-
7/25/2019 Recognition of Seriously Ill Child
1/12
1/12
3.2.1here we goM7mmad 7mmdan
Recognition of seriously ill child
Our lecture today is mainly about signs and symptoms of
respiratory andcirculatory failure, coz if we detect these S&S
we can avoid the morbidity andmortality in the children ,the most
common cause of death in children is septic orhypovolumic shock and
heart failure.
-seriously ill child : child in rapid need of assessment &is
recognized
by symptoms & signs like; tachycardia , tachypnea ,
irritability , lethargycyanosis, grunting, nasal flaring , chest
retractions , .
Aims and Objectives of the lecture
Aetiology of cardiac arrest in children
Reducing mortality and morbidity
Recognising respiratory and circulatory insufficiency and
failure
Initial management plan
The most common cause of heart failure in adults is ischemic
heart disease
We have primary and secondary cardiac arrest :
Primary Cardiac Arrest Common in adults, less common in children
Sudden, unpredictable onset Due to arrhythmia (Ventricular
fibrillation or pulseless ventricular tachycardia) Hypoxia and
acidosis not initially present Outcome depends on early
defibrillation
So the primary is sudden in nature " kan el-zlmeh methl
el-wrdeh"But if you were at ICU , NICU or ER and the nurse called
you because code blue "cardiac
arrest" and the patient was child , you must know there was
wrong in the observation and
monitoring of the patient, because before the cardiac arrest the
patient went through tachypnea, tachycardia , hypoxia, acidosis
then cardiac arrest ,so if we had good monitoring on the
patient we could save his life.
-
7/25/2019 Recognition of Seriously Ill Child
2/12
2/12
Most cases of cardiac arrest in children are preceded by
respiratory failure .
Secondary Cardiac Arrest Most common form in children Heart
stops due to ischemia or hypoxia secondary to another condition
Arrest rhythm is usually bradycardia, progressing to asystole
"most commonarrhythmia in children"
Hypoxia initially present Outcome depends on prevention or
prompt resuscitation " very poor"
so,in children the cardiac arrestcan result from either
respiratoryorcirculatorycauses
,both of them progress from compensated stage to decompensated
then both of them lead tothe same outcome; cardiorespiratory
failurethat progress to cardiorespiratory arrest
Shock: clinical state where we have poor delivery of nutrient
and oxygen to thetissue.
THE most common shock is the hypovolemic one that can result
fromgastroenteritis ,then septic shock "meningococcemia" , so dont
mix b/w
shock &cardiac arrest.
Successful resuscitation in children depends upon
early recognition of respiratory and circulatory
failure and measures to prevent progression to
cardiac arrest
Compensated respiratory
failure
Compensated circulatory
failure
Decompensated circulatoryfailure
Cardiorespiratory failure
Cardiorespiratory arrest
Decompensated respiratoryfailure
-
7/25/2019 Recognition of Seriously Ill Child
3/12
3/12
In acutely ill child always remember:
A - Airway
B - Breathing
C - Circulation
D drugs "from the doc"Assess , change , reassess
Respiratory Failure :-respiratory failure: the loss of ability
of the respiratory system tomaintain adequate blood level of Co2
&O2 , the definition that say
PaCo2 >50 mmHg or PaO2
-
7/25/2019 Recognition of Seriously Ill Child
4/12
4/12
We used to say that asthma, bronchiolitis patients etc, come to
ER in distress and
tachypnea , but sometimes especially in bronchiolitis and in
young age like 6 weeks thefirst and only presentation is apnea
"respiratory failure".
Assessment of Respiratory Insufficiency: Airway Chest movement
does not imply a clear airway Listen and feel for air movement and
noises"sometimes is only transmitted sounds
from upper airway"
Is the airway:Clear and safe? At risk? Obstructed?
Assessment of Respiratory Insufficiency: Breathing1. Respiratory
rate2. Tidal volume3. Work of breathing4. Oxygenation
1.Respiratory rate:Varies with age, fever, pain and anxiety as
well as respiratory insufficiency,fevereach 1c raise in temperature
increase the respiratory rate by 4/min and pulse by10/min.
It is more important to monitor the trend in respiratory rate
than to rely
on the absolute value
For example : Guillain-Barre patient enter ER with weakness but
then he
stabilize with RR=20 the next day RR=25 then 30 then he died
fromrespiratory failure , if the doc noticed the variation with
time not the absolute
value then he/she would save the patients life . you can see
that all the values
are within normal range in this patient.
Age 12
Resp
rate
30-40 20-30
20-24 12-20
Minute ventilation Tidal volume rate
1400ml/min 140ml 10/min
1400ml/min 70ml 20/min
1400ml/min 35ml 40/min
-
7/25/2019 Recognition of Seriously Ill Child
5/12
5/12
2. Tidal volume; look, listen, feel Compare one side with the
other" any bulging or asymmetrical movement" Subjective assessment;
breath sounds should be audible in both bases Feel for the trachea;
is it central? "collapse or pleural effusion"
Noises Stridor: Inspiratory noise; airway obstruction above the
thoracic inlet, can be expiratory
or biphasic .
Wheeze: Expiratory noise; airway obstruction below the thoracic
inlet Grunting: Expiratory noise; attempt to raise the
end-expiratory lung volume .
Signs of Respiratory Distress (increased work of breathing):
Tachypnoea Recession
Head bobbing Anxious demeanour Flared nostrils Grunting Stridor
or wheeze Exhaustion
Signs of decompensation
Increasing respiratory rate Respiratory rate 55 Sudden fall in
respiratory rate Reduced interaction with carers Exhaustion
Decreasing level of consciousness
3.OxygenationCyanosis is an unreliable sign of hypoxia
Absence of cyanosis does not imply good oxygenation
Central cyanosis does imply hypoxia ; baby with TOF will born
with cyanosis thatdoesnt relate to oxygen .
Use a pulse oximeter What FIO2 is required to maintain good
saturations?" FiO2 ; fraction of inspired O2"
Actually this depends on the age.By using oximeter detect the O2
saturation. the normal range from 95-100% IN ADULTS.
recessions
-
7/25/2019 Recognition of Seriously Ill Child
6/12
6/12
- the child suffer from circulatoryfailure manifested aspurpuric
petechial rash on his
skinfrom septic shock "gram organism" .
-hypovolumia , low BP , low or nourine output , increase
capillary refill
time .
CardiacOutput
Heart Rate
Strokevolume
Afterload
Preload
SystemicVascular
Resistance
BloodPressure
Contractility
- so as you can see: cardiac output = stroke volume*heart
ratechildren they are heart rate dependent; because the stroke
volume is toosmall so to get adequate blood heat rate should be
high .
- so this is why bradycardia is very bad sign in young
children.
blood pressure &systemic vascular resistance SVR.When BP
falls in the compensatory range the SVR will increase toCompensate
in an attempt to raise the BP , so first the perfusion to thekidney
& skin will be reduced . When compensation fail the BP will
be
low. But keep in mind the perfusion to the vital organs "brain,
heart persist intact till the last moment .
cerebral perfusion pressure should be kept around 50mmHg to
avoidhypoxia. Cerebral perfusion pressure = MAP-ICPMAP= mean
arterial blood pressure
ICP=internal cerebral pressure "intra cranial pressure"
-
7/25/2019 Recognition of Seriously Ill Child
7/12
7/12
Assessment of Circulatory Failure: Heart rate Blood pressure
Systemic vascular resistance Pre-load
Heart rate:Varies with age, fever 1c=10beats/min and anxiety as
well as circulatory failure
Normal heart (HR) and respiratory (RR) rates by age
Blood PressureAfterthe 1styear of life , the systolic BP must be
AT LEAST 70 and above.But you must know the ranges because they are
narrow so the patient become hypotensive OR
hypertensive by a little change in his BP.
Blood pressure is maintained by increases in SVR at the expense
of perfusion of:
Skin Kidneys/gut
So you must know that the kidney function is indication of
response to fluid treatment inhypovolumic patient, any urine output
5 is polyurea, normal
urine output in children {1-5}ml/kg/hour.
Skin Perfusion"Capillary refill"Gives us idea of circulation in
the patient. Gently squeeze a finger (or toe) pulp until it
blanches Release and observe the return of capillary blood > 2
seconds is abnormal
7090100130HR
X5X5X5
14182030RR
18125 ears>30Age
90120> 10 ears70 + 2x a e90 + 2x a e1 10 ears
70801 12 months
50600 1 month
Systolic BP(lower limit)
mmHg
Systolic BP(normal) mmHg
Age
-
7/25/2019 Recognition of Seriously Ill Child
8/12
8/12
Skin Perfusion "Continue" Look for colour (mottling"", pallor,
peripheral cyanosis or rashes) feel - for peripheral pulses,
temperature and the line of demarcation between warm and
cold .
Renal Perfusion
Urine output is an index of organ perfusion Nappy weights
Urinary catheter?
Pre-load Jugular venous pulsation "rarely visible coz of short
neck in children" Enlargement of liver " in cardiogenic shock"
Moist sounds in lungs CXR
Signs of decompensationin circulatory failure Increasing pulse
rate Sudden fall in pulse rate Hypotension Oliguria Reduced
interaction with carers Decreasing level of consciousness
From ro2ya but the doc didnt mention them:
Types of circulatory failure shock- shock :clinical syndrome of
circulatory dysfunction resulting in
inadequate o2 & nutrient delivery, with inability to meet
the metabolicdemand of the tissue .
-types :
1-hypovolumic:due to loss of fluid2-relative hypovolumic "
distributive ":the problem is not related to
absolute volume but to loss of vessel tone resulting in
vasodilatation&larger intravascular space with normal blood
volume .
3-cardiogenic:abnormality in cardiac function due to
depressed
myocardial contractility .
Cardiogenic
Distributive
Hypovolaemic
Pre-loadSVRBPHR
-
7/25/2019 Recognition of Seriously Ill Child
9/12
9/12
Cardiorespiratory FailureIf we have respiratory or circulatory
failure both will in cardiorespiratory arrest.
There is always some respiratory compensation for circulatory
failure and viceversa
In severe illness it is not possible to determine which came
first If untreated, this phase presages imminent cardio-respiratory
arrest
Management; based on initial assessment
Compensated Respiratory Failure
Assess airway O2 therapy (unthreatening) Monitoring (pulse
oximetry, pulse and respiratory rate) IV access with topical
anaesthesia,to reduce the pain result from iv canula. Reassess
Decompensated Respiratory Failure
Admit to ICU Maintain clear airway 100% O2 Support ventilation
with bag/mask system Consider tracheal intubation and mechanical
ventilation
Compensated Circulatory Failure
Assess airway
O2 therapy (unthreatening) Monitoring (pulse oximetry, pulse and
respiratory rate, blood pressure) IV access Fluid bolus
Reassess
Decompensated Circulatory Failure
Airway control 100% O2 Support ventilation if required
Urgent IV/IO access, fluid bolus Reassess and repeat as required
Consider inotropes
-
7/25/2019 Recognition of Seriously Ill Child
10/12
10/12
Cardiorespiratory Failure Airway control 100% O2 Support
ventilation, initially with bag/mask system Reassess (monitoring)
Urgent IV/IO access; fluid boluses if required Reassess
Consider inotropes
Notes:1-AS you see in the previous session that each management
consist of:
assessment. Change. reassessment
2-IV fluid boluses in case of hypovolumic shock and septic ;each
bolus equal to 20cc/kg ;u can give many boluses till the patient
improve ;there is 2 types of IV fluids :
A-crystalloid : effective volume expander but require 2-4 times
the volume of bloodloss to restore hemodynamic parameters and
doesn't stay for long in the vascular space so
the BP will decrease again . it is of 2 types either :1- normal
saline(most available) and the best because of its Na conc , close
to
the osmolarity of the blood (285) and we calculate it by = (Na
+k )*2
+BUN+SUGAR/22-ringer's lactate(normal saline+Ca+lactate) used in
acidosis "from hemma"
B-colloid:one of its constitute is albumin , stay longer but can
carry infections incase of"fresh frozen plasma"(type of the
colloid) like hepatitis ,HIV
usually the normal saline used in colloid compartment but others
can be used aswell.
3-inotrpes:drugs that enhance the cardiac muscle contractility
thusincrease the cardiac output and vasopressors :digitalis
,debutamine, dopamine,
Adrenaline, norepinephrine. The under lined not mentioned by the
doc
4-whenever u dont find an IV access as soon as possible(nearly
90 sec)give theresuscitation IO(intra-osseous) ; usually in the
tibia
Example 1
9 month old with breathing difficulty. On admission; respiratory
rate 45/min,heart rate 160/min, temperature 37.80C. Conscious and
fully orientated
A: Clear
B: Generalised wheeze both lungs, increased work of
breathing
C: Tachycardia, BP normal, good peripheral perfusion
This case is "Compensated respiratory failure" ;if u notice the
level ofconsciousness not altered .
-
7/25/2019 Recognition of Seriously Ill Child
11/12
11/12
Management in example 1:
O2 therapy (unthreatening) Monitoring (pulse oximetry, pulse and
resp rate) IV access with topical anaesthesia
Reassess regularly
Other Investigations
CXR? FBC & Electrolytes? Blood gases?And this patient is
Onward referral
Example 2
11 month old with 2 day history of colic. On admission;
respiratory rate 40/min,
heart rate 185/min temperature 37.20C. Drowsy and withdrawnA:
Clear
B: Good air entry bilaterally, tachypnoea, quiet respiration
C: BP 65/?, cool mottled peripheries, capillary refill time 5
seconds, dry nappy
This case is a "Decompensated circulatory failure" note that the
child is hypotensive ,
has a capillary refill 5 sec AND drowsy .
Management in example 2:
Airway control High flow O2 Support ventilation if required
Monitoring (minimum SpO2 and BP) Urgent IV access, fluid bolus
Reassess and repeat as required
Fluid boluses,20ml/kg of Balanced salt solutions initially (e.g.
0.9% NaCl, Compound
Sodium Lactate),Reassess.
But If the patient is bleeding give blood .
Assessment of Fluid Boluses
Changes in heart rate, BP, peripheral perfusion
Chest signs Jugular venous pulsation, liver edge
CXR
Other Investigations
CXR CBC, X-match & Electrolytes Blood gases
-
7/25/2019 Recognition of Seriously Ill Child
12/12
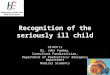
Left pic: hypovolumic shock ,heart is small "low blood volume"
,the lungare black "hypoperfusion"
Right pic:CXR for cardiogenic circulatory failure ; there is
cardiomegaly ,lung edema , this child was given overload fluid.
Tm be7md Allah
A7la t7yah ela groupi C6 "3dnan ,feras , iyad, m7mmd jehad ,
yaseen ,m7mmd iyad ,
sleem , 5leel (CR), 5ATOON, ZENAH,N3EEMH, HAJAR, FA6MH, LINA,
NUR."W shokr kbeer la Btool abo-3'zal 3la mo7adrt ro2yaT7yah la
RASHED W BSHAR , M7MMAD 3LEEMATMY dude "7ussam skaf"
Finally
i'LL BE BACK
Ella roo7 3bd-Allah Abo-6weelh "AL-FAT7EH"
M7MMAD 7AMMDAN