-
8/13/2019 Ref Firman
1/15
http://en.wikipedia.org/wiki/Tenon's_capsule
Tenon's capsuleFrom Wikipedia, the free encyclopedia
Tenon' s capsule
The right eye in sagittal section, showing the fascia bulbi
(semidiagrammatic).
Latin vagina bulbi
Gray's subject #227 1024
The fascia bulbi(also known as the capsule of Tnonand the bulbar
sheath) is a thin membrane which
envelops the eyeball from theoptic nerveto thelimbus, separating
it from the orbital fat and forming a
socket in which it moves.
Its inner surface is smooth, and is separated from the outer
surface of thescleraby theperiscleral lymph
space.
This lymph space is continuous with
thesubduralandsubarachnoidcavities, and is traversed by
delicate
bands of connective tissue which extend between the fascia and
the sclera.
The fascia is perforated behind by the ciliary vessels and
nerves, and fuses with the sheath of the optic
nerve and with the sclera around the entrance of theoptic
nerve.
In front it adheres to theconjunctiva,and both structures are
attached to the ciliary region of the eyeball.
The structure was named afterJacques-Ren Tenon(17241816),[1]
a French surgeon and pathologist.
Contents
http://en.wikipedia.org/wiki/Tenon's_capsulehttp://en.wikipedia.org/wiki/Tenon's_capsulehttp://en.wikipedia.org/wiki/Latinhttp://en.wikipedia.org/wiki/List_of_subjects_in_Gray%27s_Anatomy:227#Gray.27s_page_.231024http://education.yahoo.com/reference/gray/subjects/subject?id=227#p1024http://education.yahoo.com/reference/gray/subjects/subject?id=227#p1024http://en.wikipedia.org/wiki/Optic_nervehttp://en.wikipedia.org/wiki/Optic_nervehttp://en.wikipedia.org/wiki/Optic_nervehttp://en.wikipedia.org/wiki/Corneal_limbushttp://en.wikipedia.org/wiki/Corneal_limbushttp://en.wikipedia.org/wiki/Corneal_limbushttp://en.wikipedia.org/wiki/Sclerahttp://en.wikipedia.org/wiki/Sclerahttp://en.wikipedia.org/wiki/Sclerahttp://en.wikipedia.org/wiki/Periscleral_lymph_spacehttp://en.wikipedia.org/wiki/Periscleral_lymph_spacehttp://en.wikipedia.org/wiki/Periscleral_lymph_spacehttp://en.wikipedia.org/wiki/Periscleral_lymph_spacehttp://en.wikipedia.org/wiki/Subdural_spacehttp://en.wikipedia.org/wiki/Subdural_spacehttp://en.wikipedia.org/wiki/Subdural_spacehttp://en.wikipedia.org/wiki/Subarachnoidhttp://en.wikipedia.org/wiki/Subarachnoidhttp://en.wikipedia.org/wiki/Subarachnoidhttp://en.wikipedia.org/wiki/Optic_nervehttp://en.wikipedia.org/wiki/Optic_nervehttp://en.wikipedia.org/wiki/Optic_nervehttp://en.wikipedia.org/wiki/Conjunctivahttp://en.wikipedia.org/wiki/Conjunctivahttp://en.wikipedia.org/wiki/Conjunctivahttp://en.wikipedia.org/wiki/Jacques-Ren%C3%A9_Tenonhttp://en.wikipedia.org/wiki/Jacques-Ren%C3%A9_Tenonhttp://en.wikipedia.org/wiki/Jacques-Ren%C3%A9_Tenonhttp://en.wikipedia.org/wiki/Tenon's_capsule#cite_note-pmid12789585-1http://en.wikipedia.org/wiki/Tenon's_capsule#cite_note-pmid12789585-1http://en.wikipedia.org/wiki/Tenon's_capsule#cite_note-pmid12789585-1http://en.wikipedia.org/wiki/File:Gray891.pnghttp://en.wikipedia.org/wiki/Tenon's_capsule#cite_note-pmid12789585-1http://en.wikipedia.org/wiki/Jacques-Ren%C3%A9_Tenonhttp://en.wikipedia.org/wiki/Conjunctivahttp://en.wikipedia.org/wiki/Optic_nervehttp://en.wikipedia.org/wiki/Subarachnoidhttp://en.wikipedia.org/wiki/Subdural_spacehttp://en.wikipedia.org/wiki/Periscleral_lymph_spacehttp://en.wikipedia.org/wiki/Periscleral_lymph_spacehttp://en.wikipedia.org/wiki/Sclerahttp://en.wikipedia.org/wiki/Corneal_limbushttp://en.wikipedia.org/wiki/Optic_nervehttp://education.yahoo.com/reference/gray/subjects/subject?id=227#p1024http://en.wikipedia.org/wiki/List_of_subjects_in_Gray%27s_Anatomy:227#Gray.27s_page_.231024http://en.wikipedia.org/wiki/Latinhttp://en.wikipedia.org/wiki/Tenon's_capsule
-
8/13/2019 Ref Firman
2/15
[hide]
1 Relations to extraocular muscles
2 Sub Tenon's block for ophthalmic surgery
3 Pathology
4 References
Relations to extraocular muscles[edit]
It is perforated by the tendons of the ocular muscles, and is
reflected backward on each as a tubular
sheath.
The sheath of theObliquus superioris carried as far as the
fibrous pulley of that muscle; that on
theObliquus inferiorreaches as far as the floor of the orbit, to
which it gives off a slip.
The sheaths on the recti are gradually lost in theperimysium,but
they give off important expansions.
The expansion from theRectus superiorblends with the tendon of
theLevator palpebrae; that of
theRectus inferioris attached to theinferior tarsus.
The expansions from the sheaths of theRecti
lateralisandmedialisare strong, especially that from the
latter muscle, and are attached to the zygomatic bone and
lacrimal bone respectively.
As they probably check the actions of these two Recti they have
been named the medial and lateral check
ligaments.
Charles Barrett Lockwooddescribed a thickening of the lower part
of the fascia bulbi, which he named the
'suspensory ligament of the eye'. It is slung like a hammock
below the eyeball, being expanded in the
center, and narrow at its extremities which are attached to the
zygomatic andlacrimal bonesrespectively.
Sub Tenon's block for ophthalmic surgery[edit]
Local anaesthetic may be instilled into the space between
Tenon's capsule and the sclera to provide
anaesthesia for eye surgery, principally cataract surgery. After
applying local anaesthetic drops to
anaesthetise theconjunctiva,a small fold of conjunctiva is
lifted off the eyeball and an incision made. A
blunt, curved cannula is passed through the incision into
theperiscleral lymph spaceand a volume oflocal
anaestheticsolution is instilled. The advantages are a reduced
risk of bleeding and of penetration of the
globe, compared toperibulbarandretrobulbarapproaches. Akinesia
(paralysis of the external eye
muscles) may be less complete, however.
Pathology[edit]
Main article:Tenonitis
Tenon's capsule may be affected by a disease called idiopathic
orbital inflammation, a condition of
unknown etiology that is characterized by inflammation of one or
more layers of the eye. The disease is
http://en.wikipedia.org/wiki/Tenon's_capsulehttp://en.wikipedia.org/wiki/Tenon's_capsulehttp://en.wikipedia.org/wiki/Tenon's_capsulehttp://en.wikipedia.org/wiki/Tenon's_capsule#Relations_to_extraocular_muscleshttp://en.wikipedia.org/wiki/Tenon's_capsule#Relations_to_extraocular_muscleshttp://en.wikipedia.org/wiki/Tenon's_capsule#Sub_Tenon.27s_block_for_ophthalmic_surgeryhttp://en.wikipedia.org/wiki/Tenon's_capsule#Sub_Tenon.27s_block_for_ophthalmic_surgeryhttp://en.wikipedia.org/wiki/Tenon's_capsule#Pathologyhttp://en.wikipedia.org/wiki/Tenon's_capsule#Pathologyhttp://en.wikipedia.org/wiki/Tenon's_capsule#Referenceshttp://en.wikipedia.org/wiki/Tenon's_capsule#Referenceshttp://en.wikipedia.org/w/index.php?title=Tenon%27s_capsule&action=edit§ion=1http://en.wikipedia.org/w/index.php?title=Tenon%27s_capsule&action=edit§ion=1http://en.wikipedia.org/w/index.php?title=Tenon%27s_capsule&action=edit§ion=1http://en.wikipedia.org/wiki/Obliquus_superiorhttp://en.wikipedia.org/wiki/Obliquus_superiorhttp://en.wikipedia.org/wiki/Obliquus_superiorhttp://en.wikipedia.org/wiki/Obliquus_inferiorhttp://en.wikipedia.org/wiki/Obliquus_inferiorhttp://en.wikipedia.org/wiki/Obliquus_inferiorhttp://en.wikipedia.org/wiki/Perimysiumhttp://en.wikipedia.org/wiki/Perimysiumhttp://en.wikipedia.org/wiki/Perimysiumhttp://en.wikipedia.org/wiki/Rectus_superiorhttp://en.wikipedia.org/wiki/Rectus_superiorhttp://en.wikipedia.org/wiki/Rectus_superiorhttp://en.wikipedia.org/wiki/Levator_palpebraehttp://en.wikipedia.org/wiki/Levator_palpebraehttp://en.wikipedia.org/wiki/Levator_palpebraehttp://en.wikipedia.org/wiki/Rectus_inferiorhttp://en.wikipedia.org/wiki/Rectus_inferiorhttp://en.wikipedia.org/wiki/Rectus_inferiorhttp://en.wikipedia.org/wiki/Inferior_tarsushttp://en.wikipedia.org/wiki/Inferior_tarsushttp://en.wikipedia.org/wiki/Inferior_tarsushttp://en.wikipedia.org/wiki/Lateral_rectushttp://en.wikipedia.org/wiki/Lateral_rectushttp://en.wikipedia.org/wiki/Lateral_rectushttp://en.wikipedia.org/wiki/Medial_rectushttp://en.wikipedia.org/wiki/Medial_rectushttp://en.wikipedia.org/wiki/Medial_rectushttp://en.wikipedia.org/wiki/Charles_Barrett_Lockwoodhttp://en.wikipedia.org/wiki/Charles_Barrett_Lockwoodhttp://en.wikipedia.org/wiki/Suspensory_ligament_of_the_eyehttp://en.wikipedia.org/wiki/Suspensory_ligament_of_the_eyehttp://en.wikipedia.org/wiki/Suspensory_ligament_of_the_eyehttp://en.wikipedia.org/wiki/Lacrimal_bonehttp://en.wikipedia.org/wiki/Lacrimal_bonehttp://en.wikipedia.org/wiki/Lacrimal_bonehttp://en.wikipedia.org/w/index.php?title=Tenon%27s_capsule&action=edit§ion=2http://en.wikipedia.org/w/index.php?title=Tenon%27s_capsule&action=edit§ion=2http://en.wikipedia.org/w/index.php?title=Tenon%27s_capsule&action=edit§ion=2http://en.wikipedia.org/wiki/Conjunctivahttp://en.wikipedia.org/wiki/Conjunctivahttp://en.wikipedia.org/wiki/Conjunctivahttp://en.wikipedia.org/wiki/Periscleral_lymph_spacehttp://en.wikipedia.org/wiki/Periscleral_lymph_spacehttp://en.wikipedia.org/wiki/Periscleral_lymph_spacehttp://en.wikipedia.org/wiki/Local_anaesthetichttp://en.wikipedia.org/wiki/Local_anaesthetichttp://en.wikipedia.org/wiki/Local_anaesthetichttp://en.wikipedia.org/wiki/Local_anaesthetichttp://en.wikipedia.org/w/index.php?title=Peribulbar&action=edit&redlink=1http://en.wikipedia.org/w/index.php?title=Peribulbar&action=edit&redlink=1http://en.wikipedia.org/w/index.php?title=Peribulbar&action=edit&redlink=1http://en.wikipedia.org/wiki/Retrobulbarhttp://en.wikipedia.org/wiki/Retrobulbarhttp://en.wikipedia.org/wiki/Retrobulbarhttp://en.wikipedia.org/w/index.php?title=Tenon%27s_capsule&action=edit§ion=3http://en.wikipedia.org/w/index.php?title=Tenon%27s_capsule&action=edit§ion=3http://en.wikipedia.org/w/index.php?title=Tenon%27s_capsule&action=edit§ion=3http://en.wikipedia.org/wiki/Tenonitishttp://en.wikipedia.org/wiki/Tenonitishttp://en.wikipedia.org/wiki/Tenonitishttp://en.wikipedia.org/wiki/Tenonitishttp://en.wikipedia.org/w/index.php?title=Tenon%27s_capsule&action=edit§ion=3http://en.wikipedia.org/wiki/Retrobulbarhttp://en.wikipedia.org/w/index.php?title=Peribulbar&action=edit&redlink=1http://en.wikipedia.org/wiki/Local_anaesthetichttp://en.wikipedia.org/wiki/Local_anaesthetichttp://en.wikipedia.org/wiki/Periscleral_lymph_spacehttp://en.wikipedia.org/wiki/Conjunctivahttp://en.wikipedia.org/w/index.php?title=Tenon%27s_capsule&action=edit§ion=2http://en.wikipedia.org/wiki/Lacrimal_bonehttp://en.wikipedia.org/wiki/Suspensory_ligament_of_the_eyehttp://en.wikipedia.org/wiki/Charles_Barrett_Lockwoodhttp://en.wikipedia.org/wiki/Medial_rectushttp://en.wikipedia.org/wiki/Lateral_rectushttp://en.wikipedia.org/wiki/Inferior_tarsushttp://en.wikipedia.org/wiki/Rectus_inferiorhttp://en.wikipedia.org/wiki/Levator_palpebraehttp://en.wikipedia.org/wiki/Rectus_superiorhttp://en.wikipedia.org/wiki/Perimysiumhttp://en.wikipedia.org/wiki/Obliquus_inferiorhttp://en.wikipedia.org/wiki/Obliquus_superiorhttp://en.wikipedia.org/w/index.php?title=Tenon%27s_capsule&action=edit§ion=1http://en.wikipedia.org/wiki/Tenon's_capsule#Referenceshttp://en.wikipedia.org/wiki/Tenon's_capsule#Pathologyhttp://en.wikipedia.org/wiki/Tenon's_capsule#Sub_Tenon.27s_block_for_ophthalmic_surgeryhttp://en.wikipedia.org/wiki/Tenon's_capsule#Relations_to_extraocular_muscleshttp://en.wikipedia.org/wiki/Tenon's_capsule
-
8/13/2019 Ref Firman
3/15
also known as orbital inflammatory pseudotumor, and sometimes
may only affect thelacrimal glandor
theextraocular muscles.[2]
References[edit]
1. ^Tenon JR, Naus J, Blanken R (March 2003). "Anatomical
observations on some parts of the eye and
eyelids. 1805". Strabismus11(1):
638.doi:10.1076/stra.11.1.63.14089.PMID12789585.
2. ^Mitchell, Richard N. "Eye, Orbit". P
http://en.wikipedia.org/wiki/Lacrimal_glandhttp://en.wikipedia.org/wiki/Lacrimal_glandhttp://en.wikipedia.org/wiki/Lacrimal_glandhttp://en.wikipedia.org/wiki/Extraocular_muscleshttp://en.wikipedia.org/wiki/Extraocular_muscleshttp://en.wikipedia.org/wiki/Tenon's_capsule#cite_note-Robbins-2http://en.wikipedia.org/wiki/Tenon's_capsule#cite_note-Robbins-2http://en.wikipedia.org/wiki/Tenon's_capsule#cite_note-Robbins-2http://en.wikipedia.org/w/index.php?title=Tenon%27s_capsule&action=edit§ion=4http://en.wikipedia.org/w/index.php?title=Tenon%27s_capsule&action=edit§ion=4http://en.wikipedia.org/w/index.php?title=Tenon%27s_capsule&action=edit§ion=4http://en.wikipedia.org/wiki/Tenon's_capsule#cite_ref-pmid12789585_1-0http://en.wikipedia.org/wiki/Tenon's_capsule#cite_ref-pmid12789585_1-0http://en.wikipedia.org/wiki/Digital_object_identifierhttp://en.wikipedia.org/wiki/Digital_object_identifierhttp://dx.doi.org/10.1076%2Fstra.11.1.63.14089http://dx.doi.org/10.1076%2Fstra.11.1.63.14089http://dx.doi.org/10.1076%2Fstra.11.1.63.14089http://en.wikipedia.org/wiki/PubMed_Identifierhttp://en.wikipedia.org/wiki/PubMed_Identifierhttp://www.ncbi.nlm.nih.gov/pubmed/12789585http://www.ncbi.nlm.nih.gov/pubmed/12789585http://www.ncbi.nlm.nih.gov/pubmed/12789585http://en.wikipedia.org/wiki/Tenon's_capsule#cite_ref-Robbins_2-0http://en.wikipedia.org/wiki/Tenon's_capsule#cite_ref-Robbins_2-0http://en.wikipedia.org/wiki/Tenon's_capsule#cite_ref-Robbins_2-0http://www.ncbi.nlm.nih.gov/pubmed/12789585http://en.wikipedia.org/wiki/PubMed_Identifierhttp://dx.doi.org/10.1076%2Fstra.11.1.63.14089http://en.wikipedia.org/wiki/Digital_object_identifierhttp://en.wikipedia.org/wiki/Tenon's_capsule#cite_ref-pmid12789585_1-0http://en.wikipedia.org/w/index.php?title=Tenon%27s_capsule&action=edit§ion=4http://en.wikipedia.org/wiki/Tenon's_capsule#cite_note-Robbins-2http://en.wikipedia.org/wiki/Extraocular_muscleshttp://en.wikipedia.org/wiki/Lacrimal_gland
-
8/13/2019 Ref Firman
4/15
http://telemedicine.orbis.org/bins/volume_page.asp?cid=1-2161-2163-2172
Chapter 2: Surgical Anatomy-
Tenons capsuleLecture 8 of 22 NEXT
Tenon's capsule is a structure with definite body and substance
in childhood which
gradually atrophies in old age but not to the same degree as
conjunctiva. Tenon's
capsule has an anterior and posterior part. Anterior Tenon's
capsule is the vestigial
capsulopalpebral head of the rectus muscles. This covers the
anterior half to two-thirds
of the rectus muscles in their sheaths as well as the
intermuscular membrane. Anterior
Tenon's capsule is fused with the undersurface of conjunctiva
and attaches to sclera at
the limbus. The fused conjunctiva-anterior Tenon's capsule is
movable over underlying
posterior Tenon's capsule and episclera, the latter being the
anterior extension of
posterior Tenon's capsule. Episclera starts at the level of the
insertion of the rectus
muscles in a line around the globe, which is called the spiral
of Tillaux. Episclera joinsconjunctiva and anterior Tenon's
capsule, fusing at the limbus.
Posterior Tenon's capsule is made up of the fibrous sheath of
the rectus muscles
together with the intermuscular membrane. According to Lester
Jones, the tissues that
make up posterior Tenon's capsule form at a later evolutionary
stage than those forming
anterior Tenon's capsule. Fibrous attachments between the inner
surface of anterior
Tenon's capsule and the outer muscle sheath (part of posterior
Tenon's capsule) fuse at
a point 15 to 20 mm behind the insertion of the medial and
lateral rectus muscles to
form a barrier to extraconal fat. A condensation of fibrous
tissue and smooth muscle
between the outer surface of anterior Tenon's capsule and the
orbital wall medially and
laterally is the location of the aforementioned pulleys of the
horizontal rectus muscles. Ifthe horizontal rectus muscle is
separated completely from anterior Tenon's capsule,
exposing extraconal fat, there will be no or reduced pulley
effect on the eye muscle. This
will result in up and down slip of the muscle relative to the
globe. It is not practical or
even logical in the usual strabismus surgery to free pulleys
outside anterior Tenon's
capsule, but this could be done for special need. Eye muscle
surgery is routinely
performed entirely insideanterior Tenon's capsule with no fat
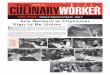
exposure (Figure 25 A-C).
Figure 25The Conjunctiva/Tenons Capsule Relationships
http://telemedicine.orbis.org/bins/volume_page.asp?cid=1-2161-2163-2172http://telemedicine.orbis.org/bins/volume_page.asp?cid=1-2161-2163-2172http://telemedicine.orbis.org/bins/volume_page.asp?cid=1-2161-2163-2173http://telemedicine.orbis.org/bins/volume_page.asp?cid=1-2161-2163-2173http://telemedicine.orbis.org/bins/volume_page.asp?cid=1-2161-2163-2173http://telemedicine.orbis.org/bins/volume_page.asp?cid=1-2161-2163-2172
-
8/13/2019 Ref Firman
5/15
AAxial view of the orbit
1 Wall of the orbit
2 Conjunctiva3 Anterior Tenons capsule
4 Posterior Tenons capsule
5 The muscle
6 Intermuscular membrane
(posterior Tenons capsule)
7 Intraconal orbital fat
8 Extraconal orbital fat
9 Horizontal pulley
10 Episclera
B1 The limbal fusion of theconjunctiva and anterior
Tenons capsule2 Potential space between
anteriorTenons capsule and episclera3 The muscle in its
sheath(posterior Tenons capsule)inserting into the sclera
4 Postinsertional musclefootplates
5 Episclera6 Conjunctiva7 Anterior Tenons capsule
CCoronal section of B at X
1 Conjunctiva
2 Anterior Tenons capsule3 Muscle sheath
4 Extraocular muscle
5 Intermuscular membrane
6 Sclera substance
Posterior Tenon's capsule, composed of the muscle's capsule and
the intermuscular
membrane, unites the rectus muscles in a ring around the globe.
The extent to which the
intermuscular membrane is cut during surgery influences how far
the rectus muscles,
particularly the medial and to some extent the lateral, will
retract during surgery.
Dissection of posterior Tenon's capsule far posteriorly leads to
exposure of intraconal fat,
so called because it resides inside the muscle cone. Excessive
dissection of anterior
Tenon's capsule exposes extraconal fat and risks disruption of
the pulleys of the medial
and lateral rectus muscles.
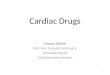
Figure 26
A
-
8/13/2019 Ref Firman
6/15
B
C
AWhen the layer of fused
conjunctiva-anterior Tenon's
capsule is retracted, the muscle
insertion in its sheath is exposed.
Fibrous attachments are seenbetween the undersurface of
anterior Tenons capsule and the
outer surface of the muscle. The
fusion of the intermuscular
membrane (posterior Tenon's
capsule), as well as of the muscle to
the sclera, is apparent. This fusion
of the intermuscular membrane to
the sclera must be incised before
the bare sclera and subposterior
Tenon's capsule space can beencountered. Only after entering
subposterior Tenon's capsule space
can the insertion of the rectus
muscle be engaged cleanly on a
muscle hook. This is the free space
used by the retina surgeon. The tip
of the scissors in the photo points
to this free space.
BPosterior Tenons capsule attaches to sclera at the muscles
insertion and in the intermuscular space forming the spiral
of
Tillaux.
CThe muscle hook is placed in a hole created in
intermuscular
membrane adjacent to the muscle insertion and glides along
bare
sclera behind the rectus muscle insertion and is exposed at
theopposite muscle border with a snip incision.
DThe muscle hook is placed in a hole created in intermuscular
membrane adjacent to the muscle insertion and
glides along bare sclera behind the rectus muscle insertion and
is exposed at the opposite muscle border with a
snip incision.With a limbal incision, the multiple layers and
surfaces associated with the rectus muscles can be
readily seen. Conjunctiva and anterior Tenons capsule shown here
separated are actually fused and separated
only with difficulty.
-
8/13/2019 Ref Firman
7/15
While extraocular muscle surgery is performed beneath anterior
Tenon's capsule, it is done within the plane of
posterior Tenon's capsule. The intermuscular membrane part of
posterior Tenon's capsule must be fenestrated in
order to place a muscle hook behind the insertion of a rectus
muscle (Figure 26 A-D). How much more
dissection is done in the intermuscular membrane beyond the
minimum required to gain access to the muscle is
the decision of the surgeon. It is probably wise to do as little
cutting of posterior Tenon's capsule as is
compatible with the conduct of the surgical procedure intended.
Retinal detachment surgery, in contrast to
extraocular muscle surgery, is carried out beneathposterior
Tenon's capsule. This enables a view of the scleral
surface far posteriorly to a point near the posterior ciliary
vessels and the optic nerve.
Surgical anatomy of the rectus musclesLecture 9 of 22 NEXT
Each rectus muscle inserts at a different distance from the
limbus. The insertions of
these muscles are the prime surgical landmarks in extraocular
muscle surgery. The
medial rectus is said to insert in the normal eye 5.5 mm from
the limbus. This figure
presumably was arrived at from study of otherwise normal eyes.
Since no specific
mention is made of whether the measurements were taken from
specimens with
strabismus, it is assumed they were not. The average distance
between the limbus and
the medial rectus insertion of 112 medial rectus muscles in 66
esotropic patients was 4.4
mm with a range of 3.0 to 6.0 mm. Eight patients had unequal
medial rectus insertion to
limbus measurements. There was no correlation found between the
angle of
esodeviation and the distance of the medial rectus insertion
from the limbus. The
variability of this insertion along with its lack of correlation
with the angle of esotropia
begs the question, Is the insertion the best landmark for
measurement of a medial
rectus recession? Since the answer is obviously no, it is
preferable to use the limbus, a
more consistent anatomical point, as the reference for recession
of the medial rectus
muscle. When measuring from the limbus, the amount of muscle
retroplacement from
the muscle's actual insertion can be noted by those surgeons
accustomed to the
traditional medial rectus recession numbers used as guidelines
for recession. For
example, if a 5.5 mm recession of the medial rectus is done in a
patient whose medial
rectus inserts 4.5 mm from the limbus (not noticed by the
surgeon) and a 5.5 mm
recession is done, the new insertion site is located 9.0 mm from
the limbus in a normal
sized eye. This could result in an undercorrection, and in all
likelihood, this occurred not
infrequently when 5.5 mm was considered the maximum medial
rectus recession. On the
other hand, if in this same patient the medial rectus were
recessed 10.0 mm from the
limbus, the resultant recession measured from the insertion
would actually be 6.5 mm, a
number perhaps considered too large for the deviation but one
which would be required
because of the medial rectus insertion site being closer to the
limbus.
Use of the limbus as the point of reference for medial rectus
recession allows thesurgeon to perform larger recessions safely by
not exceeding the landmark of theequator. The equatorial landmark
has been shown to be reliable because in patients withrefractive
errors between + or - 4.00 diopters, the axial length of the eye is
predictablefor the age of the patient. This has been confirmed by
simple to perform axial length
measurement with the A-scan device. At the same time, the
corneal dimension is alsoreliable. If it appears to be other than
the normal dimension, this is obvious andmeasurement for
confirmation is simple. Whether or not discovery of the pulleys
will
alter this thinking is not clear now. It is known, however, that
successful realignment ofcongenital esotropia occurs more
frequently when measurement is carried out from thelimbus compared
to the prior upper limit of recession of 5.5 mm. With larger
medialrectus recession measured from the insertion now being done,
first surgery alignment in
http://telemedicine.orbis.org/bins/volume_page.asp?cid=1-2161-2163-2174http://telemedicine.orbis.org/bins/volume_page.asp?cid=1-2161-2163-2174http://telemedicine.orbis.org/bins/volume_page.asp?cid=1-2161-2163-2174
-
8/13/2019 Ref Firman
8/15
congenital esotropia is improved, but the incidence of
overcorrection is not known.
The inferior rectus inserts 6.5 mm from the limbus; the lateral
rectus inserts 6.9 mm
from the limbus (range: 4.5 to 8.0 mm);* and the superior rectus
inserts 7.7 mm from
the limbus. Beginning with the medial rectus and moving
inferiorly and temporally, each
rectus muscle inserts farther from the limbus. The line
connecting these insertions iscalled the spiral of Tillaux (Figure
27). The circumference of the ring formed by closing
the spiral is approximately 80 mm. The width of the insertion of
each of the rectus
muscles is approximately 10 mm. The distance between the
adjacent insertion borders is
approximately 10 mm (Figure 28).
Figure 27
The spiral of Tillaux and the relationship of
the rectus muscle insertions.
Figure 28
Width of the rectus muscle insertions
The issue can be summed up as follows: the insertion of the
medial rectus muscle in esotropia tends to be
closer to the limbus than the 5.5 mm stated for the normal.
Therefore, recession measured from the limbus, a
more reliable landmark, allows larger recessions to be done
safely thus reducing the likelihood o
undercorrection.
The insertion of the rectus muscles can be seen relatively
easily through the intact
conjunctiva. This means that the muscles location can be
confirmed when the eye isrotated and the conjunctiva is brought
tightly over the insertion of any of the rectus
muscles. Close observation reveals the line of insertion of the
muscle, with the muscleappearing as a slightly darker and faintly
raised structure beneath conjunctiva (Figure29). By confirming the
rectus muscles insertion in this manner, the surgeon can locate
each of the rectus muscles accurately in roughly the 3, 6, 9,
and 12 o'clock positions ofthe globe. This maneuver leads to proper
traction suture or traction forceps placementand allows strategic
placement of the incision through conjunctiva leading to
accuratelocalization of the muscle to be operated upon. This
maneuver to establish the locationof the rectus muscles should be
done routinely at the outset of each eye muscle
surgicalprocedure.
The rectus muscles are all approximately 40 mm long and each
receives innervationfrom the undersurface (intraconal space) at the
junction of the middle and posterior
-
8/13/2019 Ref Firman
9/15
thirds of the muscle or 26 mm from the insertion. The six pairs
of extraocular muscles
are characterized in Table 1.
* Although the lateral rectus insertion site is variable, it is
not common to measure from the limbus for
recession of this muscle.
A B
C D
E
Figure 29
AThe superior rectus muscle seen through the intact conjunctiva
and anterior Tenons capsule.
BThe insertion of the inferior rectus muscle seen through the
intact conjunctiva. Note fat pad.
CThe insertion of the lateral rectus muscle seen through the
intact conjunctiva.
DThe insertion of the medial rectus muscle seen through the
intact conjunctiva.
EThe insertion of the lateral and inferior rectus muscles seen
through the intact conjunctiva with the
inferior temporal orbital fat pad seen just inside the lower lid
margin. The site of the incision for inferior
oblique exposure is shown. This view is shown from above.
-
8/13/2019 Ref Firman
10/15
Muscle Length(mm) Nerve Point of Innervation Tendon*
(mm)
Muscle action
Medialrectus
(MR)
40 III Inferiordivision
26 mm from insertion L: 3.7W: 10.3
Adduction
Inferior
rectus
(IR)
40 III Inferior
division
26 mm from insertion L: 5.5
W: 9.8
Depression
Excycloduction
Adduction
Lateral
rectus
(LR)
40 VI 26 mm from insertion L: 8.8
W: 9.2
Abduction
Superior
rectus(SR)
40 III
Superiordivision
26 mm from insertion L: 5.8
W: 10.8
Elevation
IncycloductionAdduction
Inferior
oblique
(IO)
36 III Inferior
division
12 mm posterior to
insertion of inferior
rectus at its lateral
border
L: < 1
W: 9.4
Elevation
Excycloduction
Abduction
Superior
oblique
(SO)
60 IV 26 mm from trochlea L: 30
W: 10.7
Depression
Incycloduction
Abduction
* L - length; W - width at insertion
Table 1 Extraocular Muscles
-
8/13/2019 Ref Firman
11/15
http://www.expertconsultbook.com/expertconsult/ob/book.do?method=display&type=bookPage&
decorator=none&eid=4-u1.0-B978-1-4377-2272-7..00005-6--s0020&isbn=978-1-4377-2272-7
Tenon's capsule
Tenon's capsule is a dense, elastic, fibrovascular connective
tissue layer that surrounds the globe,
except over the cornea. It also invests the anterior portions of
the extraocular muscle insertions. This
structure begins near the perilimbal sclera anteriorly and
extends around the globe to the optic nerve
where it blends with fibers of the dural sheath and sclera.
Anterior to the insertion of the rectus
muscles, about 2 mm behind the corneal limbus, Tenon's capsule
originates and is firmly adherent to
episclera. Over the surface of the globe, Tenon's capsule is
separated from episclera by a loose
potential space that provides a smooth surface for ocular
motility. It was the discovery of this capsule
by Tenon,[44]
and its popularization by O'Farrall and Bonnet (cited in
Snyder)[43]
that led to
development of modern enucleation techniques, and abandonment of
more barbaric and anatomically
mutilating surgery.
http://www.expertconsultbook.com/expertconsult/ob/book.do?method=display&type=bookPage&decorator=none&eid=4-u1.0-B978-1-4377-2272-7..00005-6--s0020&isbn=978-1-4377-2272-7http://www.expertconsultbook.com/expertconsult/ob/book.do?method=display&type=bookPage&decorator=none&eid=4-u1.0-B978-1-4377-2272-7..00005-6--s0020&isbn=978-1-4377-2272-7http://www.expertconsultbook.com/expertconsult/ob/book.do?method=display&type=bookPage&decorator=none&eid=4-u1.0-B978-1-4377-2272-7..00005-6--s0020&isbn=978-1-4377-2272-7http://www.expertconsultbook.com/expertconsult/ob/linkTo?type=bookPage&isbn=978-1-4377-2272-7&eid=4-u1.0-B978-1-4377-2272-7..00005-6--bb0225&appID=NGEhttp://www.expertconsultbook.com/expertconsult/ob/linkTo?type=bookPage&isbn=978-1-4377-2272-7&eid=4-u1.0-B978-1-4377-2272-7..00005-6--bb0225&appID=NGEhttp://www.expertconsultbook.com/expertconsult/ob/linkTo?type=bookPage&isbn=978-1-4377-2272-7&eid=4-u1.0-B978-1-4377-2272-7..00005-6--bb0225&appID=NGEhttp://www.expertconsultbook.com/expertconsult/ob/linkTo?type=bookPage&isbn=978-1-4377-2272-7&eid=4-u1.0-B978-1-4377-2272-7..00005-6--bb0220&appID=NGEhttp://www.expertconsultbook.com/expertconsult/ob/linkTo?type=bookPage&isbn=978-1-4377-2272-7&eid=4-u1.0-B978-1-4377-2272-7..00005-6--bb0220&appID=NGEhttp://www.expertconsultbook.com/expertconsult/ob/linkTo?type=bookPage&isbn=978-1-4377-2272-7&eid=4-u1.0-B978-1-4377-2272-7..00005-6--bb0220&appID=NGEhttp://www.expertconsultbook.com/expertconsult/ob/linkTo?type=bookPage&isbn=978-1-4377-2272-7&eid=4-u1.0-B978-1-4377-2272-7..00005-6--bb0220&appID=NGEhttp://www.expertconsultbook.com/expertconsult/ob/linkTo?type=bookPage&isbn=978-1-4377-2272-7&eid=4-u1.0-B978-1-4377-2272-7..00005-6--bb0225&appID=NGEhttp://www.expertconsultbook.com/expertconsult/ob/book.do?method=display&type=bookPage&decorator=none&eid=4-u1.0-B978-1-4377-2272-7..00005-6--s0020&isbn=978-1-4377-2272-7http://www.expertconsultbook.com/expertconsult/ob/book.do?method=display&type=bookPage&decorator=none&eid=4-u1.0-B978-1-4377-2272-7..00005-6--s0020&isbn=978-1-4377-2272-7
-
8/13/2019 Ref Firman
12/15
ANATOMI BOLA MATA. BY: FAUZAN MUTTAQIEN
RONGGA ORBITA
1. Bentuk seperti piramida
2. Dibatasi dinding tulang
3. Dibagian belakang terdapat 3 lubang : foramen optic, fisura
orbita sup et inf.
4. Isi :
a. Bola mata
b. 6 otot penggerak
c. Kelenjar air mata
d. Arteri
e. Saraf kranial iii, iv, dan vi
f. Lemak dan fascia
BOLA MATA
Terdiri dari :
1. Dinding bola mata :
a. Sklera
b. Kornea
2. Isi bola mata
Sklera
a. Jaringan ikat kolagen yang kenyal warna putih
b. Tebal 1 mm
c. Bagian belakang terdapat lamina kribrosa tempat menembusnya
saraf optik
d. Dilapisi kapsul tenon dan dibagian depan oleh konjungtiva
e. Diantara stroma, sklera dan kapsul tenon terdapat episklera
yang kaya pembuluh darah (untuk
nutrisi sklera)
f. Bagian dalam terdapat lamina fuska yang membatasi sklera dan
koroid
Kornea
a. Merupakan jaringan jernih dan bening. jernih karena
avaskular
b. Bentuk sebagai lingkaran, diameter diukur secara vertical
1112 mm
bila >12 mm pada anakglaukoma congenital
c. Tebal = 0,61 mm
d. Sumber nutrisi kornea :
- Pembuluh darah limbus
- Humour aqueos
- Air mata
e. Terdiri dari 5 lapisan :
-
8/13/2019 Ref Firman
13/15
1. Epitel; 5 6 lapisan sel, bentuk sel gepeng, ujung saraf
kornea pada epitel (cab. N. V),
regenerasi cukup baik, jika terjadi kerusakan tidak timbul
jaringan parut
2. Membran bowman; tipis yang homogen, terdiri dari serat
kolagen yang kuat, jika terjadi
kerusakan timbul jaringan parut
3. Stroma; lapisan yang paling tebal (90%), tersusun atas
serabut lamelar terjalin satu sama
lainnya, jika terjadi kerusakan timbul jaringan parut dan
leukoma4. Membran discement; lapisan tipis kenyal, kuat, bening,
tidak berstruktur, sebagai barrier
terhadap mikroorganisme dan pembuluh darah
5. Endotel; satu lapis sel, mempertahankan kejernihan kornea,
tidak ada kemampuan
regenerasi
paling tebalstroma,
paling kuatdescement
paling pekaendotel
Kelainan kornea yang menyebabkan gangguan refraksi:
1. radang
2. TIO meningkat
3. sikatriks dari ulkus yang sembuh
Isi Bola Mata
1. Lensa
a. Bening, bikonveks, tebal 5 mm, diameter 9 mm
b. Difiksasi oleh zonula zinn
c. Terdiri dari kapsul, korteks, dan nukleus
d. Bertambah usia, nukleus membesar
e. Fungsi : membias cahaya menjadi fokus
f. Merupakan salah satu media refrakta
g. Komposisi : 0,5% air, 35% protein (kristalin , , )
h. Tidak mempunyai pembuluh darah dan persarafan
i. Semakin bertambah usia nukleus semakin membesar
j. Fungsi untuk membiaskan cahayak. Kekuatan +20 Dioptri
2. Uvea
a. Lapisan kedua dinding bola mata
b. Jaringan lunak
c. Terdiri dari 3 bagian : iris, badan siliar, koroid
Iris:
a. Membran berwarna
b. Bentuk sirkular, ditengah terdapat pupil dengan diameter 35
mm
c. Berpangkal pada badan siliar
-
8/13/2019 Ref Firman
14/15
d. Permukaan iris banyak lekukan (kriptae)
e. Otot iris = otot polos : sfingter pupil, dilator pupil
f. Pembuluh darah :
- Sirkulus major = pangkal iris
- Sirkulus minor = pupil
g. Saraf : n. Nasosiliar cabang n. Iii- Simpatis = midriasi
- Parasimpatis = miosis
Badan Siliar :
a. Mulai dari pangkal iris oraserata
b. Terdiri dari :
- Prosesus siliaris, fungsi : produksi h a
- Otot silliar (sirkular, radial, meridional), fungsi :
akomodasi (lensa cembung)
Koroid :
a. Warna cokelat tua, diantara retina dan sklera
b. Mulai dari oraserata terdapat papil optik
c. Kaya pembuluh darah
d. Fungsi : nutrisi retina bagian luar
3. Badan kaca (corpus vitreus)
a. Sebagian mengisi bola mata
b. Tidak berwrna, bening, konsistensi lunak
c. Dilapisi membran hialoid
d. Avaskuler
e. Mendapat nutrisi dari koroid, badan siliar, dan retina
Kelainan, kekeruhan karena:
- pusendoftalmitis
- darahhemoftalmitis
- degenerasiretinopati diabetik
gunakan oftalmoskop untuk melihat kelainan pada korpus
vitreus
4. Retinaa. Membran bening dan tipis 1 mm
b. Terdiri dari serabut saraf optik
c. Letak antara badan kaca dan koroid berakhir pada
oraserata
d. Terdapat makula lutea (bintik kuning), diameter 12 mm sebagai
pusat penglihatan
e. 3 mm ke arah nasal terdapat papil saraf optik (bintik
buta)
f. Arteri dan vna retina sentral masuk ke bola mata ditengah
papil saraf optik
g. Ada 10 lapisan :
- Membran limitan dalam
- Lapisan serabut saraf, terdapat cabang utama pembuluh darah
retina
- Lapisan sel ganglion, sel saraf bercabang disini
- Lapisan pleksiform dalam- Lapisan nukleus dalam, terbentuk
dari badan dan nukleus sel bipolar
-
8/13/2019 Ref Firman
15/15
- Lapisan pleksiform luar
- Membran limitan luar
- Lapisan nukleus luar, terdiri dari nukleus sel kerucut dan
batang
- Lapisan sel batang dan kerucut, fungsinya menangkap sinar
- Lapisan epitel pigmen
Humor Aquos
normalnya jernih
kelainan humor aquos yang mengganggu refraksi:
- radang
- hipopion (pus)
- hifema (perdarahan)
Bilik mata depan (COA)batas kornea sampai iris dan kapsul
anterior lensa
Bilik mata belakang (COP)batas dari lapian belakang iris sampai
lensa (zonula zinn)












![Tony Firman - Making Simple Bookbinding Equipment - A Sewing Frame [10pp]](https://img.pdfslide.us/doc/110x75/577cce5d1a28ab9e788ddc4c/tony-firman-making-simple-bookbinding-equipment-a-sewing-frame-10pp.jpg)