Embed Size (px)
Citation preview

Clinical Report—Supporting the Health CareTransition From Adolescence to Adulthood in theMedical Home
abstractOptimal health care is achieved when each person, at every age, re-ceives medically and developmentally appropriate care. The goal of aplanned health care transition is to maximize lifelong functioning andwell-being for all youth, including those who have special health careneeds and those who do not. This process includes ensuring thathigh-quality, developmentally appropriate health care services areavailable in an uninterrupted manner as the person moves from ado-lescence to adulthood. A well-timed transition from child- to adult-oriented health care is specific to each person and ideally occursbetween the ages of 18 and 21 years. Coordination of patient, family,and provider responsibilities enables youth to optimize their ability toassume adult roles and activities. This clinical report represents ex-pert opinion and consensus on the practice-based implementation oftransition for all youth beginning in early adolescence. It provides astructure for training and continuing education to further understand-ing of the nature of adolescent transition and how best to support it.Primary care physicians, nurse practitioners, and physician assis-tants, aswell asmedical subspecialists, are encouraged to adopt thesematerials and make this process specific to their settings and popula-tions. Pediatrics 2011;128:182–200
1. INTRODUCTION AND METHODOLOGYWith reasonable biological certainty, most adolescents transition toadulthood. There is much less certainty about the manner in whichhealth care professionals support this transition. Transition planning,when present at all, can be inexplicit, incomplete, or late, and whennecessary, the transfer of care to an adult medical home and to adultmedical subspecialists involves more of a drift away from pediatriccare rather than a clearly planned and executed handoff. In 2002, aconsensus statement coauthored by the American Academy of Pediat-rics (AAP), the American Academy of Family Physicians (AAFP), and theAmerican College of Physicians (ACP)-American Society of InternalMedicine was published, stating the importance of supporting andfacilitating the transition of adolescents with special health careneeds* into adulthood.1 This statement represented the shared per-spectives of health care professionals, families, youth, researchers,
*TheMaternal and Child Health Bureau (MCHB) defines children and youth with special healthcare needs as “[t]hose who have or are at increased risk for a chronic physical, developmen-tal, behavioral, or emotional condition and who also require health and related services of atype or amount beyond that required by children generally.”21
AMERICAN ACADEMY OF PEDIATRICS, AMERICAN ACADEMYOF FAMILY PHYSICIANS, AND AMERICAN COLLEGE OFPHYSICIANS, TRANSITIONS CLINICAL REPORT AUTHORINGGROUP
KEY WORDShealth care transition, youth transition, medical home, childrenwith special health care needs, primary care, adolescent health,quality improvement
ABBREVIATIONSAAP—American Academy of PediatricsMCHB—Maternal and Child Health BureauCCM—chronic condition managementEHR—electronic health record
This document is copyrighted and is property of the AmericanAcademy of Pediatrics and its Board of Directors. All authorshave filed conflict of interest statements with the AmericanAcademy of Pediatrics. Any conflicts have been resolved througha process approved by the Board of Directors. The AmericanAcademy of Pediatrics has neither solicited nor accepted anycommercial involvement in the development of the content ofthis publication.
The guidance in this report does not indicate an exclusivecourse of treatment or serve as a standard of medical care.Variations, taking into account individual circumstances, may beappropriate.
www.pediatrics.org/cgi/doi/10.1542/peds.2011-0969
doi:10.1542/peds.2011-0969
All clinical reports from the American Academy of Pediatricsautomatically expire 5 years after publication unless reaffirmed,revised, or retired at or before that time.
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2011 by the American Academy of Pediatrics
Guidance for the Clinician inRendering Pediatric Care
182 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on December 12, 2016Downloaded from

and policy-makers. It provided founda-tional guidance for health care pro-cesses that include health care plan-ning and information exchange, forprofessional education and certifica-tion, and for insurance and paymentreform. Its conclusions and criticalsteps remain widely accepted stan-dards that have informed the develop-ment of pilot projects, model prac-tices, and national initiatives toimprove support for transitioningyouth. The US Department of Healthand Human Service’s Maternal andChild Health Bureau (MCHB) has beeninstrumental in promoting the im-portance of seamless, effective, andcomprehensive services for all youthand families during this major lifetransition.2
After nearly a decade of effort, wide-spread implementation of health tran-sition supports as a basic standard ofhigh-quality care has not been real-ized. To date, only limited progress canbe documented in the achievement ofthe consensus statement’s 6 criticalsteps. Although 2 National Surveys ofChildren With Special Health CareNeeds indicate improvements between2001 and 2006, there has been only lim-ited achievement of national healthpolicy goals related to transition.3,4
Outcomes-related research effortshave, so far, failed to fully address thetransition needs of adolescents withor without chronic conditions.5 A re-cent national survey revealed that pe-diatricians remain poorly informedabout the conclusions of the consen-sus statement and that most pediatricpractices neither initiate transitionplanning early in adolescence nor of-fer transition-support services, whichhave been found to be critical for en-suring a smooth transition to the adulthealth caremodel.6 The survey authorsnoted that “gaps in transition supportare due in part to limited staff training;lack of an identified staff person re-
sponsible for transition; financialbarriers; and anxiety on the part of pe-diatricians, adolescents, and their par-ents about planning for their futurehealth care.”7 Other authors have citedthe lack of developmentally appropri-ate tools for assessing child and familyreadiness for transition as a barrier totransition.8,9
The result is that many pediatricians,youth, and families have found a lim-ited availability of adult providers withwhom to arrange a smooth transitionof care.10–14 In addition, evidence indi-cates that many adult providers feelunprepared to care for young adultswith complex chronic conditions. Insome cases, there is no identified adultprimary care or specialty provider towhom care can be transitioned. Lackof time, adequate payment, and train-ing have been cited as major barriersto transition.15 Workforce shortagesexist and are anticipated to worsen forphysicians and other health profes-sionals providing care for adults of allages. In the face of an aging populationthat needs care, these shortages maybe an obstacle to the delivery of pri-mary care to more young adults withor without special health care needs.16
Family physicians caring for youthnote that no transfer of primary carewill be needed; nevertheless, there is aneed to implement an adult model ofcare; plan for the transfer of specialtycare to adult medical subspecialists;and support broader transition plan-ning that includes issues such as edu-cational attainment, career choices,and independent living needs. Inter-nists find it challenging to care for achild or youth with special health careneeds when the youth lacks prepara-tion to be his or her own health advo-cate and the referring physician sendsonly minimal information about theyouth and/or his or her condition.17 De-spite the recent spread of the family-centered medical home model for the
redesign of primary care, payment re-forms for non–encounter-based ser-vices (such as transition planning andcare coordination) still have not mate-rialized to a significant degree. Finally,with relatively few model practices ex-emplifying high-quality transition sup-ports, training providers in the princi-ples of health care transition remainschallenging.
When there are obstacles, there arealso opportunities. The need is stron-ger than ever for the seamless trans-fer of care and personal health infor-mation from pediatric care settings tomore adult settings and for all youth tofunction as independently as possiblein promoting their own health asadults. The 2007 AAP Annual Leader-ship Forum designated the resolution“transitioning youth with specialhealth care needs to adult health care”as a top-10 priority. Bright Futures pro-vides a framework for anticipatoryguidance throughout childhood andadolescence that encourages paren-tal support of self-management andindependent decision-making abouthealth.18 Explicitly planned care as theproduct of a partnership among healthcare professionals, youth, and familieshas become an essential characteris-tic of the primary care medical homefor which recognition standards havebecome more firmly established, suchas the Physician Practice Connectionfor the Patient-Centered Medical Homeof the National Committee on QualityAssurance and theMedical Home Indexof the Center for Medical Home Im-provement.19,20 Providing high-qualitytransition care and support may be-come one of the standards that bothpediatric and adult primary care prac-tices would need to meet to be recog-nized as a medical home and becomeeligible for new payment scenarios.
These new opportunities have set thestage for a reaffirmation of the princi-ples in the original consensus state-
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 128, Number 1, July 2011 183by guest on December 12, 2016Downloaded from

ment by the AAP, American Academy ofFamily Physicians, and American Col-lege of Physicians. All 3 professionalgroups also recognize the need totranslate those principles into practi-cal operational guidance for the careof all children and youth as they tran-sition to adulthood. Although youthwith special health care needs requirea broader range of considerationsduring their transitions, all youth neededucation, guidance, and planning toprepare to assume appropriate re-sponsibility for their own health andwell-being in adulthood.21 Most youthwith chronic illnesses will survive intoadulthood and, depending on the se-verity and specifics of their disability,should transition to an adult model ofcare. After the age of majority,† allyouth deserve to be treated as adultsand to experience an adult model ofcare, although some people may re-quire decision-making support from athird-party proxy, such as throughguardianship or power of attorney. Re-cent evidence has shown that higherexecutive function affecting impulsiv-ity and decision-making continues tomature through the mid-20s. Older ad-olescents and young adults may re-quire guided decision-making assis-tance from clinicians and familymembers as they enter adult systemsof care.22 Nevertheless, most youth willbenefit from advance planning andpreparation for that experience re-gardless of whether they remain withtheir pediatric provider or medicalsubspecialist after the age of 18.
This report assumes that it is theyouth, not the clinician, who is transi-tioning in his or her movement fromone stage of life and development toanother. The actions of the youth’smedical home involve not the transi-
tion of care but, rather, the transfer ofsome or all elements of care to anadult medical home setting or, in thecase of a family medicine medicalhome, to an adult medical homemodel. The medical home visit is a dif-ferent process when the patient hasreached the age of majority; adult pa-tients have specific considerationsand necessitate providers’ attention tonew requirements such as adoptingconsent for treatment processes andHealth Insurance Portability and Ac-countability Act (HIPAA)–compliantforms. Health care transfer is an ele-ment of transition and has a definedend point that may vary from patient topatient. Because both transition andtransfer are influenced by environ-mental, socioeconomic, medical, andother factors, it is the responsibility ofthe medical home—in partnershipwith patients and their families—tocoordinate efforts that ensure optimaloutcomes for every patient.
The patient- and family-centered med-ical home model of primary care in-cludes 3 distinct but interrelatedcare processes: preventive care; acuteillness management; and chronic con-ditionmanagement (CCM). CCM consti-tutes an explicit and defined ap-proach that involves planned andproactive care rooted in evidence- andconsensus-based guidelines, writtencare plans, and active care coordina-tion. The medical home uses a registryto track the status of its patients withspecial health care needs and maystratify the registry in terms of the se-verity or complexity of the patient’scondition. Those with more complexconditions may be identified for writ-ten care plans, care coordination, anda more intense, amplified transitionplan. CCM also includes an explicit ap-proach to comanagement with medi-cal subspecialists in which the roles ofprimary and specialty care are clearlyarticulated. (Comanagement involves
an explicit and transparent process inwhich providers involved in a patient’scare determine—in collaborationwiththe patient or family—which providerwill be responsible for which aspectsof the patient’s care. Comanagementcan occur between primary care pro-viders and 1 or more medical subspe-cialists. It might also occur during thetransfer of care from a pediatric to anadult setting.) Transition activities foryouth with special health care needsshould include a comanagement-transition plan that articulates theprocess and timing for the transfer ofcare from pediatric to adult medicalsubspecialists. (These components ofCCM are described in greater detaillater in this report.)
This clinical report aims to advancethe practice-based implementation ofplanning, decision-making, and docu-mentation processes for youth whoare approaching transition, includingthose who have special health careneeds and those who do not. It intendsto provide a structure for training,continuing education, and research tofurther the understanding of bestpractices for transition of adolescentsto adult care. It does not detail the ac-tivities conducted by receiving provid-ers who accept patients into an adultmodel of medical home care. Becausethere is currently only limited outcomeliterature about transition, this clinicalreport is based on expert opinion andconsensus recommendations ratherthan on specific evidence. The reportprovides a decision-making algorithm(Fig 1) for all youth, beginning at 12years of age. The algorithm includes abranch with expanded, generic guide-lines for transitioning youth with spe-cial health care needs who requireCCM.23 These chronic condition guide-lines can, in turn, provide a templatefor later, more detailed, and special-ized applications of the algorithm tospecific conditions and specialty care
†The “age of majority” is a legal definition of theage at which a person is considered to be an adult.In most states, this age is 18 years; exceptions areAlabama and Nebraska (19 years) and Washington,DC, and Mississippi (21 years).
184 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on December 12, 2016Downloaded from

situations. These guidelines, recom-mendations, and resources will alsobe useful to the medical subspecialistengaging in the transition process; pri-mary care providers and medical sub-specialists are encouraged to make
this process specific for their ownneeds.
Methodology
The AAP and the National Center forMedical Home Implementation (a co-
operative agreement between the AAPand the MCHB) have prioritized the is-sue of transitioning youth from a pedi-atric to an adult medical homewith thegoal of facilitating the effective transi-tion of all youth from pediatric to ap-
Medical Home Interaction for Patients > 12 Years of Age
Yes
STEP 1: Discuss Office Transitions
Policy With Youth & Parents
Is the Patient 12–13 Years
of Age?
NoIs the Patient 14–15 Years
of Age?
Is the Patient 16–17 Years
of Age?
STEP 3: Ensure Steps 1 & 2 Are Complete,
ThenReview & Update
Transitions Plan & Prepare for Adult
Care
No
Yes Yes
STEP 2: Ensure Step 1 Is Complete,
Then Initiate a Jointly
Developed Transition Plan With Youth &
Parents
No
Transition Component of
Interaction Complete
Is the Patient ≥18 Years
of Age?
Yes
Does Patient Have Special Health Care
Needs?b
No
STEP 4: Ensure Steps 1, 2, & 3 Are Complete,
ThenImplement Adult Care
Modela
Incorporate Transition Planning in Chronic
Condition Management
Yes
1
2a 2b 2c 2d
3a 3b 3c 3d
4
Have Age-Appropriate
Transitions Issues Been Addressed?
Yes
No
5b5a 5c
6Legend
= Start
= Stop
= Decision
= Action/Process
Row 1: Medical Home Interaction
Row 2: Age Ranges
Row 3: Action Steps for Specific Age Ranges
Row 4: Determination of
Special Needs
Initiate Follow-up Interaction
Row 5:
Follow-up
Row 6: Interaction Complete
CCM and
A
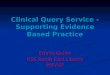
FIGURE 1A, Health care transition-planning algorithm for all youth and young adults within a medical home interaction. a For pediatric practices, transfer to adultprovider; b the MCHB defines children with special health care needs as “[t]hose who have or are at increased risk for a chronic physical, developmental,behavioral, or emotional condition and who also require health and related services of a type or amount beyond that required by children generally.” B,Reverse side of the algorithm.21
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 128, Number 1, July 2011 185by guest on December 12, 2016Downloaded from

propriate adult care. The ExecutiveCommittee and staff of the AAP Councilon Children With Disabilities (COCWD)are leading the transitions initiative,which has received funding supportfrom the National Center for MedicalHome Implementation and the COCWD.The ultimate goal of this initiative is tohelp medical home providers, pa-tients, and their families ensure a suc-cessful transition to appropriate adultcare.
In 2008, the AAP convened a meeting toreview and provide advice on pro-posed transition initiatives. Current lit-erature and activities were high-lighted, and areas in which assistanceis needed for pediatric providers toproperly address transitioning youthto adult care within their practicewere identified. The first activity of thetransitions initiative was to develop aclinical report to provide pediatric pro-viders with the information they needto facilitate youth receiving high-quality, developmentally appropriatehealth care services as they transitionto adulthood. A Transitions Clinical Re-port Authoring Group was subse-quently assembled and cochaired byDrs Carl Cooley and Paul Sagerman.Other disciplines and/or groups repre-sented on the authoring group includepediatric primary care and subspe-cialty physicians, adult health careproviders, family members, and ayoung adult who recently completedhis own health care transition.
These stakeholders partnered to de-velop this clinical report on the impor-tance of youth receiving high-quality,developmentally appropriate healthcare services as they transition toadulthood. It provides practitionerswith a clear time line and algorithmicprotocol for succeeding in this pro-cess. A draft version of this clinical re-port underwent extensive peer reviewby committees, councils, sections, andadditional groups within the AAP as
ALGORITHMCOMPONENT
DESCRIPTIVE TEXT
1. Initiate first step in the health care transition planning process at age 12.
2a, 2b, 2c, 2d. Age Ranges. By age 12, conduct surveillance to assess any special health care needs. Start actual transition planning by age 14. By ages 16–17, transition planning should be well established. At age 18, initiate an adult model of care for most youth, even if there is no transfer of care. If transition planning does not occur on the schedule described by the algorithm, a concentrated effort is required (eg, special visits) to complete the process successfully.
3a. Every practice should have a written transition policy that is prominently displayed and discussed with youth and families. The policy should explicitly state the practice’s expectations and care process for the health care transition of their adolescent patients to an adult model of care.
3b. The practice should use a standard transition plan that can be adapted for each patient’s needs. This tool should include components to obtain an accurate assessment of the patient’s ability to transition successfully. Providers should interview youth and family members to identify needs and assess the intentions and motivations for youth independence.
3c. Transition plans must be reviewed regularly and updated as necessary. The provider must also perform surveillance for changes in the youth’s medical status and address youth and family concerns that may warrant changes in transition goals. Failure to achieve transition-readiness goals warrants reevaluation of the existing plan and increased frequency of medical home interventions/visits. A “pretransfer” visit to the adult medical home could be conducted during the year before the transfer.
3d. Transition to an adult model of care occurs appropriate for youth’s developmental level, which is followed as appropriate by transfer to an adult medical home. Complete medical records should be delivered to the adult provider, along with a portable summary, which is also provided to the patientor guardian. For children and youth with special health care needs, directcommunication between pediatric and adult providers is essential, because adult medical personnel may be unfamiliar with certain pediatric conditions.
4. Transition planning for children and youth with special health care needs should include specific CCM activities such as use of registries; care plans; care coordination; CCM office visits; and comanagement with medical subspecialists. Transition goals must be individualized to account for variations in the complexity of a youth’s condition and in the youth’s intellectual ability and guardianship status.
5a. Youth with special health care needs require an expanded transition-planning process. Transition planning in CCM includes addressing the exchange of complex health information; competencies for self-care; transfers of specialty care; and issues related to insurance, entitlements, guardianship, and eligibility for adult services. In a medical home, such youth may have a written care plan as part of the medical record. At age 14, this plan should include a section titled “transition plan,” which should be expanded and developed as the youth approaches age 18 and beyond.
5b. Use of transition-planning tools and readiness checklists facilitate the provider’s ability to ensure that all age-appropriate transition issues have been addressed. Each action step must be completed in order, even if itmeans the provider has to schedule specific visits to initiate and complete steps missed earlier in the process to catch up before the next visit.
5c. Focused tasks involving little detail or complexity can be addressed by the medical home care coordinator, medical provider, or other appropriate staff through telephone or electronic media. More complex issues may necessitate face-to-face office visits.
6.The provider is finished with the transition tasks for that specific interaction or visit; transition planning is an ongoing activity that occurs at every interaction.
Medical Home Interaction for Patients >12 Years of Age
Is the Patient 12–13 Years
of Age?
Is the Patient 14–15 Years
of Age?
Is the Patient 16–17 Years
of Age?
Is the Patient ≥18 Years of Age?
STEP 1: Discuss Office Transitions
Policy with Youth & Parents
STEP 2: Ensure Step 1 is Complete,
then Initiate a Jointly
Developed Transition Plan with Youth &
Parents
STEP 3: Ensure Steps 1 & 2 are Complete,
thenReview & Update
Transitions Plan & Prepare for Adult
Care
STEP 4: Ensure Steps 1, 2, & 3 are Complete,
thenImplement Adult Care
Model**for pediatric practices
transfer to adult provider
Does Patient Have Special Health Care
Needs?**
Incorporate Transition Planning in Chronic
Condition Management
Have Age-Appropriate
Transitions Issues Been Addressed?
Initiate Follow-up Interaction
TransitionComponent of
Interaction Complete
B
FIGURE 1Continued.
186 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on December 12, 2016Downloaded from

well as by external people or groupswho were either identified as expertsin the field or had requested the re-viewing opportunity. The resultingcomments were incorporated into thereport, as appropriate. It is expectedthat all subsequent AAP transition ini-tiatives will use the publication of thisclinical report, and the guidancetherein, as a foundation for education,training, and quality measurement.
2. GETTING READY FOR TRANSITION
Transition planning should be a stan-dard part of providing care for allyouth and young adults, and every pa-tient should have a transition plan re-gardless of his or her specific healthcare needs. Successful transition in-volves the engagement and participa-tion of the medical home team (physi-cians, nurse practitioners, physiciansassistants, nurses, care coordina-tors), the family and other caregivers,and the individual youth collaboratingin a positive and mutually respectfulrelationship (ie, one that honors diver-sity and is consistent with each fami-ly’s cultural and religious beliefs). Themedical home teamdoes not engage intransition planning alone; rather, itjointly creates and implements theplan with the youth and his or her fam-ily/caregivers. The medical home teamfacilitates a process that is planned,smooth, and patient- and family-centered. The parents’ role is to ac-tively engage in the process and movein and out of the decision-making posi-tion as appropriate. The youth’s role isto maximize his or her independenceand primacy in the decision-makingprocess to foster lifelong functioningand self-determination. The receiv-ing adult providers also need to beidentified and engaged and, asneeded, to provide developmentallyappropriate support for the familyand young adult during the transi-tion process. This process is de-scribed in both the algorithm and
“Adult Medical Home (Receiving Pro-vider): Roles and Responsibilities.”
a. Provider Readiness
A key component of supporting thetransition process is the primary caremedical home having an explicit officepolicy that describes the practice’s ap-proach to health care transition, in-cluding the age and process at whichyouth shift to an adult model of care.This office policy applies to all youth(both with and without special healthcare needs), guides the process, andhelps the youth and family members(or other caregivers) understand boththeir and the medical home team’sroles and responsibilities. The officetransition policy should be visible andreadily available to patients and theirfamilies, including depicting them inbrochures, posters, and/or Web-basedinformation about the practice. This of-fice policy should clearly describe thegoal of transition as part of lifelongpreparation for a successful adult lifeand articulate how transition planningfacilitates the patient’s movementfrom a pediatric to an adult caremode.17 Additional components of theoffice policy are described later in thealgorithm.
To achieve the goal of transition plan-ning as a standard of care, themedicalhome team must receive training andtechnical assistance to implementtransitions effectively and adopttransition-related practices (eg, dis-cussing the office transition policy, as-sessing family and youth transitionreadiness, developing referral rela-tionships in the adult care system).Adult medical homes and medical sub-specialists may need to build their ca-pacities to provide services to youngadult patients, particularly those withcognitive impairments and other spe-cial health care needs. Education andclinical experience for medical hometeam members will provide essential
skills for the successful transition ofyouth both with and without specialneeds. Issues of provider readinessare described further in “Adult Medi-cal Home (Receiving Provider): Rolesand Responsibilities.”
b. Family Readiness
The medical home team membersmust understand and address pa-tients’ and parents’ perspectives andneeds during transition and recognizethat this process is complex and po-tentially emotional for parents andother caregivers/guardians. Althoughfamilies make multiple transitionsduring their children’s lives, for manyparents, the pediatrician has been aconstant, and they may find transitionfrom the known to the unknown to bestressful. This is particularly likely tobe true for parents of children withspecial health care needs. To makethe process smoother for all in-volved, transition planning must an-ticipate and address challenges thatparents may face as the youth entersadulthood.
It is important for physicians and otherhealth care professionals to engageparents and youth with education andinformation about their role in thetransition process. This educationshould include information about howthe health care environment changeswhen the youth legally becomes anadult at 18 years of age as well as dif-ferences between pediatric and adultmedicine models. The provider’s goalsare to normalize the transition pro-cess, address the families’ anxieties orquestions, and foster a team approachto help facilitate the acquisition ofskills and tools that the youth can useboth in transition and beyond. The fam-ily members or other caregiversshould be engaged and open to theprocess (eg, learning about any up-coming changes in health coverage), en-courage autonomous decision-making
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 128, Number 1, July 2011 187by guest on December 12, 2016Downloaded from

and self-care on the part of the youth,and share their questions and/or con-cerns with the provider as they adjustto their role shifting from primarydecision-maker and caregiver to amore supportive role.
c. Youth Readiness
For transition planning to succeed,providers, and parents/caregiversmust view the youth as the driver in theprocess and encourage the youth toassume increasing responsibility forhis or her own health care to the full-est extent possible. Empowering youththrough transitions fosters the devel-opment of self-management skills andtools needed for them to gain morecontrol in, and over, their lives.24 Al-though this is the case for youth bothwith and without special health careneeds, it is particularly critical for theformer, who may require a broaderrange of considerations during thetransition process.25
Although this report presents optimalages for initiating and conductingtransition planning, it is never tooearly to begin conversations amongthe provider, family/caregivers, andpatient about planning for the future.This is especially true for children withspecial health care needs. For this pop-ulation, it is likely that similar conver-sations are occurring in the educa-tional system regarding IndividualizedEducation Plans (IEPs); these variousconversations can reinforce and but-tress one another.25 Prioritizing andreinforcing the value of independenceand decision-making as part of thetransition-planning process not onlyreinforces such messages on the partof providers, family members/othercaregivers, and the broader commu-nity but also facilitates the patient’ssuccessful transition to adult medicalcare and active participation in main-taining his or her own health.
3. FRAMING THE ALGORITHM
An algorithm is a finite list of steps con-nected by various decision-makingpoints that can be taken to move froma known beginning to a predictableend state. As a decision-making tool,an algorithm presents clear-cut ques-tions that, when answered, delineatestandardized pathways that lead to theprocess’s next step(s) and a desiredoutcome. Clinical algorithms have longbeen popular and effective tools forhelping clinicians understand and im-plement a diagnostic, therapeutic, ormanagement process. Algorithms alsoprovide a logic model for the incorpo-ration of processes of care into elec-tronic health records (EHRs). Algo-rithms have been included recently inAAP policy documents as strategiesto support health care professionalsto develop a pattern and practice toaddress developmental concerns inchildren from birth through 3 yearsof age and to engage in early identi-fication of children with autism spec-trum disorders.23,26
The algorithm contained in this clinicalreport (Fig 1) specifies the protocol formanaging the transition process; as-sists physicians and other health careprofessionals to implement the transi-tion process; and provides a transitionstructure for youth and their families.It is intended for use by clinicianswithin a medical home setting as a“jumping-off point” for the identifica-tion of youth who have reached a pointin their lives at which health care tran-sition should be integrated as a rou-tinely recognized part of the officevisit. Individual steps along thetransition process will vary from oneyouth to the next depending on individ-ual patient, family/caregiver, healthcare professional, and community-resource factors. The transition pro-cess is best initiated by the time a childis 12 years of age and ideally shouldoccur during a health maintenance or
CCM visit. Transfer itself should occurwithin the 18- to 21-year age range, al-though it can occur earlier becausesome internists accept new patients at15 years of age, particularly if they seeother family members as well. Someyouth may experience a variety ofhealth care settings as theymove frompediatric to adult models of care (eg,while in college or military service),but these settings are not likely to pro-vide a comprehensive medical home.Youth should either remain in their pe-diatric medical home or be well estab-lished in their adult medical homewhile receiving episodic care in thesesettings.
a. Explanation of the AlgorithmComponents
Row 1: Medical Home Interaction
Medical Home Interaction for Patients > 12 Years of Age
All youth, regardless of whether theyhave identified special health careneeds, should be assessed for transi-tion readiness. Preparation for adultlife should be a routinely addressedtopic for any health maintenance visitthat occurs within the medical homeduring the adolescent years. TheBright Futures initiatives provide con-tent materials on this subject matter.20
Medical homes can provide appropri-ate transition services, support, andplanning. Transition planning with pa-tients and families must be initiatedduring an office visit to allow face-to-face communication, because the par-ties involved may not have previouslyconsidered this subject matter. Subse-quent medical home transition-planning “interactions” may include,but not be limited to, office visits forhealth maintenance or acute illness,CCM visits, nursing visits, telephone ore-mail consultations, provision of of-fice policies, and/or record reviewsand updates. It is of paramount impor-
188 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on December 12, 2016Downloaded from

tance that the primary care medicalhome recognize which youth in thepractice have reached the age for tran-sition planning and prompt these fam-ilies to come in for a visit to initiate theprocess. Each action step does not re-quire a separate medical home visit,and multiple action steps can be ad-dressed during a visit, although doingso requires a greater investment oftime and resources.
Although opinions differ on the age forinitiating the transition process, themost appropriate time is early adoles-cence, when youth become develop-mentally capable of engaging in activi-ties regarding their personal futures.Therefore, this clinical report recom-mends initiating the first step in thehealth care transition-planning pro-cess at the age of 12, which allows suf-ficient time to adequately prepare pa-tients, families, and medical providersbefore the youth legally becomes anadult at the age of 18. Several clinicalstudies have found this age to be anappropriate time to initiate the pro-cess to most successfully affect thetransition’s outcome.27–29
Children and youth with special healthcare needs and their families may ben-efit from discussions regarding adulttransitioning that begin earlier than 12years of age, depending on specific pa-tient circumstances. Expectations forvocation, independent living, guardian-ship, reproduction, life expectancy,and other topics should be discussedat the earliest possible opportunitywith parents and/or other appropriatecaregivers if it is determined that thechild’s transition process will be dif-ferent from that of children withoutspecial health care needs. In addition,some children with chronic medicalconditions (eg, asthma or diabetes)may be introduced to developmentallyappropriate self-care at ages youngerthan 12. The timing of these discus-sions must be individualized.
Row 2: Age Ranges
The second row of the algorithm as-sists health care providers in devel-oping a practice of recognizing theneed for transition for all patients 12years or older. The use of emerginghealth information technology islikely to aid in this process (eg,through registries and age-relatedprompts). The age ranges presentedin the algorithm are designed to aidthe provider in assessing the mostappropriate ages for implementingspecific stages of transition plan-ning. For most patients, this appro-priateness is determined by age,whereas for others, it may be modi-fied on the basis of developmentalconsiderations. The provider’s flexi-bility and judgment are important inthis process. Actual transition plan-ning should be initiated at the age of14. The goal is to identify patientswho are either entering or within the14- to 15-year age range to initiatethe development of a patient-specifictransition plan at the child’s next visit.
Is the Patient 12–13 Years
of Age?
Is the Patient 14–15 Years
of Age?
Is the Patient 16–17 Years
of Age?
Is the Patient ≥18 Years of Age?
Row 3: Action Steps for Specific AgeRanges
Transition is a dynamic and fluid pro-cess that includes 4 major actionsteps. Each of the first 3 action steps(discussion of medical home transi-tion policy, initiation of transition plan,and review/update of the transitionplan) lays the foundation for the next.The fourth action step (implementa-tion of an adult care model) preparesthe youth and/or caregiver for thetransfer to an adult care model. Re-gardless of the age at which the pa-tient’s transition process is initiated,the 4 action steps for transition plan-ning must be accomplished in a linearfashion. For example, if transition isbeing initiated for a 16-year-old whopresents for a health maintenancevisit, steps 1 and 2 of the algorithmmust be completed before moving tostep 3 (the age-appropriate stage for a16-year-old). As noted, a separatemed-ical home visit is not required for eachaction step, and multiple action stepscan be addressed in a single visit.
STEP 1: Discuss Office Transitions
Policy With Youth & Parents
In (3a) step 1, the provider shares anddiscusses the office transition policywith the youth and his or her family orother caregivers. As described previ-ously, every pediatric practice shouldhave a well-defined policy that clearlystates the expectations for the healthcare transition of their adolescent pa-tients to an adult model of care. Thispolicy should be displayed in a locationwhere youth and their caregivers caneasily read it (eg, posted in front of-fices and waiting rooms and describedin brochures and on the practice’s Website). The policy should reflect the ap-propriate level of health literacy, read-ing and language proficiency, and cul-tural norms for the population thepractice serves. Components of the
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 128, Number 1, July 2011 189by guest on December 12, 2016Downloaded from

office transition policy include, but arenot limited to:
● the expected age of patient transferto an adult model of health care;
● the patient’s responsibilities in pre-paring for transition;
● the parent, family, and/or caregiverresponsibilities in preparing fortransition; and
● the medical provider’s responsibili-ties in preparing for transition.
In addition to posting the transitionspolicy, providers should provide awrit-ten copy of the office policy to all pa-tients who are aged 12 or older andtheir families. Optimally, this policy isprovided before a face-to-face encoun-ter between the family/caregivers andthe medical provider to allow the pa-tient and family/caregivers sufficienttime to become familiar with the policyand prepare any questions they mayhave before the office visit. Office poli-cies can be given to the transitioningyouth and family/caregivers while inthe waiting room or be sent to theirhome before the visit. The delivery anddiscussion of the office transition pol-icy should be documented in the pa-tient’s medical records. Medical homeproviders should be familiar with eachof the transition policy’s componentsto facilitate discussion and respond toquestions posed during the office visit.Having a transitions policy that is pre-sented early to the patient and familyand other caregivers removes anydoubt about the timing of transfer andraises awareness that the medicalhome will be a valuable support forthose who need additional assistance.
For youth without special health careneeds, no further transition-specificactivities are required until the 14- to15-year visits. For adolescents withspecial health care needs, however,the period from 12 to 14 years of age islikely to be spent beginning prepara-tions for transition readiness. For this
reason, during the 12- to 13-year visits,the medical home provider must iden-tify those patients who are at risk ofhaving a more complicated transitionbecause of special medical, develop-mental, social, and/or environmentalneeds. Some children with particularlycomplex health care needsmay benefitfrom the early implementation of a for-mal transition plan before the ageof 14.
STEP 2: Ensure Step 1 Is Complete,
Then Initiate a Jointly
Developed Transition Plan With Youth &
Parents
In (3b) step 2, the medical home pro-vider initiates a transition plan that isjointly developed with the youth andhis or her parents. Starting at age 14(or before, for some children with spe-cial health care needs, as describedpreviously), a formal transition planshould be initiated for all youth andplaced in the medical record for re-view during future office visits. Thewritten plan should document theyouth’s current readiness to assume agreater role in self-management of hisor her health care, the steps to be con-ducted to achieve a successful transi-tion, and the transmittal of informa-tion to the youth and family/caregivers. It forms the basis forrecords to be provided to the receivingprovider and youth on the transfer ofcare between the ages of 18 and 21.Implementation and review of the tran-sition plan can be an important mea-surable quality-improvement effort onthe part of the medical home.
The starting point for this step is therecognition of patient capabilities anddelineation of responsibilities be-tween patient, family and other care-givers, andmedical providers for over-all patient care. Practices shouldselect a readiness-assessment tool touse that can be modified for specificpatient situations. Readiness tools
reveal areas of both strength andweakness on which patient educationcan be focused to accomplish futuregoals in self-management. Regardlessof the tool chosen, it should containspecific minimum components thatprovide an accurate, point-in-time as-sessment of the individual patient’sability to transition successfully.(These components are described be-low. Many readiness-assessment toolsand skills checklists exist for conduct-ing this assessment; some are listed in“Resources.”)
No matter what tool is used to assessand document readiness, providersshould interview family members orother caregivers and the youth inde-pendently of one another to identifyneeds and assess intentions and moti-vations for the patient’s independence.The identification of special healthcare needs (medical or otherwise) re-quires the medical home to be proac-tive in facilitating relationships be-tween the youth and appropriatecommunity and/or state resources.
STEP 3: Ensure Steps 1 & 2 Are Complete,
ThenReview & Update
Transitions Plan & Prepare for Adult
Care
In (3c) step 3, the medical home pro-vider reviews and updates the transi-tion plan and works with the patient toengage in the transition process. Thetransition plan documentation shouldbe reviewed on a regular basis to pro-mote recognition by the patient, thefamily/caregivers, and the provider ofsuccesses and/or deficits in readinesspreparation. Medical providers andcaregivers can reprioritize the readi-ness goals with respect to changes inthe youth’s medical status and/or con-cerns on the part of the caregivers. Al-though the number of times this re-view occurs depends on the frequencyof the patient’s visits to the medicalhome, it should be conducted at least
190 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on December 12, 2016Downloaded from

annually. Focused efforts and intensi-fied communication (among the pa-tient, family members and other care-givers, and providers) may uncoversystemic roadblocks or deficiencies inthe patient’s abilities to achieve previ-ous expectations.
If there has been a failure to achievetransition-readiness goals, a reevalua-tion of the existing plan is warranted; itmay be necessary to increase the fre-quency of medical home interventionsor visits. Because 16- to 17-year-oldsare significantly closer to the age ofexpected transfer of care to an adultmodel, accomplishing transition goalsmay not be feasible within the annualhealth maintenance schedule. Readi-ness plans will require revision onthe basis of the outcome of suchcommunication.
Successful transition requires theidentification of an adult care medicalhome, and completion of this task isone of themost important for pediatricproviders. The patient and/or family(and other caregivers) may need as-sistance identifying available and qual-ified adult care providers; when theyselect an adult provider, it is the pedi-atric medical home’s responsibility toensure appropriate communication ofany and all medical needs to the re-ceiving provider. In the final year be-fore transfer from the pediatric medi-cal home, the youth and family/caregivers might benefit from a visitwith the potential adult provider(s) toexplore the potential of a long-term re-lationship. Pediatric care occurringwithin a family medicine practice obvi-ates the need for such a visit but notthe need for preparation for an adultmodel of care.
STEP 4: Ensure Steps 1, 2, & 3 Are Complete,
ThenImplement Adult Care
Model
In (3d) step 4, the medical home pro-vider implements an adult care model
or affects the transfer to an adult med-ical home provider. After documentedcompletion of the readiness goals inthe individual youth’s transition plan,the pediatric provider’s role is to facil-itate transfer of care to an adult med-ical home. For young adults with com-plex health care issues, directcommunication between pediatric andadult providers is essential, becauseadult medical personnel may be unfa-miliar with certain pediatric condi-tions.17 For youth with complex needs,families are almost always a signifi-cant part of this conversation, becausethey are likely to be highly involved innot only caring for the youth but alsoarranging for, and supervising, otherswho provide care. The provider, youth,and family must jointly prepare a por-table medical summary and, for chil-dren with special health care needs, acare plan, which should be delivered tothe patient (or his or her legal guard-ian) and to the receiving provider.EHRs should also be provided to theadult provider. Medication reconcilia-tion should be performed by the pedi-atric medical home before the recordis transferred and by the receivingadult medical homewhen the record isreceived. (The components of thissummary are described in “Imple-menting the Algorithm.”)
Health care transition does not neces-sarily endwith transfer. Some patientsand/or caregiversmay need additionalsupport from the adult medical hometo complete specific transition tasks.Providing this support through carecoordination and consultation withinthe adult medical home optimizes thepatient’s self-management skills. Inaddition, the pediatric provider shouldmake himself or herself available tothe adult provider as a resource forany needed information or assistanceduring the immediate posttransferperiod.
Row 4: Determination of SpecialNeeds
Does Patient Have Special Health Care
Needs?
The transition process may be simplerfor youth without disabilities orchronic health conditions comparedwith those with special health careneeds. If the youth has no specialhealth care needs, the provider’s pri-mary task is to ensure that all age-appropriate transition issues are ad-dressed and that a smooth transfer toan adult model of care occurs. For theyouth with special health care needs,the transition process should be initi-ated at the age of 12 and may necessi-tate specific CCM activities (these com-ponents are described below). TheMCHB definition encompasses a widevariety of conditions and range of se-verities, including children with devel-opmental disabilities and chronic ill-nesses as well as those with mentalhealth and behavioral disorders.21 Thedevelopment of patient registries toaid in the identification of these chil-dren is a core component of CCMwithin the medical home model. An im-portant feature of such planning is therecognition that many tasks that leadto patient self-management are be-yond the capability of young adultswhose medical conditions include cog-nitive challenges. Transition goalsmust be individualized to account forsuch variations.
Row 5: CCM and Follow-up
Incorporate Transition Planning in Chronic
Condition Management
To the extent possible, basic transitionplanning and preparation for an adult
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 128, Number 1, July 2011 191by guest on December 12, 2016Downloaded from

health care model should be the samefor children and youth with and with-out special health care needs. Formany children and youth with chronicmedical, developmental, and/or behav-ioral conditions, however, an ex-panded process of transition planningis necessary to address the exchangeof more complex health information,competencies for self-care, and thetransfer of specialty care from pediat-ric to adult medical subspecialists. Inaddition, broader transitional issuesrelated to health insurance, entitle-ments, guardianship, and eligibility foradult community-based services mustbe addressed also. In a medical home,some youth with special health careneeds will have a written care plan aspart of the medical record that canserve as a script for care coordinationand care planning. At the age of 14, thiswritten care plan should begin to in-clude a section titled “transition plan”;this transition section should be devel-oped steadily as the youth approachesthe age of 18 and beyond. (Transitionplanning in CCM is more describedfully below.)
Have Age-Appropriate
Transition Issues Been Addressed?
Regardless of whether the child hasspecial health care needs, providersshould ensure that age-appropriatetransition issues have been addressedat every medical home visit and thatthe process is on track. Use of appro-priate transition-planning tools andreadiness checklists will facilitate theprovider’s ability to answer this ques-tion. The act of “addressing” transitionissues is not synonymous with the suc-cessful completion of the process,however. Identification of items inneed of attention, and the formulationof plans to accomplish them, may be
sufficient to complete this action step.If patients have fallen behind thetransition-planning schedule, provid-ers are likely to need to schedule a spe-cial visit to complete all of the tasksrelated to transition planning.
Initiate Follow-up Interaction
Follow-up interactions may take one ofseveral forms. Focused tasks that in-volve little detail or complexity can beaddressed by staff such as themedicalhome care coordinator or medicalprovider via telephone communicationor electronic media (eg, securee-mail). Larger or more complex is-sues may necessitate 1 or more face-to-face office visits, which should notbe relegated to the next periodichealth maintenance visit.
Row 6: Interaction Complete
TransitionComponent of
Interaction Complete
This point does not mean that the of-fice visit is complete or that the pro-vider does not continue to providecare, merely that the part of the pro-cess of providing care that centersaround transition planning has beencompleted for this specific office visitor interaction.
4. IMPLEMENTING THE ALGORITHM
Every youth who reaches the age oftransition from a pediatric medicalhome or becomes a legal adult withinhis or her currentmedical home needsto have a basic transition plan devel-oped through collaboration among theyouth, family, and provider. Those withspecial health care needs require ad-ditional components specifically to ad-dress their chronic care management(see “Integrating Transition Planning
Into CCM for Children and Youth WithSpecial Health Care Needs”).
a. Transition Plan Components forEvery Child and Youth
There are 4 recommended compo-nents for a transition plan, each ofwhich can be augmented by the useof specific tools to facilitate thework ofthe provider, youth, and family.
1. Assess for transition readiness. Theprovider, family, and youth begin byarticulating realistic goals for tran-sition and identifying new skills thatwill be needed by the patient tomeet those goals successfully. Al-though it is not the main focus ofthe medical home, the assessmentshould be “person-centered” andinclude identification of other areasof readiness for transition into theadult world in general, includingeducation/vocation, independentliving, and patient awareness ofmedical needs and age-appropriatepreventive care, as outlined by re-sources such as Bright Futures.18
Numerous tools are available in theform of “readiness checklists” thatallow providers to obtain a baselineidea of the current capacity of theyouth, family and other caregivers,and providers to successfullyachieve the outlined goals. Transi-tion progress should be measuredthrough periodic reassessment us-ing the same checklists at each visit(see “Resources” for selectedtransition-readiness materials).
2. Plan a dynamic and longitudinalprocess for accomplishing realisticgoals. The first step of transitionplanning is the establishment ofgoals that allow the youth toachieve as seamless a transition aspossible. A formal, written transi-tion plan that outlines specific ac-tions that are necessary to meetthe stated goals should be part ofthe patients’ medical record by the
192 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on December 12, 2016Downloaded from

age of 14. The written transitionplan should account for cultural,developmental, organizational, andcontingency-related concerns. Ingeneral, categories recommendedto be incorporated into the transi-tion plan include the plan’s maingoal(s), identification of who withinthe medical home will be responsi-ble for overseeing and/or coordi-nating the plan, the time line for ac-complishing stated goals, the skillsrequired by the youth to achievemaximum self-management, thefamilies’ or other caregivers’ role,and an articulation of proposed fi-nancing of the youth’s adult healthcare (see “Resources” for selectedtransition-planning tools).
3. Implement the plan through educa-tion of all involved parties and em-powerment of the youth in areas ofself-care. After the transition planhas been outlined and goals havebeen established, specific activitiesto ensure that the youth acquiresneeded skills should begin. Exam-ples of these goals include the abil-ity to schedule one’s own medicalappointments, obtain medications,have a one-on-one dialogue with amedical provider, and be familiarwith one’s medical history and anyneeded medications. Ongoing dis-cussion of the transition plan at allhealth care visits is a key step inaccomplishing transition goals.This should be a dynamic processthat begins gradually and is contin-ually assessed at regular intervals.The timing of these reassessmentsdepends on the capacity of theyouth and his or her family andother caregivers as well as theamount of time remaining untilthe anticipated transfer of care tothe adult medical home. Thetransition-readiness checklistsused during the initial assessmentto establish goals (outlined previ-
ously) are the tools of choice fordocumenting successful accom-plishment of specific goals andtasks. It is highly recommendedthat a medical home use the samechecklists throughout the entiretransition process for an individualpatient to provide continuity overtime and assist youth, families, andproviders to stay “on track” regard-ing specific goals that have yet to beaccomplished.
Throughout this process, the pro-vider should continually strengthenthe partnership with the patientand family members and othercaregivers by engaging in active di-alogue and information-sharing toempower the youth to take on newroles, as appropriate. It is impor-tant to recognize that, at the age ofmaturity, the youth becomes a legaladult (except when guardianship byanother person has been obtained).As a result of confidentiality laws,the youth should be seen alone un-less other arrangements have beenlegally made. One to 2 years be-fore the anticipated transfer ofmedical care, the pediatric pro-vider should assist the youthand/or family/caregivers to iden-tify potential adult practices, pre-pare the appropriate documenta-tion for transition, and suggestthat the youth interview the adultpractice before making a finaltransfer.
4. Document progress to enable ongo-ing reassessment andmovement ofmedical information to the receiv-ing (adult care) provider. Many ex-cellent tools for documenting thetransition process exist, includingsome that can be used within anEHR system and others that arepaper-based. For example, provid-ers might place a transition frontsheet on the patient’s chart or use a“dashboard” tool in the patient’s
EHR at the age of 12. Both of thesemethods work well in flagging im-portant actions that have occurredand/or need to be scheduled aspart of the transition process. Re-gardless of the specific tool used, itshould provide a flexiblemethod forassessing the youth’s readiness fortransition and progress made to-ward that goal. Gathering relevantinformation to document the pa-tient’s transition progress is of par-amount importance as the antici-pated transfer date approaches. Itis well documented that a commonbarrier to adult medical providers’acceptance of transitioning youth isa lack of accompanying medicaldocumentation.16 It is critical thatmedical documentation be portableand include 3 components: (1) thetransition plan (see above); (2) lon-gitudinal readiness checklists (seeabove), which demonstrate bothsuccesses and deficits in self-management skills; and (3) a porta-ble medical summary. The portablemedical summary contains basicmedical and social data to giveadult medical providers the infor-mation necessary to begin assum-ing care for the patient. All youthreceive this portable medical sum-mary, because the data it containsare essential topics and elementsthat are critical to the transitionsummary. Although the categoriesof the medical summary are appro-priate for all chronic health condi-tions, specific information shouldbe tailored to the patient’sconditions.
b. Integrating Transition PlanningInto CCM for Children and YouthWith Special Health Care Needs
Transition planning applies to all chil-dren and youth and should follow thesteps defined in the algorithm. Thepresence of chronic health conditionsand/or developmental disabilities (ie,
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 128, Number 1, July 2011 193by guest on December 12, 2016Downloaded from

children or youth with special healthcare needs) imposes specific primarycare requirements on the family-centered medical home characterizedas CCM. Effective CCM, in turn, de-mands additional considerations re-lated to transition planning. CCM in-volves an explicit, planned process ofcoordinated, proactive care aimed atachieving the best possible clinicaland functional outcomes for the indi-vidual patient and for the population ofpatients with chronic conditions. Whilefollowing the general sequence andtiming of the transition algorithm,transition planning for children oryouth with special health care needswill usually be incorporated into thebroader CCM process. Early in thetransition-planning process, it will beimportant to determine whether theyouth is likely to be a completely inde-pendent decision-maker as an adult orrequire decision-making support froma third-party proxy such as throughguardianship or power of attorney.Even with these considerations inmind, it is important to plan with theyouth and family/caregivers to achievethe maximum possible participation ofthe youth in the transition-planningprocess.
1. Registry. The family-centered medi-cal home CCM process may includea registry of the practice’s patientswith special health care needs. Theregistry should be searchable onthe basis of patient age so thatyouth who are ready for each stageof the transition process (see algo-rithm) can be identified. The regis-try might also include fields indicat-ing which steps in the transitionprocess are due for completion,have been completed, or are pastdue for completion. Additionalfields unique to the transition ofchildren or youth with specialhealth care needs might include
“discussed guardianship,” “identi-fied adult subspecialists,” etc.
2. Care Plan. Some children or youthwith special health care needs willhave an action-oriented care planfor tracking current problemsand health-related needs includingwhat action is needed, who will beresponsible, and by when the actionshould have occurred. When a childor youth with special health careneeds enters the age group coveredin the transition algorithm, theaction-oriented care plan shouldbegin to contain a transition sec-tion that will become the youth’stransition plan. The incorporationof the transition plan into the gen-eral action-oriented care plan willensure integration of transitionplanning with other health-relatedactions.
3. Care Coordination. Care coordina-tion is one of the foundations of thefamily-centered medical home andassumes special importance forchildren or youth with specialhealth care needs who utilize thehealth care system frequently andwho may have multiple health careand other service providers. Thosewho coordinate health care for thechild or youth with special healthcare needs will need to take intoconsideration the youth’s transitionplan and the current stage of thetransition-planning process. Carecoordination may be instrumentalin supporting the transfer of carefrom various pediatric medical sub-specialists to their adult specialtycounterparts.
4. CCM Visits. The family-centeredmedical home provides periodicCCM visits that may occur in addi-tion to health maintenance andacute illness management visits tomonitor the status of patients withchronic conditions and imple-ment/update their care plans.
These CCM visits would providethe occasions for transition edu-cation and planning.
5. Comanagement. Explicit comanage-ment between primary care physi-cians and medical subspecialistsensures communication and pre-vents both omissions and redun-dancies of care. It explicitly identi-fies the respective roles of theprimary caremedical home and themedical subspecialists in a mannerthat is clear to each provider andthe youth and family and othercaregivers. The locus of manage-ment may shift from time to timebetween primary care and spe-cialty care depending on the youth’sage and the complexity and acuityof specific health problems. Coman-agement with medical subspecial-ists assumes particular impor-tance for transition planning,because it provides the frameworkin which to plan for and implementthe transfer of care from pediatricsubspecialists to adultmedical sub-specialists and surgical specialists.Comanagement may also be thecontext for a dialogue of explicitcommunications between theyouth’s medical home and the fu-ture adult medical home provider.Comanagement planning with re-spect to transition planning shouldinclude the timing and process forspecific transfers of care in eachrelevant specialty area. In somecases, the plan may be to retain apediatric subspecialist into adult-hood because of the absence of ap-propriately qualified adult medicalsubspecialists.
It should be noted that somediagnosis-specific programs, includ-ing clinics for hemophilia and cysticfibrosis, have established strong pro-grams to guide subspecialty transfer.The National Hemophilia Foundationestablished a nationwide network of
194 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on December 12, 2016Downloaded from

hemophilia diagnostic and treatmentcenters and, in 2003, adopted transi-tion guidelines that provide age-relatedrecommendations. These models andtransition guidelines acknowledgethat there are continuing areas for im-provement such as addressing pre-ventive health needs or promoting theadult model of decision-making byyoung adult patients.30,31
i. Components of the Transition Planfor Youth With Special Health CareNeeds: Necessary Information for theReceiving Provider, Patient, andFamily Members/Caregivers
In addition to the items in the transi-tion plan for all youth (describedpreviously), additional componentsshould be included in transition plansand records for youth with disabilitiesand/or special health care needs. Alltransition plans should be tailored tothe individual patient and his or herneeds.
Additional data elements that arelikely to be included in the transferdocumentation for youth with specialhealth care needs include baselinefunctional and neurologic status; thepatient’s cognitive status, includingformal test results and date ofadministration, when possible;condition-specific emergency treat-ment plans and contacts; and the pa-tient’s health education history andassessment of his or her under-standing regarding health condi-tions, treatments, and prognosiswith particular attention to entryinto adult life, including procreationpotential and genetic information.
Information about advance directivesshould include an identification of thedecision-maker proxy or guardian andany history of advance-directive plan-ning. For patients with communicationimpairments, the transition documen-tation should include the patient’scommunication preferences and antic-
ipated needs for accommodations inboth communication and clinical care(ie, use of sign language interpreter,augmentative communication device,etc).
ii. Components of the Transition Planfor Youth With Special Health CareNeeds: Assessment andDocumentation of Readiness
As part of the transition-planning pro-cess, a member of the medical hometeam should regularly assess the pa-tient and his or her family and othercaregivers on progress toward achiev-ing transition readiness and prepara-tion for adult life. Interventions to ad-dress individual difficulties and/orprovide extra resources should beconducted during visits. Education andempowerment techniques should beused to ensure that development ofneeded skills is embraced by the pa-tient and families and continues to oc-cur. Providers must ensure that theydocument both the patient’s and fami-ly’s progress toward successfully com-pleting the plan’s components as wellas any plan revisions. A formal methodshould be used to document the step-wise completion of developmentallyappropriate tasks required to preparethe transitioning patient for adult life.Flow sheets, registry reminders, andplanned visit templates for specificages are all possiblemeans to do so. Inaddition, documentation is particu-larly important in certain specificareas.
Insurance CoverageThe 2010 Patient Protection and Af-
fordable Care Act (PPACA) health carereform legislation will affect coverage,access to care, and care coordinationin the short-term and/or long-term.Specific provisions of the PPACA ex-pand children’s and youth’s access tocoverage and ongoing care, includingchanges that permit children to re-main on their parent’s insurance until
the age of 26; eliminate insurers’ abil-ity to exclude coverage on the basis ofpreexisting conditions; improve cover-age portability; create a high-risk poolinsurance for people who cannot ac-cess coverage through other sources;enhance Medicaid payment to primarycare physicians; and mandate thatnearly all people (including youngadults) have coverage. Although thesechanges are likely to prove beneficial,it is likely that parents, caregivers, andtransitioning youth alike will need as-sistance to understand this complexlegislation and its impact on their livesand the transition process. In addition,PPACA provisions are to be imple-mented over time, and youth must beencouraged to proactively plan toavoid suffering substantial coveragegaps and/or delays in coverage be-cause of “preexisting conditions” until2014, when this practice is prohibitedunder PPACA. In addition, age eligibilityand coverage requirements may varyfor programs such as Title V, Medicaid,Supplemental Security Income (SSI),and Social Security Disability Income(SSDI). Youth with chronic conditionsshould be encouraged to evaluate fu-ture employment options that aremost likely to offer insurance coveragefor high-risk people (ie, employerswho participate in large group plansand, thereby, spread out risk). Paren-tal employment-based coverage limita-tions also vary widely; although a fewplans cover adults with disabilitieswho are dependents of their parents,they are the exception. Because of thecritical nature of insurance coveragefor people with special health careneeds, it is essential that providersdiscuss insurance issues with thesepatients and document plans to en-sure continued coverage.
Self-AdvocacyCritical topic areas for the empow-
erment of youth with special healthcare needs include self-advocacy and
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 128, Number 1, July 2011 195by guest on December 12, 2016Downloaded from

making plans about decision-makingstatus, educational and/or employ-ment opportunities, living arrange-ments, and community-inclusive op-portunities. It is critical to encouragefamilies to initiate training anddecision-making opportunities forchildren with special health careneeds at a young age. Families shouldreceive assistance from experts inself-advocacy when considering therange of potential support, which mayinclude personal informal advocates,power of attorney, and limited-to-fullguardianship. Important resources in-clude organizations, such as FamilyVoices; local chapters of The Arc; andlawyers who are experienced in dis-ability issues. Because of the impor-tance of self-advocacy for youth withspecial health care needs, it is essen-tial that providers initiate conversa-tions about decision-making and beginto plan advocacy support for theseyouth far in advance of the age ofmajority.
Legal IssuesThe assessment of the patient’s po-
tential capacity to consent occurs aspart of the ongoing CCM process. Pro-viders should suggest goals and actionsteps that help youth achieve their full-est potential and participate as muchas possible in assent and consent pro-cesses during their clinical care. It iscritical that youth and family membersand other caregivers alike understandthe significant health system changesassociated with the age of majority, in-cluding support-service or program-eligibility changes, selective serviceregistration requirements, consentand confidentiality provisions, andguardianship issues. Youth and familymembers/caregivers need to thinkabout how health care decisions willbe made once the youth turns 18. Be-cause of the particular importance oflegal issues for youth with specialhealth care needs, it is essential that
providers ensure that both the pa-tients and family members under-stand and are prepared for legalchanges associated with adulthood. Inaddition, problems can arise when ayouth is incapacitated and unable todirect his or her own care. Preparing ahealth care proxy or power of attorneyfor the young adult will avert such asituation.
Health EducationPeople with chronic conditions
should receive periodic, updatedhealth education about their condition.Necessary information includes an un-derstanding of the patient’s specificcondition; typical disease process andprognosis; current treatment andtreatment options; medication knowl-edge; self-assessment; and self-careissues, especially in defining emergentsituations and responses. Particularattention should be paid to issues ofpuberty that may not have presentedearlier, such as sexual expression, re-productive issues, and genetic trans-mission. Because of the importance ofthe patient’s understanding his or herown condition, it is essential for pro-viders to document that this informa-tion has been provided to, and under-stood by, the patient.
Caregiver’s IssuesAssessment of family/caregiver ad-
aptation is another component of thetransition-readiness assessment forfamilies of children and youth withchronic conditions. Attention shouldbe paid to coping on the part of theyouth, his or her parents and siblings,and any other appropriate familymembers and other caregivers. Par-ents and caregivers must adapt to thetransition of authority from parent toyouth that occurs when the youth hasthe capacity to accept the transfer andmay experience grief if the child lacksthe capacity to assume independentdecision-making. For this reason,providers must be ready to help par-
ents and caregivers cope with thelife changes associated with chronicconditions as well as with transferplanning. Because these situationscan be stressful for the youth andfamily members/caregivers alike, itis essential that providers assess pa-tients’ coping mechanisms and pro-vide referrals for additional care, asappropriate.
5. ADULT MEDICAL HOME(RECEIVING PROVIDER): ROLESAND RESPONSIBILITIES
The transition of a young adult willmake it necessary to identify an adultpractice that is prepared to accept thepatient and provide the full range ofcare and care coordination in anappropriate, patient-centered caremodel. Most young adults are healthyand require only the continuation ofhealth maintenance and promotionand the availability of an adult medicalhome when acute illnesses arise. Yet,even the population of young adultswithout special health care needs in-cludes those with adolescent-typerisky behaviors, mental health issues,and reproductive health needs that re-quire enhanced attention. Youngadults with disabilities and chronicmedical conditions are more vulnera-ble to failures in the transition ofhealth care services and require moreattention from providers and thehealth care system. Fundamentally,clinical hurdles and process hurdlespresent major challenges for a suc-cessful move to adult-oriented care foryoung adults with special health careneeds.
The transition of a young adult neces-sitates the identification of an adultpractice that is prepared to accept thepatient and provide the full range ofcare and care coordination in anappropriate patient-centered caremodel. Shortages in the adult medicalhome workforce may limit future ca-
196 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on December 12, 2016Downloaded from

pacity to do so. Thus, clinical hurdleslargely encompass deficits in educa-tion and/or experience of some adultproviders to effectively care for this di-verse patient population, as well as fi-nancial disincentives that limit accessto adult-oriented care. The authors ofseveral recent articles have exploredthe perspective of adult providers par-ticipating in the medical transition ofyoung adults with special health careneeds. Okumura et al15 found that,when adult medical care providerswere exposed to the process of transi-tioning young adults in the context oftheir residency training experiences,they weremuchmore likely to incorpo-rate it into their practices after resi-dency. Anecdotally, however, theseresidency training experiences are notcommon, and many practicing physi-cians have learned “on the job” toman-age patients with complex needs. A re-cent survey of internists’ needs whenaccepting a transitioning youth re-vealed that education in congenitaland childhood-onset conditions wascritical.17 In addition, the respondentscited the need for identified medicalsubspecialists to help with manage-ment decisions. Although adult med-ical providers have the role of as-suming the care and management ofthese youth, they should not be ex-pected to do so without supportsthat are more readily available to pe-diatric providers.
Caring for young adults with specialhealth care needs may represent achallenge that some adult primarycare practices are currently not pre-pared to meet. Further work is neededto characterize, demonstrate, andteach an adult model of care that isresponsive to the particular needs ofall young adults and sensitive to thespecific challenges associated withproviding high-quality care to youngadults with specific chronic conditions(eg, autism, cerebral palsy, intellectual
disability, sickle cell disease). Ideally,the health care payment system wouldencourage early and ongoing profes-sional relationships with pediatricproviders in anticipation of transitionsand also support comanagement withpediatric primary care and medicalsubspecialty providers while the pa-tient is becoming established with theadult practice. At some point, the re-sponsibility for the transitioning youngadult will become that of the adult pro-vider, at which time, the adult providerand his or her clinical team should as-sume a key role in supporting theyoung adult and his or her family andother caregivers in finding a new bal-ance in the adult medical setting. Thetransitioning youth’s developmentaland functional abilities may influencethe transition’s success. The contin-ued involvement of the family/caregiv-ers should be expected and encour-aged during this transition period. Inaddition, working with the family andother caregivers and other supportsto ensure adequate health care insur-ance and financing for these youth is amajor goal of transition.
Second, process hurdles include chal-lenges in the communication of appro-priate medical records; community re-sources; preparation of the youngadult and his or her family/caregiversto integrate into an adult-focusedmed-ical system; and issues related to pay-ment. Adult providers should notexpect a “handoff” from pediatricpractices but, rather, a “handshake.”Establishing collegial relationships be-tween pediatric and adult medical pro-viders is important for facilitating on-going access to medical care forpatients in transition. Although everytransition is different, the best transi-tions include several core elements.Receivers (providers to whom theyouth transitions for care) may rea-sonably expect that, as the adult med-ical home team, they will be provided
with concise and accurate medical in-formation about the youth and his orher condition, as described previously.In addition, receivers should ensurethat:
● the responsible party for medicaldecision-making has been clearlyidentified;
● unambiguous adult consent andconfidentiality policies have beenexplained to the patient and his orher family and other caregivers;
● communication has occurred abouthow the practice operates for is-sues such as paperwork and medi-cation refills; and
● access to the practice for routineand after-hours care has been dis-cussed with the patient and his orher family and other caregivers.
Although many young adult patientswill transition to adult practices frompediatric-based practices, the uniquerelationship that many family physi-cians have with their patients allowsfor ongoing care throughout the lifespan. Although transfer of care manynot occur in these situations, it is likelythat young adults with special healthcare needs have pediatric subspecial-ists whomay wish to facilitate transferto their adult counterparts. The familyphysician has the special responsibil-ity to be aware of these needs and, insome situations, to potentially playthe role of both the “sender” and“receiver.”
Certainly, successful transition is atest of the degree to which a practiceoperates within the ideals encom-passed in the medical home model ofcare. A team approach to the chal-lenges of transition is necessary forfacilitating the level of care for whichadult providers strive. Inclusion of lo-cal public health and community-based resources should be consideredwhenever possible to ensure that themedical home approach is followed,
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 128, Number 1, July 2011 197by guest on December 12, 2016Downloaded from

particularly for vulnerable patientpopulations with special health careneeds.
Payment for Health CareTransition Work
The steps involved in the health caretransition algorithm are intended tobe part of existing office visits usingwell-established billing codes. Foryouth without special health careneeds, transition preparation andplanning would be incorporated intoregularly scheduled health mainte-nance visits and billed as such (Cur-rent Procedural Terminology [CPT]codes 99394 and 99395). For youthwithspecial health care needs who havesufficient complexity to justify periodicCCM visits in addition to health mainte-nance visits, health care transitionpreparation and planning are in-tended to occur during a CCM visitbilled as a prolonged encounter withan established patient (CPT codes99214 or 99215). Such visits can bedocumented as involving counselingfor more than 50% of the visit. Youthwith highly complex needs may re-quire a CCM visit in which the counsel-ing provided is devoted entirely totransition, but these visits are still re-imbursable when using the prolonged-encounter codes and the counselingrule. Activity outside of office encoun-ters involved in the management of ayouth’s transition plan (whether itstands alone or is incorporated into amore general care plan for a chroniccondition) constitutes “care plan over-sight.” Such work may involve phonecalls to prospective adult primary carephysicians or medical subspecialists,conversations with the youth and fam-ily regarding transition plans, or com-munication with community agenciesintegral to the transition process.These activities can be billed by usingcare plan oversight CPT codes 99374(15–29 minutes) and 99375 (�30 min-utes) through which the physician can
bill monthly for the cumulative timespent on care (or transition) plan over-sight. Similar coding and billing op-tions may be exercised after the trans-fer of care from a pediatric medicalhome to an adult medical home.
6. CLINICAL GUIDANCE ANDFUTURE SUGGESTIONS
This report attempts to address theneed for guidance to aid practitioners’implementation of youth transitionplanning into practice. Yet, transitionscannot occur in a vacuum. Systemicbarriers that have been reported asfactors that hamper clinicians fromimplementing needed changes includelack of training and payment for tran-sition activities, receivers to acceptthese patients, research to identifybest practices, and advocacy to ad-vance the research results. Increasedtraining on the critical skill of transi-tioning can be integrated into an ado-lescent medicine rotation in internalmedicine and into the adolescent med-icine and continuity clinic rotations forpediatric residents. Med-peds, pediat-rics, and family medicine residenciesmay provide significant trainingopportunities in this area. Duallyboarded med-ped physicians wouldseem ideally equipped to care for tran-sitioning adolescents and youngadults and to assist in the training ofother primary care generalist physi-cians regarding care over this agerange. Unfortunately, the med-pedsworkforce remains too small and isnot likely to grow sufficiently to affectthe health care transition of mostyouth and young adults.
Graduatemedical education programsmay also provide a forum for pediatricand adult providers to build and main-tain relationships that are needed toenhance collaboration and improvecommunication, ultimately facilitatingcomanagement of complex conditions.Payment is a crucial element in the
promotion of transition planning. In-corporating transition planning intoCCM is a process that costs time andmoney and should be included in con-versations about care coordinationand payment. Further research is re-quired to define best practices, clini-cal pathways, and cost-effectivenessfor transition planning. Quality-improvement science may provide ad-ditional methodologies to inform theunderstanding of potential strategies.Once best practices are identified, ad-vocacy and education efforts will needto be directed toward several areasincluding:
● enhanced payment for transitionservices;
● case-finding of those in need of tran-sition services who are not receiv-ing them;
● insurance coverage for patients inneed of transition planning;
● standards of care and credentialingof providers;
● training for primary care physi-cians and medical subspecialists topromote transitions within themed-ical home; and
● promotion of training and clinicallearning experience on transitionand transfer of youth and youngadults (both with and without spe-cial needs) for trainees in all medi-cal fields.
7. CONCLUSION
A well-timed, well-planned, and well-executed transition from child- toadult-oriented health care, ideally oc-curring between the ages of 18 and 21,enables youth to optimize their abilityto assume adult roles and activities.For this reason, transition planningshould be a standard part of providingcare for all youth and young adults,and every patient should have an indi-vidualized transition plan regardlessof his or her specific health care
198 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on December 12, 2016Downloaded from

needs. The AAP, American Academy ofFamily Physicians, and American Col-lege of Physicians recognize that pro-viders need assistance to accomplishthis goal. Education of practicing andresident physicians in training is es-sential for the integration of the con-cepts of the patient- and family-centered medical home, the principlesof transition of care, and the pro-cesses for successful transfer of care.Therefore, this clinical report providesa consensus on activities to supportthe practice-based implementation oftransition planning for youth with andwithout special health care needs. Itdescribes a series of activities de-signed to ensure that uninterrupted,high-quality, and developmentally ap-propriate health care services areavailable to patients moving from ado-lescence to adulthood. The clinical re-port provides a clear time line, begin-ning at 12 years of age, to assistproviders in implementing the 4 spe-cific activities in transition: discussingthemedical home transition policy; ini-tiating a transition plan; reviewing/up-dating the transition plan; and imple-menting an adult care model. It alsoincludes an algorithm that specifiesthe protocol for managing the transi-tion process, helps providers imple-ment the transition process, and pro-vides a transition structure forpatients and their families. The algo-rithm includes a branch with ex-panded, generic guidelines for transi-tioning youth with special health careneeds who require CCM. Primary careproviders and medical subspecialistsare encouraged to make this processspecific for their own and their pa-tients’ needs.
8. RESOURCES
a. General Resources
● National Health Care Transition Cen-ter (www.gottransition.org).
● Family Voices, Inc (www.familyvoices.org).
● Family-to-Family Health Information& Education Center (www.bridges4kids.org/f2f).
● Kids as Self Advocates (KASA) (www.fvkasa.org).
● National Alliance to Advance AdolescentHealth (www.thenationalalliance.org).
b. Transition Care Plans
● AAP/National Center for MedicalHome Implementat ion (www.medicalhomeinfo.org/how/care_delivery/transitions.aspx).
● British Columbia Ministry of Chil-dren and Family Development,“Transition Planning for Youth WithSpecial Needs” (www.mcf.gov.bc.ca/spec_needs/pdf/support_guide.pdf).
● University of Washington, AdolescentHealth Transition Project (http://depts.washington.edu/healthtr).
c. Transition Assessment andEvaluation Tools
● AAP/National Center for MedicalHome Implementation (www.medicalhomeinfo.org/health/trans.html).
● JaxHATS, evaluation tools for youthand caregivers and training materi-als for medical providers (www.jaxhats.ufl.edu/docs).
● Texas Children’s Hospital transitiontemplate (http://leah.mchtraining.net/bcm/resources/tracs).
● Carolina Health and TransitionProject (CHAT) (www.mahec.net/quality/chat.aspx?a�10).
● University of Washington, Adoles-cent Health Transition Project (http://depts.washington.edu/healthtr).
● Wisconsin Community of Practiceon Transition (www.waisman.wisc.edu/wrc/pdf/pubs/THCL.pdf).
d. Portable Medical Summaries
● AAP/National Center for MedicalHome Implementat ion (www.medicalhomeinfo.org/how/care_delivery/transitions.aspx).
● National Diabetes Education Pro-gram (www.YourDiabetesInfo.orgor www.ndep.nih.gov).
● Sick Kids (www.sickkids.ca/good2go).
● University of Washington, Adoles-cent Health Transition Project, med-ical summary (http://depts.washington.edu/healthtr/medsum/portable_medsum.pdf).
LEAD AUTHORSW. Carl Cooley, MDPaul J. Sagerman, MD
TRANSITIONS CLINICAL REPORTAUTHORING GROUPW. Carl Cooley, MD, Co-chairpersonPaul J. Sagerman, MD, Co-chairpersonMichael S. Barr, MD, MBA – American Collegeof PhysiciansMary Ciccarelli, MDAlbert C. Hergenroeder, MDThomas S. Klitzner, MD, PhDMarie Mann, MD, MPH – Maternal and ChildHealth BureauLaura Pickler, MD, MPH – American Academyof Family PhysiciansBonnie Strickland, PhD – Maternal and ChildHealth BureauBrad Thompson, MAStuart T. Weinberg, MD – Partnership forPolicy Implementation (PPI)Patience H. White, MD, MANicholas C. Wilkie, MA
AAP STAFFStephanie Mucha Skipper, MPH
CONSULTANTSAmy Brin, MSN, MA, PCNS-BCSusan K. Flinn, MA
ACKNOWLEDGMENTThe development of this clinical reportwas funded by the American Academyof Pediatrics and the National Centerfor Medical Home Implementationthrough a cooperative agreement(U43MC09134) with the US Depart-ment of Health and Human Services,Health Resources and Services Ad-ministration, Maternal and ChildHealth Bureau.
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 128, Number 1, July 2011 199by guest on December 12, 2016Downloaded from

REFERENCES
1. American Academy of Pediatrics; AmericanAcademy of Family Physicians; AmericanCollege of Physicians-American Society ofInternal Medicine. A consensus statementon health care transitions for young adultswith special health care needs. Pediatrics.2002;110(6 pt 2):1304–1306
2. Stewart D. Transition to adult services foryoung people with disabilities: current evi-dence to guide future research. Dev MedChild Neurol. 2009;51(suppl 4):169–173
3. US Department of Health and Human Ser-vices, Health Resources and Services Ad-ministration, Maternal and Child Health Bu-reau. The National Survey of Children WithSpecial Health Care Needs Chartbook 2001.Rockville, MD: US Department of Health andHuman Services; 2004
4. US Department of Health and Human Ser-vices, Health Resources and Services Ad-ministration, Maternal and Child Health Bu-reau. The National Survey of Children WithSpecial Health Care Needs Chartbook2005–2006. Rockville, MD: US Department ofHealth and Human Services; 2008
5. Bloom S. Presentation to American Academy ofPediatricsTransitionAdvisoryMeeting:evidencebase for systems of care for children and youthwithspecialhealthcareneeds—transition.Pre-pared by the Center for Child and AdolescentHealth Policy at Massachusetts GeneralHospital; June 2008; Elk Grove Village, IL
6. American Academy of Pediatrics, Depart-ment of Research. Survey: transition ser-vices lacking for teens with special needs.AAP News. 2009;30(11):12
7. McManus M, Fox H, O’Connor K, Chapman T,MacKinnon J. Pediatric Perspectives and Prac-tices on Transitioning Adolescents With SpecialNeeds to Adult Health Care. Washington, DC: Na-tional Alliance to Advance Adolescent Health;2008. Fact Sheet No. 6. Available at: www.thenationalalliance.org/jan07/factsheet6.pdf.Accessed August 6, 2010
8. Tuchman LK, Schwartz LA, Sawicki GS, BrittoMT.Cystic fibrosis and transition to adult medicalcare. Pediatrics. 2010;125(3):566–573
9. Sawicki GS, Lukens-Bull K, Yin X, et al. Mea-suring the transition readiness of youthwith special healthcare needs: validation ofthe TRAQ—Transition Readiness Assess-ment Questionnaire. J Pediatr Psychol.2011;36(2):160–171
10. Viner R. Transition from paediatric to adultcare: bridging the gaps or passing thebuck? Arch Dis Child. 1999;81(3):271–275
11. Telfair J, Alexander LR, LoosierPS, Alleman-VelezPL, Simmons J. Providers’ perspectives and be-liefs regarding transition to adult care for ado-lescents with sickle cell disease. J Health CarePoor Underserved. 2004;15(3):443–461
12. FlumePA, AndersonDL, Hardy KK, GrayS. Transi-tionprograms incysticfibrosis centers: percep-tion of pediatric and adult program directors.Pediatr Pulmonol. 2001;31(6):443–450
13. Reiss JG, Gibson RW, Walker LR. Health caretransition: youth, family, and provider per-spectives. Pediatrics. 2005;115(1):112–120
14. Scal P. Transition for youth with chronicconditions: primary care physicians’ ap-proaches. Pediatrics. 2002;110(6 pt 2):1315–1321
15. Okumura MJ, Heisler M, Davis MM, CabanaMD, Demonner S, Kerr EA. Comfort of gen-eral internists and general pediatricians inproviding care for young adults withchronic illnesses of childhood. J Gen InternMed. 2008;23(10):1621–1627
16. Colwill JM, Cultice JM, Kruse RL. Will gener-alist physician supply meet demands of anincreasing and aging population? Health Aff(Millwood). 2008;27(3):w232–w241
17. Peter NG, Forke CM, Ginsburg KR, SchwarzDF. Transition from pediatric to adult care:internists’ perspectives. Pediatrics. 2009;123(2):417–423
18. Hagan JF, Shaw JS, Duncan PM, eds. BrightFutures: Guidelines for Health Supervisionof Infants, Children, and Adolescents. 3rded. Elk Grove Village, IL: American Academyof Pediatrics; 2008
19. National Committee for Quality Assurance.Stan-dards and Guidelines for Physician PracticeConnections: Patient-Centered Medical Home(PPC-PCMH). Washington, DC: National Commit-tee for Quality Assurance; 2008
20. CooleyWC,McAllisterJW,SherriebK,ClarkR.TheMedical Home Index: development and valida-tion of a new practice-level measure of imple-mentation of the medical home model. AmbulPediatr. 2003;3(4):173–180
21. McPhersonM, Arango P, Fox H, et al. A new defi-nition of childrenwith special healthcare needs.Pediatrics. 1998;102(1 pt 1):137–140
22. ShawP,KabaniNJ, LerchJP,etal.Neurodevelop-
mental trajectories of the human cerebral cor-tex. J Neurosci. 2008;28(14):3586–3594
23. American Academy of Pediatrics, Council onChildren With Disabilities, Section on Devel-opmental Behavioral Pediatrics, Bright Fu-tures Steering Committee, Medical HomeInitiatives for Children With Special NeedsProject Advisory Committee. Identifying in-fants and young children with developmen-tal disorders in the medical home: an algo-rithm for developmental surveillance andscreening [published correction appears inPediatrics. 2006;118(4):1808–1809]. Pediat-rics. 2006;118(1):405–420
24. Shapiro JP. No Pity: People With Disability,Forgiving a New Civil Rights Movements.New York, NY: Times Press; 1994
25. State of Minnesota, Revisor of Statutes.3525.2900transitionandbehavioral interventionplanning.Availableat:www.revisor.leg.state.mn.us/data/revisor/rule/current/3525/3525.2900.pdf. Accessed August 6, 2010
26. Johnson CP, Myers SM; American Academyof Pediatrics, Council on Children With Dis-abilities. Identification and evaluation ofchildren with autism spectrum disorders.Pediatrics. 2007;120(5):1183–1215
27. Wolf-BraniginM,SchuylerV,WhitePH. Improvingquality of life and career attitudes of youth withdisabilities: experience from the Adolescent Em-ploymentReadinessCenter.ResSocWorkPract.2007;17(3):324–333
28. McDonagh JE, Southwood TR, Shaw KL. Theimpact of a coordinated transitional careprogramme on adolescents with juvenile id-iopathic arthritis. Rheumatology (Oxford).2007;46(1):161–168
29. Geenen S, Powers LE, Sells W. Understand-ing the role of health care providers duringthe transition of adolescents with healthconditions and disabilities. J AdolescHealth. 2003;32(3):225–233
30. Sawicki G, Sellers D, McGuffie K, RobinsonW.Adults with cystic fibrosis report importantand unmet needs for disease information. JCyst Fibros. 2007;6(6):411–416
31. Boyle MP, Farukhi Z, Nosky ML. Strategiesfor improving transition to adult cystic fi-brosis care, based on patient and parentviews. Pediatr Pulmonol . 2001;32(6):428–436
200 FROM THE AMERICAN ACADEMY OF PEDIATRICSby guest on December 12, 2016Downloaded from

APPENDIX 1
FROM THE AMERICAN ACADEMY OF PEDIATRICS
by guest on December 12, 2016Downloaded from

APPENDIX 1 CONTINUED
by guest on December 12, 2016Downloaded from

DOI: 10.1542/peds.2011-0969; originally published online June 27, 2011; 2011;128;182Pediatrics
American College of Physicians, Transitions Clinical Report Authoring GroupAmerican Academy of Pediatrics, American Academy of Family Physicians, and
Medical HomeSupporting the Health Care Transition From Adolescence to Adulthood in the
ServicesUpdated Information &
/content/128/1/182.full.htmlincluding high resolution figures, can be found at:
References
/content/128/1/182.full.html#ref-list-1at:This article cites 23 articles, 14 of which can be accessed free
Citations /content/128/1/182.full.html#related-urls
This article has been cited by 99 HighWire-hosted articles:
Subspecialty Collections
/cgi/collection/adolescent_health:medicine_subAdolescent Health/Medicine
/cgi/collection/medical_home_subMedical Home
/cgi/collection/community_pediatrics_subCommunity Pediatricsthe following collection(s):This article, along with others on similar topics, appears in
Permissions & Licensing
/site/misc/Permissions.xhtmltables) or in its entirety can be found online at: Information about reproducing this article in parts (figures,
Reprints /site/misc/reprints.xhtml
Information about ordering reprints can be found online:
rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Grove Village, Illinois, 60007. Copyright © 2011 by the American Academy of Pediatrics. All and trademarked by the American Academy of Pediatrics, 141 Northwest Point Boulevard, Elkpublication, it has been published continuously since 1948. PEDIATRICS is owned, published, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on December 12, 2016Downloaded from

DOI: 10.1542/peds.2011-0969; originally published online June 27, 2011; 2011;128;182Pediatrics
American College of Physicians, Transitions Clinical Report Authoring GroupAmerican Academy of Pediatrics, American Academy of Family Physicians, and
Medical HomeSupporting the Health Care Transition From Adolescence to Adulthood in the
/content/128/1/182.full.html
located on the World Wide Web at: The online version of this article, along with updated information and services, is
of Pediatrics. All rights reserved. Print ISSN: 0031-4005. Online ISSN: 1098-4275.Boulevard, Elk Grove Village, Illinois, 60007. Copyright © 2011 by the American Academy published, and trademarked by the American Academy of Pediatrics, 141 Northwest Pointpublication, it has been published continuously since 1948. PEDIATRICS is owned, PEDIATRICS is the official journal of the American Academy of Pediatrics. A monthly
by guest on December 12, 2016Downloaded from