-
8/12/2019 Raine et al,. (2002) - 'Prefrontal Structural and
Functional Deficits in Schizotypal Personality Disorder'
1/13
Prefrontal Structural and Functional Deficits inSchizotypal
Personality Disorderby Adrian Raine, Todd Lencz, Paul ine Yaralian,
Susan Bihrle, Lori LaCasse,Joseph Ventura, and Patrick Colletti
AbstractStructural prefrontal deficits have been reported
inpatients with schizophrenia, but it is unclear if theyare also
found in patients with schizophrenia spec-trum personality
disorders. The hypothesis that aspectrum group will be
characterized by prefrontalstructural deficits was tested by
assessing prefrontalgray and white volumes using magnetic
resonanceimaging in a community sample of 16 individualswith
schizotypal/paranoid personality disorder, 27comparisons, and 26
psychiatric controls. Frontalneurocognitive functioning was also
assessed usingthe Wisconsin Card Sorting Test and the
ContinuousPerformance Test. The spectrum group showedreduced
prefrontal gray volumes and poorer frontalfunctioning compared to
both other groups.Structural deficits were independent of
functionaldeficits and together correctly classified 84.2 percentof
subjects. Structural but not functional deficitswere abolished
after a strict control for antisocialpersonality was made. Results
support the notionthat frontal deficits may be centrally involved
in theetiology of schizophrenia but also suggest thatcomorbid
antisocial behavior may be one factoraccounting for differences in
prefrontal structuralfindings across studies.
Keywords: Schizotypal, paranoid, prefrontalgray, MRI,
antisocial.chizophreni Bulletin 28 3):501-513, 2002.
Quantitative magnetic resonance imaging (MRI) studieshave found
evidence for frontal structural deficits inschizophrenia (Zakzanis
and Heinrichs 1999; Yaralianand Raine 2000). These imaging studies
are aboutequally divided in either showing reductions in total
vol-ume (gray and white) or area of the frontal/prefrontalregion
(e.g., Andreasen et al. 1986, 1994; Raine et al.1992*; Nopoulos et
al. 1995) or failing to find thesereductions (Andreasen et al.
1990; Bilder et al. 1994;Szeszko et al. 1999 ). Another study found
prefrontal
volume deficits in schizophrenia patients compared tonormal
controls, but not when compared to chronic alco-holics (Sullivan et
al. 1998), while one review reportspreliminary findings failing to
observe reduced pre-frontal volume in schizotypal patients (Siever
et al.2002).The significance, in part, of such frontal deficits,if
they truly exist, is that they may help account for thefunctional
frontal deficits repeatedly observed in schizo-phrenia (Buchsbaum
1990; Cannon 1996; Weinbergerand Berman 1998).Some of these
structural MRI studies have furthersegmented gray from white matter
within the frontal orprefrontal region, with mixed results. Four
studies foundreductions in prefrontal gray but not white
matter(Zipursky et al. 1992; Lim et al. 1995; Lim et al.
1996;Sullivan et al. 1998), one study that assessed only graymatter
found a reduction in the dorsolateral region(Schlaepfer et al.
1994), three studies found significantreductions in white but not
gray matter (Breier et al.1992; Buchanan et al. 1993; Buchanan et
al. 1998), andtwo studies failed to find differences in gray or
whitematter (Suddath et al. 1989; Wible et al. 1995). In con-trast
to these conflicting structural findings, at a func-tional level
hypofrontality is one of the best replicatedimaging correlates of
schizophrenia (Velakoulis andPantelis 1996). Compelling evidence
also exists fromthe neuropsychological literature for executive
functionand working memory deficits in schizophrenia patients(Park
et al. 1995), with strong overall effect sizes acrossstudies of
0.88 for the Wisconsin Card Sorting Test(WCST; 43 studies) and 1.16
for the Continuous Per-formance Test (CPT; 14 studies) (Heinrichs
and Zakza-nis 1998).
Further evidence for the etiologic significance of pre-frontal
structural deficits comes from the study of schizo-phrenia spectrum
disorders. Spectrum disorders have tra-dit ionally encompassed the
DSM odd cluster of
Send reprint requests to Dr. A. Raine, Department of
Psychology,University of Southern California, Los Angeles, CA
90089-1061; e-mail: [email protected].
50 1
-
8/12/2019 Raine et al,. (2002) - 'Prefrontal Structural and
Functional Deficits in Schizotypal Personality Disorder'
2/13
Schizophrenia Bulletin, Vol. 28, No. 3, 2002 A. Raine et al.
schizotypal, paranoid, and schizoid personality disorders(Siever
et al. 1993), although the inclusion of schizoid per-sonality
disorder has been questioned by some researcherson the grounds that
it lacks genetic relatedness with schiz-ophren ia (Nigg and
Goldsmith 1994; Torgersen 1994;Ingraham 1995) . Spect rum indiv
iduals have a s tab le(schizotypal and paranoid) personality
disorder with a his-tory of disturbances in cognition, perception,
and behaviorthat in part mirror abnormalities found in
schizophreniapatients. Research on such individuals provides a
valuableadjunct to research on inst i tut ional ized
schizophreniapatients. To the extent that the same neurobiological
corre-lates of schizophrenia can also be observed in
individualswith schizophrenia spectrum disorders who are free of
theconfounds of institutionalization, medication, and label-ing,
there is increased confidence that such processes maybe of
etiologic significance for schizophrenia. In contrast,only one MRI
s tudy appears to have tes ted whetherschizotypal personality is
related to prefrontal structuraldeficits; Raine et al. (1992ft)
showed that community vol-unteers with higher scores on self-report
schizotypal per-sonality measures had both smaller prefrontal areas
andmore perseveration errors on the WCST.
Although most other ima ging studies of schizotypal per-sonality
have focused on ventricular size (Cannon et al.1994) or temporal
lobe volumes (D ickey et al. 1999; Down-hill etal.2000), tw o
additional studies of schizotypal person-ality disorder have
relevance to the question of frontal struc-tural deficits.
Buchsbaum et al. (1997) found that patientswith schizotypal
personality disorder showed an enlarge-ment of the left anterior
horn of the lateral ventricle that wasintermediate in size between
that of normal controls andschizophrenia patients. Enlargement of
the anterior hom ofthe lateral ventricle is suggestive of tissue
loss (especially ofwhite matter) in the frontal lobe. Conversely,
Siever et al.(1995) failed to find significant differences between
anteriorhorn size in schizotypal patients, schizophrenia patients,
andcontrols. MRI studies of frontal volume in children
withschizophrenia spectrum symptoms (who may be viewed asanalogues
of schizotypy) (Yeo et al. 1997) and childhood-onset schizophrenia
(Frazier et al. 1996) have also found nullresults. In contrast,
frontal functional deficits represent thebest replicated correlate
of schizotypal personality. Specifi-cally, frontal functional
deficits have been repeatedly andreplicably found on the WCST and
the CPT with respect toboth schizotypal personality disorder and
individual differ-ences in schizotypal personality, with at least
14 studiesobtaining significant effects (e.g. , Lyons et al .
1991;Battaglia et al. 1994; Lenzenweger and Korfune 1994; Trest-man
et al. 1995; Roitman et al. 1997; Voglmaier et al. 1997;Daneluzzo
et al. 1998).
An important methodological issue in the literature isthat
studies of structural and functional frontal deficits in
schizotypal personality have rarely if ever included a
psy-chiatric control group. Similarly, despite the imp ortance
ofestablishing psychiatric specificity for structural braindeficits
in schizophrenia, the majority of structural andfunctional MRI
studies of schizophrenia do not employpsychiatric control groups.
For example, a survey foundthat of the 28 MRI studies on
schizophrenia published inth e American Journal of Psychiatry
between 1996 and2000, only 3 (10.7%) employed a psychiatric
controlgroup . Similarly, only 2 of 15 studies (13.3%) published
inArchives of General Psychiatry in this time periodemployed a
psychiatric control group, while for Schizo-phrenia Research only 2
of 14 studies (14.3%) employedpsychiatric controls. Furthermore,
studies that do use psy-chiatric controls frequently control for
only one experi-mental-group source of comorbidity that could
confoundfindings; they do not control for the full range of com
orbiddisorders that are higher in the experimental group. Itremains
to be seen, therefore, whether a schizophreniaspectrum group would
differ from a psychiatric controlgroup m atched on other Axis I and
II disorders.
The primary goal of the current study was to test thehypothesis
that individuals with schizophrenia spectrumdisorders would show a
reduction in prefrontal gray vol-ume compared to both comparisons
and psychiatric con-trols. It was also predicted that the spectrum
group wouldshow functional n eurocognitive deficits as indicated by
theWCST and the CPT and that these deficits would be predi-cated on
the structural prefrontal deficits.
MethodSu bje cts . All subjects were drawn from five tempora
ryemployment agencies in Los Angeles. This recruitmentsource was
chosen because pilot data showed that theseindividuals had higher
rates of schizotypal personality andbecause the one prior study of
prefrontal structural deficitsin schizotypy had also employed a
community sample.All subjects who wished to participate in the
study wereallowed to do so without prior screening. Subject
groupsconsisted of 27 comparisons, 26 psychiatric controls, and16
participants with a diagnosis of either schizotypal per-s ona l i t
y d i s o rde r or pa rano i d pe r s ona l i t y d i s o rde
r(referred to hereafter as the spectrum group). The spec-trum group
consisted of 10 individuals with schizotypalpersonality disorder
only, 4 individuals with paranoid per-sonality disorder only, and 2
individuals with both schizo-typal and paranoid personality
disorder. Demographic,cognitive, and physical measures for the
three groups areshown in table 1. Exclusion criteria were as
follows: ageunder 21 or over 45, nonfluency in English, history
ofepilepsy, claustrophobia, pacemaker, or metal implant.Screening
of brain scans by a neuroradiologist blind to
502
-
8/12/2019 Raine et al,. (2002) - 'Prefrontal Structural and
Functional Deficits in Schizotypal Personality Disorder'
3/13
Prefrontal Structural and Functional Deficits Schizophrenia
Bulletin, Vol. 28, No. 3, 2002
Table 1. Characteristics of the study groups
DemographicSex, maleAge,yrs, mean (SD)Social class, mean
(SD)Ethnicity, whiteCognitive and physicalEstimated
intelligence,mean (SD)Handedness, mean (SD)1Height (cm), mean
(SD)Weight (kg), mean (SD)Head circumference (in.),mean (SD)History
of head injury,
ComparisonC 27)85.230.9 (6.9)35.3(10.3)57.1101.7(14.9)33.8
(9.8)175.9(7.9)80.8(15.0)57.6(2.1)39.3
Psychiatriccontroln=2 6)88.529.0
(6.6)36.6(11.5)38.597.8(13.1)33.5
(10.5)179.7(9.1)80.9(15.7)57.2(1.7)38.5
Schizophreniaspectrum n=16 )87.532.1
(5.4)33.9(10.9)43.894.5(13.1)35.2 (9.6)176.5(10.8)78.7(11.6)57.1
(2.3)37.5
StatisticsX2= 0.9, df=2 p = 0 . 9 5F (2,67) = 1.2, p = 0.31F
(2,67) = 0.3, p = 0.72X2= 2.0,df=2 p = 0 . 3 7F (2,67) = 0.4, p =
0.68F (2,67) = 0.2, p = 0.86F (2,67) = 1.3, p = 0.27F (2,67) =
0.15, p = 0.86F (2,67) = 1.5, p = 0.39X2= 0.01,ctf=2, p = 0.99
Note.SD = standard deviation.1 High scores indicate greater
degree of right-handedness.
group membership resulted in one subject being excludedfrom
analyses because of encephalomalasia, consisting ofsignificant
atrophy to the right temporal and frontal cor-tex. Subjects were
paid $5.50 per hour for participationand were informed that the
study concerned the biologicalbasis of personal i ty and behavior
problems, includingcriminal behavior. After subjects were given
completedescriptions of the study, written informed consent
wasobtained in accordance with Institution Review Boardprocedures
at the University of Southern California.
The comparison group consisted of participants with-out a
diagnosis of schizophrenia, psychotic disorders,schizophrenia
spectrum disorders, or substance or alcoholdepen dence . A
psychiatric control group was formed froma total of63other
volunteers to obtain as close a match aspossible for the comorbid
conditions found in the spec-trum group. Results of this matching
are shown in table 2for affective and anxiety disorders, conduct
and antisocialpersonality disorders, and Cluster B and C
personality dis-orders. There were no significant differences
betweengroups, using 2 p>0-35 in all cases), with the only
trendfor significance being the psychiatric controls havingslightly
higher rates of Cluster C personality disordersthan the spectrum
group. However, there was a nonsignifi-cantly higher rate of
comorbidity for antisocial personalitydisorder in the spectrum
group (50.0%) than in the psychi-atric controls (38.5%).
Furthermore, the spectrum group(mean [M] = 9.4, standard deviation
[SD] = 4.1) had sig-nificantly higher scores on a dimensional
measure of anti-social personality disorder (see below) compared to
bothpsychiatric controls (M = 6.7, SD = 3.5; / = 2.2, d f= 40,p
=0.033) and comparisons (M = 3.7, SD = 2.4;t= 5.7, df=41 ,p =
0.0001).Because substance and alcohol use could be a con-found in
structural brain imaging correlates of schizophre-nia spectrum
disorders, details of rates of alcohol and sub-stance
abuse/dependence, together with past month usage,are given for the
psychiatric control and spectrum groupsin table 3. Similarly,
quantity and frequency of alcoholusage for these groups are given
in table 4. There were nosignificant group differences.Diagnostic,
Cognitive, Physical, and PsychosocialAssessment. Diagnoses were
made usingDSM-IV crite-ria (American Psychiatric Association 1994)
and ascer-t a i ned u s i ng t he S t ruc t u red C l i n i ca l In
t e rv i ew fo rDSM-IV Axis I Disorders (First et al. 1994a) and
theS t ruc t u red C l i n i ca l In t e rv i ew fo r DSM-IV Axis I
IPersonal i ty Disorders (SCID-II, First et al . 1994fc).Diagnoses
were made by advanced clinical psychologyPh.D. students who had
undergone a standardized trainingand quality assurance program for
diagnostic assessment(Ventura et al. 1998). Prior to diagnostic
assessments onthe study sample, diagnostic procedures were piloted
onsubjects also drawn from temporary employment agenciesand
interview tapes assessed jointly by J.V., A.R., andT.L. In addition
to diagnostic testing, an alcohol use ques-tionnaire to assess
frequency of alcohol consumption wascompleted by participants. A
dimensional measure of anti-social personal i ty disorder was
created by summingscores of the seven DSM-IV criterion C symptoms
of theS C ID-n .
503
-
8/12/2019 Raine et al,. (2002) - 'Prefrontal Structural and
Functional Deficits in Schizotypal Personality Disorder'
4/13
Schizophrenia Bulletin, Vol. 28 , N o. 3, 2002 A. Raine et
al.
Table 2. Rates of psychiatric disorder in the psychiatric
control and schizophrenia spectrum groups,together with
2analyses
Affective 1Anxiety2Conduct disorderAntisocial personality
disorderCluster B 3Cluster C 4
Psychiatriccontroln = 26)53.819.253.838.515.415.4
Schizophreniaspectrum n = 1 6 )56.318.850.050.025.5
0.0
x20.020.000.060.540.592.70
df111111
P0.880.970.810.460.440.10
1 Major depression, bipolar depression, other depressive
disorders.2 Phobia, panic, generalized anxiety.3Borderline,
histrionic, obsessive-compulsive.4A voidant, dependent,
narcissistic.
Estimated intelligence was based on the five
subtests(vocabulary, arithmetic, digit span, digit symbol,
blockdesign) of the Wechsler Adult Intelligence
Scale-Revised(Wechsler 1981). Degree of right versus left hand
preferencewas assessed using the abbreviated Oldfield Inventory
(Bry-den 1977). History of head injury was defined as headtrauma
resulting in hospitalization. Social class was mea-sured using the
Hollingshead classification system (Holling-shead 1975). A physical
exa mina tion w as conducted toderive measures of height, weight,
and head circumference.Neurocognitive M easures of Frontal
FunctioningCPT. Version 4.08 of the degraded stimulus versionof the
CPT (Nuechterlein et al. 1983) was administeredaccording to author
guidelines. Visually degraded num-bers ranging from 0 to 9 were
flashed on a computerscreen (p laced 1 meter from the subjects in
the subjects'line of vision) for 40 ms at the rate of one per
second. Thesubjects' task was to press a response button on a
Gravisjoy stick every time they saw the figure 0 but to notrespond
to all other stimuli. Targets had a 0.25 probabilityof occurrence.
After 10 presentations of the target stimu-lus only, subjects were
given 120 practice trials afterwhich 480 test stimuli (lasting 8
minutes) were presented.Hits, false alarms, sensitivity, and
response bias scoreswere computed.
WCST. A computerized version of the WCST (Grantand Berg 1948)
was administered in which subjects sorteda pack of 64 cards
according to color, shape, and number.Visual feedback (right or
wrong) was provided after eachcard placement. This task reflects
abstract reasoning, cog-nitive flexibility, and the ability to
maintain and changeset. Total errors, percent perseverative errors,
number of
categories completed, and trials to achieve the first cate-gory
were computed.MRI. Full details of MR I assessments are given in
Raineet al. (2000). Structural MRIs were conducted on a
PhilipsS15/ACS (Selton/Conn) scanner with a magnet of 1.5Tes la f i
e ld s t rength . Fol lowing an in i t i a l a l ignmentsequence of
one midsagittal and four parasagittal scans(spin-echo Tl-weighted
image acquisition, repetition time[TR] = 600 ms, time to echo [TE]
= 20 ms) to identify theanter ior commissure-pos ter ior commissure
(AC-PC)plane, 128 three-dimensional Tl-weighted
gradient-echocoronal im ages (TR 34 ms, TE 12.4 ms, flip angle 35,
1.7mm over contiguous slices, 256 X 256 matrix, field ofview [FOV]
= 23 cm) were taken in the plane directlyorthogonal to the AC-PC
line.
Brain images were reconstructed in three dimensionsusing a SPARC
workstation and semiautomated CAM RAS200 ALL EG RO sof tware used
for gray/whi te /cere -brospinal fluid (CSF) segmentation.
Segmentation of grayand white matter was performed using a
thresholdingalgorithm, with the operator blind to group
membershipapplying a cutoff va lue to the signal intensity
histogram tooptimally differentiate white from gray, areas of
whichwere defined using an automated seeding algorithm oneach
slice. Further details of the algorithm are reported inRaine et al.
(2000).
Following our earlier study (Raine et al. 1992a), thefrontal
region w as defined as all cortex a nterior to the genuof the
corpus callosum and divided into left and righthemispheres along
the longitudinal fissure. Interrater relia-bility (intraclass
correlation coefficient) based on 23 scans(raters blind to each
other's ratings and group member-
50 4
-
8/12/2019 Raine et al,. (2002) - 'Prefrontal Structural and
Functional Deficits in Schizotypal Personality Disorder'
5/13
Prefrontal Structural and Functional Deficits Schizophrenia
Bulletin, Vol. 28, No. 3 , 2002
Table 3. Lifetime rates of alcohol and substance
abuse/dependence in the psychiatric control andschizophrenia
spectrum groups, together w ith usage in the past month
AlcoholAbuseDependencePast month
Sedatives-hypnotics-anxiolyticsAbuseDependencePast month
CannabisAbuseDependencePast month
StimulantsAbuseDependencePast monthOpioids
AbuseDependencePast monthCocaine
AbuseDependencePast monthHallucinogens/PCP
AbuseDependencePast monthPoly
AbuseDependencePast monthOther
AbuseDependencePast month
Psychiatriccontroln = 26)
23.138.57.73.83.80.0
19.231.315.411.57.70.00.03.80.07.730.80.0
23.17.70.00.00.00.07.70.00.0
Schizophreniaspectrumn = 16)
31.350.00.06.30.04.8
38.137.512.525.012.50.0
6.30.00.06.350.06.30
23.16.30.00.06.30.00.06.30.0
x1.80
1.290.74
1.30.80
0.071.76
2.25
1.6
1.670.45
1.66
2.86
df2
22
22
22
2
2
12
2
2
P0.46
0.260.69
0.260.67
0.800.41
0.32
0.45
0.190.98
0.20
0.24
Note x analyses were conducted on psychiatric disorder
categorization (absent-abuse-dependence) and on substance use in
pastmonth (yes/no). PCP = Phencyclidine.
ship) was as follows: left prefrontal gray 0.99, right
pre-frontal gray 0.99, left prefrontal white 0.93, right
pre-frontal w hite 0.94, total brain vo lume 0 .99.Statistical
Analyses. Repeated measures analyses ofvariance (ANOVAs) using the
mult ivariate approach(Vasey and Thayer 1987) were conducted on
left and righthemisphere volume measures in a 3 (groups) X 2 (left
and
right hemisphere) design for gray and white matter sepa-rately.
The ability of measures to predict group member-ship independent of
confounds was assessed using logisticregression and the Wald 2
statistic using a classificationcutoff of 0.5, with the Nagelkerke
statistic used for vari-ance estimation. Brain and neurocognitive
variables wereentered using a stepwise forward procedure (Wald)
withan entry probability of 0.05 and a removal probability of
50 5
-
8/12/2019 Raine et al,. (2002) - 'Prefrontal Structural and
Functional Deficits in Schizotypal Personality Disorder'
6/13
Schizophrenia Bulletin, Vol. 28, N o. 3 , 2002 A. Raine et
al.
Table 4. Mea ns standard deviations) and results of f test
comparisons for alcohol usage in thepsychiatric control and
schizophrenia spectrum groupsPsychiatriccontroln = 26)mean SD)
Schizophreniaspectrum(n =16)mean SD) df
Times used, past weekTimes used, past monthNo. of drinks wh en
drinkingLargest no. of drinks onone occasion
0.78(1.28)3.50 (5.03)2.70 (2.63)5.85(5.61)
1.63 (2.06)5.94 (7.02)2.56 (3.05)7.00 (8.24)
1.671.270.160.54
40404040
0.110.210.870.59
0.10. Other hypotheses were tested using ANOVA and ttests. All
tests of significance are 2-tailed with an alpha of0.05.The two
neuropsychological measures of frontal func-tioning (WCST and CPT)
each yielded four performancescores reflecting different aspects of
test performance. Toreduce the number of variables for analysis,
these eightsubscores were subjected to principal component
analysis,and factor scores from the first principal component
werecalculated using the regression method.
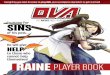
ResultsPrefrontal Structure. There was a main effect for groupon
prefrontal gray volumes, F(2,66) = 3.5, p = 0.037. Thespectrum
group had smaller prefrontal gray volumes thanboth comparisons, t=
2.6,d f=41, p = 0.011, and psychi-atric controls, / = 2.3 ,df= 40,p
=0.028 (figure 1). Th espectrum group showed a 12.4 percent
reduction in thevolume of prefrontal gray matter compared to the
compar-ison group, and a 13.2 percent reduction compared to
psy-chiatric controls .1 Corresponding effect sizes d) were0.84 and
0.73, respectively, and are in the large range(Cohen 1988). There
was no interaction between groupand hemisphere, F(2,66) = 0.1,p
=0.91 , but there was amain effect for hemisphere, F(l ,88) = 94.4,
p = 0.001,with the right hemisphere having higher gray volume
thanthe left. In contrast, there was no group difference in
pre-frontal white matter, F(2,66) = 0.14, p = 0.87 (figure 1),and
no group X he misphere interaction, F(2,66) = 0.54, p= 0.58. There
was a main effect for hemisphere, F(l,66)= 31 .5, p = 0.00 01,
indicating a larger volume of w hitematter in the left
hemisphere.
1 Groups were balanced for sex, but to assess for any
interactionsbetween group and sex, sex was entered as a second
factor in all analy-ses. No group x sex, F(2,62) = 0.78,p = 0.46,
or group x sex x hemi-sphere, F(2,62) = 0.79,p = 0.46, interactions
were observed.
Prefrontal gray was expressed as a function of wholebrain
volume. A repeated measures multivariate ANOVAconfirmed the main
effect for group, F(2,66) = 4.50,p =0.015. A breakdown of this
effect showed that the spec-trum group had smaller prefrontal/whole
brain volumesthan both comparisons,t=2.1,df= A\,p =0.044, and
psy-chiatric controls,t= 2.76,d f= 39 ,p=0.009. There was
nosignificant group X hemisphere interaction, F(2,66)
=0.09,/?=0.91,but the main effect for hemisphere, F(l,66)= 89.0,p
=0.000, again indicated relatively greater grayvolume in the right
hemisphere. There was no significantgroup difference in overall
brain volume, F(2,66) = 1.54, p=0.22.Frontal Neurocognitive
Functioning. The principalcomponent analysis of the eight subtests
from the WCSTand CPT produced a first factor that accounted for
47.9percent of the total unrotated variance. Percent persev-erative
errors was the highest loading WCST variable onthis factor, while
false alarm rate was the highest loadingCPT variable. Loadings on
this factor for the eight sub-tests were as follows: WCST percent
perseverative error0.86, total errors 0.85, number of categories
-0.79, trialsto first category 0.69; CPT false alarm rate 0.75, hit
rate-0 .45 , response bias -0.34, sensitivity -0.62. Given thatall
the loadings were greater than 0.30 and loaded in atheoretically
meaningful fashion, the factor was labeled frontal functioning,
with higher scores indicating poorerfrontal functioning.
Groups differed significantly on the frontal factor
score,F(2,59) =4.69,p=0.013 (table 5). The spectrum group
per-formed significantly more poorly on this global factor thandid
both the comparisons, t= 2.55,d f= 37 ,p =0.015, andthe psychiatric
controls,t=2.51,d f= 36 ,p=0.017.With respect to specific sub tests
of frontal functioning(table 5), groups differed significantly on
WCST trials tocomplete first trial, F(2,62) = 5.01,p = 0.010, and
CPTfalse alarms, F(2,63) = 4.85,p =0.011; and there was atrend for
CPT response bias, F(2,63) = 3.09,p =0.053.
506
-
8/12/2019 Raine et al,. (2002) - 'Prefrontal Structural and
Functional Deficits in Schizotypal Personality Disorder'
7/13
Prefrontal Structural and Functional Deficits Schizophrenia B
ulletin, Vol. 28, No. 3 , 2002
Figure 1. Prefrontal gray and white matter volumes in the three
groups
Prefrontal VolumeC on tro ls Psy chiatric
ControlsSchizotypals
cc
85
75
65
55
45 GRAY WHITETable 5. Group comparisons on the frontal factor
first principal component) and subtests of the WCSTand CPT
Frontal factorWCST
Trials to first category perseverative errorsTotal errorsNo.of
categoriesCP T
False alarmsResponse biasHit rateSensitivity
Comparisonn = 27),mean SD)
-0.27 (0.89)17.68(8.53)13.40(9.04)22.12(9.64)2.65 (1.44)0
035(0.065)0.58 (0.39)0.78 (0.26)0.91 (0.14)
Psychiatriccontrol n = 26),mean SD)
-0 .16 (0 .64 )19.36(10.21)15.21 (10.96)24.62
(9.52)2.27(1.25)0.019(0.020)0.66 (0.25)0.78 (0.25)0.93 (0.08)
Schizophreniaspectrumn = 16),mean SD)
0.60 (1.22)31.47(23.80)20.80(12.09)28.69(10.69)1.81 (1.33)0.071
(0.062)0.39 (0.40)0.70 (0.29)0.87(0.18)
F4.695.012.372.211.964.853.090.561.25
at2,592,622,652,652,652,632,632,632,63
0.0130.0100.1020.1180.1490.0110 0530 5720 294
Note CPT= Continuous Performance Test;SD=
standarddeviation;WCST=W isconsin Card Sorting Test.The spectrum
group had a significantly higher percentageof perseveration errors
on the WCST than did both com-parisons, / = 2.65,df= 38 ,p = 0.012,
and psychiatric con-trols, t= 2.23,df= 38 ,p =0.031.The spectrum
group alsohad a higher CPT false alarm rate than did psychiatric
con-trols, / = 3.86, df=38 ,p = 0.000, but the contrast with
comparisons was only marginally significant in the pre-dicted
direction, /=1.77,d f= 40,p = 0.084. The spectrumgroup had a poorer
response bias compared to psychiatriccontrols, / = 2.69,d f= 38 ,p=
0.01, but the contrast withcomparisons, while in the predicted
direction, was statisti-cally nonsignificant, t=1.57, df=
40,p=0.125.
507
-
8/12/2019 Raine et al,. (2002) - 'Prefrontal Structural and
Functional Deficits in Schizotypal Personality Disorder'
8/13
Schizophrenia Bulletin, Vol. 28, N o. 3, 2002 A. Raine et
al.
Independence of Structural and Functional PrefrontalDeficits.
The spectrum group was characterized by bothstructural and
functional prefrontal deficits. It has beenhypothesized that
structural deficits to the prefrontal cor-tex give rise to the
frontal functional deficits in this group.If this were the case,
then equating the three groups onprefrontal gray volume would
abolish the frontal func-tional deficits in the spectrum group.
This hypothesis wastested by entering prefrontal gray volumes in
the firstblock predicting spectrum grou p versus comparison
groupmembership in the logistic regression, and then enteringthe
frontal functional factor in a second block. Afterequating the
differences in prefrontal structure, group dif-ferences in frontal
functional deficits remained significant,X2=6.86, df=\,p = 0.0088,
indicating independence ofstructural and functional deficits.
Independence of struc-tural and functional deficits was confirmed
by the lack ofsignificant correlations between the frontal
functional fac-tor and prefrontal gray volumes in the entire sample
andin each of the three samples (all r 0.21).
Th i s i ndependence o f s t ruc t u ra l and func t i ona
ldeficits suggests that these factors account for
independentproportions of variance in the group difference
betweenthe spectrum and com parison groups. This hypothesis
wastested in a logist ic regression analysis with spectrumgroup
versus comparison group as the grouping variableand prefrontal gray
and the frontal factor as two predictorvariables entered on the
same block. Results are shown intable 6. Prefrontal gray h ad the
strong est relation to groupsand was entered first, accounting for
21.8 percent of thevariance in group membership. After entry of
prefrontalgray, the frontal functioning factor still significantly
pre-dicted group membership, almost doubling the percentageof
variance accounted for, from about 22 percent to about41 percent.
The variables together correctly classified 84.2percent of
subjects.Further Control for Substance Use. Although psychi-atric
controls and the spectrum group were matched onsubstance abuse, the
spectrum group had nonsignificantlyhigher rates of cocaine,
cannabis, stimulant, and sedativeuse than did psychiatric controls.
To further control for
the possible effects of these confounds on structural
andfunctional brain differences, these four variables
weresimultaneously entered as covariates and the above analy-ses
were repeated. After this control, group differencesstill remained
for prefrontal gray volume, F(2,62) = 4.29,p= 0.018 . For frontal
functioning, group differences weremarginally significant, F(2,61)
= 2.34, p = 0.066. Theabsolute group difference between spectrum
and compari-son groups was reduced only 9.7 percent after the
sub-stance abuse control, and this difference still
remainedsignificant, F(l,33) = 4.46,p=0.042.Possible C onfounding
Effect of Antisocial B ehavior.The significantly higher scores on
antisocial person ality inthe spectrum group relative to the two
other groups raisedthe question of whether prefrontal structural
deficits arean artifact of the increased antisocial behavior in the
spec-trum group. To test this possibility, a logistic
regressionanalysis was conducted in which prefrontal gray volumewas
used to predict spectrum versus comparison groupmembership after
controlling for the dimensional measureof antisocial personality
disorder. The schizotypy-pre-frontal gray relationship was
abolished, 2=0.001,d f= 1,p= 0.98, after controlling for antisocial
personality disor-der.2 In contrast, group differences on frontal
neurocogni-tive functioning remained after controlling for
antisocialpersonality, 2=7-23,df=\,p =0.007.
Because the spectrum group had nonsignificant lyhigher rates of
antisocial personality disorder and signifi-cantly higher scores on
the dimensional measure of antiso-cial personality than psychiatric
controls did, a completestatistical control was made on the
dimensional measureof antisocial personality disorder in logistic
regressions
2 Our previous findings of reductions in prefrontal gray volume
inindividuals with antisocial personality disorder (Raine et al.
2000) arenot a function of increased schizotypai personality in
this group because(1) the antisocial personality disorder group
showed reduced prefrontalvolume compared to a psychiatric control
group matched on schizophre-nia spectrum disorder, and (2) reduced
prefrontal gray differentiated theantisocial personality disorder
group from the control group after initialentry of schizotypai
personality in a logistic regression, x2 = 5.08,d f= 1,p=0.024.
Table 6. Logistic reg ression predicting schizotypai versus com
parison group m embership using pre-frontal gray and frontal
functioning as predictor variablesWald x 2entryStep 1: prefrontal
grayStep 2: frontal functioning
X26.606.86
df11
P0.0100.009
Nagelkerke R20.2180.408
Correct classification73.688 4 .2 1
Note.Nagelkerke R2 refers to total variance account for; correct
classification refers to the percentage of cases correctly
classified intogroups.
50 8
-
8/12/2019 Raine et al,. (2002) - 'Prefrontal Structural and
Functional Deficits in Schizotypal Personality Disorder'
9/13
Prefrontal Structural and Functional Deficits Schizophrenia
Bulletin, Vol. 28, No. 3, 2002
predicting group differences on structural and functionalfrontal
measures. Full control for antisocial personalityrendered the
previously significant group difference non-significant, x 2=
3.0,df= 1,p=0.08 3, but the group differ-ence in frontal
neurocognitive functioning remained sig-nificant, X2= 5.56,df=\,p
=0.018.
DiscussionFindings support the hypothesis that
schizotypal/paranoidpersonality disorder is characterized by
structural andfunctional prefrontal deficits. The spectrum group
showeda 12.4 percent reduction in the volume of prefrontal
graymatter compared to the comparison group, and a 13.2 per-cent
reduction compared to psychiatric controls. Corre-sponding effect
sizes d)were 0.84 and 0.73, respectively,and are in the large range
(Cohen 1988). These findingscould not be accounted for by
differences in whole brainvolume, alcohol and drug use, history of
head injury, orcomorbidity for affective and anxiety disorders.
Similargroup differences in functional frontal deficits were
found,with effect sizes of 0.80 for both comparisons and
psychi-atric controls. These functional frontal findings are
consis-tent with the previous literature showing robust WCSTand CPT
deficits in schizotypals, as noted earlier. Giventhat the spectrum
group also showed poorer prefrontalfunctioning compared to matched
psychiatric controls, thecurrent findings provide support for the
centrality offrontal structural and functional deficits in
schizophreniaspectrum disorders.
Structural prefrontal deficits were independent offunctional
deficits in schizophrenia spectrum patients.Though not predicted,
this result is consistent with the fail-ure of all three prior
cross-sectional studies that comparedschizophrenia patients to
controls and assessed prefrontalstructural deficits together with
frontal neurocognitivefunctioning (Andreasen et al. 1986; DeMyer et
al. 1988;DeLisi et al. 1991). Set against these three failures,
onelongitudinal study observed that frontal volume
reductionspredicted decline in executive functions over a
31-monthperiod (Gur et al. 1998), while one cross-sectional study
ofonly chronic schizophrenia patients showed that
reduceddorsolateral prefrontal area was associated with
impairedperformance on both the WCST and the CPT (Seidman etal
.1994). There are at least two possible explanations forthis lack
of structure-function association. First, if thestructural deficit
was localized to the orbitofrontal cortex,such damage might be less
likely to affect frontal neu-rocognitive measures, which have been
traditionally asso-ciated with dorsolateral prefrontal regions. In
support ofthis explanation, frontal neurocognitive measures
havebeen found within schizophrenia patients to correlate with
the dorsolateral but not the orbitofrontal area (Seidman etal .
1994). Second, it must be remembered that the neu-rocognitive
measures of frontal functioning used in thisstudy are complex
measures of executive/attentional func-tions that involve neural
networks outside of this brainregion. For example, the CPT is known
to activate bilat-eral frontal and occipital regions, together with
right tem-poral and parietal regions (Buchsbaum et al. 1990).
Fur-thermore, damage to subcortical structuresincluding thet h a l
a m u s , h i p p o c a m p u s , a n d a m y g d a l a w o u l d b
eexpected to interfere with tasks, such as the CPT andWCST, that
are dependent on the integrity of these pre-frontal-subcortical
circuits (Bilder et al. 1995). Futureimaging studies that both
segment prefrontal gray volumeinto structural subregions and assess
prefrontal and sub-cortical functioning using imaging techniques
with highspatial resolution (e.g., fMRI) are needed to elucidate
thecomplex interplay between prefrontal structure and func-tion.As
noted above, only 10.7-14.9 percent of structuralMRI studies of
schizophrenia have employed a psychi-atric control group. A
strength of the present study is theuse of a psychiatric control
group that controls for all AxisI and II disorders, unlike the few
studies that employ apsychiatric control group but control for only
one comor-bid disorder. As such , the structural and functional
deficitsfound in the spectrum group cannot be readily attributed
tomost comorbidity. Specifically, although rates of drug andalcohol
abuse/dependence in the spectrum group werequite high (possibly
reflecting self-medication for symp-toms in this
noninstitutionalized sample), we have previ-ously shown for this
sample that individuals dependent ondrugs or alcohol have
prefrontal gray volumes identical tocontrols (Raine et al. 2000).
Furthermore, the spectrumgroup was reasonably well matched to
psychiatric controlson substance use, and ad ditional control for
nonsignificantgroup differences on cannabis, sedatives, cocaine,
andstimulant use left resu lts essentially unchanged.
Findings on prefrontal structural deficits are consis-tent with
one prior community study showing an associa-tion between reduced
prefrontal volume and increasedschizotypy (Raine et al. 1992fc),
but the findings conflictwith those of a recent study by Downhill
et al. (2001)showing prefrontal volumes in schizotypal personality
dis-order that do not differ statistically from controls'.
Fur-thermore, Buchsbaum et al. (2002) have found higher, notlower,
glucose metabolic rates in Brodmann area 10 in 13patients with
schizotypy personality disorder, while areview by Siever et al.
(2002) similarly argues that schizo-typal patients may be spared
prefrontal structural deficitsand have greater prefrontal reserves
compared to schizo-phrenia patients. One possible explanation for
the contra-diction is that samples may differ in comorbidity with
anti-
50 9
-
8/12/2019 Raine et al,. (2002) - 'Prefrontal Structural and
Functional Deficits in Schizotypal Personality Disorder'
10/13
Schizophrenia Bulletin, Vol. 28, No. 3, 2002 A. Raine et al.
social personality. In the present community-derived spec-trum
sample with relatively high base rates of antisocialbehavior,
controlling for group differences in antisocialpersonality disorder
abolished the prefrontal gray volumedifference between the spectrum
and comparison groupsp = 0.98) and reduced the difference between
the spec-trum and psychiatric control groups to a
nonsignificantlevel p =0.083). Although significan t co morbidity
hasbeen reported between schizophrenia and violent criminalbehavior
(Belfrage 1998; Raesaenen et al. 1998; Volavka1999), control for
antisocial behavior has rarely, if ever,been included in studies of
schizophrenia and spectrumdisorders. On the other hand, group
differences in frontalfunctioning remained intact after controlling
for antisocialpersonal i ty and at test to the robustness of
functionalfrontal deficits in spectrum disorders. Ultimately,
patientswith both schizotypal and antisocial/impulsive featuresmay
have a somewhat different et iology compared toschizotypal patients
lacking these features. Consequently,controlling for antisocial
comorbidity in future studies ofschizophrenia and schizophrenia
spectrum disorders mayhelp clarify conflicting findings and produce
a clearer pic-ture of the unique risk factors for spectrum
disorders.
The effect size d) of 0.84 for the structural prefrontalgray
volume reduction in the spectrum group compared tothe comparison
group is relatively large (Cohen 1988).Although one limitation of
the current study is that aschizophrenia patient group with which
to compare effectsizes was not included, a recent meta-analysis
(Yaralianand Ra ine 2000) observe d an overall effect size of 0.42
forfrontal gray loss in schizophrenia patients compared tocontrols.
In comparison, the doubling of the effect size inspectrum
individuals could be interpreted as highlightingthe advantage of
studying noninstitutionalized spectrumindividuals from the
community who do not share themethodological confounds that apply
to institutionalizedschizophrenia patients. Alternatively, comorbid
antisocialbeha vior m ay contribute to the effect size obtained for
pre-frontal structure, although this argument cannot explainthe
large effect size of 0.8 found for functional
prefrontaldeficits.
In conclusion, schizophrenia spectrum disorder ischaracterized
by reduced prefrontal gray volumes andreduced frontal functioning
compared to both comparisonand psychiatric control groups. Though
these results sup-port the potential etiologic significance of
prefrontal struc-tural deficits in schizophrenia, the possibility
exists thatthese effects are abolished by careful control for
antisocialpersonality, comorbidity that may account for
discrepantfindings in the literature. In contrast, in the spectrum
groupwe observed functional deficits of equal magnitude thatcannot
be accounted for by either structural deficits orcomorbid
antisocial behavior.
ReferencesAmerican Psychiatric Association. Diagnostic and
Statis-tical Manual of Mental Disorders. 4th ed. Washington,DC:APA,
1994.Andreasen, N.C.; Ehrhardt, J.C.; Swayze, V.W.; Alliger,R.J.;
Yuh, W.T.C.; Cohen, G.; and Ziebell, S. Magneticresonance imaging
of the brain in schizophrenia. Archivesof
GeneralPsychiatry,47:35^14, 1990.Andreasen, N.C.; Flashman, L.;
Flaum, M.; Arndt, S.;Swayze, V.; O'Leary, D.S.; Ehrhardt , J .C.;
and Yuh,W.T.C. Regional brain abnormalities in
schizophreniameasured wi th magnet ic resonance imaging .
JAMA,272:1763-1769, 1994.Andreasen, N.C.; Nasrallah, H.A.; Dunn,
V.; Olson, S.C.;Grove, W.M.; Ehrhardt, J.C.; Coffman, J.A.; and
Crossett,J.H.W. Structural abnorm alities in the frontal system in
schiz-ophrenia.ArchivesofGeneralPsychiatry,43:136-144,1986.Battaglia,
M.; Abbruzzese, M.; Ferri, S.; and Scarone, S.An assessment of the
Wisconsin Card Sorting Task as anindicator of liability to
schizophrenia. SchizophreniaResearch, 14:39^15, 1994.Belfrage, H. A
ten-year follow-up of criminality in Stock-holm mental patients.
British Journal of Criminology,38:145-155, 1998.Bilder, R.M.;
Bogerts, B.; Ashtari, M.; and Wu, H. Ante-rior hippocampal volume
reductions predict frontal lobedysfunction in first episode
schizophrenia. SchizophreniaResearch, 17:47-58, 1995.Bilder, R.M.;
Wu, H.; Bogerts, B.;Degreef G.; Ashtari,M.; Alvir, J .M.J. ;
Snyder, P.J . ; and Lieberman, J .A.Absence of regional hemispheric
volume asymmetries infirst-episode schizoph renia. American Journal
of Psychia-try, 151:1437-1447, 1994.Breier, A.; Buchanan, R.W.;
Elkashef A.; Munson, R.C.;Kirkpatrick, B.; and Gellad, F. Brain
morphology and schizo-phrenia.Archiveso fGeneralPsychiatry,
49:921-926, 1992.Bryden, M.P. Measuring handedness with
questionnaires.Neuropsychologia, 15:617-624, 1977.Bucha nan, R.W.;
Breier, A.; Kirkpatrick, B .;Elkashef A.;Munson, R.C.; Gellad, F.;
and Carpenter, W.T. Structuralabnormalities in deficit and
nondeficit schizophrenia.American Journal of Psychiatry, 150:59-65,
1993.Buchanan, R.W.; Vladar, K.; Barta, P.E.; and Pearlson,G.D.
Structural evaluation of the prefrontal cortex inschizophrenia.
American Journal of Psychiatry,155:1049-1055, 1998.Buchsbaum, M.S.
The frontal lobes, basal ganglia, andtemporal lobes as sites for
schizophrenia. SchizophreniaBulletin, 16(3):379-389, 1990.
51 0
-
8/12/2019 Raine et al,. (2002) - 'Prefrontal Structural and
Functional Deficits in Schizotypal Personality Disorder'
11/13
Prefrontal Structural and Functional Deficits Schizophrenia B
ulletin, Vol. 28, No. 3 , 2002
Buchsbaum, M.S.; Nenadic, I.; Hazlett, E.A.; Spiegel-Cohen, J.;
Fleischman, M.B.; Akhavan, A.; Silverman,J.M.; and Siever, L.J.
Differential metabolic rates in pre-frontal and tempo ral Brodmann
areas in schizophrenia andschizotypal personality disorder.
Schizophrenia Research,54(l-2):141-150, 2002.Buchsbaum, M.S.;
Nuechterlein, K.H.; and Haier, R.J.Glucose metabolic rate in
normals and schizophrenics dur-ing the Continuous Performance Test
assessed by positronemiss ion tomography. British Journal of
Psychiatry,156:216-227, 1990.Buchsbaum , M .S.; Yang, S.; Hazlett,
E.; Siegel, B.V.; Ger-mans, M.; Haznedar, M.; O'Flaithbheartaigh,
S.; Wei, T.;Silverman, J.; and Siever, L.J. Ventricular volume
andasymmetry in schizotypal personality disorder and schizo-phrenia
assessed with magnetic resonance imaging.Schiz-ophrenia
Research,27:45-53, 1997.Cannon, T.D. Abnormalities of brain
structure and func-tion in schizophrenia: Implications for
aetiology in patho-physiology.Annals of Medicine,
28:533-539,1996.Cannon, T.D.; Mednick, S.A.; Parnas, J.;
Schulsinger, E;Praestholm, J.; and Vestergaard, A. Developmental
brainabnormalities in the offspring of schizophrenic mothers:II .
Structural brain characteristics of schizophrenia andschizotypal
personality disorder.Archives ofGeneralPsy-chiatry,51:955-962,
1994.Cohen, J. Statistical Power Analysis for the
BehavioralSciences.2nd ed. Hillsdale, NJ: Lawrence Erlbaum,
1988.Dane luzzo, E.; Bustini, M.; S tratta, P.; Casacchia, M.;
andRossi A. Schizotypal Personality Questionnaire and Wis-consin
Card Sorting Test in a population of DSM-IH-Rschizophrenic patients
and control subjects. Comprehen-sive Psychiatry,39:143- 148,
1998.DeLisi, L.E.; Hoff A.L.; Schwartz, J.E.; Shields,
G.W.;Halthore, S.N.; Gupta, S.M.; Henn, F.A.; and Anand, A.K.Brain
morphology in first-episode schizophrenic-like psy-chotic patients:
A quantitative magnetic resonance imag-ing study.Biological
Psychiatry,29:159-175, 1991.DeMyer, M.K.; Gilmor, R.L.; Hendrie,
H.C.; DeMyer,W.E.; Augustyn, G.T.; and Jackson, R.K. Magnetic
reso-nance brain images in schizophrenic and normal
subjects:Influence of diagnosis and education. Schizophrenia
Bul-letin, 14(l):21-33, 1988.Di ckey , C . C . ; McC ar l ey , R .
W . ; Vog l m ai e r , M. M. ;Niznikiewicz, M.A.; Seidman, L.J.;
Hirayasu, Y.; Fischer,I.; Teh, E.K.; van Rhoads, R.; Jakab, M.;
Kikinis, R.;Jolesz, F.A.; and Shenton, M.E. Schizotypal
personalitydisorder and MRI abnormalities of temporal lobe
graymatter.Biological Psychiatry,45:1392-1402, 1999.Downhil l , J
.E.; Buchsbaum, M.S.; Wei, T.; Spiegel-Cohen, J.; Hazlett, E.A.;
Haznedar, M.M.; Silverman, J.;
and Siever, L.J. Shape and size of the corpus callosum
inschizophrenia and schizotypal personality disorder.Schiz-ophrenia
Research,42:193-208, 2000.Downhill, J.E.; Hazlett, E.A.; Barth, S.;
Roitman, S.L.;Nun n , M. ; Lekarev , O . ; W ei , T . ; S h i h abu
dd i n , L . ;Mitropoulou, V.; Silverman, J.; and Siever, L.J.
Temporallobe volume determined by magnetic resonance imagingin
schizotypal personality disorder and schizophrenia.Schizophrenia
Research,48:187-199, 2001.First, M.B.; Spitzer, R.L.; Gibbon, M.;
and Williams,J.B.W. Structured Clinical Interview for Axis I
DSM-IVDisorders SCID,Version2.0).New York, NY: New YorkState
Psychiatric Institute, 1994a.First, M.B.; Spitzer, R.L.; Gibbon,
M.; Williams, J.B.W.;and Benjamin , L . Structured Clinical
Interview forDSM-IV Axis II Personality Disorders(SCID-II,
Version2.0). New York, NY: New York State Psychiatric
Institute,Frazier, J.A.; Giedd, J.N.; Hamburger, S.D.; Albus,
K.E.;Kaysen, D .; Vaituzis, A.C.; Rajapakse, J.C.; Lenan e, M.C
.;McKenna, K.; Jacobsen, L.K.; Gordon, C.T.; Breier, A.;and
Rapoport, J.L. Brain anatomic magnetic resonanceimaging in
childhood-onset schizophrenia. Archives ofGeneral
Psychiatry,53:617-624, 1996.Grant , A.D., and Berg, E.A. A
behavioral analysis ofdegree of reinforcement and ease of shift ing
to newresponses in a Weigl-type card sorting problem .Journal
ofExperimental Psychology,38:404-^11, 1948.Gur, R.E.; Cowell, P.;
Turetsky, B.I.; Gallacher, F.; Can-non, T; Bilker, W.; and Gur,
R.C. A follow-up magneticresonance imaging study of schizophrenia:
Relationship ofneuroanatomical changes to clinical and
neurobehavioralmeasures. Archives of General Psychiatry,
55:145-152,1998.Heinrichs, R.W., and Zakzanis, K.K. Neurocognit
ivedeficit in schizophrenia: A quantitative review of the
evi-dence.Neuropsychology, 12:426-445, 1998.Hollingshead, A.B. Four
Factor Index of Social Status.Unpublished manuscript,
1975.Ingraham, L.J. Familygenetic research and
schizotypalpersonality. In: Raine, A.; Lencz, T.; and Mednick,
S.A.,eds. Schizotypal Personality. Cambridge, U.K. : Cam-bridge
University Press, 1995. pp. 19-42.Lenzenweger, M.F., and Korfine,
L. Perceptual aberra-tions, schizotypy, and the Wisconsin Card
Sorting Test.Schizophrenia Bulletin, 20(2):345-357, 1994.Lim, K.O.;
Beal, M.; Harvey, R.L.; Myers, T; Lane, B.;Sullivan, E.V.;
Faustman, W.O.; and Pfefferbaum, A.Brain dysmorphology in adults
with congenital rubellaplus schizophrenia-like symptoms. Biological
Psychiatry,37:764-776, 1995.
51 1
-
8/12/2019 Raine et al,. (2002) - 'Prefrontal Structural and
Functional Deficits in Schizotypal Personality Disorder'
12/13
Schizophrenia Bulletin, Vol. 28, No. 3, 2002 A. Raine et al.
Lim , K.O .; Sulliv an, E.V.; Zipurs ky, R.B.; and Pfeffer-baum,
A. Cortical gray matter volume deficits in schizo-phrenia: A repl
icat ion. Schizophrenia Research,20:157-164, 1996.Lyons, M.J.;
Merla, M.E.; Young, L.; and Kremen, W.S.Impaired neuropsychological
functioning in symptomaticvolunteers with schizotypy: Preliminary
findings. Biologi-cal Psychiatry, 30:424-426, 1991.Nigg, J.T., and
Goldsmith, H.H. Genetics of personalityd i s o rde r s : P e r s
pec t i ves f rom pe r s ona l i t y and p s y -chopathology
research. Psycho logical Bulletin,115:346-380, 1994.Nopoulos, P. ;
Torres, I . ; Flaum, M.; Andreasen, N.C.;Ehrha rdt, J.C.; and Yuh,
W.T.C. Brain morphology in first-episode schizophrenia. American
Journal of Psychiatry,152:1721-1723, 1995.Nuechterlein, K.H.;
Parasuraman, R.; and Jiang, Q. Visualsustained at tent ion: Image
degradat ion produces rapiddecrement over time.Science, 22:327-329,
1983.Park, S.; Holzman, P.S.; and Goldman-Rakic, P.S.
Spatialworking memory deficits in the relatives of schizophrenicpat
ients . Archives of General Psychiatry, 52 : 821 -828
,1995.Raesaenen, P.; Tiihonen, J.; Isohanni, M.; Rantakallio,
P.;Lehtonen, J.; and Moring, J. Schizophrenia, alcohol abuse,and
violent behavior: A 26-year follow-up study of an un-selected birth
cohort . Schizophr enia Bulletin,24(3):437-441, 1998.Raine, A.;
Lencz, T.; Bihrle, S.; Lacasse, L.; and Colletti,P. Reduced
prefrontal gray matter volume and reducedautonomic act ivi ty in
ant isocial personal i ty disorder.Archives of General Psychiatry,
57:119-127, 2000.Raine, A.; Lencz, T.; Reynolds, G.P.; Harrison,
G.; Sheard,C ; M edley, I.; Rey nolds, L.M.; and Cooper, J.E. An
evalu-ation of structural and functional prefrontal deficits
inschizophrenia: MRI and neuropsychological measures.Psychiatry
Research: Neuroimaging, 45:123-137, 1992a.Raine, A.; Sheard, S.;
Reynolds, G.P.; and Lencz, T. Pre-frontal structural and functional
deficits associated withindividual differences in schizotypal
personality. Schizo-phrenia Research, 7:237-247, 1992ft.Roitman,
S.E.L.; Cornblatt, B.A.; Bergman, A.; and Obu-chowski, M.
Attentional functioning in schizotypal per-sonali ty disorder.
American Journal of Psychiatry,154:655-660, 1997.Schlaepfer, T.E.;
Harris, G .J.; Tien, A.Y.; Peng, L.W.; Lee,S.; Federman, E.B.;
Chase, G.A.; Barta, P.E.; and Pearl-son, G.D. Decreased regional
cortical gray matter volumein schizophrenia. American Journal of
Psychiatry,151:842-848, 1994.
Seidman, L.J.; Yurgelun-Todd, D .; Krem en, W.S.; Woods,B.T.;
Goldstein, J.M.; Faraone, S.V.; and Tsuang, M.T.Relationship of
prefrontal and temporal lobe MRI mea-sures to neuropsychological
performa nce in chronic schiz-ophrenia.Biological
Psychiatry,35:235-246, 1994.Siever, L.J.; Kalus, O.F.; and Keefe,
R.S.E. The bound-aries of schizophrenia.Psychiatric Clinics of
North Amer-ica, 16:217-244, 1993.Siever, L.J.; Koenigsberg, H.W.;
Harvey, P.; Mitropoulou,V.; Laruelle, M.; Abi-Dargham, A.; Goodman,
M.; andBuchsbaum, M. Cognitive and brain function in schizo-typal
personality disorder. Schizophrenia Research,54(1-2) :157-167.S
iever , L .J . ; Rot ter , M. ; Losonczy, M. ; Guo, S .L.
;Mitropoulou, V.; Trestman, R.; Apter, S.; Zemishlany,
Z.;Silverman, J.; Horvath, T.B.; Davidson, M.; M ohs, R.; andDavis,
K.L. Lateral ventricular enlargement in schizotypalpersonality
disorder. Psychiatry Research, 57:109-118,1995.Suddath, R.L.;
Casanova, M.F.; Goldberg, T.E.; Daniel,D.G.; Kelsoe, J.R.; and
Weinberger, D.R. Temporal lobepathology in schizophrenia: A
quantitative magnetic reso-nance imaging study. American Journal of
Psychiatry,146:464-472, 1989.Sullivan, E.V.; Mathalon, D.H.; L im,
K .O.; Marsh, L.; andPfefferbaum, A. Patterns of regional cortical
dysmorphol-ogy distinguishing schizophrenia and chronic
alcoholism.Biological Psychiatry,43:118-131, 1998.Szeszko, PR.;
Bilder, R.M.; Lencz, T.; Pollack, S.; Alvir,J.M.J.; Ashtari, M.;
Wu, H.; and Lieberman, J.A. Investi-gation of frontal lobe
subregions in first-episode schizo-phrenia. Psychiatry Research in
Neuroimaging, 90:1-15,1999.Torgersen, S. Personality deviations
within the schizo-phrenia spectrum. Ada Psychiatrica
Scandinavica,90:40-44, 1994.Trestman, R.L.; Keefe, R.S.E.;
Mitropoulou, V.; Harvey,P.D.; deVegvar, M.L.; Lees-Roitman, S.;
Davidson, M.;Aronson, A.; Silverman, J.; and Siever, L.J.
Cognitivefunction and biological correlates of cognitive
perform-ance in schizotypal personal i ty disorder.
PsychiatryResearch,59:127-136, 1995.Vasey, M.W., and Thayer, J.F.
The continuing problem offalse posi t ives in repeated measures
ANOVA in psy-chophysiology: Multivariate solution.
Psychophysiology,24:479-486, 1987.Velakoulis, D., and Pantelis, C.
What have we learnedfrom functional imaging studies in
schizophrenia? Therole of frontal, striatal, and temporal
areas.Australian andNew Zealand Journal of Psychiatry,30:195-209,
1996.
512
-
8/12/2019 Raine et al,. (2002) - 'Prefrontal Structural and
Functional Deficits in Schizotypal Personality Disorder'
13/13
Prefrontal Structural and Functional Deficits Schizophrenia
Bulletin, Vol. 28, No. 3, 2002
Ventura, J.; Liberman, R.P.; Green, M.F.; Shaner, A.; andMintz,
J. Training and quality assurance with StructuredClinical
Interviews for DSM-IV (SCID-I/P). PsychiatryResearch, 79:163-173,
1998.Voglmaier, M.M.; Seidman, L.J . ; Sal isbury, D.; andMcCarley
, R .W. Neuropsychological dysfunct ion inschizotypal personality
disorder: A profile analysis. Bio-logical Psychiatry,41:530-540,
1997.Volavka, J. The neurobiology of violence: An update.Journal of
Neuropsych iatry and Clinical Neuroscience s,11:307-314,
1999.Wechsler, D. Wechsler Adult Intelligence Scale-Revised.New
York, NY: The Psychological Corporation, 1981.Weinberger, D.R., and
Berm an, K.F. Prefrontal function inschizophrenia: Confounds and
controversies. In: Roberts,A.C. , and Robbins, T.W., eds. The
Prefrontal Cortex:Executive and Cognitive Functions. New York,
NY:Oxford University Press, 1998. pp. 165-180.Wible, C.G.; Shenton,
M.E.; Hokama, H.; Kikinis, R.;Jolesz, F.A.;Metcalf D.; and
McCarley, R.W. Prefrontalcortex and schizophrenia: A quantitative
magnetic reso-nance imaging study. Archives o f General
Psychiatry,52:279-288, 1995.Yaralian, P.S., and Raine, A. Me ta-An
alysis of Fronta lLobe Size in Schizophrenia as Assessed by
Magnetic Res-onance Ima ging. Poster presented at the Society
forResearch in Psychopathology annual meeting,
Boulder,CO,November-December 2000.Yeo, R.A.; Hodde-Vargas, J.;
Hendren, R.L.; V argas, L.A.;Brooks, W.M.; Ford, C.C.; Gangestad,
S.W.; and Hart,B.L. Brain abnormalities in schizophrenia-spectrum
chil-dren: Implications for a neurodevelopmental
perspective.Psychiatry Research: Neuroimaging,76:113, 1997.
Zakzanis, K.K., and Heinrichs, R.W. Schizophrenia andthe frontal
brain: A quantitative review. Journal of theInternational
Neurological Society, 5:556-566, 1999.Zipursky, R.B.; Lim, K.O.;
Sullivan, E.V.; Brown, B.W.;and Pfefferbaum, A. Widespread cerebral
gray matter vol-ume deficits in schizophrenia.Archives of General
Psychi-atry,49:195-205, 1992.AcknowledgmentsThe authors wish to
thank Jennifer Bobier, Nicole Diamond,Kevin H o, Blane Horvath,
Shari Mills, and K risten Taylor forassistance in data collection
and sco ring, and Keith N uechter-lein for providing the Continuous
Performance Test. Thisstudy was supported by grants to the first
author from theNational Institute of Mental Health (RO3
MH50940-O1A2,and an Independent Scientist Award K02 M H01 114-0
1).The AuthorsAdrian R aine, D.Phil., is Robert G. W right
Professor of Psy-chology, Department of Psychology, University of
SouthernCalifornia (USC), Los Angeles, CA. Todd Lencz, Ph.D.,
isResearch Psychologist, Department of Research, HillsideHospital
(North Shore-Long Island Jewish Health System),Glen Oaks, New York.
Pauline Yaralian, M.A., is ResearchAssistant; Susan Bihrle, Ph.D.,
is Research Associate; andLori LaCasse, B.A., is Research
Coordinator, Department ofPsychology, USC. Joseph Ventura, Ph.D.,
is Assistant Pro-fessor, Department of Psychiatry and Biobehavioral
Sci-ences, University of California Los Angeles, Los Angeles,CA.
Patrick Colletti, M.D., is Chief of Magnetic ResonanceImaging and
Professor of Radiology, Department of Radiol-ogy, USC School of
Medicine.