Embed Size (px)
Citation preview
Release Consent Form YMCA STORER CAMPS
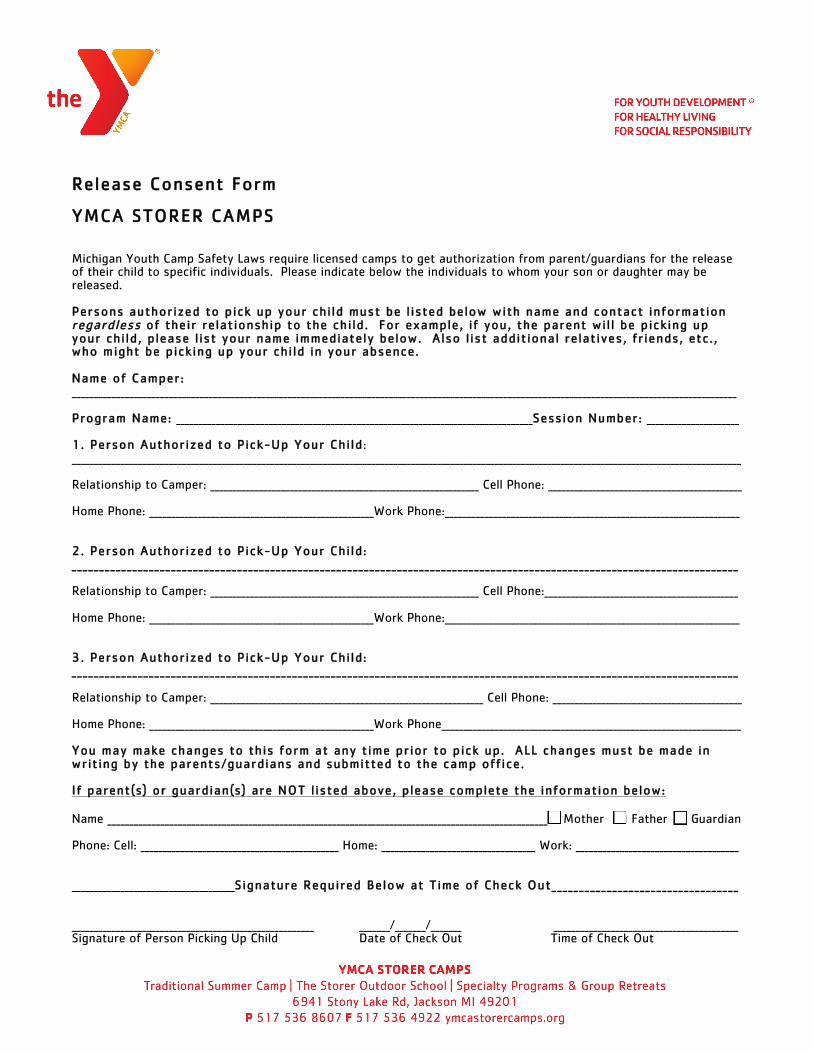
Michigan Youth Camp Safety Laws require licensed camps to get authorization from parent/guardians for the release of their child to specific individuals. Please indicate below the individuals to whom your son or daughter may be released. Persons authorized to pick up your chi ld must be l isted below with name and contact information regardless of their relationship to the child. For example, if you, the parent wil l be picking up your chi ld, please l ist your name immediately below. Also l ist additional relatives, fr iends, etc. , who might be picking up your chi ld in your absence. Name of Camper: _______________________________________________________________________________________________________________________________________________________ Program Name: _________________________________________________________________________________Session Number: _____________________ 1. Person Authorized to Pick-Up Your Child: ________________________________________________________________________________________________________________________________________________________ Relationship to Camper: _____________________________________________________________ Cell Phone: ____________________________________________ Home Phone: ___________________________________________________Work Phone:___________________________________________________________________ 2. Person Authorized to Pick-Up Your Child: _________________________________________________________________________________________________________________________ Relationship to Camper: _____________________________________________________________ Cell Phone:____________________________________________ Home Phone: ___________________________________________________Work Phone:___________________________________________________________________ 3. Person Authorized to Pick-Up Your Child: _________________________________________________________________________________________________________________________ Relationship to Camper: ______________________________________________________________ Cell Phone: ___________________________________________ Home Phone: ___________________________________________________Work Phone____________________________________________________________________ You may make changes to this form at any time prior to pick up. ALL changes must be made in writing by the parents/guardians and submitted to the camp office. If parent(s) or guardian(s) are NOT l isted above, please complete the information below: Name ____________________________________________________________________________________________________! Mother ! Father ! Guardian Phone: Cell: _____________________________________________ Home: ___________________________________ Work: _____________________________________ _____________________________________Signature Required Below at Time of Check Out__________________________________ _______________________________________________________ _______/_______/_______ __________________________________________ Signature of Person Picking Up Child Date of Check Out Time of Check Out
Page 1 of 4
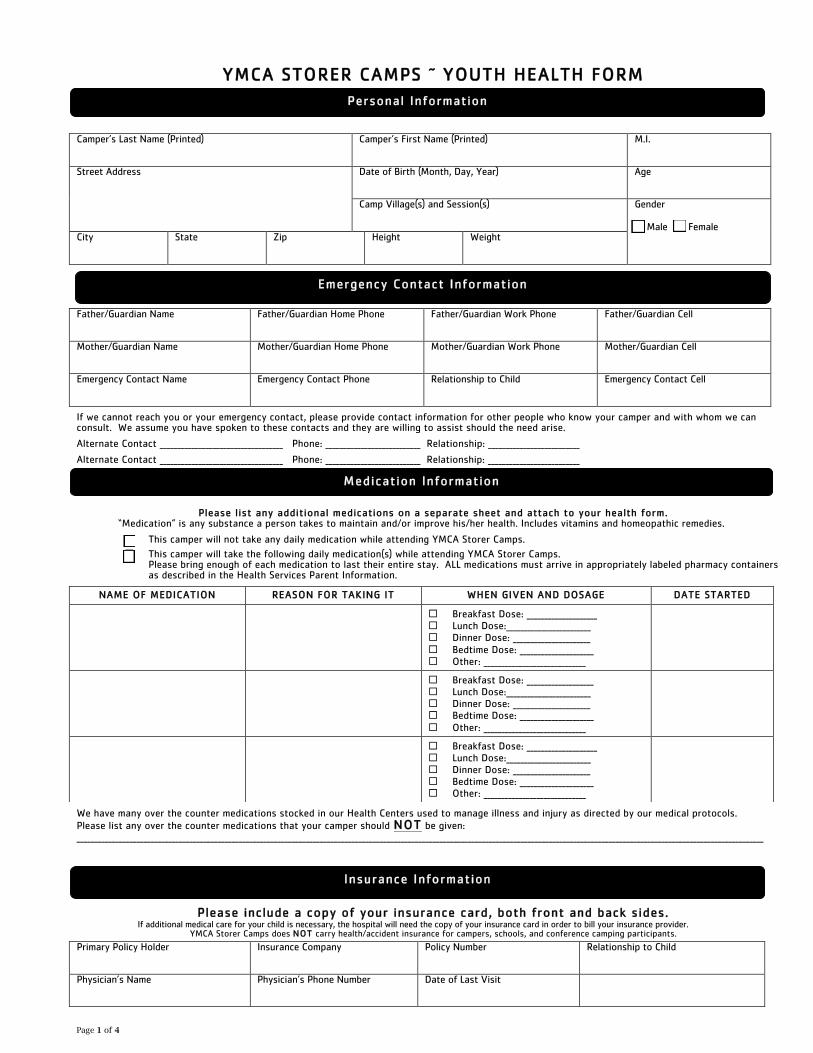
YMCA STORER CAMPS ~ YOUTH HEALTH FORM
Camper’s Last Name (Printed)
Camper’s First Name (Printed) M.I.
Street Address
Date of Birth (Month, Day, Year)
Age
Camp Village(s) and Session(s)
Gender ! Male ! Female
City
State Zip Height Weight
We will certainly call in an emergency, but we’ll also call if we have questions about your camper’s health.
Father/Guardian Name
Father/Guardian Home Phone Father/Guardian Work Phone Father/Guardian Cell
Mother/Guardian Name
Mother/Guardian Home Phone Mother/Guardian Work Phone Mother/Guardian Cell
Emergency Contact Name
Emergency Contact Phone Relationship to Child Emergency Contact Cell
If we cannot reach you or your emergency contact, please provide contact information for other people who know your camper and with whom we can consult. We assume you have spoken to these contacts and they are willing to assist should the need arise.
Alternate Contact ___________________________________ Phone: ___________________________ Relationship: __________________________
Alternate Contact ___________________________________ Phone: ___________________________ Relationship: __________________________
Please list any additional medications on a separate sheet and attach to your health form.
“Medication” is any substance a person takes to maintain and/or improve his/her health. Includes vitamins and homeopathic remedies.
" This camper will not take any daily medication while attending YMCA Storer Camps.
" This camper will take the following daily medication(s) while attending YMCA Storer Camps. Please bring enough of each medication to last their entire stay. ALL medications must arrive in appropriately labeled pharmacy containers as described in the Health Services Parent Information.
We have many over the counter medications stocked in our Health Centers used to manage illness and injury as directed by our medical protocols. Please list any over the counter medications that your camper should NOT be given: ___________________________________________________________________________________________________________________________________________________________________________________________________
Please include a copy of your insurance card, both front and back sides. If additional medical care for your child is necessary, the hospital will need the copy of your insurance card in order to bill your insurance provider.
YMCA Storer Camps does NOT carry health/accident insurance for campers, schools, and conference camping participants.
Primary Policy Holder
Insurance Company Policy Number Relationship to Child
Physician’s Name
Physician’s Phone Number Date of Last Visit
NAME OF MEDICATION REASON FOR TAKING IT WHEN GIVEN AND DOSAGE DATE STARTED
" Breakfast Dose: ____________________ " Lunch Dose:________________________ " Dinner Dose: ______________________ " Bedtime Dose: _____________________ " Other: _____________________________
" Breakfast Dose: ___________________ " Lunch Dose:________________________ " Dinner Dose: ______________________ " Bedtime Dose: _____________________ " Other: _____________________________
" Breakfast Dose: ____________________ " Lunch Dose:________________________ " Dinner Dose: ______________________ " Bedtime Dose: _____________________ " Other: _____________________________
Personal Information
Emergency Contact Information
Medication Information
Insurance Information
Camper Name:__________________________________________________________________________
Page 2 of 4
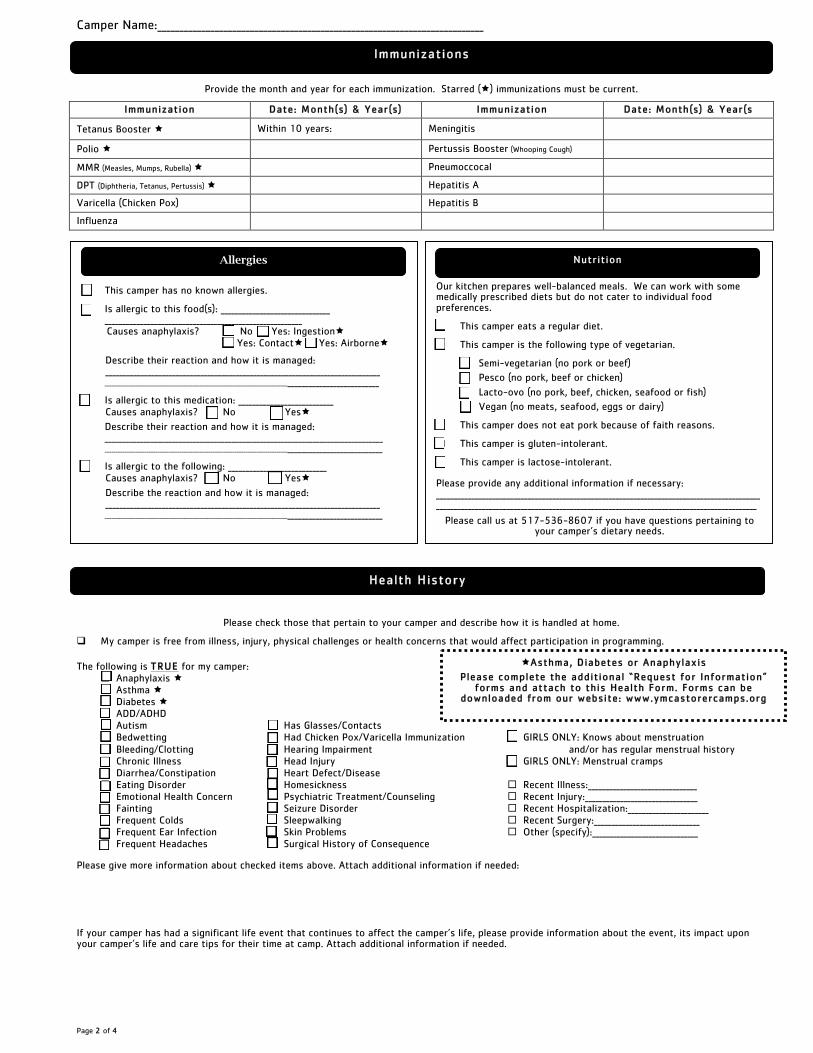
Provide the month and year for each immunization. Starred (!) immunizations must be current.
Immunization Date: Month(s) & Year(s) Immunization Date: Month(s) & Year(s
Tetanus Booster ! Within 10 years: Meningitis
Polio ! Pertussis Booster (Whooping Cough)
MMR (Measles, Mumps, Rubella) ! Pneumoccocal
DPT (Diphtheria, Tetanus, Pertussis) ! Hepatitis A
Varicella (Chicken Pox) Hepatitis B
Influenza
Please check those that pertain to your camper and describe how it is handled at home.
# My camper is free from illness, injury, physical challenges or health concerns that would affect participation in programming.
The following is TRUE for my camper: " Anaphylaxis ! " Asthma ! " Diabetes ! " ADD/ADHD " Autism " Has Glasses/Contacts " Bedwetting " Had Chicken Pox/Varicella Immunization " GIRLS ONLY: Knows about menstruation " Bleeding/Clotting " Hearing Impairment and/or has regular menstrual history " Chronic Illness " Head Injury " GIRLS ONLY: Menstrual cramps " Diarrhea/Constipation " Heart Defect/Disease " Eating Disorder " Homesickness " Recent Illness:_______________________________ " Emotional Health Concern " Psychiatric Treatment/Counseling " Recent Injury:________________________________ " Fainting " Seizure Disorder " Recent Hospitalization:_______________________ " Frequent Colds " Sleepwalking " Recent Surgery:______________________________ " Frequent Ear Infection " Skin Problems " Other (specify):______________________________ " Frequent Headaches " Surgical History of Consequence
Please give more information about checked items above. Attach additional information if needed:
If your camper has had a significant life event that continues to affect the camper’s life, please provide information about the event, its impact upon your camper’s life and care tips for their time at camp. Attach additional information if needed.
Allergies
# This camper has no known allergies.
# Is allergic to this food(s): _______________________________ ________________________________________________________ Causes anaphylaxis? " No " Yes: Ingestion!
" Yes: Contact! " Yes: Airborne!
Describe their reaction and how it is managed: ______________________________________________________________________________
_____________________________________________________________________________________________________________
# Is allergic to this medication: ___________________________ Causes anaphylaxis? " No " Yes!
Describe their reaction and how it is managed: _______________________________________________________________________________ ______________________________________________________________________________________________________________
# Is allergic to the following: ____________________________ Causes anaphylaxis? " No " Yes!
Describe the reaction and how it is managed: ______________________________________________________________________________
______________________________________________________________________________________________________________
Our kitchen prepares well-balanced meals. We can work with some medically prescribed diets but do not cater to individual food preferences.
# This camper eats a regular diet.
# This camper is the following type of vegetarian.
" Semi-vegetarian (no pork or beef)
" Pesco (no pork, beef or chicken)
" Lacto-ovo (no pork, beef, chicken, seafood or fish)
" Vegan (no meats, seafood, eggs or dairy)
# This camper does not eat pork because of faith reasons.
# This camper is gluten-intolerant.
# This camper is lactose-intolerant. Please provide any additional information if necessary: _______________________________________________________________________________________________________________________________________________________________________________________
Please call us at 517-536-8607 if you have questions pertaining to your camper’s dietary needs.
!Asthma, Diabetes or Anaphylaxis
Please complete the additional “Request for Information” forms and attach to this Health Form. Forms can be
downloaded from our website: www.ymcastorercamps.org
Nutrition
Health History
Immunizations
Camper Name:__________________________________________________________________________
Page 3 of 4
What Else Would You Like Us To Know? Let us know any information about your camper’s health that may have not been covered on this form. Any information that has an impact on your child’s ability to fully participate in our program is appreciated. Attach additional information if needed.
The information contained in this form is correct, as far as I know, and the child herein described has permission to engage in all camp activities except as noted. I understand that health/accident insurance coverage is the responsibility of the parent/guardian. I hereby give permission to YMCA Storer Camps to secure emergency medical, routine medical, surgical treatment, and non-surgical care for the child named on this form, while at camp. I also understand that the parent/guardian is fully responsible for the camper’s transportation if he/she is dismissed for disciplinary, behavior or medical reasons. I absolve the YMCA of Greater Toledo/Storer Camps and all of its employees of any and all liability, financial and/or otherwise arising from administration of medication to my child under the terms of this release. YMCA Storer Camps is not responsible for payment of any medical expenses incurred during participation at camp.
In consideration for being allowed to participate in the YMCA’s programs, I agree to assume the risk of such activities and programs, and I further agree to hold harmless the YMCA of Greater Toledo, it’s officers, employees and representatives from any and all claims, suits, losses, or related causes of action for damages, including, but not limited to, such claims that may result from injury or death, accident or otherwise, during or arising in any way from the activities. I grant permission for me or my child to participate in all planned camp activities including out of camp trips by van or bus, hiking or horseback riding. The YMCA is not responsible for lost, stolen or damaged personal articles. I also authorize the YMCA to have and use photographs, slides or video tapes of me, my child, or my family as may be needed for its public relations programs. I acknowledge that this General Release of Liability and Authorization for Treatment of the YMCA is binding on me personally and on my heirs, personal representatives, successors and assigns.
Limited Purpose Power of Attorney: Consent to Treatment of Minor (Must be signed by parent or legal guardian) By signature(s) below, the undersigned appoints YMCA Storer Camps, to act alone, or delegate to another person, the power to consent on our behalf to all emergency treatment and/or medical care (except elective surgery) of (child’s name) ______________________________________ determined to be necessary or desirable by our child’s attending physician at the hospital. This Power of Attorney shall continue through the participant’s stay at camp, or until revoked by the undersigned, whichever is earlier. Physicians or the hospital’s medical staff may assume and rely on this authorization being current and in effect during such period unless notified otherwise. The undersigned certify that they read this Power of Attorney (or had it read to them), that they understand this Power of Attorney, and sign it voluntarily. This agreement will be enforced in accordance with the law of the State of Michigan. Parent/Guardian Signature: ________________________________________ Date: _______________
" Health Office Use Only "
Date Time CHO Notes
We at YMCA Storer Camps want your child to have the best camp experience possible. The more information you are able to give, the better prepared we are to work with your child. Please contact us at (517) 536-8607 if you would like to discuss any concerns. Please tell us a little about your camper.
Additional Information
Parent/Guardian Authorization
Camper Name:__________________________________________________________________________
Page 4 of 4
What goals do you hope your camper to reach at camp? What activities does your camper enjoy? Is there anything your camper has a tendency to be afraid or anxious about? In the case of behavior or conflict, how can we best help your camper to be successful and resolve situations?
Often laugh or smile? " Never " Sometimes " Often " Always
Adjust well to change? " Never " Sometimes " Often " Always
Like group activities? " Never " Sometimes " Often " Always
Have variations in moods? " Never " Sometimes " Often " Always
Become easily frustrated? " Never " Sometimes " Often " Always
Seem sensitive to criticism? " Never " Sometimes " Often " Always
Seem difficult to motivate? " Never " Sometimes " Often " Always
Socialize well with their peers? " Never " Sometimes " Often " Always
All medications should be given to the Health Officer at time of check-in. All medications must be in the original container. All medication will be returned at the end of the stay. NOTE: * Items that can be purchased in our Trading Post
Use this list to help you pack your camper’s luggage. Involving your camper in this process familiarizes him/her with what you are sending to camp. Some items are optional and some are available for purchase at the Trading Post. What to bring to camp will depend on the length of stay and nature of the program. In some cases, there are specialty items that are mandatory for all campers. Please note these items carefully. All items brought to camp should be clearly marked with the camper’s first and last name.
� Sleeping Bag � � Sheets / Blanket � � Pillow �
� Underwear (daily change) � � Socks (daily change) � � Shorts � � Sweatshirt*/ Sweater � � T-shirts (daily change)* � � Jeans / Sweat Pants (2 pair) � � Long Sleeve Shirt* � � Light Jacket / Coat � � Raincoat (If riding horses no ponchos) � � Pajamas � � Swimsuit (one piece) / Trunks � � Shoes / Hiking Boots � � Sandals / Shoes that can get wet � � Hat / Baseball Cap* �
� Shampoo* � � Soap* � � Toothpaste & Toothbrush* � � 2 Towels � � Washcloths � � Laundry Bag � � Insect Repellent * � � Sunscreen* � � Sunglasses � � Water Bottle* �
� White T-shirt for Tye-Dyeing � � Stationary / Envelopes / Stamps* � � Books / Magazines � � Flashlights* � � Camera /Film (disposable type is best)* � � Stuffed Animal* � � Fitted Sheet for Bunk Bed �
� Wool Socks (2 or 3 pair) � � Long Underwear / Sweatpants � � Day Pack / Small Duffel Bag � � Extra Tennis Shoes (that can get wet) �
� Riding boots or close-toed boots � w/ small heel and a smooth sole. � Work Gloves (used for feeding) �
� English Riders: Riding boots � or close-toed boots w/ small heel and a smooth sole.
� Western Riders: Closed-toed shoe � with closed heel
� Long pants �
Electronic Games/CD Player/Walkman
MP3 Players/Digital Cameras/Knives/Weapons Food / Candy/Tobacco/Drugs/ipods
Cell Phones / Pagers (including Camera Phone
1/10/2014
: YMCA Storer Camps staff can arrange to pick up and drop off campers at the Detroit Metropolitan Airport. A staff member, wearing a YMCA Storer Camps staff shirt will meet the incoming camper(s) and take them to camp via a Storer Camps vehicle. On the return, a staff member will take each camper to their flight.
With heightened airport security, please check with your airlines for any additional travel requirements for dropping off/picking up un-accompanied minor children including any documentation required by the airline stating YMCA Storer Camps has your permission to pick up your child. Please call us at least two weeks prior to your camper’s arrival with specific instructions.
. The cost for this service is $50.00 per camper, each way. Registration and fees should be confirmed as early as possible, and at least two weeks prior to the campers arrival. Be sure to indicate this fee on your fee payment card and return along with this completed form
: YMCA Storer Camps staff can arrange to pick up and drop off campers in Jackson, Michigan Bus or Train Stations. A staff member, wearing a staff shirt will meet the incoming camper(s) and take them to camp. On return, a staff member will take them to their bus or train. Transportation time to the bus or train stations in Jackson, Michigan is approximately 25 minutes. The cost for this service is $15.00 per camper, each way. Registration and fees should be confirmed as soon as possible and at least two weeks prior to the camper’s arrival. Be sure to indicate this fee on your fee payment card and return along with this completed form. *Safety Information*
� If only one camper will be picked up/dropped off, a second Storer Camps staff member will be present. � Seatbelts must be worn in all camp vehicles. � Please contact YMCA Storer Camps at 517-536-8607 if any last minute changes occur. � A Storer Camp representative will contact parent /guardian of any changes on the camper’s return trip.
* * * * * * * COMPLETE THE FOLLOWING INFORMATION AND RETURN TO CAMP BY MAY 15. * * * * * * * *
1/13/2014
Everyone at YMCA Storer Camps wants your child to have the best camp experience possible. To help in this effort, we ask for parents to fill out this form only if there are special concerns or situations that you feel we need to know. The more information you are able to give, the better prepared we are to work with your child. Please feel free to contact the Summer Camp Director at (800)536-8607 if you would rather discuss this over the phone. Camper Name:_______________________________________________Program/Session:_______________________________________ Parent/Guardian Name:___________________________________________________ Phone:____________________________________ What information do we need to know? (Please use the back or additional pages if needed) ______________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________________
Parent Signature:______________________________________________________________Date:__________________________________