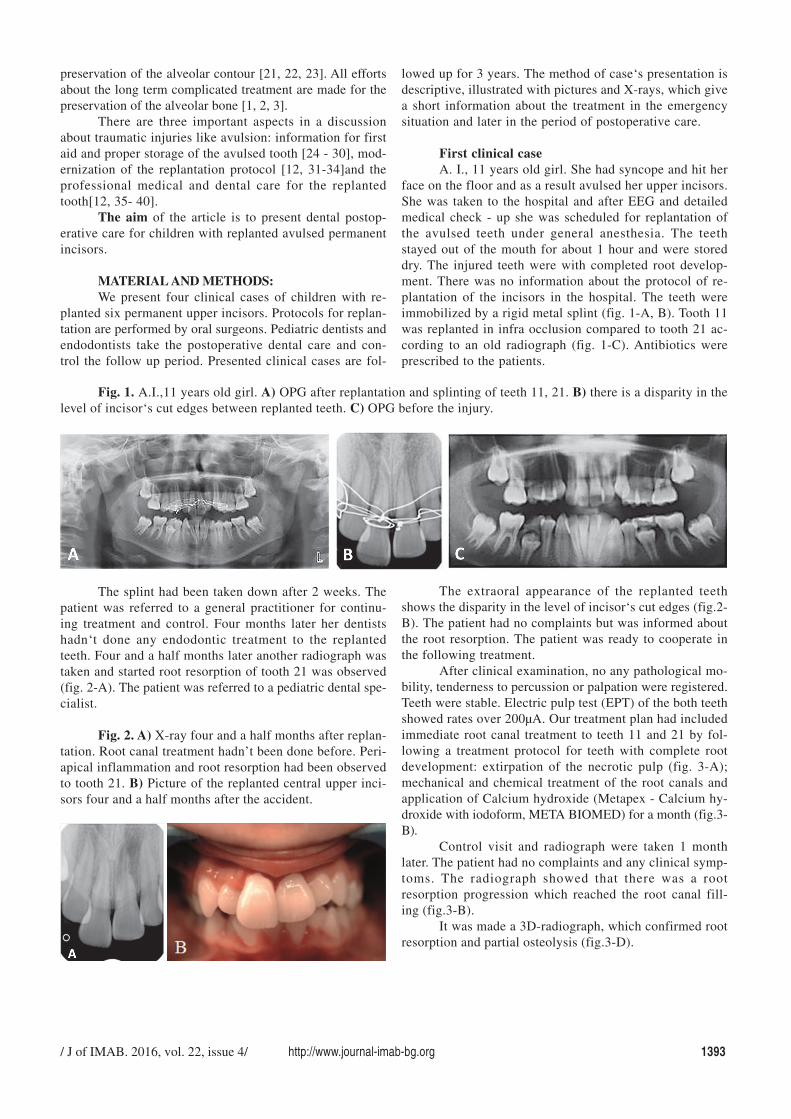
Fig. 1. A.I.,11 years old girl. A) OPG after replantation and splinting of teeth 11, 21. B) there is a disparity in thelevel of incisor‘s cut edges between replanted teeth. C) OPG before the injury.
The splint had been taken down after 2 weeks. Thepatient was referred to a general practitioner for continu-ing treatment and control. Four months later her dentistshadn‘t done any endodontic treatment to the replantedteeth. Four and a half months later another radiograph wastaken and started root resorption of tooth 21 was observed(fig. 2-A). The patient was referred to a pediatric dental spe-cialist.
Fig. 2. A) X-ray four and a half months after replan-tation. Root canal treatment hadn’t been done before. Peri-apical inflammation and root resorption had been observedto tooth 21. B) Picture of the replanted central upper inci-sors four and a half months after the accident.
The extraoral appearance of the replanted teethshows the disparity in the level of incisor‘s cut edges (fig.2-B). The patient had no complaints but was informed aboutthe root resorption. The patient was ready to cooperate inthe following treatment.
After clinical examination, no any pathological mo-bility, tenderness to percussion or palpation were registered.Teeth were stable. Electric pulp test (EPT) of the both teethshowed rates over 200µA. Our treatment plan had includedimmediate root canal treatment to teeth 11 and 21 by fol-lowing a treatment protocol for teeth with complete rootdevelopment: extirpation of the necrotic pulp (fig. 3-A);mechanical and chemical treatment of the root canals andapplication of Calcium hydroxide (Metapex - Calcium hy-droxide with iodoform, META BIOMED) for a month (fig.3-B).
Control visit and radiograph were taken 1 monthlater. The patient had no complaints and any clinical symp-toms. The radiograph showed that there was a rootresorption progression which reached the root canal fill-ing (fig.3-B).
It was made a 3D-radiograph, which confirmed rootresorption and partial osteolysis (fig.3-D).
1394 http://www.journal-imab-bg.org / J of IMAB. 2016, vol. 22, issue 4/
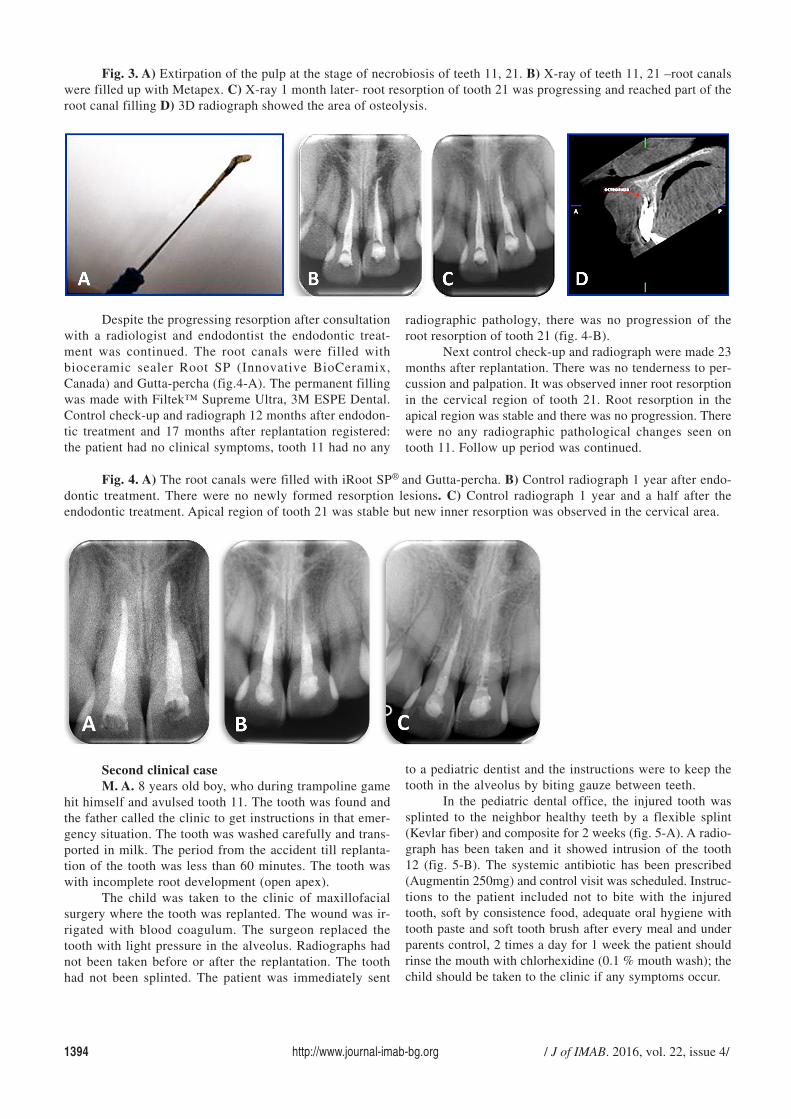
Fig. 3. A) Extirpation of the pulp at the stage of necrobiosis of teeth 11, 21. B) X-ray of teeth 11, 21 –root canalswere filled up with Metapex. C) X-ray 1 month later- root resorption of tooth 21 was progressing and reached part of theroot canal filling D) 3D radiograph showed the area of osteolysis.
Despite the progressing resorption after consultationwith a radiologist and endodontist the endodontic treat-ment was continued. The root canals were filled withbioceramic sealer Root SP (Innovative BioCeramix,Canada) and Gutta-percha (fig.4-A). The permanent fillingwas made with Filtek™ Supreme Ultra, 3M ESPE Dental.Control check-up and radiograph 12 months after endodon-tic treatment and 17 months after replantation registered:the patient had no clinical symptoms, tooth 11 had no any
radiographic pathology, there was no progression of theroot resorption of tooth 21 (fig. 4-B).
Next control check-up and radiograph were made 23months after replantation. There was no tenderness to per-cussion and palpation. It was observed inner root resorptionin the cervical region of tooth 21. Root resorption in theapical region was stable and there was no progression. Therewere no any radiographic pathological changes seen ontooth 11. Follow up period was continued.
Fig. 4. A) The root canals were filled with iRoot SP® and Gutta-percha. B) Control radiograph 1 year after endo-dontic treatment. There were no newly formed resorption lesions. C) Control radiograph 1 year and a half after theendodontic treatment. Apical region of tooth 21 was stable but new inner resorption was observed in the cervical area.
Second clinical caseM. A. 8 years old boy, who during trampoline game
hit himself and avulsed tooth 11. The tooth was found andthe father called the clinic to get instructions in that emer-gency situation. The tooth was washed carefully and trans-ported in milk. The period from the accident till replanta-tion of the tooth was less than 60 minutes. The tooth waswith incomplete root development (open apex).
The child was taken to the clinic of maxillofacialsurgery where the tooth was replanted. The wound was ir-rigated with blood coagulum. The surgeon replaced thetooth with light pressure in the alveolus. Radiographs hadnot been taken before or after the replantation. The toothhad not been splinted. The patient was immediately sent
to a pediatric dentist and the instructions were to keep thetooth in the alveolus by biting gauze between teeth.
In the pediatric dental office, the injured tooth wassplinted to the neighbor healthy teeth by a flexible splint(Kevlar fiber) and composite for 2 weeks (fig. 5-A). A radio-graph has been taken and it showed intrusion of the tooth12 (fig. 5-B). The systemic antibiotic has been prescribed(Augmentin 250mg) and control visit was scheduled. Instruc-tions to the patient included not to bite with the injuredtooth, soft by consistence food, adequate oral hygiene withtooth paste and soft tooth brush after every meal and underparents control, 2 times a day for 1 week the patient shouldrinse the mouth with chlorhexidine (0.1 % mouth wash); thechild should be taken to the clinic if any symptoms occur.
/ J of IMAB. 2016, vol. 22, issue 4/ http://www.journal-imab-bg.org 1395
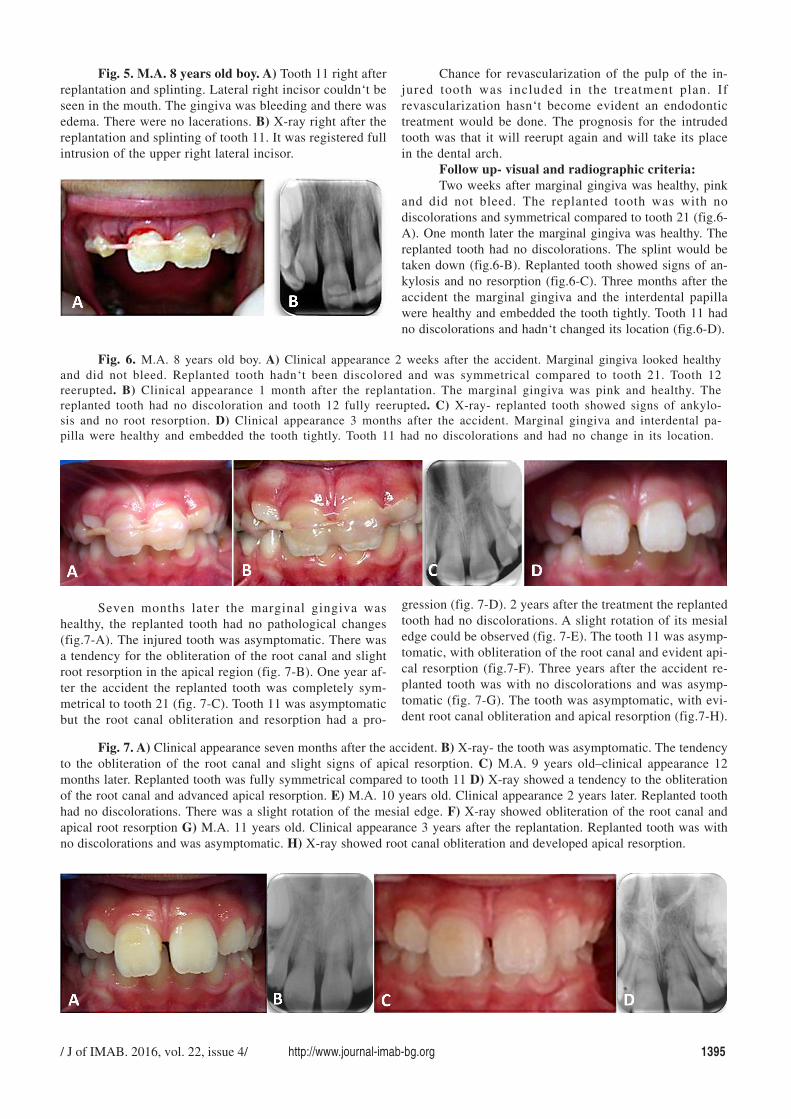
Fig. 5. M.A. 8 years old boy. A) Tooth 11 right afterreplantation and splinting. Lateral right incisor couldn‘t beseen in the mouth. The gingiva was bleeding and there wasedema. There were no lacerations. B) X-ray right after thereplantation and splinting of tooth 11. It was registered fullintrusion of the upper right lateral incisor.
Chance for revascularization of the pulp of the in-jured tooth was included in the treatment plan. Ifrevascularization hasn‘t become evident an endodontictreatment would be done. The prognosis for the intrudedtooth was that it will reerupt again and will take its placein the dental arch.
Follow up- visual and radiographic criteria:Two weeks after marginal gingiva was healthy, pink
and did not bleed. The replanted tooth was with nodiscolorations and symmetrical compared to tooth 21 (fig.6-A). One month later the marginal gingiva was healthy. Thereplanted tooth had no discolorations. The splint would betaken down (fig.6-B). Replanted tooth showed signs of an-kylosis and no resorption (fig.6-C). Three months after theaccident the marginal gingiva and the interdental papillawere healthy and embedded the tooth tightly. Tooth 11 hadno discolorations and hadn‘t changed its location (fig.6-D).
Fig. 6. M.A. 8 years old boy. A) Clinical appearance 2 weeks after the accident. Marginal gingiva looked healthyand did not bleed. Replanted tooth hadn‘t been discolored and was symmetrical compared to tooth 21. Tooth 12reerupted. B) Clinical appearance 1 month after the replantation. The marginal gingiva was pink and healthy. Thereplanted tooth had no discoloration and tooth 12 fully reerupted. C) X-ray- replanted tooth showed signs of ankylo-sis and no root resorption. D) Clinical appearance 3 months after the accident. Marginal gingiva and interdental pa-pilla were healthy and embedded the tooth tightly. Tooth 11 had no discolorations and had no change in its location.
Seven months later the marginal gingiva washealthy, the replanted tooth had no pathological changes(fig.7-A). The injured tooth was asymptomatic. There wasa tendency for the obliteration of the root canal and slightroot resorption in the apical region (fig. 7-B). One year af-ter the accident the replanted tooth was completely sym-metrical to tooth 21 (fig. 7-C). Tooth 11 was asymptomaticbut the root canal obliteration and resorption had a pro-
gression (fig. 7-D). 2 years after the treatment the replantedtooth had no discolorations. A slight rotation of its mesialedge could be observed (fig. 7-E). The tooth 11 was asymp-tomatic, with obliteration of the root canal and evident api-cal resorption (fig.7-F). Three years after the accident re-planted tooth was with no discolorations and was asymp-tomatic (fig. 7-G). The tooth was asymptomatic, with evi-dent root canal obliteration and apical resorption (fig.7-H).
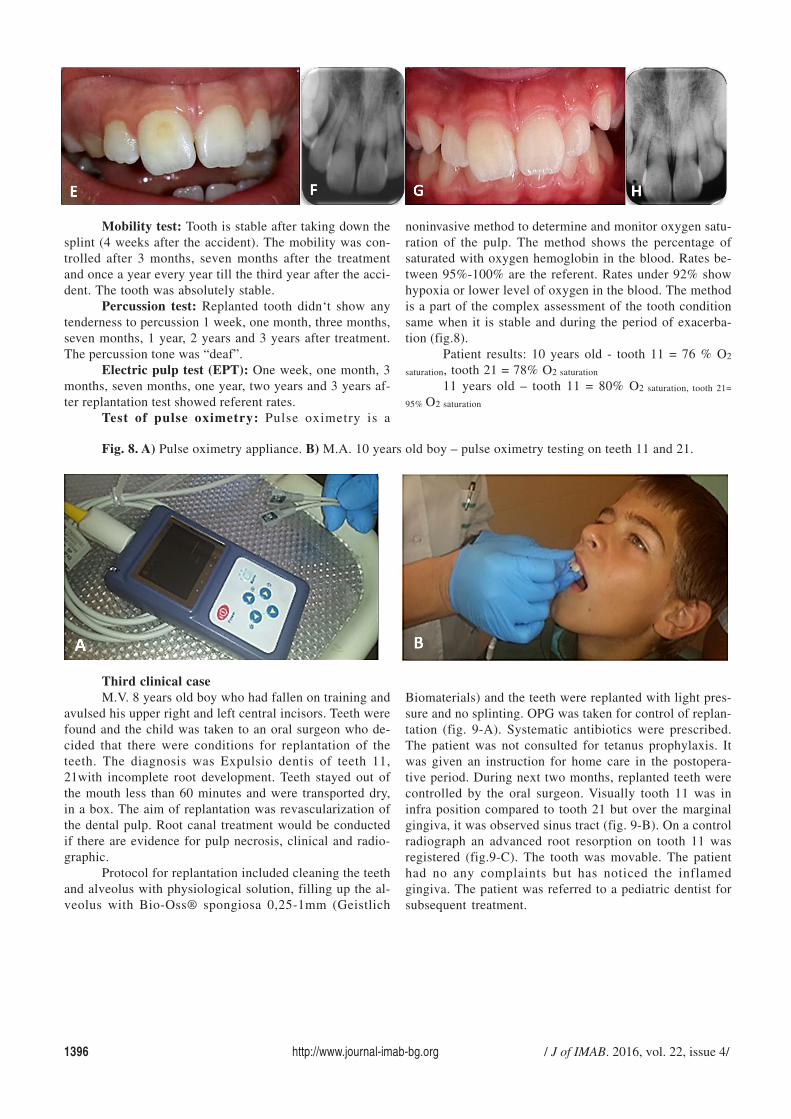
Fig. 7. A) Clinical appearance seven months after the accident. B) X-ray- the tooth was asymptomatic. The tendencyto the obliteration of the root canal and slight signs of apical resorption. C) M.A. 9 years old–clinical appearance 12months later. Replanted tooth was fully symmetrical compared to tooth 11 D) X-ray showed a tendency to the obliterationof the root canal and advanced apical resorption. E) M.A. 10 years old. Clinical appearance 2 years later. Replanted toothhad no discolorations. There was a slight rotation of the mesial edge. F) X-ray showed obliteration of the root canal andapical root resorption G) M.A. 11 years old. Clinical appearance 3 years after the replantation. Replanted tooth was withno discolorations and was asymptomatic. H) X-ray showed root canal obliteration and developed apical resorption.
1396 http://www.journal-imab-bg.org / J of IMAB. 2016, vol. 22, issue 4/
Mobility test: Tooth is stable after taking down thesplint (4 weeks after the accident). The mobility was con-trolled after 3 months, seven months after the treatmentand once a year every year till the third year after the acci-dent. The tooth was absolutely stable.
Percussion test: Replanted tooth didn‘t show anytenderness to percussion 1 week, one month, three months,seven months, 1 year, 2 years and 3 years after treatment.The percussion tone was “deaf”.
Electric pulp test (EPT): One week, one month, 3months, seven months, one year, two years and 3 years af-ter replantation test showed referent rates.
Test of pulse oximetry: Pulse oximetry is a
noninvasive method to determine and monitor oxygen satu-ration of the pulp. The method shows the percentage ofsaturated with oxygen hemoglobin in the blood. Rates be-tween 95%-100% are the referent. Rates under 92% showhypoxia or lower level of oxygen in the blood. The methodis a part of the complex assessment of the tooth conditionsame when it is stable and during the period of exacerba-tion (fig.8).
Patient results: 10 years old - tooth 11 = 76 % O2
saturation, tooth 21 = 78% O2 saturation
11 years old – tooth 11 = 80% O2 saturation, tooth 21=
95% O2 saturation
Fig. 8. A) Pulse oximetry appliance. B) M.A. 10 years old boy – pulse oximetry testing on teeth 11 and 21.
Third clinical caseM.V. 8 years old boy who had fallen on training and
avulsed his upper right and left central incisors. Teeth werefound and the child was taken to an oral surgeon who de-cided that there were conditions for replantation of theteeth. The diagnosis was Expulsio dentis of teeth 11,21with incomplete root development. Teeth stayed out ofthe mouth less than 60 minutes and were transported dry,in a box. The aim of replantation was revascularization ofthe dental pulp. Root canal treatment would be conductedif there are evidence for pulp necrosis, clinical and radio-graphic.
Protocol for replantation included cleaning the teethand alveolus with physiological solution, filling up the al-veolus with Bio-Oss® spongiosa 0,25-1mm (Geistlich
Biomaterials) and the teeth were replanted with light pres-sure and no splinting. OPG was taken for control of replan-tation (fig. 9-A). Systematic antibiotics were prescribed.The patient was not consulted for tetanus prophylaxis. Itwas given an instruction for home care in the postopera-tive period. During next two months, replanted teeth werecontrolled by the oral surgeon. Visually tooth 11 was ininfra position compared to tooth 21 but over the marginalgingiva, it was observed sinus tract (fig. 9-B). On a controlradiograph an advanced root resorption on tooth 11 wasregistered (fig.9-C). The tooth was movable. The patienthad no any complaints but has noticed the inflamedgingiva. The patient was referred to a pediatric dentist forsubsequent treatment.
/ J of IMAB. 2016, vol. 22, issue 4/ http://www.journal-imab-bg.org 1397
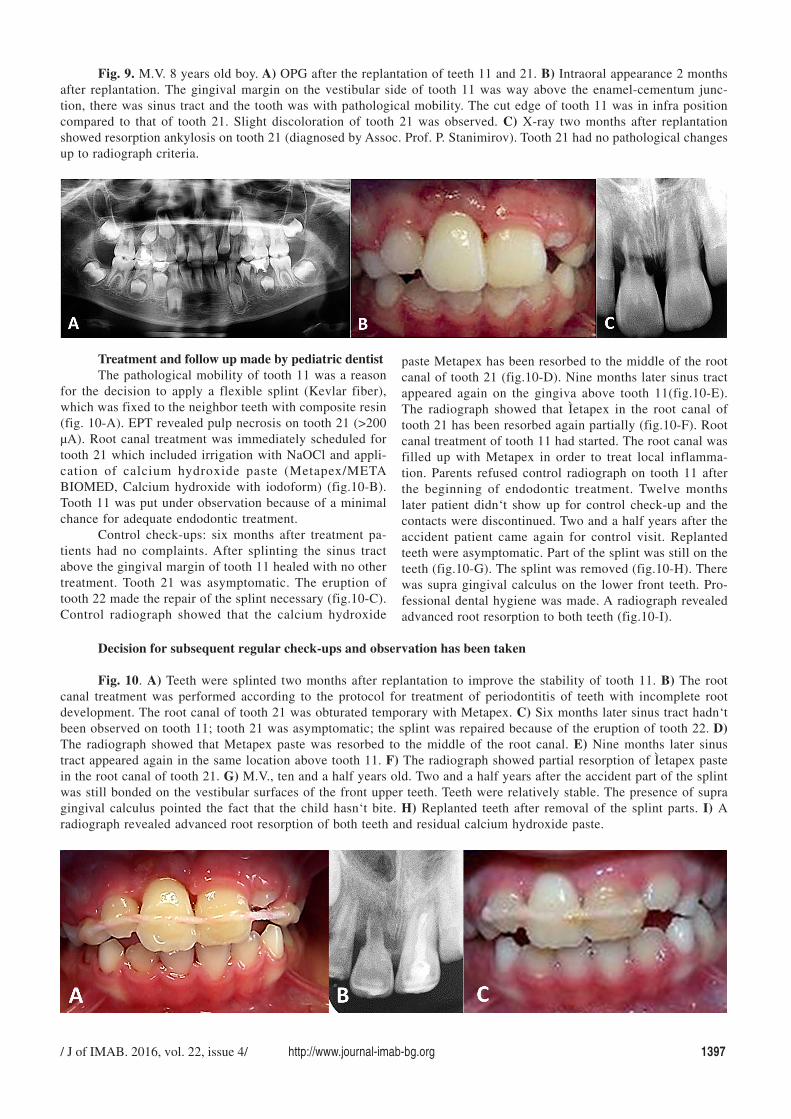
Fig. 9. M.V. 8 years old boy. A) OPG after the replantation of teeth 11 and 21. B) Intraoral appearance 2 monthsafter replantation. The gingival margin on the vestibular side of tooth 11 was way above the enamel-cementum junc-tion, there was sinus tract and the tooth was with pathological mobility. The cut edge of tooth 11 was in infra positioncompared to that of tooth 21. Slight discoloration of tooth 21 was observed. C) X-ray two months after replantationshowed resorption ankylosis on tooth 21 (diagnosed by Assoc. Prof. P. Stanimirov). Tooth 21 had no pathological changesup to radiograph criteria.
Treatment and follow up made by pediatric dentistThe pathological mobility of tooth 11 was a reason
for the decision to apply a flexible splint (Kevlar fiber),which was fixed to the neighbor teeth with composite resin(fig. 10-A). EPT revealed pulp necrosis on tooth 21 (>200µA). Root canal treatment was immediately scheduled fortooth 21 which included irrigation with NaOCl and appli-cation of calcium hydroxide paste (Metapex/METABIOMED, Calcium hydroxide with iodoform) (fig.10-B).Tooth 11 was put under observation because of a minimalchance for adequate endodontic treatment.
Control check-ups: six months after treatment pa-tients had no complaints. After splinting the sinus tractabove the gingival margin of tooth 11 healed with no othertreatment. Tooth 21 was asymptomatic. The eruption oftooth 22 made the repair of the splint necessary (fig.10-C).Control radiograph showed that the calcium hydroxide
paste Metapex has been resorbed to the middle of the rootcanal of tooth 21 (fig.10-D). Nine months later sinus tractappeared again on the gingiva above tooth 11(fig.10-E).The radiograph showed that Ìetapex in the root canal oftooth 21 has been resorbed again partially (fig.10-F). Rootcanal treatment of tooth 11 had started. The root canal wasfilled up with Metapex in order to treat local inflamma-tion. Parents refused control radiograph on tooth 11 afterthe beginning of endodontic treatment. Twelve monthslater patient didn‘t show up for control check-up and thecontacts were discontinued. Two and a half years after theaccident patient came again for control visit. Replantedteeth were asymptomatic. Part of the splint was still on theteeth (fig.10-G). The splint was removed (fig.10-H). Therewas supra gingival calculus on the lower front teeth. Pro-fessional dental hygiene was made. A radiograph revealedadvanced root resorption to both teeth (fig.10-I).
Decision for subsequent regular check-ups and observation has been taken
Fig. 10. A) Teeth were splinted two months after replantation to improve the stability of tooth 11. B) The rootcanal treatment was performed according to the protocol for treatment of periodontitis of teeth with incomplete rootdevelopment. The root canal of tooth 21 was obturated temporary with Metapex. C) Six months later sinus tract hadn‘tbeen observed on tooth 11; tooth 21 was asymptomatic; the splint was repaired because of the eruption of tooth 22. D)The radiograph showed that Metapex paste was resorbed to the middle of the root canal. E) Nine months later sinustract appeared again in the same location above tooth 11. F) The radiograph showed partial resorption of Ìetapex pastein the root canal of tooth 21. G) M.V., ten and a half years old. Two and a half years after the accident part of the splintwas still bonded on the vestibular surfaces of the front upper teeth. Teeth were relatively stable. The presence of supragingival calculus pointed the fact that the child hasn‘t bite. H) Replanted teeth after removal of the splint parts. I) Aradiograph revealed advanced root resorption of both teeth and residual calcium hydroxide paste.
1398 http://www.journal-imab-bg.org / J of IMAB. 2016, vol. 22, issue 4/
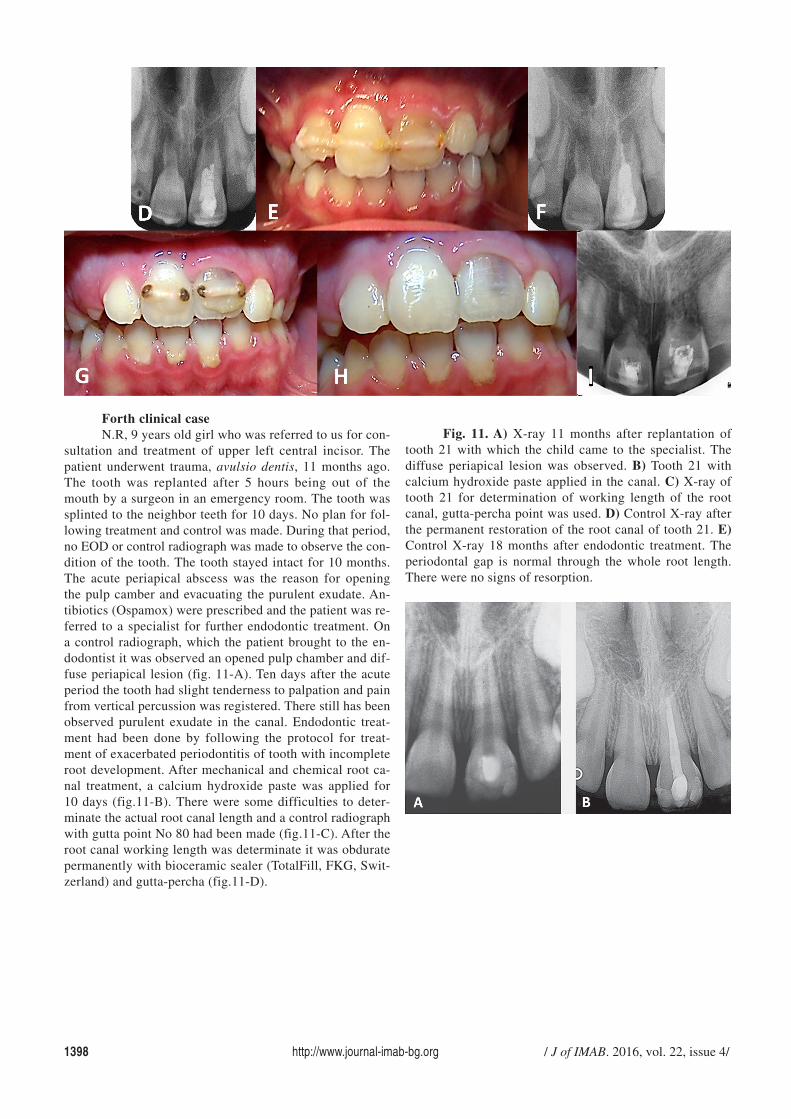
Forth clinical caseN.R, 9 years old girl who was referred to us for con-
sultation and treatment of upper left central incisor. Thepatient underwent trauma, avulsio dentis, 11 months ago.The tooth was replanted after 5 hours being out of themouth by a surgeon in an emergency room. The tooth wassplinted to the neighbor teeth for 10 days. No plan for fol-lowing treatment and control was made. During that period,no EOD or control radiograph was made to observe the con-dition of the tooth. The tooth stayed intact for 10 months.The acute periapical abscess was the reason for openingthe pulp camber and evacuating the purulent exudate. An-tibiotics (Ospamox) were prescribed and the patient was re-ferred to a specialist for further endodontic treatment. Ona control radiograph, which the patient brought to the en-dodontist it was observed an opened pulp chamber and dif-fuse periapical lesion (fig. 11-A). Ten days after the acuteperiod the tooth had slight tenderness to palpation and painfrom vertical percussion was registered. There still has beenobserved purulent exudate in the canal. Endodontic treat-ment had been done by following the protocol for treat-ment of exacerbated periodontitis of tooth with incompleteroot development. After mechanical and chemical root ca-nal treatment, a calcium hydroxide paste was applied for10 days (fig.11-B). There were some difficulties to deter-minate the actual root canal length and a control radiographwith gutta point No 80 had been made (fig.11-C). After theroot canal working length was determinate it was obduratepermanently with bioceramic sealer (TotalFill, FKG, Swit-zerland) and gutta-percha (fig.11-D).
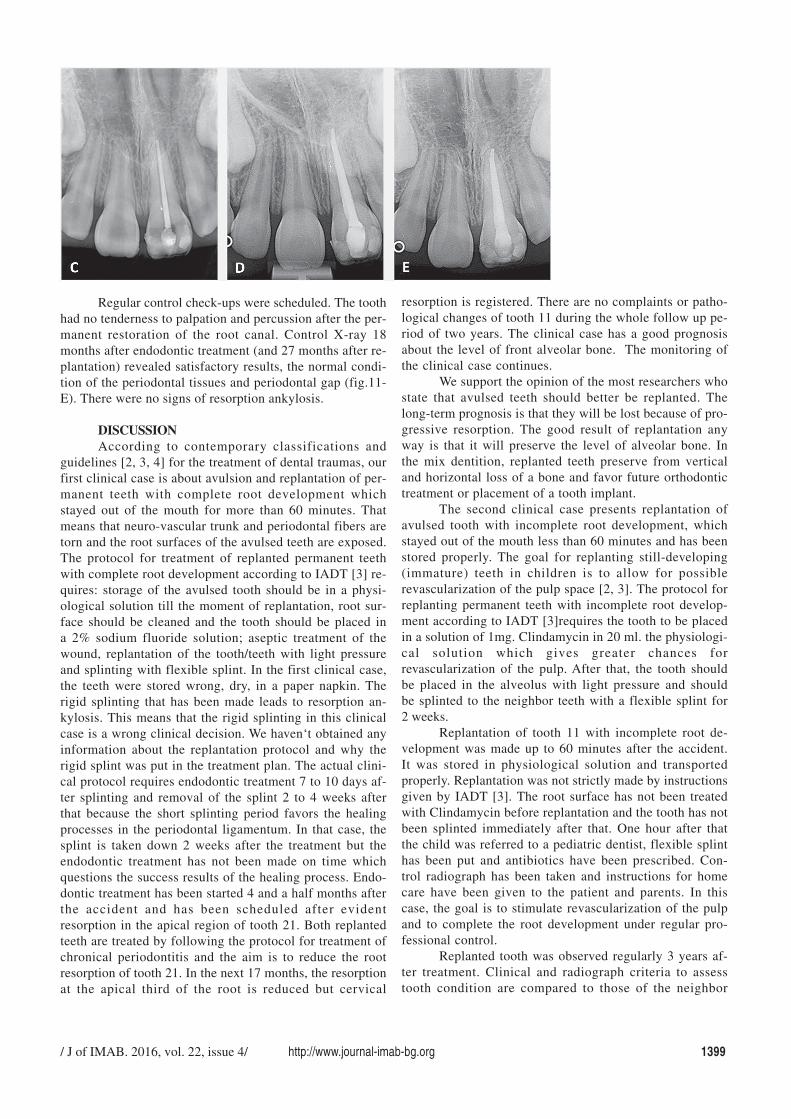
Fig. 11. A) X-ray 11 months after replantation oftooth 21 with which the child came to the specialist. Thediffuse periapical lesion was observed. B) Tooth 21 withcalcium hydroxide paste applied in the canal. C) X-ray oftooth 21 for determination of working length of the rootcanal, gutta-percha point was used. D) Control X-ray afterthe permanent restoration of the root canal of tooth 21. E)Control X-ray 18 months after endodontic treatment. Theperiodontal gap is normal through the whole root length.There were no signs of resorption.
/ J of IMAB. 2016, vol. 22, issue 4/ http://www.journal-imab-bg.org 1399
Regular control check-ups were scheduled. The toothhad no tenderness to palpation and percussion after the per-manent restoration of the root canal. Control X-ray 18months after endodontic treatment (and 27 months after re-plantation) revealed satisfactory results, the normal condi-tion of the periodontal tissues and periodontal gap (fig.11-E). There were no signs of resorption ankylosis.
DISCUSSIONAccording to contemporary classifications and
guidelines [2, 3, 4] for the treatment of dental traumas, ourfirst clinical case is about avulsion and replantation of per-manent teeth with complete root development whichstayed out of the mouth for more than 60 minutes. Thatmeans that neuro-vascular trunk and periodontal fibers aretorn and the root surfaces of the avulsed teeth are exposed.The protocol for treatment of replanted permanent teethwith complete root development according to IADT [3] re-quires: storage of the avulsed tooth should be in a physi-ological solution till the moment of replantation, root sur-face should be cleaned and the tooth should be placed ina 2% sodium fluoride solution; aseptic treatment of thewound, replantation of the tooth/teeth with light pressureand splinting with flexible splint. In the first clinical case,the teeth were stored wrong, dry, in a paper napkin. Therigid splinting that has been made leads to resorption an-kylosis. This means that the rigid splinting in this clinicalcase is a wrong clinical decision. We haven‘t obtained anyinformation about the replantation protocol and why therigid splint was put in the treatment plan. The actual clini-cal protocol requires endodontic treatment 7 to 10 days af-ter splinting and removal of the splint 2 to 4 weeks afterthat because the short splinting period favors the healingprocesses in the periodontal ligamentum. In that case, thesplint is taken down 2 weeks after the treatment but theendodontic treatment has not been made on time whichquestions the success results of the healing process. Endo-dontic treatment has been started 4 and a half months afterthe accident and has been scheduled after evidentresorption in the apical region of tooth 21. Both replantedteeth are treated by following the protocol for treatment ofchronical periodontitis and the aim is to reduce the rootresorption of tooth 21. In the next 17 months, the resorptionat the apical third of the root is reduced but cervical
resorption is registered. There are no complaints or patho-logical changes of tooth 11 during the whole follow up pe-riod of two years. The clinical case has a good prognosisabout the level of front alveolar bone. The monitoring ofthe clinical case continues.
We support the opinion of the most researchers whostate that avulsed teeth should better be replanted. Thelong-term prognosis is that they will be lost because of pro-gressive resorption. The good result of replantation anyway is that it will preserve the level of alveolar bone. Inthe mix dentition, replanted teeth preserve from verticaland horizontal loss of a bone and favor future orthodontictreatment or placement of a tooth implant.
The second clinical case presents replantation ofavulsed tooth with incomplete root development, whichstayed out of the mouth less than 60 minutes and has beenstored properly. The goal for replanting still-developing(immature) teeth in children is to allow for possiblerevascularization of the pulp space [2, 3]. The protocol forreplanting permanent teeth with incomplete root develop-ment according to IADT [3]requires the tooth to be placedin a solution of 1mg. Clindamycin in 20 ml. the physiologi-cal solution which gives greater chances forrevascularization of the pulp. After that, the tooth shouldbe placed in the alveolus with light pressure and shouldbe splinted to the neighbor teeth with a flexible splint for2 weeks.
Replantation of tooth 11 with incomplete root de-velopment was made up to 60 minutes after the accident.It was stored in physiological solution and transportedproperly. Replantation was not strictly made by instructionsgiven by IADT [3]. The root surface has not been treatedwith Clindamycin before replantation and the tooth has notbeen splinted immediately after that. One hour after thatthe child was referred to a pediatric dentist, flexible splinthas been put and antibiotics have been prescribed. Con-trol radiograph has been taken and instructions for homecare have been given to the patient and parents. In thiscase, the goal is to stimulate revascularization of the pulpand to complete the root development under regular pro-fessional control.
Replanted tooth was observed regularly 3 years af-ter treatment. Clinical and radiograph criteria to assesstooth condition are compared to those of the neighbor

1400 http://www.journal-imab-bg.org / J of IMAB. 2016, vol. 22, issue 4/
healthy tooth through the whole follow up period. The pa-tient has no complaints. Tooth function and aesthetics aresaved. The tooth is stable. All tests (visual criteria, mobil-ity test, test for tenderness to percussion, EPT confirm pos-sible revascularization of the pulp and completion of theroot development. Only the pulse oximetry test shows thatthe oxygen saturation is inadequate. This is probably thereason for the fast obliteration of the root canal as a resultof pulp irritation. The slight apical root resorption is prob-ably a result of the resorption processes in the periodon-tium. Three years after replantation EPT and the pulse oxi-metry test show that the pulp is still alive. Advanced ob-literation of the root canal requires endodontic treatmentjust to save the root canal and to slow down the rootresorption. Follow up period continues.
The prognosis for the replanted tooth is good thanksto adequate parent‘s and medical help and because of in-complete root development which gives good chances forrevascularization of the pulp. Advanced obliteration of theroot canal requires endodontic treatment. The case is oneof the successful cases of replantation.
Presented third case is about replantation of anavulsed permanent tooth with incomplete root develop-ment, which stayed out of the mouth no more than 60 min.The goal for replanting still-developing (immature) teethin children is to allow for possible revascularization of thepulp space [2, 3, 4]. The risk of infection-related rootresorption should be weighed up against the chances ofrevascularization. Such resorption is very rapid in child‘steeth. If revascularization does not occur, root canal treat-ment may be recommended. Endodontic treatment shouldprovide a chance for apexification by regular applicationof calcium hydroxide till it is necessary. After building upof an apical barrier root canal should be filled up with per-manent filling and the tooth should be finished with aes-thetic restoration [3].
In the presented case there were some mistakes made:teeth were stored dry, they were cleaned with physiologi-cal solution, the alveolus were irrigated with physiologi-cal solution as well (according to IADT [3], replantationprotocol requires the avulsed teeth to be soaked in a solu-tion of 1 mg. Clindamycin in 20 ml physiological solu-tion for 5 min)then they were filled up withBio-Oss® spon-giosa 0,25-1mm/Geistlich Biomaterials, the teeth were re-planted with light pressure but not splinted ( the instruc-tions are flexible splint to be put for 2 weeks); the patientwas not sent for future observation and treatment bypediatric dentist; endodontic treatment has been startedtoo late after advanced resorption processes have started.The parents showed negligent attitude about their child‘steeth and health.
The patient is ten and a half years old. There is achance the teeth to be lost because of advanced rootresorption. Concomitant alveolar resorption will minimizethe chance for future implant treatment. The case is an un-successful attempt for tooth replantation. The patient staysunder observation by pediatric dentist and orthodontist.
Presented forth case is about replantation of avulsedpermanent upper incisor with open apex which stayed out
of the mouth more than 60 min and has been stored in aphysiological solution [2, 3, 4]. In this case, a delayed re-plantation has a poor long-term prognosis. The periodon-tal ligament will be necrotic and will not expect to heal.The goal in doing delayed replantation of immature teethin children is to maintain alveolar ridge contour. The even-tual outcome is expected to be ankylosis and resorption ofthe root. It is important to recognize that if delayed replan-tation is done in a child, future treatment planning musttake into account the occurrence of tooth ankylosis andthe effect of ankylosis on the alveolar ridge development.When ankylosis occurs, and when the infra position of thetooth crown is more than 1 mm, it is recommended to per-form decoronation to preserve the contour of the alveolarridge. If pulp necrosis occurs endodontic treatment shouldbe made to provide conditions for apexification by regu-lar applications of calcium hydroxide for a period of time.After building up of an apical barrier root canal should befilled up with permanent filling and the tooth should befinished with aesthetic restoration [3].
In the presented case, there is no information for theprotocol of replantation. According to IADT [3], the proto-col requires replanted tooth to be splinted with a flexiblesplint for 4 weeks and the endodontic treatment should start7 to 10 days after the accident before taking off the splintInstead of that the splint has been removed 10 days afterthe accident and the endodontic treatment has not beenmade. The patient has not been referred to a pediatric spe-cialist for future treatment and observation. The endodon-tic treatment has been made too late (11 months later) af-ter pulp necrosis and periapical abscess. Antibiotics andcontemporary endodontic treatment stopped the progressof pathological processes. The inflammation has been lim-ited and now 27 months after the accident the tooth is pre-served in the alveolus, there is no complaints andresorption. Visually the tooth looks in a good condition,the patient is still under regular observation and the long-term prognosis is good.
The presented clinical case of replanted upper perma-nent central incisor with developed root and the open apexis one of the best cases for long term survival of an avulsedtooth. Delayed replantation and short term splinting do notfavor the chance for possible revascularization of the pulp.Instead of that delayed root canal treatment leads to ad-vanced periodontitis and periapical abscess. Antibiotics andendodontic treatment 18 months later have successful results.The patient is still under regular observation because of thepossible resorption ankylosis.
CONCLUSIONThe presented clinical cases show that in Bulgaria
there is a lack of dental teams for complex treatment of chil-dren with avulsed teeth. There is no good information aboutrecommended by IADT protocols for treating teeth whichundergo avulsed trauma in childhood [3]. There is a lackof information about how to store avulsed and found teethbefore replantation. This motivates us to work on a crea-tion of an interactive guideline “Teeth traumas in child-hood”, which is going to be sponsored by Console of medi-

/ J of IMAB. 2016, vol. 22, issue 4/ http://www.journal-imab-bg.org 1401
1. Andreasen JO, Andreasen FM.Avulsions. In: Textbook and color at-las of traumatic injuries to the teeth.Andreasen JO, Andreasen FM,Andersson L, editors. 4th edn. WileyBlackwell; 2007. p. 444–88.
2. Andersson L, Andreasen JO, DayP, Heithersay G, Trope M, Diangelis AJ,et al. International Association of Den-tal Traumatology guidelines for themanagement of traumatic dental inju-ries: 2. Avulsion of permanent teeth.Dent Traumatol. 2012 Apr;28(2):88-96.[PubMed]
3. Andreasen JO. The dental traumaguide. In: Andreasen JO, editor. Inter-national Association of Dental Trauma-tology. 2012. [Internet]
4. American Academy of PediatricDentistry Council on Clinical Affairs.Guideline on management of acutedental trauma. Pediatr Dent. 2008-2009; 30(7 Suppl):175-83. [PubMed]
5. Barrett EJ, Kenny DJ. Avulsed per-manent teeth: a review of the literatureand treatment guidelines. Endod DentTraumatol. 1997 Aug;13(4):153–63.[PubMed]
6. Petrovic B, Markovic D, Peric T,Blagojevic D. Factors related to treat-ment and outcomes of avulsed teeth.Dent Traumatol. 2010 Feb;26(1):52-9.[PubMed]
7. Andreasen JO. The effect of extra-alveolar period and storage media uponperiodontal and pulpal healing after re-plantation of mature permanent incisorsin monkeys. Int J Oral Surg. 1981 Feb;10(1):43-51. [PubMed]
8. Kargul B, Welbury R. An audit ofthe time to initial treatment in avulsioninjuries. Dent Traumatol. 2009 Feb;25(1):123-5. [PubMed]
9. Ebeleseder KA, Friehs S, Ruda C,Pertl C, Glockner K, Hulla H. A study
of replanted permanent teeth in differ-ent age groups. Endod Dent Traumatol.1998 Dec;14(6):274–8. [PubMed]
10. Garcia-Godoy F, Murray PE.Recommendations for using regenera-tive endodontic procedures in perma-nent immature traumatized teeth. DentTraumatol. 2012 Feb;28(1):33-41.[PubMed]
11. Andreasen JO, Andreasen FM,Bakland LK, Flores MT, Andersson L.Traumatic dental injuries, a manual.3rd edition. Wiley-Blackwell. 2011; p.48–53.
12. Trope M. Avulsion of perma-nent teeth: theory to practice. DentTraumatol. 2011 Aug;27(4):281–94.[PubMed]
13. Petrovic B, Markovic D, Peric T,Blagojevic D. Factors related to treat-ment and outcomes of avulsed teeth.Dent Traumatol. 2010 Feb;26(1):52–9.[PubMed]
14. Andersson L, Bodin I. Avulsedhuman teeth replanted within 15 min-utes – a long-term clinical follow-upstudy. Endod Dent Traumatol. 1990Feb;6(1):37–42. [PubMed]
15. Andersson L, Malmgren B. Theproblem of dentoalveolar ankylosis andsubsequent replacement resorption inthe growing patient. Aust Endod J.1999 Aug;25(2):57–61. [PubMed]
16. Kling M, Cvek M, Mejare I.Rate and predictability of pulprevascularization in therapeuticallyreimplanted permanent incisors. EndodDent Traumatol. 1986 Jun;2(3):83–9.[PubMed]
17. Andersson L, Bodin I, SorensenS. Progression of root resorption follow-ing replantation of human teeth afterextended extraoral storage. Endod DentTraumatol. 1989 Feb;5(1):38–47.[PubMed]
18. Barrett EJ, Kenny DJ. Survivalof avulsed permanent maxillary incisorsin children following delayed replanta-tion. Endod Dent Traumatol. 1997Dec;13(6):269–75. [PubMed]
19. Pohl Y, Wahl G, Filippi A,Kirschner H. Results after replantationof avulsed permanent teeth. III. Toothloss and survival analysis. DentalTraumatol. 2005 Apr;21(2):102–10.[PubMed]
20. Kinirons MJ, Gregg TA,Welbury RR, Cole BO. Variations in thepresenting and treatment features inreimplanted permanent incisors in chil-dren and their effect on the prevalenceof root resorption. Br Dent J. 2000Sep;189(5):263–6. [PubMed]
21. Filippi A, Pohl Y, von Arx T.Decoronation of an ankylosed tooth forpreservation of alveolar bone prior toimplant placement. Dent Traumatol.2001 Apr;17(2):93–5. [PubMed]
22. Cohenca N, Stabholz A.Decoronation – a conservative methodto treat ankylosed teeth for preservationof alveolar ridge prior to permanentprosthetic reconstruction: literature re-view and case presentation. DentTraumatol. 2007;23:87–94. [PubMed]
23. Malmgren B, Malmgren O,Andreasen JO. Alveolar bone develop-ment after decoronation of ankylosedteeth. Endod Top. 2006 Jul;14(1):35-40.[CrossRef]
24. Al-Asfour A, Andersson L. Theeffect of a leaflet given to parents forfirst aid measures after tooth avulsion.Dent Traumatol. 2008 Oct;24(5):515-21. [PubMed]
25. Al-Asfour A, Andersson L, Al-Jame Q. School teachers’ knowledge oftooth avulsion and dental first aid be-fore and after receiving informationabout avulsed teeth and replantation.
REFERENCES:
cal sciences by Medical University – Sofia, Bulgaria. Fastand easy internet access will give a chance to promote thatnecessary information about adequate steps that parentsand dentist should take in an emergency situation likeavulsion of permanent teeth during childhood.
Acknowledgement:The article is a part of a project No 321/15. 01. 2015, sponsored by MC- Medical University- Sofia, Bulgaria to
whom we evince our acknowledgements.The authors deny any conflicts of interest related to this study.

1402 http://www.journal-imab-bg.org / J of IMAB. 2016, vol. 22, issue 4/
Dent Traumatol. 2008 Feb;24(1):43-9.[PubMed]
26. Al-Sane M, Bourisly N, AlmullaT, Andersson L. Laypeoples’ preferredsources of health information on theemergency management of tooth avul-sion. Dent Traumatol. 2011Dec;27(6):432-7. [PubMed]
27. Feldens EG, Feldens CA,Kramer PF, da Silva KG, Munari CC,Brei VA. Understanding school teach-er’s knowledge regarding dental trauma:a basis for future interventions. DentTraumatol. 2010 Apr;26(2):158–63.[PubMed]
28. Committee on Pediatric Emer-gency Medicine and Committee onBioethics. Consent for emergency medi-cal services for children and adoles-cents. Pediatrics. 2011Aug;128(2):427-33. [PubMed]
29. Santos ME, Habecost AP, GomesFV, Weber JB, de Oliveira MG. Parentand caretaker knowledge about avul-sion of permanent teeth. DentTraumatol. 2009 Apr;25(2):203-8.[PubMed]
30. Oliviera TM, Sakai VT, MorettiAB, Silva TC, Santos CF, MachadoMA. Knowledge and attitude of moth-ers with regards to emergency manage-
ment of dental avulsion. J Dent Child(Chic). 2007 Sep-Dec;74(3):200-2.[PubMed]
31. Day P, Duggal M. Interventionsfor treating traumatised permanent frontteeth: avulsed (knocked out) and re-planted. Cochrane Database Syst Rev.2010 Jan 20;(1):CD006542. [PubMed]
32. Andreasen JO, Storgaard JensenS, Sae-Lim V. The role of antibiotics inpresenting healing complications aftertraumatic dental injuries: a literaturereview. Endod Top 2006; 14:80-92.[CrossRef]
33. Berthold C, Thaler A, PetscheltA. Rigidity of commonly used dentaltrauma splints. Dent Traumatol. 2009Jun;25(3):248–55. [PubMed]
34. Hinckfuss S, Messer LB.Splinting duration and periodontal out-comes for replanted avulsed teeth, asystematic review. Dent Traumatol.2009 Apr;25(2):150-7. [PubMed]
35. Pohl Y, Filippi A, Kirschner H.Results after replantation of avulsedpermanent teeth. I. Endodontic consid-erations. Dental Traumatol. 2005Apr;21(2):80-92. [PubMed]
36. Pohl Y, Filippi A, Kirschner H.Results after replantation of avulsed
permanent teeth. II. Periodontal healingand the role of physiologic storage andantiresorptive-regenerative therapy.Dent Traumatol. 2005 Apr;21(2):93-101. [PubMed]
37. Day PF, Gregg TA, Ashley P,Welbury RR, Cole BO, High AS, et al.Periodontal healing following avulsionand replantation of teeth: a multi-cen-tre randomized controlled trial to com-pare two root canal medicaments. DentTraumatol. 2012 Feb;28(1):55-64.[PubMed]
38. Johns DA, Shivashankar VY,Maroli RK, Vidyanath S. Novel man-agement of avulsed tooth by pulpal andperiodontal regeneration. J Endod.2013 Dec;39(12):1658-62. [PubMed]
39. Priya HM, Tambakad PB, NaiduJ, Pulp and Periodontal Regenerationof an Avulsed Permanent Mature Inci-sor Using Platelet-rich Plasma afterDelayedReplantation: A 12-monthClinical Case Study. J Endod. 2016Jan;42(1):66-71. [PubMed]
40. Qazi SR, Nasir KS. First-aidknowledge about tooth avulsionamongdentists, doctors and lay people. DentTraumatol. 2009 Jun;25(3):295-9.[PubMed]
Address for correspondence: Professor Rossitza KabaktchievaDepartment of Pediatric Dentistry, Faculty of Dental Medicine, MedicalUniversity - Sofia.1, George Sofiisky Str.,1431 Sofia, Bulgaria.E-mail: [email protected]
Please cite this article as: Kabaktchieva R, Gateva N, Gusiyska A, Stanimirov P, Milcheva N. Dental care for childrenafter replantation of avulsed permanent incisors. J of IMAB. 2016 Oct-Dec;22(4):1392-1402.DOI: https://doi.org/10.5272/jimab.2016224.1392
Received: 03/09/2016; Published online: 20/12/2016
![Intentional Replantation: An Updated Protocols in ... · conventional treatment, and accidental avulsion (unintentional replantation) [8]. On the other hand, contraindications of](https://img.pdfslide.us/doc/110x75/5ed55ef56933f508e973f125/intentional-replantation-an-updated-protocols-in-conventional-treatment-and.jpg)




























