Embed Size (px)
Citation preview
Real-time tumor tracking with preprogrammed dynamic MLC motion and adaptive dose-rate
regulationB.Y Yi, S. Han-Oh, F. Lerma,
B. Berman, C. Yu
Outline
• Abstract• Introduction• Method and Its Assessment• Results• Discussion• Conclusion and Comments
Abstract
• A new method for real-time tumor tracking with dynamic MLC motion under condition of free breathing.
• The movement of the tumor is reflected in the pre-programmed MLC sequence, the irregular breathing during the treatment is handled by real-time regulation of dose rate. This is called Dose-rate-regulated-tracking (DRRT).
• The tracking error is less than 1mm from the evaluation of 13 patients.
Introduction• The effect of breathing-induced tumor motion is a
big challenge in radiotherapy.• Current Techniques:
Gating (Phys. Med. Biol. 41, 83–91 1996.) Breath hold (Instrum. Control Syst. 49, 199–204 2001.) Abdominal press (Med. Phys. 32, 3363–3366 2005.) Motion adaptive X-ray therapy (Phys. Med. Biol. 46, 1–10 2001.) Synchronized moving aperture radiation therapy
( SMART, Phys. Med. Biol. 48, 587–598 2003) Aperture maneuver with compelled breath ( AMC, Med.
Phys. 31, 760–766 2004. )
Introduction• For techniques involving MLC:
The Good: high treatment efficiency; distributing the normal tissue dose over a greater volume,
lower the dose burden to the skin and underlying structure. The Bad:
All need patients’ breathing pattern to be perfectly consistent with that used for planning.
Neither MAX-T nor SMART includes an effective method to compensate for irregular breathing, AMC relies on the patient’s active cooperation.
The Method and Its Assessment• The Principle of DRRT
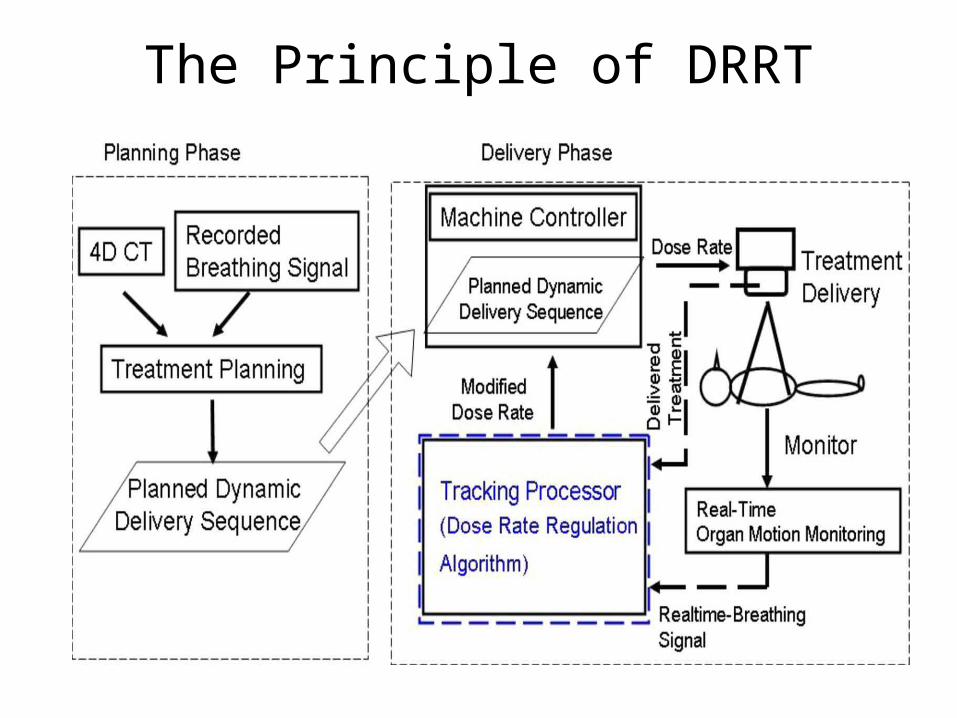
DRRT combines a preprogrammed delivery sequence and adaptive dose-regulation, which enables real-time temporal modification of MLC sequence.
Based on 4D CT simulation, the patient’s breathing signal can be recorded and the tumor position can be obtained. Assuming nominal dose rate, we can express the tumor position as a function of delivered MUs and design a MLC leaf sequence.
When irregular breathing happens, the accelerator dose rate is adaptively adjusted and DRRT effectively causes the machine to follow the patient.
The principle of DRRT• The planned motion tracking is expressed in terms of leaf
positions required to track the tumor as a function of the delivered MUs.
MLC motion from point A to point BΔMU=(Ib-Ia) *MU=ΔI*MUIndex I normalized to 1, so ΔI=ΔMU/MUAssume dose rate k, the treatment time from A to BΔt=ΔI*MU/kRewrite Δt*k=ΔI * MU = constant (The constraint)
• The breathing pattern is r times of that from planningΔt2=Δt/rSince index difference ΔI and total MU are constantK2*Δt2=k*ΔtSo the new dose rate is k2=rk
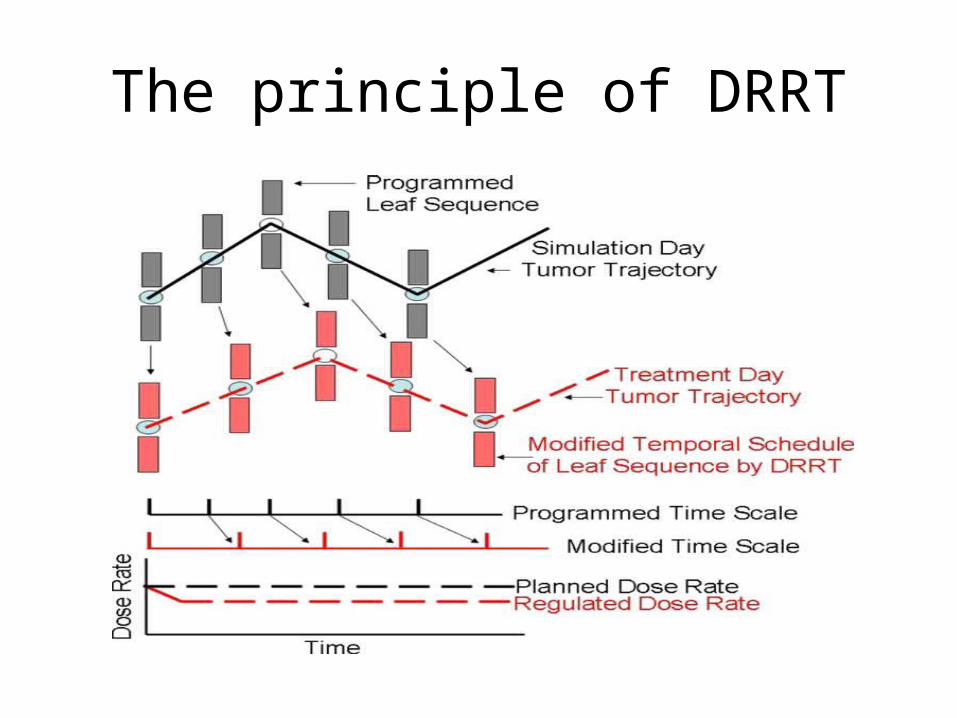
The principle of DRRT
The Principle of DRRT
Simulation and Tracking Error Evaluation
• Used RPM system to obtain patient breathing signal• Select patients based on– Peak to peak distance greater than 0.5cm– Relative std of the amplitude less than 20%
• Assumption: The tumor moves in exactly same manner as the reflective abdomen marker in one dimension
• The averaged breathing pattern was used to generate the preprogrammed MLC tracking sequence.
• The tracking and breathing signal are measured every 0.1 s, the beam dose rate is changed if the difference reaches a distance greater than 1mm.
Phantom experiments
• Phantom experiment to test DRRT• Converted a step-and-shoot intensity-modulated RT
(IMRT) plan to a dynamic tracking MLC sequence• Three cases:– The step-and-shoot IMRT– The dynamic-tracking MLC with phantom moving with
irregular frequency– The dose-rate-regulated dynamic tracking MLC with the
phantom moving irregularly• The frequency and dose rate were changed
simultaneously to achieve synchronization
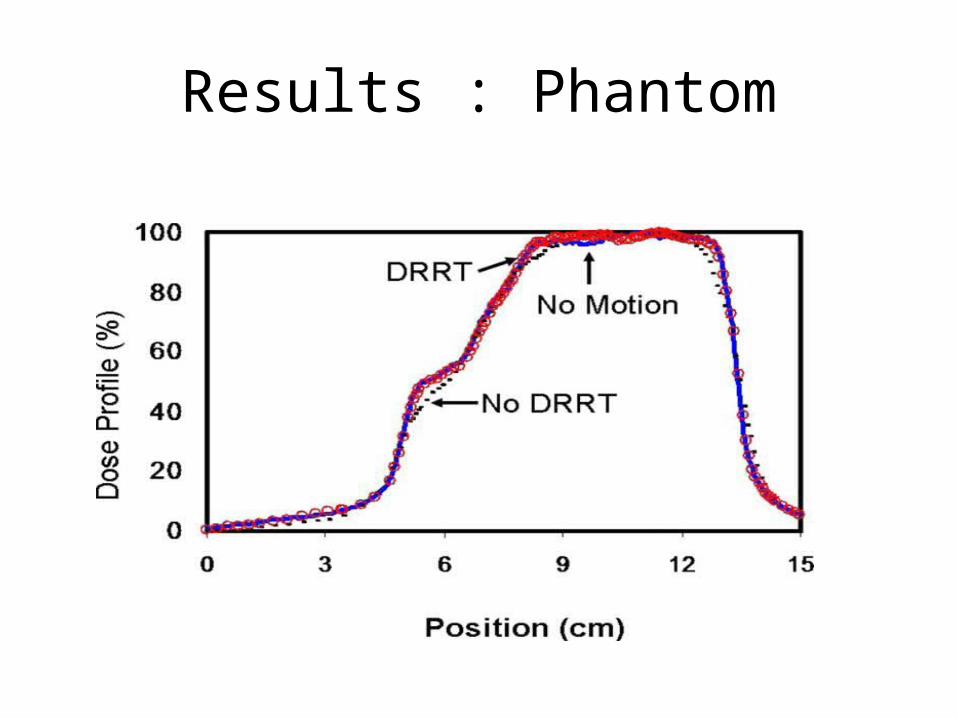
Results : Phantom
Results
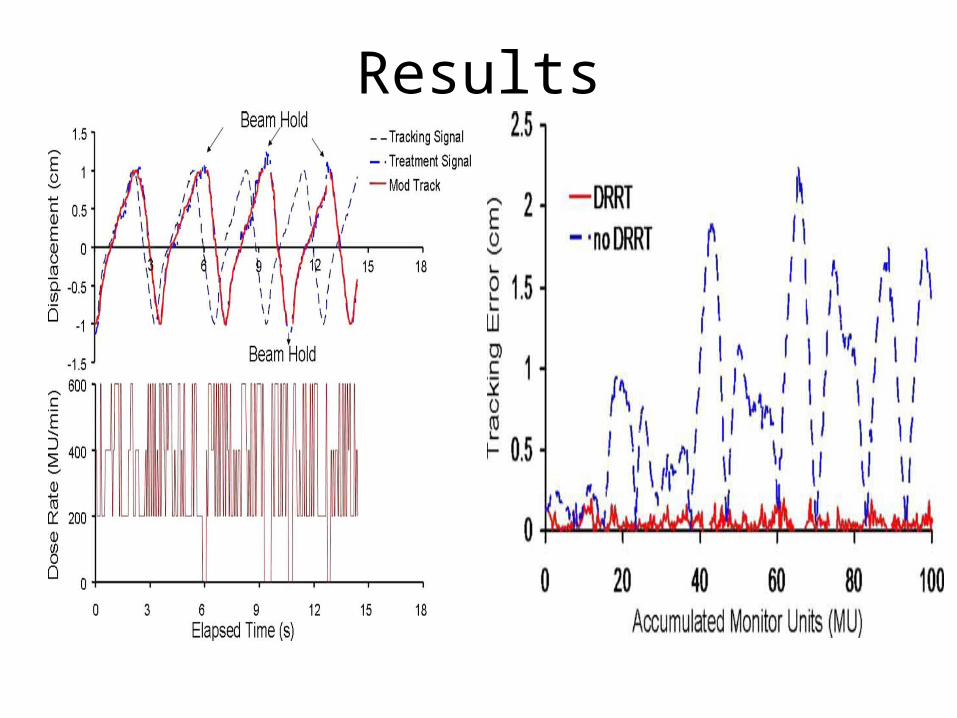
• Patient: Equate the normalized breathing pattern and the tumor location as a function of time, the tracking error becomes the difference between the tracking and the treatment breathing patterns. The tracking error is less than 1mm when the response time of the treatment machine on DRRT command is negligible.
Results
Discussions• Address two issues:– The tumor location is expressed as a function of breathing
phase ( or amplitude), handled with preprogrammed MLC– The irregularity of breathing as compared with that during
4D CT simulation, handled with DRRT• Assumptions: Fixed the relationship between the
tumor location and breathing pattern • If system time delay is less than 0.4s, the overall
tracking error is less than 2.2mm• DRRT method works for breathing irregularity in
breathing phase shift and breathing frequency variations, but less perfectly for breathing amplitude variation ( < 20% ).
Discussion
• DRRT vs DMLC (P. Keal)– DRRT allows one to track a tumor in real time with
commercially available MLC system– 2D tumor tracking is easier using DRRT, while DMLC using
1D motion– Radiation leakage can be minimized using DRRT by
designing tracking sequence prior to treatment, while the leaf end leakage in inevitable in DMLC
– Direct Visualization is essential in DMLC, not so for DRRT– A delivery leaf sequence is prepared before treatment.
DRRT treatment planning based on 4D CT, while DMLC is used with 3D planning.
Conclusion and Comments• The authors reported a new method for real-time tumor
tracking using existing MLC by using preprogrammed MLC sequence to track regular target motion and DRRT to handle irregular breathing pattern.
• Clinical challenges:– Dose rate control during treatment (hard to realize)– Online acquisition of patient breathing pattern, and breathing
prediction algorithm– Time delay in machine adjustment for dose rate change– Some base line shifts involving physiological changes may need
re-simulation and re-planning • Good approach but still not clinically applicable