Embed Size (px)
Citation preview

9=>?!.-0.*@,A12370,--GC.GGB!,--GE.,@E.,*,C.,TDE!$)484%'::#!1(":47J23!$%:4%2!W21!,F+!,--GE!!"#$%&'$()
U23464%2!'%3!5J2!W2654$%!$%!=5$:')#%8$:$8#!I2'3!'%3!X26]!W()82)#!Z::2%!90!L(a!I'):$)+!&)+!HJ'):27!L$/2)+!H$<<45522!$%!S)'65462!'%3!Z<"(:'5$)#
M"&')#)9(6$,""'%'/?"),%'/(N11"110"'#(%'(+'<)'#1()'*(CH%9*,"'7(B"$&00"'*)#%&'1(O">&'*
J551?AA///01234'5)4670$)8A684A6$%52%5A;(::A.,@A@A.,*,:$6'523!$%!5J2!O$):3!O432!O2"!'5?!
NJ2!$%:4%2!V2)74$%!$;!5J47!')546:2+!':$%8!/45J!(13'523!4%;$)<'54$%!'%3!72)V4627+!47
)48J57!)272)V230!S)4%5!>WWX?!--D.C@--*0!=%:4%2!>WWX?!.-GFC@,B*0!_)$V2![4::'82+!>::4%$47+!T---B0!H$1#)48J5!\!,--G!"#!5J2!Z<2)46'%!Z6'32<#!$;!S234'5)4670!Z::!'%3!5)'32<')]23!"#!5J2!Z<2)46'%!Z6'32<#!$;!S234'5)467+!.@.!X$)5J/275!S$4%5!L$(:2V')3+!^:]1(":46'54$%+!45!J'7!"22%!1(":47J23!6$%54%($(7:#!74%62!.G@F0!S^9>ZN`>HW!47!$/%23+!1(":47J23+!S^9>ZN`>HW!47!5J2!$;;464':!Y$()%':!$;!5J2!Z<2)46'%!Z6'32<#!$;!S234'5)4670!Z!<$%5J:#
!"#!$%!=65$"2)!,@+!,--G!///01234'5)4670$)89$/%:$'323!;)$<!
2++WSjjW%;3"+.36,_""WA#$36"+3'*,_'.9

Clinical Report—Hearing Assessment in Infants andChildren: Recommendations Beyond NeonatalScreening
abstractCongenital or acquired hearing loss in infants and children has beenlinked with lifelong deficits in speech and language acquisition, pooracademic performance, personal-social maladjustments, and emo-tional difficulties. Identification of hearing loss through neonatal hear-ing screening, regular surveillance of developmental milestones, audi-tory skills, parental concerns, and middle-ear status and objectivehearing screening of all infants and children at critical developmentalstages can prevent or reduce many of these adverse consequences.This report promotes a proactive, consistent, and explicit process forthe early identification of children with hearing loss in the medicalhome. An algorithm of the recommended approach has been devel-oped to assist in the detection and documentation of, and interventionfor, hearing loss. Pediatrics 2009;124:1252–1263
KEY POINTS
1. Every child with 1 or more risk factors on the hearing risk assess-ment should have ongoing developmentally appropriate hearingscreening and at least 1 diagnostic audiology assessment by 24 to30 months of age.
2. Periodic objective hearing screening of all children should be per-formed according to the recommendations for preventive periodichealth care.1
3. Any parental concern about hearing loss should be taken seriouslyand requires objective hearing screening of the patient.
4. All providers of pediatric health care should be proficient with pneu-matic otoscopy and tympanometry. However, it is important to re-member that these methods do not assess hearing.
5. Developmental abnormalities, level of functioning, and behavioralproblems (ie, autism/developmental delay) may preclude accurateresults on routine audiometric screening and testing. In this situa-tion, referral to an otorhinolaryngologist and a pediatric audiologistwho has the necessary equipment and expertise to test infants andyoung children should be made.
6. The results of abnormal screening should be explained carefully toparents, and the child’s medical record should be flagged to facili-tate tracking and follow-up.
Allen D. “Buz” Harlor, Jr, MD, Charles Bower, MD, THECOMMITTEE ON PRACTICE AND AMBULATORY MEDICINE,THE SECTION ON OTOLARYNGOLOGY–HEAD AND NECKSURGERY
KEY WORDhearing screening, hearing loss, audiology
ABBREVIATIONSAAP—American Academy of PediatricsOAE—otoacoustic emissionABR—auditory brainstem responseVRA—visual reinforced audiometry
The guidance in this report does not indicate an exclusivecourse of treatment or serve as a standard of medical care.Variations, taking into account, individual circumstances may beappropriate.
This document is copyrighted and is property of the AmericanAcademy of Pediatrics and its Board of Directors. All authorshave filed conflict-of-interest statements with the AmericanAcademy of Pediatrics. Any conflicts have been resolved througha process approved by the Board of Directors. The AmericanAcademy of Pediatrics has neither solicited nor accepted anycommercial involvement in the development of the content ofthis publication.
www.pediatrics.org/cgi/doi/10.1542/peds.2009-1997
doi:10.1542/peds.2009-1997
All clinical reports from the American Academy of Pediatricsautomatically expire 5 years after publication unless reaffirmed,revised, or retired at or before that time.
PEDIATRICS (ISSN Numbers: Print, 0031-4005; Online, 1098-4275).
Copyright © 2009 by the American Academy of Pediatrics
Guidance for the Clinician inRendering Pediatric Care
1252 FROM THE AMERICAN ACADEMY OF PEDIATRICS!"#!$%!=65$"2)!,@+!,--G!///01234'5)4670$)89$/%:$'323!;)$<!2++WSjjW%;3"+.36,_""WA#$36"+3'*,_'.9

7. Any abnormal objective screeningresult requires audiology referraland definitive testing.
8. A failed infant hearing screening ora failed screening in an older childshould always be confirmed by fur-ther testing.
9. Abnormal hearing test results re-quire intervention and clinicallyappropriate referral, including oto-laryngology, audiology, speech-language pathology, genetics, andearly intervention.
INTRODUCTION
Failure to detect congenital or ac-quired hearing loss in childrenmay re-sult in lifelong deficits in speech andlanguage acquisition, poor academicperformance, personal-social malad-justments, and emotional difficulties.Early identification of hearing loss andappropriate intervention within thefirst 6 months of life have been demon-strated to ameliorate many of theseadverse consequences and facilitatelanguage acquisition.2 Supportive evi-dence is outlined in the Joint Commit-tee on Infant Hearing’s “Year 2007Position Statement: Principles andGuidelines for Early Hearing Detectionand Intervention Programs,” whichwas endorsed by the American Acad-emy of Pediatrics (AAP).3 This evidencealso is part of the rationale for the AAPstatement “Newborn and Infant Hear-ing Loss: Detection and Intervention,”4
which endorses universal hearingscreening and reviews the primary ob-jectives, important components, andrecommended screeningmethods andparameters that characterize an ef-fective universal hearing screeningprogram. Furthermore, the AAPstatement “Recommendations forPreventive Pediatric Health Care”1
promotes objective newborn hearingscreening as well as periodic hear-ing screening for every child throughadolescence (Table 1).
All providers of pediatric health careneed to recognize children who are atrisk of or who suffer from congenital oracquired hearing loss, be prepared toscreen their hearing, and assist the fam-ily and arrange for proper referral andtreatment by identifying available hear-ing resources within their communities.In addition, thepediatric health carepro-fessional can play an important role incommunication with the child’s school-teacher and/or nurse and special educa-tionprofessionals to facilitate proper ac-commodation and education once ahearing deficit has been confirmed.
This clinical report replaces the previ-ous 2003 clinical report and seeks topromote a proactive, consistent, and
explicit process for the early identifi-cation of children with hearing loss inthe medical home. To assist in the de-tection and documentation of and in-tervention for hearing loss, an algo-rithm of the recommended approachwith key points has been developed(Fig 1), as have several tables.
RISK INDICATORS FOR HEARINGLOSS
Some degree of hearing loss (Table 2)is present in 1 to 6 per 1000 newborninfants.5 Most children with congenitalhearing loss are potentially identifi-able by newborn and infant hearingscreening. However, some congenitalhearing loss may not become evidentuntil later in childhood. Hearing lossalso can be acquired during infancy orchildhood for various reasons. Infec-tious diseases, especially meningitis,are a leading cause of acquired hear-ing loss. Trauma to the nervous sys-tem, damaging noise levels, and oto-toxic drugs can all place a child at riskof developing acquired hearing loss.6,7
Otitis media is a common cause of usu-ally reversible hearing loss. Certainphysical findings, historical events,and developmental conditions may in-dicate a potential hearing problem.These conditions include, but are notlimited to, anomalies of the ear andother craniofacial structures, signifi-cant perinatal events, and global devel-opmental or speech-language delays.All older infants and children should bescreened for risk factors involving hear-ing problems. A summary of high-risk in-dicators for hearing loss and develop-mental milestones are included inTables 3 and 4, respectively. All infantswith a risk indicator for hearing loss, re-gardless of surveillance findings, shouldbe referred for an audiologic assess-ment at least once by 24 to 30 months ofage, even if thechildpassed thenewbornhearing screening. Children with risk in-dicators that are highly associated withdelayed-onset hearing loss, such as hav-
TABLE 1 Recommendations for PreventivePediatric Health Care1
Stage Age SensoryScreening:6. Hearing
Infancy PrenatalNewborn a
3–5 d1 b
By 1 mo b
2 mo b
4 mo b
6 mo b
9 mo b
Early childhood 12 mo b
15 mo b
18 mo b
24 mo b
30 mo b
3 y b
4 y a
Middle childhood 5 y a
6 y a
7 y b
8 y a
9 y b
10 y a
Adolescence 11 y b
12 y b
13 y b
14 y b
15 y b
16 y b
17 y b
18 y b
19 y b
20 y b
21 y b
a To be performed.b Risk assessment, with appropriate action to follow ifpositive.
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 124, Number 4, October 2009 1253!"#!$%!=65$"2)!,@+!,--G!///01234'5)4670$)89$/%:$'323!;)$<!2++WSjjW%;3"+.36,_""WA#$36"+3'*,_'.9

ing received extracorporeal membraneoxygenation or having cytomegalovirusinfection, should havemore frequent au-diological assessments. Key point 1: Ev-ery child with 1 or more risk factors onthe hearing risk assessment shouldhave ongoing developmentally appropri-ate hearing screening and at least 1 di-agnostic audiology assessment by 24 to30 months of age (Table 1).
Although questionnaires and check-lists are useful for identifying a child atrisk of hearing loss, studies have
shown that only 50% of children withhearing loss are identified by the com-prehensive use of such question-naires.8,9 Key point 2: Periodic objectivehearing screening of all childrenshould be performed according to therecommendations for preventive peri-odic health care1 (Table 1).
If a parent or caregiver is concernedthat a child might have hearing loss,the pediatrician needs to assume thatsuch is true until the child’s hearinghas been evaluated objectively. Paren-
tal concern is of greater predictivevalue than the informal behavioral ex-amination performed in the physi-cian’s office.10 Parents often reportsuspicion of hearing loss, inattention,or erratic response to sound beforehearing loss is confirmed.11 One studyshowed that parents were as much as12 months ahead of physicians in iden-tifying their child’s hearing loss.3 Keypoint 3: Any parental concern abouthearing loss should be taken seriouslyand requires objective hearing screen-ing of the patient.
PHYSICAL EXAMINATION
Thorough physical examination is anessential part of evaluating a child forhearing loss. Findings on head andneck examination associated with po-tential hearing loss include hetero-chromia of the irises, malformation ofthe auricle or ear canal, dimpling orskin tags around the auricle, cleft lipor palate, asymmetry or hypoplasia ofthe facial structures, and microcepha-ly.12 Hypertelorism and abnormal pig-
FIGURE 1Hearing-assessment algorithm within an office visit. CMV indicates cytomegalovirus; ENT, ear, nose, and throat.
TABLE 2 Definitions of Hearing Loss
HearingLoss
Definition
Mild On average, the most quiet sounds that people can hear with their better ear arebetween 20 and 40 dB. People who suffer from mild hearing loss have somedifficulties keeping up with conversations, especially in noisy surroundings.
Moderate On average, the most quiet sounds heard by people with their better ear arebetween 40 and 70 dB. People who suffer from moderate hearing loss havedifficulty keeping up with conversations when not using a hearing aid.
Severe On average, the most quiet sounds heard by people with their better ear arebetween 70 and 95 dB. People who suffer from severe hearing loss will benefitfrom powerful hearing aids, but often they rely heavily on lip reading, evenwhen they are using hearing aids. Some also use sign language.
Adapted from: European Group on Genetics of Hearing Impairment. Martini A, ed. European Commission Directorate,Biomedical and Health Research Programme (HEAR) Infoletter 2, November 1996;8.
1254 FROM THE AMERICAN ACADEMY OF PEDIATRICS!"#!$%!=65$"2)!,@+!,--G!///01234'5)4670$)89$/%:$'323!;)$<!
2++WSjjW%;3"+.36,_""WA#$36"+3'*,_'.9

mentation of the skin, hair, or eyesalso may be associated with hearingloss, as in Waardenburg syndrome.The presence of renal abnormalities(Alport syndrome), cardiac anomalies(prolonged QT interval in Jervell andLange-Nielsen syndrome), and othersyndromes should also prompt evalu-ation of hearing. Abnormalities of theeardrum should alert the physician tothe possibility of hearing loss. Ceru-men impactions can obscure the tym-panic membrane, preventing an accu-rate examination, and may causehearing loss. Dense cerumen impac-tions should be removed before diag-nostic testing. A leading cause of ac-quired hearing loss is otitis media witheffusion. Temporary hearing losshas been demonstrated during epi-sodes of acute otitis media. The childwith repeated or chronic otitis mediawith effusion is at high risk of ac-quired hearing loss and should un-dergo comprehensive hearing evalu-ation.13,14 Key point 4: All providers ofpediatric health care should be pro-
ficient with pneumatic otoscopy andtympanometry. However, it is impor-tant to remember that these meth-ods do not assess hearing.
TOOLS FOR OBJECTIVE HEARINGSCREENING
In addition to universal newborn hear-ing screening and regular surveillanceof developmental milestones, auditoryskills, parental concerns, and middle-ear status, objective screenings forhearing loss should be performed pe-riodically on all infants and children inaccordance with the schedule outlinedin the AAP statement “Recommenda-tions for Preventive Pediatric HealthCare”1 (Table 1). The technology usedfor hearing screening should be ageappropriate. The child also should becomfortable with the testing situation;young children may need preparation.A variety of objective tools have beendeveloped for screening tests. Thechoice of tool to use in screening de-pends on the child’s age, degree of co-operation, and available resources.
Screenings should be conducted in aquiet area where visual and auditorydistractions are minimal. For childrenfor whom screening is not possible be-cause of developmental level, referralto a pediatric audiologist should beinitiated for appropriate physiologicand/or behavioral audiological as-sessment. Various tests performed byaudiologists are outlined in Table 5.
Tympanograms
Conductive hearing loss may be themost common cause of infant hearingscreening failures.15 Objective middle-ear assessment can best be per-formed by tympanometry. Tympanom-etry measures relative changes intympanic membrane movement as airpressure is varied in the external audi-tory canal. Tympanograms (Fig 2) canmost simply be classified as types A, B,and C depending on the curve shape rel-ative to 0 as the pressure is changed(www.audiologyonline.com/askexpert/display!question.asp?question!id!451).
The presence of a type A, high-peakedtympanogram significantly decreasesthe probability that middle-ear effu-sion is the cause of hearing loss. A typeB, flat tympanogram has the highestprobability of the presence of middle-ear effusion or tympanic membraneperforation, which are both likely tocause some degree of hearing loss. Atype C tympanogram, with a peakshifted toward negative pressure, hasa low probability of middle-ear fluidand associated hearing loss. Type Band C tympanograms require clinicalcorrelation and possibly further evalu-ation and treatment. Traditionally,tympanograms have been obtained byusing low-frequency probe tones.These tones have been historically in-accurate for infants younger than 6months. The use of a high-frequencyprobe tone (1000 Hz) was recentlyshown to be a better measure ofmiddle-ear status in infants and young
TABLE 3 American Academy of Pediatrics Joint Committee on Infant Hearing Year 2007 PositionStatement3: Risk Indicators Associated With Permanent Congenital, Delayed-Onset, and/orProgressive Hearing Loss in Childhood
1 Caregiver concerna regarding hearing, speech, language, or developmental delay.2 Family historya of permanent childhood hearing loss.3 Neonatal intensive care of more than 5 days or any of the following regardless of length of
stay: ECMOa, assisted ventilation, exposure to ototoxic medications (gentamicin andtobramycin) or loop diuretics (furosemide/Lasix), and hyperbilirubinemia19 that requiresexchange transfusion.
4 In utero infections such as CMVa, herpes, rubella, syphilis, and toxoplasmosis.5 Craniofacial anomalies, including those that involve the pinna, ear canal, ear tags, ear pits,
and temporal bone anomalies.6 Physical findings, such as white forelock, that are associated with a syndrome known to
include a sensorineural or permanent conductive hearing loss.7 Syndromes associated with hearing loss or progressive or late-onset hearing lossa, such
as neurofibromatosis, osteopetrosis, and Usher syndrome; other frequently identifiedsyndromes include Waardenburg, Alport, Pendred, and Jervell and Lange-Nielson.
8 Neurodegenerative disordersa, such as Hunter syndrome, or sensory motor neuropathies,such as Friedreich ataxia and Charcot-Marie-Tooth syndrome.
9 Culture-positive postnatal infections associated with sensorineural hearing lossa, includingconfirmed bacterial and viral (especially herpes viruses and varicella) meningitis.
10 Head trauma, especially basal skull/temporal bone fracturea that requires hospitalization.11 Chemotherapya.12 Recurrent or persistent otitis media for at least 3 months.
Risk indicators that aremarkedwith a are of greater concern for delayed onset hearing loss. ECMO indicates extracorporealmembrane oxygenation; CMV, cytomegalovirus.Reproduced with permission from: American Academy of Pediatrics, Joint Committee on Infant Hearing. Pediatrics. 2007;120(4):898–921.
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 124, Number 4, October 2009 1255!"#!$%!=65$"2)!,@+!,--G!///01234'5)4670$)89$/%:$'323!;)$<!2++WSjjW%;3"+.36,_""WA#$36"+3'*,_'.9

children. These tympanograms aregenerally not classified as A, B, or C butrather as peak or no peak.
Evoked Otoacoustic Emissions
Evoked otoacoustic emissions (OAEs)are acoustic signals generated fromwithin the cochlea that travel in a re-verse direction through themiddle-earspace and tympanic membrane out to
the ear canal. These signals are gener-ated in response to an auditory stimu-lus, either clicks or tone bursts. Thesignals may be detected with a verysensitive microphone/probe systemplaced in the external ear canal. TheOAE test allows for individual ear as-sessment, can be performed quickly atany age, and does not depend onwhether the child is asleep or awake.
Mild degrees of motion artifact do notinterfere with test results; however,screening results are frequently influ-enced by the presence of middle-earpathologic abnormalities. The OAE testis an effective screening measure formiddle-ear abnormalities and formod-erate or more severe degrees of hear-ing loss, because normal OAE re-sponses are not obtained if hearingthresholds are approximately 30- to40-dB hearing levels or higher. The au-tomated OAE screener provides a pass-fail report; no test interpretation by anaudiologist is required. The OAE testdoes not further quantify hearing lossor hearing threshold level. The OAE testalso does not assess the integrity of theneural transmission of sound from theeighth nerve to the brainstem and,therefore, will miss auditory neuropa-thy and other neuronal abnormalities.Infants with such abnormalities willhave normal OAE test results but ab-normal auditory brainstem response(ABR) test results. A “failed” OAE testonly implies that a hearing loss ofmore than 30 to 40 dBmay exist or thatthe middle-ear status is abnormal.
Automated ABR
One objective physiologic means ofscreening hearing is the automatedABR. This instrument measures co-chlear response in the 1- to 4-kHzrange with a broadband click stimulusin each ear. Many ABR screening in-struments incorporate built-in artifactrejection for myogenic, electrical, andenvironmental noise interference,which ensures that data collection ishalted if testing conditions are unfa-vorable. The automated screener pro-vides a pass-fail report; no test inter-pretation by an audiologist is required.A “fail” report on an automated ABR im-plies a hearing level of worse than 40 dB.AutomatedABRcan test each ear individ-ually and can be performed on childrenof any age. Motion artifacts interferewith test results. For this reason, the test
TABLE 4 Developmental Milestones in the First 2 Years of Life
Milestone Average Age ofAttainment, mo
Developmental Implications
Gross motorHead steady in sitting 2.0 Allows more visual interactionPull to sit, no head lag 3.0 Muscle toneHands together in midline 3.0 Self-discoveryAsymmetric tonic neck reflex gone 4.0 Child can inspect hands in midlineSits without support 6.0 Increasing explorationRolls back to stomach 6.5 Truncal flexion, risk of fallsWalks alone 12.0 Exploration, control of proximity to
parentsRuns 16.0 Supervision more difficult
Fine motorGrasps rattle 3.5 Object useReaches for objects 4.0 Visuomotor coordinationPalmar grasp gone 4.0 Voluntary releaseTransfers object hand to hand 5.5 Comparison of objectsThumb-finger grasp 8.0 Able to explore small objectsTurns pages of book 12.0 Increasing autonomy during book timeScribbles 13.0 Visuomotor coordinationBuilds tower of 2 cubes 15.0 Uses objects in combinationBuilds tower of 6 cubes 22.0 Requires visual, gross, and fine motor
coordinationCommunication and languageSmiles in response to face, voice 1.5 Child more active social participantMonosyllabic babble 6.0 Experimentation with sound, tactile senseInhibits to “no” 7.0 Response to tone (nonverbal)Follows 1-step command with gesture 7.0 Nonverbal communicationFollows 1-step command withoutgesture (eg, “Give it to me”)
10.0 Verbal receptive language
Speaks first real word 12.0 Beginning of labelingSpeaks 4–6 words 15.0 Acquisition of object and personal namesSpeaks 10–15 words 18.0 Acquisition of object and personal namesSpeaks 2-word sentences (eg, “Mommyshoe”)
19.0 Beginning grammaticization, correspondswith vocabulary of!50 words
CognitiveStares momentarily at spot whereobject disappeared (eg, yarn balldropped)
2.0 Lack of object permanence (out of sight,out of mind)
Stares at own hand 4.0 Self-discovery, cause and effectBangs 2 cubes 8.0 Active comparison of objectsUncovers toy (after seeing it hidden) 8.0 Object permanenceEgocentric pretend play (eg, pretendsto drink from cup)
12.0 Beginning symbolic thought
Uses stick to reach toy 17.0 Able to link actions to solve problemsPretend play with doll (gives doll bottle) 17.0 Symbolic thought
Modified from: Behrman RE, Jenson HB, Kliegman R, eds. Nelson Textbook of Pediatrics. 16th ed. Philadelphia, PA: Saunders;2003.
1256 FROM THE AMERICAN ACADEMY OF PEDIATRICS!"#!$%!=65$"2)!,@+!,--G!///01234'5)4670$)89$/%:$'323!;)$<!
2++WSjjW%;3"+.36,_""WA#$36"+3'*,_'.9
is performed best in infants and youngchildren while they are sleeping. If thetest cannot be performed because of
motion artifact, sedation may be neces-sary. The ABR is currently used in manynewborn screening programs.
ABR and OAEs are tests of auditory path-way structural integrity but are not truetests of hearing. Even if ABR or OAE test
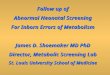
TABLE 5 Audiologic Tests for Infants and Children
DevelopmentalAge of Child
Auditory Test/Average Time
Type of Measurement Test Procedures Advantages Limitations
All ages Evoked OAEs/10-min test Physiologic test specificallymeasuring cochlear(outer hair cell)response topresentation of astimulus; stimuli may beclicks (transient evokedOAEs) or tone pairs(distortion productOAEs)
Small probe containing asensitive microphoneis placed in the earcanal for stimulusdelivery and responsedetection
Ear-specific results; notdependent onwhether patient isasleep or awake;quick test time;screening test
Infant or child must be relativelyinactive during the test; not acomprehensive test ofhearing, because it does notassess cortical processing ofsound; OAEs are very sensitiveto middle-ear effusions andcerumen or vernix in the earcanal
Birth to 9 mo Automated ABR/15-mintest
Electrophysiologicmeasurement of activityin auditory nerve andbrainstem pathways
Placement of electrodeson child’s head detectsneurologic response toauditory stimulipresented throughearphones or earinserts 1 ear at a time
Ear-specific results;responses notdependent on patientcooperation;screening test
Infant or child must remainquiet during the test(sedation is often required);not a comprehensive test ofhearing, because it does notassess cortical processing ofsound
9 mo to 2.5 y VRA/15- to 30-min test Behavioral tests measuringresponses of the child tospeech and frequency-specific stimulipresented throughspeakers or insertearphones
Technique conditions thechild to associatespeech or frequency-specific stimuli with areinforcer, such as alighted toy or videoclips; VRA requires acalibrated, sound-treated room
Assesses auditoryperception of child;diagnostic test.
When performed with speakers,only assesses hearing of thebetter ear; not ear specific; ifVRA is performed with insert,earphones can rule out aunilateral hearing loss
2.5 to 4 y Play audiometry/15–30 min
Behavioral test of auditorythresholds in responseto speech andfrequency-specificstimuli presentedthrough earphones and/or bone vibrator
Child is conditioned torespond whenstimulus tone isheard, such as to puta peg in a pegboardor drop a block in abox
Ear-specific results;assesses auditoryperception of child;screening ordiagnostic test.
Attention span of child may limitthe amount of informationobtained
4 y to adolescence Conventional audiometry/15- to 30-min test
Behavioral test measuringauditory thresholds inresponse to speech andfrequency-specificstimuli presentedthrough earphones and/or bone vibrator
Patient is instructed toraise his or her handwhen stimulus isheard
Ear-specific results;assesses auditoryperception of patient;screening ordiagnostic test
Depends on the level ofunderstanding andcooperation of the child
All ages Diagnostic ABR Electrophysiologicmeasurement of activityin auditory nerve andbrainstem pathways
Placement of electrodeson child’s headdetects auditorystimuli presentedthrough insertearphones 1 ear at atime
Ear-specific results;multiple frequenciesare tested, creating amap of hearing losssimilar to anaudiogram;responses notdependent on patientcooperation;diagnostic test
Infant or child must remainquiet during the test(sedation is often required);not a true test of hearing,because it does not assesscortical processing of sound
All ages Tympanometry Relative change in middle-ear compliance as airpressure is varied in theexternal auditory canal
Small probe placed inthe ear canal andpressure varied in theear canal
Tests for possiblemiddle-ear pathologyand pressure-equalization tubefunction
Not a test of hearing; dependson ear canal seal; high-frequency tone probe neededfor infants younger than 6 mo
Adapted with permission from: Bachmann KR, Arvedson JC. Pediatr Rev. 1998;19(5):155–165.
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 124, Number 4, October 2009 1257!"#!$%!=65$"2)!,@+!,--G!///01234'5)4670$)89$/%:$'323!;)$<!2++WSjjW%;3"+.36,_""WA#$36"+3'*,_'.9

results are normal, hearing cannot bedefinitively considered normal until achild is mature enough for a reliable be-
havioral audiogram to be obtained. Be-havioral pure-tone audiometry remainsthe standard for hearing evaluation.
Hearing thresholds at specific frequen-cies can be determined, and the degreeof hearing loss can be assigned. If therearedistractionsor theroomisnotsoundtreated, pure-tone audiometry in the of-fice should be considered solely ascreening test.
Play Audiometry
Children 2 to 4 years of age arescreened or tested more appropri-ately by play audiometry. These chil-dren are conditioned to respond to anauditory stimulus through play activi-ties, such as dropping a block when asound is heard through earphones.Air-conduction hearing threshold lev-els of greater than 20 dB at any ofthese frequencies indicate possiblehearing loss, and referral to a pediat-ric audiologist should be made.
Conventional ScreeningAudiometry
For children aged 4 years and older,conventional screening audiometrycan be used. The child is asked to raisehis or her hand when a sound is heard.The test should be performed in a quietenvironment using earphones, becauseambient noise can affect test perfor-mance significantly, especially at lowerfrequencies (ie, 500 and 1000 Hz). Eachear should be tested at 500, 1000, 2000,and 4000 Hz. Air-conduction hearingthreshold levels of greater than 20 dB atany of these frequencies indicate possi-ble hearing loss, and referral to a pedi-atric audiologist should be made.
If the child does not pass the screen-ing, earphones should be removed andinstructions carefully repeated to thechild to ensure proper understandingand attention to the test and then re-screened with the earphones reposi-tioned. A child whose repeat testshows hearing thresholds of greaterthan 20 dB at any of these frequencies,especially if there is no pathologic ab-normality of themiddle ear on physical
FIGURE 2Tympanograms. Type A: normal. Type B: abnormal, needsmedical attention. Type C, borderline normal;monitor; may need medical attention.
1258 FROM THE AMERICAN ACADEMY OF PEDIATRICS!"#!$%!=65$"2)!,@+!,--G!///01234'5)4670$)89$/%:$'323!;)$<!
2++WSjjW%;3"+.36,_""WA#$36"+3'*,_'.9

examination, should be referred forformal hearing testing. Key point 5: De-velopmental abnormalities, level offunctioning, and behavioral problems(ie, autism/developmental delay) maypreclude accurate results on routineaudiometric screening and testing. Inthis situation, referral to an otorhino-laryngologist and a pediatric audiolo-gist who has the necessary equipmentand expertise to test infants and youngchildren should be made (Table 5). Keypoint 6: The results of abnormalscreening should be explained care-fully to parents, and the child’s medi-cal record should be flagged to facili-tate tracking and follow-up.
It is important to remember that a“fail” report on any 1 of a combinationof tests warrants additional testing. Itis also important to remember thatfailure of speech, language, and hear-ing screening assessments warrantsadditional testing (Tables 6–9).
Comprehensive AudiologicalEvaluation Using Physiologic and/or Behavioral Testing
The ABR test may be used as a diagnos-tic tool by audiologists for more defin-itive diagnosis of hearing loss. Usuallyperformed in children in natural sleepup to approximately 3 to 6 months ofage and then under sedation for olderinfants, diagnostic ABR can provide notonly a general level of hearing but alsofrequency-specific hearing data. Diag-nostic ABR is performed with differentfrequency tone bursts and acrossvarying sound levels to effectively esti-mate an audiogram. Diagnostic ABRcan also be performed with bone con-duction to separate conductive fromsensorineural hearing loss. DiagnosticABR is often the definitive test used byaudiologists in children and infantswho are unable to cooperate withother methods of hearing testing. Au-diologic evaluation using ABR or audi-tory steady-state response provides
frequency-specific hearing thresholdsby air and bone conduction in each earseparately. ABR is the gold standardfor determination of hearing thresh-olds in infants younger than 6 monthsand in children who cannot be testedbehaviorally.
Children as young as 6 to 24 monthscan be tested by means of visual rein-forced audiometry (VRA). This tech-nique conditions the child to associatespeech or frequency-specific soundwith a reinforcement stimulus suchas a lighted toy or animated toy orvideo clips. VRA is performed by anaudiologist with experience testingyoung children. This testing is notreadily applied in screening pro-grams, because infants youngerthan 6 months’ developmental agecannot perform the task, and sound-treated rooms are needed. The re-sults of VRA can approximate thoseof conventional audiometry.
Children with unilateral or mild hear-ing loss also should be evaluated fur-ther. Studies have shown such chil-dren to be similarly at risk of adversecommunication skills as well as diffi-culties with social, emotional, and ed-ucational development.16
FOLLOW-UP AND DIAGNOSTICTESTING
Key point 7: Any abnormal objectivescreening result requires audiologyreferral and definitive testing. Screen-
ing will only result in benefit for thepatient if abnormal test results areconfirmed and appropriate interven-tion is provided. Most studies that haveevaluated the success rate of infanthearing screening programs have de-scribed a fairly high rate of failure toconfirm a failed screen with definitivetesting. A similar problem could alsooccur in screening older infants andchildren. Improving the physician’s in-volvement not only in screening butalso in arranging and confirming ap-propriate follow-up testing and inter-vention is necessary to achieve opti-mal speech, language, and hearing.
Key point 8: A failed infant hearingscreening or a failed screening in anolder child should always be con-firmed by further testing. Audiologistsmay repeat the audiometric test as de-scribed above in a sound booth andusing a variety of other tests. ABR canalso be used for definitive testing ofthe auditory system. A diagnostic ABRis usually performed under sedationor general anesthesia in children agedapproximately 3 to 6months and older.The test is performed with frequency-specific stimuli and presentation lev-els to approximate hearing thresholdlevels. Diagnostic ABR provides infor-mation that is accurate enough to al-low for therapeutic intervention. Hear-ing aids can be fitted with informationobtained from a diagnostic ABR. Audio-logic assessment and intervention is
TABLE 6 Ten Ways to Recognize Hearing Loss: Adolescents (11- to 21-Year Visits)
1. Do you have a problem hearing over the telephone?2. Do you have trouble following the conversation when two or more people are talking at
the same time?3. Do people complain that you turn the TV volume up too high?4. Do you have to strain to understand conversation?5. Do you have trouble hearing in a noisy background?6. Do you find yourself asking people to repeat themselves?7. Do many people you talk to seem to mumble (or not speak clearly)?8. Do you misunderstand what others are saying and respond inappropriately?9. Do you have trouble understanding the speech of women and children?10. Do people get annoyed because you misunderstand what they say?
Adapted from: National Institute on Deafness and Other Communication Disorders. Ten Ways to Recognize Hearing Loss.Bethesda, MD: National Institute of Health; 2006. NIH publication 01-4913. Available at: www.nidcd.nih.gov/health/hearing/10ways.asp.
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 124, Number 4, October 2009 1259!"#!$%!=65$"2)!,@+!,--G!///01234'5)4670$)89$/%:$'323!;)$<!2++WSjjW%;3"+.36,_""WA#$36"+3'*,_'.9
an ongoing process. The child requiresregular audiologic reevaluations to de-termine if there is fluctuating or pro-gressive hearing loss. Middle-earmon-itoring is also essential. Hearing aidselection, fitting, verification, and vali-dation require ongoing and regularvisits with the audiologist. Candidacy
for cochlear implantation should beconsidered when there is limited re-sidual hearing or when progress withamplification is insufficient. Recom-mendations to the family regarding co-chlear implantation should be basedon a team evaluation that includes au-diology, otology, psychology, speech-
language pathology, and other inter-vention personnel.
Most providers of pediatric healthcare realize the importance of refer-ring to an otolaryngologist, an audiol-ogist, and a speech-language patholo-gist. Less recognized is the potential
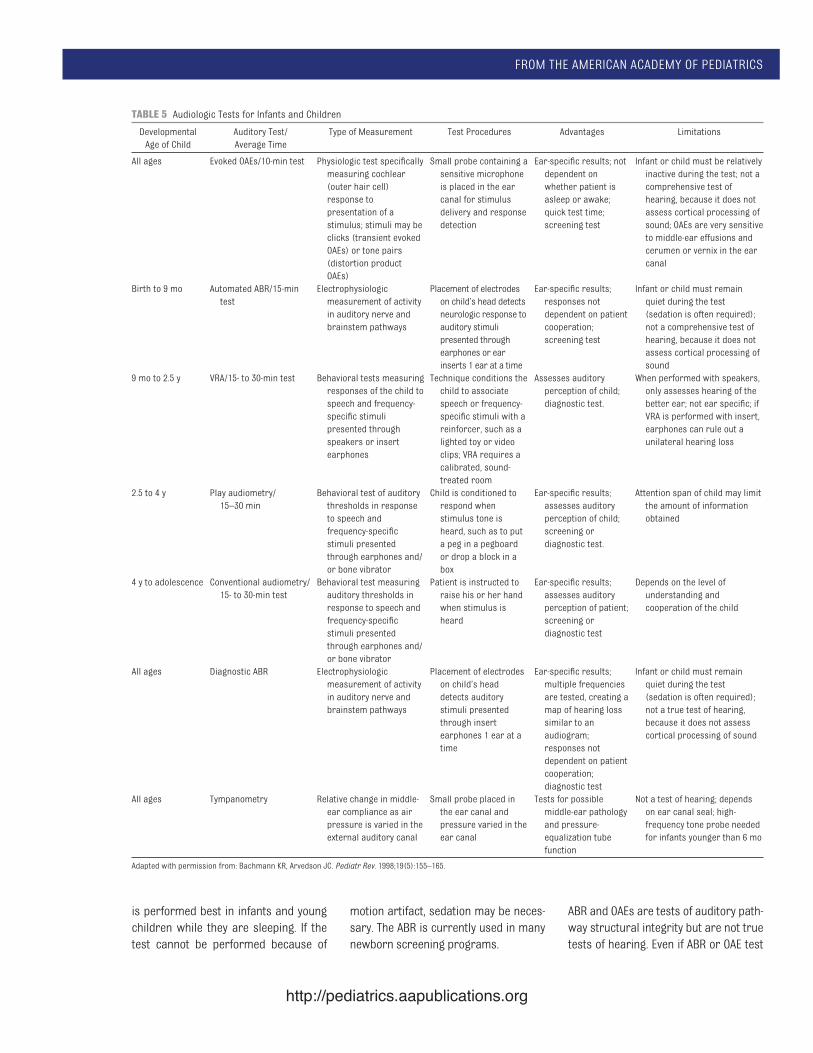
TABLE 7 Developmental/Behavioral Screening Tools
Resource Description Age Range Where to Find
General developmental screening toolsAges & Stages Questionnaire (ASQ) A series of 19 questionnaires used to screen
infants and young children fordevelopmental delays during the first 5 yof life
4–60 mo www.brookespublishing.com/tools/asq/index.htm
Ages & Stages Questionnaire: Social-Emotional(ASQ:SE)
A series of 19 questionnaires used to screeninfants and young children at risk forsocial or emotional difficulties, to identifybehaviors of concern to caregivers, andto identify any need for furtherassessment
6–60 mo www.brookespublishing.com/tools/asqse/index.htm
Parents’ Evaluation of Developmental Status(PEDS)
A method for detecting developmental andbehavioral-emotional problems inchildren
Birth to 8 y www.pedstest.com
Parents’ Evaluation of Developmental Status-Developmental Milestones (PEDS:DM)
A collection of 6–8 items per age/encounterdesigned to replace informal milestoneschecklists with highly accurate itemsknown to predict developmental status
Birth to 11 y www.pedstest.com/dm
Autism-specific screening toolsChecklist for Autism in Toddlers (CHAT) A screening tool for early detection of
autism18 to!24 mo www.autismresearchcentre.com/tests/
chat!test.aspChecklist for Autism in Toddlers (CHAT), DenverModifications
CHAT scoring modifications 18 to!24 mo
Checklist for Autism in Toddlers-23 (CHAT-23) Combination of M-CHAT and CHAT items 16–86 moChildhood Asperger Syndrome Test (CAST) A parental questionnaire to screen for
autism spectrum conditions4–11 y www.autismresearchcentre.com/tests/
cast!test.aspModified Checklist for Autism in Toddlers(M-CHAT)
23-item scale pointing to express interest,responsiveness to name, interest inpeers, showing behavior, response tojoint attention, social imitation
16–48 mo http://depts.washington.edu/dbpeds/Screening%20Tools/MCHAT.doc
Pervasive Developmental Disorders ScreeningTest-II, Primary Care Screener (PDDST-II PCS)
A parental questionnaire to screen forautism spectrum conditions
18–48 mo www.pearson-uk.com/product.aspx?n!1315&skey!2960
Autism-specific or psychosocial screening toolsPediatric intake form from Bright Futures Questionnaire to help gather a general
understanding of the history, functioning,questions and concerns of the family
Birth to 21 y www.brightfutures.org/mentalhealth/pdf/professionals/ped!intake!form.pdf
ADHD screening toolsVanderbilt rating forms Parent- and teacher-completed forms that
help a clinician diagnosis ADHD and tocategorize the problem into 1 of itsvarious subtypes
6–12 y www.brightfutures.org/mentalhealth/pdf/professionals/bridges/adhd.pdf
AAP ADHD toolkit A comprehensive toolkit developed fromevidence-based guidelines for thediagnosis and treatment of children withADHD; this resource toolkit contains awide array of screening, diagnosis,treatment, and support materials forclinicians and other health careprofessionals
6–12 y www.aap.org
ADHD indicates attention-deficit/hyperactivity disorder.
1260 FROM THE AMERICAN ACADEMY OF PEDIATRICS!"#!$%!=65$"2)!,@+!,--G!///01234'5)4670$)89$/%:$'323!;)$<!
2++WSjjW%;3"+.36,_""WA#$36"+3'*,_'.9

benefit of genetic and ophthalmologicevaluation of children and infants withsensorineural hearing loss.17
Especially in young infants and chil-dren, referral to an otolaryngologistfor a complete diagnostic assessmentis essential. More than 90% of the chil-dren with permanent hearing loss areborn to “hearing” parents, resulting ina sense of urgency for parents ofnewly identified children with hearingloss to seek out answers regarding eti-ology, risk of progression, implica-tions, and other questions. If childrenare indeed identified with sensorineu-ral hearing loss, a variety of diagnostictests can be recommended dependingon the patient’s history and physicalexamination. Otolaryngologists mayplay a role in diagnosis and treatingmiddle-ear fluid or other middle-eardisorders as well as assisting in thedefinitive diagnosis of the cause ofsensorineural hearing loss.18 Diagnos-tic testing may include imaging of thetemporal bone to identify structuraldefects; genetic tests, such as for ab-normalities of the Connexin gene; and,
occasionally, evaluation for other met-abolic defects. Evaluation by a geneti-cist and genetic testing can be impor-tant for diagnosis as well as forproviding the family with informationfor future planning purposes.
The hearing health care team (com-prising the audiologist, otolaryngolo-gist, teachers of the child with hearingimpairment, speech-language patholo-gists, and other educational and med-ical personnel) should assist the fam-ily with intervention for hearing loss.Interventions may include observationwith increased attention to speech andlanguage development, hearing aids,auditory-assisted systems for the schoolenvironment, or more invasive surgicalhearing devices such as cochlear im-plants or bone-anchored hearing aids.The goal is to provide families with ap-propriate options so that theymaymakewell-informed decisions. Interventionsshould be driven by family desires andguided by accurate and timely informa-tion from all hearing-related health careprofessionals. Family goals and expecta-tions are influenced by culture, parental
education, level of income, availability oflocal resources, language in the home,andmore. The role of the hearing healthcare team is to assist families in identi-fying all the options available to themand to support them throughout the on-going decision-making processes thatwill occur throughout the child’s devel-opment. All members of the hearinghealth care team, in conjunction withparents and on the basis of informedchoice, should recognize that no deci-sion regarding intervention is “final,”and periodic opportunities should beidentified for discussion regardingprogress, alternative interventions, andnew developments.
Medical follow-up includes ongoingevaluation and management of the ad-equacy of hearing rehabilitation; ob-servation for potential complicationsof hearing rehabilitation, such as otitisexterna and cerumen impactions; andmonitoring for appropriate speechand language development.
Speech and language evaluation by aspeech-language pathologist withtraining in working with children withhearing loss is also important for doc-umentation of baseline speech andlanguage skills and implementing aprogram of intervention that reflectsthe family’s choice regarding languagedevelopment.
At least one third of childrenwith hear-ing loss will have an additional coexist-ing condition.3 Because many causesof hearing loss are associated with ab-normal ophthalmologic findings, formalophthalmologic evaluation is appropri-ate, not only to assist with the diagnosisbut also to optimize vision. A diagnosis ofUsher syndrome with associated pro-gressive hearing and vision loss may in-fluence communication choices.
Children with hearing loss shouldalso be monitored for developmentaland behavioral problems (attention-deficit/hyperactivity disorder, autism,learning disabilities) and referred for
TABLE 8 Guidelines for Children with Abnormal Speech Development
Age, mo Referral Guidelines for Children With “Speech” Delay
12 No differentiated babbling or vocal imitation18 No use of single words24 Single-word vocabulary of!10 words30 Fewer than 100 words; no evidence of 2-word combinations; unintelligible36 Fewer than 200 words; no use of telegraphic sentences; clarity!50%48 Fewer than 600 words; no use of single sentences; clarity!80%
Source: Matkin ND. Pediatr Rev. 1984;6:151.
TABLE 9 Guidelines for Children With Suspected Hearing Loss
Age,mo
Normal Development
0–4 Should startle to loud sounds, quiet to mother’s voice, momentarily cease activity whensound is presented at a conversational level
5–6 Should correctly localize to sound presented in a horizontal plane, begin to imitate sounds inown speech repertoire or at least reciprocally vocalize with an adult
7–12 Should correctly localize to sound presented in any plane, should respond to name, evenwhen spoken quietly
13–15 Should point toward an unexpected sound or to familiar objects or persons when asked16–18 Should follow simple directions without gesture or other visual cues; can be trained to reach
toward an interesting toy at midline when a sound is presented19–24 Should point to body parts when asked; by 21 mo, can be trained to perform play audiometry
Source: Matkin ND. Pediatr Rev. 1984;6:151.
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 124, Number 4, October 2009 1261!"#!$%!=65$"2)!,@+!,--G!///01234'5)4670$)89$/%:$'323!;)$<!2++WSjjW%;3"+.36,_""WA#$36"+3'*,_'.9

additional evaluation when necessary.Health care professionals can usescreening tools to evaluate young chil-dren periodically for such concerns(Table 7) and refer for additional eval-uation when concerns arise.
A medical professional should partici-pate as an active member of a family’shearing health care team after diagno-sis and provide input to assist in theadequacy of the rehabilitative effortsto monitor the child for progressionand additional disabilities.
HEARING REFERRAL RESOURCES
Key point 9: Abnormal hearing test re-sults require intervention and clinicallyappropriate referral, including otolaryn-gology, audiology, speech-language pa-thology, genetics, and early intervention.Pediatric health care professionalsshould maintain a list of referral re-
sources available in their community forchildren with hearing loss and shouldadvocate for increasing options andchoices for families. Otolaryngologists,audiologists, and speech-language pa-thologists with special training and ex-perience in treating children should beconsulted for specific diagnosis, coun-seling, and treatment. Pediatric healthcare professionals should collaborateto refer the child for comprehensiveeducational counseling and treatmentservices. Communication among pro-fessionals caring for a child with hear-ing loss is essential to ensure appro-priate case management.
COMMITTEE ON PRACTICE ANDAMBULATORY MEDICINE, 2007–2008Robert D. Walker, MD, ChairpersonEdward S. Curry, MDLawrence D. Hammer, MDAllen D. “Buz” Harlor Jr, MD
James J. Laughlin, MDAndrea J. Leeds, MD
LIAISONSHerschel R. Lessin, MD – Section onAdministration and Practice Management
Olivia Whyte Thomas, MD – National MedicalAssociation
STAFFHeather Fitzpatrick, MPHJennifer Mansour
SECTION ON OTOLARYNGOLOGY–HEADAND NECK SURGERY, 2007–2008David H. Darrow, MD, DDS, ChairpersonCharles Bower, MDSukgi Susan Choi, MDEllen Sue Deutsch, MDScott R. Schoem, MDMark S. Volk, MD, DMD
STAFFAleksandra Stolic, MPH
CONTRIBUTORChristoph U. Lehmann, MD – Partnership forPolicy Implementation
REFERENCES
1. American Academy of Pediatrics, Committee on Practice and Ambulatory Medicine and BrightFutures Steering Committee. Recommendations for preventive pediatric health care. Pediatrics.2007;120(6):1376
2. Yoshinaga-Itano C, Sedey AL, Coulter DK, Mehl AL. Language of early and later-identified childrenwith hearing loss. Pediatrics. 1998;102(5):1161–1171
3. American Academy of Pediatrics, Joint Committee on Infant Hearing. Year 2007 positionstatement: principles and guidelines for early hearing detection and intervention programs.Pediatrics. 2007;120(4):898–921
4. American Academy of Pediatrics, Task Force on Newborn and Infant Hearing. Newborn and infanthearing loss: detection and intervention. Pediatrics. 1999;103(2):527–530
5. Bachmann KR, Arvedson JC. Early identification and intervention for children who are hearingimpaired. Pediatr Rev. 1998;19(5):155–165
6. Berg AL, Spitzer JB, Garvin JH Jr. Ototoxic impact of cisplatin in pediatric oncology patients.Laryngoscope. 1999;109(11):1806–1814
7. Brookhouser PE, Worthington DW, Kelly WJ. Noise-induced hearing loss in children. Laryngoscope.1992;102(6):645–655
8. Watkin PM, Baldwin M, McEnery G. Neonatal at risk screening and the identification of deafness.Arch Dis Child. 1991;66(10 spec No):1130–1135
9. Kittrell AP, Arjmand EM. The age of diagnosis of sensorineural hearing impairment in children. IntJ Pediatr Otorhinolaryngol. 1997;40(2–3):97–106
10. Watkin PM, BaldwinM, Laoide S, Parental suspicion and identification of hearing impairment. ArchDis Child. 1990;65(8):846–850
11. Coplan J. Deafness: ever heard of it? Delayed recognition of permanent hearing loss. Pediatrics.1987;79(2):206–213
12. Grundfast KM, Lalwani AK. Practical approach to diagnosis and management of hereditary hear-ing impairment (HHI). Ear Nose Throat J. 1992;71(10):479–493
13. American Academy of Pediatrics, OtitisMedia Guideline Panel. Managing otitismediawith effusionin young children. Pediatrics. 1994;94(5):766–773
14. American Academy of Pediatrics, Subcommittee on Otitis Media With Effusion; American Academyof Family Physicians; American Academy of Otolaryngology–Head and Neck Surgery. Clinical prac-tice guideline: otitis media with effusion. Pediatrics. 2004;113(5):1412–1429
1262 FROM THE AMERICAN ACADEMY OF PEDIATRICS!"#!$%!=65$"2)!,@+!,--G!///01234'5)4670$)89$/%:$'323!;)$<!
2++WSjjW%;3"+.36,_""WA#$36"+3'*,_'.9

15. Boone RT, Bower CM, Martin PF. Failed newborn hearing screens as presentation for otitis mediawith effusion in the newborn population. Int J Pediatr Otorhinolaryngol. 2005;69(3):393–397
16. Tharpe AM, Bess FH. Identification and management of children with minimal hearing loss. IntJ Pediatr Otorhinolaryngol. 1991;21(1):41–45
17. Moeller MP, White KR, Shisler L. Primary care physicians’ knowledge, attitudes, and practicesrelated to newborn hearing screening. Pediatrics. 2006;118(4):1357–1370
18. Strasnick B, Hoffman KK, Battista RA. Inner ear, genetic sensorineural hearing loss. eMedicine.Available at: www.emedicine.com/ent/topic223.htm. Accessed February 6, 2009
19. American Academy of Pediatrics, Subcommittee on Hyperbilirubinemia. Management of hyperbi-lirubinemia in the newborn infant 35 or more weeks of gestation [published correction appearsin Pediatrics. 2004;114(4):1138]. Pediatrics. 2004;114(1):297–316
FROM THE AMERICAN ACADEMY OF PEDIATRICS
PEDIATRICS Volume 124, Number 4, October 2009 1263!"#!$%!=65$"2)!,@+!,--G!///01234'5)4670$)89$/%:$'323!;)$<!2++WSjjW%;3"+.36,_""WA#$36"+3'*,_'.9
9=>?!.-0.*@,A12370,--GC.GGB!,--GE.,@E.,*,C.,TDE!$)484%'::#!1(":47J23!$%:4%2!W21!,F+!,--GE!!"#$%&'$()
U23464%2!'%3!5J2!W2654$%!$%!=5$:')#%8$:$8#!I2'3!'%3!X26]!W()82)#!Z::2%!90!L(a!I'):$)+!&)+!HJ'):27!L$/2)+!H$<<45522!$%!S)'65462!'%3!Z<"(:'5$)#
M"&')#)9(6$,""'%'/?"),%'/(N11"110"'#(%'(+'<)'#1()'*(CH%9*,"'7(B"$&00"'*)#%&'1(O">&'*
@(6",-%$"1A8*)#"*(+'<&,0)#%&'
J551?AA///01234'5)4670$)8A684A6$%52%5A;(::A.,@A@A.,*,4%6:(34%8!J48JC)27$:(54$%!;48()27+!6'%!"2!;$(%3!'5?!
B"<","'$"1
J551?AA///01234'5)4670$)8A684A6$%52%5A;(::A.,@A@A.,*,KL>LM'5?NJ47!')546:2!64527!.B!')546:27+!..!$;!/J46J!#$(!6'%!'66277!;$)!;)22
6;D18"$%)9#>(C&99"$#%&'1
J551?AA///01234'5)4670$)8A684A6$::2654$%A$;;462P1)'65462E<<%$"(.,)$#%$";$::$/4%8!6$::2654$%Q7R?!NJ47!')546:2+!':$%8!/45J!$5J2)7!$%!74<4:')!5$1467+!'112')7!4%!5J2
.",0%11%&'1(@(F%$"'1%'/
J551?AA///01234'5)4670$)8A<476AS2)<4774$%707J5<:5'":27R!$)!4%!457!2%54)25#!6'%!"2!;$(%3!$%:4%2!'5?!>%;$)<'54$%!'"$(5!)21)$3(64%8!5J47!')546:2!4%!1')57!Q;48()27+
B"8,%'#1J551?AA///01234'5)4670$)8A<476A)21)4%5707J5<:>%;$)<'54$%!'"$(5!$)32)4%8!)21)4%57!6'%!"2!;$(%3!$%:4%2?!
!"#!$%!=65$"2)!,@+!,--G!///01234'5)4670$)89$/%:$'323!;)$<!
2++WSjjW%;3"+.36,_""WA#$36"+3'*,_'.9