Embed Size (px)
DESCRIPTION
Relapsed and Refractory Myeloma Case 1. James R. Berenson, MD Medical & Scientific Director Institute for Myeloma & Bone Cancer Research Los Angeles, CA. Disclosures. Speakers’ bureau, research support, and consulting: Amgen, Celgene, Millennium, and Onyx. - PowerPoint PPT Presentation
Citation preview

Relapsed and Refractory Myeloma
Case 1
James R. Berenson, MD
Medical & Scientific DirectorInstitute for Myeloma & Bone Cancer Research
Los Angeles, CA

Disclosures
• Speakers’ bureau, research support, and consulting: Amgen, Celgene, Millennium, and Onyx

Relapsed/Refractory Multiple Myeloma Case 1
• 76 year-old white female presented in Oct ‘11 w/ – Severe mid-back pain– Anemia w/ hemoglobin 10.0– Workup:
• Labs– IgG 3760– M-protein 2.62– 24-hour urine paraprotein 650 mg – B2M 3.7, albumin 3.3 (Stage 2 ISS)– Creatinine 1.5
• Bone marrow 40% plasma cells• Bone survey w/ lytic lesions throughout the axial skeleton and long
bones and T10 VCF • Patient received initial treatment
– Kyphoplasty at T10– Zoledronic acid 4 mg monthly– Cyclophosphamide, bortezomib and dexamethasone

Relapsed/Refractory Multiple Myeloma Case 1 (cont’d)
• Course– Back pain resolved following kyphoplasty– After 4 cycles of initial therapy
• IgG 1170 (from 3760)• M-protein 0.59 (from 2.62)• 24-hour urine M-protein 45 mg (from 650 mg)• Other labs- creatinine 1.0, hemoglobin 11.7
– Patient continued treatment for 3 additional cycles w/ myeloma labs increasing
• IgG 1500• M-protein 0.79• 24 hour urine paraprotein 81 mg• Other labs- creatinine 1.1, hemoglobin 11.5

Relapsed/Refractory Multiple Myeloma: Case 1
At this point, you should1. Start lenalidomide and oral steroids 2. Stop CYBORD3. Repeat labs4. Continue present regimen5. Start another bortezomib-containing
combination

Relapsed/Refractory Multiple Myeloma: Case 1
Labs were repeated 1 month later– IgG now 1800– M-protein 1.01– 24 hour urine M-protein 237 mg– Creatinine 1.5; hemoglobin 10.6
What next?

Individualize Your Choice for the Myeloma Patient Based on:
Co-morbid conditions
DiseaseWork/
Lifestyle
Renal,Bone,Marrow,Subjective,Rate of ProgressionGenetics?
How active is the patient?Mobility?Is potential neuropathy an issue? (e.g.- surgeon, pianist)
Diabetes mellitus (steroids)Cardiac (Doxorubicin, PLD)Neuropathy(Thalidomide)
Prior treatments
Responseand for how long?Side effects and tolerability

Principles of Treating Relapsed/Refractory Multiple Myeloma
• Be sure a patient has really progressed before changing therapy– REPEAT MYELOMA LABS!
• Try to use drugs patient has not seen before• HOWEVER,
– progression on one drug in combination does not mean that drug will not be effective w/ another agent
• e.g., pts progressing from bortezomib w/ melphalan often respond to bortezomib w/ PLD
• Even different drugs in the same class may be active so that– bortezomib+melphalan failures may respond to other alkylating agents-
cyclophosphamide or bendamustine– LEN failures may respond to THAL or POM and vice versa– bortezomib failures respond to carfilzomib
– pts progressing from a drug at one dose may respond to the same drug at a higher dose- e.g., LEN
– the same combination may be effective again if the patient has not seen the combination in a long time

Bortezomib + PLD vs. Bortezomib in Previously Treated MM
1° Endpoint: TTP2° Endpoints: OS*, ORR
BORT 1.3 mg/m2 PLD 30 mg/m2
N=646
RANDOMI ZE
1 4 8 11Days
(n=324)
(n=322)
q 3 weeks up to 8 cycles
q 3 weeks up to 8 cycles
*Not enough events to determine statistical significance in overall survival.ORR=overall response rate; OS=overall survival; TTP=time to progression.
Ddoxorubicin HCl liposome injection Prescribing Information, Distributed by Ortho Biotech Products, L.P., Raritan, NJ. Rev’d May 2007

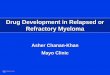
Bortezomib + Pegylated Liposomal Doxorubicin (PLD) + Dexamethasone for
Patients with Previously Untreated Myeloma:A Phase II Trial
Days 1 2 3 4 5 6 7 8 9 10 11 29
Cycle repeatsBortezomib: 1.0 mg/m2 IV
PLD: 5 mg/m2 IV infusion
Dexamethasone 40 mg IV
Berenson et al. Brit J Haematol, 2011
MR: 86% Reduced incidence of PN & PPE

Efficacy and Safety of Bendamustine plus Bortezomib in R/RMM: A Phase 1/2 trial
Patients were assigned to one of 3 cohorts receiving doses of intravenous bendamustine at 50 mg/m2 (cohort 1), 70 mg/m2 (cohort 2), or 90 (cohort 3) mg/m2 in combination with a fixed dose of intravenous bortezomib (1.0 mg/m2) according to the schedule in Figure 1.
Berenson et al. Brit J Haematol 2012

No DLT was observed at any dose level50 mg/m2 (n = 5)70 mg/m2 (n = 4)90 mg/m2 (n = 5)
The maximum dose of bendamustine (90 mg/m2) was well tolerated in combination with bortezomib 1.0 mg/m2 and was designated as the MTD Overall response rate
Overall 48% (1 CR, 2 VGPR, 9 PR, & 7 MR)At MTD (90 mg/m2) 52%Bortezomib-exposed (n=31) 42%Alkylator-exposed (n=28) 46%
Bendamustine & Bortezomib: Results

CR, complete response; nCR, near complete response; Len + Dex,lenalidomide, dexamethasone; PR, partial response; ORR, overall response rate; RRMM, relapsed/refractory multiple myeloma.
Lenalidomide + Dexamethasone in R/R MMLenalidomide + Dexamethasone in R/R MMPhase 3 Trials–ResponsePhase 3 Trials–Response1,21,2
1. Weber DM, et al. N Engl J Med. 2007;357:2133-2142. 2. Dimopoulos M, et al. N Engl J Med. 2007;357:2123-2132.
• CR rates were significantly higher in the Len + Dex arm of each trial compared with Placebo + Dex (P < .001)
• Both OS & TTP superior in Len + Dex arm

Phase II Study of Bortezomib plus Lenalidomide and Dex (VRD) in Rel/Ref MM: Updated Results After >2
Years’ Follow-up1
Richardson PG et al. ASH 2010, abstract #3049
–Endpoints: Primary: PFS; Secondary: ORR (≥MR), DOR, TTP, OS, safety
–Patients: 64 pts with relapsed/refractory MM; median age 65 years (range 32–83); ISS stage I/II/III/unknown (%): 27/25/23/25; median 2 (range 1–3) prior therapies
–Study design: – Anticoagulation with aspirin ± warfarin or LMWH, and antiviral prophylaxis against
herpes zoster were required

Richardson PG et al. ASH 2010, abstract #3049
–Safety: • Median cycles received:
11 (range 1–48)
• Median treatment duration: 7.9 months (range 0.4–36); 66% of pts completed ≥8 cycles with all three drugs
Best response,%
CR/nCR 11/14
PR/VGPR 36/3
ORR (≥MR) 78• Median duration of ≥MR: 8.3 months
• Median duration of ≥PR: 8.4 months
Outcomes
Median, mos
1-yr, %
2-yr, %
TTP 9.5 37 16
PFS 9.5 36 15
OS 26 86 55
• Results: 62 pts evaluable for response
Gr ≥3 AE, % VRD (n=64)
Neutropenia 30
Thrombocytopenia 22
Lymphopenia 11
Leukopenia 9
Hyperglycemia 9
Hyponatremia 8
Hypophosphatemia 8
Fatigue 5
Diarrhea 3
Limb edema 3
Pain in extremity 2
Phase II Study of Bortezomib plus Lenalidomide and Dex (VRD) in Rel/Ref MM: Updated Results After >2 Years’ Follow-up

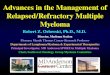
DVD-R (Bortezomib + Pegylated Liposomal Doxorubicin + Dexamethasone + Lenalidomide) for
Patients with R/R MM: A Phase II Trial
Days 1 2 3 4 5 6 7 8 9 10 11 12 13 14 29
Cycle repeatsBortezomib: 1.0 mg/m2 IV
PLD: 4 mg/m2 IV infusion
Dexamethasone 40 mg IV
Berenson et al. Leukemia 2012
Len 10 mg po qd d1-14
MR: 85% No PPE; PN only 25%

Bendamustine (B) w/ Lenalidomide (L) and Dexamethasone (D): Phase 1/2 Trial
• R/R MM patients• N=29• Regimen (28-day cycles)
– B 75-100 mg/m2 d1 & 2– L 5-10 mg qd d1-21– Dex 40 mg PO weekly
• MTD: B 75/ L 10/ D 40• Results (only 25 considered evaluable for response)
– ORR (> PR): 52% w/ 24% VGPR– MR 24%– PFS: 6.1 mo
Lentzsch et al. Blood 2012

Retreatment w/ IMiD compounds for MM Patients
• Retrospective study in 140 pts treated firstline w/– THAL/DEX- 58%– LEN/DEX- 42%
• Retreatment w/ a regimen containing– THAL- 24%– LEN- 76%
• # of treatments before retreatment - median of 2 (range 1-6)
• 89% received IMiD compound w/ DEX
• 113 considered evaluable for response– 44% > PR– MR not reported
Madan et al. Blood 2011
LEN
LEN
(n=48)
LEN
THAL
(n=11)
THAL
LEN
(n=58)
THAL
THAL (n=23)
> PR 54% 20% 48% 30%

Relapsed/Refractory Multiple Myeloma
For patients failing CYBORD regimens upfront, treatment options include all of the following except
1. PLD w/ BOR +/- steroids2. Bendamustine w/ BOR3. Len w/ steroids4. Len w/ steroids + BOR5. Len w/ oral melphalan