Embed Size (px)
Citation preview
PCI for Left Main PCI for Left Main PCI for Left Main PCI for Left Main DiseaseDisease
Jean FajadetJean FajadetCli i P t T l FCli i P t T l FClinique Pasteur, Toulouse, FranceClinique Pasteur, Toulouse, France
Valencia , September 29 , 2007Valencia , September 29 , 2007
Treatment of LM diseaseTreatment of LM disease
I.I. What have we learned?What have we learned?––BMSBMS–– DESDES–– DESDES
II.II. What are we doing in daily practice?What are we doing in daily practice?
III.III. How to select patients for PCI or CABG? How to select patients for PCI or CABG?
LM stenting with BMSLM stenting with BMS
InIn--Hospital Mortality RateHospital Mortality Rate
LM stenting with BMSLM stenting with BMS
InIn Hospital Mortality RateHospital Mortality Rate(excluding procedures during acute MI)(excluding procedures during acute MI)
0 t 4 3%0 t 4 3%0 to 4.3%0 to 4.3%
Hi h Hi h i k 6i k 6 13% 13% 9%9%« High« High--risk » group: 6risk » group: 6--13% 13% ≈≈ 9%9%« Low« Low--risk » group: risk » group: 00--2% 2% ≈≈ 1%1%
LM stenting with BMSLM stenting with BMS
Mid & lMid & l t t litt t litMid & longMid & long--term mortalityterm mortality
FollowFollow--up ranging from 7.3 to 25.5 monthsup ranging from 7.3 to 25.5 months
2% to 2% to 28 %28 %2% to 2% to 28 %28 %
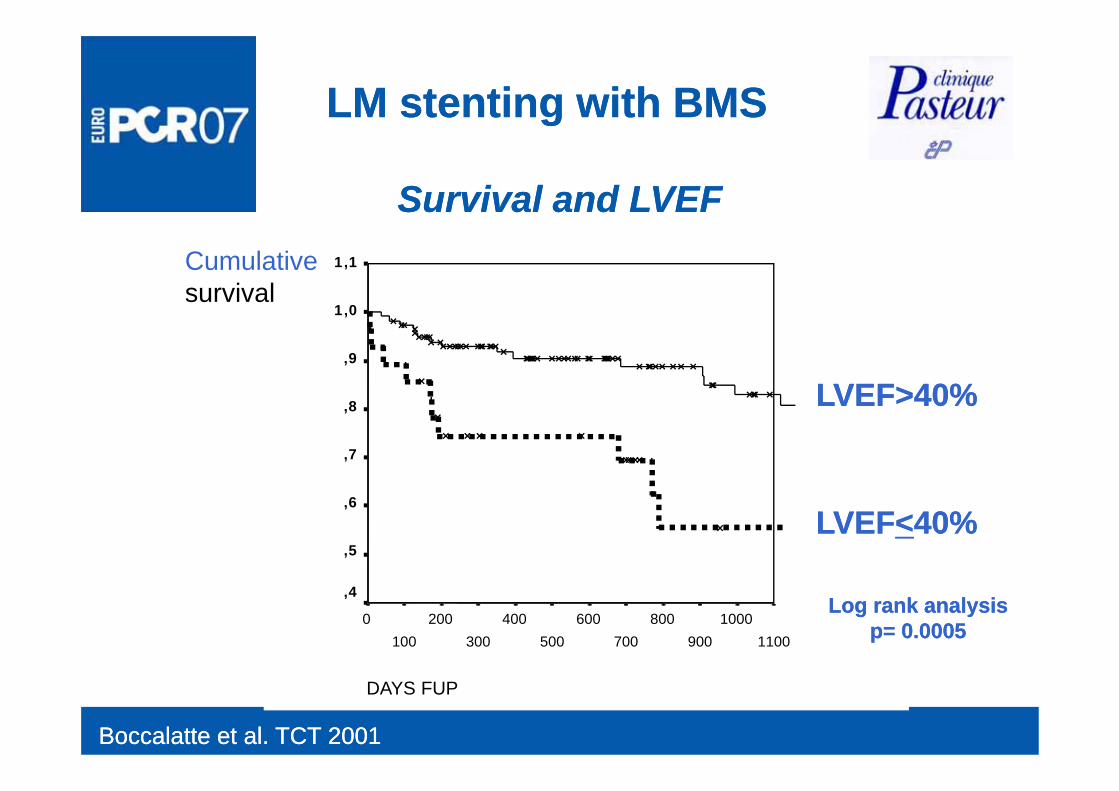
LM stenting with BMSLM stenting with BMS
Survival and LVEF Survival and LVEF Cumulativesurvival
1,1
1 01,0
,9
LVEF>40%LVEF>40%,8
,7
LVEF>40%LVEF>40%
,6
,5LVEFLVEF<<40%40%
11001000
900800
700600
500400
300200
1000
,4Log rank analysis Log rank analysis
p= 0.0005p= 0.0005
Boccalatte et al. TCT 2001Boccalatte et al. TCT 2001
DAYS FUP
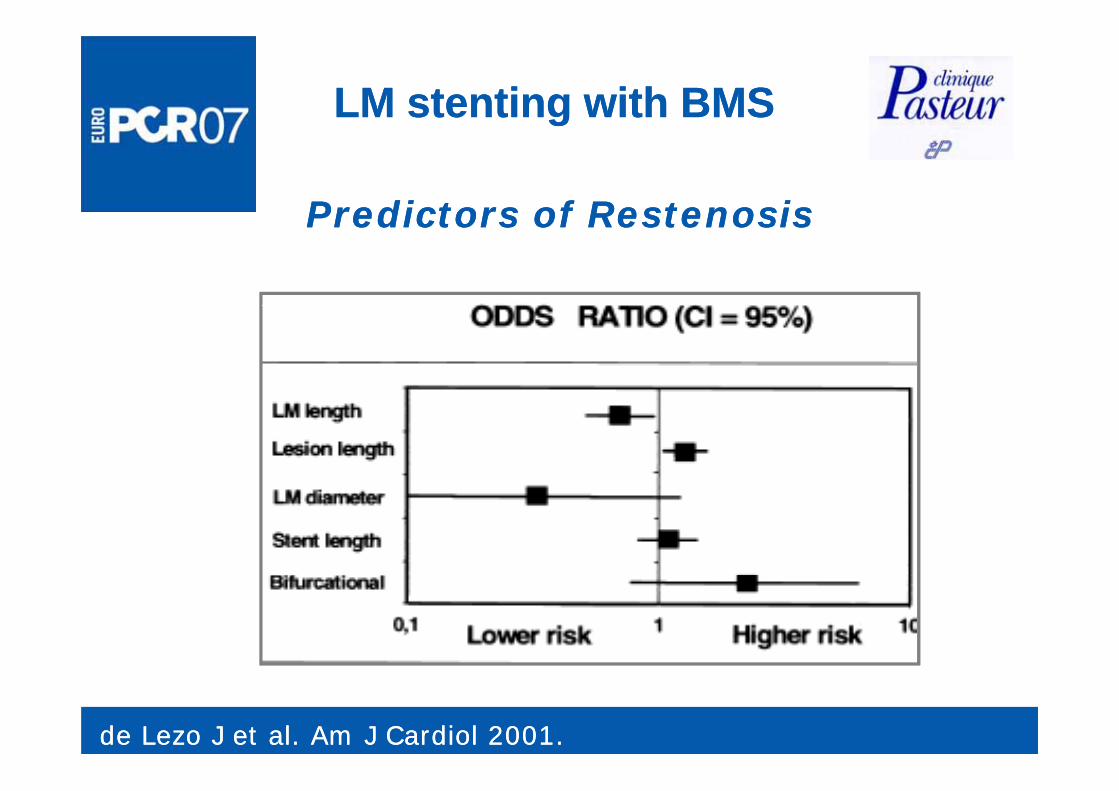
LM stenting with BMSLM stenting with BMS
Predictors of RestenosisPredictors of RestenosisPredictors of RestenosisPredictors of Restenosis
de Lezo J et al. Am J Cardiol 2001.de Lezo J et al. Am J Cardiol 2001.
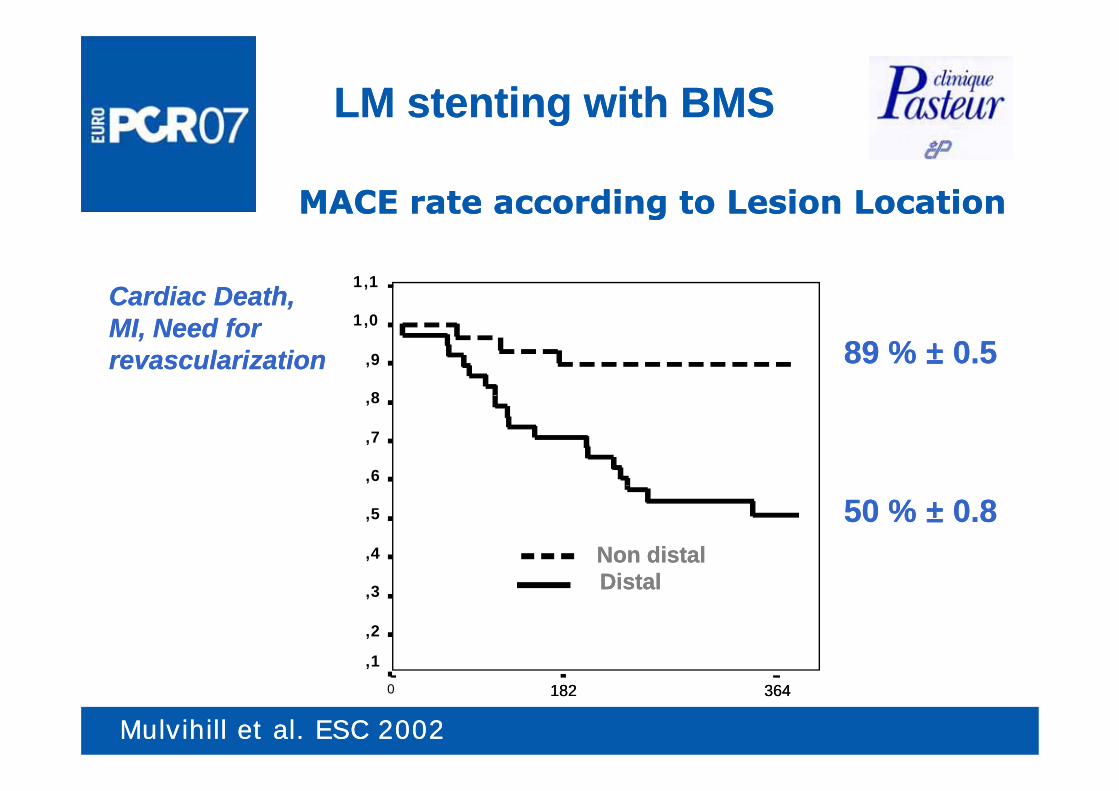
LM stenting with BMSLM stenting with BMS
MACE rate according to Lesion LocationMACE rate according to Lesion Location
1,1
gg
Cardiac Death, Cardiac Death, 1,0
,9
8
89 % 89 % ±± 0.50.5
,,MI, Need for MI, Need for revascularizationrevascularization
,8
,7
,6
Log rank=0.001,5
,4
50 % 50 % ±± 0.80.8NDNon distalNon distalDi t lDi t l,3
,2
,1
DDistalDistal
Mulvihill et al. ESC 2002Mulvihill et al. ESC 2002
3643640
,1
182182
Treatment of LM diseaseTreatment of LM disease
I.I. What have we learned?What have we learned?–– BMSBMS––DESDESDESDES
II.II. What are we doing in daily practice?What are we doing in daily practice?
III.III. How to select patients for PCI or CABG? How to select patients for PCI or CABG?
Unprotected LMCA Unprotected LMCA StentingStenting
Experience with DESExperience with DESArampatzis et al. Am J Cardiol 2003;92:327–329
De Lezo et al Am Heart J 2004;148:481–5
pp
De Lezo et al. Am Heart J 2004;148:481 5.
Chieffo et al. Circulation. 2005;111:791-795.
Park et al J Am Coll Cardiol 2005;45:351– 6Park et al. J Am Coll Cardiol 2005;45:351 6
Agostoni et al. Am J Cardiol 2005;95:644–647
Price et al J Am Coll Cardiol 2006;47:871–7Price et al. J Am Coll Cardiol 2006;47:871 7
Valgimigli et al. EuroInterv. 2007;2:435-443
Fajadet et al Cypher european registry ACC 2007Fajadet et al. Cypher european registry, ACC 2007
Erglis et al. J Am Coll Cardiol 2007;50:491-7
Carrié et al Friend registry ESC 2007Carrié et al. Friend registry, ESC 2007
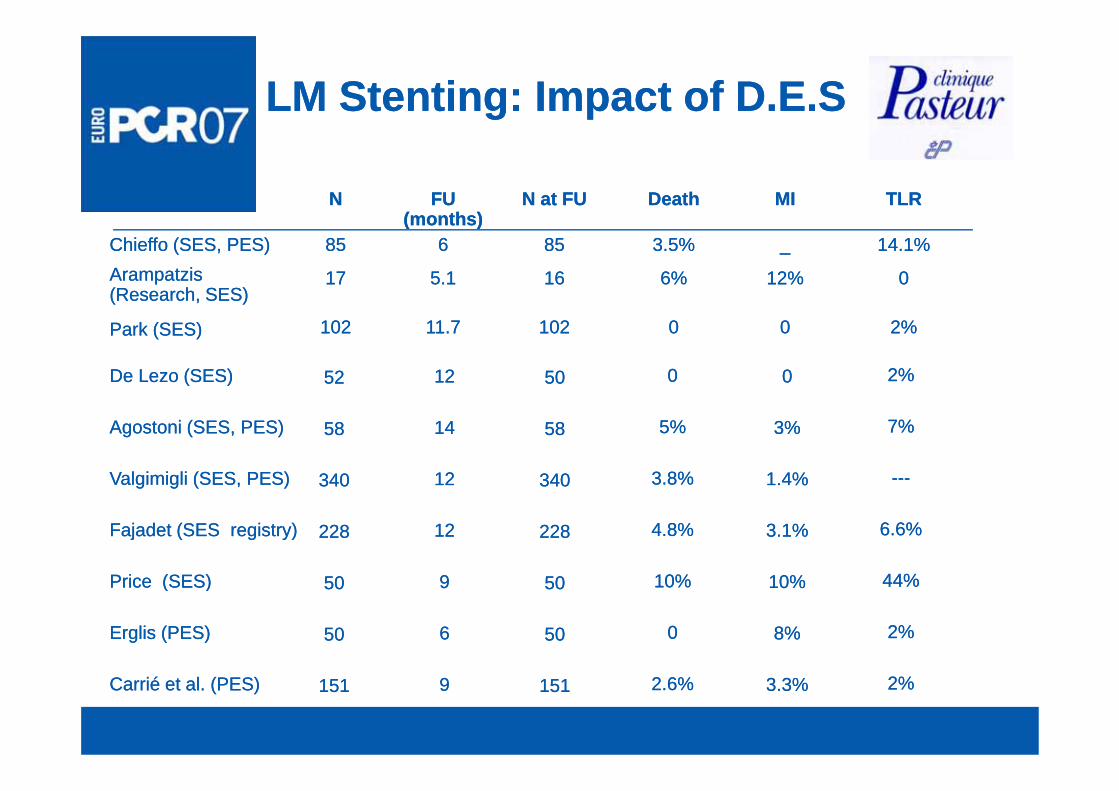
LM Stenting: Impact of D.E.SLM Stenting: Impact of D.E.S
N at FUN at FU TLRTLRMIMIDeathDeathFU FU (months)(months)
NN(months)(months)
1616
8585
0012%12%6%6%5.15.11717Arampatzis Arampatzis (Research, SES)(Research, SES)
14.1%14.1%__3.5%3.5%668585Chieffo (SES, PES)Chieffo (SES, PES)
2%2%000010210211.711.7102102Park (SES)Park (SES)
5050 2%2%000012125252De Lezo (SES)De Lezo (SES)
5858
340340
7%7%
------
3%3%
1.4%1.4%
5%5%
3.8%3.8%
1414
1212
5858
340340
Agostoni (SES, PES)Agostoni (SES, PES)
Valgimigli (SES, PES)Valgimigli (SES, PES) 340340
228228 6.6% 6.6%
44%44%
%%
3.1%3.1%
10%10%
4.8% 4.8%
10%10%
1212
99
340340
228228
g g ( , )g g ( , )
Fajadet (SES registry)Fajadet (SES registry)
P i (SES)P i (SES) 5050
5050
44%44%
2%2%
10%10%
8%8%
10%10%
00
99
66
5050
5050
Price (SES)Price (SES)
Erglis (PES)Erglis (PES)
151151 2%2%3.3%3.3%2.6%2.6%99151151Carrié et al. (PES)Carrié et al. (PES)
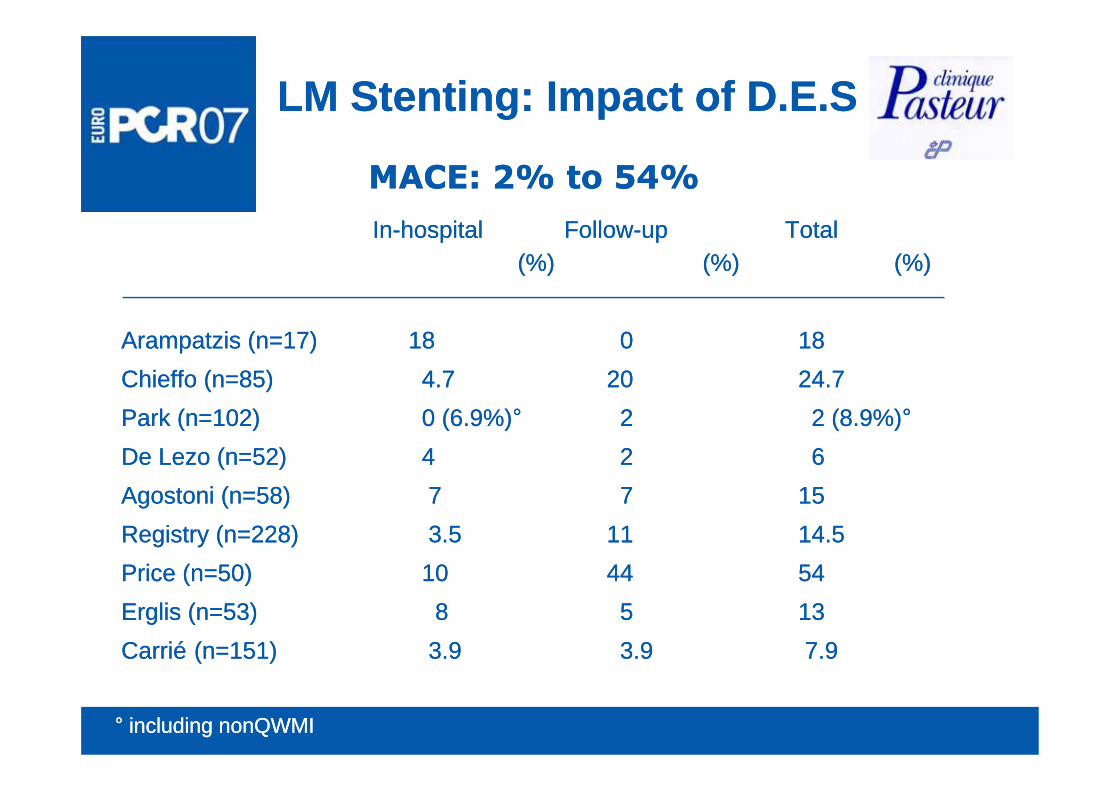
LM Stenting: Impact of D.E.SLM Stenting: Impact of D.E.S
MACE: 2% to 54%MACE: 2% to 54%
InIn--hospitalhospital FollowFollow--upup Total Total (%) (%) (%) (%) (%)(%)
Arampatzis (n=17)Arampatzis (n=17) 1818 00 1818Chieffo (n=85)Chieffo (n=85) 4.74.7 2020 24.724.7Park (n=102)Park (n=102) 0 (6.9%)0 (6.9%)°° 22 2 (8.9%)2 (8.9%)°°De Lezo (n=52) De Lezo (n=52) 44 22 66Agostoni (n=58)Agostoni (n=58) 77 77 1515Registry (n=228)Registry (n=228) 3.53.5 1111 14.514.5Price (n=50)Price (n=50) 1010 4444 5454Price (n=50)Price (n=50) 1010 4444 5454Erglis (n=53)Erglis (n=53) 88 55 1313CarriCarriéé (n=151)(n=151) 3.93.9 3.93.9 7.97.9
°° including nonQWMIincluding nonQWMI
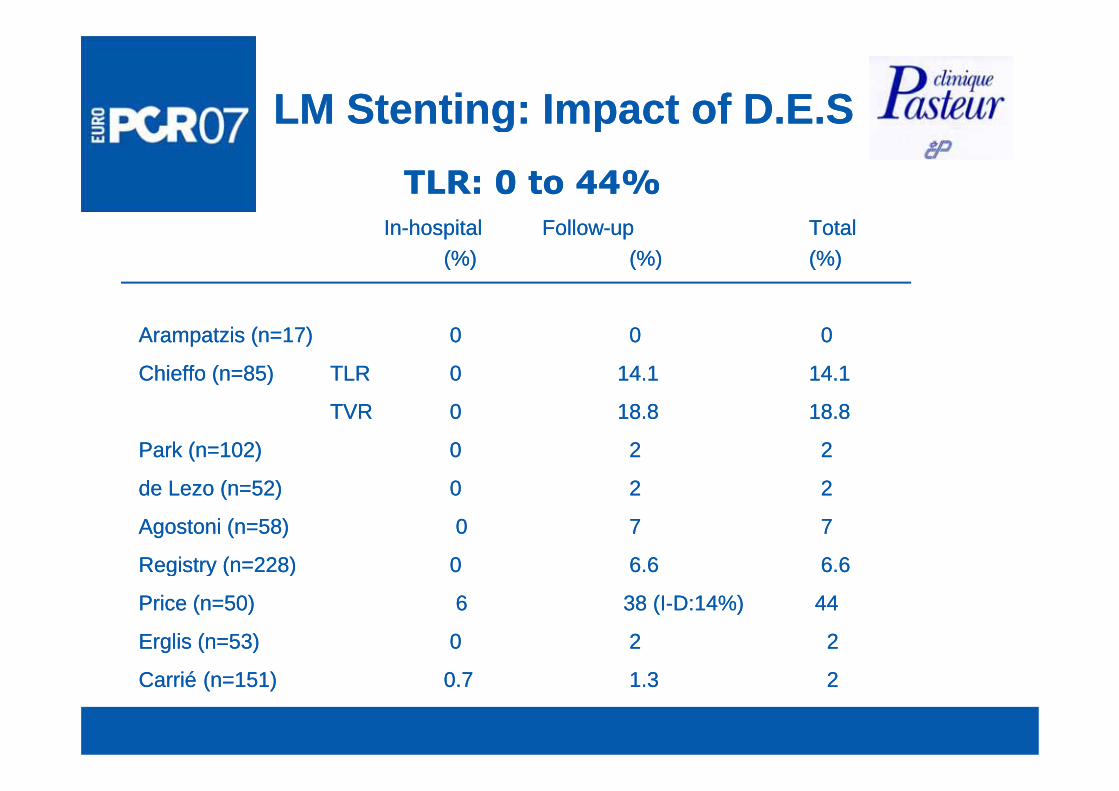
LM Stenting: Impact of D.E.SLM Stenting: Impact of D.E.Sg pg pTLR: 0 to 44%TLR: 0 to 44%
InIn--hospital Followhospital Follow--up up Total Total (%) (%) (%) (%) (%)(%)
Arampatzis (n=17)Arampatzis (n=17) 00 00 00
Chieffo (n=85) Chieffo (n=85) TLRTLR 00 14.114.1 14.114.1
TVRTVR 00 18.818.8 18.818.8
Park (n=102)Park (n=102) 0 0 22 22
de Lezo (n=52)de Lezo (n=52) 00 22 22de Lezo (n=52)de Lezo (n=52) 00 22 22
Agostoni (n=58)Agostoni (n=58) 00 77 77
Registry (n=228)Registry (n=228) 00 6.66.6 6.66.6g y ( )g y ( )
Price (n=50)Price (n=50) 66 38 (I38 (I--D:14%)D:14%) 4444
Erglis (n=53)Erglis (n=53) 00 22 22
CarriCarriéé (n=151)(n=151) 0.70.7 1.31.3 22
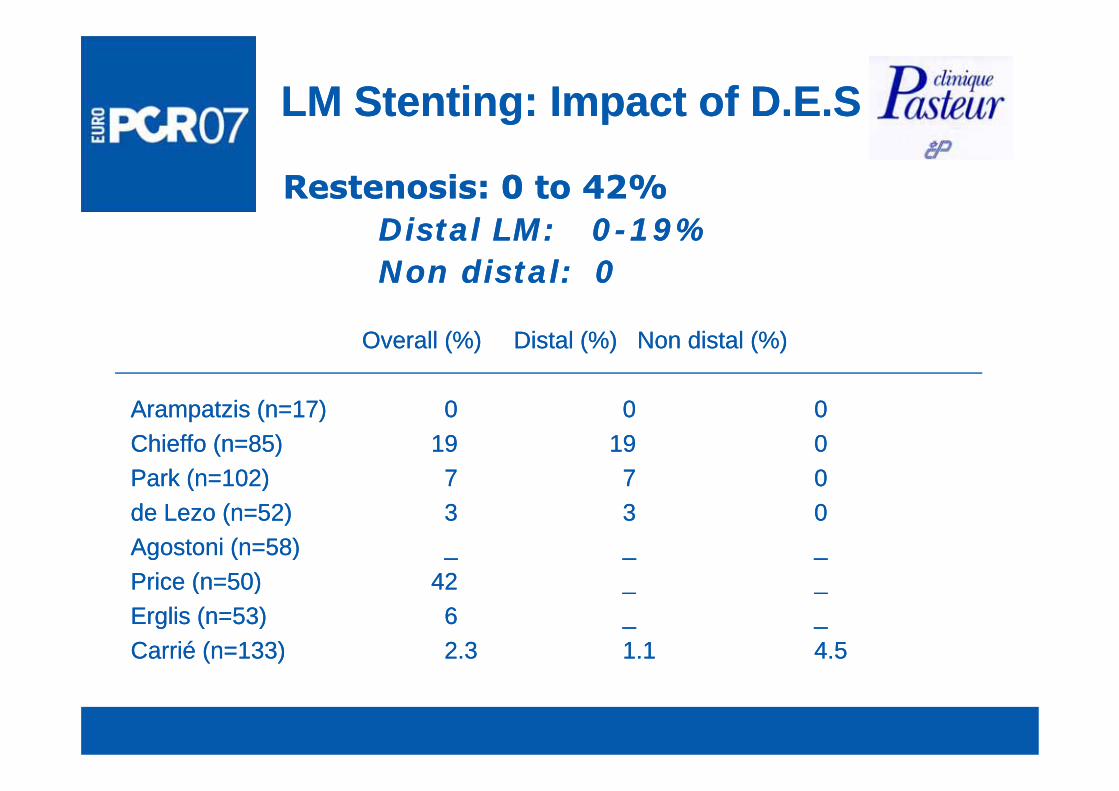
LM Stenting: Impact of D.E.SLM Stenting: Impact of D.E.S
Restenosis: 0 to 42%Restenosis: 0 to 42%Distal LM:Distal LM: 00--19%19%Non distal: 0Non distal: 0
Overall (%)Overall (%) Distal (%) Non distal (%)Distal (%) Non distal (%)
Arampatzis (n=17)Arampatzis (n=17) 00 00 00Chieffo (n=85) Chieffo (n=85) 1919 1919 00Park (n=102)Park (n=102) 77 77 00Park (n 102)Park (n 102) 7 7 77 00de Lezo (n=52)de Lezo (n=52) 33 33 00Agostoni (n=58)Agostoni (n=58) __ __ __P i ( 50)P i ( 50) 4242Price (n=50)Price (n=50) 4242 __ __Erglis (n=53)Erglis (n=53) 66 __ __Carrié (n=133)Carrié (n=133) 2.32.3 1.11.1 4.54.5
DES for unprotected LM stenosis DES for unprotected LM stenosis Clinique Pasteur experience Clinique Pasteur experience
September 2002 September 2002 –– August 2006August 2006N 147 ti ti tN 147 ti ti tN=147 consecutive patientsN=147 consecutive patients
Clinical followClinical follow--up: up: 27 327 3 ±±13 2 months13 2 months27.3 27.3 ±±13.2 months 13.2 months
in all patients in all patients
During this period, 168 patients with LM stenosis During this period, 168 patients with LM stenosis underwent CABGunderwent CABG
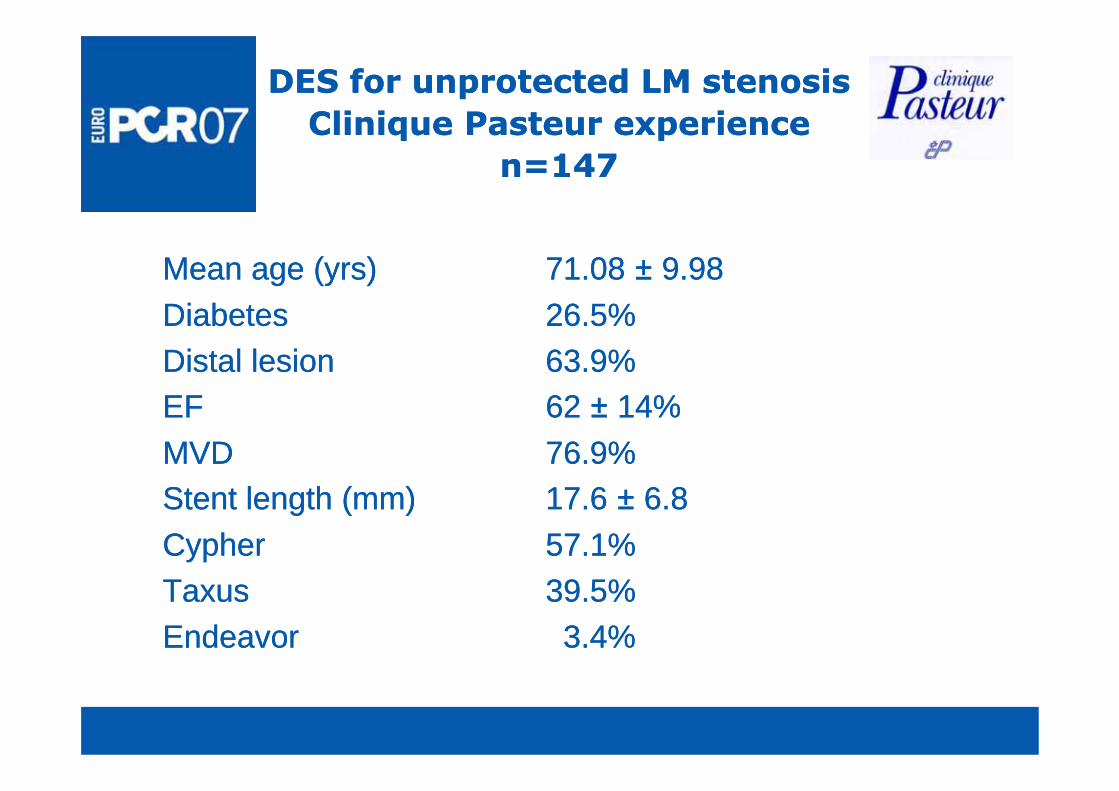
DES for unprotected LM stenosis DES for unprotected LM stenosis Clinique Pasteur experienceClinique Pasteur experienceClinique Pasteur experienceClinique Pasteur experience
n=147 n=147
Mean age (yrs)Mean age (yrs) 71.08 71.08 ±± 9.989.98Di b tDi b t 26 5%26 5%DiabetesDiabetes 26.5%26.5%Distal lesionDistal lesion 63.9%63.9%EFEF 6262 14%14%EFEF 62 62 ±± 14%14%MVDMVD 76.9%76.9%Stent length (mm)Stent length (mm) 17.6 17.6 ±± 6.8 6.8 CypherCypher 57.1%57.1%TaxusTaxus 39.5%39.5%EndeavorEndeavor 3.4%3.4%
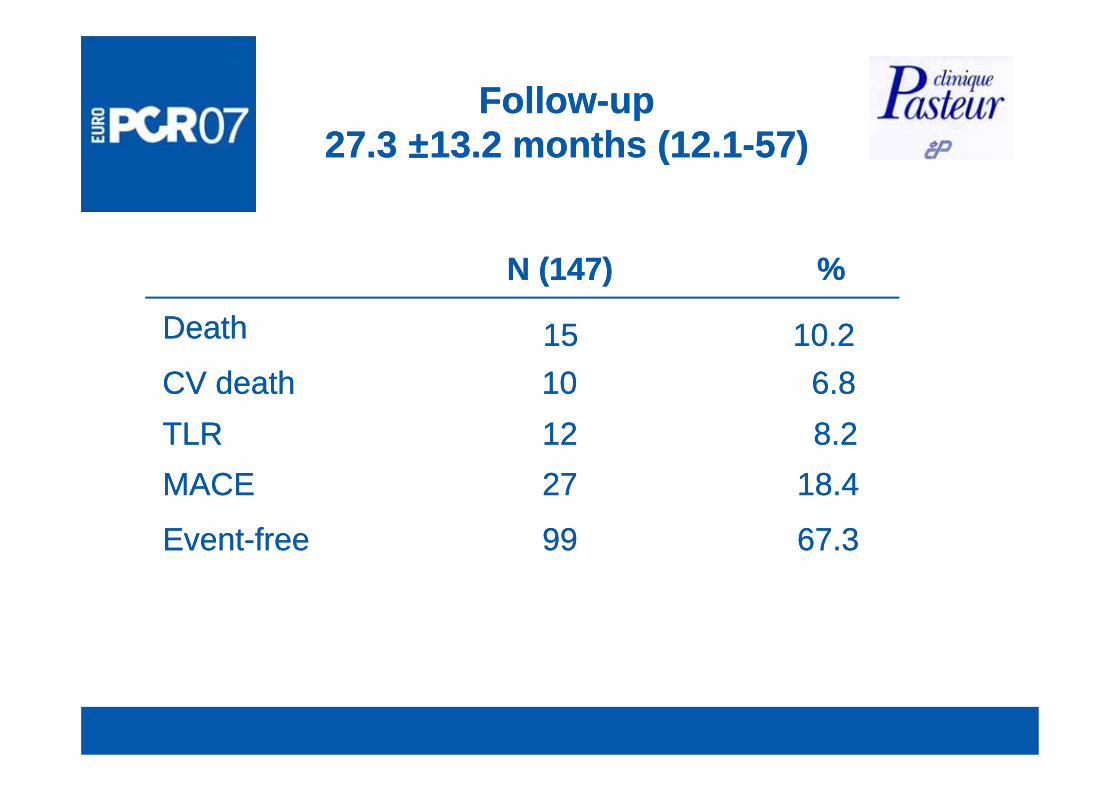
FollowFollow--up up 27.3 27.3 ±±13.2 months (12.113.2 months (12.1--57)57)
%%N (147)N (147)
DeathDeath 1515 10.210.2CV deathCV death 1010 6.86.8
18 418 42727MACEMACE8.28.21212TLRTLR
67.367.39999EventEvent--freefree
18.418.42727MACEMACE
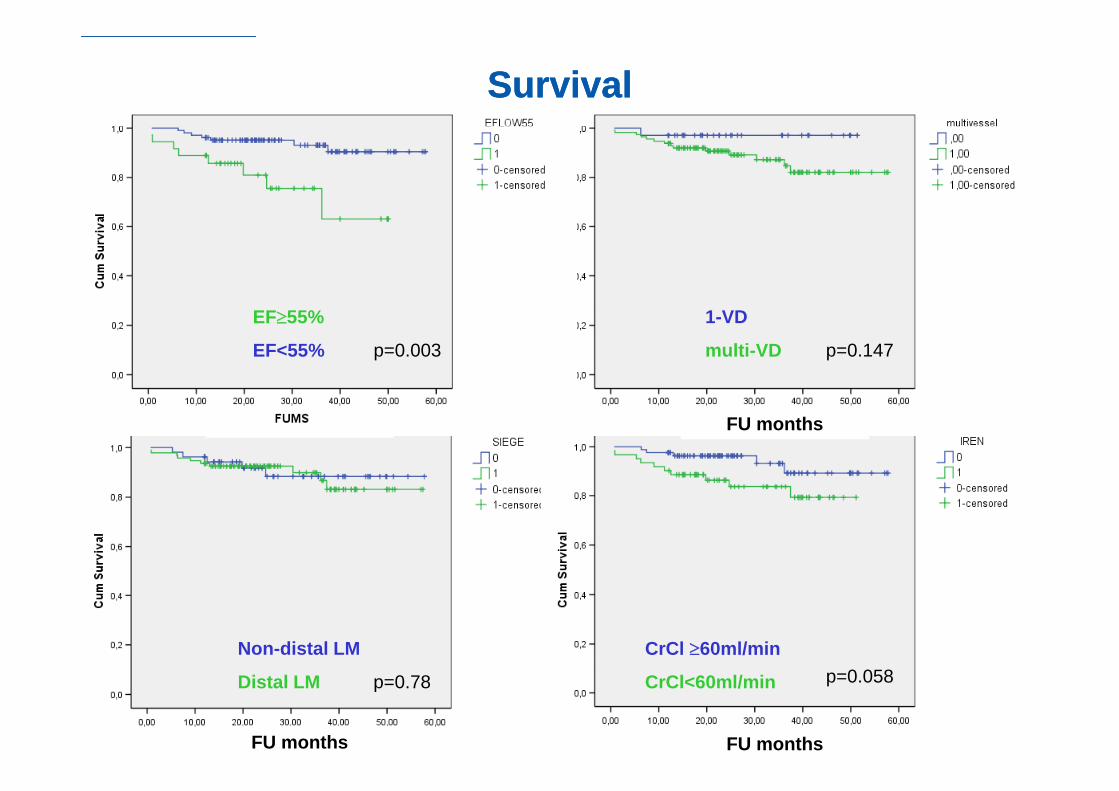
SurvivalSurvival
1-VD
multi-VD
EF≥55%
EF<55% p=0.003 p=0.147
FU months FU months
Non-distal LM CrCl ≥60ml/min
FU months FU months
Distal LM CrCl<60ml/minp=0.78 p=0.058
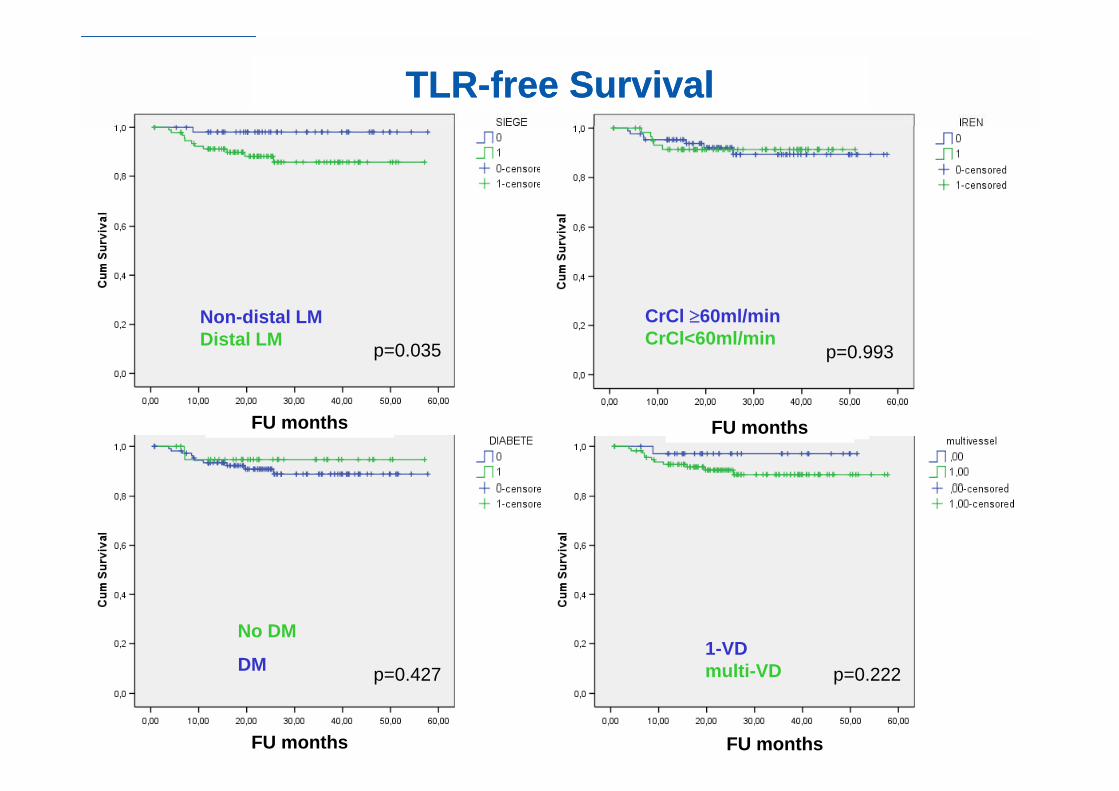
TLRTLR--free Survivalfree Survival
Non-distal LMDistal LM
CrCl ≥60ml/minCrCl<60ml/minp=0.035 p=0.993
FU months FU monthsFU months
No DM
DM1-VD
lti VD
FU months FU months
DM multi-VDp=0.427 p=0.222
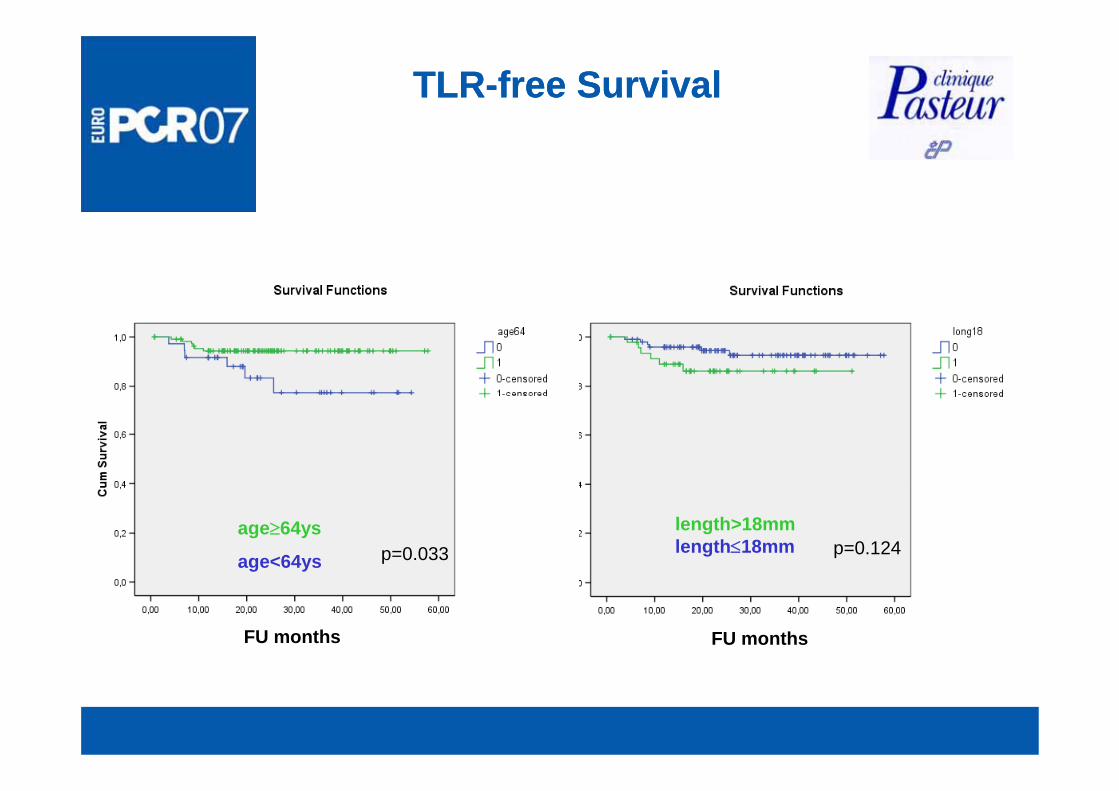
TLRTLR--free Survivalfree Survival
age≥64ys
age<64ys
length>18mmlength≤18mmp=0.033 p=0.124
FU months FU months
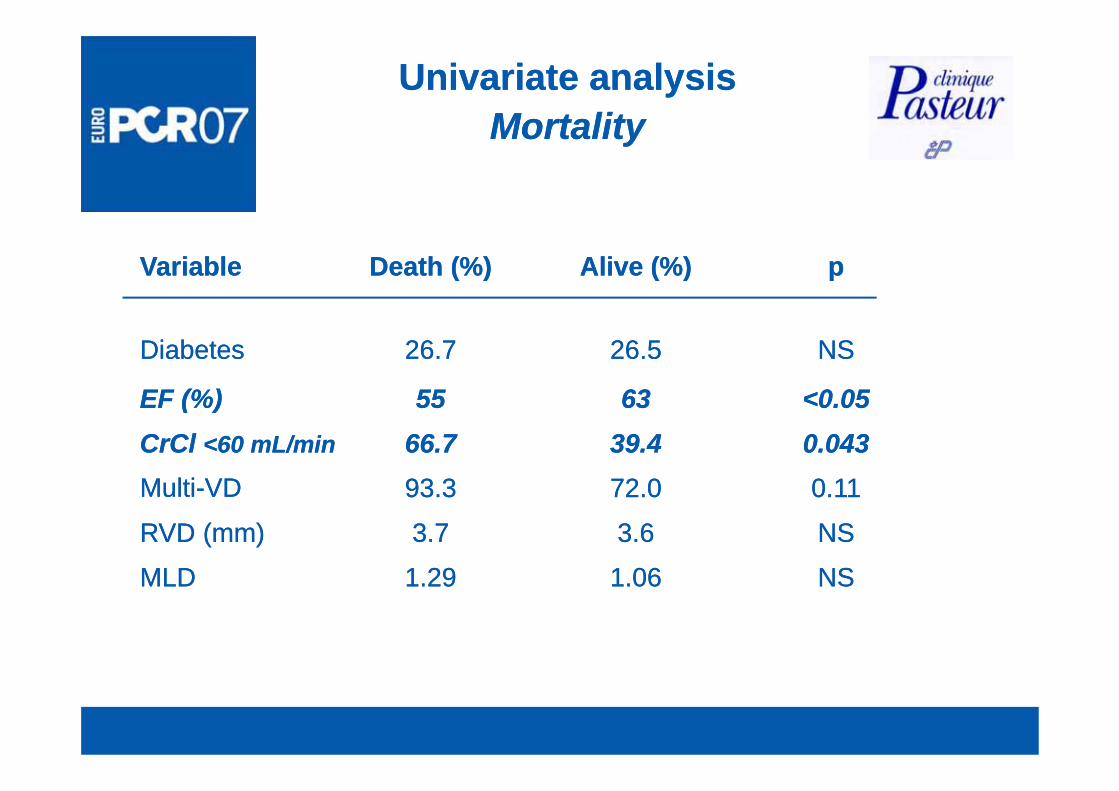
Univariate analysisUnivariate analysisMortalityMortalityMortalityMortality
Alive (%)Alive (%) ppDeath (%)Death (%)VariableVariable
6363
26.526.5 NSNS26.726.7DiabetesDiabetes
<0 05<0 055555EF (%)EF (%)
72 072 0
39.439.46363
0.0430.04366.766.7CrCl CrCl <60 mL/min<60 mL/min
0 110 1193 393 3MultiMulti VDVD
<0.05<0.055555EF (%)EF (%)
1 061 06
3.63.6
72.072.0
NSNS1 291 29MLDMLD
NSNS3.73.7RVD (mm)RVD (mm)
0.110.1193.393.3MultiMulti--VDVD
1.061.06 NSNS1.291.29MLDMLD
61.5 0.03791.7Distal LM
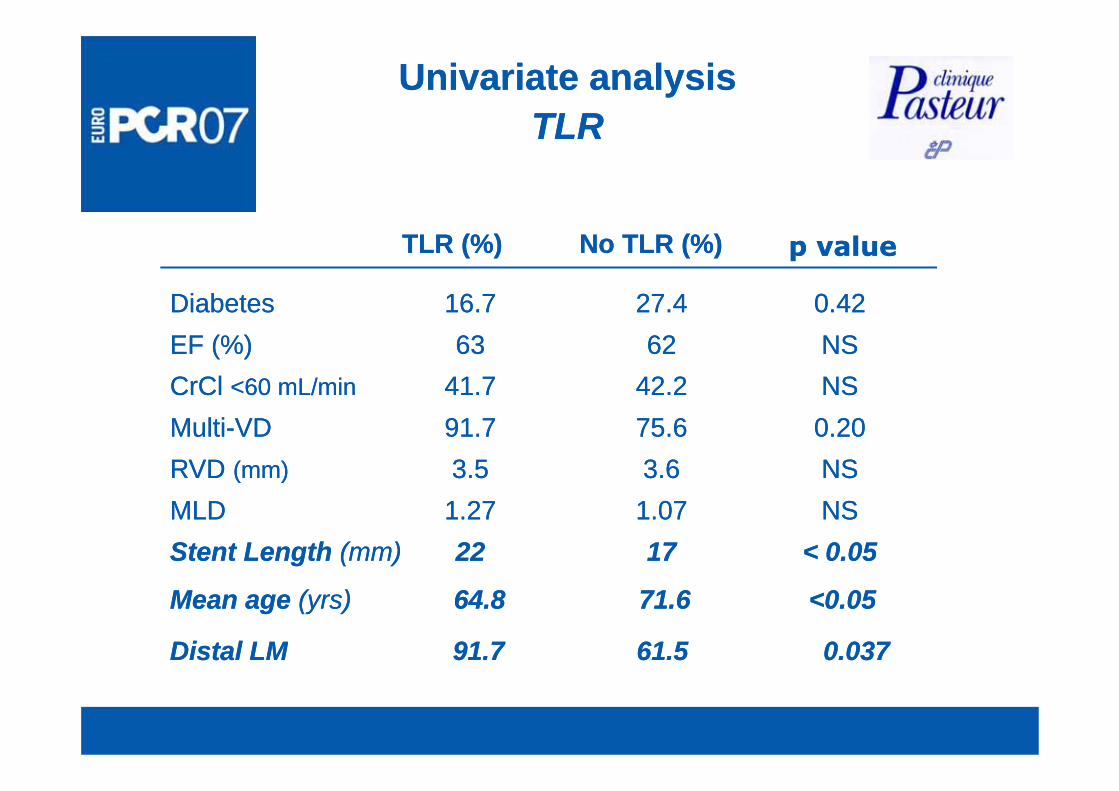
Univariate analysisUnivariate analysisTLRTLRTLRTLR
No TLR (%)No TLR (%)TLR (%)TLR (%) p valuep value
27 427 4 0 420 4216 716 7DiabetesDiabetes
42.242.26262
27.427.4 0.420.4216.716.7DiabetesDiabetesNSNS6363EF (%)EF (%)NSNS41.741.7CrCl CrCl <60 mL/min<60 mL/min
3.63.675.675.6 0.200.2091.791.7MultiMulti--VDVD
NSNS3.53.5RVD RVD (mm)(mm)
NSNS1.071.071.271.27MLDMLD< 0.05< 0.0517172222Stent Length Stent Length (mm)(mm)
61.561.5 0.0370.03791.791.7Distal LMDistal LM
Mean age Mean age (yrs)(yrs) 64.864.8 71.671.6 <0.05<0.05
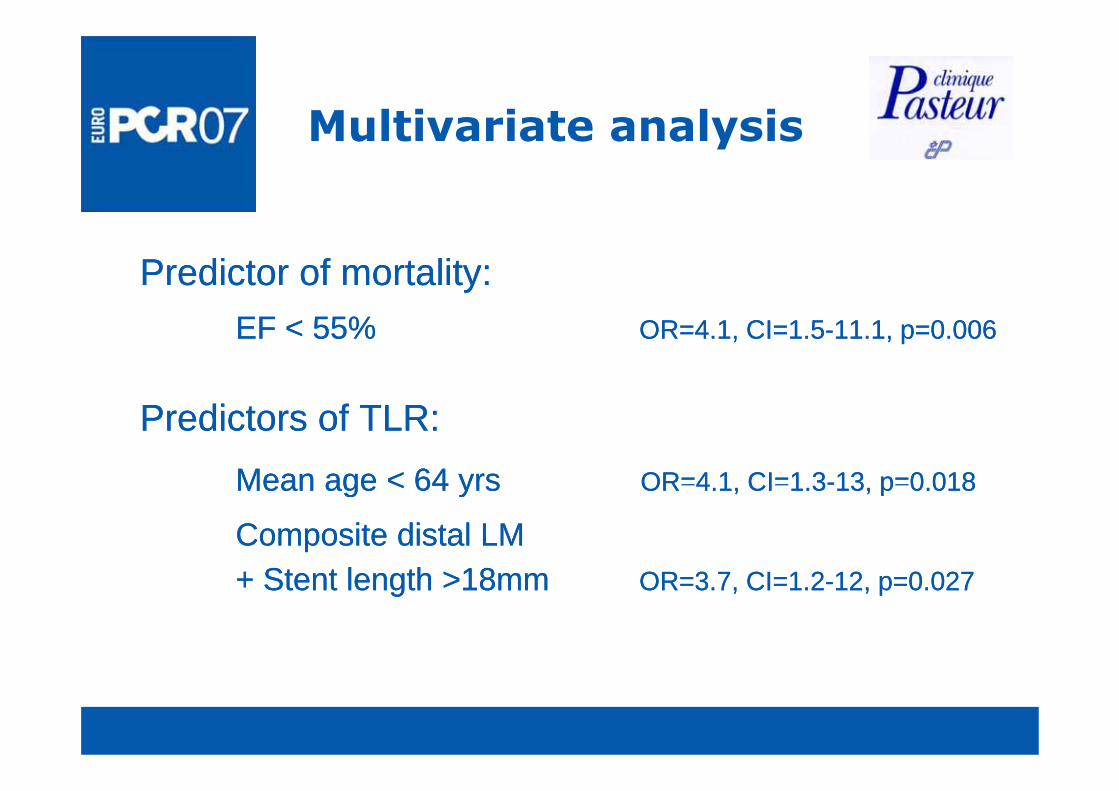
Multivariate analysisMultivariate analysis
Predictor of mortality:Predictor of mortality:EF < 55%EF < 55% OR=4.1, CI=1.5OR=4.1, CI=1.5--11.1, p=0.00611.1, p=0.006
Predictors of TLR:Predictors of TLR:Mean age < 64 yrsMean age < 64 yrs OR=4 1 CI=1 3OR=4 1 CI=1 3--13 p=0 01813 p=0 018Mean age < 64 yrsMean age < 64 yrs OR 4.1, CI 1.3OR 4.1, CI 1.3 13, p 0.01813, p 0.018
Composite distal LM Composite distal LM + Stent length >18mm+ Stent length >18mm OR 3 7 CI 1 2OR 3 7 CI 1 2 12 0 02712 0 027+ Stent length >18mm+ Stent length >18mm OR=3.7, CI=1.2OR=3.7, CI=1.2--12, p=0.02712, p=0.027
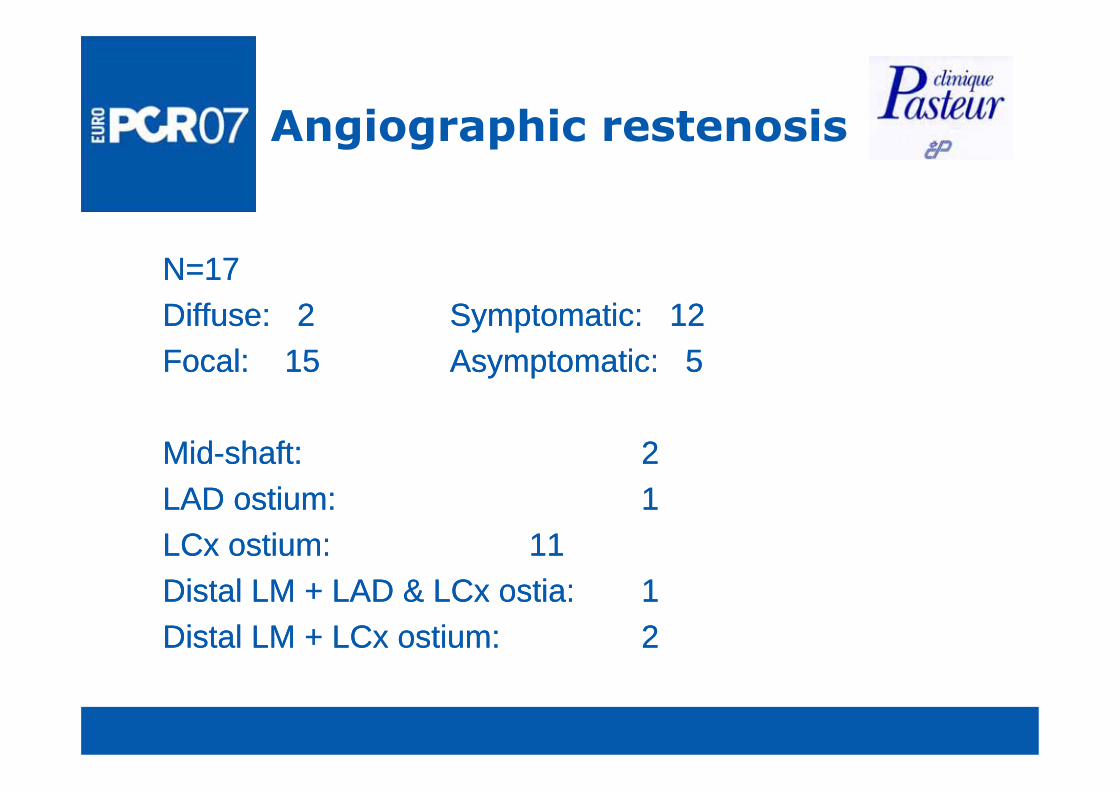
Angiographic restenosisAngiographic restenosis
N=17N=17Diff 2Diff 2 S t ti 12S t ti 12Diffuse: 2Diffuse: 2 Symptomatic: 12Symptomatic: 12Focal: 15Focal: 15 Asymptomatic: 5Asymptomatic: 5
MidMid--shaft: shaft: 22LAD ostium: LAD ostium: 1 1 LCx ostium: LCx ostium: 1111Distal LM + LAD & LCx ostia: Distal LM + LAD & LCx ostia: 11Distal LM + LCx ostium: Distal LM + LCx ostium: 2 2
Treatment of LM diseaseTreatment of LM disease
I.I. What have we learned?What have we learned?–– BMSBMS–– DESDES
IIII What are we doing in daily practice?What are we doing in daily practice?II.II.What are we doing in daily practice?What are we doing in daily practice?
III.III. How to select patients for PCI or CABG? How to select patients for PCI or CABG?
Unprotected LM diseaseUnprotected LM diseaseUnprotected LM diseaseUnprotected LM disease
Indications of PCI are based onIndications of PCI are based on
Clinical characteristicsClinical characteristicsage, diabetes, renal function, carotid age, diabetes, renal function, carotid di i di i t ti l ldi i di i t ti l ldisease, previous cardiac intervention, valvular disease, previous cardiac intervention, valvular disease, codisease, co--morbiditymorbidity
Angiographic characteristicsAngiographic characteristicsLV function, distal or no distal LM, trifurcatedLV function, distal or no distal LM, trifurcatedLV function, distal or no distal LM, trifurcated LV function, distal or no distal LM, trifurcated LM, length of LM lesion, calcification, diffuse LM, length of LM lesion, calcification, diffuse disease, MVD, complex lesions (bifurcation, CTO) disease, MVD, complex lesions (bifurcation, CTO) on the other vessels quality of the distal vesselson the other vessels quality of the distal vesselson the other vessels, quality of the distal vessels on the other vessels, quality of the distal vessels
LM stenting techniqueLM stenting techniqueLM stenting techniqueLM stenting technique
Technique of stenting is based on bifurcation anatomy Technique of stenting is based on bifurcation anatomy
distribution of plaquedistribution of plaquebifurcation anglebifurcation anglebifurcation anglebifurcation anglediameter of vesselsdiameter of vesselslength of LMlength of LMlength of LMlength of LMdiffusion of diseasediffusion of disease
Treatment of LM diseaseTreatment of LM disease
I.I. What have we learned?What have we learned?–– BMSBMS–– DESDES
IIII What are we doing in daily practice?What are we doing in daily practice?II.II. What are we doing in daily practice?What are we doing in daily practice?
III.III. How to select patients for PCI or CABG?How to select patients for PCI or CABG?
Unprotected LMCA StentingUnprotected LMCA StentingUnprotected LMCA StentingUnprotected LMCA Stenting
1. Ideal cases for stenting1. Ideal cases for stentingLowLow--risk patients, with good LV function, non distal and non risk patients, with good LV function, non distal and non calcified left main stenosis,calcified left main stenosis,calcified left main stenosis, calcified left main stenosis,
Ostial LMOstial LM
MidMid--shaft LMshaft LM
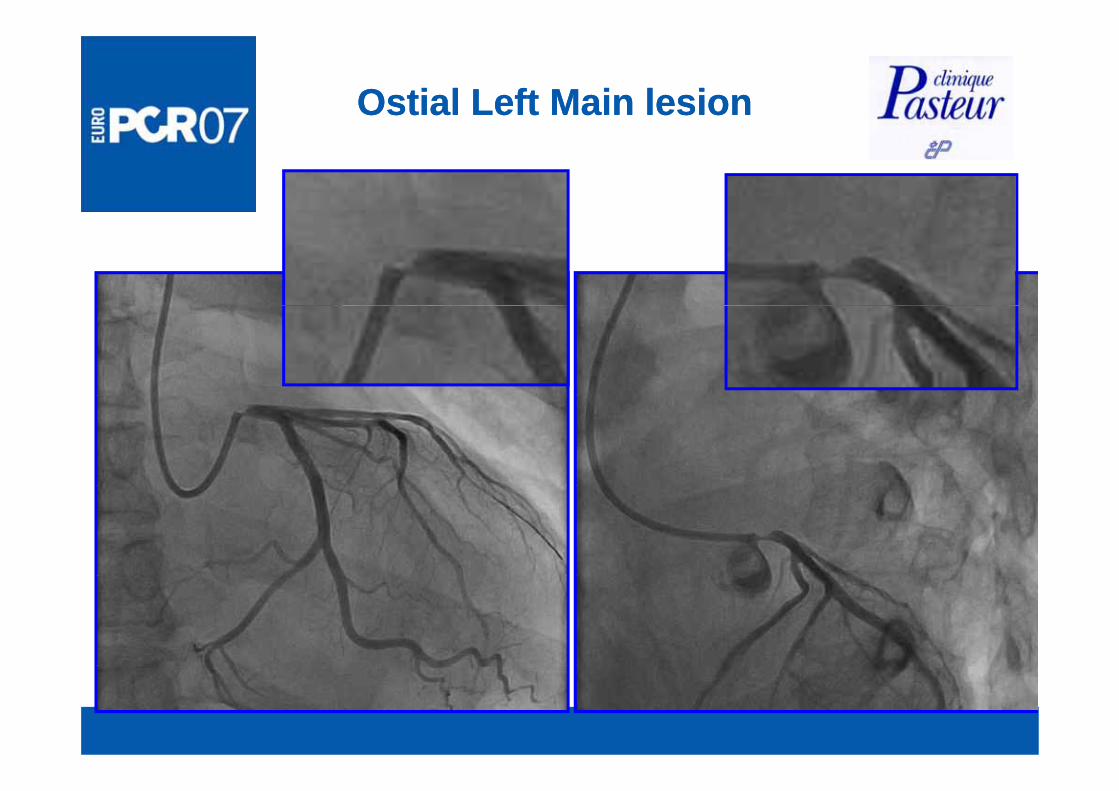
Ostial Left Main lesionOstial Left Main lesion
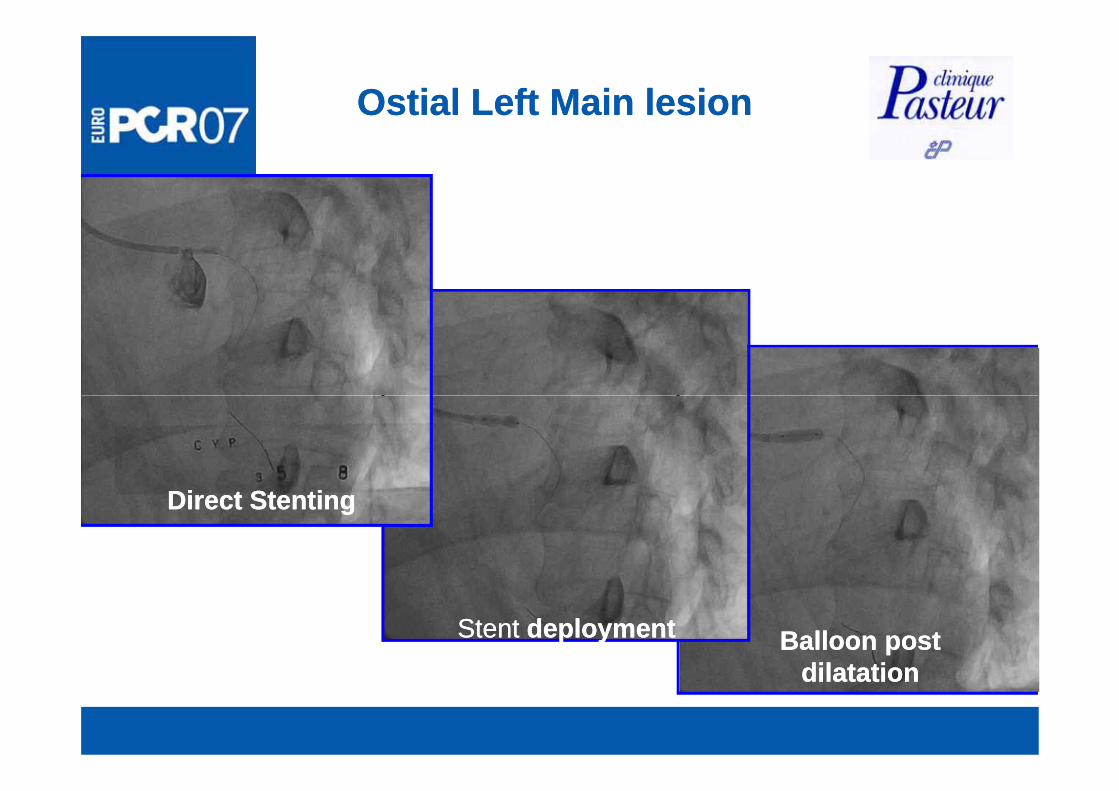
Ostial Left Main lesionOstial Left Main lesion
Direct StentingDirect Stenting
Stent Stent deploymentdeployment Balloon post Balloon post dil t tidil t tidilatationdilatation
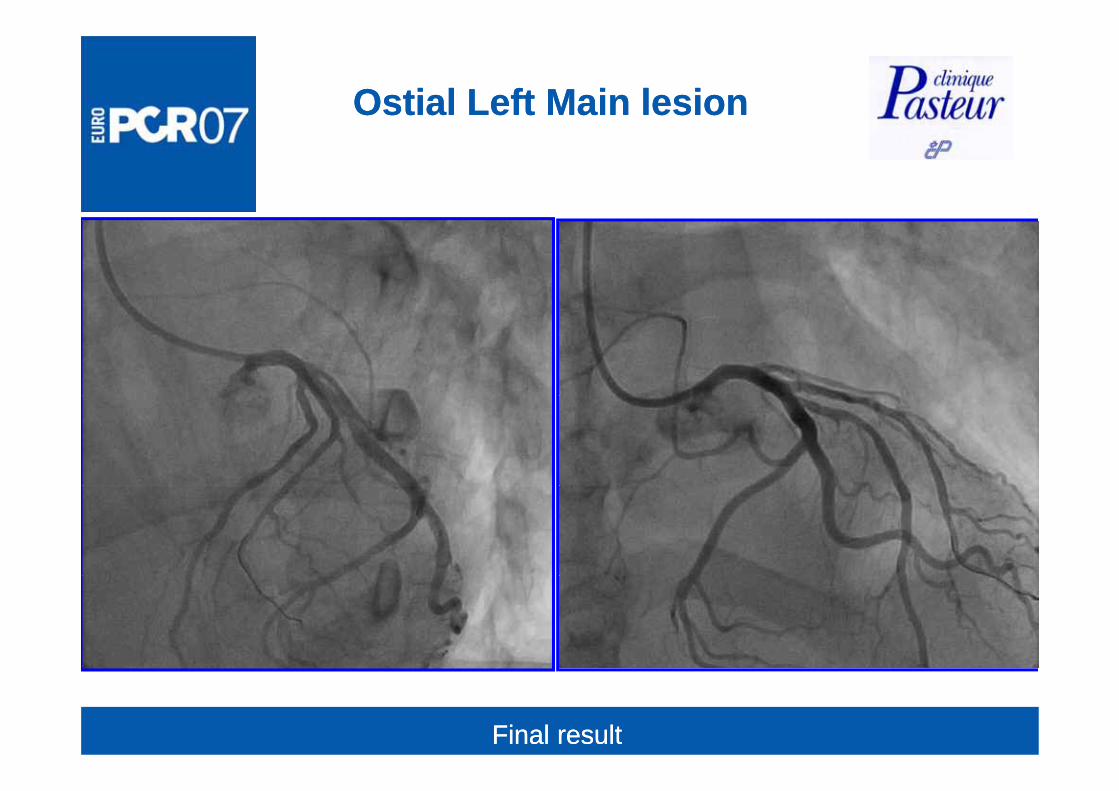
Ostial Left Main lesionOstial Left Main lesion
Final resultFinal result
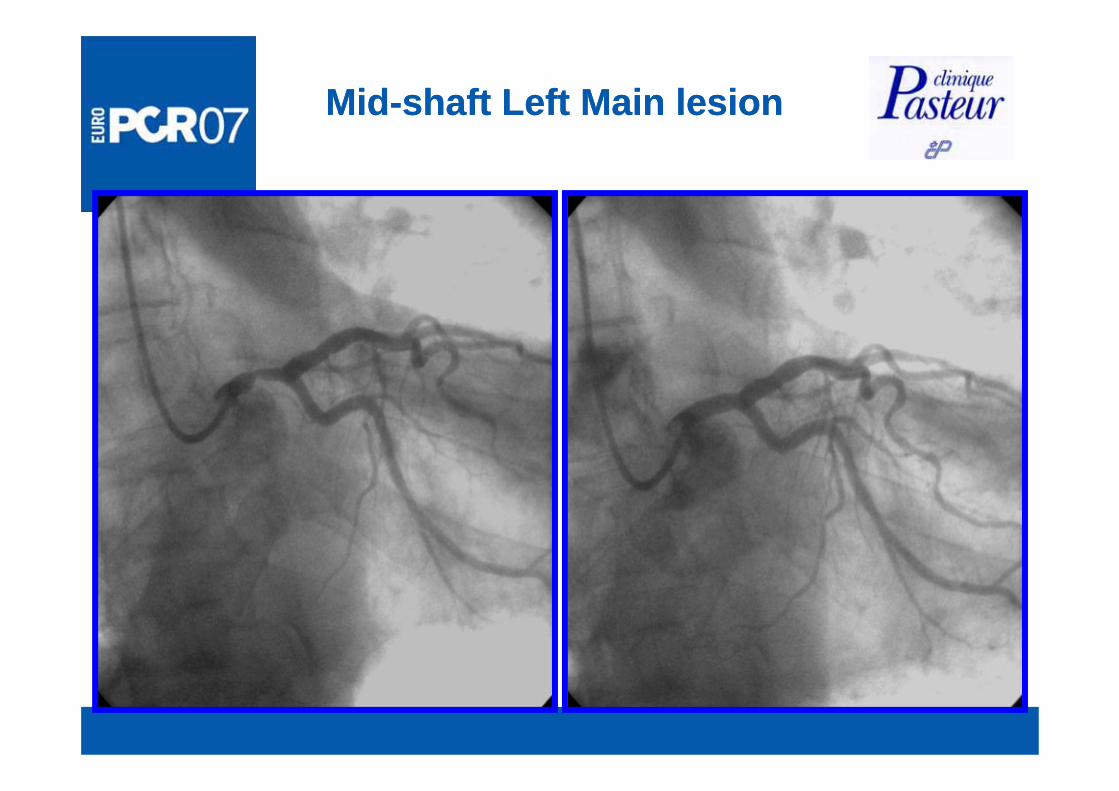
MidMid--shaft Left Main lesionshaft Left Main lesion
Unprotected LMCA StentingUnprotected LMCA StentingU p otected C Ste t gU p otected C Ste t g
2. Technically difficult and controversial2. Technically difficult and controversialPatients with preserved LV function and non calcified Patients with preserved LV function and non calcified di t l LM bif ti l i i l i th ti f LADdi t l LM bif ti l i i l i th ti f LADdistal LM bifurcation lesion involving the ostium of LAD distal LM bifurcation lesion involving the ostium of LAD and LCxand LCx
PCI could be considered whenPCI could be considered whensmall LCxsmall LCxsmall LCxsmall LCxelderlyelderlyhigh surgical risk (Euroscore)high surgical risk (Euroscore)g g ( )g g ( )distal coronary disease unfavorable to CABGdistal coronary disease unfavorable to CABGcomorbidity (chronic obstructive lung disease) comorbidity (chronic obstructive lung disease) emergency clinical situation: acute LM occlusionemergency clinical situation: acute LM occlusion
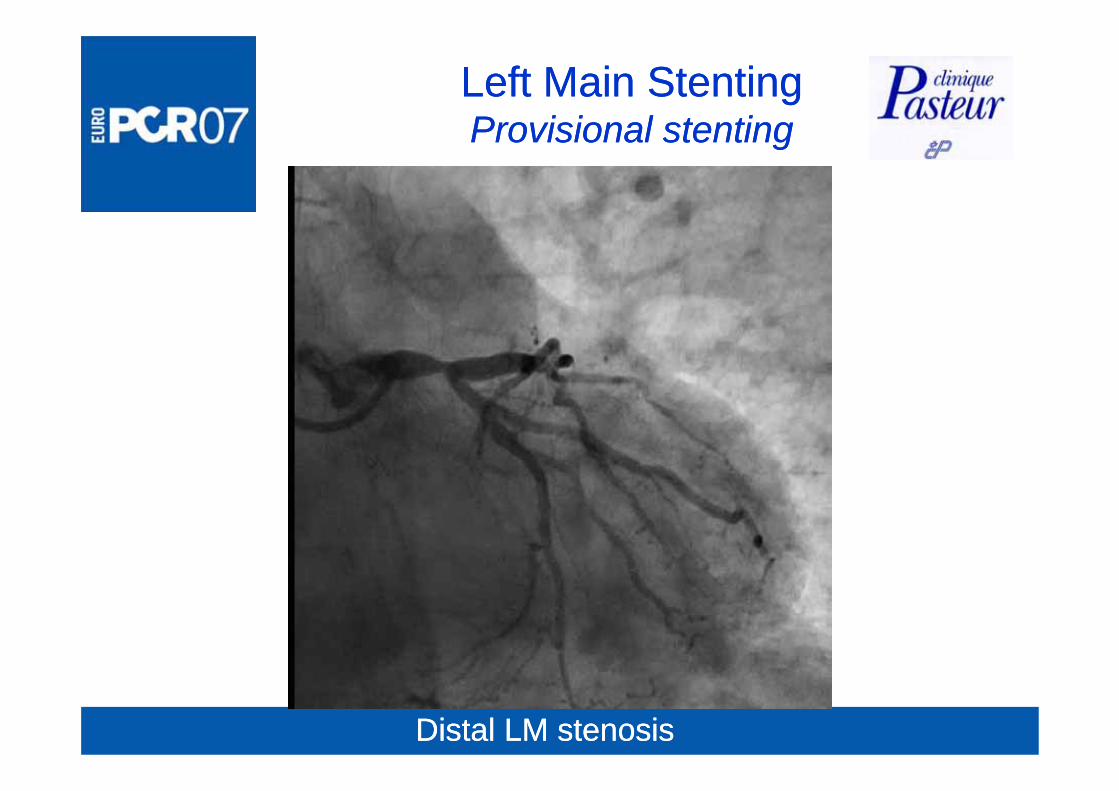
Left Main StentingLeft Main StentingProvisional stentingProvisional stentingProvisional stentingProvisional stenting
Distal LM stenosisDistal LM stenosis
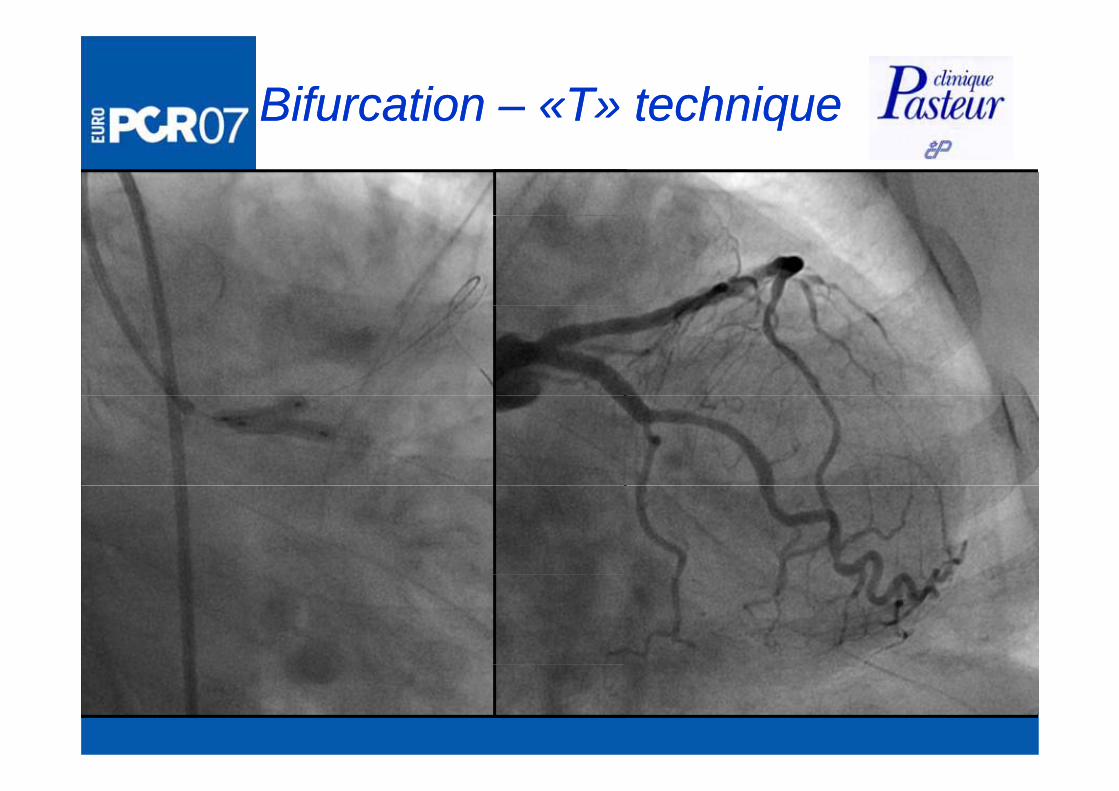
Bifurcation Bifurcation –– «T» technique«T» techniqueqq
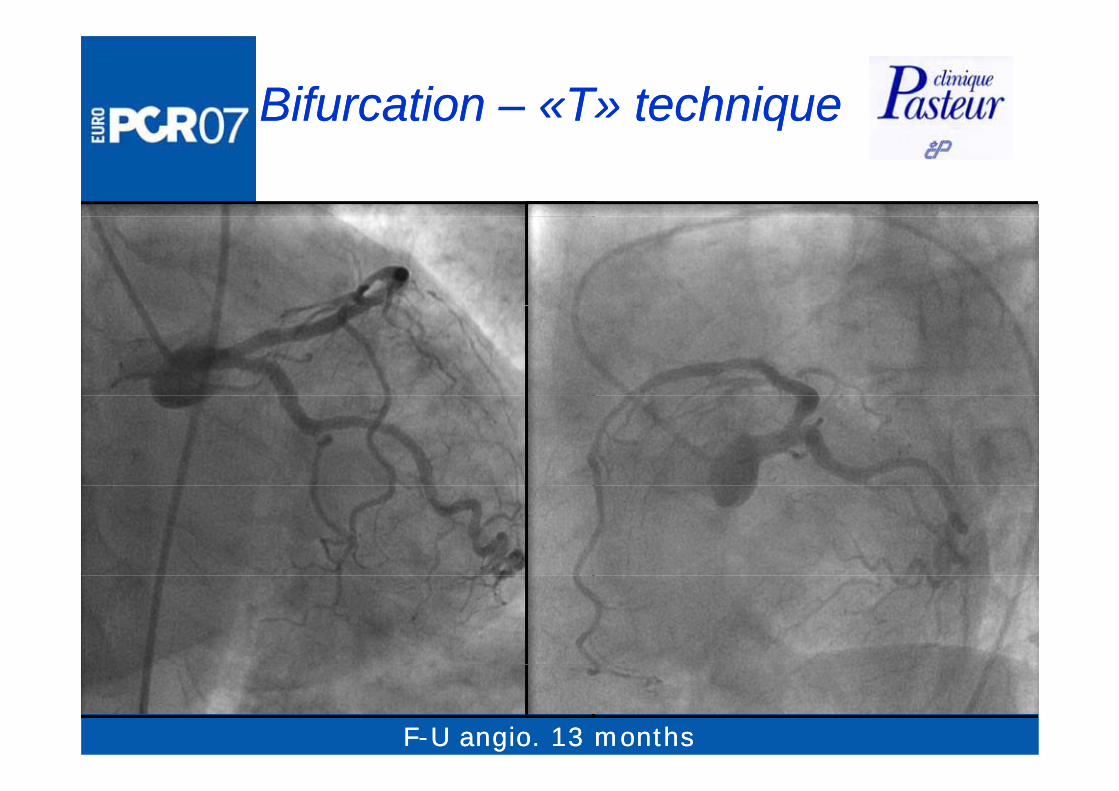
Bifurcation Bifurcation –– «T» technique«T» techniqueqq
FF--U angio. 13 monthsU angio. 13 months
Unprotected LMCA StentingUnprotected LMCA StentingUnprotected LMCA StentingUnprotected LMCA Stenting
33. Surgery preferred. Surgery preferred. Heavy calcified LM disease. Heavy calcified LM disease
. Reduced LV function. Reduced LV function
. Good candidate for surgery. Good candidate for surgery
with distal bifurcation lesion and reduced LVwith distal bifurcation lesion and reduced LVwith distal bifurcation lesion and reduced LV with distal bifurcation lesion and reduced LV functionfunction
with distal bifurcation lesion and occluded RCAwith distal bifurcation lesion and occluded RCAwith distal bifurcation lesion and occluded RCAwith distal bifurcation lesion and occluded RCA
with MVD suitable for CABGwith MVD suitable for CABG
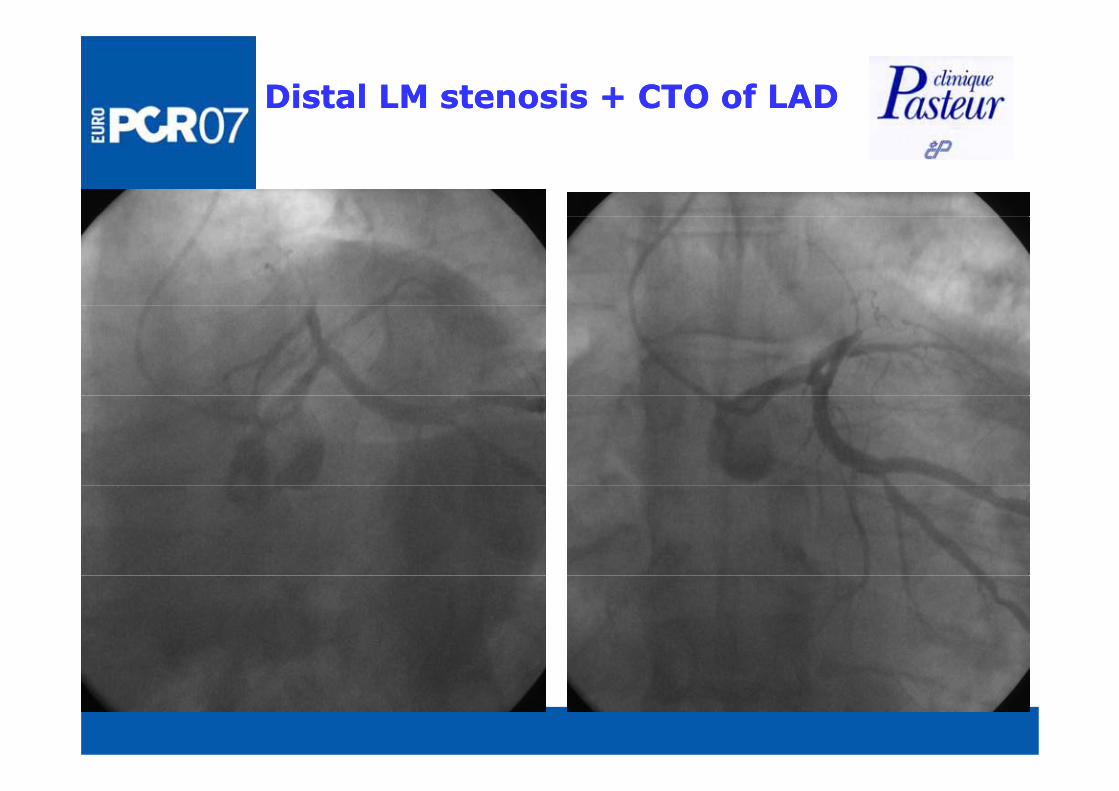
Distal LM stenosis + CTO of LADDistal LM stenosis + CTO of LAD

Distal LM stenosis + CTO of LADDistal LM stenosis + CTO of LAD
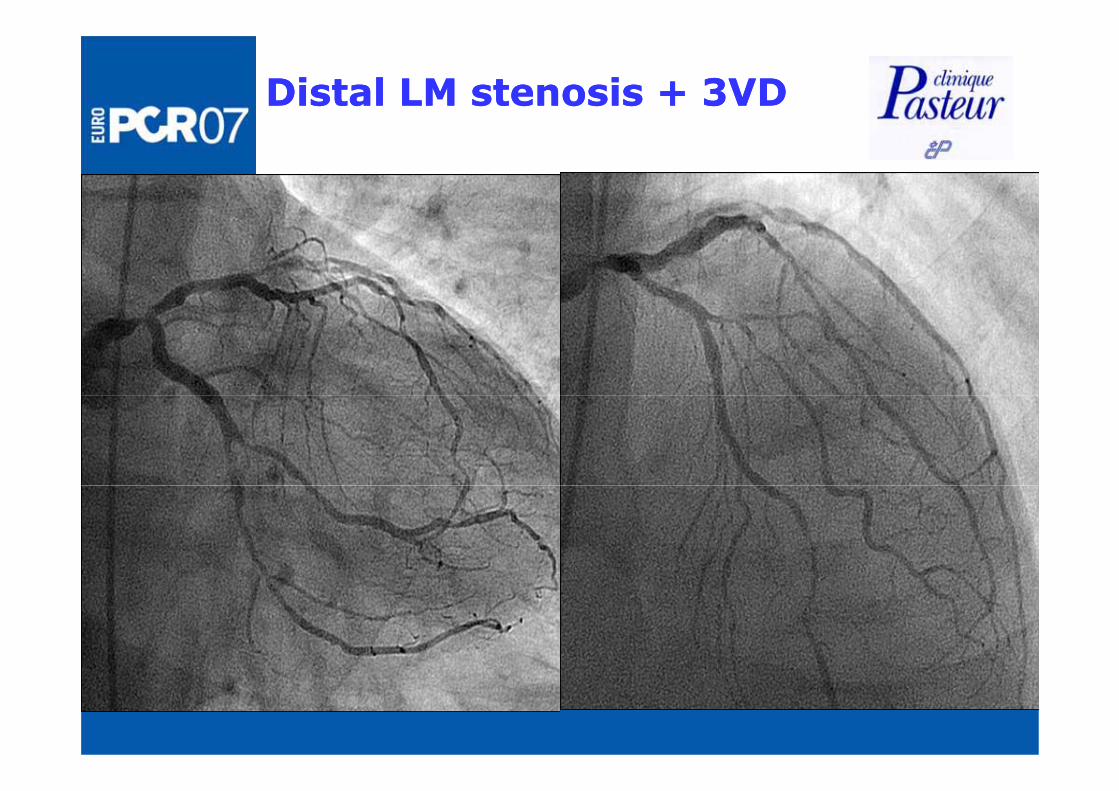
Distal LM stenosis + 3VDDistal LM stenosis + 3VD
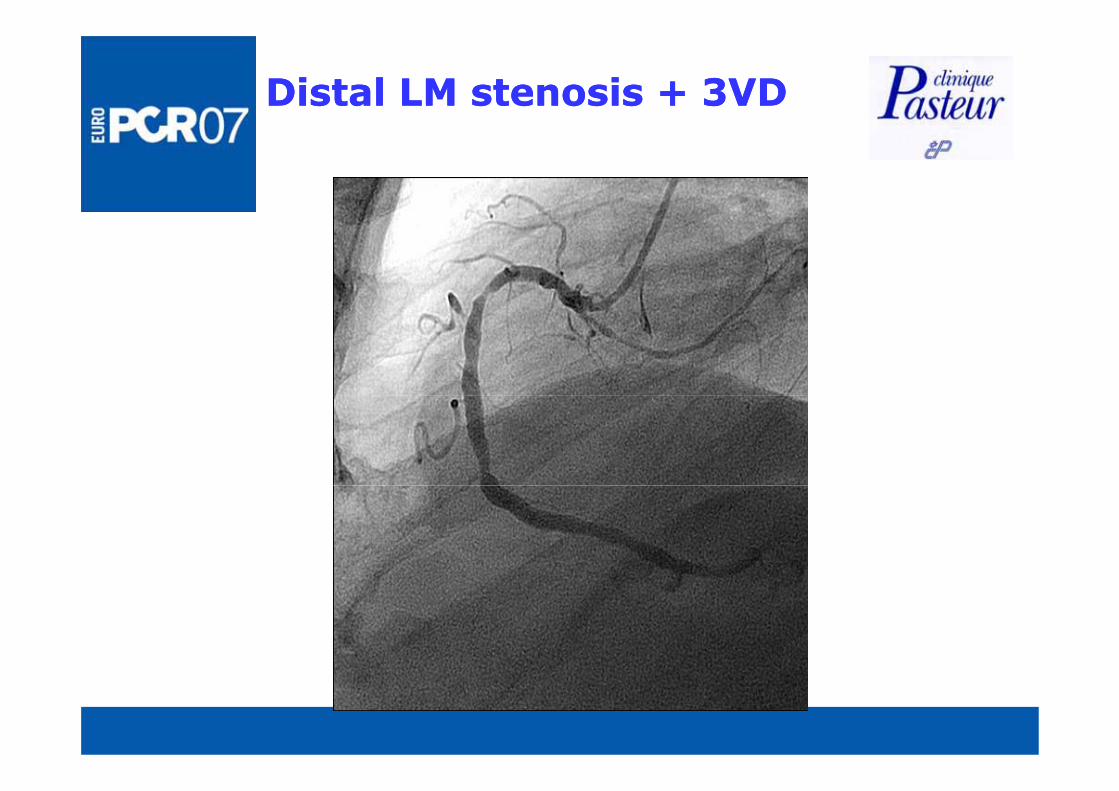
Distal LM stenosis + 3VDDistal LM stenosis + 3VD
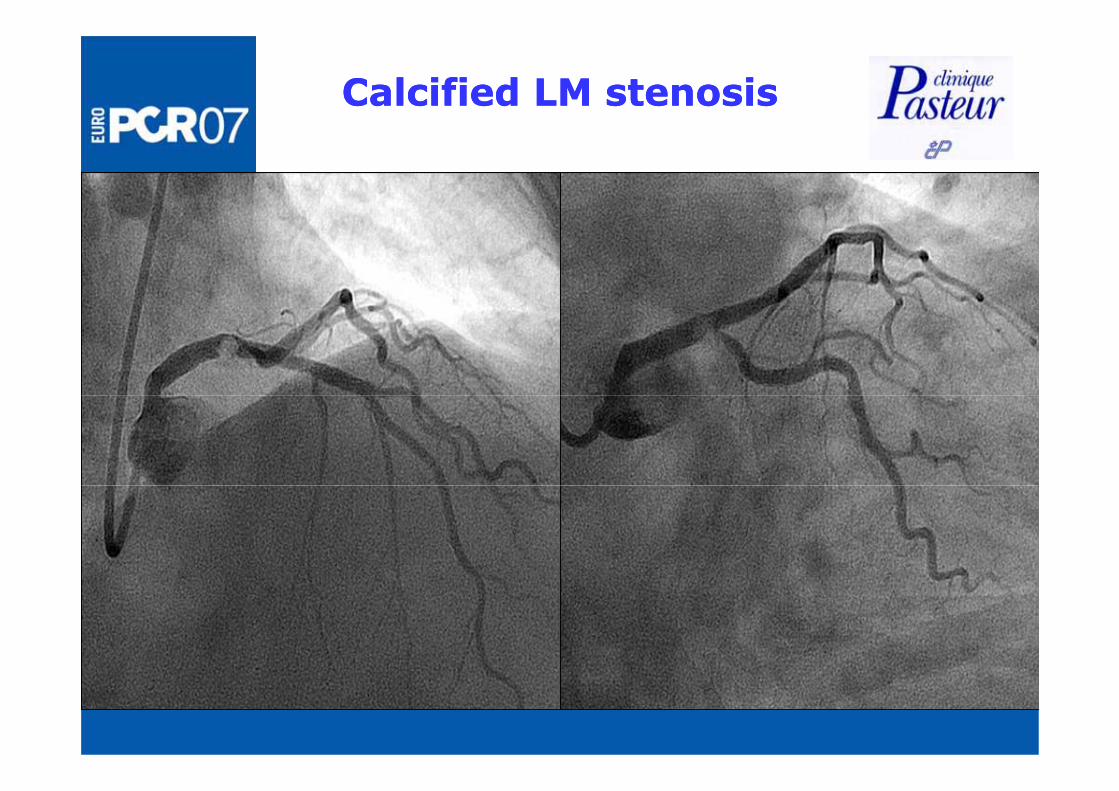
Calcified LM stenosisCalcified LM stenosis
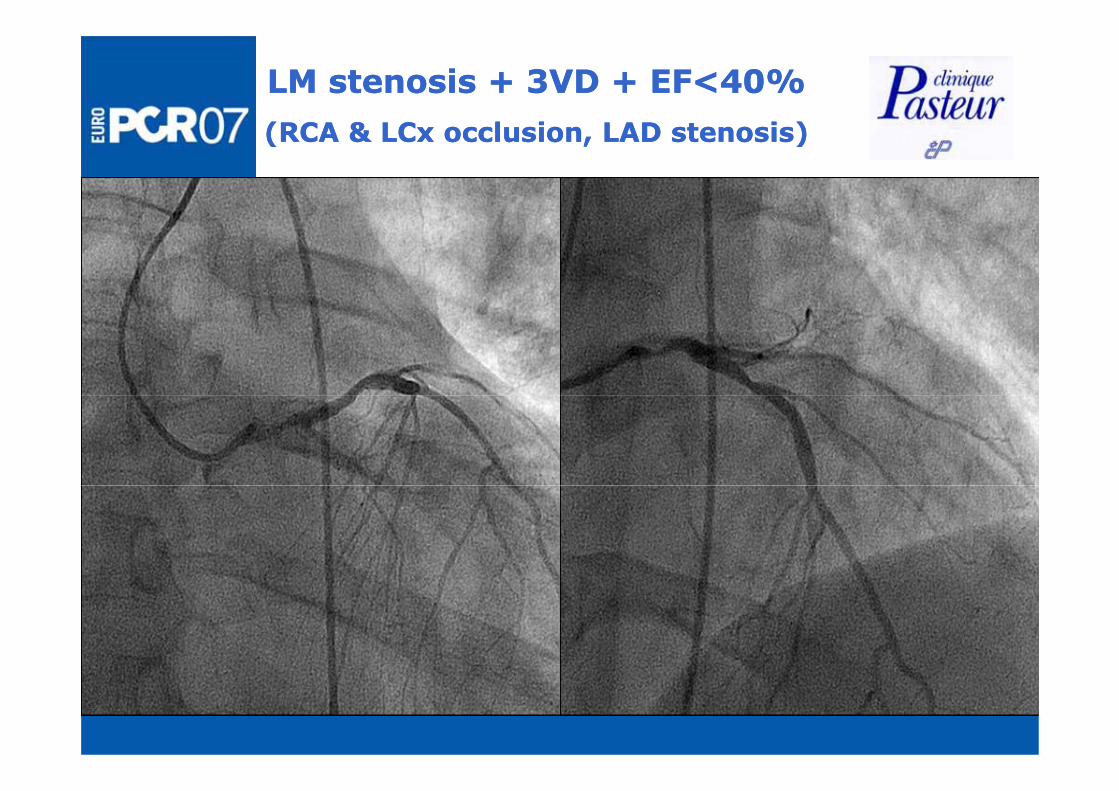
LM stenosis + 3VD + EF<40% LM stenosis + 3VD + EF<40%
(RCA & LC l i LAD t i )(RCA & LC l i LAD t i )(RCA & LCx occlusion, LAD stenosis)(RCA & LCx occlusion, LAD stenosis)
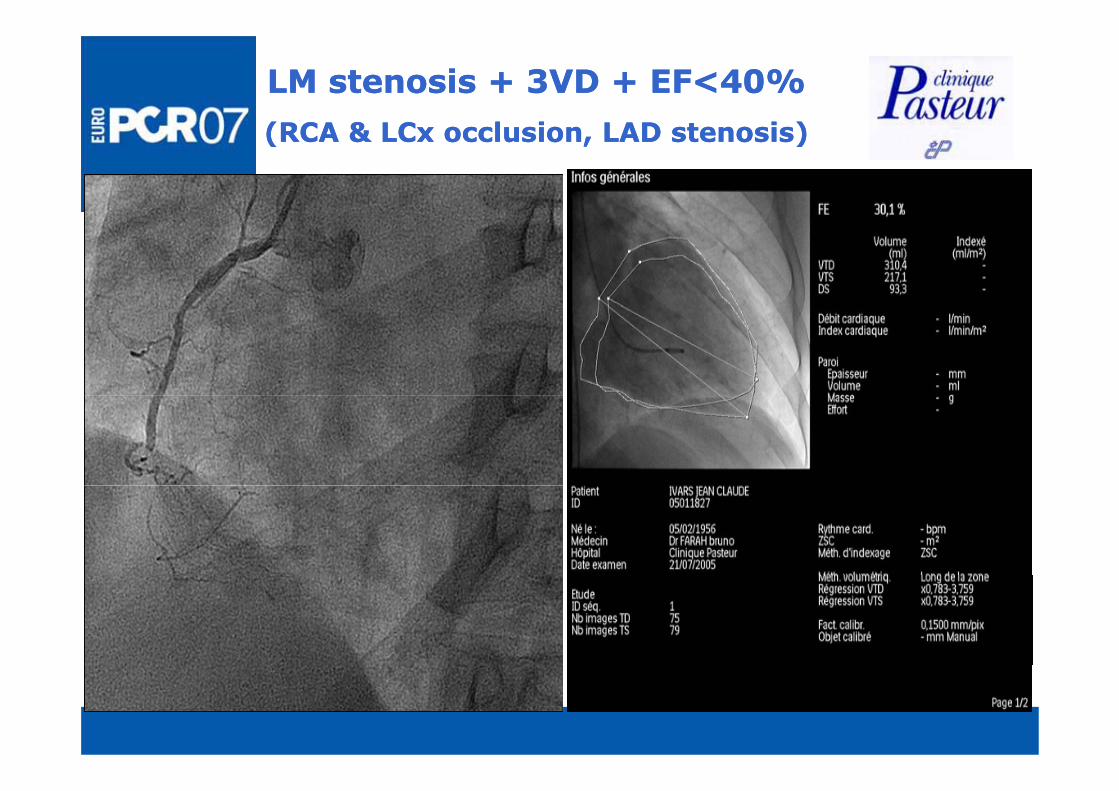
LM stenosis + 3VD + EF<40% LM stenosis + 3VD + EF<40%
(RCA & LC l i LAD t i )(RCA & LC l i LAD t i )(RCA & LCx occlusion, LAD stenosis)(RCA & LCx occlusion, LAD stenosis)
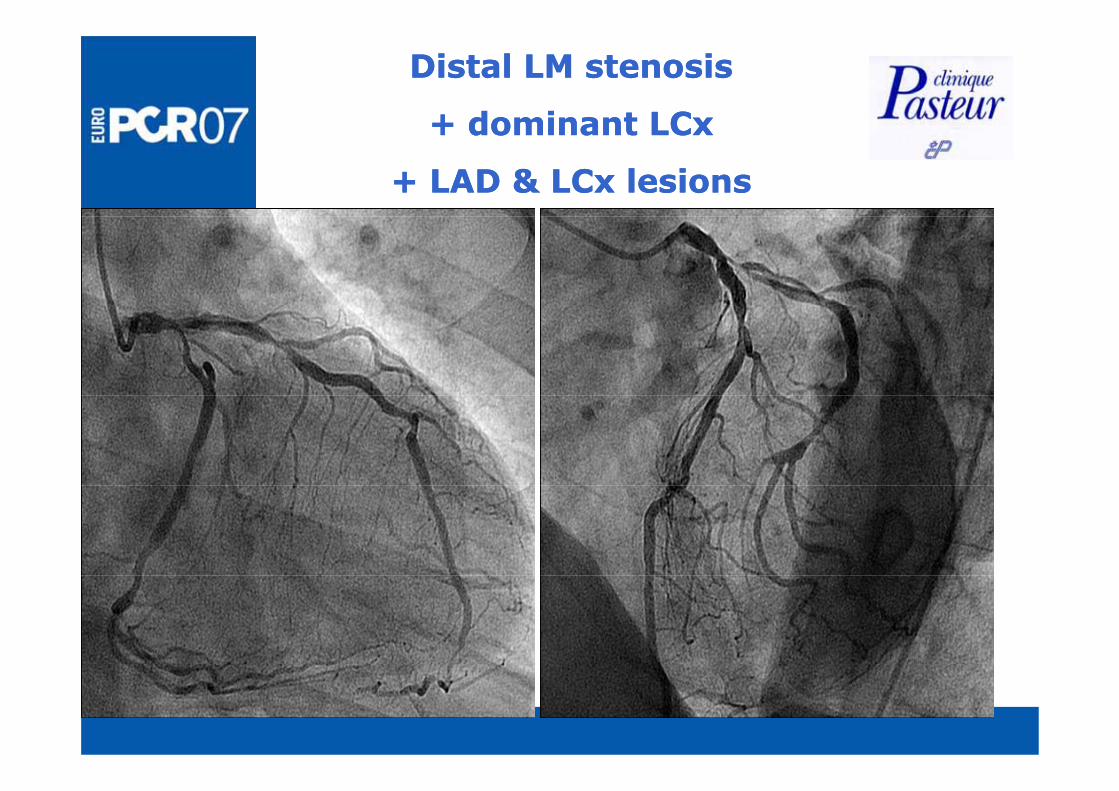
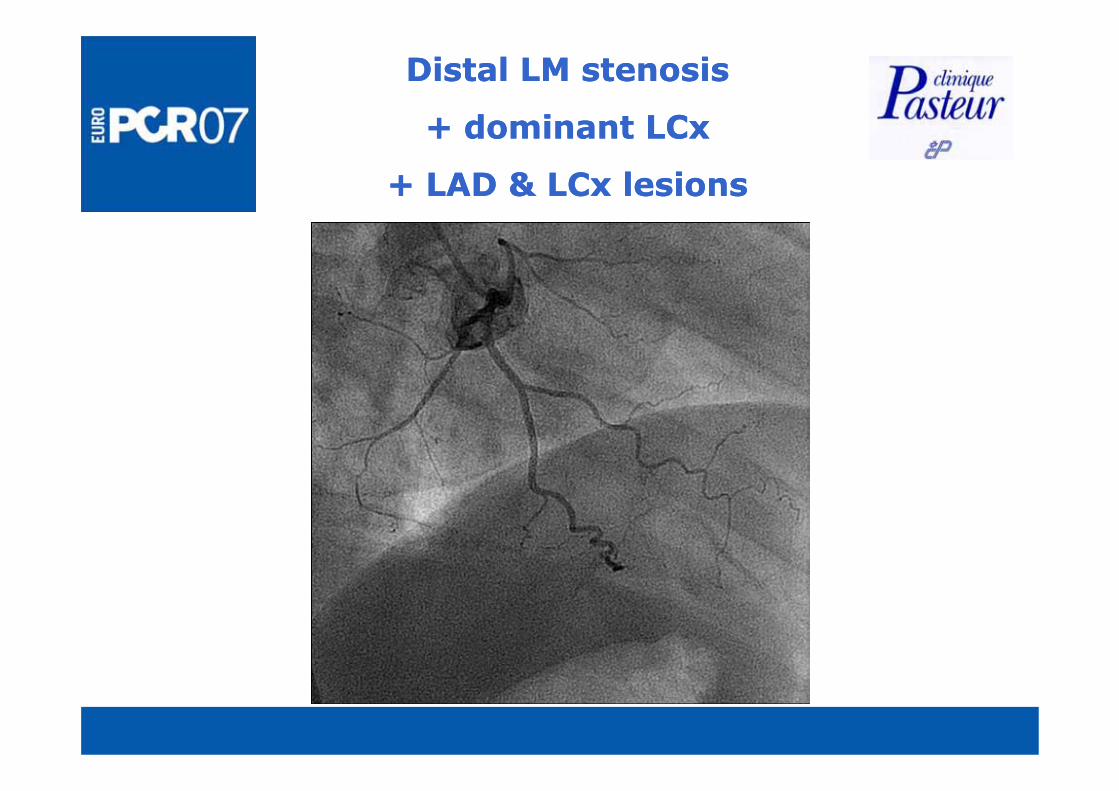
Distal LM stenosis Distal LM stenosis
+ dominant LCx + dominant LCx + dominant LCx + dominant LCx
+ LAD & LCx lesions+ LAD & LCx lesions
Distal LM stenosis Distal LM stenosis
+ dominant LCx + dominant LCx + dominant LCx + dominant LCx
+ LAD & LCx lesions+ LAD & LCx lesions
Left main stentingLeft main stentingLeft main stentingLeft main stenting
••Stenting can be performed with acceptable results in Stenting can be performed with acceptable results in selected patientsselected patientsselected patientsselected patients••Patient selection (clinical & angiographic Patient selection (clinical & angiographic h t i ti ) i i l d t b di d ithh t i ti ) i i l d t b di d ithcharacteristics) is crucial and must be discussed with characteristics) is crucial and must be discussed with
surgeonsurgeonC f l f llC f l f ll i d d t l t f t di d d t l t f t d••Careful followCareful follow--up is needed to evaluate safety and up is needed to evaluate safety and
efficacy of our proceduresefficacy of our procedures••Trials are needed Trials are needed