Embed Size (px)
Citation preview

Copyright © 2014 AAPC
Reimbursement Through CDI Presented by: Robert S. Gold, MD
Co-founder DCBA
Rae Jimenez, CPC, CPB, CPMA, CPPM, CPC-I, CCS
AAPC-VP, Member and Certification Solutions

Objectives
• Discuss the real purpose of good documentation of diagnostic
information
• Discuss how diagnosis coding and your professional billing
codes are influenced by your documentation
• Review current initiatives in the healthcare field and how good
documentation will have pervasive effects
• Identify how your practice can work into this future

Benefits of Proper Documentation
• Improves compliance
• Improves patient care
• Improves clinical data for research and education
• Protects the legal interest of the patient, facility and physician
• Enables proper reimbursement for services performed
• Achieves accurate information for the severity of conditions
treated and resource utilization

Medicine Under the Microscope
• Morbidity
• Mortality
• Cost per patient
• Resource utilization
• Length of stay
• Complications
• Outcomes
• IS IT SAFE – avoiding harm, avoidable readmissions?

Where Does This Data Come From?
• Documentation leads to identification of diagnoses and
procedures
• Recognition of diagnoses and procedures lead to ICD codes –
THE TRUE KEY
• ICD codes lead to APR-DRG “Severity” in facility
• Risk Adjustments as well as HCC category
• Severity adjusted data leads to morbidity and mortality rates
• Documentation must support services performed.

Basically what we are saying is… Just tell us….

E/M code determined by …
Where service was performed• Office/Outpatient
• New patient*
• Established patient*
• Inpatient
• Initial visit*
• Subsequent visit
• Nursing Facility
• Initial visit*
• Subsequent visit* Increased work RVUs remain “budget neutral”

E/M code determined by …
Complexity of service provided (and documented)
• History
• Chief Complaint/HPI
• ROS
• Past, Family, Social Hx
• Physical Exam
• Medical Decision-Making
• Number of problems
• Complexity/type of data
• Risk to the patient

What Does CPT Say?Per CPT:
“The extent of history is dependent upon clinical judgment
and on the nature of the presenting problem(s)”
“The extent of the examination performed is dependent on
clinical judgment and on the nature of the presenting
problem(s)”
So, “clinical judgment” and “nature of the presenting problem”
(medical decision-making) drive E/M level?

What is Medical Decision Making?
Per CPT
“Medical decision making refers to the complexity
of establishing a diagnosis and/or selecting a
management option”
Physician’s thought process

Complexity of Medical Decision Making
• Number of Diagnoses and/or Management options
• Complexity of data
• Risk of significant complications, morbidity, mortality
Based on PRESENTING PROBLEM
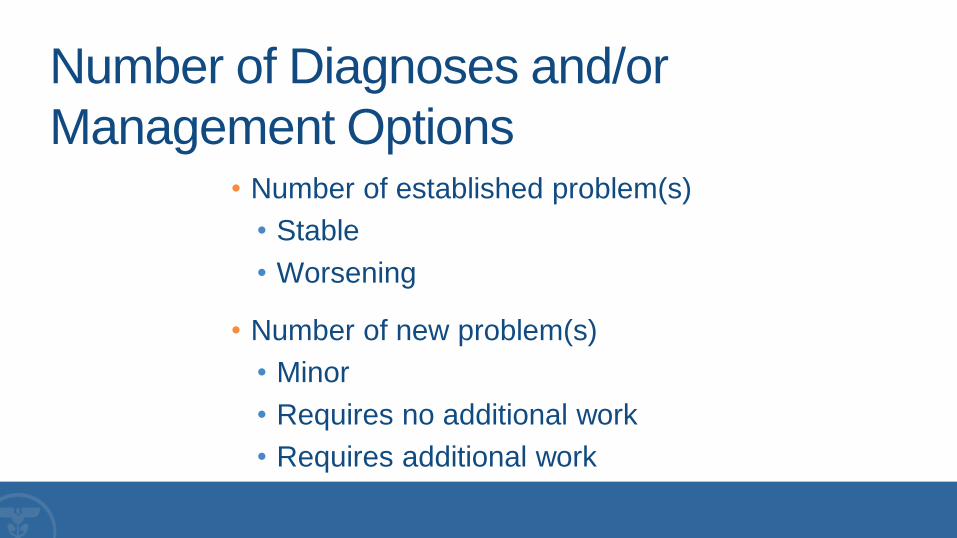
Number of Diagnoses and/or
Management Options• Number of established problem(s)
• Stable
• Worsening
• Number of new problem(s)
• Minor
• Requires no additional work
• Requires additional work

Complexity of Data
• Clinical data
• X-ray data
• Non-invasive data
• Discussion with interpreting physician
• Independent review
• Decision for patient’s previous records
• Summation of patient’s previous records

Risk to the Patient
• Presenting problem(s)
• Diagnostic procedures ordered
• Management options selected

Inpatient Consultation
76 yo patient admitted w/chest pain, now with hypoxia. Pt presented w/burning substernal
CP and dyspnea for 3 hrs PTA. Sa02 in ED = 83 - 89 on 4 L. Pt with hx of COPD, on
glucophage and lisinopril. ABGs: pH 7.30, CO2 62, O2 45; HbA1C 8.5, bicarb 35.
SH: Smoker FH: Father died of complications of DM
ROS: Some urinary incontinence, otherwise remainder of systems negative except as
noted in HPI.
PE: T-99.3, BP 135/62, P-122, R-30. WDWN male in moderate distress. Eyes:
PERRLA. ENT: No thyromegaly Chest: Retractions and accessory muscle use noted
Heart: RRR w/o murmurs, rubs or gallops. Lungs: CTA. Abd: Soft, nontender, bowel
sounds normal, no organomegaly. NEURO: Cranial nerves II-XII intact.
IMP: COPD
PLAN: BIPAP , SS insulin

What is the Level of E/M?
• History Comprehensive
• Examination Comprehensive
• Risk Straightforward
E/M Supported: 99221
ICD-9-CM Code 496 COPD unspecified

Inpatient Consultation76 yo patient admitted w/chest pain, now with hypoxia. Pt presented w/burning substernal
CP and dyspnea for 3 hrs PTA. Sa02 in ED = 83 - 89 on 4 L. Pt with hx of COPD, on
glucophage and lisinopril. ABGs: pH 7.30, CO2 62, O2 45; HbA1C 8.5, bicarb 35.
SH: Smoker FH: Father died of complications of DM
ROS: Some urinary incontinence, otherwise remainder of systems negative except as
noted in HPI.
PE: T-99.3, BP 135/62, P-122, R-30. WDWN male in moderate distress. Eyes:
PERRLA. ENT: No thyromegaly Chest: Retractions and accessory muscle use noted
Heart: RRR w/o murmurs, rubs or gallops. Lungs: CTA. Abd: Soft, nontender, bowel
sounds normal, no organomegaly. NEURO: Cranial nerves II-XII intact.
IMP: Acute exacerbation of COPD
PLAN: BIPAP , SS insulin

What is the Level of E/M?
• History Comprehensive
• Examination Comprehensive
• Risk Moderate
E/M Supported: 99222
ICD-9-CM Code 491.21 Acute Exacerbation of
COPD

Inpatient Consultation76 yo patient admitted w/chest pain, now with hypoxia. Pt presented w/burning substernal
CP and dyspnea for 3 hrs PTA. Sa02 in ED = 83 - 89 on 4 L. Pt with hx of COPD, on
glucophage and lisinopril. ABGs: pH 7.30, CO2 62, O2 45; HbA1C 8.5, bicarb 35.
SH: Smoker FH: Father died of complications of DM
ROS: Some urinary incontinence, otherwise remainder of systems negative except as
noted in HPI.
PE: T-99.3, BP 135/62, P-122, R-30. WDWN male in moderate distress. Eyes:
PERRLA. ENT: No thyromegaly Chest: Retractions and accessory muscle use noted
Heart: RRR w/o murmurs, rubs or gallops. Lungs: CTA. Abd: Soft, nontender, bowel
sounds normal, no organomegaly. NEURO: Cranial nerves II-XII intact.
IMP: Acute on chronic hypercapnic respiratory failure, uncontrolled DM2, HTN,
acute exacerbation of COPD
PLAN: BIPAP , SS insulin
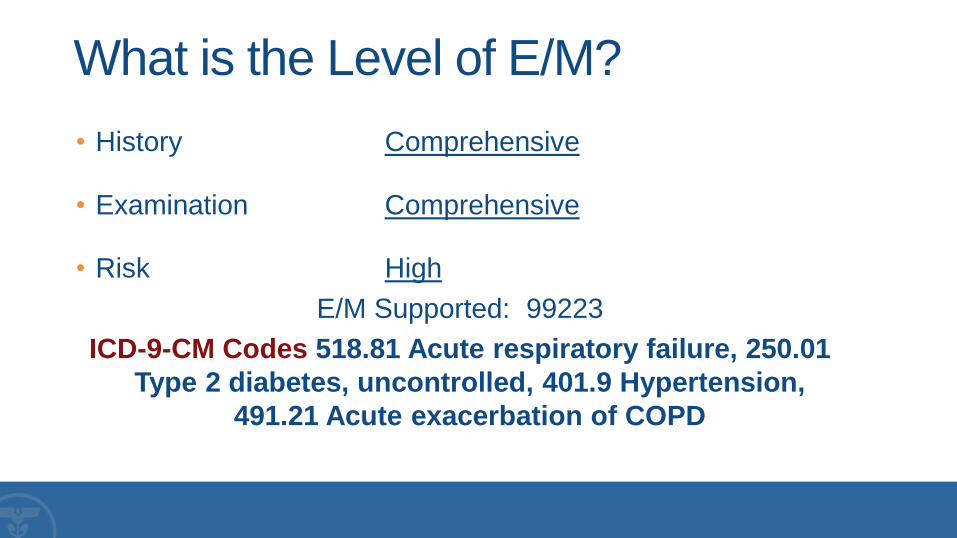
What is the Level of E/M?
• History Comprehensive
• Examination Comprehensive
• Risk High
E/M Supported: 99223
ICD-9-CM Codes 518.81 Acute respiratory failure, 250.01
Type 2 diabetes, uncontrolled, 401.9 Hypertension,
491.21 Acute exacerbation of COPD

E/M PaymentCode Work RVU National CMS Payment
99221 1.92 $102.62
99222 2.61 $138.37
99223 3.86 $204.87

Specificity is NOT Always Possible
Sign/Symptom/Unspecified Codes
In both ICD-9-CM and ICD-10-CM, sign/symptom and “unspecified” codes have acceptable, even necessary, uses. While specific diagnosis codes should be reported when they are supported by the available medical record documentation and clinical knowledge of the patient’s health condition, there are instances when signs/symptoms or unspecified codes are the best choices for accurately reflecting the healthcare encounter.
Each healthcare encounter should be coded to the level of certainty known for that encounter.
If a definitive diagnosis has not been established by the end of the encounter, it is appropriate to report codes for sign(s) and/or symptom(s) in lieu of a definitive diagnosis.
When sufficient clinical information isn’t known or available about a particular health condition to assign a more specific code, it is acceptable to report the appropriate “unspecified” code.
In fact, unspecified codes should be reported when they are the codes that most accurately reflects what is known about the patient’s condition at the time of that particular encounter.

• Semantics
• Coding guidelines and conventions
• Use of signs, symbols, arrows
• Accuracy and specificity
• Relationship between accuracy and specificity of code
assignment and Complexity of Medical Decision Making
World Health Organization and ICD Codes

Yes, yes. I can see
he’s off his rocker.
But, for billing
purposes, we have to
come up with
something that sounds
a little more clinical.

Is There a Diagnosis?
82 yo WF altered mental status, shaking chills, fevers,
decr UO, T = 103, P = 124, R = 34, BP = 70/40
persistent despite 1 L NS, on Dopamine, pO2 = 78 on
non-rebreather, pH = 7.18, pCO2 = 105, WBC =
17,500, left shift, BUN = 78, Cr = 5.4, CXR – Right UL
infiltrates, start Cefipime, Clinda, Tx to ICU. May have
to intubate – full resusc.

Is There a Diagnosis?Assessment/Plan
82 YO F patient presented to ER with:
1. Sepsis,
2. Septic Shock,
3. Acute Hypercapnic Respiratory Failure,
4. Acute Renal Failure due to #2, (don’t forget CKD and stage, if present)
5. Aspiration Pneumonia,
6. Metabolic Encephalopathy
Will transfer to ICU, continue Dopamine and monitor respiratory status for possible ARDS, renal status with hydration and initiate Cefapime/clindamycin for possible aspiration pneumonia
CC time 1hr 45 minutes
John Smith MD

So What’s the Difference?Principal Diagnosis Chills and Fever Sepsis
Secondary Diagnoses Altered Mental Status Septic Shock
Acute Respiratory Failure
Aspiration Pneumonia
Acute Renal Failure (or AKI)
Respiratory Acidosis
Metabolic Encephalopathy
Medicare MS-DRG 864 Fever w/o CC/MCC 871 Septicemia or severe
Sepsis w/o MV 96+ hrs
w/ MCC
APR-DRG 722 Fever 720 Septicemia &
Disseminated infection
APR-DRG Severity Illness 1 – Minor 4 – Extreme
APR-DRG Risk of
Mortality
1 – Minor 4 - Extreme
Medicare MS-DRG Rel Wt 0.8153 1.8437
APR DRG Relative Weight 0.3556 2.9772
National Mortality Rate
(APR Adjusted)
0.04% 62.02%

Old 1500 Form
Limited to
4 Diagnoses –
BUT
You Can Always
Turn In TWO
FORMS

New 1500 Form – Added
Eight More Dxs

HCC RAs - Here Since 2004• Hierarchical condition category risk adjustment – the
more complex the disease, the higher the risk, the higher your reimbursement
• Billing only vanilla codes reaps least rewards
• 250.00 is diabetes type 2, not stated as uncontrolled – is this ALL of your patients?
• 428.0 is CHF with no additional risk – is this ALL of your patients?
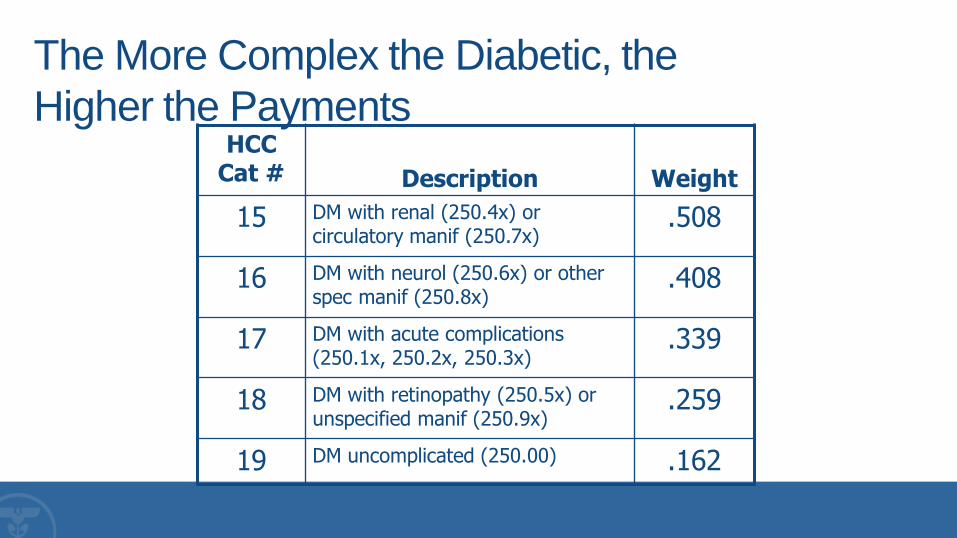
The More Complex the Diabetic, the
Higher the PaymentsHCC
Cat # Description Weight
15 DM with renal (250.4x) or circulatory manif (250.7x)
.508
16 DM with neurol (250.6x) or other spec manif (250.8x)
.408
17 DM with acute complications (250.1x, 250.2x, 250.3x)
.339
18 DM with retinopathy (250.5x) or unspecified manif (250.9x)
.259
19 DM uncomplicated (250.00) .162

Risk Adjusted HMO PaymentsProvider Members Risk Score PMPM
Cook County Average
5,011 0.963 $688.22
Providers
A 14 0.650 $508.77
B 11 0.820 $594.48
C 9 1.080 $760.94
D 14 1.220 $803.54
E 14 1.380 $866.56
F 12 1.750 $1,127.34
IDEAL 1.08-1.10

Payment Reform
• Shift from fee-for-service to quality care, improved outcomes,
and cost control
• Physician Quality Reporting System (PQRS)
• Value-Based Payment Modifier
• Accountable Care Organization (ACO)
• Bundled payments
• Patient centered medical homes

PQRS
• Selecting measures
• Clinical conditions usually treated
• Types of care typically provided – e.g., preventive, chronic,
acute
• Settings where care is usually delivered – e.g., office,
emergency department (ED), surgical suite
• Quality improvement goals for 2015
• Other quality reporting programs in use or being considered


Measure Title Measure Description
Chronic Obstructive
Pulmonary Disease (COPD):
Spirometry Evaluation
Percentage of patients aged 18 years and older with a
diagnosis of COPD who had spirometry results
documented
Chronic Obstructive
Pulmonary Disease (COPD):
Inhaled Bronchodilator
Therapy
Percentage of patients aged 18 years and older with a
diagnosis of COPD and who have an FEV1/FVC less than
60% and have symptoms who were prescribed an inhaled
bronchodilator
PQRS Example
PQRS Example
• COPD 496
• 3023F Spirometry results documented and reviewed (COPD)
• 4025F Inhaled bronchodilator prescribed (COPD)
• G8924 Spirometry test results demonstrate fev1/fvc < 60% and patient has
COPD symptoms (e.g., dyspnea, cough/sputum, wheezing)
• G8925 Spirometry test results demonstrate fev1/fvc >=60% or patient does
not have COPD symptoms
• G8926 Spirometry test not performed or documented, reason not given

Value-Based Payment Modifier
• Physician group practices of 100 or more EPs subject to VM in 2015
based on 2013 calendar year performance
• Physician group practices of 10 or more EPs subject to VM in 2016
based on 2014 calendar year performance
• For 2015 and 2016, the Value Modifier does not apply to groups of physicians
in which any of the group practice’s physicians participate in the Medicare
Shared Savings Program, Pioneer ACOs, or the Comprehensive Primary
Care Initiative.
• All physicians who participate in Fee-For-Service affected in 2017

Value-Based Purchasing Program
Beginning in FY 2013 and continuing annually, CMS will
adjust hospital payments under the VBP program based
on how well hospitals perform or improve their
performance on a set of quality measures. The initial set
of 13 measures includes three mortality measures, two
AHRQ composite measures, and eight hospital-acquired
condition (HAC) measures. The FY 2012 IPPS final rule
(available at http://tinyurl.com/6nccdoc) includes a
complete list of the 13 measures.

Goals of Implementation –
Prove You Are Value Based
• Excellence in severity adjusted data
• Reasonable occurrence of PSIs
• Lower than average Readmissions for Pneumonia,
Heart Failure, AMI
• Cooperation with quality initiatives
• Patient satisfaction

Goals of Implementation –
Prove You Are Value Based
• Excellence in severity adjusted data
• Reasonable occurrence of PSIs
• Lower than average Readmissions for Pneumonia,
Heart Failure, AMI
• Cooperation with quality initiatives
• Patient satisfaction

Worse
than
Better
than
Average Average
Death in procedures where mortality is usually very low ●
Pressure sores or bed sores acquired in the hospital ●
Death following a serious complication after surgery ●
Collapsed lung due to a procedure or surgery in or
around the chest ●
Catheter-related bloodstream infections acquired at the
hospital ●
Hip fracture following surgery ●
Excessive bruising or bleeding as a consequence of a
procedure or surgery ●
Electrolyte and fluid imbalance following surgery ●
Respiratory failure following surgery ●
Deep blood clots in the lungs or legs following surgery ●
Bloodstream infection following surgery ●
Breakdown of abdominal incision site ●
Accidental cut, puncture, perforation or hemorrhage
during medical care ●
Foreign objects left in body during a surgery or procedure
Average
0 Events

What Does This Mean?
• Properly assign complication codes when complications
• Do not assign complication codes when not complication
• If event due to disease, not a complication
• If even doesn’t exist, not a complication
• Communication with CDI and Medical Staff to validate perceived
complications of care
• Hospitals began overreporting complications of care because
they are CCs, MCCs

Goals of Implementation –
Prove You Are Value Based• Excellence in severity adjusted data
• Reasonable occurrence of PSIs
• Lower than average Readmissions for Pneumonia, Heart
Failure, AMI
• Cooperation with quality initiatives
• Patient satisfaction

Readmissions Initiative
• Identify hospitals with excess readmissions for certain selected conditions beginning in FY 2013 for discharges on or after October 1, 2012.
• Acute myocardial infarction (i.e., heart attack)
• Heart failure
• Pneumonia
• Definition of readmission: “occurring when a patient is discharged from the applicable hospital and then is admitted to the same or another acute care hospital within a specified time period from the time of discharge from the index hospitalization.” The specified time period would be 30 days.
45

What Does This Mean?
• Started with AMI, Heart Failure, Pneumonia but expanding to
all discharges
• Ensure that entire picture of all patients known for proper care
integration of services – outpatient care and inpatient care as
a continuum, addressing ALL patient problems, not just PDx
Following Heart Failure Patients After
Discharge Avoids ReadmissionsSt. John’s Regional Health Center has very low readmission rates for heart attack, heart
failure, and pneumonia—the three conditions for which hospitals report readmission rates
to the Centers for Medicare and Medicaid Services. Its rates are better than the top 10
percent of hospitals reporting.
Performance Improvement Strategies
• telephone calls to all heart failure patients to answer questions and remind them about
the importance of having a follow-up visit with their personal physician
• use of an interactive voice response telemonitoring program for heart failure patients
• telephone and electronic notification to patients’ personal physicians about patients'
hospitalization and need for follow-up visits within one week

Goals of Implementation –
Prove You Are Value Based
• Excellence in severity adjusted data
• Reasonable occurrence of PSIs
• Lower than average Readmissions for Pneumonia,
Heart Failure, AMI
• Cooperation with quality initiatives
• Patient satisfaction

Participation and Success in Reporting
of Core Measures
• Acute MI
• Heart failure
• Pneumonia
• Postoperative wound infections
• Venous thromboembolism
• Stroke
• Asthma in children’s hospitals

Value Basis Calculation
Outcome
Cost
Value=

Goals of Implementation –
Prove You Are Value Based• Excellence in severity adjusted data
• Reasonable occurrence of PSIs
• Lower than average Readmissions for Pneumonia,
Heart Failure, AMI
• Cooperation with quality initiatives
• Patient satisfaction

Patient in Proper EnvironmentOutpatient, OBS, Impatient Care
• Extended postop management in same day surgery
cases
• Inappropriate admissions for workup of symptoms in
stable patient
• Inappropriate admissions for treatment of diseases
expected to resolve in hours
• Closed system, protocol driven OBS unit efficient and
cost effective

Surgery Bundling Test Model• Disclosed May 16, 2008
• ACE (Acute Care Episode) project
• Combine Part B payments with Part A
• “Value Based Centers” started with Texas, Oklahoma, New
Mexico and Colorado
• Value based purchasing
• 28 cardiac and 9 orthopedic inpatient surgical services
• Gainsharing also permitted here
• Based on severity adjusted financial outcomes

Florida Blue and Mayo Clinic Introduce
Knee Replacement Bundled ProgramFriday, December 14, 2012
JACKSONVILLE, Fla. — Florida Blue and Mayo Clinic jointly announce a new collaboration aimed at providing the utmost in quality care for knee replacement patients in Florida. The two Florida health care leaders are teaming up to create a bundled payment agreement specific to the treatment of knee replacement surgery.
Knee replacement surgery is the most common joint replacement procedure. According to the Agency for Healthcare Research and Quality, health care professionals perform more than 600,000 knee replacements annually in the United States.

CMS Bundled Payment PlansSeptember 2, 2011
• Bundles physician and hospital payment into one lump sum could represent a long-term, revolutionary solution to that age-old question.
• Testing four new bundled payment plans, according to a Fact Sheet released August 23
• Three models involve retrospective payment, one a prospective payment determined by MS-DRG
• Aggregate Medicare payment for the episode will be reconciled against the target price. Savings beyond the discount reflected in the target price will be paid to the participants to share among the participating providers.

Bundled Payments for Care
Improvement (BPCI) Initiative
On January 31, 2013, the Centers for Medicare & Medicaid Services (CMS) announced the health care organizations selected to participate in the Bundled Payments for Care Improvement initiative, an innovative new payment model. Under the Bundled Payments for Care Improvement initiative, organizations will enter into payment arrangements that include financial and performance accountability for episodes of care.
Research has shown that bundled payments can align incentives for providers – hospitals, post-acute care providers, physicians, and other practitioners– allowing them to work closely together across all specialties and settings.
http://innovation.cms.gov/initiatives/bundled-payments/index.html

Florida Blue and Holy Cross Create
Accountable Care Arrangement
Jacksonville and Fort Lauderdale, Fla. – Florida Blue, Florida’s Blue Cross and Blue Shield Company, and Holy Cross Physician Partners are pleased to announce that effective January 1, 2013, Holy Cross Physician Partners will participate in the Florida Blue Accountable Care Program.
“Florida Blue is excited to expand our relationship with Holy Cross surrounding this exciting new partnership,” said Dr. Jonathan Gavras, chief medical officer and senior vice president for Florida Blue. “In the age of reform, both organizations realize the importance of moving away from the fee-for-service model to one that focuses on quality outcomes that will benefit our members in South Florida.”

Banner Announces Joint Venture with Blue
Cross Blue Shield of Arizona
Banner Health and Blue Cross Blue Shield of Arizona have entered into a new joint venture, Blue Cross Blue Shield of Arizona Advantage, which will bring enhanced Medicare services to Arizonans. This collaboration brings together two premier organizations with the common goal of improving the quality of patient care, enhancing wellness and assuring affordability.
"This and our other partnerships with Aetna, HealthNet and United Healthcare in Arizona and Kaiser Permanente in Colorado, as well as our selection as a Medicare Pioneer ACO organization, are helping to position Banner for continued success in a challenging and transformational health care environment."

Paint the picture of the patient properly with WORDS
So the coder can paint the same picture with codes.
What you want…
what you might get.
may notbe…

Questions?

CPT® Disclaimer
CPT copyright 2014 American Medical Association. All rights reserved.
Fee schedules, relative value units, conversion factors and/or related components are not
assigned by the AMA, are not part of CPT, and the AMA is not recommending their use. The
AMA does not directly or indirectly practice medicine or dispense medical services. The AMA
assumes no liability for data contained or not contained herein.
CPT is a registered trademark of the American Medical Association.