Embed Size (px)
DESCRIPTION
The following bookchapter reviews all aspects and details of how we do our robotic radical prostatectomy (RARP). Have a look and let us know what you think
Citation preview

ROBOT ASSISTED RADICAL PROSTATECTOMY: STEP-BY-STEP SURGICAL TECHNIQUE
Roger F. Valdivieso O’Donova and Kevin C. Zorn MD, FACS, FRCSC University of Montreal Hospital Center (CHUM)- Hopital St. Luc Montréal, Québec, Canada
Abstract: Radical prostatectomy remains the standard treatment for long-term cure of clinically localized prostate cancer, offering excellent oncologic outcomes, with cancer-specific survival approaching 95% at 15 years after surgery. The introduction of the “da Vinci Robotic Surgical System” (Intuitive Surgical, Sunnyvale, CA) has been another important step toward a minimally invasive approach to radical prostatectomy. Technologic peculiarities, such as three-dimensional vision, wristed instrumentation with seven degrees of freedom of motion, lack of tremor, a 10x-magnification and a comfortable seated position for the surgeon has added value to the surgeon and patient. In this chapter, we describe the ten-step surgical technique for robot assisted radical prostatectomy that is currently used in our institution (University of Montreal Hospital Center (CHUM) – St-Luc’s Hospital). We use the four-arm da Vinci Si Surgical System. Our experience with RARP is now over 250 cases with the senior surgeon having performed over 1200 RARPs and we have continually refined our technique to improve patient outcomes.
INTRODUCTION
Radical prostatectomy remains the standard treatment for long-term cure of clinically localized prostate cancer, offering excellent oncologic outcomes, with cancer-specific survival approaching 95% at 15 years after surgery [1]. Retropubic radical prostatectomy (RRP), laparoscopic radical prostatectomy (LRP) and robot assisted radical prostatectomy (RARP) are safe options for treatment of patients with localized prostate cancer as they present similar overall complication rates [2]. Radical retropubic prostatectomy (RRP) has long been the most common surgical technique used to treat clinically localized prostate cancer (PCa). More recently, since 2004-2005, robot-assisted radical prostatectomy (RARP) has been gaining increasing acceptance among patients and urologists, and it has become the dominant technique in the United States despite a paucity of prospective studies or randomized trials supporting its superiority over RRP [2]. RARP has been associated with decreased operative blood loss and decreased risk of transfusion when compared with retropubic radical prostatectomy [3-5]. It has also been described that, with experienced robotic surgeons, RARP yields lower positive surgical margins (PSM) rates and higher continence and potency rates [6]. Since there are no randomized trials and long-term follow-up studies that compare the three approaches definitive conclusions cannot yet be drawn. Nevertheless, RARP has become the leading option for treating patients with clinically localized prostate cancer in the United States, and it has been progressively expanding in other countries [2]. Surgeon experience and institutional volume of procedures strongly predict better outcomes in all relevant domains. Moreover, RARP is feasible using either a transperitoneal or extraperitoneal approach. Most surgeons favor the transperitoneal access and approach over the extraperitoneal approach due to the greater working space and familiar landmarks of the pelvis and its contents. Although some studies have shown that an extraperitoneal approach yields shorter mean operative time, shorter time to full diet, shorter hospital stays and earlier return to continence [7] most studies have found little or no difference in operative time and perioperative outcomes between these two approaches [8-11]. It may nevertheless be preferable to use the extraperitoneal approach in patients with previous extensive abdominal surgery or the morbidly obese [12]. With the extraperitoneal approach, the peritoneum acts as a natural barrier, minimizing the potential for bowel injury and preventing the bowels from falling into the operative field and obscuring the surgeon's view. Furthermore, this approach helps to confine any urine leak that may occur from the vesicourethral anastamosis within the extraperitoneal space. One limitation with the extraperitoneal approach is the reduced working space as compared with the relatively larger working space of the peritoneal cavity gained with transperitoneal access. Extended pelvic lymphadenectomy may also be more challenging with the extraperitoneal approach. Lastly, a higher CO2 absorption has been reported with extraperitoneal versus transperitoneal insufflation, requiring a higher minute volume to compensate for hypercarbia and associated acidosis [13].
Overall, whether to use one approach or the other is largely a matter of surgeon and institution preference and experience and there is no consistently demonstrated advantage for either approach.

PREOPERATIVE PREPARATIONS
Other than a thorough medical clearance with history and physical examination for any cardiopulmonary comorbidities and previous abdominal surgery, there is no specific bowel preparation to undergo this procedure. Patients are requested to start a liquid diet beginning at noon the day prior to surgery followed by NPO starting midnight the day of the surgery. Approximately 6 weeks prior surgery, the main surgeon obtains informed consent during an outpatient consultation. During this meeting the advantages and the multiple risks are explained. We routinely provide our patients the AUA update summary of all possible complications that have been reported with contemporary radical prostatectomy [14]. In short, decreased sexual function, urinary incontinence, incisional hernias, adjacent organ injury, conversion to open surgery and the risks involved with general anesthesia. The procedure is also explained to the patient and the experience of the main surgeon is highlighted. Patients are advised to stop taking all anticoagulants a week before surgery. However, some emerging evidence suggests that allowing continued low-dose nonsteroidal anti-inflammatory drugs or aspirin associated with the occurrence of bleeding events and could be beneficial in preventing serious adverse cardiac thrombotic events [15]. Details of post-operative penile rehabilitation [16] and a pelvic floor rehabilitation program are provided prior to surgery to allow the patient to optimize post-operative function. Patients are also invited to watch informational videos created by the surgical team that are available on the Internet (http://www.youtube.com/user/drkevinzorn) for further information about the surgery. We have also offered our patients to see the 2-week post-operative diaries of the last 250 patients which is available on Facebook (https://www.facebook.com/pages/Robotic-Urology-Dr-Kevin-Zorn-Canada-Prostate-Center/111671516833) Finally, are encouraged to communicate any questions and/or concerns through e-mail with the main surgeon in order to optimize efficient care.
Surgical Team
The surgical team consists of the surgeon, surgical assistant (usually a trained urology resident), circulating nurse, scrub nurse, the anesthetist and respiratory therapist. Each member is knowledgeable in robotic assisted surgery and have been trained and credentialed as per our institutional robotic committee. All personel play a vital role to the proficiency of the surgical case.
Patient Positioning
Once the patient is under General Anesthesia, he is placed in Trandelenburg position at 20-25° and secured with the Allen’s Hug-u-vac steep trend positioner. This device is filled with soft microbeads that enable it to inflate and deflate evenly, when suction is applied. After positioning the patient, the device is deflated with a hand-held pump and its pliable shape conforms to the contours of the patient’s body preventing sliding. Arms are tucked in with foam rolls in the palms of the hands and ‘kidney’ shaped shoulder braces are carefully placed over the acromioclavicular joint to avoid brachial plexus injury. Sequential compression stockings are put in place over the thromboembolic (TED) stockings. The patient's legs are placed in padded boot stirrups in the low lithotomy position. An orogastric tube may be placed to decompress the intestinal system. A 20-Fr Foley catheter is installed in order to drain the bladder to ensure that it is completely decompressed and outside of the field of port placement. Only after these medical acts have been complete, the patient is positioned at an inclination of 20-25 degrees. It has been demonstrated that patients undergoing this procedure in a steep Trendenlenburg position for 3-4h do not present significant cerebrovascular, respiratory or hemodynamic problems [17]. Ultimately, the abdominal, genital and perineal area is scrubbed with Solu-IV (Chlorexidine based disinfectant clear solution) followed by sterile draping.
ANESTHESIA CONSIDERATIONS
Because of the possibility of severe hemorrhage, which in laparoscopic surgery can be difficult to control, discontinuation of anticoagulants and antiplatelet agents must be ensured at a safe preoperative interval. Even though bleeding is rarely significant enough to require a transfusion, typing and screening of blood is performed for every patient. Crossmatching for units of blood for cases is not routine practice. Any lines, monitors and patient protective devices are placed and secured before draping. Special care in regard to the endotracheal tube must be taken to avoid it from becoming kinked or pulled out. Once the robot is over the patient with its arms attached to the ports, the patient cannot be moved or cardiopulmonary resuscitative measures initiated unless the robot is first detached.

The use of pneumoperitoneum with the steep Trendenlenburg position is known to cause both respiratory and hemodynamic effects [14]. Among the respiratory effects there is a decreased functional residual capacity, decreased pulmonary compliance and increased peak airway pressures. This positioning also increases the workload of the heart and elevates the mean arterial pressure, central venous pressure and systemic vascular resistance. Patients for RARP require general endotracheal anesthesia with mechanically controlled ventilations. Any of the anesthetic drugs may be used dependent on the patient’s cardiovascular status and presence of other co-morbidities. In order to achieve optimal pneumoperitoneum complete muscle relaxation is essential. Other than the standard monitoring used in any general endotracheal anesthetic case, additional monitoring and/or intravenous fluid lines is dependent upon the patient’s medical condition and the experience of the operating team. Intraoperative intravenous fluids are kept to a minimum (<2000 mL) because excessive urine output might obscure the operative field during vesico-urethral anastomosis. Fluid restriction might also minimize the facial, pharyngeal, and laryngeal edema that may occur from prolonged use of steep Trendenlenburg position. Upon induction, 5000 units of Heparin are given subcutaneously and a first generation cephalosporin (Ancef) 1g IV is used as prophylaxis. Patients are also administered 10 mg of an Opium analgesic (Supeudol) suppository as it has been documented that it reduces catheter related bladder spasms as well as the overall consumption of narcotics in the post-operative first 24 hours [18].
THE SURGICAL PROCEDURE
1) Port Placement and Robot Docking
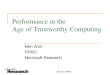
A Standard 6-port placement configuration is drawn on the patient’s abdomen prior to skin incisions. Pneumoperitoneum is established using a Verress needle through a 12mm sub-umbilical incision. An intraperitoneal pressure of 20mmHg is then achieved after which a 12-mm trocar is placed for insertion of the stereo endoscope. After pneumoperitoneum is established, primary inspection of the intraperitoneal cavity is performed to ensure that no injuries to the bowel or adjacent organs have occurred. Secondary trocars are then placed using laparoscopic guidance to avoid injuring main arteries of the abdominal wall (see Figure 1). Overall, three 8-mm metallic robotic trocars are used by the working robotic arms of the surgeon while the assistant provides retraction, suction, and irrigation and passes clips and sutures via the 12-mm and 5-mm trocars placed along the patient's right side. Finally, a total of 20ml of Marcaine is injected in all trocar incisions for post-operative anesthesia. A smoke evacuator is also used during the procedure to optimize vision.
Figure 1: Standard six-port placement for Robot Assisted Radical Prostatectomy. Two 12mm, three 8mm and one 5mm trocar are placed in the standard way providing sufficient distance between the camera and working ports to prevent internal or

external collision of instruments.
Robot Docking
The patient cart is maneuvered into position to align the patient cart tower, camera arm and target anatomy. One member of the surgical team maneuvers the patient cart while another one guides the driver. Room references are used to avoid any confusion during docking. The cart is pushed into position and the brakes at the base of the cart are hand tightened. The camera arm is the first one connected to the patient and the instrument arms follow. Once all the robotic arms are connected, the surgical team checks each arm for proper working distance and makes sure the arms are not compressing the patient. The forth arm is docked on the right side of the patient while the bed-side assistant is situated on the patient’s left side.
2) Posterior Dissection
The surgical procedure begins with the posterior dissection of seminal vesicles and vas deferens. In our experience, starting with the posterior dissection has several advantages. It improves the working space as the prostate is still suspended anteriorly by intact puboprostatic ligaments. This provides better visualization of the structures to be dissected and consequently the amount of traction and thermal energy used in the dissection is limited. It provides a safer and more reliable posterior bladder neck transection later in the procedure. Moreover, when the surgeon has to transect through the bladder to liberate the prostate, an already dissected posterior plane is easily found. This is particularly advantageous in cases of large prostates, large median lobes, patients that had previous surgery at the bladder neck such as TURP or laser surgery at the prostate, as well for those patients whom have received previous radiotherapy. This initial step also serves for teaching of residents and fellows. Finally, starting with the posterior dissection serves as a warm up for more difficult steps later in the procedure. Once docking is complete and the pneumoperitoneum is decreased to 14mmHg, the initial surgical step begins with direct visualization of the peritoneum overlying the bladder. The assistant is asked to provide upper anterior traction on the peritoneum using the Xomed Microfrance graspers. A curvilinear incision for access is made midway between the level of the Foley catheter impression and the anterior rectus wall. Monopolar scissors are used for incision of the peritoneum. Bipolar graspers are then used to dissect through and divide fibrovascular tissue to the desired plane (See Figure 2). Monopolar cautery is concomitantly used for division of all tissue between the bipolars from the left to right direction. Through the dissection of the retroprostatic tissue, the vas deferens and accompanying arteries are exposed.

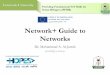
Figure 2: Posterior Dissection. A: With the bedside assistant providing anterior upper traction on the peritoneum using the Xomed Microfrance graspers and posterior downward traction using the suction tip, access through the peritoneum is granted and the vas deferens and seminal vesicles are exposed. B: Both the seminal vesicles and transected vas deferens are liberated.
Division of Vas Deferens:
The vas deferens are then divided bilaterally with bipolar control of both arteries. The monopolar scissor blade is used as a spatula to free adjoining vessels. Caution should be made not to injure or coagulate the vas deferens as doing so may increase the risk of tearing when the assistant lifts it for exposure of the seminal vesicle. This is done approximately 5 cm from the level of the prostate.
Exposure of the Seminal Vesicles:
For this part of the procedure the assistant is asked to provide upper traction of the vas deferens and downward traction with the suction tip to expose the tip of the seminal vesicle. Blunt dissection of the fibrovascular tissue overlying the surface of the seminal vesicles exposes the postero-medial surface of the seminal vesicle. Then, the lateral surface of the organ is mobilized using, again, blunt dissection. The seminal vesicle is then grasped by the bipolar instrument to help liberate the posterior avascular plane. Meticulous blunt dissection is continued to allow complete liberation of the seminal vesicle. The same steps are done on the contralateral organ. Deep posterior dissection is then continued to the level of Denonvillier’s fascia. This fascia layer will be incised later in the procedure. One of the most important aspects of posterior-first dissection is the anterior dissection to the level of the prostate of both vas deferens. This allows a safe entry into the retro-prostatic dissection during posterior bladder neck dissection. Prior to Retzius space dissection and dropping of the bladder assurance of hemostasis is made.
3) Retzius Space Dissection And Endopelvic Fascia Dissection
The umbilical ligaments and urachus are initially divided with the bipolar graspers. The forth arm Prograsp is used to provide traction. Care is made to achieve good hemostasis since occasionally these structures have patent vessels. The bladder is then liberated off the anterior surface of the abdominal wall. The avascular plane found is further blunt dissected to the pubic bone and the bladder is placed on stretch (See Figure 3). The lateral attachments to the vas deferens are liberated as well.
Figure 3: Retzius Space Dissection. After diving the umbilical ligaments and urachus the anterior surface of the bladder is

liberated off the anterior surface of the abdominal wall. It is usually an avascular plane however patent vessels can be found and good hemostasis is to be achieved. This flimsy tissue is bluntly dissected to the pubic bone.
Anterior prostatic fat (AFP) dissection:
Resting on top of the anterior wall of the prostate a layer of fat is identified. Removing this layer of fat will allow better visualization of the puboprostatic ligaments, the dorsal venous complex as well as the junction between the bladder neck and the prostate (See Figure 4). Also, Alhering et al. showed that lymph nodes are found in this tissue in 11% of patients. They found that the removal of the APF and its pathologic analysis can result in pathologic upstaging [19]. Consequently, this ‘flap’ of fat is dissected in a cephalad direction up to the junction of the bladder. It is then further dissected laterally towards the lateral pelvic sidewall. At this point the anterior surface of the prostate is seen. Thereafter, all the tissues lying on top of the prostate are dissected to demonstrate the pubo-prostatic ligaments as well as the dorsal venous complex (DVC). Lateral dissection of the bladder is carried out down toward the crossing of the median umbilical ligament and vas deferens in order to ensure optimal mobility of the bladder and to minimize future tension at the vesicourethral anastomosis. Accessory pudendal arteries traveling longitudinally along the anteromedial aspect of the prostate are easily recognized during RARP. Attempt at preservation of these arteries is important for erectile function because in some men these arteries may be the dominant source of arterial blood supply to the corpora cavernosa.
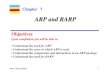
Figure 4: Anterior Prostatic Fat Dissection. A: Anterior Prostatic Fat (APF) overlying the dorsal venous complex, the anterior surface of the prostate and the prostato-vesical junction. B: En bloc dissection of the APF extended cephalad to the prostato-vesical junction and laterally toward the lateral pelvic sidewall. C: Anterior prostatic surface exposed after APF dissection.

4) Dorsal Vein Complex (DVC) Ligation The dorsal venous complex is usually responsible for significant blood loss during open surgery [20]. With the benefits of articulated instrumentation and the tamponade effect offered by the pneumoperitoneum control of important venous bleeding is achieved. The average blood loss in our institution is 200ml through RARP versus 800-1000ml during open surgery. A total of 2 suture ligations are made (one distal and another more proximal) (See Figure 5). The proximal suture will be used later for prostate traction whereas the first one provides the needed hemostasis. The suture used (Vicryl 1-0 polyglactin 910 with a CTX needle) is passed beneath the DVC and anterior to the urethra as close to the pubis and as far from the prostatic apex as possible. Securing the DVC as far away from the prostatic apex as possible can help minimize iatrogenic entry into the prostatic apex during later division of the DVC [21]. Using a square knot technique, sufficient tension of the suture is achieved to assure all the veins of the complex are controlled. A total of four knots are used. The assistant’s scissors are then introduced and used to cut the sutures. It is important to avoid damage to the anterior urethral sphincter muscle from placing the sutures. As such, a sufficient apical dissection is necessary to obtain visualization of the notch between rhabdosphincter, prostate and urethra.
Figure 5: Dorsal Venous Complex Ligation. A: Distal ligation of the Dorsal Venous Complex (DVC) using a Vicryl 1-0 suture. The suture is passed beneath the DVC and anterior to the urethra as far from the prostatic apex as possible. B: Proximal ligation of the DVC. This suture is placed to allow cephalad traction while transecting the DVC later in the procedure.
5) Bladder Neck Transection
Compared to conventional open surgery, robotic bladder neck transection is one of the most difficult aspects to acquire during a surgeon’s learning curve. Prior to incision, the robotic instruments are use to define the junction between the prostate and the bladder. Different maneuvers have been described to determine the right plane of dissection:
• Visual identification of the point of transition of the pre-vesical fat to the anterior prostate can serve as a guide.
• Intermittent and repetitive caudal retraction of the urethral catheter balloon can help identify and confirm the transition between bladder neck and prostate.
• Using a forceps to grasp and retract the dome of the bladder in a cephalad direction results in “tenting” of the bladder neck at its attachment to the prostate.

• Bimanual “palpation” or “pinch” of the bladder neck using the tips of two robotic or laparoscopic instruments.
Once the proper plane of dissection is identified, the bladder neck is divided horizontally with monopolar cauterization until the urethral catheter is identified. The anterior bladder neck incision should not be carried too laterally because branches of the dorsal vein fanning over the prostate are often encountered, resulting in unwanted bleeding. These will be controlled by Hemolock clips. The Foley catheter balloon is then deflated. With the help of the bedside assistant who is asked to create counter traction externally on the penile meatus Foley catheter, the prostate is suspended anteriorly towards the abdominal wall by grasping the tip of the catheter and lifting upwards. A visual plane is then carefully created to assure proper dissection in the correct space and not to dissect into the prostate or worse, towards the bladder trigone and ureteral orifices. At this point, an inspection of the posterior bladder neck is made in order to identify the ureteral orifices and also to look for a large median lobe. In the case that a large median lobe is found, further exposure is required to visualize behind the protruding median lobe and identify the posterior bladder neck. This is achieved by lifting it anteriorly using the ‘Prograsp’ forceps or, in our experience, to avoid unnecessary mucosal oozing, the use of suture suspension. We usually use a single 15cm 3-0 VLoc suture with several passes through the median lobe. The Microfrance grasper by the assistant lifts upwards on the suture rather than the Foley catheter. With upper traction with one hand by the assistant and downward traction at the level of the bladder neck with the suction tip, the posterior detrusor fibers as well as the mucosa are taken down from the left to right direction between the jaws of the bipolar, diamond-tipped graspers (See Figure 6). This way, the retrotrigonal fascia is exposed and it is then sharply popped through with the instruments. This will then expose the previously dissected vas deferens that lie in the midline. These structures, along with the seminal vesicles are collectively grasped, pulled through the open bladder neck and handed to the assistant for upper traction to initiate prostate pedicle control as well as neurovascular bundle dissection.
In case of a prior TURP, the bladder neck margin is less evident and often distorted as a result of prior resection and scarring. Careful inspection is made of the posterior bladder neck paying specific attention to the location of the ureteral orifices because they are often found close to the posterior bladder neck margin. If there is any doubt, the anesthesiology team is asked to administer intravenous indigo carmine to identify the orifices for their protection.
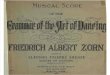
Figure 6: Bladder Neck Transection. A: The anterior bladder neck is incised and the prostate is suspended anteriorly toward the abdominal wall by the assistant’s grasper. At this point the bedside assistant also provides counter traction externally on the penile meatus Foley catheter. B: After having inspected the posterior bladder neck the assistant is asked to provide posterior traction with the suction tip at the level of the bladder neck. The posterior detrusor fibers and the bladder mucosa are then incised.

6) Athermal Sexual Nerve Sparing Technique and Vascular Pedicle Control
This aspect of RARP is of paramount importance to preserve sexual function. Other critical areas where attention is required is during the apical seminal vesical dissection as well as the urethral transection to avoid injury to the plexus and nerve fibres. It is important for the surgeon to use an athermal technique near the nerve bundles and limit the amount of stretch, which may cause traction nerve injury [2]. Dissection of the pedicle is performed using the diamond tipped bipolar instrument to isolate the pedicle of tissue to be clipped by the assistant. A medium 10mm Weck Hem-o-lok clip is introduced by the bedside assistant, which allows for proximal control. When presented with large veins, a back-lid clip can also be applied to limit amount of oozing during surgery. Once the clips have been placed, sharp scissor cutting between them helps liberate the tissue. Proper communication between the surgeon and assistant, experience and proper exposure and presentation of the tissue to be clipped is essential. Alternatively, individual vessel titanium clip ligation can be performed however in our experience not recommended due to the high likelihood for clip migration and slippage. This technique requires meticulous dissection of specifically those vessels to be cut and only placing a clip on the stay side that will remain inside the body.
NVB Preservation:
In well selected patients with low volume and low risk disease for extracapsular extension, an interfascial nerve preservation technique is used. We have previously published on our tailored technique for ipsilateral nerve sparing to minimize the risk of positive surgical margins [22, 23]. Herein, we describe an interfascial dissection. Use of the Memorial Sloan-Kettering Cancer Center nomogram developed by Dr. Kattan et al (available online at ttp://nomograms.mskcc.org/Prostate/PreTreatment.aspx) is also helpful in patient counseling for nerve preservation. After releasing the prostate from its vascular pedicles and completing the posterior plane dissection after dissecting through Denonvilliers fascia to the prostate apex, the avascular plane is followed laterally along the prostatic capsule. Meticulous care is made not to injure or violate this capsule. The back end of the monopolar scissor is used with small stroking motions to liberate the tissues. Any perforating vessel can be cut sharply and if needed, short use of the single blade of the open monopolar scissors can be used to achieve hemostasis. Aggressive hard use of the instruments could potentially lead to a positive surgical margin (PSM), which increases patient risk for disease recurrence. Gentle dissection can be carried along this plane from the base to the apex of the gland (anterograde). The apex of the gland is a challenging area to release due to the circular contour of the prostate. As such, surgical experience and technique are required for optimal and safe nerve release. Recently, a study by Patel et al, observed that a retrograde nerve sparing approach with early apical release facilitates early recovery of potency and continence compared with an antegrade approach without compromising the margin status in patients with normal preoperative erectile function and full nerve preservation. Furthermore, they found that retrograde nerve sparing technique leads to less blood loss intraoperatively [24].
7) Non-nerve Sparing Technique
Occasionally, due to cancer related factors (Gleason score, PSA, digital rectal exam, clinical stage, number and percentage of biopsy cores), the surgeon may perform a wider resection away from the prostate capsule due to a high likelihood of extracapsular disease. This is done in order to reduce the risk of positive surgical margins (PSM). As mentioned previously, we routinely use the Kattan Memorial Sloan Kettering prostate cancer nomogram to counsel our patient's risk of extracapsular disease (http://www.mskcc.org/applications/nomograms/prostate/) In order to efficiently seal tissue and vessels of the prostate pedicle, use of wider placed Hemolock clips or vessel-sealing devices such as the EnSeal (Ethicon Endosurgery, Cincinatti, OH) is preferred to assure hemostasis and maintain tissue integrity. Initially in our experience bipolar cautery was used to coagulate the tissue prior to scissor division. The tremendous amount of black burnt tissue occurred with bipolar cautery. Many surgeons still use this technique for wide resection. Care must always we made especially along the apex of the gland not to injure or enter into the rectum. Although few data are available in the literature regarding RARP for unilateral nerve-sparing techniques, a recent consensus panel believed that these techniques can be considered for patients with unilateral extraprostatic disease. In such cases, partial preservation of the neurovascular bundles limited to the side with organ-confined disease or no disease may be indicated [2].

8) Urethral Division and Specimen Liberation
One of the last remaining anchoring tissues that hold the prostate in place is via the urethra. At this time, the Foley catheter is replaced and the surgeon’s instruments are used to divide the apex of the prostate. Meticulous care must be made not to cut into the prostate and cause a positive margin. On the other hand, cutting the urethra too far away would injure the sphincter which and this will have an impact on urinary control. Care must also be made at this time to avoid injury to the neurovascular bundles that were preserved earlier. Additionally, care must be made to avoid cutting the DVC suture. Initially, the 4th arm is used to grasp the backbleed Vicryl suture that was previously placed along with the DVC suture and place cephalad traction. The bipolar instrument is then placed beneath the DVC alongside the prostatic capsule. Monopolar scissors are used to divide through the tissue between the opened blades of the bipolar (See Figure 7). Once the DVC has been transected, attention is then drawn to urethral division. If the DVC suture looses tension or slips off, use of the 3-0 15cm VLOC suture is used to oversew the loose DVC stump. The urethra is then skeletonized to delineate the end of the prostate and the released neurovascular bundles. Sharp scissor cutting through the anterior urethral wall allows for visualization of the Foley catheter, which is then withdrawn to expose its tip. The remaining posterior wall including the rectourethralis fibres are then cut sharply to liberate the prostate (See Figure 8). At this point the apex of the free prostate is inspected. The prostate is placed in an endo-catch bag for later retrieval after the vesico-urethral anastamosis. The bag is closed and the specimen, including the anterior prostatic fat is placed in the upper abdominal space for later retrieval.
Figure 7: Dorsal Venous Complex (DVC) Transection. The fourth arm grasper provides cephalad traction on the backbleed Vicryl suture that was placed proximally while the monopolar scissors divide the DVC.

Figure 8: Urethral transection. Once the dorsal venous complex has been divided the urethra is skeletonized to delineate the end of the prostate and the released neurovascular bundles. The anterior urethral wall is then transected until visualization of the Foley catheter.
9) Continuous Vesico-Urethral Anastamosis (VUA) Using VLOC Sutures [25]:
With the removal of the prostate there is a fossa defect between the bladder and the urethra. Hemostasis is first verified along with removal of all clots and blood in the field. The well-dissected bladder is free and mobile and can be easily descended into the pelvis. The anastamosis is done using a self-cinching unidirectional barbed suture (2 knotless, interlocked 6-inches 3-0 V-Loc-180 suture) as previously described [26]. The sutures could be easily interlocked via their tail loops by the scrub nurse which takes less than a minute to prepare. The bedside assistant then introduces the interlocked sutures to the surgeon’s robotic needle drivers.
Posterior Reconstruction
Posterior reconstruction helps create a posterior plate in which to buffer the anastamosis and reduce bleeding (See Figure 9). Several studies have shown that a proper posterior reconstruction could help promote earlier return to pad-free continence [27, 28] and most important, reduce urinary leaks. The bladder is brought down into the pelvis to allow for reconstruction. The left sided VLOC suture is anchored at the 5 o’clock position of the bladder neck. The cut Denonvillier’s fascia and the detrusor muscle are grasped and passed through with the needle without entering the bladder. This space is denominated as the retrotrigonal area. The suture slack is held and pulled upward using a ‘hand over hand’ technique until the part the sutures interlock are within the bladder muscle. The needle is then positioned towards the urethra and the assistant introduces the Foley catheter tip. This way the surgeon is sure to grab only the posterior cut Denonvilliers fascia. The needle is then passed through the posterior side of the urethra (the periurethral rectourethralis muscle) at the same 5 o’clock position. The suture is pulled through until the interlocked loops abut with the tissue providing resistance, as a knot would. Once the expected tension is achieved the suture can be released expecting no back cinching due to the properties of the sutures. A second bite is then taken from the midline retrotrigonal area behind the bladder followed by a 6 o’clock bite of the periurethral tissue. Special care is made to ensure there is no cephalad traction on the bladder prior to cinching. Finally, a final 7 o’clock suture is taken on the bladder-side retrotrigonal tissue again ensuring not to include any mucosa. The left arm of the interlocked V-Loc suture is then lifted cephalad and anteriorly with the left needle driver, while the open right needle driver sat on the bladder tissue to serve as a fulcrum point to avoid tissue tearing. The bladder is thus cinched down with repetitive, short pulls until the bladder neck mucosa is adjacent to the urethral stump with no gap. This provides for unprecedented hold of auto-tissue tension and allows the urethral stump to be retracted from the pelvic floor to provide increased length.

Figure 9: Posterior Reconstruction. A: The VLOC suture is passed through the bladder-side retrotrigonal area at the 5, 6 and 7 o’clock position and through the periurethral rectourethralis muscle. B: Traction is used on the VLOC suture to cinch down the bladder until its mucosa is adjacent to the urethral stump and no gap is left.
Vesico-urethral Anastamosis (See Figure 10)
The same left arm of the interlocked suture is used to begin the vesico-urethral anastamosis. An initial transmural inside-out bite of the bladder is made at the 6 o’clock position, followed by a bite of the posterior urethra. Depending on the size of the bladder neck the surgeon may take larger tissue bites to parachute down for the bladder neck – urethral stump discrepancy. The urethra is usually the size of a pen and the bladder neck could be anywhere from the size of a pen to the size of a nickel or a quarter. Other techniques of tapering down the bladder neck include:
• Figure of eight sutures at 3 and 9 o’clock positions to taper the bladder neck using 3-0 Monocryl (Ethicon Endo Surgery, Cincinnati, OH).
• An anterior or posterior tennis racket suture. This depends on surgeon’s preference and experience. The assistant reintroduces the tip of the Foley catheter to ensure the grasp of the correct tissues. The ‘outside-in’ bites along the bladder and the inside-out urethral bites are continued from 6- to 10-o’clock, each time cinching the tissue with the right needle driver straddling the suture to avoid urethral tearing. Rather than completing the left side of the VUA and obscuring the posterior anastamosis, the right arm of the V-LOC stitch is used to complete a synchronous process starting from an outside-in 5- o’clock bladder bite to a 5-o’clock ‘inside-out’ urethral throw. Care is made not to incorporate the neurovascular bundles or rhabdosphincter muscle with aggressive bites. Repetitious passes were continued for the entire right side 5- to 12-o’clock with final pass, each time, independently assuring adequate tension. The right arm is finally brought through the anterior urethral side and cut with a 2 to 3 cm stump. The left wall is then completed in a running fashion from the 10- to 12-o’clock location again finishing on the anterior urethra. Prior to cutting the left arm V-Loc suture, the integrity of the VUA is verified with 300 cc normal saline instilled in the bladder (See Figure 11). If any leakage were seen, further cinching of the suture or placement of additional V-Loc bites would be required. The needles can be snapped out and removed from the body by the assistant. The two cut-ends are left untied thus allowing for a completely, knot-free reconstruction.

Figure 10: Overview of Posterior Reconstruction (PR) and Vesico-Urethral Anastamosis (VUA) using V-LOC sutures. A: Interlocked V-LOC configuration for PR and VUA. Note the use of two six-inch sutures in which the loops of both sutures are threaded by the opposite needles. B: The left-arm of the hybrid suture is passed initially at the 5-o’clock position of the retrotrigonal tissue. The suture is pulled through until the inter-twined loops oppose the tissue providing resistance. (red asterix) Using three consecutive bites, the PR helps approximate the edge of the bladder neck to the peri-urethral tissue. C: The left arm of the suture is then passed trans-murally through the 6-o’clock bladder neck and used to initiate a standard Van Velthoven anastamosis. The right arm is then used to close the right-sided VUA. D: A visual cystogram with 300 cc of normal saline is performed to ensure no leakage.
Figure 11 : Vesico urethral Anastamosis (VUA). A: The left arm of the VLOC suture is used to start the Van Velthoven anastamosis. The right arm of the VLOC suture is then used to close the right-sided VUA. B: A visual cystogram with 300cc of saline is performed to ensure the integrity of the VUA and thus the absence of saline leakage.
10) Case Completion and Post-operative Considerations Prior to undocking the robot and removal of the specimens, the pelvis and operative field are carefully reinspected for bleeding under low insufflation pressure (<10 mm Hg). The bowel is equally examined closely to make certain that there is no injury resulting from instrument exchanges. Then, the string for the laparoscopic entrapment sack is transferred to the camera port site at the umbilicus and the abdomen is completely deflated. The specimens within the laparoscopic entrapment sack are extracted intact through extension of the periumbilical trocar site (usually 2.5 to 3.5cm in lenght. The fascial defect is then immediately closed by a 0-Vicryl suture. The skin defects are then closed with a subcuticular absorbable suture (4-0 Monocryl) followed by the skin adhesive Dermabond (Ethicon, Cincinatti, OH). Closure of the fascial defect for the 5mm and 12mm trocar sites are not necessary. Once extubated, the patient is then transferred to the recovery room where vital signs, in/outs are taken as usual for post-op patients. Regular diet is offered the evening of the surgery and patients are mobilized out of bed within hours

of surgery. For pain control all patients are given NSAIDs (Toradol) 30mg IV q6h along with regular Acetaminophen (Tylenol) 650 mg PO q6h. Narcotics are only administered in the event of severe pain. Upon discharge, patients are provided with a script of Codeine if needed with instructions on the regular use of NSAIDs (Motrin) 400mg q12h along with Acetaminophen (Tylenol) 650 q12h for 5-7 days. On the first post-operative day, the nursing team helps the patient out of bed and encourages mobilization. Early mobilization has been well documented to reduce risks of ileus, atelecetasis and thrombosis. Following surgery, patients are advised to avoid heavy lifting of anything over 20-30lbs for the next 3-4 weeks to reduce the risk of developing an incisional hernia. Thereafter, patients can resume all preoperative physical activities. Patients are advised to make regular use of oral PDE5-inhibitors (Sildenafil) as it has been suggested that their administration soon after radical prostatectomy exerts an anti-fibrotic effect in the corpora cavernosa and it helps preserve erectile tissue integrity. Therefore, their use leads to an earlier recovery of erectile function [29]. Patients are also encouraged to continue the pelvic floor muscles (PFM) reinforcement exercise program (Kegel exercises) that they had been suggested to start before the surgery. In this exercise program, patients are asked to isolate and correctly contract the PFM to increase strength and endurance. Repeated contractions are thought to improve urinary control trough increased support for the detrusor muscle and urethral sphincter [30]. Studies suggest that doing such rehabilitation program exercises on a daily basis hastens the return to urinary continence after surgery thus improving the quality of life of patients [31]. Finally, over 95% of our patients are discharged within 24 h of surgery with planned removal of the Foley catheter on post-operative day 4.. Patients are educated on how to take care of the catheter and it is left in place to a leg-bag upon discharge. A trained nurse then removes the catheter during an outpatient appointment. Upon discharge, patients are advised to avoid any aspirin-like medication for at least a week after surgery since an NSAID (Motrin) is being used regularly. They are also explained that light pink urine is typical for a week following the procedure and they are not be alarmed by it. They are told to expect a smaller bladder capacity for several weeks after surgery due to the dissection around the bladder and they may experience an increase in urinary frequency and some urinary urgency. An initial follow-up visit is scheduled 4-6 weeks after surgery to review recovery and the final surgical pathology. Serum PSA is obtained at 3, 6 and 12 months following RARP with subsequent serum assessments depending on the pathological stage, grade and margin status.

REFERENCES
1. Liss, M., K. Osann, and D. Ornstein, Positive surgical margins during robotic radical prostatectomy: a contemporary analysis of risk factors. BJU Int, 2008. 102(5): p. 603-8.
2. Montorsi, F., et al., Best Practices in Robot-assisted Radical Prostatectomy: Recommendations of the Pasadena Consensus Panel. Eur Urol, 2012.
3. Ficarra, V., et al., Retropubic, laparoscopic, and robot-assisted radical prostatectomy: a systematic review and cumulative analysis of comparative studies. Eur Urol, 2009. 55(5): p. 1037-63.
4. Boorjian, S.A., et al., A critical analysis of the long-term impact of radical prostatectomy on cancer control and function outcomes. Eur Urol, 2012. 61(4): p. 664-75.
5. Budaus, L., et al., Impact of surgical experience on in-hospital complication rates in patients undergoing minimally invasive prostatectomy: a population-based study. Ann Surg Oncol, 2011. 18(3): p. 839-47.
6. Coelho, R.F., et al., Retropubic, laparoscopic, and robot-assisted radical prostatectomy: a critical review of outcomes reported by high-volume centers. J Endourol, 2010. 24(12): p. 2003-15.
7. Eden, C.G., et al., Transperitoneal or extraperitoneal laparoscopic radical prostatectomy: does the approach matter? J Urol, 2004. 172(6 Pt 1): p. 2218-23.
8. Cathelineau, X., et al., Transperitoneal or extraperitoneal approach for laparoscopic radical prostatectomy: a false debate over a real challenge. J Urol, 2004. 171(2 Pt 1): p. 714-6.
9. Erdogru, T., et al., Comparison of transperitoneal and extraperitoneal laparoscopic radical prostatectomy using match-pair analysis. Eur Urol, 2004. 46(3): p. 312-9; discussion 320.
10. Atug, F., et al., Transperitoneal versus extraperitoneal robotic-assisted radical prostatectomy: is one better than the other? Urology, 2006. 68(5): p. 1077-81.
11. Brown, J.A., et al., Transperitoneal versus extraperitoneal approach to laparoscopic radical prostatectomy: an assessment of 156 cases. Urology, 2005. 65(2): p. 320-4.
12. Atug, F. and R. Thomas, Transperitoneal versus extraperitoneal robotic-assisted radical prostatectomy: which one? Minerva Urol Nefrol, 2007. 59(2): p. 143-7.
13. Meininger, D., et al., Prolonged intraperitoneal versus extraperitoneal insufflation of carbon dioxide in patients undergoing totally endoscopic robot-assisted radical prostatectomy. Surg Endosc, 2004. 18(5): p. 829-33.
14. DeCastro GJ, G.G., Zorn KC., Complications of Contemporary Radical Prostatectomy. AUA Update Series, 2010. 29(Lesson 2): p. 9-19.
15. Mantz, J., et al., Impact of preoperative maintenance or interruption of aspirin on thrombotic and bleeding events after elective non-cardiac surgery: the multicentre, randomized, blinded, placebo-controlled, STRATAGEM trial. Br J Anaesth, 2011. 107(6): p. 899-910.
16. Blaya R, M.J., Penile Rehabilitation after Radical Prostatectomy. AUA Update Series, 2008. 27(Lesson 36): p. 346-351. 17. Park, E.Y., et al., The effect of pneumoperitoneum in the steep Trendelenburg position on cerebral oxygenation. Acta
Anaesthesiol Scand, 2009. 53(7): p. 895-9. 18. Lukasewycz, S., et al., Does a perioperative belladonna and opium suppository improve postoperative pain following
robotic assisted laparoscopic radical prostatectomy? Results of a single institution randomized study. Can J Urol, 2010. 17(5): p. 5377-82.
19. Finley, D.S., et al., Anatomic excision of anterior prostatic fat at radical prostatectomy: implications for pathologic upstaging. Urology, 2007. 70(5): p. 1000-3.
20. Tufek, I., et al., The Use of Laparoscopic Bulldog Clamp to Control the Dorsal Vein Complex during Robot Assisted Radical Prostatectomy: A Novel Technique. J Endourol, 2012.
21. Talug, C., et al., Controlling the dorsal venous complex during robotic prostatectomy. Can J Urol, 2012. 19(1): p. 6147-54.
22. Zorn, K.C., et al., Planned nerve preservation to reduce positive surgical margins during robot-assisted laparoscopic radical prostatectomy. J Endourol, 2008. 22(6): p. 1303-9.
23. Schatloff, O., et al., Cavernosal nerve preservation during robot-assisted radical prostatectomy is a graded rather than an all-or-none phenomenon: objective demonstration by assessment of residual nerve tissue on surgical specimens. Urology, 2012. 79(3): p. 596-600.
24. Patel, V.R., et al., The role of the prostatic vasculature as a landmark for nerve sparing during robot-assisted radical prostatectomy. Eur Urol, 2012. 61(3): p. 571-6.
25. Zorn, K.C., et al., Novel method of knotless vesicourethral anastomosis during robot-assisted radical prostatectomy: feasibility study and early outcomes in 30 patients using the interlocked barbed unidirectional V-LOC180 suture. Can Urol Assoc J, 2011. 5(3): p. 188-94.
26. Zorn, K.C., et al., Prospective randomized trial of barbed polyglyconate suture to facilitate vesico-urethral anastomosis during robot-assisted radical prostatectomy: time reduction and cost benefit. BJU Int, 2012. 109(10): p. 1526-32.
27. Rocco, F., et al., Restoration of posterior aspect of rhabdosphincter shortens continence time after radical retropubic prostatectomy. J Urol, 2006. 175(6): p. 2201-6.
28. Gautam, G., et al., Posterior rhabdosphincter reconstruction during robot-assisted radical prostatectomy: critical analysis of techniques and outcomes. Urology, 2010. 76(3): p. 734-41.

29. Iacono, F., et al., Histopathologically proven prevention of post-prostatectomy cavernosal fibrosis with sildenafil. Urol Int, 2008. 80(3): p. 249-52.
30. Bo, K., Pelvic floor muscle training is effective in treatment of female stress urinary incontinence, but how does it work? Int Urogynecol J Pelvic Floor Dysfunct, 2004. 15(2): p. 76-84.
31. MacDonald, R., et al., Pelvic floor muscle training to improve urinary incontinence after radical prostatectomy: a systematic review of effectiveness. BJU Int, 2007. 100(1): p. 76-81.

FIGURES Figure 1: Standard six-port placement for Robot Assisted Radical Prostatectomy. Two 12mm, three 8mm and one 5mm trocar are placed in the standard way providing sufficient distance between the camera and working ports to prevent internal or external collision of instruments. Figure 2: Posterior Dissection. A: With the bedside assistant providing anterior upper traction on the peritoneum using the Xomed Microfrance graspers and posterior downward traction using the suction tip, access through the peritoneum is granted and the vas deferens and seminal vesicles are exposed. B: Both the seminal vesicles and transected vas deferens are liberated. Figure 3: Retzius Space Dissection. After diving the umbilical ligaments and urachus the anterior surface of the bladder is liberated off the anterior surface of the abdominal wall. It is usually an avascular plane however patent vessels can be found and good hemostasis is to be achieved. This flimsy tissue is bluntly dissected to the pubic bone. Figure 4: Anterior Prostatic Fat Dissection. A: Anterior Prostatic Fat (APF) overlying the dorsal venous complex, the anterior surface of the prostate and the prostato-vesical junction. B: En bloc dissection of the APF extended cephalad to the prostato-vesical junction and laterally toward the lateral pelvic sidewall. C: Anterior prostatic surface exposed after APF dissection. Figure 5: Dorsal Venous Complex Ligation. A: Distal ligation of the Dorsal Venous Complex (DVC) using a Vicryl 1-0 suture. The suture is passed beneath the DVC and anterior to the urethra as far from the prostatic apex as possible. B: Proximal ligation of the DVC. This suture is placed to allow cephalad traction while transecting the DVC later in the procedure. Figure 6: Bladder Neck Transection. A: The anterior bladder neck is incised and the prostate is suspended anteriorly toward the abdominal wall by the assistant’s grasper. At this point the bedside assistant also provides counter traction externally on the penile meatus Foley catheter. B: After having inspected the posterior bladder neck the assistant is asked to provide posterior traction with the suction tip at the level of the bladder neck. The posterior detrusor fibers and the bladder mucosa are then incised. Figure 7: Dorsal Venous Complex (DVC) Transection. The fourth arm grasper provides cephalad traction on the backbleed Vicryl suture that was placed proximally while the monopolar scissors divide the DVC. Figure 8: Urethral transection. Once the dorsal venous complex has been divided the urethra is skeletonized to delineate the end of the prostate and the released neurovascular bundles. The anterior urethral wall is then transected until visualization of the Foley catheter. Figure 9: Posterior Reconstruction. A: The V-LOC suture is passed through the bladder-side retrotrigonal area at the 5, 6 and 7 o’clock position and through the periurethral rectourethralis muscle. B: Traction is used on the V-LOC suture to cinch down the bladder until its mucosa is adjacent to the urethral stump and no gap is left. Figure 10: Overview of Posterior Reconstruction (PR) and Vesico-Urethral Anastamosis (VUA) using V-LOC sutures. A: Interlocked V-LOC configuration for PR and VUA. Note the use of two six-inch sutures in which the loops of both sutures are threaded by the opposite needles. B: The left-arm of the hybrid suture is passed initially at the 5-o’clock position of the retrotrigonal tissue. The suture is pulled through until the inter-twined loops oppose the tissue providing resistance. (red asterix) Using three consecutive bites, the PR helps approximate the edge of the bladder neck to the peri-urethral tissue. C: The left arm of the suture is then passed trans-murally through the 6-o’clock bladder neck and used to initiate a standard Van Velthoven anastamosis. The right arm is then used to close the right-sided VUA. D: A visual cystogram with 300 cc of normal saline is performed to ensure no leakage. Figure 11: Vesico-Urethral Anastamosis (VUA) using V-LOC sutures. A: The left arm of the VLOC suture is used to start the Van Velthoven anastamosis. The right arm of the V-LOC suture is then used to close the right-sided VUA. B: A visual cystogram with 300cc of saline is performed to ensure the integrity of the VUA and thus, the absence of fluid leakage.