Embed Size (px)
Citation preview

INFECTION
Rational antibiotic use insurgerySarah Thompson
Elisabeth J Ridgway
AbstractRational use of antibiotics is crucial to limit the evolution of resistant
organisms, reduce the occurrence of healthcare-associated infections,
and reduce costs.
Once an infection has been diagnosed, empirical therapy (started
before definitive identification of the pathogen) is common. To aid the
selection of an effective antibiotic, several variables should be consid-
ered, such as the previous microbiology results, recent antibiotics, the
patient’s journey through the hospital, antibiotic allergies and renal/
liver abnormalities.
The duration of antibiotic courses should be as short as possible, and
intravenous antibiotics can usually be switched to an oral regimen after
48 h. The presence of undrained collections, foreign bodies and infected
intravascular lines are common reasons for treatment failure despite an
appropriate antibiotic.
Keywords antibiotic; Clostridium difficile; empirical treatment;
guidelines; infection; MRSA; resistance
Most hospitals have antibiotic policies to guide the clinician in
making rational antibiotic choices. However, complex cases
should be discussed with a microbiologist.
Appropriate antibiotic use in the clinical environment is vital.
Resistant organisms are being increasingly encountered, as are
healthcare-associated infections (HCAIs) related to inappropriate
antibiotic prescribing. A logical approach to the infected patient
(i.e. choosing the correct antibiotic, giving it by the optimal route
and for the correct duration) is essential.
This contribution looks at the rationale behind antimicrobial
prescribing in the surgical patient, and should be read in
conjunction with ‘Prophylactic Antibiotics in Surgery’, on pages
431e434 of this issue.
Resistance
What is driving antibiotic resistance?
Bacterial resistance to antibiotics is not a new phenomenon.
However, decreased antibiotic susceptibility among common,
Sarah Thompson MBChB BSc is a Specialty Registrar in Medical Micro-
biology at Sheffield Teaching Hospitals Trust, Sheffield, UK and
a member in Department of Microbiology, Northern General Hospital,
Herries Road, Sheffield S5 7AU, UK. Conflicts of interest: none declared.
Elisabeth J Ridgway MBBS FRCPath MD is a Consultant Microbiologist at
Sheffield Teaching Hospitals Trust, Sheffield, UK and a member in
Department of Microbiology, Royal Hallamshire Hospital, Glossop
Road, Sheffield S10 2JF, UK. Conflicts of interest: none declared.
SURGERY 27:10 435
previously sensitive bacterial species is, and is concerning
patients, doctors and policy-makers. Widespread antibiotic use is
driving this trend and has two main consequences. First, it
promotes the emergence of organisms that are resistant to the
agents in use and, secondly, it suppresses the protective normal
flora and allows organisms such as Candida species, Steno-
trophomonas maltophilia and Clostridium difficile to become
established.1 The antibiotics in widespread use in surgical prac-
tice (e.g. co-amoxiclav, cephalosporins, quinolones) are partic-
ularly to blame in this respect as they are both broad-spectrum
and have limited activity against the common resistant
organisms.
A growing number of patients have an increased susceptibility
to infection (e.g. elderly, immunocompromised). This has
created a desire to intervene and treat infections early with
broad-spectrum agents. The mounting pressure on hospital beds
has led to a tendency to treat on suspicion, before the necessary
evidence is gathered to make a firm diagnosis of infection.
Antibiotic stewardship is the key to minimizing the trend
towards antimicrobial resistance, and preserving antibiotic effi-
cacy. This is the concept of responsible caretaking; it is based on
the premise that we don’t own resources, but simply manage
them and are responsible to future users for the maintenance of
their usefulness. It takes into account the needs of individuals
and the interests of society, and accepts significant answerability
to both.
Put simply, the challenge is to treat infected individual
patients optimally whilst preventing antibiotic overuse.
How common are resistant organisms?
Escherichia coli is a Gram-negative organism commonly impli-
cated in intra-abdominal and urinary tract infections. Between
2000 and 2007, the UK has seen increasing resistance, through
extended-spectrum b lactamases, of E. coli to cephalosporins
(12-fold increase), quinolones (5-fold increase) and amino-
glycosides (3-fold increase).2 The isolation of Gram-negative
organisms that are inherently resistant to commonly used anti-
biotics (e.g. Citrobacter spp., Serratia spp., Acinetobacter spp.) is
also rising.2
Methicillin-resistant Staphylococcus aureus (MRSA) is another
resistant organism with an increasing prevalence. It is important
because strains are resistant to flucloxacillin, and often to other
useful agents. 53% of post-operative surgical-site infections
(SSIs) are caused by S. aureus, and 64% of these are now MRSA.3
Identifying these patients and treating them appropriately is
important, as those with MRSA-associated SSI have a greater
90-day mortality, longer hospital stay and incur more costs than
those infected with methicillin-sensitive S. aureus (MRSA).4
Enterococci are enteric Gram-positive organisms often
involved in polymicrobial abdominal infections. Although they
are intrinsically resistant to many classes of antibiotics (e.g.
cephalosporins, quinolones) most are sensitive to amoxicillin.
Glycopeptides (e.g. vancomycin) are the mainstay of treatment in
amoxicillin resistance or in patients with a penicillin allergy.
Currently, 10% of enterococci are resistant to glycopeptides,2
and these organisms are also almost always amoxicillin resistant,
presenting significant therapeutic challenges.
C. difficile can cause debilitating diarrhoea (C. difficile-
associated diarrhoea, CDAD), and severe disease may lead to
� 2009 Elsevier Ltd. All rights reserved.

INFECTION
colonic perforation and sepsis; 90% of infections follow antibi-
otic use.5 Exposure to antibiotics alters the normal flora of the
gut, providing an environment in which C. difficile can flourish.
Whilst certain antibiotics (e.g. cephalosporins, ciprofloxacin,
clindamycin) are particularly associated with the development of
disease, diarrhoea can follow the use of any antibiotic,5 even
when only a single dose is given. Not only is there a substantial
mortality directly attributable to the infection, C. difficile-
associated morbidity increases the length of hospital stay by
8e21 days.5 The increasing prevalence of CDAD has led to the
review of antimicrobial policy in many hospitals, with a switch to
narrow-spectrum agents such as gentamicin and flucloxacillin, in
an attempt to lessen the negative impact of antibiotic use.
Antibiotic choice
Does choosing the correct antibiotic make a difference?
Overall, patients in whom appropriate antibiotic therapy is
delayed are more likely to experience complications, have
a longer hospital stay and have a higher mortality rate.6 In
surgery, this is illustrated by the finding that patients with peri-
tonitis, who received antibiotics to which at least one pathogen
was resistant were 2e3 times more likely to experience
re-operation, abscess formation and further infection than those
who received antibiotics correctly targeting the infecting
species.7 The effect of inappropriate antibiotics on mortality is
similar; a 42% mortality rate was seen when the antibiotics
prescribed did not cover the causative organisms, compared to
17.7% in those whose antibiotics were effective against the
pathogens isolated.8
How do I choose the correct antibiotic?
It is useful to have a logical approach to antibiotic prescribing.
Antibiotic use for prophylaxis should be distinguished from that
for therapy. Allocation to the wrong category is a significant
cause of irrational antibiotic use.
The need for therapy should be firmly established, guided by
the following features:
� clinical picture
� relevant radiology
� inflammatory markers (white cell count, CRP, procalcitonin).
In order to eradicate the organism causing the infection, the
correct antibiotic given by the correct route for the correct
duration must be chosen. This ensures the antibiotic concentra-
tions at the site of infection are optimal but that side effects are
avoided and costs minimized. However, it can be difficult to
diagnose infection, particularly in the absence of an overt focus,
and clinical progress can be unpredictable, regardless of the
antibiotic used and the in vitro sensitivity results. Some infec-
tions resolve spontaneously, whilst others continue unabated
despite appropriate therapy. Targeted therapy (when the causa-
tive organism and its sensitivities are known) is ideal. However
empirical therapy (when the pathogen has not yet been defini-
tively identified) aimed at a suspected focus of infection is more
commonly given. In both scenarios, appropriate microbiological
samples (e.g. blood cultures, sputum, urine, wound swab, stool)
should be obtained prior to antibiotics being commenced.
Cultures may be negative if taken during or after a course of
antibiotics.
SURGERY 27:10 436
Empirical regimens e Having identified a likely focus of infec-
tion (e.g. surgical-site infection with cellulitis, post-operative
pneumonia) an appropriate empirical regimen relies on knowl-
edge of the likely causative organisms and their local suscepti-
bility patterns. The latter will also be required if a pathogen has
been cultured, but sensitivity results are pending. This informa-
tion is often built into local antibiotic prescribing guidelines;
alternatively the Microbiology Department can offer advice. A
range of factors must be considered when choosing a regimen,
and answers should be available before phoning
a microbiologist:
� Recent or relevant microbiology results.
� Does the patient have a history of antibiotic resistant organ-
isms (e.g. MRSA) or C. difficile infection?
� What other antibiotics, including those used for prophylaxis,
has the patient received recently? Prior antibiotic therapy is
a major risk factor for the acquisition of resistant bacteria.
� Where has the patient been admitted from, for how long have
they been an inpatient and what kind of ward are they on?
Those patients admitted from a nursing home or transferred
from another hospital are at higher risk of resistant organisms
than those admitted from home. Acquisition of resistant
pathogens is more likely with increasing length of stay, and
specifically stays on ICU or Burns Units, and on wards where
outbreaks are in progress or background rates of resistant
organisms are high.1
� Is the patient allergic to any classes of antibiotic, and what is
the nature of the allergy?
� Are there any physiological factors that may influence which
antibiotics can be administered e such as abnormalities of
renal or liver function, pregnancy?
Empirical regimens usually provide broad-spectrum Gram-posi-
tive, Gram-negative and anaerobic cover. This may be through
the administration of a single agent, or multiple narrow-spectrum
combination antibiotic therapy.1 In general, broad-spectrum
agents are more problematic than narrow-spectrum ones.
Therefore, strategies must be in place that decrease broad
empirical therapy whilst maintaining effective cover. When
microbiological results are available, ‘de-escalating’ to a narrow-
spectrum antibiotic or discontinuing an agent may be possible
and is encouraged (e.g. switching a cephalosporin to fluclox-
acillin when a flucloxacillin-sensitive S. aureus is grown from
a wound swab). Advice from pharmacists and microbiologists
can help with this process, and it may be incorporated into
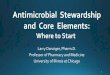
a hospital antimicrobial guidelines. Examples of empirical regi-
mens are shown in Table 1.
Targeted therapy e Targeted therapy is possible if the choice of
antibiotic is guided by the microbiology data. This may also
influence the duration of treatment. An agent with as narrow
spectrum as possible (to which the patient is not allergic) should
be chosen.
Route of administration e It is common practice in the UK to
treat life-threatening infections with parenteral antibiotics
because delivery to tissues is guaranteed. If absorption is unim-
paired, oral treatment is usually adequate for less serious infec-
tions. Quinolones, fusidic acid, linezolid, clindamycin and
metronidazole have good oral bioavailability and the intravenous
� 2009 Elsevier Ltd. All rights reserved.

Examples of empirical antibiotic choices in surgery
Infection Initial empirical choice Penicillin allergy (non-anaphylaxis) Route Duration (approximate) Cautions
Peritonitis Co-amoxiclav
or
Amoxicillin þ metronidazole þ aminoglycoside
(e.g. gentamicin)
Cefuroxime þ metronidazole i.v. 5e7 days Risk of multi-resistant Gram-negative
organisms
Biliary infections Co-amoxiclav
or
Amoxicillin þ metronidazole þ aminoglycoside
(e.g. gentamicin)
Cefuroxime þ metronidazole i.v. 7e10 days Risk of multi-resistant Gram-negative
organisms
Osteomyelitis Flucloxacillin þ fusidic acid/rifampicin Clindamycin Initially i.v. 6 weeks in total Biopsy before treatment if possible
Never use rifampicin or fusidic acid
monotherapy
Necrotizing infections of
soft tissue
Amoxicillin þ metronidazole þ aminoglycoside
(e.g. gentamicin)
or
Piperacillin/tazobactam þ clindamycin
Clindamycin þ ciprofloxacin i.v. Depends upon clinical
response/severity
An adjunct to surgery
Surgical-site infection Clean surgery: Flucloxacillin
Contaminated/dirty: Co-amoxiclav
Clindamycin
Doxycycline
Initially i.v. Depends upon clinical
response/severity
Consider likelihood of MRSA. Prophylactic
antibiotics may have altered flora
Acute pyelonephritis Aminoglycoside (e.g. gentamicin)
or
Co-amoxiclav
Aminoglycoside (e.g. gentamicin) Initially i.v. 10e14 days Risk of multi-resistant Gram-negative
organisms
Epiglottitis Cefuroxime/cefotaxime
or ciprofloxacin
Cefuroxime/cefotaxime Initially i.v. 7e10 days Seek advice on prophylaxis for contacts of
invasive Haemophilus influenzae infection
These examples are provided as a guide. Where available, local prescribing guidelines should be followed. For doses, refer to the British National Formulary or the Renal Drug Handbook (in cases of renal dysfunction).
Contact the microbiologist if there is no response, physical condition deteriorates, if there is a possibility of allergy to the empirical agents or if there is a history of MRSA infection or colonization.
Table 1
INFE
CTIO
N
SURGERY
27:1
0437
�2009
Elsevie
rLtd
.All
rights
rese
rved.

INFECTION
route offers little advantage in administration. Oral administra-
tion may avoid the need for intravenous access, thereby reducing
the risks of nosocomial bacteraemia.
Penicillin allergy e Allergy to penicillin is the most commonly
reported antibiotic reaction. The nature of the allergy should be
carefully explored and then documented in the medical notes and
on the drug chart. Many ‘allergies’ consist of gastrointestinal
upset (nausea, diarrhoea), which are common reactions to anti-
biotic administration and can be disregarded. True IgE-mediated
allergy is characterized by urticaria, laryngeal oedema, bron-
chospasm, hypotension or local swelling (including colic and
vomiting) within 1e2 h of administration. However, only
a minority of patients who claim to be penicillin allergic have
true IgE-mediated allergy. StevenseJohnson syndrome and toxic
epidermal necrolysis are more dangerous than anaphylaxis and
also require avoidance of penicillins. Delayed reactions have
many other causes. Many late-onset macular/papular rashes are
not IgE-mediated, but may be related to the drug and may still
require avoidance. It should be noted that mild previous reac-
tions do not guarantee mild reactions in the future. In general,
penicillins (including extended-spectrum agents such as co-
amoxiclav and piperacillin/tazobactam) should be avoided in
patients who report penicillin allergy. In patients without IgE-
mediated reactions, cephalosporins and other beta-lactams (e.g.
carbapenems and aztreonam) may be used with caution. Most
guidelines give options for penicillin-allergic patients but where
there is doubt, advice should be sought from pharmacy or
a microbiologist.
What are the next steps?
Having decided on the antibiotic and the route of administration,
the clinical response and inflammatory markers should be
monitored closely.
Duration e Establishing the duration of treatment is important in
order to maintain a favourable balance between adequately
treating the infection and minimizing the development of adverse
effects (e.g. resistance, CDAD). Antibiotics should be given for
the shortest duration possible and many infections can be
effectively treated with short-duration therapy (one week or less)
e particularly when an infective focus has been drained, or
source control is effective. For example, patients with compli-
cated intra-abdominal infections (e.g. peritonitis) can be safely
treated with 5e7 days of antibiotics, or even less if the infection
is localized (e.g. localized appendix perforation).8 Five days of
antibiotic therapy are adequate for most post-operative chest
infections, and three days for uncomplicated urinary tract
infections.
A review or stop date should be clearly stated on the
prescription chart and the need for continuing therapy should be
reviewed daily. Microbiological specimens taken before
commencing antibiotics that fail to grow any pathogens may be
reassuring when making a decision to stop treatment.
Switching from the IV to oral route e Many UK hospitals have
incorporated a switch from intravenous to oral antibiotics into
their prescribing guidelines. This allows parenteral therapy to be
limited to the early phase of treatment, with the course
SURGERY 27:10 438
completed via the oral route once the patient has clinically
improved. This has several advantages including earlier
discharge from hospital, reduced risk of cannula-site infection
and reduced cost.9 The criteria for switching to oral therapy
usually include:9
� clinical response
� defervescence
� improvement in inflammatory markers
� absence of co-morbidity/immunosuppression that would
necessitate intravenous treatment
� appropriate oral agent(s) being available that cover the
pathogen(s) causing the infection and that achieve adequate
penetration at the infection site
� absence of gastrointestinal problems causing reduced
absorption.
A switch to oral therapy is often appropriate after 48 h of
intravenous treatment, but this depends on the individual and
local policy. It is important to continue to monitor the clinical
response and inflammatory markers after a switch has been made.
Other measures e Antibiotics form only one part of the
treatment of surgical infection. The penetration of antibiotics
into enclosed spaces is poor and pus may render the agent
inactive. It is therefore imperative that collections are drained
and free drainage restored (adequate source control). In
a patient not clinically responding to appropriate antibiotic
therapy, imaging should be considered to search for a hidden
collection. Foreign bodies also reduce the effectiveness of
antibiotics and should be removed wherever possible, partic-
ularly if the clinical response is poor. This also applies to
intravascular devices; blood cultures from each lumen of a long
catheter (in addition to peripheral cultures) should be taken as
part of the investigation of fever in a surgical patient. Whilst
some line infections can be managed with the catheter kept in
place, others, such as S. aureus and Candida spp., almost
always necessitate line removal.
How do I take into account local epidemiology?
Many UK hospitals have local policies to direct antimicrobial use
in order to:10
� provide appropriate empirical choices for a wide range of
infections
� limit further evolution of bacterial resistance
� consider local epidemiology and resistance patterns
� control costs1
� limit the risk of healthcare-associated infections9 (e.g. CDAD).
Antibiotic prescribing guidelines are reviewed regularly so
that up-to-date resistance patterns are reflected in the recom-
mendations. An increasing national prevalence of CDAD with
several large and well-publicized outbreaks has resulted in
changes to many antibiotic policies. Cephalosporins, previ-
ously a mainstay of surgical prescribing, have been removed
from many surgical protocols due to their association with
CDAD. Replacements include co-amoxiclav, piperacilline
tazobactam and amoxicillin/gentamicin combinations,
although it should be remembered that almost all antibiotics
can result in CDAD.
To further promote prudent antibiotic prescribing, some
hospitals have introduced a list of ‘restricted’ antimicrobials.10
� 2009 Elsevier Ltd. All rights reserved.

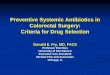
Antibiotic therapy
Is the antibiotic for prophylaxis or treatment?
Yes
Yes
No
Yes
Yes
No
No
Is there good clinical evidence of infection?Send data (cultures, WBC, CRP, imaging) to assist diagnosis
Do previous microbiology data existto guide therapy?
Can you wait formicrobiology data?
Follow prophylaxis guidelinesappropriate for the procedure
Are adjunctive measures required?
Antibiotics are not indicatedEnsure regular review of patient and laboratory results
Complicated patient or infection?Contact microbiologist
Targeted therapy is possible; base antibiotic choice on sensitivity data
Set a stop or review dateReview need for antibiotics dailySwitch to oral therapy as soon as appropriateKeep courses of antibiotic short
Empirical regimenUse local guidelines (if available), but consider:• likely focus of infection• carriage of resistant organisms (e.g. MRSA)• type of ward/outbreaks• previous use of antibiotics• allergies; liver/renal function
Set a stop or review dateReview need for antibiotics dailyNarrow the spectrum when data is available,then move to targeted therapySwitch to oral therapy as soon as appropriateKeep courses of antibiotic short
• drainage of abscess or collection• relief of obstruction• removal of foreign body• removal of catheter
WBC: White blood cell
CRP: C-reactive protein
MRSA: Methicillin-resistant Staphylococcus aureus
Figure 1
INFECTION
Such antibiotics cannot be prescribed without discussion with
a microbiologist, and their use is warranted only when no
alternative agent is available. Antibiotics that are commonly
restricted include those that are particularly broad-spectrum (e.g.
carbapenems), expensive (e.g. linezolid) or associated with the
promotion of CDAD (e.g. cephalosporins).
Guidelines never cover all eventualities and in difficult cases
(e.g. those with complex histories, previous exposure to multiple
antibiotics, multiple allergies or unusual or complicated infec-
tions) microbiological advice should always be sought. Advice
on appropriate specimens and investigations may also be vital in
these patients.
Specialist areas e Intensive care (ICU) and high-dependency
(HDU) units often appear to have their own unique bacterial flora
and the prevalence of antibiotic-resistant organisms is usually
significantly higher than on other hospital wards. This is largely
because patients usually arrive with a substantial ‘antibiotic
history’ and these units are heavy users of antibiotics, particu-
larly empirically given, broad-spectrum agents. Unusual bacterial
species and increased resistance may necessitate the use of
antimicrobials infrequently encountered elsewhere in the
hospital, and this may make appropriate antibiotic choice diffi-
cult. Advice from a microbiologist who is familiar with the
ecology of the unit is indispensable. Once returned to a regular
ward, an ex-ITU or HDU patient remains at increased risk of
SURGERY 27:10 439
resistant and unusual organisms and this should be considered
when choosing empirical antibiotics for them.
Summary
The rational use of antimicrobial agents is crucial if the effective-
ness of antibiotics is to be maintained. Figure 1 illustrates an
example of an algorithm that could be used to aid antibiotic therapy
and highlights many of the key decision areas discussed. A
REFERENCES
1 Dancer SJ. How antibiotics can make us sick: the less obvious
adverse effects of antimicrobial chemotherapy. Lancet Infect Dis
2004; 4: 611e19.
2 Antimicrobial resistance and prescribing in England, Wales and
Northern Ireland. London, UK: Centre for Infections Health
Protection Agency. Also available at: http://www.hpa.org.uk/
web/HPAweb&HPAwebStandard/HPAweb_C/1216798080755;
2008.
3 Surveillance of surgical site infection in England. London, UK: Centre
for Infections Health Protection Agency. Also available at: http://www.
hpa.org.uk/webc/HPAwebFile/HPAweb_C/1194947340094; October
1997eSeptember 2005.
4 Engemann JJ, Carmeli Y, Cosgrove SE, et al. Adverse clinical and
economical outcomes attributable to methicillin resistance among
� 2009 Elsevier Ltd. All rights reserved.

INFECTION
patients with Staphylococcus aureus surgical site infection. Clin
Infect Dis 2003; 36: 592e8.
5 Barbut F, Petit JC. Epidemiology of Clostridium difficile-associated
infections. Clin Microbiol Infect 2001; 7: 405e10.
6 Goossens H, Ferech M, Stichele R, Elseviers M. Outpatient antibiotic
use in Europe and association with resistance: a cross-national
database study. Lancet 2005; 365: 579e87.
7 Mosdell DM, Morris DM, Voltura A, et al. Antibiotic treatment for
surgical peritonitis. Ann Surg 1991; 214: 543e9.
SURGERY 27:10 440
8 Caınzos M. Review of the guidelines for complicated skin and
soft tissue infections and intra-abdominal infections e
are they applicable today? Clin Microbiol Infect 2008;
14: 9e18.
9 Sevinc F, Prins JM, Koopmans RP, et al. Early switch from intravenous to
oral antibiotics: guidelines and implementation in a large teaching
hospital. JAC 1999; 43: 601e6.
10 MacDougall C, Polk RE. Antimicrobial stewardship programs in health
care systems. Clin Microbiol Rev 2005; 18: 638e56.
� 2009 Elsevier Ltd. All rights reserved.