Embed Size (px)
Citation preview

Clinical Study Protocol
International randomized phase III study on the treatment of children and adolescents with refractory or relapsed
acute myeloid leukemia
Pediatric Relapsed AML 2010/01
To be performed within the International BFM Study Group (I-BFM-SG) and the International
Pediatric AML Group
Sponsor: Gesellschaft für Pädiatrische Onkologie und Hämatologie gGmbH
Society of Pediatric Hematology and Oncology gGmbH
Hufelandstr. 17
47147 Essen
Germany
International Study Coordinators (steering committee):
G.J.L. Kaspers (chair, I-BFM-SG)
D. Reinhardt (co-chair, Germany and I-BFM-SG)
A. Baruchel (France)
C. Rizzari (Italy)
B. Gibson (UK)
International data manager and statistician (also member of the steering committee):
M. Zimmermann
AML-BFM Group
Hannover, Germany
EudraCT number: 2010-018980-41
Protocol code number: Pediatric_Relapsed_AML2010/01
Version number: 6.2.1
Version date: 20.09.2016
- Confidential -

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 2 of 66
International study coordinators (steering committee, together with the international statistician)
Gertjan J.L. Kaspers
Chairman AML Relapse Working Group/I-BFM-
SG
Pediatric Oncology/Hematology
VU University Medical Center
De Boelelaan 1117
NL-1081 HV Amsterdam
The Netherlands.
Phone: +31 (0) 20 444 2420
Fax: +31 (0) 20 444 2422
E-mail: [email protected]
Dirk Reinhardt
Chairman AML committee/I-BFM-SG
BFM-AML representative
University Hospital Essen
Pediatric Hematology and Oncology
Hufelandstr. 55
47147 Essen
Germany
Phone:+49 (0) 723 3755
Fax: +49 (0) 723 5308
E-mail: [email protected]
Carmelo Rizzari
AIEOP representative
Pediatric Oncology/Hematology
Clinica Pediatrica, Ospedale S. Gerardo
Via Donizetti, 106
20052 Monza
Italy
Phone: +39 (0) 39 233 3513
Fax: +39 (0) 39 230 1646
E-mail: [email protected]
Andre Baruchel
FRALLE/LAME representative
University Paris Diderot and
Department of Hematology-
Immunology, Hôpital Robert
Debré
48 Bd Sérurier
75019 Paris, France
Phone:+33 1 40 03 53 88
Fax: +33 1 40 03 47 40
E-Mail: [email protected]
Martin Zimmermann, PhD (International
Statistician)
AML-BFM Trial Center
Hannover Medical School, Children's Hospital
Carl-Neuberg-Str. 1
D-30625 Hannover
Germany
Phone: +49 (0) 511 532 3764
+49 (0) 511 532 9123
Fax: +49 (0) 511 532 9029
E-mail: zimmermann.martin@mh-
hannover.de
Brenda Gibson
UK representative
Pediatric Hematology
Royal Hospital for Sick Children
Dalnair Street
Glasgow, G3 8SJ
UK
Phone: 0044 (0)141 201 0395
Fax: 0044 (0)141 201 0857
Switchboard: 0044 (0)141 201 0000
E-mail: [email protected]
Prof. Owen Smith
Irish Representative
Paediatic Haematology
Our Lady’s Children’s Hospital, Crumlin
Dublin 12
Ireland
Phone: 00353 1 4096720
Fax: 00353 1 4563041
Email:[email protected]

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 3 of 66
Central Data Office:
Martin Zimmermann, PhD (Statistician)
Jans-Enno Müller, (Documentation)
Katharina Waack (Project Management)
AML-BFM Trial Center
University Children’s Hospital
Department of Paediatric Haematology and Oncology
Hufelandstr. 55
D-47147 Essen
Germany
Phone: +49 (0) 511 532 3764 (M. Zimmermann)
+49 (0) 201 74949611 (K.Waack)
Fax: +49 (0) 201 87775484
E-mail: [email protected]
Reference Laboratory:
Dirk Reinhardt
University Hospital Essen
Pediatric Hematology and Oncology
Hufelandstr. 55
47147 Essen
Germany
Phone:+49 (0) 723 3755
Fax: +49 (0) 723 5308
E-mail: [email protected]

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 4 of 66
Principal investigators other participating groups
NCRI, United Kingdom Brenda Gibson, Glasgow
AIEOP, Italy Franco Locatelli, Rom
BFM-A, Austria Michael Dworzak, Vienna
BFM-G, Germany Dirk Reinhardt, Hannover
BSPHO (Belgium) Barbara de Moerloose, Ghent
CPH, Czech Republic Jan Stary, Prague
Croatia Josip Konja, Zagreb
DCOG, the Netherlands, Michel Zwaan, Rotterdam
Greece Helen Kosmidis, Athens
Hungary Gabor Kovac, Budapest
Ireland Prof. Owen Smith, Dublin
LAME (France) Guy Leveger, Paris
NOPHO, Nordic countries Jonas Abrahamsson, Göteborg
PPLLSG, Poland Walentyna Balwierz, Krakow
Serbia Dragana Janic, Belgrad
Slovakia Alexandra Kolenova, Bratislava
Slovenia Janez Jazbec, Ljubljana
SHOP, Spain Amparo Verdeguer, Valencia
SPOG, Switzerland Jean-Pierre Bourquin, Zurich

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 5 of 66
1 Contents
1 Contents ................................................................................................................................................... 5
2 Protocol Synopsis ...................................................................................................................................... 8
2.1 Flowchart ................................................................................................................................................ 14
2.2 Signature Pages ....................................................................................................................................... 15
2.3 Confidentiality Statement/ Disclaimer .................................................................................................... 17
2.4 Patient Insurance .................................................................................................................................... 17
2.5 List of Abbreviations ............................................................................................................................... 18
3 Summary ................................................................................................................................................. 20
3.1 Background and Introduction.................................................................................................................. 21
3.2 Gemtuzumab Ozogamicin (GO) (Mylotarg®) ............................................................................................ 21
3.2.1 Pharmacology and Pharmacodynamics ................................................................................................... 21
3.2.2 Pharmacokinetics .................................................................................................................................... 21
3.2.3 Approval Status....................................................................................................................................... 23
3.2.4 Clinical Studies ........................................................................................................................................ 23
3.2.5 Adverse Reactions (AR) / Toxicity ........................................................................................................... 26
3.3 FLA + Liposomal Daunorubicin (DX-FLA) .................................................................................................. 27
3.4 FLA .......................................................................................................................................................... 27
3.5 Other Reinduction Chemotherapy Regimens .......................................................................................... 27
3.6 Central Nervous System (CNS) Prophylaxis and Treatment ..................................................................... 28
3.7 Consolidation Chemotherapy and Stem Cell Transplantation (SCT) ......................................................... 28
3.8 Salvage Treatment .................................................................................................................................. 29
3.9 Translational Research, Add-on Studies .................................................................................................. 29
3.10 Conclusion / Risk-Benefit Ratio ............................................................................................................... 29
4 Study Objectives ..................................................................................................................................... 30
4.1 Primary Study Objective.......................................................................................................................... 30
4.2 Secondary Study Objectives .................................................................................................................... 30
5 Study Design ........................................................................................................................................... 31
5.1 Therapy Optimization Study ................................................................................................................... 31
5.2 Study Time Schedule ............................................................................................................................... 31
5.3 Number of Subjects ................................................................................................................................. 31
5.4 Inclusion Criteria ..................................................................................................................................... 31
5.5 Exclusion Criteria .................................................................................................................................... 31
6 Definitions .............................................................................................................................................. 33
6.1 Relapse ................................................................................................................................................... 33
6.1.1 Early Relapse ........................................................................................................................................... 33
6.1.2 Late Relapse ............................................................................................................................................ 33
6.1.3 Molecular Relapse .................................................................................................................................. 33
6.2 CNS Disease ............................................................................................................................................ 33
6.3 Response ................................................................................................................................................ 33
6.3.1 CR/CR but with Incomplete Regeneration (CRi) ...................................................................................... 33
6.3.2 Early Death ............................................................................................................................................. 34
6.3.3 Toxic Death ............................................................................................................................................. 34
6.3.4 Partial Remission .................................................................................................................................... 34
6.3.5 Early Treatment Response ...................................................................................................................... 34
6.3.6 Refractory Disease/Non-Response .......................................................................................................... 34

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 6 of 66
6.4 2nd Relapse ............................................................................................................................................ 34
7 Diagnostics .............................................................................................................................................. 35
7.1 Diagnostics before Start of Treatment .................................................................................................... 35
7.2 During the First Treatment Course .......................................................................................................... 35
7.3 Before the Start of the Second and Subsequent Treatment Courses ....................................................... 35
7.4 Cardiotoxicity Monitoring ....................................................................................................................... 36
8 Treatment Schedule ................................................................................................................................ 37
8.1 General Information ............................................................................................................................... 37
8.2 Dose Reduction for Children < 12 months or < 12 kg ............................................................................... 37
8.3 Special Measures for Reinduction ........................................................................................................... 37
8.3.1 Hyperleukocytosis, High Blast Cell Counts ............................................................................................... 37
8.4 Cytarabine .............................................................................................................................................. 38
8.5 Gemtuzumab Ozogamicin (GO, Mylotarg®) ............................................................................................. 38
8.6 Irradiation of Blood Products .................................................................................................................. 38
8.7 First Reinduction Course DX-FLA + GO (Mylotarg®) ................................................................................. 39
8.8 First Reinduction Course DX-FLA ............................................................................................................. 40
8.9 Second Reinduction Course FLA .............................................................................................................. 41
8.10 Consolidation -high intensity .................................................................................................................. 42
8.11 Consolidation – low intensity .................................................................................................................. 43
8.12 CNS Prophylaxis and treatment .............................................................................................................. 44
8.12.1 CNS-Prophylaxis .................................................................................................................................. 44
8.12.2 CNS treatment .................................................................................................................................... 44
8.13 Stem cell transplantation ........................................................................................................................ 44
8.14 Indications for SCT: ................................................................................................................................. 44
8.15 Premature Termination of the Study....................................................................................................... 45
9 Drug Information, Expected Toxicity and Dose Adjustments ................................................................... 46
9.1 Cytarabine .............................................................................................................................................. 46
9.2 Fludarabine ............................................................................................................................................. 46
9.3 Gemtuzumab Ozogamicin (GO, Mylotarg®) ............................................................................................. 46
9.4 Liposomal Daunorubicin (L-DNR/DX) ...................................................................................................... 47
9.5 Prednisolon ............................................................................................................................................. 47
9.6 Methotrexate .......................................................................................................................................... 47
9.7 Thioguanin .............................................................................................................................................. 47
9.8 VP-16 (Etoposide) ................................................................................................................................... 48
9.9 Source of Chemotherapeutic Drugs/IMP and Labelling ........................................................................... 49
10 Statistical Considerations and Randomization Procedure ....................................................................... 50
10.1 Endpoints ................................................................................................................................................ 50
10.2 Analysis ................................................................................................................................................... 50
10.3 Sample Size ............................................................................................................................................. 51
10.4 Interim and Final Analysis ....................................................................................................................... 51
10.5 Data Management .................................................................................................................................. 52
10.6 Data Monitoring Committee (DMC) ........................................................................................................ 52
11 Safety Evaluation .................................................................................................................................... 54
11.1 Definitions .............................................................................................................................................. 54
11.1.1 Adverse Event (AE) ............................................................................................................................. 54
11.2 Documentation and Evaluation of Adverse Events .................................................................................. 55

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 7 of 66
11.3 Documentation and Reporting of Serious Adverse Events ...................................................................... 56
11.4 SAE Reporting after the End of Trial Treatment ...................................................................................... 56
11.5 SAE Reporting Procedures and Time Limits ............................................................................................. 56
11.6 Pregnancies ............................................................................................................................................. 56
11.7 Events Associated with Pharmaceutical Quality ...................................................................................... 57
11.8 Overdosing .............................................................................................................................................. 57
11.9 SUSAR Reporting Procedures and Time Limits ........................................................................................ 57
11.10 Annual Safety Reporting ..................................................................................................................... 57
12 Publication and Other Policies ................................................................................................................ 58
12.1 Authors on Abstracts and Manuscripts ................................................................................................... 58
12.2 Acknowledgements in Manuscripts ........................................................................................................ 58
12.3 Other Guidelines ..................................................................................................................................... 58
13 Ethical, Regulatory and Administrative Aspects ...................................................................................... 59
13.1 Responsibilities ....................................................................................................................................... 59
13.2 Favorable Opinion of Independent Ethics Committee (IEC) and Approval of National Competent
Authority (NCA) ................................................................................................................................................... 59
13.3 Patient Information and Informed Consent ............................................................................................ 59
13.4 Data Protection ....................................................................................................................................... 60
13.5 Financing ................................................................................................................................................. 60
14 Sponsors ................................................................................................................................................. 61
15 Monitoring, Audits and Inspections ........................................................................................................ 62
15.1 Monitoring .............................................................................................................................................. 62
15.2 Audits and Inspections ............................................................................................................................ 62
16 Reference List ......................................................................................................................................... 63
17 Appendix ................................................................................................................................................. 66

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 8 of 66
2 Protocol Synopsis
Protocol Title International randomized phase III study on the treatment of children and
adolescents with refractory or relapsed acute myeloid leukemia
Short Term Pediatric Relapsed AML 2010/01
International
Study
Coordinators
(steering
committee,
together with the
international
statistician)
Gertjan J.L. Kaspers (chair)
Chairman AML relapse working group/International BFM Study Group
Head and Professor of Pediatric Oncology/Hematology
VU University Medical Center
De Boelelaan 1117
NL-1081 HV Amsterdam, the Netherlands
Phone: +31 (0) 20 444 2420; fax: +31 (0) 20 444 2422
E-mail: [email protected]
Dirk Reinhardt (co-chair)
Chairman AML committee/I-BFM-SG
BFM-AML representative
University Hospital Essen
Pediatric Hematology and Oncology
Hufelandstr. 55
47147 Essen
Germany
Phone:+49 (0) 723 3755
Fax: +49 (0) 723 5308
E-mail: [email protected]
Andre Baruchel
FRALLE/LAME representative
University Paris Diderot and Department of Hematology-
Immunology, Hôpital Robert Debré
48 Bd Sérurier
75019 Paris, France
Phone:+33 1 40 03 53 88 ; fax: +33 1 40 03 47 40
E-Mail: [email protected]
Carmelo Rizzari
AIEOP representative
Pediatric Oncology/Hematology
Clinica Pediatrica, Ospedale S. Gerardo
Via Donizetti, 106
20052 Monza, Italy
Phone: +39 039 233 3513; Fax: +39 039 230 1646
E-mail: [email protected]
Brenda Gibson
UK NCRI representative
Pediatric Hematology
Royal Hospital for Sick Children
Dalnair Street
Glasgow, G3 8SJ
UK
Phone: 0044 (0)141 201 0395; Fax: 0044 (0)141 201 0857; Switchboard: 0044

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 9 of 66
(0)141 201 0000
E-mail: [email protected]
Prof. Owen Smith
Irish Representative
Paediatic Haematology
Our Lady’s Children’s Hospital, Crumlin
Dublin 12
Ireland
Phone: 00353 1 4096720
Fax: 00353 1 4563041
Email: [email protected]

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 10 of 66
National clinical and
data-management
representatives,
respectively
European groups that can participate:
AIEOP, Italy
BFM-A, Austria
BFM-G, Germany
BSPHO (Belgium)
CPH, Czech Republic
Croatia
DCOG, the Netherlands
Greece
Hungary
Ireland
LAME (France)
NOPHO, Nordic countries
PPLLSG, Poland
Serbia
Slovakia
Slovenia
SHOP, Spain
SPOG, Switzerland
NCRI, United Kingdom
Sponsor GPOH gGmbH
Essen, Germany
International Data-
center
AML-BFM Group
Essen, Germany
International
Statistician
Martin Zimmermann, PhD
AML-BFM Trial Center
Hannover Medical School, Children’s Hospital
Carl-Neuberg-Str. 1
D-30625 Hannover, Germany
Phone: +49 (0) 511 532 3764 / 9020
Fax: +49 (0) 511 532 9029
E-mail: [email protected]
Data Monitoring
Committee
Y. Ravindranath, USA
P. Vyas, UK
H. van Houwelingen, NL
Trial Centers To be appointed by all participating national/local groups
Primary Study
Objective
Determination of the initial efficacy of GO when added to DX-FLA in the first
course of reinduction chemotherapy in children with relapsed or refractory AML
compared to DX-FLA only. Activity will be measured by the percentage of patients
having not more than 20% blasts in the bone marrow (BM) before the second
induction course.
The study will also determine other parameters of clinical outcome in children
with relapsed or refractory AML, as outlined in the secondary study objectives.
Secondary Study
Objectives
1. Determine clinical outcome in both treatment arms, defined as refractory
disease, complete remission rate after 2 reinduction courses, cumulative
incidence of relapse, event-free survival and overall survival.
2. Incidence of treatment related mortality and toxicity of GO (Mylotarg®)
according to the CTCAEv4 when added to DX-FLA, in terms of mucosal toxicity,
BM aplasia, liver toxicity with special respect to the development of VOD, also
called SOS), short- and long-term cardiotoxicity and other adverse reactions, as

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 11 of 66
compared to patients treated with DX-FLA only.
3.Identification of additional prognostic factors in pediatric relapsed AML, other
than early treatment response, cytogenetics and duration of complete remission
(CR)1.
4. To establish a diagnostic and logistic network to obtain an individual
characterization of AML based on morphology, immunophenotype, type I and
type II mutations, signal pathway activation, and monitoring of MRD / treatment
response for individualized stratification to targeted therapy within a short
timeframe.
Study Rationale Pediatric relapsed acute myeloid leukemia (AML) still has a poor prognosis. The
probability of survival at 4 years is 36% in the most recent study Relapsed AML
2001/01{Kaspers, 2012 11493 /id}, which is better than reported before, but not
well enough. Percentage of blasts before 2nd induction (<>20% in bone marrow at
“day 28%) was identified as the strongest predictor of outcome{Kaspers, 2008
11027 /id;Kaspers, 2012 11493 /id}. Further improvements of current treatment
are thus required. GO (Mylotarg®) consists of a calicheamicin conjugated to the
monoclonal CD33 antibody and has proven to be effective in terms of CR
achievement and better OS in adult AML studies and in pediatric AML relapse and
salvage therapy studies with moderate toxicity. Since more than 90% of pediatric
AML are CD33 positive, adding GO to the standard regimen offers a great
potential as targeted therapy for the majority of patients in our study. MRC and
COG studies have shown the feasibility of adding GO at 3 mg/m² for one dose to
either ADE or IDA-FLA induction chemotherapy in adults and children (MRC) and
to mitoxantrone and cytarabine in children (COG) with newly diagnosed AML.
Data on saturation of CD33 in relation to the dose of GO show a dose-dependent
effect, and suggest 4.5 mg/m² to be better than 3.0 mg/m². On the other hand,
GO-associated liver toxicity is clearly dose-dependent as well, with higher toxicity
at doses of 6.0 mg/m² and higher.
The international phase III study Relapsed AML 2001/01 has proven the feasibility
of large intergroup studies in pediatric AML and its results are among the best
ever reported. Therefore, the best arm of the current study, which is the
reinduction course including liposomal daunorubicin, fludarabine, and cytarabine
(DX-FLA) will constitute the standard first reinduction course of chemotherapy.
Adding liposomal daunorubicin (DX) to fludarabine (FL)/cytarabine (A) improved
the early response rate by 11%, from 69 to 80% (p=0.017).
The second reinduction element will be fludarabine/cytarabine (FLA). After
reinduction chemotherapy, all patients are eligible for allo-stem cell
transplantation (SCT). In view of reports on children surviving relapsed AML while
having been treated with chemotherapy or autologous SCT only (1), the use of
very-high risk allo-SCT (such as major mismatched unrelated donor SCT) that will
be associated with a high treatment-related mortality should be carefully
balanced against the possibility of cure with chemotherapy only in rare patients in
very good quality second CR.
Study Relapsed AML 2001/01 showed very poor outcome for patients with a poor
response to the first course of reinduction chemotherapy (>20% blasts), for
patients not achieving CR/CRi, and for patients with subsequent relapse.
Therefore, these patients will be off-study in terms of therapy (but not of follow-
up) and eligible for phase I/II studies with novel agents. However, the outcome of
these patients will be documented.
Study Population Inclusion criteria
1. Children and adolescents < 18 years of age at start of initial chemotherapy and
< 21 years of age at start of this relapsed AML treatment

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 12 of 66
2. Patients with first relapsed (including relapse after SCT) or primary refractory
AML
3. Signed written informed consent from patients and/or from parents or legal
guardians for minor patients, according to local law and regulations
4. In female patients of childbearing potential pregnancy must be excluded.
5. Sexually active patients must be using two reliable contraception methods from
the time of screening/baseline and during the study for a minimum of 3 months
after the last administration of study medication. This includes every combination
of a hormonal contraceptive (such as injection, transdermal patch, implant,
cervical ring) or of an intrauterine device (IUD) with a barrier method (e.g.
diaphragm, cervical cap, or condom) or with a spermicide.
Exclusion criteria
1. Acute promyeloblastic leukemia (AML FAB type M3; please refer to your local
group for the appropriate treatment protocol)
2. Myeloid Leukemia of Down syndrome (please refer to your local group for
treatment alternatives)
3. Symptomatic cardiac dysfunction (CTCAEv4 grade 3 or 4) and/or a Fractional
Shortening at echocardiography below 29%
4. A Karnofsky performance status < 40% (children ≥ 16 years) or an Lansky
performance status of < 40% (children < 16 years) before start of chemotherapy
5. Any other organ dysfunction (CTCAEv4 grade 4) that will interfere with the
administration of the therapy according to this protocol
6. Impaired liver function defined as > 3.0 x UNL for transaminases and for
bilirubin
7. History of VOD
8. History hepatitis C positivity
9. Renal impairment with creatinine < 30 ml/min
10. Decompensated hemolytic anemia
11. Hypersensitivity to GO and/or other chemotherapeutic drugs
12. Inability to potentially complete the treatment protocol for any other reason
13. Pregnant or breastfeeding patients
14. Current participation in another clinical trial for the time of first course of
reinduction chemotherapy
Patient Number Enrolment until 252 randomized patients are evaluable
General Study
Design
Intergroup, international, prospective, randomized, multicenter open-label two-
arm phase III therapy optimization study on the efficacy of GO added to standard
reinduction chemotherapy in children and adolescents with refractory or relapsed
AML.
Study Overview The overall design of the study is shown in the flowchart. All patients eligible for
this study will be randomized in a 1:1 fashion for the addition or not of a single
administration of GO (Mylotarg®) at 4.5 mg/m2 to DX-FLA in the first course of
reinduction chemotherapy. If GO at 4.5 mg/m2 proves to be too toxic (see
definitions in paragraph 10.4), the dose will be reduced permanently to 3.0
mg/m2. Patients who do respond poorly to this first course of chemotherapy with
> 20% BM blasts on “day 28” (before the start of the second course) are off
protocol in terms of therapy However, these patients will remain in follow-up and
overall clinical outcome will be documented.
All other patients will proceed to the second reinduction course (FLA) Patients
who do not achieve a CR/CRi after these two courses are off protocol, but will
remain in follow-up and their clinical outcome will be documented. In CR/CRi,
allo-SCT is generally recommended in all patients. If more time is needed to
perform that SCT, guidelines for intensive and low-intensity consolidation are

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 13 of 66
provided in this protocol.
Primary Endpoint Percentage of BM blasts on “day 28” (before the start of the second reinduction
course) given as ≤ 20% or > 20%.
Secondary
Endpoints
1. Determine incidence of refractory disease, CR/CRi rates after 2 courses and
efficacy (cumulative incidence of relapse, event-free survival, and overall survival)
in the different study arms
2. Determine the toxicity of GO (Mylotarg®) when added to DX-FLA in terms of BM
aplasia, liver toxicity including VOD, cardiotoxicity, mucosal toxicity and other
adverse reactions according to CTCAEv4 which are considered to be relevant in
relapsed AML and the proposed therapy when compared to treatment with DX-
FLA only.3. Identify additional prognostic factors in pediatric relapsed AML, other
than early treatment response, cytogenetics and duration of CR1.
4. Provide individual biological characterization of leukemia (morphology,
immunophenotype, cytogenetics, molecular genetics and activated signalling
pathways), for future individualized stratification to targeted therapy.
Statistical
Considerations
The analysis of the primary endpoint will be performed on all randomized patients
according to the intent-to-treat principle. The difference in response rate (yes or
no > 20% blasts in the BM at day 28, so-called poor or good early treatment
response) will be tested with a logistic regression model taking into consideration
time from first diagnosis of AML to relapse and whether patients had primary
refractory AML or relapsed disease.
The percentage of patients with > 20% BM blasts at day 28 is expected to be
about 20% in the control arm (according to the results of the experimental arm of
study Relapsed AML 2001/01). We expect a reduction of this percentage to 9%
(same reduction as has been shown for the study Relapsed AML 2001/01 from
30% to 19%).
With the patient numbers expected to be randomized and available for analysis
(N=252) the power will be 80% to detect a decrease in the number of patients
with > 20% BM blasts at day 28 from 20% to 9% (one-sided test, alpha=5%).
The early treatment response is the strongest prognostic factor in relapsed AML,
as shown in study Relapsed AML 2001/01.
The analysis of secondary endpoints will be descriptive and explorative. Standard
methods for the calculation of estimates, confidence intervals and descriptive test
will be used.
Toxicity Monitoring Toxicity monitoring will be done throughout the trial (see 7.1 – 7.4), and will be
evaluated using the CTCAEv4. All serious adverse events (SAE’s) must be reported
within 24 hours. The steering committee (international study coordinators) will
evaluate toxicity reports on a regular basis and may stop the trial at the advice of
the data monitoring committee (DMC) if an unacceptable rate of severe toxicity
(CTCAEv4 grade 3 or higher) is recognized.
Dose and treatment modifications due to toxicity are specified in the protocol.
Late toxicity will be assessed by long term follow-up. Early toxicity of this
treatment will be compared to that of study Relapsed AML 2001/01.
Trial Conduct The trial will be carried out according to the Declaration of Helsinki, the principles
of Good Clinical Practice, the Directive 2001/20/EC, as well as according to
relevant national laws and regulations, respectively.
Study Period Recruitment/ Study duration approx Q4, 2015 – Q3, 2020
Running period/Patient: approx 3 months treatment. It is planned to accrue
patients for approximately 5 years, and to have 5 years follow up after completion
of treatment.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 14 of 66
2.1 Flowchart

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 15 of 66
2.2 Signature Pages
The following persons agree with the content of the clinical study and confirm the protocol in the
latest version.
Sponsor
GPOH gGmbH
Representative, Prof. Dr. Dirk Reinhardt
____________________________ _______________________________________
Date Signature
LKP (Coordinating Investigator)
University Children’s Hospital Essen
Prof. Dr. Dirk Reinhardt
____________________________ _______________________________________
Date Signature
Biometry
Hannover Medical School
Dr. Martin Zimmermann
____________________________ _______________________________________
Date Signature

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 16 of 66
Investigator’s Protocol Approval Signature
By my signature, I agree to personally supervise the conduct of the study and to ensure its
conduct in compliance with the protocol, ICH GCP, and the applicable national and European
Regulations covering the conduct of clinical studies.
___________________________________
Name of Study Center
____________________________________
Printed Name of Principal Investigator
____________________________________
Signature of Principal Investigator
__________________________________
Date

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 17 of 66
2.3 Confidentiality Statement/ Disclaimer
The content of this protocol and the case report forms (CRF) must be treated confidentially and may not
be imparted to uninvolved persons without consent of the study chairpersons neither in oral nor in
written form.
This document describes a prospective, open-label, randomized phase III clinical trial in children and
adolescents with relapsed or refractory AML. It provides information for entering patients into this trial.
This protocol is not intended for use as a guide for the treatment of non-registered patients.
Hospitals with limited experience in AML treatment in children (less than two children with AML per
year), should consider transferring the child to a more experienced center.
Responsibility for the diagnosis, administration of protocol treatments and other interventions in study
patients lies with the participating clinician. Before entering patients into this protocol, clinicians must
ensure that the protocol has received approval from both their ethical committee and national
regulatory body.
This protocol has been written with greatest accuracy; however errors cannot be completely excluded.
Amendments may be necessary. Amendments will be circulated to known participants in the trial, but
institutions entering patients for the first time are advised to contact their appropriate study centers.
2.4 Patient Insurance In view of the complex international character of the study, there is no central patient insurance for risks
related to participating in this study.
The co-sponsor in each country will be responsible for the presence of an insurance or indemnity in
accordance with the applicable regulatory requirements for all patients within that country.
Signature:
__________________________ _________________
Principal Investigator Date

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 18 of 66
2.5 List of Abbreviations
A
Cytarabine, cytosine arabinoside,
ARA-C HAV Hepatitis A virus
AE Adverse effect HBV Hepatitis B virus
AR Adverse reaction HCV Hepatitis C virus
ALAL Acute leukemia of ambiguous lineage HIV Human immunodeficiency virus
ALAT Alanine aminotransferase HLA Human leucocyte antigen
ALL Acute lymphoblastic leukemia HSV Herpes simplex virus
AML Acute myeloid leukemia I Idarubicin
APTT Activated partial thromboplastin time ICH
International Conference on
Harmonisation
ASAT Aspartate aminotransferase IEC Independent ethics committee
AUC Area under curve IMP Investigational medicinal product
AUL
Acute leukemia with undifferentiated
lineage I.th. Intrathecally
BM Bone marrow I.v. Intravenously
BMP Bone marrow puncture LDH Lactate dehydrogenase
CMV Cytomegalovirus LP Lumbar puncture
CNS Central nervous system LV Left ventricle
CR Complete remission LVET Left ventricle ejection time
CRF Case report form M Mitoxantrone
CRi, CRp
Complete remission with incomplete
neutrophil or platelet recovery MDS Myelodysplastic syndrome
CSF Cerebral spinal fluid MRD Minimal residual disease
CT Computer tomography MSD Matched sibling donor
CTCAEv4
National Cancer Institute Common
Terminology Criteria for Adverse Events
Version 4.0 criteria MUD Matched unrelated donor
DFS Disease free survival MRI Magnetic resonance imaging
DMC Data monitoring committee NCA National competent authority
DX /
L-DNR Liposomale daunorubicin NR Non-response
DX-FLA
Liposomale daunorubicin, fludarabine,
cytarabine and G-CSF OS Overall survival
E Etoposide-phosphate p Probability, significance
EBV Epstein-Barr virus PB Peripheral blood
pEFS Probability of event-free survival
ECG Electrocardiogram PO Orally
PR Partial response
EFS Event-free survival PT Prothrombin time
EMA European medicines agency PVB19 Parvo virus B19
FAB French-American-British classification SAE Serious adverse event
FAB M0
Acute myeloid leukemia with minimal
differentiation SC Subcutaneously
FAB M1
Acute myeloid leukemia without
maturation SCT Stem cell transplantation
FAB M2 Acute myeloid leukemia with maturation SE Standard error

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 19 of 66
FAB M3 Acute promyelocytic leukemia SOS Sinusoidal obstruction syndrome
FAB M4 Acute myelomonoblastic leukaemia SUSAR
Serious unexpected suspected adverse
reaction
FAB M5 Acute monoblastic leukemia SWOG South-West Oncology Group
FAB M6 Acute erythroblastic leukemia TIF Trial investigator file
FAB M7 Acute megakaryoblastic leukaemia TKI Tyronsine kinase inhibitor
FLA Fludarabine, cytarabine and G-CSF TRM Treatment related mortality
FS Fractional shortening UNL Upper normal level
GCP Good clinical practice VOD Veno-occlusive disease
GO Gemtuzumab ozogamicin VP-16/ETO Etoposide
G-CSF Granulocyte-colony stimulating factor WBC White blood cell
ha Intermediate-dose cytarabine μl Microliter

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 20 of 66
3 Summary
Relapsed and refractory AML in children is a rare problem, but has a poor prognosis. The consequent
and intensive treatment of AML relapses according to the protocols AML-BFM REZ-93 and -97 as well as
Relapsed AML 2001/01 has led to improved outcome. Nevertheless, further efforts are needed in face of
about 65% of patients still dying from relapse. Improved knowledge about mechanisms and mutations
involved in leukemogenesis and the consecutive development of new agents targeting these
mechanisms led to the concept of targeted and tailored therapies which might further improve outcome
when added individually to conventional chemotherapy. Data on the use of these specific substances in
pediatric AML are still scarce. GO (Mylotarg®) which links the cytotoxic calicheamicin to a conjugated
monoclonal CD33 antibody has proven effective in terms of CR achievement and better survival in adult
AML studies and in pediatric AML relapse in a salvage study with moderate toxicity. Since more than
90% of pediatric AML are CD33 positive, adding GO to the standard regimen offers a great potential as
targeted therapy for the majority of patients in our study.
Primary objective of the study is to determine the initial efficacy of GO (Mylotarg®) when added to DX-
FLA in children with relapsed or refractory AML. In addition, the study will prospectively determine the
long-term clinical outcome of these patients stratified according to the different risk groups (refractory
disease, early relapse, late relapse, and the previous treatment protocol. Other secondary objectives are
to determine the efficacy of GO in well-described subgroups, the toxicity of dosing GO (Mylotarg®) at 4.5
mg/m2/dose in combination chemotherapy, the identification of novel prognostic factors, and the
characterization of relapsed AML to enable future more leukemia-specific therapy. The study expects to
accrue up to 85 patients annually, and will run 3 to 5 years. This will allow the accrual of 252 eligible,
randomized and fully evaluable patients, assuming a randomization rate of 75% and the primary
endpoint being available in 80% of randomized patients.
Reinduction treatment will be initiated with DX-FLA (Liposomal daunorubicin fludarabine, and
cytarabine) in the first course. In the first course there will be a randomization for GO (Mylotarg®) to be
added or not. GO (Mylotarg®) will be dosed at 4.5 mg/m2. According to the results from AML Relapse
2001/01 FLA will be given as a second induction. If patients have > 20% of blasts in the BM after the 1st
course as measured on “day 28”, or if they are not in CR/CRi after the 2nd course, they will go off-
protocol in terms of treatment. However, these patients remain in follow-up and clinical outcome will
be documented. Patients in CR/CRi after reinduction treatment should immediately proceed to allogenic
stem cell transplantation, the protocol provides guidelines for consolidation chemotherapy if time-to-
transplant must be bridged.
Study Relapsed AML 2001/01 showed very poor outcome for patients with a poor response to the first
course of reinduction chemotherapy, for patients not achieving CR/CRi, and for patients with
subsequent relapse. That explains why these patients will go off protocol in terms of therapy and will be
eligible for phase I/II studies with novel agents, or palliative therapy.
Reliable and fast identification of these molecular abnormalities is required at relapse. Information on
molecular characterization at initial diagnosis is not reliable enough, because instability of these
mutations has been reported, with both losses and gains at relapse. Therefore, molecular
characterization of relapsed AML cases must be established in all participating groups. A complete
characterization of the individual AML features of a patient, including morphology, immunophenotype,
molecular and cytogenetic abnormalities, treatment response and the identification of specific activated
signaling pathways is crucial to improve our understanding of leukemogenesis and is required to direct
subsequent therapeutic decisions. Hence, we aim to establish a diagnostic workup providing a detailed
individual biological characterization within 7 days from diagnosis thus enabling the future addition of
specific inhibitors on an individual basis. Some of these features will additionally serve as markers in the
monitoring of minimal residual disease (MRD). This effort will be run and coordinated by Dirk Reinhardt
(AML-BFM Group, Essen, Germany).

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 21 of 66
3.1 Background and Introduction
Newly diagnosed AML is a rare disease in children. The prognosis has improved considerably using
intensive chemotherapy with or without stem cell transplantation. However, 5-10% of patients do not
achieve first CR due to resistant disease (primary refractory AML), and 30-50% of CR patients relapse.
Primary refractory AML and relapsed AML have a poor prognosis with a long-term OS of 36% (Kaspers
JCO 2012). For AML in first relapse, the prognosis mainly depends on the time to relapse, cytogenetics,
and the early response to reinduction therapy. For early relapses, defined as within 1 year from initial
diagnosis, the second CR rate is about 50%, and OS about 20%. For late relapses, defined as after 1 year
from diagnosis, the second CR rate is 70-75% and the OS up to 50%. Multiple relapsed AML has an even
worse prognosis. Several treatment schedules have been studied recently, and improvement seems
feasible using new drugs and new drug combinations. Therefore, there is an unmet medical need for
further development of new treatment options to rescue these children. Gemtuzumab ozogamicin (GO)
holds potential in this respect. On the longer term, we might also learn that GO can replace
anthracyclines, partially or completely. This is very important, since the use of anthracyclines is limited
by long-term cardiotoxicity, which is a dose-dependent late effect of therapy. Clinical cardiotoxicity has
been reported to occur in more than 10% of patients that were treated with higher cumulative doses of
anthracyclines, and patients die from this complication, or need heart transplantation. The cytotoxic
compound of GO is calicheamicin, and is related to anthracyclines. However, because calicheamicin is
linked to anti-CD33, it does not affect the cardiac muscle like anthracyclines can do.
3.2 Gemtuzumab Ozogamicin (GO) (Mylotarg®)
3.2.1 Pharmacology and Pharmacodynamics
GO (Mylotarg®) is a conjugated monoclonal CD33 antibody that selectively targets CD33 positive cells.
CD33 is a glycoprotein belonging to the sialoadhesin family und is expressed on the surface of 90% of
AML blasts as well as on myeloid precursors, and in lesser frequency on granulocytes and monocytes but
not on CD34-positive normal hematopoietic stem cells, lymphocytes and non-hematopoietic tissues. GO
is composed of a humanized IgG4 class monoclonal antibody linked to a derivate of the antineoplastic
antibiotic calicheamicin2. Calicheamicin is an antineoplastic antibiotic which consists of two parts: an
aryltetrasaccharid part responsible for the ligation with DNA and an enediyne part causing DNA
ruptures. In the pharmacologic preparation of GO (Mylotarg®), 50% of the antibody is conjugated and
50% is unconjugated. GO (Mylotarg®) attaches via its antibody part to the CD33 molecule and is then
internalized in the cytoplasma where the two components are hydrolized. Free calicheamicin enters the
nucleus and intercalates with DNA producing double strand brakes and induced apoptosis3.
3.2.2 Pharmacokinetics
GO binds with high specificity to myeloid blasts and monocytes with maximal binding being related to
the level of CD33 expression4. As CD33 is down regulated with maturation of the myeloid lineage,
binding to granulocytes has been shown to be less, and virtually no binding to CD33-negative
lymphocytes has been observed. As the antibody represents the targeting portion of GO (Mylotarg®)
measurements of its pharmacokinetics are considered the primary surrogate of the overall
pharmacokinetic of the drug5. The highest antibody concentrations were seen shortly after the end of
infusion. CD33 saturation is dose-dependent with a near-complete saturation of CD33 antigenic site 0.5-
6 hours after infusion at dose levels at and above 4 mg/m2, while 3 mg/m2 has not been studied in that
respect.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 22 of 66
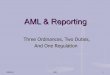
Figure 1: CD33 saturation kinetic after GO infusion, comparison of different dose levels
Wyeth personal communication (data on file)
Elimination half-life varied between mean 43.1 h at a 6 mg/m² dose level versus 63.6 h at a 9 mg/m²
dose level for the first treatment course and 49.4 h versus 57.8 h respectively for the second treatment
course6. With two-week dose intervals between GO (Mylotarg®) administrations, little accumulation of
the antibody was observed with only 1% of the maximum concentration being found just before the
next application. Antibody clearance did not significantly differ related to age or body weight.
Table 1
Dose (mg/m²) Period n C max(mg/l) t1/2 AUC (mg x h/l) CL (l/h)
6 1 14 1.70 ± 22.7 43.1±22.7 48.8± 47.6 0.61±0.94
6 2 14 1.94 ± 1.09 49.4 ± 25.6 79.7 ± 66.2 * 0.32±0.49
7.5 1 2 3.11 40 112 0.12
7.5 2 1 3 33.4 153 0.09
9 1 14 3.47 ± 1.04 63.7 ± 44.3 136 ± 107 0.16 ± 0.23
9 2 9 4.68 ± 2.18 57.8 ± 33.4 241 ± 157 * 0.21 ± 0.45 Buckwalter et al: Summary of hP67.7 Pharmakokinetic parameters by dose group for dose periods 1 and 2
* significant differences between periods 1 and 2
For both age groups - pediatric and adult patients - an increase of maximum concentration levels,
elimination half-life and area under curve (AUC) have been described between the first and second
treatment course. These differences do not seem to reflect simple reduction of tumor burden.
Decreased blast uptake, CD33 down regulation, increased plasma protein binding or resistance to GO
(Mylotarg®) induced apoptosis have been discussed as mechanisms of drug resistance.
The concentration vs. time profiles of total calicheamicin showed similar shape to the profiles of the
antibody. The intersubject variability within dose periods was large for most parameters.
Levels of potentially toxic unconjugated calicheamicin were low and only measurable shortly after the
end of infusion. Pharmacokinetic parameters were consistent for all pediatric age groups.
The main route of drug elimination is hepatobiliary. Biodistribution studies with radiolabeled CD33
antibody revealed specific BM uptake and distribution of antibody only in organs with large blood pool
such as spleen and liver7. GO (Mylotarg®) does not penetrate the blood-brain barrier8.
CD33 Saturation Over TimeCD33 Saturation Over Time
00
1010
2020
3030
4040
5050
6060
7070
8080
9090
100100
Perc
ent C
D33 s
atu
ration
Perc
ent C
D33 s
atu
ration
0.50.5 11 22 33 44 66 88 2424
Time after start of infusion, hoursTime after start of infusion, hours
00
9 mg/m2
6 mg/m2
4 mg/m2
1 mg/m2
9 mg/m2
6 mg/m2
4 mg/m2
1 mg/m2

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 23 of 66
3.2.3 Approval Status
GO (Mylotarg) was approved in May 2000 under the FDA’s accelerated approval program to treat
patients ages 60 years and older with recurrent AML who were not considered candidates for other
chemotherapy. The initial approval was based on the surrogate endpoint of response rate (i.e., the
percentage of patients whose leukemia decreased or disappeared in laboratory tests), observed in 142
patients with AML across three clinical trials (FDA news release June 21, 2001).
A confirmatory, post approval prospective randomized clinical trial was begun by Wyeth (now Pfizer) in
2004. The trial was designed to determine whether adding Mylotarg® to standard chemotherapy
demonstrated an improvement in clinical benefit (survival time) to adult AML patients. The trial was
conducted by the s South-West Oncology Group (SWOG S0106). It revealed no benefit of GO in the total
patient group. Moreover the addition of GO to the first induction course (daunorubicin/cytarabin) led to
an increase in the number of deaths in the GO group compared to the standard group (16/283=5.7%
vs.4/281=1.4%, p=0.01). Although the induction death rate in the GO treated arm was similar to what
has been reported in multiple other AML trials, but the mortality rate for the control arm was
unexpectedly low in this study9, these results lead to the voluntary withdrawal of Mylotarg® from the
U.S. market by Pfizer in June 2010.
The application for approval of GO in the European Community for the use in adult patients with
relapsed/refractory AML was rejected by the European medicines agency (EMA) based on insufficient
data on the effectiveness of the drug from clinical trials, despite the availability of data in newly
diagnosed AML showing benefit in a significant part (the majority) of the patients.
Despite a lacking evidence of benefit for GO in the total group of adult AML patients in the SWOG trial
there is still a rational for the use in the pediatric population addressed within this clinical trial:
GO has proven effective in adult AML patients within the subgroups with cytogenetic favorable and
intermediate risk in prospective randomized clinical trials (MRC15) with a significant improvement of
survival10. Again, in this clinical trial patients with cytogenetic high risk did not benefit from GO
treatment but suffered from increased toxicity and showed inferior outcome. However about 70% of
the total patient group did benefit from GO. Finally, a recent randomised French study reported a
significantly improved relapse-free, event-free and overall survival in adults (50-70 years old) with AML
when GO was added to induction chemotherapy11-13.
The toxicity profile of GO comprises besides hematotoxicity mainly liver toxicity especially VOD which
has led to increased death numbers in adult patients in the SWOG trial. Phase I/II trials in pediatric
patients with refractory and relapsed AML(AML Relapse 2001/2 „Mylotarg Salvage Study“14) however,
showed a significant smaller number of liver toxicities in young patients despite heavy pretreatment15,
suggesting that the occurrence of VOD is age and perhaps also life-style related.
3.2.4 Clinical Studies
In vitro and in vivo studies that demonstrated the ability of GO (Mylotarg®) to inhibit the proliferation of
CD33-positive AML cell lines as well as in transplanted human AML blasts in xenograft mouse models led
to a first dose-escalating clinical phase I study8. Forty patients with relapsed or refractory AML were
enrolled. 18 of 40 patients (45%) had previously undergone autologous or allogenic BM transplantation.
Patients were required to have good clinical performance (Karnofsky Index > 60%), good liver and kidney
function and a WBC ≤30.000/µl. Three to eight patients were treated at each of eight dose levels of GO
(Mylotarg®) ranging from 0.25 to 9 mg/m² i.v. at 14 days intervals. Infusion related toxicity with fever,
chills and hypotension was common and occurred 2-4 hours after infusion. Moreover, transient
elevation of liver enzymes was observed in 20% of patients. Hematologic toxicity including prolonged
neutropenia and thrombocytopenia were mainly seen at the 9mg/m² dose level. Application of more
than two doses resulted in prolonged myelosuppression in two patients, and one patient died of sepsis
in neutropenia within 30 days from application. CR rate was 7.5 %, and 12.5 % of the patients showed

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 24 of 66
remission without full platelet recovery (CRp). According to the toxicity profile the maximal tolerated
dose (MTD) was defined 9mg/m². CD33 saturation data further supported this choice.
Sievers and Larson16-18 sequentially reported the results of three open label multicenter phase II studies
including a total of 277 adult patients treated with GO (Mylotarg®) monotherapy in first relapse of AML.
GO (Mylotarg®) was administered as 2hour infusion with two doses of 9mg/m² at 14 days intervals. 13%
of patients achieved CR and 13% CRp. Remission duration was slightly higher in the CR group (median
6.4 months) than in the CRp group (median 4.5 months). A significant difference in remission duration
was observed between patients younger than 60 years of age when compared to patients older than 60
years of age. This was possibly affected by postremission therapy options, especially hematopoetic stem
cell transplantation. Achievement of remission was the most significant factor for patients at age > 60
years who were not eligible for transplantation. At this age group, patients who achieved CR and did not
get any further treatment displayed significantly longer OS with a median survival of 12.8 months than
non-responders with a median of 2.5 months. Based on these results, GO (Mylotarg®) was approved by
the FDA in May 2000 for the treatment of patients with AML relapse or refractory AML at > 60 years of
age who are not candidates for conventional chemotherapy.
In 2003 Zwaan et al19 published first experiences with GO (Mylotarg®) monotherapy in children with
relapsed and refractory AML. 15 children had been treated at dose levels between 4 and 9mg/m² with
up to three courses of GO (Mylotarg®). The overall response rate including CR and CRp was 53%. Main
toxicities were grade 3-4 myelotoxicity (15/15 pts), infusion related toxicity with 2 febrile reactions and
one case of hypotension, and liver toxicity with one case of grade 3 hyperbilirubinemia without signs of
VOD and another patient who developed VOD after a prior HSCT in first CR. Aside from liver toxicity,
non-hematologic toxicity was considerably mild, no mucositis or severe infections were reported. OS
was 13% following subsequent HSCT (2/15pts).
A larger cohort of pediatric patients was reported by Arceci et al22. 29 children with refractory and
relapsed AML were entered in an open-label dose escalation study and received 2 courses of GO
(Mylotarg®) at 14 days intervals. Dose levels were 6 and 9 mg/m², respectively. 28% of patients achieved
overall remission. Mean multidrug resistance-protein-mediated efflux was significantly lower in
leukemic blasts of patients who achieved CR. Elevation of liver enzymes (21%), grade 3-4
hyperbilrubinemia (7%) and VOD (3%) were the main non-hematologic toxicities reported and defined
the dose limiting toxicity. The MTD was determined to be 6 mg/m². Thirteen patients proceeded to
HSCT < 3.5 months after the last GO (Mylotarg®) dose; 6 of which (40%) developed VOD subsequently.
Due to its potential to induce valuable remission rates in a selected patient cohort with extremely poor
prognosis when treated in single agent studies, and because of its moderate toxicity profile apart from
liver toxicity and prolonged myelosuppression, GO (Mylotarg®) is increasingly implemented in
combination regimens. The results of these trials are heterogeneous.
In a feasibility study, Kell at al20. combined GO (Mylotarg®) at a 3 mg/m² dose level with different
intensive chemotherapy regimens as first line treatment in 72 adolescent and adult AML patients.
Chemotherapy consisted of either GO (Mylotarg®) with fludarabine, cytarabine and idarubicine, or GO
(Mylotarg®) with daunorubicine, cytarabine and thioguanine, respectively. CR rates obtained with these
regimens were 86% and the median OS was 78% at 8 months. However, incidence of VOD was 10.9 %,
and combining GO at 6 mg/m2 with conventional chemotherapy was not feasible, although this was
significantly influenced by the use of thioguanine. Combining GO with conventional chemotherapy for
two consecutive courses also was not feasible. In a subsequent study Burnett et al. compared
conventional chemotherapy with the same schedules plus a single dose of Mylotarg® at 3 mg/m2 in a
randomized study in adult and pediatric AML. Preliminary data presented at international meetings
suggest both improved disease-free and OS, at least in subgroups of patients, with GO added to
chemotherapy10,21. Similarly, COG very recently reported that Mylotarg® at 3.0 mg/m2 could be
combined safely with ADE, and with mitoxantrone and cytarabine 22, while the group from Baruchel
reported that Mylotarg® could be combined safely with cytarabine, when given at days 1, 4 and 7 at 3.0
mg/m2 for a cumulative dose of 9.0 mg/m2 per course 23-25.
Finally, a recent randomised French study reported a significantly improved relapse-free, event-free and
overall survival in adults (50-70 years old) with AML when GO was added to induction chemotherapy.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 25 of 66
In a phase 3, open-label study, 280 patients aged 50-70 years with previously untreated de novo acute
myeloid leukaemia were treated with or without five doses of intravenous gemtuzumab ozogamicin (3
mg/m(2) on days 1, 4, and 7 during induction and day 1 of each of the two consolidation chemotherapy
courses). At 2 years, EFS was estimated as 17.1% (10.8-27.1) in the control group versus 40.8% (32.8-
50.8) in the gemtuzumab ozogamicin group (hazard ratio 0.58, 0.43-0.78; p=0.0003), OS 41.9% (33.1-
53.1) versus 53.2% (44.6-63.5), respectively (0.69, 0.49-0.98; p=0.0368), and RFS 22.7% (14.5-35.7)
versus 50.3% (41.0-61.6), respectively (0.52, 0.36-0.75; p=0.0003). Haematological toxicity, particularly
persistent thrombocytopenia, was more common in the gemtuzumab ozogamicin group than in the
control group (22 [16%] vs 4 [3%]; p<0.0001), without an increase in the risk of death from toxicity.
Another study comparing the addition of low-dose GO (Mylotarg®, MY) to fludarabine, cytarabine and
idarubicin followed by Granulocyte-colony stimulating factor (G-CSF) (MY-FLAI) with historical controls
(FLAI) revealed comparable CR rates but a lower relapse frequency at two years after addition of MY at
3.0 mg/m2 (40% vs. 80%) compared to FLAI alone in de novo AML26. Patients with secondary AML had
comparable outcome with or without GO (MY). The MY-FLAI regimen was well tolerated. Hematological
toxicity was comparable to that of FLAI. Non-hematological toxicity was mild with no case of grade 3-4
liver toxicity but 4 patients experienced transient liver enzyme elevation. In addition, several groups
have demonstrated the feasibility and efficacy of GO (Mylotarg®) at even 6 mg/m² or higher with
combination chemotherapy 27-30. Chevalier et al. combined GO at 9.0 mg/m2 (day 4) with Ara-C at 1
gr/m2 twice daily for 5 days and mitoxantrone at 12 mg/m2/day for 3 days, in adults with refractory or
relapsed AML. The rate of CR/CRp was 63% and the regime was tolerable. Eom et al. reported that GO at
6.0 mg/m2 could be safely combined with idarubicin at 12 mg/m2/dose for 3 days plus ara-C at 300
mg/m2/day for 5 days, and resulted in a CR/CRp rate of 78% in a series of adults of ≥55 years of age with
de novo AML. Alvarado et al. studied GO at 6.0 mg/m2 on days 1 and 15 together with idarubicin at 12
mg/m2/dose for 3 consecutive days and Ara-C at 1.5 mg/m2/day for 4 consecutive days, in adults with
refractory or relapsed AML. The CR/CRp rate was 42% and the regime was tolerable, although liver
toxicity did occur, with VOD in 14% of patients. Finally, Tsimberidou et al. combined GO at 6.0 mg/m2 on
day 1 with fludarabine and Ara-C at 15 mg/m2 and 0.5 mg/m2 respectively on days 2-6, plus cyclosporine
A, in adults with de novo AML. The CR/CRp rate was 48% and the regime was feasible, although the
incidence of VOD was 7%. From these studies it can be concluded that a single administration of GO at a
dose of up to 6.0 mg/m2 can be combined with intensive chemotherapy in adults with AML, although
liver toxicity still seems significant at the latter dose level. Therefore, this treatment protocol will apply
GO at 4.5 mg/m2 for one dose.
The German AML-BFM Study Group, reported the treatment results of 62 children and adolescents with
refractory AML after at least two intensive regimens (n=62; male n=40; female n=22) and/or allogeneic
stem cell transplant (n=9). Twenty-eight children received GO-monotherapy (7.5mg/m2 day 1 and day
15; group A), in 34 children GO 3mg/m2 was combined with cytarabine (500mg/m2/d 96h continuous
infusion; group B). The median age at initial diagnosis was 10 years (range 0.2 to 21 years). Nine children
had secondary AML following a previous malignant disease and in 4 cases an acute leukemia of
ambiguous lineage (ALAL) had been diagnosed. The morphological subtypes were AML with minimal
differentiation (FAB M0) n=4; AML without or with maturation (FAB M1/M2) n=17 M3 n =1; acute
myelomonoblastic/monoblastic leukaemia (FAB M4/M5) n=25; M4Eo n=1; acute erythroblastic/
megakaryoblastic leukemia (FAB M6/M7) n=9, undifferentiated (AUL)/acute leukemia of ambiguous
lineage (ALAL) n=5. In cytogenetics, most patients had a normal karyotype (n=16; including 7 with FLT3-
ITD) followed by MLL-rearrangements (n=14), numerical aberrations (n=7; including FLT3-ITD n=2),
others aberrations (n=10; FLT3-ITD n=1), complex karyotype (n=3) and BCR/ABL positive AML (n=1).
Favorable translocations [t(8;21), inv 16, t(15;17)] were diagnosed in 4 patients. In 7 patients no
cytogenetic results were available.
Five children suffered acute anaphylactic reaction during or short after infusion (CTC grade III n=3, grade
IV n=2). Severe, long lasting myelosuppression has been observed in almost all patients. While the
frequency of severe infection during myelosuppression was moderate, adverse reactions such as
mucositis have rarely been reported. A VOD-like syndrome was observed in 5 children after alloSCT, in
two cases with fatal outcome.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 26 of 66
An overall response (CR, CRp, PR) has been documented in 32 children (group A n=10/28, 36%; group B
n=22/34, 65%). A higher response rate has been observed in children with AML FAB M1/2 with auer
rods (n=18 response n=12, 67%) and AML with favorable aberrations (n=3/4). Six out of 10 children with
FLT3-ITD positive AML responded to GO whereas patients with AUL/ALAL (n=9; response n=1, 11%) and
AML FAB M6/7 (n=10; response n=3, 30%) showed a poorer response. Thirty-five patients received
allogeneic SCT following GO treatment, 30 of the responders and 5 patients without GO response. In
total 13 children are alive. Out of the responders 11 children or adolescents are still in CR (follow-up 2.7
years, 0.5 to 8.2 yrs.). Again children with AML FAB M1/2 and/or favorable cytogenetics had the best
prognosis (7 /19 children alive, 37%). By contrast, none of the children with AML FAB M6/7, AUL or ALAL
survived.
Out of the 30 patients who did not respond to GO, following alloSCT 2 children are alive, however, the
follow-up of 0.5 years (0.3 to 0.9 yrs) is very short. In this particular poor group of heavily pretreated
children and adolescents with multiple relapsed, refractory AML, GO seems to improve the prognosis in
some children and enables further treatment e.g. alloSCT. Based on the specific needs of children it is of
importance that clinical trials in childhood AML continue to identify the appropriate patient group and
schedule of GO combined with chemotherapy31.
In conclusion, there is considerable evidence that GO is an effective drug in the treatment of AML in
children and adults32. GO (Mylotarg®) induces reproducible CR/CRp rates in up to 30% of patients with
second relapsed and refractory AML when administered in single agent studies. Combination studies
have shown even better results with moderate toxicity profiles. However, the risk of developing VOD is
increased when GO (Mylotarg®) is given prior to or less than 3-4 months after stem cell transplantation,
indicating that GO (Mylotarg®) treatment should be weighed against the potential risk of VOD in patients
with history of SCT, VOD and pre-existing impairment of liver function. However, this side-effect seems
to be dose-dependent, since at doses of less than 6 mg/m² Mylotarg®, as single agent or in combination
chemotherapy, gives a risk of VOD or SOS of only 3%33. Therefore, this treatment protocol will apply GO
at a single dose of 4.5 mg/m2.
3.2.5 Adverse Reactions (AR) / Toxicity
The most common adverse reactions of GO (Mylotarg®) treatment concern neutropenia and
thrombocytopenia due to the fact that CD33 is expressed not only on AML blasts but also in high
frequency on myeloid precursors and, to a lesser extent, on granulocytes, monocytes and also on a small
minority of megakaryocytes.
Infusion related symptoms occurred in a significant number of patients 2-6 hours after infusion and
consisted of fever, chills, hypotension and dyspnea and disappeared upon treatment with
acetaminophen and occasionally steroids. Infusion related syndromes have previously been described
after infusion of monoclonal antibodies (e.g. CD20 antibody Rituximab®) and tend to be more common
after first infusion. The post marketing surveillance survey 34 of GO (Mylotarg®) revealed 9 cases of
severe hypersensitivity resulting in four deaths.
Tumorlysis syndrome and adult respiratory distress syndrome (ARDS) have been reported in patients
with leukocytes > 30000/µl treated with GO (Mylotarg®). Therefore reduction of WBC below 30000/µl
prior to the start of GO (Mylotarg®) treatment is recommended.
Hepatic toxicity with elevation of liver enzymes and bilirubin is encountered in up to 30% of patients
after GO (Mylotarg®) treatment, is reversible in most cases and is dose-dependent. Frequency of severe
liver toxicity and VOD is estimated to occur in 4-5% of patients, with higher frequencies in patients after
stem cell transplantation 35,36. At doses below 6 mg/m2, GO either as single agent or in combination
chemotherapy, was associated with VOD/SOS in 3% of patients33. Therefore patients treated with GO
(Mylotarg®) should be monitored for clinical and laboratory signs of VOD closely even if they have not
been treated with SCT.
Toxicity monitoring will be done throughout the trial (see 7.1 – 7.4), and will be evaluated using the
CTCAEv4. The steering committee (international study coordinators) will evaluate toxicity reports on a

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 27 of 66
regular basis and may stop the trial at the advice of the DMC if an unacceptable rate of severe toxicity
(CTCAEv4 grade 3 or higher) is recognized.
Late toxicity will be assessed by long term follow-up. Early toxicity of this treatment will be compared to
that of study Relapsed AML 2001/01.
3.3 FLA + Liposomal Daunorubicin (DX-FLA)
Apart from cytarabine and its derivatives anthracyclines play a key role in the treatment of AML. First-
line induction regimen in AML includes high cumulative doses of anthracyclines. Therefore further use of
conventional anthracyclines in reinduction therapy is limited by the risk of cardiotoxicity. Liposomal
daunorubicin (L-DNR, DX) has proven effective in terms of CR rate in a pilot study37,38. Toxicity was
tolerable and similar as with IDA-FLAG, but treatment in experienced centers was recommended
because of high risk of infections during prolonged neutropenia. No clinical cardiotoxicity was reported.
Based on this favorable data, the impact of adding DaunoXome® to FLAG in reinduction therapy has
been subject of an open label randomized trial of the international BFM Study Group (relapsed AML
2001/01). This trial showed comparable grade 3-4 toxicity for DX-FLAG followed by FLAG as with two
courses of FLAG. Adding DX to FLAG improved the early response rate by 10%, from 70 to 80% (p=0.04).
In addition, CR rate was 9% higher with DX-FLAG, 68% versus 59% (p=0.07). OS was not different
between both arms, suggesting that additional measures are necessary to maintain the higher response
rates39. However, it should be stressed that study Relapsed AML 2001/01 did not intent and was not
powered to demonstrate any beneficial effect of DX on long-term outcome, and treatment after the first
course of reinduction chemotherapy was uncontrolled. The general conclusion from study Relapsed
AML 2001/01 has been that adding DX to cytarabine-based treatment improves early treatment
response, which is an important first step towards successful therapy.
3.4 FLA
Since the favorable effect of combining fludarabine and cytarabine had first been described by Gandhi
et al. (1993)40 and the sensitizing effect of G-CSF when added to this regimen had been reported FLAG
has been routinely used in the treatment of AML. Recent data on the effect of G-CSF on the in vitro
cytotoxicity of FLA revealed a higher leukemic cell survival upon administration of G-CSF alone whereas
combination treatment with FLAG led to additive cell killing41. These findings supported the clinical use
of this regimen. Numerous clinical studies in relapsed and refractory AML in children and adults
including own data38,42 outlined the efficacy of FLAG in achievement of second remission. Since 2001
FLAG has been implemented in the international BFM treatment protocol for refractory and relapsed
AML in childhood Relapsed AML 2001/01. G-CSF in this setting is being used as priming agent. However,
recent studies raise doubt about the beneficial role of G-CSF and a recent meta-analysis of randomized
trials did not reveal a favorable effect of adding G-CSF to chemotherapy in AML43. In addition, although
with G-CSF used between chemotherapy courses and not as priming agent, a recent analysis of the
pediatric study BFM-AML 98 identified an increased relapse risk in the subgroup of high-risk patients
associated with the use of G-CSF which could be explained at least in part by G-CSF receptor variants44 .
Finally, G-CSF as priming agent is started 1 day before chemotherapy and disadvantages are the possible
increase in white blood cells with an increased risk of hyperviscosity and the risk of unexplained lung
toxicity as has been described in several patients in study Relapsed AML 2001/01. Thus, like in several
phase I/II studies, it has been decided to omit G-CSF as priming agent and also to discourage its routine
use to decrease the duration of neutropenia.
3.5 Other Reinduction Chemotherapy Regimens
Based on the known antileukemic efficacy of cytarabine and FLAG various studies have been performed
with cytarabine derivatives such as Cladribine® (2-chloro-deoxyadenosine, 2-CDA) or clofarabine.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 28 of 66
Combination of 2-CDA with cytarabine and G-CSF (CLAG) showed a response rate of 50% among 20
patients with relapsed or refractory AML45 with a median CR duration of 22,5 weeks. Combination of
mitoxantrone with FLAG as salvage therapy 46 in 29 adult patients with relapsed and refractory AML
resulted in a CR rate of 59%, a median EFS of 3,2 months and an median OS of 6,8 months. A multidrug
reinduction protocol including topotecan, vinorelbine, thiotepa, dexamethason and gemcitabine has
been developed by Kolb et al.. The study cohort comprised a total of 28 patients of whom fourteen had
precursor B-cell ALL (acute lymphoblastic leukemia) and nine had AML. Overall response rate with this
regimen was 36% (55% for AML patients). One patient died in remission because of infectious
complication. Grade 4 neutropenia was seen in all patients and transient grade 2 liver toxicity was
reported in 10 patients (36%). Studies with GO (Mylotarg®) were summarized above, and are very rare in
pediatric relapsed AML. As single agent, it does not achieve subsequent CRs to such an extend as
FLA(G)-DX does.
Clinical results on the use of small molecules and specific inhibitors such as the inhibitor of proteasome
and NF-kappaB bortezomib in children have not been published yet.
In general, response rates with other drug combinations, although difficult to compare, are not as good
as with DX-FLA(G).
3.6 Central Nervous System (CNS) Prophylaxis and Treatment
Overt CNS leukemia is relatively rare in AML. This protocol applies high-dose chemotherapy, with an
anticipated CNS prophylactic effect as well as prophylactic intrathecal (i.th.) triple chemotherapy
consisting of cytarabine, methotrexate and prednisone. This combination has been reported to
effectively diminish the risk of CNS relapse in pediatric AML47,48.
3.7 Consolidation Chemotherapy and Stem Cell Transplantation (SCT) To consolidate an achieved CR/CRi, and to have time to prepare transplantation if not available
immediately, further chemotherapy is indicated. In these high-risk patients, further intensive treatment
seems justified. Therefore, a schedule of VP16 and cytarabine given by continuous infusion has emerged
and proven feasible and effective in maintaining CR2 until transplantation is available in study Relapsed
AML 2001/01. In case of a delayed SCT and the need to avoid further potentially severe side-effects, a
low-intensive combination of orally thioguanin and cytarabine subcutaneously is included as well.
Extensive experience with this regimen has been obtained within the AML-BFM protocols. However
since an increase of VOD after treatment with gemtuzumab ozogamicin in combination with Thioguanin
has been reported screening for signs of liver toxicity before the start of consolidation and vigorous
monitoring of liver toxicity in these patients is mandatory.
It is generally assumed that allogeneic matched sibling donor (MSD) SCT has a beneficial effect on the
prognosis in AML (Woods 2001). However, major morbidity and mortality is associated with it.
Therefore, allogeneic SCT should be considered in the context of the prognosis with chemotherapy only.
In patients with primary refractory or relapsed AML, this prognosis is poor. Moreover, only few long-
term survivors have been described after chemotherapy only for this particular disease, in contrast to
chemotherapy followed by SCT. Although not proven in properly designed randomized clinical trials,
allogeneic SCT may have a bigger impact on the prognosis than autologous SCT, because: 1) a graft-
versus-leukemia effect may be present in the allogeneic, but not in the autologous setting, and 2) the
autologous transplant is likely to contain minimal residual leukemia cells, which may cause a relapse. On
the other hand, allogeneic SCT may be complicated by graft-versus-host-disease. We do recommend
allogeneic SCT for all patients who achieve CR/CRi, preferably using a MSD, or if not available, a matched
unrelated (MUD) donor. Patients at higher risk of relapse, i.e. primary refractory disease, early relapse,
and ≥2nd relapse, might be eligible for more experimental mismatched unrelated donor (MMUD), cord
blood (CB) or haplo-identical donor (HID) SCT if both a MSD and a MUD are lacking. For patients with a
late relapse such treatment seems too experimental in view of their better prognosis, and autologous
SCT may be considered instead. There are several conditioning regimens, including a combination of
busulfan, cyclophosphamide and melphalan. Experiences using this regimen in children with

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 29 of 66
myelodysplastic syndrome were good49,50. Depending on the type of donor, additional
immunosuppression may be required in conditioning. Patients who were not irradiated previously and
who will have a SCT for the 1st time may receive TBI/cyclophosphamide (also depending on age) as
conditioning instead of busulfan, cyclophosphamide and melphalan. Detailed guidelines on conditioning
and SCT are beyond the purpose of this treatment protocol and may be reviewed in separate pediatric
AML-SCT protocols. However, patients will be monitored for toxicity and events, also after SCT.
3.8 Salvage Treatment
Patients who will not respond sufficiently to the reinduction treatment are off protocol in terms of
therapy. However, these patients remain in follow-up.
3.9 Translational Research, Add-on Studies
Translational research projects and add-on studies will be run by the I-BFM AML Study Group and will be
coordinated by Prof. Dirk Reinhardt.
3.10 Conclusion / Risk-Benefit Ratio
Conventional chemotherapy regimen based on FLAG in addition with anthracyclines did improve
outcome of AML relapse and refractory AML while exerting tolerable toxicity. However in view of only
35-40% OS in this patient group the addition of new therapeutic concepts to current standard regimen
seems mandatory.
GO (Mylotarg®) has been shown effective in the setting of relapsed and refractory AML in adults and
children with CR rates up to 30% in selected groups. We and others have shown that combining GO
(Mylotarg®) with cytarabine and with IDA-FLAG and ADE is feasible and effective with moderate toxicity
(expectable adverse reactions of GO see 3.2.5). The addition of GO (Mylotarg®) to FLA-DX based
standard reinduction chemotherapy may thus be the next step to further improvement of outcome.
Significant results can only be achieved in the setting of large intergroup trials because of the rarity of
the disease. This protocol describes such an international randomized phase III study that aims at
improving the outcome of these children and at learning more about the cause(s) of the poor treatment
response. The obtained knowledge may also be useful for the future treatment of newly diagnosed
AML, especially with respect to the use of Mylotarg® in addition with conventional chemotherapy.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 30 of 66
4 Study Objectives
The Study Relapsed AML 2010/01 aims at improving prognosis in relapsed and refractory AML in
childhood by addition of GO (Mylotarg®) to the standard FLA-DX based reinduction chemotherapy. The
use of GO (Mylotarg®) at 4.5 mg/m2/dose, a dose that has shown CD33 saturation with limited toxicity
when combined with conventional chemotherapy should reduce the risk of too high toxicity, while at
the same time an even lower dose has already been reported to improve outcome in adult AML when
combined with different chemotherapy schedules.
4.1 Primary Study Objective
Determination of the initial efficacy of GO when added to DX-FLA in the first course of reinduction
chemotherapy in children with relapsed or refractory AML compared to DX-FLA only. Activity will be
measured by the percentage of patients having not more than 20% blasts in the bone marrow (BM)
before the second induction course.
4.2 Secondary Study Objectives
1. Determine clinical outcome in both treatment arms, defined as refractory disease, complete
remission rate after 2 reinduction courses, cumulative incidence of relapse, event-free survival and
overall survival.
2. Incidence of treatment related mortality and toxicity of GO (Mylotarg®) according to the CTCAEv4
when added to DX-FLA, in terms of mucosal toxicity, BM aplasia, liver toxicity with special respect to the
development of VOD, also called SOS), short- and long-term cardiotoxicity and other adverse reactions,
as compared to patients treated with DX-FLA only.
3.Identification of additional prognostic factors in pediatric relapsed AML, other than early treatment
response, cytogenetics and duration of complete remission (CR)1.
4. Establish a diagnostic and logistic network to obtain an individual characterization of AML based on
morphology, immunophenotype, type I and type II mutations, signal pathway activation, and monitoring
of MRD / treatment response for individualized stratification to targeted therapy within a short
timeframe.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 31 of 66
5 Study Design
5.1 Therapy Optimization Study
Intergroup, international, prospective, randomized, multicenter open-label two-arm phase III therapy
optimization study on the efficacy of GO added to standard reinduction chemotherapy in children and
adolescents with refractory or relapsed AML. Many groups in Europe and in other continents have
agreed to fulfill the conditions of participation. Regulations, legal requirements and guidelines not
mentioned in this protocol may have to be followed for individual countries.
5.2 Study Time Schedule
The study is intended to open in the fourth quarterof 2015, with end of patient recruitment in the thirds
quarter of 2020 or if the required numbers of eligible patients will be completed. Final data analysis of
the primary endpoint will be done not later than 1 year after enrollment of the last patient. Interim
analyses will be done for efficacy and toxicity after randomization of 50, 100 and 200 patients.
5.3 Number of Subjects
In this study an estimated annual recruitment of 100 children with relapsed or refractory AML is
anticipated. This results in an estimated accrual of 300 patients over 3 years, which is expected to result
in 252 randomized and fully evaluable patients with having the primary endpoint available.
5.4 Inclusion Criteria
1. Children and adolescents < 18 years of age at start of initial chemotherapy and < 21 years of age at
start of this relapsed AML treatment
2. Patients with first relapsed (including relapse after SCT) or primary refractory AML
3. Signed written informed consent from patients and/or from parents or legal guardians for minor
patients, according to local law and regulations
4. In female patients of childbearing potential pregnancy must be excluded.
5. Sexually active patients must be using two reliable contraception methods from the time of
screening/baseline and during the study for a minimum of 3 months after the last administration of
study medication. This includes every combination of a hormonal contraceptive (such as injection,
transdermal patch, implant, cervical ring) or of an intrauterine device (IUD) with a barrier method (e.g.
diaphragm, cervical cap, or condom) or with a spermicide.
5.5 Exclusion Criteria
1. Acute promyeloblastic leukemia (AML FAB type M3; please refer to your local group for the
appropriate treatment protocol)
2. Myeloid Leukemia of Down syndrome (please refer to your local group for treatment alternatives)
3. Symptomatic cardiac dysfunction (CTCAEv4 grade 3 or 4) and/or a Fractional Shortening at
echocardiography below 29%
4. A Karnofsky performance status < 40% (children ≥ 16 years) or an Lansky performance status of < 40%
(children < 16 years) before start of chemotherapy
5. Any other organ dysfunction (CTCAEv4 grade 4) that will interfere with the administration of the
therapy according to this protocol
6. Impaired liver function defined as > 3.0 x UNL for transaminases and for bilirubin
7. History of VOD
8. history hepatitis C positivity

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 32 of 66
9. Renal impairment with creatinine < 30 ml/min
10. Decompensated hemolytic anemia
11. Hypersensitivity to GO and/or other chemotherapeutic drugs
12. Inability to potentially complete the treatment protocol for any other reason
13. Pregnant or breastfeeding patients
14. Current participation in another clinical trial for the time of first course of reinduction chemotherapy
Patients who fulfill all inclusion criteria and who do not meet any exclusion criteria can be enrolled in
this trial.
If a patient fulfills the inclusion criteria but also one or more exclusion criteria or cannot be treated
according to protocol, he/she should be registered and observed (status of remission (complete
remission, non-response), events (early death, 2nd relapse, death)). It is important to have such a
registry, to know which percentage of potentially eligible patients is enrolled in this clinical trial.
Patients with a combined relapse, or an isolated extramedullary relapse, or a BM relapse (isolated or
combined) with < 20% blasts in the BM are eligible, but will not be analyzed for the primary endpoint.
In order to be able to study selection bias, please register all your primary refractory and first relapsed
AML patients, also if not being eligible for this trial.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 33 of 66
6 Definitions
6.1 Relapse
Recurrence of > 20% unequivocal leukemic blasts in a representative BM, and/or evidence of leukemic
infiltration or recurrence at any site.
6.1.1 Early Relapse
Relapse occurring within 1 year from initial diagnosis.
6.1.2 Late Relapse
Relapse occurring 1 year or later from initial diagnosis.
6.1.3 Molecular Relapse
Recurrence of leukemia specific fusion genes detected by quantitative PCR (RQ-RT-PCR with a sensitivity
of at least 10-4).
Molecular relapse should be considered if the patient specific fusion gene or aberration reoccurred after
previous negativity or increased > 1 log in quantitative PCR. An increase in peripheral blood (PB) must be
confirmed in BM. Confirmation of a molecular relapse is given if the positivity at the same level or higher
in PB and BM in an independent laboratory within 2 to 3 weeks.
6.2 CNS Disease
CNS disease is defined as:
• ≥ 5 white blood cells/mm3 (ie, ≥ 5/µl, or ≥ 15/3 µl) and unequivocal evidence of blasts on cytospin
examination,
• and/or clinical (seizures, cranial nerve palsy and symptoms of increased cranial pressure) or other
signs/symptoms not readily explained by another disease
• and/or radiological evidence of leukemic infiltration in the CNS.
In all of the symptomatic cases, a magnetic resonance imaging (MRI) should be performed.
In case of traumatic lumbar puncture (LP) CNS-Status can be judged according to the following
algorithm:
Cerebral spinal fluid (CSF) WBC / CSF red blood cells (RBC) > 2x blood WBC / blood RBC and unequivocal
evidence of blasts = CNS positive.
In the case of a LP with high blood contamination (e.g. > 100 RBC/µl), the above-mentioned algorithm
may not be applicable. Please, contact the study coordinator for individual discussion of such patients
and in other cases of difficult interpretation of the findings.
6.3 Response
6.3.1 CR/CR but with Incomplete Regeneration (CRi)
CR is defined as ≤ 5% leukemic blasts in the BM with signs of normal hematopoiesis in the BM and with
clear signs of regeneration of normal blood cell production in the peripheral blood (platelets > 50x109/l
without transfusions, neutrophils > 1.0x109/l), and no leukemic cells in the PB or anywhere else.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 34 of 66
CR but with incomplete regeneration (CRi) is defined as ≤5% leukemic blasts in the BM with signs of
normal hematopoiesis in the BM and with signs of regeneration of normal blood cell production in the
peripheral blood (platelets > 20x109/l without transfusions, neutrophils > 0.5x109/l), and no leukemic
cells in the PB or anywhere else.
6.3.2 Early Death
Death during the first 42 days of treatment (i.e., before the time, that CR/CRi could have been
documented). The cause of death (disease, therapy or both) should be recorded as well as the last
known percentage of blasts in the BM. Only patients that were randomized will be included for this
analysis.
6.3.3 Toxic Death
Death due to treatment-related complications, but not caused by the leukemia itself.
6.3.4 Partial Remission
No CR/CRi, BM leukemic blasts > 5 ≤ 20% and/or no regeneration as required for CR or CRi.
6.3.5 Early Treatment Response
This will be determined by morphological and flowcytometric examination of the BM sampled at « day
28 » (in practice anytime between day 28 and 42 after start of first reinduction chemotherapy). If the
BM shows 20% of leukemic blasts or less, the response is good. If the BM shows > 20% leukemic blasts,
the response is poor.
6.3.6 Refractory Disease/Non-Response
More than 20% of leukemic blasts in the BM after first course of reinduction chemotherapy, and/or
elsewhere documented leukemic cells.
6.4 2nd Relapse
After a documented 2nd CR, the recurrence of ≥ 10% unequivocal leukemic blasts in a representative
BM, and/or evidence of leukemic infiltration or recurrence at any site. CSF with < 5 cells/mm3 but with
blasts on the cytospin examination should be investigated repeatedly, as should the BM in case of > 5%
< 10% leukemic blasts.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 35 of 66
7 Diagnostics
7.1 Diagnostics before Start of Treatment
Before the start of the treatment the following parameters need to be obtained (study):
• BM aspiration (marrow cellularity and percentage of blasts). Perform a biopsy in case of a dry tap.
This should be performed within 3 days prior to the start of the first reinduction course. BM should also
be sent to the reference laboratory for confirmation of the diagnosis, and should be studied for
immunophenotype, molecular abnormalities and cytogenetics. Please consider to participate in research
studies.
• Complete blood count (hemoglobin, platelets, white blood cell count and differentiation). This
should be determined at the date of BM aspiration and LP as well as prior to the start of the first
reinduction course.
• Lumbar puncture (LP) (quantification of cells and protein, pathological examination), also to be done
within 3 days from the start of reinduction chemotherapy.
• Medical history (with special emphasis on history of liver toxicity and/ or VOD) and physical
examination performance status (depending on age, either the Karnofsky or Lansky Performance scale)
• Serum chemistry: creatinine, sodium, potassium, calcium, phosphate, alanine aminotransferase
(ALAT), aspartate aminotransferase (ASAT), bilirubin, uric acid, lactate dehydrogenase (LDH), glucose,
total protein, albumin
• Clotting (activated partial thromboplastin time (APTT), prothrombin time (PT), fibrinogen, D-Dimers)
• Human leucocyte antigen (HLA) typing (if not done previously)
• Viral serology (antibodies: Epstein-Barr virus (EBV), herpes simplex virus (HSV), cytomegalovirus
(CMV), parvo virus B19 (PVB19), hepatitis A, B and C virus (HAV, HBV, HCV), human immunodeficiency
virus (HIV); CMV and HCV to be assessed by polymerase chain reaction (PCR))
• Urine (protein, glucose, erythrocytes)
• Abdominal ultrasound including liver perfusion status
• MRI (=NMR) of the brain in case of (the suspicion on) localized symptomatic CNS disease
• Electrocardiogram (ECG)
• Echocardiography (please refer to the more comprehensive guidelines below)
• Lung function test (optional)
7.2 During the First Treatment Course
Disease monitoring during the first treatment course should include:
• Complete blood count at least twice weekly including transaminases
• BM aspiration at day 21 after the start of reinduction treatment to determine early clinical response,
which may be different between both treatment arms and which may have prognostic significance.
Slides and heparin-BM should also be sent to the reference laboratory for morphology and
flowcytometry, together with peripheral blood slides.
• Serum chemistry as described above at least twice weekly
• Physical examination twice weekly
7.3 Before the Start of the Second and Subsequent Treatment Courses
The remission status and toxicity should be determined before the start of the second (i.e. on day 28 or
anytime between day 28 and 42 after start of first reinduction chemotherapy, respectively) and
subsequent treatment course:
• BM and peripheral blood morphology and immunophenotype (with central review by the reference
laboratories)

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 36 of 66
• LP (quantification of cells and protein, pathological examination of the CSF)
• Physical examination
• Complete blood count
• Serum chemistry (see above)
• Echocardiography (see below)
7.4 Cardiotoxicity Monitoring
To determine possible cardiotoxicity echocardiography must be performed before the start of each
reinduction course, and within 1 week prior to the conditioning regimen as part of SCT, as well as 6
months after SCT.
In case of a normal fractional shortening (FS) of > 28%, then repeat echocardiography every 3 years
(earlier if clinically indicated). In case of an abnormal FS, then repeat echocardiography at least every
year. Additional echocardiography (and other monitoring) may be indicated in case of growth spurt,
involvement in regular strenuous exercise, growth hormone and/or sex hormone replacement therapy
and in case of pregnancy.
Technique: M-mode echo measurements according to the American Heart Association guidelines.
Whenever possible, the patient should be afebrile and have a normal hemoglobin level (at least 9 g/dl).
If an ECG is not recorded simultaneously with M-mode echo, greatest and smallest left ventricle (LV)
dimensions should be used for diastolic and systolic measurements respectively.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 37 of 66
8 Treatment Schedule
8.1 General Information
Before the start of treatment, each patient must be randomized for the addition of GO or not to DX-FLA.
In case liposomal daunorubicin is unavailable, it is suggested to use daunorubicin (3 x 60 mg/m2/dose).
However, this will be a major protocol violation and implies that patients are no longer included in the
formal study. They will be analyzed as observation patients.
It is possible that liposomal daunorubicin is not available immediately. Whenever the clinical condition
of the patients allows it, it is advised to wait up to a few days before starting treatment. Such a time
period can be used for proper diagnostics, hyperhydration and the informed consent procedure. In
patients with a very high tumor burden, a prephase with for instance low dose cytarabine can be
considered. GO should be given not later than day 7, and the last dose of liposomal daunorubicin should
not be given on the same day as GO. In other words, liposomal daunorubicin ideally is given on days 1, 3
and 5, and if necessary can be given on days 2, 4 and 6. If this is not feasible, contact the national clinical
coordinator or the PI’s for advice.
8.2 Dose Reduction for Children < 12 months or < 12 kg
Because of differences in cytarabine metabolism in young children, and in line with the experiences of
many other study groups, we recommend that children younger than 12 months of age, and/or
weighting less than 12 kg, should be treated according to body weight rather than body surface area.
For dose adjustment the prescribed doses should be corrected as follows: [weight (kg) x dose (per m2)]
divided by 30.
8.3 Special Measures for Reinduction
8.3.1 Hyperleukocytosis, High Blast Cell Counts
Patients with high peripheral blast counts (> 50-100x109/l) and significant organomegaly have increased
problems related to metabolic abnormalities, bleeding, and hyperviscosity. Platelets should be
transfused if < 15-30x109/l; in this phase, hemoglobin should not be raised above 6 mmol/l (= 9.6 g/dl);
treatment of coagulation disorders is required. The use of leukapheresis, exchange transfusion, or
hemodialysis may be necessary. To prevent tumor lysis syndrome, the patient should be well hydrated
and get rasburicase before start of therapy:
Rasburicase (Fasturtec®/Uricozyme®): 0,2 mg/kg i.v. for up to 7 days;
Hydration: 3000 ml/m²/day;
Be careful with potassium containing solutions; electrolyte substitutions only based on laboratory
results; check fluid balance and consider administration of diuretics in case of decreased urine output
(the following algorithm may be useful to calculate perspiration and fluid balance: Input = output +
400ml/m²/12h). When rasburicase is prescribed, do not apply alkalinisation.
In cases without hyperleukocytosis, or in situations when leukocytes have decreased significantly and
rasburicase could be stopped, allopurinol and alkalinisation can be initiated:
Allopurinol: 200-300 mg/m² p.o. divided q 8-12 hours; if administered without prior rasburicase, give at
least 2 doses of allopurinol prior to initiation of chemotherapy
NaHCO3: 4 g/m²/day (= 50 mEq/m²/day) to maintain urine pH 7-8

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 38 of 66
8.4 Cytarabine
During cytarabine and for 24-48 hours after completion, dexamethasone ophthalmic solution or isotears
(q 6 hours) may prevent cytarabine induced conjunctivitis.
Nurses and doctors should note the relatively high (15%) incidence of neurotoxicity, which may
necessitate to interrupt or to stop high-dose cytarabine administration.
Pyridoxine/VitaminB6 (300 mg/m²/day in 2 doses) might ameliorate cytarabine-induced mucositis.
8.5 Gemtuzumab Ozogamicin (GO, Mylotarg®)
As infusion related symptoms such as fever and chills are frequent and hypotension has as well been
reported, monitoring of vital parameters of the patient is essential during and at least 4 hours after the
end of infusion. Premedication with acetaminophen and clemastin may prevent fever and chills and
should be prescribed in all patients.
Premedication:
• Acetaminophen (paracetamol): 10mg/kg p.o. at least 2 doses every 4 hours; starting 1 hour before
start of infusion
• Clemastin (Tavegil®): 25µg/kg i.v. 10 minutes before start of GO (Mylotarg®) infusion
Start the i.v. infusion with the prescribed dose of GO (Mylotarg®) infusing 10ml over the first 15 minutes,
then repeat check of vital signs. If no adverse effects are noted increase the infusion rate to finish the
administration within 2 hours.
Check vital signs (blood pressure, heart frequency, body temperature and saturation) before start of
infusion and repeatedly at least every 30 minutes during and 4-6 hours after the end of GO (Mylotarg®)
infusion.
In case of any sign of dyspnea, hypotension or any unexpected adverse event stop infusion immediately.
Fever, chills and rigor can be expected and do not require interruption of infusion.
In case of symptomatic hypotension, fluid replacement, and/or administration of cardiostimulantia and
steroids is recommended.
Any medication that might increase the GO-mediated liver toxicity should be avoided if possible.
Especially azoles (itraconazole, fluconazole, posaconazole, voriconazole) should be withheld from 3-5
days before, during and until 3 days after administration of GO (Mylotarg®).
Because it is not known whether the pharmacokinetics of calicheamicin is influenced by enzyme
induction, strong inducers of enzymes such as St. John wort, should be avoided.
To prevent tumorlysis syndrome and ARDS a reduction of WBC below 30000/µl prior to the start of GO
(Mylotarg®) treatment is recommended.
During the first course, transaminases must be monitored at least twice a week.
8.6 Irradiation of Blood Products
Mainly due to fludarabine and body irradiation, profound and long-term lymphocytopenia can be
expected to occur. Therefore, cellular blood products should be irradiated with 25 Gy to prevent
transfusion related graft versus host disease, at least up to 6 months after the last fludarabine
administration. Of course, all blood products should be leukocyte-depleted as well. Similarly, irradiation
and leukocyte-depletion of the blood products is required at least up to 6 months after SCT.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 39 of 66
8.7 First Reinduction Course DX-FLA + GO (Mylotarg®)
Randomize to know if DX-FLA or DX-FLA + GO (Mylotarg®) should be given as 1st course!
Start reinduction chemotherapy at diagnosis or immediately following cytoreductive pre-phase (WBC <
50000/µl at day 0/1). In case of hyperleucocytosis the initial LP should be delayed until sufficient blast
reduction has been achieved (WBC < 10000/µl).
Please note: BMP day 21, and record day of peripheral blood blast clearance!
Fludarabine 30 mg/m2/day by 30 minutes i.v. infusion once every 24 hours on day 1, 2, 3, 4 and 5
(5 total doses)
DaunoXome® 60 mg/m²/day by 120 minutes i.v. infusion once every 24 hours on day 1,3 and 5
(3 total doses). Begin infusion after start of Fludarabine.
Cytarabine 2000 mg/m²/day by 3 hours i.v. infusion once every 24 hours on 1, 2, 3, 4 and 5
(5 total doses). Begin infusion 4h after start of Fludarabine.
GO (Mylotarg®) 4.5 mg/m²/day by 2h i.v. infusion on day 6
Triple IT administer in age-related dosage on day 0
in case of CNS involvement weekly until 1 week after complete blast clearance of CSF.
BMP after course 1 should be performed at the 21st day. “Day 28”, BMP at start of the 2nd reinduction
(not later than day 42) is mandatory after the start of course 1.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 40 of 66
8.8 First Reinduction Course DX-FLA
Randomize to know if DX-FLA or DX-FLA + GO (Mylotarg®) should be given as 1st course!
Start induction chemotherapy at diagnosis or immediately following cytoreductive pre-phase (WBC <
50000/µl at day 0/1). In case of hyperleucocytosis the initial LP should be delayed until sufficient blast
reduction has been achieved (WBC < 10000/µl).
Please note: BMP day 21, and record day of peripheral blood blast clearance!
Fludarabine 30 mg/m2/day by 30 minutes i.v. infusion once every 24 hours on day 1, 2, 3, 4 and 5
(5 total doses)
DaunoXome® 60 mg/m²/day by 120 minutes i.v. infusion once every 24 hours on day 1,3 and 5
(3 total doses). Begin infusion after start of Fludarabine.
Cytarabine 2000 mg/m²/day by 3 hours i.v. infusion once every 24 hours on 1, 2, 3, 4 and 5
(5 total doses). Begin infusion 4h after start of Fludarabine.
Triple IT administer in age-related dosage on day 0
in case of CNS involvement weekly until 1 week after complete blast clearance of CSF.
BMP after course 1 should be performed not earlier than 28 days after the start of course 1, but in case
of delay, not later than day 42 after the start of course 1.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 41 of 66
8.9 Second Reinduction Course FLA
The second reinduction course should be started not earlier than 28 days but not later than 42 days
after the start of the first reinduction course.
To commence this block of treatment the patient must have a neutrophil count >1.0x109/l and platelets
>50x109/l (without transfusions) and be in good clinical condition.
Perform a bone marrow (MRD, morphology and immunophenotype) and lumbar puncture on day 1.
Fludarabine 30 mg/m2/day by 30 minutes IV infusion once every 24 hours on day 1, 2, 3, 4 and 5
(5 total doses)
Cytarabine 2000 mg/m²/day by 3 hours IV infusion once every 24 hours on 1, 2, 3, 4 and 5
(5 total doses). Begin infusion 4h after start of fludarabine.
Triple IT administer in age-related dosage on day 1

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 42 of 66
8.10 Consolidation -high intensity
To be given as consolidation to patients, if a SCT is not available immediately but only to patients who
will tolerate a 3rd course of intensive chemotherapy before SCT.
Perform BMP + LP first! BMP after the 2nd reinduction course not earlier than 28 days after the start of
course 2, but in case of delay, not later than day 42 after that start and only in case of good clinical
condition. The patient must have a neutrophil count >1.0x109/l and platelets >50x109/l (without
transfusions).
Cytarabine 500 mg/m²/d day 1-4
96 hrs continous infusion
etoposide 100 mg/m²/d day 1-5
3hr-infusion
Cytarabine/Pred/Mtx i.th. day 1 LP
BMP
day 1 2 3 4 5 6
In case of a body weight <12 kg, calculate dose according to weight as follows: [weight (kg) x dose (per m2)] /30.
<1 year 1<2years 2<3years ≥ 3 years
Cytarabin 16 mg 20 mg 26 mg 30 mg
MTX 6 mg 8 mg 10 mg 12 mg
Pred 4 mg 6 mg 8 mg 10 mg
Cytarabine 500 mg/m²/day by 96 hours continuous IV infusion (day 1 to 4)
Etoposide 100mg/m²/d at day 1, 2, 3, 4, 5 by 3 hours IV infusion
Triple IT administer in age-related dosage on day 1

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 43 of 66
8.11 Consolidation – low intensity
To be given as consolidation to all patients, who will not tolerate a course of intensive consolidation
before SCT and if a SCT is not available immediately. For patients who have received GO in the first
induction course liver enzymes should be monitored vigorous before the start and during consolidation
to detect early signs of VOD or increased liver toxicity.
Perform BMP and LP first! BMP after the 2nd reinduction course not earlier than 28 days after the start
of course 2, but in case of delay, not later than day 42 after that start and only in case of good clinical
condition with platelets > 50x109/l (without transfusion) and neutrophils > 1.0x109/l.
Thioguanine 100 mg/m2/day
max. 4 weeks 1 daily oral dose (evening)
Cytarabine 75 mg/m2/day
1 daily subcutaneous injectiondays 1-4 and 15-18
Cytarabine/Pred/Mtx i.th. day 1 LP
BMP
day 1 4 15 18 28
In case of a body weight <12 kg, calculate dose according to weight as follows: [weight (kg) x dose (per m2)] /30.
<1 year 1<2years 2<3years ≥ 3 years
Cytarabin 16 mg 20 mg 26 mg 30 mg
MTX 6 mg 8 mg 10 mg 12 mg
Pred 4 mg 6 mg 8 mg 10 mg
Guidelines for discontinuation or adjustment of consolidation therapy:
Dose %
6-Thioguanin
(Thioguanin)
Leukocytes > 3.0x109/l 150
Leukocytes > 2.0x109/l; < 3.0x109/l 100
Leukocytes > 1.0x109/l; < 2.0x109/l 50
Leukocytes < 1.0x109/l 0
ALAT/ASAT > 2.0 x UNL stop and reassess
Bilirubin > 1.5 x UNL stop and reassess
(including abdominal
ultrasound and clotting
analysis)
Cytarabine
(Alexan, Udicil)
Leukocytes > 2.0x109/l, and
Platelets > 80x109/l 100
Below these counts discontinuation for 1 week
Note: all patients should get high-intensity consolidation, except selected patients who might tolerate
only this low-intensity consolidation.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 44 of 66
8.12 CNS Prophylaxis and treatment
8.12.1 CNS-Prophylaxis
Triple intrathecal medication at age-adjusted doses (table), to be given by lumbar puncture. The first
dose should be given immediately before the start of reinduction course 1.
8.12.2 CNS treatment
CNS leukemia is defined in section 6.2.
Table 2. Intrathecal triple chemotherapy for CNS leukemia
Age Cytarabine
mg/dose
Methotrexate
mg/dose
Prednisolone
mg/dose
<1 year 16 6 4
1<2 years 20 8 6
2<3 years 26 10 8
≥ 3 years 30 12 10
The second and subsequent doses should be given every 7 days until 1 week after complete clearance of
the CSF of leukemic blasts. Then, 2 more doses must be given, one immediately before the start of the
second reinduction course, and the other at the start of consolidation treatment.
Intrathecal chemotherapy is to be given via lumbar puncture or reservoir.
Cranial irradiation is not recommended, but may be considered in those patients who do achieve
complete remission but who will not undergo SCT, and who did not receive cranial irradiation in the
past.
8.13 Stem cell transplantation
In CR/CRi, all patients should proceed to alloSCT. If more time is needed to perform that SCT, intensive
and low-intensity consolidation guidelines are provided in this protocol. The choice for either the
intensive or non-intensive regimen must be based on the anticipated time until SCT and on the
condition of the patient.
This protocol does not provide guidelines on conditioning regimens, because of the lack of consensus;
this is left to each individual group. However, collaborative protocols in that setting are strongly
encouraged. Please contact your local coordinator for information on available protocols.
8.13.1 Indications for SCT
Patients in complete remission after the 2 courses of reinduction chemotherapy are eligible for SCT.
Therefore, the search for a donor should start as soon as the diagnosis of refractory or relapsed AML has
been made. The preferred type of SCT depends on the risk group and the donor availability.
Low risk = late (≥1 year from initial diagnosis) first relapse
matched sibling donor SCT
matched unrelated donor SCT
special cases: haplo-identical donor SCT /cord-blood SCT
High risk = early (<1 year from initial diagnosis) first relapse, refractory disease
matched sibling donor SCT

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 45 of 66
matched unrelated donor SCT
mismatched unrelated donor SCT
haplo-identical donor SCT /cord-blood SCT
Whatever risk group, one should in general avoid a SCT within 6 months after a previous allogeneic SCT
in view of the toxicity of such procedures. If necessary, consolidation treatment according to the low
intensity regimen could be given after the 3rd course of intensive consolidation chemotherapy to achieve
this time period.
8.14 Premature Termination of the Study
The sponsor has the right to terminate the study at any time for reasonable medical or administrative
reasons.
Also, an investigator can decide to terminate the study at the corresponding study center at any time for
reasonable medical or administrative reasons.
Premature patient discontinuation (Drop-Out)
Participation in this clinical study is voluntary. Patients and/or parents or legal guardians for minor
patients (according to local law and regulations) have the right to withdraw consent and discontinue
participation in the study at any time and for any reason and without prejudice to further treatment. If a
patient withdraws consent for participation in the study, he or she should be contacted in order to
recommend a final examination and to obtain information about any potential adverse event.
In addition, the investigator has the right to withdraw a patient from the study if the patient’s safety or
well-being is compromised by further study participation or if the patient is not compliant. Concern for
the interests of the patient must always prevail over the interest of the study.
If the study is prematurely terminated for any reason, the investigator has to ensure appropriate
therapy and follow-up for study patients. As far as possible, a final examination should be performed on
all patients who do not complete the study according to the protocol. In case of pregnancy during the
study the patient is withdrawn immediately from the study and must be seen by a gynaecologist.
The following reasons may lead to drop-out:
(1) death
(2) consent withdrawal by the patient
(3) lost to follow-up
(4) other reasons

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 46 of 66
9 Drug Information, Expected Toxicity and Dose Adjustments
9.1 Cytarabine
This nucleoside analogue (pyrimidine antagonist) is an antimetabolite that is mainly metabolised in the
liver. It may cause myelosuppression, hepatotoxicity, exanthema, malaise, and gastro-intestinal toxicity
such as nausea, vomiting, stomatitis, and ileus. At high doses, fever, severe diarrhea, CNS disturbances
such as somnolence, cerebellar ataxia and nystagmus, keratitis, VOD, pneumonitis and adult respiratory
distress syndrome with streptococcus viridans infection are possible. I.th. administration has been
associated with headache, fever, vomiting, and pleiocytosis, rarely with aseptic meningitis or CNS
disturbances. To prevent keratitis, indifferent or corticoid eye drops every 4-6 hours are recommended
during and until 12 hours after stopping cytarabine. Prolonged corticoid eye drops have side-effects as
well, such as infection. Conjunctivitis should be treated with corticoid eye drops. To prevent
streptococcal infection, penicillin prophylaxis may be considered starting as soon as neutropenia
develops after high-dose cytarabine until neutrophils > 0.5x109/l.
Patients who developed grade 3 or 4 neurotoxicity following high-dose cytarabine should not receive
further high-dose cytarabine, but are eligible for continuous lower-dose cytarabine.
I.th. administration
IT cytarabine should be reconstituted with physiologic buffered diluents (lactated Ringer's, 0.9% sodium
chloride, Elliott’s B solution) or patients own CSF. Do not use Bacteriostatic Water to reconstitute for IT
administration, use only preservative free solutions.
9.2 Fludarabine
This nucleoside analogue (purine antagonist) is an antimetabolite that is excreted mainly in the urine.
After phosphorylation, it is less susceptible to deamination than cytarabine. Main side-effects are
myelosuppression, fever, chills, malaise, nausea, and vomiting. Rarer are auto-immune phenomena
(hemolytic anemia), pneumonitis, and CNS symptoms such as agitation. Since it causes profound and
long-term lymphocytopenia, irradiation of blood products to prevent graft-versus-host disease and
antifungal prophylaxis is strongly recommended, from the start of treatment until 6 months after SCT or
if SCT is not being performed until 6 months after the last administration of fludarabine.
9.3 Gemtuzumab Ozogamicin (GO, Mylotarg®)
The Investigational medicinal product (IMP) GO (Mylotarg®) is a conjugated monoclonal CD33 antibody
that selectively targets CD33 positive cells. CD33 is a glycoprotein belonging to the sialoadhesin familiy
und is expressed on granulocytes and monocytes but not on CD34 positive hematopoietic stem cells,
lymphocytes and non-hematopoietic tissues. GO (Mylotarg®) is composed of a humanized IgG4 class
monoclonal antibody linked to a derivate of the antineoplastic antibiotic calicheamicin. Calicheamicin is
an antineoplastic antibiotic. The most common adverse reactions of GO (Mylotarg®) treatment are
neutropenia and thrombocytopenia as well as infusion related fever, chills, hypotension and dyspnea
which mostly disappear upon treatment with acetaminophen and occasionally steroids. Rare cases of
severe and fatal hypersensitivity have been reported. Regarding prevention of infusion related
symptoms and treatment of hypersensitivity note guidelines for GO (Mylotarg®) infusion specified in
section 8.5. Tumorlysis syndrome and adult respiratory distress syndrome (ARDS) have been reported in
patients with leukocytes > 30000/µl treated with GO (Mylotarg®). Therefore reduction of WBC below
30000/µl prior to the start of GO (Mylotarg®) treatment is recommended.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 47 of 66
Hepatic toxicity with elevation of liver enzymes and bilirubin is encountered in about 30% of patients
after GO (Mylotarg®) treatment and is reversible in most cases. Frequency of severe liver toxicity and
VOD is estimated to occur in 4-5% of patients, with higher frequencies in patients after stem cell
transplantation. Therefore patients are required to have normal liver function defined as transaminases
and bilirubin < 3 x UNL. Patients with impaired liver function according to this criteria and/ or history of
VOD are not eligible for randomization and GO (Mylotarg®) treatment.
Any medication that might increase the GO-mediated liver toxicity should be avoided if possible.
Especially azoles (itraconazole, fluconazole, posaconale, voriconazole) should be withheld from 3-5 days
before, during and until 3 days after administration of GO (Mylotarg®).
9.4 Liposomal Daunorubicin (L-DNR/DX)
This drug is the combination of an anthracycline with a unilamellar liposomal transport system.
Daunorubicin is released slowly, and then mainly excreted in the bile, less so in the urine. Daunorubicin
itself is metabolized to daunorubicinol, which is again mainly excreted in the urine and in the bile. The
drug should be solubilized in dextrose 5% only, because of agglutination in other solutions! Although not
reported for L-DNR, the concomitant use of daunorubicin with heparin or dexamethasone i.v. is
complicated by precipitation. Therefore, these drugs should not be used simultaneously i.v. with L-DNR.
Side-effects that have been described were nausea, vomiting, mucositis, hepatotoxicity and the dose-
limiting toxicity is myelosuppression.
In case of a fractional shortening at echocardiography below 29%, L-DNR should not be given.
In case of hepatic disturbances before the first administration of L-DNR, a reduction for all three doses is
recommended:
Transaminases > 2.5 times upper normal limit (UNL): reduction of 25%.
Transaminases > 5-10 times UNL: reduction of 50%
Transaminases > 10 times UNL: not eligible
All three doses of L-DNR should be similar, in other words, no further reductions after the first dose.
9.5 Prednisolon
Injection solution: The i.th. application of prednisolon seems not to add relevant adverse
reactions/toxicities in childhood AML. To date there are no reports of specific or relevant adverse
reactions in children with acute leukemia.
9.6 Methotrexate
Injection solution
Severe systemic toxicities such as myelosuppresssion or mucositis have rarely been reported. They may
occur in particular subgroups, e.g. children with trisomy 21 (excluded in the trial). In case of systemic
adverse reactions, a rescue with 15mg/m² of leukovorin is indicated, given 48 hour following the i.th.
injection.
Subacute neurological symptoms such as seizures, somnolence or phases of aphasia, associated to i.th.
methotrexate, rarely occurred about one or two following injection. Typically the symptoms were
transient for some hours or days. Additional diagnostic (MRT / CCT) is mandatory to exclude other
complications like bleedings, thrombosis or invasive infections.
9.7 Thioguanin
This purine antagonist is an antimetabolite that is metabolized rapidly and then excreted renally. It may
cause myelosuppression, nausea, vomiting, anorexia, mucositis, diarrhea, hepatotoxicity, and veno-
occlusive disease.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 48 of 66
9.8 VP-16 (Etoposide)
This inhibitor of DNA topoisomerase II should not be infused intravenously in less than 1 hour because
of the risk of hypotension and anaphylaxis. The drug has several side-effects, including nausea, vomiting,
alopecia, and myelosuppression. More rare side-effects are fever, headache, cholestasis, mucositis and
peripheral neuropathy. Dose reduction is indicated in case of hepatic dysfunction.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 49 of 66
9.9 Source of Chemotherapeutic Drugs/IMP and Labelling
The IMP GO (Mylotarg®) will be supplied free of charge by Pfizer and will be labelled by a qualified
company charged by the sponsor.
All other chemotherapeutic drugs need to be purchased from commercial stock.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 50 of 66
10 Statistical Considerations and Randomization Procedure
This is an international multicenter open label randomized phase III clinical study on the treatment of
children with relapsed or refractory AML. All patients who fulfill the inclusion criteria and for whom no
exclusion criterion is given can be randomized to receive DX-FLA or DX-FLA/GO as the first course of
reinduction chemotherapy therapy.
The measures to minimize bias in this open label study include the following:
In order to be able to study a possible selection bias all primary refractory and first relapsed AML
patients have to be registered, also if not being eligible for the randomized trial. The treatment
sequence for patients to be randomized will not be known to the investigator since a central web based
randomization procedure will be used. The assessment of the main target criterion (percentage of BM
blasts after the first course of reinduction chermotherapy on day 28) will be done centrally at the
reference lab of each group. Randomization is done centralized via the web-database and stratified by
study group and time of relapse (early and late relapse) or nonresponse to front line treatment. The
main study question is:
Can the response to the first course of standard reinduction chemotherapy (DX-FLA) be improved by
addition of the conjugated anti-CD33 antibody GO linked to calicheamicin?
10.1 Endpoints
Primary Endpoint
The primary endpoint is the percentage of BM blasts after the first course of reinduction chemotherapy
on “day 28” (in practice anytime between day 28 and 42 after start of first reinduction chemotherapy
and before the start of the second reinduction course) given as ≤ 20% or > 20%.
Secondary Endpoints
Secondary end points are refractory disease, CR and CRi rates, cumulative incidence of relapse, OS
(event: death from any cause), EFS (events: death from any cause, non-response, relapse or second
malignancy) and DFS (events: death from any cause, relapse or second malignancy) for patients who
reach CR/CRi. Survival times will be calculated from date of diagnosis of relapse or nonresponse to
frontline therapy (or date of CR/CRi for DFS) to last follow-up or first event. These parameters of clinical
treatment response will be compared between both arms.
In addition toxicity of GO when added to DX-FLA in terms auf BM aplasia, liver toxicitiy including VOD,
cardiotoxicity, mucosal toxicity and other adverse reactions.
Toxicity will be measured by duration of bone marrow aplasia and by CTCAEv4 grading for mucosal
toxicity, short- and long-term cardiotoxicity, liver toxicity and other CTCAEv4 scales which are
considered to be relevant in relapsed AML and the proposed therapy.
Moreover, this will not only be analyzed in the total population, but also in well-described subgroups as
defined by cytogenetics (core-binding factor AML, MLL-rearranged AML, and AML with unfavorable
karyotype), duration of CR1 (early versus late relapse) and early treatment response (good versus poor).
These subgroup analyses are prospective but will be exploratory and the study cannot be powered on
these subgroups.
Additionally this study aims at identifying new prognostic factors in relapsed pediatric AML other than
early treatment response, cytogenetics and duration of first remission.
As the future integration of target therapies early in induction regimens diagnostic procedures for the
biological characterization of the leukemic cells must be realized within a short timeframe. This study
aims at providing a complete biological characterization within 8 days.
10.2 Analysis
The analysis of the primary endpoint will be performed on all randomized patients according to the
intent-to-treat principle, but with data on the treatment response available and excluding patients with

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 51 of 66
<20% leukemic cells in the BM before start of therapy. The difference in response rate (≤ 20% or > 20%
blasts in the BM at “day 28“) will be tested with a logistic regression model taking into consideration
time from first diagnosis of AML to relapse and whether patients had primary refractory AML or
relapsed disease.
For patients with less than 20% blasts in the BM the primary endpoint (the percentage of BM blasts
after the first course of reinduction chemotherapy given as ≤ 20% or > 20%.) cannot be judged. There
are only very rarely cases where the blast count increases after a block of chemotherapy. Patients with
less than 20% blasts in the BM initially will dilute the treatment effect. But a treatment effect in terms of
the secondary endpoints, especially overall survival, is expected also for those patients, e.g. patients
with isolated CNS-relapse. Therefore all patients who enter the study will be analysed for the secondary
endpoints.
A supplementary analysis of the first endpoint including all patients irrespective of the initial blast count
will be made.
10.3 Sample Size
The percentage of patients with > 20% BM blasts at “day 28” is expected to be about 20% in the control
arm (according to the results of the experimental arm of study Relapsed AML 2001/01). We expect a
reduction of this percentage to 9% (same reduction as has been shown for study Relapsed AML 2001/01
from 30% to 19%).
The expected number of patients that will be included in this trial is 85/year, based on the participation
of the above mentioned clinical groups. The study duration will be 5 years, or less in case of a higher
accrual rate. Assuming a randomization rate of 75%, about 315 patients will be randomized. Based on
experience from the study Relapsed AML 2001/01, that will provide 252 patients with known data on
the “day 28” BM. The power will then be 80% to detect a decrease in the number of patients with > 20%
BM blasts at day 28 from 20% to 9% (one-sided test, alpha=5%). If less than 252 randomized patients
with known data on the “day 28” BM have been recruited during the planned recruitment time due to
withdrawal or drop out the recruitment will be extended until the required number of patients is
reached.
10.4 Interim and Final Analysis
The final analysis of the primary endpoint will be performed approximately 6 months after
randomization of the last patient (at least within one year), final analysis of survival endpoints will be
performed 5 years after the inclusion of the last patient. Interim analyses for efficacy and toxicity are
planned after 50 (toxicity only), 100 and 200 patients. The study statistician will perform the interim
analysis. He will make the original data available to the statistician of the data monitoring committee in
order to check the results. Only members of the steering committee and the DMC will see the interim
analyses unless the study has to be amended or stopped because of the results. The O’Brien and
Fleming rules will be followed for alpha-correction of the efficacy analysis (p=0.0002 for the first, 0.012
for the second interim analysis und 0.046 for the final analysis).
Dose-reduction of GO (Mylotarg®) from 4.5 mg/m2 to 3.0 mg/m2 will be considered if mortality (see
below) and/or grade III/IV toxicity will be judged as too high by the DMC and the steering committee at
an interim-analyses (after 50, 100 and 200 patients). Toxicity will be analyzed in the perspective of
reversibility and the need to postpone treatment, and will focus on grade III/IV liver toxicity (including
VOD) which should not exceed 10%, except for raised transaminases, acute reversible non-doses
dependent allergic reactions and reversible elevation of transaminases. In addition, special attention will
be given to platelet recovery, in the context of data from study Relapsed AML 2001/01, and in the light
of the planned allo-SCT in all patients achieving CR/Cri.
The absolute death rate observed in each arm (and globally in the whole population) will be compared
to a reference rate (8% of the patients died within 70 days after diagnosis in study Relapsed AML
2001/01) in order to detect an absolute excess of deaths. All patients who die during induction therapy

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 52 of 66
up to 10 weeks of therapy or have a follow up of at least 70 days will be included to calculate the rate of
induction death (see table, left column). If with a given number of patients the number of deaths should
reach the limit (see table, right column), the DMC and the study steering committee have to decide
about stopping or continuing the study. Based on previous experience, we choose the following
parameters: p0 = 8 % and p1 = 16 % with α = 5% and β = 1%. This means that the risk to wrongly
conclude that there is an excess of deaths (whereas the real rate is equal to p0 ≤ 10) is equal to α = 5%.
On the other hand, the power to detect an excess of deaths (if the real rate is equal to p1 = 20 is equal to
1-β = 99%. Major/Serious adverse events and death rate will be monitored continuously.
Wald sequential plan to detect an excess of deaths
N (death within/follow-up of at least two months) N (death within 70 days of therapy)
-10 5
-18 6
-27 7
-36 8
-44 9
-53 10
-61 11
-70 12
-79 13
-87 14
-96 15
-105 16
-113 17
-122 18
-130 19
-139 20
-148 21
-156 22
-165 23
-174 24
10.5 Data Management
The chair of international study coordinators, the co-chair of international study coordinators and the
international study statistician will act as a co-ordination unit for the monitoring and exchange of
information and for the pooling of the data.
The Trial Data Center, in collaboration with the International Study Coordinator, the Contact Persons
and the Statisticians of each group, will be responsible for maintaining the Good clinical practice (GCP)-
compliant study web-database (based on the EDC-system MARVIN, XClinical, Munich, Germany) and
evaluating the data according to the protocol aims.
10.6 Data Monitoring Committee (DMC)
Such a committee (two clinicians and one statistician) has been installed (Y. Ravindranath, USA; P. Vyas,
UK; H. van Houwelingen, NL). Members of the DMC are experienced researchers not involved in the trial
who will be responsible for providing the principal investigators with guidance on the trial conduction
and, in case of problems, on whether the trial should be stopped, modified or continued (for details see
the DMC Charter in its actual version).

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 53 of 66
The DMC closed meetings will take place at least once a year through e-mail communications and
possibly conference calls. Additional meetings will be possible and can be scheduled in case the DMC
judges that these are needed.
The DMC will receive from the trial statistician a report approximately at annual intervals, starting from
2012. The first and second report will be focused on recruitment/trial integrity and early safety, while
the following reports will review data relating to treatment efficacy, patient safety and quality of trial
conduct and will include the interim analyses as planned in the protocol.
Before reporting on the safety and results of the trial the DMC will consider not only the interim results
of the study but also any major new information from other sources considered to be relevant to the
trial. In this perspective, the DMC will be guided by the pre-assigned statistical rules stated in the
protocol, but will not apply them automatically.
A joint meeting of DMC and the SSC will follow the closed DMC annual meeting, to discuss the issues
raised about the annual report if the DMC or the study steering committee judges that this is needed.
Such meeting will normally be organized as conference call.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 54 of 66
11 Safety Evaluation
11.1 Definitions
11.1.1 Adverse Event (AE)
An Adverse Event (AE) is any untoward medical occurrence in a patient administered the IMP (GO) and
which does not necessarily have a causal relationship with this treatment/procedure. An AE can be any
unfavorable and unintended sign (including an abnormal laboratory finding), symptom, or disease.
11.1.2 Adverse Reaction (AR)
An Adverse Reaction (AR) is any untoward and unintended response to the IMP related to any dose
administered. A response to the medicinal product is given when a causal relationship between the
adverse event and the IMP is at least a reasonable possibility.
The definition of AR also applies to the term “toxicity”.
11.1.3 Serious Adverse Event (SAE)
A serious adverse event (SAE) or serious adverse reaction (SAR) is any untoward medical occurrence that
at any dose:
� results in death
� is life threatening (i.e., in the opinion of the investigator, the subject is at immediate risk of death
from the event)
� requires inpatient hospitalization or prolongation of existing hospitalization
� results in persistent or significant disability/incapacity
� is a congenital anomaly/birth defect in the offspring
� is considered a secondary malignancy other than a relapse of the current disease
In addition, important medical events that may not result in death, be life-threatening, or require
hospitalization may be considered an SAE when, based upon appropriate medical judgment, they may
jeopardize the subject and may require medical or surgical intervention to prevent one of the outcomes
listed in the definition above.
The following events do not fulfill the definition of an SAE:
• Events which might have resulted in a life-threatening situation but did not.
• Elective hospitalization during participation in a trial for an intervention or diagnostic
procedure for a condition which was present before entering the trial.
11.1.4 Exceptions to SAE-Reporting and Expected Leukemia Treatment
Associated Events
For malignancies with a fatal outcome within the study reporting period, the disease progression must
be reported as an SAE, with death listed as the qualifying SAE criterion.
However, progression of the malignancy should NOT be reported as an SAE and hospitalization due to
signs and symptoms of malignancy progression does NOT require reporting as an SAE.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 55 of 66
11.1.5 Serious Adverse Reaction A Serious Adverse Reaction (SAR) is an Adverse Reaction (AR) that fulfills at least one of the seriousness-
criteria listed under section 11.1.3. The exceptions from reporting obligations (see section 11.1.4) apply
accordingly.
11.1.6 Suspected Unexpected Serious Adverse Reaction (SUSAR)
A SAR, the nature or severity of which is not consistent with the applicable product information of the
IMP is considered a Suspected Unexpected Serious Adverse Reaction (SUSAR).
11.1.7 Reference Document / Applicable Product Information
The applicable product information for this trial is the investigator´s brochure (IB) for the IMP GO
(Mylotarg®) in its edition 9 of November 2010 or its updates.
11.2 Documentation and Evaluation of Adverse Events
The CTCAEv4 are applied for reporting AEs. CTCEAv4 (as pfd) and instruction how to use CTCAEv4 can be
found on http://ctep.info.nih.gov/reporting/ctc.html. This will not be incorporated into the protocol.
Each AE can be graded according to its severity. CTCAEv4 categories the grades based on these general
guideline:
Grade 1 mild AE
Grade 2 Moderate AE
Grade 3 Severe AE
Grade 4 Life Threatening or disabling AE
Grade 5 Death related to AE
Any treatment-related adverse event experienced by a patient is graded using the specific adverse event
terms listed in the CTCAEv4. Grading is not modified based on a patient’s condition at baseline. If a given
AE is experienced more than once during a cycle, only the grade associated with the most severe AE is
documented. AEs not included in the CTCAEv4 should be documented and graded as “Other” and
graded 1-5 based on individual assessment.
AEs will be collected by the investigator either based on the information provided spontaneously by the
patient or evaluated by non-suggestive questions. The following information will be documented:
� Type of AE (disease, symptoms).
� Classification (serious vs. non serious).
� Start and termination date of the AE.
� Grading of AE-intensity (grade 1-5)
� Causality to the study drug
� Measures taken with regard to study medication and treatment of the AE.
� Outcome of the AE.
AEs will be documented on clinical report forms by the investigator and send to the national
documentation and data management center. The national data manager will enter documented AEs in
the web based Study Data base for central review and toxicity monitoring.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 56 of 66
11.3 Documentation and Reporting of Serious Adverse Events
In compliance with EU-Directive 2001/20/EC and ICH Guidelines for GCP, SAEs must be documented and
reported to the sponsor’s delegate immediately, i.e. within 24h, by the investigator using the protocol
specific SAE paper form by fax.
Initial SAE reports must be amended with a follow-up report when relevant details or additional
information to the case arise. This follow-up SAE report should be faxed to the sponsor’s delegate as
soon as the new relevant information is available.
The documentation and reporting period starts on the day of administration of the IMP GO (Mylotarg®)
and ends 28 days afterwards.
In case of death, an autopsy should be aimed for and the results should be forwarded to the principal
investigator and the sponsor’s delegate.
11.4 SAE Reporting after the End of Trial Treatment
During the follow-up phase (starting on day 28 after administration of the IMP GO (Mylotarg®) and
during the 5 year follow-up), the following events have to be reported to the sponsor:
• Fatalities and severe events possibly, probably or definitely related to late effects of therapy
• Disabling events
• Secondary cancer
11.5 SAE Reporting Procedures and Time Limits
The investigator or its designee must fax the SAE report form of any occurred SAE as defined by the
protocol in section 12.1.3 within 24 hours of knowledge of the event to the sponsor’s delegate for
pharmacovigilance:
AML-BFM Trial Centre
Hufelandstraße 17
45147 Essen
Fax: +49 (0)201 8777 5484
and will be forwarded from there to Pfizer Pharmacovigilance (SAE reports of the GO-group).
11.6 Pregnancies
Any pregnancies occurring within the reporting period have to be reported to:
AML-BFM Trial Centre
Hufelandstraße 17
45147 Essen
Fax: +49 (0)201 8777 5484
and will be forwarded from there to Pfizer Pharmacovigilance.
In accordance with Pfizer Pharmacovigilance requirements, pregnancies have to be followed until an
outcome of the pregnancy is documented with information about the status of both, mother and child.
Any preterm termination of pregnancy also has to be reported.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 57 of 66
11.7 Events Associated with Pharmaceutical Quality
Any findings or events that are encountered with the IMP that may be attributed to shortcomings of
pharmaceutical quality must be reported informally to:
AML-BFM Trial Centre
Hufelandstraße 55
45122 Essen
Fax: +49 (0)201 723 5308
11.8 Overdosing
Significant overdosing must be reported as a serious adverse event by the investigator to the sponsor’s
delegate.
AML-BFM Trial Centre
Hufelandstraße 55
45122 Essen
Fax: +49 (0)201 723 5308
11.9 SUSAR Reporting Procedures and Time Limits
In case of the occurrence of a SUSAR it is the responsibility of the sponsor of the study to report these to
the national competent authorities (NCA) of all countries in which study centers are initiated, the
leading Independent ethics committee (IEC) as well as to the investigators of the trial - in line with
relevant national laws and regulations.
Fatal or life-threatening SUSARs must be reported within 7 days, all other SUSARs need to be reported
within 15 days. Also, all circumstances that require reevaluation of the benefit-risk ratio of the IMP have
to be reported within 15 days in the same way as SUSARs. This includes:
• Case reports of expected SARs with an unexpected outcome.
• Increased incidence of SARs which is considered clinically relevant.
• Cases of suspected SUSARs which occurred in patients after completion of the trial participation.
• Occurrences in relationship to the trial or the IMP which might affect the safety of the
participants.
11.10 Annual Safety Reporting
Once a year throughout the clinical trial or on demand, the sponsor or his authorized delegate shall
provide the NCA of all countries in which participating trial centers are initiated and the leading IEC with
a listing of all suspected serious adverse reactions which have occurred over this period and a report of
the subject’s safety.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 58 of 66
12 Publication and Other Policies
12.1 Authors on Abstracts and Manuscripts
Final main publications to be written by international study coordinators; the manuscript on the main
study question (primary endpoint) will be written by the PI and co-PI.
Members of the steering committee of the protocol will be included.
Clinical contact persons of each of the participating groups, if a total of at least 10 patients have been
included from that group in the Pediatric Relapsed AML 2010/01 study, will be included.
Manuscripts concerning add-on studies only will include those who made a significant contribution to
that particular study, including the PI and co-PI. in case clinical data are being used, according to
international guidelines for authorship
12.2 Acknowledgements in Manuscripts
All of those who made a significant contribution to the preparation, execution and/or analysis of the
study, not included as a co-author, will be mentioned in the acknowledgements. Examples are: data
managers of each of the participating groups, and clinical representatives of groups who did not fulfill
the requirements for co-authorship. In addition, the International BFM Study Group will be mentioned
as the platform on which the study has been performed.
12.3 Other Guidelines
Any publication, abstract or presentation based on patients included in the international studies:
approval is required by both international study coordinators.
Publications (including abstracts, presentations etc.) comparing the randomized treatment arms and/or
concerning study end-points by individual groups are not allowed, until final results of the international
studies have been published. An exception will be made if the international study coordinators fail to
submit a manuscript for publication within 3 years after closure of the patient enrolment.
Participating groups are obliged to send all required patient data every 6 months to the central data
office in Hanover. Groups who fail to do so will lose their status as collaborating group.
The trial will be registered at the EU Clinical Trials Register according to current publication guidelines.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 59 of 66
13 Ethical, Regulatory and Administrative Aspects
13.1 Responsibilities
This study will be conducted in compliance with the protocol and in accordance with the ethical
principles that have their origin in the current Declaration of Helsinki, and will be consistent with
International Conference on Harmonization Good Clinical Practice (ICH GCP) and applicable regulatory
requirements.
Investigators must have sufficient time to conduct the clinical study in compliance with the study
protocol. Furthermore, they have to accurately and completely enter study data in the CRF.
Investigators are responsible for obtaining informed consent of the patients and/or from parents or
legal guardians for minor patients, according to local law and regulations as well as for the preparation
and maintenance of adequate case files in order to record observations and other data relevant for this
clinical study. Besides, they have to file the study-related records in the trial investigator file (TIF) and
have to maintain its actuality. They will permit study-related monitoring visits, audits by the sponsor or
its representatives as well as inspections by regulatory authorities. The investigator must provide direct
access to the study site’s facilities, to source documents, and to all other study documents.
The rights, safety and well-being of the trial subjects are the most important considerations and should
prevail over interests of science and society.
Study personnel involved in conducting this trial will be qualified by education, training, and experience
to perform their respective task(s), and will be authorized to perform study related procedures as laid
down in the delegation of authority log.
Systems with procedures that assure the quality of every aspect of the study will be implemented.
13.2 Favorable Opinion of Independent Ethics Committee (IEC) and
Approval of National Competent Authority (NCA)
The protocol and any amendments will receive favorable opinion of IEC and approval of NCA prior to
initiation of the study according to local laws and regulations.
13.3 Patient Information and Informed Consent
The investigator is responsible for obtaining patient’s and/or parents and/or legal guardians written
informed consent after adequate explanation of the aim, study assessments, potential risks and benefits
and consequences of the study as well as alternative treatment options. The patient
information/informed consent form has to be signed in duplicate by the patient’s and/or parents and/or
legal guardians for minor patients, according to local laws and regulations and the investigator. One
document will be given to the patient, the other one remains in the TIF at the trial site. No study
procedures are allowed to be conducted until patient’s written informed consent has been obtained.
The patient information/informed consent form has to be revised whenever important new information
becomes available that may be relevant to the subject’s consent. The patient’s and/or parents and/or
legal guardians for minor patients have to be informed and asked to give their consent to continue study
participation by signing the updated form.
Participation in this clinical trial is voluntary. Withdrawal from the trial at any time and for any reason is
without any disadvantages to the patient’s further treatment.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 60 of 66
13.4 Data Protection All study staff has to give due consideration to data protection and medical confidentiality. The
collection, transfer, storage and analysis of personal study-related data are performed pseudonymized
according to national laws and regulations.
13.5 Financing
The study is supported by Pfizer Pharma and the “Deutsche José Carreras Leukämie-Stiftung e.V“.
No financial compensation will be given to the patients for participating in this study.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 61 of 66
14 Sponsors
German Society of Pediatric Hematology and Oncology gGmbH (GPOH gGmbH) will be the international
sponsor of this study. In addition, national representatives of the international sponsor will have to be
identified, normally representing the national study group in question. Certain tasks will be delegated by
the sponsor to the national representatives, also referred to as ‘co-sponsor’..
The co-sponsor in each country will be responsible for financing the clinical trial in that country and
provide insurance or indemnity in accordance with the applicable regulatory requirements for all
patients within that country.
Any investigator who signed this protocol agrees to carry out this research in accordance with the
protocol, ICH GCP and relevant regulatory requirements.
Study personnel involved in conducting this trial will be qualified by education, training, and experience
to perform their respective task(s).
Each local investigator should provide the co-sponsor with his CV. The co-sponsors assure the sponsor
that this has been taken care off.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 62 of 66
15 Monitoring, Audits and Inspections
Monitoring, audits and inspections are performed for reasons of quality assurance and to verify that the
study is conducted according to the protocol as well as to legal and regulatory requirements applicable
for clinical trials as well as International Conference on Harmonisation ICH GCP guidelines.
15.1 Monitoring
Monitors will ensure that the clinical trial is conducted, recorded, and reported in accordance with the
protocol, ICH GCP, and the applicable regulatory requirement(s). The sponsor will delegate monitoring
activities to national/local co-sponsors.
Representatives of the sponsor and/or co-sponsor must be allowed to visit all study site locations
periodically to assess the data, quality and study integrity. On site they will review study records and
directly compare them with source documents, discuss the conduct of the study with the Investigator,
and verify that the facilities remain acceptable. Source documents are defined as: patient files, letters
and laboratory / histology records. The type and scope of monitoring will be defined in the Monitoring
Manual and documented on study specific Source Data Verification Forms.
With his participation in the study the investigator is obligated to support the activities of the monitors,
provide them with direct access to the files and give them the opportunity to inspect the laboratory
facilities, storage of the investigational product, etc.
15.2 Audits and Inspections
Audits (by the sponsor) and inspections (by regulatory authorities) may be performed in order to verify
that the clinical study is performed according to the study protocol as well as to AMG, ICH GCP and/or
other applicable regulatory requirements. The auditor or inspector is independent in regard to
personnel involved in the conduct of this clinical trial. The investigator has to provide the
auditor/inspector direct access to all study-related documents.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 63 of 66
16 Reference List
1. Kaspers GJL, Zimmermann M, Reinhardt D, Gibson B, Tamminga R, Armendariz H, Dworzak M, Ha S, Hovi L,
Maschan A, Baruchel A, Bertrand Y, Razzouk B, Rizzari C, Smisek P, Smith O, Stark B, Creutzig U. Long-Term
Continuing Second Complete Remission (CCR2) despite Allogeneic Stem Cell Transplantation in CR1: Results
from the International Randomised Phase III Study Pediatric Relapsed AML 2001/01. Blood. 2008;112:1023.
2. Hinman LM, Hamann PR, Wallace R, Menendez AT, Durr FE, Upeslacis J. Preparation and characterization of
monoclonal antibody conjugates of the calicheamicins: a novel and potent family of antitumor antibiotics.
Cancer Res. 1993;53:3336-3342.
3. Voutsadakis IA. Gemtuzumab Ozogamicin (CMA-676, Mylotarg) for the treatment of CD33+ acute myeloid
leukemia. Anticancer Drugs. 2002;13:685-692.
4. van dV, V, te Marvelde JG, Hoogeveen PG, Bernstein ID, Houtsmuller AB, Berger MS, van Dongen JJ.
Targeting of the CD33-calicheamicin immunoconjugate Mylotarg (CMA-676) in acute myeloid leukemia: in
vivo and in vitro saturation and internalization by leukemic and normal myeloid cells. Blood. 2001;97:3197-
3204.
5. Dowell JA, Korth-Bradley J, Liu H, King SP, Berger MS. Pharmacokinetics of gemtuzumab ozogamicin, an
antibody-targeted chemotherapy agent for the treatment of patients with acute myeloid leukemia in first
relapse. J Clin Pharmacol. 2001;41:1206-1214.
6. Buckwalter M, Dowell JA, Korth-Bradley J, Gorovits B, Mayer PR. Pharmacokinetics of gemtuzumab
ozogamicin as a single-agent treatment of pediatric patients with refractory or relapsed acute myeloid
leukemia. J Clin Pharmacol. 2004;44:873-880.
7. Appelbaum FR, Matthews DC, Eary JF, Badger CC, Kellogg M, Press OW, Martin PJ, Fisher DR, Nelp WB,
Thomas ED. The use of radiolabeled anti-CD33 antibody to augment marrow irradiation prior to marrow
transplantation for acute myelogenous leukemia. Transplantation. 1992;54:829-833.
8. Sievers EL, Appelbaum FR, Spielberger RT, Forman SJ, Flowers D, Smith FO, Shannon-Dorcy K, Berger MS,
Bernstein ID. Selective ablation of acute myeloid leukemia using antibody-targeted chemotherapy: a phase I
study of an anti-CD33 calicheamicin immunoconjugate. Blood. 1999;93:3678-3684.
9. Petersdorf S. Preliminary results of Southwest Oncology Group Study S0106: An international intergroup
phase 3 randomized trial comparing the addition of gemtuzumab ozogamicin to standard induction therapy
versus standard induction therapy followed by a second randomization to post-consolidation gemtuzumab
ozogamicin versus no additional therapy for previously untreated acute myeloid leukemia [abstract]. Blood.
2009;114:326.
10. Burnett AK, Kell WJ, Goldstone AH, Milligan D, Hunter A, Prentice AG, Russell NH, Gibson B, Wheatley K, Hills
RK. The addition of gemtuzumab ozogamicin to induction chemotherapy for AML improves disease free
survival without extra toxicity: Preliminary analysis of 1115 patients in the MRC AML15 trial. Blood.
2006;108:8A.
11. Castaigne S, Pautas C, Terre C, Raffoux E, Bordessoule D, Bastie JN, Legrand O, Thomas X, Turlure P, Reman
O, de Revel T, Gastaud L, de Gunzburg N, Contentin N, Henry E, Marolleau JP, Aljijakli A, Rousselot P, Fenaux
P, Preudhomme C, Chevret S, Dombret H. Effect of gemtuzumab ozogamicin on survival of adult patients
with de-novo acute myeloid leukaemia (ALFA-0701): a randomised, open-label, phase 3 study. Lancet.
2012;379:1508-1516.
12. Ravandi F, Estey EH, Appelbaum FR, Lo-Coco F, Schiffer CA, Larson RA, Burnett AK, Kantarjian HM.
Gemtuzumab ozogamicin: time to resurrect? J Clin Oncol. 2012;30:3921-3923.
13. Burnett AK, Hills RK, Hunter AE, Milligan D, Kell WJ, Wheatley K, Yin J, McMullin MF, Dignum H, Bowen D,
Russell NH. The addition of gemtuzumab ozogamicin to low-dose Ara-C improves remission rate but does
not significantly prolong survival in older patients with acute myeloid leukaemia: results from the LRF
AML14 and NCRI AML16 pick-a-winner comparison. Leukemia. 2012.
14. Zwaan CM, Reinhardt D, Zimmerman M, Hasle H, Stary J, Stark B, Dworzak M, Creutzig U, Kaspers GJ.
Salvage treatment for children with refractory first or second relapse of acute myeloid leukaemia with
gemtuzumab ozogamicin: results of a phase II study. Br J Haematol. 2010;148:768-776.
15. Kellerstrass L, Sander A, Creutzig U, Reinhardt D. Gemtuzumab ozogamicin combined with cytarabine as
salvage therapy in childhood AML. Onkologie. 2008;31.
16. Sievers EL, Larson RA, Stadtmauer EA, Estey E, Lowenberg B, Dombret H, Karanes C, Theobald M, Bennett
JM, Sherman ML, Berger MS, Eten CB, Loken MR, van Dongen JJ, Bernstein ID, Appelbaum FR. Efficacy and
safety of gemtuzumab ozogamicin in patients with CD33-positive acute myeloid leukemia in first relapse. J
Clin Oncol. 2001;19:3244-3254.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 64 of 66
17. Qian Z, Fernald AA, Godley LA, Larson RA, Le Beau MM. Expression profiling of CD34+ hematopoietic stem/
progenitor cells reveals distinct subtypes of therapy-related acute myeloid leukemia. Proc Natl Acad Sci U S
A. 2002;99:14925-14930.
18. Larson RA, Sievers EL, Stadtmauer EA, Lowenberg B, Estey EH, Dombret H, Theobald M, Voliotis D, Bennett
JM, Richie M, Leopold LH, Berger MS, Sherman ML, Loken MR, van Dongen JJ, Bernstein ID, Appelbaum FR.
Final report of the efficacy and safety of gemtuzumab ozogamicin (Mylotarg) in patients with CD33-positive
acute myeloid leukemia in first recurrence. Cancer. 2005;104:1442-1452.
19. Zwaan CM, Reinhardt D, Corbacioglu S, van Wering ER, Bokkerink JP, Tissing WJ, Samuelsson U, Feingold J,
Creutzig U, Kaspers GJ. Gemtuzumab ozogamicin: first clinical experiences in children with
relapsed/refractory acute myeloid leukemia treated on compassionate-use basis. Blood. 2003;101:3868-
3871.
20. Kell J. Treatment of relapsed acute myeloid leukaemia. Rev Recent Clin Trials. 2006;1:103-111.
21. Burnett AK. Antibody targeted chemotherapy in AML-MRC experience. Annals of Hematology. 2008;87:S94.
22. Aplenc R, Alonzo TA, Gerbing RB, Lange BJ, Hurwitz CA, Wells RJ, Bernstein I, Buckley P, Krimmel K, Smith
FO, Sievers EL, Arceci RJ. Safety and efficacy of gemtuzumab ozogamicin in combination with chemotherapy
for pediatric acute myeloid leukemia: a report from the Children's Oncology Group. J Clin Oncol.
2008;26:2390-3295.
23. Brethon B, Auvrignon A, Cayuela JM, Lapillonne H, Leverger G, Baruchel A. Molecular response in two
children with relapsed acute myeloid leukemia treated with a combination of gemtuzumab ozogamicin and
cytarabine. Haematologica. 2006;91:419-421.
24. Brethon B, Auvrignon A, Galambrun C, Yakouben K, Leblanc T, Bertrand Y, Leverger G, Baruchel A. Efficacy
and tolerability of gemtuzumab ozogamicin (anti-CD33 monoclonal antibody, CMA-676, Mylotarg) in
children with relapsed/refractory myeloid leukemia. BMC Cancer. 2006;6:172.
25. Brethon B, Yakouben K, Oudot C, Boutard P, Bruno B, Jerome C, Nelken B, de Lumley L, Bertrand Y, Dalle JH,
Chevret S, Leblanc T, Baruchel A. Efficacy of fractionated gemtuzumab ozogamicin combined with
cytarabine in advanced childhood myeloid leukaemia. Br J Haematol. 2008;143:541-547.
26. Clavio M, Vignolo L, Albarello A, Varaldo R, Pierri I, Catania G, Balocco M, Michelis G, Miglino M, Manna A,
Balleari E, Carella AM, Sessarego M, van Lint MT, Bacigalupo A, Gobbi M. Adding low-dose gemtuzumab
ozogamicin to fludarabine, Ara-C and idarubicin (MY-FLAI) may improve disease-free and overall survival in
elderly patients with non-M3 acute myeloid leukaemia: results of a prospective, pilot, multi-centre trial and
comparison with a historical cohort of patients. Br J Haematol. 2007;138:186-195.
27. Chevallier P, Delaunay J, Turlure P, Pigneux A, Hunault M, Garand R, Guillaume T, Avet-Loiseau H, Dmytruk
N, Girault S, Milpied N, Ifrah N, Mohty M, Harousseau JL. Long-term disease-free survival after gemtuzumab,
intermediate-dose cytarabine, and mitoxantrone in patients with CD33(+) primary resistant or relapsed
acute myeloid leukemia. J Clin Oncol. 2008;26:5192-5197.
28. Chevallier P, Prebet T, Turlure P, Hunault M, Vigouroux S, Harousseau JL, Blaise D, Ifrah N, Milpied N, Mohty
M. Prior treatment with gemtuzumab ozogamicin and the risk of veno-occlusive disease after allogeneic
haematopoietic stem cell transplantation. Bone Marrow Transplant. 2010;45:165-170.
29. Eom KS, Kim HJ, Min WS, Lee S, Min CK, Cho BS, Kim SY, Kim YJ, Lee DG, Choi SM, Cho SG, Kim DW, Lee JW,
Shin WS, Kim CC. Gemtuzumab ozogamicin in combination with attenuated doses of standard induction
chemotherapy can successfully induce complete remission without increasing toxicity in patients with acute
myeloid leukemia aged 55 or older. Eur J Haematol. 2007;79:398-404.
30. Tsimberidou AM, Giles FJ, Estey E, O'Brien S, Keating MJ, Kantarjian HM. The role of gemtuzumab
ozogamicin in acute leukaemia therapy. Br J Haematol. 2006;132:398-409.
31. Reinhardt D, Zwaan CM, Sander A, Neuhoff C, Kaspers GJL, Creutzig U. Gemtuzumab Ozogamicin In
Refractory Childhood Acute Myeloid Leukemia. Blood. 2010;116:1075.
32. Burnett AK, Hills RK, Milligan D, Kjeldsen L, Kell J, Russell NH, Yin JA, Hunter A, Goldstone AH, Wheatley K.
Identification of patients with acute myeloblastic leukemia who benefit from the addition of gemtuzumab
ozogamicin: results of the MRC AML15 trial. J Clin Oncol. 2011;29:369-377.
33. McKoy JM, Angelotta C, Bennett CL, Tallman MS, Wadleigh M, Evens AM, Kuzel TM, Trifilio SM, Raisch DW,
Kell J, DeAngelo DJ, Giles FJ. Gemtuzumab ozogamicin-associated sinusoidal obstructive syndrome (SOS): an
overview from the research on adverse drug events and reports (RADAR) project. Leuk Res. 2007;31:599-
604.
34. Bross PF, Beitz J, Chen G, Chen XH, Duffy E, Kieffer L, Roy S, Sridhara R, Rahman A, Williams G, Pazdur R.
Approval summary: gemtuzumab ozogamicin in relapsed acute myeloid leukemia. Clin Cancer Res.
2001;7:1490-1496.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 65 of 66
35. Arceci RJ, Sande J, Lange B, Shannon K, Franklin J, Hutchinson R, Vik TA, Flowers D, Aplenc R, Berger MS,
Sherman ML, Smith FO, Bernstein I, Sievers EL. Safety and efficacy of gemtuzumab ozogamicin in pediatric
patients with advanced CD33+ acute myeloid leukemia. Blood. 2005;106:1183-1188.
36. Roman E, Simpson J, Ansell P, Kinsey S, Mitchell CD, McKinney PA, Birch JM, Greaves M, Eden T. Childhood
acute lymphoblastic leukemia and infections in the first year of life: a report from the United Kingdom
Childhood Cancer Study. Am J Epidemiol. 2007;165:496-504.
37. Fleischhack G, Hasan C, Graf N, Mann G, Bode U. IDA-FLAG (idarubicin, fludarabine, cytarabine, G-CSF), an
effective remission-induction therapy for poor-prognosis AML of childhood prior to allogeneic or autologous
bone marrow transplantation: experiences of a phase II trial. Br J Haematol. 1998;102:647-655.
38. Reinhardt D, Hempel G, Fleischhack G, Schulz A, Boos J, Creutzig U. Liposomal daunorubicine combined with
cytarabine in the treatment of relapsed/refractory acute myeloid leukemia in children. Klinische Padiatrie.
2002;214:188-194.
39. Kaspers GJL, Zimmermann M, Reinhardt D, Gibson B, Tamminga R, Armendariz H, Dworzak M, Ha S, Hovi L,
Maschan A, Baruchel A, Bertrand Y, Razzouk B, Rizzari C, Smisek P, Smith O, Stark B, Creutzig U. Prognostic
Significance of Time to Relapse in Pediatric AML: Results from the International Randomised Phase III Study
Relapsed AML 2001/01. Blood. 2008;112:1022-1023.
40. Gandhi V, Estey E, Keating MJ, Plunkett W. Fludarabine potentiates metabolism of cytarabine in patients
with acute myelogenous leukemia during therapy. J Clin Oncol. 1993;11:116-124.
41. Hubeek I, Litvinova E, Peters GJ, Broekhuizen R, Haarman EG, Huismans DR, Cloos J, Zwaan CM, Fleischhack
G, Creutzig U, Kaspers GJ. The effect of G-CSF on the in vitro cytotoxicity of cytarabine and fludarabine in the
FLAG combination in pediatric acute myeloid leukemia. Int J Oncol. 2004;25:1823-1829.
42. Fleischhack G, Hasan C, Graf N, Mann G, Bode U. IDA-FLAG (idarubicin, fludarabine, cytarabine, G-CSF), an
effective remission-induction therapy for poor-prognosis AML of childhood prior to allogeneic or autologous
bone marrow transplantation: experiences of a phase II trial. British Journal of Haematology. 1998;102:647-
655.
43. Sung L, Nathan PC, Lange B, Beyene J, Buchanan GR. Prophylactic granulocyte colony-stimulating factor and
granulocyte-macrophage colony-stimulating factor decrease febrile neutropenia after chemotherapy in
children with cancer: a meta-analysis of randomized controlled trials. J Clin Oncol. 2004;22:3350-3356.
44. Ehlers S, Herbst C, Zimmermann M, Scharn N, Germeshausen M, von Neuhoff N, Zwaan CM, Reinhardt K,
Hollink IH, Klusmann JH, Lehrnbecher T, Roettgers S, Stary J, Dworzak M, Welte K, Creutzig U, Reinhardt D.
Granulocyte colony-stimulating factor (G-CSF) treatment of childhood acute myeloid leukemias that
overexpress the differentiation-defective G-CSF receptor isoform IV is associated with a higher incidence of
relapse. J Clin Oncol. 2010;28:2591-2597.
45. Robak T, Wrzesien-Kus A, Lech-Maranda E, Kowal M, Dmoszynska A. Combination regimen of cladribine (2-
chlorodeoxyadenosine), cytarabine and G-CSF (CLAG) as induction therapy for patients with relapsed or
refractory acute myeloid leukemia. Leuk Lymphoma. 2000;39:121-129.
46. Hanel M, Kroger N, Kroschinsky F, Birkmann J, Hanel A, Herbst R, Naumann R, Friedrichsen K, Ehninger G,
Zander AR, Fiedler F. Salvage chemotherapy with mitoxantrone, fludarabine, cytarabine, and cisplatin
(MIFAP) in relapsing and refractory lymphoma. J Cancer Res Clin Oncol. 2001;127:387-395.
47. Pui CH, Thiel E. Central nervous system disease in hematologic malignancies: historical perspective and
practical applications. Semin Oncol. 2009;36:S2-S16.
48. Pui CH. Prophylactic cranial irradiation: going, going, gone. Lancet Oncol. 2009;10:932-933.
49. Locatelli F, Labopin M, Ortega J, Meloni G, Dini G, Messina C, Yaniv I, Fagioli F, Castel V, Shaw PJ, Ferrant A,
Pession A, Socie G, Frassoni F. Factors influencing outcome and incidence of long-term complications in
children who underwent autologous stem cell transplantation for acute myeloid leukemia in first complete
remission. Blood. 2003;101:1611-1619.
50. Strahm B, Nollke P, Zecca M, Korthof ET, Bierings M, Furlan I, Sedlacek P, Chybicka A, Schmugge M, Bordon
V, Peters C, O'Marcaigh A, de Heredia CD, Bergstraesser E, Moerloose BD, Van den Heuvel-Eibrink MM,
Stary J, Trebo M, Wojcik D, Niemeyer CM, Locatelli F. Hematopoietic stem cell transplantation for advanced
myelodysplastic syndrome in children: results of the EWOG-MDS 98 study. Leukemia. 2011;25:455-462.

Clinical Study Protocol Relapsed AML 2010/01 EudraCT-Nr.: 2010-018980-41
Version 6.2.1, dated 20.09.2016
Page 66 of 66
17 Appendix
Karnofsky and Lansky performance status scales
Lansky score: 0-16 years
Fully active 100
Minor restriction in normal physical activity 90
Active, but tires more quickly 80
Both greater restriction and less time spent in active play 70
Minimal active play, busy with quieter activities 60
Gets dressed, but no active play, able to participate in all quiet play
and activities
50
Mostly in bed, participates in quiet activities 40
In bed, needs assistance even for quiet play 30
Often sleeping, play limited to passive activity 20
No play, does not get out of bed 10
Unresponsive 0
Karnofsky score: 16 years and older
Normal, no complaints, no evidence of disease 100
Able to carry on normal activities 90
Normal activity with effort 80
Cares for self, unable to carry on normal activity or to do active
work
70
Requires occasional assistance, is able to care for most of own
needs
60
Requires considerable assistance, frequent medical care 50
Disabled, requires special care/assistance 40
Severely disabled, hospitalization 30
Hospitalization, very sick, active treatment 20
Moribund, fatal processes in progression 10
Dead 0