Embed Size (px)
Citation preview

1
1
An Introduction to the Toxicology of the Kidney.
Rhian B. Cope BVSc BSc(Hon 1) PhD DABT ERT
2
Content Outline of the Two Lectures.
1. Section 1: A Revision of the Basic Anatomy, Physiology and Pathophysiology of the Kidney, Reasons for the Susceptibility of the Kidney to Toxic Injury and Reactions of the Kidney to Toxic Injury.
2. Section 2: Clinical Signs of Kidney Disease, Assessment of Renal Function and the Pathophysiology and Effects of Classical “Must Know” Renal Toxins/Toxicants.
3
Lecture 1. A Revision of the Basic Anatomy, Physiology and
Pathophysiology of the Kidney, Reasons for the Susceptibility of the Kidney to Toxic Injury and
Reactions of the Kidney to Toxic Injury.

2
4
Learning Tasks. • Learning task 1: Understand the key physiological
functions of the kidneys and the potential consequences of malfunction.
• Learning task 2: Understand the basic anatomy and physiology of the nephron and how this relates to toxic damage.
• Learning task 3: Understand the factors that make the kidneys prone to toxic damage.
• Learning task 4: Understand the kidney’s responses to toxic injury and its compensatory mechanisms.
5
Learning Task 1: Understand the key physiological functions of the kidneys and the potential
consequences of malfunction. .
6
Key Physiological Functions of the Kidney • Filtration and active secretion of body wastes, particularly ammonia,
urea, and other nitrogenous compounds. • Water conservation. • Active re-absorption of essential and useful materials filtered by the
kidney, notably glucose, amino acids and small proteins. • Regulation of body ion levels, notably: sodium, chloride, potassium,
calcium, phosphorus, magnesium. • Regulation of total body water and blood volumes and long-term
blood pressure. • Regulation of TBW and blood osmalality. • Regulation of acid/base status. • Conversion of 25-hydroxy Vitamin D to 1, 25-dihydroxy Vitamin D
(most biologically active form) by renal 1-∞-hydroxylase. • Production of erythropoeitin (stimulated by hypoxia) • Regulation of the availability of mevalonic acid, a necessary
precursor for hepatic cholesterol synthesis • Removal of insulin from the circulation.

3
7
Potential Consequences of Abnormal Kidney Function.
• _____________________________________________ • _____________________________________________ • _____________________________________________ • _____________________________________________ • _____________________________________________ • _____________________________________________ • _____________________________________________ • _____________________________________________ • _____________________________________________ • _____________________________________________ • _____________________________________________
8
Key Physiological Features of the Kidney
• ~ 10% of body oxygen consumption occurs in the kidneys. Prone to hypoxia, particularly the PCT and the thick ascending limb of the Loop of Henle.
– Re-absorption of NaCl accounts for most of the energy expenditure by the kidneys
• All renal artery branches are end branches without significant collateral supply
• The kidneys receive ~ 25% of the cardiac output; blood flow per gram of tissue is higher in the kidneys than in any other tissue
• 85% of renal blood flow occurs in the cortex; ~ 14% of blood flow occurs in the outer medulla and ~ 1% of blood flow occurs in the renal papilla
9
Learning Task 2: Understand the basic anatomy and physiology of the nephron and how this relates
to toxic damage.

4
10
The Nephron: The Fundamental Sub-Unit of the Kidney.
11
Basic Functional Anatomy of the Kidney.
• The glomerulus: the basic filtering unit – Filtration membrane is formed by the 3 layers:
• Fenestrated capillary endothelium. • Glomerular basement membrane constructed of
Type IV collagen and polyanionic proteoglycans (particularly heparan sulfate). What do you think is the functional consequence of these polyanionic sites?
• Visceral epithelial cells of Bowman’s capsule (podocytes) whose pedicels form the filtration slits (remember, the parietal layer of Bowman’s capsule and its basement membrane are continuous with the proximal convoluted tubule).
12

5
13
14
15
Three cell types make up the glomerulus: endothelial (red), mesangial (blue) and the visceral epithelial cellular podocyte (yellow). Squamous epithelial cells of the Bowman capsule are easily seen (green). The macula densa (black) is part of the distal tubule. A collecting duct is in the upper left. Bar = 50 Microns

6
16
Basic Functional Anatomy of the Kidney: The Glomerulus. • The formation of the glomerular ultrafiltrate is the net
result of the balance between the glomerular blood hydrostatic pressure (GHP), the hydrostatic pressure in Bowman’s space (HBS), the blood colloid oncotic pressure (BCOP), and the effective hydraulic permeability of the filtration membrane (the ultrafiltration coefficient or Kf)
• The effective net filtration pressure (Pnet) = GHP - (HBS + BCOP); Pnet is typically 10 mm of Hg
• Single nephron glomerular filtration rate (SNGFR) = PNET x Kf
– Kf is determined by the total surface area available for filtration and the hydraulic permeability of the capillary wall
17
An Overview of the Regulation of GFR
18
Basic Functional Anatomy of the Kidney: The Glomerulus.
• Autoregulation of glomerular filtration: glomerular hydrostatic pressure, and thus Pnet and GFR are regulated by the cells of the macula densa, the NaCl concentration at the macula densa of the distal convoluted tubule of the nephron, the renin/angiotensin system and the vascular smooth muscle of the afferent and efferent arterioles:
• Renin release is a critical part of the renin-angiotensin-aldosterone system

7
19
20
The renin-angiotensin system (RAS) or the renin-angiotensin-aldosterone system (RAAS) is a hormone system that helps regulate long-term blood pressure and blood volume in the body. The system can be activated when there is a loss of blood volume or a drop in blood pressure (such as in a hemorrhage). If the perfusion of the juxtaglomerular apparatus in the kidneys decreases, then the juxtaglomerular cells release the enzyme renin. Renin cleaves an inactive peptide called angiotensinogen, converting it into angiotensin I. Angiotensin I is then converted to angiotensin II by angiotensin-converting enzyme (ACE), which is found mainly in lung capillaries.
21
Renin release from Goormaghtigh’s cells is triggered by ↓ renal perfusion due to: (1) ↓ pressure in the afferent arteriole; and/or (2) activation of β1-adrenergic receptors in the juxtaglomerular apparatus. Note the close anatomical relationship between the macula densa, the efferent and afferent arterioles, the glomerulus and the Goormaghtigh’s cells. This close anatomical relationship is critical for normal glomerular autoregulation.

8
22
Basic Functional Anatomy of the Kidney: The Glomerulus.
• Under normal circumstances, the filtration membrane provides a significant barrier to macromolecules greater than ~ 100 Å in size.
• Filtration of cationic molecules tends to be more restricted compared with neutral molecules ions of the same size due to the presence of anionic binding sites on the filtration membrane; the filtration of cationic molecules is facilitated.
• This filtration size approximately equates to the size of serum albumin and free hemoglobin; unbound free hemoglobin enters urine more readily than albumin because of its shape (serum hemoglobin is not normally filtered because it binds to a haptoglobin, a large protein).
23
Basic Functional Anatomy of the Kidney: The Glomerulus.
• The Mesangium – The filtration membrane is supported by the mesangium which
consists of Type IV collagen, proteoglycans and other proteins. Damage to or alteration of the messangial collagen is an important mechanism in toxicological damage to the glomerulus.
– Contains mesangial stellate cell • Contractile and responds to vasoactive hormones (i.e.
angiotensin II) • Synthesizes and secretes the mesangial matrix
– Contains phagocytic cells • Function as antigen clearing and presentation cells • Antigen uptake and clearance from the mesangium is
relatively slow
24
Basic Functional Anatomy of the Kidney: Reasons Why The Glomerulus is Prone to Toxic Injury.
• High exposure to systemically distributed toxicants: glomeruli are exposed to ~ 70% of plasma that reaches the kidney.
• Anionic sites of glomerular filtration membrane – àElectrostatic interactions with polycations (e.g.
aminoglycosides, particularly gentamicin) --> decrease GFR
• Damage to endothelial and epithelial cells by puromycin, adriamycin, mitomycin, cyclosporine (messangiolysis).
• Prone to protein deposition and damage to the filtration membrane.
• Prone to immune complex deposition.

9
25
Basic Functional Anatomy of the Kidney: Some Useful Formulae Pertaining to Glomerular Filtration.
• Some important concepts and formulae relating to glomerular filtration:
– Clearance: volume of plasma completely cleared of a xenobiotic per unit time. C = clearance; U = urine concentration; V = urine flow; P = plasma concentration; U*V = urinary excretion
– Clearance is a key measurement of renal function. It is an indirect measure of GFR.
– It is most commonly measured clinically using urine and plasma creatinine levels.
– More accurate measurements are made using inulin, an oligosaccharaide which is 100% removed from the body by glomerular filtration and is not re-absorbed by the nephron. For all practical purposes, inulin clearance = GFR
26
Basic Functional Anatomy of the Kidney: Some Useful Formulae Pertaining to Glomerular Filtration.
• Effective renal plasma flow – Effective renal plasma flow can be measured by para-
aminohippurate (PAH) clearance (“effective” is applied because it measures the fraction of the total renal plasma flow that perfuses functional portions of the nephron where it can be filtered and secreted).
– PAH is not reabsorbed, metabolized or synthesized by the kidney. PAH undergoes both glomerular filtration and tubular secretion by a rate limited active transport mechanism. If the afferent arteriolar PAH concentration (Ax) is low enough that the peritubular load of PAH is below the PAH transport maximum, then PAH will be completely cleared from the plasma in a single pass through the kidney.
– Ux = urine concentration; f = urine flow rate; Vx = renal vein concentration; ER = extraction ratio=1 – Vx/Ax;
ERAxfUx
VxAxfUxERPF
***
=−
=
27
Basic Functional Anatomy of the Kidney: Some Useful Formulae Pertaining to Glomerular Filtration. • Effective renal plasma flow:
– Vx is impossible to measure, so it is either assumed to be 0 (which results in a slight underestimation of the RPF) or an ER can be applied (ER is typically 0.9 – 0.95). The ER is necessary since some PAH (5-10%) is distributed in blood to the non-filtration functioning areas of the kidney and appears in the renal vein.
• Effective renal blood flow is an important measurement of renal perfusion:
• ERBF is the volume of blood delivered to the kidney per unit time. In humans, the kidneys together receive roughly 20% of cardiac output, amounting to 1 L/min in a normal 70-kg adult male.
HematocritERPFERBF
−=1

10
28
• Filtration fraction:
• The filtration fraction (FF) is defined as the ratio of the GFR to the RPF and is calculated as the ratio of inulin clearance to PAH clearance.
• Under normal conditions approximately 180 l /day of plasma flows through the kidneys and the average adult produces a urine volume of 1 to 2 L over the same period. This means that greater than 99% of the filtrate must be reabsorbed by the tubules.
• The FF is a measure of tubular re-absorptive efficiency, particularly in the proximal convoluted tubule where the bulk of the re-absorption occurs.
ERPFGFRFF =
Basic Functional Anatomy of the Kidney: Some Useful Formulae Pertaining to Glomerular Filtration.
29
Basic Functional Anatomy of the Kidney: The Proximal Convoluted Tubule.
• PCT is THE most common site of toxic damage in the kidney.
• Absorbs ~ 60 – 80% of solute and water present in the
glomerular filtrate due to numerous transport systems that operate against the osmotic and concentration gradient present in the proximal tubule (i.e. the net effect is concentration of the fluid in the proximal tubule).
• Cells of the proximal tubule have the highest rate of oxidative metabolism in the kidney and are thus the most prone to hypoxic injury, particularly the pars recta.
30
Basic Functional Anatomy of the Kidney: Metabolic Features of The Proximal Convoluted Tubule.
• Main site of re-absorption of glucose, amino acids, lactic acid, uric acid, creatine, citric acid, ascorbic acid, phosphate, sulfate, calcium, potassium, and sodium ions by active transport
• Re-absorption of chloride ions and other negatively charged ions occurs passively due to electrochemical attraction because of the active uptake of Na+; Na+ uptake is mediated by the Na+/K+ ATPase located on the basolateral cell membranes of the proximal tubular epithelium
• Active secretion of substances such as penicillin, histamine, creatine, and hydrogen ions occurs in the proximal tubule

11
31
Basic Functional Anatomy of the Kidney: The Proximal Convoluted Tubule.
• Proximal tubule reabsorbs almost 100% of the low molecular weight proteins and amino acids present in the glomerular filtrate via specific endocytic protein re-absorption processes.
– Most of this re-absorption occurs in the first 1 mm of the proximal tubule (S1).
– Protein uptake is a low affinity, high capacity process. – Factors affecting the efficiency of protein uptake include size
and charge: cationic proteins are more efficiently reabsorbed than anionic proteins of the same size.
• Proximal convoluted tubule is the main site of weak organic acid uptake; weak organic acids are actually anionic at normal urine pH and are taken up by the apical OAT-K transporters.
32
Basic Functional Anatomy of the Kidney: The Proximal Convoluted Tubule.
• Proximal convoluted tubule is the main site of re-absorption of bicarbonate and thus plays an important role in body acid-base regulation.
• Biotransformation of xenobiotics – Inducible CYP mixed function oxidases are present at high
levels in the S2 or S3 segment of the proximal tubule (i.e. proximal convoluted tubule or pars recta depending upon species): the proximal tubule is a major site of damage for xenobiotics that undergo toxication by phase I metabolism (i.e. formation of reactive electrophiles)
– Cyclooxygenase is present in relatively high amounts in the renal vascular endothelium and medullary interstitium and co-oxygenation rather than metabolism by CYP is an important mechanism of pathological Phase I metabolism in the kidney
33
Schematic model of organic anion transporters in renal proximal tubule. Uptake of organic anions (OA) across the basolateral membrane is mediated by the classic sodium-dependent organic anion transport system, which includes -ketoglutarate (-KG2)/OA exchange via the organic anion transporter (OAT1) and sodium-ketoglutarate cotransport via the Na+/dicarboxylate cotransporter (SDCT2). A second sodium-independent uptake system for bulky OA has recently been identified, but its molecular identity is unknown. Intracellular accumulation occurs for substrates of both transport systems in mitochondria and vesicles of unknown origin. The apical (brush-border) membrane contains various transport systems for efflux of OA into the lumen or re-absorption from lumen into the cell. The multidrug resistance transporter, MRP2, mediates primary active luminal secretion. The organic anion transporting polypetide, OATP1, and the kidney-specific OAT-K1 and OAT-K2 might mediate facilitated OA efflux but could also be involved in re-absorption via an exchange mechanism. PEPT1 and PEPT2 mediate luminal uptake of peptide drugs, whereas CNT1 and CNT2 are involved in re-absorption of nucleosides.
12
34
Basic Functional Anatomy of the Kidney: The Proximal Convoluted Tubule.
• Functionally, the PCT is divided into 3 segments: S1, S2 an S3.
– S1 (or P1) = short segment connecting to the glomerular space;
– S2 (or P2) = represents the bulk of the proximal convoluted tubule
– S3 (or P3) = represents the bulk of the pars recta
• Each segment of the PCT is physiologically and functionally different: this is important toxicologically.
35
Basic Functional Anatomy of the Kidney: Toxicological Characteristics of the Segments of the PCT. PCT Segment Toxicological Features
S1 1. Site of bulk of water, amino acid and protein re-absorption in the PCT. 2. Capable of re-absorption by endocytosis (filtered proteins). 3. High levels of OAT3: important in excretion of uremic toxins. 4. MRP2 is present. Important in the protection of the PCT. 5. OCT1 is present. Prone to damage due to concentration of OCT1 substrates in the cell. 6. MDR1/P-glycoprotein (ATP-binding cassette sub-family B member 1) is present. Prone to damage due to concentration of substrates in the lumen. 7. High levels of PEPT1. Prone to damage due to re-absorption and concentration of substrates within the cell.
S2 1. High levels of CYP (particularly CYP2E1): prone to damage by Phase I toxication. 2. High level of OAT1: prone to damage by concentration of OAT1 substrates in the cell and lumen (e.g. ochratoxin A, β-lactamine antibiotics). Site of active excretion of PAH. OAT1 is important in the excretion of uremic toxins. 3. Active re-absorption of α-2U globulin: site of α-2U globulin/hyaline droplet nephropathy in ♂ rats. 4. MRP2 is present. Important in the protection of the PCT. 5. OCT1 is present. Prone to damage due to concentration of OCT1 substrates in the cell. 6. MDR1/P-glycoprotein (ATP-binding cassette sub-family B member 1) is present. Prone to damage due to concentration of substrates in the lumen.
S3 1. Contains high levels of brush border gamma-glutamyl transpeptidase -> converts GSH conjugates to cysteine-glycine conjugates which can then be re-absorbed by the neutral amino acid transporter: prone to damage due to re-absorption and toxication of GSH conjugates. 2. High levels of intracellular β-lyase which converts cysteine conjugates to reactive thiols. 2. Highest rate of oxidative metabolism in the kidney; particularly prone to hypoxia and vascular disturbances. 3. High levels of CYP (particularly CYP2E1): prone to damage by Phase I toxication. 4. High levels of OATP on the brush border. Prone to damage due to concentration of OATP substrates in the lumen. 5. MRP2 is present. Important in protection of the PCT. 6. MDR1/P-glycoprotein (ATP-binding cassette sub-family B member 1) is present. Prone to damage due to concentration of substrates in the lumen. 7. High levels of PEPT2. Prone to damage due to re-absorption and concentration of substrates within the cell. 8. High levels of OAT-K1 and OAT-K2. Active re-absorption of anions from the lumen. Prone to damage due to re-absorption and concentration of substrates within the cell.
36
Basic Functional Anatomy of the Kidney: The Loop of Henle.
• Divided into 3 parts: thin descending limb, thin ascending limb and the thick ascending limb
• There is a marked change in tubule diameter between the pars recta and the thin descending limb; this is important in both pathology and toxicology: obstruction due to luminal crystal formation.
• Main function of the loop of Henle is the passive re-absorption of water which is accomplished by a counter current multiplier effect.

13
37
Basic Functional Anatomy of the Kidney: The Loop of Henle Counter Current Multiplier.
• Selective permeability is the key feature: • Water can leave descending limb but not the ascending limb of
the loop of Henle. • Na+ cannot leave descending limb but can leave the ascending
limb of the loop of Henle.
38
Basic Functional Anatomy of the Kidney: The Loop of Henle Counter Current Multiplier.
• Counter current multiplier of the loop of Henle is important toxicologically because of the potential for the concentration of toxicants within the tubular lumen.
• Thick ascending limb of the loop of Henle has high levels of Na active transport and is heavily dependent on oxidative metabolism: prone to hypoxic damage.
39
Basic Functional Anatomy of the Kidney: Distal Convoluted Tubule.
• Regulates body pH by absorbing bicarbonate and secreting protons (H+) into the filtrate.
• Regulates body sodium and potassium levels by secreting K+ and absorbing Na+ using the Na+/K+
ATPase.
• Sodium absorption by the distal tubule is mediated by the hormone aldosterone. Aldosterone increases sodium re-absorption.

14
40
41
Basic Functional Anatomy of the Kidney: Collecting Ducts.
• Accounts for 4-5% of the kidney's re-absorption of sodium and 5% of the kidney's re-absorption of water. At times of extreme dehydration, over 24% of the filtered water may be reabsorbed in the collecting duct system.
• The collecting ducts, particularly the outer medullary and cortical collecting ducts, are largely impermeable to water without the presence of antidiuretic hormone (ADH, or vasopressin).
• In the absence of ADH, water in the renal filtrate is left alone to enter the urine, promoting diuresis.
• When ADH is present, aquaporins allow for the re-absorption of this water, thereby inhibiting diuresis.
42

15
43
Basic Functional Anatomy of the Kidney: Collecting Ducts.
• Water and sodium re-absorption in the collecting ducts is also regulated by atrial natriuretic peptide which acts to decrease water and sodium re-absorption
44
45
Learning Task 3: Understand the factors that make the kidneys prone to toxic damage.

16
46
Factors Predisposing the Kidney to Toxic Injury.
• High blood flow -> 25% of cardiac output à glomeruli and PCT have high exposures to toxicants in blood
• Active re-absorption and concentration of toxicants by the PCT
• Ability of S3 PCT to dissociate, re-absorb and metabolize glutathione-conjugates to reactive thiols.
47
GSH-X
Brush border G
GT
Cysteine-glycine-X
NAT*
*NAT = neutral amino acid transporter
“X” = typically halogenated alkenes such as hexochloro-1,3-butadiene, trichloroehtylene, tetrafluoroethylene, bromohydroquinone (metabolite of bromobenzene).
Aminodipeptidase Cysteine-X
X-S- (reactive thiol)
β-lyase
Apical Brush Border
S3 PCT
Renal Tubular Epithelial Cell
S3 PCT
48
Factors Predisposing the Kidney to Toxic Injury.
• Change in pH in tubular fluid --> change in ionization state --> increased re-absorption of non-ionized (lipophilic) toxicants or ion trapping and concentration within the lumen (depends on the lipophilicity of the toxicant, which in turn depends on the ionization state of the toxicant, which in turn depends on the pKa of toxicant).
• Remember and be able to use the following (Henderson-Hasselbach equations):
• For Acids:
• For bases:
• pKa = 14 - pKb
][][log
ionizedunionizedpHpKa =−
][][log
unionizedionizedpHpKa =−
17
49
Factors Predisposing the Kidney to Toxic Injury.
• High CYP, particularly in S2 & S3 of PCT and particularly CYP2E1. Prone to Phase I toxication.
• High rates of oxidative metabolism in PCT and thick ascending limb of the loop of Henle: prone to hypoxic injury.
• Concentration of toxicants within the PCT, loop of Henle and collecting ducts.
• Kidney lacks collateral blood supply. The medullar is particularly prone to ischemia. Vasodilatation in the medulla and renal papilla is dependent on PgE2 and the presence of functional cyclooxygenase (inhibited by NSAIDs).
• High levels of prostaglandin hydroperoxidase in the renal papilla i.e. high levels of co-oxidation.
50
Learning Task 4: Understand the kidney’s responses to toxic injury and its compensatory
mechanisms.
51
Responses of Kidney to Toxic Injury
• Toxic responses include:
– Damage to the glomeruli à glomerulonephritis.
– Acute renal failure, which in toxicology is most commonly associated with nephrotoxic acute tubular necrosis (particularly the PCT).
– Damage to the interstitium + the tubules à tubulo-interstitial nephritis.
– Chronic progressive nephropathy or chronic renal failure.

18
52
Responses of Kidney to Toxic Injury: Glomerulonephritis.
• The glomerular filtration membrane, particularly the basement membrane, is prone to binding immune complexes (IgM –Ag, IgG-Ag or polymerized IgA). This activates C’ (particularly C’3) and triggers an inflammatory response.
• The glomeruli are also the targets in secondary thrombotic thrombocytopenic purpura (associate with penicillins, platelet aggregation inhibitors such as ticlopidine and clopidogrel, and Immunosuppressants cyclosporin, mitomycin, tacrolimus/FK506, and interferon-α). Disease is due to binding of platelet-fibrin complexes to the glomerular capillaries. Micro-infarction and inflammation then ensue.
• The glomeruli are also the targets in hemolytic uremic syndrome due to the verotoxins produced by E. coli O157:H7.
53
Responses of Kidney to Toxic Injury: Glomerulonephritis.
• Glomerulonephritis is divided into acute and chronic-progressive. Chronic-progressive GN represents the end-stage of all forms of progressive glomerulonephritis.
• The hallmark of chronic-progressive GN is the presence of permanently destroyed/non-functional glomeruli. Hyalinosclerosis i.e. the total replacement of glomeruli and Bowman's space with hyaline, is present.
– The hyaline is an amorphous, pink, homogeneous material , resulting from combination of plasma proteins, increased mesangial matrix and collagen. Obstruction of blood flow results in secondary tubular atrophy, interstitial fibrosis and thickening of the arterial wall by hyaline deposits. A lymphocytic inflammation is typically present in the interstitium.
54
End-stage of glomerular hyalinosclerosis. Glomeruli are totally replaced by hyaline connective tissue. There is atrophy of the tubules, which appear shrunken and are surrounded by a thickened basement membrane. There is also fibrosis of the interstitium with arterio- and arteriolosclerosis.

19
55
Responses of Kidney to Toxic Injury: Glomerulonephritis.
• There are 5 types of acute GN based upon the histopathology – Acute diffuse membranoproliferative GN: classically due to a
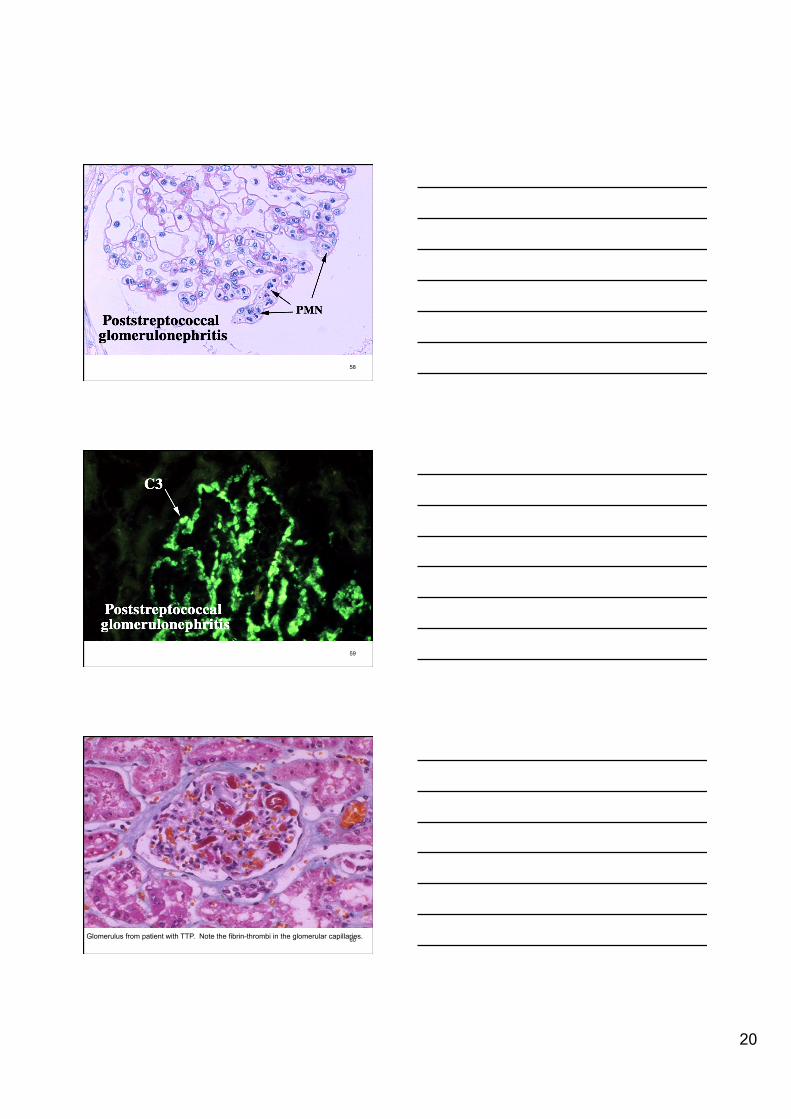
Type III hypersensitivity response following Group A Streptococcus infection or drug treatment. Characterized by hypercellularity due to proliferation of endothelial and mesangial cells, inflammatory infiltrate with neutrophils and with monocytes. Triggered by C’ activation, the formation of C’3-Ag complexes and the formation of C’3-Ag-Ab complexes that deposit in the glomeruli. This is a commonly observed xenobiotic-induced glomerulonephritis (Type III hypersensitivity reaction).
– Rapidly progressive GN (Crescentic GN): due to increased permeability of the filtration membrane and leakage of fibrin into Bowman’s space. Renal failure rapidly develops. A mild form of this type of glomerulonephritis is commonly associated with treatment with aminoglycoside antibiotics, particularly gentamicin, which damage the anionic sites on the filtration membrane.
56
Responses of Kidney to Toxic Injury: Glomerulonephritis.
• There are 5 types of acute GN based upon the histopathology
– Microangiopathic GN: observed in TTP and HUS. Characteristic is the presence of fibrin-thrombi in the glomerular capillaries. Often progresses to membranoproliferative GN. TTP can be drug-induced!
– Mesangial proliferative GN: due to deposition of polymerized IgA1 in the mesangium, with a localized proliferation of tissue.
– Minimal change GN: due to a mutation in the nephrin which leads to podocyte fusion. This is a genetic rather than a toxicological reaction.
57 Acute GN. Note the neutrophils.
20
58
59
60 Glomerulus from patient with TTP. Note the fibrin-thrombi in the glomerular capillaries.

21
61 Drug-induced TTP. Note the purpura i.e. extensive subcutaneous hemorrhages. The prognosis with advanced TTP is very poor.
62
Responses of Kidney to Toxic Injury: Glomerulonephritis.
• Hallmarks of glomerulonephritis
– Hematuria i.e. increased RBCs in urine – Proteinuria – Decreased GFR and signs of renal failure (see later) – ± signs of a systemic immune reaction e.g.
arthralgia, malaise, fever – Hypoproteinemia – Peripheral edema due to hypoproteinemia – Fatigue – Oliguria or polyuria – Progression to renal failure and end-stage kidney
63
Responses of Kidney to Toxic Injury: Acute Renal Failure.
• Acute renal failure (ARF) is defined as an abrupt or rapid decline in renal function. A rise in serum blood urea nitrogen (BUN) or serum creatinine concentrations, with or without a decrement in urine output, is usually evidence of ARF. The condition is often transient and completely reversible.
• ARF may occur following 3 types of event: (1) as an adaptive response to severe volume depletion and hypotension, with structurally and functionally intact nephrons; (2) in response to cytotoxic, ischemic or hypoxic insults to the kidney, with structural and functional damage; and (3) with obstruction to the passage of urine. Therefore, ARF may be classified as pre-renal, intrinsic, and post-renal.
• In toxicology, we mostly deal with intrinsic ARF which is usually due to tubular (commonly the PCT) or glomerular damage.
22
64
Responses of Kidney to Toxic Injury: Acute Renal Failure.
• The intrinsic form of the syndrome may be accompanied by a well-defined sequence of events. The first is an initiation phase, characterized by daily increases in serum creatinine and BUN, and reduced urinary volume; the second is a maintenance phase, during which the glomerular filtration rate (GFR) is relatively stable and urine volume may be increased (inability to concentrate urine); and the third is a recovery phase, in which serum creatinine/BUN levels fall and tubular function is restored. This sequence of events is not always apparent, and oliguria may not be present.
• A physiologic hallmark of intrinsic ARF is a failure to maximally concentrate urine i.e. failure to excrete concentrated urine, even in the presence of oliguria This defect is not responsive to vasopressin. The injured kidney fails to generate and maintain a high medullary solute gradient because the accumulation of solute in the medulla depends on normal distal nephron function. In intrinsic ARG, urine osmolality is usually less than 300 mOsm/kg irrespective of the volume of urine produced.
65
Responses of Kidney to Toxic Injury: Acute Renal Failure.
• Classifying ARF as oliguric or nonoliguric based on daily urine excretion may be useful. Oliguria is defined as a daily urine volume of less than 500 ml/d. Anuria is defined as a urine output of less than 50 ml/d and, if abrupt in onset, is suggestive of obstruction.
• Because of the large functional reserve, a substantial amount of damage must occur before blatant (i.e. presence of uremia) ARF occurs. Blatant clinically recognizable renal failure, as evidenced by uremia, will occur when the GFR has decreased by ~ 50 – 84%.
66
Responses of Kidney to Toxic Injury: Acute Renal Failure.
• Intrarenal vasoconstriction is the dominant mechanism for the reduced GFR in patients with ARF.
• The stressed renal microvasculature is more sensitive to potentially vasoconstrictive drugs and otherwise-tolerated changes in systemic blood pressure making the decline in GFR seen in the early stages of ARF worse.
• Prolonged vasoconstriction may evolve into intrinsic ARF, especially when concomitant large vessel arterial disease occurs. Renal failure caused by prolonged vasoconstriction (especially with concomitant large vessel arterial disease) often is induced by the use of angiotensin-converting enzyme (ACE) inhibitors and/or diuretics.

23
67
Responses of Kidney to Toxic Injury: Acute Renal Failure.
• Causes of intrarenal ARF can be grouped into vascular, tubular, interstitial, and glomerular factors.
– Vascular factors- Renal Ischemic Tubulonecrosis: any agent that damages the renal blood supply (vasculitis, embolism) will produce RITN. Classical example is toxic thrombotic thrombocytopenic purpura or hemolytic uremic syndrome (toxins of E. coli O157:H7) which damages the renal vasculature.
– Nephrotoxic Acute Tubular Necrosis: a multitude of agent are capable of damaging the renal tubular epithelial cells, particularly the PCT. NATN is undoubtedly THE MOST COMMON FORM OF TOXIC KIDNEY INJURY! Tubules become obstructed due to cell debris.
68
Classical Acute Nephrotoxic Tubular Necrosis involving the PCT.
69
Responses of Kidney to Toxic Injury: Acute Renal Failure.
• Causes of intrarenal ARF can be grouped into vascular, tubular, interstitial, and glomerular factors.
– Crystaline Acute Tubular Necrosis. Hallmark is the presence of crystals within the tubules ± tubular epithelial necrosis. Classical examples are ethylene glycol and oxalate poisoning.
– Interstitial nephritis usually results from a reaction to a specific drug or a group of drugs. Classically has an allergic mechanism. Typical drugs causing this reaction include: NSAIDs, penicillins, diuretics, cimetidine, and allopurinol.

24
70
Responses of Kidney to Toxic Injury: Acute Renal Failure.
• Irrespective of cause, intrarenal ARF results in the death of the renal tubular epithelial cells, most commonly those of the PCT. The hallmarks of this are:
– Enzymeuria à brush border enzymes like ALP and γ-GT or intracellular enzymes like lactate dehydrogenase, α-GST and N-acetylglucosaminidase are present in the urine.
– Failure of re-absorption of glomerular filtrate à amino aciduria, glucoseuria, low molecular weight proteins (cystatin C, α1-microglobulin, β2-microglobulin, retinol binding protein)
– Presence of sloughed tubular epithelial cells and debris in the urine à tubular epithelial cell casts, cell remnants.
– Proteinuria à Increase in high molecular weight proteins.
71
Responses of Kidney to Toxic Injury: Acute Renal Failure.
• Recovery in ARF – If the nephron basement membrane and
primordial stem cells remain intact, the nephron has the potential to recover. If the basement membrane is destroyed, the nephron probably will not recover.
– If the individual can be supported through the uremic phase of ARF and survives long enough, recovery from ARF is likely. The problem is that if nephrons are lost, then progression from ARF to chronic progressive nephropathy is inevitable.
72
Responses of Kidney to Toxic Injury: Tubulo-Interstitial Nephritis.
• Divided into acute and chronic.
• Toxic acute TIN is usually due to drug-induced hypersensitivity responses. Classically: NSAIDs, rifampicin, penicillins, sulfa antibiotics. Classically a Type I hypersensitivity reaction is involved. Typically reversible. Damage may or may not be sufficient to produce acute renal failure.
• Toxic chronic TIN is a potential outcome of any xenobiotic that damages the renal tubules. This either produces neo-antigens or allows exposure to previously protected antigens. Characterized by chronic inflammation of the interstitium mediated by hypersensitivity mechanisms, tubular degeneration and progression to chronic progressive nephropathy. Classic causes are NSAIDs, thiazide diuretics, furosemide, allopurinol, phenytoin, rifampicin, interferon-α.
25
73
Responses of Kidney to Toxic Injury: Tubulo-Interstitial Nephritis.
• Clinical signs – Except in patients with TIN induced by rifampicin and NSAIDs:
• Evidence of a systemic immune reaction i.e. fever, rash, arthralgia.
• Elevated serum and urine IgE levels. • ± renal failure. • ± hematuria. • Evidence of tubular dysfunction i.e. glycosuria, aminoacid
uria, presence of small proteins in urine. • Elevated eosinophils in urine. • Gross proteinuria (large proteins) is rare
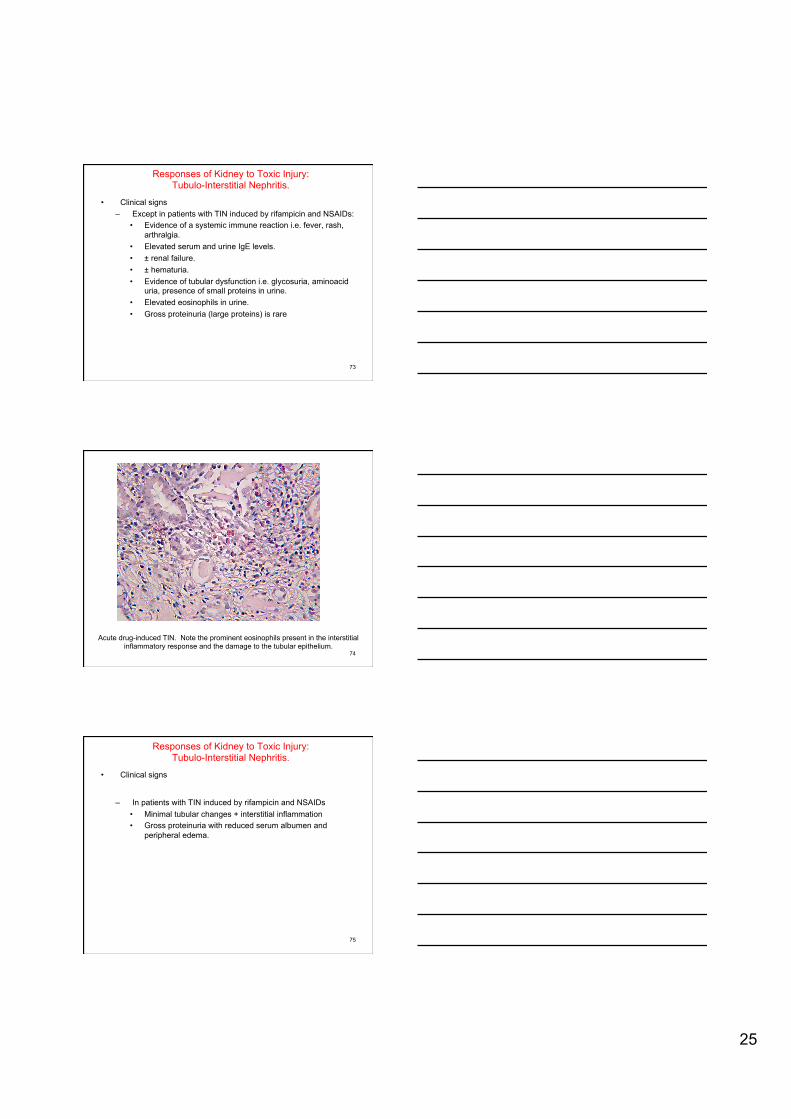
74
Acute drug-induced TIN. Note the prominent eosinophils present in the interstitial inflammatory response and the damage to the tubular epithelium.
75
Responses of Kidney to Toxic Injury: Tubulo-Interstitial Nephritis.
• Clinical signs
– In patients with TIN induced by rifampicin and NSAIDs • Minimal tubular changes + interstitial inflammation • Gross proteinuria with reduced serum albumen and
peripheral edema.
26
76
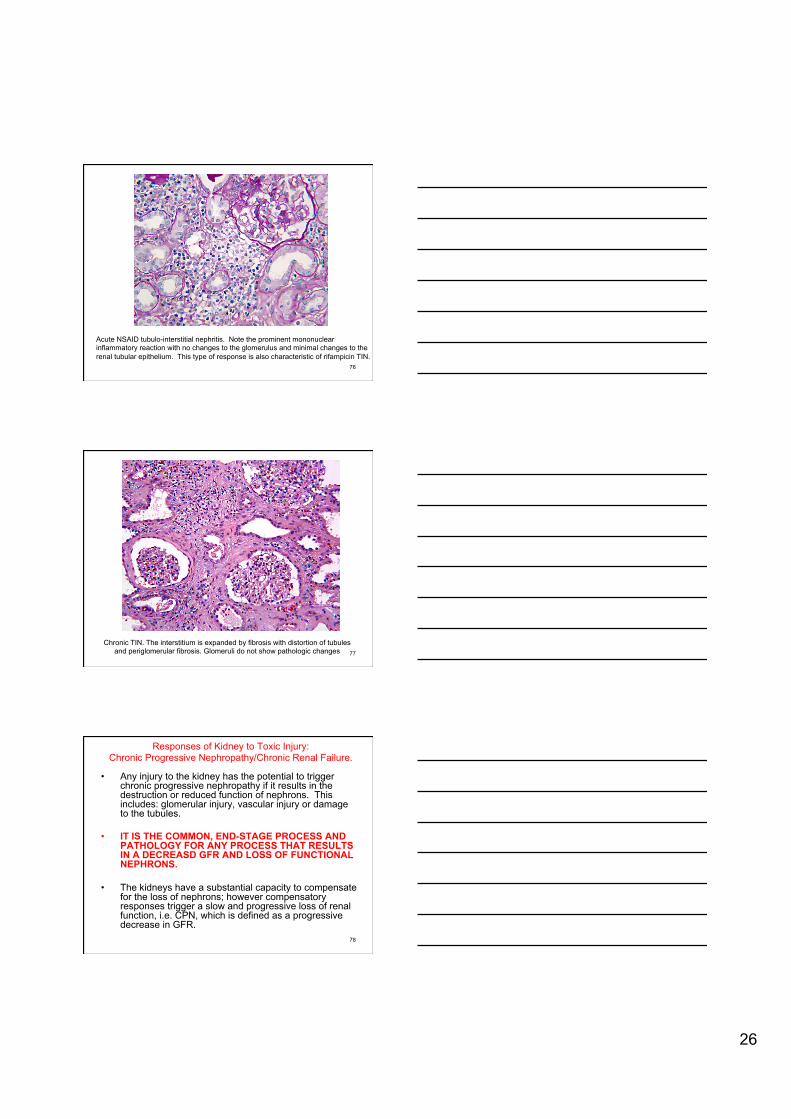
Acute NSAID tubulo-interstitial nephritis. Note the prominent mononuclear inflammatory reaction with no changes to the glomerulus and minimal changes to the renal tubular epithelium. This type of response is also characteristic of rifampicin TIN.
77
Chronic TIN. The interstitium is expanded by fibrosis with distortion of tubules and periglomerular fibrosis. Glomeruli do not show pathologic changes
78
Responses of Kidney to Toxic Injury: Chronic Progressive Nephropathy/Chronic Renal Failure.
• Any injury to the kidney has the potential to trigger chronic progressive nephropathy if it results in the destruction or reduced function of nephrons. This includes: glomerular injury, vascular injury or damage to the tubules.
• IT IS THE COMMON, END-STAGE PROCESS AND PATHOLOGY FOR ANY PROCESS THAT RESULTS IN A DECREASD GFR AND LOSS OF FUNCTIONAL NEPHRONS.
• The kidneys have a substantial capacity to compensate for the loss of nephrons; however compensatory responses trigger a slow and progressive loss of renal function, i.e. CPN, which is defined as a progressive decrease in GFR.

27
79
Responses of Kidney to Toxic Injury: Chronic Progressive Nephropathy/Chronic Renal Failure.
• Classification of CPN:
– Stage 1: Kidney damage with normal or increased GFR (>90 mL/min/1.73 m2); clinically normal.
– Stage 2: Mild reduction in GFR (60-89 mL/min/1.73 m2); asymptomatic.
– Stage 3: Moderate reduction in GFR (30-59 mL/min/1.73 m2); asymptomatic.
– Stage 4: Severe reduction in GFR (15-29 mL/min/1.73 m2); uremia present.
– Stage 5: Kidney failure (GFR <15 mL/min/1.73 m2 or dialysis); end stage renal failure.
80
Responses of Kidney to Toxic Injury: Chronic Progressive Nephropathy/Chronic Renal Failure.
• Any injury to the kidney has the potential to trigger chronic progressive nephropathy if it results in the destruction or reduced function of nephrons.
• The kidneys have a substantial capacity to compensate for the loss of nephrons by attempting to increase the single nephron GFR; however, irrespective of the cause of the original loss of nephrons, the compensatory responses trigger a slow and progressive loss of renal function, i.e. CPN, which is defined as a progressive decrease in GFR.
81
Loss of functional nephrons
Decreased GFR
Glomerular autoregulation system triggered
Glomerular hypertension
↑ GHP
40 – 60% ↑ in SNGFR
Protein overload of the glomerular filtration barrier , mechanical injury of capillary structure
Proteinuria, mesangial expansion, ↑ mesangial matrix and basement membrane thickening
Focal segmental glomerular sclerosis
Cycle of Nephron Loss in CPN
28
82
Responses of Kidney to Toxic Injury: Chronic Progressive Nephropathy/Chronic Renal Failure.
• Common Effects of CPN: – Hyperkalemia usually develops when GFR falls to less than
20-25 ml/min because of the decreased ability of the kidneys to excrete potassium.
– Metabolic acidosis due to: (1)inability to produce enough ammonia in the proximal tubules to excrete the endogenous acid into the urine in the form of ammonium; and (2) accumulation of phosphates, sulfates, and other organic anions.
– Extracellular volume expansion and total-body volume overload results from failure of sodium and free water excretion. This generally becomes clinically manifest when GFR falls to less than 10-15 mL/min, when compensatory mechanisms have become exhausted. Patients present with peripheral and, not uncommonly, pulmonary edema and hypertension.
83
Responses of Kidney to Toxic Injury: Chronic Progressive Nephropathy/Chronic Renal Failure.
• Common Effects of CPN: – Normochromic normocytic anemia principally develops from
decreased renal synthesis of erythropoietin.
– Secondary hyperparathyroidism develops because of hypocalcemia, decreased renal synthesis of 1,25-dihydroxycholecalciferol (1,25-dihydroxyvitamin D, or calcitriol), and hyperphosphatemia.
– Uremic encephalopathy is a marker of the late stages (often terminal) of CPN. The exact cause of UE is unknown. Accumulating metabolites of proteins and amino acids affect the entire neuraxis. Changes in sensorium include loss of memory, impaired concentration, depression, delusions, lethargy, irritability, fatigue, insomnia, psychosis, stupor, catatonia, and coma. Patients may complain of slurred speech, pruritus, muscle twitches, or restless legs.
84
Responses of Kidney to Toxic Injury: Chronic Progressive Nephropathy/Chronic Renal Failure.
• Common Effects of CPN: – GI symptoms – anorexia, nausea, vomiting, diarrhea – Skin manifestations - dry skin, pruritus, ecchymosis – Fatigue, increased somnolence, failure to thrive
• Less Common Effects of CPN – Pericarditis - Can complicate with cardiac tamponade, possibly
resulting in death – Peripheral neuropathy – Restless leg syndrome – Malnutrition – Erectile dysfunction, decreased libido, amenorrhea – Platelet dysfunction with tendency to bleeding

29
85
Questions?
Lecture 2. Clinical Signs of Kidney Disease,
Assessment of Renal Function and the Pathophysiology and Effects of Classical
“Must Know” Renal Toxins/Toxicants.
Learning Tasks. • Learning task 5: Understand the clinical signs of renal
disease.
• Learning task 6: Understand the techniques used to assess renal function and disease.
• Learning task 7: Understand the pathophysiology and effects of the classical “must know” renal toxins/toxicants.

30
Learning Task 5: Understand the clinical signs of renal disease.
Clinical Signs of Renal Disease. • Signs of renal failure:
– Elevated serum creatinine and blood urea nitrogen (BUN) à azotemia (no clinical signs) à uremia (clinical signs present).
– Decreased urine production (oliguria)
– Inability to concentrate (i.e. form high specific gravity urine) urine despite reduced urine volume (hyposthenuria). Urine specific gravity between 1.007 and 1.010 (plasma SG is 1.020)
Clinical Signs of Renal Disease. • Assessment of severity of acute renal failure:
– At Risk: serum creatinine increased 1.5 times OR urine production of <0.5 ml/kg body weight for 6 hours.
– – Renal Injury Present: creatinine 2.0 times OR urine
production <0.5 ml/kg for 12 h.
– Renal Failure: creatinine 3.0 times OR creatinine >355 µmol/l (with a rise of >44) or urine output below 0.3 ml/kg for 24 h.
– – Loss of Renal Function: persistent ARF or more than four
weeks complete loss of kidney function

31
Clinical Signs of Renal Disease. • Clinical effects of uremia:
– Uremia is a clinical syndrome associated with fluid, electrolyte, and hormone imbalances and metabolic abnormalities, which develop in parallel with deterioration of renal function.
– Uremia usually develops only after the creatinine clearance falls to less than 10 mL/min, although some patients may be symptomatic at higher clearance levels, especially if renal failure acutely develops.
– The syndrome may be heralded by the clinical onset of nausea, vomiting, fatigue, anorexia, weight loss, muscle cramps, pruritus, change in mental status, uremic encephalopathy
Clinical Signs of Renal Disease. • Clinical effects of uremia:
– Other effects: • Acidosis (metabolic) • Hyperkalemia • Hypocalcemia, hyperphosphatemia, and increased PTH
levels • Reduced insulin clearance and increased insulin
secretion can lead to increased episodes of hypoglycemia
• Cardiovascular abnormalities, including uremic pericarditis, pericardial effusions, calcium and phosphate deposition–associated worsening of underlying valvular disorders, and uremic suppression of myocardial contractility
Learning Task 6: Understand the techniques used to assess renal function and disease.

32
Assessment of Renal Function. • Blood BUN/Creatinine
– Insensitive measures of renal function – GFR must decrease by 50 – 80% before changes in blood
BUN/creatinine are seen – Creatinine clearance is often used as a clinical measure of
GFR
• Assessment of GFR – Inulin clearance
• Assessment of renal blood flow – PAH clearance
Urinalysis. • Presence or absence of protein
– Protein can be from: blood (e.g. albumen), failure of re-absorption of low molecular weight proteins (e.g. beta-2 microglobulin), or from tubular injury. Excessive protein in the urine is always abnormal
– Presence of small proteins (e.g. beta-2 microglobulin) suggest PCT damage (failure of re-absorption).
• Presence or absence of blood/hemoglobin – Test does not distinguish between blood or hemoglobin – Neither are normally filtered – Presence suggests severe hemolytic disease (i.e.
presence of free Hb in circulation) or severe damage to the nephron or bleeding into the urinary tract.
– Presence in urine is always abnormal.
Urinalysis. • Presence or absence of protein
– Glucose: except following meals, presence of glucose in urine suggests either high blood glucose (diabetes mellitus) or PCT injury (failure of re-absorption).
• Specific gravity – Tests for the ability to concentrate urine
• pH
• Ketone bodies – Acetoacetate, acetate and beta-hydroxybutyrate – Indicators of ketogenesis i.e. consumption of fatty acids for
energy

33
Urinalysis.
• WBC number: increased suggests interstitial nephritis, glomerulonephritis or infection within the urinary tract
• Eosinophil count: increased suggests allergic interstitial nephritis
• Neoplastic cells
• Parasites
Urinalysis.
• Casts – RBC casts: suggests haemorrhage – WBC casts: suggests inflammation – Granular casts: remnants of sloughed tubular epithelium
i.e. suggests tubular injury
• Crystals – Ca oxalate (ethylene glycol) – Urate – Stones
Granular cast: remnants of sloughed tubular epithelial cells

34
WBC cast
THE Gold Standard!.
• Renal biopsy is still THE gold standard for assessment of kidney disease!
Learning Task 7: Understand the pathophysiology and effects of the classical “must know” renal
toxins/toxicants.

35
Classical “Must Know Renal Toxicants.”
• ACE inhibitors • Acetominophen • α-2U globulin/hyaline
droplet nephrosis • Aminoglycoside
antibiotics • Amphoteracin B • Bromobenzene and
halogenated alkenes • Carbon tetrachloride • Chloroform • Cadmium • Cephalosporins • Cis-platin
• Cyclosporin A • Doxorubicin • Mercury • Gold • Methoxyfluorane • Sevofluorane • Ocratoxin/citrinin • NSAID nephropathy • Lead • Puromycin
Angiotensin Converting Enzyme Inhibitors. • Types of toxicity:
– Hemodynamic resulting in ↓ GFR
– Immune mediated glomerulonephritis
Acetominophen Renal Toxicity. • Classical example of S2 PCT damage in humans and mice due to high
CYP2E1 levels. • Mechanism differs in rats: primarily a S3 toxicant in rats (metabolite is
para-aminophenol) .
Acetominophen CYP2E1 N-acetyl-p-benzoquinone imine (nucleophile)
Sulfonation
Detoxified if Low Dose
Conjugation to GSH
Mercapturic acid
Damage to S2 PCT (high CYP2E1)
Long-term alcohol abuse has been established as potentiating acetaminophen toxicity via induction of CYP2E1 and depletion of glutathione. Alcoholic patients may develop
severe liver and kidney damage after ingestion of standard therapeutic doses of acetaminophen.

36
α-2u Globulin Nephrosis. • Unique to the ♂ rat. Does not occur in any other laboratory or domestic
animal or humans.
• Only affects the S2 segment of the PCT of the ♂ rat.
• Important artefact in pre-clinical toxicology screening.
• Predisposes to renal carcinogenesis in the ♂ rat.
• Classical causes are: – Trimethylpenatne (unleaded gasoline) – d-Limonene (lemon scent, citrus oils) – JP-4 jet fuel (shale derived) – JP-5 jet fuel (shale derived) – Parafins – Decalin (decahydronaphthalene) – Methyl isobutyl ketone – Pentachloroethane
α-2u Globulin Nephrosis.
α-2u globulin synthesized in the liver
Solvent CYP Epoxidation
Epoxide metabolite
α-2u globulin-epoxide conjugate
Released into circulation and filtered by the kidney
Reabsorbed by S2 of PCT
Very slowly degraded in lysosome
Cell death
PCT dysfunction
Compensatory cell proliferation acts as a tumor promoter
S2 hyaline droplet nephrosis in a ♂ rat subchronically exposed to JP-4 jet fuel vapor.
37
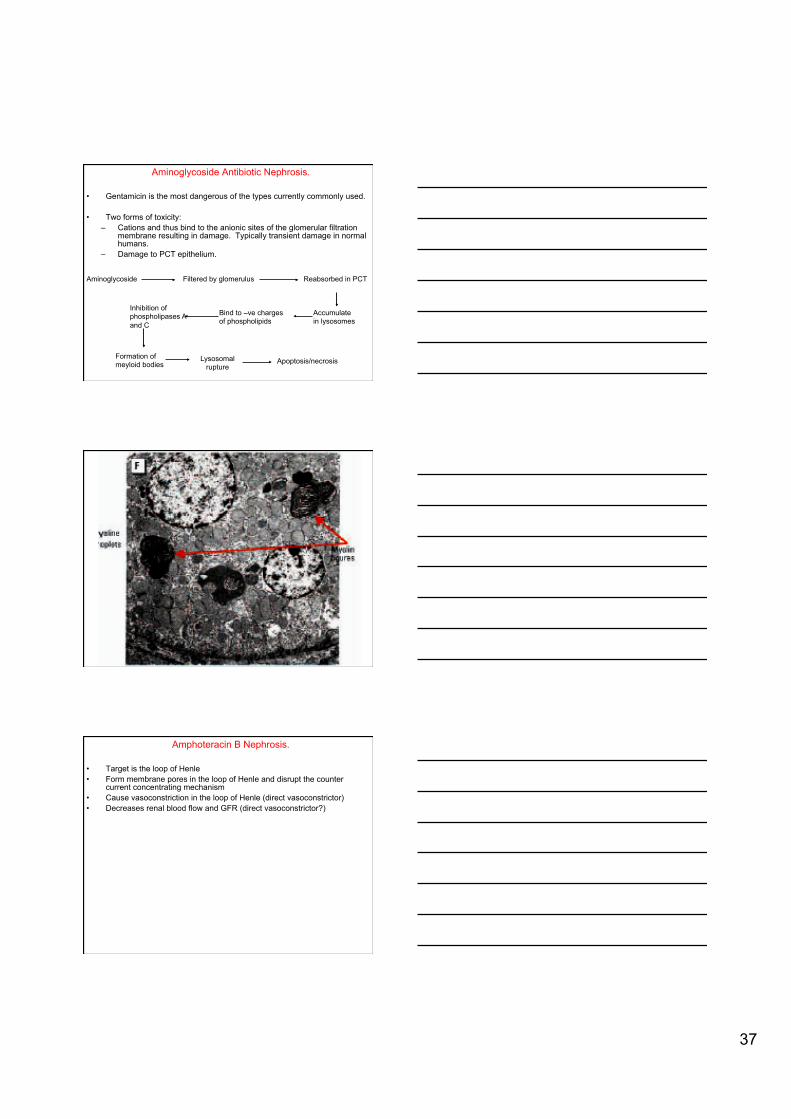
Aminoglycoside Antibiotic Nephrosis.
• Gentamicin is the most dangerous of the types currently commonly used.
• Two forms of toxicity: – Cations and thus bind to the anionic sites of the glomerular filtration
membrane resulting in damage. Typically transient damage in normal humans.
– Damage to PCT epithelium.
Aminoglycoside Filtered by glomerulus Reabsorbed in PCT
Accumulate in lysosomes
Bind to –ve charges of phospholipids
Inhibition of phospholipases A and C
Formation of meyloid bodies
Lysosomal rupture
Apoptosis/necrosis
Amphoteracin B Nephrosis.
• Target is the loop of Henle • Form membrane pores in the loop of Henle and disrupt the counter
current concentrating mechanism • Cause vasoconstriction in the loop of Henle (direct vasoconstrictor) • Decreases renal blood flow and GFR (direct vasoconstrictor?)

38
Bromobenzene and Halogenated Alkenes. • THE classical example of β-lyase-induced renal damage to the S3 of the
PCT. • Mechanism:
CYP2
E1
Liver Circulation
Epoxide hydrolase
Renal filtration
Kidney
BB-hydroquinone-
TCE Metabolism and Renal Damage
GSH-X
Brush border G
GT
Cysteine-glycine-X
NAT*
*NAT = neutral amino acid transporter
Aminodipeptidase Cysteine-X
X-S- (reactive thiol)
β-lyase
Apical Brush Border
S3 PCT
Renal Tubular Epithelial Cell
S3 PCT
“X” = typically halogenated alkenes such as hexochloro-1,3-butadiene, trichloroehtylene, tetrafluoroethylene, bromohydroquinone (metabolite of bromobenzene).

39
Carbon Tetrachloride.
• Target is the PCT, particularly S3 in rats, due to high CYP2E1 levels
• Trichloromeithyl radical acts to: – Reacts with hydrogen to form chloroform which is then metabolized to
a radical – Reacts with itself to form hexachloroethane – Reacts with proteins -> SUICIDE SUBSTRATE FOR CYP2E1 – Peroxidizes the polyenoic lipids of the endoplasmic reticulum and
triggers the subsequent generation of secondary free radicals derived from the lipids in the membrane --> destroys the endoplasmic reticulum resulting in decreased CYP activity and decreased protein synthesis
CYP2E1
Chloroform. • Target is the PCT, particularly S3 in rats, due to high CYP2E1 levels • Similar pathophysiology to CCl4
NU = tissue nuleophile
Phosgene
Organohalides That Do Not Produce Renal Damage.
• Most organohalides produce renal damage, particularly damage to the PCT, either via CYP metabolism to a radical or by β-lyase mediated radical formation.
• Renal damage is often NOT the primary effect.
• Important exceptions to this rule:
– Methylene chloride – Vinyl chloride and vinylidine chloride – Dichloroethanes

40
Cadmium.
• T arget is S1/S2 of PCT.
• 50% of total body burden is concentrated in kidnye; long T1/2 (~10 years).
• Damage is progressive and irreversible.
• Damage is due to redox cycling of Cd2+; Cd also produces immune-mediated glomerulonephritis.
• Soluble Cd salts are more toxic.
Cadmium.
• Decreased renal synthesis of 1,25 dihydroxy vitamin D --> decreased uptake of Ca from gut à “Itai Itai” disease (“Ouch Ouch disease).
• Induces metallothioneine in liver and kidney
• Markers of damage – Urine Cd level (usually Cd-MT) --> indicator of total body
burden. – Low molecular weight proteins e.g. beta-2 microglobulins,
elevated urinary metallothionein, glucose uria, amino acid uria (due decrease resorption in PCT due to damage)
Bile Hepatocyte Plasma Kidney PCT Epithelium (S1/S2)
Cd2+
Cd-Albumen
Cd2+
Cd-MT
Cd-GSH
Cd-
GS
H
Cd-MT
Lysosome
Cd-MT
Cd2+
Redox cycling
41
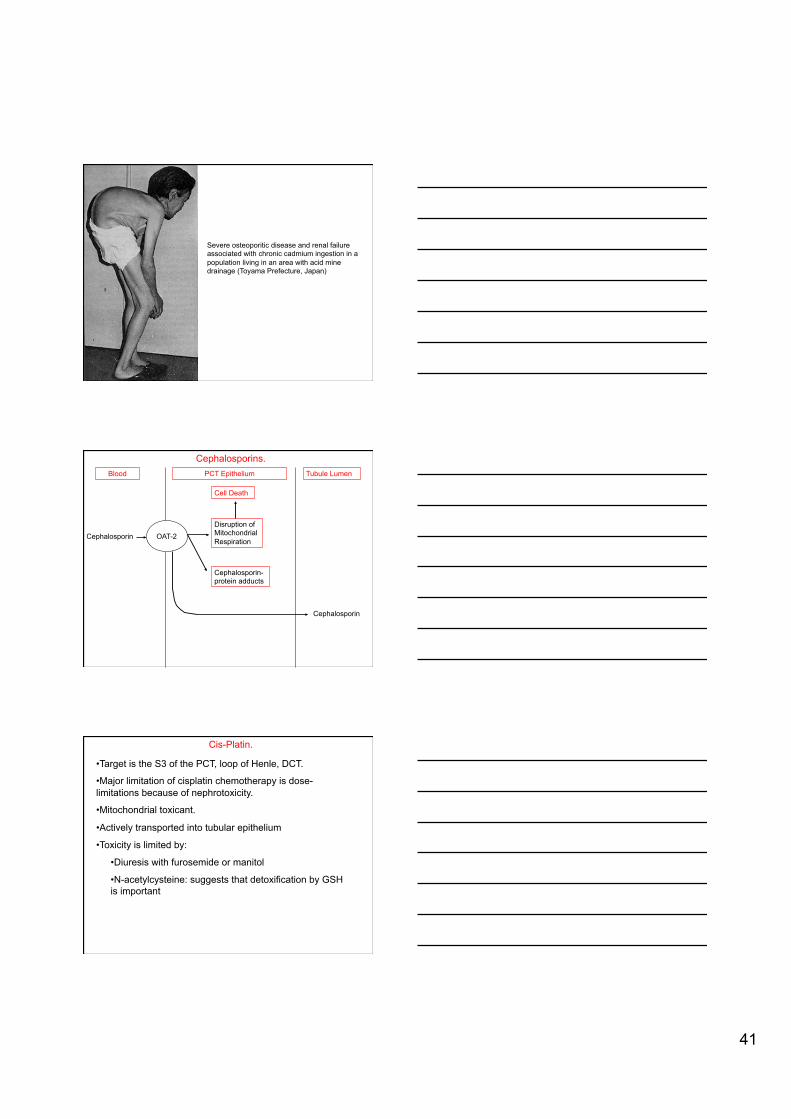
Severe osteoporitic disease and renal failure associated with chronic cadmium ingestion in a population living in an area with acid mine drainage (Toyama Prefecture, Japan)
Cephalosporins.
Cephalosporin
Blood
OAT-2
PCT Epithelium
Disruption of Mitochondrial Respiration
Cell Death
Cephalosporin-protein adducts
Tubule Lumen
Cephalosporin
Cis-Platin. • Target is the S3 of the PCT, loop of Henle, DCT.
• Major limitation of cisplatin chemotherapy is dose-limitations because of nephrotoxicity.
• Mitochondrial toxicant.
• Actively transported into tubular epithelium
• Toxicity is limited by:
• Diuresis with furosemide or manitol
• N-acetylcysteine: suggests that detoxification by GSH is important

42
Cyclosporin A. • Targets
• Interstitium
• Glomerulus
• Vasculature
• Mechanisms:
• Direct damage to the renal vascular endothelium à glomerular thrombotic microangiopathy à ischemia à enhanced synthesis of extracellular matrix proteins à interstitial fibrosis
• Altered eicosanoid metabolism à increased thromboxane synthesis à renal vasoconstriction à decreased renal perfusion à ↓ GFR
Increased glomerular cellularity following cyclosporin endothelial damage
Glomerular focal segmental glomerulosclerosis following cyclosporine exposure.

43
Renal tubular epithelial damage following cyclosporin exposure. Note the vacuoles.
Cyclosporin interstitial fibrosis (trichrome stain)
Doxorubicin (Adriamycin). • Target: glomerulus (early onset) à target is vascular endothelium

44
Doxorubicin (Adriamycin). • Target: PCT (late onset) and glomerular (early onset)
Doxorubicin Filtered by the glomerulus
Diffuses from the lumen into the PCT
epithelium
Pumped back into the tubular lumen via p-glycoprotein
Mitochondrial accumulation
Redox damage, damage to mitochondrial DNA
Mercury Toxicokinetics. • HgO vapor: lipophilic nature allows accumulation in CNS (HgO à catalase à Hg2+)
• Hg+ (mercurous) salts à Poorly absorbed, very slowly converted to Hg2+ by catalase; major target is skin (acrodynia).
• Hg2+ (mercuric) salts • ~ 10% absorbed from GI • Distributes both in plasma and in RBCs; undergoes conjugation to GSH • GSH-Hg2+ accumulates in lysosomes of S3 renal PCT (major target)
• Pheyl (aryl) mercury --> behaves like Hg2+ salts
Mercury Toxicokinetics.
• Methyl and ethyl Hg (alkyl Hg) • High lipid solubility • Forms a cystein complex and actively transported across the BBB by the neutral amino acid transporter • Accumulate in CNS particularly in visual cortex (=calcarine cortex, Brodman area 17) • Very slowly metabolized to Hg2+ (ultimate toxicant in CNS)
• Excretion • Salts --> urine • Organic --> bile (glutathione conjugate)

45
Acute Kidney Injury by Mercuric Salts. • Target is S3 of PCT • Selectively accumulates in S3 via mechanisms that are poorly understood • Luminal uptake:
• Seems to involve GSH-Hg2+ complex and conversion to a cyst-cyst-Hg2+ compound which is re-absorbed by the PCT NAT • The site of formation of GSH-Hg2+ is uncertain: suggestions include within the blood, within the renal luminal fluid
• Basolateral uptake • Via the OAT and dicarboxylate transporters

46
Acute mercuric salt proximal tubular nephrosis. Note the absence of epithelium in the PCT tubules (eosinophilic remnants of the cells remain in the tubules)
Acute Kidney Injury by Mercuric Salts. • Mechanisms of PCT epithelial damage:
• Hg2+ have an affinity for thiol (SH) groups: disruption of the functions of a wide range of proteins.
• Damage mitochondria • Damage membrane proteins • Damage enzymes
• Changed membrane permeability to Ca ions • Binds to GSH and metallothionien à induces both these proteins à protective effect?

47
Chronic Kidney Injury by Mercuric Salts. • Target is the glomerulus. • Produces an immune-mediated glomerulonephropathy. • Characterized by deposition of IgG-C’ complexes within the glomerulus. • Induces autoantibodies to laminin, an important component of the glomerular basement membrane.
Gold Salts. • Gold salts are/were used as a treatment for rheumatoid arthritis. • Damage the PCT epithelium
Methoxyfluorane.
Methoxyfluorane CYP
Oxidative dehalogenation
Fluoride
Filtered by glomerulus
Renal tubular damage

48
Sevofluorane. • Significance of renal toxicity is controversial; observed in rats but limited evidence in humans.
Sevofluorane + sodalime Compound A
fluoromethyl-2,2-difluoro-1-[trifluoromethyl) vinyl ether
Inhaled Liver: conjugation to GSH
Circulation Glomerular filtration
S3-brush border γ-GGT
Cys-Cys-Compound A S3 uptake by NAT β-lyase
Reactive thiol
Ochratoxin/Citrinin: Porcine Mycotoxin Nephropathy, Balkan Endemic Nephropathy.
• Produces PCT damage in acute exposure and renal carcinogenesis on chronic exposure.
• Cinrinin and ochratoxin produce essentially the same clinical syndromes and are produced by the same fungi: Apsergillus sp. and Penicillium sp. (particularly A. ochraceus, P. verrucosum, P. citrinum).
• Classification of ochratoxins. • Classified A, B and C; A is the most toxic. • Ochratoxin α is the non-toxic product of ochratoxin hydrolysis by rumen and large intestine bacterial metabolism.
Ochratoxin/Citrinin: Porcine Mycotoxin Nephropathy, Balkan Endemic Nephropathy.
• Particular problem in high energy grains, nuts, pepper, coffee, decaying vegetation, ham.
• Ochratoxin A is relatively stable and a significant fraction survives autoclaving and similar treatments.
• Concentrates in PCT due to re-absorption via the OAT system.
• Also competes with PAH for transport into the PCT epithelium.

49
Ochratoxin/Citrinin: Porcine Mycotoxin Nephropathy, Balkan Endemic Nephropathy.
• Mechanisms of action:
• Damages the mitotic spindle
• Inhibition of phenylalanine metabolism à results are: suppression of DNA, RNA and protein synthesis; suppression of renal gluconeogenesis due to inhibition of phosphoenolpyruvate carboxykinase (the major rate-limiting enzyme in this pathway)
• Promotion of lipid peroxidation
Ochratoxin/Citrinin: Porcine Mycotoxin Nephropathy, Balkan Endemic Nephropathy.
• Mechanisms of action:
• Competitive inhibitor of mitochondrial carrier proteins à suppression of mitochondrial respiration à ATP depletion
• Immunosuppression due to inhibition of lymphocyte proliferation and NK-cell function
• Teratogen in rodents
• Necrosis of tonsils and lymphoid tissues (particularly germinal centers) in dogs
NSAID Nephropathy.
• 2 basic diseases: • Damage to the loop of Henle and renal papilla due to NSAID-induced ischemia
• Immune-mediated interstitial nephritis
• Mechanism of loop of Henle/renal papilla injury (acute overdose)
• Blood flow in the renal medulla (vasa recta and renal papilla) is dependent on PgE2-mediated vasodilation. • NSAIDs inhibit COX resulting in decreased PgE2 à vasoconstriction à ischemia • Because of high oxygen demand, the thick ascending limb of the loop of Henle is particularly sesitive

50
NSAID Nephropathy.
• Mechanism of loop of NSAID interstitial nephritis:
• Immune-mediated hypersensitivity reaction to the NSAID.
• Initial target is the inerstitial tissues although immune complex deposition in the gomeruli may eventually occur.
• Concurrent treatment with caffeine and acetominophen seem to promote the problem.
Acute NSAID Interstitial Nephritis
Lead Nephropathy.
• High blood levels results in lead excretion in urine.
• Accumulates as a lead-protein complex in the nuclei of PCT epithelium à lead inclusions.
• Produces degeneration/necrosis of the PCT.

51
Lead intranuclear inclusion in the PCT epithelium
Case Studies
152





























