Embed Size (px)
Citation preview

6/2/2014
1
Left Main Coronary Disease:Assessment and Treatment for
Imagers, Interventionalists and
Surgeons
Michael Ragosta MD
Director, Cardiac Catheterization Laboratories
Professor of Medicine
University of Virginia Health System
Charlottesville, VA
Disclosure Information
Michael Ragosta MD
The following relationships exist related to this presentation:
Grant support (GS), consultant (C), speakers bureau (SB), stock options (SO), equity interest (EI):
Grant Support: Principal Investigator of EXCEL
Off label use of products discussed in this presentation:
NONE
A Brief History of Left Main Coronary Disease…..
First described in 1912 by Herrick
Recognized as high risk subgroup in 1960’s
Cathing left main disease during 60’s-70’s was
dangerous! (10-15% mortality) Cohen et al Circ 1972 45 Suppl I. I: 57 and Lavine et al AJH 1972;30:791
Early 1970’s: Survival with CABG better than
natural history
Late 1970’s: Trials of medical therapy vs CABG
Gruntzig: Balloon for left main disease in 1978.

6/2/2014
2
What’s so special about left
main disease?
1. Left main supplies 75% myocardium if right
dominant; 100% if left dominant
2. 4-6% of patients undergoing coronary
angiography
3. Disease is more complex; higher rate of multi-
vessel disease (70-80%)
Some facts about Left Main
Disease Anatomy…
1. Several, very different patterns of left main
involvement (ostial, mid-body, distal
bifurcation)
2. Isolated left main stem disease is rare! (9%)
3. Most patients (70-80%) with left main stem
disease have multivessel disease.
4. That other disease is usually very complex.
The Spectrum of Left Main Disease
ANATOMY
OstialDistal bifurcation/trifurc

6/2/2014
3
Unprotected Left Main StemExtent of Coexisting CAD
%
Pts
Number of Vessels Diseased
Ragosta et al CCI 2006;67:357–362.
Isolated
Left Main
9%
Unprotected Left Main StemPrevalence of Unfavorable Characteristics for PCI
%
Pts
AnyUnfavorable
Characteristic
Ragosta et al CCI 2006;67:357–362.
Diagnosis of Left Main Disease
1. Non-invasive imaging
2. Coronary angiography
3. Adjuncts to coronary angiography
Intravascular ultrasound
Fractional flow reserve (FFR)

6/2/2014
4
Non-Invasive Imaging of Left Main Disease
1. Yes, there are findings on stress testing
associated with left main disease
2. No, they are not very specific or helpful.
“High risk” findings also associated with multi-
vessel disease, LV dysfunction.
Concept of “balanced ischemia” might limit
conventional MPI at identifying significant left
main disease
CTA can identify left main disease but…
Coronary Angiography and Left Main Disease
1. Left main is surprisingly difficult to clearly
image on coronary angiography
2. Left main is subject to greatest degree of
observer variability than any other segment (Int J
Cardiol 2007;120:254-61)
Limitations of Coronary Angiography for
Assessment of Left Main Disease
Short segment
Foreshortening
Overlapping vessels
Diffuse disease: what is reference?
Catheter artifacts
Eccentric lesions
Ostial lesions hard to see
Reflux of contrast in aortic sinus
Bifurcation hard to see

6/2/2014
5
Percent Stenosis is Often Wrong!
In an IVUS study of left main disease:
33% of LM lesions with <30% stenosis had
minimal luminal area by IVUS of < 6 mm2
43% of LM lesions with >50% stenosis had
minimal luminal area by IVUS of > 6 mm2
JACC 2011;58:351-8

6/2/2014
6
Adjuncts to Coronary Angiography Are Often
Necessary for Optimal Left Main Assessment
1. Fractional Flow Reserve (FFR)• FFR < 0.80 is “significant”
• Can be problematic if disease in LAD/LCX (which
there often is)
2. Intravascular Ultrasound
FFR limited by
downstream disease
JACC Intv 2012;5:697-707
What is a “Significant” Left Main Lesion by IVUS?
MLA
(mm2)
n Validation Citation
< 7.5 214 Outcomes with deferral JACC 2005;45:204-11
< 5.9 55 Correlated with FFR < 0.75 Circ 2004;110:2831-36
< 4.8 55 Correlated with FFR < 0.80
Note: Korean population
JACC Intv 2011;4:1168-74
< 6.0 351 Outcomes with deferral JACC 2011;58:351-8
MLA < 6.0 mm2 generally
accepted as the cut-off value for
significant left main disease by
IVUS

6/2/2014
7
Treatment of Left Main Disease
Surgery
Percutaneous Coronary Intervention
Surgery for Management of Left Main
Disease
1. CABG considered the “gold standard”
2. Data comes from ancient and small,
randomized controlled trials
3. Need to understand current outcomes data
regarding surgery for left main stem disease
Randomized Trials of Medical Therapy vs CABG
Left Main Disease
Three trials:
VA Cooperative Study
European Coronary Surgery Study Group
Collaborative Study in Coronary Artery Surgery (CASS)
Enrolled patients in the early 1970’s
VA 1972-1974
CASS 1974-1979
ECSSG 1973-1976
Randomized to CABG or medical therapy
Different enrollment criteria.
CASS excluded significant L main disease

6/2/2014
8
VA Cooperative
StudyRandomized, angina
>50% stenosis
Medical n = 43
Surgical n = 48Circulation 1982;66:14-22
European Coronary Surgery Study GroupRandomized, mild to moderate angina, >50% stenosis
Medical n = 31; Surgical n = 28Lancet 1982;1173-1180
CASS Registry1492 patients with LM disease, Not randomized
Medical n = 309; Surgical n = 1183Am J Cardiol 1981;48:765-777

6/2/2014
9
CASS Registry: 15 yr survivalBased on % stenosis of left main
Caracciolo E et al. Circulation 1995;91:2325-2334
Surgery
Medical
Medical n = 25
Surgical n = 26Circulation. 1989;79:1171-1179
CASS Registry
Asymptomatic Patients
Criticisms of This Evidence
1. Very small data sets
2. Angiographic based, 50-70% stenosis group is
problematic
3. Quality of medical therapy was pathetic (66%
on beta blocker, 18% on aspirin, no statins)
4. Surgery group wasn’t optimal either (10% got
IMA)

6/2/2014
10
Current Outcomes Data with Surgery
Taggart et al JACC 2008;51:885-892
AVERAGE
Time Survival Freedom from
Revasc
30 day 97.6% 99.7%
1 year 93.6% 98.9%
5 year 83% 89%
10 year 64% 76%
Sabik et al Circ 2007;116(Suppl)I:232-239
“Benchmark” Data Regarding Outcomes of
CABG for Left Main Disease
A study of long term outcomes of 3803 patients
with LMCD operated on at the Cleveland Clinic
from 1971-1998
PCI for Left Main Disease:
Balloon Angioplasty
Gruentzig first attempted (unsuccessfully) in 1978 (Lancet 1978;311:263)
First series published in 1989 (Am J Cardiol 1989;64:144-7)
33 elective, unprotected left main POBA
9.1% procedural mortality
36% 3 year survival
6/2/2014
11
PCI for Left Main Disease:
Bare Metal Stents
Lots of non-randomized series and registries in
highly selected patients
Highly variable outcomes depending on
population enrolled
Restenosis was, of course, a problem and was
sometimes associated with sudden death
PCI for Left Main Disease:
Drug Eluting Stents
Again, began with lots of non-randomized series
showing good outcomes
Huge selection bias regarding anatomy and
patient characteristics
Evolving randomized trials comparing surgery to
drug eluting stents
The Spectrum of Left Main PCICLINICAL SCENARIOS
“Bailout” procedure due
to complication of cath
Acute MI with an
occluded left main stem
Poor surgical candidate
from comorbid illness
Surgical candidate but
patient refuses surgery
Good operative
candidate

6/2/2014
12
Unprotected LMCA PCI: Bail-Out IndicationExisting LMCA disease with closure during diagnostic cath
Determining options……..
PATIENT
CHARACTERISTICS
LV Function
Clinical Syndrome
Aortic calcification
Comorbidity
Age
Lungs
Kidneys
Vascular disease
Dementia
Frailty
DAPT
Other
ANGIOGRAPHIC
CHARACTERISTICS
Extent of disease
Quality of targets
Likelihood of successful PCI
Completeness of revascularization

6/2/2014
13
Patient Selection: Surgical Candidacy
Tools to estimate patient risk:
STS Calculator
Euroscore
Don’t account for variables such as pulmonary
hypertension, cirrhosis of the liver, “porcelain
aorta”.
“Heart Team” approach, similar to those used
for transcatheter valve procedures, should be
applied to left main patients
Patient Selection: The SYNTAX Score
Takes into consideration multiple features:• Dominance
• Number of lesions and segments involved
• Presence of total occlusion, age and features
predicting success
• Nature and presence of disease of trifurcation or
bifurcation
• Aorto-ostial disease
• Severe tortuosity
• Length > 20 mm
• Heavy calcification
• Thrombus
• Diffuse disease
www.syntaxscore.com
What do our Guidelines say about
unprotected left main PCI?
PCI Guidelines
Appropriate Use Criteria

6/2/2014
14
A Heart Team approach to revascularization is
recommended in patients with unprotected
left main or complex CAD.
Calculation of the STS and SYNTAX scores is
reasonable in patients with unprotected left
main and complex CAD.
Heart Team Approach to
Revascularization Decisions
I IIa IIb III
I IIa IIb III
CABG to improve survival is recommended for patients with significant (≥50% diameter stenosis) left main CAD.
PCI to improve survival is reasonable as an alternative to CABG in selected stable patients with significant LM CAD with: 1) anatomic conditions associated with a low risk of PCI procedural complications and a high likelihood of a good long-term outcome (low SYNTAX score [≤22], ostial or trunk left main CAD); and 2) clinical characteristics that predict an increased risk of adverse surgical outcomes (STS-predicted risk of operative mortality ≥5%).
Revascularization to Improve Survival:
Unprotected Left Main CAD Revascularization
I IIa IIb III
I IIa IIb III
PCI to improve survival is reasonable in patients with UA/NSTEMI when LM is the culprit lesion and patient not eligible for CABG.
PCI to improve survival is reasonable in patients with acute STEMI when LM is the culprit lesion, distal coronary flow is <TIMI 3 and PCI can be performed more rapidly and safely than CABG.
I IIa IIb III
I IIa IIb III
PCI to improve survival may be reasonable in selected stable patients with LM CAD with:
1) anatomy associated with low- intermediate risk of PCI complications and an intermediate to high likelihood of good long-term outcome (SYNTAX score of <33, bifurcation left main)
and
2) clinical characteristics that predict an increased risk of adverse surgical outcomes (COPD, prior stroke, or cardiac surgery; STS-predicted risk of operative mortality >2%).
I IIa IIb III

6/2/2014
15
PCI to improve survival should not be
performed in stable patients with
significant (≥50% diameter stenosis)
unprotected left main CAD who have
unfavorable anatomy for PCI and who
are good candidates for CABG.
I IIa IIb III
Harm
When is Unprotected Left Main PCI Appropriate?
JACC 2012;59:857-81
Attractive features:
• proximal location
• large diameter vessel
High risk/Unattractive features:
• large vascular territory
• potential cardiovascular collapse with ischemia
• often involves bifurcation or ostium
• presence of other CAD not treatable by PCI
• restenosis
• stent thrombosis likely a fatal event
Unprotected Left Main PCI
6/2/2014
16
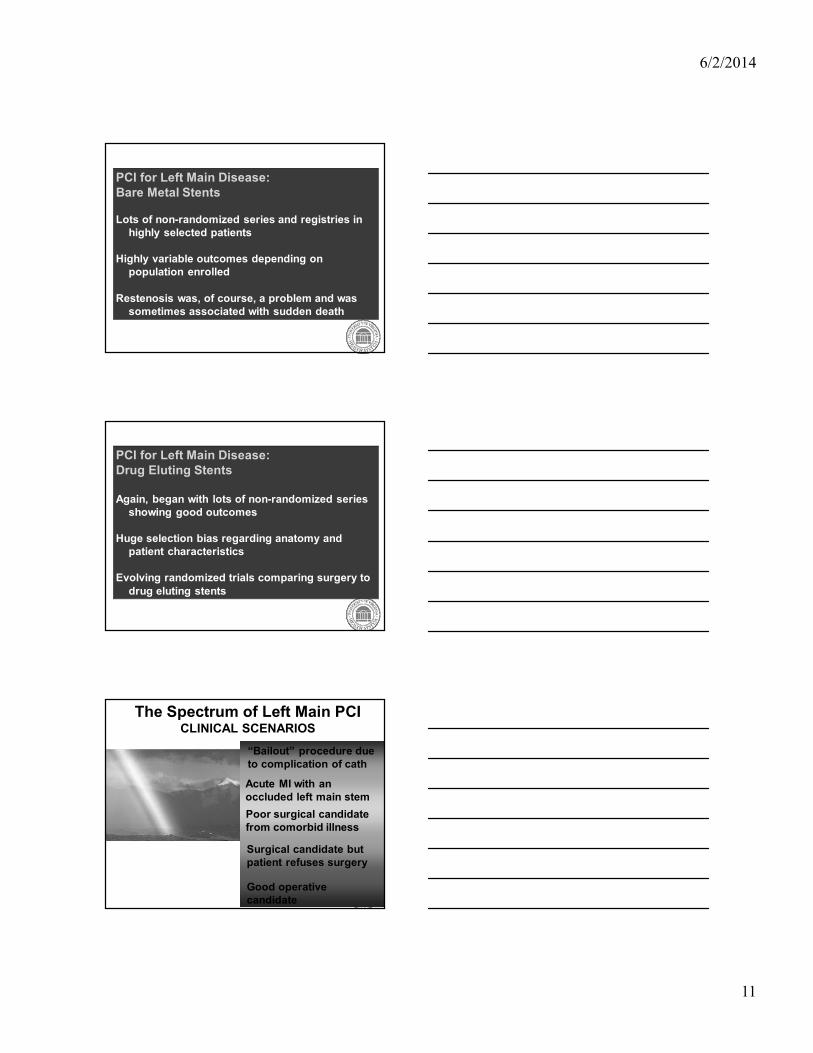
Left Main PCI
Few randomized controlled trials in the modern era comparing PCI to CABG
Major trials:
SYNTAX
LEMANS
PRECOMBAT
Boudriot et al
EXCEL trial (completed enrollment)
Meta Analysis of Existing Trials Comparing PCI
to CABG (n=1611)
PCI CABG p value
1 year MACCE 14.5% 11.8% 0.11
Death 3.0% 4.1% 0.29
MI 2.8% 2.9% 0.95
CVA 0.1% 1.7% 0.013
TVR 11.4% 5.4% <0.001
Capodanno et al J Am Coll Cardiol 2011;58:1426-32
No difference in death or MI
Less stroke with PCI
Less repeat revascularization with CABG
Meta Analysis of Existing Trials Comparing PCI
to CABG (n=1611)
Capodanno et al JAm Coll Cardiol 2011;58:1426-32
1 Year
MACCE

6/2/2014
17
Complexity and extent of
disease AND the ability to
achieve complete
revascularization is an
important determinant of
outcome with PCI versus
CABG
Capodanno, D. et al. J Am Coll Cardiol Intv 2009;2:731-738
Score < 34Score > 34
Importance of the SYNTAX Score in Determining
Outcome for PCI versus CABG
Capodanno, D. et al. J Am Coll Cardiol Intv 2009;2:731-738
Relationship Between SYNTAX Score and Ability
to Achieve Complete Revascularization with PCI
versus CABG

6/2/2014
18
The SYNTAX Trial
• Largest trial of PCI vs CABG in
complex, multi-vessel disease
including left main disease.
• Left main subset consisted of 705
patients
PPPP=0.12=0.12=0.12=0.12
31.031.031.031.0%%%%
0000
Cumulative Event Rate (%)
Cumulative Event Rate (%)
Cumulative Event Rate (%)
Cumulative Event Rate (%)
25252525
50505050
Months Since AllocationMonths Since AllocationMonths Since AllocationMonths Since Allocation
<1 year
13.7% vs 15.8%
P=0.44
1-2 years
7.5% vs 10.3%
P=0.22
2-3 years
5.2% vs 5.7%
P=0.78
3-4 years
6.4% vs 8.3%
P=0.35
36.936.936.936.9%%%%
TAXUSTAXUSTAXUSTAXUS (N=357)(N=357)(N=357)(N=357)CABGCABGCABGCABG (N=348)(N=348)(N=348)(N=348)
MACCE to 5 YearsLeft Main Subset
4-5 years
5.9% vs 5.5%
P=0.82
0000 12121212 6060606024242424 36363636 48484848
Serruys PW et al. Lancet 2013;381:629Serruys PW et al. Lancet 2013;381:629Serruys PW et al. Lancet 2013;381:629Serruys PW et al. Lancet 2013;381:629––––38383838
PPPP=0.12=0.12=0.12=0.12 PPPP=0.53=0.53=0.53=0.53 PPPP=0.03=0.03=0.03=0.03 PPPP=0.10=0.10=0.10=0.10 PPPP<0.001<0.001<0.001<0.001
MACCE to 5 YearsLeft Main Subset
Event rate (%)
Event rate (%)
Event rate (%)
Event rate (%)
TAXUS (n=357)TAXUS (n=357)TAXUS (n=357)TAXUS (n=357)CABG (n=348)CABG (n=348)CABG (n=348)CABG (n=348)
Serruys PW et al. Lancet 2013;381:629Serruys PW et al. Lancet 2013;381:629Serruys PW et al. Lancet 2013;381:629Serruys PW et al. Lancet 2013;381:629––––38383838

6/2/2014
19
TAXUSTAXUSTAXUSTAXUS (N=135)(N=135)(N=135)(N=135)
CABGCABGCABGCABG (N=149)(N=149)(N=149)(N=149)CABG PCI
p
value
Death 14.1% 20.9% 0.11
CVA 4.9% 1.6% 0.13
MI 6.1% 11.7% 0.13
Death,
CVA or
MI22.1% 26.1% 0.40
Revasc 11.6% 34.1% <0.001
LM DiseaseLM DiseaseLM DiseaseLM Disease
MonthsMonthsMonthsMonths
MACCE (%)
MACCE (%)
MACCE (%)
MACCE (%)
0000 12121212 24242424
50505050
0000
25252525
4848484836363636 60606060
MACCE to 5 Years by SYNTAX Score Tercile LM Subset High Scores ≥33
46.546.546.546.5%%%%
29.7%29.7%29.7%29.7%
PPPP=0.003=0.003=0.003=0.003
Serruys PW et al. Lancet 2013;381:629–38
CABG PCIp
value
Death 15.1% 7.9% 0.02
CVA 3.9% 1.4% 0.11
MI 3.8% 6.1% 0.33
Death,
CVA or
MI19.8% 14.8% 0.16
Revasc 18.6% 22.6% 0.36
LM DiseaseLM DiseaseLM DiseaseLM Disease
TAXUSTAXUSTAXUSTAXUS (N=221)(N=221)(N=221)(N=221)
CABGCABGCABGCABG (N=196)(N=196)(N=196)(N=196)
31.331.331.331.3%%%%
32.1%32.1%32.1%32.1%
Months Since AllocationMonths Since AllocationMonths Since AllocationMonths Since Allocation
Cumulative Event Rate (%)
Cumulative Event Rate (%)
Cumulative Event Rate (%)
Cumulative Event Rate (%)
0000 12121212 24242424
50505050
0000
25252525
4848484836363636 60606060
PPPP=0.74=0.74=0.74=0.74
Serruys PW et al. Lancet 2013;381:629Serruys PW et al. Lancet 2013;381:629Serruys PW et al. Lancet 2013;381:629Serruys PW et al. Lancet 2013;381:629––––38383838
MACCE to 5 Years by SYNTAX Score Tercile LM Subset Low to Intermediate Scores (0-32)
What have we learned?• Complexity and extent of disease is an
important determinant of outcome in PCI vs
CABG debate.
• High SYNTAX score (>33) does better with
CABG
• Data suggests less risk of stroke and lower
mortality with PCI for low-intermediate
SYNTAX score (<33).
• Studies not designed or powered to definitely
answer this question
• Thus, there is clinical equipoise regarding
choice of revascularization for SYNTAX score
<33.
6/2/2014
20
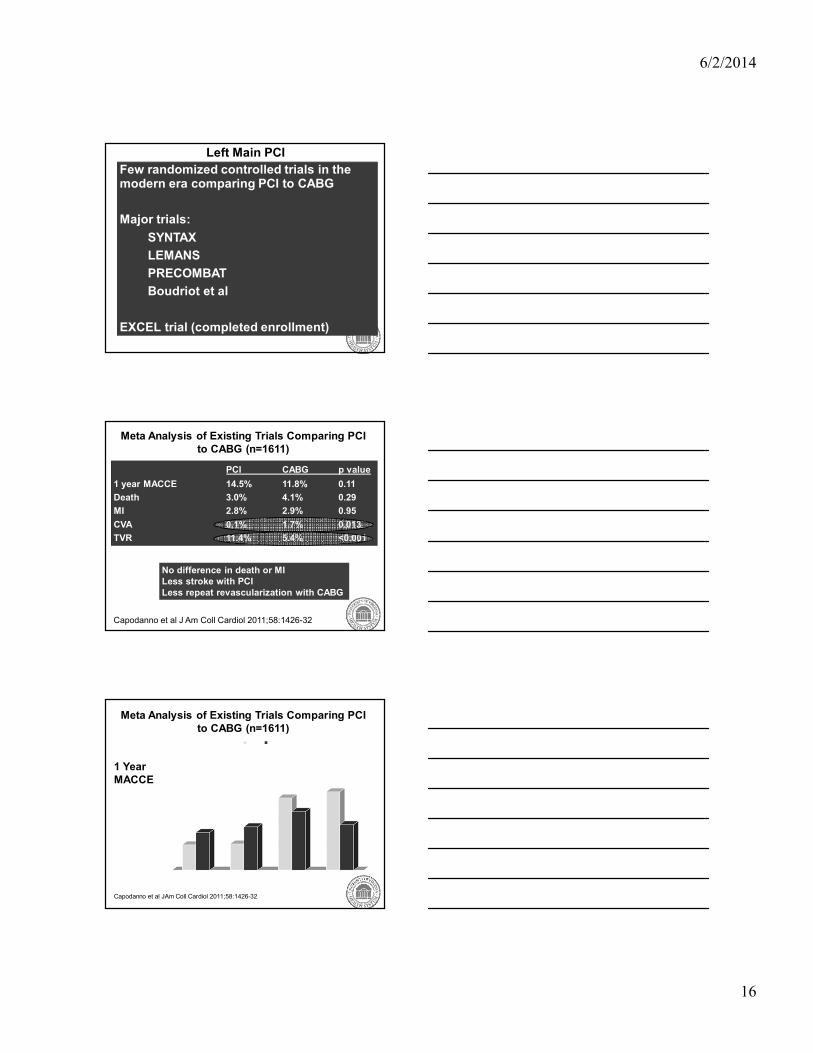
EXCEL Trial
R
Clinical follow-up:1 mo, 6 mo and yearly through 5 years
EXCEL: Study Design
3600 pts with unprotected left main disease
SYNTAX score ≤32
Consensus agreement by heart team
Yes
(N=2600)
No
(N=1000)
Enrollment
registry
PCI (Xience Prime)
(N=1300)
CABG
(N=1300)
@ 165 international sites
EXCEL: Inclusion Criteria
• Clinical and anatomic eligibility for both PCI and CABG by heart team consensus
• Silent ischemia, stable angina, unstable angina or recent MI
• Significant LM disease by heart team consensus
- Angiographic DS ≥70%, or
- Angiographic DS ≥50% to <70% with
- a markedly positive noninvasive study, and/or
- IVUS MLA <6.0 mm2, and/or
- FFR <0.80

6/2/2014
21
EXCEL: Principal Exclusion Criteria
• Prior PCI within 1 year, or prior LM PCI anytime
• Prior CABG anytime
• Need for any cardiac surgery other than CABG
• Additional surgery required within 1 year
• Unable to tolerate, obtain or comply with dual antiplatelet therapy for 1 year
• Non cardiac co-morbidities with life expectancy <3 years
• Left main RVD <2.25 mm or >4.5 mm
EXCEL: Principal Exclusion Criteria
• The presence of any condition(s) which leads the surgeon to believe that clinical equipoise is not present (i.e. the subject should not be treated by CABG, but rather should be managed with PCI or medical therapy
• The presence of any condition(s) which leads the Interventionalist to believe that clinical equipoise is not present (i.e. the subject should not be treated by PCI, but rather should be managed with CABG or medical therapy
EXCEL: Principal Endpoints• Primary endpoint: Death, MI, or stroke at 3 years
Powered for sequential noninferiority and
superiority testing
• Major secondary endpoints (powered):
1. Death, MI, or stroke at 30 days
2. Stroke at 30 days
3. Unplanned repeat revascularization for
ischemia at 3 years
• Additional secondary endpoint (powered):
1. Death, MI, stroke or unplanned
revascularization for ischemia at 3 years
• Quality of life and cost-effectiveness assessments:
At baseline, 1 month, 1 year, 3 years and 5 years
6/2/2014
22
EXCEL Case Review
Left Main PCI
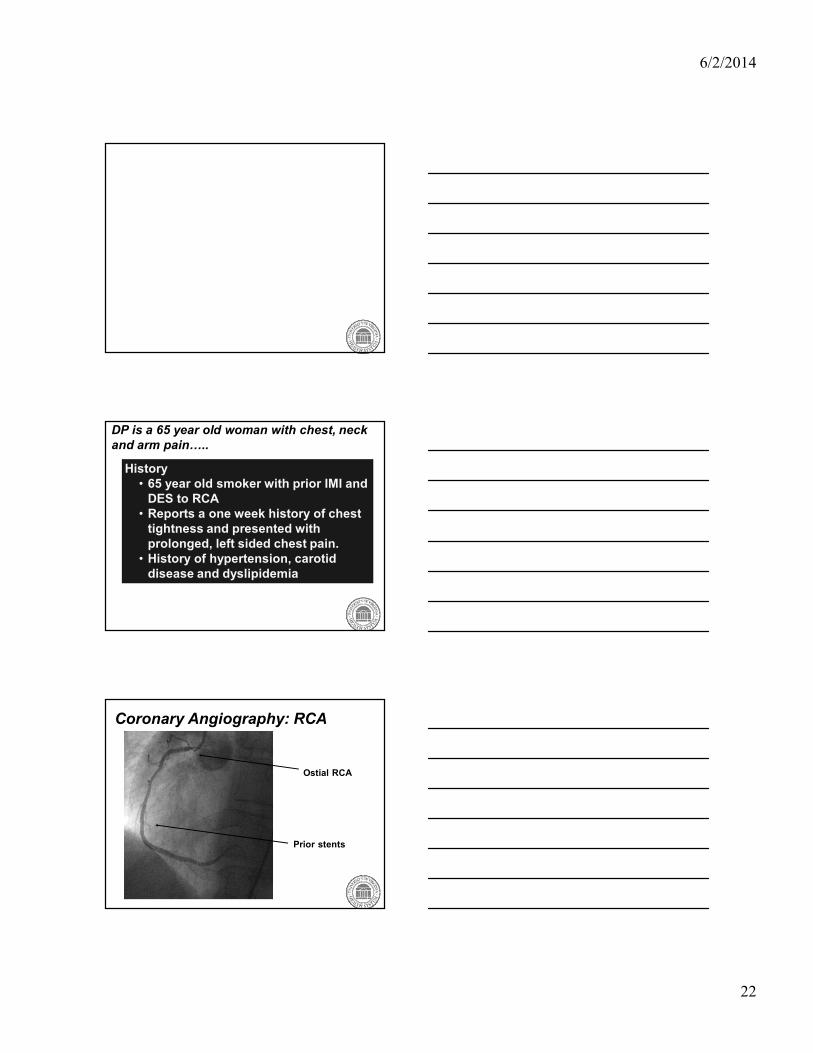
DP is a 65 year old woman with chest, neck
and arm pain…..
History
• 65 year old smoker with prior IMI and
DES to RCA
• Reports a one week history of chest
tightness and presented with
prolonged, left sided chest pain.
• History of hypertension, carotid
disease and dyslipidemia
Coronary Angiography: RCA
Ostial RCA
Prior stents

6/2/2014
23
Coronary Angiography: LCAOstial
LM
Coronary Angiography: LCA
Ostial LAD lesion
OM lesion
IVUS
Ostial LAD MLA = 3.6 mm2
Ostial LM MLA = 3.7 mm2

6/2/2014
24
SYNTAX
SCORE =28
Enrolled in
EXCEL
Randomized
to PCI
Ramus/OM Stenting
LAD Stenting
6/2/2014
25
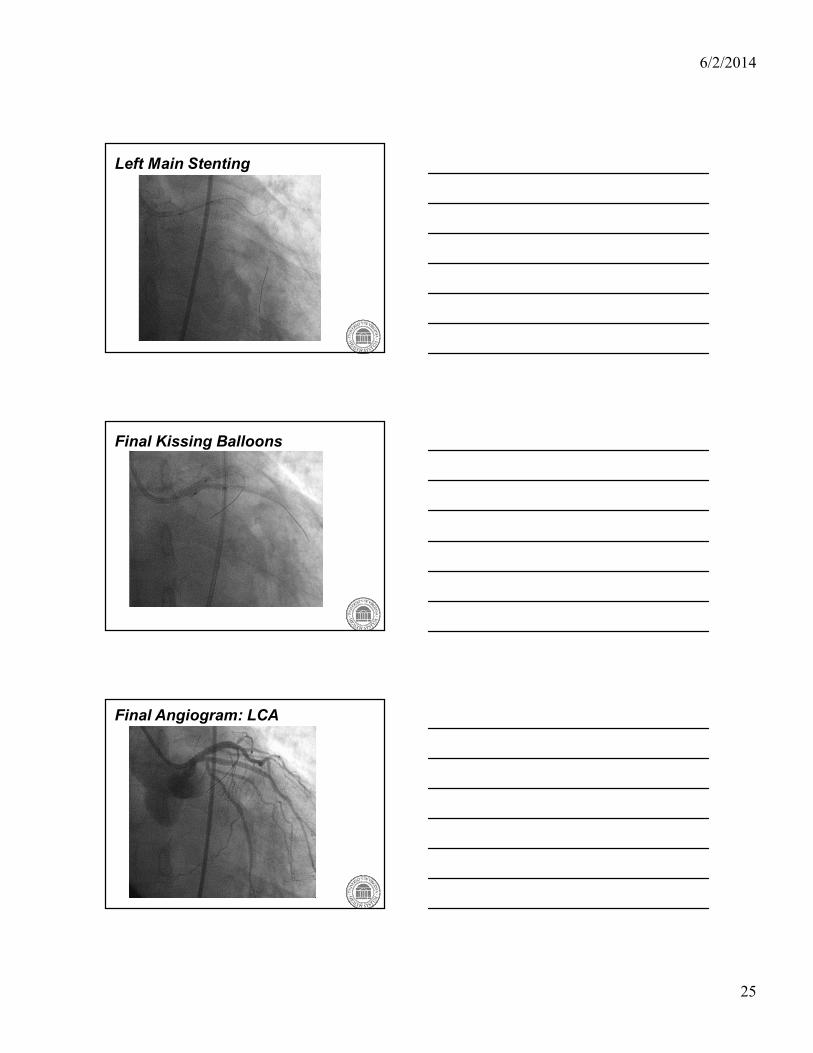
Left Main Stenting
Final Kissing Balloons
Final Angiogram: LCA

6/2/2014
26
Final Angiogram: RCA
Issues in Unprotected Left Main Stenting
Technical aspects
Management of bifurcation
Staging if multi-vessel disease
Need for Hemodynamic Support
Choice of Stents (does not seem to matter)
Adjunctive Pharmacology
Role of IVUS
Follow-up
Bifurcation Strategies
• The bifurcation is involved in over 50% of LM
cases.
• PCI of bifurcation associated with high risk of
MACE as compared to ostial/mid shaft lesions (JACC Intv 2013:6:1242-9)
• Optimal strategy is not yet known. Most favor
a “provisional stent” strategy (JACC Intv 2014;7:255-63).
• If 2 stent strategy used, “Double-kissing-
crush” technique has lower rate of TVR and
ST than “Culotte” technique (JACC 2013;61:1482-8)
• Need proper RCT to answer this important
question.

6/2/2014
27
Double Kissing Crush Technique

6/2/2014
28
From Fajadet J and Chieffo A. Eur H J 2012;33:36-50
Need for Support
Devices available for support of high risk PCI
IABP
IMPELLA
TANDEM
Not needed for most Left Main PCI cases. Need
based on:
LV function
Hemodynamic status (LVEDP, CO etc)
Status of the RCA
Anticipated ischemic time with PCI
Complexity of intervention
Unsupported, left main PCI
Balloon
Inflated
Here
Consider
New Career
Here

6/2/2014
29
Baseline
With TANDEM Heart
Unprotected,
complex left main
PCI with occluded
RCA and EF 20%
Adjunctive Pharmacology
Stent thrombosis would likely be a
fatal event in the left main setting.
How long to treat with dual anti-
platelet therapy? (ISAR-LEFT MAIN
data is reassuring regarding late stent
thrombosis)
Should we be assessing platelet
inhibition?
Role of IVUS Imaging
Optimizes sizing
Determines involvement of the side branches
Assesses ostial coverage and identifies stent
apposition/expansion.
Should be done in all cases.
3 year freedom
from
IVUS No IVUS p value
MACE (overall) 88.7% 83.6% 0.04
MACE (distal LM) 90% 80.7% 0.03
Stent thrombosis 0.6% 2.2% 0.04
JACC Intv 2014;7:244-54

6/2/2014
30
Surveillance Post-PCI of Left Main
Disease
Optimal surveillance during follow-up is unclear.
Symptoms? Stress test? Angiography?
Concern about asymptomatic restenosis and
risk of sudden death led many to advocate
routine angiography at 2-6 months.
However, this strategy has not been shown to
predict outcome so now classified as Class III
indication in the guidelines.
SUMMARY: Left Main PCI
Patients with left main disease often have complex,
coexisting coronary disease.
Patient selection is important. Value of heart team
approach, assessment based on STS and SYNTAX
scores.
Currently, PCI is of uncertain appropriateness in
operative candidates with low-moderate SYNTAX score
and is INAPPROPRIATE in operative candidates with
high SYNTAX score. EXCEL trial designed to shed more
light on low-moderate SYNTAX score patients.
PCI of left main requires skill with management of ostial
lesions, bifurcation techniques, support devices and
IVUS.



















![Bifurcation and Left Main Stenting[1]](https://img.pdfslide.us/doc/110x75/5466ba34b4af9ffd748b4bcf/bifurcation-and-left-main-stenting1.jpg)