Embed Size (px)
Citation preview
Renal Pathophysiology I
Review of Renal Function
Role of the Kidneys in Maintaining Blood Volume and Pressure
Main Functions of Kidneys
• Regulation of Blood Volume and Pressure– (focus of today’s lecture)
• Regulation of Plasma Composition– (focus of Lecture 2)
• Elimination of Wastes– (focus of Lecture 3)
• Excretion of foreign chemicals
• Endocrine functions
Role of Kidneys in Disease
• Innocent bystanders in other problems or pathologies– Most often, kidneys help solve these
problems– Sometimes the kidney can contribute to
problems
• Often damaged by other disease processes
• Indicator of disease elsewhere in the body
The Burden of Kidney Disease
• In 2008, nearly 550,000 people were being treated for end stage renal disease.
• Of these, about 70% were on dialysis. – Most are treated at dialysis centers, typically 3
times per week, about 4 hours each time.– Cost = $77,000 per patient per year– All Americans who need dialysis are covered by
Medicare, regardless of age
Major Causes of Renal Disease
• Diabetes: 205,724 cases per year
• Hypertension: 133,537
• Glomerulonephritis: 83,268
• Cystic kidney: 26,094
• Urologic disease: 13,065
• All other: 86,294
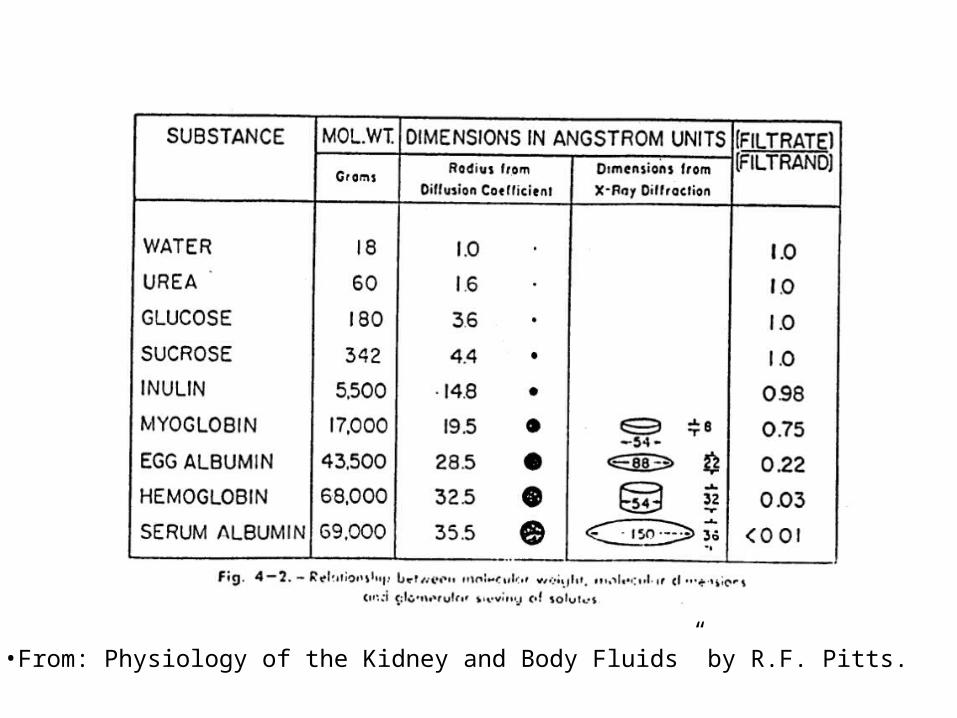
•From: Physiology of the Kidney and Body Fluids” by R.F. Pitts.
Glomerular Filtration Rate (GFR)
• Good indicator of renal function
• Declines with age, but large safety factor
• Significance of changes:– Moderate changes in GFR provide information
to kidney about blood volume– A significant fall in GFR causes substances
that are normally eliminated by the kidneys to remain in the blood = renal failure
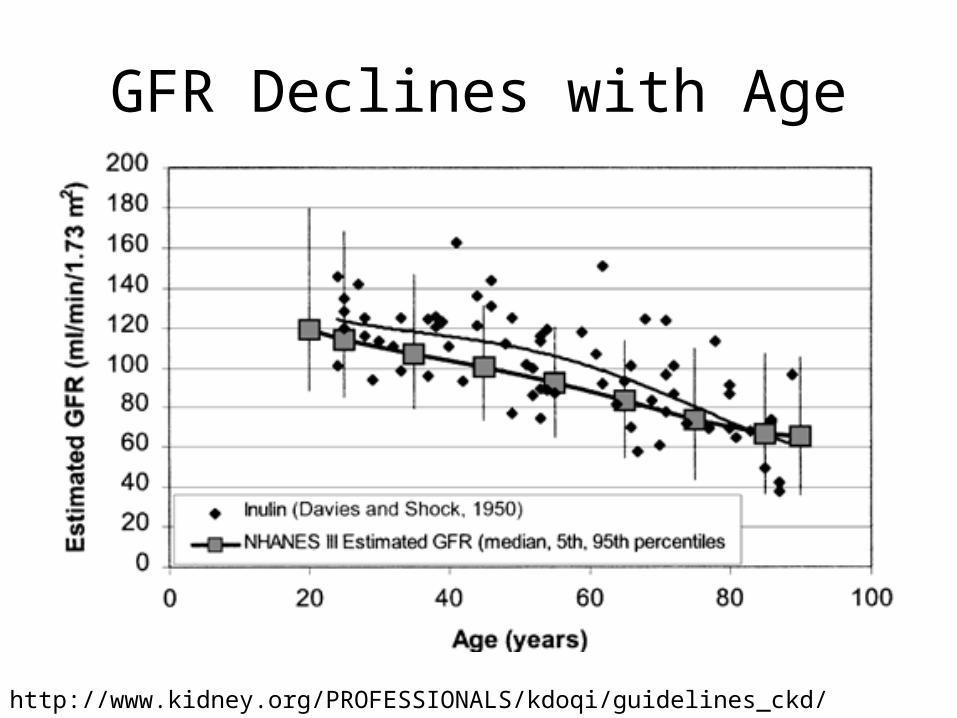
GFR Declines with Age
http://www.kidney.org/PROFESSIONALS/kdoqi/guidelines_ckd/Gif_File/kck_f9.gif
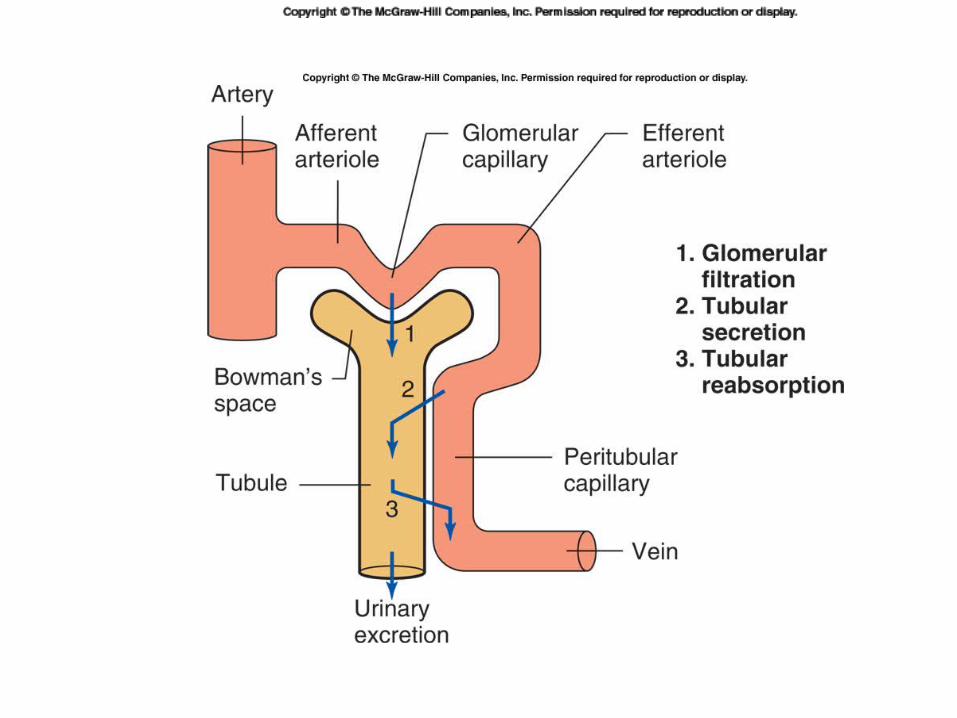
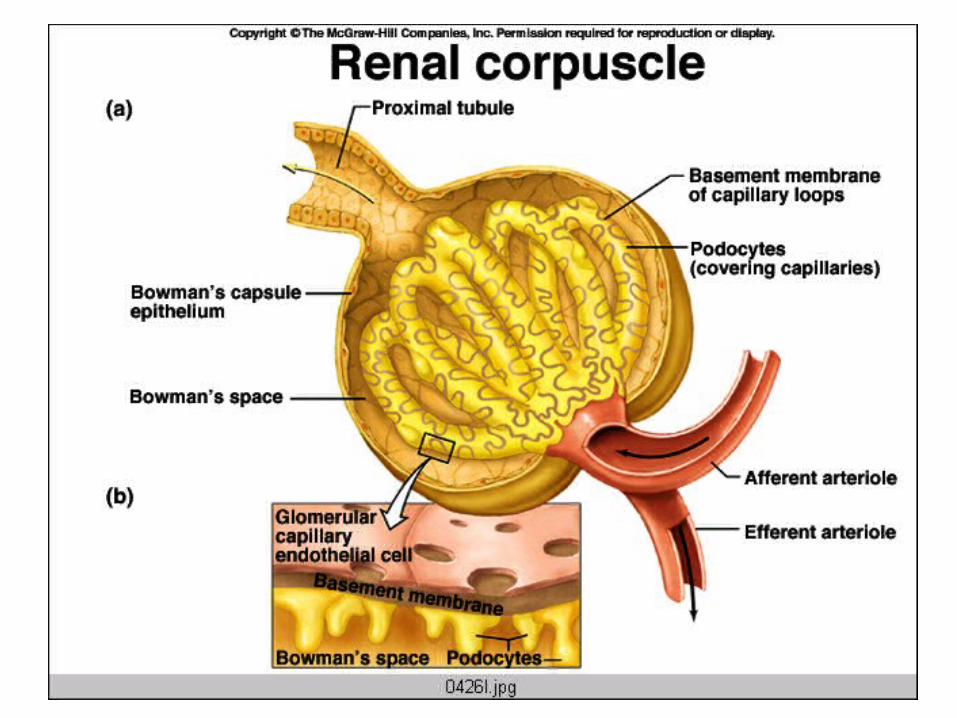
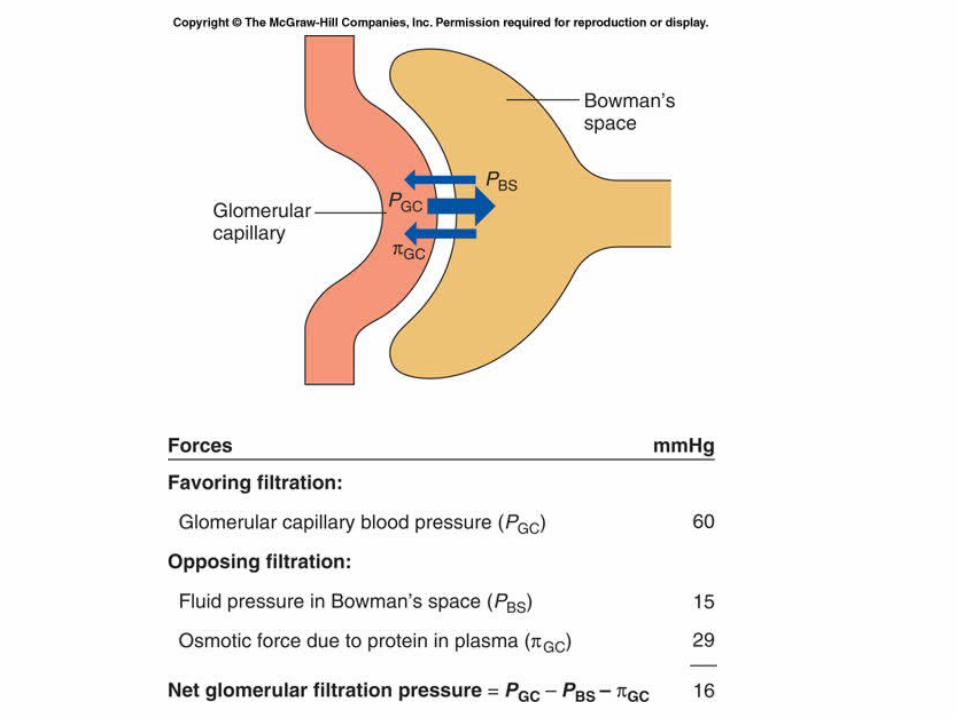
Determinants of GFR
• Rate of filtration = hydraulic permeability x surface area x net filtration pressure.
or: • Rate of filtration = Kf x net filtration pressure.
• The forces that determine the net filtration pressure are the same Starling Forces that affect all capillaries:– Capillary hydrostatic pressure, interstitial hydrostatic
pressure, capillary oncotic pressure, interstitial oncotic pressure
These determinants can change with injury or disease
• Diabetes – deposition of extracellular matrix material decreases Kf.
• Obstruction of kidney tubule (due to inflammation or scarring) will increase PBS,
which will decrease GFR.• Autoimmune diseases such as lupus (SLE)
involves production of immune complexes that can damage the glomerulus, ultimately decreasing the Kf.
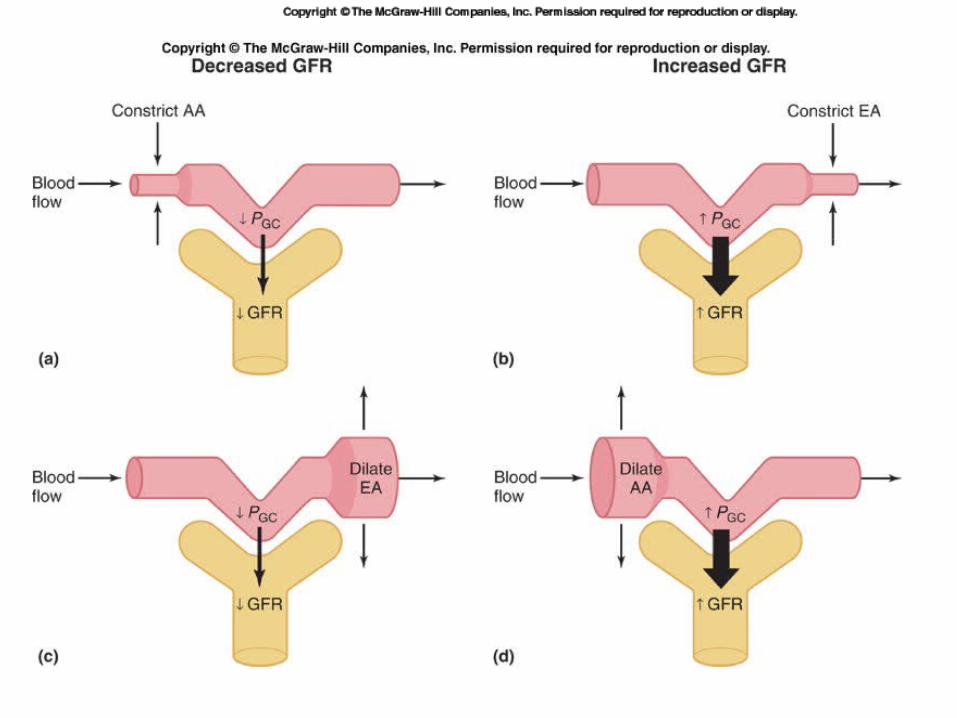
Regulation of GFR
• Changes in MAP change renal blood flow
• Changes in contraction of renal arterioles can shift the GFR.
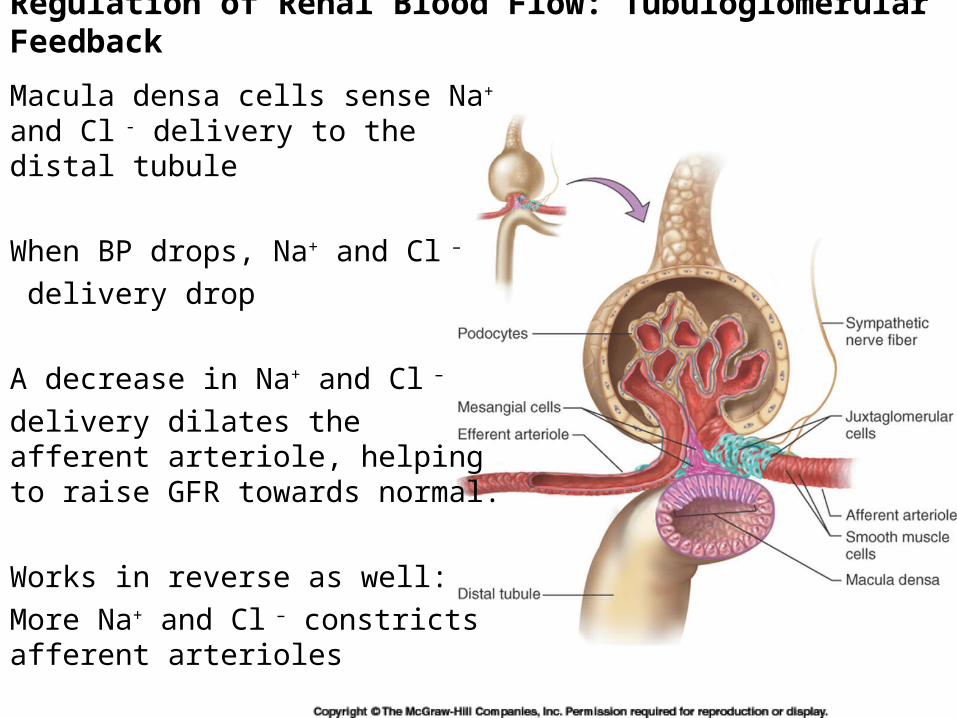
Macula densa cells sense Na+ and Cl - delivery to the distal tubule
When BP drops, Na+ and Cl –
delivery drop
A decrease in Na+ and Cl –
delivery dilates the afferent arteriole, helping to raise GFR towards normal.
Works in reverse as well:
More Na+ and Cl – constricts afferent arterioles
Regulation of Renal Blood Flow: Tubuloglomerular Feedback
Regulation of Sodiumand Blood Volume
What is the connection between sodium and blood volume?
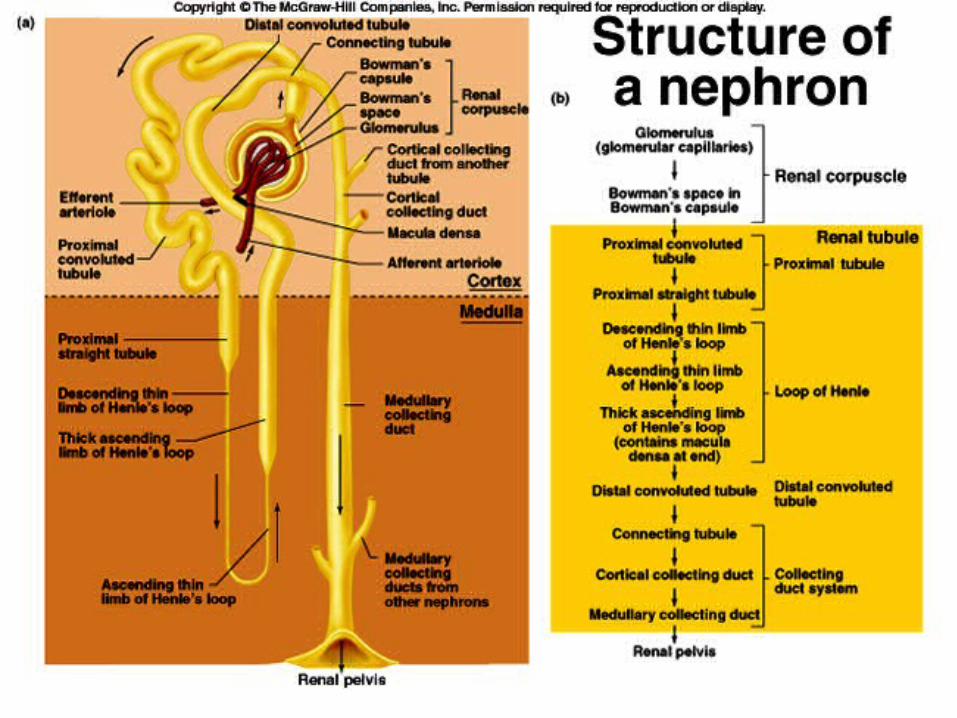
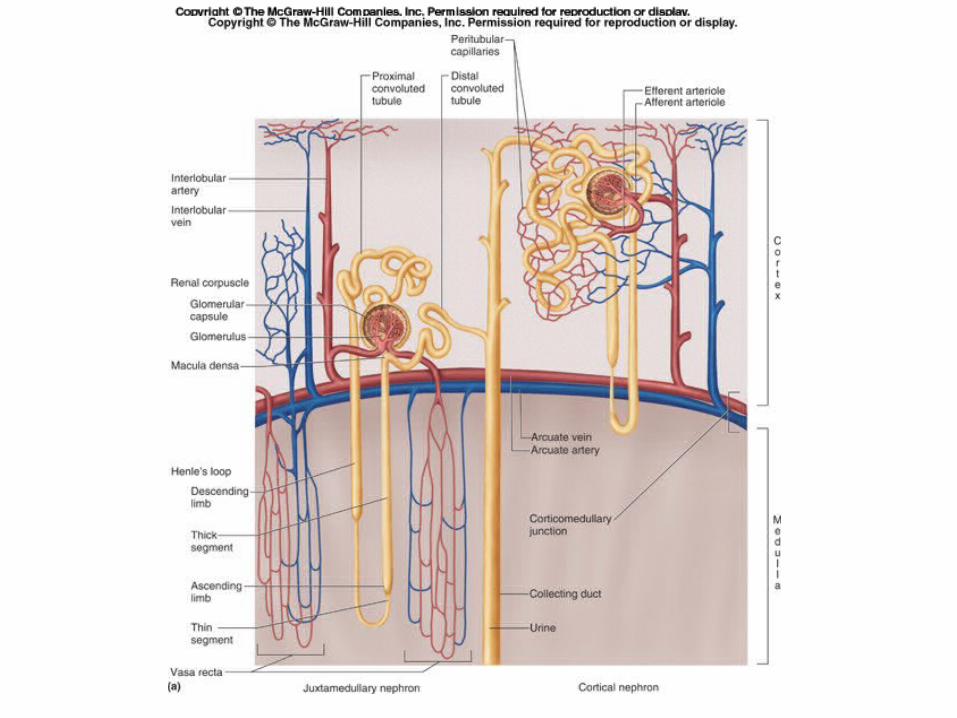
• Sodium is freely filtered at the glomerulus– About 65% is reabsorbed in the proximal tubule– Another 25% is reabsorbed in the loop of Henle– Most of the remaining 10% is reabsorbed in the
distal convoluted tubule and collecting duct.– Less than 1% winds up in the urine
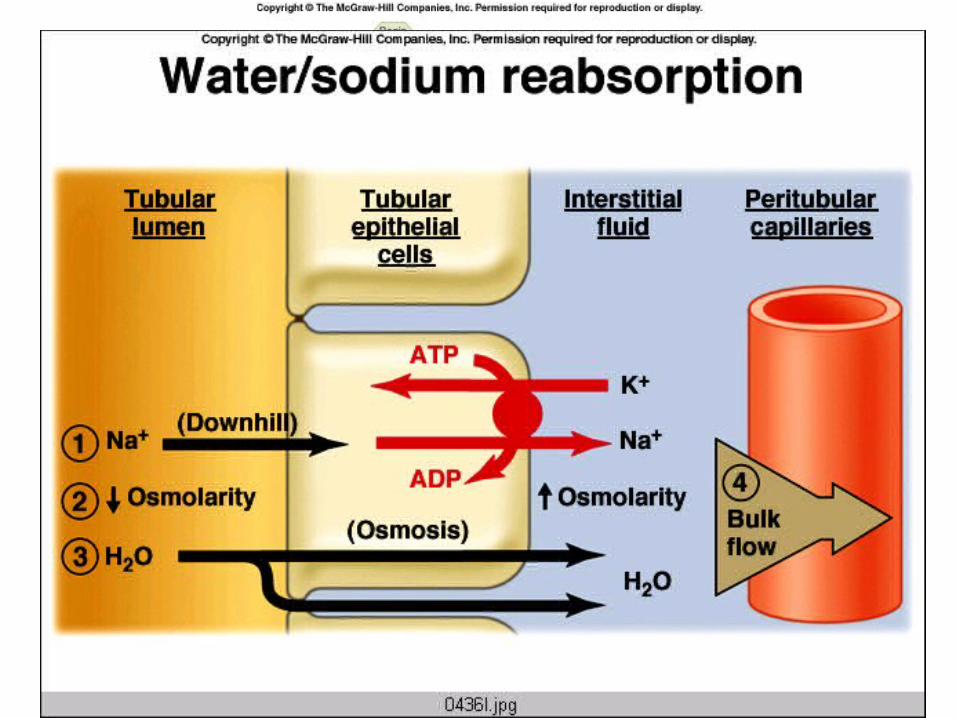
• The reabsorption of water follows the reabsorption of sodium, down the osmotic gradient.
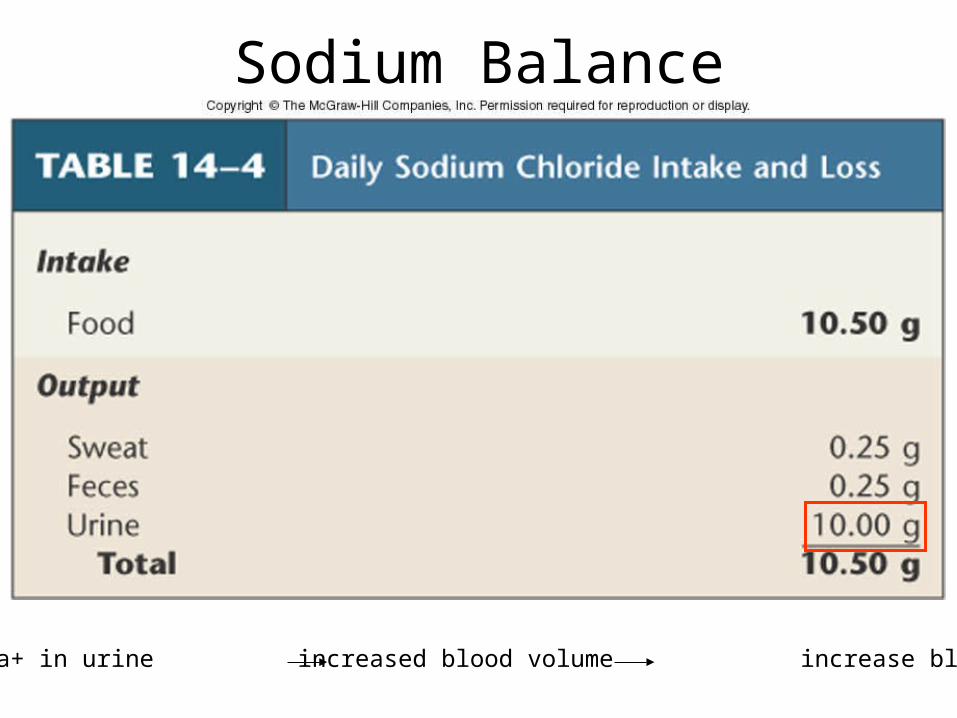
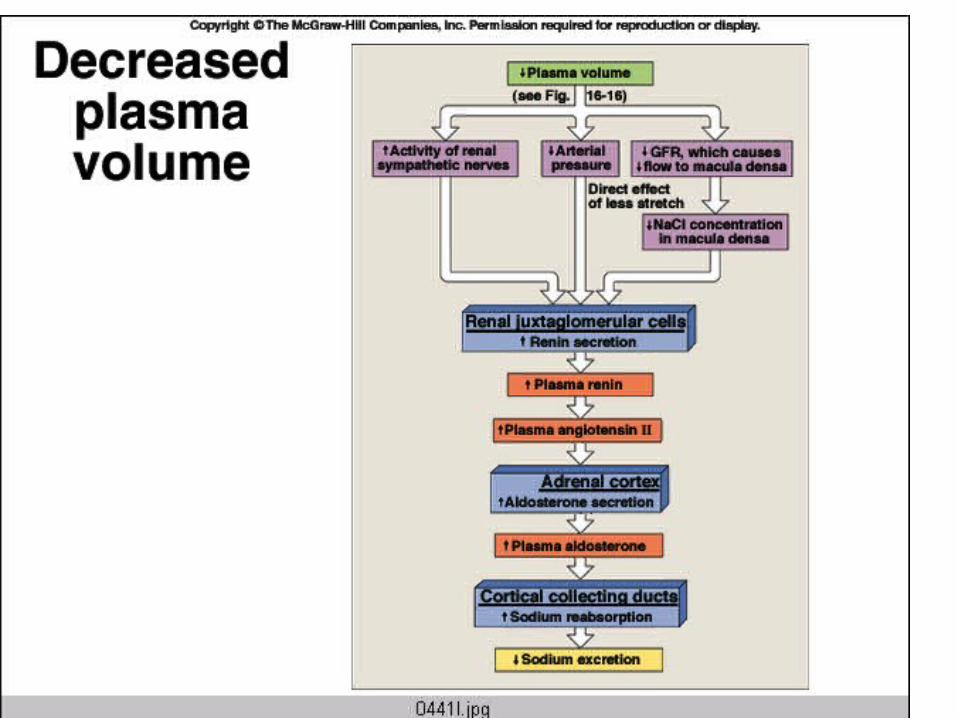
Decrease Na+ in urine increased blood volume increase blood pressure
Sodium Balance
Regulation of Sodium Excretion
• Most important sensors are ones that detect blood pressure, both inside (the juxtaglomerular apparatus) and outside (the arterial baroreceptors) the kidney.
• The controlled variable is the amount of sodium excreted in the urine.
Regulation of Sodium Excretion
• Two Hormone Systems Involved:
– Renin/Angiotensin/Aldosterone
– Atrial Natriuretic Peptide (ANP)
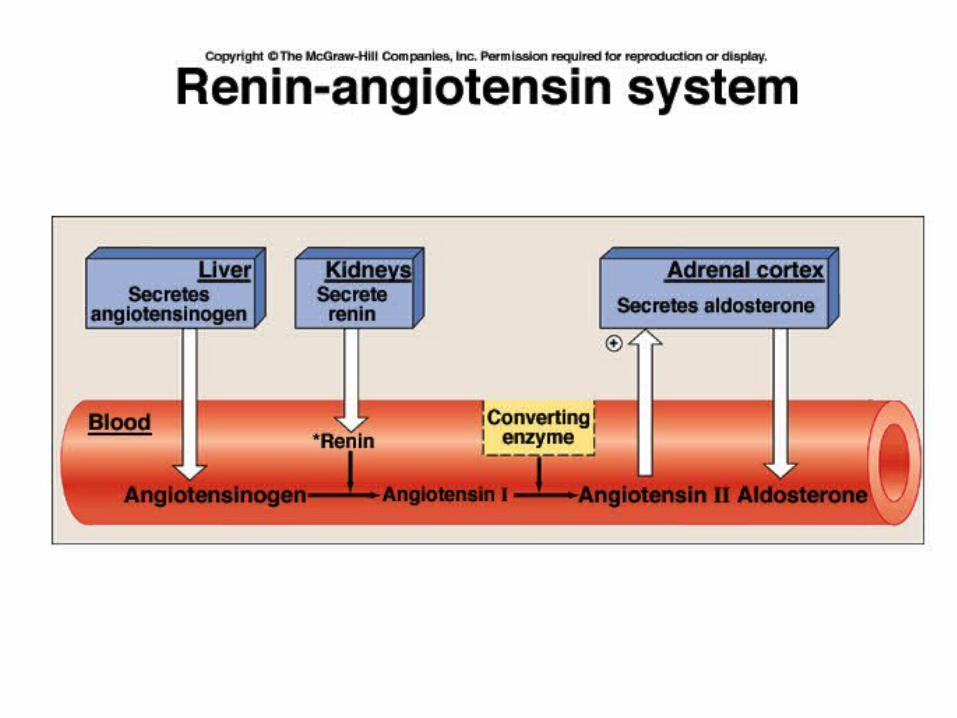
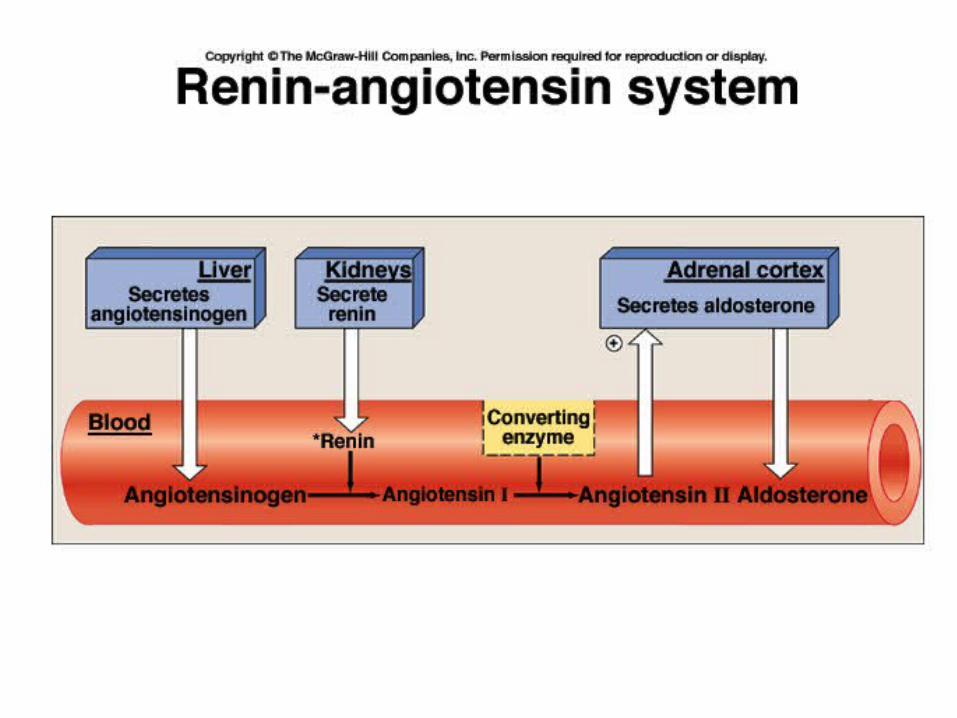
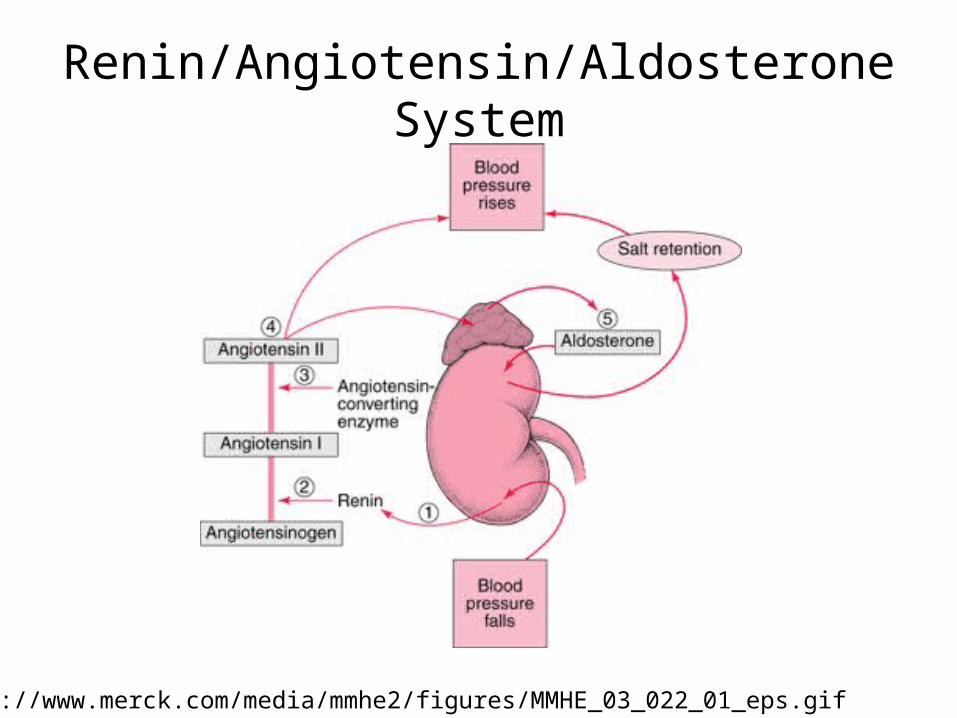
Renin• Made by juxtaglomerular cells
• An enzyme that splits angiotensinogen to form angiotensin I. Angiotensin I (AI) is then converted to angiotensin II (AII) in the lungs via angiotensin converting enzyme (ACE)
• Stimuli for release include sympathetic nerve activity, decreased intrarenal BP, decreased delivery of Na+ and Cl- to macula densa
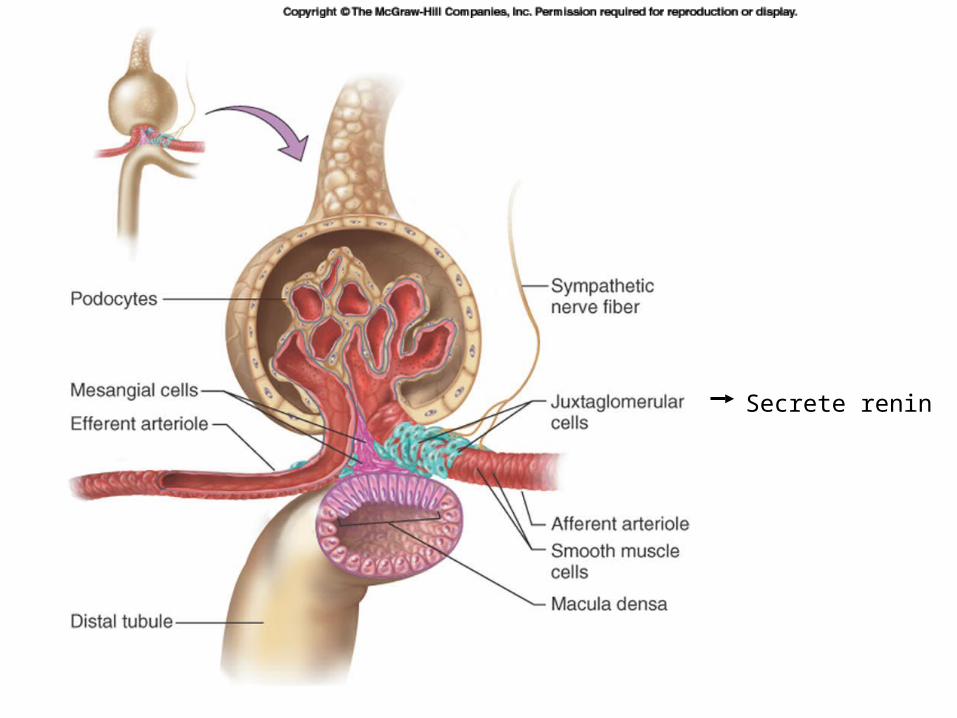
Secrete renin
Actions of Angiotensin II
• Release of Aldosterone
• Vasoconstriction
• Release of ADH (antidiuretic hormone)
• Stimulation of Thirst
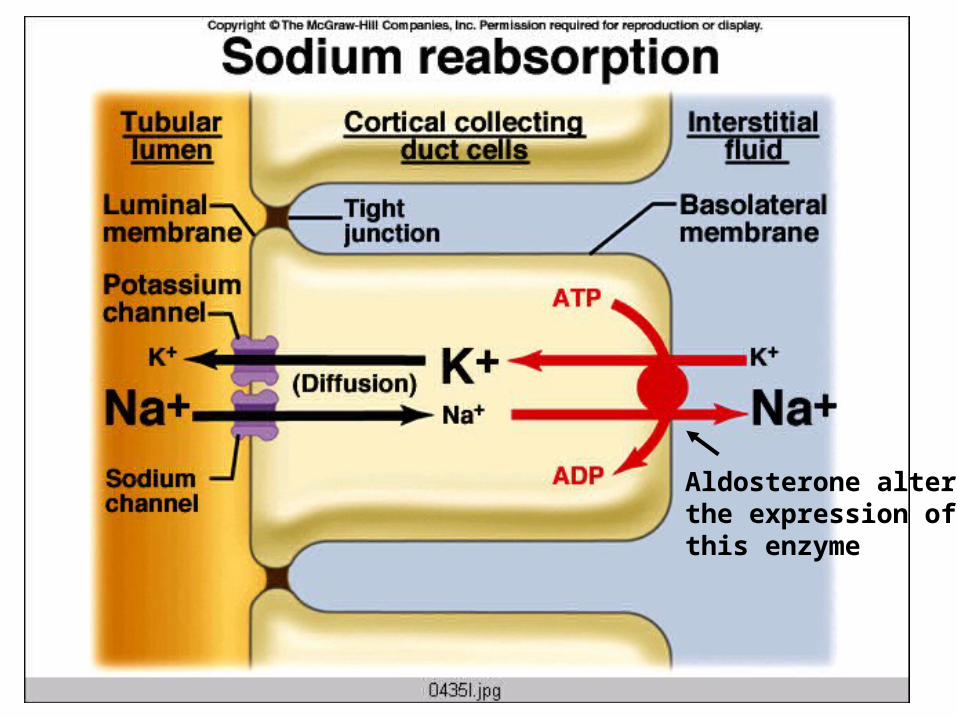
Aldosterone• Steroid hormone made by adrenal cortex.
• Controls activity and/or number of Na+/K+/ATPase pumps in distal tubules and collecting ducts.
• Increased aldosterone leads to increased reabsorption of Na+ and water (assuming distal tubules and collecting ducts are permeable to water, which is under the control of ADH).
• Release triggered by angiotensin II, and by high extracellular K+ (more on this later).
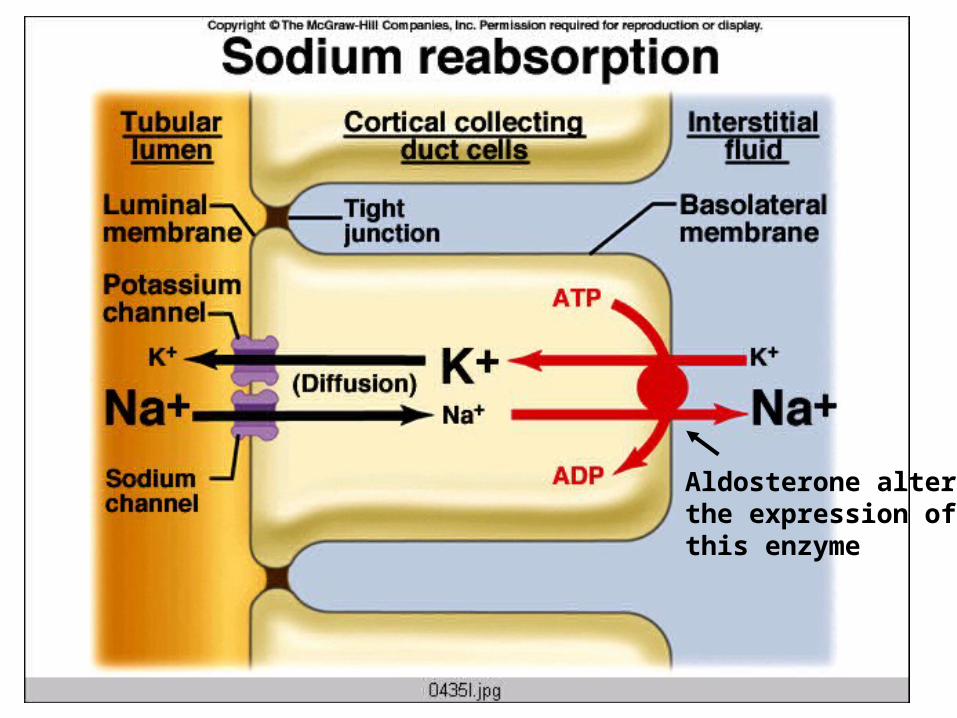
Aldosterone altersthe expression of this enzyme
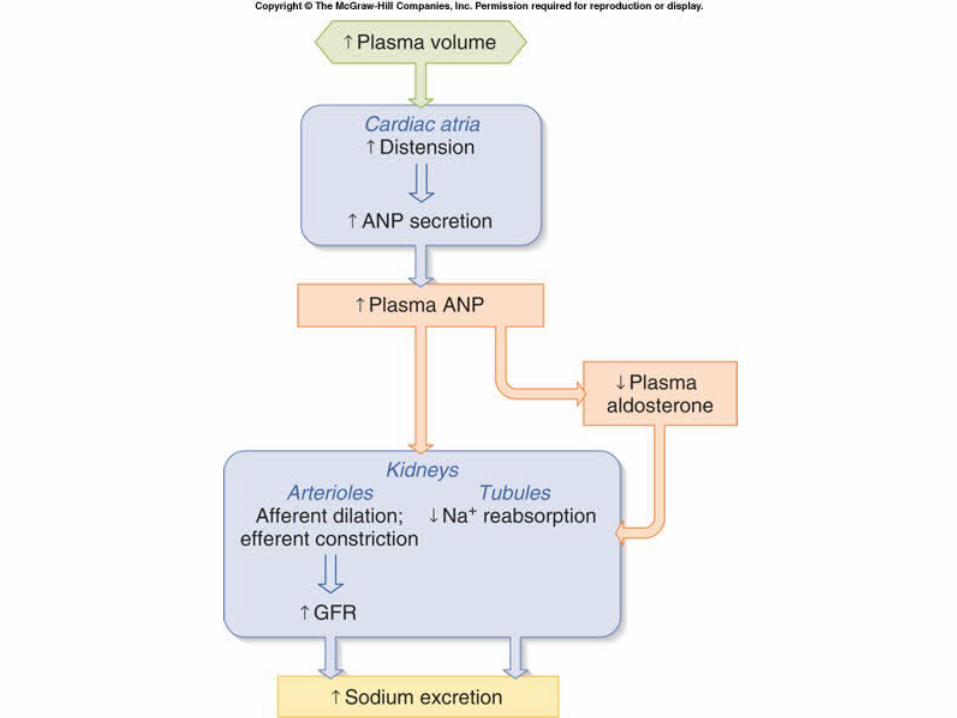
Atrial Natriuretic Peptide
• Made by atria of the heart
• Release triggered by increased stretch of atria (indicating increased blood volume)
• Actions include:– Dilates glomerular afferent arterioles,
increasing GFR.– This increases the amount of sodium filtered,
thereby increasing sodium excretion– Inhibits Na+ reabsorption in collecting ducts
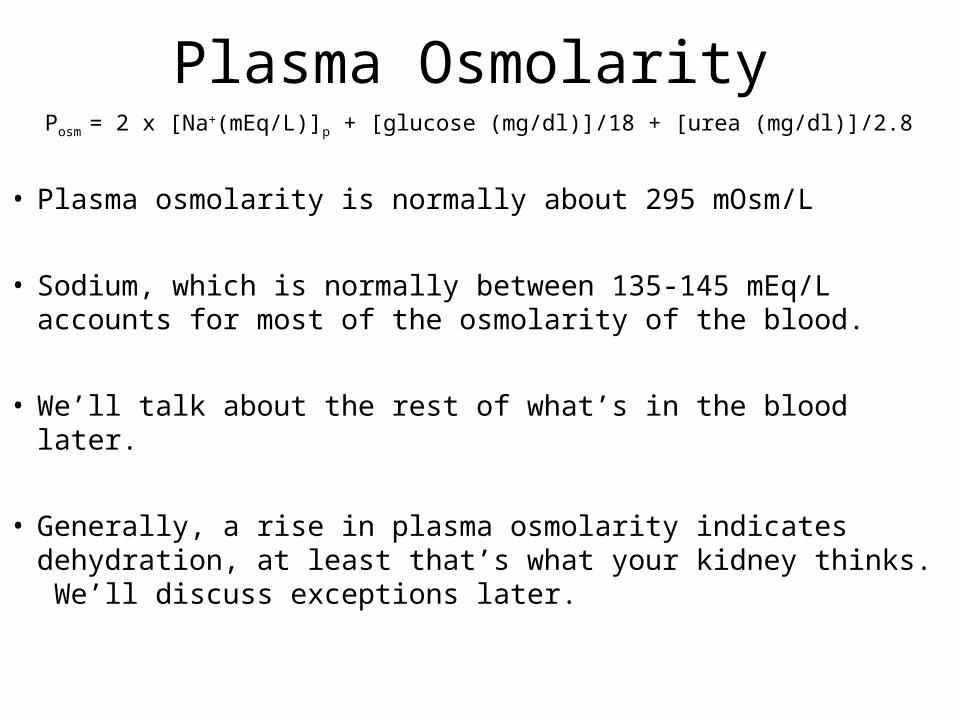
Plasma OsmolarityPosm = 2 x [Na+(mEq/L)]p + [glucose (mg/dl)]/18 + [urea (mg/dl)]/2.8
• Plasma osmolarity is normally about 295 mOsm/L
• Sodium, which is normally between 135-145 mEq/L accounts for most of the osmolarity of the blood.
• We’ll talk about the rest of what’s in the blood later.
• Generally, a rise in plasma osmolarity indicates dehydration, at least that’s what your kidney thinks. We’ll discuss exceptions later.
Regulation of Osmolarity
• Osmolarity is sensed by osmoreceptors in hypothalamus
• Controlled variables: – Urine volume and osmolarity– Thirst and fluid consumption
Urine Volume and Osmolarity is Largely Regulated by ADH
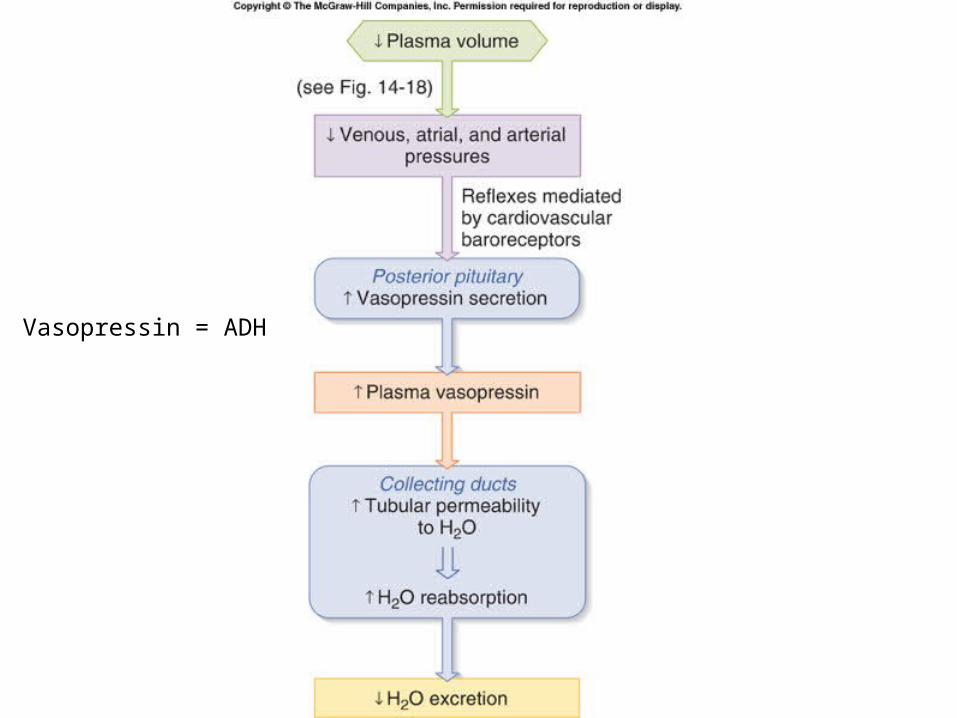
• ADH = Antidiuretic Hormone = Vasopressin
• Actions of ADH:– Increases reabsorption of water in the distal
tubules and collecting ducts.– Contraction of arteriolar smooth muscle
throughout the body, increasing TPR
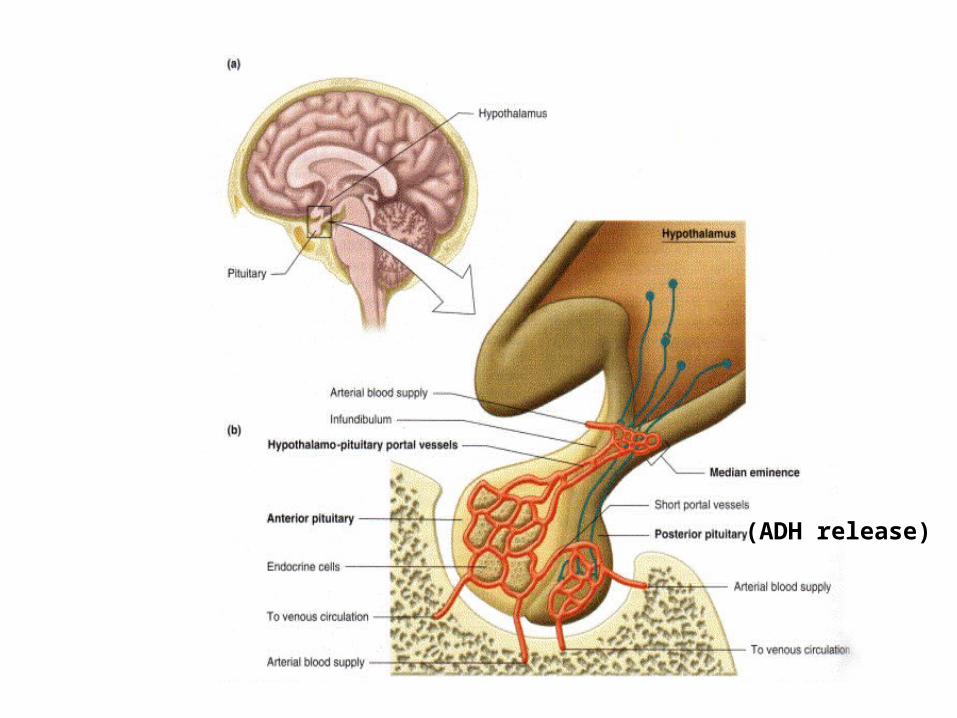
(ADH release)
Mechanism of ADH Action• Distal tubules and collecting ducts are normally
nearly impermeable to water.• In presence of ADH, they become permeable,
allowing water to move out of the tubule, down its osmotic gradient.
• Depending of levels of ADH, the osmolarity of urine can be very high (around 1400 mOsm) or low (100 mOsm).
• Likewise the volume of the urine can be high or low.
Stimuli for ADH Release
• An increase in plasma osmolarity (as little as a 2% change)
• A decrease in blood volume (need about 10% change to trigger release). Sensed by atrial volume receptors and arterial baroreceptors
• Angiotensin II• Certain drugs (nicotine, narcotics) • Inhibited by alcohol
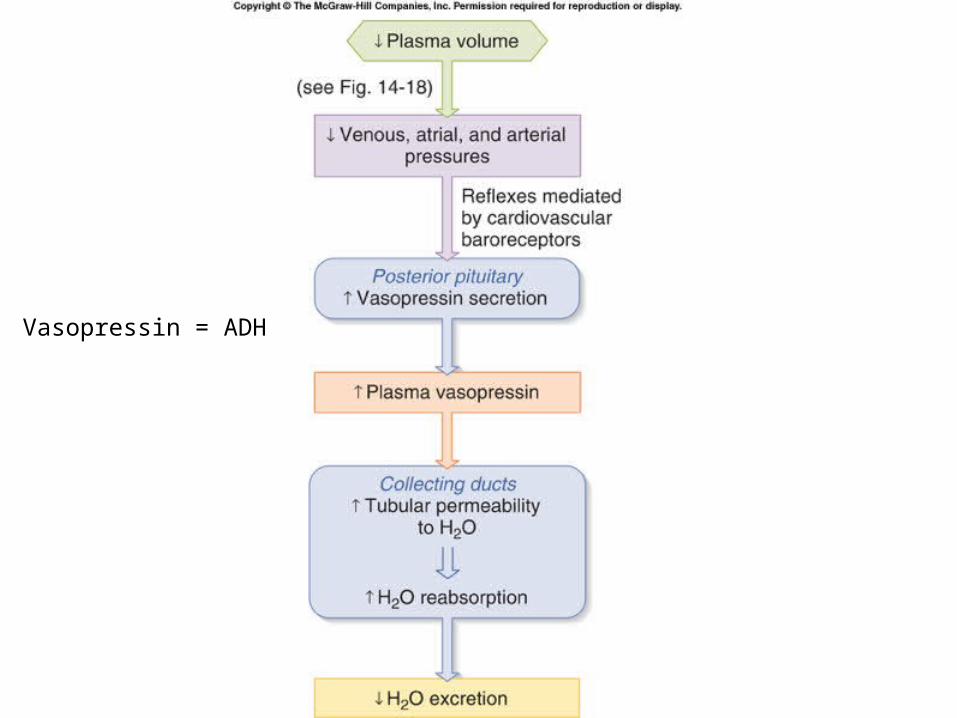
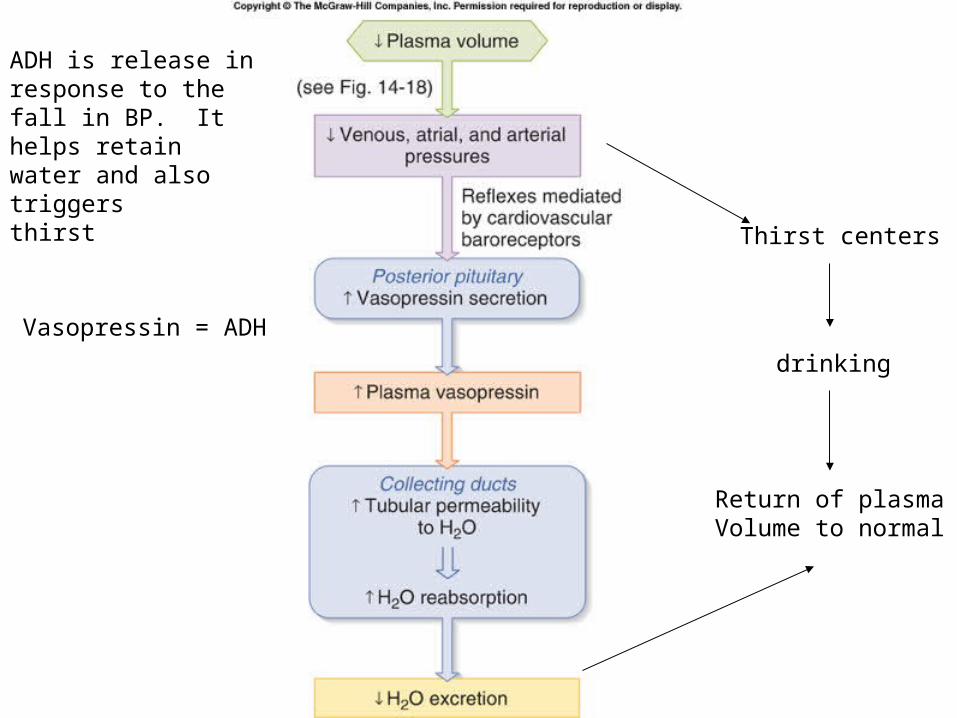
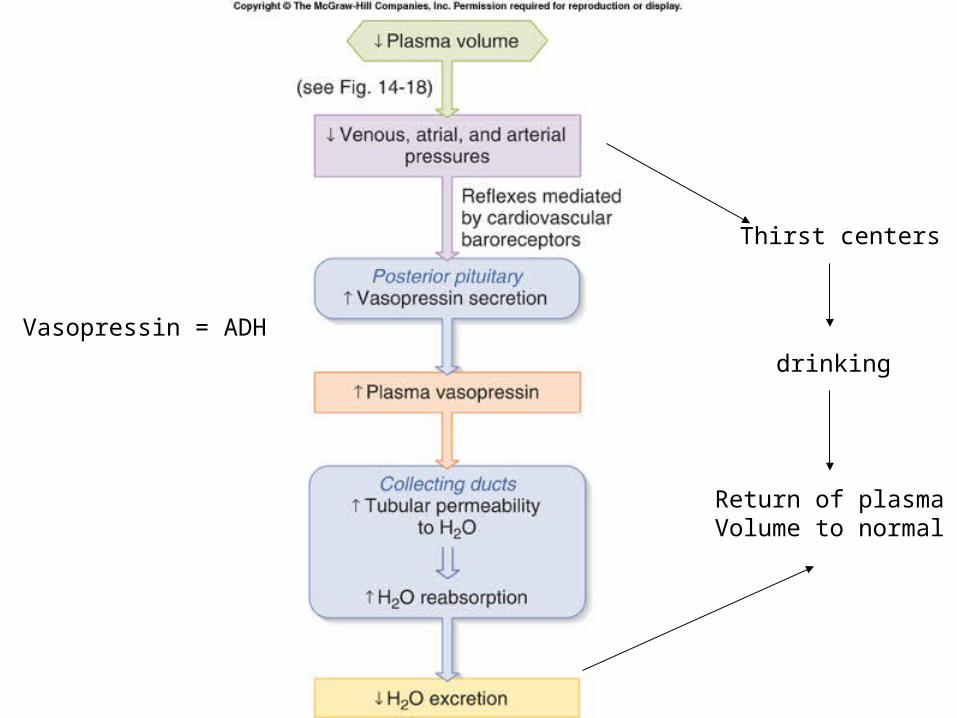
Vasopressin = ADH
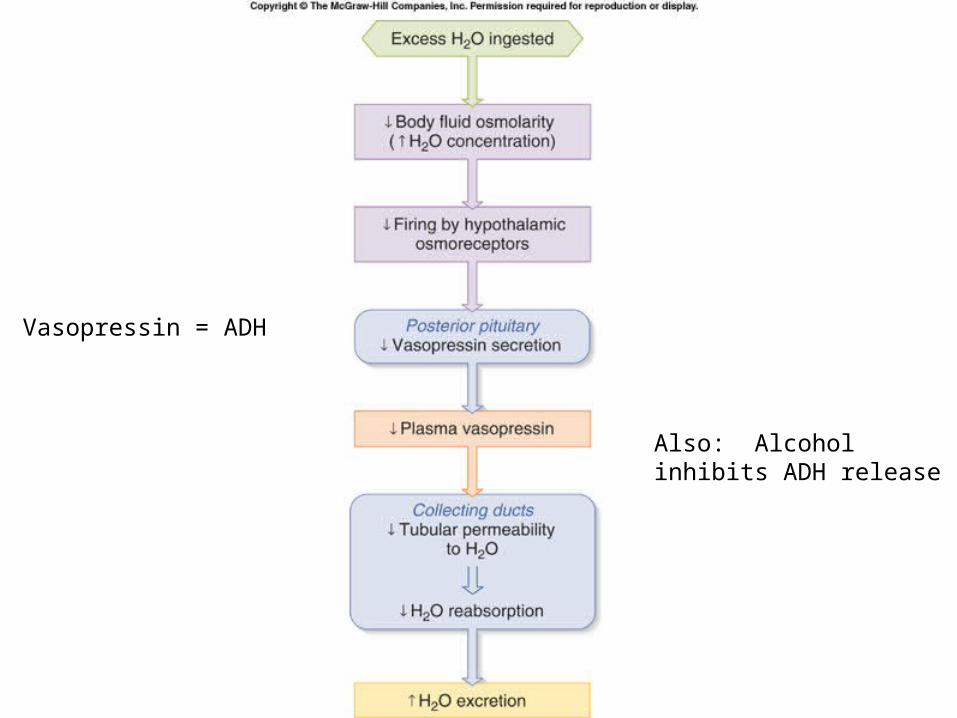
Vasopressin = ADH
Also: Alcohol inhibits ADH release
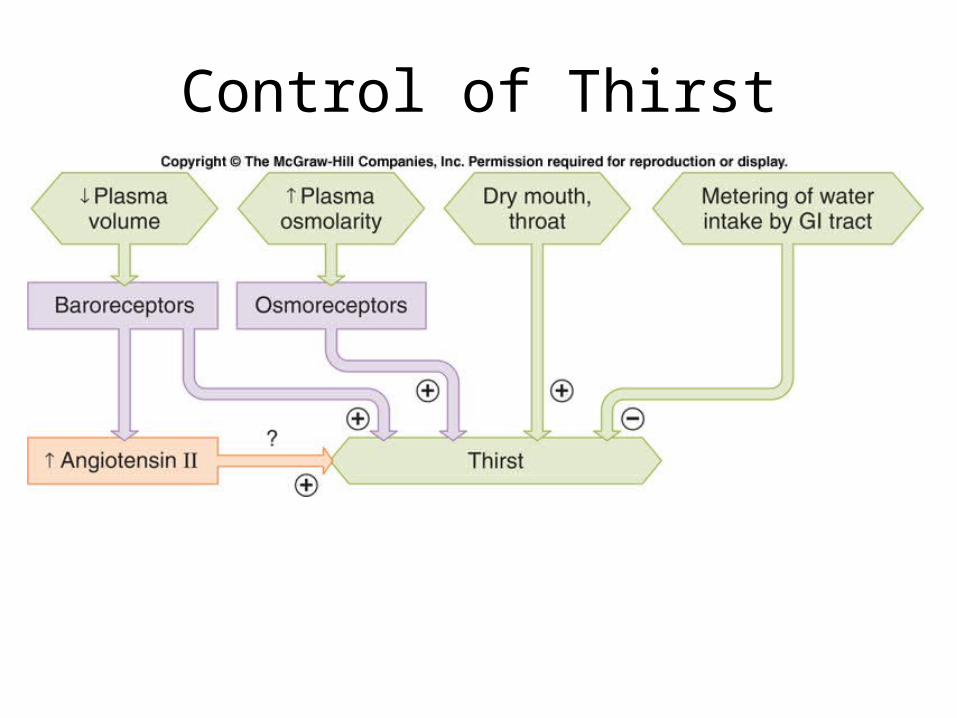
Control of Thirst
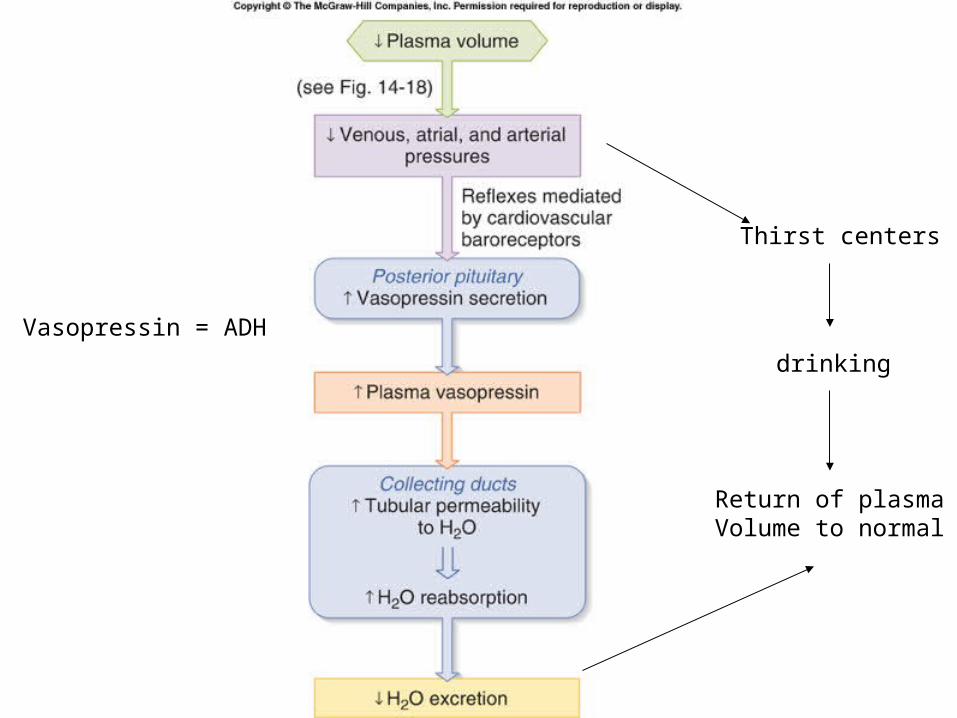
Vasopressin = ADH
Thirst centers
drinking
Return of plasmaVolume to normal
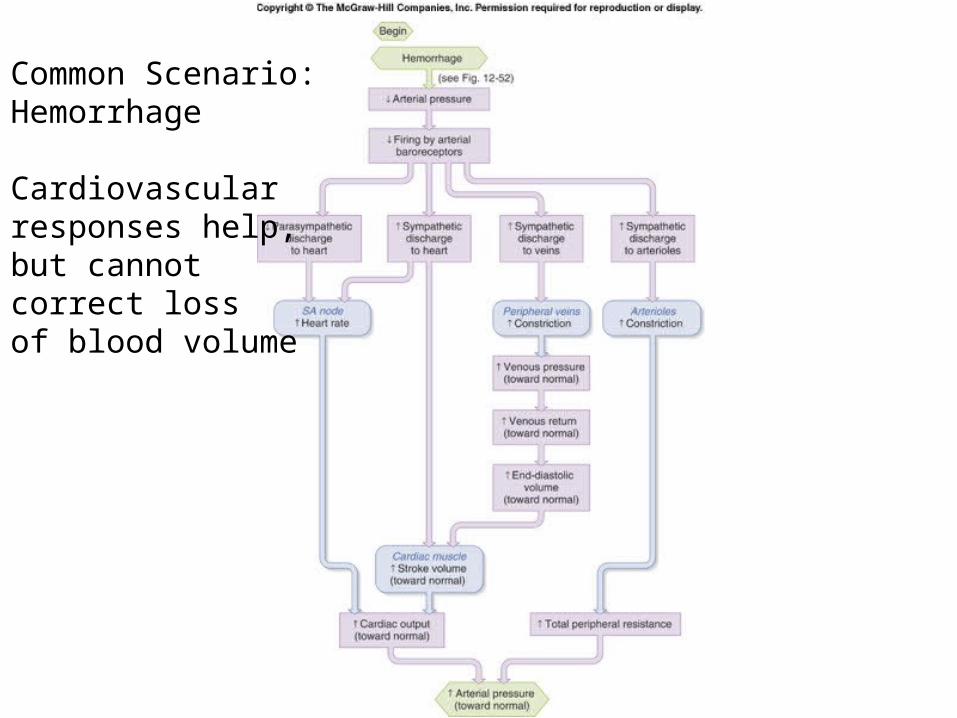
Common Scenario:Hemorrhage
Cardiovascularresponses help, but cannot correct lossof blood volume
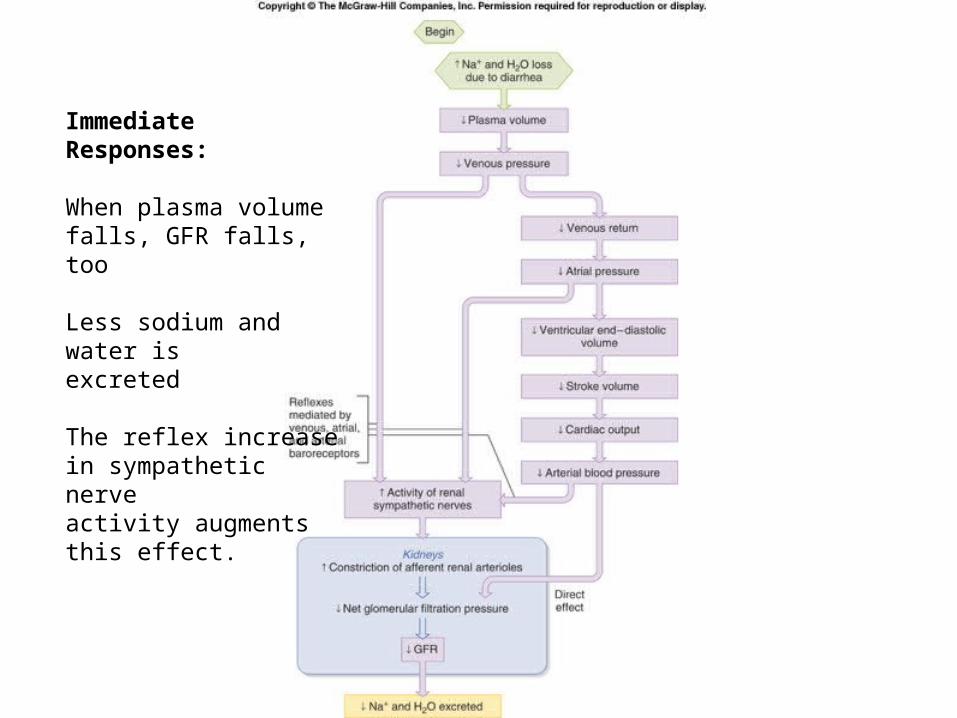
Immediate Responses:
When plasma volumefalls, GFR falls, too
Less sodium and water is excreted
The reflex increasein sympathetic nerve activity augmentsthis effect.
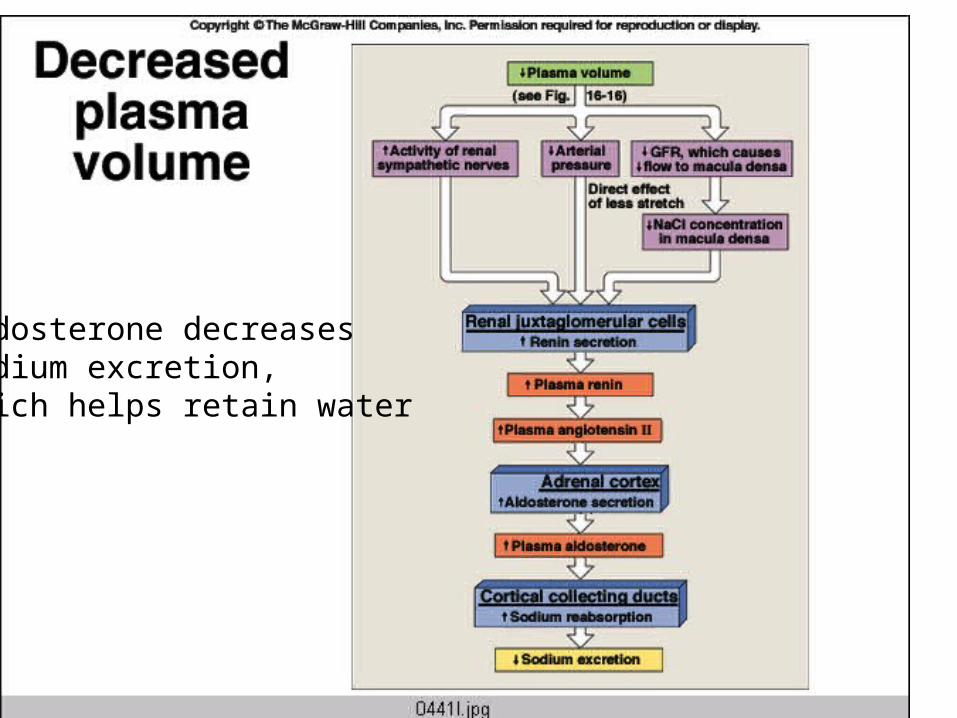
Aldosterone decreasessodium excretion,which helps retain water
Vasopressin = ADH
Thirst centers
drinking
Return of plasmaVolume to normal
ADH is release inresponse to the fall in BP. It helps retainwater and also triggers thirst
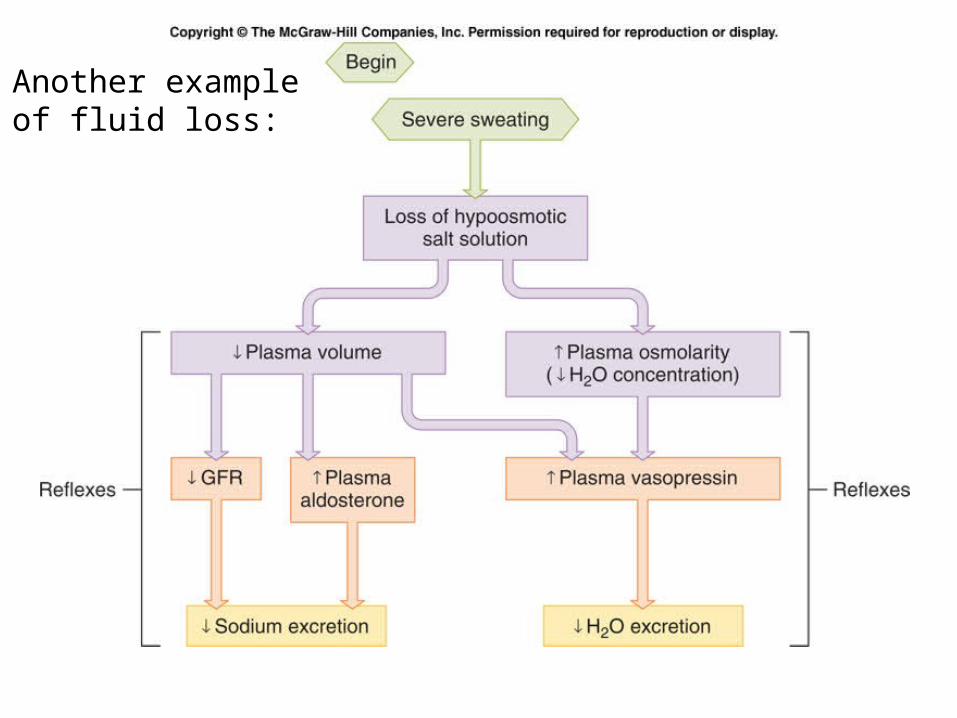
Another exampleof fluid loss:
When can this response go wrong?
• If there is no true fall in blood pressure, just a decrease in blood flow to the kidney. This could occur if there is atherosclerosis of the renal artery, or an anatomic malformation of this blood vessel.
• If there is heart failure, blood pressure is low due to failing heart, not blood loss.
Heart Failure
• Basic problem is a decrease in blood pressure due to insufficient cardiac output.
• Kidneys respond as those there has been a hemorrhage – by increasing:– Sympathetic nerve activity– Renin release– ADH release
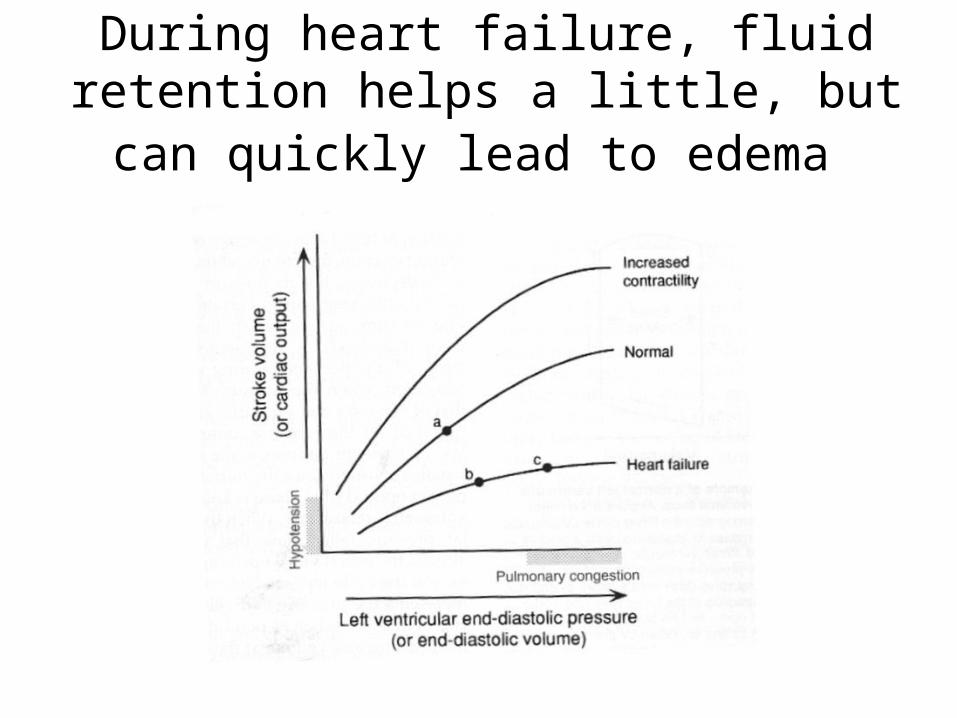
• This response can be maladaptive, as excessive amounts of retained fluid cause peripheral and pulmonary edema.
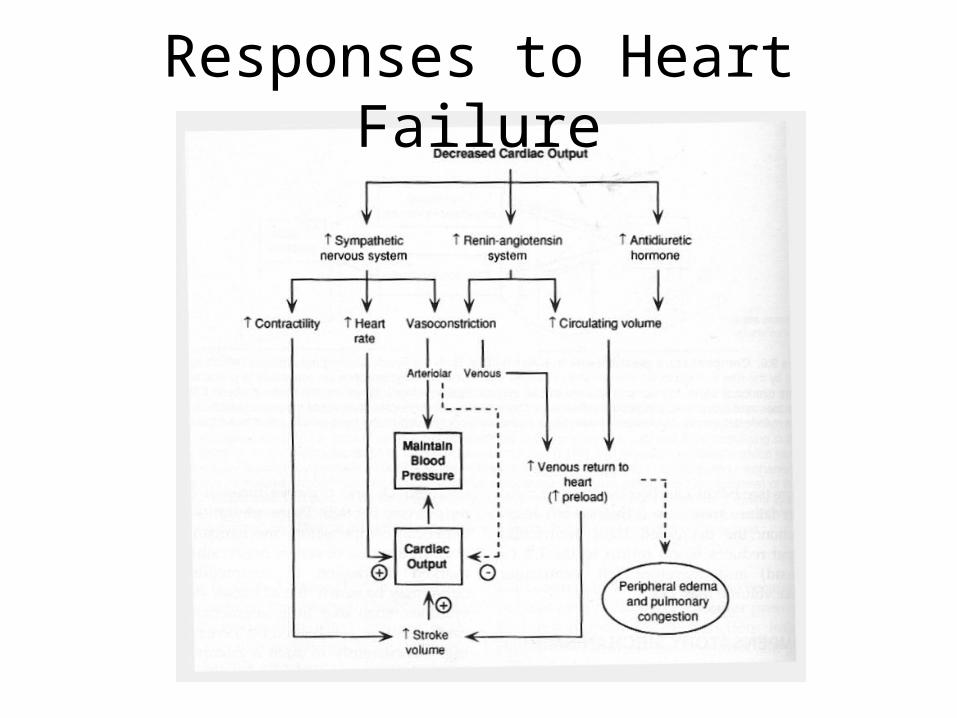
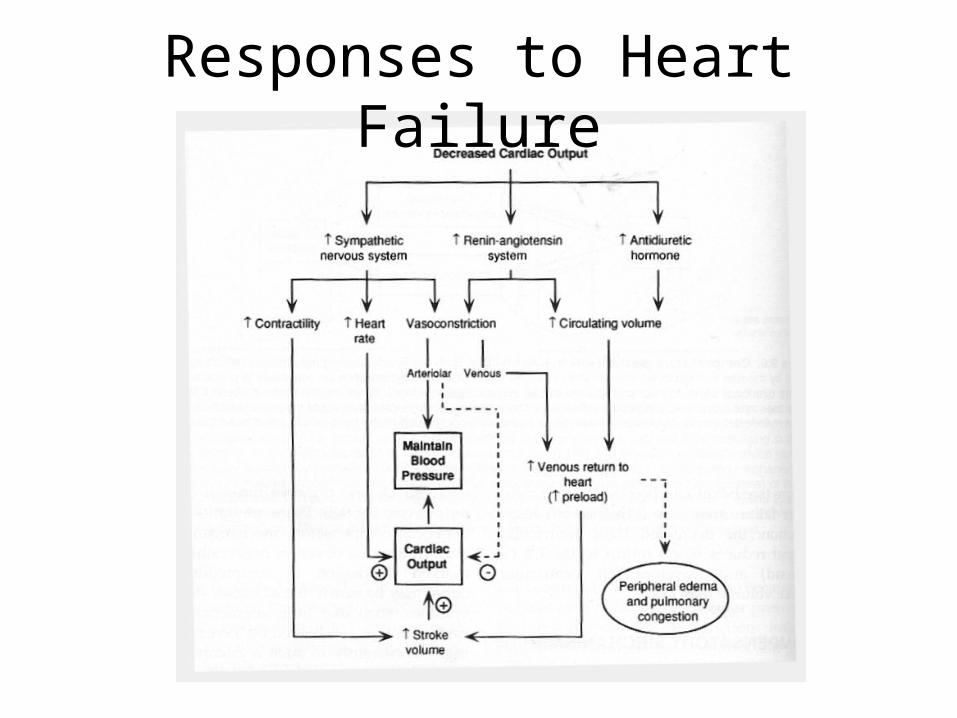
Responses to Heart Failure
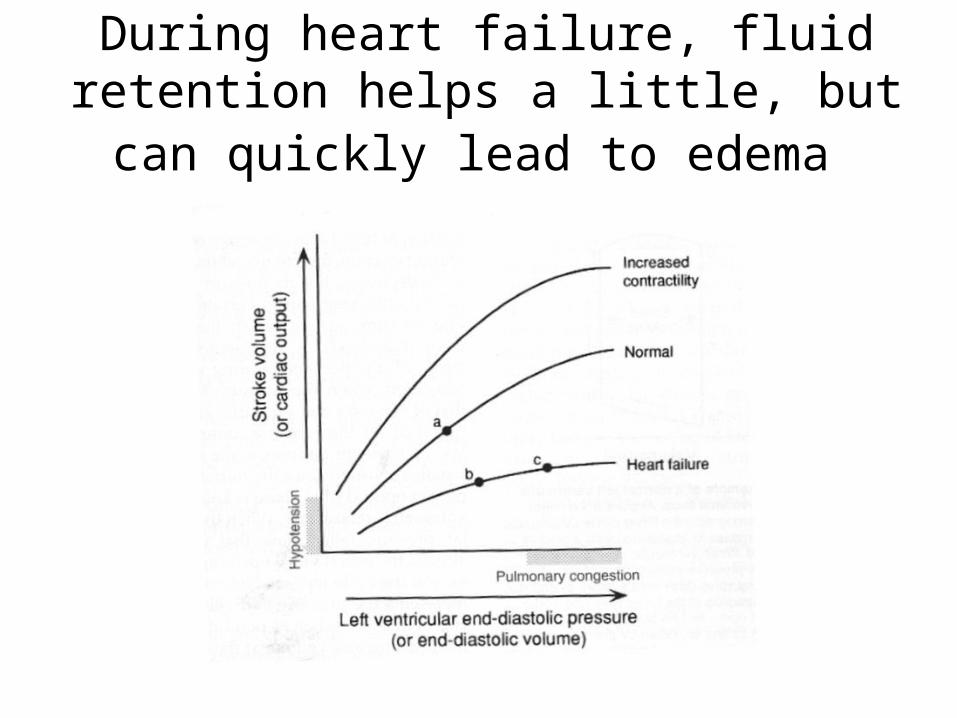
During heart failure, fluid retention helps a little, but can quickly lead to edema
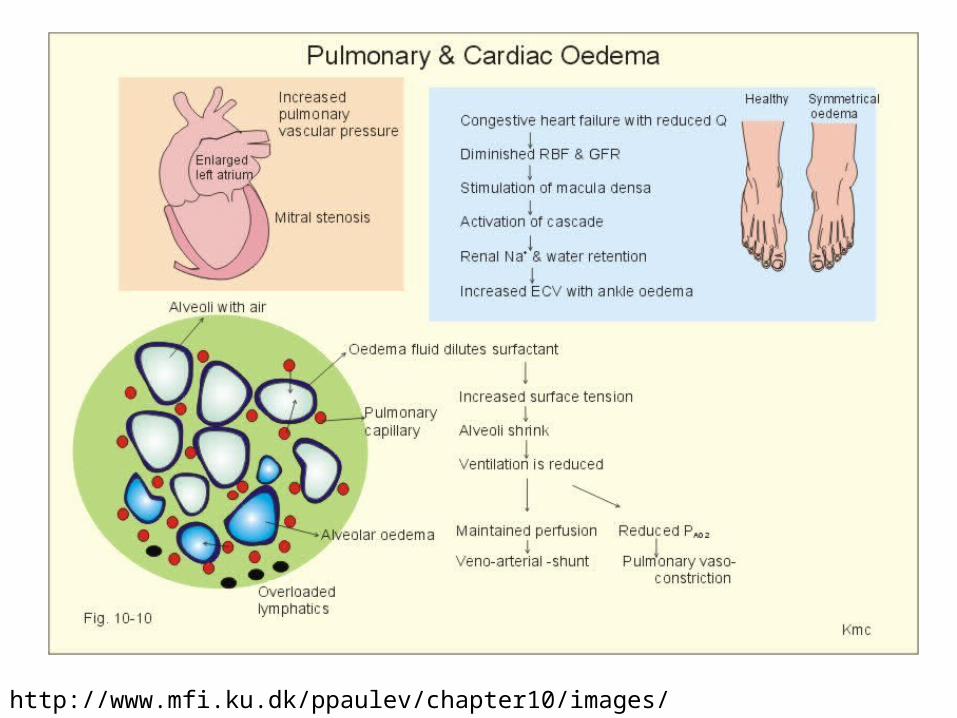
http://www.mfi.ku.dk/ppaulev/chapter10/images/10-10.jpg
Extra slides – Add as needed
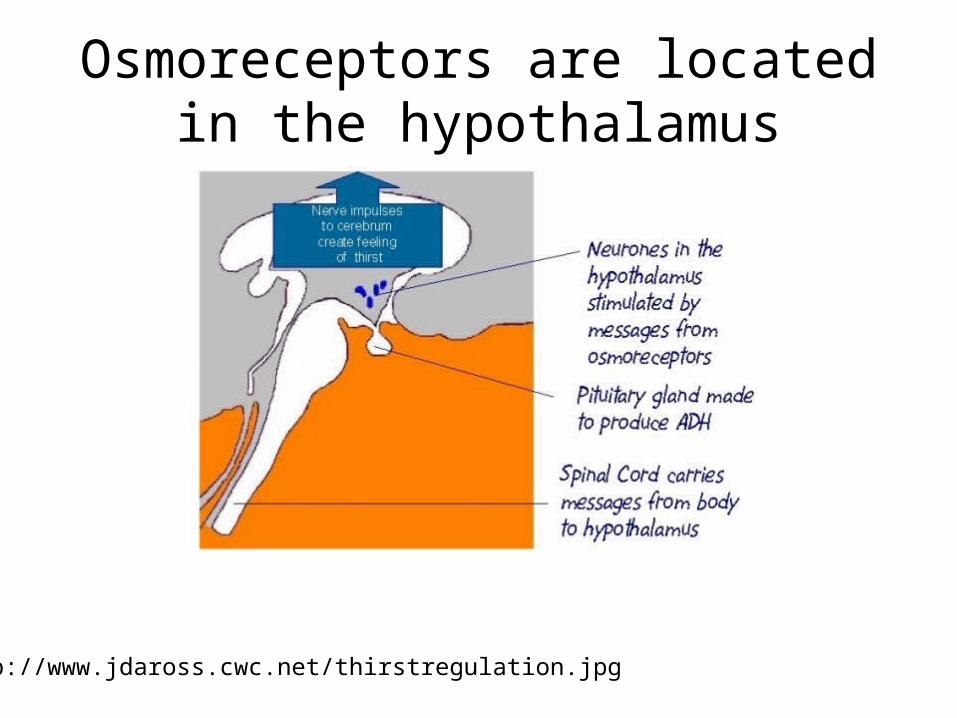
Osmoreceptors are located in the hypothalamus
http://www.jdaross.cwc.net/thirstregulation.jpg
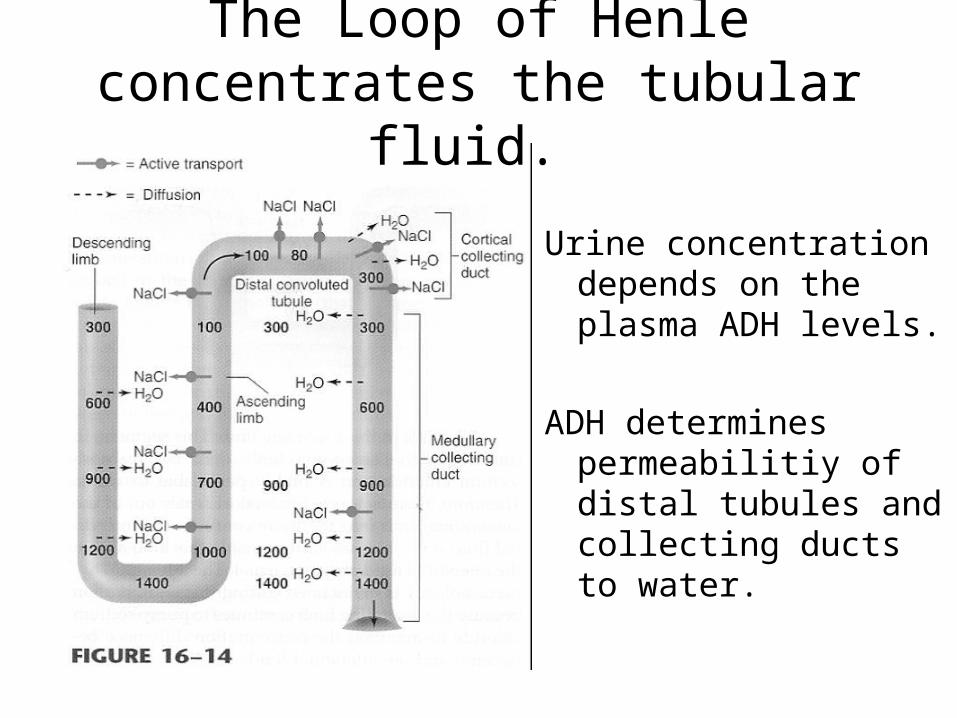
The Loop of Henle concentrates the tubular fluid.
Urine concentration depends on the plasma ADH levels.
ADH determines permeabilitiy of distal tubules and collecting ducts to water.
Stimuli for ADH release
• Increased plasma osmolarity
• Decreased plasma volume
• Angiotensin II
• Certain drugs (incl. nicotine, narcotics)
Inhbitors of ADH Release
• A decrease in plasma osmolarity
• An increase in blood volume
• Atrial Natriuretic Peptide (ANP) (also known as atrial natriuretic factor)
• Certain drugs (ethanol)
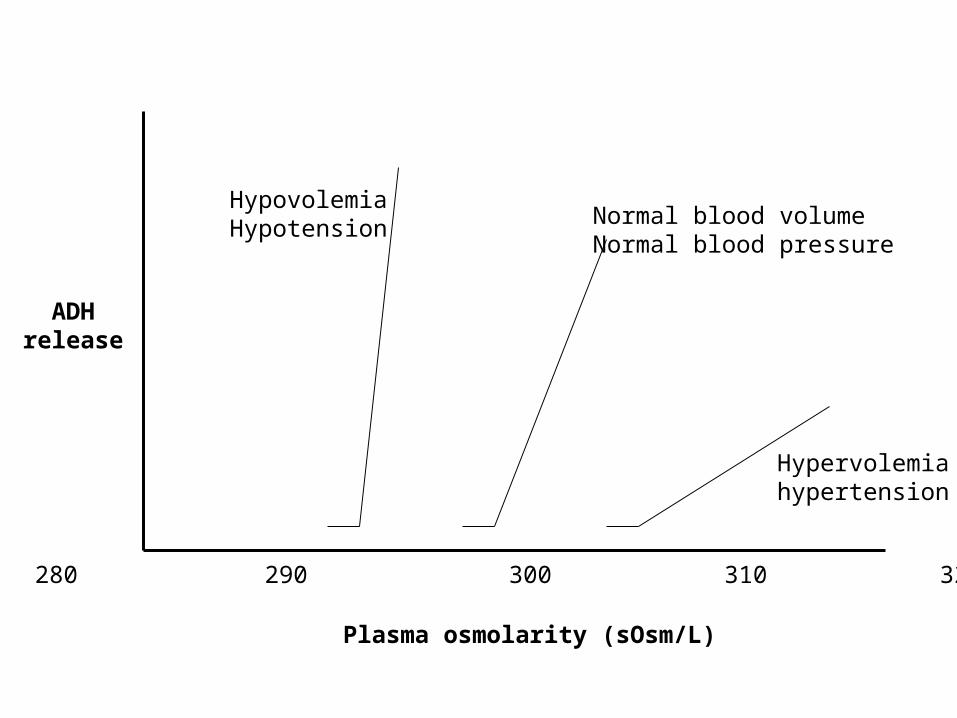
ADHrelease
Plasma osmolarity (sOsm/L)
280 290 300 310 320
Hypervolemiahypertension
HypovolemiaHypotension Normal blood volume
Normal blood pressure
Control of Thirst
• Activity of osmoreceptors (increased osmolarity stimulates thirst)
• Activity of blood volume receptors and baroreceptors (a decrease in blood volume or pressure stimulates thirst)
• Angiotensin II stimulates thirst
Vasopressin = ADH
Thirst centers
drinking
Return of plasmaVolume to normal
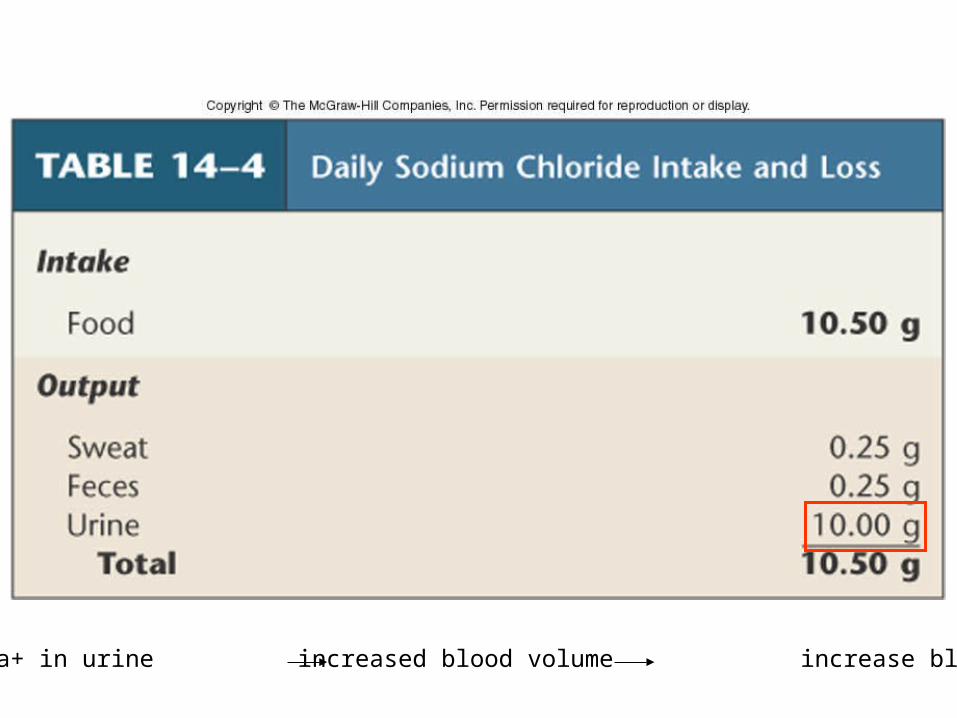
Decrease Na+ in urine increased blood volume increase blood pressure
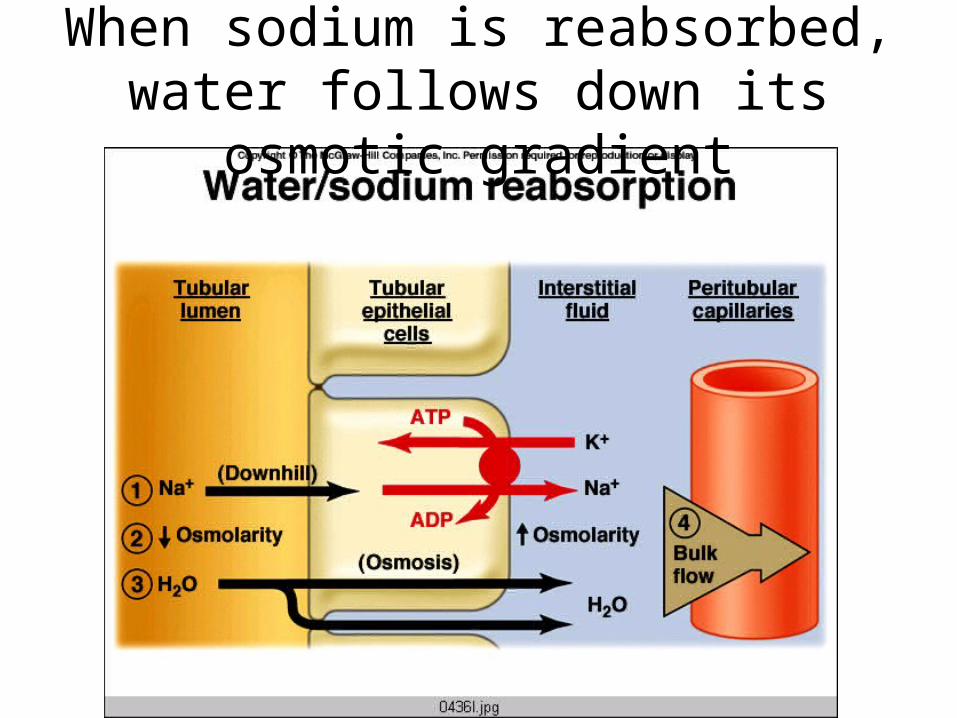
When sodium is reabsorbed, water follows down its osmotic gradient
Sensing of plasma sodium is mostly through indirect signals that reflect blood volume and pressure
• Baroreceptors inside and outside the kidney:– Carotid baroreceptors– Juxtaglomerular apparatus
• Macula Densa – senses delivery and reabsorption of chloride (which generally reflects sodium delivery)
http://www.merck.com/media/mmhe2/figures/MMHE_03_022_01_eps.gif
Renin/Angiotensin/Aldosterone System
Stimuli for Renin Release
• Sympathetic nerve activity
• Decreased firing of intrarenal baroreceptors
• Decreased chloride delivery to macula densa
Actions of Angiotensin II
• Stimulates release of aldosterone
• Potent vasoconstrictor
• Stimulates release of ADH
• Stimulates thirst
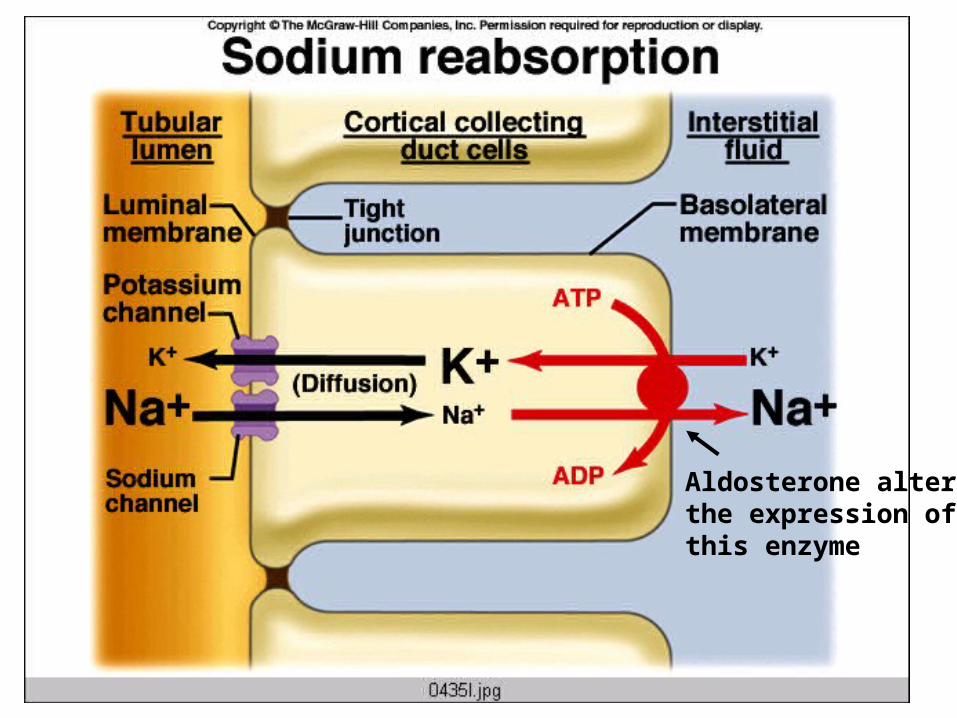
Aldosterone altersthe expression of this enzyme
Atrial Natriuretic Peptide (ANP)
• Made by the atria of the heart, and released in response to an increase in the stretch of the atria
• Actions of ANP– Dilates glomerular afferent arterioles –
increase amount of sodium filtered and thereby excreted
– Inhibits Na+ reabsorption in collecting tubule
Potassium Regulation
• Most (55%) of the filtered potassium is reabsorbed in the proximal tubule, another 30% is absorbed in the loop of Henle.
• Depending on diet, potassium may be reabsorbed or secreted in the distal convoluted tubule and the cortical collecting duct.
Regulation of potassium secretion
• Na+/K+/ATPase A high K+ diet enhances update of K+ into the principal cells (the ones that line the tubule)
• Aldosterone increases K+ uptake into the principal cells (via Na+/K+/ATPase), and makes the luminal membrane more permeable to K+
• K+ secretion is flow dependent – high urine production can lead to K+ deficiency.
Aldosterone altersthe expression of this enzyme
Hypertension and the Kidney
Kidney malfunction is implicated in most cases of hypertension (i.e. the kidney should be able to respond to high BP by increasing salt and water excretion).
Drugs to treat hypertension often target the kidney
• Diuretics act at various points along the renal tubules to increase water loss in the urine– Can lead to potassium depletion– Increases sensitivity to heat stress
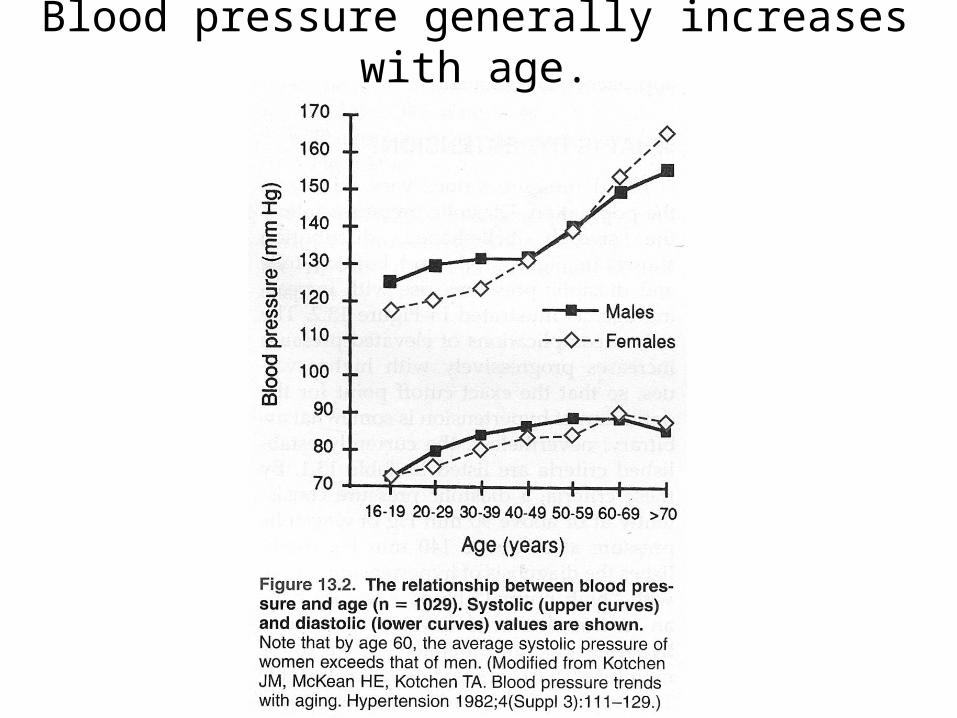
Blood pressure generally increases with age.
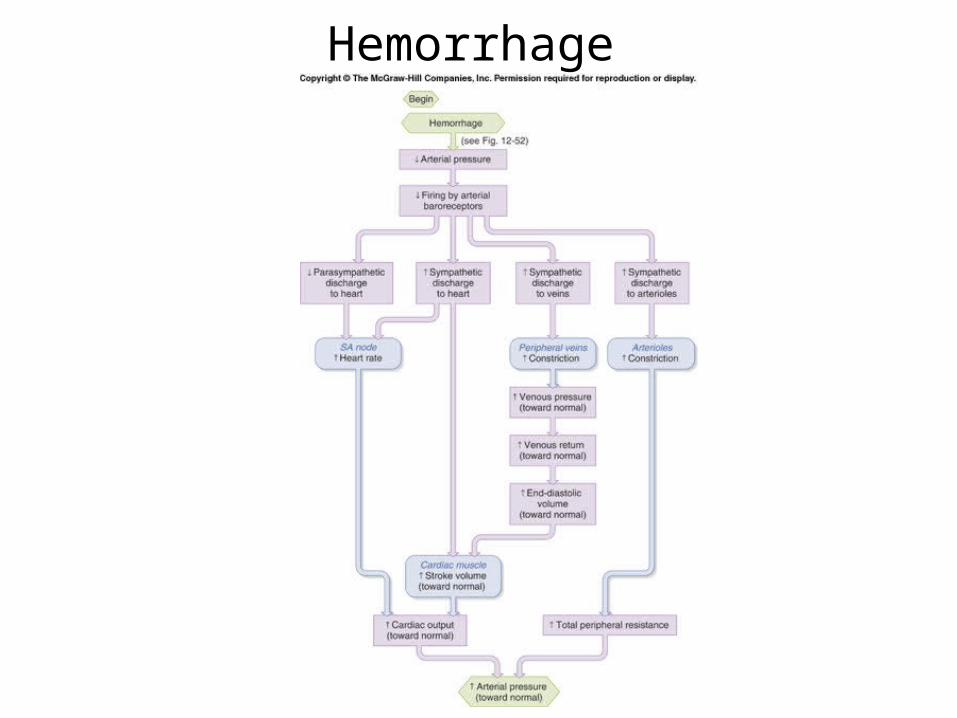
Hemorrhage
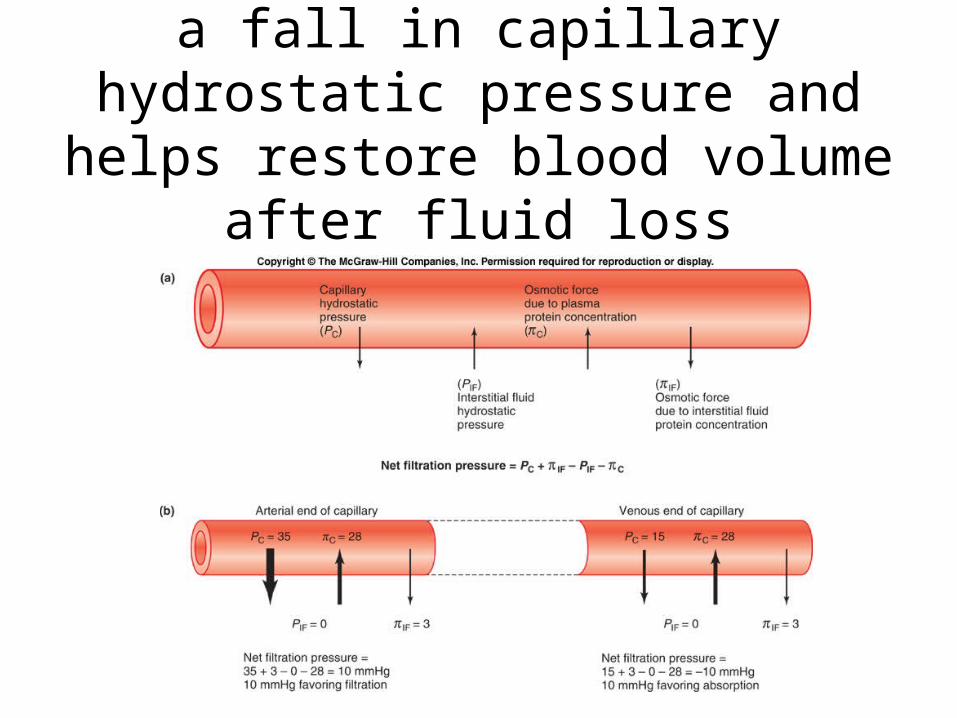
Autotransfusion results from a fall in capillary hydrostatic pressure and helps
restore blood volume after fluid loss
Vasopressin = ADH
Heart Failure
• Basic problem is a decrease in blood pressure due to insufficient cardiac output.
• Kidneys respond as those there has been a hemorrhage – by increasing:– Sympathetic nerve activity– Renin release– ADH release
• This response can be maladaptive, as excessive amounts of retained fluid cause peripheral and pulmonary edema.
Responses to Heart Failure
During heart failure, fluid retention helps a little, but can quickly lead to edema
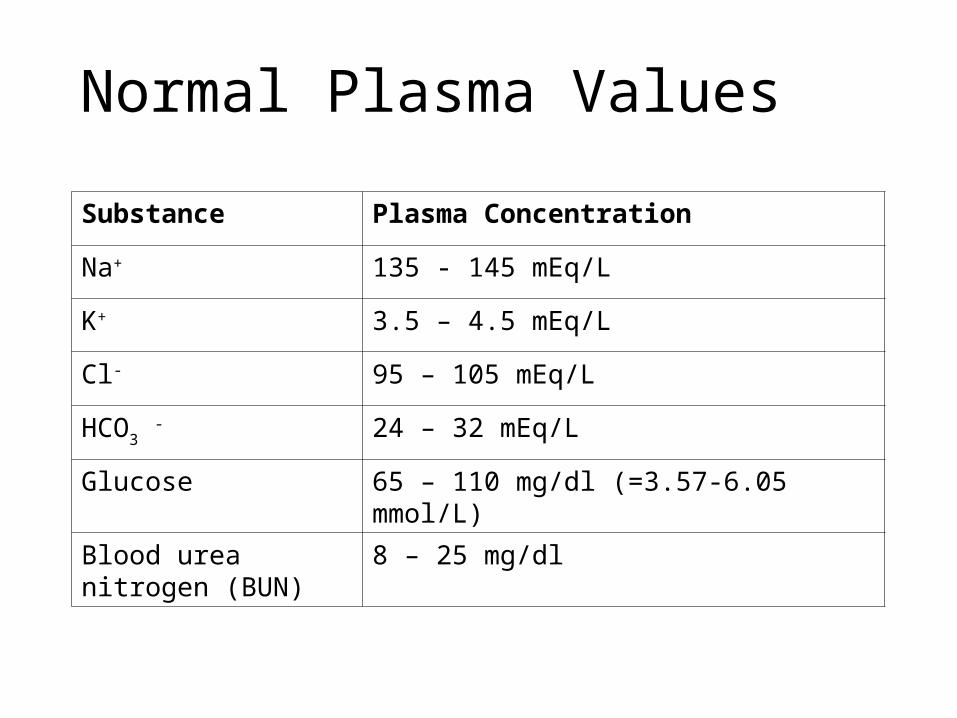
Normal Plasma Values
Substance Plasma Concentration
Na+ 135 - 145 mEq/L
K+ 3.5 – 4.5 mEq/L
Cl- 95 – 105 mEq/L
HCO3 - 24 – 32 mEq/L
Glucose 65 – 110 mg/dl (=3.57-6.05 mmol/L)
Blood urea nitrogen (BUN)
8 – 25 mg/dl
Sodium regulation
• Controlled variable: Sodium excretion in urine
• Hormonal systems involved:– Renin/Angiotensin/Aldosterone– Atrial Natriuretic Peptide

Sensing of plasma sodium is mostly through indirect signals that reflect blood volume and pressure
• Baroreceptors inside and outside the kidney:– Carotid baroreceptors– Juxtaglomerular apparatus
• Macula Densa – senses delivery and reabsorption of chloride (which generally reflects sodium delivery)





























