Embed Size (px)
Citation preview

Re-DoubleRe-Double
Ron Teed, M.D. 12 January 2007 Vanderbilt Eye Institute Alfred Bielschowsky

Patient History IPatient History I
cc: vertical binocular diplopia 63 yo male with 4 week history of diplopia;
first intermittent, then constant Worse in right gaze No antecedent trauma, CVA, craniofacial
surgery No history strabismus No history thyroid disease, myasthenia

Patient History IIPatient History II
POH: none PMH: DJD, hernias Meds: ibuprofen FH: no ocular disease SH: tobacco use in past ROS: no dizziness, weakness, HA, jaw
claudication, fatigue, numbness, paresthesia

Differential Diagnosis ofDifferential Diagnosis ofVertical Binocular DiplopiaVertical Binocular Diplopia
Superior Oblique Palsy Thyroid Ophthalmopathy Myasthenia Gravis Brown Syndrome Orbital fracture with entrapment Cyclovertical paresis or overaction Skew Deviation/Ocular Tilt Dissociated Vertical Deviation

Exam IExam I General: alert and oriented; no anomalous head
posture; no nystagmus BCVA 20/20, 20/20 Fields: Full OU Tonometry: 15,14 Pupils: no rAPD, no anisocoria External Exam: no proptosis, ptosis, lid retraction;
no fatigue SLE: unremarkable, quiet eyes DFE: unremarkable, no optic nerve edema/pallor

VersionsVersions
+
0
0
0
0
0
0
0
0
0
0
0

MeasurementsMeasurements
0
5 LHT
8 LHT
3 LHT8 LHT
4 LHT 10 LHT

Additional ClinicalAdditional ClinicalTestsTests
“fourth step”– Measurement of ocular torsion– Double Maddox Rod: 5° excylotorsion OS
Vertical Fusional Amplitudes- Large amplitudes suggest congenital etiology- 3 prism diopters

Superior Oblique PalsySuperior Oblique Palsy
Clinical diagnosis from Three-step test What do we do now?

Superior Oblique PalsySuperior Oblique Palsy
Determine if this is a ISOLATED CN IVpalsy
No neurological symptoms on history Cursory neurological exam unremarkable

Isolated Superior Oblique PalsyIsolated Superior Oblique Palsy
Most common etiologies are congenital andtraumatic
Also vascular; less commonly tumor,demyelinating
In absence of other neurological symptomsand presence of vascular risk factors,reasonable to observe

Isolated Superior Oblique Palsy:Isolated Superior Oblique Palsy:Management PlanManagement Plan
Our patient did not have obvious vascularrisk factors other than age– No known HTN, hyperlipidemia, DM
Patient was observed– To return if diplopia changes, ptosis develops,
or he has any numbness, weakness,paresthesias, disorientation, unsteadiness,vertigo, headache

Patient Follow-upPatient Follow-up
Pt returns 8 weeks later “double vision is a bit better…” “…ever since I had the radiation treatment”

Follow Up ExamFollow Up Exam
0
2 LHT
4 LHT
5 LHT5 LHT
10 LHT 8 LHT
DMR: 5° excylotorsion OS

More HistoryMore History
A few weeks after first visit, pt developedunsteady gait, disequilibrium associatedwith flank pain
No longer isolated fourth nerve palsy– Measurements no longer map to superior
oblique palsy Now what do we think is going on? Now what would we do?

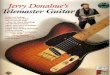
ImagingImaging
CT
MRI

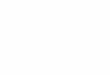
Vertical Vertical DiplopiaDiplopia and Pontine and PontineMassMass
Does this lesion explain vertical diplopia?– Lesion to CN IV nucleus or nerve?– Lesion to other pathways encoding vertical
gaze?

Back to the originalBack to the originalpresentationpresentation
Was it right to observe an apparent isolated CN IVpalsy?– Texts, review articles suggest that observation is
acceptable, particularly if the palsy is suspected to becongenital, traumatic, or there is a vascular risk factor
– Spontaneous resolution of CN IV palsy occurs within 3months in 50-95% of patients (better in presumedvascular etiology)
– Up to one third have undetermined etiology

Watching the CN IV palsyWatching the CN IV palsy
“evaluation for an isolated fourth nerve palsyusually yields little information... Older patientsshould be followed” (BCS, Neuro-ophthalmology)
“MRI…for all patients younger than 45 years withno definite history of significant head trauma, andpatients aged 45 to 55 years with no vasculopathicrisk factors or trauma” (Wills Eye Manual)

The EvidenceThe Evidence
Multiple case series of presumed isolated CN IVpalsies– No documented tumors as etiology (Keane 1993: 0/81)– But may fail to adequately confirm true isolation or
confirm true CN IV palsy Lee et al (1998) reviewed cost-effectiveness of
imaging– No need to image suspected congenital, traumatic, or
vasculopathic palsies

The RebuttalThe Rebuttal
A few case reports of isolated CN IV palsies frombrainstem strokes
Feinberg and Newman (1999): 6/68 isolated CNIV palsies related to trochlear nerve Schwannoma
Scattered other reports of isolated CN IV palsyfrom other conditions:– Pituitary macroadenoma– MS, polycythemia rubra

So what do we do?So what do we do?
What is your level of comfort? How good is your neurological exam?
Reasonable and cost-effective to observe,but you may miss an important lesion

Take Home PointsTake Home Points
Determine if an apparent superior obliquepalsy is truly isolated
If isolated, it may be reasonable to observe Understand basic anatomy of the pathways
encoding vertical eye movements

ReferencesReferences Brodsky MC, Donahue SP, Vaphiades M, and Brandt T (2006). Skew
Deviation Revisited. Survey of Ophthalmology. 51:105-128. Donahue SP, Lavin PJM, and Hamed LM (1999). Tonic Ocular Tilt Reaction
simulating a superior oblique palsy. Archives of Ophthalmology. 117:347-352. Feinberg AS and Newman NJ (1999) Scwannoma in patients with isolated
unilateral trochlear nerve palsy. American Journal of Ophthalmology 127:183-88.
Keane JR (1993). Fourth nerve palsy: Historical review and study of 215inpatients. Neurology. 43:2439-2443.
Kusher BJ (1989). Errors in the Three-Step Test in the Diagnosis of VerticalStrabismus. Ophthalmology. 96:127-132.
Lee AG, Hayman LA, Beaver HA, et al (1999). A guide to the evaluation offourth cranial nerve palsies. Strabismus 6(4): 191-200.
Petermann SH and Newman NJ (1999). Pituitary Macroadenoma manifestingas an isolated fourth nerve palsy. American Journal of Ophthalmology127:235-6.
Thomke F and Ringle K (1999). Isolated superior oblique palsies withbrainstem lesions. Neurology. 53(5):1126-27.

CTCT
.

T1 MRIT1 MRI

T2 MRIT2 MRI

AxialAxial
.

CN IV nucleusCN IV nucleus

OtolithicOtolithic Pathways Pathways