Embed Size (px)
Citation preview

A. SPECIFIC AIMS. This application is from investigators at five Michigan institutions with expertise in the conduct of longitudinal cohort studies initiated in early pregnancy, in environmental and nutritional assessment, and in measurement of the four ECHO health outcomes. We have two cohorts totaling nearly 1,000 women enrolled, interviewed and sampled early in pregnancy (most before 14 weeks) with serum, plasma and urine aliquoted and frozen at -80°C. A 3rd cohort is expanding the larger of our two cohorts from a convenience sample to a statewide probability sample of 10 Michigan hospitals and 20 prenatal clinics, in which recruitment is well underway (n = 82) with an intended final enrollment of 1,000 pregnancies. The expanded cohort will have advanced placental studies and microbiome collection among other enhancements, permitting fuller assessment of our study hypotheses, and providing a richer resource to the ECHO consortium. We are in contact with more than 84% of cohort families. With parental consent, we will use newborn dried blood spots (NDBS) from the Michigan Neonatal Biobank (MNB), retained after genetic screening since 1987, and frozen at -20°C since 2009. With these spots, we can quantify exposures, examine epigenomic changes, and, by accessing both the child’s and the mother’s newborn spots, study environmental effects across generations, including in Flint, MI where we will examine the effects of recent water contamination on fetus and child. Our organizing principle is that for many environmental exposures we study – toxic, nutritional, inflammatory - the most sensitive period of risk for child health is pregnancy and the perinatal period, and that these exposures are best ascertained from maternal self-report, biological specimens and objective environmental data collected during pregnancy and immediately after birth. We hypothesize that these exposures interact with each other and with host characteristics in their effects on outcomes, and may be mediated by epigenetic changes identifiable on NDBS and in some cases, by the placenta and the infant microbiome. Aims and hypotheses will be examined in relation to perinatal outcomes, obesity, and neurodevelopment (mainly at age 4), all examined within the psychosocial context of the family. Asthma will not be a primary target, but we have the capacity to assess asthma if required in the UH3 phase. We set out several focused exemplary hypotheses below. UG3 PHASE: We will re-contact families with children in our cohorts to consent them for new studies and to enhance follow-up rates beyond 84%. We will conduct pilot studies of new procedures, and assess hypotheses in 125 children. UH3 PHASE: We will test our hypotheses in all mother-infant pairs with assessment at age 4 or above. POOLED COHORT: The application describes how our hypotheses can be integrated into the pooled cohort AIM 1: To determine the effects of persistent organic pollutants (POPs) and heavy metals assessed across two generations, on cognitive outcomes. We hypothesize that (1a) in utero exposure to POPs/metals will be associated with increased risk, especially in poor families; (1b) effects identified in hypothesis 1a will be mediated by epigenetic changes measured on NDBS; (1c) grand-maternal exposure to POPS/metals (measured on mother’s blood spot when she was a newborn) will amplify the effects identified in 1a and 1b; and (1d) recent in utero lead exposure in Flint, MI, as assessed in NDBS, and in the shed teeth of exposed children, will be associated with epigenetic changes and impaired cognitive outcomes. AIM 2: To assess the effect of maternal nutritional and weight status in pregnancy on cognitive outcomes and childhood obesity. We hypothesize that (2a) low pregnancy iodine and/or iron status, agents interfering with thyroid iodine uptake (perchlorate, thiocyanate), and abnormal thyroid hormone function will be associated with adverse cognitive outcomes; (2b) pregnancy-related weight and social circumstances will be linked to childhood obesity and will amplify associations found in hypothesis 2a; and (2c) the exposure → outcome effects found in 2a and 2b will be mediated by differences in the infant gut microbiome and infant feeding patterns. AIM 3: To assess the effects of pregnancy viral infection and weight-associated inflammation in placenta and NDBS, on perinatal outcomes and behavior related to the autism spectrum. We hypothesize that (3a) increasing maternal BMI and/or viral infection, with neonatal inflammation, will be associated with heightened indicators of autism risk at ages two and four. (3b) viral infections and maternal obesity most strongly associated with placental inflammation will have the strongest relationships with autism-like behaviors (3c) Maternal/placental viral infection will induce a heightened inflammatory response to placental microflora at the maternal-fetal interface, identified in a subset of frozen placentas. Interactions of all hypotheses in this aim will be examined in relation to maternal and infant antibiotic use and the infant gut microbiome.
Specific Aims Page 415
Contact PD/PI: Paneth, Nigel S

A. SIGNIFICANCE 1. EXPLORING THE FETAL ENVIRONMENT: Interest in the fetal origins of childhood disease preceded1
the more recent interest in the fetal origins of adult disease.2 Yet we have only limited information on the nature of the in utero environmental exposures that leave a lasting imprint on a child’s risk of disease, largely because by the time a childhood disorder is ascertained, pregnancy is over, and can only be examined by maternal recall or use of medical records. The scientific premise underlying our aims is that careful and detailed exploration of the biological and social environment of pregnancy is the best strategy for uncovering underlying causes of ECHO outcomes, especially the neurodevelopmental disorders, none of which have declined in frequency for the past 50 years. Our experienced investigators will use the latest scientific techniques to address plausible mechanisms for in utero harm to the developing fetal brain and other organs.
2. POPULATION-BASED RESEARCH: An important component of our effort is the population-based pregnancy cohort we are building in our state. For cohort studies, it is widely accepted that the population-based study provides more generalizable conclusions than do cohorts derived from convenience samples. Indeed, we think that our probability sample of pregnancies can validate hypotheses uncovered in convenience samples, not just our own, but also in other ECHO cohorts. We also have access to a population-based biological sample – the archived newborn dried blood spot (NDBS). In previous research, including our current ARCH cohort (see below) we have received written consent to examine this spot from more than 95% of participants. We can thus examine hypotheses requiring the blood spot with excellent generalizability.
3. STATISTICAL POWER: We anticipate having a cohort of 2,000 pregnancies for the ECHO consortium. Nearly all mother-child pairs will have early prenatal blood and urine specimens, and subsets will have other specimens. This is sample size provides excellent power to address our Aims.
4. ADDRESSING A MAJOR ENVIRONMENTAL CONTAMINATION EPISODE: We are in a position to assess one component of the recent environmental contamination of water in Flint - the extent of in-utero, infant and early childhood contamination with lead and other substances leached from the Flint water by studying maternal lead levels, NDBS and shed teeth of exposed children. Because we will also evaluate psychosocial factors in the women we recruit, we will be able to contextualize environmental contamination among the overall range of stressors to which Flint women and children are subject.
5. ENGAGING MANY INVESTIGATORS AND DISCIPLINES: The institutions represented in this application (the Henry Ford Health Center (HFHS), the Michigan Department of Health and Human Services (MDHHS), Michigan State University (MSU), the University of Michigan (U of M) and Wayne State University (WSU) account for >95% of all NIH research funding in Michigan. Our science reflects a wide range of biological, social, mathematical and clinical disciplines, from junior to senior (ensuring continuity) and prioritizes collaboration and the study of interactions among our several aims, which will not be pursued in isolation from each other. Our strong state position makes it likely that the policy implications of our work for Michigan will be attended to, and we place a major emphasis on dissemination of results to policymakers and the public.
B. INNOVATION 1. USE OF ARCHIVED NEWBORN BLOOD SPOTS: Few studies in the US have taken full advantage of
the millions of NDBS archived in many states. Legitimate concerns with privacy and consent have often made it difficult to use this extraordinary resource for understanding child health. Michigan, however, has been prominent in addressing these problems, and in satisfying the residents of our state that the NDBS archive will be used appropriately for science and medicine. Several members of our team have shown, often despite considerable skepticism, how much information on environmental agents, epigenomic alterations, and gene expression can reliably and validly be obtained from this universally collected biological matrix.
2. ENVIRONMENTAL EXPOSURE IN TWO GENERATIONS: Because the MNB has an archive of NDBS extending back to 1987, we can show effects of environmental toxins operating across two generations. As we continue to recruit pregnancies, the number of mothers with archived NDBS will increase.
3. INCORPORATING BODY COMPOSITION: Our approach to obesity is based on more than just body mass index. Few studies, like ours, incorporate measures of body composition into assessments of both mothers and children. Also rarely measured are all 3 components of pregnancy-related weight,3 - pre-pregnancy weight, pregnancy weight gain, and post-partum weight loss – all to be assessed in this study.
Research Strategy Page 416
Contact PD/PI: Paneth, Nigel S

4. VIRAL STUDIES IN PREGNANCY AND PLACENTA: The acceptance of the Fetal Inflammatory Response Syndrome4 as a factor in both preterm delivery and neurodevelopmental difficulties in children has focused the attention of the biomedical world on bacterial infections in pregnancy and their effects. The role of viruses, either direct, or via stimulation of bacterial processes, has been much less investigated. We plan to systematically study evidence of in-utero viral infection with placental inflammation and with later outcomes.
5. QUANTITATIVE APPROACHES TO THE PLACENTA: We introduce the first large scale application of a quantitative imaging approach to assessing placental shape and the branching of both large surface and fine interior blood vessels of the placenta, characteristics that have been linked to pregnancy inflammation5 6 and, in pilot work, to risk of autism spectrum disorder (ASD).7 D. APPROACH The remainder of this application is in four parts: • Pages 3-10. Background to the study, including a description of our cohorts, our research expertise, and the special circumstances in Michigan relevant to this research (Sections D1 – D3). • Pages 10-16 A description of our overall approach to the research – scientific rigor, organization of our consortium, division of work into UG3/UH3 phases including transition metrics and contributions to the ECHO pooled cohort, dissemination of results, ethical considerations and biostorage (D4). • Pages 16-20 Our general data collection approaches including cost-efficiencies, recruitment and cohort maintenance, and assessment of ECHO outcomes and exposures that apply to all aims (D5). • Pages 20-30. Elaboration of our 3 aims and their hypotheses, including their rationale, the exposures, mediators and effect modifiers to be measured, and the statistical analysis section (D6,7). D1. COHORT DESCRIPTIONS
a. WHY COHORTS INITIATED IN EARLY PREGNANCY ARE SO IMPORTANT: For outcomes ascertained at birth or earlier, such as preterm birth or fetal growth impairment, the entire exposure matrix must be prenatal by definition. The risk of neurodevelopmental disorders is affected in important ways by prenatal infections (e.g. cytomegalovirus, rubella), nutrient deficiencies (e.g. iodine, folate), and chemical agents (e.g. phenytoin, methylmercury), several of which exert their strongest effect early in pregnancy, when organs are in formation. This basic insight has guided our interest in developing pregnancy cohorts in Michigan. While a cohort assembled in infancy cannot obtain pregnancy specimens, a pregnancy cohort can assess later infant and child exposures. The pregnancy cohorts described below include ongoing pregnancy enrollment, providing a great advantage to the ECHO program, allowing ECHO to choose exposures to measure in pregnancy, at birth, in infancy or in childhood that may not have been measured in earlier protocols.
b. ARCH – THE ARCHIVE FOR RESEARCH IN CHILD HEALTH: Since 2008, supported primarily by internal funds from MSU, ARCH (PI – Nigel Paneth) has enrolled 836 women in two (at times, three) Lansing prenatal clinics. Exclusions were age < 18 years and inability to be interviewed in English. The goal of ARCH is to incorporate collection of research-quality data into routine prenatal care, without a large investment of resources. Efficiencies in research are key. Women are informed of ARCH when they make their first appointment for their first prenatal visit, and are consented and enrolled at first visit. The mean gestational age (GA) of enrollment is 13.1 weeks. The research protocol has four core elements: 1. Consent, enrollment and interview at the first prenatal visit. 2. Permission to access state-archived data on pregnancy and birth:
• The confidential portion of the birth certificate (100 perinatal variables) • Maternal/infant hospital discharge abstracts (diagnoses, procedures, length of stay) • The newborn blood spot archived after genetic screening. • Medical records, but we reserve these for amplification of diagnoses and for sub-studies.
3. Storage of biological specimens. The laboratory serving the clinics sets aside an extra red top (plain) and lavender top (k2EDTA) tube at the first prenatal blood draw and at the routine 24-28 week glucose tolerance test. Blood and urine samples are divided into multiple 250-µL aliquots for repeated retrieval and analysis; mean N of aliquots stored per collection is 11.3 for serum, 11.0 for plasma and 29.7 for urine. Maternal serum, plasma, blood lysate, filter paper (5 x 0.5 cm2 spots) and urine aliquots are frozen at -80°C. Having the clinical laboratory obtain blood is both less costly and more acceptable to participants than arranging separate phlebotomies for research. A sample of placental cord, parenchyma and membrane is stored in formalin,
Research Strategy Page 417
Contact PD/PI: Paneth, Nigel S

whenever possible (n = 185). Urine collections were the first collection initiated in ARCH, with blood collections only starting after some 6-9 months of recruitment. Thus blood collections are less complete than urine. 4. Follow-up of families is by telephone at one month, and annually (re-consented for five more years at age
5), with assessment of child development, and recording of new illnesses and diagnoses.
Item 2 in the new rigor and transparency requirements for NIH applications is “rigorous experimental design for robust and unbiased results”. Although this cohort is derived from a convenience sample of clinics in Lansing, MI, several of its procedures enhance “robust and unbiased results”, including: 1. The clinics from which we recruit are general population clinics not targeted to women at high risk. 2. All forms of payment are accepted in the clinics from which we recruit, so there is limited selection of
patients for socio-economic status. 3. The only exclusions are for age below 18, and not-speaking English (<5% of our sample). 4. We enroll at first prenatal visit whenever it occurs, even if late in gestation 5. We maintain a descriptive log of women approached in the clinic who refuse enrollment, including also the
reasons for refusal. Our acceptance rate (women enrolled divided by women approached for participation) has ranged between 60-70% over the duration of the study.
6. We have had post-natal contact with 85.2% of the ARCH cohort after birth, most multiple times. Contacts are kept up to date. 88.2% of women followed have been interviewed at least once since 2014; nearly a third of all participants have had a follow up interview so far in 2016.
7. Our sample size is large enough to provide power for many important exposure-outcome relationships. 8. The design of our study focuses on prospective, real-time data collection. The information we obtain about
pregnancy exposures is not dependent on the memory of the mother. 9. Much of our data (e.g. birth certificates, hospital abstracts) is obtained from a single statewide source and
thus less subject to the variability of different data collection systems. 10. We aliquot multiple specimens from each blood (µ = 22 aliquots) and urine (µ = 30 aliquots) sample,
avoiding freeze-thaw cycles and making pooling with other ECHO cohorts more feasible. ARCH has generated several sub-studies funded by other sources (Table 1). Each sub-study adds to the ARCH database. In one study, 100 3-5 year olds have been assessed for neurodevelopment using the NIH tool kit, and BMI and body composition (by impedance) is obtained on mothers and children. Other ARCH sub-studies investigate the relationship of the placental microbiome to inflammation, the evolution of the infant gut microbiome in relation to the maternal gut microbiome, and physical activity, maternal cholesterol and fetal growth. The last of these studies is supported by NIH. The cohort has served as a resource for several masters and doctoral theses.8 9 10
c. MMIP – THE MICHIGAN MOTHER-INFANT PAIR STUDY: Since 2012, supported largely by internal funds from the U of M, MMIP (PI – Vasantha Padmanabhan) has enrolled 136 subjects at first prenatal visit to the UM Women’s Hospital clinic with GA at enrollment limited to 8-14 weeks. Exclusion criteria were age < 18 years, infertility treatment and multiple fetuses. At this initial visit, participants had blood drawn, urine samples collected, and participants completed a one-page questionnaire on socio-demographic factors, health behaviors, food consumption, personal care product use and other items (see Table 2). Women were re-contacted between 34 to 38 weeks of pregnancy and provided study materials for blood and urine collection upon admission in labor. After delivery of the placenta, cord blood samples were collected via venipuncture from the umbilical cord, which was clamped proximal to the placenta. For the two maternal blood samples and the cord blood sample, four tubes were collected, each aliquoted into 4 samples: an 8.5ml PAXgene DNA tube; a 2.5 ml PAXgene blood RNA tube; and two 5ml lavender-top k2 EDTA tubes (7 ml for cord blood). Genomic DNA and RNA were extracted from leukocytes in PAXgene blood collection tubes using the PAXgene Blood RNA / DNA Kits (PreAnalytiX/Qiagen, Hombrechtikon, Switzerland) in a subset; others are awaiting extraction.
Table 1: ARCH SUB-STUDIES NAME SUB-STUDY FOCUS FUNDING
ARCH CHILD DEVELOPMENT
Maternal obesity/fat mass, prenatal urinary iodide levels and child development
MSU RAIND Institute
ARCH GUT The maternal/infant gut microbiome and infant allergy
Start-up funds
IUGR/ENDOGLIN 1st trimester beta-endoglin and IUGR Hospital funds
ARCH PLACENTA The placental microbiome and inflammation Start-up funds ARCH MISCARRIAGE
Pre-miscarriage immunologic findings in miscarrying and term pregnancies
Scored at 26th percentile
ARCH PALS The association of physical activity and lipid levels in each trimester to IUGR
1R03 HD073275
Research Strategy Page 418
Contact PD/PI: Paneth, Nigel S

Analysis of data from MMIP has been supported by two NIH grants (ES016541 [V Padmanabhan, PI ] and P01 ES022844 [K Peterson, PI])
The socio-demographic characteristics of the two cohorts differ considerably (Table 3). MMIP participants are older, wealthier and more educated than those of ARCH. This kind of difference, which will be seen across many ECHO cohorts, underlines the value of probability sampling in creating cohorts.
d. MARCH – THE MICHIGAN ARCHIVE FOR RESEARCH IN CHILD HEALTH: MARCH extends the cost-efficient modalities of ARCH from a convenience sample in one city to a probability-based sample that closely reflects the pregnant population of Michigan. Three scientific reasons underlie this expansion. The first is that, in keeping with the rigor and transparency requirements for NIH applications, no better experimental design exists for observational research than the population-based prospective cohort study. The advantages derived from recruiting a population-based sample include accurate estimation of the probability of outcome in relation to exposure, and unbiased estimates of relative risk. Meta-analyses of exposure-outcome relationships often find different odds ratios in convenience samples than in population-based cohorts, especially for non-genomic risk factors.11 12 13 For this reason, many meta-analyses include only population-based studies. Even more importantly, the frequency of conditions ascertained in MARCH – whether outcomes or exposures – are generalizable to our state, and can serve as the basis for public policy choices and priorities. This feature of probability-based sampling is widely acknowledged, and is the basis of all political polling and surveys. The second reason for expanding the ARCH cohort is to fulfill the goals of our aims and hypotheses, which require assessment of the infant microbiome, the placenta, shed primary teeth, more extensive interviewing in pregnancy, and far more detailed and comprehensive assessment of outcomes. A third reason is to have greater statistical power, both to investigate our own aims in the UH3 phase and for the pooled ECHO cohort. In the January 14, 2016 webinar, Dr. Tabak, responding to a questioner who asked: “Will ECHO support collection of new subjects and supplement an existing cohort?” stated “Yes, it’s possible. Again, the applicant would have to justify what unique questions will be made possible to answer by adding an additional subject”. In the webinar of February 1, 2016, in response to a question “Can cohorts or potential cohorts that are already under recruitment be expanded if needed to address our new cohort specific gains and/or extend recruiting to new sites to broaden the diversity of the cohorts? Dr. Tabak answered “the answer to both questions is yes. Again, obviously driven by the scientific questions that are being posed. But in both instances that could be an appropriate use of funds by ECHO.” A follow-up conversation with Dr. Carole Blaisdell of NHLBI confirmed that such recruitment could take place in the UG3 phase. The plan for a statewide pregnancy cohort evolved from the work of the Michigan Alliance for the National Children’s Study (MANCS), in which we recruited pregnant women living in 15 sampled segments in Wayne
Table 2. DATA ROUTINELY COLLECTED IN ARCH AND MMIP ARCH MMIP
Prenatal Physical activity; diet; depression scale; spousal abuse; PUQE scale (emesis), permission to access records and NDBS, urine in each trimester, plasma, serum, maternal DBS in 1st and 2nd trimesters
landfill exposure, canned food /fast food/vegetable usage, dental fillings, usage of personal care products, stress perception. Consent to re-contact after birth. 1st trimester plasma, serum, urine
Birth Placental sample; birth certificate and hospital discharge abstract data
Maternal blood & urine during labor, cord blood samples.
Postatal Telephone interview at 1 month and annually: child health; developmental milestones; infant feeding. Consent to re-contact every five years.
Email and phone contact with participants
Both cohorts collect maternal age, marital status, parity, gravidity, race, ethnicity, height, weight, income, education, smoking status; infant sex, birthweight, gestational age, Apgar score, delivery type.
SAMPLED HOSPITALS DETROIT AREA
Hutzel, Detroit Oakwood, Dearborn St. John, Novi St. Joseph Mercy, Ann Arbor Sinai Grace, Detroit U of Michigan, Ann Arbor
REST OF STATE Covenant, Saginaw Munson, Traverse City Spectrum, Grand Rapids Sturgis, Sturgis
Traverse City
Saginaw
Grand Rapids
Sturgis Detroit Area
Research Strategy Page 419
Contact PD/PI: Paneth, Nigel S

County in their prenatal care provider’s offices. These segments accounted for just 2% of county births, but were spread widely around Wayne; residents of the segments used nearly all 150 prenatal provider groups in the county and 28 different hospitals for delivery. In spite of this difficulty, we enrolled 75% of all
geographically eligible women identified in prenatal care. We scanned prenatal care rosters of the 73 largest practices for addresses. Of women approached in clinics by providers, 81% gave permission for us to speak to them, among whom we successfully arranged a home visit in 92%. We visited 116 eligible women in their homes, largely African-American women in Detroit, and obtained consent and participation from all 116. Of scheduled 12-month interviews, 99% were completed in the time window.14 Our success, coupled with the recognition that the goals of the NCS had not been achieved, persuaded us to remain an alliance, and we made plans to design a study in our state that could address, on a smaller scale, many of the issues that engaged the NCS. As in the original design of the NCS, we sought to enroll a probability sample derived from virtually all pregnancies in our state. In pursuit of that objective, in 2014, we began to form a 15-member executive committee, representing the five institutions participating in this application, and in 2015, created a 12-member advisory council of leading administrative figures in health. The state’s Chief Medical Executive, Eden Wells MD MPH serves on our executive committee, and Susan Moran, Deputy Director, Population Health and Community Services for MDHHS,
serves on our advisory council. With support from the University Research Corridor, an institution that supports collaborative initiatives across state universities, we received funding to sample hospitals and clinics in the lower peninsula of Michigan (97% of the state’s population) and to engage hospitals and clinics to create a diverse, representative, probability-based sample of state pregnancies for research. The UM Survey Research Organization (SRO), under the leadership of co-PI Michael Elliott, and using data provided on the location of births and the names of all birth attendants by co-PI Glenn Copeland of MDHHS, drew a stratified random sample of 10 of the 84 hospitals in lower Michigan. A back-up sample of another 10 hospitals was drawn. Hospitals were divided into quintiles by percent African-American births and two hospitals were randomly selected (selection probability proportional to size) from each of the five strata. We grouped all birth attendants (from birth certificates) into their prenatal practices and selected, also using a proportional to size algorithm, two practices that deliver largely or exclusively in the sampled hospitals. Using funds provided by MSU, we have begun recruitment for MARCH in four communities – Grand Rapids, Detroit, Flint and Traverse City. As of April 11, 2016, 82 participants have been enrolled.
e. SPECIAL FLINT COHORT: In April 2014, Flint, Michigan, under state-appointed emergency management, changed its water supply from Detroit-supplied Lake Huron water to the Flint River as a temporary measure, awaiting a new pipeline to Lake Huron in 2016. Intended to save money, the change in source water severed a 50-year relationship with the Detroit Water and Sewage Department (DWS). Shortly after the switch to Flint River water, residents voiced concerns regarding water color, taste, and odor, and various health complaints including skin rashes. Water from the DWS did not corrode lead in pipes as indicated by low chloride, low chloride-to-sulfate mass ratio, and presence of an orthophosphate corrosion inhibitor. By contrast, Flint River water had high chloride, high chloride-to-sulfate mass ratio, and no corrosion inhibitor. The
Table 3: ARCH, MMIP AND MARCH COHORTS PARTICIPANT CHARACTERISTICS (ARCH, MMIP)
ARCH* (n = 786)
MMIP (n = 136)
Mean age at enrollment (years) 25.5 31.3 Ethnicity African-American 28.0% 4.8%
Hispanic 14.8% 0.8% Education > College graduate 18.3% 80.2%
Some College 33.0% 18.8% High school graduate 32.4%
< high school 16.3% Income < $25,000 69.0% 11.8%
$25,000-$49,999 20.6% 12.1% $50,000-$74,999 5.7% 14.4% > $75,000 5.3% 62.1%
Gestational age
at first visit (weeks) 13.2 11.8 at birth (weeks) 38.9 39.3
Birthweight (grams) 3,285 3,438 Pre-eclampsia 5.2% 5.9%
Gestational Diabetes 2.6% 2.2% SPECIMEN AVAILABILITY (ARCH, MMIP, MARCH)
Adding 82 MARCH participants to 836 ARCH and 136 MMIP = 1,054 enrolled
ELIGIBLE AVAILABLE
First visit blood 1,054 808 (77%) First visit urine 1,054 993 (94%) 2nd trimester blood* 794 375 (47%) 2nd trimester urine* 794 453 (57%) 3rd trimester urine* 786 456 (58%) Labor blood 136 136 (100%) Cord blood 136 136 (100%) *42 fetal losses excluded from 2nd trimester counts and 50 losses from 3rd trimester counts and from N of ARCH participants. First visit blood, urine from all cohorts. Second trimester bloods and urine from ARCH. Labor and cord samples from MMIP.
Research Strategy Page 420
Contact PD/PI: Paneth, Nigel S

aging Flint water distribution system contains a high percentage of lead pipes and lead plumbing, with estimates of lead service lines ranging from 10% to 80%. Switching from Detroit’s Lake Huron to Flint River water thus created a perfect storm for lead and other toxins leaching into drinking water. In a 2016 AJPH cover article, co-investigator Hanna-Attisha and colleagues showed that the increased water lead levels in Flint after the switch correlated with increased blood levels15 Hurley hospital in Flint and two of its affiliated clinics were in the back-up hospital sample, and are included as special additions to MARCH.
f. MICHIGAN COHORTS COMBINED: The number of pregnancies enrolled thus far in our three cohorts is: ARCH - 836; MMIP – 136; MARCH – 73, totaling 1,045 pregnancies whose offspring range from newborns to age 7 (Table 3). We know of 50 fetal losses and 4 child deaths in ARCH. All cohorts obtained 1st trimester blood and urine; ARCH has 2nd trimester blood and 2nd and 3rd trimester urine; MMIP has blood and urine from mothers in labor and cord blood. Because blood collection was initiated 6-9 months after the beginning of ARCH, blood collection is less complete than urine. Placental histology is available in ARCH, but this was also introduced later, and is available for about a quarter of enrollees. MARCH first visit biological collections are above 95% complete. All variables collected on birth certificates and hospital discharge abstracts in Michigan, and access to NDBS, are available from ARCH and MARCH pregnancies, and will be available in MMIP upon consent of mothers. We anticipate enrolling 1,000 pregnancies in MARCH, giving us a child cohort derived from some 2,000 pregnancies to contribute to the ECHO pooled cohort.
D2. RESEARCH EXPERIENCE OF OUR CONSORTIUM a. ASSEMBLY AND FOLLOW UP OF PREGNANCY AND BIRTH COHORTS: Drs. Paneth, Sokol and
Johnson have each led several large prospective studies with enrollment in pregnancy or at birth funded by NIH, and with follow-up for years, and in some cases, decades. These studies are described in the biosketches of the investigators. Table 4 details the number of subjects enrolled in some of these studies, and the follow-up rates achieved, to show that our investigative team has substantial experience in longitudinal studies starting in pregnancy and birth and in achieving high rates of follow up.
b. ECHO OUTCOMES: Our skills and expertise combined form a team capable of handling the work proposed and assisting the ECHO consortium as it moves into the phases of consolidating data. 1. PREGNANCY OUTCOMES: Robert Sokol MD and Shobha Mehta MD are maternal-fetal medicine specialists. Sokol has published on gestational diabetes, pre-eclampsia, fetal growth, preterm labor and is a pioneer in large cohort studies of the effects of alcohol and cocaine use in pregnancy. His ground-breaking work with fetal EEG showed how brain damage often occurs well before labor. Mehta’s research has focused on delivery complications, especially shoulder dystocia, and obesity and metabolism in pregnancy. Gwendolyn Norman RN, MPH, PhD was the Perinatal Research Nurse Coordinator for the WSU site of the NICHD Maternal-Fetal Medicine Network for 17 years, participating in the design, development and implementation of more than 30 randomized trials, cohort studies and registries addressing pregnancy outcomes. Jennifer Straughen PhD is a perinatal epidemiologist who has published on maternal obesity, preterm birth, pre-eclampsia, low birthweight and social factors in pregnancy, and is developing research on the relationship of placental findings to autism. 2. NEURODEVELOPMENT: Nicole Talge PhD and Daniel Keating PhD have collaborated on follow-up of the ARCH cohort, demonstrating the team’s capability to execute the protocol planned for this application. Keating has published on cognitive and social neurodevelopment from neonates to late adolescence, and has experience with large longitudinal studies such the NICHD Study of Early Child Care and Youth Development. Talge investigates perinatal pathways to cognitive and behavioral problems in childhood, studying sources of heterogeneity in these associations, including markers of biological functioning and socio-demographic risk. Nigel Paneth MD MPH has studied cognitive, motor and emotional development children born prematurely for decades, with a special focus on the ascertainment and epidemiology of cerebral palsy, which will not be an outcome in this study, but should be a key outcome in the pooled ECHO cohort.
Table 4:NIH-SUPPORTED LONGITUDINAL STUDIES BY ECHO INVESTIGATORS
Investigator Study name/ID Initial Sample (N)
Age at follow up
Percent complete
Paneth (PI) NBH - RO1 NS 20713 1,105 2 years 86%
Paneth (co-I) ELGAN - UO1 NS 040069 1,506 2 years 92% 10 years 92%
Sokol (co-I) SCHOOBE – R01 DA 08524 624 7years 85% Johnson (co-I) CAS R01AI051598 832 18 years 81%
Research Strategy Page 421
Contact PD/PI: Paneth, Nigel S

3. 3. OBESITY AND BODY COMPOSITION: Our expertise in obesity includes the environmental, epigenomic and metabolomic research of Dana Dolinoy PhD that uses weight, body composition and hormonal levels as outcomes.16 17 The research of Andrea Cassidy-Bushrow PhD links the developing gut microbiome with childhood obesity, in relation to mode of delivery. 18 19 20 Vasantha Padmanabhan PhD studies developmental programming of reproductive and metabolic diseases with a focus on environmental exposures. 21 22 23 24 25 Jean Kerver PhD, MSc, RD is PI of an R21 breastfeeding and postpartum weight intervention trial focused on maternal obesity, and brought measures of body fat into the ARCH study. Elizabeth Pearce MD MSc is a recognized authority in the study of dietary iodine, thyroid function in pregnancy and thyroidal effects of perchlorate exposure. Kelly Hirko PhD studies hormonal factors, dietary patterns, other lifestyle factors and racial disparities in breast cancer and obesity. 26 27 28 29 30 4. ASTHMA: While asthma is not a focus of this application, with the guidance of co-investigator Christine Cole Johnson, PhD, noted asthma epidemiologist, we are prepared to collect measures related to asthma as determined by the Steering Committee. Our team has experience in performing, training and assuring QA on such key asthma measures as the ISAAC31 and ACT questionnaires,32 pulmonary function tests,33 and measuring total and allergen-specific IgE, FeNO.34
c. EXPOSURE ASSESSMENTS 1. THE CHEMICAL AND TOXICOLOGIC ENVIRONMENT: Douglas Ruden PhD was first to show that DNA methylation changes associated with a woman’s exposure to lead while she was in-utero can be transmitted to her children,35 providing the scientific justification for the two-generation approach we propose in this application. Susan Land PhD directs WSU’s Applied Genomics Technology Center which will implement whole-genome DNA methylation arrays and validation of the most biologically significant methylation sites. Dana Dolinoy PhD investigates bisphenol A (BPA), lead, and phthalate in animals and humans to identify species, dose, and tissue-specific alterations in DNA methylation and histone profiles associated with metabolic disorders. Christine Cole Johnson PhD, leads a program project on asthma using large birth cohorts with collection of biologic and environmental samples, detailed characteristics of housing and neighborhoods and social and clinical variables. Cassidy-Bushrow measures metals in the pre and postnatal period in naturally shed primary teeth, and also uses the microbiome in her research on childhood obesity. Stuart Batterman PhD has conducted pioneering work using NDBS to measure exposure to organic contaminants. Manish Arora, PhD has developed laboratory methods to measure markers of prenatal and early childhood environmental chemical exposures shed primary teeth. 2. NUTRITION AND DIETARY ASSESSMENT: Dr. Kerver’s core research interest is in nutritional and diet patterns during pregnancy in the etiology of neurodevelopment and obesity,36 while Sarah Comstock, who, like Kerver, has a PhD in nutrition, examines pregnancy nutritional factors and the infant microbiome. Dolinoy has shown how nutrition can counter adverse environmental exposures mediated by the epigenome.37 38 3. INFECTION/INFLAMMATION: Lixin Zhang PhD is an infectious disease epidemiologist, who works on the molecular epidemiology of pathogens. Karen Racicot PhD is a reproductive immunologist with expertise in immune-related pregnancy loss. She studies viral-associated changes in placental inflammation in animal models, and is now collecting fresh-frozen placental specimens to study the human placental microbiome. Raina Fichorova MD, PhD has published extensively on reproductive tract infections, inflammation, the vaginal microbiome and their effects on child health.39 40 41 Sarah Comstock PhD researches the neonatal immune system, the maternal and infant gut microbiome and gastrointestinal development 42 43 44
d. BIOSTATISTICAL AND BIOINFORMATICS METHODS: The statistical group icludes Michael Elliott, PhD, Robert Podolsky, PhD, Samiran Ghosh, PhD and H.V.Jagadish PhD. Elliott has extensive experience in the survey design and data analysis, causal inference, and longitudinal data. His sample design method to ensure equal size clustering with maximum heterogeneity was designed for the NCS.45 Podolsky has extensive experience developing novel bioinformatics methods and applying advanced statistical models to genetic and genomic data. Ghosh’s primary area of research is developing novel statistical methods for adaptive intervention trials for longitudinal/clustered observational studies. Jagadish is expert in the integration and analysis of data from multiple heterogeneous sources, an important resource for pooled ECHO cohorts.
e. EPIGENOME: Dr. Ruden is Director of Epigenomics at WSU. His work on multi-generational epigenetic inheritance mechanisms46 has been cited hundreds of times, and he was senior author of the paper describing the software program SnpEff for annotating drosophila SNP’s, cited over a thousand times since
Research Strategy Page 422
Contact PD/PI: Paneth, Nigel S

2012, and included in the Broad Institute Genome Analysis Toolkit.47 Dolinoy uses epigenomics in both animal 48 49 50 51 52 53 and human studies from the MMIP cohort.54
f. THE MICROBIOME: Our team has both capacity and expertise in generating and analyzing microbiome data. Comstock, 55 Cassidy-Bushrow 56 and Zhang57 58 59 incorporate microbiomic findings in their research. Zhang’s lab uses both microarray and next generation sequencing platforms, including Illumina sequencing of 16s amplicon and whole genome sequencing. Illumina MiSeq and HiSeq 2500 are used for sequencing at the MSU Genomics Core, while large sequences are processed at the MS High Performance Computing Center. Johnson has studied the microbiome in asthma and allergy.60
g. PLACENTAL SCIENCE: Dr. Racicot has studied human placental specimens from the first and third trimester for histology, molecular analysis and primary trophoblast isolation and culture. Carolyn Salafia MD is a clinical pathologist with three decades of experience in placental pathology and its maternal clinical correlates and their joint relation to perinatal outcomes such as ASD risk, work in which she collaborates with Straughen. She directs Placental Analytics, LLC, which focuses on the development and implementation of a novel 2D/3D imaging technology to identify at-risk children based on placental features.
h. BIOETHICS: Tom Tomlinson PhD is Professor of Philosophy and directs MSU’s Center for Ethics in the Life Sciences. His international research ethics training grant was supported by the Fogarty International Center from 2004-2008. He teaches research ethics, has participated in reviewing NIH applications on this topic, and has a special interest in ethical challenges in biospecimen research and biostorage.61
D3. SPECIAL CIRCUMSTANCES IN MICHIGAN a. THE MICHIGAN NEONATAL BIOBANK: Archived NDBS constitute a remarkable scientific resource
in which it is possible to identify over 160 biomarkers and compounds, and, has been used, by this research team for studies of environmental contaminants, epigenetic changes over two generations, and gene expression.62 63 64 65 While Michigan, like many states,66 archives blood spots after newborn screening, our state is unique in its promotion of scientific use of its 4 million stored spots. Ambient storage dates to 1987, and since 2009, all new spots have been archived at -20°C. Since 2010, signed informed consent has been sought from all parents for anonymous research using the spots, with fewer than 10% of parents refusing consent. State law originally mandated retaining spots for 21 years; this was recently extended to indefinite storage. Identified research, as in this study, requires parental consent. The MNB is directed by Gail Kusch who will direct biostorage for this study in the WSU Integrative Biosciences (Ibio) Building adjacent to the MNB. A state program of community engagement, overseen by the Michigan Biotrust for Health, held community forums across the state and established a Community Values Advisory Board to monitor the use of the spot archive. A survey of more than 3,000 state residents found only 7% strongly or somewhat opposed use of archived newborn blood samples for research.67 Ruden, Cassidy-Bushrow and Paneth are members of the trust’s Scientific Advisory Board, which evaluates research applications for scientific merit, a step taken before required review by the Institutional Review Board of MDHHS.
b. HISTORY OF INSTITUTIONAL COLLABORATION: The group submitting this application has worked together across institutional boundaries for many years. In 2002 scientists from the five institutions involved in this application decided to mount a joint application when the NCS RFA came out. In 2004, we learned that Michigan had five counties in the national sample, and in 2007, our organization, which we called the Michigan Alliance for the NCS (MANCS), submitted applications to conduct the NCS in all 5 counties. Our design for recruiting, enrolling and following women made use of skills sets from each of our institutions. MDHHS provided nearly-instantaneous enumeration of county births by neighborhood; we had a list of 95% of 2010 Wayne County births on January 20, 2011. Environmental sampling was organized by HFHS. Hospital and clinic engagement, and meeting women in clinics was the responsibility of WSU, while the UM SRO interviewed women at home and handled all data management, just as we propose in this ECHO application. MSU, working through its land-grant based extension program, collaborated with HFHS in community engagement, and organized the overall operation. Four of the five co-PI’s in this investigation were investigators in our MANCS effort. Paneth was the PI of MANCS, Elliott led the sampling and enrollment core, Barone led the pediatric core and Copeland served as PI of the MDHHS sub-contract. Ruden, Paneth, Batterman and Keating have collaborated in the BLEEP project (Michigan Bloodspot Environmental Epidemiology Project) since 2011. Initiated by Howard Hu, then director of Environmental Science at UM, now Dean of Public Health at the University of Toronto, the project distributed pilot funds to
Research Strategy Page 423
Contact PD/PI: Paneth, Nigel S

investigators in all three universities to study blood spot technologies. Keating took over as PI of the project, and Paneth and Ruden directed sub-contracts at their respective institutions. The results were presented at a day-long conference in Ann Arbor in 2013 and are described in a forthcoming monograph edited by Ruden.68
D4. GENERAL CONSIDERATIONS FOR OUR RESEARCH: a. RIGOR AND REPRODUCIBILITY IN OUR RESEARCH: NIH guidelines require us to address four
components of our scientific research: 1) the scientific premise forming the basis of the proposed research, 2) rigorous experimental design for robust and unbiased results, 3) consideration of relevant biological variables, and 4) authentication of key biological and/or chemical resources. Item 1 is addressed in the significance section and in the discussion of each aim. Item 2 is noted when we discuss our cohorts, with the special focus on population-based research. As item 3 requires, we consider all relevant biological variables, including sex, age, weight, and underlying health conditions in our analyses. Our team is rich in epidemiologic and statistical expertise, and our statistical analysis section describes how we account for confounding, mediation and effect modification in all of our analyses. Our section on data acquisition describes the rigorous features of our data collection instruments and protocols. Item 4 is the subject of the required attachment.
b. ORGANIZATION OF THE CONSORTIUM AND MULTIPLE PI ARRANGEMENTS: Our experience in MANCS confirmed the need to assign specific responsibilities for components of a large study to sub-groups of investigators in a specific arena with a designated leader. We are fortunate that our organization builds on an existing structure. Most of our core leaders were also core leaders, or had other roles, in MANCS, but we have incorporated several new investigators into our leadership structure to provide expertise in the scientific domains relevant to the ECHO program. Table 5 shows these cores and their leadership. The core leadership (N = 12) which includes the 5 co-PI’s (bolded in Table 5), each of whom leads or co-leads a core, will meet by conference call weekly to review progress in achieving study goals and to address problems as they come up.
c. MULTIPLE PI PLAN: In the MANCS operation, all major decisions were made by consensus. We had no instance where major disagreement emerged, nor even where a vote was needed of the investigative team. Our organizational structure, which we adopt in modified form here, defines functional cores with assigned responsibilities to the team members most qualified to direct efforts in that direction. The five co-Pi’s will jointly provide oversight of the entire program and development and implementation of all policies, procedures and processes to achieve our scientific goals. Each co-PI is responsible for a core function. The assessment cores are responsible for developing our protocol. Paneth and Ruden will have central responsibility for establishing the protocol, including the laboratory measurements to be made, working with other assessment core leaders. Once the detailed protocol is in place, its implementation is the responsibility of the management cores, beginning with the enrollment work in clinics and hospitals, coordinated by Barone and Sokol. The Survey Operations and Data Management core, led by Elliott, will take on the large role of
Table 5: Organization of our study and leadership assignments MANAGEMENT CORES ASSESSMENT CORES ANALYTIC CORES
These cores are operational and logistic, focusing on participant enrollment, protocol adherence, follow up and communications
These cores address implementation of key measures to ensure both that all ECHO outcomes and all exposures of importance are assessed appropriately
These cores ensure that the data collected is appropriately archived and analyzed
Core Leader Core Leader Core Leader
Study Center Paneth Asthma Johnson Biostatistics/ Bioinformatics
Elliott
Communications and Publications
Thompson Neuro-development Keating Biological Specimens
Kusch
Survey Operations/Data Management
Elliott Nutritional/ Metabolic
Kerver Environmental Specimens
Johnson
Hospital/Clinic Relations Barone/Sokol Pregnancy Outcomes Sokol/Paneth State and Vital Data
Copeland
Bioethics and Protection of Human Subjects
Tomlinson Environmental and Epigenomic
Ruden Placentas Racicot
Social/Behavioral Norman These individuals will link our activities to national ECHO activities supported by the four ECHO Centers Patient-reported Outcomes Freed Data Analysis Elliott Coordinating Center Paneth CHEAR Resource Dolinoy
Research Strategy Page 424
Contact PD/PI: Paneth, Nigel S

conducting home visits and phone calls and coordinating all data elements. As data and specimens flow into the study, analytic cores will be tasked with ensuring that the data is transported, stored and integrated with the overall data management system. Elliott will play a key role in this integration, as well as with providing biostatistical consultation (along with our three other biostatisticians/bioinformaticians). Fiscal coordination will be provided by experienced grant administrators at each institution, led by Tina Munro of MSU, who coordinated all budgets for the MANCS project. Communications and publications (see Dissemination of Results below) will be the responsibility of Tracy Thompson MPH, a former NCI communications leader. We have assigned investigators to serve as liaisons to the ECHO cores. While we do not anticipate intellectual property emerging from this study, any issues relating to that function will be a joint responsibility of the five co-PI’s. Disagreements on any matter among the five PI’s will be handled by a vote.
d. OUR APPROACH TO PHASES OF THIS STUDY 1. THE UG3 PHASE: In the UG3 phase, we follow the RFA in planning for the later phases of this study in three ways. First we will test each of our procedures for feasibility, including testing our biostorage capacity, specimen transport mechanisms, recruitment and follow-up rates, developmental assessments, and measurements of body composition. We will also examine our capacity in important biological arenas used sparingly in our extant cohorts - obtaining consistent epigenomic and environmental information from NDBS, gut microbiome data from infants, evaluating our new placenta protocol, and collecting shed teeth. The evaluation during UG3 also includes increased contact with our extant cohorts. A very important metric to assess will be our capacity to track all data collected and integrating it with already collected data in the extant cohorts. We will continue to refine our ongoing enrollment of the MARCH cohort, with enrollment supported by this grant to begin in year 2. Recruitment underway now is supported by MSU, and we attach a letter from the Michigan Health Endowment Fund indicating their interest in further developing the MARCH cohort as a public policy resource for our state, and soliciting our application to them in the round of funding next month. The feasibility work will feed into the second way in which we plan for the study and that is the preparation of a detailed manual of procedures covering all aspects of the planned UH3 phase of the study. We will work closely with the ECHO Steering Committee to harmonize our efforts with those of other centers, especially those that share common data elements with us, such as real-time pregnancy collections. We hope to learn which aspects of our protocol and our data are most suitable for merging with other cohorts for eventual use in the pooled cohort phase of ECHO. The third component of our UG3 planning follows the RFA in seeking to “leverage retrospective and newly collected prospective data from longitudinal cohorts that have existing…. clinical data and biospecimens for exposures analyses of relevance to at least one of the four focus areas” As detailed in the Aims below, we will evaluate most hypotheses in our extant ARCH-MMIP cohorts, using post-natal assessments in a sufficient number of children in these cohorts to refine our hypotheses. For example, in the UG3 phase, we will examine neurodevelopmental outcomes in children in relation to a large number of POC’s; our results will hopefully allow us to focus down on a more select number of suspect chemicals so that we can test less expensively in the UH3 phase with its greater number of subjects. At the end of UG3, we anticipate having a set of protocols that are efficient, rigorous, practical and field-tested, along with exciting preliminary data that will set us on the path to fuller testing of important, policy-relevant scientific hypotheses in the UH3 phase in the ECHO pooled cohort. Metrics for the transition to the UH3 phase are set out in Table 6.
2. THE UH3 PHASE: In years 3-7 of this research, we plan to test our hypotheses with much greater statistical power and with an expanded array of data collections, as described below. Our expanded prenatal cohort will have the following enhancements:
• Regular and extensive annual developmental follow-up, both in person and by telephone. • More extensive prenatal interviews on psychosocial factors • Collection of placental specimens, with placental microbiome on a subset. • Collection of infant microbiome at age three months • Collection of shed primary teeth • In Flint, collected of shed teeth and developmental assessment of exposed siblings
As we set out below under the aims, these collections on new enrollees, added to new assessments to be made onexisting cohort members and specimens, such as blood spot POC and epigenomics, supported by the feasibility work and preliminary results of the UG3 phase, will permit us to make real, policy-relevant
Research Strategy Page 425
Contact PD/PI: Paneth, Nigel S

contributions to understanding of the role of the environment, inflammation, nutrition and perinatal epigenomic changes to three key ECHO outcomes.
3. THE POOLED COHORT: The pooling of several cohorts into a single cohort or a series of large cohorts is complex and hard to fully anticipate absent knowledge of the nature of several cohorts to be pooled. ECHO cohorts will differ in size, date of enrollment, age of enrollment and data collected. For some purposes, many cohorts will be appropriate, while for others, only a few cohorts will meet criteria for pooling. We advise obtaining as much data as possible that are national in scope. Two examples are state-archived NDBS and state birth certificates. Many states archive NDBS, and birth certificates are invaluable in that they cover all births, and collect much the same data using state versions of either of the two very similar 1989 or 2003 revisions of the US standard certificate. Another commonality that we hope is shared with other cohorts is our use of the both the NIH toolbox and the PhenX toolkit in our research. We have experience in pooling research data. From 1996-1999, Paneth directed analyses of four birth cohorts, to which a fifth was later added via a minority investigator supplement. These five databases (all population-based) were pooled to assess the long term effects of different neonatal care practices in premature infants. We examined common data elements among infants whose BW and GA were found in all cohorts. We showed that infants at the verge of viability were treated more selectively in Holland than in the US, with higher mortality in Holland and higher rates of disability in the US.69 We also found remarkable similarities in behavioral profiles of school age children in the cohorts who had weighed less than 1,000g at birth,70 and similarly high rates of school problems in all countries.71 This experience will be available to ECHO leadership as it pools its cohorts. For the integration of high dimensional biologic data, ECHO will benefit from Jagadish’s extensive research in methodologies for integrating data sets, including the determination of appropriate transformations and on maintaining data provenance to permit walking back through the chain of manipulations to understand subtleties in the original data. He has designed data management structures to capture and compare transcriptomic, metabolomic, and phenotype data in the context of diabetic complications. 72 Michigan
Table 6: PERFORMANCE METRICS FOR TRANSITION TO UH3 PHASE UG3 TASK GROUP SPECIFIC TASK PERFORMANCCE METRIC
Developing Protocols Establish biostorage facility to handle all projected specimens
Facility in place
Create manual of procedures for the combined ARCH/MMIP/MARCH cohort studies
Finalize manual
Conduct NIH toolbox developmental assessments in home
At least 30 successfully completed new NIH toolbox assessments at age 48 months
Placental protocol for UH3 phase Placental protocol agreed to by all study hospitals. At least 20 placentas shipped and processed
Linking to Participants and Data
Re-contact all participants in both extant cohorts to obtain follow up data
Successful recent contact with 85% of combined ARCH/MMIP participants
Continue pilot and early recruitment in MARCH sites
At least 50 MARCH and 40 Flint enrollees by end of year 2
Pilot Studies Examine approach to placental collection, both unfrozen and frozen
Finalized placenta protocol of two types
Extract and describe analytes from MMIP and ARCH serum/plasma
Distribution of at least 5 relevant analytes in the two collections tabulated
Obtain samples of archived newborn blood from the MNB of infants and their mothers
At least 80% of NDBS of infants and age-eligible mothers retrieved from MI neonatal biobank
Pilot test extraction of environmental toxins from NDBS
At least three different POP species/metals successfully measured on NDBS
Pilot test of CP reporting by parents Report of findings Data Management and
Analysis Database including all ARCH/MMIP and MARCH
data created Samples of data structure and content available
Examine Aims 1-3 in MARCH/MMIP data At least one draft manuscript available for each Aim
Prepare analysis of at least one Aim that makes use of biological materials
At least one draft manuscript with use of archived biological materials
Linkage to ECHO Steering Committee
Regularly attend steering committee meetings Attendance at meetings Propose plan to pool our cohort data with other
ECHO cohorts that have pregnancy data Draft pooling plan available
Research Strategy Page 426
Contact PD/PI: Paneth, Nigel S

Molecular Interactions (MiMI) was a bioinformatics project devoted to combining the overlapping and only partially consistent data in multiple datasets of protein interactions.73 4. PATIENT-REPORTED OUTCOMES FOR THE POOLED COHORT: The RFA requires that we propose at least one patient or proxy reported outcome for use in the pooled cohort. For this purpose, we propose the diagnosis of cerebral palsy (CP). No local cohort will have sufficient power to examine new risk factors for CP, but a pooled cohort of 50,000 will allow consideration of CP, a condition most recently reported to have a school-age prevalence of more than 3.0/1,000 in the US. The PI of this application, Dr. Paneth has worked extensively on the problem of CP diagnosis and on its etiology (see biosketch) and our team will undertake, during the UG3 phase, tests of the reliability of reporting of CP if parents are queried in different ways. We have access to some 200 cases of CP from our recent case-control study (R01 NS 055101), with all parents consented to be approached for new research, and we also have incorporated questions about the presence of CP in the Michigan Twin Registry (R01 MH 082054) which has assembled >10,000 twin pairs (R01 MH 082054). Dr. Gary Freed, pediatrician and noted health services researcher, will liaise with the Patient Report Outcomes Core to coordinate implementation of patient-reported outcomes.
e. DISSEMINATION OF RESULTS: While scientific publication in peer-reviewed journals is the standard approach to disseminate research findings, in recent years more attention has been given to informing the public of scientific research findings in formats that are targeted to lay people and placed in their appropriate human context. Another important constituency is the participants themselves, a community of more than 2,000 families if this application is supported. Our Communications and Publications Core will be tasked with overseeing all three aspects of communication – scientific publications, communications with the general public, and communications with our participants. Scientific publication in large research consortia requires guidelines that protect the interests of all investigators, and ensure that younger investigators, some of whom may not have been involved at the outset of the study, have opportunities to test hypotheses within the data. Dr. Paneth was the principal developer of the Authorship Guidelines used in the ELGAN study, a 12-hospital consortium that enrolled a large cohort of premature infants and followed them to age 10. The focus of the guidelines was to ensure that all authors fulfill accepted criteria for authorship; that all papers resulting from the research were appropriately designed and analyzed; that appropriate credit was given to all research participants; and that younger authors were especially encouraged to participate in analysis and lead authorship. Communications with the general public include conversations with the media on scientific topics, press releases on study milestones, and web-based information. We will host an ECHO website with information on the start-up of the study, ongoing events and milestones, and results of the study, written using NIH Plain Language guidelines and emphasizing the real-world value of any findings we have. Press releases will be sent to a developed list of media contacts located near each site. A telephone tree of key media relations contacts will be developed to manage any inquiries from the media. The tree will identify spokespeople for the sites and for different inquiries. Media inquiries will be directed to a primary point person who will then quickly ascertain the purpose, deadline, person requested, and contact information from the inquirer. The inquiry will then be directed to the appropriate person. Participants in research studies wish to receive information regarding their participation.74 75 Sharing information with participants has been shown to keep participants engaged, satisfied with their experience, and more likely to participate again or encourage others to do so. Newsletters that describe the purpose of the study and milestones—such as number of recruitments obtained, or new sites opening—will be regularly mailed or emailed to participants. Newsletters will thank participants for their help and answer frequently asked questions, Password-protected areas of our website will allow participants to provide feedback to investigators, and will include locations for participants to ask questions and leave comments. We aim for communication between study staff and participants that is bi-directional. Social media, such as Facebook and Twitter, will be utilized to further encourage participant communication with each other and with the investigative team Messages for social media will be crafted in accordance with the CDC’s Guide to Writing for Social Media. At recruitment, we will ask participants which method they prefer to receive information, and we will adjust communication methods accordingly. Periodic surveys will be given to participants to ascertain their response to our communication efforts. Individual outcomes will be shared when appropriate either upon participant request (e.g. results of developmental assessments) or if clinically indicated (e.g. elevated lead level). Decisions about when
Research Strategy Page 427
Contact PD/PI: Paneth, Nigel S

thresholds for disclosure will be reached will be made by the study’s executive committee in consultation with our bioethicist, Dr. Tomlinson. The Communications Core will develop the message and means to deliver such information to the participant. Initial communication efforts and responses will be tracked by Ms. Thompson, study Project Director and Co-Director of the Communications Core. Outcomes of participant communication may be published in peer-reviewed journals to add to the growing literature about the best ways to efficiently, safely, and satisfactorily communicate with study participants. Ms. Thompson was formerly Head of the Office of Communications at CCR in the National Cancer Institute. While in that role she received an NIH Plain Language Award in 2006, as well as other awards for recruitment materials, newsletters, and press materials.
f. ETHICAL CONSIDERATIONS: We include this section to outline some ethical principles guiding our research; the specific ways in which we protect human subjects are detailed in the required attachment. We need to take account of the complexity, length, and low-risk nature of the project, the variety of data and specimens to be collected, communication with participants about newly emerging findings, and biospecimen storage. These principles are incorporated into our approach to consent, confidentiality, incidental and research findings, incentives, biorepository, and IRB review. Consent: Consent and assent will be obtained over the course of the study, keeping participants fully informed and active in the consent process. Consent on enrollment is short and general. Later, specific assents will be sought for low-risk collections, offering an opportunity for us to remind participants of the project goals. If collections are added that require more formal consent, it will be sought on the occasion of the planned collection. While our consent form is comprehensive, we do not rely on a single point of contact to fully inform participants on all aspects of the research. We will supplement the initial information by creating a website and providing a newsletter to all participants (see dissemination section). We want our participants to have more understanding of the project, and more control over their participation, than can be provided by a one-time omnibus consent. Confidentiality: Participants will be assured that their personal information will not be shared outside the research team, and that project members have signed a pledge to that effect. Information will flow on a need-to-know basis. Data or analysis sent to others will always be coded or otherwise de-identified. This is a critical issue for ECHO when we move into the pooled cohort stage, and Dr. Tomlinson’s experience in bioethical deliberations will be of value to the ECHO consortium. Incidental research findings: four types of findings arise in research with humans: 1. Identification of modifiable risks (such as high lead levels in the home) 2. Identification of non-modifiable risks (past heavy metal exposure in pregnancy) 3. Identification of emerging research findings of potentially modifiable risks, but of uncertain health import 4. Identification of emerging research findings of potentially unmodifiable risks of uncertain health import There are no easy answers to the scenarios above, and often such situations need to be handled on a case-by-case basis. We will create a project advisory board including participants and experienced clinicians to advise us on individual cases. A major principle guiding our research is that no research goal is more important than patient health and safety.
g. BIOSTORAGE ISSUES: Our biostorage team will ensure that best practices are followed: appropriate collection and processing, maintaining chain of custody, proper aliquoting, shipping conditions, storage at appropriate temperatures, and efficient retrieval. Our team has seven years of experience with ARCH. WSU’s Clinical Research Service maintains a Biobank Core in a new building, the Integrative Biosciences Center (iBIO). We have noted already that Gayle Kusch, director of the MNB, which archives all state blood spots, will also serve as the Biobank Director for this project, providing experienced leadership and ready access to the blood spot collection which is housed adjacent to the iBio building. Local collection sites will prepare specimens for same-day shipment via FedEx to the WSU iBIO. The iBIO staff will aliquot and store specimens within 24 hours of collection. Participants’ blood will be collected in clinical settings during the first and second trimester, urine in each trimester. Protocols will be tested monthly for 3 months and quarterly for the project’s duration. The lab coordinator will ensure additional training for any site out of compliance. Each specimen will have barcoded and eye-readable identification codes assigned by the study with identification, date/time, and study center recorded. Initial processing at the site laboratory will
Research Strategy Page 428
Contact PD/PI: Paneth, Nigel S

include centrifugation of bloods, blood spotting, and preparation for daily shipping to the study center. Local labs will maintain and ship daily shipping packages, using gel paks to maintain specimens at 1̊ C- 3̊ C .The iBIO will log and aliquot specimens on day of receipt. Multiple 250µL aliquots will be created and placed in 96 well containers that have embedded bar codes for specimen linking, tracking and retrieval. Plasma, serum and urine specimens will be separated into as many 250 µl aliquots as possible to permit shipping to multiple laboratories, as follows: 1. Urine and blood for POC’s and metals to Dr. Stuart Batterman at U of M (Aim 1) 2. Urine for iodine and blood for thyroid hormones to Dr. Elizabeth Pearce of Boston University (Aim 2) 3. NDBS for inflammatory markers to Dr. Raina Fichorova of Harvard University (Aim 3) All biospecimens will be stored in secure -80 C freezers dedicated solely to the ECHO project. Teeth are mailed to us by families and will be logged in upon receipt to our study database, and assigned a unique ID and sample number. Processing includes lightly scrubbing and cleaning in a sterile environment to remove blood or contamination. Work surfaces will be cleaned and sanitized before and after this process. Teeth are then stored in Eppendorf tubes in cardboard boxes in a locked cabinet at room temperature in a clean, dry environment away from direct sunlight. The placenta protocol is described with Aim 3 below. Placentas will be shipped from hospitals directly to Dr. Salafia’s lab without use of our biostorage facility. Stool samples will go to Dr. Zhang’s lab at MSU. WSU iBIO utilizes the biospecimen management function of OnCore allowing in-depth tracking of each biospecimen from the time it enters the core to the time it is shipped to the requestor. BSM creates parent samples as well as multiple aliquots using unique barcode labels that capture biospecimen information such as description, acquisition, preparation procedures, quality control measures, specific specimen location, and special requests. WSU iBio freezers are supported by 2 backup generators. The freezers are monitored by the Smart-Vue wireless temperature monitoring system which is auditable and 21 CFR part 11 compliant. Research Coordinators receive real time temperature change alerts to both their e-mail and text messages to their cell phone. Monthly quality control inspections are conducted by the WSU Biobank manager.
D5. DATA COLLECTION a. RECRUITMENT OF THE MARCH COHORT: Our plan for expanding our extant cohort aims to recruit
pregnant women in a way that is feasible, cost-effective, acceptable and timely in twenty prenatal clinics, referring to ten hospitals, located in five regions of lower Michigan that constitute the MARCH sampling frame for the selection of participants. We have extensive experience in all of the procedures we here set out. 1. OBTAINING COOPERATION WITH PROVIDERS, HOSPITALS, & LABORATORIES: The efforts of the Hospital and Clinic Relations Core to obtain provider cooperation operate on two levels – group and individual. We have developed a positive working relationship with healthcare providers, study hospitals, and laboratories by creating an umbrella of support among relevant medical societies, engaging especially the Michigan State Medical Society, county medical societies, and medical specialty societies such as the Michigan sections of the American College of Obstetrics and Gynecology (ACOG) and the American Academy of Pediatrics (AAP). This effort will continue to be facilitated by our Advisory Council, which includes many notables figure in health care in our state. We will attend medical staff meetings of each sampled hospital’s obstetric departments, and offer to provide grand rounds describing the MARCH concept. At the individual provider level, we will meet with practitioners and staff, bringing lunch or equivalent as appropriate in recognition of time devoted to listening to our plans. We will review the goals and requirements of the study. Participating clinics will receive framed plaques for mounting in waiting rooms, alongside MARCH posters indicating that the clinic is a supporter of/participant with MARCH. Brochures and newsletters will be available in the waiting rooms, and if resources are available, we will develop a MARCH video to show in waiting rooms. 2. RECRUITMENT IN PRENATAL CLINICS: The Hospital and Clinic Relations Core will work directly with obstetricians and other prenatal and delivery care providers to ensure that MARCH tasks are completed accurately, on time and efficiently. The core will develop our enrollment protocols and implement them in prenatal care settings, including making arrangements for the collection of biological specimens, the transfer of survey data to the Survey Operations/Data Management Core, monitoring delivery rooms to organize the collection of placentas. The provider role is critical in recruitment in prenatal clinics, but the sharing of patient information by the provider must be done without violating HIPAA rules. At the same time, the burden on the provider must be minimal, with the operating rule that no study procedure can be allowed to interfere with
Research Strategy Page 429
Contact PD/PI: Paneth, Nigel S

patient care, and all work provided by clinic staff in support of MARCH will be appropriately compensated. The process of MARCH recruitment is developed to work best with each individual clinic or practice. For example, some clinics perform all intakes on one day per week, while others perform intakes throughout the week. Some have phlebotomists on staff and others send women to off-site contract laboratories. Some clinics prefer a formal signed document to allow MARCH staff to talk to their patients, while others accept the MSU IRB views that verbal consent obtained by the provider from the participant is HIPAA compliant and a sufficient basis to allow us to contact potential subjects. We now recruit in regularly in six Michigan prenatal clinics (two in ARCH, four in MARCH) and recruited briefly in more than 70 Wayne County clinics in the National Children’s Study. 3. COORDINATION WITH CLINICAL LABORATORIES: Once cooperation of the provider practice or clinic is established, in-house, hospital-based, or contract medical laboratories utilized by the provider are identified. These laboratories are approached to cooperate with the MARCH protocol. Depending on the laboratory location and arrangement, several options for coordination of sample collection exist. At the Traverse City site, for example, study blood collection tubes and urine containers are kept in the laboratory and patients with a flagged file have additional blood collected at standard-of-care blood draws and extra urine collected. Those samples may be stored in the laboratory until picked up or shipped to the biospecimen core. By contrast, at our Flint site, patients are given the collection tubes in a specimen bag and asked to take them to the hospital-based laboratory. Other arrangements are developed based on the specific set up of the clinic or practice. The budget includes modest compensation to offset the efforts of the laboratories efforts in collecting specimens. 4. COORDINATION WITH HOSPITALS: All hospitals in our sample will be approached well before launch of the formal MARCH study. This process is underway and likely to have been completed by the end of 2016. We anticipate that most hospitals will require their own IRB approval for the hospital component of the protocol. We will implement a system for accessing placentas, for which we will have obtained consent in our prenatal care enrollment.
b. FOLLOW UP: We emphasize cohort retention using social media, messaging, and frequent mail and telephone contact; periodic engagement with participants is essential (Table 7). Participant data will be utilized to produce the date of birthday cards to be sent. With 1,000 total participants, approximately 20 birthday cards will be sent out each week.
c. COST EFFICIENCES IN DATA COLLECTION: In large data collection efforts, costs mount quickly and efficiencies are critically important. Below we list the ways in which our experiences so far in large cohorts are translated into procedures for data collection that are cost-efficient 1. UTILIZING CLINICAL LABORATORIES FOR OBTAINING BIOSPECIMENS IN PREGNANCY: In the ARCH cohort, we arranged with service laboratories to obtain two extra tubes of blood (one with, the other without, anticoagulant) from the ARCH participant when she attended her routine first prenatal laboratory visit and her routine 24-28 week glucose tolerance test. The extra tubes were provided to the mother to bring to the laboratory. The research project was charged $5 initially, now $10, for the extra laboratory effort. We have made similar or more favorable arrangements in our first four MARCH enrollment sites. 2. WORKING WITH HOSPITAL PROTOCOLS IN OBTAINING KEY SPECIMENS: We worked with the pathology department of Sparrow Hospital (Lansing, MI) in ARCH to develop an efficient system to identify participant placentas, and then to obtain samples that would not interfere with standard hospital practices. Sparrow Hospital, like many, archives all placentas for 72 hours to see whether newborn indications require placental study. Removal of a small sample of parenchymal tissue, membranes and cord and storing them in formalin after standard placental measurements had been obtained, as we do in ARCH does not interfere with clinical needs. The pathology department charges $10 for our specimen. In MARCH, the demand on hospitals will be less because the entire pre-processed placenta will be sent in formalin (after clinical needs have been
Table 7: FOLLOW UP COMMUNICATION APPROACHES TO BE USED Approach Audience Frequency
Newsletters Clinic Staff & Participants Quarterly Facebook Participants Weekly posts Website Clinic Staff, Hospital Partners,
Community Partners, Participants Monthly Updates
Gifts at Birth Participants Once per participant Birthday Cards Participants’ Child Once per year per
participant Survey of preferred
method of communication
Participants, Clinic Staff, Hospital Partners, Community Partners
Once per participant at beginning of
enrollment/participation Survey of satisfaction and engagement with
study
Participants, Clinic Staff, Hospital Partners, Community Partners
Periodically
Research Strategy Page 430
Contact PD/PI: Paneth, Nigel S

addressed) to Dr. Salafia’s lab. Obtaining hospital cooperation is markedly enhanced by our having prenatal consent from the participant for out study examination of the placenta. 3. USE OF THE STATE’S NEONATAL BLOOD SPOT COLLECTION: All newborns in Michigan have archived blood on filter paper left over after screening. Since 2009, all such spots have been frozen at -20°C. The number of parents who request destruction of such leftover material, a step allowed by state law, numbers fewer than 100 per year among > 100,000 births. We routinely consent for permission to obtain the blood spot in ARCH. In over one thousand requests for permission for such access in ARCH and other studies, refusal rates are below 1%. The state charges $36 for one 0.5cm2 spot, much less for 3 mm punches. We can make 12 3 mm punches from a full blood spot. 4. USE OF UNIVERSALLY COLLECTED DATA ON HEALTH: Medical record data is often expensive to retrieve because of multiple electronic systems across hospitals and because of varying hospital procedures for accessing data, even with patient permission. We thus have arranged with the MDHHS to obtain birth certificate variables describing pregnancy and birth (e.g. complications of pregnancy, birthweight, gestational age from LMP and from clinical estimates, Apgar scores, mode of delivery, etc.) The Michigan Hospital Association creates a file of all hospital discharge abstracts (diagnoses, major procedures, length of stay), and maternal and newborn abstracts are archived by MDHHS. Both of these data elements are downloaded to us on a secure, password protected file sharing platform at a total cost for all three files of $20 per subject. 5. USE OF A SINGLE IRB FOR COLLABORATIVE RESEARCH: IRB review will be simplified as much as possible. We are presently negotiating to extend the agreement made when the National Children’s Study contract was operative in Michigan (2007-2013) that all protocols of ECHO be reviewed by an MSU IRB with reliance agreements from our four partners. This system worked extremely efficiently in MANCS, and we were able to replace five separate IRB reviews with one review.
d. ASSESSMENT OF ECHO OUTCOMES: We here describe outcomes used in all three study aims. 1. PREGNANCY OUTCOMES: Pregnancy outcome data, as well as data concerning obstetric/medical complications and interventions, which can serve as mediators, modifiers or confounders will be derived from Birth Certificates and Hospital Discharge Abstracts, obtained with written permission from participants. Since 2008 all births in Michigan were recorded in the 2003 revised US standard birth certificate; these contain approximately 100 pregnancy and perinatal variables. About one half of these relate to the offspring, allowing us to use standard outcomes of GA (clinical estimate is now recorded in addition to LMP), fetal growth, Apgar score, transfer and NICU admission. Maternal variables include pre-eclampsia, gestational diabetes, and delivery procedures. Hospital discharge abstracts (both maternal and newborn), available through the Michigan Department of Health & Human Services from the Michigan Hospital Association, provides diagnoses and procedure codes, as well as length of stay in the hospital. Consent to abstract medical records from hospitals of birth will be obtained, as noted above. 2. NEURODEVELOPMENTAL ASSESSMENTS: We plan neurodevelopmental assessments for the three cohorts in the proposed research (MARCH, ARCH, and MMIP) in the home at age 2, 4 and 6, and via telephone interviews at ages 1, 3, and 5. Age 4 is our primary age of assessment, but some children in ARCH/MMIP will be over 4 before we can assess them. Age 6 also provides greater reliability of cognitive and behavioral assessments. Age two will give us useful information, and we think it unwise to wait till age 4 for the first home visit. Specification of tasks, timing, and age of administration are shown in Table 8. For the in-home assessments, entries are further specified for child assessments, parent assessments, and parent-child interactions. Direct assessments in person at all ages are not feasible owing to budgetary constraints, and thus selections for such assessments were based on considerations of maximum developmental sensitivity. At age 2 years, both cognitive and neurodevelopmental assessments are feasible, and have been employed in multiple large-scale longitudinal studies, such as the Early Childhood Longitudinal Study-Birth Cohort (ECLS-B).76 Primary data collection for all telephone interviews will be the Ages and Stages Questionnaire (ASQ) completed by a parent or primary caregiver. The ASQ has been used often when direct assessments are not feasible. It has been validated in comparison to direct assessments (e.g., Bayley III) and among children with typical and atypical neurodevelopmental trajectories (e.g., preterm infants). 77 78 At age 2 years the primary assessment will be the Bayley III, well-validated for this age range. 79 80 Assessment of both motor development and general cognitive functioning are assessed in the Bayley III instrument, as are measures of both expressive and receptive communication. Neurodevelopment in the
Research Strategy Page 431
Contact PD/PI: Paneth, Nigel S

social domain will be assessed using a parent-child interaction task, the Two Bags task, which provides an assessment of parenting dimensions (e.g., warmth, sensitivity, detachment, intrusiveness) that influence children’s adaptation to current and future developmental challenges. 81 82 Due to budgetary constraints, the videotapes will be archived for later analysis based on future funding. This is a reasonable trade-off, in order to obtain a full analysis of key parenting dimensions. These early assessments provide both a broad-based assessment of neurodevelopment at the transition point to early childhood and a baseline assessment of developmental trajectories. Maternal (or primary caregiver) IQ will be assessed using the Wechsler Abbreviated Scale of Intelligence WASI.83 This will be used as a control variable in analyses of environmental
impacts on child neurodevelopment. Although direct assessments provide valuable objective indicators, they capture a picture of development at only one point in time. To supplement this with more extensive information, the parent or primary caregiver will respond to a set of validated questionnaires designed to assess child functioning in multiple domains. These include the Children’s Behavior Checklist (CBCL) to assess internalizing and externalizing behavioral problems, 84 Conners’ Parent Rating Scales-Short Form (CPRS-R:SF) to provide separate assessments of the inattention and hyperactivity/impulsivity dimensions that comprise attention deficit hyperactivity disorder (ADHD) 85, and the Social Responsiveness Scale-Second Edition (SRS-2) to assess dimensions of social communication, including those associated with ASD (ASD) as well as other etiologies. 86 At ages 4 and 6 years, the primary cognitive neurodevelopmental assessment will employ the NIH Toolbox, including the following assessments. The Flanker task assesses inhibitory control, the Dimensional Change Card Sort task to assess cognitive set shifting, the Picture Vocabulary test to assess receptive language, and the Picture Sequence Memory Test to assess episodic memory. As noted in the section on Prior Work, the investigators (Keating and Talge) have administered these instruments to children at age 4 years. Nearly all
children were able to complete these tasks, which was not the case at age 3 years, and thus we have confidence that this approach will yield valuable information on general cognitive functioning, but even more so on specific aspects of executive functioning, which are likely to be more sensitive indicators of subtle neurodevelopmental indicators.87 88 In addition, we will repeat the CBCL and SRS-2 to obtain information on developmental trajectories. In combination, these assessments will provide a detailed, longitudinal profile of child neurodevelopment, with sufficient sensitivity to detect meaningful environmental impacts. Cognition is assessed by the WPPSI at age 4 and the WISC at age 6.
Table 8: HOME ASSESSMENTS FOR AGES 2, 4, AND 6 YEARS Topic Instrument Time
Child (min) Motor Development Bayley III1 20 Cognitive Functioning (general) Bayley III1/WPPSI2 /WISC2 20 Cognitive Functioning (specific) NIH Toolbox Cognitive flexibility DCCS Inhibitory control Flanker 30 Receptive vocabulary PVT Episodic memory Picture Sequence Memory Working memory List Sorting 5 Processing speed Pattern Comparison 5 Language Expressive & Receptive Comm. Bayley III1/NIH Toolbox 20 / 5 Behavioral Problems Internalizing & Externalizing CBCL 10-20 ADHD Symptoms Conners (short form) 10 ASD symptoms MCHAT / SRS-2 10 / 15 Educational/Day Care History ARCH Study questionnaire 5 Quality of stimulation/support at home HOME Scale 5 Anthropometrics Impedance scale, skinfolds 10 Parent (min) Cognitive Functioning (general) WASI3 15 Behavioral Problems Internalizing & Externalizing ASR 10 ASD symptoms BAPQ1 5 History of childhood maltreatment CTQ1 5 Anthropometrics Impedance scale, skinfolds 10 Family (min) Parent-child interaction Two bags task1 10 Home environment HSQ 10 Family conflict/cohesion FES 10 Significant life events Turner, Wheaton , & Lloyd 5 Total Administration Time/Visit (min) = 60-80 (child); 85-95 (parent) 1Age 2 only; 2Two subscale version; 3Age 4 only. Abbreviations: ASD (Autism Spectrum Disorder); ASR (Adult Self Report-Achenbach); BAPQ (Broad ASD Phenotype Questionnaire); CBCL (Child Behavioral Checklist); CTQ (Childhood Trauma Questionnaire); DCCS (Dimensional Change Card Sort) ; FES: (Family Environment Scale); HBQ (Health & Behavior Questionnaire); HOME: Home Observation for Measurement of the Environment; HSQ (Home Screening Questionnaire); MCHAT (Modified Checklist for ASD in Toddlers); PVT: (Picture Vocabulary Test); WISC (Wechsler Intelligence Scale for Children); WPPSI (Wechsler Preschool and Primary Scale of Intelligence); WASI (Wechsler Abbreviated Scales of Intelligence)
Research Strategy Page 432
Contact PD/PI: Paneth, Nigel S

3. OBESITY AND BODY COMPOSITION: Height, weight, waist circumference, triceps and subscapular skinfolds will be measured with protocols derived from the CDC NHANES Anthropometry Manual (2007). Measurements will be completed for both the child and mother/caregiver. Maternal measurements will be used as covariates, and we have also found that observing the maternal measurements puts the child at ease and better prepares them for further assessment. Body mass index (BMI) (wt[kg]/ht[m2]) will be used as our primary measure of childhood obesity given its correlation with adiposity,89 ease of collection in the field, and likely ability to harmonize with results from other cohorts. BMI will be calculated and child BMI z-score derived using CDC age- and sex-specific reference growth data.90 Additional measures of body composition, including waist circumference, skinfolds, and bioelectrical impedance analysis (BIA), will be assessed because of their ability to improve prediction of body fatness and their correlation with chronic disease risk in children.91 92 93 Height will be measured using a Seca 213 portable stadiometer after checking the individual’s position and posture. Waist circumference will be taken with a Seca retractable tape measure after making a temporary mark on the skin at the midaxillary line just above the lateral border of the right ilium. Holtain Calipers will be used for measurement of each skinfold. All measurements will be taken in duplicate, or triplicate when readings differ excessively, and all measurement sets will be averaged for analysis, per NHANES procedures. Each individual will be weighed (in duplicate) without shoes or heavy clothing using a portable Tanita Body Composition Analyzer Model #SC331-S. This model measures weight and impedance and will be used for the estimation of total body fat percent, muscle mass, and bone mass. We use this method because it requires no specialized facilities or expertise, measurements can be taken quickly and easily, and it has been validated for use in healthy adults and children age 5-17 y with accuracy estimated to be within 5% of dual-energy X-ray absorptiometry (DEXA, the gold standard for body composition assessment).93 Scales will be calibrated each morning using a standard weight. Because we will collect multiple measures of body composition (i.e. BIA and skinfolds, and waist circumference), we will be able to test the validity of the BIA estimates of body fat in children younger than 5 y. 4. PSYCHOSOCIAL STATUS: Social determinants of health are economic and social conditions that affect the health of individuals and communities. They include safe and affordable housing, education, job security, social connection and safety, living wages, availability of transportation and food and psychological distress. While not primary exposures in our study, every association we find of ECHO outcomes with nutrition, environmental toxins, and inflammation will be examined in the context of the variables described below. • Socioeconomic Status: Socioeconomic status (SES) has consistently been associated with a wide range of developmental health outcomes in children94 95 We will obtain data at enrollment in pregnancy that permit analyses of the many ways in which SES can produce such effects. At the individual level, demographic information on parental education, marital/partner status, Medicaid status, income, wealth (reflected in home/car/securities ownership), ethnicity, race and family composition will be recorded. At the two year visit, we will have direct observation of the home environment using a brief version of the HOME scale. • Neighborhood Disadvantage: Residential location has effects beyond individual SES. This may be attributable to the social characteristics of neighborhoods (average SES of households; level of racial/ethnic segregation; food deserts; evidence of criminal activity or neighborhood disorder) or may reflect differences in environmental pollutants such as the POPs and heavy metals to be studied in Aim 1, or both. Working with our partners in MDHHS, we will have geocoded measures of neighborhood SES, racial segregation and other characteristics. • Psychosocial Stressors: We will use several instruments to assess psychosocial risk. We survey pregnant women and mothers with the Edinburgh Depression Scale (for current status) and the Adverse Childhood Experience Questionnaire (for history of life adversity). We will also employ instruments that address perceived neighborhood safety, stressful life events, daily hassles, and discrimination/racism). The pervasive effect of psychosocial stressors on many developmental and health outcomes require us to examine effect modification of these stressor for each exposure/outcome relationship we test. Early life adversity may be associated with stress-dysregulation by an epigenetic pathway involving the glucocorticoid receptor gene NR3C1. 96 97 98 Chronic stressful conditions may alter the cervico/vaginal immune environment increasing risk for preterm birth, or exacerbate the neurodevelopmental impact of lead exposure. By the same token, high SES at the individual and neighborhood levels, and low levels of reported individual life stressors, may moderate the negative effects of physical exposures.
Research Strategy Page 433
Contact PD/PI: Paneth, Nigel S

D6. THE THREE AIMS OF THIS STUDY
a. AIM 1: ENVIRONMENTAL TOXINS AND ECHO OUTCOMES: Epidemiological and laboratory data both suggest that early maternal exposure to heavy metals and persistent organic pollutants (POPs) can impair child development.99 100 101 Exposure to environmental chemicals is ubiquitous and includes lead from old pipes and paint, PCBs (insulation), DDEs (pesticides), PBDEs (flame retardants), and BPA (plastics) (Table 9). BPA exposure can alter cognition and behavior in both rodents 102 103 104 105 106 107 108 and humans.109 110 111 The regions of Michigan we study, notably Detroit and Flint, experience large racial disparities in pregnancy outcomes and neurodevelopment, and, at the same time, having once been leading centers in the automotive industry, are situated in regions heavily exposed to industrial contaminants. The Detroit-Warren-Flint area, according to the EPA, has 68 Superfund sites and 281 facilities releasing more than 21,000 tons of toxic chemicals every year (https://www.epa.gov/superfund). This region, according to Forbes Magazine’s analysis of EPA data, is the second most polluted region in the country. Michigan experienced one of the most notable environmental contamination episodes in US history, when in 1973, endocrine-disrupting polybrominated biphenyls (PBBs) were accidentally put into livestock feed exposing consumers of Michigan-raised beef, milk, and even eggs to PBBs, with elevated levels detectable in serum and breast milk of many Michigan mothers.112 The persistence of PBB’s is remarkable, and public concern remains about the higher levels found in serum of Michigan residents 40 years post-exposure.113 PCB’s derived from consumption of fish from the Great Lake s into which factory effluent were drained is also persistent in serum over decades, especially in high fish consumers.114 A Superfund site has recently been created to clean up dioxin contamination of the Saginaw Bay region, location of one of our study sites.115 In this aim, we hope to advance the field in three ways – By assessing the in-utero effects of these environmental toxins (hypothesis 1a), by assessing the mediating role of epigenomics (hypothesis 1b) and by further examining their transgenerational effects, an area in which we have pioneered116 (hypothesis 1c). In a special sub-study, we will add additional data collection to more thoroughly explore the effects of the recent water contamination in Flint (hypothesis 1d). Hypothesis 1a: In utero exposure to POPs listed in Table 9 and heavy metals (lead, arsenic, and mercury) assessed in maternal 1st trimester serum and urine will be associated with increased risk of impaired cognitive outcomes in the child at age 4. Among many POPs that may affect development, we will focus on agents that have been validated for accuracy, precision and sensitivity in NDBS. 117 118 All are widespread in the general population, have very long half-lives, and cross the placenta. Table 9 shows the range of detection of several POPs by high performance liquid chromatography tandem mass spectrometry in NDBS.
• UG3 PHASE: Hypothesis 1a will be piloted in 125 children assessed at age 4 or above in the ARCH/MMIP cohorts. POPs and metals will be measured in the mother’s stored NDBS (for grand-maternal exposure) and her first trimester serum and urine (for maternal exposure).
• UH3 PHASE: Using UG3 findings, we will assess only POPs and metals measurable in maternal samples, and showing suggestions of a relationship to age 4 cognitive tests in children assessed at age 4 or above. We estimate a total of 949 children available for this analysis in the UG3+UH3 phase.
• POOLED COHORT: We will contribute our data to the pooled cohort sample with prenatal biospecimens to examine rarer neurodevelopmental outcomes, such as cerebral palsy, severe cognitive impairment and ASD. We will also assist the pooled cohort to examine interactions with ethnicity, maternal age, other host characteristics for and other exposures for which power will be limited in any one cohort. In addition, we will see if it possible to incorporate, with other sites with similar data, environmental data collected by the Michigan
Table 9: PERSISTENT ORGANIC POLLUTANTS (POPs) TESTABLE IN DRIED BLOOD SPOTS
Abbreviation
Chemical Common use Quantification
Limit PCB 138/153 Polychlorinated biphenyls
Insulation, coolant fluids
0.002 ng/mL
PCB 118 0.008 ng/mL PBDE 47 Polybrominated diphenyl ethers Flame retardants 0.01 ng/mL p,p’-DDE Dichlorodiphenyldichloroethylene Pesticides 0.02 ng/mL beta-HCH Beta-hexachlorocyclohexane Pesticides 0.02 ng/mL HCB Hexachlorobenzene Pesticides 0.003 ng/mL
PFOS/PFOA
Perfluorooctane sulfonate/perfluoroocatanoic acid
Water and oil resistant properties
0.06/0.05 ng/mL
BPA Bisphenol A Plastics 0.4 ng/mL
Research Strategy Page 434
Contact PD/PI: Paneth, Nigel S

Figure 1: Lead exposure to mothers in utero increases DNA methylation of 149 genes in offspring neonatal blood.
Department of Environmental Quality and transferred to us by our MDHHS colleagues. Air quality is monitored at 41 sites and includes ozone, PM10 and PM2.5. Water quality data include surface monitoring sites (coliforms, fish contaminants, wastewater discharge), wastewater disposal system reports, EPA reports in relation to federal Clean Water Act regulations and contaminants of community water (atrazine, DEHP, PCE, TCE, Radium, Uranium, Nitrate, Arsenic, DBP). Sport fish have been monitored since 1980 by species, water body and date for a number of persistent contaminants including mercury, DDT/DDE, PCBs and dioxins.119 A fuller detailing of these resources is provided in the appendix. Hypothesis 1b: Developmental effects identified in hypothesis 1a will be mediated by epigenetic changes measured on NBS. A tantalizing but untested possibility is that prenatal exposure to metals and POPs at the one-cell stage (estimated from 1st trimester biospecimens) alters epigenetic patterns in all offspring cells, and that these changes in DNA methylation can be measured in the DNBS of these offspring. We will determine whether epigenetic changes in NBS are statistically correlated with metals/POPs exposures on the one hand, and with cognitive test scores on the other, indicating a mediation pathway for epigenetic changes between exposure and outcome. Of particular interest are human metastable epialleles (MEs). MEs are characterized by high inter-tissue correlation of DNA methylation among distinct germ layer lineages (liver, kidney, brain, blood), which suggests that blood can be a surrogate for the brain in studying the effects of heavy metals and POPs on DNA methylation. ME’s may be especially sensitive to environmental circumstances, such as maternal pregnancy nutrition. 120 121 This observation prompts us to explore interactions between POPs/metals and the nutritional/anthropometric data to be collected in Aim 2.
• UG3 PHASE: Hypothesis 1b will be pilot tested in 125 children assessed at age 4 or above in the ARCH/MMIP cohorts. Epic HM850K arrays will be done on child NDBS and correlated with maternal and grand-maternal POPs and metals exposures, as well as with cognitive outcomes.
• UH3 PHASE: Using UG3 findings, we will learn which epigenetic changes are especially likely to serve as mediators of the POPs/metals relationship to cognition, so as to more fully work out these relationships in the full sample available to us in the UH3 phase.
• POOLED COHORT: We can pool our epigenomic work with cohorts with access to NDBS, permitting us to examine epigenomic changes found important in our local cohort to the rarer neurodevelopmental outcomes that will be available in the pooled cohort. Hypothesis 1c: Grand-maternal exposure to POPs and metals will amplify the adverse cognitive outcomes and DNA methylation changes in the grandchildren due to environmental toxins. Animal studies have shown that parental exposure to toxicants can affect the health of future unexposed generations,122 and that prenatal lead exposure alters expression of DNA methyltransferases in the brain through adulthood.116 We thus decided to study the effects of maternal and grand-maternal lead exposure on DNA methylation in the human newborn (R01 ES012933-10). In a cohort of 35 mothers and their children, we found that high blood lead levels in the mother’s neonatal blood (obtained from the MNB) increases DNA methylation in 149 genes in her child’s neonatal blood.123 (Fig 1) To our knowledge, this is the first evidence for multi-generational effects of lead on human DNA methylation. Because a woman’s germ cells have completed their development by the end of the 3rd trimester, in utero exposures can affect her germ cells, and thus impact the following generation. With MARCH recruitment beginning now and extending to 2020, most participants will have been born since NDBS archiving began in 1987, and likely experienced higher in utero exposures than their offspring. Our preliminary work with mothers suggests that better than 95% will consent to access these spots for our studies We will measure heavy metals and POPs in the mothers’ NDBS and correlate these exposures to changes in DNA methylation in the children’s DNBS, as we have done for lead. We will thus extend our work to evaluate the effect of POPs on DNA methylation across generations, including possible interactions with lead exposure, and to see whether maternal in-utero exposure to POPs and lead impairs brain development in her children.
Research Strategy Page 435
Contact PD/PI: Paneth, Nigel S

UG3 PHASE: Hypothesis 1c will be pilot-tested in 125 children assessed at age 4 or above in the ARCH/MMIP cohorts. We will measure POPs and metals in the mother’s NDBS (grand-maternal exposure) and correlate them with the DNA methylation changes in the children’s NDBS and their cognitive scores.
• UH3 PHASE: Using UG3 findings, we will learn which epigenetic changes are especially likely to be changed by grand-maternal exposures while the mother was in utero, setting the stage for us to examine more closely these relationships in the full sample available to us in the UH3 phase.
• POOLED COHORT: California, and perhaps other states have NDBS collections
dating from the 1980’s permitting assessment of maternal in-utero exposures. Extending our ideas in hypothesis 1c to examine rarer neurodevelopmental outcomes and important interactions in a national cohort is an exciting prospect. Hypothesis 1d: Recent in utero lead exposure in Flint, as assessed in NDBS, and in the shed teeth of exposed children will be associated with epigenetic changes and impaired cognitive outcomes. Women in Flint will have bone stores of lead that may be mobilized in pregnancy and be transferred readily across the placenta, where in-utero exposure is toxic at lower levels than later.124 125 The 21 months (April 2014 - December 2015) when acidic Flint River water supplied Flint is the period of maximum exposure to lead and other toxins, though Flint water has yet to be deemed safe. The Flint pregnancy cohort we are now recruiting is thus past the period of maximum exposure. However their mothers and older siblings were likely exposed, and we will modify our protocols to make two additional assessments in Flint: 1) a validated water consumption questionnaire will be administered to pregnant participants during recruitment, largely in the first trimester. 2) Retrieval of NDBS and shed teeth, and neurodevelopmental assessment, of older siblings exposed to Flint River water. We also plan to obtain XRF (X-ray fluorescence) measurements of tibial bone lead levels in mothers post-partum, but this procedure is not included here, because arrangements were incomplete at time of submission. Inclusion criteria for older siblings are birth and residence in Flint between July 1, 2013 and September 1, 2016 to cover both in-utero and early childhood exposure. Metals and POPs can both be measured in shed deciduous teeth. 126 127 128 129 130 In unpublished data, Cassidy-Bushrow, with collaborator Arora, has used laser scanning inductively coupled plasma mass spectroscopy (ICP-MS) to measure heavy metals in 152 shed baby teeth from Wayne County children, showing small differences in lead by trimester of deposition, but lead levels twice as high in Black as in White children (data not shown). We budget only for tooth collection, not analysis, anticipating that, like XRF bone measures, this will be funded by other sources.
• UG3 PHASE: We will pilot tooth collection and NDBS collection in the first 20 Flint enrollees and sibs. • UH3 PHASE: We will examine the relationship of in-utero lead exposure as measured in maternal blood
and NDBS in all offspring of Flint participants, and as assessed in NDBS and shed teeth in their older siblings, in relation to cognitive outcome.
• POOLED COHORT: Although this waterborne exposure is unique, we can pool the findings with any other cohort making similar lead assessments. METHODS USED IN THIS AIM NEONATAL DRIED BLOOD SPOTS: In Michigan, five 0.5 cm2 NDBS are collected on Guthrie cards from all newborns (mostly day 1-2) to test for treatable genetic disorders, typically using only 1-2 spots. NDBS will be retrieved from the Michigan Neonatal Biobank, with half a spot sent to WSU’s Applied Genomics Technology Center (AGTC) for epigenetics, and one spot to Dr. Batterman’s UM lab for POPs/metals. Several "blank" 4mm punches from unspotted areas of card will be controls for each year of birth included in the analysis.
Figure 2. Mother’s (F2) neonatal bloodspots will be used to measure heavy metals and POPs. The mother (F2) who had fetal germline exposure (from F1) will have the brain of her child (F3) studied with behavioral assessment assays.
Research Strategy Page 436
Contact PD/PI: Paneth, Nigel S

EPIGENETICS: Epigenetic analyses will be done in AGTC using the Human Methylation 850K (HM850K) Epic array (Ilumina, Inc.). We have published several papers using this assay and have described novel experimental and bioinformatics approaches for validating and analyzing the data. 131 132 PERSISTENT ORGANIC POLLUTANTS: For the analysis of PFAAs and BPA, a 16-mm diameter disc (equivalent of 50 μL whole blood) is taken from the NDBS filter card. For the analysis of PCB congeners (#138/153, 118, other PCBs), PBDE congeners (#47, other PBDEs, PBB and other BFRs) and organochlorine pesticides (p,p’-DDE, β-HCH, HCB), each NDBS sample is cut using solvent-cleaned scissors and placed in a 10 mL glass tube. The methodology is described here. 133 134 135 This lab has reliably measured heavy metals and POPs in both blood and NDBS.136 137 138 139 140 141 142 143 144 TOOTH MATRIX BIOMARKERS: Maternal pregnancy measures of environmental chemicals may not fully reflect actual fetal exposure because of variability in placental transport and metabolism.145 146 147 This limitation may be overcome by examining human deciduous teeth, whose process of prenatal mineralization accumulates bone-seeking elements such as lead. Our collaborator, Dr. Arora, takes advantage of teeth as chemical repositories and uses histologic and chemical analysis to sample dentine layers that permit the reconstruction of in-utero exposure. 148 149 150 He has shown week-by-week exposure history for lead and manganese may be ascertained 151 152 153 and trimester-specific exposure history for organics throughout early development. 154 155
b. AIM 2: MATERNAL NUTRITION AND ECHO OUTCOMES: Overt micronutrient deficiency in pregnancy causes severe adverse effects in offspring (e.g. iodine deficiency → cretinism; relative folate deficiency→ neural tube defects), but it is uncertain whether marginal nutrient status affects subtler health outcomes, including those measured on a continuous scale, such as cognitive function. Moreover, nutrient metabolism is complex, includes multiple interactions with other substrates, and can only be fully understood in the context of the contemporary environment. An increasingly common form of “mal” nutrition is characterized by the double burden of obesity and sub-optimal micronutrient status, which reflects a US cultural food environment that is abundant in energy but low in nutrient-density. Dietary intake, the primary exposure affecting nutritional status, is one of the most ubiquitous environmental exposures (perhaps second only to air) and is modifiable on both societal and individual levels, thus making it a critical scientific target. Globally, the most common micronutrient deficiencies are iodine, iron, folate, vitamin A, and zinc; all are contributors to perinatal complications, poor growth, and intellectual impairments. In the US, deficiencies of the latter 3 are no longer common (prevalence < 1%), but iodine and iron are lacking, especially among women.156 IODINE: An adequate supply of thyroid hormone in utero and early childhood is essential for normal neurodevelopment.161, 162 Since iodine is an integral component of thyroid hormone, iodine deficiency, which affects over 2.2 billion people worldwide, is the world’s leading preventable cause of intellectual disability.163 Prior to gestational weeks 16-20, the fetus does not make any thyroid hormone,164 and even after the fetus begins to produce thyroid hormone, the maternal thyroid is still required for adequate brain development.165 Severe iodine deficiency in pregnancy produces the syndrome of endemic cretinism, characterized by profound mental retardation, deaf-mutism, and usually severe motor impairment. Less severe iodine deficiency in pregnancy has been associated with increased rates of miscarriage, stillbirth, and increased perinatal and infant mortality.166 More recently, investigations into marginal or mild iodine deficiency have found associations with adverse neurodevelopmental outcomes. A recent study from the UK found marginally low iodine levels, assessed only once in pregnancy, to be linked to lower cognitive ability in offspring at 8-9 y.167 It has also been suggested that mild iodine deficiency in utero may be associated with ADHD.168 In many studies of maternal thyroid function, iodine is not assessed, but even mildly low maternal thyroid (T4) in pregnancy may result in cognitive impairment in offspring,169,170, 171,172,173,174 Most recently, a strong link between low maternal thyroid levels in the 1st trimester and ASD-like behavior in the offspring has been documented.175 Since salt iodization was initiated in 1924, US dietary iodine has been considered adequate. However, the adult median urinary iodine concentration (UIC) fell from 320 µg/L in NHANES I (early 1970s) to 145 µg/L in NHANES III (early 1990s) as shown in Table 10, close to the WHO population-level threshold for iodine sufficiency in pregnancy of 150 µg/L. Could low levels of iodine be playing a role in the observed 73% increase in the US incidence of
Table 10: Urinary Iodine Concentrations (UIC) in NHANES157, 158, 159, 160 1971-74 1988-94 2005-06 2007-10 Median UIC (µg/L) in adults 320 145 164 133 Median UIC in pregnancy (µg/L) 327 141 NA 135 N of pregnant women assessed 208 348 NA 76 % UIC < 50µg/L in pregnancy 1% 7% 11% 17% % UIC < 50µg/L in women 15-44 y 4% 15% 17% 13%
Research Strategy Page 437
Contact PD/PI: Paneth, Nigel S

congenital hypothyroidism between 1987 and 2002?176 Two environmental contaminants - perchlorate and thiocyanate – are competitive inhibitors of thyroidal iodine uptake and lead to decreases in thyroid hormone synthesis. Among the 36% of women with urinary iodine values <100 μg/L in NHANES 2001-2002, urinary perchlorate was directly correlated with serum thyroid stimulating hormone (TSH), and inversely correlated with serum T4.177 Our consultant Elizabeth Pearce has reported associations between 1st trimester maternal perchlorate exposure and decreased offspring IQ in a UK pregnancy cohort.178 Thiocyanate, found in some vegetables and as a smoking byproduct,179 is much less potent than perchlorate as an iodine competitor, 180 but maternal smoking has been linked to lower serum T4, increased TSH, and thyroid enlargement in newborns,181,182 and to lower breast milk iodine. 183 Pearce found T4 levels in the first trimester were significantly lower in smoking than in non-smoking women.184 IRON: Iron deficiency is found in 9.5% of US women aged 12-49; the prevalence in non-Hispanic black and Mexican-American women is double that in White women.156 Low prenatal levels of iron can alter myelination of neurons and affect dopamine metabolism and hippocampal development.185 Iron deficiency has been shown to be a risk factor for hypothyroxinemia, independent of iodine and thyroid autoimmunity, in both pregnant and non-pregnant women.186 Even sub-clinical iron deficiency may be involved in modulating immune responses during pregnancy,187 and sufficient iron intake can mitigate harmful effects of prenatal lead exposure.188 OBESITY: As many as 20% of US women enter pregnancy with a BMI ≥ 30 kg/m2,189 putting their children at risk of being overweight or obese.190 Our own research (Johnson, Cassidy-Bushrow) shows a doubling of the odds of obesity in 2 year olds when mothers were obese before pregnancy.191 Of even greater concern are developmental deficits associated with maternal obesity. Delayed infant motor development has been seen in the offspring of obese mothers,192 and in a large study, kindergartners born to obese mothers had a higher prevalence of learning and behavioral disabilities.193 The US Collaborative Perinatal Project showed a U-shaped relationship between maternal pre-pregnancy weight and child IQ at age 7 y.194 Researchers in this team (Mehta, Kerver, Sokol, Keating, Paneth) recently reviewed the growing literature linking maternal obesity to cerebral palsy, ASD, cognitive deficits, and ADHD.3 Obesity and micronutrient deficiency are linked. In non-pregnant US women (NHANES), deficiencies in micronutrients, including vitamins A, C, D, E, and carotenoids are more common in obese than in non-obese women.195 In convenience samples, obese pregnant women also had lower levels of essential fatty acids, carotenoids, and micronutrients than leaner counterparts.196 197 198 It is unclear whether these low nutrient levels are due to insufficient dietary intake, altered metabolic processes, or both. A small but growing body of literature suggests that interactions between environmental exposures, micronutrient status, and characteristics of the gut microbiome contribute to obesity199 200 201 although this has not yet been adequately studied in humans. We do not know how maternal pre-pregnancy obesity interacts with prenatal environmental insults to the fetus that produce later ill health. Potential etiologic/mechanistic theories are underdeveloped and must take account of the broad social and biological context in which obesity is embedded, including maternal dietary intake, inflammation, epigenetic modification, and characteristics of the gut microbiome. In this aim, we will assess the individual and combined effects of iodine and iron status, thyroid function, and pregnancy related weight on perinatal complications, cognitive outcomes, and child obesity. Hypothesis 2a: Low pregnancy iodine and/or iron status, agents interfering with thyroid iodine uptake (perchlorate, thiocyanate), and abnormal thyroid hormone function will be associated with cognitive outcomes.
• UG3 PHASE: With 125 mother-child pairs in the ARCH/MMIP cohort in the UG3 phase, we will have insufficient power to fully test our hypotheses, but we will pilot test all required study components using continuous measures of key exposures and outcomes.
• UH3 PHASE: We will increase our sample size with complete data to formally test hypothesis 2a. • POOLED COHORT: We will study pregnancy nutrition in relation to major neurodevelopmental outcomes
– ASD, severe cognitive impairment and cerebral palsy – for which the pooled cohort will have sufficient power. Use of the ECHO cohorts can help us to predict how specific groups respond to environmental exposures, such as perchlorates, thiocyanates and lead, and whether better nutritional status may mitigate harmful effects. We will investigate additional micronutrients, beyond iodine and iron, for independent effects as well as interactions between nutrients and exposures including maternal smoking and POPS and other environmental chemicals.
Research Strategy Page 438
Contact PD/PI: Paneth, Nigel S

Hypothesis 2b: Pregnancy-related weight and weight changes and social circumstances will be linked to childhood obesity, and will amplify associations found in hypothesis 2a.
• UG3 PHASE: We will assess direct relationships between pregnancy related weight (pre-pregnancy weight, pregnancy weight gain, and postpartum weight retention at child age 4 y) and child obesity at age 4 y.
• UH3 PHASE: We will assess modification of the associations found from testing hypothesis 2a by pre-pregnancy weight status, which we will be able to undertake with sufficient power because of our larger samples size by the time of UH3. We will use analytic procedures described later in this application.
• POOLED COHORT: We propose to assess effects of uncommon nutrition-related exposures (e.g. extreme maternal obesity, “healthy” pregnancy diet) on both common and rare ECHO outcomes. Hypothesis 2c: The exposure → outcome effects found in 2a and 2b will be mediated by differences in the maternal and/or child gut microbiome and infant feeding patterns.
• UG3 PHASE: In the 2nd year of UG3, we will test our procedures for stool sample collection and assaying from prospective MARCH enrollees to assess the gut microbiome.
• UH3 PHASE: We will assess mediation of our exposure outcome effects by the gut microbiome. • POOLED COHORT: Other cohorts may have collected gut microbiome samples, and we welcome the
opportunity to pool our information and examine the microbiome in relation to nutrition and other factors. ECHO can encourage collaboration among the community of scientists interested in the infant microbiome. METHODS: MICRONUTRIENTS: Stored maternal samples from the children who undergo cognitive testing at age 4 y or older will be assessed. We will use 1st trimester maternal serum to measure iron status (ferritin) and thyroid function (FT4, TSH, and TPO-Ab), and 1st, 2nd and 3rd trimester urine to measure iodine, perchlorate, and thiocyanate. Because of variation in urinary iodine intake, single spot urine samples cannot be used to fully determine iodine status in individuals, although a recent Australian study reported that averaging two separate spot UIC’s to correct for within-person variation in urinary iodine excretion reduced the proportion of individuals with spuriously low or high values.202 Our access to urine from each trimester will provide a good sense of overall iodine nutriture in pregnancy, as well as group variations by trimester. Our urine aliquots are collected prior to any dipstick measurements, since some test strips are known to contain iodine as a reagent for blood and glucose testing.203 DIETARY MEASURES: ARCH survey measures were selected from the PhenX Toolkit (consensus measures of Phenotypes and eXposures Ver 5.6)204 in the domains of demographics, psychosocial, reproductive health, nutrition, and physical activity. This “Toolkit” contains well-established, broadly applicable, low-burden measures intended for use in large-scale studies.205 Dietary measures we will use in this study were selected from the PhenX Toolkit (Ver 5.6) and include questions to assess usual intake of fat (% energy), fiber (g), fruit and vegetables (servings/d), dairy food (servings/d), and added sugars (tsp/d) because they are low burden, have been validated against the 24-hour dietary recall206 207 208and represent dietary components likely to affect weight and chronic disease.209 210 211 Maternal diet will be assessed to characterize participants’ 1st trimester dietary intake for assessing the relationships between prenatal nutritional status and other factors in relation to ECHO outcomes. In addition to assessing perchlorate and thiocyanate as inhibitors of iodine uptake, thiocyanate is also a marker of exposure to cigarette smoke and we will use it in conjunction with smoking history on the birth certificate to assess direct and interacting effects of maternal smoking on child outcomes. INFANT GUT MICROBIOME: Infant fecal samples will be obtained at age three months using the procedure of our ARCH GUT study. A stool collection kit is mailed to the participant’s home and returned by mail after the sample is collected. Received samples will be homogenized and aliquots will be stored at -800c until processing. The microbiome will be profiled using a 16S rRNA gene sequencing approach. Total fecal DNA will be extracted using a PowerSoil bacterial DNA Isolation Kit (Mo Bio Laboratories) and PCR-amplified with universal bacteria primers targeting V34 variable region of the 16S rRNA genes.212 Amplicons will be multiplexed and sequenced using paired end 2 x 250 bp runs on the Illumina MiSeq platform at the MSU Genomic Core. Sequences will be analyzed using the Mothur software package,213 following its standard operation procedures for MiSeq data. Sequence reads will be filtered based on quality scores (>35) and chimeric reads removed. Cleaned sequence reads will be aligned to the reference SILVA database provided in Mothur and operational taxonomic units (OTU) will be then generated by clustering sequences using the
Research Strategy Page 439
Contact PD/PI: Paneth, Nigel S

average neighbor setting in Mothur at 97 % similarity. Each OTU will be assigned a taxonomic classification from phylum to genus using the reference Ribosomal Database Project (RDP) database provided in Mothur.
AIM 3: VIRAL INFECTION, OBESITY, INFLAMMATION AND AUTISM RISK Viral infection in pregnancy: Although it has been more than 70 years since Gregg described the association of prenatal rubella and cataract,214 much remains unknown about the relationship of viral infection in pregnancy to fetal development. Congenital infection of the fetus with cytomegalovirus (CMV), herpes simplex virus-2 (HSV2) and rubella can cause major neurosensory deficits,215 216 217 218 learning disabilities and psychiatric disorders.219 However, congenital CMV and HSV2 infections are rare (estimated birth prevalence of 0.5%220 and 0.35%221 respectively) and congenital rubella has been virtually eliminated in the US,222 largely because the placenta is an effective barrier to most viral transmission.223 But maternal infection and/or reactivation with CMV, HSV-2 and influenza is common (60-90%, 18% and 40%, respectively), and can induce systemic and placental inflammation with potentially harmful effects on fetal brain development. We and others have shown224 225 that viral infection of decidua and placenta occurs absent congenital infection, a mechanism proposed for Zika virus-induced brain damage.226 Such indirect harm has been proposed for the effects of influenza, a virus linked to systemic maternal inflammation, on risk of behavioral disorders in the offspring, including autism and schizophrenia,227 228 229 230 231 232 233 without evidence of fetal transmission.234 By simultaneously identifying pregnancy viral infection in maternal serum, maternal, placental and neonatal inflammation, and neurodevelopmental disorders in offspring, as we propose in this study, we can determine the distinct roles of viruses and inflammation in relation to neurodevelopment. Maternal obesity: Infectious agents are not the only stimulus to inflammation. Obesity is an inflammatory state, and in pregnancy can produce intrauterine and neonatal inflammation.235 Obesity-related perturbation of maternal inflammatory cytokines and related pathways may alter placental cytokine expression 236 237 and lead to acute and chronic placental inflammation that impacts both placental function and fetal development. 238 239 Few studies have assessed the effects of maternal obesity on placental inflammation in human placentas and related this to neonatal inflammation and neurodevelopmental disorders such as autism. Autism: Prenatal inflammation has been associated with elevated risk of offspring ASD or autism-like behaviors in both animal models 240 241 and human population studies.242 243 Maternal obesity has also been linked to ASD.3
A common pathway from both exposures might be placental and neonatal inflammation. While we do not have power to study ASD, as described earlier, we obtain several measures correlated with and predictive of, ASD. Hypothesis 3a: Increasing maternal BMI and/or viral infection, with neonatal inflammation, will be associated with heightened MCHAT/SRS-2 scores, indicators of autism risk.
• UG3 PHASE: We will examine 125 ARCH/MMPI pregnancies to assess the relationship between BMI and/or viral infections in pregnancy, neonatal inflammation, and children’s 2-year MCHAT/4-year SRS-2 scores (i.e. autism risk).
• UH3 PHASE: This hypothesis will be extended to the larger sample size available in the full study. BMI will be measured at first pregnancy visit and both pregnancy weight gain and post-partum weight loss will be assessed in association with outcomes. Maternal influenza infection, CMV and/or HSV-2 infection/reactivation will be assessed in first visit specimens.
• POOLED COHORT: The focus of this hypothesis is on the effect of maternal viral infection, which could be assessed in any other cohort with maternal blood samples in relation to formally diagnosed ASD. If newborn blood spots are available, the mediating role of neonatal inflammation can also be studied. METHODS: Influenza A virus: Measured Influenza A IgG (Abcam, ab108745) in pregnancy, with maternal interview to assess influenza immunization status. Cytomegalovirus: Third trimester maternal serum will be evaluated for CMV IgG and IgM using enzyme-linked immunosorbent assay (ELISA; Abcam Ab108725, Ab108724); CMV seronegative= CMV-IgM and CMV-IgG negative; CMV seropositive: CMV-IgM negative and CMV-IgG positive; Primary CMV infection= CMV-IgM positive and CMV-IgG negative. Herpes simplex virus-2: Third trimester maternal serum will be evaluated for HSV2 IgG and IgM using ELISA (Abcam Ab108739, Ab108740); HSV2 seronegative= HSV2-IgM/HSV2-IgG negative; HSV2 seropositive: HSV2-IgM negative/HSV2-IgG positive; primary HSV2 infection= HSV2-IgM positive/HSV2-IgG negative. Newborn inflammation: Newborn blood spots will be analyzed by Dr. Raina Fichorova of the Genital Tract
Research Strategy Page 440
Contact PD/PI: Paneth, Nigel S

Biology Laboratory, Brigham and Women’s Hospital as previously described.244 Samples will be analyzed in duplicate using the Meso Scale Discovery electrochemiluminescence multiplex platform and Sector Imager 2400, which has been validated by comparisons with traditional ELISA. Cytokines and other inflammatory factors to be assayed are listed in table 11. This is a well-established panel of proteins that is inclusive of multiple measures of inflammation including factors that regulate immune cell recruitment and function, regulators of the vasculature, indicators of systemic inflammation, and tissue modifying enzymes. Hypothesis 3b: Maternal viral infections and/or obesity that induce placental inflammation and reduce villus branching will have the strongest relationships to neonatal inflammation and increased risk for autism.
• UG3 PHASE for Hypotheses 3b and 3c. Both hypotheses require placental samples prepared as planned in this study. The UG3 phase will thus consist of piloting the placental protocol in a limited number of specimens. Because enrollment of new pregnancies begins in year 2, the first placentas will only become available in the second half of the year. But the protocol will be in place, and collection initiated by year 3.
• UH3 PHASE - ADDITION OF PLACENTAL DATA: We will examine all MARCH pregnancies with complete data to assess the relationship between placental inflammation and reduced villus branching in a model that includes BMI, viral infections in pregnancy and neonatal inflammation and age 4 SRS scores.
• POOLED COHORT: Any cohort with placental histology recorded should be able to be pooled with ours to examine this exposure in relation to diagnosed ASD. The 3D imagers are available for purchase, and training and consulting can be provided. 3D imaging of placentas can also be provided as a service PLACENTAL METHODS: Histologic Assessment: Whole placentas will be collected from MARCH births and shipped in formalin to Dr. Salafia, who will obtain one cross-sectional slice each from either end of the umbilical cord and a “roll” of extra-placental membranes from the disk edge to the site of membrane rupture. One full-thickness sample of grossly normal placental parenchyma (including chorionic plate, villi and basal plate) will be taken from each placental quadrant and scanned and processed for histological evaluation. In addition, placental areas of interest (identified by imaging below) will undergo H & E staining and histological analysis to identify acute and/or chronic inflammatory lesions and reduced chorionic branching. Placental inflammation will be distinguished by cell type (chronic-lymphocytes and monocytes, acute-neutrophils) and anatomical site (chronic-chorionic villi/acute-membrane). Identification of placental inflammation and reduced villus branching with 3D placental scanning: Neurogenesis in general, and in autism spectrum disorders in particular, depends on vascular networks. The placenta is a fetal organ with a branching structure driven by fetal angiogenesis. Salafia and colleagues have shown in pilot work that placentas from children with ASD showed reduced umbilical cord displacement and perimeter variability, and a nearly 50% reduction in chorionic surface branch points, or a placental “simplification”, compared to unaffected controls. This was associated with evidence of both acute and chronic placental inflammation. These changes were identified using 2D and 3D scanning, image segmentation and automated analysis of branching and inflammation, technology and expertise developed by Dr. Salafia and colleagues.5 This approach minimizes inter-rater variability by scoring through digitized “regions of interest”. Hypothesis 3c: Maternal viral infection will induce a heightened placental inflammatory response to the bacterial microflora at the maternal-fetal interface and this response will be positively correlated with concentration of the LPS-containing gram-negative species.
• UH3 PHASE: INCORPORATION OF THE PLACENTAL MICROBIOME: While the upper reproductive tract was once thought to be sterile in pregnancy, recent evidence indicates that the healthy placenta is home to a vibrant microflora245 in a constant state of homeostatic immune activation to maintain appropriate numbers and kinds of organisms while avoiding excessive inflammation that could damage mother or fetus. We and others have found that viral infections can affect the host response to bacteria by affecting the innate immune signaling within the placenta246 and/or by inducing maternal glucocorticoids.247 We have found that placental
Table 11: INFLAMMATORY MARKERS TO BE ASSESSED Interleukin-6 (IL-6) and IL-6R Interleukin-1 β (IL-1β) Matrix Metalloproteinase-9 (MMP-9) Myeloperoxidase (MPO)
Vascular Endothelial Growth Factor (VEGF) and VEGF-R2
Intercellular Adhesion Molecule -1 (ICAM-1; CD54)
Tumor Necrosis Factor-α (TNF-α) and TNF Receptor-2 (TNF-R2)
RANTES
C-Reactive Protein (CRP) Erythropoietin (EPO) Serum amyloid (SAA) Thyroid-stimulating hormone (TSH)
Research Strategy Page 441
Contact PD/PI: Paneth, Nigel S

viral infection enhances inflammation in response to lipopolysaccharide (LPS), a key antigenic component of many gram-negative bacteria. Could viral infection be inducing a sensitized placental inflammatory response to the placental flora that are usually harmless? We will collect frozen placental biopsies within 4 hours of labor for 200 pregnancies. We will then select placentas from 50 mothers with viral infection and 50 controls and determine if they have placental inflammation and if degree of inflammation is associated with LPS-containing placental microflora.
• POOLED COHORT: We anticipate that some cohorts (for example the ELGAN cohort in which Paneth participates) will have placental microbiome data which may be pooled for conjoined analyses. METHODS: Frozen placental specimens: Collection of frozen placentas is currently underway in a sub-study of ARCH (referred to in Table 2 as ARCH-PLACENTA) and will be continued in the MARCH cohort in selected hospitals who can carry out the protocol required. Placental specimens are flash frozen within 6 hours of delivery. Upon hospital admission, consented ARCH/MARCH participants are identified and the study team coordinator on call is notified. The placenta is moved to the pathology department and ARCH staff collect biopsies for freezing. The placenta is placed with the maternal side (basal plate) facing upwards and a sterile scalpel and forceps are used to remove the top 3-5mm, which is the maternal basal plate. 1 cm3 sections are removed, not including the chorionic plate, and this is repeated 4 times in a circumferential manner approximately 4 cm from the cord insertion site. Tissue is placed in sterile closed vials with ARCH ID and is snap frozen immediately in liquid nitrogen. Placental DNA analysis for microbiome: Approximately 100 mg of tissue from the 4 samples collected per placenta will be used for DNA extraction using MO-BIO Powersoil DNA isolation kit. We will then use 16S sequencing to identify the placental bacterial composition as previously described.248 The 16S sequencing and analysis will be performed by the MSU Genomics Core Facility. The current implementation of Mothur assigns OTU only to genus level, so in addition to using Mothur, as described in Aim 3, we will also use a classifier from the Ribosomal Database Project at MSU to classify cleaned sequence reads directly. This process could provide assignments up to species level which will facilitate the tabulation of LPS-containing bacteria.
D7. STATISTICAL ANALYSIS While our aims are distinct, the common ECHO outcomes make it feasible to discuss the analytic approach to all aims together, noting procedures specific to any aim or hypothesis. Our aims deal primarily with continuous outcomes, be they cognitive tests scores from the executive function arm of the toolbox assessment or behavioral assessments such as SRS-2. All aims consider unadjusted associations, associations adjusted for potential confounders, effect mediation and effect modification, all of which we address here. Unadjusted Analyses. The primary outcome for Aims 1 and 2 will be the WPPSI, and for Aim 3, the SRS-2 score, both at age four. If data are missing at age four, we will consider examining the Bayley Score at age two and/or WISC at the age six. In the unlikely event that scores are not normally distributed, we will consider transformations to normality (e.g., log, Box-Cox), after assessment of potential outlying observations. We hypothesize that higher exposure to POPs/metals (Aim 1), lower levels of micronutrients (Aim 2) will be inversely correlated with cognitive score, while higher levels of inflammation will be inversely correlated with SRS-2 score. As the primary outcomes and key exposures are of interest are continuous, our first analyses will use linear regression; we will assess the possibility of non-linear associations between exposure and outcome using splines and other forms of functional data analysis.249 For assessment of the SRS-2 in infants with and without evidence of maternal viral infection (Aim 3), we use a two-sample t test in the univariate stage. Because Aim 1 and Aim 3 involve assessments of multiple exposures (as many as 11 POPs/metals, 16 inflammatory markers), we will also create summary exposure measures using the first principal component of the POPS/metals measures and the inflammatory markers measures respectively. For Aim 3, we will conduct a preliminary analysis to determine which inflammatory markers are associated with viral infection using a logistic model with viral infection status as the dichotomous exposure and each inflammation marker as a separate outcome. We will use the Holm procedure250 251 to correct for multiple testing. The results of this preliminary analysis will be used to construct an index of the difference in the average level for markers positively associated with viral infection and the average level negatively associated with viral infection. Adjusted Analyses. Our adjusted primary analyses for continuous cognitive test scores will use multivariate linear regression, adjusted for known correlates of child IQ, such as maternal IQ, education, race, income, marital status, neighborhood measures of socioeconomic status, and other potential confounders, basing our
Research Strategy Page 442
Contact PD/PI: Paneth, Nigel S

judgement on the extent to which they are related to exposure and outcome. The set of variables to control for in SRS-2 analyses are less well-known, and we will carefully consider potential confounders, whose insertion into regression models will be guided largely by scientific considerations and on the extent of change in regression coefficients for the outcome when the variable is in or out of the model. Type I error in these analyses will be controlled using Bonferroni or false discovery rate (FDR) corrections.252 We will also consider extremes of exposure and outcome (e.g. top decile of exposure, bottom decile in cognition) using either ANOVA (for categorical exposure measures) or logistic regression (for dichotomized developments measures). For analyses involving dichotomous covariates (e.g. viral infection status) we will use logistic regression models. In Aim 3, we must consider the perinatal outcome of gestational age carefully, because premature birth is both a consequence of inflammation and a potent risk factor for nearly all neurodevelopmental outcomes. While we are aware of arguments to the contrary,253 we will adjust for GA in assessing the association of inflammation with SRS-2 scores, but also look closely at the unadjusted finding. Mediation. We assess mediation by proportion of treatment effect explained (PTE) by the mediator. We will use traditional approaches based on the change in the association of the primary predictor with the outcome after adjustment for the hypothesized mediator, as well as more recent methods that relax the assumption of no interaction between the exposure and the mediator.254 We will also consider sensitivity analyses that relax the assumption of no unmeasured confounding between the mediator and the outcome.255 For Aim 1, mediators of interest are epigenetic changes on blood spots; for Aim 2, they include maternal thyroid function; for Aim 3, placental/neonatal inflammation. Mediation by epigenomic and microbiomic findings is addressed below. Effect Modification. We are attentive to the interactions among our hypotheses and avoid considering them in isolation from each other. Our models will incorporate interactions among the three key exposures of interest: POPS/metals; nutrition deficiencies, and viral infection and inflammation, as well as other exposures such as social/neighborhood characteristics, psychosocial factors, and other host factors. Because we do not have clear prior hypotheses for these interactions, we will adjust for multiple comparisons as above. Power. The UG3 phase is for pilot testing, but with a sample of 125, we have 80% power to detect a 0.25 standard deviation (SD) difference in WPPSI for each SD change in unadjusted exposure measure (assuming a linear relationship and Type I error =.05). For the UH3 phase, with the sample size we anticipate enrolling and testing, we will have 80% power to detect a 0.09 SD difference with the same assumptions. For the UH3 phase, with a Bonferroni correction for multiple comparisons, we have 80% power to detect a 0.12 SD difference for POP/metals and 0.13 for inflammatory markers. For construction of the inflammation index, we have 80% power to detect a 0.7- 0.9 SD change in inflammation markers between infected and non-infected births (after Bonferroni correction), depending on the prevalence of infection. For mediation assessment, we have 80% power to detect PTE of 6% or greater for a single hypothesized mediator.256 In our small Flint sample, we have 80% power to detect a 0.28 SD change in IQ per SD in blood lead. Microbiome: The microbiome is hypothesized to mediate Aim 2 and 3 hypotheses. Testing the association of microbiome composition with exposure or outcome variables using OTU abundances directly is difficult due to high dimensionality, non-normality and inherent phylogenetic relationships in the OTU data. We will use distance-based statistical tests in our analyses. The unweighted and weighted UniFrac distances are widely used distance measures for beta diversity and we will calculate them with UniFrac algorithms implemented in Mothur. Our goal is to evaluate whether early infant microbiome composition is associated with maternal nutritional status (such as measures of iodine and iron status) as well as whether microbiome composition is also associated with outcomes (such as cognitive function). To accomplish this, we will use distance-based non-parametric testing. We will apply the PERMANOVA procedure,257 which partitions the distance matrix among sources of variation, fits linear models to distance matrices and uses a permutation test with pseudo-F ratios to obtain the P-values. These analyses will be accomplished using the ‘adonis’ function from R package ‘vegan’. While causal mediation analysis258 can be used to examine whether alpha metrics of the gut microbiome (e.g. richness, evenness and diversity) mediate associations described in Aim 2, given the large number of individual taxa present in the human gut, alternative approaches will be needed to examine taxa-specific mediation. We will use a two-step modeling approach to identify taxa associated with both an exposure of interest (e.g. maternal obesity) and outcome (child body size). In both stages, we will fit multi-taxa generalized linear models (GLM) using an elastic net approach;259 resulting taxa will then be tested individually as potential mediators. A q≤0.05 (i.e. FDR threshold) will be used to determine significance.260
Research Strategy Page 443
Contact PD/PI: Paneth, Nigel S

Epigenome: The processing of epigenomic data in Aim 1 yields a normalized methylation percent (β value). β values will annotated using the “exprmethy450” object created using Illumina Methylation Analyzer (IMA), in the R environment (R> 2.13.0). The probe IDs of the β values will be matched with appropriate annotations to prevent errors in methylation analysis. Normalized probe values will be further filtered by the detection p value (i.e., a test of the target signal being different from the background). Probes with a detection p value ≤ 0.05 will be selected for analysis. These filtered β values will be used in the subsequent analyses for Aim 1. We will use the Welch t-test for unequal variances for unadjusted analyses comparing exposed and unexposed groups. Adjusted analyses will use beta regression with a probit link using the betareg package,261 which accommodates the heteroscedasticity inherent in methylation data. We will also consider using the methylation data in mediation models, where the β value will be both a dependent variable in a mediator model and an independent variable in an outcome model. We will identify CpG sites associated with exposures using beta regression and adjust for multiple testing using the qvalue package in R to estimate the false discovery rates (FDR).262 Only single CpG sites having an FDR ≤ 0.10 will be carried forward to the analysis of outcome models. Because neighboring methylation or methylation sites associated by their relative distance from each other may jointly be affected by environmental exposure to toxicants, we will use the boundedClusterMaker function in the minfi package to generate regional clusters of CpG sites, and use the average methylation percent for all sites within a cluster as the dependent variable in the mediator models.263 Outcome models will include either the β value for single sites or the average β value for regional clusters. Additionally, we will use annotations of the identified sites and clusters to group the sites and clusters. We will create an index for each group of sites/clusters with similar annotations (e.g., promoter for a specific gene, located in a known enhancer) and calculate an index of the difference in the average levels between CpG sites/clusters positively associated with outcome and CpG sites/clusters negatively associated with outcome. The potential function of any single site associated with outcome will be examined using Gene Set Enrichment Analysis (GSEA)264 to determine if any functional annotations are enriched among the significant CpG sites. Other Considerations and problems anticipated. A number of additional statistical issues may have to be addressed in the proposed analyses; space precludes detailed consideration, but we summarize them here. Transformations: If transformations to normality for the continuous outcome fail, we will consider use of generalized linear models with differing link functions (log; power functions) to improve model fit. Loss to follow-up: As in any cohort study, we anticipate missing data either at the variable level (failure to answer a survey question, loss of a blood draw for assay) or the unit level (failure to complete a scheduled data collection; loss to follow-up). For small amounts of variable-level missing data (<5%), we will conduct complete case analyses or incorporate missingness indicators in the regression. For larger amounts of variable-level missing data, we will utilize multiple imputation using sequential regression imputation 265 to handle general missing data patterns. For unit non-response, we will develop non-response weights by estimating probability of non-response using all available information in previous waves. Longitudinal data: While our descriptions of the analyses focus on single cross-sectional outcomes (e.g. cognition at age 4), other secondary analyses may have outcomes that are measured repeatedly in the same individual (e.g. BMI). Such analyses will make use of standard methods to account for within-subject correlation, including use of linear/generalized linear mixed models and generalized estimating equations. Sampling weights: When analyzing data from the MARCH probability sample, we will use sampling weights to adjust for unequal probability of selection, nonresponse, and calibration to known Michigan population distributions. Taylor Series linearization estimates of regression parameter variances will be used to account for sampling weights, sampling strata, and sampling units. Separate analysis of the probability (MARCH) and convenience sample (ARCH) datasets will be conducted. Where differences are small, analysis will proceed with the datasets combined. If larger differences are found, analyses will be done separately, and the differences will be the subject of discussion of results.
Research Strategy Page 444
Contact PD/PI: Paneth, Nigel S

OMB Number: 0925-0002
Tracking Number: GRANT12144486 Funding Opportunity Number: RFA-OD-16-004. Received Date: 2016-04-14T17:20:31.000-04:00
Cumulative Inclusion Enrollment ReportThis report format should NOT be used for collecting data from study participants.
Study Title: Prenatal Exposures and Child Health Outcomes: A Statewide Study
Comments: ARCH n-1542
Racial Categories
Ethnic Categories
Not Hispanic or Latino
Female Male Unknown/Not Reported
Hispanic or Latino
Female Male Unknown/Not Reported
Unknown/NotReported Ethnicity
Female Male Unknown/Not Reported
Total
American Indian/Alaska Native 0 0 0 0 0 0 0 0 0 0
Asian 0 0 0 0 0 0 0 0 0 0
Native Hawaiian orOther Pacific Islander 0 0 0 0 0 0 0 0 0 0
Black or African American 326 106 0 0 0 0 0 0 0 432
White 666 216 0 0 0 0 0 0 0 882
More than One Race 0 0 0 0 0 0 0 0 0 0
Unknown or Not Reported 0 0 0 172 56 0 0 0 0 228
Total 992 322 0 172 56 0 0 0 0 1542
Study 1 of 3
Page 445
Contact PD/PI: Paneth, Nigel S

OMB Number: 0925-0002
Tracking Number: GRANT12144486 Funding Opportunity Number: RFA-OD-16-004. Received Date: 2016-04-14T17:20:31.000-04:00
Cumulative Inclusion Enrollment ReportThis report format should NOT be used for collecting data from study participants.
Study Title: Prenatal Exposures and Child Health Outcomes: A Statewide Study
Comments: MMIP n=272 (University of Michigan)
Racial Categories
Ethnic Categories
Not Hispanic or Latino
Female Male Unknown/Not Reported
Hispanic or Latino
Female Male Unknown/Not Reported
Unknown/NotReported Ethnicity
Female Male Unknown/Not Reported
Total
American Indian/Alaska Native 0 0 0 0 0 0 0 0 0 0
Asian 0 0 0 0 0 0 0 0 0 0
Native Hawaiian orOther Pacific Islander 0 0 0 0 0 0 0 0 0 0
Black or African American 10 3 0 0 0 0 0 0 0 13
White 193 64 0 0 0 0 0 0 0 257
More than One Race 0 0 0 0 0 0 0 0 0 0
Unknown or Not Reported 0 0 0 2 0 0 0 0 0 2
Total 203 67 0 2 0 0 0 0 0 272
Study 2 of 3
Page 446
Contact PD/PI: Paneth, Nigel S

OMB Number: 0925-0002
Tracking Number: GRANT12144486 Funding Opportunity Number: RFA-OD-16-004. Received Date: 2016-04-14T17:20:31.000-04:00
Cumulative Inclusion Enrollment ReportThis report format should NOT be used for collecting data from study participants.
Study Title: Prenatal Exposures and Child Health Outcomes: A Statewide Study
Comments: MARCH n=82
Racial Categories
Ethnic Categories
Not Hispanic or Latino
Female Male Unknown/Not Reported
Hispanic or Latino
Female Male Unknown/Not Reported
Unknown/NotReported Ethnicity
Female Male Unknown/Not Reported
Total
American Indian/Alaska Native 0 0 0 0 0 0 0 0 0 0
Asian 0 0 0 0 0 0 0 0 0 0
Native Hawaiian orOther Pacific Islander 0 0 0 0 0 0 0 0 0 0
Black or African American 8 3 0 0 0 0 0 0 0 11
White 50 17 0 0 0 0 0 0 0 67
More than One Race 0 0 0 0 0 0 0 0 0 0
Unknown or Not Reported 0 0 0 3 1 0 0 0 0 4
Total 58 20 0 3 1 0 0 0 0 82
Study 3 of 3
Page 447
Contact PD/PI: Paneth, Nigel S

PROTECTION OF HUMAN SUBJECTS Risks to Human Subjects a. Human Subject Involvement, Characteristics, and Design This Human Subjects Research meets the definition of “Clinical Research”. The Michigan Archive for Research in Child Health cohort is an efficient design to study the ECHO outcomes, with minimal risks to human subjects. IRB approval has already been granted for East Lansing based ARCH cohort and the pilot expansion of that work into four new sites. Approval was obtained from Michigan State University’s Committee on Research Involving Human Subjects (UCRIHS), now called Biomedical and Health IRB or BIRB, for enrolling subjects into ARCH and MARCH. Characteristics of the Proposed Population: We will recruit approximately 1000 pregnant women from the general population who are arriving for first prenatal visit. Excluded are only minor age (under 18) and non-English speaking women. Subjects will be recruited from 22 ob/gyn practices and clinics that send births to 11 hospitals across Michigan, that have been chosen as able to provide a weighted, probability based sample. We will include the following special populations for this investigation of etiology of cerebral palsy which originates in the perinatal period and thus involves mothers and their children: • pregnant women, incidentally when they are mothers of CP children or controls • children ages 2-15 (in special cases siblings without CP from age 1 and age 16 and older) • children with disability (cases), including children of diminished mental capacity b. Sources of Research Material: Subjects will be asked permission for the following data collection activities: 1) Maternal interview and questionnaires specifically designed for the study, and medical records review from pregnancy, labor and delivery; 2) Neonatal medical records review 3) Laboratory study of previously collected blood specimens from mother (prenatal) and child (neonatal) and their previous test results. 4) DNA collection and storage of salivary samples from parents and child for analysis of genetic variations 6) For cases only, classification of case status by neurologist or other physician Data will be collected by interviewing the mother (by phone, in person, or by mail) and abstracting medical records from multiples sources, including prenatal and pediatric care, neurology practices, and hospital records of labor and delivery and newborn care, including birth certificates and hospital discharge summaries. Mothers of cases will also complete several brief questionnaires about their child’s CP and functioning. At time of enrollment at the recruiting physician’s office or later at home, mothers, fathers and children will be asked to provide saliva samples obtained by spitting into a vial (or swabbing cheek cells) for genetic studies. Saliva samples collected at home will be mailed to the central study office in special mailing packages. Area neurology practices and other health care providers will provide access to CP cases and area primary care practices access to controls. The MSU Prenatal Screening Program will provide stored maternal serum for biomarkers of cerebral palsy. Michigan Department of Community Health will provide newborn screening dried blood spots for tests of biomarkers, and data from newborn screening results. Laboratory measurements of biomarkers will be provided by the laboratories of the following co-investigators: for mRNA analyses on newborn blood spots: Dr.Julia Busik, MSU Department of Physiology; Dr. James Resau of the Laboratory of Microarray Technology of the Van Andel Research Institute, mRNA laboratory of the Van Andel Research
Protection of Human Subjects Page 448
Contact PD/PI: Paneth, Nigel S

institute. And for viral DNA analyses of blood spots: Dr. Mark Schleiss, University of Minnesota Department of Pediatrics; for analyses of maternal serum, Dr. Sainan Wei, MSU Prenatal Screening Laboratory. The study investigator and office and field directors, and their designated assistants, will have access to individual identifiable private information. All study information will be kept confidential by the investigators and study team, and kept in locked file cabinets in locked offices. Specimens sent to laboratories are bar-coded and contain no names or other personal identifying information. The computerized RIX database is password protected and study team members only have access to those parts of the database that are necessary for their work activities. Laboratory personnel do not have access to personal health information (PHI) in the RIX database. c. Potential risks: This case-control study will collect data both from previously collected sources and from non-invasive procedures specifically initiated by the study. Observational data obtained from medical records and stored blood samples is not known to entail risks other than possible loss of confidentiality. Minor noninvasive procedures such as maternal interview and salivary sample are considered low risk. Upon parental request, we will inform parents about study laboratory results, which may evoke emotions in parents concerned about the causes of CP in their child, or in control parents, about findings that have unexpected prognostic implications. Test results, if not kept confidential, could affect medical care and insurance, employment, and psychological state. Utmost care will be used to communicate and interpret these results to parents, including referral to medical personnel or genetic counselors, if indicated. 4.1.2 Adequacy of Protection against risks a. Recruitment and Informed consent: Subjects will be recruited through offices of physicians and other medical practitioners who care for patients with CP; educational and rehabilitative facilities serving disabled children; and the CPON network of families with children with CP. Specially trained study team members will contact parents and approach for informed consent. Written information will be provided about the purpose of the study, procedures, risks and benefits, and privacy protections, in the informed consent document itself and in supplemental materials. Written consent will be obtained from mother, and if available also the father, after meeting in person at the office of the referring physician, or through the mail after contact by phone with opportunity to ask questions. For children, many indirectly collected study items such as laboratory testing of specimens, and medical record review will not reasonably be well understood, and therefore consent for these items will be requested only from the parent. However, for the salivary sample which requires direct involvement and cooperation of the child, we will request verbal or signed assent from children age 7 and above who are capable of understanding the assent, per recommendation of our local IRBs, in addition to the prior consent of the parent. b. Protection against risk: To minimize potential breach of confidentiality, all study files will be stored in locked file cabinets in locked rooms and only the Principal Investigator and Project Coordinator, or designated assistants, will have access to these files. All study samples are shipped to the laboratory with only barcode ID labels. Laboratory test results will be HIPAA compliant with no personally identifiable information attached, and will be stored without names and identified only by study code. Additionally, confidentiality of health information is protected by keeping PHI and study health data in separate sections of the computerized RIX data base. Laboratory personnel will not have access to PHI in the database. All computerized data will be protected by password access, and only designated study team members will be issued passwords providing access to data collected for the study. Informed consent documents, which must be maintained in non-electronic form, and which contain PHI/PII, will be stored in locked file cabinets in locked rooms. The study document files will be accessed only when necessary and upon request of the Institutional Review Board. Privacy protection procedures are of highest priority in staff training, and are reinforced throughout our operations for everyday effectiveness. 4.1.3 Potential Benefit to Individual Subjects and Society For the majority of subjects there are few direct benefits in this study except for the feeling of being involved in an important study that may contribute to prevention of CP. Information related to etiology obtained through laboratory tests may be of high interest to parents who choose to participate. The potential benefit to society in better understanding processes leading to perinatal brain injury, and eventual reduction of CP prevalence, is substantial.
Protection of Human Subjects Page 449
Contact PD/PI: Paneth, Nigel S

Risk/Benefit Ratio: The benefit-risk ratio is favorable given the potentially large societal benefits and negligible risk to the participants. 4.1.4. Importance of the knowledge to be gained: The commonest severe motor disability of childhood, CP is also commonly associated with other developmental disorders. Reducing physical, psychological and economic burdens on the developing child, family and society may become possible through new knowledge of the timing, nature and pathways of this brain injury.
Protection of Human Subjects Page 450
Contact PD/PI: Paneth, Nigel S

Inclusion of Women and Minorities: Since this study focuses on environmental influences of child health, it involves mothers and their children. We will be recruiting to create a cohort that accurately reflects the Michigan population and thus all ethnic/race groups. Since all data collection activities can be completed with mothers, fathers are not asked to consent.
Women & Minorities Inclusion Page 451
Contact PD/PI: Paneth, Nigel S

OMB Number: 0925-0002
Tracking Number: GRANT12144486 Funding Opportunity Number: RFA-OD-16-004. Received Date: 2016-04-14T17:20:31.000-04:00
Planned Enrollment ReportThis report format should NOT be used for collecting data from study participants.
Study Title: Prenatal Exposures and Child Health Outcomes: A Statewide Study
Domestic/Foreign: Domestic
Comments:
Racial CategoriesEthnic Categories
Not Hispanic or LatinoFemale Male
Hispanic or LatinoFemale Male
Total
American Indian/Alaska Native 0 0 0 0 0
Asian 0 0 0 0 0
Native Hawaiian or Other Pacific Islander 0 0 0 0 0
Black or African American 198 66 0 0 264
White 1226 416 0 0 1642
More than One Race 0 0 70 24 94
Total 1424 482 70 24 2000
Study 1 of 1
Page 452
Contact PD/PI: Paneth, Nigel S

Inclusion of Children Children are included as the major focus of this study on the environmental influences of child health. The investigative team is well versed in working with children. The PI is a pediatrician epidemiologist, and the staff is trained in interviewing mothers and children, and has prior experience in working with children, including those with disabilities, in medical and educational settings. Because data collection does not directly involve the participation of the child, we do not include items for their assent. If required by the IRB, we will ask for assent. Target sample numbers (for an overall total of 2000) were chosen to provide sufficient power to detect rare birth outcomes.
Inclusion Of Children Page 453
Contact PD/PI: Paneth, Nigel S

We propose a multiple PI organization. Our experience in Michigan Alliance for the National Children’s Study (MANCS) confirmed the need to assign specific responsibilities for components of a large study to sub-groups of investigators in a specific arena with a designated leader. We are fortunate that our organization builds on an existing structure. Most of our core leaders were also core leaders, or had other roles, in MANCS, but we have incorporated several new investigators into our leadership structure to provide expertise in the scientific domains relevant to the ECHO program. The table below shows these cores and their leadership. The core leadership (N = 12) which includes the 5 co-PI’s (bolded in the Table), each of whom leads or co-leads a core, will meet by conference call weekly to review progress in achieving study goals and to address problems as they come up.
In the MANCS operation, all major decisions were made by consensus. We had no instance where major disagreement emerged, nor even where a vote was needed of the investigative team. Our organizational structure, which we adopt in modified form here, defines functional cores with assigned responsibilities to the team members most qualified to direct efforts in that direction. The five co-Pi’s will jointly provide oversight of the entire program and development and implementation of all policies, procedures and processes to achieve our scientific goals. Each co-PI is responsible for a core function. The assessment cores are responsible for developing our protocol. Paneth and Ruden will have central responsibility for establishing the protocol, including the laboratory measurements to be made, working with other assessment core leaders. Once the detailed protocol is in place, its implementation is the responsibility of the management cores, beginning with the enrollment work in clinics and hospitals, coordinated by Barone and Sokol. The Survey Operations and Data Management core, led by Elliott, will take on the large role of conducting home visits and phone calls and coordinating all data elements. As data and specimens flow into the study, analytic cores will be tasked with ensuring that the data is transported, stored and integrated with the overall data management system. Elliott will play a key role in this integration, as well as with providing biostatistical consultation (along with our three other biostatisticians/bioinformaticians).
Table 5: Organization of our study and leadership assignments
MANAGEMENT CORES ASSESSMENT CORES ANALYTIC CORES
These cores are operational and logistic, focusing on participant enrollment, protocol adherence, follow up and communications
These cores address implementation of key measures to ensure both that all ECHO outcomes and all exposures of importance are assessed appropriately
These cores ensure that the data collected is appropriately archived and analyzed
Core Leader Core Leader Core Leader
Study Center Paneth Asthma Johnson Biostatistics/Bioinformatics Elliott
Communications and Publications
Thompson Neuro-development Keating Biological Specimens Kusch
Survey Operations/Data Management
Elliott Nutritional/
Metabolic
Kerver Environmental Specimens Johnson
Hospital/Clinic Relations
Barone/Sokol Pregnancy Outcomes Sokol/Paneth State and Vital Data Copeland
Bioethics and Protection of Human
Subjects
Tomlinson Environmental and Epigenomic
Ruden Placentas Racicot
Social/Behavioral Norman
These individuals will link our activities to national ECHO activities supported by the four ECHO Centers
Patient-reported Outcomes Freed Data Analysis Elliott Coordinating Center Paneth CHEAR Resource Dolinoy
Multiple PI Leadership Plan Page 454
Contact PD/PI: Paneth, Nigel S

REFERENCES 1 Paneth N: The Origins of Fetal Origins. International Journal of Epidemiology 2016, in press 2 Barker DJ: Fetal Origins of Cardiovascular and Lung Disease. New York: Marcel Dekker, 2001 3 Mehta S, Kerver J, Sokol RJ, Keating D, Paneth N: The Association between Maternal Obesity and
Neurodevelopmental Outcomes of Offspring. J Pediatr 2014: Nov;165(5):891-6 4 Gomez R, Romero R, Ghezzi F, Yoon BH, Mazor M, Berry SM: the fetal inflammatory response syndrome.
Am J Obstet Gynecol. 1998 Jul;179(1):194-202. 5 Yampolsky M, Salafia CM, Shlakhter O, Haas D, Eucker B, Thorp J. Modeling the variability of shapes of a
human placenta. Placenta. 2008;29(9):790-7. PMID: 18674815 6 Haeussner E, Aschauer B, Burton GJ, Huppertz B, Edler von Koch F, Müller-Starck J, Salafia C, Schmitz C,
Frank HG: Does 2D-Histologic identification of villous types of human placentas at birth enable sensitive and reliable interpretation of 3D structure? Placenta. 2015 Dec;36(12):1425-32.
7 Salafia CM, Misra DP, Yampolsky M, Girardi T: Placental Vascular Tree as Biomarker of Autism/ASD Risk. Report of DOD grant W81XWH-10-1-0626. September 2012
8 Schlaff RA, Holzman C, Maier KS, Pfeiffer KA, Pivarnik JM: Associations among gestational weight gain, physical activity, and pre-pregnancy body size with varying estimates of pre-pregnancy weight. Midwifery. 2014 Nov;30(11):1124-31.
9 Schlaff RA, Holzman C, Mudd LM, Pfeiffer K, Pivarnik JM; Body mass index is associated with appropriateness of weight gain but not leisure-time physical activity during pregnancy. J Phys Act Health. 2014 Nov;11(8):1593-9.
10 Marshall MR, Paneth N, Gerlach JA, Mudd LM, Biery L, Ferguson DP, Pivarnik JM. Insulin-like growth factor 2 is differentially methylated in offspring of physically active pregnant women. 2016. Eur J Appl Physiol. In preparation.
11 Xia H, Ma S, Wang S, Sun G. Meta-Analysis of Saturated Fatty Acid Intake and Breast Cancer Risk. Medicine (Baltimore). 2015 Dec;94(52):e2391.
12 Schouten LR, Veltkamp F, Bos AP, van Woensel JB, Serpa Neto A, Schultz MJ, Wösten-van Asperen RM. Incidence and Mortality of Acute Respiratory Distress Syndrome in Children: A Systematic Review and Meta-Analysis. Crit Care Med. 2015 Oct 27. [Epub ahead of print]
13 Tian SB, Yu JC, Kang WM, Ma ZQ, Ye X, Cao ZJ. Association between dairy intake and gastric cancer: a meta-analysis of observational studies. PLoS One. 2014 Jul 9;9(7):e101728.
14 Kerver JM, Elliott MR, Norman GS, Sokol RJ, Keating DP, Copeland GE, Johnson CC, Cislo KK, Alcser KH, Kruger-Ndiaye SR, Pennell BE, Mehta S, Joseph CL, Paneth N; MANCS Executive Committee. Pregnancy recruitment for population research: the National Children's Study vanguard experience in Wayne County, Michigan. Paediatr Perinat Epidemiol. 2013 May;27(3):303-11.
15 Hanna-Attisha, M, LaChance J, Sadler RC, Champney Schnepp A; Elevated Blood Lead Levels in Children Associated With the Flint Drinking Water Crisis: A Spatial Analysis of Risk and Public Health Response. Am J Public Health, 2016 Feb;106(2):283-90.
16 Anderson O.S., Peterson K.E., Sanchez B.N., Zhang Z. Mancuso P.M., Dolinoy, D.C. Perinatal bisphenol A exposure promotes hyperactivity, lean body composition, and hormonal responses across the murine life-course. The FASEB Journal. 27(4): 1784-1792, 2013. PMCID: 3606526.
17 Faulk C., Barks A., Sánchez B., Zhang Z, Anderson O.S., Peterson K.E., Dolinoy D.C. Perinatal lead (Pb) exposure results in sex-specific effects on weight, food intake, fat, and insulin response across the murine life-course. PLOS-ONE, 9(8):e104273. 2014. PMCID: 4126699.
References Cited Page 455
Contact PD/PI: Paneth, Nigel S

18 Cassidy AE, Bielak LF, Zhou Y, Sheedy PF, Turner ST, Breen JF, Araoz PA, Lin X, Peyser PA. Progression of Subclinical Coronary Atherosclerosis: Does Obesity Make a Difference? Circulation, 111(15):1877-82, 2005.
19 Cassidy-Bushrow AE, Wegienka G, Havstad S, Levin AM, Lynch SV, Ownby DR, Rundle AG, Woodcroft KJ, Zoratti AM, Johnson CC. Does Pet-Keeping Modify the Association of Delivery Mode with Offspring Body Size? Maternal and Child Health Journal, 19(6):1426-33, 2015. PMCID: PMC4446256.
20 Cassidy-Bushrow AE, Havstad S, Basu N, Ownby DR, Park SK, Ownby DR, Johnson CC, Wegienka G. Detectable Blood Lead Level and Body Size in Early Childhood. Biological Trace Elements Research, 2015 (in press) (DOI: 10.1007/s12011-015-0500-7).
21 Eng DS, MD, Lee JM, Gebremariam A, Meeker JD, Peterson K, Padmanabhan V 2013 Bisphenol A and chronic disease risk factors in US children. Pediatrics. 132(3):e637-645. PMCID: PMC3876757.
22 Vandenberg LN, Gerona RR, Kannan K, Taylor JA, van Breemen RB, Dickenson CA, Liao C, Yuan Y, Newbold RR, Padmanabhan V, vom Saal FS, Woodruff TJ 2014 A Round Robin Approach to the Analysis of Bisphenol A (BPA) in Human Blood Samples. Environmental Health 13: 25 PMCID:PMC4066311.
23 Veiga-Lopez A, Pennathur S, Kannan K, Patisaul HB, Dolinoy DC, Zeng L, Padmanabhan V. Impact of gestational bisphenol A on oxidative stress and free fatty acids: human association and interspecies animal testing studies. Endocrinology 156(3):911-22 PMCID: PMC4330308.
24 Neier K, Marchlewicz EH, Dolinoy DC, Padmanabhan V 2015 Assessing Human Health Risk to Endocrine Disrupting Chemicals: a Focus on Prenatal Exposures and Oxidative Stress. Endocrine disruptors 3:1, e1069916. http://dx.doi.org/10.1080/23273747.2015.1069916, NIHMS760022.
25 Veiga-Lopez A, Kannan K, Liao C, Ye W, Domino S, Padmanabhan V 2015 Gender-specific effects on gestational length and birth weight by early pregnancy BPA exposure. Clin Endocrinol Metab. 100(11):E1394-403. PMCID:PMC4702459.
26 Hirko KA, Chen WY, Willett WC, Rosner BA, Hankinson SE, Beck AH, Tamimi RM, Eliassen AH. Alcohol consumption and risk of breast cancer by molecular subtype: Prospective analysis of nurses’ health study after 26 years of follow-up. International Journal of Cancer. 2015 Sept 18. PMID 26384849.
27 Hirko KA, Willett WC, Hankinson SE, Rosner BA, Beck AH, Tamimi RM, Eliassen AH. Healthy dietary patterns and risk of breast cancer by molecular phenotype. Breast Cancer Res Treat. 2016 Feb;155(3):579-88. PMID:26872903.
28 Hirko KA, Spiegelman D, Barnett JB, Cho E, Willett WC, Hankinson SE, Eliassen A.H. Dietary patterns and plasma sex hormones, prolactin and sex hormone-binding globulin in premenopausal women. Cancer Epidemiol Biomarkers Prev (accepted February 2016).
29 Hirko KA, Spiegelman D, Barnett JB, Cho E, Willett WC, Hankinson SE, Eliassen AH: Dietary patterns and plasma sex hormones, prolactin and sex hormone-binding globulin in premenopausal women. Cancer Epidemiol Biomarkers Prev. 2016 Mar 15. Epub ahead of print]
30 Hirko KA, Willett WC, Hankinson SE, Rosner BA, Beck AH, Tamimi RM, Eliassen AH: Healthy dietary patterns and risk of breast cancer by molecular subtype. Breast Cancer Res Treat. 2016 Feb;155(3):579-88.
31 Asher MI, Keil U, Anderson HR, Beasley R, Crane J, Martinez F, Mitchell EA, Pearce N, Sibbald B, Stewart AW. International Study of Asthma and Allergies in Childhood (ISAAC): rationale and methods. Eur Respir J 1995;8(3):483-9
32 Liu AH, Zeiger R, Sorkness C, Mahr T, Ostrom N, Burgess S, Rosenzweig JC, Manjunath R. Development and cross-sectional validation of the Childhood Asthma Control Test. J Allergy Clin Immunol 2007;119(4):817-25
33 Beydon N, Davis SD, Lombardi E, Allen JL, Arets HG, Aurora P, Bisgaard H, Davis GM Ducharme FM, Eigen H, Gappa M, Gaultier C, Gustafsson PM, Hall GL, Hantos Z, Healy MJ, Jones MH, Lug B, Lodrup Carlsen KC, McKenzie SA, Marchal F, Mayer OH, Merkus PG, Morris MG, Oostveen E, Pillow JJ, Seddon
References Cited Page 456
Contact PD/PI: Paneth, Nigel S

PC,Silverman M, Sly PD, Stocks J, Tepper RS, Vilozni D, Wilson NM. An official American Thoracic Society/European Respiratory Society statement: pulmonary function testing in preschool children. Am J Respir Crit Care Med 2007;175(12):1304-45.
34 Dweik RA, Boggs PB, Erzurum SC, Irvin CG, Leigh MW, Lundberg JO, Olin AC, Plummer AL, Taylor DR: An official ATS clinical practice guideline: interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med 2011;184(5):602-20.
35 Sen A, Heredia N, Senut MC, Land S, Hollocher K, Lu X, Dereski MO, Ruden DM: Multigenerational epigenetic inheritance in humans: DNA methylation changes associated with maternal exposure to lead can be transmitted to the grandchildren. Sci Rep. 2015 Sep 29;5:14466.
36 Kerver JM, Yang EJ, Obayashi S, Bianchi L, and Song WO. Meal and snack patterns are associated with dietary intake of energy and nutrients in U.S. adults. J Am Diet Assoc. 2006 Jan;106(1):46-53.
37 Dolinoy, D.C., Huang, D., and Jirtle, R.L. Maternal nutrient supplementation counteracts bisphenol A-induced DNA hypomethylation in early development. Proceedings of the National Academy of Sciences. 104: 13056-13061, 2007. PMCID: 1941790.
38 Weinhouse C., Anderson O.S., Bergin I.L, Vandenbergh D.J., Gyekis J.P., Dingman M.A., Yang J., Dolinoy D.C. Dose-dependent incidence of hepatic tumors following perinatal bisphenol A exposure. Environmental Health Perspectives. 122(5): 485-491, 2014. PMCID: 4014767.
39 Fichorova, R.N., N. Beatty, R.R. Sassi, H.S. Yamamoto, E.N. Allred, A. Leviton, and E. Investigators. 2015. Systemic inflammation in the extremely low gestational age newborn following maternal genitourinary infections. Am. J. Reprod. Immunol. 73:162-174.
40 Fichorova, R.N., A.B. Onderdonk, H. Yamamoto, M.L. Delaney, A.M. DuBois, E. Allred, and A. Leviton. 2011. Maternal microbe-specific modulation of inflammatory response in extremely low-gestational-age newborns. mBio 2:e00280-00210.
41 Fichorova, R.N., N. Richardson-Harman, M. Alfano, L. Belec, C. Carbonneil, S. Chen, L. Cosentino, K. Curtis, C.S. Dezzutti, B. Donoval, G.F. Doncel, M. Donaghay, J.C. Grivel, E. Guzman, M. Hayes, B. Herold, S. Hillier, C. Lackman-Smith, A. Landay, L. Margolis, K.H. Mayer, J.M. Pasicznyk, M. Pallansch-Cokonis, G. Poli, P. Reichelderfer, P. Roberts, I. Rodriguez, H. Saidi, R.R. Sassi, R. Shattock, and J.E. Cummins, Jr. 2008. Biological and technical variables affecting immunoassay recovery of cytokines from human serum and simulated vaginal fluid: a multicenter study. Anal. Chem. 80:4741-4751.
42 Comstock SS, Hortos K, Kovan B, McCaskey S, Pathak DR, Fenton JI. (2014) Adipokines and obesity are associated with colorectal polyps in adult males: a cross-sectional study. PLoS One, 9(1):e85939. PMID: 24465801 PMCID: PMC3895019.
43 Pickens CA, Sordillo LM, Comstock SS, Harris WS, Hortos K, Kovan B, Fenton JI. (2015) Plasma phospholipids, non-esterified plasma polyunsaturated fatty acids and oxylipids are associated with BMI. Prostaglandins, Leukotrienes and Essential Fatty Acids, 95:31-40. PMID: 25559239 PMCID: PMC4361296.
44 Comstock SS, Lewis MM, Pathak DR, Hortos K, Kovan B, Fenton JI. (2014) Cross-sectional analysis of obesity and serum analytes in males identifies sRAGE as a novel biomarker inversely associated with diverticulosis. PLoS One, 9(4):e95232. PMID: 24740401 PMCID: PMC3989304.
45 Elliott MR. A simple method to generate equal-sized homogenous strata or clusters for population-based sampling. Ann Epidemiol. 2011 Apr;21(4):290-6.
46 Sollars V, Lu X, Xiao L Garfinkel MD, Ruden DM. Evidence for an epigenetic mechanism by which Hsp90 acts as a capacitor for morphological evolution. Nature Genetics, 2003. 33(1): p. 70-4.
47 Cingolani P, Platts A, Wang le L, Coon M, Nguyen T, Wang L, Land SJ, Lu X, Ruden DM. A program for annotating and predicting the effects of single nucleotide polymorphisms, SnpEff: SNPs in the genome of Drosophila melanogaster strain w1118; iso-2; iso-3. Fly (Austin), 2012. 6(2): p. 80-92.
References Cited Page 457
Contact PD/PI: Paneth, Nigel S

48 Wu J, Wen XW, Faulk C, Boehnke K, Zhang H, Dolinoy DC, Xi C: Perinatal lead (Pb) exposure alters gut
microbiota composition and results in sex-specific bodyweight increases in adult mice. Toxicol Sci, 2016. 49 Sant KE, Dolinoy DC, Jilek JL, Shay BJ, Harris C: Mono-2-ethylhexyl phthalate (MEHP) alters histiotrophic
nutrition pathways and epigenetic processes in the developing conceptus. J Nutr Biochem, 2016. 27: p. 211-8.
50 Rozek LS, Dolinoy DC, Sartor MA, Omenn GS: Epigenetics: relevance and implications for public health. Annu Rev Public Health, 2014. 35: p. 105-22.
51 O'Brien E, Dolinoy DC, Mancuso P: Bisphenol A at concentrations relevant to human exposure enhances histamine and cysteinyl leukotriene release from bone marrow-derived mast cells. J Immunotoxicol, 2014. 11(1): p. 84-9.
52 O'Brien E, Dolinoy DC, Mancuso P: Perinatal bisphenol A exposures increase production of pro-inflammatory mediators in bone marrow-derived mast cells of adult mice. J Immunotoxicol, 2014. 11(3): p. 205-12.
53 Kim J.H, Rozek LS, Soliman AS, Sartor MA, Hablas A, Seifeldin IA, Colacino JA, Weinhouse C, Nahar MS, Dolinoy DC: Bisphenol A-associated epigenomic changes in prepubescent girls: a cross-sectional study in Gharbiah, Egypt. Environ Health, 2013. 12: p. 33.
54 Virani S, Dolinoy DC, Halubai S, Jones TR, Domino SE, Rozek LS, Nahar MS, Padmanabhan V: Delivery type not associated with global methylation at birth. Clin Epigenetics. 2012 Jun 9;4(1):8.
55 Li M, Monaco MH, Wang M, Comstock SS, Kuhlenschmidt TB, Fahey GC, Miller MJ, Kuhlenschmidt MS, Donovan SM. (2014) Human milk oligosaccharides shorten rotavirus diarrhea and modulate piglet mucosal immunity and colonic microbiota. ISME J, 8(8):1609-20. PMID: 24522264
56 Cassidy-Bushrow A. E., Sitarik A., Levin A. M., et al. (2016). Maternal group B Streptococcus and the infant gut microbiota. J Dev Orig Health Dis, 7(1), 45-53. doi:10.1017/s2040174415001361.
57 Zhang L, Xie J, Patel M, Bakhtyar A, Ehrlich GD, Ahmed A, Earl J, Marrs CF, Clemans D, Murphy TF, Gilsdorf JR. 2012. Nontypeable Haemophilus influenzae genetic islands associated with chronic pulmonary infection. PLoS One. 7(9):e44730. doi: 10.1371. PMC3435294.
58 Lo Y, Zhang L, Foxman B, Zöllner S. 2015. Whole-genome sequencing of uropathogenic Escherichia coli reveals long evolutionary history of diversity and virulence. Infect Genet Evol. 34:244-50. doi: 10.1016/j.meegid. PMC4530057.
59 Foxman B, Srinivasan U, Wen A, Zhang L, Marrs CF, Goldberg D, Weyant R, McNeil D, Crout R, Marazita M. 2014. Exploring the effect of dentition, dental decay and familiality on oral health using metabolomics. Infect Genet Evol. 22:201-7. doi: 10.1016. PMC3943654
60 Johnson CC, Ownby DR: Allergies and Asthma: Do Atopic Disorders Result from Inadequate Immune Homeostasis arising from Infant Gut Dysbiosis? Expert Rev Clin Immunol. 2016 Apr;12(4):379-88.
61 Tomlinson T, De Vries R, Ryan K, Kim HM, Lehpamer N, Kim, S: Moral Concerns and the Willingness to Donate to a Research Biobank. JAMA. 2015;313(4):417-419.
62 Slaughter J, Wei C, Korzeniewski SJ, Lu Q, Beck JS, Khoo SK, Brovont A, Maurer J, Martin D, Lenski M, Paneth N. High correlations in gene expression between paired umbilical cord blood and neonatal blood of healthy newborns on Guthrie cards. J Matern Fetal Neonatal Med 2013;26:1765-7.
63 Haak PT, Busik JV, Kort AJ, Tikhonenko M, Paneth N, Resau JH: Archived unfrozen neonatal blood spots are amenable to microarray gene expression analysis. Neonatology 2009;95:210-216.
64 Wei C, Lu Q, Khoo S-K, Lenski M, Paneth N, Fichorova R, Leviton A: Comparison of Frozen and Unfrozen newborn blood spots for Gene Expression Studies. J Pediatrics 2014;164:189-191.
References Cited Page 458
Contact PD/PI: Paneth, Nigel S

65 Ho NT, Furge K, Fu W, Busik J, Khoo SK, Lu Q, Lenski M, Wirth J, Hurvitz E, Dodge N, Resau J, Paneth N.
Gene expression in archived newborn blood spots distinguishes infants who will later develop cerebral palsy from matched controls. Pediatr Research 2013;73:450-6
66 Olney RS, Moore CA, Ojodu JA etal: Storage and use of residual dried blood spots from state newborn screening programs. J Pediatr. 2006;148:618-22.
67 Duquette D, Rafferty AP, Fussman C Gehring J, Meyer S, Bach J: Public Support for the Use of Newborn Screening Dried Blood Spots in Health Research. Public Health Genomics. 2011;14(3):143-52
68 Ruden D, editor: Using Archived Neonatal Dried Blood Spots in State Biobanks for Toxicogenomics Analyses. Frontiers in Research, in press.
69 Lorenz JM, Paneth N, Jetton JR, den Ouden L, Tyson JE: Comparison of management strategies for extreme prematurity in New Jersey and the Netherlands: outcomes and resource expenditures. Pediatrics 2001;108;1269-1274
70 Hille ETM, den Ouden AL, Wolke DFH, Saigal S, Lambert M, Meyer R, Whitaker A, Pinto-Martin JA, Feldman JF, Verloove-Vanhorick SP, Paneth N: Behavioral problems reported in children who weigh 1000g or less at birth in four countries. Lancet 2001; 357: 1641-3. [Selected by Health Canada as one of 10 papers published in 2001 most likely to help foster children’s social and emotional development].
71 Saigal S, den Ouden L, Wolke D, Hoult L, Paneth N, Streiner DL, Whitaker A, Pinto-Martin JA: School-age outcomes in children who were extremely low birth weight from four international population-based cohorts. Pediatrics 2003;112:943-50.
72 Hur J, O’Brien PD, Nair V et al: Transcriptional networks of murine diabetic peripheral neuropathy and nephropathy: Common and distinct gene expression patterns. Diabetologia, in press
73 Jayapandian M, Chapman A, Tarcea AG et al: Michigan Molecular Interactions (MiMI): putting the jigsaw puzzle together. Nucleic Acids Res. 2007; 35 (suppl 1): D566-D571.
74 Shalowitz DI, Miller FG. Communicating the results of clinical research to participants: attitudes, practices, and future directions. PLoS Med. 2008 May 13;5(5):e91.
75 Dorsey ER, Beck CA, Adams M, Chadwick G, de Blieck EA, McCallum C, Briner L, Deuel L, Clarke A, Stewart R, Shoulson I; Huntington Study Group TREND-HD Investigators. Communicating clinical trial results to research participants. Arch Neurol. 2008 Dec;65(12):1590-5.
76 U.S. Department of Education, National Center for Education Statistics. (2006). ECLS-B Longitudinal 9-Month—2-Year Restricted-Use Data File and Electronic Codebook (CD-ROM) (NCES 2006–044). Washington, DC.
77 Schonhaut, L., Armijo, I., Schönstedt, M., Alvarez, J., & Cordero, M. (2013). Validity of the Ages and Stages Questionnaire among term and preterm infants. Pediatrics, 131, e1468-e1474.
78 Hardy, S., Haisley, L., Manning, C., & Fein, D. (2015). Can screening with the Ages and Stages Questionnaire detect ASD? Journal of Developmental and Behavioral Pediatrics, 36, 536-543.
79 Bayley N. (2006). Bayley Scales of Infant and Toddler Development. 3rd ed. San Antonio, TX: Harcourt Assessment Inc.
80 Johnson, S., Moore, T., & Marlow, N. (2014). Using the Bayley-III to assess neurodevelopmental delay: which cut-off should be used? Pediatric Research, 75, 670-674.
81 Sroufe, L.A. (2005). Attachment and development: A prospective, longitudinal study from birth through adulthood. Attachment and & Human Development, 7, 349-367.
82 Carlson, E.A., Sampson, M.C., & Sroufe, L.A. (2003). Implications of attachment theory for developmental-behavioral pediatrics. Journal of Developmental and Behavioral Pediatrics, 24, 364-379.
83 Wechsler, D. (1999). Wechsler Abbreviated Scale of Intelligence. The Psychological Corporation: Harcourt Brace & Company. New York, NY.
References Cited Page 459
Contact PD/PI: Paneth, Nigel S

84 Achenbach, T. M. (2009). The Achenbach System of Empirically Based Assessemnt (ASEBA):
Development, Findings, Theory, and Applications. Burlington, VT: University of Vermont Research Center for Children, Youth, & Families.
85 Conners CK. (2008). Conners’ Rating Scales—Revised (CRS-R). Technical Manual. Tonawanda, NY: Multihealth Systems; 2001.
86 Constantino, J.N., & Gruber, C.P. (2005). The social responsiveness scale manual. Los Angeles: Western Psychological Services.
87 Gershon, R., Wagster, M.V., Hendrie, H.C., Fox, N.A., Cook, K.F., & Nowinski, C.J. (2013). NIH Toolbox for assessment of neurological and behavioral function. Neurology, 80, S2-S6.
88 Weintraub, S., Bauer, P.J., Zelazo, P.D., Wallner-Allen, K., Dikmen, S.S., Heaton, R.K., Tulsky, D.S., Slotkin, J., Blitz, D.L., Carlozzi, N.E., Havlik, R.J., Beaumont, J.L., Mungas, D., Manly, J.J., Borosh, B.G., Nowlinski, C.J., & Gershon, R.C. (2013). NIH Toolbox Cognition Battery: Introduction and pediatric data. Monographs of the Society for Research in Child Development, 78, 1–172.
89 Jensen NS, Camargo TF, Bergamaschi DP. Comparison of methods to measure body fat in 7 to 10 year old children: a systematic review. Public Health. 2016 Jan 13.pii:S0033-3506(15)0049-6. doi:10.1016/j.puhe.2015.11.025 [Epub ahead of print]
90 Kuczmarski RJ, Ogden CL, Guo SS et al: 2000 CDC growth charts for the United States: methods and development. Vital Health Stat 11. 2002;(246):1-190.
91 Freedman DS, Ogden CL, Kit BK. Interrelationships between BMI, skinfold thickness, percent body fat, and
cardiovascular disease risk factors among US children and adolescents. BMC Pediatr 2015; Nov 18;15:188. 92 Kahn HS, Imperatore G, Cheng YJ. A comparison between BMI, waist circumference, and waist-to-height
ratio for identifying cardiometabolic risk in children and adolescents. J Pediatr. 2005;146(4):482-488.
93 Kabiri LS, Hernandez DC, Mitchell K. Reliability, validity, and diagnostic value of a pediatric bioelectrical
impedance analysis scale. Child Obes. 2015 Oct;11(5):650-5. 94 Keating, D. P., & Hertzman, C. (Eds.). (1999). Developmental health and the wealth of nations: Social,
biological, and educational dynamics. New York: Guilford Press 95 Keating, D. P. (Ed.). (2011). Nature and nurture in early child development. New York: Cambridge
University Press. 96 Conradt, E., Hawes, K., Guerin, D., Armstrong, D. A., Marsit, C. J., Tronick, E., & Lester, B. M. (2016). The
contributions of maternal sensitivity and maternal depressive symptoms to epigenetic processes and neuroendocrine functioning. Child Development, 87(1), 73-85.
97 Lester BM, Conradt E. Marsit C. Introduction to the special section on epigenetics. Child Development, 2016; 87(1), 29-37.
98 Keating, DP: Transformative role of epigenetics in child development research: Commentary on the special section. Child Development, 2016; 87(1), 135-142.
99 Cantonwine DE, Ferguson KK, Mukherjee B, Chen YH, Smith NA, Robinson JN, Doubilet PM, Meeker JD, McElrath TF: Utilizing Longitudinal Measures of Fetal Growth to Create a Standard Method to Assess the Impacts of Maternal Disease and Environmental Exposure. Plos One, 2016. 11(1).
100 Park SK: Environmental Risk Score as a New Tool to Examine Multi-Pollutants in Epidemiologic Research: An Example from the NHANES Study Using Serum Lipid Levels. Plos One, 2014. 9(6).
101 Meeker JD: Exposure to Environmental Endocrine Disruptors and Child Development. Archives of Pediatrics & Adolescent Medicine, 2012. 166(10): p. 952-958.
References Cited Page 460
Contact PD/PI: Paneth, Nigel S

102 Li J Wang Y, Fang F, Chen D, Gao Y, Liu J, Gao R, Wang J, Xiao H: Bisphenol A disrupts glucose transport
and neurophysiological role of IR/IRS/AKT/GSK3beta axis in the brain of male mice. Environ Toxicol Pharmacol, 2016. 43: p. 7-12.
103 Tiwari SK, Agarwal S, Chauhan LK, Mishra VN, Chaturvedi RK: Bisphenol-A impairs myelination potential during development in the hippocampus of the rat brain. Mol Neurobiol, 2015. 51(3): p. 1395-416.
104 Elsworth JD, Jentsch JD, Groman SM, Roth RH, Redmond ED Jr, Leranth C: Low circulating levels of bisphenol-A induce cognitive deficits and loss of asymmetric spine synapses in dorsolateral prefrontal cortex and hippocampus of adult male monkeys. J Comp Neurol, 2015. 523(8): p. 1248-57.
105 Leranth C, Hajszan T, Szigeti-Buck K, Bober J, MacLusky NJ: Bisphenol A prevents the synaptogenic response to estradiol in hippocampus and prefrontal cortex of ovariectomized nonhuman primates. Proc Natl Acad Sci U S A, 2008. 105(37): p. 14187-91.
106 Otsuka S, Coderre JA, Micca PL, Morris GM, Hopewell JW, Rola R, Fike JR: Depletion of neural precursor cells after local brain irradiation is due to radiation dose to the parenchyma, not the vasculature. Radiat Res, 2006. 165(5): p. 582-91.
107 MacLusky, N.J., T. Hajszan, and C. Leranth: The environmental estrogen bisphenol a inhibits estradiol-induced hippocampal synaptogenesis. Environ Health Perspect, 2005. 113(6): p. 675-9.
108 Carr R, Bertasi F, Betancourt A, Bowers S, Gandy BS, Ryan P, Willard S: Effect of neonatal rat bisphenol a exposure on performance in the Morris water maze. J Toxicol Environ Health A, 2003. 66(21): p. 2077-88.
109 Perez-Lobato R, Mustieles V, Calvente I, Jimenez-Diaz I, Ramos R, Caballero-Casero N, Lopez-Jimenez FJ, Rubio S, Fernandez MF: Exposure to bisphenol A and behavior in school-age children. Neurotoxicology, 2016. 53: p. 12-9
110 Casas M, Forns J, Martinez D, Avella-Garcia C, Valvi D, Ballesteros-Gomez A, Luque N, Rubio S, Julvez J, Sunyer J, Vrijheid M: Exposure to bisphenol A during pregnancy and child neuropsychological development in the INMA-Sabadell cohort. Environ Res, 2015. 142: p. 671-9.
111 Mustieles V, Perez-Lobato R, Olea N, Fernandez MF: Bisphenol A: Human exposure and neurobehavior. Neurotoxicology, 2015. 49: p. 174-84.
112 Fries GF: The PBB episode in Michigan: an overall appraisal. Crit Rev Toxicol, 1985. 16(2): p. 105-56. 113 Erb R: Researcher: PBB from 1970s still in Michiganders' blood. Detroit Free Press. 12/28/2014. 114 He JP, Stein AD, Humphrey HE, Paneth N, Courval JM: Time trends in sport-caught Great Lakes fish
consumption and serum polychlorinated biphenyl levels among Michigan Anglers, 1973-1993. Environ Sci Technol. 2001 Feb 1;35(3):435-40.
115 EPA: Timeline for Achieving Comprehensive Cleanup: Tittabawassee River, Saginaw River & Bay Contamination Site. 2009.
116 Schneider, J.S., S.K. Kidd, and D.W. Anderson, Influence of developmental lead exposure on expression of DNA methyltransferases and methyl cytosine-binding proteins in hippocampus. Toxicol Lett, 2013. 217(1): p. 75-81.
117 Ma WL, Gao C, Bell EM, Druschel CM, Caggana M, Aldous KM, Louis GM, Kannan K: Analysis of polychlorinated biphenyls and organochlorine pesticides in archived dried blood spots and its application to track temporal trends of environmental chemicals in newborns. Environ Res 2014. 133: p. 204-10.
118 Ma WL, Yun S, Bell EM, Druschel CM, Caggana M, Aldous KM, Buck Louis GM, Kannan K: Temporal trends of polybrominated diphenyl ethers (PBDEs) in the blood of newborns from New York State during 1997 through 2011: analysis of dried blood spots from the newborn screening program. Environ Sci Technol, 2013. 47(14): p. 8015-21.
119 Michigan Environmental Surveillance Systems (see appendix)
References Cited Page 461
Contact PD/PI: Paneth, Nigel S

120 Waterland RA: Epigenetic mechanisms affecting regulation of energy balance: many questions, few
answers. Annu Rev Nutr, 2014. 34: p. 337-55. 121 Dominguez-Salas P, Moore SE, Baker MS, Bergen AW, Cox SE, Dyer RA, Fulford AJ, Guan Y, Laritsky E,
Silver MJ, Swan GE, Zeisel SH, Innis SM, Waterland RA, Prentice AM, Hennig BJ: Maternal nutrition at conception modulates DNA methylation of human metastable epialleles. Nat Commun, 2014. 5: p. 3746.
122 Anway MD, Cupp AS, Uzumcu M, Skinner MK: Epigenetic transgenerational actions of endocrine disruptors and male fertility.[see comment]. Science, 2005. 308(5727): p. 1466-9.
123 Sen A, Heredia N, Senut MC, Land S, Hollocher K, Lu X, Dereski MO, Ruden DM: Multigenerational epigenetic inheritance in humans: DNA methylation changes associated with maternal exposure to lead can be transmitted to the grandchildren. Sci Rep, 2015. 5: p. 14466.
124 Bellinger D, Leviton A, Waternaux C, Needleman H, Rabinowitz M. Longitudinal analyses of prenatal and postnatal lead exposure and early cognitive development. N Engl J Med. 1987 Apr 23;316(17):1037-43.
125 Mushak P, Davis JM, Crocetti AF, Grant LD: Prenatal and postnatal effects of low-level lead exposure: integrated summary of a report to the U.S. Congress on childhood lead poisoning. Environ Res, 1989. 50(1): p. 11-36.
126 Shepherd TJ, Dirks W, Roberts NM, Patel JG, Hodgson S, Pless-Mulloli T, Walton P, Parrish RR: Tracing fetal and childhood exposure to lead using isotope analysis of deciduous teeth. Environ Res, 2016. 146: p. 145-53.
127 Alomary A, Al-Momani IF, Obeidat SM, Massadeh AM: Levels of lead, cadmium, copper, iron, and zinc in deciduous teeth of children living in Irbid, Jordan by ICP-OES: some factors affecting their concentrations. Environ Monit Assess, 2013. 185(4): p. 3283-95
128 Orzechowska-Wylegala B, Obuchowicz A, Malara P, Fischer A, Kalita B: Cadmium and lead accumulate in the deciduous teeth of children with celiac disease or food allergies. Int J Stomatol Occlusion Med, 2011. 4(1): p. 28-31.
129 Bellis DJ, Parsons PJ, Jones J, Amarasiriwardena D: Evaluation of Laser Ablation Inductively Coupled Plasma Mass Spectrometry for the Quantitative Determination of Lead in Different Parts of Archeological Human Teeth. Spectrosc Lett, 2009. 42(8): p. 491-496.
130 Adams JB, Romdalvik J, Ramanujam VM, Legator MS: Mercury, lead, and zinc in baby teeth of children with ASD versus controls. J Toxicol Environ Health A, 2007. 70(12): p. 1046-51.
131 Sen A, Cingolani P, Senut MC, Land S, Mercado-Garcia A, Tellez-Rojo MM, Baccarelli AA, Wright RO, Ruden DM: Lead exposure induces changes in 5-hydroxymethylcytosine clusters in CpG islands in human embryonic stem cells and umbilical cord blood. Epigenetics, 2015. 10(7): p. 607-21.
132 Sen A, Heredia N, Senut MC, Hess M, Land S, Qu W, Hollacher K, Dereski Mo, Ruden DM: Early life lead exposure causes gender-specific changes in the DNA methylation profile of DNA extracted from dried blood spots. Epigenomics, 2015. 7(3): p. 379-93.
133 Batterman SA, Chernyak SM, Su YF: Measurement and Comparison of Organic Compound Concentrations in Plasma, Whole Blood and Dried Blood Spot Samples. Frontiers in Genetics (Toxicogenomics)2016; in press.
134 Lu D, Wang D, Ip HS, Barley F, Ramage R, She J: Measurements of polybrominated diphenyl ethers and polychlorinated biphenyls in a single drop of blood. Journal of Chromatography B-Analytical Technologies in the Biomedical and Life Sciences, 2012; 891: 36-43.
135 Ma W, Kannan K, Wu Q, Bell EM, Druschel CM, Caggana M, Aldous KM: Analysis of polyfluoroalkyl substances and bisphenol A in dried blood spots by liquid chromatography tandem mass spectrometry. Anal Bioanal Chem, 2013. 405(12): p. 4127-38.
References Cited Page 462
Contact PD/PI: Paneth, Nigel S

136 Batterman S, Su FC, Li S, Mukherjee B, Jia C, HEI Health Review Committee: Personal exposure to
mixtures of volatile organic compounds: modeling and further analysis of the RIOPA data. Res Rep Health Eff Inst, 2014(181): p. 3-63.
137 Huang L, Bohac SV, Chernyak SM, Batterman SA: Composition and Integrity of PAHs, Nitro-PAHs, Hopanes and Steranes In Diesel Exhaust Particulate Matter. Water Air Soil Pollut, 2013. 224(8).
138 Chin JY, Godwin C, Jia C, Robins T, Lewis T, Parker E, Max P, Batterman S: Concentrations and risks of p-dichlorobenzene in indoor and outdoor air. Indoor Air, 2013. 23(1): p. 40-9.
139 Jia, C., S.A. Batterman, and G.E. Relyea, Variability of indoor and outdoor VOC measurements: an analysis using variance components. Environ Pollut, 2012. 169: p. 152-9.
140 Batterman S, Su FC, Jia C, Naidoo RN, Robins T, Naik I: Manganese and lead in children's blood and airborne particulate matter in Durban, South Africa. Sci Total Environ, 2011. 409(6): p. 1058-68.
141 Miller MF, Chernyak SM, Batterman S, Loch-Caruso R: Polybrominated diphenyl ethers in human gestational membranes from women in southeast Michigan. Environ Sci Technol, 2009. 43(9): p. 3042-6.
142 Erickson RJ, McKim JM, Lien GJ, Hoffman AD, Batterman SL: Uptake and elimination of ionizable organic chemicals at fish gills: II. Observed and predicted effects of ph, alkalinity, and chemical properties. Environ Toxicol Chem, 2006. 25(6): p. 1522-32.
143 Chaudhuri SN, Butala SJ, Ball RW, Braniff CT, Rocky Mountain Biomonitoring Consortium Pilot study for utilization of dried blood spots for screening of lead, mercury and cadmium in newborns. J Expo Sci Environ Epidemiol, 2009. 19(3): p. 298-316.
144 Batterman S, Chernyak S: Performance and storage integrity of PCB, PBDE and pesticide measurements using dried blood spots. Science of the Total Environment 2014; Oct 1;494-495:252-60
145 Needham LL, Grandjean P, Heinzow B, Jorgensen PJ, Nielsen F, Patterson DG Jr, Sjodin A, Turner WE, Weihe P: Partition of environmental chemicals between maternal and fetal blood and tissues. Environ Sci Technol, 2011. 45(3): p. 1121-6.
146 Rudge CV, Rollin HB, Nogueira CM, Homassen Y, Rudge MC, Odland JO: The placenta as a barrier for toxic and essential elements in paired maternal and cord blood samples of South African delivering women. J Environ Monit, 2009. 11(7): p. 1322-30.
147 Yoon M, Nong A, Clewell HG 3rd, Taylor MD, Dorman DC, Andersen ME: Evaluating placental transfer and tissue concentrations of manganese in the pregnant rat and fetuses after inhalation exposures with a PBPK model. Toxicol Sci, 2009. 112(1): p. 44-58.
148 Hare D, Austin C, Doble P, Arora M: Elemental bio-imaging of trace elements in teeth using laser ablation-inductively coupled plasma-mass spectrometry. J Dent, 2011. 39(5): p. 397-403.
149 Hu H, Rabinowitz M, Smith D: Bone lead as a biological marker in epidemiologic studies of chronic toxicity: conceptual paradigms. Environ Health Perspect, 1998. 106(1): p. 1-8.
150 Pascual JA, Diaz D, Sequra J, Garcia-Algar O, Vall O, Zuccaro P, Pacifici R, Pichini S: A simple and reliable method for the determination of nicotine and cotinine in teeth by gas chromatography/mass spectrometry. Rapid Commun Mass Spectrom, 2003. 17(24): p. 2853-5.
151 Arora M, Bradman A, Austin C, Vedar M, Holland N, Eskenazi B, Smith DR: Determining fetal manganese exposure from mantle dentine of deciduous teeth. Environ Sci Technol, 2012. 46(9): p. 5118-25.
152 Arora M, Kennedy BJ, Elhlou S, Pearson NJ, Walker DM, Bayl P, Chan SW: Spatial distribution of lead in human primary teeth as a biomarker of pre- and neonatal lead exposure. Sci Total Environ, 2006. 371(1-3): p. 55-62.
153 Arora M, Austin C, Sarrafpour B, Hernandez-Avila M, Hu H, Wright RO, Tellez-Rojo MM: Determining prenatal, early childhood and cumulative long-term lead exposure using micro-spatial deciduous dentine levels. PLoS One, 2014. 9(5): p. e97805.
References Cited Page 463
Contact PD/PI: Paneth, Nigel S

154 Camann DE, Schultz ST, Yau AY, Heilbrun LP, Zuniga MM, Palmer RF, Miller CS: Acetaminophen,
pesticide, and diethylhexyl phthalate metabolites, anandamide, and fatty acids in deciduous molars: potential biomarkers of perinatal exposure. J Expo Sci Environ Epidemiol, 2013. 23(2): p. 190-6.
155 Jan J, Milka V, Azra P, Dominik G, Matjaz Z: Distribution of organochlorine pollutants in ovine dental tissues and bone. Environ Toxicol Pharmacol, 2006. 21(1): p. 103-7.
156 Centers for Disease Control and Prevention. National Report on Biochemical Indicators of Diet and Nutrition in the US population, Second Nutrition Report. http://www.cdc.gov/nutritionreport. Accessed 4/4/16.
157 Hollowell JG, Staehling NW, Hannon WH, Flanders DW, Gunter EW, Maberly GF, Braverman LE, Pino S, Miller DT, Garbe PL, DeLozier DM, Jackson RJ: Iodine nutrition in the United States. Trends and public health implications: iodine excretion data from NHANES I and III (1971-1974 and 1988-1991). J Clin Endocrinol Metab 1998;83:3401-8.
158 Caldwell KL, Pan Y, Mortensen ME, Makhmudov A, Merrill L, Moye J: Iodine status in pregnant women in the National Children's Study & in US women (15-44 years), NHANES 2005-2010.Thyroid 2013;23:927-37.
159 Caldwell KL, Makhmudov AA, Ely EK, Jones RL, Wang RY: Iodine Status of the U.S. Population, NHANES 2005-2006 Thyroid 2009;19:S26-S27.
160 Holowell JG, Haddow JE. The prevalence of iodine deficiency in women of reproductive age in the United States of America. Publ Health Nutr 2007;10:1532-9.
161 Iskaros J, Pickard M, Evans I, Sinha A, Hardiman P, Ekins R: Thyroid hormone receptor gene expression in first trimester human fetal brain. J Clin Endocrinol Metab 2000;85:2620-3.
162 De Escobar GM, Obregon MJ, del Rey FE. Role of thyroid hormone during early brain development. Eur J Endocrinol 2004;151:U25-U37.
163 Iodine Global Network, www.ign.org 164 De Escobar GM, Obregon MJ, del Rey FE. Role of thyroid hormone during early brain development. Eur J
Endocrinol 2004;151:U25-U37. 165 Navarro D, Alvarado M, Morte B: Late Maternal Hypothyroidism Alters the Expression of Camk4 in
Neocortical Subplate Neurons: A Comparison with Nurr1 Labeling. Cereb Cortex. 2013 May 24. [Epub ahead of print]
166 Zimmerman MB. Iodine deficiency and endemic cretinism. In Braverman LE, Utiger RD, eds:Werner and Ingbar’s The Thyroid, 10th edition, Lippincott, Williams and Wilkins, Philadelphia, PA, 2013, pp. 217-41.
167 Bath SC, Steer CD, Golding J, Emmett P, Rayman MP: Effect of inadequate iodine status in UK pregnant women on cognitive outcomes in their children: results from the Avon Longitudinal Study of Parents and Children (ALSPAC). Lancet 2013;382:331-37.
168 Vermiglio ZF, Lo Presti VP, Moleti M Sidoti M, Tortorella G, Scaffidi G, Castagna MG, Mattina F, Violi Ma, Crisa A, Artemisia A, Trimarchi F: Attention deficit and hyperactivity disorders in the offspring of mothers exposed to mild-moderate iodine deficiency: A possible novel iodine deficiency disorder in developed countries. J Clin Endocrinol Metab 2004;89:60454-60.
169 Pop VJ, Brouwers EP, Vader HL, Vulsma T, van Baar AL, de Vijlder JJ: Maternal hypothyroxinaemia during early pregnancy and subsequent child development: a 3-year follow-up study. Clin Endocrinol 2003;59:282-8.
170 De Escobar GM, Obregon MJ, del Rey FE. Maternal thyroid hormones early in pregnancy and fetal brain development. Best Pract Res Clin Metab 2004;18:225-48.
171 WHO, UN Children’s Fund, and International Council for the Control of Iodine Deficiency Disorders. Assessment of iodine deficiency disorders and monitoring their elimination. A guide for programme managers, 3rd Edition. Geneva, Switzerland: WHO, 2007.
References Cited Page 464
Contact PD/PI: Paneth, Nigel S

172 Vermiglio F, Lo Presti VP, Castagna MG, Violi MA, Moleti M, Finocchiaro MD, Mattina F, Artemisia A,
Trimarchi F: Increased risk of maternal thyroid failure with pregnancy progression in an iodine deficient area with major iodine deficiency disorders. Thyroid 1999;9:19-24.
173 Morreale de Escobar G, Obregon MJ, Escobar del Rey F. Iodine deficiency and brain development in the first half of pregnancy. Publ Health Nutr 2007;10:1554-70.
174 Haddow JE, Palomaki GE, Allan WC, Williams JR, Knight GJ, Gagnon J, O’Heir CE, Mitchell ML, Hermos RJ, Waisbren SE, Faix JD, Klein RZ: Maternal thyroid deficiency during pregnancy and subsequent neuropsychological development of the child. N Engl J Med 1999;341:549-55.
175 Roman GC, Ghassabian A, Bongers-Schokking JJ, Jaddoe VW, Hofman A, de Rijke YB, Verhulst FC, Tiemeier H: Association of Gestational Maternal Hypothyroxinemia and Increased ASD Risk. Ann Neurol 2013; Nov;74(5):733-42.
176 Harris KB, Pass KA. Increase in congenital hypothyroidism in New York state and in the United States. Mol Genet Metab 2007;91:268-77.
177 Blount BC, Pirkle JL, Osterloh JD, Valentine-Blasini L, Caldwell KL: Urinary perchlorate & thyroid hormone levels in adolescent & adult men & women living in the US. Environ Health Persp 2006;114:1865-71.
178 Taylor P, Okosieme OE, Channon S et al: Maternal Perchlorate levels during pregnancy and offspring cognitive development: Data from the Controlled Antenatal Thyroid Screening Study. American Thyroid Association 83rd Annual Meeting, San Juan, PR, October 2013.
179 Dorea JG. Maternal thiocyanate and thyroid status during breast-feeding. J Am Coll Nutr 2004;23:97-101. 180 T Tonacchera M, Pinchera A, Dimida A, Ferrarini E, Agretti P, Vitti P, Santini F, Crump K, Gibbs J: Relative
Potencies and Additivity of Perchlorate, Thiocyanate, Nitrate, and Iodide on the Inhibition of Radioactive Iodide Uptake by the Human Sodium Iodide Symporter. Thyroid 2004;14:1012-9.
181 Meberg A, Marstein S. Smoking during pregnancy – effects on the fetal thyroid function. Acta Pediatrica Scand 1986;75:762-6.
182 Chanoine JP, Toppet V, Bourdoux P, Spehl M, Delange F: Smoking during pregnancy: a significant cause of neonatal thyroid enlargement. Br J Obstet Gynaecol 1991;98:65-8.
183 Laurberg P, Nohr SB, Pedersen KM, Fuglsang E: Iodine nutrition in breast-fed infants is impaired by maternal smoking. J Clin Endocrinol Metab 2004;89:181-7.
184 Pearce EN, Oken E, Gillman MW, Lee SL, Magnani B, Platek D, Braverman LE: Association of 1st trimester thyroid function test values w/thyroperoxidase antibody status, smoking, &multivitamin use. Endocr Pract 2008;14:33-9.
185 Lozoff B, Georgieff MK. Iron deficiency and brain development. Semin Pediatr Neurol 2006;13:158-65. 186 Yu X, Shan Z, Li C, Mao J, Wang W, Xie X, Liu A, Teng X, Zhou W, Li C, Xu B, Bi L, Meng T, Du J, Zhang
S, Gao Z, Zhang X, Yang L, Fan C, Teng W: Iron deficiency, an independent risk factor for isolated hypothyroxinemia in pregnant and nonpregnant women of childbearing age in China. J Clin Endocrinol Metab. 2015:100(4):1594-601.
187 Harvey L and Boksa P. Do prenatal immune activation and maternal iron deficiency interact to affect neurodevelopment and early behavior in rat offspring. Brain, Behavior, and Immunity 2014:35:144-204.
188 Shah-Kulkarni S, Ha M, Kim BM Kim E, Hong YC, Park H, Kim Y, Kim BN, Chang N, Oh SY, Kimʼs YJ, Lee B, Ha EH: Neurodevelopment in early childhood affected by prenatal lead exposure and iron intake. Medicine 2016:95(4):1-9.
189 Fisher SC, Kim SY, Sharma AJ, Rochat R, Morrow B: Is obesity still increasing among pregnant women? Prepregnancy obesity trends in 20 states, 2003-2009. 2013:Prev Med, 56(6), 372-8.
190 Yu Z, Han S, Zhu J, Sun X, Ji C, Guo X: Pre-pregnancy body mass index in relation to infant birth weight and offspring overweight/obesity: a systematic review and meta-analysis. 2013:PLoS One, 8(4), e61627.
References Cited Page 465
Contact PD/PI: Paneth, Nigel S

191 Cassidy-Bushrow AE, Wegienka G, Havstad S, Levin AM, Lynch SV, Ownby DR, Rundle AG, Woodcroft
KJ, Zoratti EM, Johnson CC: Does Pet-Keeping Modify the Association of Delivery Mode with Offspring Body Size? Matern Child Health J. 2014:19(6):1426-33.
192 Wylie A, Sundaram R, Kus C, Ghassabian A, Yeung EH: Maternal prepregnancy obesity and achievement of infant motor developmental milestones in the upstate KIDS study. Obesity 2015:23(4), 907-13.
193 Hinkle SN, Sharma AJ, Kim SY et al: Maternal prepregnancy weight status and associations with children's development and disabilities at kindergarten. International journal of obesity 2013:37(10), 1344-51.
194 Huang L, Yu X, Keim S, Li L, Zhang L, Zhang J: Maternal prepregnancy obesity and child neurodevelopment in the Collaborative Perinatal Project. Int J Epidemiol 2014:43(3), 783-92.
195 Kimmons JE, Blanck HM, Tohill BC, Zhang J, Khan LK: Associations between body mass index and the prevalence of low micronutrient levels among US adults. MedGenMed 2006:19:8(4):59.
196 Tomedi LE, Chang CC, Newby PK, Evans RW, Luther JF, Wisner KL, Bodnar LM: Pre-pregnancy obesity and maternal nutritional biomarker status during pregnancy: a factor analysis. Public Health Nutr 2013:16(8):1418-8.
197 Garcia-Valdes L, Campoy C, Hayes H, Florido J, Rusanova I, Miranda MT, McArdle HJ: The impact of maternal obesity on iron status, placental transferrin receptor expression and hepcidin expression in human pregnancy. Int J Obes 2015:39(4):571-8.
198 Sen S, Iver C, Meydani SN. Obesity during pregnancy alters maternal oxidant balance and micronutrient status. J Perinatol 2014:34(2):105-11.
199 Snedeker SM, Hay AG Do interactions between gut ecology and environmental chemicals contribute to obesity and diabetes? Environ Health Perspect 2012:120(3):332-9.
200 Lu K, Abo RP, Schlieper KA, Graffam ME, Levine S, Wishnok JS, Swenberg JA, Tannenbaum SR, Fox JG: Arsenic exposure perturbs the gut microbiome and its metabolic profile in mice: an integrated metagenomics and metabolomics analysis. Environ Health Perspect 2014:122(3), 284-91.
201 Breton J, Massart S, Vandamme P, De Brandt E, Pot B, Foligne B: Ecotoxicology inside the gut: Impact of heavy metals on the mouse microbiome. BMC Pharmacology & Toxicology 2013:14, 62.
202 Mackerras DE, Eastman CJ, Singh GR. Iodine status of Aboriginal teenagers in the Darwin region before mandatory iodine fortification of bread. Med J Aust 2011;194(3):126-30.
203 Pearce EN, Lazarus JH, Smyth PP, He X, Smith DF, Pino S, Braverman LE: Urine test strips as a source of iodine contamination. Thyroid 2009;19:919.
204 Hamilton CM, Strader LC, Pratt JG, Maiese D, Hendershot T, Kwok RK, Hammon JA, Huggins W, Jackman D, Pan H, Nettles DS, Beaty TH, Farrer La, Kraft P, Marazita ML, Ordovas JM, Pato CN, Spitz MR, Wagener D, Williams M, Junkins HA, Harlan WR, Ramos EM, Haines J: The PhenX Toolkit: Get the most from your measures. American Journal of Epidemiology. 2011;174(3):253-260.
205 Hendershot T, Pan H, Haines J, Harlan WR, Junkins HA, Ramos Em, Hamilton CM: Using the PhenX Toolkit to Add Standard Measures to a Study. Current protocols in human genetics / editorial board, Jonathan L. Haines et al: 2011;Chapter 1:Unit1 21.
206 Thompson FE, Midthune D, Subar AF, Kipnis V, Kahle LL, Schatzkin A. Development and evaluation of a short instrument to estimate usual dietary intake of percentage energy from fat. Journal of the American Dietetic Association. 2007;107(5):760-767.
207 Thompson FE, Midthune D, Williams GC, Yaroch AL, Hurley TG, Resnicow K, Herbert JR, Toobert DJ, Greene GW, Peterson K, Nebeling L: Evaluation of a short dietary assessment instrument for percentage energy from fat in an intervention study. The Journal of Nutrition. 2008;138(1):193S-199S.
208 National Cancer Institute. Five-Factor Screener National Health Interview Survey (NHIS) Diet and Nutrition. 2005;NAC.010–NAC.138.
References Cited Page 466
Contact PD/PI: Paneth, Nigel S

209 Lin JS, O'Connor E, Whitlock EP, Beil TL: Behavioral counseling to promote physical activity and a healthful
diet to prevent cardiovascular disease in adults: a systematic review for the U.S. Preventive Services Task Force. Annals of Internal Medicine. Dec 7 2010;153(11):736-750.
210 Rees K, Dyakova M, Ward K, Thorogood M, Brunner E. Dietary advice for reducing cardiovascular risk. The Cochrane Database of Systematic Reviews. 2013;3:CD002128.
211 Schaefer EJ. Lipoproteins, nutrition, and heart disease. The American Journal of Clinical Nutrition. Feb 2002;75(2):191-212.
212 Kozich JJ, Westcott SL, Baxter NT, Highlander SK, Schloss PD. Development of a dual-index sequencing strategy and curation pipeline for analyzing amplicon sequence data on the MiSeq Illumina sequencing platform. Appl Environ Microbiol. 2013; 79(17):5112-20.
213 Schloss PD, Westcott SL, Ryabin T, Hall JR, Hartmann M, Hollister EB, Lesniewski RA, Oakley BB, Parks DH, Robinson CJ, Sahl JW, Stres B, Thallinger GG, Van Horn DJ, Weber CF. Introducing mothur: open-source, platform-independent, community-supported software for describing and comparing microbial communities. Appl Environ Microbiol. 2009; 75(23):7537-41.
214 Gregg N McA. Congenital cataract following German measles in the mother. Trans Ophthalmol Soc Aust
1941; 3: 35-46 215 Silasi M, Cardenas I, Kwon JY, Racicot K, Aldo P, Mor G. Viral infections during pregnancy. American
journal of reproductive immunology. 2015;73(3):199-213. doi: 10.1111/aji.12355. PubMed PMID: 25582523; PMCID: PMC4610031.
216 Cheeran MC, Lokensgard JR, Schleiss MR. Neuropathogenesis of congenital cytomegalovirus infection: disease mechanisms and prospects for intervention. Clinical microbiology reviews. 2009;22(1):99-126, Table of Contents. doi: 10.1128/CMR.00023-08. PubMed PMID: 19136436; PMCID: PMC2620634.
217 Enright AM, Prober CG. Neonatal herpes infection: diagnosis, treatment and prevention. Seminars in Neonatology. 2002;7(4):283-91. doi: 10.1053/siny.2002.0115.
218 Kenneson A, Cannon MJ. Review and meta-analysis of the epidemiology of congenital cytomegalovirus (CMV) infection. Reviews in medical virology. 2007;17(4):253-76.
219 Buka SL, Cannon TD, Torrey EF, Yolken RH, Collaborative Study Group on the Perinatal Origins of Severe Psychiatric D. Maternal exposure to herpes simplex virus and risk of psychosis among adult offspring. Biological psychiatry. 2008;63(8):809-15. doi: 10.1016/j.biopsych.2007.09.022. PubMed PMID: 17981263.
220 Korndewal MJ, Vossen AC, Cremer J, VAN Binnendijk RS, Kroes AC, VAN DER Sande MA, Oudesluys-Murphy AM, DE Melker HE: Disease burden of congenital cytomegalovirus infection at school entry age: study design, participation rate and birth prevalence. Epidemiol Infect. 2015 Nov 11:1-8.
221 Brown Z, Benedetti J, Ashley R, Burchett S, Selke S, Berry S, Corey L. Neonatal Herpes simples virus infection in relation to asymptomatic maternal infection at the time of labor. NEJM. 1991;324:1247-52.
222 Reef SE, Frey TK, Theall K, Abernathy E, Burnett CL, Icenogle J, McCauley MM, Wharton M: The changing epidemiology of rubella in the 1990s: on the verge of elimination and new challenges for control and prevention. JAMA. 2002;287(4):464.
223 Racicot K, Mor G: Inflammation and Placentation. In The Placenta and Neurodisability. 2015 Mac Keith Press; Second Edition Edited by Ian Crocker and Martin Bax: pp 50-60.
224 Racicot K, Kwon JY, Aldo P, Abrahams V, El-Guindy A, Romero R, Mor G. Type I Interferon Regulates the Placental Inflammatory Response to Bacteria and is Targeted by Virus: Mechanism of Polymicrobial Infection-Induced Preterm Birth. American journal of reproductive immunology. 2016;75(4):451-60. doi: 10.1111/aji.12501. PubMed PMID: 26892235.
225 Cardenas I, Means RE, Aldo P, Koga K, Lang SM, Booth CJ, Manzur A, Oyarzun E, Romero R, Mor G. Viral infection of the placenta leads to fetal inflammation and sensitization to bacterial products predisposing
References Cited Page 467
Contact PD/PI: Paneth, Nigel S

to preterm labor. Journal of immunology. 2010;185(2):1248-57. Epub 2010/06/18. doi: 10.4049/jimmunol.1000289. PubMed PMID: 20554966; PMCID: 3041595.
226 Mor G. Placental Inflammatory Response to Zika Virus may Affect Fetal Brain Development. American journal of reproductive immunology. 2016;75(4):421-2. doi: 10.1111/aji.12505. PubMed PMID: 26892436.
227 Atladottir HO, Thorsen P, Ostergaard L, Schendel DE, Lemcke S, Abdallah M, Parner ET. Maternal infection requiring hospitalization during pregnancy and autism spectrum disorders. J Autism Dev Disord. 2010;40(12):1423-30. doi: 10.1007/s10803-010-1006-y. PubMed PMID: 20414802.
228 Choi G, Yim Y, Wong H, Kim S, Kim H, Kim S, Hoeffer C, Littman D, Huh J. The maternal IL17a pathway in mice promotes autism phenotypes in offspring. Science. 2016;351(6276).
229 Straley ME, Togher KL, Nolan AM, Kenny LC, O'Keeffe GW. LPS alters placental inflammatory and endocrine mediators and inhibits fetal neurite growth in affected offspring during late gestation. Placenta. 2014. Epub 2014/06/26. doi: 10.1016/j.placenta.2014.06.001. PubMed PMID: 24961461.
230 Brown AS. Prenatal infection as a risk factor for schizophrenia. Schizophrenia bulletin. 2006;32(2):200-2. Epub 2006/02/14. doi: 10.1093/schbul/sbj052. PubMed PMID: 16469941; PMCID: 2632220.
231 O'Callaghan E, Sham P, Takei N, Glover G, Murray RM. Schizophrenia after prenatal exposure to 1957 A2 influenza epidemic. Lancet. 1991;337(8752):1248-50. Epub 1991/05/25. PubMed PMID: 1674062.
232 Shi L, Fatemi SH, Sidwell RW, Patterson PH. Maternal influenza infection causes marked behavioral and pharmacological changes in the offspring. The Journal of neuroscience : the official journal of the Society for Neuroscience. 2003;23(1):297-302. Epub 2003/01/07. PubMed PMID: 12514227.
233 Raj RS, Bonney EA, Phillippe M. Influenza, immune system, and pregnancy. Reproductive sciences. 2014;21(12):1434-51. doi: 10.1177/1933719114537720. PubMed PMID: 24899469; PMCID: PMC4231130.
234 Shi L, Tu N, Patterson PH. Maternal influenza infection is likely to alter fetal brain development indirectly: the virus is not detected in the fetus. International journal of developmental neuroscience : the official journal of the International Society for Developmental Neuroscience. 2005;23(2-3):299-305. PMID: 15749254.
235 van der Burg JW, Allred EN, McElrath TF, Fichorova RN, Kuban K, O'Shea TM, Dammann O, Leviton A: Is maternal obesity associated with sustained inflammation in extremely low gestational age newborns? Early Hum Dev. 2013 Dec;89(12):949-55.
236 Challier JC, Basu S, Bintein T, Minium J, Hotmire K, Catalano PM, Hauguel-de Mouzon S. Obesity in pregnancy stimulates macrophage accumulation and inflammation in the placenta. Placenta. 2008;29(3):274-81. Epub 2008/02/12. doi: 10.1016/j.placenta.2007.12.010. PubMed PMID: 18262644.
237 Roberts KA, Riley SC, Reynolds RM, Barr S, Evans M, Statham A, Hor K, Jabbour HN, Norman JE, Denison FC. Placental structure and inflammation in pregnancies associated with obesity. Placenta. 2011;32(3):247-54. doi: 10.1016/j.placenta.2010.12.023. PubMed PMID: 21232790.
238 Kramer BW, Kaemmerer U, Kapp M, Herbst D, Marx A, Berg D, Groneck PA, Speer CP. Decreased expression of angiogenic factors in placentas with chorioamnionitis after preterm birth. Pediatr Res. 2005;58(3):607-12. doi: 10.1203/01.PDR.0000175641.39056.7A. PubMed PMID: 16148081.
239 Aye IL, Lager S, Ramirez VI, Gaccioli F, Dudley DJ, Jansson T, Powell TL. Increasing maternal body mass index is associated with systemic inflammation in the mother and the activation of distinct placental inflammatory pathways. Biology of reproduction. 2014;90(6):129. Epub 2014/04/25. doi: 10.1095/biolreprod.113.116186. PubMed PMID: 24759787.
240 Patterson PH. Immune involvement in schizophrenia and autism: etiology, pathology and animal models. Behavioural brain research. 2009;204(2):313-21. Epub 2009/01/13. doi: 10.1016/j.bbr.2008.12.016. PubMed PMID: 19136031.
241 Fatemi SH, Pearce DA, Brooks AI, Sidwell RW. Prenatal viral infection in mouse causes differential expression of genes in brains of mouse progeny: a potential animal model for schizophrenia and autism. Synapse. 2005;57(2):91-9. doi: 10.1002/syn.20162. PubMed PMID: 15906383
References Cited Page 468
Contact PD/PI: Paneth, Nigel S

242 Atladottir HO, Thorsen P, Ostergaard L, Schendel DE, Lemcke S, Abdallah M, Parner ET. Maternal
infection requiring hospitalization during pregnancy and autism spectrum disorders. J Autism Dev Disord. 2010;40(12):1423-30. doi: 10.1007/s10803-010-1006-y. PubMed PMID: 20414802.
243 Kuban KC, O'Shea TM, Allred EN, Fichorova RN, Heeren T, Paneth N, Hirtz D, Dammann O, Leviton A, Investigators ES. The breadth and type of systemic inflammation and the risk of adverse neurological outcomes in extremely low gestation newborns. Pediatric neurology. 2015;52(1):42-8. doi: 10.1016/j.pediatrneurol.2014.10.005. PubMed PMID: 25459361; PMCID: PMC4276530.
244 Leviton A, Allred EN, Fichorova RN, Kuban KC, O'Shea TM, Dammann O, Investigators ES. Antecedents of inflammation biomarkers in preterm newborns on days 21 and 28. Acta Paediatr. 2016;105(3):274-80. doi: 10.1111/apa.13286. PubMed PMID: 26610180; PMCID: PMC4747803.
245 Aagaard K, Ma J, Antony KM, Ganu R, Petrosino J, Versalovic J. The placenta harbors a unique microbiome. Science translational medicine. 2014;6(237):237ra65. doi: 10.1126/scitranslmed.3008599. PubMed PMID: 24848255.
246 Racicot K, Kwon JY, Aldo P, Abrahams V, El-Guindy A, Romero R, Mor G: Type I Interferon Regulates the Placental Inflammatory Response to Bacteria and is Targeted by Virus: Mechanism of Polymicrobial Infection-Induced Preterm Birth. Am J Reprod Immunol. 2016 Apr;75(4):451-60
247 Jamieson AM, Yu S, Annicelli CH, Medzhitov R. Influenza virus-induced glucocorticoids compromise innate host defense against a secondary bacterial infection. Cell host & microbe. 2010;7(2):103-14. Epub 2010/02/18. doi: 10.1016/j.chom.2010.01.010. PubMed PMID: 20159617; PMCID: 2836270.
248 Aagaard K, Ma J, Antony KM, Ganu R, Petrosino J, Versalovic J. The placenta harbors a unique microbiome. Science translational medicine. 2014;6(237):237ra65. doi: 10.1126/scitranslmed.3008599. PubMed PMID: 24848255.
249 Ramsey JO, Silverman BW: Functional Data Analysis, 2nd Edition. Springer, 2005. 250 Holm S: A simple sequentially rejective multiple test procedure. Scandinavian Journal of Statistics 1979; 6 (2): 65–70. 251 Ye Y, Li A, Liu L, Yao B: A group sequential Holm procedure with multiple primary endpoints. Stat Med.
2013 Mar 30;32(7):1112-24. 252 Benjamini, Y., & Hochberg, Y. (1995). Controlling the false discovery rate: a practical and powerful approach
to multiple testing. Journal of the Royal Statistical Society. Series B (Methodological), 57:289-300. 253 VanderWeele TJ, Mumford SL, Schisterman E: Conditioning on intermediates in perinatal epidemiology.
Epidemiology. 2012 Jan;23(1):1-9. 254 Baron R M, Kenny DA:The moderator–mediator variable distinction in social psychological research:
Conceptual, strategic, and statistical considerations. Journal of personality and social psychology, 1986: 51(6), 1173.
255 VanderWeele TJ: Bias formulas for sensitivity analysis for direct and indirect effects. Epidemiology 2010;21:540-551.
256 Vittinghoff E, Sen S, McCulloch CE: Sample size calculations for evaluating mediation. Statistics in Medicine, 2009; 28:541-557.
257 McArdle BH, Anderson MJ. Fitting multivariate models to community data: a comment on distance-based redundancy analysis. Ecology 2001; 82:290–297.
258 Imai K, Keele L, Tingley D. A general approach to causal mediation analysis. Psychological methods. 2010;15(4):309-334.
259 Waldron L, Pintilie M, Tsao MS, et al. Optimized application of penalized regression methods to diverse genomic data. Bioinformatics. 2011;27(24):3399-3406.
References Cited Page 469
Contact PD/PI: Paneth, Nigel S

260 Storey JD, Tibshirani R. Statistical significance for genomewide studies. Proc Natl Acad Sci U S A.
2003;100(16):9440-9445. 261 Cribari-Neto F, Zeileis A: Beta Regression in R. Journal of Statistical Software 2010; 34(2): 1-24. 262 Bass JD, Storey, JD, Dabney A and Robinson D (2015). qvalue: Q-value estimation for false discovery rate
control. R package version 2.2.2, http://github.com/jdstorey/qvalue 263 Aryee MJ, Jaffe AE, Corrada-Bravo H, Ladd-Acosta C, Feinberg AP, Hansen KD, Irizarry RA: Minfi: a flexible and
comprehensive Bioconductor package for the analysis of Infinium DNA methylation microarrays. Bioinformatics 2014; 30(10): 1363-1369.
264 Subramanian A, Tamayo P, Mootha VK, Mukherjee S, Ebert BL, Gillette MA, Paulovich A, Pomeroy SL, Golub TR, Lander ES, Mesirov JP. Gene set enrichment analysis: a knowledge-based approach for interpreting genome-wide expression profiles. Proc Natl Acad Sci U S A. 2005 Oct 25;102(43):15545-50.
265 Raghunathan, T. E., Lepkowski, J. M., Van Hoewyk, J., & Solenberger, P. (2001). A multivariate technique for multiply imputing missing values using a sequence of regression models. Survey methodology, 27: 85-96
References Cited Page 470
Contact PD/PI: Paneth, Nigel S
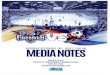
























![Nirvana - [Book] in Utero - Guitar Songbook 3](https://img.pdfslide.us/doc/110x75/5695cff41a28ab9b02904a8a/nirvana-book-in-utero-guitar-songbook-3.jpg)