Embed Size (px)
Citation preview

For peer review only
RANDOMISED CONTROLLED TRIAL OF TOPICAL KANUKA
HONEY FOR THE TREATMENT OF ROSACEA
Journal: BMJ Open
Manuscript ID: bmjopen-2015-007651
Article Type: Research
Date Submitted by the Author: 12-Jan-2015
Complete List of Authors: Braithwaite, Irene; Medical Research Institute of New Zealand, Hunt, Anna; Medical Research Institute of New Zealand, Riley, Judith; Medical Research Institute of New Zealand, Fingleton, James; Medical Research Institute of New Zealand, Kocks, Janwillem; Medical Research Institute of New Zealand, Corin, Andrew; Clinical Horizons, Helm, Colin; Clinical Horizons, Sheehan, Davitt; Papamoa Pines Medical Centre,
Tofield, Chris; Cameron Medical Clinic, Montgomery, Barney; Optimal Clinical Trials, Holliday, Mark; Medical Research Institute of New Zealand, Weatherall, Mark; University of Otago Wellington, Beasley, Richard; Medical Research Institute of New Zealand,
<b>Primary Subject Heading</b>:
Complementary medicine
Secondary Subject Heading: Complementary medicine, Dermatology, Infectious diseases
Keywords: Rosacea, Kanuka honey, randomised controlled trial
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on D
ecember 5, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-007651 on 24 June 2015. D
ownloaded from

For peer review only
Page 1
RANDOMISED CONTROLLED TRIAL OF TOPICAL KANUKA HONEY FOR THE
TREATMENT OF ROSACEA
Irene Braithwaite1, Anna Hunt1, Judith Riley1, James Fingleton1, Janwillem Kocks1
Andrew Corin2, Colin Helm2 Davitt Sheahan3, Chris Tofield4, Barney Montgomery5, Mark
Holliday1, Mark Weatherall6, Richard Beasley1
1Medical Research Institute of New Zealand, Wellington, New Zealand, 2 Clinical Horizons,
Tauranga, New Zealand, 3 Papamoa Pines Medical Centre, Tauranga, New Zealand, 4
Cameron Medical Clinic, Tauranga, New Zealand, 5 Optimal Clinical Trials, , Auckland, New
Zealand, 6University of Otago, Wellington
Word count: (Abstract 298), manuscript 2,459
Key words: Rosacea, kanuka honey, randomised controlled trial
Ethics approval: Central Health and Disability Ethics Committee (13/CEN/118) Funding: This study was funded by HoneyLab. HoneyLab provided the medical grade kanuka honey.
Contact: Dr Irene Braithwaite Medical Research Institute of New Zealand Private Bag 7902, Wellington 6242, New Zealand Telephone: +64-4-805 0233 Fax: +64-4-389 5707 Email:[email protected]
Page 1 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 2
ABSTRACT (298 words including registration statement)
Objective: To investigate the efficacy of topical 90% medical grade kanuka honey and 10%
glycerine (Honevo®) as a treatment for rosacea.
Design: Randomised controlled trial with blinded assessment of primary outcome variable.
Setting: Outpatient primary healthcare population from 5 New Zealand sites.
Participants: 138 adults aged ≥16, with a diagnosis of rosacea, and a baseline blinded
Investigator Global Assessment of Rosacea Severity Score (IGA-RSS) of ≥2. 69 participants
were randomised to each treatment arm. One participant was excluded from the Honevo®
group, and 7 and 15 participants withdrew from the Honevo® and control groups
respectively.
Interventions: Participants were randomly allocated 1:1 to Honevo® or control cream
(cetomacrogol), applied twice daily for 8 weeks.
Main outcome measures: The primary outcome measure was the proportion of subjects
who had a ≥ 2 improvement in the 7-point IGA-RSS at week 8 compared to baseline.
Secondary outcomes included change in IGA-RSS and subject-rated visual analogue score
of change in severity (VAS-CS) on a 100mm scale (0mm ‘much worse’, 100mm ‘much
improved’) at weeks 2 and 8.
Results: 24/68 (34.3%) in the Honevo® group and 12/69 (17.4%) in the control group had a
≥ 2 improvement in IGA-RSS at week 8 compared to baseline (relative risk 2.03; 95% CI
1.11 to 3.72, P=0.020). The change in IGA-RSS for Honevo® compared to control at week 2
minus baseline was -1 (Hodges-Lehman estimate, 95%CI -1 to 0, P=0.03), and at week 8
minus baseline was -1 (Hodges-Lehman estimate, 95%CI -1 to 0, P=0.005). The VAS-CS at
week 2 was 9.1 (95%CI 3.5 to 14.7), P=0.002, and at week 8 was 12.3 (95%CI 5.7 to 18.9)¸
P<0.001 for Honevo® compared to control.
Conclusion: Honevo® is an effective treatment for rosacea.
Trial registration: This trial was registered in the Australian and New Zealand Clinical Trials
Registry ACTRN12614000004662
Page 2 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 3
WHAT IS KNOWN ABOUT THE TOPIC?
Honey is a potential topical treatment for rosacea as it has antimicrobial and anti-
inflammatory effects. A recent pilot study has demonstrated that medical grade (sterilised
and filtered), kanuka honey is an acceptable and potentially effective treatment for rosacea
WHAT THIS STUDY ADDS
Our study has shown that Honevo® is an effective treatment for rosacea, with clinical
efficacy observed within 2 weeks of treatment.
STRENGTHS AND LIMITATIONS
• This is a randomised placebo-controlled trial of topical 90% medical-grade kanuka
honey and 10% glycerine cream (Honevo®) versus a non-ionic paraffin based cream
(cetomacragol) for the treatment of rosacea
• The primary outcome variable for this study (Investigator Global Assessment of
Rosacea Severity Score) was assessed by investigators who were blinded to
randomisation throughout the trial.
• Due to the nature of the products being assessed, participants were not able to be
blinded to the treatment arms
• Further randomised controlled trials comparing Honevo® with topical metronidazole
and azelaic acid are required to determine its relative efficacy and side effect profile
compared to these agents
Page 3 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 4
INTRODUCTION
Rosacea is a common chronic inflammatory skin condition which primarily affects the face,
and occurs in up to 10% of the adult population.1-3 There is no cure, and affected individuals
may experience substantial morbidity. There is a range of treatment options, including
several topical and oral antibiotics, however these are only partially effective and side effects
may limit their use3-6 Also there are global concerns about the increasing rates of antibiotic
resistance resulting from the widespread use of antibiotics, particularly with long term use in
chronic conditions.7,8 This has led to the United Kingdom Standing Medical Advisory
Committee recommending that the fewest number of antibiotic courses should be prescribed
for the shortest period possible.9
This has led to the investigation of alternative therapies such as medical grade kanuka
honey, due to its potent antibacterial and anti-inflammatory activities.10-14 The
pathophysiological rationale underlying its use is that rosacea is an inflammatory disorder,
and that antigenic proteins related to the bacterium Bacillus oleronius isolated from the
Demodex folliculorum mite, which infests the skin in rosacea, exacerbates this inflammatory
response.15,16 Furthermore, people with rosacea express abnormally high levels of the
antimicrobial peptide cathelicidin, which promotes the inflammatory response in rosacea.17
A recent pilot study of topical medical-grade kanuka honey as a treatment for rosacea found
it to be an acceptable and potentially effective treatment.18 The addition of 10% glycerine to
the honey has resulted in a product that is easier to apply to the skin. In this randomised
controlled trial we have investigated the efficacy of kanuka honey in the treatment of
rosacea. We designed the trial to overcome the recognised limitations of previous studies, in
particular to ensure that there was blinded investigator assessment of rosacea severity.5
Page 4 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 5
METHODS
This parallel group randomised controlled trial with assessor blinding was undertaken at a
hospital-based research facility and 4 community-based research and / or primary care sites
in New Zealand. Adults aged 16 or over with a doctor’s diagnosis of rosacea on the face,
and a baseline blinded Investigator Global Assessment of Rosacea Severity Score (IGA-
RSS) of facial rosacea of ≥2 were recruited. The IGA-RSS is a 7-point scale (from 0: ‘clear’,
to 6: ‘severe’) that provides an integrated assessment of rosacea severity based on the
principal facial signs of papules/pustules, inflammatory lesions, erythema and telangiectasia4
(Table S1). Subjects were identified at the time of first presentation or, with their primary
care practitioner’s consent, from pre-existing databases, or by public advertisement.
Exclusion criteria included current requirement for systemic corticosteroids, or systemic
corticosteroid treatment in the 4 weeks prior to Visit 1, current requirement for oral or topical
antibiotic therapy for rosacea, current requirement for topical corticosteroid treatment for
rosacea, known or suspected allergy to honey, or Cetomacrogol control cream, or any other
condition which, at the investigators discretion, it was believed may present a safety risk or
impact the feasibility of the study or the study results.
Participants attended for 3 visits (Table S2). Visit 1 (week 0) consisted of consent, baseline
assessments (the IGA-RSS), a participant-rated rosacea severity visual analogue score
(VAS–S) on a 100mm scale (0mm being ‘mildest possible’ symptoms and 100mm being
‘worst possible’ symptoms), and a participant-rated dermatology quality of life index
(DLQI)19, followed by randomisation to Honevo® or Cetomacrogol cream (control). At Visit 2
(week 2) and Visit 3 (week 8), as well as the IGA-RSS and the DLQI, participants completed
a subjective rosacea ‘change in severity’ visual analogue scale (VAS-CS) on a 100mm scale
(0mm being ‘much worse’ and 100mm being ‘much improved’). Subjects’ diaries were used
throughout the study to capture each participant’s weekly subjective VAS-S, their use of
Page 5 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 6
randomised treatment throughout the 8 week study period, and any general comments
including adverse events throughout the study.
Randomisation and blinding
Treatment allocation was randomised using a computer generated sequence concealed to
investigators. Subjects were randomised in a 1:1 ratio to the topical application of Honevo®
or control cream. Due to the nature of Honevo® it was not possible to blind the participants
and primary investigators to the treatment allocation. An independent investigator at each
site remained blinded to the treatment allocation throughout the study to perform the blinded
IGA.
Randomised treatments
The Investigational Product was topical medical grade Kanuka honey with 10% glycerine
content (Honevo®). The control cream was Cetomacrogol, a liquid paraffin and white soft
paraffin topical emollient.20,21 The participants were instructed to apply an appropriate
amount of cream to the affected area twice daily for 30-60 minutes per application, for eight
weeks, and to remove the treatment with warm water as desired. Subjects were asked not
to use any additional treatment for their rosacea for the duration of the study, as per the
exclusion criteria.
Outcome measures
The primary outcome measure was the proportion of subjects who had a ≥2 improvement
(reduction) in the IGA-RSS at week 8 (designated ‘responders’). This measure represents a
clinically meaningful improvement in rosacea severity. The secondary outcome measures
included the change from baseline in IGA-RSS at week 2 and week 8; the participant-rated
VAS-CS at weeks 2 and 8; the change from baseline in participant-rated VAS-S at week 2
and week 8; the weekly diary-documented Rosacea severity VAS-S from participant diaries;
the change from baseline in the participant-rated DLQI19 at weeks 2 and 8; withdrawals due
Page 6 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 7
to worsening of Rosacea; adverse events; and the daily self-reported use of Honevo®
(applications per day).
Sample size and study power
We anticipated the proportion of participants in the control group who respond with a ≥2
reduction in blinded IGA would be between 25 and 50%.5 A total of 124 participants (62 in
each group) has 80% power at 5% significance to detect a 25% response rate in the control
group and a 50% response rate in the Honevo® group. We recruited 138 participants to
allow for a 10% drop-out rate.
Statistical methods
The study was analysed by an intention to treat, with the participants who withdrew
considered to be non-responders. The pre-specified statistical analysis was logistic
regression for the difference in proportions with response.
Relative risks for a ≥2 point change in IGA-RSS at week 8 from baseline and for total study
withdrawal were calculated, with P values using Fishers exact test. Odds ratios were also
calculated from logistic regression
For the Likert scaled variables the Wilcoxon test and Hodges-Lehman estimator of location
shift for the difference between treatments were used. DLQI and VAS variables were
analysed by ANCOVA with the baseline value as a continuous covariate and the
randomization as the main predictor variable. The estimates for these analyses are
interpreted as the difference between randomized groups adjusted for baseline.
Applications per day was analysed by ANOVA with the response variable the mean average
number of applications per day, predictor variable randomization group, and using the
Page 7 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 8
number of days in the trial as a weight, to account for variations in the number of days of
application.
In a post-hoc analysis, the proportion of participants in whom the IGA-RSS was zero (clear
of rosacea) at week 8 was calculated.
SAS version 9.3 was used.
Page 8 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 9
RESULTS
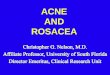
The flow of participants in the study is shown in Figure 1. There were 69 subjects
randomised to control and 69 to Honevo®. One Honevo® participant was subsequently
excluded as they were using a prohibited medication on enrolment, and their data was not
used in the consequent analysis. The characteristics of the participants are shown in Table
1. Participants were predominantly aged between 50 and 70, and had had rosacea for a
mean of 15 years. 19% of participants in each group had previously used oral antibiotics for
rosacea, while 44% and 38% had previously used any topical treatments for rosacea in the
Honevo® and control group respectively. There were 7/68 (10.3%) withdrawals in the
Honevo® group (3 worsening rosacea, 2 took prohibited medications, 2 for other reasons
unrelated to the study) and 15/69 (21.7%) withdrawals in the control group (8 worsening
rosacea, 2 took prohibited medications, 1 did not want to take the control medication, 1
found the study inconvenient and 3 for reasons unrelated to the study).
Primary outcome
There were 24/68 (34.3%) in the Honevo® group and 12/69 (17.4%) in the control group
who had a ≥2 improvement in IGA-RSS at week 8 compared to baseline (relative risk 2.03
(95% CI 1.11 to 3.72), P=0.020. The corresponding odds ratio was 2.59 (1.17 to 5.74).
Secondary outcomes
The change from baseline in IGA-RSS for participants who did not withdraw is shown in
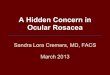
Table 2, Table S3 and Figure 2.The change in IGA-RSS for Honevo® compared to control at
week 2 minus baseline was -1 (Hodges-Lehman estimate, 95% CI -1 to 0, P=0.03), and at
week 8 minus baseline was -1 (Hodges-Lehman estimate, 95% CI -1 to 0, P=0.005),(Table
3). The subject-rated VAS-CS at week 2 was 9.1 (CI 3.5 to 14.7), P=0.002, and at week 8
was 12.3 (CI 5.7 to 18.9), P<0.001for Honevo® compared to control, representing greater
improvement with Honevo®. There was no significant difference in diary-captured VAS-S,
Page 9 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 10
adjusted for baseline, at any of the time points between week 2 and 8 (Table S4).There was
no significant difference in the participant-rated DLQI adjusted for baseline at week 2 (-0.3,
CI-1.1 to 0.6, P=0.51) or week 8 (-0.01, CI -0.7 to 0.7,P=0.97).
The number of applications per day between the randomised treatments was similar (mean
(SD) 1.84(0.23) vs 1.86(0.20) for the Honevo® and control groups respectively, difference: -
0.02 (95% CI -0.10 to 0.05), P=0.55).
In a post hoc analysis, the proportion of participants in whom the IGA-RSS score at week 8
was zero, (i.e. full resolution of rosacea) was 9/68 (13.2%) and 2/69 (2.9%) in the Honevo®
and control groups respectively, relative risk 4.6 (95%CI 1.0 to 20.4, P=0.031).
In the Honevo® group 23 participants reported 31 adverse events; 17 rosacea related, (3 of
which resulted in withdrawal of the participants), and 14 unrelated to rosacea (Table S5). In
the control group, 27 participants reported 36 adverse events; 22 rosacea related, (8 of
which resulted in withdrawal of participants), and 14 unrelated to rosacea.
Page 10 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 11
DISCUSSION
This randomised controlled trial has demonstrated that topical 90% medical grade kanuka
honey and 10% glycerine (Honevo®) is an effective and well tolerated treatment for rosacea.
About one third of participants had a clinically significant improvement in the IGA-RSS after
8 weeks of Honevo® treatment, two-fold greater than that observed with the control
treatment. We recommend consideration of the use of kanuka honey as a treatment for
rosacea.
There are a number of methodological issues that are important in the consideration of the
study findings. There are no standard validated tools for assessing the severity of rosacea,
which is inherently difficult due to its varied clinical characteristics. The priority with this study
of a honey product was to reduce potential bias by blinding of clinical assessments where
possible, as the participant could not be blinded due to the appearance and smell of
Honevo®. It was for this reason we chose to use the 7 point IGA-RSS representing a global
assessment of rosacea severity that was undertaken by an investigator who was blinded to
treatment. A 2 point reduction in IGA-RSS represents a clinically meaningful improvement,
for example a change from ‘severe’ to ‘moderate’, or from ‘moderate’ to ‘mild’ rosacea
severity. In addition, we assessed patient-reported outcomes, based on participant’s
assessment of current severity of symptoms (VAS-S), participant’s perceived change in
severity (VAS-CS) and the DLQI questionnaire, to provide a comprehensive assessment of
efficacy. The VAS-CS at the 2-week and 8-week clinic visits were significantly better with
Honevo®, but there was no difference with the 2-week and 8-week DLQI assessments or
the weekly diary VAS-S measures. The greater number of withdrawals due to worsening
rosacea in the control group (12% vs 4%), is likely to have led to an under-estimation of the
efficacy of Honevo®, as these participants did not undergo assessment of the secondary
outcome variables following withdrawal.
Page 11 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 12
Cetomacrogol cream was chosen as a comparator as it is a non-ionic moisturising cream,
often used as a vehicle for delivery of topical medications. The treatment was administered
for 8 weeks to allow both the speed of onset and the duration of effect to be assessed. This
identified that honey had efficacy within 2 weeks of treatment, with further efficacy obtained
during the 8 week treatment period. Adverse event data did not allow us to reliably ascertain
whether the rosacea specific adverse events such as burning, itching, peeling, stinging, dry
skin and pain were associated only with the application of the investigational medicine or
whether they were ongoing rosacea symptoms. However it was reassuring that the number
of participants with rosacea specific adverse events was similar between Honevo® and the
paraffin-based emollient control cream.
It is interesting to compare our findings with those from studies of topical metronidazole or
azelaic acid, two of the more commonly used treatments of rosacea.3-6 While
acknowledging the different primary outcome variables, in placebo controlled studies of
topical metronidazole the relative risk of improvement with the physician’s global evaluation
of improvement was 1.95 (95% CI 1.5 to 2.6), and in the placebo controlled studies of
azelaic cream the relative risk of participant-assessed improvement was 1.52 (95% CI 1.3 to
1.8)5,22. By comparison, the relative risk of IGA-RSS improvement with Honevo® was 2.0
(95%CI 1.1 to 3.7) and in the post hoc analysis the relative risk of resolution was 4.6 (95%CI
1.0 to 20.4). Randomised controlled trials comparing Honevo® with topical metronidazole or
azelaic cream are now indicated.
The mechanism of action was not assessed in this study, however there a number of
potential mechanisms relevant to the efficacy demonstrated with kanuka honey in this study.
Firstly kanuka honey has a number of different anti-inflammatory effects, including inhibition
of neutrophil superoxide production,12 reduction in inflammatory leucocyte infiltration and
arachidonic- induced oedema,12 and stimulation of macrophage release of tumour necrosis
factor a (TNFa),14 a cytokine with a crucial role in wound healing.23,24 These properties may
Page 12 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 13
be relevant as rosacea is a chronic inflammatory disorder, characterised by inflammatory cell
infiltration, vascular dilatation and tissue oedema.1,2,5 In addition, kanuka honey has high
antibacterial activities against a wide range of bacteria, including Bacillus subtilis,
Propionibacterium acne and Staph Aureus,10,11,13 properties which may be beneficial in view
of the proposed role of Bacillus oleronius in the inflammatory response in rosacea. The
effect of honey on Bacillus oleronius and the Demodex folliculum mite require further
investigation.
In conclusion, this randomised controlled trial has demonstrated the clinical efficacy and
tolerability of 90% medical grade kanuka honey and 10% glycerine (Honevo®) in the
treatment of rosacea. Honevo® can be recommended for the treatment of rosacea;
however, further randomised controlled trials comparing Honevo® with topical metronidazole
and azelaic acid are now required to determine its relative efficacy and side effect profile
compared to these agents.
Page 13 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 14
STATEMENTS
Corresponding Author Statement: The Corresponding Author has the right to grant on
behalf of all authors and does grant on behalf of all authors, an exclusive licence on a
worldwide basis to the BMJ Publishing Group Ltd to permit this article (if accepted) to be
published in BMJ editions and any other BMJPGL products and sublicences such use and
exploit all subsidiary rights, as set out in our licence.
Competing interest statement: All authors have completed the Unified Competing Interest
form atwww.icmje.org/coi_disclosure.pdf (available on request from the corresponding
author) and declare: HoneyLab Ltd provided funding to undertake this study and provided
the product Honevo® for the purpose of the study; Dr Shaun Holt, the Medical Director of
HoneyLab Ltd was previously the Programme Director of Complementary Medicine at the
Medical Research Institute of New Zealand. There are no other competing interests to
declare.
Role of the funding source: HoneyLab was consulted in the design of the study and
preparation of the report, but had no involvement in the collection, analysis and interpretation
of the data, or decision to submit for publication.
Contributorship statement: Study concept and design: JF, JK, MH, MW, RB. Acquisition of
Data: IB, AH, JR, AC, CH, DS, CT, BM. Drafting of the manuscript: RB, IB, MW. Critical
revision of the manuscript for important intellectual content: all authors. Statistical analysis:
MW. Administrative, technical and material support: All authors. Study supervision: MH.
Guarantor: Dr I Braithwaite had access to all the data on the study and takes responsibility
for the integrity of the data and accuracy of the data analysis.
Transparency declaration: The lead author affirms that the manuscript is an honest,
accurate, and transparent account of the study being reported; that no important aspects of
the study have been omitted; and that any discrepancies from the study as planned (and, if
relevant, registered) have been explained
Data sharing statement: Patient level data available from the corresponding author.
Consent was not obtained from participants for data sharing, but the presented data are
anonymised and the risk of identification is low. Data may be obtained by contacting the
corresponding author.
Page 14 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 15
Table 1: Baseline characteristics of participants
Mean (SD) Median (IQR) Min to Max
Age at enrolment
Honevo® N-68 57.7 (13.7) 58.2 (46.7 to 68.3) 23.4 to 86.5
Control N=69 58.9 (15.9) 60.1 (49.0 to 68.6) 18.2 to 90.1
All N=137 58.3 (14.8) 58.9 (48.1 to 68.6) 18.2 to 90.1
Age at Diagnosis
Honevo® N=64 42.2 (15.4) 40 (30 to 51.5) 19 to 80
Control N=67 43.6 (15.4) 43 (35 to 55) 10 to 79
All N=131 42.9 (15.4) 41 (32 to 54) 10 to 80
Honevo® N (%) N=68
Control N (%) N=69
Female 32 (47.1) 36 (52.2)
History of oral antibiotics 13 (19.1) 13 (18.8)
History of topical therapy 24 (35.3) 20 (29.0)
History of topical steroid 6 (8.8) 6 (8.7)
European 64 (94.1) 68 (98.6)
Maori 4 (5.9) 0 (0)
Asian 0 (0) 1 (1.5)
SD – standard deviation IQR – inter quartile range
Page 15 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 16
Table 2: Contingency table of blinded Investigator Global Assessment of Rosacea
Severity Score (IGA-RSS) week 8 change from baseline by randomisation in the
subjects who completed the study
Change from baseline Honevo® N/61 (%) Control N/54 (%)
-3 11 (18.0) 1 (1.9)
-2 13 (21.3) 11 (20.4)
-1 20 (32.8) 17 (31.5)
0 14 (23.0) 15 (27.8)
1 3 (4.9) 8 (14.8)
2 0 (0) 2 (3.7)
IGA-RSS: blinded Investigator Global Assessment of Rosacea Severity Score based on a 7 point scale (0 ‘clear’ to 6 ‘severe’
Page 16 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 17
Table 3: Clinic-based secondary outcome variables (all Honevo® minus control)
Comparison Hodges-Lehman estimate (95% CI)
P
IGA-RSS week 2 0 (-1 to 0) 0.26
IGA-RSS week 8 0 (-1 to 0) 0.06
IGA-RSS week 2 minus baseline -1 (-1 to 0) 0.03
IGA-RSS week 8 minus baseline -1 (-1 to 0) 0.005
Estimate (95% CI) P
IGA-RSS week 8 adjusted for baseline1 -0.6 (-1.1 to -0.2) 0.003
Mean difference (95% CI) P
VAS-CS week 2 9.1 (3.5 to 14.7) 0.002
VAS-CS week 8 12.3 (5.7 to 18.9) <0.001
VAS-S week 2 -3.6 (-9.9 to 2.7) 0.26
VAS-S week 2 minus baseline -2.9 (-9.2 to 3.5) 0.38
VAS-S week 8 -4.5 (-11.6 to 2.6) 0.21
VAS-S week 8 minus baseline -11.0 (-18.0 to -3.9) 0.003
IGA-RSS: blinded Investigator Global Assessment of Rosacea Severity Score, based on a 7 point scale (0 ‘clear’ to 6 ‘severe’) VAS-CS: Participant-rated assessment of Change in Severity of rosacea based on a 100mm VAS scale (0mm ‘much worse’ to 100mm ‘much improved’) VAS-S: Participant-rated assessment of Severity of rosacea based on a 100mm VAS scale (0mm ‘mildest possible’ symptoms and 100mm ‘worst possible’ symptoms) ANOVA with baseline reading as a covariate, normality assumptions not well met
Page 17 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 18
Supplement Table S1: Blinded Investigator Global Assessment of Rosacea Severity Score (IGA-RSS)
Numerical Score
Definition Description
0 Clear Almost no Rosacea (i.e. no papules and/or pustules); no or residual erythema; mild to moderate degree of telangiectasia may be present
1 Minimal Rare papules and/or pustules; residual to mild erythema; mild to moderate degree of telangiectasia may be present
2 Mild Few papules and/or pustules; mild erythema; mild to moderate degree of telangiectasia may be present
3 Mild to moderate Distinct number of papules and/or pustules; mild to moderate erythema; mild to moderate degree of telangiectasia may be present
4 Moderate Pronounced number of papules and/or pustules; moderate erythema; mild to moderate degree of telangiectasia may be present
5 Moderate to Severe
Many papules and/or pustules, occasionally with large inflamed lesions; moderate erythema; moderate degree of telangiectasia may be present
6 Severe Numerous papules and/or pustules, occasionally with confluent areas of inflamed lesions; moderate to severe erythema; moderate to severe degree of telangiectasia may be present
Page 18 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 19
Supplement Table S2: Schedule of Assessments
Visit Number Visit 1 Visit 2 Visit 3
Time Point Week 0 Day 1
Week 2 Day 15
Week 8 Day 57
Informed Consent X
Eligibility criteria checked X
Demographics and medical history X
Randomisation X
Administer DLQI X X X
Administer IGA X X X
Participant-rated severity VAS-S completiona X X X
Participant-rated change VAS-CS severity completion
X X
Provision of participant diary X X
Collection of participant diary X X
Safety monitoring X X X
DLQI: Dermatology Life Quality Index
IGA-RSS blinded Investigator Global Assessment of Rosacea Severity Score VAS-S: Participant-rated assessment of severity of rosacea VAS-CS: Participant-rated assessment of change in severity of rosacea a VAS-S to be completed weekly from Visit 1 until Visit 3, within the subject diary
Page 19 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 20
Supplement Table S3: Clinic-based secondary outcome variables
Mean (SD) Median (IQR) Min to Max
IGA-RSS week Zero
Control N=69 3 (0.9) 3 (2 to 4) 2 to 5 Honevo® N=68 3 (0.9) 3 (2 to 3.5) 2 to 6
IGA-RSS week 2
Control N=66 2.5 (1.4) 2 (2 to 3) 0 to 6 Honevo® N=66 2.2 (1.2) 2 (1 to 3) 0 to 6
IGA-RSS week 8
Control N=54 2.4 (1.3) 2 (1 to 3) 0 to 6 Honevo® N=61 1.8 (1.2) 2 (1 to 3) 0 to 5
Difference IGA-RSS week 2 to week Zero Control N=66 -0.5 (0.9) 0 (-1 to 0) -3 to 1 Honevo® N=66 -0.8 (1.0) -1 (-2 to 0) -3 to 2
Difference IGA-RSS week 8 to week Zero
Control N=54 -0.6 (1.1) 0 (-1 to 0) -3 to 2 Honevo® N=61 -1.2 (1.1) -1 (-2 to 0) -3 to 1
VAS-CS week 2
Control N=66 50.1 (16.6) 51 (47 to 55) 0 to 89 Honevo® N=66 59.2 (16.1) 59 (50 to 71) 21 to 98
VAS-CS week 8
Control N=54 55.2 (18.2) 51 (48 to 61) 15 to 98 Honevo® N=61 67.6 (17.4) 69 (52 to 79) 25 to 99
VAS-S week Zero
Control N=69 32.0 (19.1) 28 (18 to 44) 1 to 87 Honevo® N=68 36.8 (21.2) 31.5 (21 to 54) 1 to 78
VAS-S week 2
Control N=66 34.9 (19.6) 32.5 (21 to 50) 1 to 84 Honevo® N=66 31.2 (16.9) 29.5 (20 to 42) 1 to 68
VAS-S week 8
Control N=54 30.8 (19.2) 31 (13 to 46) 3 to 78 Honevo® N=61 26.3 (19.2) 24 (12 to 38) 2 to 96
Difference VAS-S week 2 to week Zero
Control N=66 3.0 (16.7) 0.5 (-6.0 to 8.0) -30 to 73 Honevo® N=66 -5.2 (16.1) -6 (-16 to 1) -37 to 38
Difference VAS-S week 8 to week Zero
Control N=54 2.1 (14.5) -1 (-9 to 11) -39 to 41 Honevo® N=61 -8.9 (22.4) -10(-24 to 9) -66 to 38
IGA-RSS: blinded Investigator Global Assessment of Rosacea Severity Score, based on a 7 point scale (0 ‘clear’ to 6 ‘severe’) VAS-CS: Participant-rated assessment of Change in Severity of rosacea based on a 100mm VAS scale (0mm ‘much worse’ to 100mm ‘much improved’) VAS-S: Participant-rated assessment of Severity of rosacea based on a 100mm VAS scale (0mm ‘mildest possible’ symptoms and 100mm ‘worst possible’ symptoms)
Page 20 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 21
Supplement Table S4: Diary-based VAS-S adjusted for baseline
Honevo® minus Control
Estimate (95% CI) P
VAS-S week 2 -4.0 (-8.5 to 0.6) 0.088
VAS-S week 3 -1.3 (-6.8 to 4.2) 0.65
VAS-S week 4 -4.0 (-10.3 to 2.4) 0.21
VAS-S week 5 -2.0 (-7.8 to 3.9) 0.50
VAS-S week 6 -5.3 (-2.5 to 14.2) 0.13
VAS-S week 7 -2.1 (-8.9 to 4.7) 0.54
VAS-S week 8 -5.7 (-6.2 to 13.3) 0.15
VAS-S: Participant-rated assessment of Severity of rosacea based on a 100mm VAS scale (0mm ‘mildest possible’ symptoms and 100mm ‘worst possible’ symptoms)
Page 21 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 22
Supplement Table S5: Adverse events reported in the Honevo® and Control groups.
Honevo® N
Control N
Rosacea related adverse events resulting in withdrawal
Worsening Rosacea 3 8
Rosacea related adverse events without withdrawal
Worsening Rosacea 0 2
Itching 5 1
Tingling 3 2
Red spots 2 0
Eczema 1 0
Dry skin 1 0
Peeling 1 0
Pain 1 0
Stinging 0 4
Burning 0 2
Blisters 0 1
Bleeding 0 1
Possible fungal skin infection 0 1
Non-rosacea related adverse events resulting in withdrawal
0 0
Non-rosacea related adverse events without withdrawal
Other skin problem 1 0
Infection 6 7
Trauma 3 1
Indigestion 1 0
Worsening Asthma 1 0
Headache / Migraine 1 2
Elevated PSA 1 0
Cardiovascular 0 2
Allergy / Hayfever 0 2
Note: Participants may report more than one adverse event
Page 22 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 23
FIGURE LEGENDS
Figure 1: Flow of participants through trial.
Figure 2: The difference from baseline in IGA-RSS at week 8 for control and Honevo®.
Horizontal lines are the 25%, median and 75% quantiles, the symbol is the mean and
the whiskers go from maximum to minimum.
Page 23 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 24
REFERENCES
1. Buechner SA. Rosacea: an update. Dermatology. 2005;210(2):100-8. 2. Berg M, Liden S. An epidemiological study of rosacea. Acta Derm Venereol. 1989;69(5):419-23. 3. Powell FC. Clinical practice. Rosacea. N Engl J Med. 2005 Feb 24;352(8):793-803. 4. Elewski BE, Fleischer AB, Jr., Pariser DM. A comparison of 15% azelaic acid gel and 0.75% metronidazole gel in the topical treatment of papulopustular rosacea: results of a randomized trial. Arch Dermatol. 2003 Nov;139(11):1444-50. 5. van Zuuren EJ, Kramer S, Carter B, Graber MA, Fedorowicz Z. Interventions for rosacea. Cochrane Database Syst Rev. (3):CD003262. 6. Elewski BE. Rosacea trial comparing twice-daily azelaic acid gel 15% with once-daily metronidazole gel 1%. Cutis. 2007 Jan;79(1):57-8; author reply 8. 7. World Health O. Antimicrobial resistance: global report on surveillance 2014; 2014. Report No.: ISBN: 978 92 4 156474 8 Contract No.: Document Number|. 8. Costelloe C, Metcalfe C, Lovering A, Mant D, Hay AD. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ.340:c2096. 9. Department of Health UKSMAC. The path of least resistance. 1998. 10. Wu Q. Antimicrobial effect of Manuka honey and Kanuka honey alone and in combination with the bioactives against the growth of Propionibacterium acnes ATCC 6919: a thesissubmitted in partial fulfilment of the requirements for the degree Master of Food Technology, Massey University, Albany, New Zealand; 2011. 11. Lu J, Carter DA, Turnbull L, Rosendale D, Hedderley D, Stephens J, et al. The effect of New Zealand kanuka, manuka and clover honeys on bacterial growth dynamics and cellular morphology varies according to the species. PLoS One.8(2):e55898. 12. Leong AG, Herst PM, Harper JL. Indigenous New Zealand honeys exhibit multiple anti-inflammatory activities. Innate Immun. Jun;18(3):459-66. 13. Allen KL, Molan PC, Reid GM. A survey of the antibacterial activity of some New Zealand honeys. J Pharm Pharmacol. 1991 Dec;43(12):817-22. 14. Gannabathula S, Skinner MA, Rosendale D, Greenwood JM, Mutukumira AN, Steinhorn G, et al. Arabinogalactan proteins contribute to the immunostimulatory properties of New Zealand honeys. Immunopharmacol Immunotoxicol. Aug;34(4):598-607. 15. Lacey N, Delaney S, Kavanagh K, Powell FC. Mite-related bacterial antigens stimulate inflammatory cells in rosacea. Br J Dermatol. 2007 Sep;157(3):474-81. 16. Bonnar E, Eustace P, Powell FC. The Demodex mite population in rosacea. J Am Acad Dermatol. 1993 Mar;28(3):443-8. 17. Yamasaki K, Di Nardo A, Bardan A, Murakami M, Ohtake T, Coda A, et al. Increased serine protease activity and cathelicidin promotes skin inflammation in rosacea. Nat Med. 2007 Aug;13(8):975-80. 18. Fingleton JS, D. Cave, N. Brinded, A. Weatherall, M. Perrin, K. Beasley,R. Topical kanuka honey for the treatment of rosacea. Focus on Alternative and Complementary Therapies. 2013;18(4):221-2. 19. Lewis V, Finlay AY. 10 years experience of the Dermatology Life Quality Index (DLQI). J Investig Dermatol Symp Proc. 2004 Mar;9(2):169-80. 20. (Datapharm) ew. Cetomacrogol Cream BP 1988 Formula A. https://wwwmedicinesorguk/emc/medicine/25140. Last accessed Dec 24,2014. 21. Kingdom NNHSU. Cetomacrogol Cream Formula A. http://wwwnhsuk/medicine-guides/pages/MedicineOverviewaspx?medicine=Cetomacrogol%20Cream%20Formula%20A. Last accessed Dec 24, 2014. 22. van Zuuren EJ, Kramer SF, Carter BR, Graber MA, Fedorowicz Z. Effective and evidence-based management strategies for rosacea: summary of a Cochrane systematic review. Br J Dermatol. Oct;165(4):760-81. 23. Fu X, Tian H, Hsu S, Wang D, Sheng Z. In vivo effects of tumor necrosis factor-alpha on incised wound and gunshot wound healing. J Trauma. 1996 Mar;40(3 Suppl):S140-3.
Page 24 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 25
24. Mooney DP, O'Reilly M, Gamelli RL. Tumor necrosis factor and wound healing. Ann Surg. 1990 Feb;211(2):124-9.
Page 25 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
56x67mm (300 x 300 DPI)
Page 26 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
11x9mm (600 x 600 DPI)
Page 27 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
CONSORT 2010 checklist Page 1
CONSORT 2010 checklist of information to include when reporting a randomised trial*
Section/Topic Item No Checklist item
Reported on page No
Title and abstract
1a Identification as a randomised trial in the title title
1b Structured summary of trial design, methods, results, and conclusions (for specific guidance see CONSORT for abstracts) 2
Introduction
Background and
objectives
2a Scientific background and explanation of rationale 4
2b Specific objectives or hypotheses 4
Methods
Trial design 3a Description of trial design (such as parallel, factorial) including allocation ratio 5
3b Important changes to methods after trial commencement (such as eligibility criteria), with reasons n/a
Participants 4a Eligibility criteria for participants 5
4b Settings and locations where the data were collected 5
Interventions 5 The interventions for each group with sufficient details to allow replication, including how and when they were
actually administered
6
Outcomes 6a Completely defined pre-specified primary and secondary outcome measures, including how and when they
were assessed
6-7
6b Any changes to trial outcomes after the trial commenced, with reasons n/a
Sample size 7a How sample size was determined 8
7b When applicable, explanation of any interim analyses and stopping guidelines n/a
Randomisation:
Sequence
generation
8a Method used to generate the random allocation sequence 6
8b Type of randomisation; details of any restriction (such as blocking and block size) 6
Allocation
concealment
mechanism
9 Mechanism used to implement the random allocation sequence (such as sequentially numbered containers),
describing any steps taken to conceal the sequence until interventions were assigned
6
Implementation 10 Who generated the random allocation sequence, who enrolled participants, and who assigned participants to
interventions
6
Blinding 11a If done, who was blinded after assignment to interventions (for example, participants, care providers, those 6
Page 28 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on December 5, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-007651 on 24 June 2015. Downloaded from

For peer review only
CONSORT 2010 checklist Page 2
assessing outcomes) and how
11b If relevant, description of the similarity of interventions n/a
Statistical methods 12a Statistical methods used to compare groups for primary and secondary outcomes 7
12b Methods for additional analyses, such as subgroup analyses and adjusted analyses 7
Results
Participant flow (a
diagram is strongly
recommended)
13a For each group, the numbers of participants who were randomly assigned, received intended treatment, and
were analysed for the primary outcome
9, fig 1
13b For each group, losses and exclusions after randomisation, together with reasons 9, fig 1
Recruitment 14a Dates defining the periods of recruitment and follow-up 5
14b Why the trial ended or was stopped n/a
Baseline data 15 A table showing baseline demographic and clinical characteristics for each group 15
Numbers analysed 16 For each group, number of participants (denominator) included in each analysis and whether the analysis was
by original assigned groups
9
Outcomes and
estimation
17a For each primary and secondary outcome, results for each group, and the estimated effect size and its
precision (such as 95% confidence interval)
9-10
17b For binary outcomes, presentation of both absolute and relative effect sizes is recommended 9-10
Ancillary analyses 18 Results of any other analyses performed, including subgroup analyses and adjusted analyses, distinguishing
pre-specified from exploratory
9-10
Harms 19 All important harms or unintended effects in each group (for specific guidance see CONSORT for harms) 10
Discussion
Limitations 20 Trial limitations, addressing sources of potential bias, imprecision, and, if relevant, multiplicity of analyses 11-12
Generalisability 21 Generalisability (external validity, applicability) of the trial findings 11-12
Interpretation 22 Interpretation consistent with results, balancing benefits and harms, and considering other relevant evidence 12-13
Other information
Registration 23 Registration number and name of trial registry abstract
Protocol 24 Where the full trial protocol can be accessed, if available uploaded
Funding 25 Sources of funding and other support (such as supply of drugs), role of funders title
*We strongly recommend reading this statement in conjunction with the CONSORT 2010 Explanation and Elaboration for important clarifications on all the items. If relevant, we also
recommend reading CONSORT extensions for cluster randomised trials, non-inferiority and equivalence trials, non-pharmacological treatments, herbal interventions, and pragmatic trials.
Additional extensions are forthcoming: for those and for up to date references relevant to this checklist, see www.consort-statement.org.
Page 29 of 29
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on December 5, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-007651 on 24 June 2015. Downloaded from

For peer review only
RANDOMISED CONTROLLED TRIAL OF TOPICAL KANUKA
HONEY FOR THE TREATMENT OF ROSACEA
Journal: BMJ Open
Manuscript ID: bmjopen-2015-007651.R1
Article Type: Research
Date Submitted by the Author: 17-Apr-2015
Complete List of Authors: Braithwaite, Irene; Medical Research Institute of New Zealand, Hunt, Anna; Medical Research Institute of New Zealand, Riley, Judith; Medical Research Institute of New Zealand, Fingleton, James; Medical Research Institute of New Zealand, Kocks, Janwillem; Medical Research Institute of New Zealand, Corin, Andrew; Clinical Horizons, Helm, Colin; Clinical Horizons, Sheehan, Davitt; Papamoa Pines Medical Centre,
Tofield, Chris; Cameron Medical Clinic, Montgomery, Barney; Optimal Clinical Trials, Holliday, Mark; Medical Research Institute of New Zealand, Weatherall, Mark; University of Otago Wellington, Beasley, Richard; Medical Research Institute of New Zealand,
<b>Primary Subject Heading</b>:
Complementary medicine
Secondary Subject Heading: Complementary medicine, Dermatology, Infectious diseases
Keywords: Rosacea, Kanuka honey, randomised controlled trial
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on D
ecember 5, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-007651 on 24 June 2015. D
ownloaded from

For peer review only
Page 1
RANDOMISED CONTROLLED TRIAL OF TOPICAL KANUKA HONEY FOR THE
TREATMENT OF ROSACEA
Irene Braithwaite1, Anna Hunt1, Judith Riley1, James Fingleton1, Janwillem Kocks1
Andrew Corin2, Colin Helm2 Davitt Sheahan3, Chris Tofield4, Barney Montgomery5, Mark
Holliday1, Mark Weatherall6, Richard Beasley1
1Medical Research Institute of New Zealand, Wellington, New Zealand, 2 Clinical Horizons,
Tauranga, New Zealand, 3 Papamoa Pines Medical Centre, Tauranga, New Zealand, 4
Cameron Medical Clinic, Tauranga, New Zealand, 5 Optimal Clinical Trials, , Auckland, New
Zealand, 6University of Otago, Wellington
Word count: (Abstract 298), manuscript 2,786
Key words: Rosacea, kanuka honey, randomised controlled trial
Funding: This study was funded by HoneyLab. HoneyLab provided the medical grade kanuka honey.
Contact: Dr Irene Braithwaite Medical Research Institute of New Zealand Private Bag 7902, Wellington 6242, New Zealand Telephone: +64-4-805 0233 Fax: +64-4-389 5707 Email:[email protected]
Page 1 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 2
ABSTRACT (298 words including registration statement)
Objective: To investigate the efficacy of topical 90% medical grade kanuka honey and 10%
glycerine (Honevo®) as a treatment for rosacea.
Design: Randomised controlled trial with blinded assessment of primary outcome variable.
Setting: Outpatient primary healthcare population from 5 New Zealand sites.
Participants: 138 adults aged ≥16, with a diagnosis of rosacea, and a baseline blinded
Investigator Global Assessment of Rosacea Severity Score (IGA-RSS) of ≥2. 69 participants
were randomised to each treatment arm. One participant was excluded from the Honevo®
group, and 7 and 15 participants withdrew from the Honevo® and control groups
respectively.
Interventions: Participants were randomly allocated 1:1 to Honevo® or control cream
(cetomacrogol), applied twice daily for 8 weeks.
Main outcome measures: The primary outcome measure was the proportion of subjects
who had a ≥ 2 improvement in the 7-point IGA-RSS at week 8 compared to baseline.
Secondary outcomes included change in IGA-RSS and subject-rated visual analogue score
of change in severity (VAS-CS) on a 100mm scale (0mm ‘much worse’, 100mm ‘much
improved’) at weeks 2 and 8.
Results: 24/68 (34.3%) in the Honevo® group and 12/69 (17.4%) in the control group had a
≥ 2 improvement in IGA-RSS at week 8 compared to baseline (relative risk 2.03; 95% CI
1.11 to 3.72, P=0.020). The change in IGA-RSS for Honevo® compared to control at week 2
minus baseline was -1 (Hodges-Lehman estimate, 95%CI -1 to 0, P=0.03), and at week 8
minus baseline was -1 (Hodges-Lehman estimate, 95%CI -1 to 0, P=0.005). The VAS-CS at
week 2 was 9.1 (95%CI 3.5 to 14.7), P=0.002, and at week 8 was 12.3 (95%CI 5.7 to 18.9)¸
P<0.001 for Honevo® compared to control.
Conclusion: Honevo® is an effective treatment for rosacea.
Trial registration: This trial was registered in the Australian and New Zealand Clinical Trials
Registry ACTRN12614000004662
Page 2 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 3
WHAT IS KNOWN ABOUT THE TOPIC?
Honey is a potential topical treatment for rosacea as it has antimicrobial and anti-
inflammatory effects. A recent pilot study has demonstrated that medical grade (sterilised
and filtered), kanuka honey is an acceptable and potentially effective treatment for rosacea
WHAT THIS STUDY ADDS
Our study has shown that Honevo® is an effective treatment for rosacea, with clinical
efficacy observed within 2 weeks of treatment.
STRENGTHS AND LIMITATIONS
• This is a randomised placebo-controlled trial of 8 weeks of treatment for rosacea with
either topical 90% medical-grade kanuka honey and 10% glycerine cream
(Honevo®) or a non-ionic paraffin based cream (cetomacragol).
• Due to the nature of the products being assessed, participants were not able to be
blinded to the treatment arms
• The primary outcome variable for this study (Investigator Global Assessment of
Rosacea Severity Score) was assessed by investigators who were blinded to
randomisation throughout the trial.
Page 3 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 4
INTRODUCTION
Rosacea is a common chronic inflammatory skin condition which primarily affects the face,
and occurs in up to 10% of the adult population.1-4 There is no cure, and affected individuals
may experience substantial morbidity. There is a range of treatment options, including
several topical and oral antibiotics, however these are only partially effective and side effects
may limit their use4-7 Also there are global concerns about the increasing rates of antibiotic
resistance resulting from the widespread use of antibiotics, particularly with long term use in
chronic conditions.8,9 For example, the United Kingdom Standing Medical Advisory
Committee now recommends the fewest number of antibiotic courses should be prescribed
for the shortest period possible.10
Amongst the alternative therapies to antibiotics, medical grade kanuka honey is of interest
due to its potent antibacterial and anti-inflammatory activities.11-15 The pathophysiological
rationale underlying its use is that rosacea is an inflammatory disorder, and that antigenic
proteins related to the bacterium Bacillus oleronius isolated from the Demodex folliculorum
mite, which infests the skin in rosacea, exacerbates this inflammatory response.16,17
Furthermore, people with rosacea express abnormally high levels of the antimicrobial
peptide cathelicidin, which promotes the inflammatory response in rosacea.18
A recent pilot study of topical medical-grade kanuka honey as a treatment for rosacea found
it to be an acceptable and potentially effective treatment.19The addition of 10% glycerine to
the honey has resulted in a product that is easier to apply to the skin. In this randomised
controlled trial we have investigated the efficacy of kanuka honey in the treatment of
rosacea. We designed the trial to overcome the recognised limitations of previous studies, in
particular to ensure that there was blinded investigator assessment of rosacea severity.6
Page 4 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 5
METHODS
This parallel group randomised controlled trial with assessor blinding was undertaken at a
hospital-based research facility and 4 community-based research and / or primary care sites
in New Zealand. Ethics approval was obtained from the Central Health and Disability Ethics
Committee (13/CEN/118). Adults aged 16 or over with a doctor’s diagnosis of rosacea on the
face, and a baseline blinded Investigator Global Assessment of Rosacea Severity Score
(IGA-RSS) of facial rosacea of ≥2 were recruited. The IGA-RSS is a 7-point scale (from 0:
‘clear’, to 6: ‘severe’) that provides an integrated assessment of rosacea severity based on
the principal facial signs of papules/pustules, inflammatory lesions, erythema and
telangiectasia5 (Supplement Table S1). Subjects were identified at the time of first
presentation or, with their primary care practitioner’s consent, from pre-existing databases,
or by public advertisement.
Exclusion criteria included current requirement for systemic corticosteroids, or systemic
corticosteroid treatment in the 4 weeks prior to Visit 1, current requirement for oral or topical
antibiotic therapy for rosacea, current requirement for topical corticosteroid treatment for
rosacea, known or suspected allergy to honey, or Cetomacrogol control cream, or any other
condition which, at the investigators discretion, it was believed may present a safety risk or
impact the feasibility of the study or the study results.
Participants attended for 3 visits (Supplement Table S2). Visit 1 (week 0) consisted of
consent, baseline assessments (the IGA-RSS), a participant-rated rosacea severity visual
analogue score (VAS–S) on a 100mm scale (0mm being ‘mildest possible’ symptoms and
100mm being ‘worst possible’ symptoms), and a participant-rated dermatology quality of life
index (DLQI)20, followed by randomisation to Honevo® or Cetomacrogol cream (control). At
Visit 2 (week 2) and Visit 3 (week 8), as well as the IGA-RSS and the DLQI, participants
completed a subjective rosacea ‘change in severity’ visual analogue scale (VAS-CS) on a
Page 5 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 6
100mm scale (0mm being ‘much worse’ and 100mm being ‘much improved’). Subjects’
diaries were used throughout the study to capture each participant’s weekly subjective VAS-
S, their use of randomised treatment throughout the 8 week study period, and any general
comments including adverse events throughout the study.
Randomisation and blinding
Treatment allocation was randomised using a computer generated sequence concealed to
investigators by enclosing the proposed treatment arm in an opaque envelope that was only
opened by primary investigators after informed consent was obtained by each participant.
Subjects were randomised in a 1:1 ratio to the topical application of Honevo® or control
cream. Due to the nature of Honevo® it was not possible to blind the participants and
primary investigators to the treatment allocation. An independent investigator at each site
remained blinded to the treatment allocation throughout the study to perform the blinded
IGA. The blinded investigator undertook only the IGA-RSS assessment for this study, and
was not involved in any other study procedures. Participants were instructed not to
communicate with the blinded investigator during the assessments.
Randomised treatments
The Investigational Product was topical medical grade Kanuka honey with 10% glycerine
content (Honevo®). The control cream was Cetomacrogol, a liquid paraffin and white soft
paraffin topical emollient.21,22 The participants were instructed to apply an appropriate
amount of cream to the affected area twice daily for 30-60 minutes per application, for eight
weeks, and to remove the treatment with warm water as desired. Subjects were asked not
to use any additional treatment for their rosacea for the duration of the study, as per the
exclusion criteria.
Outcome measures
Page 6 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 7
The primary outcome measure was the proportion of subjects who had a ≥2 improvement
(reduction) in the IGA-RSS at week 8 (designated ‘responders’). This measure represents a
clinically meaningful improvement in rosacea severity. The secondary outcome measures
included the change from baseline in IGA-RSS at week 2 and week 8; the participant-rated
VAS-CS at weeks 2 and 8; the change from baseline in participant-rated VAS-S at week 2
and week 8; the weekly diary-documented Rosacea severity VAS-S from participant diaries;
the change from baseline in the participant-rated DLQI20 at weeks 2 and 8; withdrawals due
to worsening of Rosacea; adverse events; and the daily self-reported use of Honevo®
(applications per day). Data for all participants was included for analysis up until the time the
participant withdrew from the study or became ineligible due to the use of prohibited
medications.
Sample size and study power
We anticipated the proportion of participants in the control group who respond with a ≥2
reduction in blinded IGA would be between 25 and 50%.6 A total of 124 participants (62 in
each group) has 80% power at 5% significance to detect a 25% response rate in the control
group and a 50% response rate in the Honevo® group. We recruited 138 participants to
allow for a 10% drop-out rate.
Statistical methods
The study was analysed by an intention to treat, with the participants who withdrew
considered to be non-responders. The pre-specified statistical analysis was logistic
regression for the difference in proportions with response.
Relative risks for a ≥2 point change in IGA-RSS at week 8 from baseline and for total study
withdrawal were calculated, with P values using Fishers exact test. Odds ratios were also
calculated from logistic regression
Page 7 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 8
For the Likert scaled variables the Wilcoxon test and Hodges-Lehman estimator of location
shift for the difference between treatments were used. DLQI and VAS variables were
analysed by ANCOVA with the baseline value as a continuous covariate and the
randomisation as the main predictor variable. The estimates for these analyses are
interpreted as the difference between randomised groups adjusted for baseline.
Applications per day was analysed by ANOVA with the response variable the mean average
number of applications per day, predictor variable randomisation group, and using the
number of days in the trial as a weight, to account for variations in the number of days of
application.
In a post-hoc analysis, the proportion of participants in whom the IGA-RSS was zero (clear
of rosacea) at week 8 was calculated.
SAS version 9.3 was used.
Page 8 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 9
RESULTS
The flow of participants in the study is shown in Figure 1. There were 69 subjects
randomised to control and 69 to Honevo®. One Honevo® participant was subsequently
excluded due to the use of a prohibited medication on enrolment, and their data was not
used in the consequent analysis. The characteristics of the participants are shown in Table
1. Participants were predominantly aged between 50 and 70, and had had rosacea for a
mean of 15 years. 19% of participants in each group had previously used oral antibiotics for
rosacea, while 44% and 38% had previously used any topical treatments for rosacea in the
Honevo® and control group respectively. There were 7/68 (10.3%) withdrawals in the
Honevo® group (3 worsening rosacea, 2 took prohibited medications, 2 for other reasons
unrelated to the study) and 15/69 (21.7%) withdrawals in the control group (8 worsening
rosacea, 2 took prohibited medications, 1 did not want to take the control medication, 1
found the study inconvenient and 3 for reasons unrelated to the study).
Primary outcome
There were 24/68 (34.3%) in the Honevo® group and 12/69 (17.4%) in the control group
who had a ≥2 improvement in IGA-RSS at week 8 compared to baseline (relative risk 2.03
(95% CI 1.11 to 3.72), P=0.020. The corresponding odds ratio was 2.59 (1.17 to 5.74).
Secondary outcomes
The change from baseline in IGA-RSS for participants who did not withdraw is shown in
Table 2, Supplement Table S3 and Figure 2.The change in IGA-RSS for Honevo®
compared to control at week 2 minus baseline was -1 (Hodges-Lehman estimate, 95% CI -1
to 0, P=0.03), and at week 8 minus baseline was -1 (Hodges-Lehman estimate, 95% CI -1 to
0, P=0.005),(Table 3). The subject-rated VAS-CS at week 2 was 9.1 (CI 3.5 to 14.7),
P=0.002, and at week 8 was 12.3 (CI 5.7 to 18.9), P<0.001for Honevo® compared to
control, representing greater improvement with Honevo®. There was no significant
Page 9 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 10
difference in diary-captured VAS-S, adjusted for baseline, at any of the time points between
week 2 and 8 (Supplement Table S4).There was no significant difference in the participant-
rated DLQI adjusted for baseline at week 2 (-0.3, CI-1.1 to 0.6, P=0.51) or week 8 (-0.01, CI
-0.7 to 0.7,P=0.97).
The number of applications per day between the randomised treatments was similar (mean
(SD) 1.84(0.23) vs 1.86(0.20) for the Honevo® and control groups respectively, difference: -
0.02 (95% CI -0.10 to 0.05), P=0.55).
In a post hoc analysis, the proportion of participants in whom the IGA-RSS score at week 8
was zero, (i.e. full resolution of rosacea) was 9/68 (13.2%) and 2/69 (2.9%) in the Honevo®
and control groups respectively, relative risk 4.6 (95%CI 1.0 to 20.4, P=0.031).
In the Honevo® group 23 participants reported 31 adverse events; 17 rosacea related, (3 of
which resulted in withdrawal of the participants), and 14 unrelated to rosacea (Supplement
Table S5). In the control group, 27 participants reported 36 adverse events; 22 rosacea
related, (8 of which resulted in withdrawal of participants), and 14 unrelated to rosacea.
Page 10 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 11
DISCUSSION
This randomised controlled trial has demonstrated that topical 90% medical grade kanuka
honey and 10% glycerine (Honevo®) is an effective and well tolerated treatment for rosacea.
About one third of participants had a clinically significant improvement in the IGA-RSS after
8 weeks of Honevo® treatment, two-fold greater than that observed with the control
treatment. We recommend consideration of the use of kanuka honey as a treatment for
rosacea.
There are a number of methodological issues that are important in the consideration of the
study findings. There are no standard validated tools for assessing the severity of rosacea,
which is inherently difficult due to its varied clinical characteristics. The priority with this study
of a honey product was to reduce potential bias by blinding of clinical assessments where
possible, as the participant could not be blinded due to the appearance and smell of
Honevo®. It was for this reason we chose to use the 7 point IGA-RSS representing a global
assessment of rosacea severity that was undertaken by an investigator who was blinded to
treatment.
The primary outcome variable identified the proportion in each treatment arm who had a 2
point reduction or more in IGA-RSS, representing a clinically meaningful improvement in
rosacea severity, for example a change from ‘severe’ to ‘moderate’, or from ‘moderate’ to
‘mild’. 34% of those who were randomised to Honevo® had an IGA-RSS improvement of 2
or more at 8 weeks compared to 17% of the placebo group, and 13% achieved full resolution
of rosacea compared to 3% in the placebo group. The estimate of the location shift for the
difference between the treatments was -1, (95% CI -1 to 0) at both week 2 and week 8 and
the estimated change in IGA-RSS at week 8 adjusted for baseline was -0.6 (95% CI -1.1 to -
0.2). These findings reflect the variability in response to Honevo®, perhaps dependent on
sub-types of rosacea2 which were not assessed in this study.
Page 11 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 12
In addition, we assessed patient-reported outcomes, based on participant’s assessment of
current severity of symptoms (VAS-S), participant’s perceived change in severity (VAS-CS)
and the DLQI questionnaire, to provide a comprehensive assessment of efficacy. The VAS-
CS at the 2-week and 8-week clinic visits were significantly better with Honevo®. However,
there was no difference with the 2-week and 8-week DLQI assessments or the weekly diary
VAS-S measures. In the absence of a validated VAS for rosacea severity, it is difficult to
comment on the clinical relevance of a reduction of 11 points from baseline in the VAS-S or
the 12.3 improvement in VAS-CS in the Honevo® group compared to the control group after
8 weeks. As these outcomes were participant assessed and participants could not be
blinded to the interventions, there is a risk of detection bias in this methodology. The DLQI is
a questionnaire non-specific to rosacea and may not have been sensitive enough to capture
changes associated with this condition alone. The greater number of withdrawals due to
worsening rosacea in the control group (12% vs 4%), is likely to have led to an under-
estimation of the efficacy of Honevo®, as these participants did not undergo assessment of
the secondary outcome variables following withdrawal.
Cetomacrogol cream was chosen as a comparator as it is a non-ionic moisturising cream,
often used as a vehicle for delivery of topical medications. The treatment was administered
for 8 weeks to allow both the speed of onset and the duration of effect to be assessed. This
identified that honey had efficacy within 2 weeks of treatment, with further efficacy obtained
during the 8 week treatment period. Adverse event data did not allow us to reliably ascertain
whether the rosacea specific adverse events such as burning, itching, peeling, stinging, dry
skin and pain were associated only with the application of the investigational medicine or
whether they were ongoing rosacea symptoms. However it was reassuring that the number
of participants with rosacea specific adverse events was similar between Honevo® and the
paraffin-based emollient control cream.
Page 12 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 13
Notwithstanding the limitations of comparing different primary outcome variables utilised in
other studies of rosacea, it is interesting to note the findings from placebo-controlled studies
of topical metronidazole or azelaic acid, two of the more commonly used treatments of
rosacea.4-7 In studies of topical metronidazole the relative risk of improvement with the
physician’s global evaluation of improvement was 1.95 (95% CI 1.5 to 2.6), and in studies of
azelaic cream the relative risk of participant-assessed improvement was 1.52 (95% CI 1.3 to
1.8)6,23. In our study, the relative risk of IGA-RSS improvement with Honevo® was 2.0
(95%CI 1.1 to 3.7) and in the post hoc analysis the relative risk of resolution was 4.6 (95%CI
1.0 to 20.4). Given the apparent superiority of all three treatments compared to placebo,
randomised controlled trials comparing Honevo® with topical metronidazole or azelaic
cream are now indicated.
The mechanism of action was not assessed in this study, however there a number of
potential mechanisms relevant to the efficacy demonstrated with kanuka honey in this study.
Firstly kanuka honey has a number of different anti-inflammatory effects, including inhibition
of neutrophil superoxide production,13 reduction in inflammatory leucocyte infiltration and
arachidonic- induced oedema,13 and stimulation of macrophage release of tumour necrosis
factor a (TNFa),15 a cytokine with a crucial role in wound healing.24,254 These properties may
be relevant as rosacea is a chronic inflammatory disorder, characterised by inflammatory cell
infiltration, vascular dilatation and tissue oedema.1,3,6 In addition, kanuka honey has high
antibacterial activities against a wide range of bacteria, including Bacillus subtilis,
Propionibacterium acne and Staph Aureus,11,12,14 properties which may be beneficial in view
of the proposed role of Bacillus oleronius in the inflammatory response in rosacea. The
effect of honey on Bacillus oleronius and the Demodex folliculum mite require further
investigation.
In conclusion, this randomised controlled trial has demonstrated the clinical efficacy and
tolerability of 90% medical grade kanuka honey and 10% glycerine (Honevo®) in the
Page 13 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 14
treatment of rosacea. Honevo® can be recommended for the treatment of rosacea;
however, further randomised controlled trials comparing Honevo® with topical metronidazole
and azelaic acid are now required to determine its relative efficacy and side effect profile
compared to these agents.
Page 14 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 15
STATEMENTS
Corresponding Author Statement: The Corresponding Author has the right to grant on
behalf of all authors and does grant on behalf of all authors, an exclusive licence on a
worldwide basis to the BMJ Publishing Group Ltd to permit this article (if accepted) to be
published in BMJ editions and any other BMJPGL products and sublicences such use and
exploit all subsidiary rights, as set out in our licence.
Competing interest statement: All authors have completed the Unified Competing Interest
form atwww.icmje.org/coi_disclosure.pdf (available on request from the corresponding
author) and declare: HoneyLab Ltd provided funding to undertake this study and provided
the product Honevo® for the purpose of the study; Dr Shaun Holt, the Medical Director of
HoneyLab Ltd was previously the Programme Director of Complementary Medicine at the
Medical Research Institute of New Zealand. There are no other competing interests to
declare.
Role of the funding source: HoneyLab was consulted in the design of the study and
preparation of the report, but had no involvement in the collection, analysis and interpretation
of the data, or decision to submit for publication.
Contributorship statement: Study concept and design: JF, JK, MH, MW, RB. Acquisition of
Data: IB, AH, JR, AC, CH, DS, CT, BM. Drafting of the manuscript: RB, IB, MW. Critical
revision of the manuscript for important intellectual content: all authors. Statistical analysis:
MW. Administrative, technical and material support: All authors. Study supervision: MH.
Guarantor: Dr I Braithwaite had access to all the data on the study and takes responsibility
for the integrity of the data and accuracy of the data analysis.
Transparency declaration: The lead author affirms that the manuscript is an honest,
accurate, and transparent account of the study being reported; that no important aspects of
the study have been omitted; and that any discrepancies from the study as planned (and, if
relevant, registered) have been explained
Data sharing statement: Patient level data available from the corresponding author.
Consent was not obtained from participants for data sharing, but the presented data are
anonymised and the risk of identification is low. Data may be obtained by contacting the
corresponding author.
Page 15 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 16
Table 1: Baseline characteristics of participants
Mean (SD) Median (IQR) Min to Max
Age at enrolment
Honevo® N-68 57.7 (13.7) 58.2 (46.7 to 68.3) 23.4 to 86.5
Control N=69 58.9 (15.9) 60.1 (49.0 to 68.6) 18.2 to 90.1
All N=137 58.3 (14.8) 58.9 (48.1 to 68.6) 18.2 to 90.1
Age at Diagnosis
Honevo® N=64 42.2 (15.4) 40 (30 to 51.5) 19 to 80
Control N=67 43.6 (15.4) 43 (35 to 55) 10 to 79
All N=131 42.9 (15.4) 41 (32 to 54) 10 to 80
Honevo® N (%) N=68
Control N (%) N=69
Female 32 (47.1) 36 (52.2)
History of oral antibiotics 13 (19.1) 13 (18.8)
History of topical therapy 24 (35.3) 20 (29.0)
History of topical steroid 6 (8.8) 6 (8.7)
European 64 (94.1) 68 (98.6)
Maori 4 (5.9) 0 (0)
Asian 0 (0) 1 (1.5)
SD – standard deviation IQR – inter quartile range
Page 16 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 17
Table 2: Contingency table of blinded Investigator Global Assessment of Rosacea
Severity Score (IGA-RSS) week 8 change from baseline by randomisation in the
subjects who completed the study
Change from baseline Honevo® N/61 (%) Control N/54 (%)
-3 11 (18.0) 1 (1.9)
-2 13 (21.3) 11 (20.4)
-1 20 (32.8) 17 (31.5)
0 14 (23.0) 15 (27.8)
1 3 (4.9) 8 (14.8)
2 0 (0) 2 (3.7)
IGA-RSS: blinded Investigator Global Assessment of Rosacea Severity Score based on a 7 point scale (0 ‘clear’ to 6 ‘severe’
Page 17 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 18
Table 3: Clinic-based secondary outcome variables (all Honevo® minus control)
Comparison N with data Hodges-Lehman
estimate (95% CI) P
Honevo® Control
IGA-RSS week 2 66 66 0 (-1 to 0) 0.26
IGA-RSS week 8 61 54 0 (-1 to 0) 0.06
IGA-RSS week 2 minus baseline 66 66 -1 (-1 to 0) 0.03
IGA-RSS week 8 minus baseline 61 54 -1 (-1 to 0) 0.005
Estimate (95% CI) P
IGA-RSS week 8 adjusted for baseline1
61 54 -0.6 (-1.1 to -0.2) 0.003
Mean difference (95% CI)
P
VAS-CS week 2 66 66 9.1 (3.5 to 14.7) 0.002
VAS-CS week 8 61 54 12.3 (5.7 to 18.9) <0.001
VAS-S week 2 66 66 -3.6 (-9.9 to 2.7) 0.26
VAS-S week 2 minus baseline 66 66 -2.9 (-9.2 to 3.5) 0.38
VAS-S week 8 61 54 -4.5 (-11.6 to 2.6) 0.21
VAS-S week 8 minus baseline 61 54 -11.0 (-18.0 to -3.9) 0.003
IGA-RSS: blinded Investigator Global Assessment of Rosacea Severity Score, based on a 7 point scale (0 ‘clear’ to 6 ‘severe’) VAS-CS: Participant-rated assessment of Change in Severity of rosacea based on a 100mm VAS scale (0mm ‘much worse’ to 100mm ‘much improved’) VAS-S: Participant-rated assessment of Severity of rosacea based on a 100mm VAS scale (0mm ‘mildest possible’ symptoms and 100mm ‘worst possible’ symptoms) ANOVA with baseline reading as a covariate, normality assumptions not well met
Page 18 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 19
FIGURE LEGENDS
Figure 1: Flow of participants through trial.
Figure 2: The difference from baseline in IGA-RSS at week 8 for control and Honevo®.
Horizontal lines are the 25%, median and 75% quantiles, the symbol is the mean and
the whiskers go from maximum to minimum.
Page 19 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 20
REFERENCES
1. Buechner SA. Rosacea: an update. Dermatology. 2005;210(2):100-8. 2. Wilkin J, Dahl M, Detmar M, Drake L, Liang M, Odom R et al. Standard grading system for rosacea: Report of the National Rosacea Society Expert Committee on the classification and staging of rosacea. J Am Acad Dermatol 2004;50:907-12. 3. Berg M, Liden S. An epidemiological study of rosacea. Acta Derm Venereol. 1989;69(5):419-23. 4. Powell FC. Clinical practice. Rosacea. N Engl J Med. 2005 Feb 24;352(8):793-803. 5. Elewski BE, Fleischer AB, Jr., Pariser DM. A comparison of 15% azelaic acid gel and 0.75% metronidazole gel in the topical treatment of papulopustular rosacea: results of a randomized trial. Arch Dermatol. 2003 Nov;139(11):1444-50. 6. van Zuuren EJ, Kramer S, Carter B, Graber MA, Fedorowicz Z. Interventions for rosacea. Cochrane Database Syst Rev. (3):CD003262. 7. Elewski BE. Rosacea trial comparing twice-daily azelaic acid gel 15% with once-daily metronidazole gel 1%. Cutis. 2007 Jan;79(1):57-8; author reply 8. 8. World Health O. Antimicrobial resistance: global report on surveillance 2014; 2014. Report No.: ISBN: 978 92 4 156474 8 Contract No.: Document Number|. 9. Costelloe C, Metcalfe C, Lovering A, Mant D, Hay AD. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ.340:c2096. 10. Department of Health UKSMAC. The path of least resistance. 1998. 11. Wu Q. Antimicrobial effect of Manuka honey and Kanuka honey alone and in combination with the bioactives against the growth of Propionibacterium acnes ATCC 6919: a thesissubmitted in partial fulfilment of the requirements for the degree Master of Food Technology, Massey University, Albany, New Zealand; 2011. 12. Lu J, Carter DA, Turnbull L, Rosendale D, Hedderley D, Stephens J, et al. The effect of New Zealand kanuka, manuka and clover honeys on bacterial growth dynamics and cellular morphology varies according to the species. PLoS One.8(2):e55898. 13. Leong AG, Herst PM, Harper JL. Indigenous New Zealand honeys exhibit multiple anti-inflammatory activities. Innate Immun. Jun;18(3):459-66. 14. Allen KL, Molan PC, Reid GM. A survey of the antibacterial activity of some New Zealand honeys. J Pharm Pharmacol. 1991 Dec;43(12):817-22. 15. Gannabathula S, Skinner MA, Rosendale D, Greenwood JM, Mutukumira AN, Steinhorn G, et al. Arabinogalactan proteins contribute to the immunostimulatory properties of New Zealand honeys. Immunopharmacol Immunotoxicol. Aug;34(4):598-607. 16. Lacey N, Delaney S, Kavanagh K, Powell FC. Mite-related bacterial antigens stimulate inflammatory cells in rosacea. Br J Dermatol. 2007 Sep;157(3):474-81. 17. Bonnar E, Eustace P, Powell FC. The Demodex mite population in rosacea. J Am Acad Dermatol. 1993 Mar;28(3):443-8. 18. Yamasaki K, Di Nardo A, Bardan A, Murakami M, Ohtake T, Coda A, et al. Increased serine protease activity and cathelicidin promotes skin inflammation in rosacea. Nat Med. 2007 Aug;13(8):975-80. 19. Fingleton JS, D. Cave, N. Brinded, A. Weatherall, M. Perrin, K. Beasley,R. Topical kanuka honey for the treatment of rosacea. Focus on Alternative and Complementary Therapies. 2013;18(4):221-2. 20. Lewis V, Finlay AY. 10 years experience of the Dermatology Life Quality Index (DLQI). J Investig Dermatol Symp Proc. 2004 Mar;9(2):169-80. 21. (Datapharm) ew. Cetomacrogol Cream BP 1988 Formula A. https://wwwmedicinesorguk/emc/medicine/25140. Last accessed Dec 24,2014. 22. Kingdom NNHSU. Cetomacrogol Cream Formula A. http://wwwnhsuk/medicine-guides/pages/MedicineOverviewaspx?medicine=Cetomacrogol%20Cream%20Formula%20A. Last accessed Dec 24, 2014.
Page 20 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 21
23. van Zuuren EJ, Kramer SF, Carter BR, Graber MA, Fedorowicz Z. Effective and evidence-based management strategies for rosacea: summary of a Cochrane systematic review. Br J Dermatol. Oct;165(4):760-81. 24. Fu X, Tian H, Hsu S, Wang D, Sheng Z. In vivo effects of tumor necrosis factor-alpha on incised wound and gunshot wound healing. J Trauma. 1996 Mar;40(3 Suppl):S140-3. 25. Mooney DP, O'Reilly M, Gamelli RL. Tumor necrosis factor and wound healing. Ann Surg. 1990 Feb;211(2):124-9.
Page 21 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
56x67mm (300 x 300 DPI)
Page 22 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
11x9mm (600 x 600 DPI)
Page 23 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Supplement Table S1: Blinded Investigator Global Assessment of Rosacea Severity Score (IGA-RSS)
Numerical Score
Definition Description
0 Clear Almost no Rosacea (i.e. no papules and/or pustules); no or residual erythema; mild to moderate degree of telangiectasia may be present
1 Minimal Rare papules and/or pustules; residual to mild erythema; mild to moderate degree of telangiectasia may be present
2 Mild Few papules and/or pustules; mild erythema; mild to moderate degree of telangiectasia may be present
3 Mild to moderate Distinct number of papules and/or pustules; mild to moderate erythema; mild to moderate degree of telangiectasia may be present
4 Moderate Pronounced number of papules and/or pustules; moderate erythema; mild to moderate degree of telangiectasia may be present
5 Moderate to Severe
Many papules and/or pustules, occasionally with large inflamed lesions; moderate erythema; moderate degree of telangiectasia may be present
6 Severe Numerous papules and/or pustules, occasionally with confluent areas of inflamed lesions; moderate to severe erythema; moderate to severe degree of telangiectasia may be present
Page 24 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Supplement Table S2: Schedule of Assessments
Visit Number Visit 1 Visit 2 Visit 3
Time Point Week 0 Day 1
Week 2 Day 15
Week 8 Day 57
Informed Consent X
Eligibility criteria checked X
Demographics and medical history X
Randomisation X
Administer DLQI X X X
Administer IGA X X X
Participant-rated severity VAS-S completiona X X X
Participant-rated change VAS-CS severity completion
X X
Provision of participant diary X X
Collection of participant diary X X
Safety monitoring X X X
DLQI: Dermatology Life Quality Index
IGA-RSS blinded Investigator Global Assessment of Rosacea Severity Score VAS-S: Participant-rated assessment of severity of rosacea VAS-CS: Participant-rated assessment of change in severity of rosacea a VAS-S to be completed weekly from Visit 1 until Visit 3, within the subject diary
Page 25 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Supplement Table S3: Clinic-based secondary outcome variables
Mean (SD) Median (IQR) Min to Max
IGA-RSS week Zero
Control N=69 3 (0.9) 3 (2 to 4) 2 to 5 Honevo® N=68 3 (0.9) 3 (2 to 3.5) 2 to 6
IGA-RSS week 2
Control N=66 2.5 (1.4) 2 (2 to 3) 0 to 6 Honevo® N=66 2.2 (1.2) 2 (1 to 3) 0 to 6
IGA-RSS week 8
Control N=54 2.4 (1.3) 2 (1 to 3) 0 to 6 Honevo® N=61 1.8 (1.2) 2 (1 to 3) 0 to 5
Difference IGA-RSS week 2 to week Zero Control N=66 -0.5 (0.9) 0 (-1 to 0) -3 to 1 Honevo® N=66 -0.8 (1.0) -1 (-2 to 0) -3 to 2
Difference IGA-RSS week 8 to week Zero
Control N=54 -0.6 (1.1) 0 (-1 to 0) -3 to 2 Honevo® N=61 -1.2 (1.1) -1 (-2 to 0) -3 to 1
VAS-CS week 2
Control N=66 50.1 (16.6) 51 (47 to 55) 0 to 89 Honevo® N=66 59.2 (16.1) 59 (50 to 71) 21 to 98
VAS-CS week 8
Control N=54 55.2 (18.2) 51 (48 to 61) 15 to 98 Honevo® N=61 67.6 (17.4) 69 (52 to 79) 25 to 99
VAS-S week Zero
Control N=69 32.0 (19.1) 28 (18 to 44) 1 to 87 Honevo® N=68 36.8 (21.2) 31.5 (21 to 54) 1 to 78
VAS-S week 2
Control N=66 34.9 (19.6) 32.5 (21 to 50) 1 to 84 Honevo® N=66 31.2 (16.9) 29.5 (20 to 42) 1 to 68
VAS-S week 8
Control N=54 30.8 (19.2) 31 (13 to 46) 3 to 78 Honevo® N=61 26.3 (19.2) 24 (12 to 38) 2 to 96
Difference VAS-S week 2 to week Zero
Control N=66 3.0 (16.7) 0.5 (-6.0 to 8.0) -30 to 73 Honevo® N=66 -5.2 (16.1) -6 (-16 to 1) -37 to 38
Difference VAS-S week 8 to week Zero
Control N=54 2.1 (14.5) -1 (-9 to 11) -39 to 41 Honevo® N=61 -8.9 (22.4) -10(-24 to 9) -66 to 38
IGA-RSS: blinded Investigator Global Assessment of Rosacea Severity Score, based on a 7 point scale (0 ‘clear’ to 6 ‘severe’) VAS-CS: Participant-rated assessment of Change in Severity of rosacea based on a 100mm VAS scale (0mm ‘much worse’ to 100mm ‘much improved’) VAS-S: Participant-rated assessment of Severity of rosacea based on a 100mm VAS scale (0mm ‘mildest possible’ symptoms and 100mm ‘worst possible’ symptoms)
Page 26 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Supplement Table S4: Diary-based VAS-S adjusted for baseline
Honevo® minus Control N with data Estimate (95% CI) P
Honevo® Control
VAS-S week 2 52 50 -4.0 (-8.5 to 0.6) 0.088
VAS-S week 3 60 53 -1.3 (-6.8 to 4.2) 0.65
VAS-S week 4 59 54 -4.0 (-10.3 to 2.4) 0.21
VAS-S week 5 55 55 -2.0 (-7.8 to 3.9) 0.50
VAS-S week 6 56 50 -5.3 (-2.5 to 14.2) 0.13
VAS-S week 7 53 50 -2.1 (-8.9 to 4.7) 0.54
VAS-S week 8 48 38 -5.7 (-6.2 to 13.3) 0.15
VAS-S: Participant-rated assessment of Severity of rosacea based on a 100mm VAS scale (0mm ‘mildest possible’ symptoms and 100mm ‘worst possible’ symptoms)
Page 27 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Supplement Table S5: Adverse events reported in the Honevo® and Control groups.
Honevo® N
Control N
Rosacea related adverse events resulting in withdrawal
Worsening Rosacea 3 8
Rosacea related adverse events without withdrawal
Worsening Rosacea 0 2
Itching 5 1
Tingling 3 2
Red spots 2 0
Eczema 1 0
Dry skin 1 0
Peeling 1 0
Pain 1 0
Stinging 0 4
Burning 0 2
Blisters 0 1
Bleeding 0 1
Possible fungal skin infection 0 1
Non-rosacea related adverse events resulting in withdrawal
0 0
Non-rosacea related adverse events without withdrawal
Other skin problem 1 0
Infection 6 7
Trauma 3 1
Indigestion 1 0
Worsening Asthma 1 0
Headache / Migraine 1 2
Elevated PSA 1 0
Cardiovascular 0 2
Allergy / Hayfever 0 2
Note: Participants may report more than one adverse event
Page 28 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
CONSORT 2010 checklist Page 1
CONSORT 2010 checklist of information to include when reporting a randomised trial*
Section/Topic Item No Checklist item
Reported on page No
Title and abstract
1a Identification as a randomised trial in the title title
1b Structured summary of trial design, methods, results, and conclusions (for specific guidance see CONSORT for abstracts) 2
Introduction
Background and
objectives
2a Scientific background and explanation of rationale 4
2b Specific objectives or hypotheses 4
Methods
Trial design 3a Description of trial design (such as parallel, factorial) including allocation ratio 5
3b Important changes to methods after trial commencement (such as eligibility criteria), with reasons n/a
Participants 4a Eligibility criteria for participants 5
4b Settings and locations where the data were collected 5
Interventions 5 The interventions for each group with sufficient details to allow replication, including how and when they were
actually administered
6
Outcomes 6a Completely defined pre-specified primary and secondary outcome measures, including how and when they
were assessed
6-7
6b Any changes to trial outcomes after the trial commenced, with reasons n/a
Sample size 7a How sample size was determined 8
7b When applicable, explanation of any interim analyses and stopping guidelines n/a
Randomisation:
Sequence
generation
8a Method used to generate the random allocation sequence 6
8b Type of randomisation; details of any restriction (such as blocking and block size) 6
Allocation
concealment
mechanism
9 Mechanism used to implement the random allocation sequence (such as sequentially numbered containers),
describing any steps taken to conceal the sequence until interventions were assigned
6
Implementation 10 Who generated the random allocation sequence, who enrolled participants, and who assigned participants to
interventions
6
Blinding 11a If done, who was blinded after assignment to interventions (for example, participants, care providers, those 6
Page 29 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on December 5, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-007651 on 24 June 2015. Downloaded from

For peer review only
CONSORT 2010 checklist Page 2
assessing outcomes) and how
11b If relevant, description of the similarity of interventions n/a
Statistical methods 12a Statistical methods used to compare groups for primary and secondary outcomes 7
12b Methods for additional analyses, such as subgroup analyses and adjusted analyses 7
Results
Participant flow (a
diagram is strongly
recommended)
13a For each group, the numbers of participants who were randomly assigned, received intended treatment, and
were analysed for the primary outcome
9, fig 1
13b For each group, losses and exclusions after randomisation, together with reasons 9, fig 1
Recruitment 14a Dates defining the periods of recruitment and follow-up 5
14b Why the trial ended or was stopped n/a
Baseline data 15 A table showing baseline demographic and clinical characteristics for each group 15
Numbers analysed 16 For each group, number of participants (denominator) included in each analysis and whether the analysis was
by original assigned groups
9
Outcomes and
estimation
17a For each primary and secondary outcome, results for each group, and the estimated effect size and its
precision (such as 95% confidence interval)
9-10
17b For binary outcomes, presentation of both absolute and relative effect sizes is recommended 9-10
Ancillary analyses 18 Results of any other analyses performed, including subgroup analyses and adjusted analyses, distinguishing
pre-specified from exploratory
9-10
Harms 19 All important harms or unintended effects in each group (for specific guidance see CONSORT for harms) 10
Discussion
Limitations 20 Trial limitations, addressing sources of potential bias, imprecision, and, if relevant, multiplicity of analyses 11-12
Generalisability 21 Generalisability (external validity, applicability) of the trial findings 11-12
Interpretation 22 Interpretation consistent with results, balancing benefits and harms, and considering other relevant evidence 12-13
Other information
Registration 23 Registration number and name of trial registry abstract
Protocol 24 Where the full trial protocol can be accessed, if available uploaded
Funding 25 Sources of funding and other support (such as supply of drugs), role of funders title
*We strongly recommend reading this statement in conjunction with the CONSORT 2010 Explanation and Elaboration for important clarifications on all the items. If relevant, we also
recommend reading CONSORT extensions for cluster randomised trials, non-inferiority and equivalence trials, non-pharmacological treatments, herbal interventions, and pragmatic trials.
Additional extensions are forthcoming: for those and for up to date references relevant to this checklist, see www.consort-statement.org.
Page 30 of 30
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on December 5, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-007651 on 24 June 2015. Downloaded from

For peer review only
RANDOMISED CONTROLLED TRIAL OF TOPICAL KANUKA
HONEY FOR THE TREATMENT OF ROSACEA
Journal: BMJ Open
Manuscript ID: bmjopen-2015-007651.R2
Article Type: Research
Date Submitted by the Author: 04-May-2015
Complete List of Authors: Braithwaite, Irene; Medical Research Institute of New Zealand, Hunt, Anna; Medical Research Institute of New Zealand, Riley, Judith; Medical Research Institute of New Zealand, Fingleton, James; Medical Research Institute of New Zealand, Kocks, Janwillem; Medical Research Institute of New Zealand, Corin, Andrew; Clinical Horizons, Helm, Colin; Clinical Horizons, Sheehan, Davitt; Papamoa Pines Medical Centre,
Tofield, Chris; Cameron Medical Clinic, Montgomery, Barney; Optimal Clinical Trials, Holliday, Mark; Medical Research Institute of New Zealand, Weatherall, Mark; University of Otago Wellington, Beasley, Richard; Medical Research Institute of New Zealand,
<b>Primary Subject Heading</b>:
Complementary medicine
Secondary Subject Heading: Complementary medicine, Dermatology, Infectious diseases
Keywords: Rosacea, Kanuka honey, randomised controlled trial
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on D
ecember 5, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-007651 on 24 June 2015. D
ownloaded from

For peer review only
Page 1
RANDOMISED CONTROLLED TRIAL OF TOPICAL KANUKA HONEY FOR THE
TREATMENT OF ROSACEA
Irene Braithwaite1, Anna Hunt1, Judith Riley1, James Fingleton1, Janwillem Kocks1
Andrew Corin2, Colin Helm2 Davitt Sheahan3, Christopher Tofield4, Barney Montgomery5,
Mark Holliday1, Mark Weatherall6, Richard Beasley1
1Medical Research Institute of New Zealand, Wellington, New Zealand, 2 Clinical Horizons,
Tauranga, New Zealand, 3 Papamoa Pines Medical Centre, Tauranga, New Zealand, 4
Cameron Medical Clinic, Tauranga, New Zealand, 5 Optimal Clinical Trials, , Auckland, New
Zealand, 6University of Otago, Wellington
Word count: (Abstract 298), manuscript 3,026
Key words: Rosacea, kanuka honey, randomised controlled trial
Funding: This study was funded by HoneyLab. HoneyLab provided the Honevo® (medical grade kanuka honey and 10% glycerine) for the study.
Contact: Dr Irene Braithwaite Medical Research Institute of New Zealand Private Bag 7902, Wellington 6242, New Zealand Telephone: +64-4-805 0233 Fax: +64-4-389 5707 Email:[email protected]
Page 1 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 2
ABSTRACT (298 words including registration statement)
Objective: To investigate the efficacy of topical 90% medical grade kanuka honey and 10%
glycerine (Honevo®) as a treatment for rosacea.
Design: Randomised controlled trial with blinded assessment of primary outcome variable.
Setting: Outpatient primary healthcare population from 5 New Zealand sites.
Participants: 138 adults aged ≥16, with a diagnosis of rosacea, and a baseline blinded
Investigator Global Assessment of Rosacea Severity Score (IGA-RSS) of ≥2. 69 participants
were randomised to each treatment arm. One participant was excluded from the Honevo®
group, and 7 and 15 participants withdrew from the Honevo® and control groups
respectively.
Interventions: Participants were randomly allocated 1:1 to Honevo® or control cream
(cetomacrogol), applied twice daily for 8 weeks.
Main outcome measures: The primary outcome measure was the proportion of subjects
who had a ≥ 2 improvement in the 7-point IGA-RSS at week 8 compared to baseline.
Secondary outcomes included change in IGA-RSS and subject-rated visual analogue score
of change in severity (VAS-CS) on a 100mm scale (0mm ‘much worse’, 100mm ‘much
improved’) at weeks 2 and 8.
Results: 24/68 (34.3%) in the Honevo® group and 12/69 (17.4%) in the control group had a
≥ 2 improvement in IGA-RSS at week 8 compared to baseline (relative risk 2.03; 95% CI
1.11 to 3.72, P=0.020). The change in IGA-RSS for Honevo® compared to control at week 2
minus baseline was -1 (Hodges-Lehman estimate, 95%CI -1 to 0, P=0.03), and at week 8
minus baseline was -1 (Hodges-Lehman estimate, 95%CI -1 to 0, P=0.005). The VAS-CS at
week 2 was 9.1 (95%CI 3.5 to 14.7), P=0.002, and at week 8 was 12.3 (95%CI 5.7 to 18.9)¸
P<0.001 for Honevo® compared to control.
Conclusion: Honevo® is an effective treatment for rosacea.
Trial registration: This trial was registered in the Australian and New Zealand Clinical Trials
Registry ACTRN12614000004662
Page 2 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 3
WHAT IS KNOWN ABOUT THE TOPIC?
Honey is a potential topical treatment for rosacea as it has antimicrobial and anti-
inflammatory effects. A recent pilot study has demonstrated that medical grade (sterilised
and filtered), kanuka honey is an acceptable and potentially effective treatment for rosacea
WHAT THIS STUDY ADDS
Our study has shown that Honevo® is an effective treatment for rosacea, with clinical
efficacy observed within 2 weeks of treatment.
STRENGTHS AND LIMITATIONS
• This is a randomised placebo-controlled trial of 8 weeks of treatment for rosacea with
either topical 90% medical-grade kanuka honey and 10% glycerine cream
(Honevo®) or a non-ionic paraffin based cream (cetomacragol).
• Due to the nature of the products being assessed, participants were not able to be
blinded to the treatment arms
• The primary outcome variable for this study (Investigator Global Assessment of
Rosacea Severity Score) was assessed by investigators who were blinded to
randomisation throughout the trial.
Page 3 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 4
INTRODUCTION
Rosacea is a common chronic inflammatory skin condition which primarily affects the face,
and occurs in up to 10% of the adult population.[1-4] There is no cure, and affected
individuals may experience substantial morbidity. There is a range of treatment options,
including several topical and oral antibiotics, however these are only partially effective and
side effects may limit their use [4-7] Also there are global concerns about the increasing
rates of antibiotic resistance resulting from the widespread use of antibiotics, particularly with
long term use in chronic conditions.[8,9] For example, the United Kingdom Standing Medical
Advisory Committee now recommends the fewest number of antibiotic courses should be
prescribed for the shortest period possible.[10]
Amongst the alternative therapies to antibiotics, medical grade kanuka honey is of interest
due to its potent antibacterial and anti-inflammatory activities.[11-15] The pathophysiological
rationale underlying its use is that rosacea is an inflammatory disorder, and that antigenic
proteins related to the bacterium Bacillus oleronius isolated from the Demodex folliculorum
mite, which infests the skin in rosacea, exacerbates this inflammatory response.[16,17]
Furthermore, people with rosacea express abnormally high levels of the antimicrobial
peptide cathelicidin, which promotes the inflammatory response in rosacea.[18]
A recent pilot study of topical medical-grade kanuka honey as a treatment for rosacea found
it to be an acceptable and potentially effective treatment.[19] The addition of 10% glycerine
to the honey has resulted in a product that is easier to apply to the skin. In this randomised
controlled trial we have investigated the efficacy of kanuka honey in the treatment of
rosacea. We designed the trial to overcome the recognised limitations of previous studies, in
particular to ensure that there was blinded investigator assessment of rosacea severity.[6]
Page 4 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 5
METHODS
This parallel group randomised controlled trial with assessor blinding was undertaken at a
hospital-based research facility and 4 community-based research and / or primary care sites
in New Zealand. Ethics approval was obtained from the Central Health and Disability Ethics
Committee (13/CEN/118). Adults aged 16 or over with a doctor’s diagnosis of rosacea on the
face, and a baseline blinded Investigator Global Assessment of Rosacea Severity Score
(IGA-RSS) of facial rosacea of ≥2 were recruited. The IGA-RSS is a 7-point scale (from 0:
‘clear’, to 6: ‘severe’) that provides an integrated assessment of rosacea severity based on
the principal facial signs of papules/pustules, inflammatory lesions, erythema and
telangiectasia [5] (Supplement Table S1). Subjects were identified at the time of first
presentation or, with their primary care practitioner’s consent, from pre-existing databases,
or by public advertisement.
Exclusion criteria included current requirement for systemic corticosteroids, or systemic
corticosteroid treatment in the 4 weeks prior to Visit 1, current requirement for oral or topical
antibiotic therapy for rosacea, current requirement for topical corticosteroid treatment for
rosacea, known or suspected allergy to honey, or Cetomacrogol control cream, or any other
condition which, at the investigators discretion, it was believed may present a safety risk or
impact the feasibility of the study or the study results.
Participants attended for 3 visits (Supplement Table S2). Visit 1 (week 0) consisted of
consent, baseline assessments (the IGA-RSS), a participant-rated rosacea severity visual
analogue score (VAS–S) on a 100mm scale (0mm being ‘mildest possible’ symptoms and
100mm being ‘worst possible’ symptoms), and a participant-rated dermatology quality of life
index (DLQI) [20], followed by randomisation to Honevo® or Cetomacrogol cream (control).
At Visit 2 (week 2) and Visit 3 (week 8), as well as the IGA-RSS and the DLQI, participants
completed a subjective rosacea ‘change in severity’ visual analogue scale (VAS-CS) on a
Page 5 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 6
100mm scale (0mm being ‘much worse’ and 100mm being ‘much improved’). Subjects’
diaries were used throughout the study to capture each participant’s weekly subjective VAS-
S, their use of randomised treatment throughout the 8 week study period, and any general
comments including adverse events throughout the study.
Randomisation and blinding
Treatment allocation was randomised using a computer generated sequence concealed to
investigators by enclosing the proposed treatment arm in an opaque envelope that was only
opened by primary investigators after informed consent was obtained by each participant.
Subjects were randomised in a 1:1 ratio to the topical application of Honevo® or control
cream. Due to the nature of Honevo® it was not possible to blind the participants and
primary investigators to the treatment allocation. An independent investigator at each site
remained blinded to the treatment allocation throughout the study to perform the blinded
IGA. The blinded investigator undertook only the IGA-RSS assessment for this study, and
was not involved in any other study procedures. Participants were instructed not to
communicate with the blinded investigator during the assessments.
Randomised treatments
The Investigational Product was topical medical grade Kanuka honey with 10% glycerine
content (Honevo®). The control cream was Cetomacrogol, a liquid paraffin and white soft
paraffin topical emollient.[21,22] The participants were instructed to apply an appropriate
amount of cream to the affected area twice daily for 30-60 minutes per application, for eight
weeks, and to remove the treatment with warm water as desired. Subjects were asked not
to use any additional treatment for their rosacea for the duration of the study, as per the
exclusion criteria.
Page 6 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 7
Outcome measures
The primary outcome measure was the proportion of subjects who had a ≥2 improvement
(reduction) in the IGA-RSS at week 8 (designated ‘responders’). This measure represents a
clinically meaningful improvement in rosacea severity. The secondary outcome measures
included the change from baseline in IGA-RSS at week 2 and week 8; the participant-rated
VAS-CS at weeks 2 and 8; the change from baseline in participant-rated VAS-S at week 2
and week 8; the weekly diary-documented Rosacea severity VAS-S from participant diaries;
the change from baseline in the participant-rated DLQI [20] at weeks 2 and 8; withdrawals
due to worsening of Rosacea; adverse events; and the daily self-reported use of Honevo®
(applications per day). Data for all participants was included for analysis up until the time the
participant withdrew from the study or became ineligible due to the use of prohibited
medications.
Sample size and study power
We anticipated the proportion of participants in the control group who respond with a ≥2
reduction in blinded IGA would be between 25 and 50%.6 A total of 124 participants (62 in
each group) has 80% power at 5% significance to detect a 25% response rate in the control
group and a 50% response rate in the Honevo® group. We recruited 138 participants to
allow for a 10% drop-out rate.
Statistical methods
The study was analysed by an intention to treat, with the participants who withdrew
considered to be non-responders. The pre-specified statistical analysis was logistic
regression for the difference in proportions with response.
Relative risks for a ≥2 point change in IGA-RSS at week 8 from baseline and for total study
withdrawal were calculated, with P values using Fishers exact test. Odds ratios were also
calculated from logistic regression
Page 7 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 8
For the Likert scaled variables the Wilcoxon test and Hodges-Lehman estimator of location
shift for the difference between treatments were used. DLQI and VAS variables were
analysed by ANCOVA with the baseline value as a continuous covariate and the
randomisation as the main predictor variable. The estimates for these analyses are
interpreted as the difference between randomised groups adjusted for baseline.
Applications per day was analysed by ANOVA with the response variable the mean average
number of applications per day, predictor variable randomisation group, and using the
number of days in the trial as a weight, to account for variations in the number of days of
application.
In a post-hoc analysis, the proportion of participants in whom the IGA-RSS was zero (clear
of rosacea) at week 8 was calculated.
SAS version 9.3 was used.
Page 8 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 9
RESULTS
The flow of participants in the study is shown in Figure 1. There were 69 subjects
randomised to control and 69 to Honevo®. One Honevo® participant was subsequently
excluded due to the use of a prohibited medication on enrolment, and their data was not
used in the consequent analysis. The characteristics of the participants are shown in Table
1. Participants were predominantly aged between 50 and 70, and had had rosacea for a
mean of 15 years. 19% of participants in each group had previously used oral antibiotics for
rosacea, while 44% and 38% had previously used any topical treatments for rosacea in the
Honevo® and control group respectively. There were 7/68 (10.3%) withdrawals in the
Honevo® group (3 worsening rosacea, 2 took prohibited medications, 2 for other reasons
unrelated to the study) and 15/69 (21.7%) withdrawals in the control group (8 worsening
rosacea, 2 took prohibited medications, 1 did not want to take the control medication, 1
found the study inconvenient and 3 for reasons unrelated to the study).
Primary outcome
There were 24/68 (34.3%) in the Honevo® group and 12/69 (17.4%) in the control group
who had a ≥2 improvement in IGA-RSS at week 8 compared to baseline (relative risk 2.03
(95% CI 1.11 to 3.72), P=0.020. The corresponding odds ratio was 2.59 (1.17 to 5.74).
Secondary outcomes
The change from baseline in IGA-RSS for participants who did not withdraw is shown in
Table 2, Supplement Table S3 and Figure 2.The change in IGA-RSS for Honevo®
compared to control at week 2 minus baseline was -1 (Hodges-Lehman estimate, 95% CI -1
to 0, P=0.03), and at week 8 minus baseline was -1 (Hodges-Lehman estimate, 95% CI -1 to
0, P=0.005),(Table 3). The subject-rated VAS-CS at week 2 was 9.1 (CI 3.5 to 14.7),
P=0.002, and at week 8 was 12.3 (CI 5.7 to 18.9), P<0.001for Honevo® compared to
control, representing greater improvement with Honevo®. There was no significant
Page 9 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 10
difference in diary-captured VAS-S, adjusted for baseline, at any of the time points between
week 2 and 8 (Supplement Table S4).There was no significant difference in the participant-
rated DLQI adjusted for baseline at week 2 (-0.3, CI-1.1 to 0.6, P=0.51) or week 8 (-0.01, CI
-0.7 to 0.7,P=0.97).
The number of applications per day between the randomised treatments was similar (mean
(SD) 1.84(0.23) vs 1.86(0.20) for the Honevo® and control groups respectively, difference: -
0.02 (95% CI -0.10 to 0.05), P=0.55).
In a post hoc analysis, the proportion of participants in whom the IGA-RSS score at week 8
was zero, (i.e. full resolution of rosacea) was 9/68 (13.2%) and 2/69 (2.9%) in the Honevo®
and control groups respectively, relative risk 4.6 (95%CI 1.0 to 20.4, P=0.031).
In the Honevo® group 23 participants reported 31 adverse events; 17 rosacea related, (3 of
which resulted in withdrawal of the participants), and 14 unrelated to rosacea (Supplement
Table S5). In the control group, 27 participants reported 36 adverse events; 22 rosacea
related, (8 of which resulted in withdrawal of participants), and 14 unrelated to rosacea.
Page 10 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 11
DISCUSSION
This randomised controlled trial has demonstrated that topical 90% medical grade kanuka
honey and 10% glycerine (Honevo®) is an effective and well tolerated treatment for rosacea.
About one third of participants had a clinically significant improvement in the IGA-RSS after
8 weeks of Honevo® treatment, two-fold greater than that observed with the control
treatment. We recommend consideration of the use of kanuka honey as a treatment for
rosacea.
There are a number of methodological issues that are important in the consideration of the
study findings. There are no standard validated tools for assessing the severity of rosacea,
which is inherently difficult due to its varied clinical characteristics. The priority with this study
of a honey product was to reduce potential bias by blinding of clinical assessments where
possible, as the participant could not be blinded due to the appearance and smell of
Honevo®. It was for this reason we chose to use the 7 point IGA-RSS representing a global
assessment of rosacea severity that was undertaken by an investigator who was blinded to
treatment.
The primary outcome variable identified the proportion in each treatment arm who had a 2
point reduction or more in IGA-RSS, representing a clinically meaningful improvement in
rosacea severity, for example a change from ‘severe’ to ‘moderate’, or from ‘moderate’ to
‘mild’. 34% of those who were randomised to Honevo® had an IGA-RSS improvement of 2
or more at 8 weeks compared to 17% of the placebo group, and 13% achieved full resolution
of rosacea compared to 3% in the placebo group. Although these point estimates are
consistent with effectiveness, the confidence intervals are wide which could be consistent
with a small effect or quite large effect. This is especially the case for the post hoc analysis
of IGA-RSS for the proportion of participants with complete resolution, which although it
favours the active treatment, could be consistent with quite a small effect. The estimate of
Page 11 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 12
the location shift for the difference between the treatments was -1, (95% CI -1 to 0) at both
week 2 and week 8 and the estimated change in IGA-RSS at week 8 adjusted for baseline
was -0.6 (95% CI -1.1 to -0.2). These findings reflect the variability in response to Honevo®,
perhaps dependent on sub-types of rosacea2 which were not assessed in this study.
In addition, we assessed patient-reported outcomes, based on participant’s assessment of
current severity of symptoms (VAS-S), participant’s perceived change in severity (VAS-CS)
and the DLQI questionnaire, to provide a comprehensive assessment of efficacy. The VAS-
CS at the 2-week and 8-week clinic visits were significantly better with Honevo®. However,
there was no difference with the 2-week and 8-week DLQI assessments or the weekly diary
VAS-S measures. Thus the patient assessments were not completely consistent with the
other assessments of efficacy. This could mean that the variability in these lead to
insufficient statistical power to detect a difference, or in the context of rosacea that an ideal
measurement related to efficacy that is sensitive to change needs further development. The
RosaQoL instrument has been recently reviewed in addition to the DLQI and a generic
health-related quality of life instrument, the SF-36, in rosacea, and may be a suitable
instrument for future research.[21] In the absence of a validated VAS for rosacea severity, it
is difficult to comment on the clinical relevance of a reduction of 11 points from baseline in
the VAS-S or the 12.3 improvement in VAS-CS in the Honevo® group compared to the
control group after 8 weeks. As these outcomes were participant assessed and participants
could not be blinded to the interventions, there is a risk of detection bias in this methodology.
The DLQI is a questionnaire non-specific to rosacea and may not have been sensitive
enough to capture changes associated with this condition alone. The drop-out rate for this
study was greater than anticipated, which will need to be factored into future research in
similar clinical studies. The greater number of withdrawals due to worsening rosacea in the
control group (12% vs 4%), and overall withdrawals is likely to have led to an under-
estimation of the efficacy of Honevo®, as these participants did not undergo assessment of
the secondary outcome variables following withdrawal.
Page 12 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 13
Cetomacrogol cream was chosen as a comparator as it is a non-ionic moisturising cream,
often used as a vehicle for delivery of topical medications.[22,23] The treatment was
administered for 8 weeks to allow both the speed of onset and the duration of effect to be
assessed. This identified that honey had efficacy within 2 weeks of treatment, with further
efficacy obtained during the 8 week treatment period. Adverse event data did not allow us to
reliably ascertain whether the rosacea specific adverse events such as burning, itching,
peeling, stinging, dry skin and pain were associated only with the application of the
investigational medicine or whether they were ongoing rosacea symptoms. However it was
reassuring that the number of participants with rosacea specific adverse events was similar
between Honevo® and the paraffin-based emollient control cream.
Notwithstanding the limitations of comparing different primary outcome variables utilised in
other studies of rosacea, it is interesting to note the findings from placebo-controlled studies
of topical metronidazole or azelaic acid, two of the more commonly used treatments of
rosacea.[4-7] In studies of topical metronidazole the relative risk of improvement with the
physician’s global evaluation of improvement was 1.95 (95% CI 1.5 to 2.6), and in studies of
azelaic cream the relative risk of participant-assessed improvement was 1.52 (95% CI 1.3 to
1.8).[6,24] In our study, the relative risk of IGA-RSS improvement with Honevo® was 2.0
(95%CI 1.1 to 3.7) and in the post hoc analysis the relative risk of resolution was 4.6 (95%CI
1.0 to 20.4). It is difficult to indirectly compare the results of these studies of two other active
treatments against placebo with the study reported here, as the characteristics of the
research participants may have been quite different and the outcome variable of global
improvement may not correspond to that used in this study. We favour despite this, that we
have found sufficient evidence of efficacy, albeit with wide confidence intervals, that a
reasonable next stage is to conduct randomised controlled trials comparing Honevo® with
topical metronidazole or azelaic cream.
Page 13 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 14
The mechanism of action was not assessed in this study, however there a number of
potential mechanisms relevant to the efficacy demonstrated with kanuka honey in this study.
Firstly kanuka honey has a number of different anti-inflammatory effects, including inhibition
of neutrophil superoxide production,[13] reduction in inflammatory leucocyte infiltration and
arachidonic- induced oedema,[13] and stimulation of macrophage release of tumour
necrosis factor a (TNFa),[15] a cytokine with a crucial role in wound healing.[25,26] These
properties may be relevant as rosacea is a chronic inflammatory disorder, characterised by
inflammatory cell infiltration, vascular dilatation and tissue oedema.[1,3,6] In addition,
kanuka honey has high antibacterial activities against a wide range of bacteria, including
Bacillus subtilis, Propionibacterium acne and Staph Aureus,[11,12,14] properties which may
be beneficial in view of the proposed role of Bacillus oleronius in the inflammatory response
in rosacea. The effect of honey on Bacillus oleronius and the Demodex folliculum mite
require further investigation.
In conclusion, this randomised controlled trial has demonstrated the clinical efficacy and
tolerability of 90% medical grade kanuka honey and 10% glycerine (Honevo®) in the
treatment of rosacea. Honevo® can be recommended for the treatment of rosacea;
however, further randomised controlled trials comparing Honevo® with topical metronidazole
and azelaic acid are now required to determine its relative efficacy and side effect profile
compared to these agents.
Page 14 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 15
STATEMENTS
Corresponding Author Statement: The Corresponding Author has the right to grant on
behalf of all authors and does grant on behalf of all authors, an exclusive licence on a
worldwide basis to the BMJ Publishing Group Ltd to permit this article (if accepted) to be
published in BMJ editions and any other BMJPGL products and sublicences such use and
exploit all subsidiary rights, as set out in our licence.
Competing interest statement: All authors have completed the Unified Competing Interest
form atwww.icmje.org/coi_disclosure.pdf (available on request from the corresponding
author) and declare: HoneyLab Ltd provided funding to undertake this study and provided
the product Honevo® for the purpose of the study; Dr Shaun Holt, the Medical Director of
HoneyLab Ltd was previously the Programme Director of Complementary Medicine at the
Medical Research Institute of New Zealand. There are no other competing interests to
declare.
Role of the funding source: HoneyLab was consulted in the design of the study and
preparation of the report, but had no involvement in the collection, analysis and interpretation
of the data, or decision to submit for publication.
Contributorship statement: Study concept and design: JF, JK, MH, MW, RB. Acquisition of
Data: IB, AH, JR, AC, CH, DS, CT, BM. Drafting of the manuscript: RB, IB, MW. Critical
revision of the manuscript for important intellectual content: all authors. Statistical analysis:
MW. Administrative, technical and material support: All authors. Study supervision: MH.
Guarantor: Dr I Braithwaite had access to all the data on the study and takes responsibility
for the integrity of the data and accuracy of the data analysis.
Transparency declaration: The lead author affirms that the manuscript is an honest,
accurate, and transparent account of the study being reported; that no important aspects of
the study have been omitted; and that any discrepancies from the study as planned (and, if
relevant, registered) have been explained
Data sharing statement: Patient level data available from the corresponding author.
Consent was not obtained from participants for data sharing, but the presented data are
anonymised and the risk of identification is low. Data may be obtained by contacting the
corresponding author.
Page 15 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 16
Table 1: Baseline characteristics of participants
Mean (SD) Median (IQR) Min to Max
Age at enrolment
Honevo® N-68 57.7 (13.7) 58.2 (46.7 to 68.3) 23.4 to 86.5
Control N=69 58.9 (15.9) 60.1 (49.0 to 68.6) 18.2 to 90.1
All N=137 58.3 (14.8) 58.9 (48.1 to 68.6) 18.2 to 90.1
Age at Diagnosis
Honevo® N=64 42.2 (15.4) 40 (30 to 51.5) 19 to 80
Control N=67 43.6 (15.4) 43 (35 to 55) 10 to 79
All N=131 42.9 (15.4) 41 (32 to 54) 10 to 80
Honevo® N (%) N=68
Control N (%) N=69
Female 32 (47.1) 36 (52.2)
History of oral antibiotics 13 (19.1) 13 (18.8)
History of topical therapy 24 (35.3) 20 (29.0)
History of topical steroid 6 (8.8) 6 (8.7)
European 64 (94.1) 68 (98.6)
Maori 4 (5.9) 0 (0)
Asian 0 (0) 1 (1.5)
SD – standard deviation IQR – inter quartile range
Page 16 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 17
Table 2: Contingency table of blinded Investigator Global Assessment of Rosacea
Severity Score (IGA-RSS) week 8 change from baseline by randomisation in the
subjects who completed the study
Change from baseline Honevo® N/61 (%) Control N/54 (%)
-3 11 (18.0) 1 (1.9)
-2 13 (21.3) 11 (20.4)
-1 20 (32.8) 17 (31.5)
0 14 (23.0) 15 (27.8)
1 3 (4.9) 8 (14.8)
2 0 (0) 2 (3.7)
IGA-RSS: blinded Investigator Global Assessment of Rosacea Severity Score based on a 7 point scale (0 ‘clear’ to 6 ‘severe’
Page 17 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 18
Table 3: Clinic-based secondary outcome variables (all Honevo® minus control)
Comparison N with data Hodges-Lehman
estimate (95% CI) P
Honevo® Control
IGA-RSS week 2 66 66 0 (-1 to 0) 0.26
IGA-RSS week 8 61 54 0 (-1 to 0) 0.06
IGA-RSS week 2 minus baseline 66 66 -1 (-1 to 0) 0.03
IGA-RSS week 8 minus baseline 61 54 -1 (-1 to 0) 0.005
Estimate (95% CI) P
IGA-RSS week 8 adjusted for baseline1
61 54 -0.6 (-1.1 to -0.2) 0.003
Mean difference (95% CI)
P
VAS-CS week 2 66 66 9.1 (3.5 to 14.7) 0.002
VAS-CS week 8 61 54 12.3 (5.7 to 18.9) <0.001
VAS-S week 2 66 66 -3.6 (-9.9 to 2.7) 0.26
VAS-S week 2 minus baseline 66 66 -2.9 (-9.2 to 3.5) 0.38
VAS-S week 8 61 54 -4.5 (-11.6 to 2.6) 0.21
VAS-S week 8 minus baseline 61 54 -11.0 (-18.0 to -3.9) 0.003
IGA-RSS: blinded Investigator Global Assessment of Rosacea Severity Score, based on a 7 point
scale (0 ‘clear’ to 6 ‘severe’)
VAS-CS: Participant-rated assessment of Change in Severity of rosacea based on a 100mm VAS
scale (0mm ‘much worse’ to 100mm ‘much improved’)
VAS-S: Participant-rated assessment of Severity of rosacea based on a 100mm VAS scale (0mm
‘mildest possible’ symptoms and 100mm ‘worst possible’ symptoms)
ANOVA with baseline reading as a covariate, normality assumptions not well met
Page 18 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 19
FIGURE LEGENDS
Figure 1: Flow of participants through trial.
Figure 2: The difference from baseline in IGA-RSS at week 8 for control and Honevo®.
Horizontal lines are the 25%, median and 75% quantiles, the symbol is the mean and
the whiskers go from maximum to minimum.
Page 19 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 20
REFERENCES
1. Buechner SA. Rosacea: an update. Dermatology 2005;210:100-8.
2. Wilkin J, Dahl M, Detmar M, et al. Standard grading system for rosacea: Report of the
National Rosacea Society Expert Committee on the classification and staging of
rosacea. J Am Acad Dermatol 2004;50:907-12.
3. Berg M, Liden S. An epidemiological study of rosacea. Acta Derm Venereol.
1989;69:419-23.
4. Powell FC. Clinical practice. Rosacea. N Engl J Med 2005;352:793-803.
5. Elewski BE, Fleischer AB, Jr, Pariser DM. A comparison of 15% azelaic acid gel and
0.75% metronidazole gel in the topical treatment of papulopustular rosacea: results of
a randomized trial. Arch Dermatol 2003;139:1444-50.
6. van Zuuren EJ, Kramer S, Carter B, et al. Interventions for rosacea. Cochrane
Database Syst Rev 2011;(3):CD003262.
7. Elewski BE. Rosacea trial comparing twice-daily azelaic acid gel 15% with once-daily
metronidazole gel 1%. Cutis 2007;79:57-8; author reply 8.
8. World Health O. Antimicrobial resistance: global report on surveillance 2014. 2014;
Report No. ISBN: 978 92 4 156474 8 Contract No. Document Number|.
9. Costelloe C, Metcalfe C, Lovering A, et al. Effect of antibiotic prescribing in primary
care on antimicrobial resistance in individual patients: systematic review and meta-
analysis. BMJ 2010;340:c2096.
10. Department of Health UKSMAC. The path of least resistance. 1998.
11. Wu Q. Antimicrobial effect of Manuka honey and Kanuka honey alone and in
combination with the bioactives against the growth of Propionibacterium acnes ATCC
6919: a thesis submitted in partial fulfilment of the requirements for the degree Master
of Food Technology, Massey University, Albany, New Zealand; 2011.
Page 20 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 21
12. Lu J, Carter DA, Turnbull L, et al. The effect of New Zealand kanuka, manuka and
clover honeys on bacterial growth dynamics and cellular morphology varies according
to the species. PLoS One 2013;8:e55898.
13. Leong AG, Herst PM, Harper JL. Indigenous New Zealand honeys exhibit multiple anti-
inflammatory activities. Innate Immun 2012;18:459-66.
14. Allen KL, Molan PC, Reid GM. A survey of the antibacterial activity of some New
Zealand honeys. J Pharm Pharmacol 1991;43:817-22.
15. Gannabathula S, Skinner MA, Rosendale D, et al. Arabinogalactan proteins contribute
to the immunostimulatory properties of New Zealand honeys. Immunopharmacol
Immunotoxicol 2012;34:598-607.
16. Lacey N, Delaney S, Kavanagh K, et al. Mite-related bacterial antigens stimulate
inflammatory cells in rosacea. Br J Dermatol 2007;157:474-81.
17. Bonnar E, Eustace P, Powell FC. The Demodex mite population in rosacea. J Am
Acad Dermatol 1993;28:443-8.
18. Yamasaki K, Di Nardo A, Bardan A, et al. Increased serine protease activity and
cathelicidin promotes skin inflammation in rosacea. Nat Med 2007;13:975-80.
19. Fingleton JS, D. Cave, N. Brinded, et al. Topical kanuka honey for the treatment of
rosacea. Focus on Alternative and Complementary Therapies 2013;18:221-2.
20. Lewis V, Finlay AY. 10 years experience of the Dermatology Life Quality Index (DLQI).
J Investig Dermatol Symp Proc. 2004;9:169-80.
21. Van der Linden MM, van Rappard DC, Daams JG, et al. Health-related quality of life in
patients with cutaneous rosacea: a systematic review. Acta Derm Venereol
2015;95:395-400.
22. (Datapharm) ew. Cetomacrogol Cream BP 1988 Formula A.
https://wwwmedicinesorguk/emc/medicine/25140. Last accessed Dec 24,2014.
23. Kingdom NNHSU. Cetomacrogol Cream Formula A. http://wwwnhsuk/medicine-
guides/pages/MedicineOverviewaspx?medicine=Cetomacrogol%20Cream%20Formul
a%20A. Last accessed Dec 24, 2014.
Page 21 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Page 22
24. van Zuuren EJ, Kramer SF, Carter BR, et al. Effective and evidence-based
management strategies for rosacea: summary of a Cochrane systematic review. Br J
Dermatol 2011;165:760-81.
25. Fu X, Tian H, Hsu S, et al. In vivo effects of tumor necrosis factor-alpha on incised
wound and gunshot wound healing. J Trauma 1996;40(3 Suppl):S140-3.
26. Mooney DP, O'Reilly M, Gamelli RL. Tumor necrosis factor and wound healing. Ann
Surg 1990;211:124-9.
Page 22 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
56x67mm (300 x 300 DPI)
Page 23 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Supplement Table S1: Blinded Investigator Global Assessment of Rosacea Severity Score (IGA-RSS)
Numerical Score
Definition Description
0 Clear Almost no Rosacea (i.e. no papules and/or pustules); no or residual erythema; mild to moderate degree of telangiectasia may be present
1 Minimal Rare papules and/or pustules; residual to mild erythema; mild to moderate degree of telangiectasia may be present
2 Mild Few papules and/or pustules; mild erythema; mild to moderate degree of telangiectasia may be present
3 Mild to moderate Distinct number of papules and/or pustules; mild to moderate erythema; mild to moderate degree of telangiectasia may be present
4 Moderate Pronounced number of papules and/or pustules; moderate erythema; mild to moderate degree of telangiectasia may be present
5 Moderate to Severe
Many papules and/or pustules, occasionally with large inflamed lesions; moderate erythema; moderate degree of telangiectasia may be present
6 Severe Numerous papules and/or pustules, occasionally with confluent areas of inflamed lesions; moderate to severe erythema; moderate to severe degree of telangiectasia may be present
Page 24 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Supplement Table S2: Schedule of Assessments
Visit Number Visit 1 Visit 2 Visit 3
Time Point Week 0 Day 1
Week 2 Day 15
Week 8 Day 57
Informed Consent X
Eligibility criteria checked X
Demographics and medical history X
Randomisation X
Administer DLQI X X X
Administer IGA X X X
Participant-rated severity VAS-S completiona X X X
Participant-rated change VAS-CS severity completion
X X
Provision of participant diary X X
Collection of participant diary X X
Safety monitoring X X X
DLQI: Dermatology Life Quality Index
IGA-RSS blinded Investigator Global Assessment of Rosacea Severity Score VAS-S: Participant-rated assessment of severity of rosacea VAS-CS: Participant-rated assessment of change in severity of rosacea a VAS-S to be completed weekly from Visit 1 until Visit 3, within the subject diary
Page 25 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Supplement Table S3: Clinic-based secondary outcome variables
Mean (SD) Median (IQR) Min to Max
IGA-RSS week Zero
Control N=69 3 (0.9) 3 (2 to 4) 2 to 5 Honevo® N=68 3 (0.9) 3 (2 to 3.5) 2 to 6
IGA-RSS week 2
Control N=66 2.5 (1.4) 2 (2 to 3) 0 to 6 Honevo® N=66 2.2 (1.2) 2 (1 to 3) 0 to 6
IGA-RSS week 8
Control N=54 2.4 (1.3) 2 (1 to 3) 0 to 6 Honevo® N=61 1.8 (1.2) 2 (1 to 3) 0 to 5
Difference IGA-RSS week 2 to week Zero Control N=66 -0.5 (0.9) 0 (-1 to 0) -3 to 1 Honevo® N=66 -0.8 (1.0) -1 (-2 to 0) -3 to 2
Difference IGA-RSS week 8 to week Zero
Control N=54 -0.6 (1.1) 0 (-1 to 0) -3 to 2 Honevo® N=61 -1.2 (1.1) -1 (-2 to 0) -3 to 1
VAS-CS week 2
Control N=66 50.1 (16.6) 51 (47 to 55) 0 to 89 Honevo® N=66 59.2 (16.1) 59 (50 to 71) 21 to 98
VAS-CS week 8
Control N=54 55.2 (18.2) 51 (48 to 61) 15 to 98 Honevo® N=61 67.6 (17.4) 69 (52 to 79) 25 to 99
VAS-S week Zero
Control N=69 32.0 (19.1) 28 (18 to 44) 1 to 87 Honevo® N=68 36.8 (21.2) 31.5 (21 to 54) 1 to 78
VAS-S week 2
Control N=66 34.9 (19.6) 32.5 (21 to 50) 1 to 84 Honevo® N=66 31.2 (16.9) 29.5 (20 to 42) 1 to 68
VAS-S week 8
Control N=54 30.8 (19.2) 31 (13 to 46) 3 to 78 Honevo® N=61 26.3 (19.2) 24 (12 to 38) 2 to 96
Difference VAS-S week 2 to week Zero
Control N=66 3.0 (16.7) 0.5 (-6.0 to 8.0) -30 to 73 Honevo® N=66 -5.2 (16.1) -6 (-16 to 1) -37 to 38
Difference VAS-S week 8 to week Zero
Control N=54 2.1 (14.5) -1 (-9 to 11) -39 to 41 Honevo® N=61 -8.9 (22.4) -10(-24 to 9) -66 to 38
IGA-RSS: blinded Investigator Global Assessment of Rosacea Severity Score, based on a 7 point scale (0 ‘clear’ to 6 ‘severe’) VAS-CS: Participant-rated assessment of Change in Severity of rosacea based on a 100mm VAS scale (0mm ‘much worse’ to 100mm ‘much improved’) VAS-S: Participant-rated assessment of Severity of rosacea based on a 100mm VAS scale (0mm ‘mildest possible’ symptoms and 100mm ‘worst possible’ symptoms)
Page 26 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Supplement Table S4: Diary-based VAS-S adjusted for baseline
Honevo® minus Control N with data Estimate (95% CI) P
Honevo® Control
VAS-S week 2 52 50 -4.0 (-8.5 to 0.6) 0.088
VAS-S week 3 60 53 -1.3 (-6.8 to 4.2) 0.65
VAS-S week 4 59 54 -4.0 (-10.3 to 2.4) 0.21
VAS-S week 5 55 55 -2.0 (-7.8 to 3.9) 0.50
VAS-S week 6 56 50 -5.3 (-2.5 to 14.2) 0.13
VAS-S week 7 53 50 -2.1 (-8.9 to 4.7) 0.54
VAS-S week 8 48 38 -5.7 (-6.2 to 13.3) 0.15
VAS-S: Participant-rated assessment of Severity of rosacea based on a 100mm VAS scale (0mm ‘mildest possible’ symptoms and 100mm ‘worst possible’ symptoms)
Page 27 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
Supplement Table S5: Adverse events reported in the Honevo® and Control groups.
Honevo® N
Control N
Rosacea related adverse events resulting in withdrawal
Worsening Rosacea 3 8
Rosacea related adverse events without withdrawal
Worsening Rosacea 0 2
Itching 5 1
Tingling 3 2
Red spots 2 0
Eczema 1 0
Dry skin 1 0
Peeling 1 0
Pain 1 0
Stinging 0 4
Burning 0 2
Blisters 0 1
Bleeding 0 1
Possible fungal skin infection 0 1
Non-rosacea related adverse events resulting in withdrawal
0 0
Non-rosacea related adverse events without withdrawal
Other skin problem 1 0
Infection 6 7
Trauma 3 1
Indigestion 1 0
Worsening Asthma 1 0
Headache / Migraine 1 2
Elevated PSA 1 0
Cardiovascular 0 2
Allergy / Hayfever 0 2
Note: Participants may report more than one adverse event
Page 28 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
11x9mm (600 x 600 DPI)
Page 29 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on Decem
ber 5, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-007651 on 24 June 2015. Dow
nloaded from

For peer review only
CONSORT 2010 checklist Page 1
CONSORT 2010 checklist of information to include when reporting a randomised trial*
Section/Topic Item No Checklist item
Reported on page No
Title and abstract
1a Identification as a randomised trial in the title title
1b Structured summary of trial design, methods, results, and conclusions (for specific guidance see CONSORT for abstracts) 2
Introduction
Background and
objectives
2a Scientific background and explanation of rationale 4
2b Specific objectives or hypotheses 4
Methods
Trial design 3a Description of trial design (such as parallel, factorial) including allocation ratio 5
3b Important changes to methods after trial commencement (such as eligibility criteria), with reasons n/a
Participants 4a Eligibility criteria for participants 5
4b Settings and locations where the data were collected 5
Interventions 5 The interventions for each group with sufficient details to allow replication, including how and when they were
actually administered
6
Outcomes 6a Completely defined pre-specified primary and secondary outcome measures, including how and when they
were assessed
6-7
6b Any changes to trial outcomes after the trial commenced, with reasons n/a
Sample size 7a How sample size was determined 8
7b When applicable, explanation of any interim analyses and stopping guidelines n/a
Randomisation:
Sequence
generation
8a Method used to generate the random allocation sequence 6
8b Type of randomisation; details of any restriction (such as blocking and block size) 6
Allocation
concealment
mechanism
9 Mechanism used to implement the random allocation sequence (such as sequentially numbered containers),
describing any steps taken to conceal the sequence until interventions were assigned
6
Implementation 10 Who generated the random allocation sequence, who enrolled participants, and who assigned participants to
interventions
6
Blinding 11a If done, who was blinded after assignment to interventions (for example, participants, care providers, those 6
Page 30 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on December 5, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-007651 on 24 June 2015. Downloaded from

For peer review only
CONSORT 2010 checklist Page 2
assessing outcomes) and how
11b If relevant, description of the similarity of interventions n/a
Statistical methods 12a Statistical methods used to compare groups for primary and secondary outcomes 7
12b Methods for additional analyses, such as subgroup analyses and adjusted analyses 7
Results
Participant flow (a
diagram is strongly
recommended)
13a For each group, the numbers of participants who were randomly assigned, received intended treatment, and
were analysed for the primary outcome
9, fig 1
13b For each group, losses and exclusions after randomisation, together with reasons 9, fig 1
Recruitment 14a Dates defining the periods of recruitment and follow-up 5
14b Why the trial ended or was stopped n/a
Baseline data 15 A table showing baseline demographic and clinical characteristics for each group 15
Numbers analysed 16 For each group, number of participants (denominator) included in each analysis and whether the analysis was
by original assigned groups
9
Outcomes and
estimation
17a For each primary and secondary outcome, results for each group, and the estimated effect size and its
precision (such as 95% confidence interval)
9-10
17b For binary outcomes, presentation of both absolute and relative effect sizes is recommended 9-10
Ancillary analyses 18 Results of any other analyses performed, including subgroup analyses and adjusted analyses, distinguishing
pre-specified from exploratory
9-10
Harms 19 All important harms or unintended effects in each group (for specific guidance see CONSORT for harms) 10
Discussion
Limitations 20 Trial limitations, addressing sources of potential bias, imprecision, and, if relevant, multiplicity of analyses 11-12
Generalisability 21 Generalisability (external validity, applicability) of the trial findings 11-12
Interpretation 22 Interpretation consistent with results, balancing benefits and harms, and considering other relevant evidence 12-13
Other information
Registration 23 Registration number and name of trial registry abstract
Protocol 24 Where the full trial protocol can be accessed, if available uploaded
Funding 25 Sources of funding and other support (such as supply of drugs), role of funders title
*We strongly recommend reading this statement in conjunction with the CONSORT 2010 Explanation and Elaboration for important clarifications on all the items. If relevant, we also
recommend reading CONSORT extensions for cluster randomised trials, non-inferiority and equivalence trials, non-pharmacological treatments, herbal interventions, and pragmatic trials.
Additional extensions are forthcoming: for those and for up to date references relevant to this checklist, see www.consort-statement.org.
Page 31 of 31
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on December 5, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-007651 on 24 June 2015. Downloaded from
![Rosacea: Molecular Mechanisms and Management of a Chronic ...€¦ · rosacea in childhood also exists, although the exact age of onset of rosacea remains to be explored [6,7]. Furthermore,](https://img.pdfslide.us/doc/110x75/60078c74cf08d82d801aacc7/rosacea-molecular-mechanisms-and-management-of-a-chronic-rosacea-in-childhood.jpg)