Embed Size (px)
Citation preview

REEDA: EVALUATING POSTPARTUM: HEALING
NANCY DAVIDSON
C.N.M., M.S.
Nancy Davidson is an Assistant Professor of Maternal-Child Nursing, Washington State University at the Zntercollegiate Center for Nursing Education.
A nursing tool, REEDA, has been devised to evaluate post partum healing of the peri- neum following an episiotomy. Based on the method’s scoring process, normal healing may now be described and related to the comfort and discomfort of a patient and nursing measures instituted that will in- crease patient comfort.
The process of healing, though well de- scribed in the professional literature for ab- dominal wounds and for abdominal-peri- neal resection, has not been discussed to a great extent in regard to the normal healing process expected after delivery of a normal infant to a healthy mother. Oxorn and Foote (1%8)l refer to various reasons for poor perineal healing: poor operator technique, too much or too heavy suture material used, poor tissue status in the patient, too long a labor, a traumatic delivery, etc.
REEDA, devised by Davidson in 19702 and revised by Carey in 19713 and Bolles in
1972: is being implemented by students in the Master of Science in Maternal and New- born Nursing and Nurse-Midwifery pro- gram at the University of Utah College of Nursing. Healing of a midline episiotomy (or a first or second degree perineal laceration) was the standard upon which the tool was based, since this technique of performing an episiotomy is the one generally used at the University’s Medical Center. Scoring of pa- tients with mediolateral episiotomies and extensive lacerations of the perineum should employ the same principles.
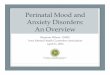
The acronym REEDA was derived from the five components of the healing process which it evaluates: the amount of redness, edema, and ecchymosis of the perineal area, discharge from the episiotomy, and approx- imation of skin edges at the site of the episi- otomy. The numerical breakdown of each of these components can be seen on the accom- panying chart.
In evaluating the postpartum mother’s perineum, the nurse investigators use dis- posable paper tapes cut to 4-cm. lengths and capable of measuring .25 cm. in precision. With the mother in a lateral Sims’ position and with an additional light source, the tape is placed perpendicular to the line of inci- sion so that its midportion centimeter mark- ing is aligned with the incision. In this man- ner, the amount of redness, edema and ecchymosis on each side of the episiotomy can be measured precisely in relation to their proximity to the incision. Areas of ecchymosis found in the perineal area, but not meeting the criteria of the tool as de- pigned, were not included in the numerical score but were noted on the recording sheet.
As indicated in the chart, a woman with no perineal redness, edema, or ecchymosis, whose episiotomy has no discharge and whose skin edges are approximated would have a score of 0. Each specific area, then, has one additional point given for progres- sive increase in severity of inflammatory signs.
Ranges of scores for evaluating postpar- tum healing have varied from 0-6 on the first
6 /Summer 1974, Vol. XZX, No. 2
REE
DA
SC
ALE
RED
NES
S PO
INTS
0 N
one
1 W
ithin
.25
cm.
of in
cisi
on
bila
tera
lly
2 W
ithin
.5 c
m.
of in
cisi
on
bila
tera
lly
3 B
eyon
d .5 cm
. of
inci
sion
bi
late
rally
SCO
RE
EDEM
A
ECC
HY
MO
SIS
DIS
CH
AR
GE
Non
e N
one
Non
e
Perin
eal,
less
W
ithin
.25 c
m.
Seru
m
than
1 cm
. fro
m
inci
sion
.5
cm. u
nila
tera
lly
Perin
eal a
nd/o
r B
etw
een
25
to
Sero
sang
uino
uc
Vul
var,
betw
een
1 cm
. bila
ter-
1
to 2
cm. f
rom
al
ly o
r bet
wee
n in
cisi
on
.5 to
2 c
m.
unila
tera
lly
bila
tera
lly o
r
Perin
eal a
nd/o
r G
reat
er th
an 1
B
lood
y, pu
rule
nt
Vul
var,
grea
ter
cm. b
ilate
rally
th
an 2
cm. f
rom
in
cisi
on
unila
tera
lly
or 2
cm.
APP
RO
XIM
ATI
ON
Clo
sed
Skin
sepa
ratio
n 3
mm
. or l
ess
Skin
and
sub
- cu
tane
ous
fat
sepa
ratio
n
Skin
, sub
- cu
tane
ous
fat
and
fasc
ia1
laye
r sep
arat
ion
postpartum day and from 0-8 on the second postpartum day, as found by three investi- gators. Fourth postpartum day scores ranged from 0-6; eighth postpartum day scores ranged from 0-7; fourteenth postpar- tum day scores ranged from 0-1, as shown by two investigators.
It was found that although women dif- fered in the amount of pigmentation of the perineum, redness that was due to inflam- mation could be distinguished from the red- ness of tissue that would normally be ex- pected in a fair-skinned woman.
Each investigator found no statistically significant difference among postpartum mothers in the rate of healing of the peri- neum as indicated by the REEDA score, or in the amount of comfort provided by using several different methods for relief of dis- comfort (sitz bath, perineal light, cold appli- cations).
Carey (1971) found that mothers who de- livered heavier babies had higher REEDA scores reflecting greater tissue trauma. Mothers indicated that at different times different comfort measures might be prefer- able. It was found that the ranges of treat- ment possibilities open to them to increase their perineal comfort were considered with interest and were evaluated for their useful- ness and acceptance by each woman.
Each investigator found that postpartum mothers were greatly interested in the evalu- ation of their perineal area and responded positively to a description of their healing. For example, a woman with an area of ecchymosis might understand better why she hurts more on one side of her perineum when the information is shared with her that, “The bruised area on the right side of your bottom is where some blood vessels have broken and bled into the skin and tis- sues under it: It is an area about the sue of the end of my little finger, and the blood in the tissue is what makes it uncomfortable. Sometimes it takes a little longer for the in- cision to heal when this happens. There are several ways we can try to help you become more comfortable while your tissues are
healing. Among those we can try are . . .” Davidson and Carey included home visits
for evaluation of postpartum healing as part of their methodology and spaced them from the seventh to the twenty-eighth day after delivery. Both found that while some pa- tients still showed elevations of REEDA scores on the seventh to fourteenth days, few stated they had any but mild discomfort, and most stated their perineal area could be rated as “comfortable.” No patient of the ten included in Davidson’s study (1970) was found to have an elevated REEDA score on the twenty-eighth day following delivery. All patients visited had questions ranging from concerns about child care to resumption of sexual intercourse. It was recommended by both Davidson and Carey that postpartum referrals to community nursing agencies be considered for all mothers.
Use of the REEDA scoring method has proved valuable with students in nursing as a method of increasing their powers of ob- servation for potential problems with post- partum patients. By breaking down the areas of perineal discomfort to their smallest component parts, and by rating these against a standard known for healing in other areas of the body, information about the healing process in the perineal region can be gained. This information can then be used to assist the postpartum patient to achieve a greater degree of comfort while her body is healing.
REFERENCES Oxorn, H. & Foote, W.R. Human labor and birth. (2nd ed.) New York; Apple- ton-Century-Croft, 1968. Davidson, N.R.S. Healing of the peri- neum. Unpublished master’s thesis, University of Utah, 1970. Carey, I.L.P. Healing of the perineum, a follow-up study. Unpublished mas- ter’s thesis, University of Utah, 1971. Bolles, N.C. Postpartum perineal com- fort. Unpublished master’s thesis, Uni- versity of Utah, 1972.
8 /Summer 1974, Vol. XIX, No. 2