Embed Size (px)
Citation preview

1
Antimicrobial Prophylaxis in
Digestive Surgery
Toar JM. Lalisang, MD, PhD
Digestive Surgery Division
Cipto Mangunkusumo Hospital
Medical Faculty Universitas Indonesia
Antibiotic must be present before bacteria is
introduced.
Given shortly before surgery
Miles and Burke
Laid the scientific basis for the use of prophylactic antibiotics in surgery
PGMEDICALWORLD.COM
Prophylaxis Antibiotic
Antimicrobial Prophylaxis
• The goal is to prevent SSI by reducing the burden of microorganisms at the surgical site during the operative procedure
• Antibiotic must be present before bacteria is introduced
• Patients who receive prophylactic antibiotics within one to two hours before the initial incision have lower rates of SSI than receive antibiotics sooner or later than this window
• Antimicrobial therapy administered in the setting of contaminated wounds is not considered prophylactic; in such cases a therapeutic course of antimicrobial therapy is warranted

2
Single dose sufficient
•Further dose waste of resources & more complication
•long surgeries- multiple doses
Antibiotic must be active against common expected
pathogens
Stop dosing when side effects outweigh benefits
Prophylactic Antibiotic cover – decisive period
•Body responds to a breach in defense after the decisive
period
•Decisive period last up to 4hrs
PGMEDICALWORLD.COM
Prophylaxis Antibiotic
Surgical Side Wound Infections(SSI)
• The second most common healthcare-associated infection
• Among surgical patients, SSIs are the most common nosocomial
infection, accounting for 38 percent of nosocomial infections
• It is estimated that SSIs develop in 2 to 5 percent of the more than 30
million patients undergoing surgical procedures each year
• The cost of SSIs is substantial
Pathophysiology
Whether a wound infection occurs after surgery depends on a complex interaction between the following:
1. Patient-related factors (e.g., host immunity, nutritional
status, the presence or absence of diabetes)
2. Procedure-related factors (e.g., implantation of foreign bodies, degree of trauma to the host tissues)
3. Microbial factors (tissue adherence and invasion)
4. Perioperative antimicrobial prophylaxis

3
General Principles
in the prevention of SSIs
• A number of interventions have been used over the years to reduce the risk
of SSIs, including :
Preoperative showering with antimicrobial soaps
Preoperative application of antiseptics to the skin of the patient
Washing and gloving of the surgeon's hands
Use of sterile drapes
Use of gowns and masks by operating room personnel
• The most important factors are meticulous operative techniques and
timely administration of effective preoperative antibiotics
Preventing SSI
Antibiotic prophylaxis
• Drugs- which when, how many doses?
Non antibiotic measures- evidence based
• Hair removal
• Normothermia
• Oxygen supplementation
• Normoglycemia
0
4
8
1 2
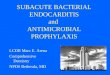
Alexander JW et al. Arch Surg. 1983;118:347–352.
Hair-Removal Techniques and SSIs
Infe
ction
, %
Discharge
30-Day Follow-up
5.2%
(14/271)
8.8%
(23/260)
6.4%
(17/266)
10%
(26/260)
4%
(10/250)
7.5%
(18/241)
1.8%
(4/226)
3.2%
(7/216)
PM AM PM AM
Razor Razor Clipper Clipper

4
Preoperative Strategies to Limit SSIs: Skin Surface Preparations
Antiseptic showers
– Reduced bacterial counts by 3.5 log10 from
baseline1
– No evidence that they affect SSIs2
• Skin preparation in the operating room (OR)
– Usually iodophors, alcohol-containing
products,
or chlorhexidine gluconate2
1. Seal LA et al. Am J Infect Control. 2004;32:57–62.
2. Mangram AJ et al. Am J Infect Control. 1999;27:97–134.
Perioperative Normothermia
• 200 CRS patients
– Control: Routine intraoperative thermal care
(mean temperature 34.7°C)
– Treatment: Active warming
(mean temperature 36.6°C)
• Incidence of SSI
– Control 19% (18/96)
– Treatment 6% (6/104); P=0.009
Kurz A et al. N Engl J Med. 1996;334:1209–1215.
Supplemental Oxygen
• 500 CRS patients
– 80% or 30% inspired oxygen during operation and for 2 hours post surgery
– All patients received prophylactic antibiotics
• Results
– Arterial and subcutaneous PO2 higher in
80% oxygen group
– Lower incidence of SSIs with higher supplemental oxygen (5.2% vs 11.2%; P=0.01)
Greif et al. N Engl J Med. 2000;342:161–167.

5
• 1,000 cardiothoracic surgery patients with preoperative hemoglobin A1c (HbA1c) levels measured
– 300 known diabetic patients
– 42 with undiagnosed diabetes
• Incidence of SSI
– Diabetes (known and undiagnosed) 5.8% (20/342)
– Without diabetes 1.5% (10/658)
– Diabetes with HbA1c ≥8% 7.9% (10/126)
– Diabetes with HbA1c <8% 4.0% (7/174)
Latham R et al. Infect Control Hosp Epidemiol. 2001;22:607–612.
SSIs and Glucose Levels (cont)
Latham R et al. Infect Control Hosp Epidemiol. 2001;22:607–612. Adapted with
permission from the University of Chicago Press © 2001.
SSIs and Post-op Glucose Levels
Glucose level
(mg/dL)
Infected patients
(n=72)
Noninfected
patients (n=902)
Odds
ratio
<200
(referrent) 35 (49%) 651 (72%) 1.00
200–249 21 (29%) 154 (17%) 2.54
250–299 11 (15%) 69 (8%) 2.97
≥300 5 (7%) 28 (3%) 3.32
SSIs and Glucose Levels
0
1
2
3
4
5
6
7
8
100–150 150–200 200–250 250–300
Day 1 Blood Glucose (mg/dL)
Deep
In
fecti
on
Rate
, %
Zerr KJ et al. Glucose control lowers the risk of wound infection in diabetics after open heart
operations, page 360. Reprinted from The Annals of Thoracic Surgeons, Vol. 63. Copyright
1997, with permission from the Society of Thoracic Surgeons. All rights reserved.
1.3% 1.6%
2.5%
6.7%
P=0.002

6
Antimicrobial Prophylaxis
Antimicrobial agent to prevent or reduce infection
Ideally
Targeted antibiotic
Narrow spectrum agent
Targeting few pathogens
Short term
Preoperative antibiotics are
warranted
if there is a high risk of infection or
if there is high risk of deleterious outcomes
should infection develop at the surgical site
(immune compromise, cardiac surgery,
and/or implantation of a foreign device)
Timing of prophylaxis
• Antimicrobial therapy should be administered within 60 minutes prior to the surgery to ensure adequate drug tissue levels at the time of initial incision
• This practice also reduces the likelihood of antibiotic-associated reactions at the time of induction of anesthesia
• If the 60 minute window for prophylaxis has past, administration of antimicrobial therapy 30 to 60 minutes prior to surgery appears to be more effective than administration immediately before surgery

7
Perioperative Prophylactic Antibiotics: Timing of Administration
Infe
ctio
ns, %
Hours From Incision
14/369
5/699
5/1,009
2/180
1/61
1/41
1/47
15/441
0
1
2
3
4
≤–3 >–2 >–1 0 1 2 3 4 ≥5
Classen DC et al. N Engl J Med. 1992;326:281–286. Copyright © 1992 Massachusetts Medical
Society. All rights reserved.
Repeat dosing
• Antibiotic concentration > MIC pathogen at the time of incision and throughout the procedure
• In general, repeat antimicrobial dosing following wound closure is not necessary and may increase antimicrobial resistance
• Repeat dosing is indicated every one to two half-lives of the drug in patients with normal renal function
for procedures lasting more than four hours
or in the setting of major blood loss

8
Prophylaxis Antibiotic Indication
• Clean wound with prostheses
• Clean Contaminated
Class I Wound (Clean)
• Atraumatic wound
without inflammation
• Do not enter GI, GU,
biliary, or respiratory
tract
• 1.5% infection rate
Class II Wound
(Clean-Contaminated)
• Respiratory, GI, GU,
or biliary tract entered
under controlled
conditions
• 7.5% infection rate
expected

9
Class III Wounds
(Contaminated) • Traumatic wounds
• Breaks in sterile technique
• Gross spillage from GI tract
• Acute, nonpurulent inflammation
• 15% anticipated infection rate
Class IV Wounds (Dirty)
• Old traumatic wounds
• Devitalized tissue
• Clinical infection
present
• Perforated viscus
• 40% expected
infection rate
SENIC Risk Index
• Abdominal operation
• Operation greater than
2 hours
• Class III or IV surgical
wounds
• Three or more
diagnosis at time of
discharge
Risk of Infection
0 1%
1 3.6%
2 9%
3 17%
4 27%

10
Classification SSI
Superfici
al
Dee
p
Digestive Surgery
• Among the highest risk procedures for SSI due to the presence of intraluminal bacteria
• The regimen should include activity against enteric gram-negative bacilli, anaerobes, and enterococci
• Bowel preparation consists of two components: mechanical bowel preparation and administration of antibiotics (ciprofloxacin plus metronidazole)
Oesophagogastric Surgery
Organisms encountered – Enterobacterium, Enterococci
Prophylactic regimen – Second generation cephalosporin & Metronidazole

11
Biliary Surgery
Organisms encountered
– Enterobacterium,
Enterococci
Prophylactic regimen –
One dose second
generation
cephalosporin
Small Bowel Surgery
Organisms encountered
– Enterobacterium,
Anaerobes
Prophylactic regimen –
Second generation
cephalosporin &
Metronidazole
Colorectal Surgery
Organisms encountered
– Enterobacterium,
Anaerobes
Prophylactic regimen –
Second generation
cephalosporin &
Metronidazole

12
0%
5%
10%
15%
20%
Infe
cti
on
s, %
Major Pathogens in SSI
NNIS Report. Am J Infect Control. 1996;24:380–388.
Surgical Prophylaxis
Wound
Classification
Antibiotic PCN Allergy
I 1st generation
Cephalosporin
Vancomycin Clindamycin
II-Biliary,GU, Upper
Digestive
1st generation
Cephalosporin
Vancomycin Clindamycin
II-Distal Digestive 2nd generation
Cephalosporin
Aztreonam and
Clindamycin/Flagyl
III/IV Generally Therapeutic
Pedoman Penggunaan Antibiotik
Departemen Ilmu Bedah
RSUPN-CM 2013

13
Digestive Division
Cipto Mangunkusumo Hospital 2012
• First Line
– Metronidazole
– Gentamycin
• Second Line
– Ampicillin-Sulbactam
– Cephalosporin third
Generation
– Carbapenem
Clean Contaminated
RSUPN-CM
MARCH 2013
• 67 Abdominal Operation
• 28 procedures used Prophylaxis Antibiotic
– LCC & Bilier operation = 15
– Incisional biopsy n debulking tumor = 5
– Elective Hernia repaired with mesh = 4
– Colostomy = 4
Prophylaxis Ab. : Genta + Metronidazol = 23 Cases
Cefazolin & Doripenem One case
SSI debulking tumor cases

14
Antibiotic Prophylaxis-Caveats
• You can’t kill everything
• Adverse drug effects
• Select resistant pathogens
• C diff colitis
• Select more virulent pathogens
• Avoid drugs/classes that are used for therapy
Surgical Prophylaxis Summary
• Its not the tool it’s the craftsman
• Is an adjunct to, not a substitute for, good surgical technique
• Decrease SSI
• Focus on likely pathogens-what are you cutting?
• Narrow spectrum, long half life drugs
• Single pre-op dose adequate for most
• Dose timing- pre-incision,
• Short Term better ( > 72 hours)
Thank You For Your Attention