Embed Size (px)
Citation preview
Recognition of
Nonverbal Facial and
Vocal Affect After TBI Barbra Zupan, Ph.D., Brock University, Canada
Duncan R. Babbage, Ph.D., Massey University, NZ
Dawn Neumann, Ph.D., Indiana University, USA
Barry Willer, Ph.D., University at Buffalo, USA
Affect Recognition Difficulties
Research has shown that people with TBI have perceptual
deficits in the recognition of facial affect (Babbage et al., 2011;
Green et al., 2004; Hopkins et al., 2002) and vocal affect (Dimoska et al.,
2010; Pell, 2006; Pell & Baum, 1997; Pell et al., 2011)
BUT few studies have simultaneously examined recognition
of facial and vocal affect in the same group of people
Do these deficits co-occur?
Is one modality impacted more greatly than the other?
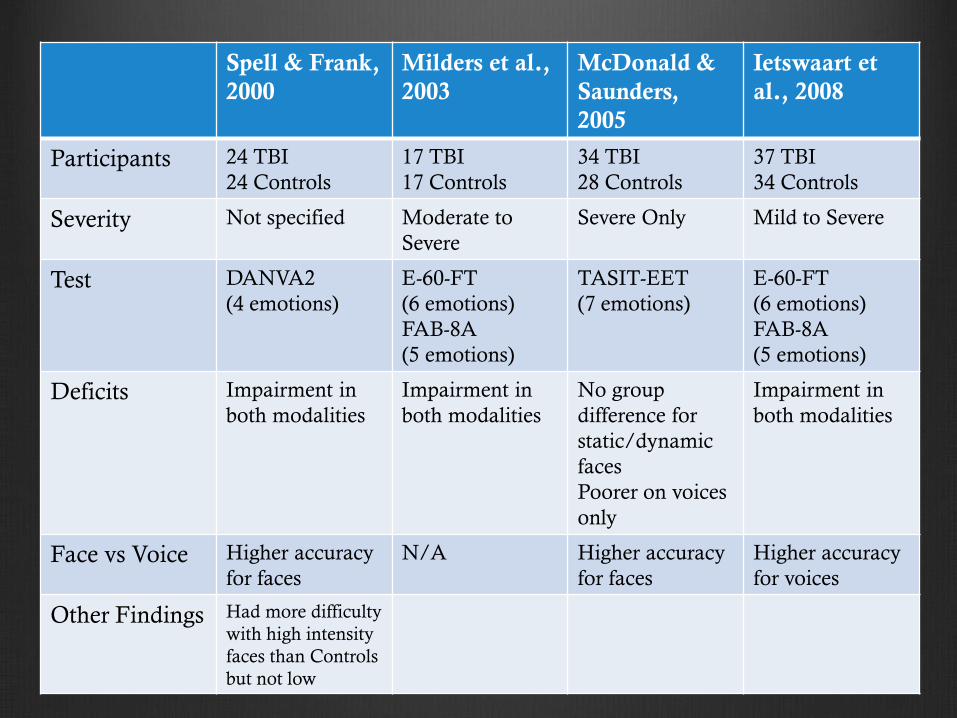
Spell & Frank,
2000
Milders et al.,
2003
McDonald &
Saunders,
2005
Ietswaart et
al., 2008
Participants 24 TBI
24 Controls
17 TBI
17 Controls
34 TBI
28 Controls
37 TBI
34 Controls
Severity Not specified Moderate to
Severe
Severe Only Mild to Severe
Test DANVA2
(4 emotions)
E-60-FT
(6 emotions)
FAB-8A
(5 emotions)
TASIT-EET
(7 emotions)
E-60-FT
(6 emotions)
FAB-8A
(5 emotions)
Deficits Impairment in
both modalities
Impairment in
both modalities
No group
difference for
static/dynamic
faces
Poorer on voices
only
Impairment in
both modalities
Face vs Voice Higher accuracy
for faces
N/A
Higher accuracy
for faces
Higher accuracy
for voices
Other Findings
Had more difficulty
with high intensity
faces than Controls
but not low

The Current Study
Data collected as part of a Randomized Clinical Trial
Funded by the National Institute on Disability and Rehabilitation
Research (H133G080043)
Three sites
Canada, United States, New Zealand
Comparing two treatment programs to one control group
Facial Affect Recognition
Social Emotional Inferencing
Extensive testing done to evaluate eligibility and changes due
to treatment
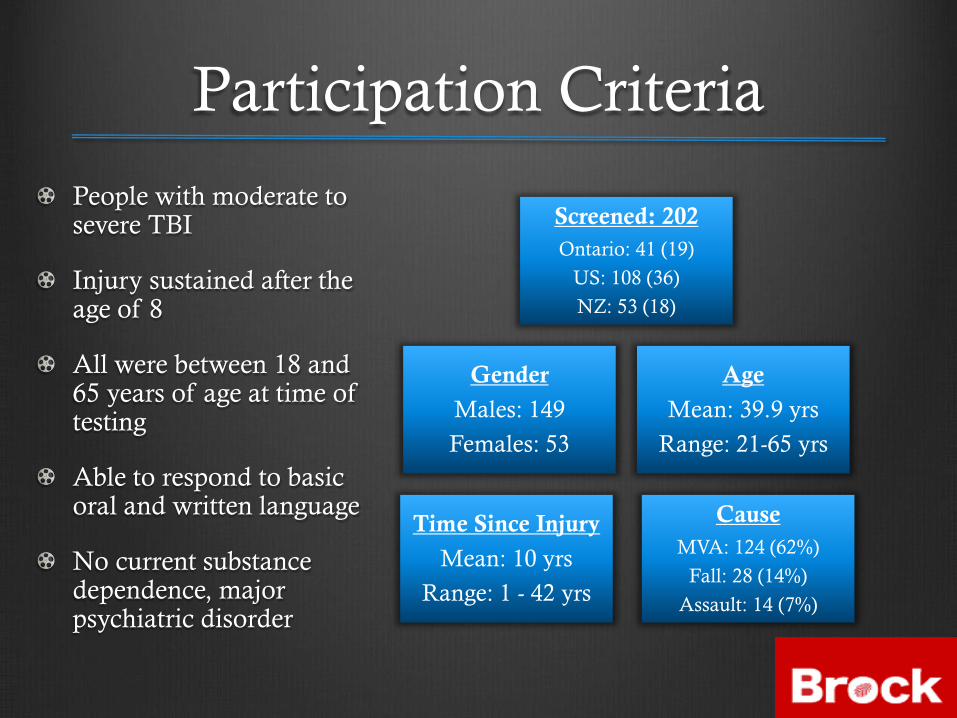
Participation Criteria
People with moderate to severe TBI
Injury sustained after the age of 8
All were between 18 and 65 years of age at time of testing
Able to respond to basic oral and written language
No current substance dependence, major psychiatric disorder
Screened: 202
Ontario: 41 (19)
US: 108 (36)
NZ: 53 (18)
Cause
MVA: 124 (62%)
Fall: 28 (14%)
Assault: 14 (7%)
Gender
Males: 149
Females: 53
Age
Mean: 39.9 yrs
Range: 21-65 yrs
Time Since Injury
Mean: 10 yrs
Range: 1 - 42 yrs
Diagnostic Analysis of Nonverbal
Affect-2 (Nowicki, 2008)
24 coloured photographs
6 of each emotion
Happy, sad, angry, fearful
3 high intensity expressions
3 low intensity expressions
Displayed 15 seconds
Adult Faces
Diagnostic Analysis of Nonverbal
Affect-2 (Nowicki, 2008)
Adult Paralanguage
24 repetitions portrayed by one male and one female actor
“I’m going out of the room now and I’ll be back later”
6 of each emotion
Happy, sad, angry, fearful
3 high and 3 low intensity exemplars within each category
Heard each sentence one time only

Results
Not impaired Faces Only Voices Only Both Modalities
48% 17% 14% 21%
n=92 n=32 n=26 n=40
Over half of the participants showed impaired
recognition in one or both modalities (n=98)
Facial stimuli recognized significantly better than vocal
stimuli, 2 (2)= 22.16, p < .001
Supports previous work by Spell and Frank (2000)
and McDonald and Saunders (2005)
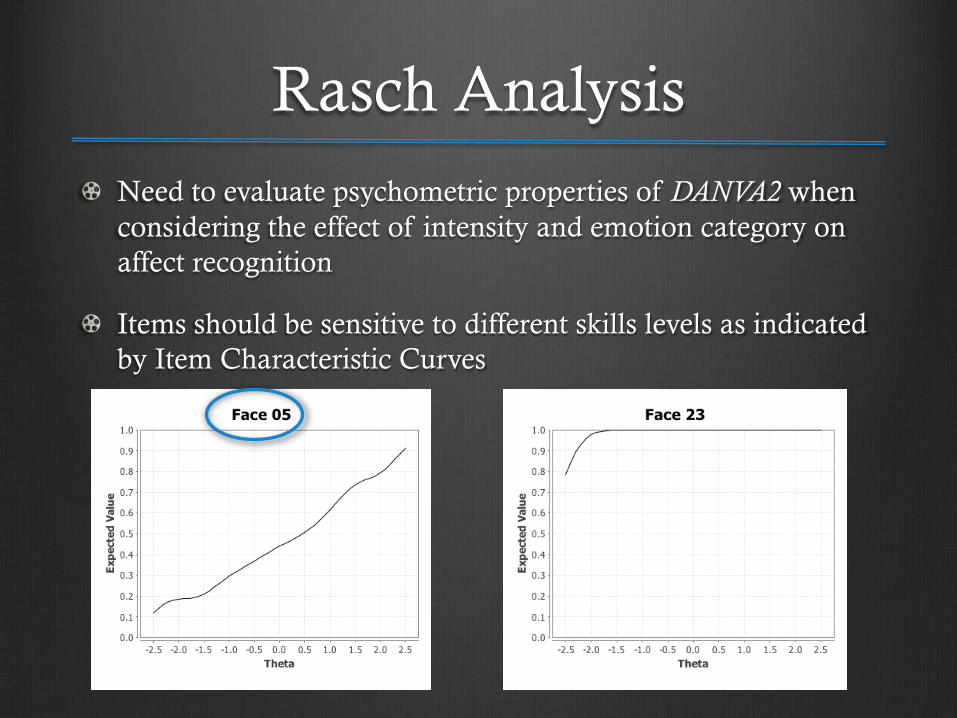
Rasch Analysis
Need to evaluate psychometric properties of DANVA2 when
considering the effect of intensity and emotion category on
affect recognition
Items should be sensitive to different skills levels as indicated
by Item Characteristic Curves
Happy
Fearful
Angry
Sad
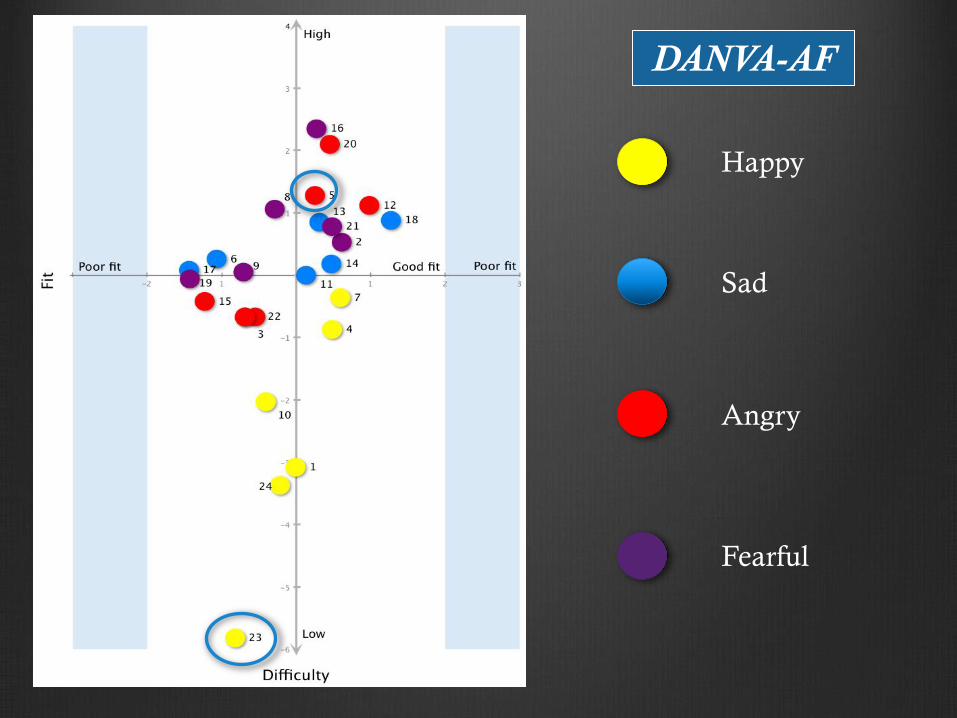
DANVA-AF
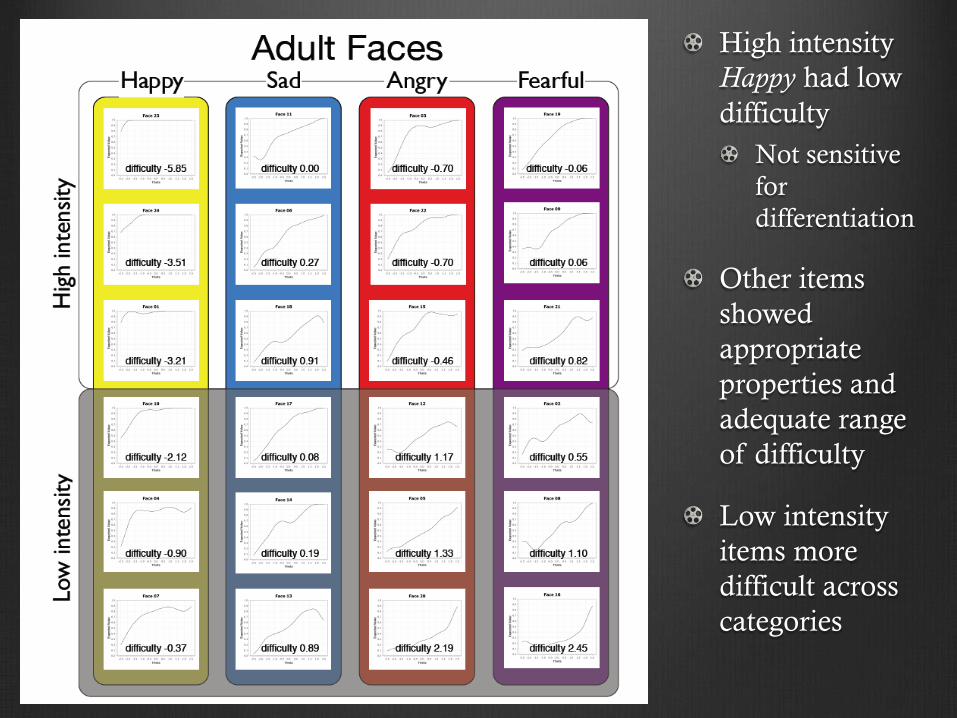
High intensity
Happy had low
difficulty
Not sensitive
for
differentiation
Other items
showed
appropriate
properties and
adequate range
of difficulty
Low intensity
items more
difficult across
categories

Happy
Fearful
Angry
Sad
DANVA-AP
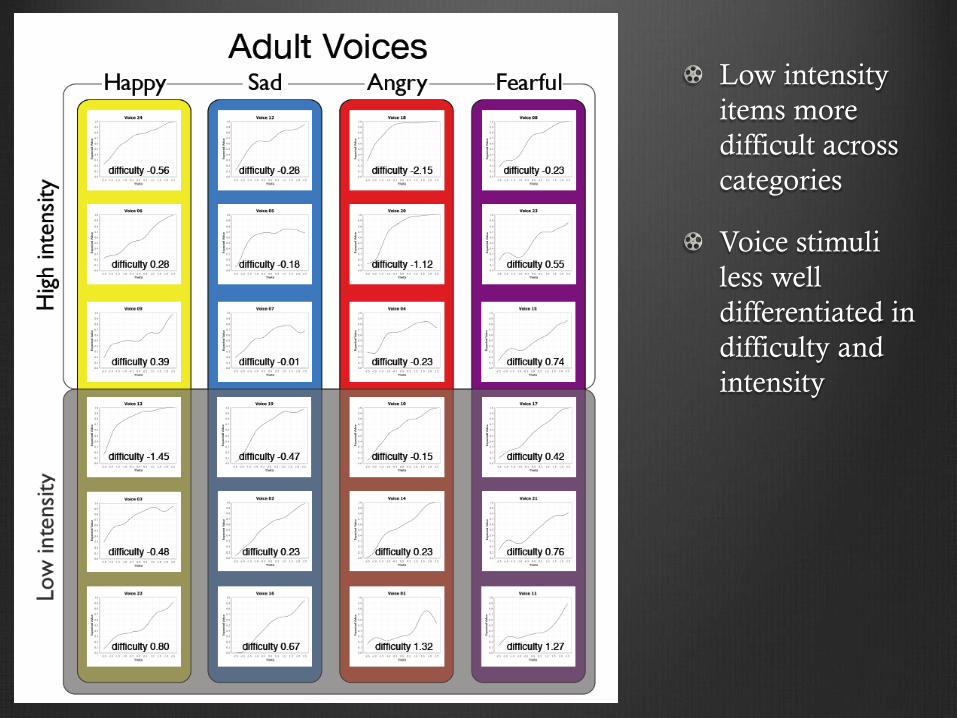
Low intensity
items more
difficult across
categories
Voice stimuli
less well
differentiated in
difficulty and
intensity
Conclusion
More than half of the 202 participants screened showed deficits in
the recognition of one or both modalities
Significantly more participants had difficulty with faces
Happy faces easier to identify than other emotions
No differentiation by emotion category for voices
High intensity expressions easier than low for both modalities
With the exception of high intensity Happy faces, the DANVA2
appears to provide a suitable range of difficulty to assess facial and
vocal affect recognition in people with moderate to severe TBI
References Babbage, D.R., Yim, J., Zupan, B., Neumann, D., Tomita, M.R., & Willer, B. (2011). Meta-analysis of facial affect recognition difficulties after traumatic
brain injury, Neuropsychology, 25(3), 277-285.
Dimoska, A., McDonald, S., Pell, M.C., Tate, R.L., & James, C.M. (2010). Recognizing vocal expressions of emotion in patients with social skills deficits following traumatic brain injury. Journal of International Neuropsychological Society, 16, 369-382.
Green, R.E.A., Turner, G.R., & Thompson, W.F. (2004). Deficits in facial emotion perception in adults with recent traumatic brain injury. Neuropsychologia, 42, 133-141.
Hopkins, M.J., Dywan, J., & Segalowitz, S.J. (2002). Altered electrodermal response to facial expression after closed head injury. Brain Injury, 16, 245-257.
Ietswaart, M., Milders, M., Crawford, J.R., Currie, D., Scott, C.L. (2008). Longitudianl aspects of emotion recognition in patients with traumatic brain injury. Neuropsychologica, 46, 148159.
McDonald, S., & Saunders, J.C. (2005). Differential impairment in recognition of emotion across different media in people with severe traumatic brain injury. Journal of the International Neuropsychological Society, 11, 392-299.
Milders, M., Fuchs, S., & Crawford, J.R. (2003). Neuropsychological impairments and changes in emotional and social behavior following severe traumatic brain injury. Journal of Clinical and Experimental Neuropsychology, 25(2), 157-172.
Nowicki, S. (2008). The Manual for the Receptive Tests of the Diagnostic Analysis of Nonverbal Accuracy 2 (DANVA 2). Atlanta, GA: Department of Psychology, Emory University.
Pell, M.D. (2006). Cerebral mechanisms for understanding emotional prosody in speech. Brain and Language, 96, 221-234.
Pell, M.D., & Baum, S.R. (1997). The ability to perceive and comprehend intonation in linguistic and affective contexts by brain-damaged adults. Brain and Language, 57, 80-99.
Pell, M.D., Jaywant, A., Monetta, L., & Kotz, S.A. (2011). Emotional speech processing: Disentangling the effects of prosody and semantic cues, Cognition and Emotion, 25(5), 834-853.
Spell, L.A., & Frank, E. (2000). Recognition of nonverbal communication of affect following traumatic brain injury. Journal of Nonverbal Behavior, 24(4), 285-300.