CHAPTER I
INTRODUCTION
Femoral fracture is the most common orthopedic injuries of
children and required hospitalization. Epidemiological studies from
Indiana in 2006 mentioned from almost 10.000 femoral fracture, 1076
(11%) occurred in children aged less than 2 years, 2119 (21%) in
children aged 2 to 5 years, 3237 (33%) in children aged 6 up to 12
years, and 3528 (35%) in adolescents aged 13 to 18 years. 71% of
incident femoral fracture occurred in males with two-thirds cause
of the motorcycle accident. Incidence of fall drive greater
occurred in young people and incidence of collision was more common
in adults. 15% of femoral fractures occurred in children less than
2 years due to child abuse.1
Pediatric femoral fracture is one of the most prevalent kinds of
fractures with an incident rate of 1.6% and about 4% of them are
open fractures and most of these fractures (90%) are resulted from
high energy trauma. Studies also show that these fractures are
associated with more complications. Therefore, it is important to
do special treatment as well as improved safety for children
considering the complications due to a femoral fracture seriously
can cause shock, a fat embolism and disruptions of growth if there
is epiphysis plate injury. The following will discuss about the
treatment of femoral fracture on children.1-2CHAPTER II
REVIEW OF LITERATUREA. FEMUR ANATOMY
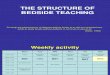
Thefemur, the longest and strongest bone in the skeleton, is
almost perfectly cylindrical in the greater part of its extent. In
the erect posture it is not vertical, being separated above from
its fellow by a considerable interval, which corresponds to the
breadth of the pelvis, but inclining gradually downward and
medialward, so as to approach its fellow toward its lower part, for
the purpose of bringing the knee-joint near the line of gravity of
the body. The degree of this inclination varies in different
persons, and is greater in the female than in the male,on account
of the greater breadth of the pelvis. The femur, like other long
bones, is divisible into a bodyandtwo extremities.3
Picture 1. Right femur. Anterior surface.
The upper extremity presents for examination
ahead,aneck,agreaterand alesser trochanter.
The Head (caput femoris).The head which is globular and forms
rather more than a hemisphere, is directed upward, medialward, and
a little forward, the greater part of its convexity being above and
in front. Its surface is smooth, coated with cartilage in the fresh
state, except over an ovoid depression, thefovea capitis
femoris,which is situated a little below and behind the center of
the head, and gives attachment to the ligamentum teres.4
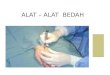
Picture 2 . Upper extremity of right femur viewed from behind
and above.
The Neck (collum femoris).The neck is a flattened pyramidal
process of bone, connecting the head with the body, and forming
with the latter a wide angle opening medialward. The angle is
widest in infancy, and becomes lessened during growth, so that at
puberty it forms a gentle curve from the axis of the body of the
bone. In the adult, the neck forms an angle of about 125 with the
body, but this varies in inverse proportion to the development of
the pelvis and the stature. In the female, in consequence of the
increased width of the pelvis, the neck of the femur forms more
nearly a right angle with the body than it does in the male. The
angle decreases during the period of growth, but after full growth
has been attained it does not usually undergo any change, even in
old age; it varies considerably in different persons of the same
age. It is smaller in short than in long bones, and when the pelvis
is wide. In addition to projecting upward and medialward from the
body of the femur, the neck also projects somewhat forward; the
amount of this forward projection is extremely variable, but on an
average is from 12 to 14.3-4The Trochanters.The trochanters are
prominent processes which afford leverage to the muscles that
rotate the thigh on its axis. They are two in number, the greater
and the lesser.
TheGreater Trochanter(trochanter major; great trochanter) is a
large, irregular, quadrilateral eminence, situated at the junction
of the neck with the upper part of the body. It is directed a
little lateralward and backward, and, in the adult, is about 1 cm.
lower than the head. It has two surfaces and four borders.
Thelateral surface,quadrilateral in form, is broad, rough, convex,
and marked by a diagonal impression, which extends from the
postero-superior to the antero-inferior angle, and serves for the
insertion of the tendon of the Glutus medius. Above the impression
is a triangular surface, sometimes rough for part of the tendon of
the same muscle, sometimes smooth for the interposition of a bursa
between the tendon and the bone. Below and behind the diagonal
impression is a smooth, triangular surface, over which the tendon
of the Glutus maximus plays, a bursa being interposed. Themedial
surface,of much less extent than the lateral, presents at its base
a deep depression, thetrochanteric fossa(digital fossa), for the
insertion of the tendon of the Obturator externus, and above and in
front of this an impression for the insertion of the
Obsturatorinternus and Gemelli. Thesuperior borderis free; it is
thick and irregular, and marked near the center by an impression
for the insertion of the Piriformis. Theinferior bordercorresponds
to the line of junction of the base of the trochanter with the
lateral surface of the body; it is marked by a rough, prominent,
slightly curved ridge, which gives origin to the upper part of the
Vastus lateralis. Theanterior borderis prominent and somewhat
irregular; it affords insertion at its lateral part to the Glutus
minimus. Theposterior borderis very prominent and appears as a
free, rounded edge, which bounds the back part of the trochanteric
fossa.TheLesser Trochanter(trochanter minor; small trochanter) is a
conical eminence, which varies in size in different subjects; it
projects from the lower and back part of the base of the neck. From
its apex three well-marked borders extend; two of these are
aboveamedial continuous with the lower border of the neck,
alateralwith the intertrochanteric crest; the inferior borderis
continuous with the middle division of the linea aspera.
Thesummitof the trochanter is rough, and gives insertion to the
tendon of the Psoas major.The Body or Shaft (corpus femoris).The
body, almost cylindrical in form, is a little broader above than in
the center, broadest and somewhat flattened from before backward
below. It is slightly arched, so as to be convex in front, and
concave behind, where it is strengthened by a prominent
longitudinal ridge, thelinea aspera.It presents for examination
three borders, separating three surfaces. Of the borders, one, the
linea aspera, is posterior, one is medial, and the other,
lateral.Thelinea asperais a prominent longitudinal ridge or crest,
on the middle third of the bone, presenting a medial and a lateral
lip, and a narrow rough, intermediate line. Above, the linea aspera
is prolonged by three ridges. The lateral ridge is very rough, and
runs almost vertically upward to the base of the greater
trochanter. It is termed thegluteal tuberosity,and gives attachment
to part of the Glutus maximus: its upper part is often elongated
into a roughened crest, on which a more or less well-marked,
rounded tubercle, thethird trochanter,is occasionally developed.
The intermediate ridge orpectineal lineis continued to the base of
the lesser trochanter and gives attachment to the Pectineus; the
medial ridge is lost in the intertrochanteric line; between these
two a portion of the Iliacus is inserted. Below, the linea aspera
is prolonged into two ridges, enclosing between them a triangular
area, thepopliteal surface,upon which the popliteal artery rests.
Of these two ridges, the lateral is the more prominent, and
descends to the summit of the lateral condyle. The medial is less
marked, especially at its upper part, where it is crossed by the
femoral artery. It ends below at the summit of the medial condyle,
in a small tubercle, theadductor tubercle,which affords insertion
to the tendon of the Adductor magnus.Theanterior surfaceincludes
that portion of the shaft which is situated between the lateral and
medial borders. It is smooth, convex, broader above and below than
in the center. From the upper three-fourths of this surface the
Vastus intermedius arises; the lower fourth is separated from the
muscle by the interventionof the synovial membrane of the
knee-joint and a bursa; from the upper part of it the Articularis
genu takes origin. Thelateral surfaceincludes the portion between
the lateral border and the linea aspera; it is continuous above
with the corresponding surface of the greater trochanter, below
with that of the lateral condyle: from its upper three-fourths the
Vastus intermedius takes origin. Themedial surfaceincludes the
portion between the medial border and the linea aspera; it is
continuous above with the lower border of the neck, below with the
medial side of the medial condyle: it is covered by the Vastus
medialis.The Lower Extremity (distal extremity)
The lower extremity, larger than the upper, is somewhat cuboid
in form, but its transverse diameter is greater than its
antero-posterior; it consists of two oblong eminences known as
thecondyles.In front, the condyles are but slightly prominent, and
are separated from one another by a smooth shallow articular
depression called thepatellar surface;behind, they project
considerably, and the interval between them forms a deep notch,
theintercondyloid fossa.Thelateral condyleis the more prominent and
is the broader both in its antero-posterior and transverse
diameters, themedial condyleis the longer and, when the femur is
held with its body perpendicular, projects to a lower level. When,
however, the femur is in its natural oblique position the lower
surfaces of the two condyles lie practically in the same horizontal
plane. The condyles are not quite parallel with one another; the
long axis of the lateral is almost directly antero-posterior, but
that of the medial runs backward and medialward. Their opposed
surfaces are small, rough, and concave, and form the walls of the
intercondyloid fossa. This fossa is limited above by a ridge,
theintercondyloid line,and below by the central part of the
posterior margin of the patellar surface. The posterior cruciate
ligament of the knee-joint is attached to the lower and front part
of the medial wall of the fossa and the anterior cruciate ligament
to an impression on the upper and back part of its lateral wall.
Each condyle is surmounted by an elevation, the epicondyle.
Themedial epicondyleis a large convex eminence to which the tibial
collateral ligament of the knee-joint is attached. At its upper
part is the adductor tubercle, already referred to, and behind it
is a rough impression which gives origin to the medial head of the
Gastrocnemius. Thelateral epicondyle,smaller and less prominent
than the medial, gives attachment to the fibular collateral
ligament of the knee-joint. Directly below it is a small depression
from which a smooth well-marked groove curves obliquely upward and
backward to the posterior extremity of the condyle. This groove is
separated from the articular surface of the condyle by a prominent
lip across which a second, shallower groove runs vertically
downward from the depression. In the fresh state these grooves are
covered with cartilage. The Popliteus arises from the depression;
its tendon lies in the oblique groove when the knee is flexed and
in the verticalgroove when the knee is extended. Above and behind
the lateral epicondyle is an area for the origin of the lateral
head of the Gastrocnemius, above and to the medial side of which
the Plantaris arises.
Picture 2a. Lower extremity of right femur viewed from
below.
B. DEFINITION OF FRACTUREFracture is the breaking continuity of
the bones tissues determined according to the type and extent
usually caused by the forced movement or external pressure which
comes greater than what is acceptable by bone.1,3,5To find out why
and how the bone fractures occur, physical condition of bone and
traumatic circumstances that can lead to bone fractures must be
known in advance. Cortical bone has a structure that can withstand
the compression and the pressure of shearing.
Most of fracture occurs due to failure of the bone hold the
bending, twisting, and pulling of trauma that is directly or
indirectly. Immediate trauma causing pressure directly on bone and
fracture occurs in the area of pressure. A fracture that occurs
usually tends to be comunitive and soft tissue are also damaged
while the indirect trauma occurs when the trauma delivered to areas
further away from the fractures, for example fell by hand
extensions can cause fracture of clavicle. In these circumstances
typically soft tissue remains intact.Pressure on the bones can be
in form of : (1) rotating pressure that can causes oblique or
spiral fracture, (2) bending pressure causing transversal fracture,
(3) the pressure along the length of the bone that can lead to
impaction fracture or dislocation, (4) vertical compression
fracture can cause comunitive or split fracture, for example on the
vertebrae, (5) direct trauma accompanied with resistance at a
certain distance will cause an oblique fracture or Z fracture, (6)
trauma due to the pull of the ligaments or tendons will draw some
bones.6C. CLSSIFICATION OF FRACTUREFracture can be distinguished
based on the connection with the surrounding bone tissue, bone
fracture shape, and location of the physical bones.5Based on the
connection of bone with surrounding bone tissue:1. Closed fracture
: there is no connection between the bone fragments with the
outside bone.
2. Open fracture : when there is a connection between the bone
fragments with outside bone due to an injury of the skin.
D. FEMORAL FRACTUREFemoral fracture is the break of bone
continuity groin can be caused by direct trauma (traffic accidents,
falls from high place), muscle fatigue and certain conditions such
as osteoporosis /degeneration of bone. There are 2 types of femur
fracture : 31. Intracapsuler fracture : fracture that occurs in the
joints, the pelvic and the capsule.
a. through the head of the femur (capital fracture)
b. Only below of the head femur
c. Through the neck of the femur2. Extracapsuler Fracture;a.
Occur outside of the joint and capsule, through the larger
trochanter femur / smaller/ on intertrochanter area.b. Occurs in
the distal part of the femur to the neck but not more than 2 inches
below the small trochanter.
E. ETIOLOGY OF FEMORAL FRACTURES Based on the causes of femoral
fractures, can be divided into three based on major of trauma
causes:1. High energy trauma or trauma due to considerable energy,
the type of accidents that cause this type of fracture including
vehicle accident trauma (accident motorcycle, car accidents, plane
crashes, etc.); sports-especially those related to speed such as:
skiing, bike racing, mountain climbing; falling, falling from a
high place; and gunshot wounds.
2. Low energy trauma or trauma due to weak energy, because the
structure of the femur is strong enough structures, there is a
tendency trauma due to weak energy is mainly due to loss of bone
strength, especially in people who experience a decrease in bone
density due to osteoporosis; bone metastasis of cancer patients and
people taking long-term corticosteroids are also at high risk of
femur fractures for bone strength will be reduced.
3. Stress fracture or fracture due to pressure, the third cause
of femur fractures is repeated stress or trauma. This kind of
trauma resulting in different types of fractures as usually happens
gradually. Repetitive stress trauma resulting in internal damage of
the structure of bone architecture. This type of fracture often
occurs on athletes or on the military people who undergo weight
training. This type of fracture typically affects the area of the
corpus femoris.F. PATHOPHYSIOLOGY OF FRACTUREChildren fracture is
usually as a result of trauma from motor vehicle accidents, falls,
or soft on child maltreatment. Soft tissue is usually still
flexible, so that fractures occur more frequently than tissue
injury (Muscari, 2001). Fractures can be also caused by the impulse
directly on bone, underlying pathological condition such as rickets
which lead to spontaneous fractures, strong and sudden muscle
contraction, and another indirect encouragement (Betz and Sowden,
2004). Another causes are metastatic of neuroblastoma, embryo
deficiency, osteomyelitis, an injury due to overdose and
immobilization which leads to osteoporosis.These fractures occur
when bone resistance against pressure transported by the pressure
force. The most common fractures seen in children are:71. Bend
Fracture
Characterized by bending at the point of the broken bones and
cannot be corrected without intervention.
2. Buckle Fracture
Caused by compression of the bone failure characterized by bones
that break through himself
3. Greenstick Fracture
An incomplete fractureFractures usually causes bone cells will
be damaged and causes bleeding in the area of the fracture that
cause multiple fractures of the soft tissue in the area are
damaged. When a fracture occurs, it will activate the inflammatory
response and causes the release of leukocytes agent, white blood
cells, and mast cells to repair the fracture condition. The release
of the inflammatory agent causes an increase in blood flow to the
area of the fracture and causes vasodilatation of blood vessels in
the area that causes the heat, redness and swelling. As the
inflammatory response, fibrin will form a mesh for new cells and
cause stimulated ostevlas and will form callus and later they will
form true bone.G. CLASSIFICATION OF FEMORAL FRACTURES ON
CHILDREN
1. Femoral Subtrochanter Fractures When there is a femur
fracture in the area of subtrochanter, muscles come into the
proximal fragment, especially partially illiopsoas and gluteus
muscles that form the position of flexion, external rotation, and
abduction.8-9
Picture 3. Photo of anteroposterior, proximal fragment flexion
90 degrees so it looks medullary cavity with a circular radiolucent
pictureTo correct the alignment of the fracture, skeletal traction
should be given continuously to pull the distal part into skeletal
traction in line posititon. Position of skeletal traxy come into
the distal metaphysis of the femur bone with a thigh flexion,
external rotation, and abduction. Mostly subtrocanter femoral
fractures occur on children who aged more than 10 years. At this
age, they can use the locked intramedullary rod or ORIF with the
nail plate.
Picture 4. Skeletal traction with pins inserted into
the distal femoral metaphysic.
Picture 5. subtrochanter femur fractures corrected with ORIF
with screw and plate nail.2. Femur Neck Fractures
a. Frequency and Mechanism of InjuryThe femur neck on children
is very strong unlike adults, just great trauma that can cause
fracture. Femoral neck Fracture is a rare type of fracture but
requires serious handling. Fracture around the hip joint due to a
force such as high-energy trauma, or in rare circumstances often
associated with pathological condition. Femoral neck fracture is
also often associated with violence against children (child abuse).
The incidence of femoral neck fractures on children is less than
1%. These fractures can occur on children of all ages, but the
highest incidence at the age of 11 years and 12 years, with 60-70%
occur in. In developing countries the most common cause is a
traffic accident while in developed countries generally cause is
falling from height such as trees and house roof. 30% of patients
had injuries associated with chest, head, and abdomen. Injury on
extremities such as femur fractures, tibia - fibula, and often
pelvic. Another thing that often lead to fracture of the femur on
children is child abuse.1,2,4b. classification
Fractures of the hip on children - children are classified by
location and first morphology. Cromwell is the first who explained
fractures of the femoral neck on children. Delbet publish standard
classification of fractures of the proximal femur in 1907. This
classification is not well known until Collona (1929) reported 12
cases using Delbet classification.Table 1. Classification of pelvic
fractures on children (Delbet)Type ITrans epiphyseal separation
(with or without dislocation of the femoral head from
acetabulum)
Type IITranservical
Type IIICervikotrochantrik
Type IVIntertrokanter
Table 2. pediatric femoral neck fractures - the type and the
importance characteristics Delbet type IncidenceCausesimportant
characteristics
Type I8% High energy trauma
Child abuse The difficult Breech childbirth
50% of cases occur in the epiphyseal head dislocation
High risk of AVN (20-100%) when associating with epiphyseal
dislocation
Differential diagnosis of septic arthritis, hip dislocation,
loss of femoral head epiphysis.
Type II45%severe trauma Variation of the most widely 70-80% are
displaced High risk of AVN (up to 50%). In displaced fractures,
loss of reduction, malunion, non-union, varus deformity.
Type III35%Severe traumaAVN 20-25% depending on the placement at
the time of injury.
Type IV12%traumaNon-Union and rarely AVN
Picture 6. Classification of proximal femur fractures on
children, based on the classification of Colonna and Delbet.c.
Assessment and Diagnosis
In addition, clinically diagnosis is often confusing. Usually
children who are traumatized often get pain in the pelvic region
and shortening, extremity rotated outwards. Children are usually
fear of passive limb movement and cannot move actively. Diagnose is
enforced using radiography, which is generally used on two planets
photograph, if it is not painful. Sonography is also often used on
condition that raises doubts e.g. pelvic pain on children. Fracture
line or hematoma intracapsular can be detected using fracture
ultrasound. With unknown fractures on the femur, the radiography
cannot be used as supporting diagnostic. Computed tomography (CT)
can be used to assess the degree of fracture and other
intracapsular hematoma. A bone scan at 3 months post-injury also
helps in detecting necrosis of the femoral head, which is a
possible complication. Magnetic resonance imaging (MRI) detects
previously avascular.In the state of femoral fractures, dorsalis
pedis arterial pulsation are palpated. In femoral fracture should
also be a secondary inspection because most patients only complain
of pain so things that can danger life such as internal bleeding in
the spleen rupture is often overlooked. Hence, the blood pressure
is also important to be supervised.10d. ManagementFractures of the
femoral neck on children are very unstable as like adults and
cannot be done adequately handling both with closed reduction,
external immobilization, or traction continuously.1 principles of
management including: 11-12 Minimize the potential complications in
avascular necrosis (AVN).
Avoid injury to the physical plate.
Reduction of fragments anatomically
Stabilization with pins or screws leads early protection to
withstand the weight.Decompression of the hemarthrosis and stable
internal fixation is an important aspect of the treatment for all
fractures with the shift. Fractures were not shifting can be
managed conservatively by using hip spica cast immobilization.
Based on studies conducted in 71 cases of the British Orthopedic
Association reported in 1962, Ratliff said that the high incidence
of non-union fractures occured in type II or type III treated
conservatively. Canale and Bourland in 1974, reported that the
observed fixation surgery showed better results.
According to Anil Arora (2006) treatment of traumatic fractures
of the femoral neck on children is based on the type and number of
shifts due to fractures, and skeletal maturity of children.
Internal fixation for femoral neck fracture type I, type II, and
type III, a smooth pin can be used on infants, screw cannula 4.0 mm
on children; screw cannula 6.5 mm on adolescents. For type IV
fracture fixation, in theory pediatric pelvic screws (pediatric hip
screw) is better on children and adults pelvic screws for
teenagers. Hip spica cast used a lot for postoperative
immobilization, especially on children