Embed Size (px)
Citation preview

Randomized comparison of intraaortic balloon counterpulsation
versus optimal medical therapy in addition to early
revascularization in acute myocardial infarction complicated by cardiogenic shock
Holger Thiele, MDUwe Zeymer, MD; Franz-Josef Neumann, MD; Miroslaw Ferenc,
MD; Hans-Georg Olbrich, MD; Jörg Hausleiter, MD; Gert Richardt, MD; Marcus Hennersdorf, MD; Klaus Empen, MD; Georg Fuernau, MD; Steffen Desch, MD;
Ingo Eitel, MD; Rainer Hambrecht, MD; Jörg Fuhrmann, MD; Michael Böhm, MD; Henning Ebelt, MD; Steffen Schneider, PhD;
Gerhard Schuler, MD; Karl Werdan, MD
on behalf of the IABP-SHOCK II Trial Investigators
University of Leipzig – Heart Center

DisclosuresFunding:German Research FoundationGerman Heart Research Foundation German Cardiac SocietyArbeitsgemeinschaft Leitende Kardiologische Kranken hausärzteUniversity of Leipzig – Heart CenterUnrestricted grant by:Maquet Cardiopulmonary AG, Hirrlingen, Germany Teleflex Medical, Everett, MA, USA
Potential Conflict of Interest:Research Funding:Terumo, Lilly, Maquet Cardiovascular, Teleflex MedicalConsulting:Maquet Cardiovascular, LillySpeaker Honoraria:Lilly, Astra Zeneca, Daiichi Sankyo, Boehringer Ingelheim, Maquet Cardiovascular, Medicines Company

IABP in Cardiogenic Shock
History:
1962 Animal studiesMoulopoulos et al. Am Heart J 1962;63:669-675
1968 First clinical description in shockKantrowitz et al. JAMA 1968;203:135-140
1973 Hemodynamic effects in shock,Mortality unchangedScheidt et al. NEJM 1973;288:979-984
> 40 years > 1 Million patients treated, low complication rate , Benchmark registry Ferguson et al. JACC 2001;38:1456-1462
Background

Guidelines
IABP in AMI complicated by cardiogenic shock
Class IB
ACC/AHA
ESC
Class IC
Van de Werf et al. Eur Heart J 2008;29:2909-2945Wijns et al. Eur Heart J 2010;31:2501-2555Antman et al. Circulation 2004;110:82-292
Background

Sjauw et al. Eur Heart J 2009;30:459-468
-1 -0.5 0.5 10
No IABP betterIABP better
30-day mortalityRisk difference
IABPn/N
No IABPn/N
Trial
-0.29 (-0.47 to -0.12)
No reperfusion24/34
24/34
15/15
15/15
Moloupoulos
Overall
-0.11 (-0.13 to -0.09)Overall 2488/5146 3332/5283
-0.18 (-0.20 to -0.16)Overall
ThrombolysisStomel
Kovack
BengtsonWaksman
GUSTO-1
SHOCK registry
NRMI-2 TT
28/51
10/27
48/99
11/20
30/62
220/439
1068/2180
1415/2878
10/13
13/19
58/101
17/21
146/248
300/417
2346/3501
2890/4320
Overall 1049/2234 0.06 (0.03 to 0.10)
Primary PCINRMI-2 PCIAMC CS
956/2035
93/199
401/955
26/93
427/1048
Mortality IABP vs no IABP - MetaanalysisBackground

25 2531
3951
86
2211
22
0102030405060708090
ALKK
GUSTO IGUSTO II
I
Euro H
eart
Survey
Worce
ster-R
egist
ryNRM
I-2NRM
I 2-4
SHOCK-Reg
istry
SHOCK-Tria
l
IAB
P U
se(%
)
IABP-Use in Cardiogenic Shock
Thiele et al. Eur Heart J 2010,31:1828-1835
Background

Study Sites and Organisation
DSMB:Kurt HuberFerenc FollathBernhard MaischJohannes HaertingSteering committee:Holger ThieleKarl WerdanUwe ZeymerGerhard SchulerSupport + Patronage:
Methods
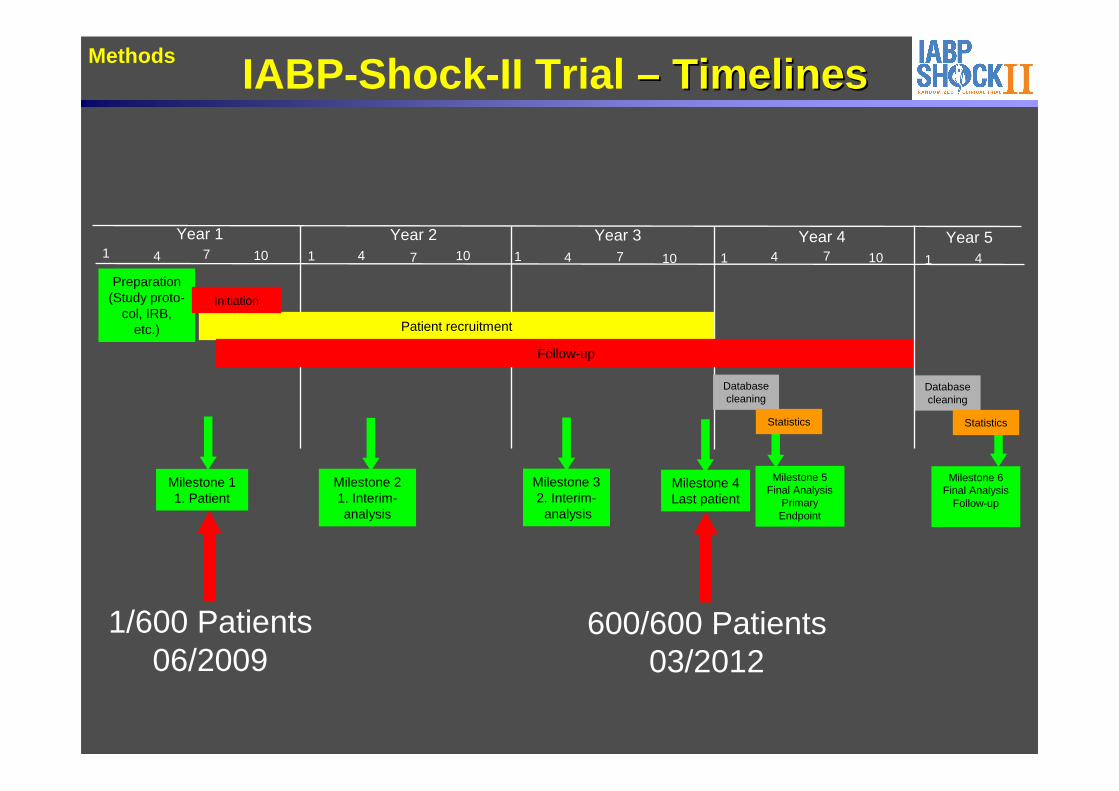
IABP-Shock -II Trial –– TimelinesTimelines
Milestone 32. Interim-
analysis
Milestone 4Last patient
Year 1 Year 2 Year 3 Year 4 Year 5
Patient recruitment
Follow-up
Preparation (Study proto-
col, IRB, etc.)
1 1 44 7 7 1010 1 4 7 10 1 4 7 10 1 4
Milestone 5Final Analysis
Primary Endpoint
Database cleaning
Statistics
Milestone 6Final Analysis
Follow-up
Database cleaning
Statistics
Milestone 21. Interim-analysis
Milestone 11. Patient
Initiation
600/600 Patients03/2012
Methods
1/600 Patients06/2009

Statistical MethodologySample Size
– Estimated 12% absolute difference in survival rates– Sequential statistical design with 2 interim analys es (33% and 66% of patients)– Significance level 0.0005 at 1st or 0.014 at 2nd in terim analysis.
Final analysis at α-level 0.044 → 564 patients– To compensate losses in follow-up and putative cent er effect → 600 patients
Thiele et al. Am Heart J 2012;163:938-45
Methods
Primary Study Endpoint :30-day all-cause mortality
Secondary Study Endpoints:- Hemodynamic parameters (mean BP, heart rate pre and post revascularization)- Serum-lactate (every 8 h for 48 h)- SAPS-2 Score- Serial creatinine-level and creatinine-clearance (C ockcroft-Gault-formula)- Inflammatory reaction (CRP)Process of care- Time until hemodynamic stabilization- Catecholamine dose and duration- Requirement for LVAD-implantation or HTx- Requirement for renal replacement therapy- Length of ICU-stay- Length of mechanical ventilation- Mortality after 6 and 12 months

298 primary endpoint analysis
600 randomized
299 randomized to control• 269 received control therapy• 30 cross-over to IABP (22 first day, 8 day 1-8)
- 4 mechanical complications- 25 protocol violation- 1 unknown reason
Allocation
300 with 30-day follow-up- 1 lost to follow-up
298 with 30-day follow-up- 1 withdrew informed consent
Follow-up
300 primary endpoint analysis
Primary endpointanalysis
790 patients with AMI and cardiogenic shock screene d
299 intended early revascularization• 288 primary PCI• 3 primary CABG• 8 no revascularization
- 1 not suitable for revascularization- 2 coronary artery disease with no identifiable culprit lesion- 5 no coronary artery disease
Revascularization
190 excluded because of exclusion criteria- 60 no informed consent- 47 resuscitation >30 minutes- 19 shock duration >12 hours- 18 severe peripheral artery disease- 14 participation in another trial- 13 no intrinsic heart activity- 9 mechanical complication- 3 shock of other cause- 3 comorbidity with life expectancy <6 months- 2 severe cerebral deficit- 2 age >90 years
Results Trial Flow and Treatment
301 randomized to IABP• 288 received IABP• 13 did not receive IABP
- 10 died before IABP insertion- 3 protocol violation
(2 not suitable for revascularization, 1 serious kinking)
301 intended early revascularization• 287 primary PCI• 3 primary CABG• 11 no revascularization
- 3 not suitable for revascularization - 4 coronary artery disease with no identifiable culprit lesion- 4 no coronary artery disease

Patient CharacteristicsResults
121/293 (41.3)57/293 (19.5)79/293 (27.0)28/293 (9.6)8/293 (2.7)
132/293 (45.1)55/293 (18.8)73/293 (24.9)26/293 (8.9)7/293 (2.4)
Infarct related artery; n/total (%)LADLCXRCALeft mainBypass graft
56.8 (39.7-78.1)60.7 (43.4-86.6)Creatinine clearance (ml/min); median (IQR)
20/299 (6.7)28/301 (9.3)Fibrinolysis < 24 h before randomization; n/total ( %)
35 (25-45)35 (25-45)Left ventricular ejection fraction (%); median (IQR )
228/293 (77.9)235/296 (79.4)Multivessel disease; n/total (%)
232/299 (77.6)245/299 (81.9)99/299 (33.1)218/298 (73.2)
215/300 (71.7)257/300 (85.7)90/300 (30.0)226/300 (75.3)
Signs of impaired organ perfusion; n/total (%)Altered mental statusCold, clammy skin and extremitiesOliguriaSerum lactate >2.0 mmol/l
143/299 (47.8)127/301 (42.2%)Resuscitation before randomization; n/total (%)
212/298 (71.1)81/298 (27.2)
200/300 (66.7)96/300 (32.0)
STEMI/LBBB; n/total (%)NSTEMI; n/total (%)
12/299 (4.0)20/300 (6.7)Prior CABG; n/total (%)
52/299 (17.4)63/299 (21.1)Prior PCI; n/total n (%)
61/299 (20.4)71/300 (23.7)Prior myocardial infarction; n/total n (%)
26.9 (24.7-29.4)27.5 (24.7-30.1)Body mass index (kg/m 2); median (IQR)
108/299 (36.1)199/299 (66.6)105/299 (35.1)90/299 (30.1)
96/295 (32.5)213/296 (72.0)122/295 (41.4)105/297 (35.4)
Current Smoking; n/total (%)Hypertension; n/total (%)Hypercholesterolemia; n/total (%)Diabetes mellitus; n/total (%)
211 (70.6)202 (67.1)Male sex; n (%)
69 (58-76)70 (58-78)Age (years); median (IQR)
Control (n=299)IABP (n=301)

Treatment + Process of Care OutcomesResults
0.503.0 (1.0-6.0)3.0 (1.0-5.0)Time to hemodynamic stabilization (days); median (IQR)
0.813.0 (1.0-6.0)3.0 (1.0-5.0)Duration of catecholamines (days), median (IQR)
0.760.730.590.25
4.2 (3.6-8.3)0.4 (0.1-1.1)0.3 (0.2-1.4)9.0 (4.8-17.6)
4.1 (2.9-7.7) 0.3 (0.1-1.2)0.3 (0.1-1.3)
10.2 (4.9-20.6)
Catecholamines (μg/kg per minute); median (IQR)DopamineNorepinephrineEpinephrineDobutamine
0.070.400.730.520.63 0.030.940.34
284/298 (95.3)206/298 (69.1)76/298 (25.5)15/228 (6.6)
143/298 (48.0)275/298 (92.3)59/298 (19.8)36/298 (12.1)
293/299 (98.0)216/299 (72.2)80/299 (26.8)19/234 (8.1)
138/299 (46.2)288/299 (96.3)60/299 (20.1)29/299 (9.7)
Antiplatelets and anticoagulation; n/total (%)AspirinClopidogrelPrasugrelTicagrelor*Glycoprotein IIb/IIIa-inhibitorsUnfractionated heparinLow molecular weight heparinBivalirudin
0.1247/299 (15.7)62/301 (20.6)Renal replacement therapy; n/total (%)
0.346.0 (3.0-13.0)6.0 (3.0-12.0)Duration of intensive care treatment (days); median (IQR)
0.443.0 (1.0-8.0)3.0 (1.0-8.0)Duration of mechanical ventilation (days); median (IQR)
0.15252/299 (84.3)240/301 (79.7)Mechanical ventilation; n/total (%)
0.21120/299 (40.1)106/301 (35.2)Mild hypothermia; n/total (%)
0.05322/299 (7.4)11/301 (3.7)Active left ventricular assist device; n/total (%)
0.724/299 (1.3)3/301 (1.0)Staged bypass surgery; n/total (%)
0.6210/299 (3.3)8/301 (2.7)Immediate bypass surgery; n/total (%)
0.4581/299 (27.1)90/301 (29.9)Immediate PCI of non-culprit lesions; n/total (%)
0.86123/299 (41.1)126/301 (41.9)Drug-eluting stent; n/total (%)
0.48266/299 (89.0)273/301 (90.7)Stent implanted; n/total (%)
0.55288/299 (96.3)287/301 (95.3)Primary PCI; n/total (%)
pControl (n=299)IABP (n=301)Variable

0
10
20
30
40
50
60
70
80
P=0.34 P=0.14P=0.005P=0.02P=0.89
Sim
plifi
ed A
cute
Phy
siol
ogy
Sco
re-I
I
Baseline Day 1 Day 2 Day 3 Day 4
Simplified Acute Physiology Score-IIResults
ControlIABP

0
10
20
30
40
50
60
70
80
90
100 P=0.55 P=0.34P=0.55P=0.96P=0.12
Baseline Day 1 Day 2 Day 3 Day 4
Est
imat
ed G
lom
erul
ar F
iltra
tion
Rat
e (m
l/min
)
Results Renal Function (eGFR)
ControlIABP

0
1
2
3
4
5
6
7
8
9
P=0.43
P=0.12
P=0.06
P=0.32P=0.32 P=0.37
Baseline 8 hours 16 hours 24 hours 32 hours 40 hours 48 hours
Ser
um L
acta
te (
mm
ol/l)
P=0.09
ControlIABP
Results Serum Lactate

0
50
100
150
200
250
300
P=0.39
P=0.55
P=0.85
P=0.56
P=0.01C-R
eact
ive
Pro
tein
(m
g/l)
Baseline Day 1 Day 2 Day 3 Day 4
Results Inflammatory Reaction (CRP)
ControlIABP

Mor
talit
y (%
)
Time after Randomization (Days)
P=0.92 by log-rank testRelative risk 0.96; 95% CI 0.79-1.17; P=0.69 by Chi2-Test
Primary Study Endpoint (30-Day Mortality)Results
Control41.3%
IABP 39.7%
0
10
20
30
40
50
0 5 10 15 20 25 30

0 0.5 1 1.5 2 2.5IABP better Control better
Results Subgroups (30-Day Mortality)
187411
Baseline Variable N30-Day Mortality (%)
IABP ControlRelative Risk
(95% CI)P-Value forInteraction
FemaleMale
Age <50 yearsAge 50-75 yearsAge >75 years
DiabetesNo diabetes
HypertensionNo hypertension
STEMI/LBBBNSTEMI
Anterior STEMI Non-anterior STEMI
Previous infarctionNo previous infarction
HypothermiaNo hypothermia
70334194
195399
410183
412177
216196
131466
226372
44.437.3
19.434.653.7
42.937.2
42.928.9
41.037.5
35.448.3
47.937.3
48.135.1
43.240.5
44.136.540.0
46.738.9
40.443.0
42.938.3
43.742.2
33.343.3
44.239.3
1.03 (0.74-1.43)0.92 (0.72-1.18)
0.44 (0.21-0.95)0.95 (0.71-1.27)1.07 (0.81-1.41)
0.92 (0.67-1.26)0.96 (0.74-1.23)
1.06 (0.84-1.34)0.67 (0.45-1.01)
0.96 (0.77-1.21)0.98 (0.67-1.43)
0.81 (0.58-1.13)1.16 (0.85-1.57)
1.44 (0.93-2.21)0.86 (0.69-1.07)
1.09 (0.82-1.44)0.89 (0.68-1.16)
0.61
0.09
0.82
0.05
0.76
0.14
0.04
0.31
Blood pressure <80 mmHgBlood pressure ≥80 mmHg
161432
50.735.9
46.439.2
1.09 (0.79-1.50)0.92 (0.72-1.17)
0.76

Safety
IABP (n=300) Control (n=298) P
Stroke in-hospital n/total (%) 2/300 (0.7) 5/298 (1.7) 0.28
GUSTO bleeding; n/total n (%)
Life-threatening/severeModerate
10/300 (3.3) 52/300 (17.3)
13/298 (4.4) 49/298 (16.4)
0.51 0.77
Peripheral ischemic complication requiring intervention; n/total n (%) 13/300 (4.3) 10/298 (3.4) 0.53
Sepsis; n/total n (%) 47/300 (15.7) 61/298 (20.5) 0.15
Results

Trial n/N n/NRelative Risk
95% CIRelative Risk95% CI
0 0.5 1 2 3
Randomized Studies in Cardiogenic ShockFollow-up
Revascularization (PCI/CABG)SHOCKSMASHTotal
76/15222/32
103/184
83/14918/23
117/172
0.80 (0.66;0.98)0.87 (0.66;1.29)0.82 (0.70;0.98)
1-year30 days
Early revascularization better
Medical treatmentbetter
0.75 1.5 2.50.25
Norepinephrinebetter
0.75 (0.55;0.93)64/145 50/13528 daysDopamine better
CatecholaminesSOAP II (CS Subgroup)
In-hospital 15/40 13/40 1.15 (0.59;2.27)Up-stream Abciximabbetter
Standard treatmentbetter
Glycoprotein IIb/IIIa-InhibitorsPRAGUE-7
97/20124/59
4/15125/275
30 days30 days30 days
76/1807/20
10/1593/215
1.14 (0.91;1.45)1.16 (0.59;2.69)0.40 (0.13;1.05)1.05 (0.85;1.29)
NO Synthase inhibitionbetter
Placebobetter
NO Synthase InhibitorsTRIUMPHSHOCK-2Cotter et alTotal
30 days30 days30 days
9/219/196/13
24/53
9/205/146/13
20/47
0.95 (0.48;1.90)1.33 (0.57-3.10)1.00 (0.44-2.29)1.06 (0.68-1.66)
LVADbetter
IABPbetter
LVADThiele et alBurkhoff et alSeyfarth et alTotal
Updated from Thiele et al. Eur Heart J 2010,31:1828-1835
30 days30 days
7/19119/300126/319
6/21123/298129/319
IABPbetter
Standard treatmentbetter
1.28 (0.45;3.72)0.96 (0.79;1.17)0.98 (0.81;1.18)
IABPIABP-SHOCK IIABP-SHOCK IITotal

Summary + Conclusions
• IABP support in cardiogenic shock is safe without significant inherent complications.
• However, IABP support did not reduce 30-day mortality in this large, randomized, multicenter trial in cardiogenic shock patients complicating myocardial infarction undergoing early revascularization.
• The primary study endpoint results are supported by a lack of benefit in secondary endpoints.

Acknowledgement and Thank You
H. Thiele (Chair)G. SchulerK. WerdanU. Zeymer
J. Haerting (Chair)F. FollathK. HuberB. Maisch
DFGDSHFDGKALKKUniversity of Leipzig –Heart CenterMaquet CardiovascularTeleflex Medical
H. ThieleU. Zeymer
Steering Committee
DSMB
CEC
Funding
IABP-SHOCK II Investigators from 37 German Sites
S. Schneider (Statistics chair)T. Oarrak (Statistics)U. ZeymerK. VonderschmittZ. AlkisogluS. FreyB. Messemer
CRO IHF Ludwigshafen
Leipzig; H. Thiele, G. Schuler, S. Desch, G. Fuernau, I. Eitel, S. de Waha, S. Wetzel, T. Pausewang, A. LeuschnerBad Krozingen: F.-J. Neumann, M. FerencLangen. H.-G. Olbrich, H.-B. HopfMunich German Heart Center: J. Hausleiter, A. de Waha, M. Orban, C. Lennerz, M. SeyfarthBad Segeberg: G. Richardt, B. Schwarz, M. Abdel-Wahab, R. Toelg, V. Geist, M. Bahnsen-MaaßHeilbronn: M. Hennersdorf, U. Rieman, J. Graf, A. Kuhn, D. ScharpfGreifswald: K. Empen. S. FelixHalle (Saale): K. Werdan, H. Ebelt, A. Schlitt, M. BuerkeBremen: R. Hambrecht, E. Fiehn, A. FachLudwigshafen: U. .Zeymer, A. K. Gitt, B. Mark, R.WinklerBad Berka: B. Lauer, J. FuhrmannHomburg/Saar: M. Böhm, A. LinkJena: H.R. Figulla, M. Ferrari, C. Jung, S. UtschigLübeck: V. Kurowski, S. Wolfrum, P.W. Radke, H. SchunkertHennigsdorf: H.-H. MindenMagdeburg: R. C. Braun-Dullaeus, F. Walz, A. SchmeißerCottbus – Heart Center: J. Krülls-Münch, K. RochorDresden: R. H. Strasser, G. SimonisWürzburg: S. Maier, G. ErtlMunich – Neuperlach: H. Mudra, M. HugRegensburg: P. Bomba, P. SickBerlin – Banjamin Franklin: C. Tschöpe, H.-P. SchutlheissBerlin – Vivantes am Urban: H. Roth, D. AndresenCottbus – Carl-Thiem-Klinikum: C. Kurek, J. Krülls-MünchRostock: C. Nienaber, H. Ince, H. SchneiderBad Nauheim: C. Hamm, H. MöllmannErfurt: H. LappBerlin – Charité Mitte: G. Baumann, F. KnebelMunich – Großhadern: W. FranzBerlin – Vivantes AVK: H. Schühlen, L. U. SttrackeWeiden: R. H. Schwinger, H. BäumlFulda: V. SchächingerEssen: M. LichtenbergUnna: D. GießmannMerseburg: R. ProndzinskyDetmold: U. TebbeVillingen-Schwenningen: R. Birkemeyer
Study Sites





























