Embed Size (px)
Citation preview

Redesigning care to meet nationalrecommendation of four or moreyearly clinic visits in patients withcystic fibrosis
A Berlinski,1,2 M J Chambers,1 L Willis,1 K Homa,3 G Com1,2
▸ Additional material ispublished online only. To viewplease visit the journal online(http://dx.doi.org/10.1136/bmjqs-2013-002345).
1Arkansas Cystic Fibrosis CareCenter, Arkansas Children’sHospital, Little Rock, Arkansas,USA2Pulmonology Section,Department of Pediatrics,University of Arkansas forMedical Sciences, Little Rock,Arkansas, USA3Leadership Preventive MedicineResidency Program, DartmouthHitchcock Medical Center,Lebanon, New Hampshire, USA
Correspondence toDr A Berlinski, PulmonologySection, Department ofPediatrics, University of Arkansasfor Medical Sciences,1 Children’s Way, Slot 512-17,Little Rock, AR 72202, USA;[email protected]
Received 22 July 2013Revised 11 September 2013Accepted 4 December 2013
To cite: Berlinski A,Chambers MJ, Willis L, et al.BMJ Qual Saf 2014;23:i42–i49.
ABSTRACTCystic fibrosis (CF) is a chronic disease requiringpatients to have frequent specialty healthcarevisits to delay progression of lung disease,prevent and treat failure to thrive and initiateearly interventions to prevent acute illness andcomplications. The CF Foundation recommendsthat patients have visits with the CF care team atleast every 3 months. During participation in theCF Foundation Learning and LeadershipCollaborative IV, the CF team at ArkansasChildren’s Hospital initiated quality improvementwork with the aim to increase the percentage ofpatients attending clinic four or more times ayear from 35% in 2004 and 56% in 2005 (CFFoundation Registry data) to 90% or greater. Weredesigned our scheduling system, rescheduledmissed patient appointments in a timely fashionand created a process to monitor attendance.This quality improvement work led to a sustainedincrease in the percentage of patients attendingclinic visits four or more times a year reachingour goal of 90% in 2012. Improvements werealso noted in the number of patients with bodymass index/weight-for-length centile of 25 orgreater, which could be related to more frequentclinic attendance.
INTRODUCTIONCystic fibrosis (CF) is a complex life-threatening genetic disease affectingapproximately 30 000 children andadults in the USA.1 The genetic defectresults in abnormal production/functionof the Cystic Fibrosis TransmembraneRegulator protein. This leads to multior-gan disease involvement affecting thelungs, sinuses, intestinal absorption, liver,pancreas and others. Lung disease isresponsible for most of the mortality inthis patient population.2
CF care centres that monitor patientsmore frequently and are more adherent tonationally recommended treatment guide-lines exhibit higher lung function andbetter patient outcomes.3 Having patientscome to clinic also allowed healthcarepractitioners to obtain more respiratorycultures and perform pulmonary functiontesting. Although not reported by theseauthors, several others have demonstrateda direct correlation between good nutri-tional status, better lung function andoverall outcomes.4–6 This rationale sup-ports the importance of nutrition improv-ing lung health that translates to increasedlongevity. CF care centres that have amore aggressive approach to nutritionhave reported better patient outcomes.7
Periodic evaluation of patients with CFallows for early detection and promptintervention for several health problems.The latter includes failure to thrive, acqui-sition of new organisms (ie, Pseudomonasaeruginosa) in their sputum, decline inlung function, CF-related liver disease,CF-related diabetes and others. Thisconcept has also been shown for otherchronic diseases such as diabetes.8 The CFFoundation (CFF) guidelines recommendthat patients over the age of 1 attendroutine clinic appointments every3 months and more frequently if needed.9
The Arkansas Children’s Hospital(ACH) CF Care Center is the only paedi-atric CF care centre accredited by the CFFin the state of Arkansas, with approxi-mately 160 patients seeking care at thecentre. The ACH CF care team respondedto a request for applications from the CFFto participate in a quality improvement(QI) collaborative, CFF Learning andLeadership Collaborative IV (LLCIV), in
SUPPLEMENT
i42 Berlinski A, et al. BMJ Qual Saf 2014;23:i42–i49. doi:10.1136/bmjqs-2013-002345
group.bmj.com on June 3, 2016 - Published by http://qualitysafety.bmj.com/Downloaded from

2005. This collaborative was designed to accelerate therate of improvement in CF care by training teams fromcentres in methods of QI.10 In January 2006, ACH CFCare Center leadership team members participated inLLCIV. Part of our work at the LLCIV was to examineour centre-level reports from the CFF Registry anddetermine where we wanted to focus our improvementwork. Regular clinic attendance has been directly cor-related with better patient outcomes. The percentageof patients attending clinic four or more times per yearat our centre was at 35 in 2004 and 56 in 2005.Therefore, we thought an area for improvement wasmeeting the guideline of patients having four or moreclinic visits per year. We developed Project 4 or Morewith the aim of increasing the percentage of patientsattending clinic four or more times a year to 90% orgreater. Having patients attend clinic four or moretimes per year was viewed as an opportunity toimprove patient care. A nutritional pathway was alsoestablished later to consistently provide nutritionalsupport to those patients who needed it.
METHODSOur QI work involved intensive training and coachingdone under the auspices of the LLCIV during an18-month period. A mentor/coach provided trainingand tools in QI methodology included in the CFAction Guide.11 A local QI team consisting of the CFCenter Director, CF Nurse Coordinator, socialworker, respiratory therapist, nursing clinic director,statistician and parent representative participated inbimonthly conference calls with the coach and peri-odic webinars. In addition, a subgroup attended two2-day off-site collaborative meetings. We completed
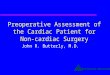
assigned tasks including clinical microsystems analysisand established an internal dissemination strategy.Lessons learned from QI assignments were discussedin monthly CF Leadership Team meetings, whichincluded hospital administration. Additionally, teammembers were provided access to informationthrough postings in a shared computer drive and onan internal display.We developed a fishbone diagram (figure 1) to
document factors that were linked to patients attend-ing clinic less than four times a year. These factorswere External, Internal, Communication and Patient/Family Perceptions, which were obtained from severalsources. The medical charts of patients who attendedclinic less than four times in 2005 were reviewed todetermine common patterns of non-attendance inregards to age, gender, distance from centre, season,CF physician or insurance carrier. To obtain patients’and family members’ perspective, they were asked toparticipate in a survey to identify issues relative toclinic attendance. Additionally, CF team members par-ticipated in brainstorming sessions to further identifyother factors.Another area of assessment was to understand how
our scheduling system influenced patients having lessthan four visits per year. Process evaluation includedhow appointments were made, reminder letters/phonecalls, a clinic time cycle analysis and number of CFappointment slots (see figure 2). In 2006, the transi-tion to a centralised appointment scheduling centrewas announced at our hospital, which providedfurther impetus to refine the internal process. Patientswith CF were traditionally assigned to an individualpaediatric pulmonologist who saw them during their
Figure 1 Fishbone diagram outlining barriers to clinic attendance at Arkansas Children’s Hospital Cystic Fibrosis Care Center.
Supplement
Berlinski A, et al. BMJ Qual Saf 2014;23:i42–i49. doi:10.1136/bmjqs-2013-002345 i43
group.bmj.com on June 3, 2016 - Published by http://qualitysafety.bmj.com/Downloaded from

scheduled clinic days along with other pulmonarypatients. There was no plan to ensure appointmenttimes were available in the schedule for the four ormore visits, so specific CF appointment slots weredeveloped. There was also no standard process toreschedule patients who missed their appointments.Increasing patients’ attendance to clinic four or
more times/year was viewed as an opportunity tointervene with other QI work. Therefore, parallel tothis improvement work focused on clinic attendance,a nutritional pathway was implemented during thelast quarter of 2006 by some members of the CF teamsince good nutritional status has been associated withimproved lung health.4–6 12 All patients were screenedat each clinic visit and categorised in nutritional riskzones according to either their body mass index(BMI) centile for those 2 years old or older or theirweight-for-length (W-L) centile for those youngerthan 2 years old (acceptable >25th, nutrition risk 10–25th and urgent nutrition risk <10th). Calculationswere done using the BMI centile calculator supportedby the Centers for Disease Control and Prevention(http://apps.nccd.cdc.gov/dnpabmi/) andweight-for-length calculator (http://www.uptodate.com/contents/calculator-cdc-nchs-infant-weight-for-length-percentiles-less-than36-months). Enzyme dosingwas calculated at every nutritional encounter tomonitor for underdosing or overdosing. Individualisednutrition plan and consultation were available uponphysician’s request. A standardised consultation formthat included assessment for need for oral glucose tol-erance test, bone densitometry and vitamin replace-ment was developed. The use of appetite stimulantsand timing for gastrostomy tube placement were notincluded in the pathway and were left to individualphysicians. Oral supplements were recommended forall patients with a BMI/W-L centile less than 25th, andreturn clinic visits were scheduled within 4–6 weeks.Education was provided to patients and familiesregarding the importance of nutrition and their crucialrole in monitoring and improving outcomes. This
included more frequent clinic visits for weight checks,completing diet and stool records and ensuring intakeof supplements and high-calorie, high-fat foods.Nutrition risk categories were revised in 2008 in con-currence with CFF goals for BMI/W-L >50thcentile.12 The use of the pathway became standardisedto include nutritional consult with a dietician for allpatients <50th BMI/W-L centile. The nutrition educa-tion booklet was revised to include the new nutritioncategories and updated information regarding gastros-tomy placement.
Measuring the impact of the interventionsThe CFF Registry has a composite quality measurethat reports the percentage of patients that had fouror more visits per year, sputum culture and lung func-tion testing. This composite measure reports only onenrolled patients and does not account for patientspresent less than four quarters. Therefore, we devel-oped our own measure of clinical attendance, whichwas the number of patients seen per quarter (fourvisits per year) divided by the number of patients fol-lowed at the centre during the year. Patients newlydiagnosed or who transferred care and were not atACH all four quarters were excluded. Additionally,hospitalisations were not included as a clinic visit.Statistical process control (SPC) charts were used to
evaluate our QI work. SPC charts have the ability todistinguish between common cause and special causevariation. A measure in a stable system will vary overtime, and the variation is just common cause orrandom variation. When something new enters thesystem, then the result will be a special cause vari-ation. To determine whether clinic attendancechanged significantly, we compared the annual ratefrom 2006 to 2012 using analysis of means(ANOM).13 ANOM for percent data contains thesame formulas as the p-chart; however, there were notenough data points to evaluate the yearly data using ap-chart. The ANOM compared the annual ratesagainst the overall rate and if the yearly rate of clinical
Figure 2 Flowchart of the clinic process at Arkansas Children’s Hospital Cystic Fibrosis Care Center. Review of the clinic processuncovered that there was no standardised procedure to reschedule patients that did not keep their appointments.
Supplement
i44 Berlinski A, et al. BMJ Qual Saf 2014;23:i42–i49. doi:10.1136/bmjqs-2013-002345
group.bmj.com on June 3, 2016 - Published by http://qualitysafety.bmj.com/Downloaded from

attendance crossed either the upper or lower controllimit then it was considered special cause in whichsomething different entered the system that created astatistical significant result. Control limits were set at2 σ (approximately to 2 SDs), which was at the 5%risk level; however, traditionally limits are set at 1%risk, but we wanted to be sure to identify a significantresult and thus we accepted a higher risk of type 1error.We also used an ANOM to determine whether
there was an improvement in the annual percentage ofpatients with BMI/W-L <50th centile that had aconsult with a dietician.To determine whether the patients’ nutritional
status improved over time, we used a SPC X chart.14
Nutritional status measure was percentage of patientswith a greater than 25th centile BMI/W-L per quarterand was based on the highest centile BMI/W-Lrecorded during that period. The special cause vari-ation rule that would represent a sustained improve-ment in patients’ BMI/W-L centile would be eight ormore consecutive points above the central line. TheX chart displays quarterly measure of BMI/W-Lcentile over time, a centre line (the average ofBMI/W-L centile measures) and upper and lowercontrol limits that are similar to 3 SDs above andbelow the average.The QI work was submitted to the University of
Arkansas for Medical Sciences Institutional ReviewBoard and was classified as exempt.
RESULTSAs a result of the initial assessment work from ourparticipation in the LLCIV, communication andpatient/family perception barriers were identified asimportant areas for improvement. To address patient
and family involvement and improve communication,a family advisory board (FAB) was established in thespring of 2006 and family members participated inthis QI work.15 The FAB’s first newsletter describedthe importance of attending clinic appointments on aquarterly basis. Also, families started to receive awritten summary of their clinic visit in the form of aCF Action Plan.16
The Appointment Center became operational inMay 2007. They received 6-month rolling physicianclinic calendars to allow creation of appointmentslots. To address the scheduling barriers, an adequatenumber of appointment slots were created for eachphysician according to the number of CF patientsunder their care to ensure quarterly visits could bescheduled. Patients were assigned their follow-upappointment based on the information provided bythe physician in a return appointment form completedat the end of the clinic visit. The system assignedappointments based on the physician’s slot availabilityand did not provide families the option to choose aspecific date and time. A decision tree outlining howto reschedule patients with CF was developed, andthe appointment reminder system was revised (seefigure 3). We established primary and secondary pro-cesses to reschedule patients who missed appoint-ments. The CF office assistant received a dailyautomated email of appointment status from the pre-vious day’s clinic. The assistant then would send thelist of patients who needed to be rescheduled to theAppointment Center to reschedule them within2–3 weeks per the decision tree. If the patient couldnot be rescheduled within this timeframe, theAppointment Center would contact the nurse for thatpatient’s doctor to assist in finding a new slot or over-book the clinic. Additionally, the CF Coordinator ran
Figure 3 Centralised Appointment Center’s Cystic Fibrosis (CF) rescheduling decision tree at Arkansas Children’s Hospital CF CareCenter.
Supplement
Berlinski A, et al. BMJ Qual Saf 2014;23:i42–i49. doi:10.1136/bmjqs-2013-002345 i45
group.bmj.com on June 3, 2016 - Published by http://qualitysafety.bmj.com/Downloaded from

a monthly query from the CFF Registry (Port CF)about patients who were due a visit. After removingpatients who were just seen or about to be seen, thefinalised list was sent to the doctors and their nursesto contact and overbook patients immediately. Toaddress the limitations of the existing monitoringsystems, an internal database was created. The CFSocial Worker tracked patient quarterly attendanceand sent the list of patients not seen during thequarter to their doctors and nurses so that thesepatients would be rescheduled (see figure 4).The online supplementary appendix 1 reports the
timeline of different activities related to this improve-ment work from February 2006 to the end of the yearin 2012.
Outcomes of the interventionsBetween 2006 and 2012, 81% of our patients had fouror more visits per year. The ANOM chart (figure 5) ofannual rates of patients having four or more visitsshows the first year of 2006 of 72% was significantlylower than the succeeding years. From 2007 through2011, the improvement was sustained and, in 2012,90% of the patients had four or more visits, whichwas our goal and was significantly better than theoverall rate. Figure 6 is another ANOM of annualrates of patients with BMI/W-L less than the 50thcentile seen by a dietician. In 2005, it was 68%,which was significantly lower than the succeedingyears and significantly improved to 100% in 2009.
Figure 7 shows the X chart of percentage of patientshaving a greater than 25th centile BMI/W-L. In 2007,80% of the patients had a BMI/W-L greater than25th centile and in the third quarter of 2008 thisincreased to 82%.
DISCUSSIONAfter implementation of QI interventions, the per-centage of patients attending four or more clinic visitssignificantly improved, and in 2012 we met our goalof 90% of patients attending four or more times ayear. A systematic approach to scheduling processes,timely rescheduling of patients who missed appoint-ments and monitoring of attendance resulted in a sig-nificant increase in the number of patients who metthe CFF national recommendation of four or morevisits per year. This improvement was sustained over a7-year period and is the standard of practice at ourcentre. One of the factors that we believe helpedmake the QI work successful was the internal moni-toring and tracking of patients’ clinic attendance,which is still continued in our clinic. Since the CFFRegistry reports did not factor out patients who werenot followed a full year (ie, diagnosed late in the yearor who transferred care) and could not have attendedfour appointments, developing an internal outcome-specific database proved instrumental in achieving ourgoals. Additionally, other QI works led to an increasein the number of patients with 25th centile BMI/W-Lor greater as well as the number of patients with BMI/W-L <50th seen by a dietitcan.12
Figure 4 Standardised process to follow-up cystic fibrosis (CF) patients who ‘do not keep appointments’ (DNKA) to ensure four ormore clinic visits per year at Arkansas Children’s Hospital CF Care Center.
Supplement
i46 Berlinski A, et al. BMJ Qual Saf 2014;23:i42–i49. doi:10.1136/bmjqs-2013-002345
group.bmj.com on June 3, 2016 - Published by http://qualitysafety.bmj.com/Downloaded from

Although there was a sustained improvement in thepercentage of patients attending CF clinic four ormore times per year, a marked improvement wasnoted in 2012. We speculate that the inclusion of thenurses in the notification of those patients that neededto be rescheduled was responsible for such an incre-ment (see online supplementary appendix 1).We viewed the increase in clinic attendance as an
opportunity to monitor our patients more closely andto be able to implement other QI work. The nutri-tional pathway was one of the QI projects that werestarted.The percentage of patients with BMI/W-L <50th
seen by a dietician improved tremendously in 2009after the nutritional consult changed from ‘at physi-cians discretion’ to mandatory. We speculate that
nurses and nutritionists felt empowered to complywith this new requirement.Although the increase in the percentage of patients
with greater than 25th centile for BMI/W-L from 80%to 82% might seem small, it represents a positive impacton a few more patients and provides more opportunitiesfor improvement. We speculate that the increase inclinic attendance allowed for better implementation ofthe nutritional pathway and synergistically impacted theimprovement gains in BMI/W-L. Our data are in agree-ment with Johnson et al,3 who reported that frequentmonitoring among other interventions made possibledue to patients being seen more in clinic was associatedwith improved outcomes in CF.Our successful experience in developing internal
processes to improve the percentage of patients being
Figure 5 An analysis of means chart of percentage of patients per year attending cystic fibrosis clinic four times or more (2006–2012). Baseline line is the overall mean, each bar represents the individual data point and dashed lines are the upper and lowercontrol lines set at 2 σ. Any value outside these lines is considered statistically different.
Figure 6 An analysis of means chart of percentage of patients with body mass index /weight-for-length <50th centile seen bydietician (2005–2011). Baseline line is the overall mean, each bar represents the individual data point and dashed lines are the upperand lower control lines set at 2 σ. Any value outside these lines is considered statistically different. Data extracted from Cystic FibrosisFoundation Registry. 2008 data were not collected due to local Institutional Review Board determination.
Supplement
Berlinski A, et al. BMJ Qual Saf 2014;23:i42–i49. doi:10.1136/bmjqs-2013-002345 i47
group.bmj.com on June 3, 2016 - Published by http://qualitysafety.bmj.com/Downloaded from

seen in the clinic four or more times a year can beadopted in other outpatient settings that require a spe-cific number of scheduled visits/procedures over aperiod of time. Replication of these processes couldbe hindered by lack of personnel, lack of buy-in bythe hospital administration and lack of patient/familyinvolvement. A major challenge was maintaining con-sistency of the processes despite frequent personnelchanges. Glitches in the current appointmentreminder system sometimes result in late/missedletters and phone calls. Although we improved sched-uling processes to ensure patients had appointments,there were still external barriers to attendance. Thosebarriers included rising fuel costs, transportation lim-itations, child care issues, missed workdays by care-givers and average low-income population.Although changing processes of care can be met
with resistance, our behaviours evolved by showingthe value and the positive results that our processredesign brought. The overall acceptability of theneed for QI crosses all disciplines. Hospitals havebegun to strengthen their QI departments and areincorporating it in all areas of practice. Physicians arerequired to participate in QI work to obtainre-certification in their respective field. This improve-ment work was sustainable over time because ofseveral factors such as Section Chief support, CFcentre leadership commitment and the internalisationof the need for patients to be seen four or moretimes.Many lessons were learned through our experience.
We noticed our clinic attendance started to improvebefore the processes were fully implemented. Wespeculate this was due to the heightened awareness ofour efforts by patients, families and our CF team. Welearned that families are eager to have input and be
involved in our centre processes. We found that thisimprovement work strengthened the interdisciplinaryteamwork at our centre. We learned that QI workimproves patient outcomes but requires institutionalsupport, dedication and perseverance. Although theimprovement work is labour intensive in a busy clin-ical setting, improved outcomes result in team motiv-ation and pride of accomplishment.An area of future improvement that is currently
being evaluated is the patient’s ability to scheduletheir return appointment before leaving clinic.Another possible improvement could be having a12-month rolling physician clinic calendar to allowscheduling of all four appointments at one time.Additionally, availability of online scheduling wouldmake the process more family centred. The creationof a hospital-wide electronic reminder system (textmessage/email) could potentially decrease non-attendance. This will require the availability of currentand valid demographic information.Lastly, participation in the LLCIV resulted in a posi-
tive culture change at the ACH CF Care Centerregarding the use of QI methods to improve patientcare. Our work was recognised by the CFF with the2010 Annual CFF Quality Care Award.
CONCLUSIONSImprovement work that focused on developing a sys-tematic approach to scheduling and reschedulingresulted in a sustained improvement in the number ofpatients attending our CF clinic four or more timesper year. In addition, the increased attendance facili-tated the implementation of other QI work andimprovement of an important patient nutritionaloutcome in CF care.
Figure 7 A statistical process control chart of nutrition assessment per quarter at Arkansas Children’s Hospital Cystic Fibrosis CareCenter (2007–2012). Control limits set at 3 σ.
Supplement
i48 Berlinski A, et al. BMJ Qual Saf 2014;23:i42–i49. doi:10.1136/bmjqs-2013-002345
group.bmj.com on June 3, 2016 - Published by http://qualitysafety.bmj.com/Downloaded from

Acknowledgements We are indebted to the families andpatients with CF and to the CF care team at ArkansasChildren’s Hospital.
Contributors AB was responsible for the conception and design,analysis and interpretation of data and critical revision and finalapproval of the version to be published. MJC was responsiblefor the conception and design, drafting the article, criticalrevision and final approval of the version to be published. LWand GC were responsible for the conception and design, criticalrevision and final approval of the version to be published. KHwas responsible for the analysis and interpretation of data andcritical revision and final approval of the version to bepublished.
Competing interests None.
Ethics approval University of Arkansas for Medical SciencesIRB.
Provenance and peer review Not commissioned; externallypeer reviewed.
REFERENCES1 O’Sullivan BP, Freedman SD. Cystic fibrosis. Lancet
2009;373:1891–904.2 Cystic Fibrosis Foundation Patient Registry. Annual data report
to the center directors. Bethesda, MD: Cystic FibrosisFoundation, 2010.
3 Johnson C, Butler SM, Konstan MW, et al. Factors influencingoutcomes in cystic fibrosis: a center-based analysis. Chest2003;123:20–7.
4 Konstan MW, Butler SM, Wohl ME, et al. Growth andnutritional indexes in early life predict pulmonary function incystic fibrosis. J Pediatr 2003;142:624–30.
5 Steinkamp G, Wiedemann B. Relationship between nutritionalstatus and lung function in cystic fibrosis: cross sectional andlongitudinal analyses from the German CF quality assurance(CFQA) project. Thorax 2002;57:596–601.
6 McPhail GL, Acton JD, Fenchel MC, et al. Improvements inlung function outcomes in children with cystic fibrosis areassociated with better nutrition, fewer chronic pseudomonasaeruginosa infections, and dornase alfa use. J Pediatr2008;153:752–7.
7 Matel JL, Milla CE. Nutrition in cystic fibrosis. Semin RespirCrit Care Med 2009;30:579–86.
8 Morrison F, Shubina M, Turchin A. Encounter frequency andserum glucose level, blood pressure, and cholesterol levelcontrol in patients with diabetes mellitus. Arch Int Med2011;171:1542–50.
9 Cystic Fibrosis Foundation Concepts in Care ConsensusConference. Preventative and Maintenance Care for the Patientwith Cystic Fibrosis Vol 1, Section 2, page 6.
10 Marshall BC, Penland CM, Hazle L, et al. Cystic fibrosisfoundation: achieving the mission. Respir Care 2009;54:788–95.
11 Cystic Fibrosis Foundation. Action Guide for AcceleratingImprovement in Cystic Fibrosis Care. 2006. http://www.clinicalmicrosystem.org/assets/materials/workbooks/cystic_fibrosis_action_guide.pdf
12 Harden H, Com G. Maintaining the gains: ongoing assessmentof quality improvement outcomes in nutrition status of CFpatients [abstract]. Pediatr Pulmonol 2010;45(S33):405.
13 Homa K. Analysis of means used to compare providers’referral patterns. Q Manage Health Care 2007;16:256–64.
14 Amin SG. Control charts 101: a guide to healthcareapplications. Q Manage Health Care 2001;9:1–27.
15 Chambers MJ, Willis L, Vaught F, et al. Improving patient andfamily involvement in the CF care center at Arkansas children’shospital through development of a family advisory board[abstract]. Pediatr Pulmonol 2006;41(S29):367.
16 Willis LM. Cystic fibrosis action plan: caregivers and healthcareteam [abstract]. Pediatr Pulmonol 2010;45(S33):403.
Supplement
Berlinski A, et al. BMJ Qual Saf 2014;23:i42–i49. doi:10.1136/bmjqs-2013-002345 i49
group.bmj.com on June 3, 2016 - Published by http://qualitysafety.bmj.com/Downloaded from

visits in patients with cystic fibrosisrecommendation of four or more yearly clinic Redesigning care to meet national
A Berlinski, M J Chambers, L Willis, K Homa and G Com
doi: 10.1136/bmjqs-2013-0023452014 23: i42-i49 BMJ Qual Saf
http://qualitysafety.bmj.com/content/23/Suppl_1/i42Updated information and services can be found at:
These include:
MaterialSupplementary
2345.DC1.htmlhttp://qualitysafety.bmj.com/content/suppl/2014/03/07/bmjqs-2013-00Supplementary material can be found at:
References #BIBLhttp://qualitysafety.bmj.com/content/23/Suppl_1/i42
This article cites 13 articles, 2 of which you can access for free at:
serviceEmail alerting
box at the top right corner of the online article. Receive free email alerts when new articles cite this article. Sign up in the
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on June 3, 2016 - Published by http://qualitysafety.bmj.com/Downloaded from