Embed Size (px)
Citation preview

PIERPaediatric Innovation, Education
& Research Network
Relevant or Red Herring?
‘Moving on Up Together’ Study Day
31.01.20
M RajaPaediatric Nephrology
Registrar
A NagraPaediatric Nephrology
Consultant

PIERPaediatric Innovation, Education
& Research Network
Case
§ EJW § 16y § Creatinine 120micromol/l - incidental
finding § Repeat 144 micromol/l § NFAW

PIERPaediatric Innovation, Education
& Research Network
November 2017• Phone call
from local hospital
• Creatinine rising - 200micromol/l
• Normal Autoimmune screen locally
• Urgent Outpatient review arranged
March 2018• Review in OP • Creatinine improved
150mircromol/l • Autoimmune screen:
• Bordeline CTD • Complement screen
normal• Nucleosome antibodies
– ‘positive’ -106 U/ml • Discussion with
immunologist and MDT - ?non specific advise to repeat
Late March 2018 UpperGI endoscopy• Creatinine
195micromol/l
• Renal team not aware
August 2018 : OP review• Creatinine
145micromol/l
• microalbuminuria – enalapril commenced
Novemeber 2018: • Creatinine
186 micromol/l
• Nucleosome antibodies 138.4U/ml
• Renal Biopsy • MMF and
prednisolone commenced
Urinalysis: no haematuria, no proteinuria on dipstick

PIERPaediatric Innovation, Education
& Research Network
Jan 2019 • Creatinine 168 micromol/l
• CTD negative • Nucleosome 45.5U/ml
• Enalapril for protienuria
• Continuing on MMF and Prednisolone weaning regim
April 2019 • Creatinine 155 micromol/l
• Nucelosome antibodies 44.54u/ml
• Continues on MMF• Enalapril for proteinuria
July 2019 • Creatinine 200 micromol/l
• Nucelosome antibodies 11.5 U/ml
• ?compliance issues
On regular MMF and enalapril
November 2019 • Creatinine 193micromol/l
• Nucelosome antibodies 15.5u/ml
• MMF
Jan 2020 • Creatinine 171 micromol/l
• MMF
Urinalysis: no haematuria, no proteinuria on dipstick

PIERPaediatric Innovation, Education
& Research Network
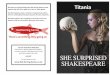
0
50
100
150
200
250
Renal function and Antibody Titres
Nucleosome Antibody titres (U/mL) Serum Creatinine (micromol/L) eGFR (ml/min/1.3m2)
Renal Biopsy --> MMF+Pred
Compliance issues
Normal range 20 -40 U/mL

PIERPaediatric Innovation, Education
& Research Network
Other relevant investigations Urine dipstick – no blood , no protein
Renal ultrasound scans – normal
Complement screen – normal
ESR 30-50; normal CRPs
dsDNA negative
Upper GI endoscopy – normal

PIERPaediatric Innovation, Education
& Research Network
Histopathology November 2018

PIERPaediatric Innovation, Education
& Research Network
EM Results

PIERPaediatric Innovation, Education
& Research Network
22/08/2019

PIERPaediatric Innovation, Education
& Research Network
GeneticsNPHP4 c.3368_3369del p.(Val1123Glyfs*43); heterozygous -Likely pathogenic -Predicted to cause premature termination of NPHP4 protein
NPHP4 c.3920T>C p.(Leu1307Pro)-VUS but in silico predicts pathogenic-Uncertain clinical significance
• Results from parents • RELEVANT or RED HERRING?

PIERPaediatric Innovation, Education
& Research Network

PIERPaediatric Innovation, Education
& Research Network

PIERPaediatric Innovation, Education
& Research Network
“determining circulating anti-nucleosome antibody levels has higher sensitivity for lupus flares than other markers such as anti-dsDNA and can be detected in serum of SLE patients in strict concomitance with the abrupt onset of the disease”

PIERPaediatric Innovation, Education
& Research Network
• Systematic review • 1 x metanalysis • Anti- nucleosome antibodies, in Dx of SLE
• Sensitivity 61% • Specificity of 94%

PIERPaediatric Innovation, Education
& Research Network
Differential Diagnoses
Differential diagnosis
Nephronopthisis Lupus Nephritis Ig-G4 related renal disease

PIERPaediatric Innovation, Education
& Research Network
Red Herring or Relevant?
Nucleosome antibodies –
initial positivity- negative after
MMF Rx
CTD screen – ANA initially ‘borderline’ +
positive
cyclical vomiting; polyuria;
headaches;
NPHP4 mutationX2 variants
Renal biopsy - immune complex
mediated GN

PIERPaediatric Innovation, Education
& Research Network
Management Summary Further biopsy
staining for IgG4 – outcome?
negative IH not IgG4 -
related renal disease
MMF and weaning course Prednisolone commenced
(16/01/2019)
d/w vasculitis expert and
rheumatologist Since commencing MMF – repeat
nucleosome antibody screen negativecontinues on
MMF
Albuminuriaongoing ,
continues on enalapril
NPHP4 mutation ? Significance ?proteinuria parents tested -
Psychosocial support
ongoing cyclical vomiting, polyuria
compliance transition to adult care 2020

PIERPaediatric Innovation, Education
& Research Network
Apart from her kidneys…
Episodic vomiting Discharged from gastroenterology, no cause found specifically
Headaches No organic cause foundEEG normal , MRI normal ?seizures
Compliance with medications Polyuria > Polydipsia Endocrine referral to exclude all organic
causes; No joint pain/swellingsNo rashes

PIERPaediatric Innovation, Education
& Research Network
MDT
• Youth Workers – psychosocial support and help with transition
• Paediatric Nephrologist• Adult Nephrologist• Immunologist• Rheumatology • Endocrinology• CAHMS • Counselling from Bernados

PIERPaediatric Innovation, Education
& Research Network
Learning Points Renal limited lupus: In CKD cases with borderline/positive CTD screen – anti-nucleosome antibodies may be ‘relevant’
• in the absence of systemic features • dsDNA negative
Nucleosome antibodies -Not widely used
• not available in all labs• not a routine test
When treatment commenced, Nucleosome antibody levels decrease
• ?significance

PIERPaediatric Innovation, Education
& Research Network
Relevant?.. Or Red herring?
Nephronopthisis Lupus nephritisGenetics Nucleosome antibodiesPolyuria, Vomiting -episodic IV rehydration
Initially borderline CTD screen
Albuminuria but <30mg/mmol Immune complex process on biopsy
Presentation Presentation
Psychological overlay : • Polyuria• Cyclical nature of vomiting episodes • Compliance issues

PIERPaediatric Innovation, Education
& Research Network
Differential diagnoses
Nephronopthisis Lupus NephritisIg-G4 related renal disease

PIERPaediatric Innovation, Education
& Research Network
References 1Maziad AS, Torrealba J, Seikaly MG, Hassler JR, Hendricks AR. Renal-limited “lupus-like” nephritis: How much of a lupus. Case reports in nephrology and dialysis. 2017;7(2):43-8. 2Huerta A, Bomback AS, Liakopoulos V, Palanisamy A, Stokes MB, D’Agati VD, Radhakrishnan J, Markowitz GS, Appel GB. Renal-limited ‘lupus-like’nephritis. Nephrology Dialysis Transplantation. 2012 Jun 1;27(6):2337-42 3Simmons SC, Smith ML, Chang-Miller A, Keddis MT. Antinuclear antibody-negative lupus nephritis with full house nephropathy: a case report and review of the literature. American journal of nephrology. 2015;42(6):451-9. 4Min DJ, Kim SJ, Park SH, Seo YI, Kang HJ, Kim WU, Cho CS, Kim HY. Anti-nucleosome antibody: significance in lupus patients lacking anti-double-stranded DNA antibody. Clinical and experimental rheumatology. 2002 Jan 1;20(1):13-8. 5Ghiggeri GM, D’Alessandro M, Bartolomeo D, Degl’Innocenti ML, Magnasco A, Lugani F, Prunotto M, Bruschi M. An Update on Antibodies to Necleosome Components as Biomarkers of Sistemic Lupus Erythematosus and of Lupus Flares. International journal of molecular sciences. 2019 Jan;20(22):5799. 6Bizzaro N, Villalta D, Giavarina D, Tozzoli R. Are anti-nucleosome antibodies a better diagnostic marker than anti-dsDNA antibodies for systemic lupus erythematosus? A systematic review and a study of metanalysis. Autoimmunity reviews. 2012 Dec 1;12(2):97-106.

PIERPaediatric Innovation, Education
& Research Network
![DRAFT RED HERRING PROSPECTUS - Cmlinks.com RED HERRING PROSPECTUS Dated [ ] Please read Section 60B of the Companies Act, 1956 (The Draft Red Herring Prospectus will be updated upon](https://img.pdfslide.us/doc/110x75/5aaddf3f7f8b9a3a038b7820/draft-red-herring-prospectus-red-herring-prospectus-dated-please-read-section.jpg)