Embed Size (px)
Citation preview
AAPM REPORT NO. 40
RADIOLABELED ANTIBODYTUMOR DOSIMETRY
REPORT OFTASK GROUP NO. 2
AAPM NUCLEAR MEDICINE COMMITTEE
MembersBarry W. Wessels, Chairman
A. Bertrand BrillDonald J. Buchsbaum
Laurence P. ClarkeDarrell R. FisherJohn L. Humm
Timothy K. JohnsonJerry L. Klein
Kenneth F. KoralCheuk S. Kwok
Virginia LangmuirPeter K. LeichnerDaniel J. MaceyGeorge SgourosJeffry A. Siegel
Edward A. SilversteinMike Stabin
Sven-Erik StrandEvelyn E. Watson
Lawrence E. WilliamsLatresla A. Wilson
Ellen D. YorkePat Zanzonico
April 1993
Published for theAmerican Association of Physicists in Medicine
by the American Institute of Physics

DISCLAIMER: This publication is based on sources and information believed to bereliable, but the AAPM and the editors disclaim any warranty or liability based on orrelating to the contents of this publication.
The AAPM does not endorse any products, manufacturers, or suppliers. Nothing inthis publication should be interpreted as implying such endorsement.
Further copies of this report ($10 prepaid) may be obtained from:
American Institute of Physicsc/o AIDC
64 Depot RoadColchester, Vermont 05446
(l-800-488-2665)
International Standard Book Number: 1-56396-233-0International Standard Serial Number: 0271-7344
©1993 by the American Association of Physicists in Medicine
All rights reserved. No part of this publication may be reproduced, stored in a retrievalsystem, or transmitted in any form or by any means (electronic, mechanical, photo-copying, recording, or otherwise) without the prior written permission of the publisher.
Published by the American Institute of Physics, Inc.336 East 45th Street, New York, NY 10017-3463
Printed in the United States of America

CONTENTS
Journal Editor’s PrefaceJ o h n S . L a u g h l i n . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Co-Editors’ PrefaceDavid A. Weber and Amin I. Kassis........................................................................................................................................
Introduction: Radiolabeled antibody tumor dosimetryDonald J. Buchsbaum and Barry W. Wessels.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Selection of radionuclides for radioimmunotherapyLeonard F. Mausner and Suresh C. Srivastava..................................................................................................................
MIRD formulationEvelyn E. Watson, Michael G. Stabin, and Jeffry A. Siegel . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Pharmacokinetic modelingSven-Erik Strand, Pat Zanzonico, and Timothy K. Johnson.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Tumor dosimetry in radioimmunotherapy: Methods of calculation for beta particlesPeter K. Leichnerand Cheuk S. Kwok.................................................................................................................................
Microdosimetric concepts in radioimmunotherapyJ. L. Humm, J. C. Roeske, D. R. Fisher, and G. T. Y. Chen.. . . . . . . . . . . . . . . . . . . . . , . . . . . . . . . . , . . . . . . . . . . . . . . .
Multicellular dosimetry for beta-emitting radionuclides: Autoradiography, thermoluminescentdosimetry and three-dimensional dose calculations
E. D. Yorke, L. E. Williams, A. J. Demidecki, D. B. Heidorn, P. L. Roberson, and B. W. Wessels.. . . . . . . . . . . . . . .
Experimental radioimmunotherapyDonald J. Buchsbaum, Virginia K. Langmuir, and Barry W. Wessels . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
An overview of imaging techniques and physical aspects of treatment planning inradioimmunotherapy
Peter K. Leichner, Kenneth F. Koral, Ronald J. Jaszczak, Alan J. Green, George T. Y. Chen, andJ o h n C . R o e s k e . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . ,
Radioimmunotherapy dose estimation in patients with B-cell lymphomaJ. A. Siegel, D. M. Goldenberg, and C. C. Badger.. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Dosimetry of solid tumorsRuby F. Meredith, Timothy K. Johnson, Gene Plott, Daniel J. Macey, Robert L. Vessella, Latresia A. Wilson,Hazel B. Breitz, and Lawrence E. Williams . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Dosimetry of intraperitoneally administered radiolabeled antibodiesJohn C. Roeske, George T. Y. Chen, and A. Bertrand Brill . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Radiobiology of radiolabeled antibody therapy as applied to tumor dosimetryV. K. Langmuir, J. F. Fowler, S. J. Knox, B. W. Wessels, R. M. Sutherland, and J. Y. C. Wong . . . . . . . . . . . . . . . . .
497
497
499
503
511
515
529
535
543
551
569
579
583
593
601

Journal Editor’s Preface
The AAPM, through its Science Council, asked Medical Physics to accept theresponsibility for the scientific review of all of the manuscripts proposed for this reportand to consider the final manuscripts for publication in Medical Physics. This respon-sibility was accepted by the Editor and Editorial Board. The Editor then asked Dr.David A. Weber, Associate Editor and Head of Nuclear Medicine Research at theBrookhaven National Laboratory, and one of his scientific colleagues, Dr. Amin I.Kassis, Director of Radiation Biology, Brigham and Women’s Hospital, HarvardMedical School, to accept the responsibility for scientific reviews of the material to beprovided for the report and to serve as the Co-Editors of a special issue of the journal.This arrangement was approved by the Science Council of the AAPM and by theEditorial Board.
This review, a major task, has been carried out in a comprehensive and scientificallyrigorous manner by the Editors for this special issue with the vital assistance of theexpert referees, authors and Task Group members. Medical Physics appreciates thedecision of the Task Group to offer this important collection of articles written byauthorities in the field of radiolabeled antibody tumor dosimetry for publication in theAAPM journal.
John S. Laughlin
Co-Editors’ Preface
Monoclonal antibodies have been considered particularly appealing as selectivecarriers of diagnostic and therapeutic radionuclides in vivo. Their target specificitycontinues to attract investigators to identify and produce new agents for clinical use.In spite of the limited number of clinical applications at present, it is extremelyimportant that factors influencing the localization and clearance properties of radio-immunoconjugates, especially tumor-associated, antigen-specific antibodies, be consid-ered and understood by those administering them to patients so as to assess thosevariables that influence the absorbed radiation dose from internal emitters. The ab-sorbed radiation dose has been, and will continue to be, a pivotal factor in assessing therisks and therapeutic utilities of radiopharmaceuticals.
The AAPM Nuclear Medicine Task Group, under the leadership of Dr. BarryWessels, sought qualified experts in various specialties concerned with the dosimetryof radiolabeled antibodies to develop a well-balanced review of the multiple concernsand factors that influence the clinical use of radiolabeled anti-tumor antibodies. Dr.Donald J. Buchsbaum, a member of the Task Group, chaired a subcommittee respon-sible for coordinating and overseeing the preparation of all manuscripts. In the 13manuscripts produced, many of the approaches employed to estimate absorbed radi-ation dose in radioimmunotherapy have been evaluated, and the physical, physiologic,chemical, and biologic parameters affecting tumor dosimetry presented. In addition,the decay properties of various radionuclides and their radiobiologic effects have beendiscussed, and dose calculations at the organ, tissue, cellular, and subcellular levelscompared. The manuscripts, containing extensive, up-to-date reference lists, will bevery useful to those interested in the use of radiolabeled antibodies in the diagnosis andtreatment of disease.
We are pleased to have had the opportunity to explore with the authors the mul-tifaceted topic of radiolabeled-antibody tumor dosimetry. Since many of the experts inthis field are contributors to this supplement, it required some extra attention to findequally qualified referees. Having accomplished this, we would like to express oursincere gratitude to those who have volunteered their time to review and comment onthe manuscripts.
David A. Weber and Amin I. Kassis

Introduction: Radiolabeled antibody tumor dosimetryDonald J. Buchsbauma)
Department of Radiation Oncology, University of Alabama at Birmingham, Birmingham,Alabama 35233-6832
Barry W. WesselsDepartment of Radiology, George Washington University Medical Center, Washington, DC 20037
(Received 18 March 1992; accepted for publication 8 January 1993)
I. INTRODUCTION
Through the sponsorship of the Nuclear Medicine Com-mittee of the American Association of Physicists in Med-icine (AAPM), a Nuclear Medicine Task Group 2, “Do-simetry of Radiolabeled Antibodies” was established inJuly 1987 under the Chairmanship of Dr. Barry Wessels toproduce reports on radiolabeled antibody dosimetry, whichwould include an extensive literature search and an analy-sis of how to approach the dosimetry to normal tissues andtumor of radiolabeled antibody therapy (radioimmuno-therapy). The first report published in 19901 summarized a“Bone Marrow Dosimetry and Toxicity for RadiolabeledAntibodies” symposium held in conjunction with the 1988American Society for Therapeutic Radiology and Oncol-ogy (ASTRO) annual meeting. In 1989, the Steering Com-mittee on the Nuclear Medicine Task Group 2 decided atthe Society of Nuclear Medicine (SNM) Annual Meetingthat the new focus area for the Task Group would be tu-mor dosimetry for radiolabeled antibody therapy. TheTask Group members and invited guests active in radiola-beled antibody research from the physics, radiation biol-ogy, nuclear medicine, and oncology communities hadbeen invited to attend meetings to plan and prepare thisreport on “Radiolabeled Antibody Tumor Dosimetry.”These meetings were held in conjunction with the annualmeetings of the ASTRO, the AAPM, the SNM, the “In-ternational Conference on Monoclonal Antibody Immuno-conjugates for Cancer” and the “Third Conference on Ra-dioimmunodetection and Radioimmunotherapy ofCancer.” The purpose of this report is to provide an exten-sive literature search and review the various approachesthat are being pursued in preclinical and clinical studies toestimate tumor dosimetry associated with radioimmuno-therapy (RIT), and to suggest future directions for dosim-etry research in this field. Included in this report is a dis-cussion of the radiobiological aspects of tumor dosimetryof radiolabeled antibody therapy.
Radiolabeled monoclonal antibodies (MoAbs) offer thepotential of highly localized, targeted radiation treatmentof cancer. The effectiveness of radiation treatment of ma-lignant disease is correlated with the total dose delivered,with increasing dose producing increasing cell kill. Simi-larly, normal tissue damage is also directly related to thetotal dose deposited. The ability to quantify the dose de-livered to tumor and normal tissues when using radiola-beled MoAbs has been a perplexing problem.
As noted in the review of a National Cancer Instituteworkshop,2 techniques for evaluating the dosimetry of ra-
diolabeled antibody therapy are essential to support thedevelopment of RIT in the treatment of neoplastic diseases.Radiation dosimetry is important for treatment planningand the assessment of results. It is necessary to determinethe quantity of radiolabeled antibody to administer to max-imize the radiation dose to the tumor while not exceedingtolerance levels of critical normal tissues, In contrast toexternal beam radiation therapy dosimetry, the tumor do-simetry for radiolabeled antibody therapy is dependent ona number of variables including: ( 1) kinetics of biodistri-bution, tumor uptake and retention of the radiolabeled an-tibody, (2) the uniformity of distribution of the radiola-beled ant ibody wi thin tumor , (3) the radionucl ideattached to the antibody, and (4) the radiobiological re-sponse of tumor cells to continuously decreasing low-dose-rate radiation.
The 12 papers in this special issue of Medical Physicssummarize the problems, various techniques that are beingused to estimate the tumor dosimetry associated with ra-diolabeled antibody therapy, and future directions as high-lighted below.
II. TOPICS DISCUSSED IN THIS REPORT
A. Selection of radionuclides for RIT
The contribution by Mausner and Srivastava3 to thisspecial issue reviews the factors that influence the choice ofa radionuclide for RIT. A potential advantage of some ofthe radionuclides would be a higher tumor/whole-bodydose, resulting in less toxicity to normal tissue, particularlybone marrow. It is essential to carefully consider the choiceof radionuclide in conjunction with the in vivo pharmaco-kinetic (localization and clearance in tumor and normaltissues) properties of the radiolabeled MoAb, the physicalhalf-life of the radionuclide, the chemistry of conjugationto MoAbs, and the toxicity of free radionuclide.
The choice of radionuclide also depends on the micro-distribution of the radiolabeled MoAb relative to the radi-osensitive target sites, involving uniform versus nonuni-form deposition in tumors or localization on cell surfacesversus internalization of radionuclides to the cell cytoplasmor nuclei.
To optimize the efficacy of RIT, it will be necessary todevelop combinations of MoAbs or antibody fragmentsand radionuclides whose pharmacokinetics, physical half-lives and emissions are matched to give the largest possibletumor dose and the least normal tissue toxicity, i.e., thelargest possible therapeutic ratio.
499 Med. Phys. 20 (2), Pt. 2, Mar/Apr 1993 0094-2405/93/020499-04$01.20 © 1993 Am. Assoc. Phys. Med. 499
500 D. J. Buchsbaum and B. W. Wessels: Introduction: Radiolabeled antibody tumor dosimetry 500
B. MIRD formulation
The approach developed by the Medical Internal Radi-ation Dose (MIRD) Committee of the Society of NuclearMedicine for the estimation of average absorbed dose frominternally deposited radionuclides has been applied to ra-diolabeled MoAb therapy in animals and humans, as de-scribed in the paper by Watson et al. 4 in this report. Theclassic MIRD formulation widely used for macroscopicdosimetry problems assumes a uniform distribution of cu-mulated activities of radiolabeled MoAbs within eachsource region and a uniform deposition of energy withineach target region. The experimental animal and clinicalpatient studies clearly demonstrate that radiolabeledMoAbs are not uniformly distributed within solid tumors.There are point-source calculations available within theMIRD pamphlets to deal with the problem of dose heter-ogeneity encountered in RIT.
In addition to the problem of nonuniform uptake ofradiolabeled MoAbs in solid tumors, the macroscopicMIRD approach does not distinguish between a uniformdistribution of radiolabeled MoAb that binds to the cellsurface and a uniform distribution of nonspecific radiola-beled MoAb.
Conventional MIRD type calculations for radiolabeledMoAbs give approximate average dose estimates whichmay not be sufficiently accurate, especially for alpha andAuger emitters. With these types of radionuclides, a mi-crodosimetric approach will be required, as described be-low.
C. Pharmacokinetics modeling
Pharmacokinetics modeling involves an attempt to esti-mate the biokinetics of tumor and normal organ uptake ofradiolabeled MoAbs on both a macroscopic and micro-scopic level, and then to perform the dosimetric calcula-tions. It is an essential component for estimation of cumu-lated activities in the various source regions of the body.Research is still required to find accurate and predictivemodels of both macroscopic and microscopic pharmaco-kinetics. This subject is reviewed by Strand et al. 5
D. Calculation techniques for RIT
Leichner and Kwok6 in this report provide a criticalanalysis of the calculational approaches that have beenused for beta particle tumor dosimetry in RIT. In modelingof absorbed dose distributions, analytical, numerical, andMonte Carlo methods have been used to investigate theeffects of uniform and nonuniform activity distributionsassociated with RIT.
E. Microdosimetry
Alpha emitters and internalized Auger electron emittersmay be useful in RIT because of their high LET and RBE.However, the methodology to calculate dosimetry for shortrange alpha emitters and internalized Auger emitters mustconsider energy deposition at the cellular and subcellularlevel. Such a microdosimetric approach which analyzes the
Medical Physics, Vol. 20, No. 2. Pt. 2, Mar/Apr 1993
effect of source microdistribution on individual cells hasbeen taken by a number of investigators, because of thelimitations of the macroscopic MIRD formulation and thenonuniformity of the radiolabeled antibody in tumor.
Humm et al.7 in this report summarize approaches thatare being used to estimate the microdosimetry of RIT. Itshould be noted, however, that microdosimetry estimatesare based on modeling and are difficult to substantiate ex-perimentally.
F. Autoradiography, thermoluminescent dosimetry,and three-dimensional dose calculations
Radionuclide activity variations within tumors can bemeasured by quantitative autoradiography. However,quantitative autoradiography alone cannot provide totaldose measurements, because of the temporal change in ra-diolabeled antibody uptake, penetration, and clearance.’
Yorke et al.8 note that autoradiography and thermolu-minescent dosimetry are complementary techniques. Au-toradiography shows the activity distribution at a particu-lar point in time, whereas TLDs are integrating dosimetersperforming spatial and temporal integrations within thevolume they occupy, and can be used to calibrate the au-toradiographs.
Griffith et al9 and Roberson et al.10 conver ted datafrom serial autoradiographs to derive three-dimensionalactivity matrices in animal tumor xenografts. Using pointsource function calculation techniques, two-dimensionalisodose curves’ or three-dimensional dose-rate curves 1 0
were generated showing marked dose heterogeneity inmost tumor systems examined. Further studies remain tobe performed to be able to relate the dose-rate distributionsto time averaged dose distributions, cell kill, and eventuallyto therapeutic efficacy.
G. Experimental RIT
Radiolabeled MoAbs have been used for RIT of sphe-roids and a variety of murine syngeneic tumors and humantumor xenografts. The results are summarized in the paperby Buchsbaum et al. in this report.” The approaches takento estimate tumor dosimetry in the experimental animalstudies include the MIRD approach, thermoluminescentdosimetry, autoradiography, and comparison to externalbeam irradiation. The uniform geometry of the spheroidhas facilitated the estimation of radiation dose. The twomost important factors for therapeutic efficacy in thespheroid model are good penetration of the radiolabeledMoAb and an adequate half-life of the radionuclide to ex-ceed the time of penetration. The results in animal studiesindicate that MoAbs radiolabeled with a variety of radio-nuclides have been effective in inhibiting tumor growth orproducing cures against a variety of tumor types. The ma-jority of investigators have estimated the dose to tumorusing the MIRD formalism. A few investigators have esti-mated the dose to tumor using TLDs and autoradiography.The effectiveness of RIT depends on a variety of factorsincluding antibody specificity, affinity and immunoreactiv-ity, tumor vascularity, and differential radiation sensitivity
501 D. J. Buchsbaum and B. W. Wessels: Introduction: Radiolabeled antibody tumor dosimetry 501
of the various tumor types. It must be kept in mind thatthere are limitations of spheroid and animal models inmodeling what occurs in the clinical situation.11,12
H. Imaging techniques and treatment planning
Leichner et al. 13 in another section of this report havereviewed the various imaging techniques that have beenused for RIT treatment planning. They discuss tumor andnormal organ volume computations from CT and MRIdata, correlative image analysis, and treatment planningfor RIT.
I. Clinical studies with dosimetry
There have been a large number of clinical RIT studiesthat have included tumor dosimetry estimates. The ap-proaches that have been taken in lymphoma, solid tumors,and intraperitoneal therapy are described in three manu-scripts in this report.14-16
Radiation dosimetry in B-cell lymphoma patients hasbeen done using the MIRD approach. Organ and tumorradionuclide activity measurements have usually been donewith conjugate view planar scintillation camera imaging.14
Organ and tumor volumes have been obtained by CT,SPECT, or the published values of the MIRD committee.The range of tumor absorbed dose estimates in five clinicallymphoma studies is reported.1 4
For solid tumors, the MIRD approach, planar imagingand tumor volumetrics have been performed in a similarmanner as in lymphoma studies.15 There have been widevariations in estimated tumor doses in different studies,and no definite dose-response relationship has been ob-served. The spatial resolution limits of planar or SPECTimaging devices prevents detection of the nonuniformity ofradiolabeled MoAb deposition, and thus permits only theestimation of average dose to tumor.
Regional administration of radiolabeled MoAbs hasbeen used in the peritoneum, the cerebral spinal fluid, thepleural/pericardial cavity, and within cystic brain tumors.Roeske et al.16 have reviewed the methods and results thathave been used for intraperitoneal dosimetry.
J. Radiobiology of RIT
Langmuir et al.17 elsewhere in this report reviewed theinformation available on the radiobiology of low-dose- rateexternal beam irradiation and RIT as applied to tumordosimetry, and have discussed comparisons between thetwo. Langmuir et al. 17 have concluded that tumors mostlikely to respond to RIT would be those types that areinherently radiosensitive, those with a poor capacity to re-pair radiation damage or with long repair half-times, thosetumors that are susceptible to blockade in sensitive phasesof the cell cycle, and tumors that reoxygenate rapidly.
A comparison of alpha and beta emitters for RIT indi-cates an advantage for beta emitters if the linear-quadraticalpha/beta ratio for tumors is greater than that of the crit-ical organ of toxicity, as is the usual case. However, there
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
is a potential advantage in therapeutic ratio predicted foralpha particle radiation when bone marrow (high linear-quadratic alpha/beta ratio) is considered as the criticalorgan. 17
ACKNOWLEDGMENTS
We thank Donell Berry for typing the manuscript. Sup-ported by NIH Grant CA44173 and the Elaine SnyderCancer Research Award.
“Correspondence should be sent to: Donald J. Buchsbaum, Ph.D., De-partment of Radiation Oncology, University of Alabama at Birming-ham, 619 South 19th Street. Birmingham, AL 35233-6832.
1J. A. Siegel, B. W. Wessels, E. E. Watson, M. G. Stabin. H. M. Vrie-sendorp, E. W. Bradley, C. C. Badger, A. B. Brill, C. S. Kwok, D. R.Stickney, K. F. Eckerman. D. R. Fisher, D. J. Buchsbaum, and S. E.Order, “Bone marrow dosimetry and toxicity for radioimmunother-apy,” Antib. Immunoconj. Radiopharm. 3, 213-233 (1990).
2S. A. Leibel, S. E. Order, D. R. Fisher, J. R. Williams, and R. J.Morton, “Physics and biology of radiolabeled antibodies workshop,sponsored by the Radiation Research Branch, National Cancer Insti-tute, Division of Cancer Treatment, February 12-13, 1987, Bethesda,Maryland,” Antib. Immunoconj. Radiopharm. 1, 271-282 (1988).
‘L. F. Mausner and S. C. Srivastava, “Selection of radionuclides forradioimmunotherapy,” Med. Phys. 20, 503-509 (1993).
4E. E. Watson, M. G. Stabin, and J. A. Siegel, “MIRD formulation,”Med. Phys. 20, 511-514 (1993).
5S.-E. Strand, P. Zanzonico, and T. K. Johnson, “Pharmacokineticmodeling,” Med. Phys. 20, 515-527 (1993).
6P. K. Leichner and C. S. Kwok, “Tumor dosimetry in radioimmuno-therapy: Methods of calculation for beta particles,” Med. Phys. 20,529-534 (1993).
7J. L. Humm, J. C. Roeske, D. R. Fisher, and G. T. Y. Chen, “Micro-dosimetric concepts in radioimmunotherapy,” Med. Phys. 20, 535-541(1993).
8E. D. Yorke, L. E. Williams, A. J. Demidecki, D. B. Heidorn, P. L.Roberson, and B. W. Wessels, “Multicellular dosimetry for beta-emitting radionuclides: Autoradiography, thermoluminescent dosime-try and three-dimensional dose calculations,” Med. Phys. 20, 543-550(1993).
9M. H. Griffith, E. D. Yorke, B. W. Wessels, G. L. DeNardo, and W. P.Neacy, “Direct dose confirmation of quantitative autoradiography withmicro-TLD measurements for radioimmunotherapy,” J. Nucl. Med.29, 1795-1809 (1988).
1 0P. L. Roberson, D. J. Buchsbaum, D. B. Heidom, and R. K. TenHaken, “Three-dimensional tumor dosimetry for radioimmunotherapyusing serial autoradiography,” Int. J. Radiat. Oncol. Biol. Phys. 24,329-334 (1992).
11D. J. Buchsbaum, V. K. Langmuir, and B. W. Wessels, “Experimentalradioimmunotherapy,” Med. Phys. 20, 551-567 ( 1993).
12B. W. Wessels, “Current status of animal radioimmunotherapy,” Can-cer Res. (Suppl.) 50, 970s-973s (1990).
1 3P. K. Leichner, K. F. Koral, R. J. Jaszczak, A. J. Green, G. T. Y.Chen, and J. C. Roeske, “An overview of imaging techniques andphysical aspects of treatment planning in radioimmunotherapy,” Med.Phys. 20, 569-577 (1993).
14J. A. Siegel, D. M. Goldenberg, and C. C. Badger, “Radioimmuno-therapy dose estimation in patients with B-cell lymphoma,” Med. Phys.20, 579-582 (1993).
15R. F. Meredith, T. K. Johnson, G. Plott, D. J. Macey, R. L. Vessella,L. A. Wilson, H. B. Breitz, and L. E. Williams, “Dosimetry of solidtumors,” Med. Phys. 20, 583-592 (1993).
16J. C. Roeske, G. T. Y. Chen, M. Reese, and A. B. Brill, “Dosimetry ofintraperitoncally administered radiolabeled antibodies,” Med. Phys. 20,593-600 (1993).
1 7V. K. Langmuir, J. F. Fowler, S. J. Knox, B. W. Wessels, R. M.Sutherland, and J. Y. C. Wong, “Radiobiology and radiolabeled anti-body therapy as applied to tumor dosimetry,” Med. Phys. 20, 601-610(1993).

Selection of radionuclides for radioimmunotherapyLeonard F. Mausner and Suresh C. SrivastavaMedical Department, Brookhaven National Laboratory, Upton. New York I I973
(Received 18 March 1992; accepted 6 October 1992)
I. INTRODUCTION
The potential of utilizing monoclonal antibodies (MoAb)as carriers of radionuclides for the selective destruction oftumors (radioimmunotherapy, RIT) has stimulated muchresearch activity. The approach should be specially bene-ficial for treatment of tumors not easily amenable to sur-gical control, for treatment of early recurrence and of dis-tant metastases. However, from dosimetric and otherconsiderations, the choice of radiolabel is an importantfactor that needs to be optimized for maximum effective-ness of RIT. Most therapeutic trials to date have utilized131I, largely due to its ready availability at moderate cost,the ease of halogenation techniques for proteins, and itslong history of use in treating thyroid malignancy, ratherthan any careful analysis of its suitability for RIT. Thispaper briefly reviews the present and future radionuclidesthat are considered particularly suitable for RIT.
II. SELECTION CRITERIA
The selection criteria must be based on the physical dataabout the radionuclide, its production and chemistry andthe biological variables governing its use. The importantphysical variables to consider include the radionuclidehalf-life, the type, energy, and branching ratio of particu-late radiation and the gamma-ray energies and abun-dances. It is important to match the physical half-life withthe antibody in vivo pharmacokinetics. If the half-life is tooshort, most decay will have occurred before the MoAb hasreached maximum tumor/background ratio.
Conversely, considerations of tumor radiobiology andlow radionuclide/antibody specific activity may also limitthe use of long-lived radionuclides. For equal radioactivityconcentrations in the target, radionuclides with long halflives will produce a lower absorbed dose rate than thosewith short lifetimes. If the maximum absorbed dose ratefrom beta particles is much lower than that typical inbrachytherapy (40-64 cGy/h) , ce l l k i l l per cGy isdecreased.1,2 The theoretical low specific activity of longerlived radionuclides would thus require a large mass of ra-dionuclide, ligand, and antibody to achieve adequate doserate. This can make the use of long-lived radiolabels lessdesirable. However, if a two or three-stage therapy ap-proach is utilized,3 it becomes useful to consider the use oflong-lived beta emitters, e.g., 3 2P and others. To some ex-tent the problem of low target dose rate may be counter-acted by a number of factors including high nonpenetrat-ing equilibrium dose constant, high target to nontargetratio, high carrier labeling efficiency, and the ability toadminister a large protein mass (tumor saturation effect).
The type of particulate emission also must be consid-ered. The potent lethality of Auger and low-energy conver-
sion electrons has been demonstrated.4-8 This effect canbest be realized with intranuclear localization of the radi-onuclide, which does not generally occur with radiolabeledMoAb. Of course, a particles have a high linear energytransfer (LET) effective in cell killing and a range of sev-eral cell diameters, 40-80 µm. The short ranges will accen-tuate inhomogeneous absorbed dose particularly when theMoAb deposition is inhomogeneous. Beta particles are lessdensely ionizing and have a range longer than a’s so thatthe distribution requirements are less restrictive for RIT ofbulky disease. On the other hand, for micrometastases, theabsorbed fraction for higher energy beta particles (range> tumor size) is decreased, leading to a less favorable tu-mor absorbed dose. The gamma-ray energies and abun-dances are also important physical properties, because thepresence of gamma rays offers the possibility of externalimaging but also adds to the whole body dose. These phys-ical properties alone can be used to calculate radiation ab-sorbed dose at the cellular level. This approach has beenused by Jungerman et al.9 to estimate delivered doses forRIT. An approach which explicitly includes biodistribu-tion and kinetic data by using an idealized time-dependentaveraged target-to-nontarget uptake ratio is that of Wesselsand Rogus.1 0 Although the quantitative dose ratios arehighly dependent on the input biodistribution data, a com-parison of the relative effectiveness of the radiolabels wasdemonstrated. This relative efficacy was approximatelyconstant for reasonable variation of model parameters inaccordance with observed biological data. A similar ap-proach was used recently by Yorke et al. 11 Also, Humm1 2
has considered the effect on MoAb dosimetry of varyingtumor size and of cold regions. These papers underscorethe importance for therapy of a high ratio of nonpenetrat-ing to penetrating (γ) radiations. The complex relation-ship between tumor curability with different radionuclidesand tumor size has been reviewed by Wheldon andO’Donoghue.13
The main chemical variables to be considered in choos-ing a radionuclide for therapy with monoclonal antibodiesare the radionuclide specific activity achievable, metal-ioncontamination, the number of labels per MoAb moleculeobtainable without loss of immunological activity, and thestability of the radionuclide-protein attachment. The spe-cific activity, or amount of activity per mass of the elementin question (MBq/mg), depends primarily on the methodof production. Simple neutron absorption reactions (e.g.,n ,γ) generally give low specific activity since the radionu-clide cannot be chemically separated from a target of thesame element. Accelerator-based proton, deuteron, oralpha-induced reactions are intrinsically no-carrier-added(NCA) methods that do allow chemical separation of
503 Med. Phys. 20 (2). Pt. 2, Mar/Apr 1993 0094-2405/93/020503-08$01.20 © 1993 Am. Assoc. Phys. Med. 503
504 L F. Mausner and S. C. Srivastava: Radionuclides for radioimmunotherapy 504
product from the target. This can also be achieved at re-actors by neutron absorption reactions leading to an inter-mediate product with a beta decay to the desired finalproduct, or by fast neutron reactions such as (n,p). Theachievable specific activity of these NCA methods thenlargely depends on the impurity levels of the product ele-ment in the target or in various reagents used in processing.An often overlooked source of carrier is due to the directproduction of stable isotopes of the product element. Al-though this effect is often negligible compared to carrierintroduced with the target, it can become significant withvery pure targets and high bombarding energies. With in-creasing energy, the typical peaks in nuclear excitationfunctions broaden, usually reaching a plateau at approxi-mately 150-200 MeV and reaction cross sections for neigh-boring isotopes become comparable over large energyranges. Some of these issues have been reviewed recentlyfor therapeutic radionuclides.1 4
The presence of metal ions other than the product is aconcern as they can compete for binding sites on chelate-MoAb conjugates. It is largely controlled by the selectivityof the chemical separation scheme, but this process is notperfect. For example, a normally adequate separation fac-tor of 10-7 on a 10 g target still leaves 1 µg of target in theproduct which may be of concern when labeling at lowprotein concentrations. Indeed, measurement of these sta-ble species at low concentration in radioactive solutions isoften a very difficult practical problem. Although variousanalytical procedures exist for detecting ions at subpart permillion levels, for example atomic absorption, emissionspectroscopy, and x-ray fluorescence, these techniques of-ten take time, utilize expensive instrumentation, and mayrequire a large fraction of the final product solution for themeasurement. Generally, the sooner the radionuclide isused the better, because its specific activity is highest, andthis need competes with the desire to measure the specificactivity and the impurity levels. Also, it is typical for manyresearch groups that the expensive analytical apparatus isnot wholly owned. Instead, access is through a shared-usefacility whose operators are very reluctant to introduceradioactive material into their equipment. Thus the fastest,albeit indirect method, of determining carrier levels maysimply be by titration with chelate during labeling.
The convenience, efficiency, and gentleness of variousradiolabeling procedures as well as the stability of the ra-dionuclide attachment to the antibody are all very impor-tant factors which are being actively investigated by manygroups. They will not be considered further here as thesetopics are beyond the scope of this paper and have beenreviewed several times.15-18 While recognizing the difficul-ties in designing new conjugation schemes, at this point, itis simply assumed that adequate radiolabeling techniqueseither exist or will become available for use with radionu-clides to be discussed.18 However, another practical aspectto be considered is that of radionuclide production-theroutine availability, at reasonable cost, of quantities of ra-dioactivity suitable for therapy. At present, only 131I trulymeets all of these production criteria. However, this situ-
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
ation is changing for several other attractive radionuclidesto be discussed below.
These physical and chemical factors must then beviewed in light of available biological information. There issubstantial variation in antibody uptake, macro- andmicro-distribution, kinetics and processing (metabolism/catabolism) depending on the particular antibody, anti-body dose, the variability of antigenic expression in thetumor, its size and stage, etc. Limitations due to normaltissue radiotoxicity are not entirely the function of radio-nuclide emissions but are largely governed by the pharma-cokinetics of the antibody. For many of the MoAbs andMoAb fragments currently being investigated for immuno-therapy some generalities emerge. It is generally believedthat one-half to three days is usually required to reachmaximum tumor uptake19-22 although optimum contrastwith whole MoAbs may take longer. Despite the presenceof numerous antigen sites on cancer cells, evidence fromtumor implanted microthermoluminescent dosimeterprobes2 3 , 2 4 and autoradiography2 5 indicates a nonuniformcellular distribution of the MoAb in most cases. This maybe due to cell type heterogeneity, 26 heterogeneity of anti-genic expression,27 poor delivery, and spatial inaccessibil-ity. These factors considerably reduce the attractiveness ofshort-ranged alpha-emitting radionuclides for radioimmu-notherapy. A role for alpha emitters may be feasible inspecific cases such as for micrometastases or intracavitaryadministration for some types of cancers, such as perito-neal injection for ovarian carcinoma.28,29 The longer rangeof beta particles can still permit uniform tumor irradiationdespite a marked heterogeneity of distribution of radioac-tivity within the tumor. It appears desirable to deliver ion-izing radiation with a range of one to several millimeters intissue, as from intermediate to high-energy beta particles.
Ill. CANDIDATE RADIONUCLIDES
Relatively few alpha emitting radionuclides have beenconsidered for RIT. Bismuth-212 (t1/2= 60.5 min, E α = 7.8MeV) and 2 1 1At ( t1/2 = 7.2 h, E α = 6.8 MeV) are the twonuclides that have been most studied.30-36 The 212Bi can beavailable via a 2 2 4Ra generator system,37 while 2 1 1At is ac-celerator produced.38,39 The short half-life of 2 1 2Bi is notwell matched to MoAb uptake kinetics but it might bepossible to conjugate its parent 212Pb, with a 10.6 h half-life, to a MoAb or MoAb fragment and thus generate thealpha emitter in vivo. The feasibility of this approach isunder investigation.4 0 Nevertheless, the peak of 2 1 2B igrowth occurs at 3.8 h which is probably still too short forthe peak in tumor uptake. The short life time of 211At andlimited availability may impede its use except in very spe-cial situations.4 1
It has been suggested28 that the 20.1 h half-life of 255F mis more appropriate for RIT. Unfortunately this nuclideand similar alpha emitting heavy radionuclides (atomicnumber > 82) are the parents or members of long decaychains involving both alpha and beta emission. Because thenuclear recoil from the alpha (and some of the beta) de-cays are considerably more energetic than chemical bondstrengths, these transitions are capable of rupturing the
505 L. F. Mausner and S. C. Srivastava: Radionuclides for radioimmunotherapy 505
radionuclide-ligand bond. Unless the daughter half-life isless than a few minutes it will be free to diffuse away fromthe tumor. Worse still, most of these heavy elements tendto irreversibly lodge in bone.
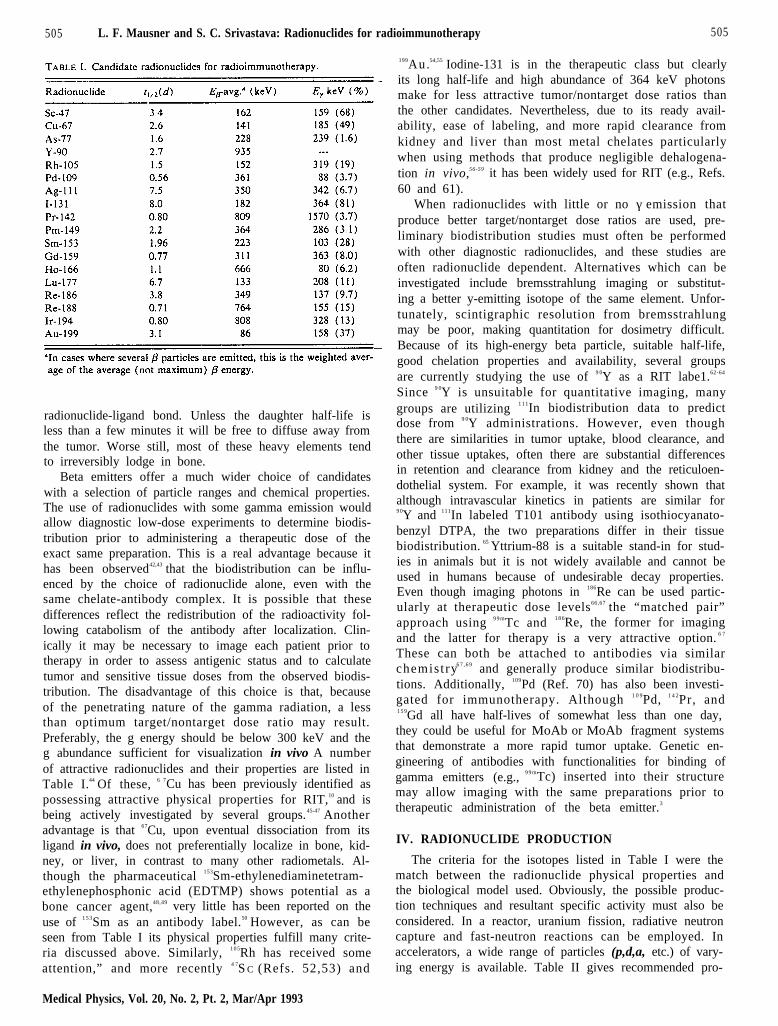
Beta emitters offer a much wider choice of candidateswith a selection of particle ranges and chemical properties.The use of radionuclides with some gamma emission wouldallow diagnostic low-dose experiments to determine biodis-tribution prior to administering a therapeutic dose of theexact same preparation. This is a real advantage because ithas been observed42,43 that the biodistribution can be influ-enced by the choice of radionuclide alone, even with thesame chelate-antibody complex. It is possible that thesedifferences reflect the redistribution of the radioactivity fol-lowing catabolism of the antibody after localization. Clin-ically it may be necessary to image each patient prior totherapy in order to assess antigenic status and to calculatetumor and sensitive tissue doses from the observed biodis-tribution. The disadvantage of this choice is that, becauseof the penetrating nature of the gamma radiation, a lessthan optimum target/nontarget dose ratio may result.Preferably, the g energy should be below 300 keV and theg abundance sufficient for visualization in vivo A numberof attractive radionuclides and their properties are listed inTable I.44 Of these, 6 7Cu has been previously identified aspossessing attractive physical properties for RIT,10 and isbeing actively investigated by several groups.45-47 Anotheradvantage is that 67Cu, upon eventual dissociation from itsligand in vivo, does not preferentially localize in bone, kid-ney, or liver, in contrast to many other radiometals. Al-though the pharmaceutical 153Sm-ethylenediaminetetram-ethylenephosphonic acid (EDTMP) shows potential as abone cancer agent,48,49 very little has been reported on theuse of 1 5 3Sm as an antibody label.50 However, as can beseen from Table I its physical properties fulfill many crite-ria discussed above. Similarly, 1 0 5Rh has received someattention,” and more recently 4 7S C (Refs. 52,53) and
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
199Au.54,55 Iodine-131 is in the therapeutic class but clearlyits long half-life and high abundance of 364 keV photonsmake for less attractive tumor/nontarget dose ratios thanthe other candidates. Nevertheless, due to its ready avail-ability, ease of labeling, and more rapid clearance fromkidney and liver than most metal chelates particularlywhen using methods that produce negligible dehalogena-tion in vivo,56-59 it has been widely used for RIT (e.g., Refs.60 and 61).
When radionuclides with little or no γ emission thatproduce better target/nontarget dose ratios are used, pre-liminary biodistribution studies must often be performedwith other diagnostic radionuclides, and these studies areoften radionuclide dependent. Alternatives which can beinvestigated include bremsstrahlung imaging or substitut-ing a better y-emitting isotope of the same element. Unfor-tunately, scintigraphic resolution from bremsstrahlungmay be poor, making quantitation for dosimetry difficult.Because of its high-energy beta particle, suitable half-life,good chelation properties and availability, several groupsare currently studying the use of 9 0Y as a RIT labe1.62-64
Since 9 0Y is unsuitable for quantitative imaging, manygroups are utilizing 1 1 1In biodistribution data to predictdose from 9 0Y administrations. However, even thoughthere are similarities in tumor uptake, blood clearance, andother tissue uptakes, often there are substantial differencesin retention and clearance from kidney and the reticuloen-dothelial system. For example, it was recently shown thatalthough intravascular kinetics in patients are similar for9 0Y and 111In labeled T101 antibody using isothiocyanato-benzyl DTPA, the two preparations differ in their tissuebiodistribution. 65 Yttrium-88 is a suitable stand-in for stud-ies in animals but it is not widely available and cannot beused in humans because of undesirable decay properties.Even though imaging photons in 186Re can be used partic-ularly at therapeutic dose levels66,67 the “matched pair”approach using 9 9 mTc and 1 8 6Re, the former for imagingand the latter for therapy is a very attractive option. 6 7
These can both be attached to antibodies via similarchemis t ry6 7 , 6 9 and generally produce similar biodistribu-tions. Additionally, 109Pd (Ref. 70) has also been investi-gated for immunotherapy. Although 1 0 9Pd, 1 4 2Pr, and1 5 9Gd all have half-lives of somewhat less than one day,they could be useful for MoAb or MoAb fragment systemsthat demonstrate a more rapid tumor uptake. Genetic en-gineering of antibodies with functionalities for binding ofgamma emitters (e.g., 9 9 mTc) inserted into their structuremay allow imaging with the same preparations prior totherapeutic administration of the beta emitter.3
IV. RADIONUCLIDE PRODUCTION
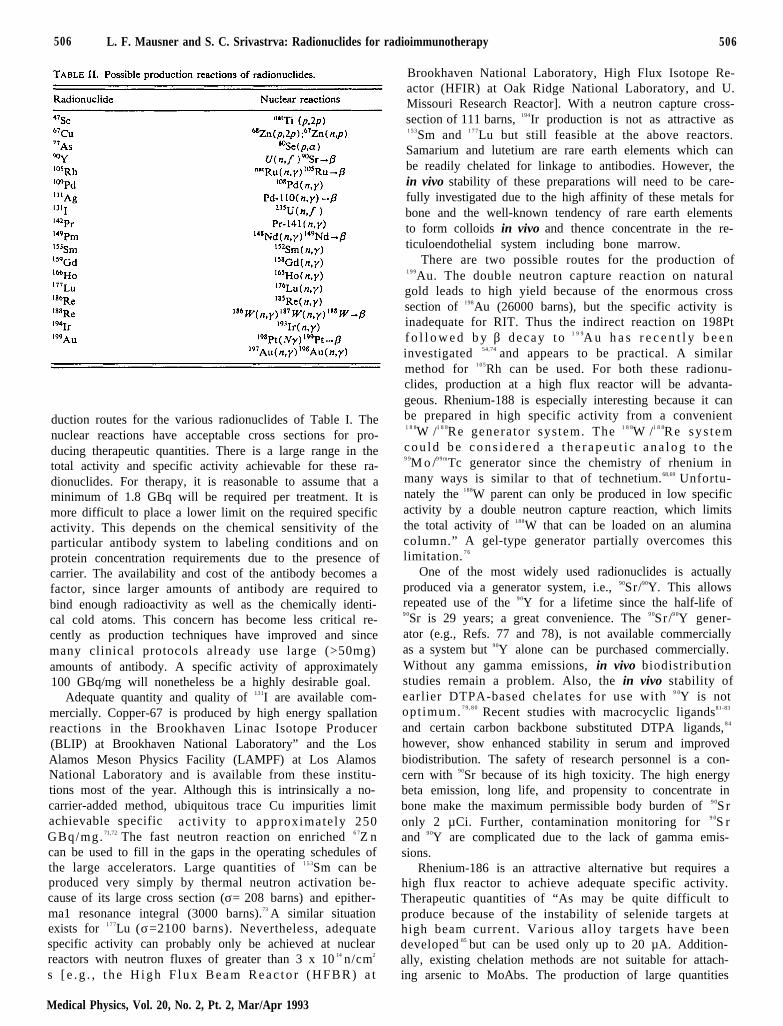
The criteria for the isotopes listed in Table I were thematch between the radionuclide physical properties andthe biological model used. Obviously, the possible produc-tion techniques and resultant specific activity must also beconsidered. In a reactor, uranium fission, radiative neutroncapture and fast-neutron reactions can be employed. Inaccelerators, a wide range of particles (p,d,a, etc.) of vary-ing energy is available. Table II gives recommended pro-
506 L. F. Mausner and S. C. Srivastrva: Radionuclides for radioimmunotherapy 506
duction routes for the various radionuclides of Table I. Thenuclear reactions have acceptable cross sections for pro-ducing therapeutic quantities. There is a large range in thetotal activity and specific activity achievable for these ra-dionuclides. For therapy, it is reasonable to assume that aminimum of 1.8 GBq will be required per treatment. It ismore difficult to place a lower limit on the required specificactivity. This depends on the chemical sensitivity of theparticular antibody system to labeling conditions and onprotein concentration requirements due to the presence ofcarrier. The availability and cost of the antibody becomes afactor, since larger amounts of antibody are required tobind enough radioactivity as well as the chemically identi-cal cold atoms. This concern has become less critical re-cently as production techniques have improved and sincemany clinical protocols already use large (>50mg)amounts of antibody. A specific activity of approximately100 GBq/mg will nonetheless be a highly desirable goal.
Adequate quantity and quality of 131I are available com-mercially. Copper-67 is produced by high energy spallationreactions in the Brookhaven Linac Isotope Producer(BLIP) at Brookhaven National Laboratory” and the LosAlamos Meson Physics Facility (LAMPF) at Los AlamosNational Laboratory and is available from these institu-tions most of the year. Although this is intrinsically a no-carrier-added method, ubiquitous trace Cu impurities limitachievable specific act iv i ty to approximately 250GBq/mg. 71,72 The fast neutron reaction on enriched 6 7Z ncan be used to fill in the gaps in the operating schedules ofthe large accelerators. Large quantities of 1 5 3Sm can beproduced very simply by thermal neutron activation be-cause of its large cross section (σ= 208 barns) and epither-ma1 resonance integral (3000 barns).73 A similar situationexists for 1 7 7Lu (σ=2100 barns). Nevertheless, adequatespecific activity can probably only be achieved at nuclearreactors with neutron fluxes of greater than 3 x 10 14 n/cm2
s [ e . g . , t h e H i g h F l u x B e a m R e a c t o r ( H F B R ) a t
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
Brookhaven National Laboratory, High Flux Isotope Re-actor (HFIR) at Oak Ridge National Laboratory, and U.Missouri Research Reactor]. With a neutron capture cross-section of 111 barns, 194Ir production is not as attractive as1 5 3Sm and 1 7 7Lu but still feasible at the above reactors.Samarium and lutetium are rare earth elements which canbe readily chelated for linkage to antibodies. However, thein vivo stability of these preparations will need to be care-fully investigated due to the high affinity of these metals forbone and the well-known tendency of rare earth elementsto form colloids in vivo and thence concentrate in the re-ticuloendothelial system including bone marrow.
There are two possible routes for the production of1 9 9Au. The double neutron capture reaction on naturalgold leads to high yield because of the enormous crosssection of 198Au (26000 barns), but the specific activity isinadequate for RIT. Thus the indirect reaction on 198Ptf o l l o w e d b y β decay to 1 9 9A u h a s r e c e n t l y b e e ninvestigated 54,74 and appears to be practical. A similarmethod for 1 0 5Rh can be used. For both these radionu-clides, production at a high flux reactor will be advanta-geous. Rhenium-188 is especially interesting because it canbe prepared in high specific activity from a convenient1 8 8W /1 8 8Re generator sys tem. The 1 8 8W /1 8 8Re sys t emc o u l d b e c o n s i d e r e d a t h e r a p e u t i c a n a l o g t o t h e9 9M o /9 9 mTc generator since the chemistry of rhenium inmany ways is similar to that of technetium.68,69 Unfortu-nately the 188W parent can only be produced in low specificactivity by a double neutron capture reaction, which limitsthe total activity of 188W that can be loaded on an aluminacolumn.” A gel-type generator partially overcomes thislimitation. 7 6
One of the most widely used radionuclides is actuallyproduced via a generator system, i.e., 90Sr/90Y. This allowsrepeated use of the 9 0Y for a lifetime since the half-life of9 0Sr is 29 years; a great convenience. The 9 0Sr/9 0Y gener-ator (e.g., Refs. 77 and 78), is not available commerciallyas a system but 90Y alone can be purchased commercially.Without any gamma emissions, in vivo biodistributionstudies remain a problem. Also, the in vivo stability ofearlier DTPA-based chelates for use with 9 0Y is notopt imum. 7 9 , 8 0 Recent studies with macrocyclic ligands81-83
and certain carbon backbone substituted DTPA ligands, 8 4
however, show enhanced stability in serum and improvedbiodistribution. The safety of research personnel is a con-cern with 90Sr because of its high toxicity. The high energybeta emission, long life, and propensity to concentrate inbone make the maximum permissible body burden of 9 0Sronly 2 µCi. Further, contamination monitoring for 9 0S rand 9 0Y are complicated due to the lack of gamma emis-sions.
Rhenium-186 is an attractive alternative but requires ahigh flux reactor to achieve adequate specific activity.Therapeutic quantities of “As may be quite difficult toproduce because of the instability of selenide targets athigh beam current. Various alloy targets have beendeveloped 85 but can be used only up to 20 µA. Addition-ally, existing chelation methods are not suitable for attach-ing arsenic to MoAbs. The production of large quantities
507 L F. Mausner and S. C. Srivastava: Radionuclides for radioimmunotherapy 507
o f 1 0 9Pd is straightforward, but with a specific activity atthe lower end of this compilation. Since this may not be aserious problem in the future, its ease of production andfavorable labeling chemistry” make it a possible candidatefor RIT.
The remaining entries in Table II are rare earth ele-ments and would be expected to have chemical behaviorsimilar to 153Sm. There are two possible reactions to make142Pr, offering either high yield or high specific activity, asituation analogous to 199Au. Promethium-149, 166Ho, and159Gd could be produced in adequate yield and high spe-cific activity and so are also reasonable candidates.
ACKNOWLEDGMENTS
We would like to acknowledge the valuable discussionsand critical review contributed by E. D. Yorke and B. W.Wessels. The comments of D. J. Buchsbaum, K. E. Brit-ton, J. Humm, and W. A. Volkert were also helpful in thepreparation of this manuscript. This work was supportedby the Office of Health and Environmental Research, U.S.Department of Energy, under Contract No. DE-AC02-76CH00016. Thanks are due to Ms. S. Cataldo for helpwith the preparation of this manuscript.
1J. F. Fowler, “Radiobiological aspects of low dose rates in radioimmu-notherapy,” Int. J. Radiat. Oncol. Biol. Phys. 18, 1261-1269 (1991).
2R. G. Dale, “The application of the linearquadratic dose-effect equa-tion to fractionated and protracted radiotherapy,” Br. J. Radiol. 58,515-528 (1985).
3K. E. Britton, S. J. Mather, and M. Granowska, “Radiolabelled mon-oclonal antibodies in oncology III. Radioimmunotherapy,” Nucl. Med.Commun. 12, 333-347 ( 1991).
4E. W. Bradley, P. C. Chan, and S. J. Adelstein, “The radiotoxicity ofI-125 in mammalian cells. I. Effects on the survival curve of radioiodineincorporated into DNA,” Radiat. Res. 64, 555-563 (1975).
5P. C. Chan, E. Lisco, H. Lisco, and S. J. Adelstein, “The radiotoxicityof I-125 in mammalian cells. II. A comparative study on cell survivaland cytotoxic responses to IUdR-125, IUdR-132, and HTdR-3,” Ra-diat. Res. 67, 332-343 (1976).
6A. I. Kassis, S. J. Adelstein, C. Haycock, K. S. R. Sastry, K. D.McElvany, and M. J. Welch, “Lethality of Auger electrons from thedecay of Br-77 in the DNA of mammalian cells,” Radiat. Res. 90,362-373 (1982).
7S. J. Adelstein and A. I. Kassis, “Radiobiologic implications of themicroscopic distribution of energy from radionuclides,” Nucl. Med.Biol. 14, 165-169 (1987).
8L. E. Feinendegen, “Biological damage from the Auger effect: Possiblebenefits,” Radiat. Environ. Biophys. 12, 85-99 (1975).
9J. A. Jungerman, P. Yu Kin-Hung, and C. I. Zanelli, “Radiation ab-sorbed dose estimates at the cellular level for some electron emittingradionuclides for radioimmunotherapy,” Int. J. Appl. Radiat. Isot. 35,883-888 (1984).
10B. W. Wessels and R. D. Rogus, “Radionuclide selection and modelabsorbed dose calculations for radiolabeled tumor-associated antibod-ies,” Med. Phys. 11, 638-645 (1984).
11E. D. Yorke, P. L. Beaumier, B. W. Wessels, A. R. Fritzberg, and A.C. Morgan, Jr., “Optimal antibody-radionuclide combinations for clin-ical radioimmunotherapy: A predictive model based on mouse phar-macokinetics,” Nucl. Med. Biol. 18, 827-835 ( 1991).
12J. L. Humm, “Dosimetric aspects of radiolabeled antibodies for tumortherapy,” J. Nucl. Med. 27, 1490-1497 (1986).
13T. E. Wheldon and J. A. O'Donoghue, “The radiobiology of targetedradiotherapy,” Int. J. Radiat. Biol. 58, 1-21 (1990).
14W. A. Volkert, W. F. Goeckeler, G. J. Ehrhardt, and A. R. Ketring,“Therapeutic radionuclides: Production and decay property consider-ations,” J. Nucl. Med. 32, 174-185 (1991).
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
“A. R. Fritzberg, R. W. Berninger, S. W. Hadley. and D. W. Webster,“Approaches to radiolabeling of antibodies for diagnosis and therapy ofcancer," Pharm. Res. 5, 325 (1988).
16D. I. Hnatowich, “Antibody radiolabeling, problems and promises,”Nucl. Med. Biol. 17, 49-55 (1990).
17O. A. Gansow, “Newer approaches to the radiolabeling of monoclonalantibodies by use of metal chelates,” Nucl. Med. Biol. 18, 369-381(1991).
18S. C. Srivastava and R. C. Mease, “Progress in research on ligands,nuclides and techniques for labeling monoclonal antibodies,” Nucl.Med. Biol. 18, 589-603 (1991).
19S.J. DeNardo, K. Erickson, E. Benjamini, H. Hines, R. Scibienski, andG, DeNardo, “Monoclonal antibodies for radiation therapy of mela-noma,” in Nuclear Medicine and Biology, edited by C. Raynaud (Per-gamon, Paris, 1982), p. 182.
20S. Larson. J. Carrasquillo, J. Reynolds, A. Keenan, P. Sugarbaker, D.Colcher, J. Schlom, R. Neumann, I. Hellstrom, K. Hellstrom, J.Mulshine, M. Lotz, and P. Strudler, “The National Institutes of Healthexperience with radiolabeled monoclonal antibodies: Lymphoma, mel-anoma and colon cancer,” in Radiolabeled Monoclonal Antibodies forImaging and Therapy, edited by S. C. Srivastava Vol. 152 (Plenum,New York, 1988). pp. 393-407.
21G. DeNardo, S. J. DeNardo, and D. J. Macey, “Quantitative pharma-cokinetics of radiolabeled monoclonal antibodies for imaging and ther-apy in patients,” in Radiolabeled Monoclonal Antibodies for Imagingand Therapy, edited by S. C. Srivastava (Plenum, New York, 1988),pp. 293-3 10.
22D. A. Scheinberg and M. A. Strand, “Kinetic and catabolic consider-ations of monoclonal antibody targeting in erythroleukemia mice,”Cancer Res. 43, 265-272 (1983).
23B.W. Wessels, M. H. Griffith, E. W. Bradley, and B. Skibinski, “Do-simetric measurements and radiobiological consequences of radioim-munotherapy in tumor bearing mice,” in Fourth International Radiop-harmaceutical Dosimetry Symposium, edited by A. T. Schlafek-Stelsonand E. E. Watson (Oak Ridge Associated Universities, Oak Ridge,1985), pp. 446-457.
24M. H. Griffith, E. D. Yorke, B. W. Wessels, G. L. DeNardo, and W. P.Neacy. “Direct dose confirmation of quantitative autoradiography withmicro-TLD measurements for radioimmunotherapy,” J. Nucl. Med.29, 1795-1809 (1988).
25F. Buchegger, A. Vacca, S. Carrel, M. Schreyer, and J. P. Mach, “Ra-dioimmunotherapy of human colon carcinoma by 131I-labeled mono-clonal anti-CEA antibodies in a nude mouse model,” Int. J. Cancer 41,127-134 (1988).
26N.Buick, R. Pullam, J. B. Bizzari, and W. J. Mackillop, “Thephenotypic heterogeneity of human ovarian tumor cells in relation tocell function,” in Radioimmunoimaging and Radioimmunotherapy, ed-ited by S. W. Burchiel and B. A. Rhodes (Elsevier, New York, 1983),pp. 3-10.
27J.W. Fabre and A. S. Daar, “Expression of normal epithelial mem-brane antigens on human colorectal and breast carcinomas,” in Radio-immunoimaging and Radioimmunotherapy, edited by S. W. Burchieland B. A. Rhodes (Elsevier, New York, 1983), pp. 143-157.
28R. E. Bigler and P. B. Zanzonico, “Adjuvant radioimmunotherapy formicrometases,” in Radiolabeled MonoclonaI Antibodies for Imagingand Therapy, edited by S. C. Srivastava (Plenum, New York, 1988),pp. 409-428.
29D. S. Wilbur, “Potential use of alpha emitting radionuclides in thetreatment of cancer,” Antib. Immunoconj. Radiopharm. 4, 85-97(1990).
30C. L. Ruegg, W. T. Anderson-Berg, M. Brechbiel, S. Mirzadeh, O. A.Gansow, and M. Strand, “Improved in-vivo stability and targeting ofbismuth labeled antibody,” Cancer Res. 50, 4221-4226 (1990).
3 1R. W. Kozak, R. W. Atcher, O. A. Gansow, A. M. Friedman, J. J.Hines, and T. A. Waldman, “Bismuth-212 labeled anti-TAC mono-clonal antibody: a particle emitting radionuclides as modalities forradioimmunotherapy,” Proc. Natl. Acad. Sci. 83, 474-478 (1986).
32R. M. Macklis, W. D. Kaplan, J. L. M. Ferrara, R. W. Atcher, J. J.Hines, S. J. Burakoff, and N. C. Coleman, “Alpha particle radioimmu-notherapy: animal models and clinical prospects,” Int. J. Radiat. On-col. Biol. Phys. 16, 1377a-1387a (1989).
“A. Harrison and L. Royle, “Preparation of a 211At-IgG conjugatewhich is stable in-vivo,” Int. J. Appl. Radiat. Isot. 35, 1005-1008(1984).
“A. T. M. Vaughan, W. J. Bateman, and D. R. Fisher, “The in-vivo fate
508 L. F. Mausner and S. C. Srivastava: Radionuclides for radioimmunotherapy 508
of At labeled monoclonal antibody with known specificity in a murinesystem,” Int. J. Radiat. Oncol. Biol. Phys. 8. 1943-1946 (1982).
35D. S. Wilbur, M. D. Hylarides, and A. R. Fritzberg, “Reactions oforganometallic compounds with astatine-211 and applications to pro-tein labeling,” Radiochemica Acta 47, 137-142 (1989).
36I. Brown, “Astatine radiopharmaceuticals. Astatine-211: its possibleapplications in cancer therapy,” Int. J. Appl. Radiat. Isot. 37, 789-798(1986).
37R. W. Atcher, A. M. Friedman, and J. J. Hines, “An improved gen-erator for the production of 212Pb and 212Bi from 224Ra,” Int. J. Appl.Radiat. Isot. 39, 283-286 (1988).
38R. M. Lambrecht, and S. Mirzadeh, “Cyclotron isotopes andradiopharmaceuticals-XXXV Astatine-211I,” Int. J. Appl. Radiat.Isot. 36, 443-450 (1985).
39R. D. Neirinckx and J. A. Smit, “Separation of Astatine-211 frombismuth metal,” Anal. Chim. Acta. 63, 201-204 ( 1973).
40C. Wu, S. Mirzadeh, A. Raubitschek, K. Kumar, D. Parker, and O.Gansow, “The chemical fate of 212Bi-chelates formed by β decay of212Pb-chelates in solution and localized in cells by linkage to internal-izing monoclonal antibodies,” American Chemical Society NationalMeeting, 23-28 August 1992 (abstract).
41M. R. Zalutsky, P. K. Garg, H. S. Friedman, and D. D. Bigner, “La-beling monoclonal antibodies and F(ab’)2 with the a-particle-emittingnuclide astatine-211: Preservation of immunoreactivity and in-vivo lo-calizing capacity,” Proc. Natl. Acad. Sci. USA 86, 7149-7153 (1989).
42D. J. Hnatowich, F. Virzi, and P. W. Doherty, “DTPA-coupled anti-bodies labeled with Y-90,” J. Nucl. Med. 26, 503-509 (1985).
43S. C. Srivastava and G. E. Meinken, “Correlating labeling chemistryand in vitro test results with the biological behavior of radiolabeledproteins,” Int. J. Biol. Markers 1, 111 l-120 ( 1986).
“D. C. Kocher, “Radioactive decay data tables,” DOE/TIC-11026(1981).
4 5S. Mirzadeh, L. F. Mausner, and S. C. Srivastava, “Production ofno-carrier-added Cu-67,” Int. J. Appl. Radiat. Isot. 37, 29-36 (1986).
46S. V. Deshpande, S. J. DeNardo, C. F. Meares, M. J. McCall, G. P.Adams, M. K. Moi, and G. L. DeNardo, “Copper-67-labeled mono-clonal antibody LYM-1, a potential radiopharmaceutical for cancertherapy: Labeling and biodistribution in RAJI tumored mice,” J. Nucl.Med. 29, 217-225 (1988).
47J.A. Mercer Smith, N. J. Segura, F. J. Steinkruger, Z. V. Svitra, W. A.Taylor, and P. M. Wanek, “Synthesis and biodistribution of Cu-67meso-tetra (4-carboxyphenyl) porphine,” Los Alamos National Lab.Rep., LA-10429-PR, p. 145 (1984).
48J. Simon, W. F. Goeckler, B. Edwards, L. Stringham, W. A. Volkert,D. E. Troutner, R. A. Holmes, and S. Harry, “Sm-153-EDTMP, apotential therapeutic bone agent,” J. Labelled Comp. Radiopharm. 23,1344-1346 (1986).
49J. H. Turner, P. G. Caringbold, E. L. Hetherington, P. Sorby, and A.A. Martindale, “A phase I study of 153Sm-EDTMP therapy for dissem-inated skeletal metastases,” J. Clin. Oncol. 30, 1814-1818 (1989).
50G. R. Boniface, M. E. Izard, K. Z. Walken, D. R. McKay, P. Sorby, J.H. Turner, and J. G. Morris, ‘Labeling of monoclonal antibodies with153Srn for combined radioimmunoscintigraphy and radioimmunother-apy,” J. Nucl. Med. 30, 683-691 (1989).
51B. Grazman and D. E. Troutner, “Rh-105 as a potential radiothera-peutic agent,” J. Labelled Comp. Radiopharm. 23, 1371-1373 (1986).
52K.L. Kolsky, L. Pietrelli, L. F. Mausner, and S. C. Srivastava, “Prep-aration of carrier-free scandium-47,” J. Nucl. Med. 32, 945 ( 1991)(abstract).
53L. Pietrelli, L. F. Mausner, and K. L. Kolsky. “Chemical separation ofcarrier-free 47Sc from titanium targets,” J. Radioanal. Nucl. Chem.157, 335 (1992).
54P. Anderson, A. T. Vaughan, and N. R. Varley, “Antibodies labeledwith 199Au: Potential of l99Au for radioimmunotherapy,” Nucl. Med.Biol. 15, 293-297 ( 1988).
55J. F. Hainfeld, C. J. Foley, S. C. Srivastava, L. F. Mausner, N. I. Feng,G. E. Meinken, and Z. Steplewski, ‘Radioactive gold cluster immuno-conjugates: Potential agents for cancer therapy,” Nucl. Med. Biol. 17,287-294 (1990).
56M. R. Zalutsky, M. A. Nosh, E. V. Colapinto, P. K. Garg, and D. D.Bigner, “Enhanced tumor localization and in vivo stability of a mono-clonal antibody radioiodinated using N-succinimidyl-3-(tri-n-butylstannyl)benzoate,” Cancer Res. 49, 5543-5549 (1989).
57D. S. Wilbur, S. W. Hadley, M. D. Hylarides, P. G. Abrams, P. A.Beaumier, A. C. Morgan, J. M. Reno, and A. R. Fritzberg, “Develop
ment of a stable radioiodinating reagent to label monoclonal antibodiesfor radiotherapy of cancer,” J. Nucl. Med. 30. 216-226 (1989).
5 8L. A. Khawli and A. I. Kassis. “Synthesis of 125I labeledN-succinimidyl p-iodobenzoate for use in radiolabeling antibodies,”Nucl. Med. Biol. 16, 727-733 (1989).
59G. Vaidyanathan and M. R. Zalutsky, “Protein radiohalogenation ob-servations on the design of N-succinimidyl ester acylation agents,”Bioconjugate Chem. 1, 269-273 (1990).
60J. F. Eary. O. W. Press, C. C. Badger, L. D. Durack. K. Y. Richter, S.J. Addison, K. A. Krohn. D. R. Fisher, B. A. Porter, D. L. Williams,P. J. Martin, F. R. Appelbaum, R. Levy, S. L. Brown, R. A. Miller, W.B. Nelp, and I. D. Bernstein. “Imaging and treatment of B-cell lym-phoma.” J. Nucl. Med. 31. 1257-1268 (1990).
61S. M. Larson, A. Raubitschek. J. C. Reynolds, R. D. Neumann, K.Erik-Hellstrom, I Hellstrom, D. Colcher, J. Schlom, E. Glatstein, andJ. A. Carrasquillo, “Comparison of bone marrow dosimetry and toxiceffect of high dose 131I-labeled monoclonal antibodies administered toman.” Nucl. Med. Biol. 16, 153-158 (1989).
62L. C. Washburn, T. T. Hwa Sun, J. E. Crook, B. L. Byrd, J. E. Carlton,Y. W. Hung, and Z. S. Steplewski. “Y-90-labeled monoclonal antibod-ies for cancer therapy,” Nucl. Med. Biol. 13, 453-456 (1986).
6 3S. E. Order, J. L. Klein, P. K. Leichner, J. Frinke, C. Lollo, and J.Carlo, “Yttrium-90 antiferritin. A new therapeutic radiolabeled anti-body,” Int. J. Radiat. Oncol. Biol. Phys. 12, 227-281 (1986).
64D. J. Hnatowitch, M. Chinol, D. A. Siebecker, M. Gionet, T. Griffin, P.W. Doherty, R. Hunter, and K. R. Kase, “Patient biodistribution ofintraperitoneally administered yttrium-90 labeled antibody,” J. Nucl.Med. 29, 1428-1435 (1988).
65J. A. Carrasquillo, B. Kramer, T. Fleisher, P. Perentesis, C. J. Boland,F. Foss, M. Rotman, J. C. Reynolds, J. L. Mulshine, L. Camera, J.Frincke, C. Lollo, R. D. Neumann, S. M. Larson, and A. Raubitschek,“In-111 versus Y-90 T101 biodistribution in patients with hematopoi-etic malignancies,” J. Nucl. Med. 32, 970 (1991) (abstract).
66J. F. Eary, L. Durak, D. Williams, and J-L. Vanderheyden, “Consid-erations for imaging Re-188 and Re-186 isotopes,” Clin. Nucl. Med.15, 911-916 (1990).
67H. B. Breitz, P. L. Weiden, J-L Vanderheyden, J. W. Appelbaum, M.J. Bjorn, M. F. Fer, S. B. Wolf, B. A. Ratliff, C. A. Seiler, D. C. Foisie,D. R. Fisher, R. W. Schroff, A. R. Fritzberg, and P. G. Abrams,“Clinical experience with rhenium-186-labeled monoclonal antibodiesfor radioimmunotherapy: Results of phase I trials,” J. Nucl. Med. 33,1099-1112 (1992).
6 8S. M. Quadri and B. W. Wessels, “Radiolabeled biomolecules withRe- 186: Potential for radioimmunotherapy,” Nucl. Med. Biol. 13, 447-451 (1986).
69H. Breitz, B. Ratliff, R. Schroff, J. L. Vanderheyden, A. Fritzberg, J.Appelbaum, D. R. Fisher, P. Abrams, and P. Weiden, “Phase I studiesof 186Re whole MoAb and F(ab’)2 fragment for radioimmunotherapyin solid tumors,” J. Nucl. Med. 31, 724-725 ( 1990).
70R. A. Fawwaz, T. S. T. Wang, S. C. Srivastava, J. M. Rosen, S. Fer-rone, M. A. Hardy, and P. O. Alderson, “Potential of Pd-109-labeledantimelanoma monoclonal antibody for tumor therapy,” J. Nucl. Med.25, 796-799 (1984).
71A. K. DasGupta, L. F. Mausner, and S. C. Srivastava, “A new sepa-ration procedure for Cu from proton irradiated Zn,” Int. J. Appl.Radiat. Isot. 42, 371-376 (1991).
72D. W. McPherson, T. W. Lee, and F. F. Knapp, “A simple colorimet-tic method for determination of the specific activity of spallation pro-duced copper-67 using phenylglyoxal (PG) bis-(4N-methyl)thiosemicarbazone (TSC) derivatives,” Int. J. Appl. Radiat. Isot. 41,689-692 (1990).
73Chart of the Nuclides (Knoll Atomic Power Lab., General Electric Co.,San Jose, CA, 1988), 14th ed.
74K. L. Kolsky, L. F. Mausner, J. F. Hainfeld. G. E. Meinken, and S. C.Srivastava, “199Au production for use as a radiolabel of gold cluster
immunoconjugates,” J. Label. Compds. Radiopharm. 30, 211-213(1990).
7 5A. P. Callahan, D. E. Rice, and F. F. Knapp, “ 188Re for therapeuticapplications from an alumina-based 188W/188Re radionuclide genera-
tor,” Nucl. Compact. 1, 3-5 (1989).7 6G. J. Ehrhardt, A. R. Ketring, T. A. Turpin, M. S. Razavi, J. L.
Vanderheyden, F. M. Su, and A. R. Fritzberg, , “A convenient188W/188Re generator for therapeutic applications using low specific
activity 188W,” in Technetium and Rhenium in Chemistry and Nuclear
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

509 L. F. Mausner and S. C. Srivastava: Radionuclides for radioimmunotherapy 509
Medicine edited by M. Nicolini, G. Bandoli, and U. Maggi (Raven,New York, 1990). 3rd ed.. pp. 631-634.
77R. Doering, W. Tucker, and L. Stang, “A simple device for milkinghigh purity Y-90 from Sr-90,” J. Nucl. Med. 4, 55-59 (1963).
78M. Chino1 and D. Hnatowich, “Generator produced 90Y for radioim-munotherapy,” J. Nucl. Med. 29, 1465-1470 ( 1987).
79D. J. Hnatowich, “Antibody radiolabeling: Problems and promises,”Nucl. Med. Biol. 17, 49-55 ( 1990).
80 L.C. Washburn, T. T. H. Sun, Y.-C.C. Lee, B. L. Byrd, E. C. Hollo-way, J. E. Crook, J. B. Stubbs, M. G. Stabin, M. W. Brechbiel, O. A.Gansow, and Z. Steplewski, “Comparison of five bifunctional chelatetechniques for 90Y-labeled monoclonal antibody CO17-1A,” Nucl.Med. Biol. 18, 313-321 (1991).
8 1S. V. Deshpande, S. J. DeNardo, D. L. Kukis, M. K. Moi, M. J.McCall, G. L. DeNardo, and C. F. Meares, “Yttrium-90-labeled mon-
oclonal antibody for therapy: Labeling by a new macrocyclic bifunc-tional chelating agent.” J. Nucl. Med. 31, 473-479 ( 1990).
82O. A. Gansow, “Newer approaches to the radiolabeling of monoclonalantibodies by use of metal chelates,” Nucl. Med. Biol. 18, 369-381(1991).
83C. F. Meares, M. K. Moi, H. Diril, D. L. Kukis, M. J. McCall, S. V.Deshpande, S. J. DeNardo, D. Snook, and A. Epenetos, “Macrocyclicchelates of radiometals for diagnosis and therapy.” Br. J. Cancer 62,21-26 (1990).
84M. W. Brechbiel and O. A. Gansow, “Backbone substituted DTPAligands for 90Du radioimmunotherapy,” Biconjugate Chem. 2, 187-194(1991).
85W. Vaalburg, A. M. J. Paans, J. W. Terpstra, T. Weigman, K. Dekens,A. Rikamp, and M. G. Woldring, “Fast recovery by dry distillation ofBr-75 induced in reusable metal selenide targets via Se-76 (p,2n) Br-75reaction,” Int. J. Appl. Radiat. Isot. 36, 961-964 (1985).
Medical Physics, Vol. 20. No. 2, Pt. 2, Mar/Apr 1993

M I R D f o r m u l a t i o n
Evelyn E. Watson and Michael G. StabinOak Ridge Institute for Science and Education, Oak Ridge, Tennessee 37831
Jeffry A. SiegelCooper Hospital, Camden, New Jersey 08103
(Received 18 March 1992; accepted for publication 15 September 1992)
The Medical Internal Radiation Dose (MIRD) Commit-tee of the Society of Nuclear Medicine has provided guid-ance on methods for calculating radiation absorbed doseestimates since 1968. The MIRD Primer1 gives a completeexplanation of the schema which is a series of general equa-tions adaptable for use with either simple or complex an-atomical and kinetic models. By definition, the absorbeddose is the energy absorbed from ionizing radiation perunit mass of tissue. Because absorbed dose from internallydistributed radionuclides is never completely uniform,’ theMIRD equations give the average, or mean, absorbed doseto a volume of tissue.
The schema is useful for estimating absorbed dose tovolumes as small as a cluster of cells or as large as the totalbody. Microdosimetric techniques that account for statis-tical aspects of particle track structures and energy distri-bution patterns in microscopic volumes can be used to ex-press energy deposition in tissues from materials labeledwith alpha-particle or Auger-electron emitters, particularlythose incorporated within cells.
The equation for calculating the absorbed dose may bewritten in various forms depending on available informa-tion. An example is shown in Eq. (1):
where D(rk ← r h) is the mean absorbed dose in-a targetregion r k from activity in a source region r h, Ah is thecumulated activity (time integral of activity over the timeinterval of interest) in the source, ∆ ι is the mean energyemitted by a radionuclide per nuclear transition, φ i ( rk ← rh)is the absorbed fraction (fraction of energy emitted in re-gion rh that is absorbed in region rk), and mk is the mass ofthe target rk. The absorbed fraction divided by the massmay be represented by Φ (rk ← rh), the specific absorbedfraction. The total mean absorbed dose in a target region iscalculated by summing the doses from all source regions tothe target. Equation ( 1) can be divided into two types ofparameters-physical and biological.
I. PHYSICAL PARAMETERS
A. Mean energy emitted per transition (A)
The most readily obtainable and the most accurate val-ues required for dose calculation are probably those relatedto the energy emitted from a radioactive source. Each typeof radiation emitted by a radionuclide is characterized byits own mean energy per particle E i and its own intensity ornumber of particles emitted per transition n i. The mean
energy emitted per transition ∆ i is equal to kni E i where kis a constant that depends on the units used for the termsin Eq. (1). The Brookhaven National Laboratory main-tains a file of decay information that can be used to deter-mine the intensities and energies of the different emissionsassociated with the transformation of any known radionu-clide. In 1989, the MIRD Committee published this infor-mation on 242 radionuclides in a form that can be easilyused for dose calculation.* In addition to intensities andenergies, delta (A) values are given in both traditional(rad g/µCi h) and SI (Gy kg/Bq s) units. Diagrammaticdecay schemes are provided along with the physical half-lives, daughter products, and other related data.
B. Absorbed fraction (φ)
The absorbed fraction varies with the type and energy ofthe radiation, the type of material through which the radi-ation passes, and the geometric configuration and the com-position of the source and the target. Its value cannot beless than 0 or greater than 1. For convenience in estimatingabsorbed fractions, radiation types are sometimes classifiedas penetrating and nonpenetrating. If the amount of energyimparted to any target other than the source is so insignif-icant as to have little effect on the absorbed dose, the ra-diation is considered to be nonpenetrating. The absorbedfraction in the source is equal to one, and absorbed frac-tions for all other targets are zero. The classification ofradiation as penetrating or nonpenetrating is determinedby the absorption properties of the radiation, the nature ofthe model describing the source and target, and the type ofcalculation. Radiations may be considered nonpenetratingin the calculation of mean absorbed dose to a source vol-ume but penetrating when the spatial distribution of ab-sorbed dose is required, such as in tumor dosimetry.
Several techniques have been used to calculate absorbedfractions, such as Monte Carlo and buildup factormethods. 3-8 Software for determining energy deposition intissue include the ALGAMP code which has been used tocalculate absorbed fractions for humans at various agesand the Electron Gamma Shower package, commonlycalled EGS4, which is particularly useful for calculatingthe spatial distribution of absorbed dose from electrons andbeta particles. In some instances, the reciprocity principle’has been applied when absorbed fractions could not becalculated to the desired level of accuracy by other tech-niques. Symbolically, the reciprocity relationship can beillustrated as follows:
511 Med. Phys. 20 (2). pt. 2, Mar/Apr 1993 0094-2405/93/020511-04$01.20 © 1993 Am. Assoc. Phys. Med. 511

512 Watson, Stabin, and Siegel: MIRD formulation 512
Frequently specific absorbed fractions Φ ( rk ← r h), orφ (rk ← rh)/mk, are calculated rather than absorbed frac-tions. By reciprocity,Absorbed fractions and specific absorbed fractions for pho-tons in organs of a 70-kg Reference Man have been pub-lished by the MIRD Committee.3,4 The committee has alsoprovided absorbed fractions for photons in spheres, cylin-ders, and ellipsoids from one gram to 200 kg in mass. 5,6 InMIRD Pamphlet No. 7,8 Berger provided information onabsorbed dose distributions around point sources that canbe used in calculating specific absorbed fractions from betaparticles and electrons. Leichner et al.9 developed a gener-alized, empirical point-source function for calculating ab-sorbed doses in tumors from beta particles based on Berg-er’s tabulated absorbed-dose distributions.8
C. Mean dose per unit cumulated activity (S)
The product of ∆ and Φ is a constant for a given radi-onuclide and a given source-target combination, a valuedesignated by the MIRD Committee as the S value. Themean absorbed dose equation can thus be written as
(3)
where S(rk ← r h) = Σ ι∆ ιΦ ι ( rk+ rh). Values Of S have beenpublished in MIRD Pamphlet No. 1110 for a mathematicalmodel representing an adult male (Reference Man) withmost of the important organs. Absorbed fractions and spe-cific absorbed fractions for other mathematical models canbe used to calculate S values as needed. Cristy andEckerman11 have developed models and calculated specificabsorbed fractions from internal photon sources for Refer-ence Woman (also used to represent a 15-yr-old male) aswell as a 10-yr-old, a 5-yr-old, a 1-yr-old, and a newbornchild. Mathematical descriptions of organs and regions ofthe body have been designed to supplement or improvethose included in the original models. Of particular interestfor monoclonal antibody dosimetry are models of the bloodvessels12,13 and the peritoneal cavity. 1 4
Absorbed fractions and S values have also been calcu-lated for small or irregularly shaped structures in theb o d y ? ‘ * Johnson et al. determined the radiation dosefrom 1 6 6H o , 1 8 6Re and 1 5 3Sm at a bone-to-marrow inter-face using the EGS4 code and including the contribution ofbackscattered radiation to the marrow dose.15 H u m m1 6
calculated absorbed fractions and dose rates for solid tu-mors with “cold-regions” surrounded by uniform distribu-tion of radiolabeled monoclonal antibodies to illustrate theabsorbed dose-rate profile for different radionuclides. How-ell et al. 17 published dose-rate profiles for 3 2P, 6 7Cu. 9 0Y ,1 1 1AG, 1 3 1I, 1 8 8Re, and 1 9 3 mPt in spherical “tumors” withradii of 0.05 and 0.5 cm. Akabani et al. have published betaabsorbed fractions for a large number of radionuclides inspheres with radii ranging from 0.1-2.0 cm (Ref. 18).
Most absorbed dose calculations are based on the as-sumption that the absorbed fractions and the mass of thetarget remain constant during the time of irradiation. This
is not always the situation. Howell et al. have studiedchanges in absorbed dose for rapidly growing tumors.” Inradionuclide therapy, the volumes of the tumors maychange greatly during the period over which the dose isdelivered. Folding the tumor masses into the calculationmay result in more accurate doses and a more meaningfuldetermination of the dose-response relationships.
Several investigators have calculated absorbed fractionsfor cellular configurations.20-22 A few examples will sufficeto illustrate this. Kassis et al. determined absorbed frac-tions and absorbed dose rates to cells for nuclear transi-tions occurring inside the cell, in other cells, and in theextracellular medium.20 Makrigiorgos et al. 21 used thistechnique to calculate absorbed doses for cell clusters withdifferent cellular diameters and different fractions of thecell volume that are labeled. Bardies and Myers have pre-sented a model for cellular and cell cluster dosimetry foruse in targeted radionuclide therapy. 22 Some of these mod-els have been proposed as evidence of the limitations of theMIRD technique; however, the components of the calcu-lations are the same as those in the MIRD schema. Forexample, the absorbed dose may be given as a function ofdistance along a defined axis, but the calculation is basedon absorbed fractions or specific absorbed fractions definedas a function of distance along the axis.
II. BIOLOGICAL PARAMETERS
A. Cumulated activity (A)
The cumulated activity A h represents the total numberof nuclear transformations occurring during the time ofinterest in the source region rh and may be expressed inunits of microcurie hours, Becquerel seconds, or an appro-priate multiple of these units. A compilation of cumulatedactivities for various radionuclides or radioactive com-pounds has not been published by the MIRD Committeebecause the source regions differ for each radiolabeled ma-terial, and the source regions and their cumulated activitiesoften change as new research results become available.
The residence time τ of a radionuclide in a source regionis equal to the cumulated activity in the source divided bythe administered activity; that is
(4)
Although activity can sometimes be measured directly byexternal measurements with a scintillation camera in eitherthe planar or SPECT modes, cumulated activities and res-idence times are not always available because of difficultiesin directly measuring the activity in organs or regions ofthe body. Frequently, these values are determined indi-rectly through measurements that can be made, such astotal body retention, excretion, blood clearance, etc., andthe use of compartmental analysis techniques.23 Computersoftware has been developed that permits the application ofcompartmental analysis to the development of models thatwill yield residence times in the organs or regions of inter-est. One such program is the Simulation, Analysis, andModeling (SAAM) program.24 This software is availablewithout cost from the Resource Facility for Kinetic Anal-
Medical Physics. Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

513 Watson, Stabin, and Siegel: MIRD formulation 513
ysis, Center for Bioengineering, FL-20, University ofWashington, Seattle, WA 98195. Versions of the softwareare available for use on several computers such as theVAX, IBM-compatible personal computers, and manyothers.
Although data collected in humans are always prefera-ble, data collected in animals may sometimes be extrapo-lated to give estimates of the time-activity behavior of aradionuclide in humans.2 5 No single technique for suchextrapolation has been generally accepted; however, greatcare must be taken in collecting the data and in performingthe extrapolation to assure that these extrapolations areperformed as accurately as possible.26 Data should be pre-sented in a manner that will allow other investigators tomake use of the information and possibly recalculate ifbetter extrapolation techniques are determined.
The MIRD Committee has published 15 dose estimatereports1,27-29 for nuclear medicine radiopharmaceuticals.Each report includes the biological models used for calcu-lating cumulated activities needed for the dose estimate.These models can sometimes be adapted for other situa-tions and other radionuclides. They also can be useful indetermining how models may be developed and how datashould be collected.
III. EXTENSION OF MIRD SCHEMA TOMONOCLONAL ANTIBODY DOSIMETRY
The MIRD schema is accepted as a useful technique forestimating the radiation dose from radioactive materialwithin the human body. With respect to the dosimetry ofradiolabeled antibodies, the MIRD Committee has pro-vided a description of the ingredients that produce an ab-sorbed dose estimate. The basic equations are applicable totissues of various sizes and shapes and in different geomet-ric relationships with each other. The committee has pub-lished data for calculating the mean absorbed dose in tar-gets from activity that can be considered to be uniformlydistributed in source organs or in small spheres andellipsoids. 3-7
Absorbed fractions or specific absorbed fractions fornonuniform activity distributions or for nonstandard ge-ometries will need to be calculated for some situations.Investigators have already generated absorbed fractionsand specific absorbed fractions of energy from alpha andbeta particles and electrons for some spherical tumors atthe macroscopic or millimeter level16-18 and for nonuni-form distribution within cell clusters.20-22 Such values arenot usually required for photon radiations.
Autoradiographic studies have clearly shown nonuni-form distribution of radiolabeled monoclonal antibodies intumors. The MIRD schema can be used to estimate ab-sorbed doses for nonuniform distributions if the necessarydata are obtained. The limitation is in the lack of an ade-quate model rather than in the schema. As the volume forwhich the absorbed dose is calculated becomes smaller, thenonuniformity of dose within that volume also becomessmaller.
From the standpoint of absorbed dose, localization ofactivity in individual structures of a cell or in parts of a
tumor mass is analogous to localization of activity in or-gans of the body. The greatest obstacles to estimating ab-sorbed doses for radiotherapy agents are the measurementof activity distributions over time and the assessment ofgeometric relationships among sources and targets withinthe tissue. Calculating residence times or cumulated activ-ities is not difficult if necessary biological data are obtained,and computer software is available to calculate absorbedfractions of energy if the tissue volumes of interest aredefined.
A possible technique for circumventing these problemsmay be to calculate a range of doses as well as a meanabsorbed dose for a region as presented by Robersonet al. 30 for radiolabeled microsphere therapy. This gives anestimate of the variations in absorbed dose that exist inregions where the activity distributions are significantlynonuniform.
IV. SUMMARY
The MIRD schema is not restricted to calculating meanabsorbed doses in organs but can be extended to any tissuefor which distribution and retention data can be obtainedand for which a reasonably accurate mathematical descrip-tion of the source and target tissues can be determined.
The development of more accurate absorbed dose esti-mates and the correlation of these estimates with radiationeffects will lead to a better understanding of the resultsfrom radiotherapeutic agents such as radiolabeled mono-clonal antibodies. Therefore, radiobiologists and internaldosimetrists need to combine their efforts and work towardthe common goal of improving the treatment of malignantdiseases.
1R. Loevinger, T. F. Budinger, and E. E. Watson, MIRD Primer forAbsorbed Dose Calculations (Society of Nuclear Medicine, New York,NY, 1988).
2D. A. Weber, K. F. Eckerman, L. T. Dillman, and J. C. Ryman,MIRD: Radionuclide Data and Decay Schemes (Society of NuclearMedicine, New York, NY, 1989).
3W. S. Snyder, M. R. Ford, G. G. Warner, and H. L. Fisher, Jr.,‘Estimates of absorbed fractions for monoenergetic photon sourcesuniformly distributed in various organs of a heterogeneous phantom,MIRD Pamphlet No. 5,” J. Nucl. Med. 10, Suppl. 3 (1969).
4W. S. Snyder, M. R. Ford, and G. G. Warner, Estimates of SpecificAbsorbed Fractions for Photon Sources Uniformly Distributed in VariousOrgans of a Heterogeneous Phantom, MIRD Pamphlet No. 5, Revised(Society of Nuclear Medicine, New York, NY, 1978).
5G. L. Brownell, W. H. Ellett, and A. R. Reddy, “Absorbed fractionsfor photon dosimetry, MIRD Pamphlet No. 3,” J. Nucl. Med. 9, Suppl.No. 1, 27-39 (1968).
6W. H. Ellett and R. M. Humes, “Absorbed fractions for small volumescontaining photon-emitting radioactivity, MIRD Pamphlet No. 8,” J.Nucl. Med. 12, Suppl. No. 5, 25-32 ( 1971).
7M. J. Berger, “Energy deposition in water by photons from point iso-tropic sources, MIRD Pamphlet No. 2,” J. Nucl. Med. 9, Suppl. No. 1,15-25 (1968).
8M. J. Berger, “Distribution of absorbed dose around point sources ofelectrons and beta particles in water and other media, MIRD PamphletNo. 7,” J. Nucl. Med. 12, Suppl. No. 5, 1-23 (1971).
9P. K. Leichner, W. G. Hawkins, and N.-C. Yang, “A generalized,empirical point-source function for beta-particle dosimetry,” Antib.Immunoconjug. Radiopharm. 2, 125-144 (1989).
Medical Physics. Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

514 Watson, Stabin, and Siegel: MIRD formulation 514
1 0W. S. Snyder, M. R. Ford, G. G. Warner, and S. B. Watson, "S"Absorbed Dose Per Unit Cumulated Activity for Selected Radionuclidesand Organs, MIRD Pamphlet No. 11 (Society of Nuclear Medicine,New York, NY, 1975).
11M. Cristy and K. F. Eckerman, “Specific absorbed fractions of energyat various ages from internal photon sources,” ORNL/TM-8381, Vols.1-7 (1987).
1 2G. Akabani and J. W. Poston, Sr., “Absorbed dose calculations toblood and blood vessels for internally deposited radionuclides,” J.Nucl. Med. 32, 830-834 (1991).
13R. E. Faw and J. K. Shultis, “Dosimetry calculations for concentriccylindrical source and target regions with application to blood vessels,”Health Phys. 62, 344-350 (1992).
1 4E. Watson, M. G. Stabin, J. L. Davis, and K. F. Eckerman, “Amodel of the peritoneal cavity for use in internal dosimetry,” J. Nucl.Med. 30, 2002-2011 (1989).
15J. C. Johnson, S. M. Langhorst, S. K. Loyalka, W. A. Volkert. and A.R. Ketring, “Calculation of radiation dose at a bone-to-marrow inter-face using Monte Carlo modeling techniques (EGS4),” J. Nucl. Med.33, 623-628 (1992).
16J. L. Humm, “Dosimetric aspects of radiolabeled antibodies for tumortherapy,” J. Nucl. Med. 27, 1490-1497 (1986).
17 R.W. Howell, D. V. Rao, and K. S. R. Sastry, “Macroscopic dosim-etry for radioimmunotherapy: Nonuniform activity distributions insolid tumors,” Med. Phys. 16, 66-74 (1989).
18G. Akabani, J. W. Poston, Sr., and W. E. Belch, “Estimates of betaabsorbed fractions in small tissue volumes for selected radionuchdes.”J. Nucl. Med. 32, 835-839 (1991).
19R. W. Howell, V. R. Narra, and D. V. Rao, “Absorbed dose calcula-tions for rapidly growing tumors,” J. Nucl. Med. 33, 277-281 (1992).
20A. I. Kassis, S. J. Adelstein, C. Haydock, and K. S. R. Sastry,“Thallium-201: An experimental and a theoretical radiobiological ap-proach to dosimetry,” J. Nucl. Med. 24, 1164-1175 (1983).
21G. M. Makrigiorgos, S. J. Adelstein, and A. I. Kassis, “Limitations ofconventional internal dosimetry at the cellular level,” J. Nucl. Med. 30,1856-1864 (1989).
22M. Bardies and M. J. Myers, “Development and validation of a simple
model for cellular and ceil cluster dosimetry with practical applicationin targeted radionuclide therapy," in Fifth International Radiopharma-ceutical Dosimetry Symposium, CONF-910529. edited by E. E. Watsonand A. T. Schlafke-Stelson (Oak Ridge Associated Universities, OakRidge, TN, 1992), pp. 531-543.
23M. Berman, Kinetic Models for Absorbed Dose Calculalions. MIRDPamphlet No. 12 (Society of Nuclear Medicine, New York, NY,1977).
24M. Berman and M. F. Weiss, SAAM Manual (U.S. DHEW PublicationNo. (NIH) 78-108, US. Government Printing Office, Washington,DC, 1978).
25H. D. Roedler, “Accuracy of internal dose calculations with specialconsideration of radiopharmaceutical biokinetics,” in Third Interna-tional Radiopharmaceutical Dosimetry Symposium, edited by E. E.Watson, A. T. Schlafke-Stelson, J. L. Coffey, and R. J. Cloutier (OakRidge Associated Universities, Oak Ridge, TN, 1981), pp. I-20.
26K.A. Lathrop,” Collection and presentation of animal data relating tointernally distributed radionuclides,” Third International Radiophar-maceutical Dosimetry Symposium, edited by E. E. Watson, A. T.Schlafke-Stelson, J. L. Coffey, and R. J. Cloutier (Oak Ridge Associ-ated Universities, Oak Ridge, TN, 1981). pp. 198-203.
2 7D. A. Weber, P. Todd Makler, Jr., E. E. Watson, J. L. Coffey, S. R.Thomas, and J. London, “MIRD Dose Estimate Report No. 13. Ra-diation absorbed dose from technetium-99m-labeled bone imagingagents,” J. Nucl. Med. 30, 1117-I 122 (1989).
2 8H. L. Atkins, S. R. Thomas, U. Buddemeyer, and L. R. Chervu,“MIRD Dose Estimate Report No. 14. Radiation absorbed dose fromtechnetium-99 m-labeled red blood cells,” J. Nucl. Med. 31, 378-380(1990).
29J.S. Robertson, M. D. Exekowitz, M. K. Dewanjee, M. G. Lotter, andE. E. Watson, “MIRD Dose Estimate Report No. 15. Radiation ab-
sorbed dose for radioindium-labeled autologous platelets,” J. Nucl.Med. 33, 777-780 (1992).
30P. L. Roberson, R. K. Ten Haken, D. L. McShan, P. E. McKeever, andW. D. Ensminger, “Threedimensional tumor dosimetry for hepaticyttrium-90-microsphere therapy,” J. Nucl. Med. 33, 735-738 (1992).
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

Pharmacokinetic modelingSven-Erik StrandDepartment of Radiation Physics, Lund University, University Hospital, S-221 85, Lund, Sweden
Pat ZanzonicoDivision of Nuclear Medicine. New York Hospital-Cornell Medical Center, New York. New York
Timothy K. JohnsonDepartment of Radiology. University of Colorado, Denver, Colorado
(Received 18 March 1992; accepted for publication 27 November 1992)
For radiation dosimetry calculations of radiolabeled monoclonal antibodies, (MAb), pharma-cokinetics are critical. Specifically, pharmacokinetic modeling is a useful component of estima-tion of cumulated activity in various source organs in the body. It is thus important to formulategeneral methods of pharmacokinetic modeling and of pharmacokinetic data reduction, leadingto cumulated activities. In this paper different types of models are characterized as “empirical,”“analytical,” and “compartmental” pharmacokinetic models. There remains a pressing need forquantitative studies in man for a proper understanding of the pharmacokinetics of MAb. Phar-macokinetic modeling of radiolabeled MAb in vivo has relied on relatively limited studies in manand complementary detailed measurements in animals. In either case, any model chosen foranalysis of such data is inevitably based on measurements of limited accuracy and precision aswell as assumptions regarding human physiology. Very few macroscopic compartmental phar-macokinetic models for MAb, have been tested over a range of conditions to determine theirpredictive ability. Extracorporeal immunoadsorption represents one approach for drasticallyaltering the biokinetics of antibody distribution, and may serve to validate a given pharmacok-inetic model. In addition to macroscopic modeling, the microscopic evaluation of the time-dependent distribution of radiolabeled MAb in tissues is of utmost importance for a properunderstanding of the kinetics and radiobiologic effect. Many tumors do not exhibit homogeneousuptake. A mathematical understanding of that distribution is thus essential for accurate tumordosimetry estimates. This review summarizes methodologies for pharmacokinetic modeling,critically reviews specific pharmacokinetic models and demonstrates the capability of modelingfor predictive calculations of altered pharmacokinetics, emphasizing its use in dosimetriccalculations.
1. INTRODUCTION
Epitomizing Ehrlich’s century-old conceptualization of the“magic bullet,” radiolabeled monoclonal antibodies(MAb) against tumor-specific and/or associated antigenshave spurred an unprecedented worldwide effort in nuclearmedicine research. A sound quantitative understanding ofthe pharmacokinetics and thus a systematic approach tothe radiation dosimetry of these target tissue-specific ra-diopharmaceuticals has largely remained elusive, however.Indeed, the general difficulties inherent in generating rea-sonably accurate and precise cumulated activity and ab-sorbed dose estimates for internal radionuclides are exac-erbated for radiolabeled MAb because of the markedqualitative as well as quantitative differences in their phar-macokinetics among different species, different individuals,different antibodies, different radionuclides, differentmodes of administration, and different administeredamounts.
Accordingly, radiation dosimetry of sufficient accuracyand precision for therapeutic application of radiolabeledMAb, as dictated by the generally marginal therapeuticindex (i.e., the tumor-to-critical normal tissue absorbeddose ratio), must be performed on an individualized basis.Thus the general treatment planning paradigm used, for
example, in radioiodine treatment of metastatic thyroidcancer’ should be considered for radioimmunotherapy: alow-activity tracer administration, kinetic studies consist-ing of serial measurements of tissue activities, absorbeddose estimation and projection to the maximum “safe” andthe minimum “therapeutically effective” administered ac-tivities, and a high-activity therapy administration (withadditional kinetic studies for verification of the actual ther-apeutic absorbed doses). Nonetheless, practical quantita-tive radionuclide imaging methods including planar,single-photon emission computed tomography (SPECT),and positron emission tomography (PET), as well asprobe-based organ and total. body activity measurementsand ex vivo blood activity concentration measurementshave been developed and published in detail;1-36 the readeris referred to the pertinent contributions in this volume foradditional information.
II. PRACTICAL SIGNIFICANCE OFPHARMACOKINETIC MODELING
Pharmacokinetic modeling is a useful component of es-timation of cumulated activities (i.e., the number of nu-clear transformations) in the various source regions of thebody. Although a general concept in internal radionuclide
515 Med. Phys. 20 (2). ft. 2, Mar/Apr 1993 0094-2405/93/020515-14501.20 © 1993 Am. Assoc. Phys. Med. 515

516 Strand, Zanzonico, and Johnson: Pharmacokinetic modeling 516
radiation dosimetry, the precise meaning of “cumulatedactivity” will be illustrated using the formalism promul-gated by the Medical Internal Radiation Dosimetry(MIRD) Committee, the International Commission onRadiation Units and Measurements (ICRU), and the In-ternational Commission on Radiological Protection( I C R P ) .3 8 - 5 1 The mean absorbed dose, D(rk ← rh), to atarget region, rk, from a radionuclide in a source region, rh,is given by the following equations:
and
(1)
(2)
where Ah is the cumulated activity (e.g., in Bq-h) in sourceregion rh, Ah(t) is the radioactive decay-uncorrected activ-ity (e.g., in Bq) in source region rh at time t p o s t -administration (e.g., in h), and S(rk ← rh) is the “S factor”(e.g., in Gy/Bq-h) for target region r k and source regionrh, that is, the absorbed dose to target region r k per unitcumulated activity in source region rh.
Since there are generally multiple source regions, rh, foran internally distributed radionuclide, the total absorbeddose to the target region, rk, is given by the summation ofthe expression on the right side of Eq. ( 1) over all of thesource regions, rh:
(3)
The S factor, S(rk ← rh), is a physical quantity related tothe nuclear properties (i.e., the number, type, and energyof nuclear radiations and related emissions accompanyingradioactive decay) of a particular radionuclide, the geo-metric orientation of and distance between the target re-gion, rk, and the source region, rh, and the electron andmass densities, elemental composition, and effective atomicnumber of the target region, rk, the source region, rh, andthe intervening tissues.” For specific anthropomorphic an-atomic models (e.g., “Standard Man”42,48), the values of Sfactors, S ( rk ← rh), for many radionuclides and targetregion-source region pairs are tabulated and published.
On the other hand, knowing the physical half-life of aradionuclide, the cumulated activities, Ah, are biologicalquantities related to the pharmacokinetics of a particularradioactive material. In view of the practically infinitenumber of combinations of materials, radionuclides, phys-iological and pathological conditions, and amounts andmodes of administration, it is obviously impractical to use-fully tabulate pharmacokinetic parameters and/or cumu-lated activities of radioactive materials. It is therefore es-sential to formulate general methods of pharmacokineticmodeling and of pharmacokinetic data reduction leading tocumulated activities.
III. TYPES OF PHARMACOKINETIC MODELS
In the broadest sense, a pharmacokinetic model is sim-ply a mathematical description of the distribution of somematerial over time. Although the following distinctions are
Medical Physics, Vol. 20, No. 2. Pt. 2, Mar/Apr 1993
neither rigorous nor standardized, it is didactically usefulto separately consider the various types of pharmacokineticmodels and their advantages and disadvantages. In radia-tion dosimetry practice, at least three general types ofpharmacokinetic models can be identified: “empirical,”“analytic,” and “compartmental.”
Whatever approach to pharmacokinetic modeling oneadopts, the insightful admonition of Dr. Robert Loevingershould be borne very much in mind.5 2
“It is never possible to calculate the dose to a patient;one can only calculate the dose to a model. The model,of course, is the totality of the assumptions necessary tomake the calculation; these assumptions define a class ofpatients, and the dose applies to this class. How well agiven patient fits the model is only conjectural...For in-ternally distributed radionuclides, the models are crude,and the difference between the patient and model isvast...”
A. Empirical pharmacokinetic models
In applying radiotracer methodology, serial measure-ments of the amount or concentration of the radiotracer inone or more tissues are typically graphed as a function oftime post-administration. (It is implicitly assumed that tis-sues of interest, including the target and/or critical organs,are, in fact, “measurable.“) The resulting time-activitycurve itself may be characterized as an “empirical” phar-macokinetic model in that it is a mathematical descriptionof the distribution of the radiotracer incorporating infor-mation derived only by direct measurement. If the activitymeasurements are not corrected for radioactive decay, thenthe area under the time-activity curve represents the time-integral of the activity, that is, the cumulated activity [Eq.(2)]. The area under the time-activity curve may be eval-uated by planimetry or some method of numeric integra-tion (e.g., the trapezoidal rule, Simpson’s rule, etc.). How-ever, the accuracy of such integration is highly dependenton judicious timing and adequate frequency of the mea-sured data. An important advantage of empirical pharma-cokinetic models is that no simplifying assumptions areintroduced regarding the analytic form of the time-activitydata or the biology of the radiotracer distribution.
While it is difficult to measure the “zero-time” activity(in percent of administered activity) in a given tissue, onecan reasonably equate this parameter with the percent ofthe total body volume of distribution of the radiotracer(e.g., plasma volume, extracellular water volume, etc.)contained in that tissue. It is also impossible to measure theactivity or activity concentration indefinitely. It is thereforedesirable but often impractical to include a sufficiently“late” final measurement (e.g., after five physical half-lives, after the total body activity has decreased to less than10% of the administered activity, etc.), to sufficiently min-imize this source of error. Accordingly, one must generallyassume that after the final measurement in a given tissue,its time-activity curve simply parallels that of the totalbody or there is no biological elimination (i.e., there iselimination only by radioactive decay in situ); this latterapproach, which is used for blood and for the total body in
517 Strand, Zanzonico, and Johnson: Pharmacokinetic modeling 517
the kinetic analysis of the low-activity tracer administra-tion for planning radioiodine treatment of metastatic thy-roid cancer,’ may result in overestimation of cumulatedactivities.
B. Analytic pharmacokinetic models
In part to overcome the inability of empirical pharma-cokinetic models to reasonably extrapolate beyond the gen-erally limited time-activity data, one may fit these data toan analytic function (sometimes referred to as a “distribu-tion function”). Implicit in such an “analytic” pharmacok-inetic model is the assumption that the time-activity curvefollows the fitted time-dependent function before the firstmeasurement as well as after the final measurement. Sincebiological processes (such as the exchange of materialamong tissues) are generally assumed to follow first-orderkinetics, time-activity curves are generally fit to a sum ofexponentials (“by eye,” by exponential "curve stripping,”or, more commonly, by a computerized “least-squares” fit-ting algorithm5 3) :
where qh(t) is the distribution function for source regionrh, that is, the radioactive decay-corrected activity (e.g., inBq) in source region rh at time t post-administration (e.g.,in h) of the radiotracer, (Ah) j is the activity (e.g., in Bq)for the jth exponential component in source region r h, attime t=0, and (λ h)j is the biological disappearance con-stant (e.g., in h-1) of the jth exponential component of thetime-activity curve in source region rh, that is, the fractionof activity eliminated per unit time for the jth exponentialcomponent of the time-activity curve for source region r h.
Time-activity data are generally plotted in semi-logarithmic graphs, that is, the activity or activity concen-tration is plotted on a logarithmic ordinate scale versus thetime on an arithmetic abscissa scale. In this way, eachexponential component of the distribution function, q h(t),appears as a linear segment of the time-activity curve, andthe number of exponential components corresponds to theidentifiable number of linear segments. (If the “slopes” ofthe linear segments are not widely different, however, theresolution of the time-activity curve into distinct exponen-tial components may be problematic). If the empiricaltime-activity curve is monotonically decreasing, the biolog-ical disappearance constants, (λ h)j, are negative (See Ap-pendix I). In this case, the generally rising initial portion(i.e., the so-called “uptake phase”) of the time-activitycurve has not been sampled and will not be accuratelyrepresented by the resulting distribution function, q h(t). Ifthe empirical time-activity curve is more complex, consist-ing of both increasing and decreasing segments, the respec-tive biological disappearance constants, (λ h), are positiveand negative. Note that, in addition to the experimentalerror, or uncertainty, associated with each activity mea-surement, fitting the time-activity curve to an analyticfunction introduces an error in the estimated values of the
Medical Physics, Vol. 20, No. 2, pt. 2, Mar/Apr 1993
function parameters [i.e., (Ah)j and (λ h )j ], related to thedeviation of the measured time-activity curve from the fit-ted distribution function, q h(t).
Incorporating the distribution function notation into theexpression for the cumulated activity, A h, Eq. (3) can bereformulated as follows:
where λ is the physical decay constant (e.g., in h - 1) of theradionuclide in the radiotracer, that is, the fraction of ac-tivity eliminated per unit time by radioactive decay.
Substituting the expression for the distribution function,( qh(t), in Eq. (4) into the expression for the cumulatedactivity, Ã h, in Eq. (5) and evaluating the resulting definiteintegral yields the following expression:
C. Compartmental pharmacokinetic models
1. General aspects
An alternative, “physiological” approach to the deter-mination of cumulated activities is based upon compart-mental analysis ,4 9 , 5 4 - 5 6 wherein a biological system istreated as an assortment of interconnected compartmentseach consisting of an ensemble of identical chemical orphysical units. Each such ensemble is somehow localized inan identifiable anatomic entity (e.g., an organ such as theliver), an identifiable functional entity (e.g., the reticuloen-dothelial system), or an identifiable physical entity (e.g.,the extracellular water space). Any such anatomically,functionally, or physically localized ensemble constitutes a“compartment.” Such an ensemble may not, however, ac-tually be localized in any such identifiable entity and itsexistence as a discrete compartment is then purely concep-tual. Normally, compartments tend to remain constant interms of the size of the ensemble (i.e., the number of chem-ical or physical units), while undergoing continual turn-over, by the net rate of input equaling the net rate of out-put. The existence of such a dynamic equilibrium, or“steady state,” the identifiability of specific compartmentsand the detectability of the flux of a non-perturbing tracerthrough various such compartments are implicit assump-tions of compartmental analysis. A compartmental modelis thus characterized by the number of compartments andby transition probabilities, or “exchange rates,” betweencompartments and may be represented mathematically bya set of coupled ordinary differential equations:
where dF(i,t)/dt is the flux of the tracer (e.g., in Bq/hthrough compartment i, that is, the net amount of tracerper unit time traversing compartment i, F(i,t),F(j,t) i sthe amount of tracer (e.g., in Bq) in compartments i and j,respectively, at time t post-administration (e.g., in h),L(i,j,t),L(j,i,t) are the fractional exchange rates (e.g., in
518 Strand, Zanzonico, and Johnson: Pharmacokinetic modeling 518
h -l) of the amount of tracer to compartment i from com-partment j and to compartment j from compartment i,respectively, and n is the number of compartments in themodel.
The exchange rates, L(i,j,t) and L(j,i,t), are generallyconstant with time (i.e., time-invariant) and the flux of thetracer, dF(i,t)/dt, is generally a linear (i.e., first-order)function of the compartmental tracer contents, F(i,t) andF(j,t), yielding a set of coupled linear differential equa-tions (i.e., a=b=1) and a so-called linear model.
When solved, the time-dependent amount of tracer incompartment i, F(i,t), is represented by a sum of exponen-tials.
2. MAb nonlinear compartment models
In a compartmental model of systemically administeredantibody, the finite antigen concentration and the resultingsaturability of antigenic binding sites requires a non-linearcompartmental model (i.e., a set of coupled differentialequations including at least one non-linear differentialequation), since the rates of association of the antigen andantibody and of dissociation of the antigen-antibody com-plex are not constant but dependent on the instantaneousconcentrations of antigen, antibody, and antibody-antigencomplex.57,58 If “Ag,” “Ab,” and “AgAb” represent anti-gen, antibody, and antibody-antigen complex, respectively,then the antigen-antibody interaction can be representedby the following chemical reaction, characteristic of revers-ible bimolecular binding reactions:
where k+ 1 is the association rate constant (e.g., in h - 1
M -1), that is, the fractional amount of antibody binding toantigen per unit time per unit concentration of antigen andk -1 is the dissociation rate constant (e.g., in h - 1), that is,the fractional amount of antibody-antigen complex disso-ciating into free antigen and antibody per unit time.
Accordingly, the gross rate of antibody binding to anti-gen to form the antibody-antigen complex and the grossrate of dissociation of the antibody-antigen complex toyield free antibody and antigen are given by Eqs. (10) and(11), respectively. (It is important to note that Eqs. (10)and (11) represent the gross, not the net [as is usuallypresented], binding and dissociation rates, respectively andpresented to demonstrate the mathematical relationshipbetween conventional antigen-antibody binding parametersand compartmental model exchange rates.):
where [Ab] is the concentration (e.g., in M) of free anti-body, [Ag] is the concentration (e.g., in M) of free antigen,and [AbAg] is the concentration (e.g., in M) of antibody-antigen complex.
Equations (10) and (11) can be re-arranged to yieldEqs. (12) and (13), respectively, giving the fractional ratesof antibody binding to antigen and of dissociation of theantibody-antigen complex:
If one now identifies a free antibody compartment and abound antibody (i.e., an antibody-antigen complex) com-partment, then the free antibody-to-bound antibody andthe bound antibody-to-free antibody exchange rates aregiven, by definition, by Eqs. (12) and (13), respectively.Because the free antigen concentration is not constant, thefree antibody-to-bound antibody exchange rate is not con-stant [Eq. (12)] and a nonlinearity is thereby introduced.Nonetheless, Eq. (11) can be reformulated entirely interms of evaluable quantities to yield a time-varying ex-pression for the gross free antibody-to-bound antibody ex-change rate:
where [Ag]0 is the total antigen concentration (e.g., in M)in the antigen-positive tissue, F[AbAg,t] is the amount ofantibody (e.g., in mole) in the bound antibody compart-ment, and Vd is the volume of distribution (e.g., in l) of theantibody in the antigen-positive tissue. (This may be ap-proximated by the total volume or, preferably, the extra-cellular water volume of the antigen-positive tissue.)
Note that if the amount of administered antibody issufficiently small, the total concentration of antigen, [Ag] 0,will greatly exceed the concentration of antibody-antigencomplex, [AbAg] = F(AbAg,t)/Vd. It is mathematically ob-vious that the gross exchange rate of antibody binding toantigen is thus essentially constant and the overall com-partmental model is thereby linearized.
3. Compartment model solution
To “solve” a compartmental model, that is, to derive acompartmental model for which discrete values of the cal-culated compartmental contents, F(i,t), agree with thecorresponding experimental data, within the respective un-certainty of each datum, the number of compartments andthe values of the exchange rates, L(i,j,t), must be deter-mined. There is actually no unique solution for a given setof experimental data since any compartmental model canbe enlarged beyond the “resolution” possible from the data
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
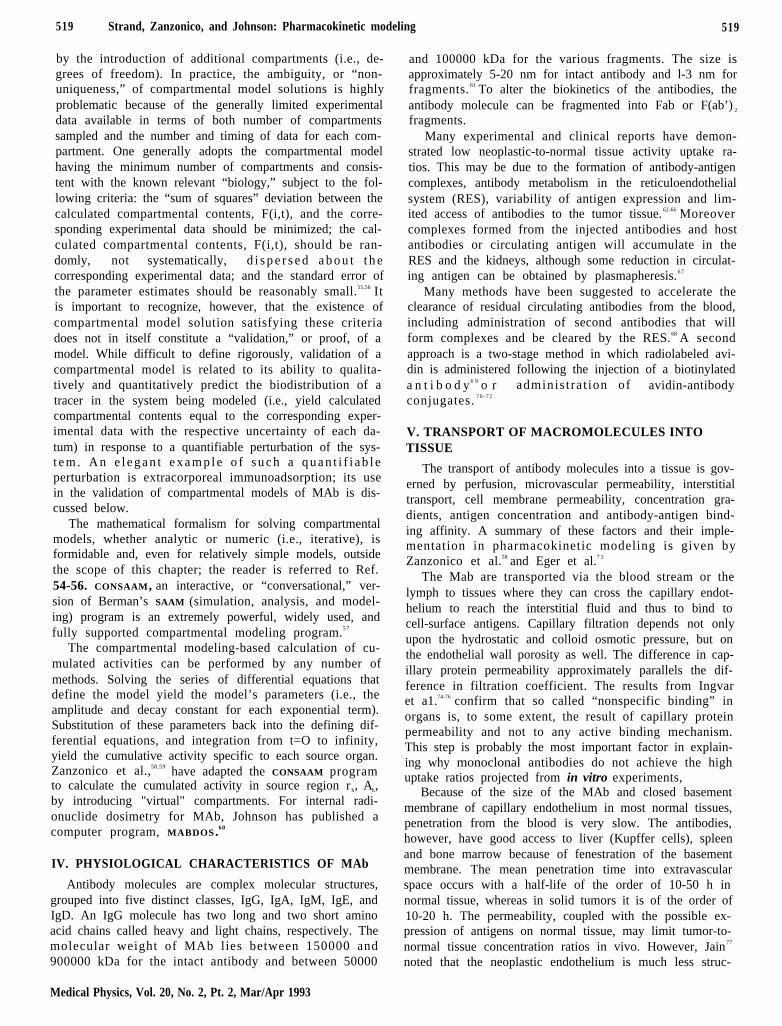
519 Strand, Zanzonico, and Johnson: Pharmacokinetic modeling 519
by the introduction of additional compartments (i.e., de-grees of freedom). In practice, the ambiguity, or “non-uniqueness,” of compartmental model solutions is highlyproblematic because of the generally limited experimentaldata available in terms of both number of compartmentssampled and the number and timing of data for each com-partment. One generally adopts the compartmental modelhaving the minimum number of compartments and consis-tent with the known relevant “biology,” subject to the fol-lowing criteria: the “sum of squares” deviation between thecalculated compartmental contents, F(i,t), and the corre-sponding experimental data should be minimized; the cal-culated compartmental contents, F(i,t), should be ran-domly, not systematically, d i s p e r s e d a b o u t t h ecorresponding experimental data; and the standard error ofthe parameter estimates should be reasonably small.55,56 Itis important to recognize, however, that the existence ofcompartmental model solution satisfying these criteriadoes not in itself constitute a “validation,” or proof, of amodel. While difficult to define rigorously, validation of acompartmental model is related to its ability to qualita-tively and quantitatively predict the biodistribution of atracer in the system being modeled (i.e., yield calculatedcompartmental contents equal to the corresponding exper-imental data with the respective uncertainty of each da-tum) in response to a quantifiable perturbation of the sys-t e m . A n e l e g a n t e x a m p l e o f s u c h a q u a n t i f i a b l eperturbation is extracorporeal immunoadsorption; its usein the validation of compartmental models of MAb is dis-cussed below.
The mathematical formalism for solving compartmentalmodels, whether analytic or numeric (i.e., iterative), isformidable and, even for relatively simple models, outsidethe scope of this chapter; the reader is referred to Ref.54-56. CONSAAM, an interactive, or “conversational,” ver-sion of Berman’s SAAM (simulation, analysis, and model-ing) program is an extremely powerful, widely used, andfully supported compartmental modeling program.5 7
The compartmental modeling-based calculation of cu-mulated activities can be performed by any number ofmethods. Solving the series of differential equations thatdefine the model yield the model’s parameters (i.e., theamplitude and decay constant for each exponential term).Substitution of these parameters back into the defining dif-ferential equations, and integration from t=O to infinity,yield the cumulative activity specific to each source organ.Zanzonico et al.,58,59 have adapted the CONSAAM programto calculate the cumulated activity in source region rh, Ah,by introducing "virtual" compartments. For internal radi-onuclide dosimetry for MAb, Johnson has published acomputer program, MABDOS.60
IV. PHYSIOLOGICAL CHARACTERISTICS OF MAb
Antibody molecules are complex molecular structures,grouped into five distinct classes, IgG, IgA, IgM, IgE, andIgD. An IgG molecule has two long and two short aminoacid chains called heavy and light chains, respectively. Themolecular weight of MAb lies between 150000 and900000 kDa for the intact antibody and between 50000
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
and 100000 kDa for the various fragments. The size isapproximately 5-20 nm for intact antibody and l-3 nm forfragments. 61 To alter the biokinetics of the antibodies, theantibody molecule can be fragmented into Fab or F(ab’) 2
fragments.Many experimental and clinical reports have demon-
strated low neoplastic-to-normal tissue activity uptake ra-tios. This may be due to the formation of antibody-antigencomplexes, antibody metabolism in the reticuloendothelialsystem (RES), variability of antigen expression and lim-ited access of antibodies to the tumor tissue. 62-66 Moreovercomplexes formed from the injected antibodies and hostantibodies or circulating antigen will accumulate in theRES and the kidneys, although some reduction in circulat-ing antigen can be obtained by plasmapheresis.6 7
Many methods have been suggested to accelerate theclearance of residual circulating antibodies from the blood,including administration of second antibodies that willform complexes and be cleared by the RES.68 A secondapproach is a two-stage method in which radiolabeled avi-din is administered following the injection of a biotinylateda n t i b o d y6 9 o r adminis t ra t ion of avidin-antibodyconjugates. 7 0 - 7 2
V. TRANSPORT OF MACROMOLECULES INTOTISSUE
The transport of antibody molecules into a tissue is gov-erned by perfusion, microvascular permeability, interstitialtransport, cell membrane permeability, concentration gra-dients, antigen concentration and antibody-antigen bind-ing affinity. A summary of these factors and their imple-mentation in pharmacokinetic modeling is given byZanzonico et al.58 and Eger et al.7 3
The Mab are transported via the blood stream or thelymph to tissues where they can cross the capillary endot-helium to reach the interstitial fluid and thus to bind tocell-surface antigens. Capillary filtration depends not onlyupon the hydrostatic and colloid osmotic pressure, but onthe endothelial wall porosity as well. The difference in cap-illary protein permeability approximately parallels the dif-ference in filtration coefficient. The results from Ingvaret a1.74-76 confirm that so called “nonspecific binding” inorgans is, to some extent, the result of capillary proteinpermeability and not to any active binding mechanism.This step is probably the most important factor in explain-ing why monoclonal antibodies do not achieve the highuptake ratios projected from in vitro experiments,
Because of the size of the MAb and closed basementmembrane of capillary endothelium in most normal tissues,penetration from the blood is very slow. The antibodies,however, have good access to liver (Kupffer cells), spleenand bone marrow because of fenestration of the basementmembrane. The mean penetration time into extravascularspace occurs with a half-life of the order of 10-50 h innormal tissue, whereas in solid tumors it is of the order of10-20 h. The permeability, coupled with the possible ex-pression of antigens on normal tissue, may limit tumor-to-normal tissue concentration ratios in vivo. However, Jain77
noted that the neoplastic endothelium is much less struc-
520 Strand, Zanzonico, and Johnson: Pharmacokinetic modeling 520
tured and has a higher probability of being more permeableto macromolecules than normal tissue endothelia.
In the study of Covell et al. the transcapillary move-ment of antibodies was greatest in the lung, liver andspleen with the values 0.53, 0.35 and 0.20 ml min -1 g - 1,respectively. For other organs, the values are: kidney, 0.09,gut, 0.006, and carcass (skin, bone and muscle), 0.0003m l m i n- 1 g - 1. A comparison was also made with otherdata79 in which the transport of Dextrans with differentmolecular weights (equivalent Stoke’s radii for whole IgGand fragments) had been measured: Dextran (110000),0 .0023 ml /min and IgG, 0 .0036 ml /min; Dext ran(20000)) 0.0061 ml/min and F(ab’)2, 0.0041 ml/min; andDextran (10000), 0.029 ml/min and Fab’, 0.050 ml/min.
The red bone marrow is characterized by large pores(<100nm) and allows free flow of plasma through themarrow parenchyma and rapid (i.e., within minutes afteri.v. injection) equilibration of large molecules. It wasfound that there is rapid, high uptake of labeled antibodiesin the bone marrow.80-82
These considerations were incorporated into a whole-body compartmental model of systemically administeredradioiodinated MAb, where Zanzonico et al.58 postulated a“rapidly exchanging tissue” (most visceral tissue) with anexchange rate constant from the vascular space to the ex-travascular space of the order of 0.07 h - 1. For a “slowlyexchanging tissue” (most nonvisceral tissue), a rate con-stant of 0.02 h-1 was assumed. Plasma and reticuloendot-helial tissue (bone marrow, lymph nodes, and spleen) werecombined into one compartment due to the rapid equili-bration of plasma-borne antibodies with these tissues; forclarification, the reader is referred to the definition of a“compartment” presented above.
VI. TUMOR MAb UPTAKE
Human tumors and cultured human cells express anti-genic heterogeneity, perhaps related to cell size, cell func-tion, stage of cell cycle, invasiveness, etc. This will result ina very uneven antibody distribution.8 3
Ingvar et al.8 4 showed that in 58 metastases from 27patients with malignant melanoma, evaluated by immuno-histochemistry and three different MAb’s, all of the me-tastases were positive for at least one of the three antibod-ies. In 15 patients where more than one metastases wasremoved, four patients showed both positive and negativestaining for two of the antibodies, in different metastases.In autoradiographic studies large variations in the activitydistribution within tumors has been observed.85-89
In a number of studies, it has been shown that thereexists an inverse relationship between the specific tumorantibody uptake and tumor mass.90-96 Data from the Lundgroup9 6 for different labeling methods show such an in-verse relationship for specific antibodies, whereas for un-specific antibodies, uptake is unrelated to the tumor size.These results are in accordance with Cheung et al. 92 I ncontrast, however, Williams et al.93 showed such a rela-tionship for unspecific antibodies.
An explanation for these observations may be related totumor surface area,91 geometry of tumor blood flow,93 or
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
surface vascularization of tumor.94 Although all of thesedata have been obtained in animals, there is evidence forthe same phenomenon occurring in man.
VII. MICROSCOPIC PHARMACOKINETIC MODELS
The principal factor affecting a favorable diffusion ofantibodies into tumors is the concentration gradient.9 7
Theoretical studies of MAb penetration into tumors havebeen undertaken by Weinstein et al.97-99 They have devel-oped a mathematical model incorporating capillary trans-port, tumor interstitial diffusion and antigen-antibody in-teraction. The time varying plasma concentration of MAbis also modeled. The results have been evaluated as totaland free MAb distribution profiles, average total MAb con-centration, and an index of nonuniformity of MAb distri-bution. They have found a “binding-site barrier” causing aheterogeneous MAb distribution within the tumor nodulebecause of retarding of the free MAb entering the nodule.They also observed that a high affinity gives a high MAbconcentration close to the capillaries but with no increasein the average concentration. Also, decreasing theantibody-antigen binding affinity will result in a small de-crease in average concentration, but will improve the per-colation for a given MAb concentration. In addition byincreasing the MAb concentration in plasma the “binding-site barrier” could by overcome at the expense of loweruptake ratios between tumor and normal tissues. Aspointed out by the authors this is strictly a theoreticalmodel with no experimental verification. However, it sug-gests possible investigations on the micropharmacologicallevel are necessary for a better understanding of MAb be-havior and therapeutic results. Combined with dosimetriccalculations, such a mathematical model may lead to ab-sorbed dose profiles within tumors.
VIII. MACROSCOPIC PHARMACOKINETIC MODELS
A. Human models
As noted, a whole-body compartmental model forsystemically administered radioiodinated antibody hasbeen developed by Zanzonico et a1.58 based on theoreticalphysiological considerations and literature data (Fig. 1). Itcomprises a MAb-nonspecific part with “rapid” and“slowly” exchangeable tissue compartments, and a“humped” compartment of plasma and RES with a livercompartment responsible for the rapid uptake of damagedantibodies. The model also includes a MAb-specific bind-ing part with nonlinear exchange rates dependent on theAg concentration. Thus compartments for tumor and nor-mal tissue with free and bound Ab are included. Tumor isrepresented as a rapidly exchanging tissue. Additionally acompartment with lumped plasma and RES to model cir-culating antigen-antibody complexes is included. Finallycatabolism and deiodination were treated in a coupled lin-ear compartment model for iodine kinetics. With thismodel (see Fig. 1) the influence of administered amount ofantibody and size of tumor on the distribution of Ab-Agcomplexes in plasma, normal tissue and tumor were inves-tigated. The theoretical model was then simplified (exclud-
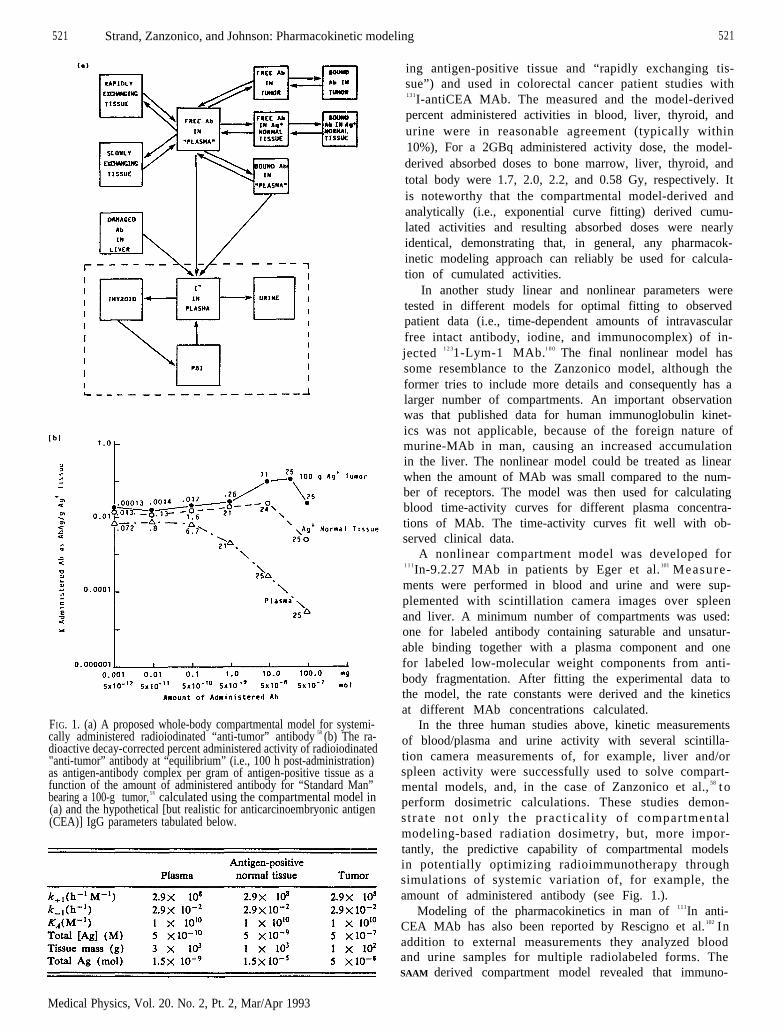
521 Strand, Zanzonico, and Johnson: Pharmacokinetic modeling 521
FIG. 1. (a) A proposed whole-body compartmental model for systemi-cally administered radioiodinated “anti-tumor” antibody 58 (b) The ra-dioactive decay-corrected percent administered activity of radioiodinated"anti-tumor” antibody at “equilibrium” (i.e., 100 h post-administration)as antigen-antibody complex per gram of antigen-positive tissue as afunction of the amount of administered antibody for “Standard Man”bearing a 100-g tumor, 5 8 calculated using the compartmental model in(a) and the hypothetical [but realistic for anticarcinoembryonic antigen(CEA)] IgG parameters tabulated below.
Medical Physics, Vol. 20. No. 2, Pt. 2, Mar/Apr 1993
ing antigen-positive tissue and “rapidly exchanging tis-sue”) and used in colorectal cancer patient studies with131I-antiCEA MAb. The measured and the model-derivedpercent administered activities in blood, liver, thyroid, andurine were in reasonable agreement (typically within10%), For a 2GBq administered activity dose, the model-derived absorbed doses to bone marrow, liver, thyroid, andtotal body were 1.7, 2.0, 2.2, and 0.58 Gy, respectively. Itis noteworthy that the compartmental model-derived andanalytically (i.e., exponential curve fitting) derived cumu-lated activities and resulting absorbed doses were nearlyidentical, demonstrating that, in general, any pharmacok-inetic modeling approach can reliably be used for calcula-tion of cumulated activities.
In another study linear and nonlinear parameters weretested in different models for optimal fitting to observedpatient data (i.e., time-dependent amounts of intravascularfree intact antibody, iodine, and immunocomplex) of in-jected 1 2 31-Lym-1 MAb.1 0 0 The final nonlinear model hassome resemblance to the Zanzonico model, although theformer tries to include more details and consequently has alarger number of compartments. An important observationwas that published data for human immunoglobulin kinet-ics was not applicable, because of the foreign nature ofmurine-MAb in man, causing an increased accumulationin the liver. The nonlinear model could be treated as linearwhen the amount of MAb was small compared to the num-ber of receptors. The model was then used for calculatingblood time-activity curves for different plasma concentra-tions of MAb. The time-activity curves fit well with ob-served clinical data.
A nonlinear compartment model was developed for1 1 1In-9.2.27 MAb in patients by Eger et al. 101 Measure-ments were performed in blood and urine and were sup-plemented with scintillation camera images over spleenand liver. A minimum number of compartments was used:one for labeled antibody containing saturable and unsatur-able binding together with a plasma component and onefor labeled low-molecular weight components from anti-body fragmentation. After fitting the experimental data tothe model, the rate constants were derived and the kineticsat different MAb concentrations calculated.
In the three human studies above, kinetic measurementsof blood/plasma and urine activity with several scintilla-tion camera measurements of, for example, liver and/orspleen activity were successfully used to solve compart-mental models, and, in the case of Zanzonico et al., 58 t operform dosimetric calculations. These studies demon-stra te not only the pract ical i ty of compartmentalmodeling-based radiation dosimetry, but, more impor-tantly, the predictive capability of compartmental modelsin potentially optimizing radioimmunotherapy throughsimulations of systemic variation of, for example, theamount of administered antibody (see Fig. 1.).
Modeling of the pharmacokinetics in man of 111In anti-CEA MAb has also been reported by Rescigno et al. 102 Inaddition to external measurements they analyzed bloodand urine samples for multiple radiolabeled forms. TheSAAM derived compartment model revealed that immuno-
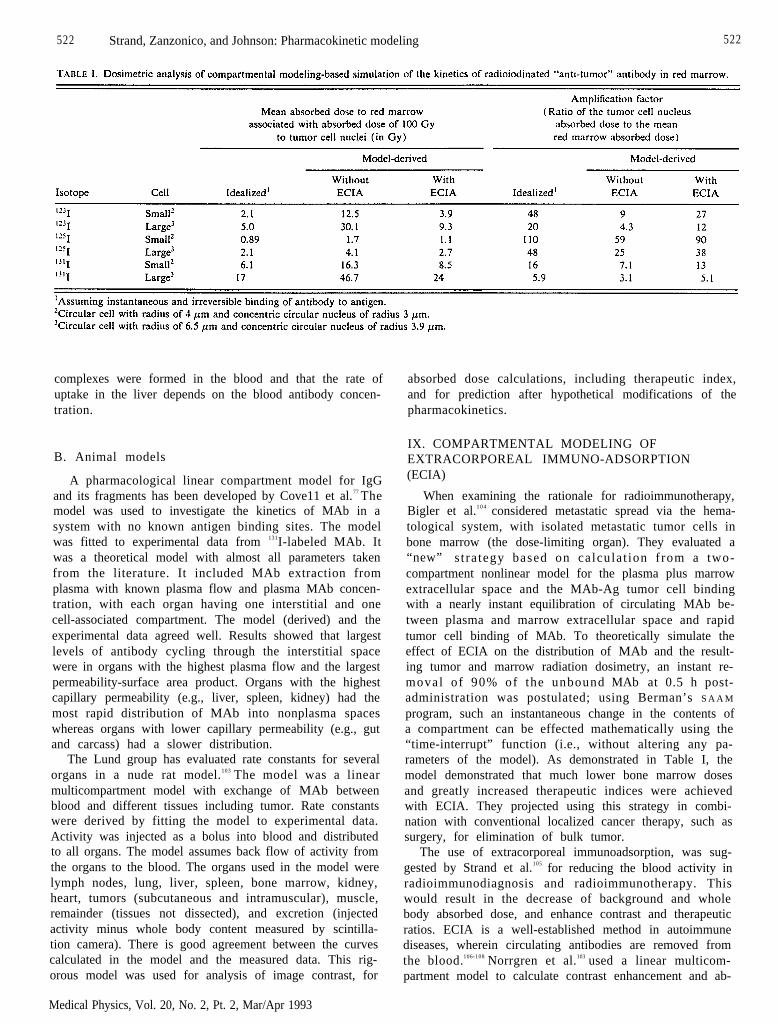
522 Strand, Zanzonico, and Johnson: Pharmacokinetic modeling 522
complexes were formed in the blood and that the rate ofuptake in the liver depends on the blood antibody concen-tration.
B. Animal models
A pharmacological linear compartment model for IgGand its fragments has been developed by Cove11 et al.77 Themodel was used to investigate the kinetics of MAb in asystem with no known antigen binding sites. The modelwas fitted to experimental data from 131I-labeled MAb. Itwas a theoretical model with almost all parameters takenfrom the literature. It included MAb extraction fromplasma with known plasma flow and plasma MAb concen-tration, with each organ having one interstitial and onecell-associated compartment. The model (derived) and theexperimental data agreed well. Results showed that largestlevels of antibody cycling through the interstitial spacewere in organs with the highest plasma flow and the largestpermeability-surface area product. Organs with the highestcapillary permeability (e.g., liver, spleen, kidney) had themost rapid distribution of MAb into nonplasma spaceswhereas organs with lower capillary permeability (e.g., gutand carcass) had a slower distribution.
The Lund group has evaluated rate constants for severalorgans in a nude rat model.103 The model was a linearmulticompartment model with exchange of MAb betweenblood and different tissues including tumor. Rate constantswere derived by fitting the model to experimental data.Activity was injected as a bolus into blood and distributedto all organs. The model assumes back flow of activity fromthe organs to the blood. The organs used in the model werelymph nodes, lung, liver, spleen, bone marrow, kidney,heart, tumors (subcutaneous and intramuscular), muscle,remainder (tissues not dissected), and excretion (injectedactivity minus whole body content measured by scintilla-tion camera). There is good agreement between the curvescalculated in the model and the measured data. This rig-orous model was used for analysis of image contrast, for
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
absorbed dose calculations, including therapeutic index,and for prediction after hypothetical modifications of thepharmacokinetics.
IX. COMPARTMENTAL MODELING OFEXTRACORPOREAL IMMUNO-ADSORPTION(ECIA)
When examining the rationale for radioimmunotherapy,Bigler et al.1 0 4 considered metastatic spread via the hema-tological system, with isolated metastatic tumor cells inbone marrow (the dose-limiting organ). They evaluated a“new” stra tegy based on calculat ion f rom a two-compartment nonlinear model for the plasma plus marrowextracellular space and the MAb-Ag tumor cell bindingwith a nearly instant equilibration of circulating MAb be-tween plasma and marrow extracellular space and rapidtumor cell binding of MAb. To theoretically simulate theeffect of ECIA on the distribution of MAb and the result-ing tumor and marrow radiation dosimetry, an instant re-moval of 90% of the unbound MAb at 0.5 h post-administration was postulated; using Berman’s S A A M
program, such an instantaneous change in the contents ofa compartment can be effected mathematically using the“time-interrupt” function (i.e., without altering any pa-rameters of the model). As demonstrated in Table I, themodel demonstrated that much lower bone marrow dosesand greatly increased therapeutic indices were achievedwith ECIA. They projected using this strategy in combi-nation with conventional localized cancer therapy, such assurgery, for elimination of bulk tumor.
The use of extracorporeal immunoadsorption, was sug-gested by Strand et al.105 for reducing the blood activity inradioimmunodiagnosis and radioimmunotherapy. Thiswould result in the decrease of background and wholebody absorbed dose, and enhance contrast and therapeuticratios. ECIA is a well-established method in autoimmunediseases, wherein circulating antibodies are removed fromthe blood.106-108 Norrgren et al.103 used a linear multicom-partment model to calculate contrast enhancement and ab-
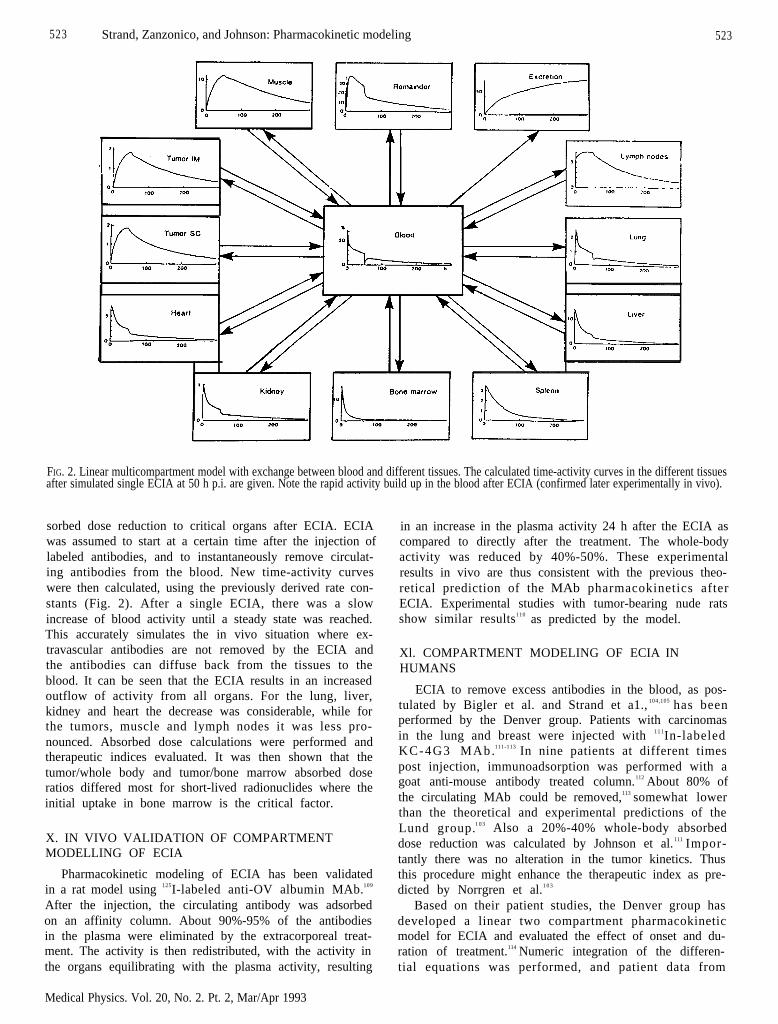
523 Strand, Zanzonico, and Johnson: Pharmacokinetic modeling 523
FIG. 2. Linear multicompartment model with exchange between blood and different tissues. The calculated time-activity curves in the different tissuesafter simulated single ECIA at 50 h p.i. are given. Note the rapid activity build up in the blood after ECIA (confirmed later experimentally in vivo).
sorbed dose reduction to critical organs after ECIA. ECIAwas assumed to start at a certain time after the injection oflabeled antibodies, and to instantaneously remove circulat-ing antibodies from the blood. New time-activity curveswere then calculated, using the previously derived rate con-stants (Fig. 2). After a single ECIA, there was a slowincrease of blood activity until a steady state was reached.This accurately simulates the in vivo situation where ex-travascular antibodies are not removed by the ECIA andthe antibodies can diffuse back from the tissues to theblood. It can be seen that the ECIA results in an increasedoutflow of activity from all organs. For the lung, liver,kidney and heart the decrease was considerable, while forthe tumors, muscle and lymph nodes it was less pro-nounced. Absorbed dose calculations were performed andtherapeutic indices evaluated. It was then shown that thetumor/whole body and tumor/bone marrow absorbed doseratios differed most for short-lived radionuclides where theinitial uptake in bone marrow is the critical factor.
X. IN VIVO VALIDATION OF COMPARTMENTMODELLING OF ECIA
Pharmacokinetic modeling of ECIA has been validatedin a rat model using 125I-labeled anti-OV albumin MAb.109
After the injection, the circulating antibody was adsorbedon an affinity column. About 90%-95% of the antibodiesin the plasma were eliminated by the extracorporeal treat-ment. The activity is then redistributed, with the activity inthe organs equilibrating with the plasma activity, resulting
Medical Physics. Vol. 20, No. 2. Pt. 2, Mar/Apr 1993
in an increase in the plasma activity 24 h after the ECIA ascompared to directly after the treatment. The whole-bodyactivity was reduced by 40%-50%. These experimentalresults in vivo are thus consistent with the previous theo-retical prediction of the MAb pharmacokinetics afterECIA. Experimental studies with tumor-bearing nude ratsshow similar results110 as predicted by the model.
Xl. COMPARTMENT MODELING OF ECIA INHUMANS
ECIA to remove excess antibodies in the blood, as pos-tulated by Bigler et al. and Strand et a1., 104,105 has beenperformed by the Denver group. Patients with carcinomasin the lung and breast were injected with 1 1 1In-labeledKC-4G3 MAb.111-113 In nine patients at different timespost injection, immunoadsorption was performed with agoat anti-mouse antibody treated column.112 About 80% ofthe circulating MAb could be removed,113 somewhat lowerthan the theoretical and experimental predictions of theLund group.1 0 3 Also a 20%-40% whole-body absorbeddose reduction was calculated by Johnson et al.111 Impor-tantly there was no alteration in the tumor kinetics. Thusthis procedure might enhance the therapeutic index as pre-dicted by Norrgren et al.1 0 3
Based on their patient studies, the Denver group hasdeveloped a linear two compartment pharmacokineticmodel for ECIA and evaluated the effect of onset and du-ration of treatment.114 Numeric integration of the differen-tial equations was performed, and patient data from

524 Strand, Zanzonico, and Johnson: Pharmacokinetic modelling 524
plasma and adsorption column were fit to the model toobtain the unknown model parameters. The model wasthen used to simulate plasma and ECIA-column data. Val-idation of the model was performed by adding noise tosimulated time-activity curves and compared to patientdata for goodness of fit. Statistical analysis indicated thatthe model was reliable. Their model predicted the observedredistribution of activity after ECIA. No data for tumorwas evaluated.
These results illustrate the usefulness of pharmacoki-netic modeling for predictive calculations and for furtheruse in dosimetric calculations.
XII. SUMMARY
In general, any pharmacokinetic modeling approachcan reliably be used for reduction of kinetic data to cumu-lated activities. However, among the many potential ad-vantages of compartmental analysis-based pharmacoki-netic modeling and cumulated activity calculation are thefollowing. Available biological data (e.g., independentlydetermined antibody-antigen binding parameters in thecase of radiolabeled MAb) may be incorporated into acompartmental model, constraining the model (i.e., mini-mizing the degrees of freedom), and thereby improving theoverall “goodness of fit” compared to curve fitting. “Con-servation of mass” is implicitly incorporated into a com-partmental model, also constraining the model, andthereby likewise improving the overall “goodness of fit.”Otherwise indeterminable cumulated activities in non-sampled microscopic source regions (e.g., extracellularspace, cell surface, cytoplasm, and nucleoplasm) can bededuced. It is now clear that the activity, cumulated activ-ity, and absorbed dose distributions of systemically admin-istered radiolabeled MAb in tissue, particularly antigen-positive tissue such as tumor, is microscopically as well asmacroscopically nonuniform.116-122 And, perhaps most im-portantly, parameters of validated compartment modelscan be systematically varied to elucidate the magnitude ofthe effect of such variations on the pharmacokinetics of thetracer and to determine optimum model parameter values(e.g., to maximize the tumor-to-normal tissue activity con-centration ratios in the case of radioimmunotherapy) 5 8’115
and optimum timing and frequency of data acquisition.Simulated “parameter variation” studies can thus assist inprioritizing research efforts (by identifying which modelparameters most dramatically affect the radiotracer tissuedistribution) and predicting the effects of various patholo-gies and other conditions on the outcome of future studies.
In practice (especially clinical practice), however, com-partmental analysis-based pharmacokinetic modeling andcumulated activity calculation is problematic. Besides be-ing computer- and effort-intensive, a compartmental modelmust be formulated and validated. In addition, for com-partmental models as large and complex as those for sys-temically administered radiolabeled MAb58,100 and for thegenerally sparse kinetic data available in clinical studies,the uncertainty of the model parameters and therefore ofany model-derived quantities (e.g., cumulated activities)may be prohibitively large. Nonetheless, absolute time-
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
activity measurements of blood and/or plasma, solid tu-mors, one or more major organs, and the total body can beperformed in patients. Together with the in vitro measure-ment of the antigen-antibody binding parameters (whichshould be part of the preclinical evaluation of all MAbundergoing clinical testing), the necessary input data forsolution of a compartmental model should be available.Compartmental modeling software and the necessary com-puter hardware are now almost universally available inacademic medical centers. Thus, as discussed above, com-partmental analysis-based pharmacokinetic modeling andcumulated activity distribution are a practical reality.
XIII. CONCLUSION
In concert with continuing efforts to find more tumor-specific MAb, more reliable and predictive modeling tech-niques and specific models of both microscopic and mac-roscopic pharmacokinetics must be pursued. Some of theresearch areas to be addressed are more accurate and pre-cise data on macroscopic and microscopic activity distri-butions measured in vivo, absolute quantitation of kineticdata in clinical trials, and for the purpose of compartmen-tal models, kinetic measurements under quantifiably per-turbated conditions in vivo.
ACKNOWLEDGMENTS
This study has been supported by grants from John andAugusta Perssons Foundation for Medical Research,Lund, Swedish National Cancer Society, Grant No. 2353-B91-05XAB, Swedish National Board for Technical De-velopment, Grant No. 90-01878P, Mrs. Berta Kamprad’sFoundation, Lund, Sweden, Nilssons’ Foundation, Hels-ingborg, Sweden and U.S. National Cancer Institute, Con-tract N01-CM37565.
APPENDIX I
In the completely general development of the analytictheory of linear compartmental systems, the solution to asystem of linear differential equations with constant coef-ficients is exponential of the form q=ue λ t, u being the con-stant vector. q=ue λ t is a solution if A is an eigenvalue of fand u is the corresponding eigenvector (i.e., fu= λ u). Con-vention has deemed that the appearance of substance in acompartment is assigned to be positive, the disappearanceof substance to be negative. Thus we see that the eigenvalueλ1 for a simple two compartment system, with materialleaving compartment 1 and entering compartment 2, to beequal to -ƒ2 1. - ƒ21 is the rate at which substance leavescompartment 1 and enters compartment 2. The generalsolution for this model is given by q=ue λ t where λ is neg-ative and equal to -ƒ2 1.
1 2 3
525 Strand, Zanzonico, and Johnson: Pharmacokinetic modeling 525
1P. B. Zanzonico, C. Edwards, F. Sgouros. A. Strauss, R. E. Bigler, J. R.Hurley, and D. V. Becker, “Practical dosimetry: Quantitative imagingin radionuclide therapy, ” in Dosimetry of Administered Radionuclides,edited by S. J. Adelstein, A. I. Kassis. and R. W. Burt (Society ofNuclear Medicine-American College of Nuclear Physicians JointSymposium, Frontiers in Nuclear Medicine Series, Washington, DC,Department of Energy, September 21-22. 1989), pp. 275-294.
2J. R. Watts, R. E. Johnson, and A. Brill. “Methods of approach toproblems of absolute quantitation of radioactivity distributions in hu-mans,” J. Nucl. Med. 11, 374 (Abstract) (1970).
3J. A. Sorenson, “Quantitation of radioactive content in vivo using com-bined emission-transmission,” J. Nucl. Med. 11, 401 (1970) (Ab-stract).
4L. P. Clarke, J. S. Laughlin, and K. Mayer, “Quantitative organ-uptakemeasurements,” Radiology 102, 375-382 (1972).
5S. L. Graham and R. Neil, “In vivo quantitation using the Angercamera,” Radiology 112, 441-442 (1974).
6J. A. Sorenson, “Quantitative measurement of radioactivity in vivo bywhole-body counting,” in Instrumentation in Nuclear Medicine, editedby G. J. Hine and J. A. Sorenson (Academic, New York, 1974), Vol.2, pp. 31 1-348.
7T. F. Budinger, “Quantitative nuclear medicine imaging: Applicationsof computers to the gamma camera and whole-body scanning,” in Re-cent Advances in Nuclear Medicine, Progress in Atomic Medicine, editedby J. H. Lawrence (Grune and Stratton, New York, 1974), Vol. 4, pp.41-130.
8S. R. Thomas, H. R. Maxon, J. G. Kereiakes, and E. L. Saenger,“Quantitative external counting techniques enabling improved diagnos-tic and therapeutic decisions in patients with well-differentiated thyroidcancer,” Radiology 122, 731-737 (1977).
9A. Ferrant and F. Cauwe, “Quantitative organ-uptake measurementwith a gamma camera,” Eur. J. Nucl. Med. 4, 223-229 (1979).
10J. S. Fleming, “A technique for the absolute measurement of activityusing a gamma camera and computer,” Phys. Med. Biol. 24, 176-180(1979).
11S.R Thomas, H. R. Maxon, and J. G. Kereiakes, “In vivo quantitationof lesion radioactivity using external counting methods,” Med. Phys. 3,253-255 (1976).
1 2M. J. Myers, J. P. Lavender, J. B. de Oliveira, and A. Maseri, “Asimplified method of quantitating organ uptake using a gamma cam-era,” Br. J. Radiol. 54, 1062-1067 (1981).
13D. J. Macey and R. Marshall, “Absolute quantitation of radiotraceruptake in lungs using a gamma camera,” J. Nucl. Med. 23, 731-735(1981).
14S. R. Thomas, M. J. Gelfan, G. S. Bums, R. C. Purdom, J. G. Kere-iakes, and H. R. Maxon, “Radiation absorbed-dose estimates for theliver, spleen, and metaphyseal growth complexes in children undergo-ing gallium-67 citrate scanning,” Radiology 146, 817-820 (1983).
15M. D. Hammond, P. J. Moldofsky, M. R. Beardsley, and C. B. Mul-hem, Jr., “External imaging techniques for quantitation of distributionof I-131 F(ab’)2 fragments of monoclonal antibody in humans,” Med.Phys. 11, 778-783 (1984).
1 6R. K. Wu and J. A. Siegel, “Absolute quantitation of radioactivityusing the buildup factor,” Med. Phys. 11, 189-192 (1984).
1 7L. W. Grossman, M. Fernandes-Ulloa, S. J. Lukes. and J. Mantil,“Gallium-67 lung uptake: Conjugate-view counting,” Radiology 157,789-793 (1985).
18K. A. Lathrop, R. D. Bartlett, C. T. Chen, J. S. Chou, P. F. Faulhaber,P. V. Harper, and V. J. Stark, “Quantitative clinical uptake measure-ments using conjugate counting,” in Proceedings of the Fourth Interna-tional Symposium on Radiopharmaceutical Dosimetry, edited by A. T.Shlafke-Stelson and E. Watson [U.S. Department of Energy,DE86010102 (CONF-851113), Oak Ridge, TN, 1985], pp. 135-147.
19P. Doherty, R. Schwinger, M. King, and M. Gionet, “Distribution anddosimetry of indium-111 labeled F(ab’)2 fragments in humans,” in(Eds), Proceedings of the Fourth International Symposium on Radiop-harmaceutical Dosimetry, edited by A. T. Shlafka-Stelson and E. Wat-son [U.S. Department of Energy, DE86010102 (CONF-851113), OakRidge, TN, 1985], pp. 464-476.
20R. J. Jaszczak, K. L. Greer, and R. E. Coleman, “SPECT quantifica-tion of regional radionuclide distributions,” in Proceedings of theFourth International Symposium on Radiopharmaceutical Dosimetry,edited by A. T. Shlafke-Stelson and E. Watson [U.S. Department ofEnergy, DE86010102 (CONF-851113), Oak Ridge, TN, 1985],pp. 82-96.
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
21E. J. Hoffman, “Quantitation of radiopharmaceutical distributions foruse in dose estimates with positron emission tomography,” in Proceed-ings of the Fourth International Symposium on RadiopharmaceuticalDosimetry, edited by A. T. Shlafke-Stelson and E. Watson [U.S. De-partment of Energy, DE86010102 (CONF-851113), Oak Ridge, TN,1985], pp. 97-104.
22T. E. Budinger, S. E. Derenzo, W. L. Greenberg, G. T. Gullberg, andR. H. Huesman, “Quantitative potentials of dynamic emission com-puted tomography,” J. Nucl. Med. 19, 309-315 (1978).
23R. J. Jaszczak, R. E. Coleman, and F. R. Whitehead. “Physical factorsaffecting quantitative measurements using camera-based single photonemission computed tomography (SPECT),” IEEE Trans. Nucl. Sci.NS-28. 69-80 (1981).
2 4R. J. Jaszczak, K. L. Greer, C. E. Floyd, C. C. Harris, and R. E.Coleman, “Improved SPECT quantitation using compensation forscattered photons,” J. Nucl. Med. 25, 893-900 (1984).
25D. Osbom, R. I. Jaszczak. K. Greer, M. Lischko, and R. E. Coleman,“SPECT quantification of technetium-99m microspheres within the ca-nine lung,” J. Comput. Assist. Tomogr. 9, 73-77 ( 1985).
26D. Osbom, R. J. Jaszczak, R. E. Coleman, K. Greer, and M. Lischko,“In vivo regional quantitation of intrathoracic Tc-99 m using SPECT:Concise communication,” J. Nucl. Med. 23, 446-450 (1982).
27S. E. Strand, K. Norrgren, C. Ingvar, T. Brodin, L. Hallstadius, and M.Ljungberg, “Parameters required in a dose planning model for radio-immunotherapy,” in Radionuclides for Therapy, Bottsteiner ColloquiumIV (Villigen, Switzerland, 1986), pp. 75-90.
28M. Ljungberg and S. E. Strand, “Dose planning with SPECT,” Int. J.Cancer Suppl. 2, 67-70 (1988).
29M. Ljungberg and S. E. Strand, “Quantitative SPECT in oncologicalnuclear medicine: Application in dose planning for radionuclide ther-apy,” Hospimedica 6, 17-21 (1988).
30S. E. Strand and M. Ljungberg, “Absorbed dose planning in radionu-clide therapy based on quantitative SPECT,” Antib. Immunoconj. Ra-diopharm, 4, 673-680 ( 1991).
31L.T. Kircos, J. E. Carey, and J. W. Keyes, “Quantitative organ visu-alization using SPECT,” J. Nucl. Med. 28, 334-341 (1987).
32G. L. DeNardo, D. J. Macey, S. J. DeNardo, C. G. Zhang, and T. R.Custer, “Quantitative SPECT of uptake of monoclonal antibodies,”Semin. Nucl. Med. 19, 22-32 (1989).
33G. Iosilevsky, O. Israel, A. Frenkel, E. Even-Sapir, S. Ben-Haim, A.Front, G. M. Kolodny, and D. Front, “A practical technique for quan-titation of drug delivery to human tumors and organ absorbed radia-tion dose,” Semin. Nucl. Med. 19, 33-46 (1989).
34P. B. Zanzonico, R. E. Bigler, G. Sgouros, and A. Strauss, “Quantita-tive SPECT in radiation dosimetry,” Semin. Nucl. Med. 19, 47-61(1989).
35K. F. Koral, “Calculating radiation absorbed dose for pheochromocy-toma tumors in 131-I MIBG therapy,” Int. J. Oncol. Biol. Phys. 17,211-218 (1989).
16K. F. Koral, F. M. Swailem, S. Buchbinder, N. H. Clinthome, W. L.Rogers, and B. M. W. Tsui, “SPECT dual-energy-window Comptoncorrection: Scatter multiplier required for quantification,” J. Nucl.Med. 31, 90-98 (1990).
37R. Loevinger and M. Berman, “A schema for absorbed dose calcula-tions for biologically distributed radionuclides,” MIRD Pamphlet No1, J. Nucl. Med. 9 (Suppl. l), 7-14 (1968).
38R. Loevinger and M. Berman, “A schema for absorbed dose calcula-tions for biologically distributed radionuclides,” MIRD Pamphlet No1, Revised, Society of Nuclear Medicine, New York ( 1976).
39M. J. Berger, “Energy deposition in water by photons from point iso-tropic sources,” MIRD Pamphlet No. 2, J. Nucl. Med. 9 (Suppl. l),15-25 (1968).
40G. L. Brownell, W. H. Ellett, and A. R. Reddy, “Absorbed fractionsfor photon dosimetry,” MIRD Pamphlet No. 3, J. Nucl. Med. 9(Suppl. 1), 27-39 (1968).
41L.T. Dillman, “Radionuclide decay schemes and nuclear parametersfor use in radiation dose estimation,” MIRD Pamphlet No. 4, J. Nucl.Med. 10 (Suppl. 2), 5-32 (1969).
42W.S. Snyder, M. R. Ford, G. G. Warner, and H. L. Fisher Jr., “Es-timates of absorbed fractions for monoenergetic photon sources uni-formly distributed in various organs of a heterogeneous phantom,”MIRD Pamphlet No. 5, J. Nucl. Med. 10 (Suppl. 3), 5-52 (1969).
43W.S. Snyder, M. R. Ford, and G. G. Warner, “Estimates of absorbedfractions for monoenergetic photon sources uniformly distributed invarious organs of a heterogeneous phantom,” MIRD Pamphlet No. 5,
526 Strand, Zanzonico, and Johnson: Pharmacokinetic modeling 526
Revised, Society of Nuclear Medicine, New York ( 1978).44L. T. Dillman, “Radionuclide decay schemes and nuclear parameters
for use in radiation dose estimation,” Part 2, MIRD Pamphlet No. 6,J. Nucl. Med. 11 (Suppl. 4), 5-32 (1970).
45M. J. Berger, “Distribution of absorbed doses around point sources ofelectrons and beta particles in water and other media,” MIRD Pam-phlet No. 7, J. Nucl. Med. 12 (Suppl. 5), 5-23 (1971).
46W.H. Ellett and R. M. Humes, “Absorbed fractions for small volumescontaining photon-emitting radioactivity,” MIRD Pamphlet No. 8, J.Nucl. Med. 12 (Suppl. 5). 25-32 (1971).
47L. T. Dillman and F. C. Von der Lage, “Radionuclide decay schemesand nuclear parameters for use in radiation dose estimation,” MIRDPamphlet No. 10, Society of Nuclear Medicine, New York (1975).
4 8W.S. Snyder, M. R. Ford, G. G. Warner, and S. B. Watson, "'S',absorbed dose per unit cumulated activity for selected radionuclidesand organs,” MIRD Pamphlet No. 11, Society of Nuclear Medicine,New York (1975).
49M. Berman, “Kinetic models for absorbed dose calculations,” MIRDPamphlet No. 12, Society of Nuclear Medicine, New York (1977).
5 0International Commission on Radiation Units and Measurements,ICRU Rep. 32, “Methods of assessment of absorbed dose in clinical useof radionuclides,” Washington, D.C. (1979).
51The International Commission on Radiobiological Protection, ICRPPublication 53, Radiation Dose to Patients from Radiopharmaceuticals,Pergamon, Oxford, England, 1987.
52R. Loevinger, “Some remarks on the MIRD schema for absorbed-dosecalculations for biologically-distributed radionuclides,” in Medical Ra-dionuclides: Radiation Dose and Effects, AEC Symposium Series 20,edited by R. J. Cloutier, C. L. Edwards, and W. S. Snyder (Oak Ridge,TN, 1969), pp. 481-489.
53W. Per1 “A method for curve-fitting by exponential functions,” Int. J.Appl. Radiat. Isotopes 8, 211-222 ( 1960).
54R.A. Shipley and R. E. Clark, Tracer Methods for In Vivo Kinetics(Academic, New York, 1972).
55M. Berman, E. Shahn, and M. F. Weiss, “The routine fitting of kineticdata to models-A mathematical formalism for digital computers,”Biophys. J. 2, 275-287 ( 1962).
56M. Berman, M. Weiss, and E. Shahn, “Some formal approaches to theanalysis of kinetic data in terms of linear compartmental systems,”Biophys. J. 2, 289-298 (1962).
57R. C. Boston, P. C. Greif, and M. Berman, “ConversationalSAAM-An interactive program for kinetic analysis of biological sys-tems,” Comput. Program. Biomed. 13, 111-119 (1981).
58P. B. Zanzonico, R. E. Bigler, F. J. Primus, E. Alger, R. De Jager, S.Stowe, E. Ford, K. Brennan, and D. M. Goldenberg, “A compartmen-tal modeling approach to the radiation dosimetry of radiolabeled anti-body,” in Proceedings of the Fourth International RadiopharmaceuticalDosimetry Symposium, A. T. Schlafke-Stelson and E. E. Watson P.S.Department of Energy, DE86010102 (CONF-X51113), Oak Ridge,TN, 1985], pp. 421-445.
59G. Sgouros, R. E. Bigler, and P. B. Zanzonico, “Techniques for thedirect determination of cumulated activity from computer simulationsof linear and non-linear compartmental models,” Society of NuclearMedicine 34th Annual Meeting, Toronto, Canada ( 1987).
60 T. K. Johnson, “MABDOS: A generalized program for internal radi-onuclide dosimetry,” Computer Methods and Programs in Biomedi-cine 27, 159-167 (1988).
61L. M. Cobb, “Intratumoural factors influencing the access of antibodyto tumor cells,” Cancer Immunol. Immunother. 28, 235-240 ( 1989).
62A. M. Keenan, J. C. Harbert, and S. M. Larson, “Monoclonal anti-bodies in nuclear medicine,” J. Nucl. Med. 26, 531-537 ( 1985).
63S. M. Larson, “Radiolabeled monoclonal anti-tumor antibodies in di-agnosis and therapy,” J. Nucl. Med. 26, 53X-545 (1985).
6 4A. R. Bradwell, D. S. Fairwether, P. W. Dykes, A. Keeling, A.Vaughan, and J. Taylor, “Limiting factors in the localization of tumorswith radiolabelled antibodies,” Immunology Today 6, 163-170 (19X5).
65A.J. Fishman, B. A. Khaw, and H. W. Strauss, “Quo vadis radioim-munk imaging?,” Editorial, J. Nucl. Med. 30, 1911-1915 (1989).
6 6D. A. Goodwin, “Pharmacokinetics and antibodies,” Editorial, J.Nucl. Med. 28, 135X-1362 (1987).
67T.C.Meeker, J. Lowder, D. G. Maloney, R. A. Miller, K. Thielemans,R. Warnke, and R. Levy, “A clinical trail of anti-idiotype therapy forB cell malignancy,” Blood 65, 1349-1363 (1985).
68D. Goodwin, C. Meares, C. Diamanti, M. McCall, C. Lai, F. Torti, M.McTigue, and B. Martin, “Use of specific antibody for rapid clearance
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
of circulating blood background from radiolabelled tumor imaging pro-teins.” Eur. J. Nucl. Med. 9, 210-215 (1984).
69P. Oehr, J. Westermann, and H. J. Biersack. “Streptavidin and biotinas potential tumor imaging agents,” J. Nucl. Med. 29.72x-729 ( 1988).
70A. L. Klibanov, A. V. Martynov, M. A. Slinkin, I. Y. Sakharov, M. D.Smirnov. V. R. Muzykantov, S. M. Danilov, and V. P. Torchilin,“Blood clearance of radiolabelled antibody: enhancement by lactosam-ination and treatment with biotin-avidin or anti-mouse IgG antibod-ies,” J. Nucl. Med. 29. 1951-1956 (1988).
71V. V. Sinitsyn, A. G. Mamontova, Y. Y. Checkneva, A. A. Shnyra. andS. P. Domogaatsky, “Rapid blood clearance of biotinylated IgG afterinfusion of avidin,” J. Nucl. Med. 30, 66-69 (1989).
7 2D.J. Hnatowich, F. Virzi, and M. Rusckowski, “Investigations ofavidin and biotin for imaging applications,” J. Nucl. Med. 28, l294-1304 (1987).
73R.R. Eger D. G. Covell, and J. A. Carrasquillo, “Kinetic model forthe biodistribution of an 111-In-labeled monoclonal antibody in hu-mans,” Cancer Res. 47, 3328-3336 (1987).
74C. Ingvar, K. Norrgren, S. E. Strand, T. Brodin, P. E. Jonsson, and H.O. Sjogren, “Biokinetics of radiolabelled monoclonal antibodies in het-erotransplanted nude rats: Evaluation of corrected specific tissue up-take,” J. Nucl. Med. 30, 1224-1234 (1989).
75C. Ingvar, K. Norrgren, S. E. Strand, T. Brodin, P. E. Jonsson, and H.O. Sjogren, “Subcutaneous injection of monoclonal antibody 96.5.Biokinetics in the nude rat heterotransplanted with malignant mela-noma,” Acta Oncologica 29, 1047-1053 ( 1990).
76C. Ingvar, K. Norrgren, S. E. Strand, T. Brodin, P. E. Jonsson, and H.O. Sjogren, “Tumor uptake of monoclononal antibody after regionalintraarterial injection. Biokinetics in the nude rat heterotransplantedwith malignant melanoma,” Acta Oncologica (1991).
77R.K. Jain, “Transport of macromolecules in tumor microcirculation,”Biotechnol. Prog. 1, 81-94 (1985).
78D. C. Covell, J. Barbet, O. D. Holton, C. D. V. Black, R. I. Parker, andJ. N. Weinstein, “Pharmacokinetics of monoclonal immunoglobulinGl, F(ab’)2, and Fab’ in mice,” Cancer Res. 46, 3969-3978 (1986).
79D.G. Garlick and E. M. Renkin, “Transport of large molecules fromplasma to interstitial fluid and lymph in dogs,” Am. J. Physiol. 219,1595-1605 (1970).
80R. E. Bigler, P. B. Zanzonico, R. Leonard, M. Cosma, F. J. Primus, E.Alger, R. DeJager, S. Stowe, E. Ford, K. Brennan, and D. M. Gold-enberg, “Bone marrow dosimetry for monoclonal antibody therapy,” inProceedings of the Fourth International Radiopharmaceutical DosimetrySymposium, edited by A. T. Schlafke-Stelson and E. E. Watson [U.S.Department of Energy, DE86010102 (CONF-851113), Oak Ridge,TN, 1985], pp. 535-544.
81J. A. Siegel, B. W. Wessels, E. E. Watson, M. G. Stabin, H. M. Vrie-sendorp, E. W. Bradley, C. C. Badger, A. B. Brill, C. S. Kwok, D. R.Stickney, F. K. Echerman, D. R. Fisher, D. J. Buchsbaum, and S. E.Order, “Bone marrow dosimetry and toxicity for radioimmunother-apy,” Antib. Immunoconj. Radiopharm. 3, 213-233 (1990).
82B. A. Jonsson, S. E. Strand, and L. Andersson, “Radiation dosimetryfor indium-111-labeled anti-CEA-F(ab’), fragments evaluated fromtissue distribution in rats,” J. Nucl. Med. 33, 1654-1660 (1992).
83P. A. W. Edwards, “Heterogenous expression of cell surface antigens innormal epithelia and their tumors revealed by monoclonal antibodies,”Br. J. Cancer 51, 149 (1985).
84C. Ingvar, B. Jacobsson, T. Brodin, P. E. Jonsson, and S. E. Strand,“Tumor antigen heterogeneity within melanoma metastases-An eval-uation by immunohistochemistry,” Anticancer Res. 10, 219-223(1990).
85C. Ingvar, K. Norrgren, S. E. Strand, and P. E. Jonsson, “Heteroge-neous distribution of radiolabelled monoclonal antibody. Autoradio-graphic evaluation in the nude rat model,” AntiCancer Res. ( 1991).
86S. E. Strand, K. Ljunggren, K. Kairemo, A. Svedberg, K. Norrgren, C.Ingvar, and O. Wanying, “Functional imaging and dosimetric applica-tions of beta camera in RID and RIT,” Antib. Immunoconj. Radiop-harmarm. 4, 631-635 (1991).
87P. L. Jones, B. M. Gallagher, and H. Sands, “ARG analysis of mon-oclonal antibody distribution in human colon and breast tumor xe-nografts,” Cancer Immunol. Immunothe. 22, 134-143 (1986).
“J. M. Esteban, J. Schlom, F. Mornex, and D. Colcher, “RIT of athymicmice bearing human colon carcinomas with monoclonal antibodyB72.3. Histological and ARC) study of effects on tumors and normalorgans,” Eur. J. Cancer Clin. Oncol. 23, 643-655 (1987).
“M. H. Griffith, E. D. Yorke, and B. W. Wessels, “Direct dose confir-

527 Strand, Zanzonico, and Johnson: Pharmacokinstic modeling 527
mation of quantitative autoradiography with micro-TLD measure-ments for RIT,” J. Nucl. Med. 29, 1795-1809 (1988).
90K. Ydstrom. S. E. Strand, C. Ingvar, P. E. Jonsson, T. Brodin, and H.O. Sjogren, “Parameters influencing the uptake of radiolabelled mon-oclonal antibody 96.5 in heterotransplanted malignant melanoma innude rats,” in Proceeding of Advances in the Application of MonoclonalAntibodies in Clinical Oncology, London (abstract) (1984).
91R. B. Pedley, J. Boden, P. J. Harwood, A. J. Green, and G. T. Rogers,“Relationship between tumor size and uptake of radiolabelled anti-CEA in colon tumor xenograft,” Eur. J. Nucl. Med. 13, 197-202(1987).
92N. K. V. Cheung, J. E. Neely, B. Landmeier, D. Nelson, and F. Mi-raldi, “Targeting of ganglioside GD2 monoclonal antibody to neuroblas-toma,” J. Nucl. Med. 28, 1577-1583 (1987).
93L.E. Williams, R. B. Duda, R. T. Proflitt, B. G. Beatty, J. D. Beatty,J. Y. C. Wong, J. E. Shively, and R. J. Paxton, “Tumor uptake as afunction of tumor mass: A mathematical model,” J. Nucl. Med. 29,103-109 (1988).
94E. A. Cornelius, “Analysis of monoclonal antibody uptake in tumors:The significance of surface area,” in Proceeding of Third InternationalConference on Monoclonal Antibody Immunoconjugates for Cancer(1988).
95V.J. Philben, J. G. Jakowatz, B. G. Beatty, W. G. Vlahos, R. J.Paxton, L. E. Williams, J. E. Shively, and J. D. Beatty, “The effect oftumor CEA content and tumor size on tissue uptake of indium 111labelled anti-CEA monoclonal antibody,” Cancer 57, 571-576 ( 1986).
96C. Ingvar, “Radiolabelled monoclonal antibodies,” Thesis, Lund Uni-versity, Sweden (1990).
97J. N. Weinstein, R. R. Eger, and D. G. Covell, “The pharmacology ofmonoclonal antibodies,” Ann. N. Y. Acad. Sci. 199-210 (1988).
98K. Fujimori, D. G. Covell, J. E. Fletcher, and J. N. Weinstein, “Mod-eling analysis of the global and microscopic distribution of immuno-globin G, F(ab’)S, and Fab in tumors,” Cancer Res. 49, 5656-5663(1989).
9 9K. Fujimori, D. G. Covell, J. E. Fletcher, and J. N. Weinstein, “Amodeling analysis of monoclonal antibody percolation through tumors:A binding-site barrier,” J. Nucl. Med. 31, 1191-1198 ( 1990).
100K. Koizumi. G. L. DeNardo, S. J. DeNardo, M. T. Hays, H. H. Hines,P. O. Scheibe, J. S. Peng, D. J. Macey, N. Tonami, and K. Hisada,“Multicompartmental analysis of the kinetics of radioiodinated mono-clonal antibody in patients with cancer,” J. Nucl. Med. 27, 1273-1254(1986).
101R. R. Eger, D. G. Covell, J. A. Carrasquillo, P. G. Abrams, K. A.Foon, J. C. Reynolds, R. W. Schroff, A. C. Morgan, S. M. Larsson, andJ. N. Weinstein, “Kinetic model for the biodistribution of an 111In-labelled monoclonal antibody in humans,” Cancer Res. 47, 3328-3336(1987).
102A. Rescigno, H. Bushe, A. B. Brill, M. Rusckowski, T. W. Griffin, andD. J. Hnatowich. “Pharmacokinetics modeling of radiolabeled anti-body distribution in man,” Am. J. Physiol. Imaging. 5, 141-150(1990).
103K. Norrgren, S. E. Strand, and C. Ingvar, “Contrast enhancement inRII and modification of the therapeutic ratio in RIT. A theoreticalevaluation of simulated extracorporeal immunoadsorption,” Antibody,Immunoconjugates and Radiopharmaceuticals 5, 61-73 (1992).
104R. E. Bigler and P. B. Zanzonico. “Adjuvant radioimmunotherapy formicrometastases: A strategy for cancer cure,” in Radiolabeled Mono-clonal Antibodies for Imaging and Therapy, edited by S. C. Srivastava(Plenum, New York, 1988), pp. 409-429.
105S. E. Strand, K. Norrgren, C. Ingvar, K. Erlandsson, and E. C. Pers-son, “Plasmapheresis as a tool for enhancing contrast in radioimmu-noimaging and modifying absorbed doses in radioimmunotherapy,”Med. Phys. 16, 465 (Abstract) (1989).
106B. Charlton and K. Schindhelm, “The effect of extracorporeal antibodyremoval on antibody synthesis and catabolism in immunized rabbits,”Clin. Exp. Immunol. 60, 457-464 (1985).
107B. Charlton. K. Schindhelm, L. C. Smeby, and P. C. Farrell, “Analysisof immunoglobulin G kinetics in the non-steady state,” J. Lab. Clin.Med. 3. 312-320 (1985).
108A. M. Zimmer, T. Steven, S. T. Rosen, S. M. Spies, R. Goldman-Leikin. J. M. Kazikiewics, E. A. Silverstein, and E. H. Kaplan, “Ra-dioimmunotherapy of patients with cutaneous T-cell lymphoma usingan iodine-131-labeled monoclonal antibody: Analysis of retreatmentfollowing plasmapheresis,” J. Nucl. Med. 29, 174-180 (1988).
109K. Norrgren, S. E. Strand, R. Nilsson, L. Lindgren, and P. Lillehom,“Evaluation of extracorporeal immunoadsorption for reduction of theblood background in diagnostic and therapeutic applications of radio-labelled MAb’s,” Antib. Immunoconj. Radiopharm.4, 907-914(1991).
110K. Norrgren, S. E. Strand, R. Nilsson, L. Lindgren, and H.-O. Sjogren,“A general extracorporeal immunoadsorption method to increasetumor-to-normal tissue ratio in radioimmunoimaging and radioimmu-notherapy,” J. Nucl. Med. 34 (1993).
111T. K. Johnson, S. Maddock, R. Kasliwal, D. Bloedow, C. Hartman, A.Feyerabend, D. Dienhart, S. Glenn, R. Gonzales, J. Lear, and P. Bunn,“Radioimmunoadsorption of KC-4G3 antibody in peripheral blood:Implications for radioimmunotherapy,” Antib. Immunoconj. Radiop-harm. 4, 24 (Abstract) (1990).
112M. McAteer, H. Pastusiak, A. Hamstra, E. Maddock, D. Dienhart, R.Kasliwal, S. Glenn, A. Heal, P. Bunn, and S. Maddock, “Performanceof an immunoadsorption column used to improve radioimmunodetec-tion,” Antib., Immunoconj. Radiopharm. 4, 23 (Abstract) (1990).
113S. Maddock, P. Bunn, D. Dienhart, A. Feyerabend, S. Glenn, T.Johnson, R. Kasliwal, J. Lear, E. Maddock, and M. McAteer, “Strat-egy and use of immunoadsorption to improve RAIT,” Antib. Immu-noconj. Radiopharm. 4, 34 (Abstract) (1990).
114C. Hartman, D. C. Bloedow, D. Dienhart, R. Kasliwal, T. K. Johnson,S. W. Maddock, S. D. Glenn, G. M. Butchko, A. Feyerabend, R.Gonzales, J. L. Lear, and P. A. Bunn, “A pharmacokinetic modeldescribing the removal of circulating radiolabelled antibody by extra-corporeal immunoadsorption,” J. Pharmacokinet. Biopharm. 19, 385(1991).
115G. Sgouros, R. E. Bigler, and P. B. Zanzonico, “Compartmental modelsimulations of antibody kinetics: What parameters most influence an-tibody dosimetry?,” Supplement, J. Nucl. Med. 28, 617 (Abstract)(1987).
116R. E. Bigler, P. B. Zanzonico, M. Cosma, and G. Sgouros, “Adjuvantradioimmunotherapy for micrometastases: A strategy for cancer cure,”in Radiolabeled Monoclonal Antibodies for Imaging and Therapy, ed-ited by S. Srivastava (Plenum, New York, 1988, pp. 409-429.
117R. W. Howell, D. V. Rao, and K. S. R. Sastry, “Macroscopic dosim-etry for radioimmunotherapy: Nonuniform activity distributions in
solid tumors,” Med. Phys. 12, 405-412 (1989).118J. L. Humm, “Dosimetric aspects of radiolabeled antibodies for tumor
therapy,” J. Nucl. Med. 27, 1490-1497 (1986).119J. L. Humm and L. M. Cobb, “Nonuniformity of tumor dose in radio-
immunotherapy,” J. Nucl. Med. 31, 75-83 (1990).120G. M. Makrigiorgos, S. J. Adelstein, and A. I. Kassis, “Limitations of
conventional internal dosimetry at the cellular level,” J. Nucl. Med. 30,1856-1864 (1989).
121M. H. Griffith, E. D. Yorke, B. W. Wessels, G. L. DeNardo, and W. P.Neacy, “Direct dose confirmation of quantitative autoradiography withmicro-TLD measurements for radioimmunotherapy,” J. Nucl. Med.29, 1795-1809 (1988).
122J. A. Jungerman, K. P. Yu, and C. I. Zanelli, “Radiation absorbed doseestimates at the cellular level for some electron-emitting radionuclidesfor radioimmunotherapy,” Int. J. Appl. Radiat. Isot. 35, 883-888(1984).
123J. A. Jacquez, Compartmental Analysis in Biology and Medicine (Uni-versity of Michigan, Ann Arbor, 1985), pp. 20-28.
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

Tumor dosimetry in radioimmunotherapy: Methods of calculationfor beta particles
Peter K. LeichnerUniversity of Nebraska Medical Center, Department of Radiology. Omaha, Nebraska 68198-1045
Cheuk S. KwokHamilton Regional Cancer Centre, Ontario Cancer Treatment and Research Foundation and McMasterUniversity, Hamilton. Ontario, Canada
(Received 18 March 1992; accepted for publication 23 October 1992)
Calculational methods of beta-particle dosimetry in radioimmunotherapy (RIT) are reviewedfor clinical and experimental studies and computer modeling of tumors. In clinical studies,absorbed-dose estimates are usually based on the in-vivo quantitation of the activity in tumorsfrom gamma camera images. Because of the limited spatial resolution of gamma cameras,clinical dosimetry is necessarily limited to the macroscopic level (macrodosimetry ) and theMIRD formalism for absorbed-dose calculations is appropriate. In experimental RIT, tumordimensions are often comparable to or smaller than the beta-particle range of commonly usedradionuclides (for example, 1 3 1I, 6 7Cu, 1 8 6Re , 1 8 8Re, 9 0Y) and deviations from the equilibriumdose must be taken into account in absorbed-dose calculations. Additionally, if small tumors aregrowing rapidly at the time of RIT, the effects of tumor growth will need to be included inabsorbed-dose estimates. In computer modeling of absorbed-dose distributions, analytical, nu-merical, and Monte Carlo methods have been used to investigate the consequences of uniformand nonuniform activity distributions and the effects of inhomogeneous media. Measurementsand calculations of the local absorbed dose at the multicellular level have shown that variationsin this dose are large. Knowledge of the absorbed dose is essential for any form of radiotherapy.Therefore, it is important that clinical, experimental, and theoretical investigations continue toprovide information on tumor dosimetry that is necessary for a better understanding of theradiobiological effects of RIT.
I. INTRODUCTION
There is an increasing body of clinical evidence whichshows that antibodies labeled with beta-emitting radionu-elides have resulted in tumor remissions in some patientswith certain cancers. In experimental RIT, several investi-gators have reported complete remissions of tumor xe-nografts following the administration of radiolabeled anti-bodies. In clinical and experimental RIT, absorbed-dosecalculations are essential to gain an understanding of thedose-response relationship for different cancers and vari-eties of antibodies labeled with beta emitters, evaluation ofnormal-tissue toxicity, and treatment planning.
Tumor dosimetry of radiolabeled antibodies poses diffi-cult problems, and a number of sophisticated models hasbeen developed to address these problems. As discussed byLoevinger, 1 absorbed-dose estimates for administered radi-onuclides by their very nature are made for mathematicalmodels rather than patients. This is true of the modelsincluded in this review. However, they resemble the actualbiological situation as much as possible so that the resultsprovide meaningful information for clinical and experi-mental RIT.
The purpose of this article is to summarize some of therecently published techniques for tumor dosimetry in RITwith beta-particle emitting radionuclides. These includeimage-based dosimetry (macrodosimetry) often used inclinical trials, and numerical, analytical and Monte Carlomethods which have been employed for the dosimetry of
human and experimental tumors and tumor modelingstudies.
II. CALCULATIONAL METHODS
A. Macrodosimetry
In clinical studies, absorbed-dose estimates are basedon the in-vivo quantitation of the activity of radiolabeledantibodies in tumors from planar gamma camera images,single-photon emission computed tomography (SPECT),positron emission tomography (PET), or a combination ofplanar imaging and SPECT. Because of the limited spatialresolution of gamma cameras, clinical dosimetry is neces-sarily limited to the macroscopic level (macrodosimetry).Macrodosimetry is nonstochastic and due to the lack ofsufficiently detailed information about source distributions,the MIRD schema for absorbed-dose calculations are used.
A dosimetry model for clinical RIT was developed byLeichner et al.2,3 based on the MIRD formalism.4 In thisformulation of radiolabeled antibody dosimetry, tumorvolumes were obtained from patients’ CT examinations.’Thus, although the MIRD schema for formulating dose-rate equations was adopted, different tumor volumes weretaken into account for each patient. The basic dose-rateequations’ were subsequently confirmed by Wessels andRogus6 in a radionuclide model calculation which demon-strated that methods of calculation for clinical dosimetryand computer modeling were in agreement to within 4%.In clinical or macrodosimetry, the beta radiations were
529 Med. Phys. 20 (2), Pt. 2, Mar/Apr 1993 0094-2405/93/0205294%3s01.20 © 1993 Am. Assoc. Phys. Med. 529

530 P. K. Leichner and C. S. Kwok: Tumor dosimetry In radioimmunotherapy 530
treated as nonpenetrating radiations because the tumor andnormal organ volumes were large compared with the rangeof 131I or 9 0Y beta particles.“’ Tumor and normal organactivities were quantitated from planar gamma camera im-ages so that, due to a lack of more detailed information, theassumption of a uniform distribution of activity was in-voked in absorbed-dose calculations. The justification forthis was that tumor volumes were large enough so thatonly a small fraction of the beta-particle energy escapedfrom the tumors.2 Under this circumstance, the dose froma uniform distribution equals the mean dose from a non-uniform distribution.’ Consequently, dose calculations pro-vided a mean absorbed dose but provided no informationabout the range of absorbed doses. A further difficulty withthis approach to macrodosimetry was that tumor volumescomputed from CT scans were not necessarily the same asthe volumes in which radiolabeled antibodies localized (lo-calization volumes) because the physiological uptake ofradiolabeled antibodies may not have corresponded exactlyto the anatomical configuration of an organ or tumor.These difficulties can potentially be overcome with quanti-tative SPECT and PET which provide localization vol-umes and distributions of activity directly from radionu-clide images.8 However, even with quantitative SPECT orPET clinical dosimetry will remain macrodosimetry.
6. Numerical and analytical methods
These methods have been used to calculate absorbed-dose distributions in tumors and normal tissues resultingfrom uniform and nonuniform distributions of beta emit-ters. In general, point-source functions or tabulated point-source data were used to make numerical or analyticalcalculations of the absorbed dose. An empirical point-source function developed by Loevinger et al.9 was em-ployed by Kwok et al.1 0 to compute absorbed-dose distri-but ions resul t ing from radial ly symmetr ic act ivi tyconcentrations of 1 3 1I and 3 2P beta particles in soft tissue.The same function was also used by Griffith et al. 11 t ocalculate the absorbed dose for 131I and 9 0Y beta particlesfor activity distributions obtained from quantitative auto-radiography. In the latter investigation, measurementswere obtained with miniaturized thermoluminescent de-vices (TLD’s) and compared with calculations. The vari-ation in measured absorbed dose throughout an experimen-tal tumor was approximately 400%. Both studies showedthat the absorbed-dose distributions depended strongly onthe activity distributions and that for the assumed” andmeasured” distributions and volumes, the higher energybeta particles resulted in larger absorbed doses. Addition-ally, the variation in absorbed dose was greater for 1 3 1Ithan for 9 0Y beta particles due to the higher energy of thelatter.
The measurements by Cross12 and theoretical work byBerger13 and Cross et al.14 showed that Loevinger's point.source was inaccurate at small and large distances from apoint source. Additionally, this function breaks down forlow-energy beta emitters.15 Several authors have thereforeutilized the tabulated data13,14 to develop more general an-alytic representations for absorbed dose distributions
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
around point sources or used these data directly in numer-ical calculations. For example, using tabulated values ofmonoenergetic electron point kernels in water calculatedby Berger,13 Kwok et al.1 6 have developed analytical andnumerical methods to derive dose point kernels in waterfor radionuclides with allowed beta transitions. The advan-tage of analytical representations and solutions is that theysimplify calculations significantly. These authors also in-vestigated the effects of tissue heterogeneity on absorbed-dose distributions. A polystyrene (PST)-aluminum inter-face was used to simulate a soft tissue-bone interface anddose measurements were made at distances ranging from 0to 314 mg/cm2, with a 3 2P point source placed at the in-terface. A maximum increase of 12% in the absorbed dosewas measured at approximately 30 mg/cm2 from the inter-face. The implication of this study is that there may be anincrease in the absorbed dose at marrow-bone interfacesresulting from backscattered radiation. In contrast, therewas a decrease in absorbed dose when a PST-air interfacewas used to simulate a soft tissue-air interface. For low-energy electrons, the exact positions of the point sourcesand the dose scoring region have an important effect on thedose enhancement.”
Langmuir and Sutherland18 have investigated the effectof tumor size on absorbed-dose distributions from betaemitters when radiolabeled antibodies are not uniformlydistributed in tumors. Two theoretical dosimetry modelswere considered; one for vascularized tumors and one formicrometastases without vasculature. In dose calculations,it was assumed that there was no penetration of radiola-beled antibodies into the tumors. These were compared tocalculations based on uniform activity distributions withintumors. Absorbed-dose rates for 131I and 9 0Y beta particleswere calculated by numerical integration and the use ofBerger’s point source data.13 The results showed that forsmall lesions (1 mm or less in diameter) a given concen-tration of 1 3 1I resulted in a higher dose rate than that ob-tained from an equal concentration of 9 0Y beta particles,due to the lower absorbed fraction of the latter. On theother hand, for vascularized tumors, ?-labeled antibodiesyielded higher absorbed dose rates and more uniform dosedistributions within tumors because of overlapping contri-butions from multiple sources. Similar conclusions werereached by Howell et al.1 9 who made numerical calcula-tions of absorbed-dose distributions for several beta emit-ters (3 2P , 6 7C u , 9 0Y , 1 1 1A g , 1 3 1I, 1 8 8Re) and for a low-energy electron emitter, 1 9 3 mP t . I n t h e i r m o d e lcalculations, activity distributions were spherically sym-metric and depended linearly and exponentially on the ra-dial coordinate. The results demonstrated that for largertumors (1 cm or greater in diameter) high-energy betaemitters, such as 3 2P or 9 0Y, would be most effective,whereas for smal ler tumors (~1 mm in d iameter)medium-energy beta particles (e.g., 131I, 6 7Cu) were bettersuited. To treat micrometastases, these authors suggestedthe use of 1 9 3 mPt .
A generalized empirical point-source function for beta-particle dosimetry was developed by Leichner et al.20 fromBerger’s tabulated absorbed-dose distributions for point

531 P. K. Leichner and C. S. Kwok: Tumor dosimetry in radioimmunotherapy 531
sources in water.1 3 Absorbed-dose distributions for eightradionucl ides (3H, 1 4C, 3 5S, 1 3 1I, 1 1 1Ag, 3 2P, 9 0Y, 1 0 6R h )with average beta-particle energies ranging from 5.7 keV(3H) to 1.43 MeV (106Rh) were computed from this point-source function. The results demonstrated agreement withtabulated data over the entire energy range and for a widerange of distances from point sources. Analytical solutionsin terms of absorbed fractions were derived for two sourcegeometries, a thin source of infinite extent and a planesource of finite thickness and infinite extent. Beta-particledose calculations for a plane source of finite thickness werecarried out for 1 3 1I- and v-labeled antiferritin depositedin experimental tumor lines and determined to be in agree-ment with measurements.2 1’22 These calculations showedthat even for uniform distributions of activity, the absorbeddose was nonuniform when tumor dimensions were com-parable to or smaller than twice the distance r 9 0. The dis-tance r9 0 is a useful parameter that indicates the distancefrom a point source within which 90% of the energy isabsorbed. 13 Second, the absorbed dose in small tumors issignificantly less than the absorbed dose for complete ab-sorption of energy. Consequently, in experimental RITwhere tumors tend to be small, absorbed-dose calculationsshould take tumor dimensions into consideration to deter-mine tumor dose-response relationships.
An investigation of the multicellular dosimetry of131I-labeled antibody in follicular lymphoma was carriedout by Hui et al.23 In this work, photomicrographs of alymph node specimen were analyzed to determine themean value and statistical variation of the radii of follicles,interfollicular distances, and number densities of follicles.These measurements were used to construct two geometricmodels, a cubic lattice model and a randomized distribu-tion model. The cubic lattice model assumed no variationin follicular radii and interfollicular distance. In the ran-domized distribution model, Monte Carlo methods wereused to simulate the distribution of follicular radii, inter-follicular distances, and the number density of follicles.The 1 3 1I-labeled antibodies were considered to be pointsources, and absorbed-dose calculations were performedusing Berger’s tabulated values for point sources of betaparticles in water.13 From the granular density in photo-micrographs, it was determined that the activity ratio ofradiolabeled antibody for follicular-to-interfollicular areaswas approximately 10:1, and the spatial distribution of lo-calized absorbed dose was calculated for an average tumordose of 40 Gy. It was assumed that the activity distributionwas fairly uniform within the follicles and uniform in theinterfollicular space. Based on these data and assumptions,calculations of the local absorbed dose were made. Thesecalculations showed that the local dose varied from 20 to90 Gy. Additionally, 70% to 80% of the tissue (by vol-ume) had an absorbed dose that was lower than the aver-age dose. In this study, no significant difference was foundfor calculations based on the cubic lattice model and therandomized distribution model, demonstrating that insome cases a relatively simple geometric model can be avalid starting point for a difficult dosimetric problem.
Simple, analytic representations for dose-rate distribu-
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
tions due to regions containing beta-particle sources weredeveloped by Werner using the energy-averaged transportm o d e l . 2 4 - 2 8 Solutions of the model were presented for pla-nar and spherical symmetry, and for random and nonuni-form source distributions.
The effects of tumor size on energy absorbed fractionsand antibody binding heterogeneity were further discussedby Humm.29 Absorbed fractions for-beta sources were cal-culated using a computer code developed specifically forthat purpose. For solid tumors, a spherical model wasadopted to investigate the effects of tumor size on absorbeddose. Two cases were considered, a spherical volume con-taining a uniform distribution of activity (“hot sphere”)and a “cold sphere” containing no activity but surroundedby a uniform distribution of activity. For “hot spheres” ofradii 100 and 500 µm, absorbed fractions were computedfor 2 1 1At, 9 0Y, 7 7As, 1 3 1Au, and 1 3 1I. For such small tumorspheres, At and low-energy beta emitters (7 7As, 1 9 9Au)had the largest absorbed fractions (highest energy deposi-tion). For “cold spheres,” dose profiles were generated forradii 0.5, 1, 2, and 4 mm. These showed that high-energybeta emitters, such as 90Y, resulted in the highest absorbeddose in “cold regions” resulting from the surrounding ac-tivity. The dosimetry of radiolabeled antibodies for non-solid tumors; that is, isolated tumor cells as is the case forcirculating leukemia cells was also considered by Humm.For assumed cellular and nuclear diameters of 20 and 10µm, respectively, it was calculated that only one in 16particles emitted on a cell surface membrane wouldtraverse the nucleus. It was, therefore, suggested that forthis type of RIT, radionuclides that emit large numbers oflow-energy electrons, e.g., 119Sb might be optimal, as pre-viously mentioned by Sastry et al.3 0
These dosimetric considerations were developed furtherby Humm and Cobb31 in calculations of the energy depo-sition at the cellular level. One tumor model consisted of arandom distribution of cells, and absorbed-dose calcula-tions were made for two different source distributions: auniform distribution of sources and sources geometricallyplaced on cell membranes. For a uniform distribution ofsources, the MIRD schema for absorbed dose calculationswas valid if the tumor was large enough so that boundaryeffects could be ignored. For cell-surface bound antibodiesthe energy deposited in cell nuclei was expressed as thesum of two components: the energy deposition in the cellnucleus from sources bound to the membrane of that celland the energy deposition to neighboring cell nuclei towhich the source was not bound. The energy deposited percell nucleus per decay was calculated for 211At, 199Au, 131I,and 90Y with internuclear distances ranging from 10 to 100µm. The results showed that of the three beta emitters, 90Ydeposited the largest amount of energy per nucleus perdecay for both source distributions and all internucleardistances considered. Additionally, 90Y required the small-est number of decays per cell membrane for 99% cell in-activation. We note, however, that in this model 211At wassuperior to the three beta emitters in energy deposition andnumber of decays required for cell inactivation.
In all of the models discussed, calculations of the ab-
532 P. K. Leichner and C. S. Kwok: Tumor dosimetry in radioimmunotherapy 532
sorbed dose for tumors were made for constant tumormass. This assumption is justified in many experimentaland clinical trials in RIT because tumors are either nolonger growing or are growing at a slow rate. However,small tumors and micrometastases may be growing rapidlyat the time of antibody administration so that tumor massand the absorbed fraction can change significantly duringtreatment. This dosimetric problem was investigated byHowell et al.33 who generalized the MIRD Schema to in-clude the time dependence of tumor mass and absorbedfractions in absorbed-dose calculations. The modifiedMIRD equations were applied to an in-vitro model (mul-ticellular V79 spheroids) and an in-vivo tumor (myeloma).The results of this work show that tumor growth can be asignificant factor in tumor dosimetry and that in rapidlygrowing tumors the absorbed dose will be overestimated ifsuch growth is not taken into account in calculations.
III. MONTE CARLO METHODS
The widely used tables of beta-particle dose kernels byBerger 13 and Cross14 are based on Spencer’s 33,34 numericalsolution of the transport equation of primary electrons in auniform unbounded medium in the continuous slowing-down approximation (csda). Calculations based on Spen-cer’s theory agreed well with measurements 12 and this pro-vided a sound basis for beta-particle dosimetry. Animportant advance has been the development of MonteCarlo methods for the simulation of electron transport. Bydividing the electron path into small segments, Berger3 5
took into account multiple scattering and energy loss fluc-tuations. Departures from csda due to delta-ray and brems-strahlung production were also incorporated and resultedin improved point kernels for monoenergetic electrons inw a t e r . 36 These resul ts were spect ra l ly weighted byPrestwich et al.37 to calculate beta dose point kernels for3 2P, 6 7Cu, 9 0Y, 1 3 1I, 1 8 6Re, and 1 8 8Re. Addit ional ly , theauthors provided an analytic representation of the pointkernels.
A different approach was taken by Simpkin andMackie 38 who employed the EGS4 Monte Carlo computercode to generate point kernels in water for 3 2P, 6 7Cu, 9 0Y ,1 0 5Rh, 1 3 1I, 1 5 3Sm, 1 8 6Re, and 1 8 8Re beta particles. Origi-nally developed for high-energy physics, the EGS4 codehas become very useful in medical physics and can be ob-tained from Oak Ridge National Laboratory. 39 Simpkinand Mackie compared their results with those published byBerger36 and Prestwich et al.33 and concluded that for ra-dionuclides of interest in RIT, the agreement in point ker-nels obtained by different authors was remarkably good.
The EGS4 Monte Carlo code was also used by Johnsonet al.4 0 to calculate the radiation-absorbed dose at a bone-to-marrow interface for 1 5 3Sm, 1 8 6Re, and 1 8 6Ho. Theseradionuclides were chosen because they are of current in-terest as radiotherapeutic agents for metastatic bone can-cers and for marrow ablation. In this calculation, activitywas taken to be distributed uniformly at midplane in theendosteum which was modeled as a 10-µm-thick slab be-tween marrow and cortical bone. The calculated absorbeddose distributions included contributions from atomic elec-
Medical Physics, Vol. 20, No. 2, Pt. 2. Mar/Apr 1993
trons, beta particles, and photons. An important result ofthis investigation was that the backscatter contribution tothe absorbed dose in the marrow increased from 3% to 4%at the source to 6% to 8% at a marrow depth of 100 µm.These results are consistent with those obtained by Kwoket al.1 7
Humm41 has described a Monte Carlo computer modelto calculate energy deposition in tumor cell nuclei follow-ing the administration of “‘At-labeled antibodies. This ap-proach to the dosimetry of radiolabeled antibodies wassubsequently extended by Humm and Cobb31 to simulatethe tubular structure of differentiated colon carcinoma.Cells of 10-µm radii containing 5-µm spherical nuclei wereassumed to be packed along cylinders which were sepa-rated by a variable distance. The sources ( 2 1 1At or 1 3 1I )were placed on the outer surfaces of the cylinders. For 131I,a constant LET (0.2 keV/µm) model was used withstraight line tracks of range 487 µm. The energy depositionper cell nucleus per decay was calculated for a uniformdistribution of sources throughout the tumor volume andfor sources bound to the outer surface of the cylinders withan outer radius of 50 µm and an inner radius of 30 µm. Thecell nuclei were centered at 40 µm from the cylinder axis.A geometric enhancement factor was computed by divid-ing the energy deposition resulting from bound sources bythe energy deposition from uniformly distributed (un-bound) sources. These calculations were made for dis-tances between cylinders ranging from 0 to 200 µm. Thegeometric enhancement factor was greater than one at allintercylinder distances showing that the energy depositedper cell nucleus per decay was greater for sources bounduniformly to the outer surfaces than for sources distributeduniformly throughout the tumor. This theoretical tumormodel demonstrated that the geometric enhancement fac-tor, and hence the absorbed dose, depended strongly on thespatial source-to-nuclei relationship at the micrometerlevel.
IV. DISCUSSION
In this article, we have summarized some of the calcu-lational methods for tumor dosimetry in RIT, with empha-sis on beta particles. There are several reasons for this. Asstated in the Introduction, antibodies conjugated to beta-particle emitting radionuclides have resulted in tumor re-missions. Second, currently used radiolabels in clinicalRIT, such as 1 3 1I, 6 7Cu, 1 8 6Re, 1 8 8Re, and 9 0Y emit betaparticles that span a wide range of energies and it was,therefore, important to review methods used and resultsobtained by different authors in the computation of point-source kernels. In general, Monte Carlo calculations haveresulted in improved beta and electron point-dosekemels35-38 as compared to those based on electron trans-port theory.3 3 , 3 4 However, for beta emitters of interest inRIT, differences in point-source kernels obtained by differ-ent methods were determined to be small.38 For these betaemitters it is, therefore, appropriate to use tabulatedvalues12,13 of absorbed-dose distributions in analytical ornumerical dose calculations. For completeness, we notethat in all references cited, bremsstrahlung has not been

533 P. K. Leichner and C. S. Kwok: Tumor dosimetry In radioimmunotherapy 533
included in tumor dose calculations because in soft tissueless than 1% of the beta-particle energy is converted tobremsstrahlung. 42,43
The type of information needed for tumor dosimetry inRIT is under most circumstances no different than thatneeded for other biologically distributed radionuclides:physical data for the decay of the radionuclide, the distri-bution of absorbed energy of the emitted radiations, andcumulated activities or residence times in the tumor. Anadded difficulty, not usually encountered in normal-tissuedosimetry, may occur if a tumor is rapidly growing. In thiscase, the time dependence of tumor mass and absorbedfractions will need to be included in dose calculations.3 2
Activity distributions as a function of time and cumu-lated activities in tumors are difficult to obtain. This isespecially true in clinical studies and to a lesser extent inexperimental RIT where serial necropsies can provide thenecessary information. The shortcomings of image-basedmacrodosimetry are well-understood: limited spatial reso-lution and difficulties associated with the extraction ofquantitative information from planar gamma camera oremission-tomographic images. Although for most tumorsthat can be imaged a mean value of activity and henceabsorbed dose can be determined, this information is notsufficient to unravel the radiobiological effects of RIT.Therefore, macrodosimetry will need to be augmented bydosimetry on the cellular or multicellular level. For exam-ple, the dosimetry of 131I-labeled antibodies in follicularlymphoma 23 has shown that calculations of the local ab-sorbed dose can be used to make improved estimates of thecell killing efficiency of radiolabeled antibodies. Knowledgeof the absorbed dose is central to radiation oncology andfor gaining an understanding of dose-response relation-ships in RIT.
ACKNOWLEDGMENTS
One of the authors (PKL) gratefully acknowledges sup-port under DOE Grant No. DE-FG02-91ER61195. Theother author (CSK) acknowledges support by Natural Sci-ences and Engineering Research Council of Canada andU.S. NC1 Grant No. CA50872.
1R. Loevinger, “Distributed radionuclide sources,” in Radiation Dosim-etry, edited by F. H. Attix and E. Tochilin (Academic, NY, 1969)Volume III.
2P. K. Leichner, J. L. Klein, J. B. Garrison, R. E. Jenkins, E. L. Nick-oloff, D. S. Ettinger, and S. E. Order, “Dosimetry of 131I-labeled anti-ferritin in hepatoma: A model for radioimmunoglobulin dosimetry,”Intl. J. Rad. Oncol. Biol. Phys. 7, 323-333 (1981).
3P. K. Leichner, J. L. Klein, S. S. Siegelman, D. S. Ettinger, and S. E.Order, “Dosimetry of “‘I-labeled antiferritin hepatoma,” CancerTreat. Rep. 67, 647-658 (1983).
4R. J. Cloutier, E. E. Watson, R. H. Rohrer, and E. M. Smith, “Calcu-lating the radion dose to an organ,” J. Nucl. Med. 14, 53-55 (1973).
5N.-C. Yang, P. K. Leichner, E. K. Fishman, S. S. Siegelman, T. L.Frankel, J. R. Wallace, D. M. Loudenslager, W. G. Hawkins, and S. E.Order, “CT volumetrics of primary liver cancers,” J. Comput. Assist.Tomogr. 10, 621-628 (1896).
6B. W. Wessels and R. D. Rogus, “Radionuclide selection and modelabsorbed dose calculations for radiolabeled tumor associated antibod-ies,” Med. Phys. 11, 638-645 (1984).
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
7P. K. Leichner, N.-C. Yang, T. L. Frankel, D. M. Loudenslager, W. G.Hawkins, J. L. Klein, and S. E. Order, “Dosimetry and treatmentplanning for y-labeled antiferritin in hepatoma,” Intl. J. Rad. Oncol.Biol. Phys. 14, 1033-1042 (1988).
8P. K. Leichner, W. G. Hawkins, and N.-C. Yang, “QuantitativeSPECT in radioimmunotherapy,” Antib. Immunoconjug. and Radiop-harm. 4, 25 (1990).
9R. Loevinger, E. M. Japha, and G. L. Brownell, “Discrete radioisotopesources,” in Radiation Dosimetry, edited by G. J. Hine and G. L.Brownell (Academic, NY, 1956).
10C. S. Kwok, W. V. Prestwich, and B. C. Wilson, “Calculation of radi-ation doses for nonuniformly distributed β and γ radionuclides in softtissue,” Med. Phys. 12, 405-412 (1985).
11M. H. Griffith, E. D. Yorke, B. W. Wessels, G. L. DeNardo, and W. P.Neacy, “Direct dose confirmation of quantitative autoradiography withmicro-TLD measurements for radioimmunotherapy,” J. Nucl. Med.29, 1795-1809 (1988).
12W. G. Cross, “The distribution of absorbed energy from a beta pointsource,” Can. J. Phys. 45, 2021-2040 (1967).
13M. J. Berger, “Distribution of absorbed dose around point sources ofelectrons and beta particles in water and other media,” Medical Inter-nal Radiation Dose (MIRD) Committee, Pamphlet No. 7 (The Soci-ety of Nuclear Medicine, NY, 1971).
14W. G. Cross, H. Ing, N. O. Freedman, and J. Mainville, “Tables ofbeta-ray distributions in water, air, and other media,” Atomic Energyof Canada Ltd., Report No. AECL-7617, Chalk River Nuclear Labo-ratories, Chalk River, Ontario, Canada (1982).
15K. Tagden and W. Scheuerman, “Estimation of absorbed dose in thecell nucleus after incorporation of 3H- or 14C-labeled thymidine,” Rad.Res. 41, 202-216 (1970).
16C. S. Kwok, M. Irfan, L. B. Chan, and W. V. Prestwich, “Beta dosim-etry for radioimmunotherapy of cancer using labeled antibodies,” NC1Monographs 3, 73-82 (1987).
17C. S. Kwok, P. J. Bialobzyski, S. K. Yu, and W. V. Prestwich, “Effectof tissue inhomogeneity on dose distribution of point sources of low-energy electrons,” Med. Phys. 17, 786-793 (1990).
18V. K. Langmuir and R. M. Sutherland, “Dosimetry models for radio-immunotherapy,” Med. Phys. 15, 867-873 (1988).
19R. W. Howell, D. V. Rao, and K. S. R. Sastry, “Macroscopic dosim-etry for radioimmunotherapy: nonuniform activity distributions insolid tumors,” Med. Phys. 16, 66-74 ( 1989).
20P. K. Leichner, W. G. Hawkins, and N.-C. Yang, “A generalized,empirical point-source function for beta-particle dosimetry,” Antib.Immunoconj. Radiopharm. 2, 125-144 (1989).
21J. L. Klein, T. H. Nguyen, P. Laroque, K. A. Kopher, J. R. Williams,B. W. Wessels, L. E. Dillehay, J. Frincke, S. E. Order, and P. K.Leichner, “Yttrium-90 and iodine-131 radioimmunoglobulin therapy ofan experimental hepatoma,” Cancer Res. 49, 6383-6389 (1989).
22P. K. Leichner, N.-C. Yang, B. W. Wessels, W. G. Hawkins, S. E.Order, and J. L. Klein, "Dosimetry and treatment planning in radio-immunotherapy,” in Frontiers of Radiation Therapy and Oncologv, ed-ited by J. M. Vaeth and J. L. Meyer (Karger Verlag, Basel, Switzer-land, 1990), Vol. 24, pp. 109-122.
23T. E. Hui D. R. Fisher, O. W. Press, J. F Eary, J. N. Weinstein, C. C.Badger, and I. D. Bernstein, “Localized beta dosimetry of “‘I-labeledantibodies in follicular lymphoma,” Med. Phys. 19, 97-104 (1992).
24B. L. Werner and I. J. Das, “Dose distributions in regions containingbeta sources: Plane interfaces in a homogeneous medium,” Med. Phys.14, 797-806 (1987).
25B. L. Werner, “Dose distributions in regions containing beta source:small-scale nonuniformities,” Med. Phys. 14, 807-808 (1987).
26B. L. Werner, C. S. Kwok, and I. J. Das, “Dose distributions in regionscontaining beta sources: Large spherical regions in a homogeneousmedium,” Med. Phys. 15, 358-363 (1988).
27B. L. Werner, C. S. Kwok, and I. J. Das, “Dose distributions in regionscontaining beta sources: uniform spherical source regions in homoge-neous media,” Med. Phys. 18, 1181-1191 (1991).
28B. L. Werner, “Dose distributions in regions containing beta sources:Irregularly shaped source distributions in homogeneous media,” Med.Phys. 18, 1192-1194 (1991).
29J. L. Humm, “Dosimetric aspects of radiolabeled antibodies for tumortherapy,” J. Nucl. Med. 27, 1490-1497 (1986).
30K. S. R. Sastry, C. Haydock, A. M. Basha, and D. V. Rao, “Electrondosimetry for radioimmunotherapy: Optimal electron energy,” Radiat.Prot. Dosim. 13, 249-252 (1985).

534 P. K. Leichner and C. S. Kwok: Tumor dosimetry In radioimmunotherapy 534
31J. L. Humm and L. M. Cobb, “Nonuniformity of tumor dose in radio-immunotherapy,” J. Nucl. Med. 31, 75-83 (1990).
32R. W. Howell, V. R. Narra, and D. V. Rao. “Absorbed dose calcula-tions for rapidly growing tumors,” J. Nucl. Med. 33, 277-281 (1992).
33L. V. Spencer, “Theory of electron penetration,” Phys. Rev. 98, 1597-1615 (1955).
34L. V. Spencer, “Energy dissipation by fast electrons,” National Bureauof Standards, Monograph 1 (U.S. Department of Commerce, Wash-ington, D.C., 1959).
35M. J. Berger, “Monte Carlo calculation of the penetration of diffusionof fast charged particles,” in Methods in Compututional Physics editedby B. Alder, S. Fembach, and M. Rotenerg (Academic, NY, 1963).
36M. J. Berger, “Improved point kernels for electron and beta-ray do-simetry,” NBSIR 73-107 (Center for Radiation Research, U.S. Depart-ment of Commerce, Washington, D.C., 1973).
37W. V. Prestwich, J. Nunes, and C. S. Kwok, “Beta dose point kernelsfor radionuclides of potential use in radioimmunotherapy,” J. Nucl.Med. 30, 1036-1046 (1989); ibid 30, 1739-1740 (1989).
38D. J. Simpkin and T. R. Mackic, “EGS4 Monte Carlo determination ofthe beta dose kernel in water,” Med. Phys. 17, 179-186 (1990).
39Radiation Shielding Information Center, Oak Ridge National Labora-tory, P.O. Box 2008, Oak Ridge, TN 37831-6362.
40J. C. Johnson, S. M. Langhorst, S. K. Loyalka, W. A. Volkert, and A.R. Ketring, “Calculation of radiation dose at a bone-to-marrow inter-face using Monte Carlo modeling techniques (EGS4),” J. Nucl. Med.33, 623-628 (1992).
41J. L. Humm, “A microdosimetric model of astatine-211 labeled anti-bodies for radioimmunotherapy,” Intl. J. Radiat. Oncol. Biol. Phys. 13,1767-1773 (1987).
42M. J. Berger and S. M. Seltzer, “Tables of energy losses and ranges ofelectrons and positrons,” (National Aeronautics and Space Adminis-tration, Washington, DC., 1964).
43L. E. Williams, J. Y. C. Wang, D. O. Findley, and B. W. Forell,“Measurement and estimation of organ bremsstrahlung radiationdose,” J. Nucl. Med. 30, 1373-1377 (1989).
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

Microdosimetric concepts in radioimmunotherapyJ. L. HummJoint Center for Radiation Therapy, Harvard Medical School, 50 Binney Street, Boston,Massachussetts 02115
J. C. RoeskeUniversity of Chicago Medical Center. Radiation Therapy, 5841 S. Maryland Avenue. Box 440, Chicago,Illinois 60637
D. R. FisherBattelle, Pacific Northwest Laboratories, P. O. Box 999, K3-53, Richland, Washington 99352
G. T. Y. ChenUniversity of Chicago Medical Center, Radiation Therapy, 5841 S. Maryland Avenue, Box 440, Chicago,Illinois 60637
(Received 18 March 1992; accepted for publication 15 September 1992)
In microdosimetry particular emphasis is placed on the stochastic fluctuation of dose in smalltarget volumes such as individual cell nuclei or chromatin fiber, and their relevance to radiobi-ologic toxicity. Thus microdosimetry is intimately associated with models of radiation action.There are three principal areas where microdosimetry has been applied: (1) radiation protec-tion, (2) high LET radiotherapy, e.g., neutron therapy, and (3) incorporated radionuclides, andin this latter category the importance of microdosimetry to the radiobiology of radiolabeledantibodies is becoming increasingly recognized. The objective of microdosimetry is the com-plete characterization of energy deposition within all target volumes throughout the tissue ofinterest, The importance and relevance of this pursuit will depend upon the properties of theradionuclide emissions and the spatial distribution of the radionuclide relative to the targetvolumes. If the distribution of internal emitters within both malignant and normal tissue isuniform, the application of microdosimetry to radioimmunotherapy (RIT) is limited toa-emitters and Auger emitters. Under such circumstances the traditional MIRD formalism forthe evaluation of tumor and tissue doses from the commonly used P-emitters is entirely ade-quate. This, however, is rarely the case. When the distribution of radiolabeled antibody isnonuniform, techniques of dose averaging over volumes greater in size than the individual targetvolumes can become inadequate predictors of the biological effect. The concepts, methods, andrealm of applicability of microdosimetry within the field of radioimmunotherapy are emphasizedin this paper.
Key words: microdosimetry, radiolabeled antibodies, energy deposition, alpha emitters, betaemitters
I. CONCEPTS IN MICRODOSIMETRY
A. IntroductionRadiation dosimetry is the study of the physical propertiesof radiation energy deposition in tissue. Radiation dose inconventional dosimetry is a macroscopic concept.’ Targetvolumes are many orders of magnitude greater than theindividual cellular entities which make up tissue. The doseto a macroscopic multicellular volume is obtained by thesummation of the total energy deposited by multiple radi-ation tracks over the volume divided by the mass of thatvolume. Microdosimetry is the study of radiation energydeposition within microscopic volumes, where “micro-scopic” encompasses sensitive target volumes ranging fromthe diameter of a cell (typically 20 µm) down to the di-ameter of the DNA molecule (2 nm). Although microdo-simetry is concerned with the same concept of energy dep-osition per unit mass as dosimetry, the difference in size ofthe target volume of interest introduces stochastic effectswhich are negligible in conventional dosimetry. The mag-
nitude and importance of stochastic fluctuations in the tar-get volumes depend greatly on the target diameter, on theenergy and linear energy transfer (LET) of the particles,and on the relative number of particles, i.e., the magnitudeof the radition dose. For example, bulk tissue receiving anabsorbed dose of 1 cGy of γ− rays, results in an averagenumber of electron track traversals of approximately 50per cell, with a standard deviation of 7 hits. The same 1cGy absorbed dose of a-particles would result in a spec-trum of individual cell doses ranging from 0-30 cGy, witha mean number of α− particle hits per cell of only 0.1, andwith 90% of the cells experiencing zero hits. 2
B. The sensitive target
Several radiobiological studies point to the nucleus3
and more specifically the DNA as the primary sensitivetarget for cellular inactivation.- The evidence that DNAis the principal target for radiation cell sterilization comesfrom studies with radionuclides which result in a dense
535 Med. Phys. 20 (2), Pt. 2, Mar/Apr 1993 0094-2405/93/020535-0-08$01.20 © 1993 Am. Assoc. Phys. Med. 535
536 Humm et al.: Microdosimetric concepts in radioimmunotherapy 536
cluster of ionizations within 2 nm of the decay site. Theseradionuclides exhibit extreme positional effects, i.e., if di-rectly incorporated into the DNA they may be many foldmore radiotoxic than when appended to other cellularstructures. Recent debates at the radiation research con-ference (March 1992) at Salt Lake City alluded to thevariation of DNA radiosensitivity with organizationalstructure, i.e., the degree of supercoiling. This topic is,however, beyond the scope of the current article.
If the genome is the relevant target for cell sterilization,and the genome is assumed to be randomly distributedthroughout the cell nucleus, then the magnitude of energydeposition within the cell nucleus appears to be an appro-priate choice for the target dimensions with which to relatecell toxicity. If some physical parameter of dose to the cellnucleus can be related to the probability of cell death, andthis parameter obtained for all cells within the tissue ofinterest, then a method should exist to calculate the frac-tion of cell survivors within a tumor following treatmentby a radiolabeled antibody. This is the goal of microdosim-etry in RIT.
Although the use of energy deposition in the cell nu-cleus as the correlate for cell inactivation should be feasiblefor a- and P-particle emitters, it may be inappropriate forradionuclides which decay by electron capture or internalconversion, e.g., iodine-125 These isotopes decay by theinduction of an inner shell vacancy in the atom. The pro-cess of electronic de-excitation of the atom results in theemission of electrons, referred to as “Auger electrons” af-ter their discoverer, Pierre Auger.’ Since filling one va-cancy by an Auger process, results in two further vacan-cies, a cascade of Auger transitions ensues which persistsuntil all the vacancies have risen to the outermost atomicorbitals. Therefore, an atom which decays by electron cap-ture or internal conversion gives rise to several low energyelectrons (corresponding to the differences between the or-bital electron binding energies). Such local clusters of lowenergy Auger electrons at the decay site have been shownto exhibit high LET-like toxicity, if the source decayswithin 1 or 2 nm of the DNA molecule, but low LETradiotoxicity at greater distances from the DNA target. 4,5
Under such circumstances radiation dose to the cell nu-cleus may be inadequate as a predictor of radiation toxic-ity, and determination of the energy deposition to theDNA molecule may be necessary. Although studies havebeen performed with 125I-radiolabeled antibody,’ this classof radionuclide will not be discussed further in this paper.The interested reader is referred to the literature.’
C. Criteria for the applicability of microdosimetry
The basic criterion for determining the necessity ofmicrodosimetry w a s e s t a b l i s h e d b y K e l l e r e r a n dChmelevsky. 1 0This principle states that the stochastic na-ture of energy deposition within the target should be takeninto account when the relative deviations of the local dosefrom the mean in the target exceeds 20%. For a uniformdistribution of a long range β− source such as 90Y within thetumor, even at doses as low as 1 cGy, the average numberof &particle traversals per cell nucleus is so great that the
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
concept of absorbed dose is entirely adequate. However, asKellerer noted, the requirement of microdosimetric tech-niques for α− particles is almost always necessary. For ex-ample, a spherical target of diameter 5 µm requires anaverage dose of > 100 Gy for the use of the average dose tobe sanctioned. When the distribution of sources is nonuni-form, as in radioimmunotherapy, microdosimetric analysismay also be required for P-particle sources, if the fluctua-tion of target cell doses exceeds 20%.
D. Microdosimetric quantities
The most fundamental parameter in microdosimetryis the energy deposition ε1 from a single event (track in-tersection) with a target volume. Given a specific irradia-tion geometry, target size and shape and particle type, theentire probability distribution of energy deposits ƒ ( ε1)within the target volume from single traversals is referredto as a single event energy deposition spectrum. A morecommonly used quantity is the single event specific energyz1. The quantity z1 is the energy deposition ε1 divided bythe mass of the target volume m. The quantity z1 has beencalculated and also measured, using a Rossi proportionalcounter, for a number of radiations.” For high dose radi-ation fields, of concern for therapy, one is primarily inter-ested in multiple event spectra, where the stochastics ofindividual target hits is convoluted with the hit probabilitydistribution. The microdosimetric quantity, specific energyz, used to denote the stochastic energy deposition per unitmass from multiple track traversals is the microdosimetricanalog of absorbed dose. Indeed the frequency mean (zF)of a multiple event specific energy spectrum f(z) is undermost circumstances equal to the absorbed dose. However,identical zF’s resulting from differing specific energy spec-tra do not imply equitoxicity. This notion is of immenseimportance for radioimmunotherapy, since microdosime-try can predict widely differing tissue toxicities resultingfrom identical average tissue doses.
E. The scope of microdosimetry
Although traditional microdosimetry from its incep-tion by Rossi and colleagues places emphasis on the sto-chastics of energy deposition primarily at low doses, in thispaper a broader usage of the term has been employed tocover all studies which investigate the deposition of energywithin small target, in particular cell nuclear volumes.
II. METHODS
There are multiple factors which influence the distribu-tion of energy deposition within the sensitive target of thetumor cells: the energy and type of emission, the geometricrelation between the source and target distributions, thekinetics of the radiolabeled antibody uptake, redistributionand clearance from the tumor tissue. For example, radio-labeled antibody may be distributed within the interstitialfluid surrounding the cell; on the surface of the cell; ortaken up and retained within the cytoplasm or nucleusfollowing antibody internalization. The full three-dimensional distribution of activity as a function of time is

537 Humm et al.: Microdosimetric concepts In radioimmunotherapy 537
required for the exact evaluation of a microdosimetricspectrum. Such spectra have been calculated from theoret-ical distributions.12-15
The theory of Rossi and colleagues1 has been used forthe analytical determination of microdosimetric spectra forseveral external radiation fields. The technique involves ob-taining the single event spectrum for the type of radiationin the target volume. The advantage of this method is thatthe single event spectrum needs only to be calculated once.The two event spectrum is the convolution of two singleevent spectra. The three event spectrum is given by theconvolution of a two event spectrum and a single eventspectrum, and so on. By summation of these multiple con-volutions the multiple event energy deposition spectrum isobtained. Roesch expanded this theory to internal emitters,and obtained analytical solutions for a number of nonuni-form distributions of 239Pu particles in tissue.16 Single eventspectra for 2 3 9Pu a-particles were determined by MonteC a r l o m e t h o d s , a n d f r o m p r o p o r t i o n a l c o u n t e rmeasurements.” Using Fourier or Laplace transformmethods to combine single event spectra, specific energyspectra can be evaluated for several geometries very rap-idly. Fisher applied the work of Roesch to evaluate micro-dosimetric spectra for a-emitting radiolabeled antibodiesover a broad class of irradiation geometries.1 2
An alternative approach is the point dose summationmethods by Monte Carlo or other methods. A distributionof sources (which may be located extracellular, on the cellsurface, or intracellular) may be simulated, or obtainedfrom digitized images of autoradiographs.18,19 Each sourcedecay is simulated, an energy and direction of the emissionchosen. For a-particles the tracks are assumed to bestraight. If the line intersects a biological target, the spe-cific energy z deposited is determined by
where m is the target mass, dE/dx the energy depositedper unit track length, tl and t2 are the entrance and exitcoordinates of the track through the target. If the trackends in the target, t2 is the coordinate of the end of rangeof the particle. If a track begins in the target, t 1 is zero.
The total distribution of specific energy f(z) for thecellular targets represents a complete description of thephysical dose deposition throughout the target volume.These physical data can be combined with a biological cellinactivation model to estimate the fraction of cell survi-vors. Such inactivation models evaluate the fraction of cellsurvivors within each energy deposition bin and then per-form a weighted sum of these surviving fractions over thecell populations. 13-15,20
The acquisition of such data from tissue specimens isseverely limited in practice. For the treatment of malignantascites, where the targeted disease may consist of individ-ual free floating cells within the peritoneal cavity, suchdata may be obtainable by in-vitro assay. Small biopsy sam-ples may be retrievable, for example from colorectal ma-lignancies by sigmoidoscopy. Autoradiographic analysisfrom histological sections prepared from biopsies enables
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
the investigator to obtain a detailed picture of a piece of thetumor microcosmos. The usefulness of such data will de-pend upon how representative the specimen proves to be ofthe tumor bulk left remaining. A major limitation of theautoradiographic technique is the loss of temporal infor-mation. An autoradiograph is a “freeze frame” of the ac-tivity distribution in a slice of tissue at the time of specimenfixation. Techniques to adjust autoradiographic grain den-sity data for the redistribution of radiolabeled antibody asa function of time have been proposed by Griffith et al 21 Inthis method micro-thermoluminescent dosimeters (200×400×5000 µm3) are inserted into the tumor tissue toobtain cumulative dose data within a small tumor volumewhich enables the normalization of grain densities acrosseach section. This technique may be of considerable powerwhen considering doses averaged over voxels of severalhundred to thousand micrometer dimensions. It encoun-ters problems when the requirements of source and targetresolution approach those of cellular dimensions, since theTLD integrates indiscriminately the energy depositionfrom all sources within range of the crystal (for P-sources,possibly several millimeters). Thus the fluctuation of doseto individual cells within each voxel over time cannot bedealt with by this approach.
The existence of a time variant nonuniform source dis-tribution gives rise to a formidable microdosimetric prob-lem. Success of the therapy depends upon tumor eradica-tion. Tumor eradication depends upon the sterilization ofmost or possibly all clonogenic tumor cells, which neces-sitates the adequate deposition of dose to each and everyclonogenic tumor cell. Nonuniformity of radiolabeled an-tibody distribution can lead to two sets of opposing conse-quences.
Penetration of the antibody into tumor tissue may resultin antibody collecting in pools as a result of heterogeneityof antigen expression and interstitial fluid flow gradients.The patchy appearance of radiolabeled antibody distribu-tion (apparent from autoradiographs) results in a contin-ual undulation of dose through the tumor. The magnitudesof the dose maxima and minima depend upon the spatialseparation of the sources and the range of the radionuclideemissions. The mean dose can be quite different from theactual dose deposited to the individual tumor cell nuclei,and therefore not a good predictor of biological response.For example, partial radiolabeled antibody localization inthe tumor results in split tumor doses, some regions receiv-ing radiation doses greater than the average tumor dose,and others less. Normalized to the same energy depositionin the tumor, heterogeneity of radiolabel distribution com-monly results in lower cellular toxicity than when the ra-diolabels are uniformly distributed.2 2
Certain conditions of nonuniformity of source distribu-tion can result in a higher level of cell killing than a uni-form distribution. If the sources carried by the antibodyselectively localize on cell surface antigens of some or alltumor cells, then these cells can receive much higher dosesthan the average tissue dose. The antigen expressing tumorcells act to concentrate the radioactivity at the target sites.The magnitude of the dose to cell nuclei from radiolabeled
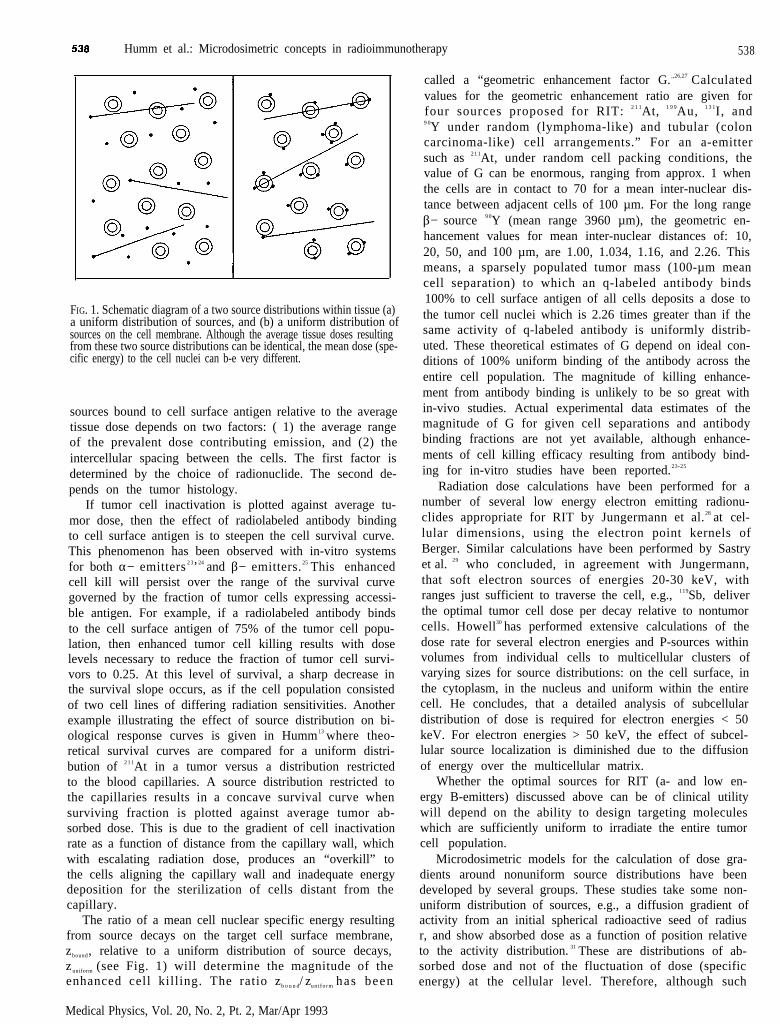
Humm et al.: Microdosimetric concepts in radioimmunotherapy 538
FIG. 1. Schematic diagram of a two source distributions within tissue (a)a uniform distribution of sources, and (b) a uniform distribution ofsources on the cell membrane. Although the average tissue doses resultingfrom these two source distributions can be identical, the mean dose (spe-cific energy) to the cell nuclei can b-e very different.
sources bound to cell surface antigen relative to the averagetissue dose depends on two factors: ( 1) the average rangeof the prevalent dose contributing emission, and (2) theintercellular spacing between the cells. The first factor isdetermined by the choice of radionuclide. The second de-pends on the tumor histology.
If tumor cell inactivation is plotted against average tu-mor dose, then the effect of radiolabeled antibody bindingto cell surface antigen is to steepen the cell survival curve.This phenomenon has been observed with in-vitro systemsfor both α− emitters 2 3’24 and β− emitters. 25 This enhancedcell kill will persist over the range of the survival curvegoverned by the fraction of tumor cells expressing accessi-ble antigen. For example, if a radiolabeled antibody bindsto the cell surface antigen of 75% of the tumor cell popu-lation, then enhanced tumor cell killing results with doselevels necessary to reduce the fraction of tumor cell survi-vors to 0.25. At this level of survival, a sharp decrease inthe survival slope occurs, as if the cell population consistedof two cell lines of differing radiation sensitivities. Anotherexample illustrating the effect of source distribution on bi-ological response curves is given in Humm13 where theo-retical survival curves are compared for a uniform distri-bution of 2 1 1At in a tumor versus a distribution restrictedto the blood capillaries. A source distribution restricted tothe capillaries results in a concave survival curve whensurviving fraction is plotted against average tumor ab-sorbed dose. This is due to the gradient of cell inactivationrate as a function of distance from the capillary wall, whichwith escalating radiation dose, produces an “overkill” tothe cells aligning the capillary wall and inadequate energydeposition for the sterilization of cells distant from thecapillary.
The ratio of a mean cell nuclear specific energy resultingfrom source decays on the target cell surface membrane,zbound, relative to a uniform distribution of source decays,z uniform (see Fig. 1) will determine the magnitude of theenhanced cell killing. The ratio zb o u n d/ zun i fo rm has been
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
called a “geometric enhancement factor G. ,,26,27 Calculatedvalues for the geometric enhancement ratio are given forfour sources proposed for RIT: 2 1 1At, 1 9 9Au, 1 3 1I, and9 0Y under random (lymphoma-like) and tubular (coloncarcinoma-like) cell arrangements.” For an a-emittersuch as 2 1 1At, under random cell packing conditions, thevalue of G can be enormous, ranging from approx. 1 whenthe cells are in contact to 70 for a mean inter-nuclear dis-tance between adjacent cells of 100 µm. For the long rangeβ− source 9 0Y (mean range 3960 µm), the geometric en-hancement values for mean inter-nuclear distances of: 10,20, 50, and 100 µm, are 1.00, 1.034, 1.16, and 2.26. Thismeans, a sparsely populated tumor mass (100-µm meancell separation) to which an q-labeled antibody binds100% to cell surface antigen of all cells deposits a dose tothe tumor cell nuclei which is 2.26 times greater than if thesame activity of q-labeled antibody is uniformly distrib-uted. These theoretical estimates of G depend on ideal con-ditions of 100% uniform binding of the antibody across theentire cell population. The magnitude of killing enhance-ment from antibody binding is unlikely to be so great within-vivo studies. Actual experimental data estimates of themagnitude of G for given cell separations and antibodybinding fractions are not yet available, although enhance-ments of cell killing efficacy resulting from antibody bind-ing for in-vitro studies have been reported.23-25
Radiation dose calculations have been performed for anumber of several low energy electron emitting radionu-clides appropriate for RIT by Jungermann et al.28 at cel-lular dimensions, using the electron point kernels ofBerger. Similar calculations have been performed by Sastryet al. 29 who concluded, in agreement with Jungermann,that soft electron sources of energies 20-30 keV, withranges just sufficient to traverse the cell, e.g., 119Sb, deliverthe optimal tumor cell dose per decay relative to nontumorcells. Howell30 has performed extensive calculations of thedose rate for several electron energies and P-sources withinvolumes from individual cells to multicellular clusters ofvarying sizes for source distributions: on the cell surface, inthe cytoplasm, in the nucleus and uniform within the entirecell. He concludes, that a detailed analysis of subcellulardistribution of dose is required for electron energies < 50keV. For electron energies > 50 keV, the effect of subcel-lular source localization is diminished due to the diffusionof energy over the multicellular matrix.
Whether the optimal sources for RIT (a- and low en-ergy B-emitters) discussed above can be of clinical utilitywill depend on the ability to design targeting moleculeswhich are sufficiently uniform to irradiate the entire tumorcell population.
Microdosimetric models for the calculation of dose gra-dients around nonuniform source distributions have beendeveloped by several groups. These studies take some non-uniform distribution of sources, e.g., a diffusion gradient ofactivity from an initial spherical radioactive seed of radiusr, and show absorbed dose as a function of position relativeto the activity distribution. 31 These are distributions of ab-sorbed dose and not of the fluctuation of dose (specificenergy) at the cellular level. Therefore, although such
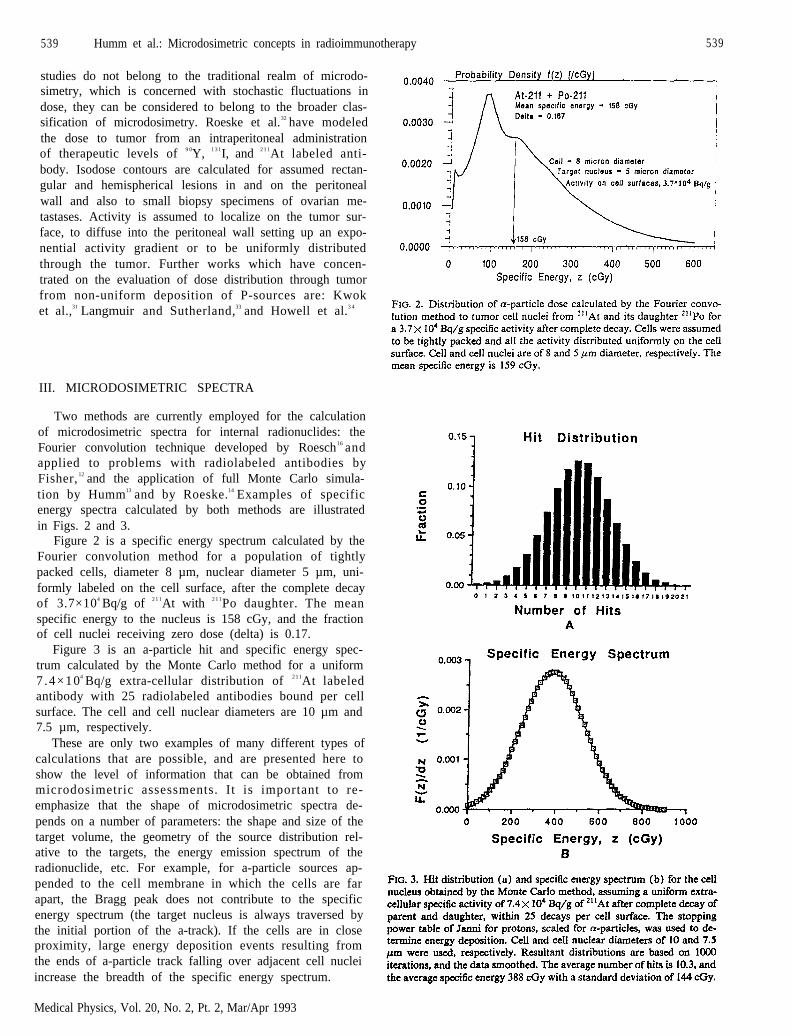
539 Humm et al.: Microdosimetric concepts in radioimmunotherapy 539
studies do not belong to the traditional realm of microdo-simetry, which is concerned with stochastic fluctuations indose, they can be considered to belong to the broader clas-sification of microdosimetry. Roeske et al.32 have modeledthe dose to tumor from an intraperitoneal administrationof therapeutic levels of 9 0Y, 1 3 1I, and 2 1 1At labeled anti-body. Isodose contours are calculated for assumed rectan-gular and hemispherical lesions in and on the peritonealwall and also to small biopsy specimens of ovarian me-tastases. Activity is assumed to localize on the tumor sur-face, to diffuse into the peritoneal wall setting up an expo-nential activity gradient or to be uniformly distributedthrough the tumor. Further works which have concen-trated on the evaluation of dose distribution through tumorfrom non-uniform deposition of P-sources are: Kwoket al.,31 Langmuir and Sutherland,33 and Howell et al.3 4
III. MICRODOSIMETRIC SPECTRA
Two methods are currently employed for the calculationof microdosimetric spectra for internal radionuclides: theFourier convolution technique developed by Roesch16 andapplied to problems with radiolabeled antibodies byFisher, 12 and the application of full Monte Carlo simula-tion by Humm13 and by Roeske.14 Examples of specificenergy spectra calculated by both methods are illustratedin Figs. 2 and 3.
Figure 2 is a specific energy spectrum calculated by theFourier convolution method for a population of tightlypacked cells, diameter 8 µm, nuclear diameter 5 µm, uni-formly labeled on the cell surface, after the complete decayof 3.7×104 Bq/g of 2 1 1At with 2 1 1Po daughter. The meanspecific energy to the nucleus is 158 cGy, and the fractionof cell nuclei receiving zero dose (delta) is 0.17.
Figure 3 is an a-particle hit and specific energy spec-trum calculated by the Monte Carlo method for a uniform7 .4×104 Bq/g extra-cellular distribution of 2 1 1At labeledantibody with 25 radiolabeled antibodies bound per cellsurface. The cell and cell nuclear diameters are 10 µm and7.5 µm, respectively.
These are only two examples of many different types ofcalculations that are possible, and are presented here toshow the level of information that can be obtained frommicrodosimetric assessments. It is important to re-emphasize that the shape of microdosimetric spectra de-pends on a number of parameters: the shape and size of thetarget volume, the geometry of the source distribution rel-ative to the targets, the energy emission spectrum of theradionuclide, etc. For example, for a-particle sources ap-pended to the cell membrane in which the cells are farapart, the Bragg peak does not contribute to the specificenergy spectrum (the target nucleus is always traversed bythe initial portion of the a-track). If the cells are in closeproximity, large energy deposition events resulting fromthe ends of a-particle track falling over adjacent cell nucleiincrease the breadth of the specific energy spectrum.
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

540 Humm et al.: Microdosimetric concepts in radioimmunotherapy 540
IV. CONCLUSIONS
The application of microdosimetry to RIT is the pursuitof the accurate determination of the distribution of dose toindividual tumor cell nuclei comprising the viable tumormass. These data form the basis for a more accurate eval-uation of tumor toxicity. Radiation toxicity which is esti-mated on the basis of a single average dose is practical, butperhaps only a first approximation to the true assessmentof tissue toxicity. How accurate tumor response relationscan be based on average tumor radiation doses is notknown. The usefulness of average radiation doses to pre-dict the level of tumor cell inactivation will most certainlydepend on the antibody/tumor model investigated. How-ever, one may ask whether microdosimetry offers true ad-vantages over traditional dosimetric methods? If the ques-tion is “does microdosimetry assist our understanding ofthe radiobiology of antibody targeted therapy, and will itlead to improved dose-response relations,” the answer ismost definitely in the affirmative. If the question refers tothe clinical utility of microdosimetry, then the answer is areserved yes. Information on the spatial distribution of ra-dionuclide in tumor biopsy samples will assist the clinicianto make judgements on how well and how uniform hisradiolabeled antibody is localizing in tumor tissue. Thedisadvantage of microdosimetry, at the cellular level, is thesize of specimen and the amount of data which can bemeasured and analyzed. In practice one is limited to theevaluation of a few tissue sections from a biopsy specimenwhich may be far less than 1% of the tumor mass. Thefulfillment of the objective of determining the energy dep-osition for all viable tumor cells in a patient belongs to thevery distant future.
One compromise between microdosimetry and macro-dosimetry, is the evaluation of radiation doses within tissuevoxels one or more orders of magnitude greater than indi-vidual cellular dimensions.*’ This technique evaluates theresponse to cell clusters. If only the activity levels varybetween voxels, and not the spatial relationship of thesources to cells, then the evaluation of cell kill on a voxelby voxel basis is an elegant method of data reduction. Theaccuracy in predicting dose-response between this methodand a full microdosimetric method is not known. Cer-tainly, if the greater accuracy of microdosimetry forβ− sources proves superfluous, then its necessity in the fieldmight be restricted to α− and Auger-emitting radionuclidesonly. But until this is proven, study of the microdosimetryof all radionuclides of possible application in RIT needs tobe rigorously investigated.
ACKNOWLEDGMENTS
One of the authors (J. L. Humm) was supported byNCI Grant No. lR03 CA50886. Many thanks to VirginiaLangmuir from SRI International, Menlo Park, California,and Ken Kase from the University of Massachusetts Med-ical Center for their useful remarks and critical appraisal ofthe manuscript.
1H. H. Rossi, “Microscopic energy distributions in irradiated matter,”in Radiation Dosimetry, edited by F. H. Attix, W. C. Roesch, and E.
Medical Physics, Vol. 20, No. 2. Pt. 2, Mar/Apr 1993
Tochlin (Academic, New York, 1968), Vol. I, pp. 43-92.2D.T. Goodhead, “Relationship of microdosimetric techniques to ap-plications in biological systems, ” in The Dosimetry of Ionizing Radia-tion. edited by K. R. Kase, B. E. Bjarngard, and F. H. Attix (Aca-demic, Orlando, 1987), Vol. II, pp. l-89.
3T. R. Munro, “The relative radiosensitivity of the nucleus and cyto-plasm of the chinese hamster fibroblasts,” Radiat. Res. 42, 451-470(1970).
4A. I. Kassis, R. W. Howell, K. S. R. Sastry, and S. J. Adelstein,“Positional effects of Auger decays in mammalian cells in culture,” inDNA Damage by Auger Emitters, edited by K. F. Baverstock and D. E.Charlton (Taylor & Francis, London, 1988), pp. l-13.
5K. G. Hofer. “Radiation biology and potential therapeutic applicationsof radionuclides,” Bull Cancer (Paris) 67, 343-353 (1980).
6R. B. Painter, “The role of DNA damage and repair in cell kill inducedby ionizing radiation,” in Radiation Biology of Cancer Research, editedby R. E. Meyn and H. R. Withers (Raven, New York, 1980), pp.59-68.
7P. Auger. “Sur les rayons β secondaires produit dans un gaz par desrayons X,” Comptes Rendus 180, 65-68 ( 1925).
8D. V. Woo, D. Li. J. A. Mattis, and Z. Steplewski, "Selective chromo-somal damage and cytotoxicity of I-125-labeled monoclonal antibody17-l-A in human cancer cells," Cancer Res. 49, 2952-2958 (1989).
9J. L. Humm and D. E. Charlton, “A new calculation method to assessthe therapeutic potential of Auger electron emission,” Int. J. Radiat.Oncol. Biol. Phys. 17, 351-360 (1989).
10A. M. Kellerer and D. Chmelevsky, “Criteria for the applicability ofLET,” Radiat. Res. 63, 226-234 (1975).
11ICRU Report 36, “Microdosimetry,” International Commission onRadiation Units and Measurements. Bethesda, Maryland, 1983.
12D. R. Fisher, “The Microdosimetry of monoclonal antibodies labeledwith alpha particles,” 4th Int. Symp. Radiopharm. Dosim. Symp.,CONF-851113: pp. 446-457, edited by A. T. Schlafke-Stelson and E.E. Watson (Oak Ridge, Tennessee, 1986).
13J. L. Humm “A microdosimetric model of astatine-211 labeled anti-bodies for radioimmunotherapy.” Int. J. Radiat. Oncol. Biol. Phys. 13,1767-1773 (1987).
14J. C. Roeske, G. T. Y. Chen, R. A. Atcher, J. Fang, M. Becket, and R.R. Weiselbaum, “A microdosimetric analysis of cell survival curvesfrom irradiation of SQ-20B cells to bismuth labeled monoclonal anti-body 425,” J. Nut. Med. 31, 788 (abstract) (1990).
15D. E. Charlton and R. Sephton, “A relationship between microdosim-etric spectra and cell survival for high-LET irradiation,” Int. J. Radiat.Biol. 59, 447-457 (1991).
16W. C. Roesch, “Microdosimetry of internal sources,” Radiat. Res. 70,494-510 (1977).
17W. A. Glass and L. A. Braby, “A wall-less detector for measuringenergy deposition spectra,” Radiat. Res. 39, 230-240 (1969).
18T. E. Hui, D. R. Fisher, O. W. Press, J. F. Eary, J. N. Weinstein, C. C.Badger, and I. D. Bernstein, “Localized beta dosimetry of I-131-labeledantibodies in follicular lymphoma,” Med. Phys. 19, 97-104 (1992).
19P. L. Roberson, R. K. Ten Haken, D. L. McShan, P. E. McKeever, andW. D. Ensminger, “Three dimensional tumor dosimetry for hepaticyttrium-90-microsphere therapy,” J. Nucl. Med. 33, 735-738 (1992).
20V. P. Bond, M. N. Varma, C. A. Sondhaus, and L. E. Feinendegen,“An alternative to absorbed dose, quality and RBE at low exposure,”Radiat. Res. Suppl. 104, S52-257 (1985).
21M. H. Griffith, E. D. Yorke, B. W. Wessels, G. L. DeNardo, and W. P.Ncacy, “Direct dose conformation of quantitative autoradiographywith micro-TLD measurements for radioimmunotherapy,” J. Nucl.Med. 29, 1795-1809 (1988).
22E. D. Yorke, B. W. Wessels, and E. W. Bradley, “Dose averages anddose heterogeneities in radioimmunotherapy,” Antib. Immunoconj.Radiopharm. 4, 623-630 (1991).
23R. W. Kozak, R. W. Atcher, O. A. Gansow, A. M. Friedman, J. J.Hines, and T. A. Waldmann, “Bismuth-212-labeled anti-Tat mono-clonal antibody: a-particle emitting radionuclides as modalities for ra-dioimmunotherapy,” Proc. Natl. Acad. Sci. USA 83, 474-478 (1986).
24R. M. Macklis, B. M. Kinsey, A. I. Kassis, J. L. M. Ferrara, R. W.Atcher. J. J. Hines, C. N. Coleman, S. J. Adelstein, and S. J. Burakoff,“Radioimmunotherapy with alpha-particle-emitting immunoconju-gates.” Science 240, 1024-1026 (1988).
25F. S. Gaedicke, J. L. Humm, C. C. Lau, R. M. Macklis, G. Bastert, andR. C. Knapp, “Analysis of cytotoxicity of I-131-labeled OC125 F(ab’)s

541 Humm et al.: Microdosimetric concepts In radioimmunotherapy 541
on human epithelial ovarian cancer ceil lines,” Radiother. Oncol. 23,150-159 (1992).
26J. L. Humm and L. M. Cobb, “Nonuniformity of tumor dose in radio-immunotherapy,” J. Nucl. Med. 31, 75-83 (1990).
27J. L. Humm, L. M. Chin, L. M. Cobb, and R. Begent, “Microdosim-etry in radioimmunotherapy,” Radiat. Prot. Dosim. 31, 433-436(1990).
28J. A. Jungermann, K. H. P. Yu, and C. I. Zanelli, “Radiation absorbeddose estimates at the cellular level for some electron-emitting radionu-elides for radioimmunotherapy,” Int. J. Appl. Radiat. Isot. 35, 883-888(1984).
29K. S. R. Sastry, C. Haydock, A. M. Basha, and D. V. Rao, “Electrondosimetry for radioimmunotherapy: Optimal electron energy,” Radiat.Prot. Dosim. 13, 249-252 (1985).
30R. W. Howell, D. V. Rao, and C. Haydock, “Dosimetry techniques fortherapeutic applications of incorporated radionuclides,” in Dosimetry
of Administered Radionuclides, edited by S. J. Adelstein, A. I. Kassis,and R. W. Burt (The American College of Nuclear Physicians, U. S.Department of Energy, 1990), pp. 215-252.
“C. S. Kwok. W. V. Prestwich. and B. C. Wilson, “Calculation of radi-ation doses for nonuniformly distributed β and γ radionuciides in softtissue,” Med. Phys. 12, 405-414 (1985).
32J. C. Roeske, G. T. Y. Chen, R. A. Atcher. C. Pelizzari, J. Rotmensch,D. Haraf, A. Montag, and R. Weichselbaum, “Modeling of dose totumor and normal tissue from intraperitoneal radioimmunotherapywith alpha and beta emitters,” Int. J. Radiat. Oncol. Biol. Phys. 19,1539-1548 (1990).
33V. K. Langmuir and R. M. Sutherland, “Dosimetry models for radio-immunotherapy,” Med. Phys. 15, 867-873 (1988).
34R. W. Howell, D. V. Rao, and K. S. R. Sastry, “Macroscopic dosim-etry for radioimmunotherapy: Nonuniform activity distributions insolid tumors,” Med. Phys. 16, 66-74 ( 1989).
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993


Multicellular dosimetry for beta-emitting radionuclides: Autoradiography,thermoluminescent dosimetry and three-dimensional dose calculations
E. D. YorkeGeorge Washington University Medical Center, Washington. DC 20037
L. E. Williams and A. J. DemideckiCity of Hope Medical Center, Duarte, California 91010
D. B. Heidorn and P. L. RobersonUniversity of Michigan Medical School, Ann Arbor, Michigan 48109
B. W. WesselsGeorge Washington University Medical Center, Washington, DC 20037
(Received 18 March 1992; accepted for publication 23 November 1992)
Inhomogeneities in activity distributions over distances from 10 to 104µm are observed in manytumors treated with radiolabeled antibodies. Resulting nonuniformities in absorbed dose mayhave consequences for the efficacy of radioimmunotherapy. Activity variations may be directlystudied with quantitative autoradiography (ARG). Converting these data to absorbed dosedistributions requires additional information about pharmacokinetics, the use of a point sourcefunction and consideration of the complete three-dimensional activity distribution, as obtainedfrom sequential autoradiographic slices. Thermoluminescent dosimetry with specially preparedCaSO4:Dy dosimeters implanted into tissue can directly measure absorbed dose in selectedregions. The conditions under which thermoluminescent dosimeters (TLD) are used differmarkedly from “normal” use conditions in external beam radiotherapy. Therefore special cali-bration and quality assurance precautions are needed to assure the precision of this technique.Procedures and pitfalls in the use of both techniques in radioimmunotherapy are described.
I. INTRODUCTION
A major concern of external beam radiotherapy is the de-sign of beam configurations which produce a uniform dosedistribution over the tumor volume. In radioimmunother-apy, (RIT) as with other radiopharmaceutical therapies,the activity distribution is determined by biological factorswith large associated uncertainty. Nonuniform distribu-tions of activity and of absorbed dose may result.
The technique of autoradiography (ARG) is wellknown.’ For over a decade ARG has been used to demon-strate activity heterogeneity on the multicellular size scale(10 -104µm) for conventional radiopharmaceuticals?”and more recently for radiolabeled antibodies5-7 The filmdensity may be calibrated with standard activity samples,leading to quantitative measurements of activity of distri-butions with submillimeter spatial resolution in the planeof the tissue section.
Calculations of absorbed dose distributions for idealizedactivity distributions of beta particle emitters demonstratethat when the absorbed dose is delivered primarily by par-ticulate radiation of short range, heterogeneous activitydistributions will lead to doses which are nonuniform onapproximately the same distance scale.8-11 Autoradiogra-phy frequently reveals irregular activity distributions intumors. In such situations, calculations based upon geo-metrically simple shapes are of limited utility. QuantitativeARG can provide the spatial activity distribution neededto calculate instantaneous dose rate distributions. But this
technique cannot yield total absorbed dose distributionswithout further assumptions. This is because absorbed dosedistributions are as much determined by pharmacokineticsof antibody uptake and clearance as by the geometric dis-tribution of activity. Autoradiography, however, showsonly a “freeze frame” of the activity distribution at thetime the tumor was resected and frozen.
Direct in vivo measurements of cumulative doses to tis-sues during RIT can be made using thermoluminescentdosimeter(s) (TLD). This technique is well established inmedical and health physics.12,13 TLD materials used forRIT beta dosimetry must meet some special criteria. Thephysical size of the dosimeter should be small compared tothe average beta range (e.g., 0.4 mm for I-131) in orderthat the dosimeter not perturb the dose distribution in itsvicinity. Small size is also necessary to assure good spatialresolution and to avoid disruption of the tissues into whichthey are implanted. The light output per unit absorbeddose must be large enough to produce a useful signal de-spite the small volume of material. Additionally, since theabsorbed dose is delivered by a spectrum of beta particles,it is necessary to choose a material whose thermolumines-cent response is insensitive to beta energy for the radionu-clide of interest. Using TLD that meet these criteria, largevariations in absorbed dose in association with autoradio-graphs which show strong activity heterogeneity have beendirectly measured.’
ARG and thermoluminescent dosimetry are comple-mentary techniques. ARG provides a wealth of “geo-
543 Med. Phys. 20 (2), Pt. 2, Mar/Apr 1993 0094-2405/93/020543-08$01.20 © 1993 Am. Assoc. Phys. Med. 543
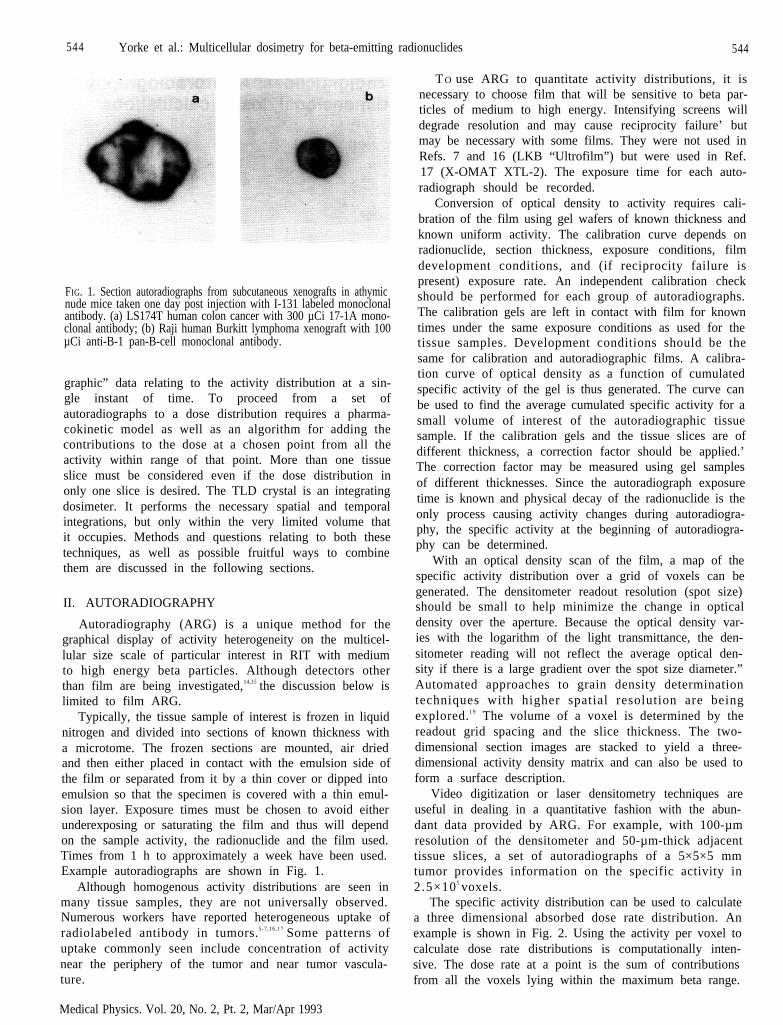
544 Yorke et al.: Multicellular dosimetry for beta-emitting radionuclides 544
FIG. 1. Section autoradiographs from subcutaneous xenografts in athymicnude mice taken one day post injection with I-131 labeled monoclonalantibody. (a) LS174T human colon cancer with 300 µCi 17-1A mono-clonal antibody; (b) Raji human Burkitt lymphoma xenograft with 100µCi anti-B-1 pan-B-cell monoclonal antibody.
graphic” data relating to the activity distribution at a sin-gle instant of time. To proceed from a set ofautoradiographs to a dose distribution requires a pharma-cokinetic model as well as an algorithm for adding thecontributions to the dose at a chosen point from all theactivity within range of that point. More than one tissueslice must be considered even if the dose distribution inonly one slice is desired. The TLD crystal is an integratingdosimeter. It performs the necessary spatial and temporalintegrations, but only within the very limited volume thatit occupies. Methods and questions relating to both thesetechniques, as well as possible fruitful ways to combinethem are discussed in the following sections.
II. AUTORADIOGRAPHY
Autoradiography (ARG) is a unique method for thegraphical display of activity heterogeneity on the multicel-lular size scale of particular interest in RIT with mediumto high energy beta particles. Although detectors otherthan film are being investigated,14,15 the discussion below islimited to film ARG.
Typically, the tissue sample of interest is frozen in liquidnitrogen and divided into sections of known thickness witha microtome. The frozen sections are mounted, air driedand then either placed in contact with the emulsion side ofthe film or separated from it by a thin cover or dipped intoemulsion so that the specimen is covered with a thin emul-sion layer. Exposure times must be chosen to avoid eitherunderexposing or saturating the film and thus will dependon the sample activity, the radionuclide and the film used.Times from 1 h to approximately a week have been used.Example autoradiographs are shown in Fig. 1.
Although homogenous activity distributions are seen inmany tissue samples, they are not universally observed.Numerous workers have reported heterogeneous uptake ofradiolabeled antibody in tumors.5-7,16,17 Some patterns ofuptake commonly seen include concentration of activitynear the periphery of the tumor and near tumor vascula-ture.
Medical Physics. Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
T O use ARG to quantitate activity distributions, it isnecessary to choose film that will be sensitive to beta par-ticles of medium to high energy. Intensifying screens willdegrade resolution and may cause reciprocity failure’ butmay be necessary with some films. They were not used inRefs. 7 and 16 (LKB “Ultrofilm”) but were used in Ref.17 (X-OMAT XTL-2). The exposure time for each auto-radiograph should be recorded.
Conversion of optical density to activity requires cali-bration of the film using gel wafers of known thickness andknown uniform activity. The calibration curve depends onradionuclide, section thickness, exposure conditions, filmdevelopment conditions, and (if reciprocity failure ispresent) exposure rate. An independent calibration checkshould be performed for each group of autoradiographs.The calibration gels are left in contact with film for knowntimes under the same exposure conditions as used for thetissue samples. Development conditions should be thesame for calibration and autoradiographic films. A calibra-tion curve of optical density as a function of cumulatedspecific activity of the gel is thus generated. The curve canbe used to find the average cumulated specific activity for asmall volume of interest of the autoradiographic tissuesample. If the calibration gels and the tissue slices are ofdifferent thickness, a correction factor should be applied.’The correction factor may be measured using gel samplesof different thicknesses. Since the autoradiograph exposuretime is known and physical decay of the radionuclide is theonly process causing activity changes during autoradiogra-phy, the specific activity at the beginning of autoradiogra-phy can be determined.
With an optical density scan of the film, a map of thespecific activity distribution over a grid of voxels can begenerated. The densitometer readout resolution (spot size)should be small to help minimize the change in opticaldensity over the aperture. Because the optical density var-ies with the logarithm of the light transmittance, the den-sitometer reading will not reflect the average optical den-sity if there is a large gradient over the spot size diameter.”Automated approaches to grain density determinationtechniques with higher spatial resolution are beingexplored.1 9 The volume of a voxel is determined by thereadout grid spacing and the slice thickness. The two-dimensional section images are stacked to yield a three-dimensional activity density matrix and can also be used toform a surface description.
Video digitization or laser densitometry techniques areuseful in dealing in a quantitative fashion with the abun-dant data provided by ARG. For example, with 100-µmresolution of the densitometer and 50-µm-thick adjacenttissue slices, a set of autoradiographs of a 5×5×5 mmtumor provides information on the specific activity in2.5×105 voxels.
The specific activity distribution can be used to calculatea three dimensional absorbed dose rate distribution. Anexample is shown in Fig. 2. Using the activity per voxel tocalculate dose rate distributions is computationally inten-sive. The dose rate at a point is the sum of contributionsfrom all the voxels lying within the maximum beta range.

Yorke et al.: Multicellular dosimetry for beta-emitting radionuclides 545
FIG. 2. Three-dimensional dose rate distributions for tumor xenograftsfrom Fig. 1. The color scale is black, dark blue, light blue, pink, lightgreen, dark green, light peach, dark peach, dark red, red, orange in equalascending dose-rate intervals. Higher dose rate regions cycle back toblack, dark blue, etc. (a) LS174T human colon cancer with 17-1A mon-oclonal antibody, dose-rate interval 2.5 cGy/h, mean dose rate 7.6 cGy/h;(b) Raji human Burkitt lymphoma xenograft with anti-B-1 pan-B-cellmonoclonal antibody, dose-rate interval 0.4 cGy/h, mean dose rate 2.4cGy/h.
This includes voxels both in and out of the autoradio-graphic slice containing the point of interest. A suitablepoint source function must be used to provide the distancedependence appropriate to the radionuclide.20-23 Robersonet al.17 adapted brachytherapy software to perform thistask. A “voxel dose rate distribution” per unit activity wasgenerated using up to 500 equally spaced point sourcesdistributed over a voxel and the dose point kernel of Ref.21. This voxel dose rate calculation was carried out beyondthe range of the beta particles. Each of 5000 to 8000 voxelpositions (0.5-mm voxel spacing for I-131) were assignedthe voxel dose rate distribution, weighted by the specificactivity in that voxel. The source distributions were thensummed in three dimensions. The calculation time invest-ment (100-200 h on a VAX 8800) limited the number ofsource positions which could be used. Based on the meanbeta range, the optimal voxel size for I-131 is approxi-mately 100 µm, which increases the number of source
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
points by a factor of 125. To reduce the calculation time,Fourier transforms could be used.9
In general, activity distributions which vary over dis-tances comparable to the beta particle range will producedose-rate distributions which vary strongly over the samelength scale. Smaller scale (less than beta range) activityheterogeneities will produce less dramatic dose rate varia-tions, since the dose at a point is delivered by beta particlesfrom both “hot” and “cold” portions of the tissue. 7-11,17,24
Thus computational effort to produce three-dimensionaldose or dose rate distributions depends on the range of thebeta particles and the tumor size.
Conversion of the activity distributions obtained byARG to the cumulative absorbed dose distribution pro-duced during the administration of RIT-that is, duringthe time that the tissue was in a living host-is notstraightforward. The dose distribution depends on the in-dividualized pharmacokinetics of the radiolabeled antibodyin vivo. The autoradiograph provides only a “freeze frame”view of the activity distribution at the time of tumor resec-tion. At best ARG gives indirect information about thetime dependence of the biological processes of uptake andclearance of the antibody during the RIT.
To provide the necessary missing kinetic information, itmight be possible to model the pharmacokinetics. Diffu-sion model equations have been applied to dosimetry cal-culations for multicellular spheroids25 and simulated tu-mor nodules.26 It may be possible to extend such models totumors in vivo to provide kinetic input to cumulated dosedistribution calculations.
In an alternative approach many groups have measuredaverage specific activity as a function of time for tumorsand various organs by noninvasive imaging techniques inhumans and by serial sacrifice in small animal models for avariety of antibody carrier/radionuclide combinations.27-30
Assumptions must then be made as to how small scaleheterogeneities vary with time (e.g., do “hot” and “cold”regions remain in the same ratio to the average throughoutRIT?). The resulting time dependence must be combinedwith the radionuclide’s physical decay to obtain a modelcumulated activity distribution based on the autoradio-graphic information. While several groups have discussedsuch a program, it has not yet been carried out. Griffith,et al.7 used purely physical decay to generate dose distri-butions from autoradiographs. Recently Roberson,et al. 17,24 generated three-dimensional dose rate distribu-tions characteristic of discrete times of sacrifice and rec-ommended sampling the dose rate distributions at a mini-mum of four to six time points.24 For tumors which wereapproximately matched in size, the variability in dose pervolume element was observed to be small compared to thevariability at different time points. Thus it might be possi-ble to sum dose rate calculations from different tumors,resected at different time points, by identifying areas ofsimilar composition (e.g., similar vascularization and/orproximity to the periphery). Further work is needed todevelop and validate models of antibody carrier pharma-cokinetics on the multicellular size scale in order to reli-ably translate the activity distributions visualized with
546 Yorks et al.: Multicellular dosimetry for beta-emitting radionuclides 546
quantitative autoradiography into absorbed dose distribu-tions.
III. THERMOLUMINESCENT DOSIMETRY
Studies done with thermoluminescent dosimetry give in-formation which is complementary to that provided byARG. TLD materials are crystalline solids in which ion-izing radiation can excite electrons into metastable trappedstates. The number of such electrons is proportional to theabsorbed dose received. The electrons can be released fromthese states by heating. Thereupon they recombine withholes, giving off excess energy in the form of thermolumi-nescent photons, which can be counted with a photoelec-tric tube. The light output is proportional to the absorbeddose received by the TLD but also depends on materialproperties, irradiation conditions, heating conditions, andthe electronics of the TLD reader. Therefore, if thermolu-minescent dosimeters are to be used for absorbed dosemeasurements, they must be calibrated.
Appropriately calibrated TLD implanted directly intotissue yields the total dose absorbed by the TLD materialduring its time in situ. The TLD automatically integratesover the spatial and temporal distribution of all the activitywithin the beta particle range of its location (and, ofcourse, also accounts for the absorbed dose contributed bypenetrating radiation from distant sites). However, thedose in only a small volume is recorded, as opposed to theglobal activity distribution information provided by ARG.
The conditions under which TLD are used in RIT do-simetry differ markedly from those in health physics orradiation therapy. This leads to special requirements in thefabrication and calibration of the dosimeters. As noted inthe Introduction, the TLD must be of small cross sectioncompared to the beta particle range. Wessels and co-workers found that CaSO4:Dy met the dual requirementsof high sensitivity (light output gm-1 c G y- 1) and weakenergy dependence for I-131 and higher energy betaemitters. 31 They and others7,27,32-39 have fabricated TLDsof dimensions 0.2×0.4×5 mm or less, implanted theminto animals or tumor model systems receiving RIT andperformed in vivo absorbed dose measurements. Tech-niques of fabrication, quality assurance, calibration and invivo use of these TLDs were developed by Wessels andGriffith. 7,31 Similar procedures have been adopted at ap-proximately 15 institutions including those involved inRefs. 32-39. In the following discussion, CaSO4:Dy dosim-eters are emphasized because of their extensive applicationin RIT dosimetry.
The starting materials are 400-µm-thick 1.2-cm-diameter CaS04:Dy impregnated teflon disks (Teledyne,Inc.). The disks are imbedded in a 2x2 cm paraffin blockand sliced with a well-sharpened tissue section microtometo a thickness of 200 µm and a length of 500 µm, yieldingdosimeters of final dimensions 0.2x0.4x5 mm. These do-simeters conveniently fit inside a 20-gauge needle. Eachdosimeter is measured (by micrometer) to insure geomet-ric batch uniformity (±3%). For initial studies31 the do-simeters were also weighed using a microgram balance.
Medical Physics, Vol. 20, No. 2. Pt. 2, Mar/Apr 1993
After being cut, the excess paraffin is removed and theTLD are annealed. External beam calibration may be per-formed using a calibrated low megavoltage (4 MV or Co-60) beam with full buildup. The dosimeters are then readin a commercial TLD reader under dry nitrogen. Differentgroups have used slightly different heat cycle settings (e.g.,Ref. 7 uses a 5-s preheat at 115° followed by glow peakintegration over 50 s from 115°C to 275°C with tempera-ture ramping at 3.6°C/s). Batches of “mini-TLD” withresponse uniformity better than ±10% are readily ob-tained.
Linearity of light output (LO) versus dose should bemeasured with external beam over the entire range of ab-sorbed doses expected in RIT (5 to 5000 cGy). Deviationof a log-log plot of LO versus absorbed dose from a 45° lineindicates supralinearity or saturation. Supralinearity hasbeen reported above 500 cGy by some workers36,40 but notseen up to 1000 cGy by others.29 This effect may depend onthe batch of material or on preparation techniques. Supra-linearity can be appreciable. Demidecki and co-workershave seen an increase by a factor of 1.7 of the LO per cGyor calibration factor as absorbed dose is increased from 50to 3000 cGy.40,41 Therefore it is essential to use a measureddose-response curve and not to assume that the calibrationfactor is independent of dose.
External beam exposures are of short (minutes) dura-tion, after which the TLD material is stored in air at roomtemperature and usually read out within 1-2 days. In RITapplications, the TLD is imbedded in tissue at mammalianbody temperature and physiological pH. The tissue con-tains an activity distribution of beta-emitting radionuclide,exposing the TLD to low dose rate (approximately 10cGy/hr) beta and gamma radiation for times ranging froma few days to two weeks. Upon removal, the TLD must becleaned of residual tissue before being read. The TLD is arelative dosimeter; absorbed dose in an investigational sit-uation is determined by the ratio of the LO to the outputfrom a similar (or the same) TLD given a known dose.Additional calibration should therefore be performed un-der conditions which closely resemble the conditions ofactual use, as the calibration factor may well depend onthese conditions.
For this purpose the TLD are cross calibrated with uni-form activity distributions of the radionuclide of interest.The dosimeters are immersed for times ranging from min-utes to 2 weeks in gels (e.g., Knox Gelatin) prepared withknown uniform activity. After removal from the gel, eachdosimeter must be thoroughly washed and then read on theTLD reader. The calibration medium is large compared tothe beta range so the absorbed dose to the medium can becalculated via the beta particle equilibrium dose constantand an absorbed fraction of one. If the TLD are to be usedunder conditions where the penetrating radiation dose isexpected to be important, calibration in a larger phantomor with an added external x-ray irradiation might be ad-visable to obtain a combined calibration factor.
The radionuclide calibration factor may well be differ-ent from the standard external x-ray beam factor. Refer-ence 31 reports the same (15%) factor for 4 MV as for

547 Yorke et al.: Multicellular dosimetry for beta-emitting radionuclides 547
I-131, Y-90 and P-32 gels. However, in later work from thesame laboratory, I-131 calibration factors as low as 60% ofthe 4-MV factor were measured and a calibration factor ofapproximately 70% was measured for a smaller (0.1 X0.14X2.5 mm) set of TLD.39 Heidorn observed a similar (ap-proximately 40%) discrepancy between Co-60 and I-131.42
Stewart et al.43 saw similar differences between 4-Mev elec-trons and I-131 solutions using 6×1×1 mm Lif rods whileY-90 solution data coincided with 4-Mev electrons.
There are at least three reasons for expecting a differ-ence in calibration factor between external megavoltagex-rays and beta particle irradiation in solution or gel.
( 1) The LO of the TLD may have intrinsic energy de-pendence. This may be checked using external irradiationat different nominal electron beam energies or with betasources. At least part of this effect is due to the thickness ofthe TLD relative to the beta particle range in TLDmaterial. 4 4 Demidecki, et al. find that for Y-90, the energydependence is within 10% for mini-TLD.4 1
(2) In radioactive gel or solution, the finite size of theTLD excludes radioactive material from points within itsvolume. Demidecki, et al. have called this the “void vol-ume” effect.20,41 The absence of radioactivity reduces theabsorbed dose to the TLD. Demidecki et al. have per-formed calculations of this effect for Y-90 and I-131. Thedose reduction depends on the TLD density as well as itssize (i.e., on the beta particle range versus TLD size).Calculations 41 indicate that especially for I-131, the pre-dicted decrease in calibration factor relative to 4-MVx-rays is substantial.
(3) The LO of the TLD also varies with time in themedium. When the TLD are irradiated with external beamand stored in air at room temperature, they show less than5% fading per month. However, for irradiation in mediumover days to weeks, the fading properties depend upon themedium (e.g., temperature and pH) as well as the time inthe medium and the total dose. The surface to volume ratioof the TLD material probably plays a role; the effect mayalso depend on the batch of material purchased from thevendor.
Experiments performed by Wessels and co-workersfrom 1984 to 1988 with one group of TLD material showedno fading for TLD irradiated in aqueous media 31 at roomtemperature. However, experiments with newer materialby Demidecki and collaborators,41 and Svenberg45 showfading by a factor of up to 50% in 20 days for mini-TLDirradiated in Y-90 gel for 20 days. The effect is larger forgeometries with a larger surface to volume ratio. For a6-mm diameter, 20-µm-thick CaSO4:Dy disk, Demideckiet al40,41 report an approximately exponential decrease inLO with time by a factor of five over 20 days in cell me-dium and by a factor of 10 for the same time in gel. Thisfading appears to be irreversible. After the TLD has beencleaned, read, and annealed it does not regain its initialsensitivity.
Since it is not presently possible to theoretically accountfor these effects, it is necessary to calibrate the dosimetersfor in vivo RIT dosimetry using conditions as close as pos-sible to those under which they are used. This will mini-
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
mize the impact of pH, temperature and the “void volume”effect and will help account for possible interplay betweensupralinearity and fading.
The mini-TLD can be implanted into animal modelsundergoing RIT and left in place for days to several weeks.They can also be implanted into animals receiving externalbeam (e.g., 4 MV) irradiation to a known dose as a checkon the effect of biological conditions on the thermolumi-nescent response. A recent study reports fading underthese circumstances.4 6 Mini-TLD have also been exten-sively checked for signs of degradation due to biologicalconditions.’ None were seen. Before reading a TLD whichhas been implanted in tissue it is important that it be care-fully cleaned and dried.
In RIT, the mini-TLD yield an average (over the lengthof the dosimeter) dose to the nearby surrounding tissue.Agreement with average doses calculated from organ ortumor-average cumulated activities obtained by serial sac-rifice of similarly treated animal models is generallygood. 27,33,34 These calculations have incorporated bound-ary corrections as necessary for organs or tumors whichare small compared to the beta particle range. Activityheterogeneity within the tissue is not included. In thiswork, possible fading due to time in aqueous medium, pH,temperature and “void volume” effects have been correctedfor, at least in part, by appropriate calibration.
The mini-TLD have good spatial resolution for dosegradients along their thin (0.2 and 0.4 mm) dimensions.However the LO depends on the summed dose along thelong (5 mm) axis. Steep dose gradients were measured incylindrical phantoms containing I-131, Y-90, and P-32.3 1
The spatial resolution along the 5-mm axis can be ex-tracted by slicing the dosimeter. This is the techniquewhich was applied in conjunction with autoradiography.’The tissue sample containing the TLD was quickly frozenin liquid nitrogen. The frozen tissue was then microtomedinto sections (e.g., 20-50 µm) appropriate for autoradiog-raphy, with the slices being approximately perpendicularto the long TLD axis. The resulting micro-TLD chips wereremoved, cleaned, air dried, and read in the same readerand with the same heat cycle as is used for the mini-TLD.
The uniformity of response of the micro-TLD was in-vestigated by Wessels and Griffith31 and by Heidorn et al..47
and by Langmuir et al..3 9 Mini-TLD were exposed to cal-ibrated external beams under standard conditions. The do-simeters were then imbedded in suitable solid medium andmicrotomed as described above. Micro-TLD were selectedat random from these samples and read. A standard devi-ation of 10% was observed in Ref. 31 while a standarddeviation ranging from 22% to 32% was reported in thestudy Ref. 47, and a standard deviation of 29% (for 50-µmsections) and 50% for 30-µm sections was reported in Ref.39. The reason for the very different dispersions measuredby different investigators is not, at present, understood butmay be related to differences in TLD grain size. Heidom4 7
using a dissection microscope at 50X magnification, ob-served differences in grain size distribution between micro-TLD batches. Some micro-TLD contained large CaS04:Dycrystals, some had large voids due to crystals pulled from

540 Yorke et al.: Multicellular dosimetry for beta-emitting radionuclides 548
the Teflon matrix by the microtome knife and some had auniform distribution of small crystals. In general, slicethickness must be carefully regulated to improve light out-put uniformity.
There is no predictive index to determine the uniformityof response of a group of micro-TLD. However precisioncan be optimized by individually calibrating each micro-TLD as described by Heidorn, et al.47 Through use of in-dividual calibration factors, standard deviations of 12%were achieved in measurement of a known external beamdose gradient.
IV. COMBINATION OF TECHNIQUES
When absorbed doses measured with micro-TLD ex-tracted from autoradiographs were considered in the con-text of the optical density in the region from which theTLD had been removed, qualitative agreement was ob-served between high absorbed dose and high optical den-sity for tumors7’ 34 and spheroids.39 Good agreement wasfound between micro-TLD measurements and calculateddose gradients in a spheroid model39 where physical decayof I-131 provided the only time dependence. While suchagreement is self evident in situations where physical decayprovides the only time dependence, it is not assured intumors with more complex pharmacokinetics. Addition-ally, the micro-TLD provide the magnitude of the ab-sorbed dose. The combined use of ARG and thermolumi-nescent dosimetry demonstrated quantitatively that largeabsorbed dose gradients can be found in tumors treatedwith RIT. In one sample’ a 200% dose variation was mea-sured within a single slice and a 400% variation was ob-served between slices which were only 500 µm apart.
Since the micro-TLD integrate absorbed dose over time,no biokinetic model is needed to calculate the dose at thesite of the TLD. Wessels et al.48 have suggested that themicro-TLD be used to calibrate the optical density of theautoradiographs. That is, rather than associate optical den-sity with specific activity, one could make a direct relation-ship between OD and absorbed dose via the micro-TLD.Ideally, there should be several micro-TLD at sites in aslice with different OD’s allowing an individualized cali-bration curve (OD versus dose measured by the TLD) tobe generated for a particular tissue sample. Since the TLDintegrates over the spatial as well as the temporal activitydistribution, there is also no need to use a point sourcefunction or to correlate the activity distribution in differentslices. Instead, the OD would be translated directly to ab-sorbed dose through the calibration curve. The accuracy ofthis technique (which estimates the absorbed dose via in-terpolation between micro-TLD readings at two or threepoints per slice) versus the pharmacokinetic modeling ap-proach discussed previously requires further investigation.The use of electronic probes such as MOSFET detectors 49
may be helpful in providing in vivo measurements of doseversus time at a few locations in tissue.
Theoretically, both approaches have potential draw-backs and possible advantages. Autoradiography, by defi-
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
nition, is a destructive process in relation to unique tumorarchitecture. Modeling approaches used to correct autora-diographic information for time varying concentrations areconstrained to use average bulk tumor biodistribution dataor repetitive activity distribution phenomena (e.g., time-varying but predictable tumor rim enhancement) to cor-rect for antibody pharmacokinetics and gross tumor heter-ogenei ty . The combinat ion TLD/ARG methods doinclude a directly measured time integration factor in theabsorbed dose along with a dose distribution which isbased on ARC. However, some uncertainty is entered intothis method by assuming that the “local” assignment of anabsorbed dose value to a particular optical density valueapplies universally throughout the tumor. Perhaps a safestarting point or working hypothesis for both methods isthat any correction for time dependence of antibody phar-macokinetics is superior to simply using physical decay toderive a cumulated activity distribution from autoradiog-raphy patterns.
V. DISCUSSION
The goal of the dosimetric studies presented above is tohelp relate the therapy technique of RIT to the outcome(e.g., tumor regression). ARG demonstrates that tumorsoften exhibit activity distributions which are inhomoge-neous on a distance scale of 10 - 10 4 µm. Both calculationsand in vivo TLD measurements show that these spatialactivity variations are associated with large dosimetricvariations on the same distance scales. The validity of ap-proximating the tumor dose distribution by a single aver-age absorbed dose may therefore be questioned.
In addition to spatial dosimetric inhomogeneities, otherfactors may alter the biological effectiveness of the ab-sorbed dose. Among these are the variation of the dose ratewith time and the possible relationship of cell viability tolocal activity deposition. An understanding of the interre-lationships between tumor pharmacokinetics and spatialand temporal variations of dose rate and total dose depo-sition may be required for reliable prediction of the out-come of tumor therapy. However, a necessary step towardthis goal is improved quantitation of absorbed dose at themulticellular level in tumors.
ACKNOWLEDGMENTS
This work was supported in part by NCI Grants No.CA33572, CA43904 and CA44173.
1A. W. Rogers, Techniques of Autoradiography (Elsevier/North-Holland Biomedical, New York, 1979).
2W. K. Sinclair, J. D. Abbatt, H. E. A. Farran, E. B. Harriss, and L. F.Lamerton, “A quantitative autoradiographic study of radioiodine dis-tribution and dosage in human thyroid glands,” Br. J. Radiol. 29,36-41 (1950).

549 Yorke et al.: Multicellular dosimetry for beta-emitting radionuclides 549
3T. K. Lewellen. M. M. Graham, and A. M. Spence, “Quantitativeautoradiography using a personal computer,” J. Nucl. Med 27, 549-554 (1986).
4Y. Yonekura, A. B. Brill, P. Som, G. W. Bennett, and I. Fand, “Quan-titative autoradiography with radiopharmaceuticals, part 1: Digital filmanalysis system by videodensitometry: Concise Communication.” J.Nucl. Med. 24, 231-237 (1983).
5P. L. Jones, B. M. Gallagher, and H. Sands, “Autoradiographic anal-ysis of monoclonal antibody distribution in human colon and breasttumor xenografts,” Cancer Immunol. Immunother. 22, 134-143(1986).
6J. M. Esteban, J. Schlom, F. Momex, and D. Colcher, “Radioimmu-notherapy of athymic mice bearing human colon carcinomas with mon-oclonal antibody B72.3: Histologic and autoradiographic study of ef-fects on tumors and normal organs,” Eur. J. Cancer Clin. Oncol. 23,643-655 (1987).
7M. H. Griffith, E. D. Yorke, B. W. Wessels, G. L. DeNardo, and W. P.Neacy, “Direct dose confirmation of quantitative autoradiography withmicro-TLD measurements for radioimmunotherapy,” J. Nucl. Med.29, 1795-1809 (1988).
8J. L. Humm, “Dosimetric aspects of radiolabeled antibodies for tumortherapy,” J. Nucl. Med. 27, 1490-1497 (1986).
9C. S. Kwok, W. V. Prestwich, and B. C. Wilson, “Calculation of radi-ation doses for non uniformly distributed beta and gamma radionu-clides in soft tissues,” Med. Phys. 12, 405-412 (1985).
10V. K. Langmuir and R. M. Sutherland, “Dosimetry models for radio-immunotherapy,” Med. Phys. 15, 867-873 (1988).
11R. W. Howell, D. V. Rao, and K. Sastry, “Macrodosimetry for radio-immunotherapy:Nonuniform activity distributions in solid tumors,”Med. Phys. 16, 66-74 (1989).
12Applied Thermoluminescence Dosimetry, edited by M. Oberhofer andA. Scharmann (Adam Hilger Ltd. Bristol, 1981).
“Thermoluminescence and Thermoluminescent Dosimetry, Vols. I, II,and III, edited by Y. L. Horowitz (CRC, Inc., Boca Raton, FL, 1984).
14J. L. Humm, L. M. Chin, R. C. Lanza, C. M. Schaefer, M. Speidel, andR. L. Greene, “Digital imaging for autoradiography,” in ComputedDigital Radiography in Clinical Practice edited by R. E. Greene and J.W. Oestmann (Thieme Medical Publishers, Inc., New York, 1992). pp.167-172.
15R. Mayer, L. E. Dillehay, Y. Zhang, Y. Shao, S. Song, W. C. Lam, andJ. R. Williams, “New method for microdosimetry in radioimmunother-apy using GAF TM chromic media,” Antib. Immunoconj. Radiop-harm. 5, 336 (1992).
16R. L. Vessella, P. H. Lange, D. F. Palme, R. K. Chiou, M. K. Elson,and B. W. Wessels, “Radioiodinated monoclonal antibodies in the im-aging and treatment of human renal cell carcinoma xenografts in nudemice,” in Antibody Mediated Delivery Systems, edited by J. D. Rodwell(Marcel Dekker, Inc., NY, 1988), pp. 245-282.
17P. L. Roberson, D. J. Buchsbaum, D. B. Heidom, and R. K. TenHaken, “Three-dimensional tumor dosimetry for I-131 labeled MoAbusing serial autoradiography,” Int. J. Radiat. Oncol. Biol. Phys. 24329-334 (1992).
18L. J. Van Battron and H. Huizenga, “Film dosimetry of clinical elec-tron beams,” Int. J. Radiat. Oncol. Biol. Phys. 18, 69-76 (1990).
19K. E. Eklund and J. R. Williams, “A method for quantitative autora-diography over stained sections of tumors exposed in vivo to radiola-beled antibodies,” Int. J. Radiat. Oncol. Biol. Phys. 21, 1635-1642(1992).
20R Locvinger, E. M. Japha, and G. L. Brownell, “Discrete radioisotopesources,” in Radiation Dosimetry, edited by G. J. Hine and G. L. M.Brownell (Academic,, NY, 1956), pp. 693-799.
21W. V. Prestwich, J. Nunes, and C. S. Kwok, “Beta dose point kernelsfor radionuclides of potential use in radioimmunotherapy,” J. Nucl.Med. 30, 1036-1046 (1989).
22P. K. Leichner, W. G. Hawkins, and N. C. Yang, “A generalizedempirical point source function for beta particle dosimetry,” Antib.Immunoconj. Radiopharm. 2, 125-144 (1989).
23P. K Leichner and C. S. Kwok, “Tumor dosimetry in radioimmuno-therapy:Methods of calculation for beta particles,” Med. Phys. 20, 529-534 (1993).
24P. L. Roberson, D. J. Buchsbaum, D. B. Heidom, and R. K. TenHaken, “Variations in 3-D distributions of tumor uptake and dosedeposition for I-131 labeled MoAb,” Antib., Immunoconj. Radiop-harm. 4, 43 (1991).
25R. McFadden and C. S. Kwok, “Mathematical model of simultan-
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
eous diffusion and binding of antitumor antibodies in multicellularhuman tumor spheroids,” Cancer Res. 48, 4032-4037 ( 1988).
26K. Fujimori. D. G. Covell, J. E. Fletcher, and J. N. Weinstein, “Amodeling analysis of monoclonal antibody percolation through tumors:A binding site barrier,” J. Nucl. Med. 31, 1191-1198 ( 1990).
27P. K. Leichner, N. C. Yang, B. W. Wessels, W. G. Hawkins, S. E.Order, and J. L. Klein, “Dosimetry and treatment planning in radio-immunotherapy,” in The Present and Future Role of Monoclonal Anti-bodies in the Management of Cancer, edited by J. M. Vaeth and J. L.Meyer (Karger, Basel, Switzerland, 1990), pp. 109-120.
28D. G. Covell, J. Barbet, O. D. Holton, C. D. Black, R. J. Parker, andJ. N. Weinstein, “Pharmacokinetics of monoclonal immunoglobulinG1, F (ab’)2 and Fab’ in mice,” Cancer Res. 46, 3969-3978 (1986).
29J. A. Carrasquillo, P. Sugarbaker, D. Colcher, J. C. Reynolds, J. Es-teban, G. Bryant, A. M. Keenan, P. Perentesis, K. Yokoyama, D. E.Simpson, P. Ferroni, R. Farkas, J. Schlom, and S. M. Larson, “Radio-immunoscintigraphy of colon cancer with I-131 labeled B72.3 mono-clonal antibody,” J. Nucl. Med. 29, 1022-1030 (1988).
30F. Buchegger, A. Vacca, S. Carrel, M. Schreyer, and J-P. Mach, “Ra-dioimmunotherapy of human colon carcinoma by I-131 labeled mon-oclonal anti CEA antibodies in a nude mouse model,” Int. J. Cancer 41,127-134 (1988).
31B. W Wessels and M. H. Griffith, “Miniature thermoluminescent do-simeter absorbed dose measurements in tumor phantom models,” J.Nucl. Med. 27, 1308-1314 (1986).
32B. W. Wessels, R. L. Vessella, D. F. Palme, J. M. Berkopec, G. K.Smith, and E. W. Bradley, “Radiobiological comparison of externalbeam irradiation and radioimmunotherapy in renal cell carcinoma xe-nografts,” Int. J. Radiat. Oncol. Biol. Phys. 17, 1257-1263 (1989).
33J. L. Klein, T. H. Nguyen, P. Laroque, K. A. Kopher, J. R. Williams,B. W. Wessels, L. E. Dillehay, J. Frincke, S. E. Order, and P. K.Leichner, “Yttrium-90 and I-131 radioimmunoglobulin therapy of anexperimental human hepatoma,” Cancer Res. 49, 6383-6389 (1989).
34J. A. Williams, B. W. Wessels, J. A. Edwards, K. A. Kopher, P. M.Wanek, M. D. Wharam, S. E. Order, and J. L. Klein, “Targeting andtherapy of human glioma xenografts in vivo utilizing radiolabeled an-tibodies,” Cancer Res. (Suppl.) 50, 974s-979s (1990).
35D. F. Palme, J. M. Berkopec, B. W. Wessels, M. K. Elson, P. H. Lange,and R. L. Vessella, “Dosimetry and pharmacokinetics of monoclonalantibody A6H with human renal cell carcinoma xenografts: Single dosestudy,” Int. J. Nucl. Med. Biol. 18, 527-537 (1991).
36R. Wessely. H. Bihl, E. Friedrich, and S. Matzku, “Assessment ofradiation dose distribution in xenografts,” in Monoclonal Antibodies:Application in Clinical Oncology, edited by A. Epenetos (Chapman andHall Medical, NY, 1991), pp. 315-322.
37R. K. Chiou, B. W. Wessels, M. Woodson, and C. Limas, “Study ofclinical thermoluminescent dosimeters (CL.TLD) in direct measure-ment of absorbed radiation dose for radioimmunotherapy,” Radiat.Appl. Isot. 42, 181-186 (1991).
38J. Y. C. Wong, L. E. Williams, A. J. Demidecki, B. W. Wessels, and X.W. Yan, “Radiobiologic studies comparing yttrium-90 irradiation andexternal beam irradiation in vitro,” Int. J. Radiat. Oncol. Biol. Phys.20, 715-722 (1991).
39V K. Langmuir, B. W. Wessels, H. L. Mendonca, E. D. Yorke, and L.Montilla, “Comparisons of sectioned micro-tld dose measurementswith predicted dose from I-131 labeled antibody,” Med. Phys. 19,1213-1218 (1992).
40A. J. Demidecki, L. E. Williams, and J. Y. C. Wong, “Calibration ofthermoluminescent dosimeters for beta radiation,” Antib. Immuno-conj. Radiopharm. 4, 52 (1991).
41A. J. Demidecki, L. E. Williams, J. Y. C. Wong, B. W. Wessels, E. D.Yorke, M. Strandh, and S. Strand, “Considerations on the calibrationof small thermoluminescent dosimeters (TLDs) used for measurementof beta particle absorbed doses in liquid environments,” in press, Med.Phys. (1993).
42D. B. Heidom, personal communication.43J. S. W. Stewart, V. Hird, D. Snook, M. Sullivan, G. Hooker, N.
Courtenay-Luck, G. Sivdapenko, M. Griffiths, M. J. Meyers, H. E.Lambert, A. J. Munro, and A. A. Epenetos, “Intraperitoneal radioim-munotherapy for ovarian cancer: Pharmacokinetics, toxicity and effi-cacy of I-131 labeled monoclonal antibodies,” Int. J. Radiat. Oncol.Biol. Phys. 16, 405-413 (1989).
44A. S. Pradhar and R. C. Bhatt, “Graphite mixed CaSo4:Dy teflon TLDdiscs for beta dosimetry,” Phys. Med. Biol. 22, 873-879 (1977).
45A. Svenberg, personal communication.

550 Yorke et al.: Multicellular dosimetry for beta-emitting radionuclides 550
46S-E Strand, A. Svenberg, M. Strandh, and K. Norrgren. “Parametersaffecting the accuracy of in vivo dosimetry with mini-TLD,” Med.Phys. 19. 781 (1992).
4 7B Heidorn, D. J. Buchsbaum. P. L. Roberson, and R. K. TenHaken, “A sensitivity study of micro-TLD’s for in vivo dosimetry ofradiolabeled antibodies,” Med. Phys. 18, 1195-1199 (1991).
48B. W. Wessels and E. D. Yorke. Biology of Radionuclide Therapy,edited by G. L. DeNardo, J. P. Lewis, A. Raventos, and R, W. Burt(ACNP Publication No. 308, Washington, DC, 1989). pp. 216-222.
49D. J. Gladstone and L. M. Chin, “Automated data collection andanalysis system for MOSFET radiation detectors,” Med. Phys. 18,542-548 (1991).
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

Experimental radioimmunotherapyDonald J. Buchsbauma )
Department of Radiation Oncology, University of Alabama at Birmingham, Birmingham, Alabama 35233
Virginia K. LangmuirLife Sciences Division, SRI International, Menlo Park, California 94025
Barry W. WesselsDepartment of Radiology, George Washington University Medical Center, Washington, DC 20037
(Received 18 March 1992; accepted for publication 20 October 1992)
Radiolabeled monoclonal antibodies have been used for radioimmunotherapy studies with hu-man tumor spheroids and murine and human tumor xenografts in experimental animals. Thispaper reviews the work that has been performed in these models with different types of cancer,and highlights those papers that have presented dosimetry estimates and attempts to correlatethe findings. Radioimmunotherapy studies in multicell spheroids, as a model for microme-tastases, have been performed in human neuroblastoma, colon cancer, and melanoma cell linesusing 1 3 1I-, 1 2 5I-, 1 8 6Re-, and 212Bi-labeled antibodies. The uniform geometry of the spheroid hasallowed radiation dose estimates to be made. Up to three logs of cell kill have been achieved with1311- and 186Re-specific antibody with minimal toxicity from labeled nonspecific antibody, but212Bi-antibody had little effect because of its short half-life as shown by Langmuir. It appearsthat the two most important factors for therapeutic efficacy in this model are good penetrationof the radiolabeled antibody and an adequate radionuclide half-life to allow penetration of theimmunoconjugate prior to significant radionuclide decay. Radioimmunotherapy studies in ani-mals bearing transplants of colon cancer, leukemia, lymphoma, hepatoma, renal cell carcinoma,neuroblastoma, glioma, mammary carcinoma, small cell lung carcinoma, cervical carcinoma,ovarian carcinoma, and bladder cancer have been performed with 1 3 1I, 9 0Y, 1 8 6Re, 1 5 3Sm, and177Lu beta emitting, and 212Bi alpha emitting radionuclides conjugated to monoclonal antibodies.A few studies compared different radionuclides in the same model system. The approaches thathave been used in these studies to estimate tumor dosimetry include the MIRD approach,thermoluminescent dosimetry, autoradiography, and comparison to external irradiation. Themajority of investigators have estimated the dose to tumor and normal organs using MIRD-based calculations (time-activity curve and equilibrium dose constant method). The range oftumor doses has been between 17 and 11 171 mGy/MBq of administered radioactivity. Theeffectiveness of radiolabeled monoclonal antibody therapy depends on a number of factorsrelating to the antibody such as specificity, affinity, and immunoreactivity. The density, location,and heterogeneity of expression of tumor-associated antigen within tumors will affect the local-ization and therapeutic efficacy of radiolabeled antibodies, as will physiological factors such asthe tumor vascularity, blood flow, and permeability. These factors are discussed and examplesare presented. In the future, it is recommended that investigators make comparisons of differentradionuclides in the same system, which should include an analysis of the relative toxicity. It isalso recommended that comparisons to external beam radiation be made for both tumor andnormal tissue damage. It is also recommended that investigators look at radiation dose hetero-geneity using thermoluminescent dosimeters and autoradiography, so that the range of tumorradiation dose and dose-rate is reported. It is hoped that an answer to how heterogeneity inradiolabeled antibody deposition in experimental tumors and spheroids affects absorbed dosedistribution and the radiobiological consequences will be understood. It is also hoped that adefinitive answer will be obtained for what radionuclides and forms of antibody are optimum forradioimmunotherapy of leukemias, micrometastases, and solid tumors, and most importantlyhow best to apply these techniques and information to the treatment of cancer clinically.
I. INTRODUCTION
Radiolabeled monoclonal antibodies (MoAbs) have beenused for radioimmunotherapy (RIT) of spheroids in vitroand in a variety of murine syngeneic tumors and humantumor xenografts in vivo A recent review of the animalRIT literature by Wessels1 will be updated and expandedupon in this review. Those papers that have presented do-simetry estimates in experimental RIT studies are dis-
cussed, and the presentation is organized by tumor type.The majority of the work has been with 131I- or 90Y-labeledMoAbs and human tumor xenografts. There are a fewmanuscripts available describing 1 8 6Re-, 1 7 7Lu- , and153Sm-labeled MoAb therapy in experimental animals. Inaddition to these studies with beta emitting radionuclides,alpha emitters (2 1 2Bi or 2 1 1At) and the Auger emitter 1 2 5Ihave been investigated in experimental RIT studies. A dis-
551 Med. Phys. 20 (2), Pt. 2, Mar/Apr 1993 0094-2405/93/020551-18$01.20 © 1993 Am. Assoc. Phys. Med. 551

552 Buchsbaum, Langmuir, and Wessels: Experimental radioimmunotherapy 552
cussion of the physical and chemical properties of theseradionuclides is presented in another manuscript in thisspecial issue.2
The approaches that have been taken to estimate tumordosimetry include the MIRD approach, thermolumines-cent dosimetry, autoradiography, and comparison to exter-nal irradiation. Most authors have used MIRD infinitemedia/equilibrium dose constant calculations,3 but calcu-lations for long range beta emitters (e.g., 9 0Y) in smalltumors (less than l-cm diameter) should use point sourcecalculations. 4 The comparison to the external irradiationapproach is reviewed in another section of this report byLangmuir et al.5 It is hoped that these studies in experi-mental animal models and with spheroids will provide in-formation useful to clinical RIT trials, such that bettertherapeutic results with less toxicity will ultimately be ob-tained.
II. RESULTS OF PUBLISHED STUDIES
A. The multicell spheroid as a three-dimensionalmodel for RIT dosimetry research
Multicell spheroids have been used by several investiga-tors to assess the efficacy of radiolabeled antibodytherapy. 6 - 1 5 Multicell spheroids are clusters of tumor cellsgrown in vitro in spinner flasks which can grow to diame-ters of 1 mm or more. The cells become differentiated andproduce extracellular matrix. Gradients of oxygen and nu-trient concentrations develop, thus mimicking what occursin vivo. The spheroid is therefore a useful in vitro three-dimensional (3D) tumor model. Autoradiography ofspheroid sections can be used to evaluate the distributionof radiolabeled compounds. Clonogenic assay of dissoci-ated spheroid cells can be used to evaluate the toxicity ofvarious treatments. Because of the simple spherical geom-etry, more accurate dose estimates can be made than arepossible with in vivo tumors.16-19 Because of the impor-tance of delayed antibody penetration and radionuclidecross-fire in RIT, an in vitro 3D tumor model can be veryuseful, particularly as a model for tumor microregions andfor studies of radiobiological and dosimetric aspects ofRIT. Comparisons between different radionuclides can bemade as well as between different extents of radiolabeledantibody penetration. 14,15 This model does not allow eval-uation of the roles of normal host cells, the vasculature, orpharmacokinetics.
The main problem in determining the dose-response re-lationship in RIT is the heterogeneity of radiolabeled an-tibody deposition. Because of this, tumor doses are gener-ally reported as average doses over the whole tumorvolume, without differentiating between necrotic and via-ble regions. The response of the spheroid can be measuredusing either clonogenic assay of cells from dissociatedspheroids or regrowth assays of intact spheroids. The av-erage dose to the region of viable cells can be calculatedseparately from the dose to the necrotic center resulting inmore meaningful dose estimates to the potentially viablecell population. 10
In general, it is possible to reach higher radiation dose-
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
rates and doses than are presently achievable with RIT invivo and a complete dose-response curve can be con-structed using a uniform population of spheroids. Endpoints used have included regrowth delay, 7,9 proportion ofspheroids sterilized,’ and clonogenic assay of dissociatedspheroid cells.9-11 Using 131I-labeled anticarcinoembryonicantigen (CEA) or 131I-labeled NR-LU-10, it has been pos-sible to achieve up to 99.9% to 99.99% (3 to 4 log) cell killin 0.8 to 1.0 mm diameter LS174T human colon cancerspheroids. 10,14,15 Calculated absorbed doses to the outer 0.2mm of the spheroids, which contains the viable cells inuntreated spheroids, were 30 to 40 Gy at this level of cellkill. Approximately 10% of the dose was from 1 3 1I in theincubating medium. When 1 3 1I was compared with 1 8 6Re ,similar doses produced similar toxicity. 14 For 1 3 1I, it wasshown that a more even distribution of radionuclide pro-duced a higher absorbed dose and more cell kill. 15 Studiesusing 212Bi-labeled NR-LU-10, which has a half-life of only1 h, produced little cell kill in spheroids despite substantialcell kill in monolayer cells.” This occurred because the2 1 2Bi decayed before there was significant penetration ofthe immunoconjugate into the spheroids. Pretargeting witha bifunctional antibody followed by administration of che-lated 212Bi may get around this problem, as well as the useof longer half-life alpha emitters such as 2 1 2Pb or 2 1 1At .Both of these solutions would allow higher tumor/normaltissue (T/NT) ratios to be reached prior to full decay ofthe radionuclide. Alpha emitters have the advantage ofhigh linear energy transfer (LET) which results in morekilling for a given radiation dose. However, normal tissueswould also receive this high LET radiation which onceagain emphasizes the importance of high T/NT ratioswhen alpha emitters are used. Bardies et al. 18 have pre-dicted doses of up to 417 Gy with 153Sm and 135 Gy with9 in 0.2-mm-diam ovarian cancer spheroids based onuptake data using “‘In-labeled OC125 F(ab’)2 fragments.
B. Radioimmunotherapy of human colon cancer inanimal models
Goldenberg et al.2 0 evaluated RIT of GW-39 humancolonic carcinoma xenografts in the hamster cheek pouchfollowing administration of 131I-labeled goat anticarcino-embryonic antigen (CEA) polyclonal antibody. With asingle injection of 37 MBq 131I-labeled antibody, there wasmarked tumor growth inhibition and an increase in animalsurvival time compared to an equivalent radionuclide doseof normal goat IgG. Radiation dose estimates to the tumorusing biodistribution data and the MIRD technique were13 250 mGy to the tumor over a 20-day period from thespecific antibody, and 4111 mGy for the normal IgG, fol-lowing the administration of 37 MBq of 131I-labeled anti-body. A summary of these and other results presented be-low are shown in Fig. 1 and Table I. Sharkey et al. 2 1
investigated the therapeutic efficacy of a single injection of131I-labeled NP-4 MoAb against CEA in hamsters bearingthe GW-39 tumor in the cheek pouch. A dose of 18.5 MBqof 131I-labeled NP-4 was able to reduce the growth rate of4-day-old GW-39 tumors by 84% on day 14 after treat-ment compared to untreated controls. Thirty-seven MBq
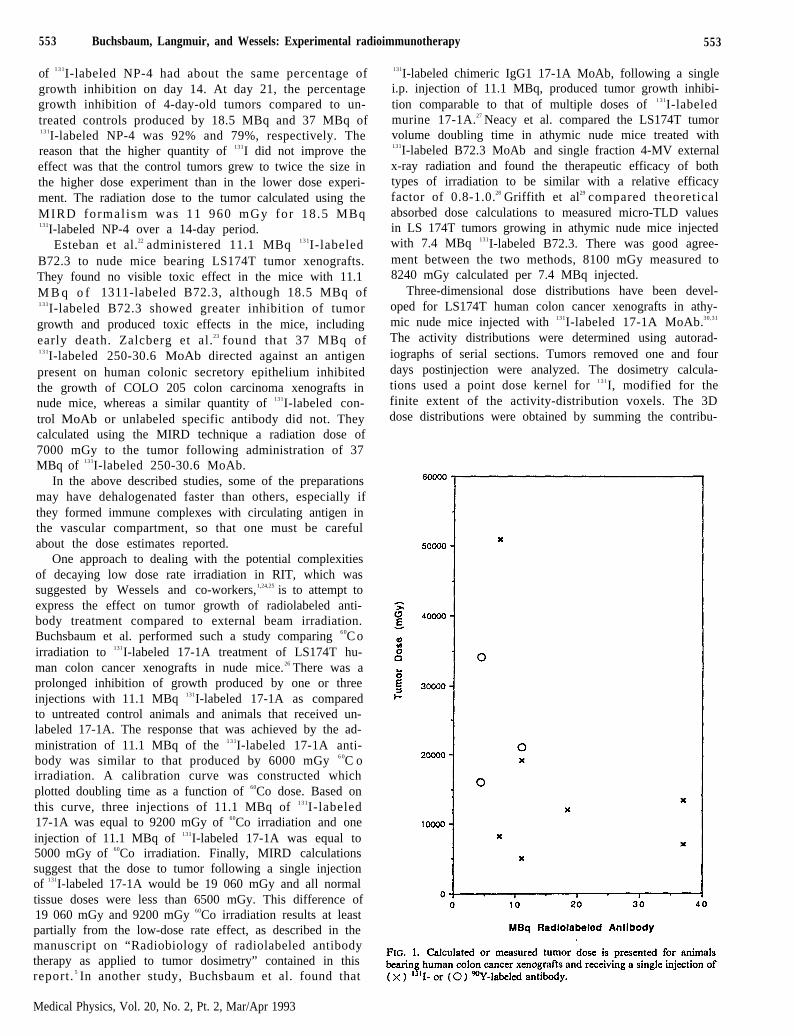
553 Buchsbaum, Langmuir, and Wessels: Experimental radioimmunotherapy 553
of 1 3 1I-labeled NP-4 had about the same percentage ofgrowth inhibition on day 14. At day 21, the percentagegrowth inhibition of 4-day-old tumors compared to un-treated controls produced by 18.5 MBq and 37 MBq of1 3 1I-labeled NP-4 was 92% and 79%, respectively. Thereason that the higher quantity of 131I did not improve theeffect was that the control tumors grew to twice the size inthe higher dose experiment than in the lower dose experi-ment. The radiation dose to the tumor calculated using theMIRD formal ism was 11 960 mGy for 18 .5 MBq131I-labeled NP-4 over a 14-day period.
Esteban et al.22 administered 11.1 MBq 1 3 1I-labeledB72.3 to nude mice bearing LS174T tumor xenografts.They found no visible toxic effect in the mice with 11.1M B q o f 1311-labeled B72.3, although 18.5 MBq of1 3 1I-labeled B72.3 showed greater inhibition of tumorgrowth and produced toxic effects in the mice, includingearly death. Zalcberg et al.23 found that 37 MBq of1 3 1I-labeled 250-30.6 MoAb directed against an antigenpresent on human colonic secretory epithelium inhibitedthe growth of COLO 205 colon carcinoma xenografts innude mice, whereas a similar quantity of 131I-labeled con-trol MoAb or unlabeled specific antibody did not. Theycalculated using the MIRD technique a radiation dose of7000 mGy to the tumor following administration of 37MBq of 131I-labeled 250-30.6 MoAb.
In the above described studies, some of the preparationsmay have dehalogenated faster than others, especially ifthey formed immune complexes with circulating antigen inthe vascular compartment, so that one must be carefulabout the dose estimates reported.
One approach to dealing with the potential complexitiesof decaying low dose rate irradiation in RIT, which wassuggested by Wessels and co-workers,1,24,25 is to attempt toexpress the effect on tumor growth of radiolabeled anti-body treatment compared to external beam irradiation.Buchsbaum et al. performed such a study comparing 6 0C oirradiation to 131I-labeled 17-1A treatment of LS174T hu-man colon cancer xenografts in nude mice.26 There was aprolonged inhibition of growth produced by one or threeinjections with 11.1 MBq 131I-labeled 17-1A as comparedto untreated control animals and animals that received un-labeled 17-1A. The response that was achieved by the ad-ministration of 11.1 MBq of the 1 3 1I-labeled 17-1A anti-body was similar to that produced by 6000 mGy 6 0C oirradiation. A calibration curve was constructed whichplotted doubling time as a function of 60Co dose. Based onthis curve, three injections of 11.1 MBq of 1 3 1I-labeled17-1A was equal to 9200 mGy of 60Co irradiation and oneinjection of 11.1 MBq of 131I-labeled 17-1A was equal to5000 mGy of 60Co irradiation. Finally, MIRD calculationssuggest that the dose to tumor following a single injectionof 131I-labeled 17-1A would be 19 060 mGy and all normaltissue doses were less than 6500 mGy. This difference of19 060 mGy and 9200 mGy 60Co irradiation results at leastpartially from the low-dose rate effect, as described in themanuscript on “Radiobiology of radiolabeled antibodytherapy as applied to tumor dosimetry” contained in thisreport. 5 In another study, Buchsbaum et al. found that
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
131I-labeled chimeric IgG1 17-1A MoAb, following a singlei.p. injection of 11.1 MBq, produced tumor growth inhibi-tion comparable to that of multiple doses of 1 3 1I-labeledmurine 17-1A.27 Neacy et al. compared the LS174T tumorvolume doubling time in athymic nude mice treated with131I-labeled B72.3 MoAb and single fraction 4-MV externalx-ray radiation and found the therapeutic efficacy of bothtypes of irradiation to be similar with a relative efficacyfactor of 0.8-1.0.28 Griffith et al29 compared theoreticalabsorbed dose calculations to measured micro-TLD valuesin LS 174T tumors growing in athymic nude mice injectedwith 7.4 MBq 131I-labeled B72.3. There was good agree-ment between the two methods, 8100 mGy measured to8240 mGy calculated per 7.4 MBq injected.
Three-dimensional dose distributions have been devel-oped for LS174T human colon cancer xenografts in athy-mic nude mice injected with 131I-labeled 17-1A MoAb.30,31
The activity distributions were determined using autorad-iographs of serial sections. Tumors removed one and fourdays postinjection were analyzed. The dosimetry calcula-tions used a point dose kernel for 1 3 1I, modified for thefinite extent of the activity-distribution voxels. The 3Ddose distributions were obtained by summing the contribu-
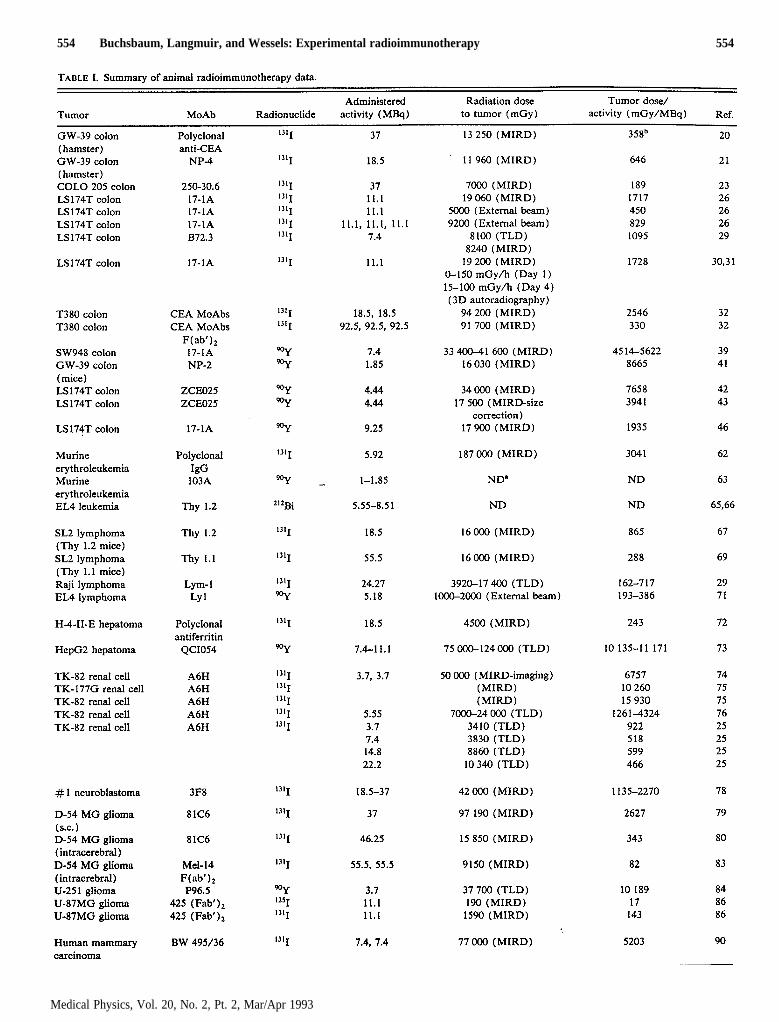
554 Buchsbaum, Langmuir, and Wessels: Experimental radioimmunotherapy 554
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
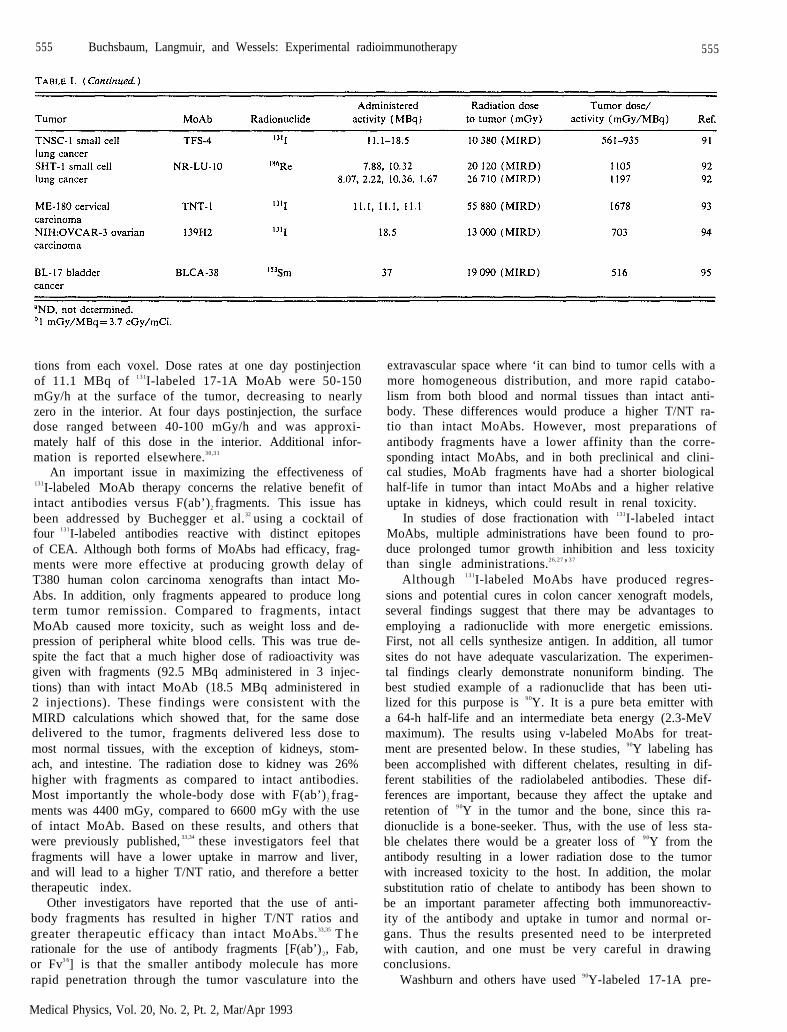
555 Buchsbaum, Langmuir, and Wessels: Experimental radioimmunotherapy 555
tions from each voxel. Dose rates at one day postinjectionof 11.1 MBq of 1 3 1I-labeled 17-1A MoAb were 50-150mGy/h at the surface of the tumor, decreasing to nearlyzero in the interior. At four days postinjection, the surfacedose ranged between 40-100 mGy/h and was approxi-mately half of this dose in the interior. Additional infor-mation is reported elsewhere.30,31
An important issue in maximizing the effectiveness of131I-labeled MoAb therapy concerns the relative benefit ofintact antibodies versus F(ab’)2 fragments. This issue hasbeen addressed by Buchegger et al.32 using a cocktail offour 131I-labeled antibodies reactive with distinct epitopesof CEA. Although both forms of MoAbs had efficacy, frag-ments were more effective at producing growth delay ofT380 human colon carcinoma xenografts than intact Mo-Abs. In addition, only fragments appeared to produce longterm tumor remission. Compared to fragments, intactMoAb caused more toxicity, such as weight loss and de-pression of peripheral white blood cells. This was true de-spite the fact that a much higher dose of radioactivity wasgiven with fragments (92.5 MBq administered in 3 injec-tions) than with intact MoAb (18.5 MBq administered in2 injections). These findings were consistent with theMIRD calculations which showed that, for the same dosedelivered to the tumor, fragments delivered less dose tomost normal tissues, with the exception of kidneys, stom-ach, and intestine. The radiation dose to kidney was 26%higher with fragments as compared to intact antibodies.Most importantly the whole-body dose with F(ab’)2 frag-ments was 4400 mGy, compared to 6600 mGy with the useof intact MoAb. Based on these results, and others thatwere previously published, 33,34 these investigators feel thatfragments will have a lower uptake in marrow and liver,and will lead to a higher T/NT ratio, and therefore a bettertherapeutic index.
Other investigators have reported that the use of anti-body fragments has resulted in higher T/NT ratios andgreater therapeutic efficacy than intact MoAbs.33,35 T h erationale for the use of antibody fragments [F(ab’)2, Fab,or Fv3 6] is that the smaller antibody molecule has morerapid penetration through the tumor vasculature into the
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
extravascular space where ‘it can bind to tumor cells with amore homogeneous distribution, and more rapid catabo-lism from both blood and normal tissues than intact anti-body. These differences would produce a higher T/NT ra-tio than intact MoAbs. However, most preparations ofantibody fragments have a lower affinity than the corre-sponding intact MoAbs, and in both preclinical and clini-cal studies, MoAb fragments have had a shorter biologicalhalf-life in tumor than intact MoAbs and a higher relativeuptake in kidneys, which could result in renal toxicity.
In studies of dose fractionation with 131I-labeled intactMoAbs, multiple administrations have been found to pro-duce prolonged tumor growth inhibition and less toxicitythan single administrations.26,27’3 7
Although 1 3 1I-labeled MoAbs have produced regres-sions and potential cures in colon cancer xenograft models,several findings suggest that there may be advantages toemploying a radionuclide with more energetic emissions.First, not all cells synthesize antigen. In addition, all tumorsites do not have adequate vascularization. The experimen-tal findings clearly demonstrate nonuniform binding. Thebest studied example of a radionuclide that has been uti-lized for this purpose is 9 0Y. It is a pure beta emitter witha 64-h half-life and an intermediate beta energy (2.3-MeVmaximum). The results using v-labeled MoAbs for treat-ment are presented below. In these studies, 90Y labeling hasbeen accomplished with different chelates, resulting in dif-ferent stabilities of the radiolabeled antibodies. These dif-ferences are important, because they affect the uptake andretention of 9 0Y in the tumor and the bone, since this ra-dionuclide is a bone-seeker. Thus, with the use of less sta-ble chelates there would be a greater loss of 9 0Y from theantibody resulting in a lower radiation dose to the tumorwith increased toxicity to the host. In addition, the molarsubstitution ratio of chelate to antibody has been shown tobe an important parameter affecting both immunoreactiv-ity of the antibody and uptake in tumor and normal or-gans. Thus the results presented need to be interpretedwith caution, and one must be very careful in drawingconclusions.
Washburn and others have used 90Y-labeled 17-1A pre-
556 Buchsbaum, Langmuir, and Wessels: Experimental radioimmunotherapy 556
pared with cyclic DTPA as the chelate or the more stablep - N H2-Bz-DTPA chelate to treat nude mice bearingSW948 human colon cancer xenografts.38 After injectionwith unlabeled 17-IA, the tumors continually increased insize. In animals receiving 7.4 MBq 90Y-labeled 17-1A pre-pared with cyclic DTPA, tumor volume was unchangedfrom base line. As the quantity of v-labeled 17-1A in-creased from 3.7 to 7.4 MBq, the rate of tumor growthdecreased, but all experimental animals died between 14and 21 days after treatment. In contrast, 7.4 MBq9 0Y-labeled 17-1A prepared with p-NH2-Bz-DTPA pro-duced a maximum tumor volume reduction of 87% by day15, and no deaths were noted for 71 days after treatment.Dose-response curves again showed increased tumoricidaleffects with increased quantities of 90Y-labeled 17-IA. Us-ing the MIRD approach, a radiation dose to tumor of33 400 or 41 600 mGy was calculated for 7.4 MBq9 0Y-labeled 17-1A administered with each of these che-lates, respectively.39 In another study,40 groups of athymicnude mice bearing SW 948 xenografts were injected with5.55 or 7.4 MBq 9 0Y-labeled 17-1A MoAb prepared withthe stable p-NH2-Bz-Mx-DTPA chelate. At 49 and 125days after the first injection, the treatment group receiving7.4 MBq was reinjected with 5.55 MBq of 90Y-labeled 17-1A. There were no deaths from treatment in this group.The reduction in the initial tumor size reached nadirs of96% at 39 days, 88% at 74 days, and 44% at 147 days.The treatment group receiving 5.55 MBq was reinjectedwith 7.4 MBq 9 0Y-labeled 17-1A at 49 days after the firstinjection. There was a maximum reduction in the initialtumor size of 85% at 21 days, but all the animals in thisgroup died within 17 to 21 days after reinjection at 49 days,probably due to hematopoietic death.
Sharkey et al.4 1 reported that 1.85 MBq of 9 0Y-labeledNP-2 anti-CEA MoAb conjugated with cyclic DTPA in-hibited growth of the GW-39 tumor in athymic mice by77% as compared to control animals given 1.85 MBqv-labeled irrelevant MoAb at 21 days after injection. Theestimated radiation dose to the tumor using the MIRDformulation was 16 030 mGy after 1.85 MBq 9 0Y-labeledNP-2 administration over a 14-day period. Doses to lungs,kidneys, and liver were 5730, 5960, and 7420 mGy, respec-tively. Buras and colleagues have performed a similarstudy with s.c. LS174T solid tumor xenografts of coloncancer.42 As was the case with 17-1A and NP-2, whileunlabeled antibody had no affect on tumor growth,y-labeled ZCE025 (anti-CEA antibody conjugated witha proprietary bifunctional chelating agent) arrested tumorsfor 2 to 3 weeks. They performed a series of MIRD calcu-lations to estimate the dose to the tumor and normal tis-sues produced by specific and nonspecific MoAbs. Therewas no correction for the small tumor volume and thedeposition of a fraction of the beta particle energy outsidethe tumor. The tumor was calculated to receive 34 000mGy with the administration of 4.44 MBq 9 0Y-labeledanti-CEA antibody as compared to 14 000 mGy with thenonspecific antibody. However, some normal tissues re-ceived potentially significant doses as well. For instance,the liver dose was calculated to be 37 000 mGy compared
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
to 18000 mGy with a control antibody against melanoma.With regard to spleen, they calculated similar degrees ofdose of 29 000 mGy with the specific antibody, 27000mGy with the nonspecific antibody, and the dose to kidneywas similar with 17000 mGy with the specific antibodyand 16000 mGy with the nonspecific antibody. In a morerecent study, Buras et al. corrected for the loss of betaparticle energy outside the tumor and normal organs andestimated that the tumor dose from a single 4.44 MBqadministration of 9 0Y-labeled ZCE025 was 17500 mGy. 4 3
In another study by the same group of investigators it wasshown that interferon increased the amount of CEA ex-pression in tumors by a factor of 6.9. In animals treatedwith interferon, there was enhanced localization of90Y-labeled ZCE025 (using a stable benzyl DTPA chelate)in WiDr human colon cancer xenografts by a factor of2.4.4 4 The dose to tumor produced by 4 .44 MBq9 0Y-labeled ZCE025 increased from 12 170 mGy in ani-mals treated without interferon to 24 770 mGy in animalstreated with interferon.4 4
Another therapeutic approach that has been studied in anude mouse xenograft system has been to give multipleadministrations of low quantities (between 1.48 and 5.55MBq) of 9 0Y-labeled antibody prepared using the GYK-DTPA chelate. However, tumors regrow as soon as theinjections are stopped.4 5
In a preliminary experiment on 9 0Y-labeled 17-1A tu-mor growth inhibition, groups of 8 mice each were injectedi.p. with 0, 5.55, 9.25, 12.95, and 16.65 MBq of 90Y-labeled17-1A prepared using the p-NH2-Mx-DTPA s tab lechelate. 4 6 There was tumor growth inhibition producedwhich was proportional to the quantity of 9 0Y- labe led17-1A administered. The toxicity (decrease in peripheralwhite blood cells and death of animals) of the q-labeledantibody treatments was proportional to dose. The resultsof a comparison of the tumor growth inhibition producedby 131I- and 9 0Y-labeled 17-1A indicate that similar tumorgrowth inhibition was produced by 9.25 MBq 9 0Y- and5.55 MBq 1 3 1I-labeled 17-1A. In this study, 9.25 MBq90Y-labeled 17-1A MoAb was estimated to deliver 17 900mGy to the tumor based on MIRD calculations. However,9.25 MBq 90Y-labeled 17-1A showed considerably greatertoxicity in terms of decreased peripheral white blood cellsand animal deaths than 5.55 MBq 1 3 1I-labeled 17-1AMoAb, which was estimated to deliver 9530 mGy to thetumor by MIRD calculations. Higher doses of 131I-labeled17-1A (14.8 and 18.5 MBq) produced greater tumorgrowth inhibition without toxicity. The differences in tu-mor growth inhibition were in part due to a lower degree oftumor localization of the 9 0Y-labeled antibody, and be-cause about 25% of the 90Y dose was deposited outside thetumor as determined by 3D dose distributions calculatedusing autoradiography data.
Sharkey et a1.47 conducted biodistribution studies with131I- and 9 0Y-labeled (using the ITC-Bz-Mx-DTPA stablechelate) intact NP-4 anti-CEA MoAb and fragments innude mice bearing human colonic tumor xenografts. Radi-ation dose estimates derived from these studies suggest thatthe maximum tolerated dose of 1 3 1I-labeled intact MoAb
557 Buchsbaum, Langmuir, and Wessels: Experimental radioimmunotherapy 557
would deliver a greater dose to a small tumor thanv-labeled intact antibody, principally due to the in-creased toxicity of ?-labeled antibody brought on by thehigher and prolonged retention of 9 0Y in the normal or-gans, especially bone. It was concluded that 9 0Y-labeledMoAb fragments would not be useful due to the higherdoses to the kidneys than to the tumor, but that“‘I-labeled fragments administered in a fractionated regi-men might have an advantage over multiple treatmentswith 131I-labeled intact antibody due to less bone marrowtoxicity.
One of the chief stumbling blocks in achieving curesusing radiolabeled MoAb therapy is that hematologic tox-icity limits the dose that can be delivered. Two potentialmethods of increasing the dose of labeled antibody that canbe delivered are through the use of autologous bone mar-row transplantation (ABMT) and colony stimulatingfactors. 48-51 The potential role of ABMT in colon cancerwas assessed by Morton and colleagues.48 In their studiesusing nude mouse xenografts, they found that 4.44 MBq of9 0Y-labeled anti-CEA antibody (prepared with a propri-etary bifunctional chelating agent) alone produced a me-dian survival of 45 days. This represented an increase from31 or 35 days, which was observed in the control group andin those receiving nonspecific antibody, respectively.Higher doses of antibody could be tolerated only if ABMTwas performed. This allowed administration of up to 8.325MBq of anti-CEA antibody, which increased median sur-vival to 63 days.
An alternative to bone marrow transplantation whichmay allow dose escalation of RIT includes the use of ra-dioprotective agents. Interleukin-1 (IL-1) is the most stud-ied hematopoietic growth factor with regard to radiopro-tection. It, as well as other hematopoietic stimulatoryfactors, has a radioprotective effect on bone marrow pro-genitor cells in vitro when given before, during, or shortlyafter acute external radiation exposure.51,52 In mice, theprotective effect has been greater when given 24 h prior toa s o p p o s e d t o a f t e r s u b l e t h a l o r l e t h a l d o s e s o fradiation.53-57 IL-1 stimulates growth of pluripotent he-matopoietic cells.58 In mice, survival was increased most byadministering 100-1000 ng 20 h before lethal radiationcompared to 4 or 45 h prior to radiation. 53,54 Some radio-protective effect resulted from l-5 µg doses given up to 3 hafter radiation but not at longer time intervals 54-57 Initialtesting of IL-l in conjunction with RIT has been carriedo u t b y B l u m e n t h a l e t a l5 0 T h e y s h o w e d t h a t t h e131I-labeled antibody induced decline in circulating whiteblood cells in hamsters could be prevented by a single in-jection of IL-l 20 h prior to radiolabeled antibody injec-tion, or reversed by IL-l injection 7 days after “‘I-labeledantibody administration. Thrombocytopenia has been thedose limiting toxicity in most clinical RIT trials. IL-l hasnot been shown to be effective in stimulating the growth ofmegakaryocytes. The adjunctive use of IL-l and othergrowth factors that stimulate megakaryocyte proliferationmay allow the use of higher doses of radiolabeled MoAbsdue to their protective effect on bone marrow stem cells orthe accelerated proliferation of cells surviving RIT.
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
Another approach to enhancing the efficacy of RIT is totarget cells not well targeted by the antibody. Hypoxic cellsare in this category as they are generally at a distance fromblood vessels. Hypoxic cells are also relatively radioresis-tant decreasing even further the effectiveness of RIT. Mi-sonidazole, an hypoxic cell radiosensitizer, has been eval-uated in combination with 1 3 1I - labeled ant i -CEA inLS174T human colon cancer xenografts.59 They found thatthe addition of misonidazole resulted in significant prolon-gation of tumor growth inhibition as compared to the ra-diolabeled antibody alone. SR 4233, a benzotriazine hy-poxic cytotoxin, has been used in the same tumor model incombination with 1311-labeled NR-LU-10 and tumorgrowth delay was significantly prolonged.60 It was esti-mated that the combined treatment produced 10 timesmore cell kill than radiolabeled antibody alone. The appli-cation of hypoxic cell sensitizers in clinical studies withexternal beam radiation has been disappointing, which hasbeen attributed largely to the fact that doses were limitedto inadequate levels because of toxicity. New sensitizershave been synthesized that are less toxic, and these arebeing evaluated in clinical trials.
C. Radioimmunotherapy of leukemias andlymphomas in animal models
MoAbs labeled with 1 3 1I have been used for RIT ofleukemia and lymphoma in experimental animal models. Afeature of many lymphomas and leukemias is that they aremore radiosensitive than carcinomas.6 1
RIT of Rauscher murine erythroleukemia was studiedwith 1 3 1I-labeled 103A MoAb reactive with the envelopeglycoprotein expressed on Rauscher murine erythroleuke-mia cells62 Dose-response studies showed that about 90%reduction in spleen size occurred at 2.96 MBq injected peranimal. Similar results were obtained with an irrelevantMoAb, indicating that RIT with 1 3 1I was not antibodyspecific in this system. Using the MIRD formulation, thecalculated mean absorbed doses to the spleen and wholebody of a mouse treated with 5.92 MBq of 131I-polyclonalbovine IgG were 18000 and 1650 mGy, respectively. RITusing 90Y-labeled 103A MoAb prepared with cyclic DTPAwas also studied.63 Doses of 0.999 to 1.85 MBq 90Y-labeled103A antibody resulted in complete remission with no mi-croscopic evidence of tumor foci in either spleen or liver,whereas a dose of 1.85 MBq of control bovine IgG hadareas of abnormal erythropoiesis suggestive of tumor fociin lymphoid tissue. The specific radiation dose delivered tothe tumor or whole body was not calculated. However,analysis of the MBq/g present in tumor and normal tissuesover 9 days, indicated that over 20-fold greater radiationdoses were delivered to the tumor than to any other organexamined.
Gansow et al.64 labeled the 103A MoAb with 2 1 2Bi andtreated mice bearing Rauscher erythroleukemia cells. Withwhole body doses of 1270 mGy, tumor foci in spleens ofleukemic mice were mostly eliminated without substantivetoxicity.
M a c k l i s e t a l .6 5 , 6 6 p e r f o r m e d R I T s t u d i e s w i t h212Bi-labeled anti-Thy 1.2 IgM MoAb for the treatment of
558 Buchsbaum, Langmuir, and Wessels: Experimental radioimmunotherapy 558
EL4 (Thy1.2+) leukemic T-cells injected i.p. in mice.Mice inoculated i.p. with 5.55 or 8.51 MBq of 212Bi-labeledantibody in 2 to 4 injections 24 h after EL4 injection wereoften cured (80% survival) of their ascites. Animalstreated with 1.48 to 3.7 MBq of 2 1 2Bi-labeled antibodygiven i.p. over 4 to 8 h showed significant prolongation insurvival. Nonspecific IgM labeled with 212Bi did not pro-long survival at the same doses. No attempts were made toestimate the absorbed radiation dose to the tumor cells.The high LET (about 100 keV/µ) and S-7 cell-diameterpath length of the alpha particle ejected from the 2 1 2B inucleus make it a potentially useful radionuclide for theRIT of ascites, leukemia, and micrometastases. The shorthalf-life (60.55 min) may be advantageous in limiting nor-mal tissue doses if there is good tumor localization at earlytime points after injection; however, the short half-life cre-ates logistical problems with regard to shipping the radio-nuclide or even if a cyclotron is nearby.
Badger et al.67 evaluated the use of 131I-labeled anti-Thy1.1 differentiation antigen MoAb (31E6.4) to deliver ra-diotherapy to established AKR/J SL2 (Thy 1.1+) murineT-cell lymphoma nodules of 0.5 to 1.0 cm in diametergrowing s.c. in congenic AKR/Cum (Thy 1.2+) mice.Based on kinetic biodistribution data and the MIRD for-mulation, the mean calculated dose to tumor was 16000mGy following injection of 18.5 MBq of 131I-labeled anti-Thy 1.1 antibody which led to regression of the tumor in44% of animals. Mice treated with more than 18.5 MBq1 3 1I-labeled anti-Thy 1.1 antibody died of bone marrowaplasia. In comparison, 18.5 MBq 131I-labeled irrelevantantibody was calculated to deliver a mean dose of 3800mGy to tumor and had an effect on tumor growth in 6% ofanimals. Nourigat et al.6 8 using the same model demon-strated that 55.5-62.9 MBq 1 3 1I-labeled anti-Thy 1.1MoAb produced 92% complete regression of SL2 lym-phoma nodules containing 0.3% to 1% variant lymphomacells that do not express the Thy 1.1 antigen. This studydemonstrated that emitted radiation from radiolabeled an-tibody bound to antigen-positive tumor cells killed adja-cent tumor cells that do not express the target antigen. Allanimals treated with radiolabeled antibody died by day 12from anticipated bone marrow aplasia. Badger et a1.69 alsoexamined RIT with 131I-labeled MoAb against Thy 1.1 fortreating solid SL2 tumor masses in syngeneic AKR/J (Thy1.1+) mice, where the antibody also reacts with normalT-cells. The results demonstrated that it was possible tocause regressions of lymphoma in spite of reactivity withnormal cells. RIT of AKR/J mice bearing established s.c.lymphoma nodules with 55.5 MBq of 131I-labeled anti-Thy1.1 MoAb 24 h after infusion of 1mg of unlabeled anti-Thy1.1 resulted in complete regression of the tumors in 71% ofanimals and had a greater cure rate than 27.75 MBq of131I-labeled irrelevant antibody (23% complete regression,p<0.00l), which delivered equivalent radiation doses tonormal organs except for bone marrow. All animalstreated with 55.5 MBq 131I-labeled anti-Thy 1.1 antibodydied of bone marrow aplasia. Radiation doses to tumor andvarious tissues were calculated from the biodistributiondata using the MIRD formulation assuming uniform dis-
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
tribution of the radiolabeled antibody within individual or-gans. The dose to tumor following treatment with 55.5MBq 131I-labeled anti-Thy 1.1 after 1 mg unlabeled anti-body was estimated to be 16000 mGy.
Adams et al.7 0 successfully treated Raji Burkitt lym-phoma xenografts in athymic nude mice with a single in-jection of 11.47-14.54 MBq of 1 3 1I-labeled Lym-1 panB-cell MoAb reactive with this tumor. In 3 mice treatedwith 1 3 1I-labeled Lym-1, 4 of 6 tumors regressed com-pletely and did not recur. Griffith et a1.29 performed quan-titative autoradiography on Raji tumors with implantedmini-TLDs from animals injected with 131I-labeled Lym-1.A maximum radiation dose to tumor of 17400 mGy wasmeasured (range of 3920-17 400 over all TLD sections)per 24.27 MBq 131I-labeled Lym-1 injected.
Schmidberger et al.7 1 radiolabeled the Ly1 anti-T-cellMoAb, the murine homologue of human CD5, with 9 0Y .When tested in an aggressive model of T-cell lymphoma, asingle 5.18 MBq i.p. dose of 90Y-anti-Ly1, given 1 day afteri .v . in ject ion of a le thal dose of 104 E L 4 m o u s eT-lymphoma cells, resulted in significant, but transient im-provement in survival. Protection was selective since a9 0Y-labeled irrelevant control antibody did not prolongsurvival. Comparison with external whole-body irradiationstudies indicated that the partially protective effect of 5.18MBq 9 0Y-anti-Lyl was equivalent to external radiation of1000-2000 mGy.
D. Radioimmunotherapy of hepatoma in animalmodels
Tumor doses of 4500 mGy were calculated by Rostocket al.72 using the MIRD formulation following injection of18.5 MBq of 131I-labeled anti-ferritin polyclonal antibodyin the H-4-11-E syngeneic rat hepatoma model. The dosedeposited in tumor was calculated to be 1550 mGy follow-ing injection of 18.5 MBq of 131I-labeled normal IgG. Kleinet al.73 performed RIT studies with 1 3 1I- and 9 0Y-labeled(prepared using a proprietary bifunctional chelatingagent) anti-ferritin MoAbs in athymic nude mice bearingHepG2 human hepatoma s.c. xenografts of 2 to 3 mm indiameter. Animals injected with a single dose of 14.8 MBqof 131I-labeled anti-ferritin MoAb QCI054 showed inhibi-tion of tumor growth and significantly prolonged survivalcompared to untreated controls, but there were no long-term survivors, whereas 7.4 or 11.1 MBq of 1 3 1I-labeledantibody did not inhibit tumor growth nor produce in-creased survival compared to controls. Animals treatedwith 3.7, 7.4, or 11.1 MBq of 9 0Y-labeled anti-ferritinMoAb had inhibition of tumor growth and significantlyprolonged survival compared to untreated control animals.Miniature TLDs were implanted into some of the tumorsfor radiation dose measurements. Tumor absorbed dosecalculations were performed using biodistribution data andthe MIRD formulation. Tumor doses of 10000 to 15000mGy produced an inhibition of tumor growth and an ex-tension in survival, but no regressions. Tumor doses of20000 to 50000 mGy produced greater tumor growth in-hibition and a more pronounced increase in survival. Atthe highest tumor doses, 75000 to 124000 mGy, obtained

559 Buchsbaum, Langmuir, and Wessls: Experimental radioimmunotherapy 559
with 7.4 and 11.1 MBq of 9 0Y-labeled MoAb, there wasconsiderable tumor regression and increased survival.Those animals showing a significant increase in survivalreceived up to 124000 mGy to the center of the tumor.The radiation doses to tumors measured with implantedTLDs were in good agreement with the calculated tumordoses. It was estimated that v-labeled anti-ferritin MoAbdeposited approximately 7 times the dose deposited to tu-mor as equivalent levels of 131I-labeled anti-ferritin MoAb,which is higher than that expected based on the relativeenergy deposited by each radionuclide under equilibriumconditions, and may be a result of higher nonspecific tumoruptake or retention of 9 0Y-labeled MoAbs.
E. Radioimmunotherapy of renal cell carcinoma inanimal models
Renal cell carcinoma is relatively resistant to externalbeam radiation. Tumor localization studies have demon-s t ra ted a h igh uptake (grea ter than 50% ID/g) of1 3 1I-labeled A6H MoAb reactive with human renal cellcarcinoma in tumor xenografts weighing 100 mg. Vessellaet al.74 treated athymic nude mice bearing established s.c.TK-82 human renal cell carcinomas weighing about 50 mgwith 3.7 MBq of 1 3 1I-labeled A6H MoAb reactive withhuman renal carcinoma cells at day 0 and day 20. Therewas tumor regression to about 20% of initial size, andtumor growth was inhibited for at least 90 days. Controlmice treated with 1 3 1I-labeled irrelevant MoAb showedprogressive increase in tumor size. Dosimetry calculationsusing the MIRD formulation and external imaging indi-cated that the tumors received up to 50000 mGy fromeach of the 3.7 MBq 1 3 1I-labeled MoAb doses, whereasnormal tissues and organs received less than 2500 mGy.
Chiou et al.75 carried out dosimetry studies with 1.37 to6.55 MBq 131I-labeled A6H MoAb in athymic nude micebearing TK-82 or TK-177G renal cell carcinoma xe-nografts. Using quantitative imaging and the MIRD for-mulation, the median radiation dose delivered to TK-177Gtumors was 10 260 mGy/MBq 1311-labeled A6H adminis-tered in a single dose, and the median dose to TK-82 tu-mors was 15 930 mGy/MBq. Normal mouse tissues re-ceived a mean dose of 243 mGy/MBq administered. Twodoses of 1311-labeled A6H MoAb (4.07 to 4.81 MBq/dose)arrested the tumor growth or caused regression of bothrenal ce l l carc inoma xenograf ts . Similar doses of131I-labeled irrelevant MoAb did not inhibit tumor growth.
Using TLDs and autoradiography, Vessella et al. 76 re-ported a measured tumor dose of 7000 to 24 000 mGy fora 5.55 MBq injected dose of 131I-labeled A6H MoAb in theTK-82 renal cell carcinoma xenograft. In another study,Wessels et al.25 reported TLD average doses to TK-82 xe-nografts of 3410, 3830, 8860, and 10 340 mGy following asingle administration of 3.7, 7.4, 14.8, and 22.2 MBq of131I-labeled A6H antibody, respectively. The range of ab-sorbed doses was estimated to be 300% based on autorad-iography density data. Wessels et al.25 found that MIRDcalculations for tumors were usually higher than TLDmeasurements by up to 50%, which is thought to be aresult of the peripheral deposition of radiolabeled antibody
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
in contrast to the centrally located TLD. Comparisons toexternal beam radiation were reported in this study, 25 a swere discussed above for colon cancer models, and they arediscussed in more detail in the radiobiology section of thisreport.5
F. Radioimmunotherapy of human neuroblastoma inanimal models
131I-labeled UJ13A MoAb reactive with neuroblastomacells was administered to athymic nude mice with TR14human neuroblastoma xenografts.77 Tumors of approxi-mately 1 cm3 regressed to 10% of their original volumeover a 21-day period following administration of 5.55 MBq131I-labeled UJ13A antibody. Repeated injection caused tu-mors to disappear, but regrowth at the original site alwaysoccurred. 1 2 51- and 1 2 3-I-labeled UJ13A antibody at thesame radionuclide level had no effect on tumor growth.
Cheung et al. 7a treated athymic nude mice bearing neu-roblastoma xenografts with 4.63 to 37 MBq of 131I-labeled3F8 anti-GD2 MoAb present on neuroblastoma cells.There was a dose dependent inhibition of tumor growth.Complete tumor ablation was achieved with 18.5 to 37MBq of 1 3 1I-labeled 3F8. The dose to tumor was greaterthan 42 000 mGy using the MIRD technique. It should beemphasized that neuroblastoma is a highly radiosensitivetumor.
G. Radioimmunotherapy of human glioma andleptomeningeal tumors in animal models
Lee et al.7 9 evaluated the therapeutic efficacy of1 3 1I-labeled MoAb 81C6 of the IgG2b subclass, reactivewith an epitope of the glioma-associated extracellular ma-trix protein tenascin, in athymic nude mice bearing s.c.human D-54 MG glioma xenografts of 100-500 mm3. Spe-cific tumor growth inhibition was noted with 9.25 and 18.5MBq i.v. administered 1 3 1I-labeled 81C6 antibody. Thepercentage of animals with tumor regression progressivelyincreased with increasing doses of radiolabeled MoAb. Sta-tistically significant tumor regression was seen at doses of18.5 and 37 MBq 131I-labeled 81C6. The estimated dose totumor over an 11-day period using biodistribution data andthe MIRD formalism was 97 190 mGy following adminis-tration of 37 MBq 131I-labeled 81C6, whereas the dose withan equivalent quantity of irrelevant MoAb of the sameisotype was 23 460 mGy. Doses to other organs rangedfrom 1350 mGy for brain to 24 150 mGy for lung. Animportant finding in this study was that tumor radiationdosimetry based on prior 1251-labeled 81C6 localizationdata underestimated the dose to tumor by 35%-52% dueto differences in tumor growth in the localization and ther-apy studies. This has important implications for comparingthe results obtained by various investigators with differenttumor systems.
Lee et al.8 0 evaluated the therapeutic efficacy of131I-labeled 81C6 in athymic rats bearing intracranial D-54MG xenografts. For animals with an average intracranialtumor volume of 16 to 20 mm3, a statistically significantincrease in animal survival was found for animals treated
560 Etuchsbaum, Langmuir, and Wessels: Experlmental radioimmunotherapy 560
with 46.25 or 92.5 MBq 131I-labeled 81C6. The estimatedradiation dose to intracranial tumors of about 3.4 mm indiameter using the MIRD technique following the i.v. ad-ministration of 46.25 MBq 131I-labeled MoAb was 15 850mGy over a 12-day period for 81C6 and 1680 mGy for thecontrol antibody. Doses to the other organs ranged from310 mGy to the brain to 7340 mGy to the bone marrow.These data were similar to the radiation doses predictedfrom localization studies.
Schuster et al.81 compared the growth delay of s.c. D-54MG tumors produced by 1 3 1I-labeled 81C6 MoAb pre-pared using Iodogen (IOD) to that prepared usingN-succinimidyl-3-(tri-n-butylstannyl) benzoate (ATE).Growth delay with 81C6 ATE was significantly longerthan with 81C6 IOD. Biodistribution data gave estimatedradiation doses to tumors of 150 mm3 initial tumor volumeof 77 230 and 52 000 mGy for 18.5 MBq of 1 3 1I-labeled81C6 ATE or 81C6 IOD, respectively. It was previouslyshown that labeling of 81C6 using ATE increased tumoruptake and T/NT ratios and decreased deiodination com-pared with labeling using IOD,a2 which explains the dif-ference in tumor growth delay produced by the two radio-iodinated MoAbs.
Colapinto et al.8 3 evaluated the efficacy of 131I-labeledF(ab’)2 fragments of MoAb Mel-14, an Ig2a reactive witha chondroitin sulfate proteoglycan antigen expressed ongliomas, in prolonging survival of athymic nude mice bear-ing intracerebral D-54 MG human glioma xenografts. In-travenous injection of 55.5 or 74 MBq of 1 3 1I-labeledMel-14 F(ab’)2 6-7 days after tumor implantation resultedin a significant increase in animal survival over controluntreated animals or animals treated with 131I-labeled non-specific antibody. The injection of 111 MBq of 131I-labeledMel-14 F(ab’)2 in two doses of 55.5 MBq, 48 h apart,significantly increased animal survival over untreated con-trol animals. A single injection of 111 MBq of 131I-labeledMel-14 did not improve survival over controls which wasprobably due to hematologic toxicity. The estimated radi-ation dose to tumor was 9150 mGy after the two 55.5 MBqadministrations using the MIRD formulation, which was ahigher dose than that delivered to normal organs. The onlynormal tissue to receive a substantial dose was kidney(7490 mGy), which is expected with F(ab’)2 fragments. Asingle dose of 55.5 MBq 1 3 1I-labeled Mel-14 F(ab’)2 w a sestimated to deliver 3900 mGy to tumor and 3790 mGy tokidney. No cures were reported in any of the above RITstudies with glioma, which is known to be relatively ra-dioresistant.
Williams et al.84 evaluated the tumor dosimetry of9 0Y-labeled P96.5 MoAb of the IgG2a subclass, reactivewith P97, a cell surface glycoprotein expressed on glioma,administered to athymic nude mice bearing s.c. U-251 hu-man glioma xenografts 0.3-0.4 g in weight. MiniatureTLDs were implanted into tumors and normal tissues.Seven days after administration of 3.7 MBq of 90Y-labeled96.5, average absorbed doses of 37 700, 9800, and 3530mGy were measured in tumor, liver, and contralateral s.c.tissue.
Zalutsky et al.85 demonstrated that 2 1 1At-labeled 81C6
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
MoAb injected intrathecally into athymic nude rats 8 daysafter intrathecal injection of 5×105 TE-671 human rhab-domyosarcoma cells improved survival. 211At-labeled 81C6at a dose of 0.44 MBq increased survival by 113% com-pared to saline treated animals (median survival of 22.5days) and produced 3 apparent cures at 6 months, while 6out of 10 rats receiving 0.67 MBq of 211At-labeled 81C6were alive with no evidence of disease at 6 months.
Bender et al.86 reported that 5.55 MBq 125I-labeled 425F(ab’)2 fragments reactive with the epidermal growth fac-tor receptor administered at 4 and 11 days after tumor cellinoculation exhibited greater anti-tumor effects than 5.55MBq 131I-labeled F(ab’), fragments in athymic nude micebearing U-87MG human glioma xenografts. These differ-ences may be due to enhanced nuclear damage caused bythe high LET Auger electrons emitted by 1 2 5I followinginternalization of the 125I-labeled antibody fragments intothe glioma cells. The radiation dose to tumor using thestandard MIRD procedure was 190 mGy/11.1 MBq of1 2 5I-labeled F(ab’)2 fragments and 1590 mGy/11.1 MBqof 1 3 1I-labeled F(ab’), fragments. The radiation dose de-livered to normal organs for 125I-labeled fragments was 3 to60 mGy/11.1 MBq as compared to 26 to 400 mGy/11.1MBq with 31I-labeled fragments. No effort was made to usemicrodosimetry to calculate the dose to tumor and normaltissues. 8 7
H. Radioimmunotherapy of human mammarycarcinoma in animal models
Ceriani et al.88 conducted experimental RIT studieswith 4 MoAbs, raised against human milk fat globulemembrane glycoproteins also present on normal breast ep-ithelial cells, in athymic nude mice bearing MX-1 humanbreast cancer xenografts. 1311-labeled MoAbs injected as amixture (“cocktail”) inhibited growth of the tumor in adose dependent fashion. A single injection of 18.5 MBq of“‘I-labeled cocktail inhibited growth for 30 days while asimilar dose of 1 3 1I-labeled control IgG had no effect. Asecond administration of 18.5 MBq of 131I-labeled cocktailinjected at an appropriate interval inhibited tumor growthfor another 20 days. No estimate of radiation dose to tu-mors was made in this study. Ceriani et al. 89 gave singlei.p. injections of 1 3 1I- or 9 0Y-labeled Mc5 or BrE-1 anti-breast MoAbs to athymic nude mice bearing MX-1 s.c.xenografts. The maximum tolerated dose for McS was 55.5MBq for the 1 3 1I-conjugate and 9.25 MBq for theq-conjugate. For the BrE-1 MoAb, the maximum toler-ated doses for these radionuclides were 40.7 and 5.55 MBq,respectively. Dose dependent growth inhibition of MX-1tumors was observed with each of the radiolabeledMoAbs. The highest tumoricidal effectiveness was ob-tained with 131I-labeled Mc5. A second injection of 55.5MBq of 131I-labeled Mc5 at 20 days after the first injectionproduced prolonged inhibition of tumor growth.
Senekowitsch and colleague?’ investigated the thera-peutic efficacy of 1 3 1I-labeled BW 495/36 MoAb againsthuman mammary carcinoma xenografts. Two injections of7.4 MBq 131I-labeled BW 495/36 1 week apart resulted ina mean reduction of tumor volume of 88% within 42 days
561 Buchsbaum, Langmuir, and Wessels: Experimental radioimmunotherapy 567
post injection. 1 3 1I-labeled nonspecific antibody causedslight inhibition of tumor growth. The estimated radiationdose to tumor using scintigraphic imaging and the MIRDformulation was 77 000 mGy within 38 days.
I. Radioimmunotherapy of human small cell lungcarcinoma in animal models
Small cell lung cancer cells are relatively radiosensitive.Yoneda et a1.91 evaluated RIT of human small cell lungcancer xenografts of 0.5-1 cm in diameter in athymic nudemice using 131I-labeled TFS-4 MoAb reactive with humansmall cell lung cancer cells. Administration of 7.4 MBq of131I-labeled TFS-4 inhibited tumor growth when comparedwith 131I-labeled control MoAb. The tumor growth inhibi-tion was dose dependent. A radiation dose to tumor of10 380 mGy was estimated by scintigraphy and the MIRDformulation following the administration of 11.1-18.5MBq 1 3 1I-labeled TFS-4. Two injections of 18.5 MBq of1 3 1I-labeled TFS-4 at a 5 week interval inhibited tumorgrowth for about 60 days.
B e a u m i e r a n d c o l l e a g u e s9 2 evaluated the use of1 8 6Re-labeled MoAb NR-LU-10 reactive with small celllung carcinoma cells in athymic nude mice bearing s.c.SHT-1 small cell lung carcinoma xenografts. A multipledose regimen of 18.13 MBq 186Re-labeled NR-LU-10 di-vided into 4 doses over 10 days was less toxic than a singledose of 15.91 MBq 186Re-labeled NR-LU-10. Several doseregimens were evaluated. Radiation doses to tumor wereestimated by biodistribution data and the MIRD formula-tion with an infinite volume boundary correction factor of0.75 to account for the size of tumors used in this study.Two doses of 7.88 MBq on day 0 and 10.32 MBq on day 7(18.2 MBq total) were estimated to deliver 20 120 mGy totumor. Four doses of 8.07 MBq on day 0,2.22 MBq on day3, 10.36 MBq on day 7, and 1.67 MBq on day 10 (22.31MBq total) were estimated to deliver 26 710 mGy to tu-mor. This dose produced a 53 day mean growth delay thatwas statistically greater than equal doses of 186Re-labeledirrelevant antibody, with a few complete remissions, butmost tumors recurred.
J. Radioimmunotherapy of human cervical andovarian carcinoma in animal models
Human cervical carcinoma has a moderate radiosensi-tivity. Chen and collaborators93 performed RIT studieswith 131I-labeled TNT-1 IgG2a MoAb, with specificity fornuclear histones, against ME-180 human cervical carci-noma s.c. xenografts of approximately 0.5 cm3 in athymicnude mice. The 131I-labeled antibody was administered i.v.on days 1, 8, and 15. Tumor radiation dosimetry was esti-mated using tissue counting and imaging data and theMIRD formalism. The administration of 11.1 MBq1 3 1I-labeled TNT-l antibody for three successive weeklydoses, produced significant inhibition of tumor growthcompared to 131I-labeled irrelevant antibody, with regres-sions in 88% of treated animals and complete regressionsin 25% of the mice. After the first week of treatment with11.1 MBq 131I-labeled TNT-1 antibody, the mean radiation
Medical Physical, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
dose delivered to tumor was 10 660 mGy. In the secondand third weeks of therapy with 11.1 MBq 1 3 1I-labeledantibody, the mean tumor doses were 20 460 and 24 760mGy, respectively.
Molthoff et al. tested the therapeutic efficacy of1 3 1I-labeled 139H2 anti-episialin IgG1 MoAb in theNIH:OVCAR-3 human ovarian cancer s.c. xenograftmodel.94 The radiation dose to the tumor after a single i.v.injection of 18.5 MBq 131I-labeled 139H2 MoAb was esti-mated to be 13 000 mGy over a 7-day period calculatedfrom the biodistribution of the radiolabeled MoAb, andassuming uniform distribution within the tumor and or-gans, using the MIRD formalism. Well vascularized or-gans such as the liver, spleen, heart, lungs, and kidneysreceived between 4000 and 8000 mGy.
K. Radioimmunotherapy of human bladder cancer inan animal model
Lightfoot et al.9 5 evaluated the RIT of UCRU-BL-17CL human bladder cancer s.c. xenografts in athymicnude mice following a single i.p. injection of 153Sm-labeledBLCA-38 murine MoAb reactive with human bladder can-cers. Tumors in mice that received 9.25 MBq 153Sm-labeledBLCA-38 had a tumor doubling time of 8.4 days, whereastumors in mice injected with 9.25 MBq 153Sm-labeled con-trol antibody had a tumor doubling time of 5.7 days. Thisdifference became significant from day 21 onward. The ra-d i a t i o n d o s e t o t u m o r a n d n o r m a l o r g a n s f r o m153Sm-labeled BLCA-38 was estimated using biodistribu-tion studies and the MIRD technique. For an injection of37 MBq of 153Sm-labeled BLCA-38, the dose to tumor wasestimated to be 19 000 mGy, whereas the kidneys and liverwould receive a dose of 21 900 and 52 300 mGy, respec-tively. All other normal tissues would receive a lower dosethan tumor, but the whole-body dose was estimated to be8500 mGy. This radiolabeling was performed using thecyclic anhydride of DTPA, and the use of a more stablechelate might result in a lower dose to normal organs.
III. DISCUSSION
The use of the spheroid model has demonstrated theimportance of adequate antibody penetration prior to ra-dionuclide decay in micrometastases. Theoretical dosime-try modeling using the spheroid model has shown that,although high energy beta emitters are likely best for thetreatment of solid tumors, this may not be the case inmicrometastases, and in fact, lower energy emitters may bemore efficacious because a smaller proportion of the radi-ation dose is lost outside of the target volume, particularlywhen there is poor penetration.1 6
The results presented above indicate that RIT with 131I,9 0Y, 1 8 6Re, and 153Sm beta emitting, and 212Bi alpha emit-ting radionuclides attached to MoAbs has been effectiveagainst a variety of tumor types transplanted in animalsincluding leukemia and lymphoma, colon cancer, he-patoma, renal cell carcinoma, neuroblastoma, glioma,breast cancer, lung cancer, cervical carcinoma, ovariancarcinoma, and bladder cancer. The majority of investiga-
562 Buchsbaum, Langmuir, and Wessels: Experimental radioimmunotherapy 562
tors have estimated the dose to tumor and normal organsusing MIRD-based calculations (time-activity curve andequilibrium dose constant method).3*4 A few investigatorshave estimated the dose to tumor and normal organs usingTLDs and autoradiography. A summary of the results re-ported is shown in Table I. Recently, RIT studies havebeen conducted with the beta emitting radionuclide1 7 7Lu ,96 although no dosimetry estimates were made. Asingle injection of 7.4 or 12.95 MBq of 177Lu-labeled CC49reactive with human colon cancer was shown to producecomplete regression of established LS174T tumor xe-nografts.
The effectiveness of radiolabeled MoAb therapy de-pends on such factors as antibody specificity, immunore-activity and affinity; antigen density, availability, shedding,and heterogeneity; stability of the radiolabeled antibody;tumor vascularity, blood flow, and permeability. 8 0’ 9 7 , 9 8
Each of these factors will be discussed in some detail.Monoclonal antibodies have great specificity for recog-
nizing and selectively binding to antigens on tumor cells,and cell surface antigenic targets such as B-cell immuno-globulin idiotypes, growth factor receptors, and othertumor-associated, accessible, high density antigens havebeen defined for effective MoAb action.99 In principle, themore specific the antibody for a particular tumor type, thegreater the opportunity for the MoAb to show selectiveuptake in the tumor. A quantitative increase of an anti-genic substance on tumor cells or in the milieu of a tumorcan suffice for targeting MoAbs to this site.100 RadiolabeledMoAbs offer potential advantages over conventional ther-apeutic procedures by providing greater specificity as a re-sult of preferential binding of the antibodies to tumor cells.
The immunoreactivity of radiolabeled MoAb prepara-tions has been shown to affect the localization in tumor andnormal t i ssues .101-104 Yokoyama et al.101 p repared twohigh performance liquid chromatography fractions of1 2 5I-labeled Fab 96.5 MoAb reactive with human mela-noma. One fraction had relatively low immunoreactivity(25%-38%) and the second fraction had high immuno-reactivity (70%-81%). The two fractions had similar af-finity constants. In biodistribution studies in athymic nudemice bearing FEMX-11 human melanoma xenografts, thehigh immunoreactivity preparation rapidly cleared fromthe blood and normal organs while retention of radioactiv-ity in the tumor was prolonged. The low immunoreactivitypreparation had slower blood and normal organ clearancebut faster tumor clearance than the high immunoreactivityfraction. Thus highly immunoreactive antibody gavehigher tumor to normal tissue ratios. Koizumi et al.102compared the uptake in human osteogenic sarcoma xe-nografts of three 7 5Se-, 1 1 1In-, and 1 2 5I-labeled MoAbs re-active with human osteogenic sarcoma, and correlated theresults to their immunoreactivity. For “‘In-labeledMoAbs, increasing immunoreactivity resulted in higher tu-mor uptake, whereas with 7 5Se- and 1 2 5I-labeled MoAbs,there was not a direct correlation between increasing im-munoreactivity and increased tumor uptake. Sakaharaet al.103 found that as the molar ratio of cyclic DTPA con-jugated to a MoAb reactive with human α− fetoprotein in-
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
creased from 1.0 to 5.5, the immunoreactivity of the anti-body decreased and the uptake in an α− fetoprotein-producing human testicular tumor was lower by 35% butthe liver uptake was 71% higher. Similarly, Matzkuet al.104 reported that as the level of 1 2 5I substitution wasincreased in the M.2.9.4 MoAb reactive with human mel-anoma, the immunoreactivity decreased and the specificityindex of tumor localization decreased.
A potential method to increase the uptake and retentionof radiolabeled MoAbs in tumor and increase their thera-peutic efficacy is the use of MoAbs with greater affinity.However, if circulating tumor-associated antigen ispresent, then the higher affinity may result in greater non-tumor binding and less tumor localization than if a loweraffinity MoAb was used. Muraro et al.105 produced a seriesof MoAbs with different affinities for the TAG-72 antigenexpressed in human carcinomas. A direct correlation wasfound between the affinity of these six 125I-labeled MoAbs(range of 3.6 to 27.7×109M - 1) and the uptake in LS-174T human colon cancer xenografts.106 The effect ofMoAb affinity on LS174T anti-tumor efficacy was studiedwith three of the 1 3 1I-labeled MoAbs (range of 2.5 to27.7×10 9M - 1) reactive with the TAG-72 antigen.“’ Theresults of these studies demonstrated a substantial thera-peutic advantage of the two higher affinity antibodies ver-sus the lower affinity antibody at five radionuclide doselevels. Greater anti-tumor effects were seen using 2.5- to3-fold less of the higher affinity antibodies. Andrew et al.108
correlated the in vitro binding characteristics of fourMoAbs reactive with the murine Ly-2.1 or Ly-3.1 antigenwith their in vivo tumor localization characteristics. Theranking of the antibodies by affinity (range of 2.1 to28 .4×105M - 1) agreed with the ranking in terms of theirlocalization in tumors, but the immunoreactivity of theantibodies did not correlate with their tumor localization.In contrast, McCready et al.109 did not find that the in vitrobinding characteristics of two MoAbs reactive with humanmelanoma correlated with their localization in three hu-man melanoma xenografts. There is no good experimentaldata yet in humans to support the hypothesis that in-creased MoAb affinity results in better tumor localization.Langmuir et al. have shown that a lower affinity antibodyproduced a more even radionuclide distribution in multi-cell spheroids. When equivalent amounts of activity boundwere compared, the lower affinity antibody (3-fold lower)labeled with 125I produced significantly more cell killing,presumably because the range of 125I is so small.1 3
In regard to antigen density, Philben et al. 110 found thathuman colon cancer xenografts that had a higher CEAcontent (ng/g of tumor) had a higher tumor uptake of111In-labeled anti-CEA MoAb. Several other investigatorshave demonstrated a relationship between tumor antigencontent in human tumor xenografts and uptake of radiola-labeled antibody.100,111-113 It has also been shown in a num-ber of tumor systems that interferon enhances the expres-sion of tumor-associated antigens on tumor cells both invitro and in vivo, which results in increased localization ofradiolabeled MoAbs in tumors in animal models 44,114-116
and patients,1 1 7 and has produced greater therapeutic
563 Buchsbaum, Langmuir, ad Wessels: Experimental radioimmunotherapy 563
results. 4 4 This approach may also result in higher levels ofcirculating tumor-associated antigen, which may interferewith the localization of radiolabeled antibody in tumor.
In regard to tumor antigen availability, it is not possibleto generalize regarding the best location of antigen.Whether the tumor-associated antigen needs to be on thetumor cell membrane, in the extracellular milieu, or acces-sible intracellularly may vary for each tumor type, site ofgrowth, and radionuclide.100 Blumenthal et al.118 evaluatedthe localization of 131I-labeled NP-4 anti-CEA antibody infour size-matched human colon cancer xenografts (L174T,GW-39, GS-2, and Moser) grown s.c. in athymic nudemice. Intratumoral distribution of antigen, and intracellu-lar accessibility of antigen affected localization. Tumor-associated antigens shed into the serum have been found tocomplex with injected radiolabeled MoAbs,100,118 and thesecomplexes may accumulate in reticulonedothelial tissues,resulting in radiation toxicity to these tissues.
A concern in the use of radiolabeled MoAbs has beenthe degree of heterogeneity of binding to target cells withina tumor, due to the inability of antibody to penetrate uni-formly in a solid tumor mass and bind to all cells, 119-122 a swell as whether or not all cells within the tumor expressantigen. 123,124 It has been postulated that low affinity anti-bodies or antibody fragments would penetrate tumorsbetter.112,114 Andrew et al. 123 found that a cocktail of twoor three MoAbs reactive with different antigens expressedby human colon cancer showed a 2- to 3-fold higher %ID/g in the L1M1899 human colon cancer xenograft thandid single antibodies. Blumenthal et al.124 reported thathamsters bearing GW-39 human colon cancer xenograftsgiven a mixture of 1 3 1I-labeled NP4 anti-CEA antibodyand Mu-9 anti-colon-specific antigen-p showed better tu-mor growth inhibition of tumor masses less than 0.5 cm3 insize than was produced by either antibody alone at anequal radionuclide dose. Interestingly, the radiation dosedelivered to tumor by the antibody mixture was estimatedby the MIRD procedure to be 35 980 mGy/37 MBq,whereas the dose for the individual antibodies was esti-mated to be 11 500 mGy/37 MBq for NP-4 alone and41 370 mGy/37 MBq for Mu-9 alone. Thus, the enhancedtherapeutic efficacy of the antibody cocktail cannot be ex-plained by the radiation dose delivered, but it may be aresult of targeting a greater number of tumor cells or achange in the microdistribution of the antibodies with theantibody mixture.
Tumor vascularity, blood flow, and permeability arefactors that affect the localization and distribution of radi-olabeled MoAbs in tumors and influence their therapeuticeffectiveness. 100,121,122,125 As discussed above, the perme-ability of antibody fragments is greater than intact anti-body, and this may explain their greater therapeutice f f e c t i v e n e s s .3 2 - 3 5 , 1 0 0 , 1 1 1 , 1 2 1 , 1 2 2 B l u m e n t h a l e t a l .1 1 2 i m -planted the GW-39 human colon tumor in the cheekpouch, muscle, subcutaneously, or in the liver of hamstersor nude mice. They found that the tumors with a higherblood flow rate, vascular volume, and/or vascular perme-ability had a higher tumor uptake of 1 3 1I-labeled NP-4anti-CEA antibody. Blumenthal et al.126 reported that 5.55
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
MBq 1 3 1I-labeled Mu-9 antibody reduced the number ofblood vessels in GW-39 xenografts in athymic nude miceby 60% to 70%, reduced the vascular volume by 75%, theblood flow rate by 65%, and the vascular permeability toan IgG by 60% at 7 to 14 days after injection. These func-tional changes in tumor blood vessels reduced the tumoruptake of a second dose of radiolabeled antibody by 90%.Cope et al.1 2 7 found an enhanced localization of both spe-cific and control F(ab’)2 fragments in human glioma xe-nografts over a limited time period following local hyper-thermia which is known to increase tumor blood flow.
It must be kept in mind, however, that there are limi-tations of spheroid and animal models in mimicking whatoccurs in the clinical situation.1,97 The limitations of thespheroid model are that it does not allow for an evaluationof the role of normal host cells, the vasculature, blood flow,vascular permeability, or pharmacokinetics on the dose totumor. The limitations of the animal models in predictingwhat will occur in humans are their smaller size and there-fore smaller volume of radiolabeled antibody distribution,differences in tumor cell cycle and volume doubling timeswhich influence radioresponsiveness, the difference inplasma half-life of radiolabeled MoAbs in animals as com-pared to humans, lack of cross-reactive antigens in ani-mals, and the differences in bone marrow radiosensitivityand repopulation kinetics following RIT. These differencesmake it difficult to design studies in animals that will pre-dict what will occur in the clinical situation. The greateruse of disseminated tumor models in animals would comecloser to the clinical situation than a simple subcutaneoustumor model, and more effort should be paid experimen-tally to regional therapy models such as intracerebral orintraperitoneal that should allow for a greater tumor dose.
A few studies attempted to compare different radionu-clides in the same model system.46,47,73 It is recommendedthat in the future more investigators make such compari-sons which should include an analysis of the relative tox-icity including comparisons for both tumor and normaltissue damage to external beam therapy (see radiobiologysection 5). Alpha emitters and Auger electron emitters havethe potential advantage of high LET and radiobiologicaleffectiveness (RBE) which produces greater tumor cellkilling per quantity of radioactivity administered than lowand medium LET gamma ray and beta emitters. 5 Therewould be an advantage for alpha emitters if the radiola-beled MoAbs were uniformly distributed in tumors. How-ever, for bone marrow or other tissues more radiosensitivethan tumor, alpha emitters conjugated to MoAbs wouldhave less toxicity than beta emitters for an equivalent tu-mor cell kill. For normal tissues less radiosensitive thantumor, beta emitters would produce less toxicity. 5
It is also recommended that more investigators look atradiation dose heterogeneity using TLDs and autoradiog-raphy, so that the range of tumor radiation dose and doserate is reported. It is hoped that in the future, an answer tohow heterogeneity in antibody deposition affects absorbeddose distribution and the radiobiological consequences willbe understood for the various radionuclides and tumortypes studied in experimental RIT. It is hoped that a de-

564 Buchsbaum, Langmuir, and Wessels: Experimental radioimmunotherapy 564
finitive answer will be obtained for what radionuclides andforms of antibody are optimum for RIT of leukemias, mi-crometastases, and solid tumors, and most importantlyhow best to apply these techniques and information to thetreatment of tumors clinically.
ACKNOWLEDGMENTS
We thank Dr. Michael Zalutsky for his helpful com-ments and Renee Kite and Done11 Berry for typing themanuscript. Supported by NIH Grant CA44173.
a)Correspondence should be sent to: Donald J. Buchsbaum, Ph.D., De-partment of Radiation Oncology, University of Alabama at Birming-ham, 619 South 19th Street, Birmingham, AL 35233.
1B. W. Wessels, “Current status of animal radioimmunotherapy,” Can-cer Res. (Suppl.) 50, 970s-973s (1990).
2L. F. Mausner and S. C. Srivastava. “Selection of radionuclides forradioimmunotherapy,” Med. Phys. 20, 503-509 (1993).
3L. T. Dillman and F. C. Von der Lage, “Radionuclide decay schemesand nuclear parameters for use in radiation-dose estimation,” in, Med-ical Internal Radiation Dose (MIRD), (Society of Nuclear Medicine,New York, NY, 1975) Pamphlet No. 10, pp. 5-119.
4M. J. Berger, “Biodistribution of absorbed dose around point sources ofelectrons and beta particles in water and other media,” MIRD Pam-phlet No. 7, J. Nucl. Med. (Supp.) 12(5), 1-23 (1971).
5V. K. Langmuir, J. F. Fowler, S. J. Knox, B. W. Wessels, R. M.Sutherland, and J. Y. C. Wong, “Radiobiology and radiolabeled anti-body therapy as applied to tumor dosimetry,” Med. Phys. 20, 601-610(1993).
4R. Sutherland, F. Buchegger, M. Schreyer, A. Vacca, and J. -P. Mach,“Penetration and binding of radiolabeled anti-carcinoembryonic anti-gen monoclonal antibodies and their antigen binding fragments in hu-man colon multicellular tumor spheroids,” Cancer Res. 47, 1627-1633(1987).
5K. A. Walker, T. Murray, T. E. Hilditch, T. E. Wheldon, A. Gregor,and I. M. Harm, “A tumour spheroid model for antibody-targetedtherapy of micrometastases,” Br. J. Cancer 58, 13-16 (1988).
8C. S. Kwok, S. E. Cole, and S. -K. Liao, “Uptake kinetics of mono-clonal antibodies by human malignant melanoma multicell spheroids,”Cancer Res. 48, 1856-1863 (1988).
9C. S. Kwok, A. Crivici, W. D. MacGregor, and M. W. Unger, “Opti-mization of radioimmunotherapy using human malignant melanomamulticell spheroids as a model,” Cancer Res. 49, 3276-3281 (1989).
10V. K. Langmuir, J. K. McGann, F. Buchegger, and R. M. Sutherland,“131I-anticarcinoembryonic antigen therapy of LS174T human colonadenocarcinoma spheroids,” Cancer Res. 49, 3401-3406 (1989).
11V. K. Langmuir, R. W. Atcher, J. J. Hines, and M. W. Brechbiel,“Iodine-125-NRLU-10 kinetic studies and bismuth-212-NRLU-10 tox-icity in LS174T multicell spheroids,” J. Nucl. Med. 31, 1527-1533(1990).
12V, K. Langmuir, J. K. McGann, F. Buchegger, and R. M. Sutherland,“The effect of antigen concentration, antibody valency and size, andtumor architecture on antibody binding in multicell spheroids,” Nucl.Med. Biol. 18, 753-764 (1991).
13V. K. Langmuir, H. L. Mendonca, and D. V. Woo. “Comparisonsbetween two monoclonal antibodies that bind to the same antigen buthave differing affinities: Uptake kinetics and 125I-antibody efficacy inmulticell spheroids,” Cancer Res. 52, 4728-4734 (1992).
14V. K Langmuir, H. L. Mendonca, J. -L. Vanderheyden, and F. -M. Su,“Comparisons of the efficacy of 186Re- and 131I-labeled antibody inmulticell spheroids,” Int. J. Radiat. Oncol. Biol. Phys. 24, 127-132(1992).
15V. K. Langmuir and H. L. Mendonca, “The role of radionuclide dis-tribution in the efficacy of 131I-labeled antibody as modeled in multicellspheroids,” Antib. Immunoconj. Radiopharm. 5, 273-283 (1992).
16V. K. Langmuir and R. M. Sutherland, “Dosimetry models for radio-immunotherapy,” Med. Phys. 15, 867-873 (1988).
17M. Bardies, I. Lame, M. J. Myers, and J. P. Simoen, “A simplifiedapproach to beta dosimetry for small spheres labelled on the surface,”Phys. Med. Biol. 35, 1038-1050 (1990).
18M. Bardies, P. Thedrez. J. F. Gestin, and M. B. Marcille, “Use ofmulticell spheroids of ovarian carcinoma as an intraperitoneal radio-immunotherapy model: Uptake, retention kinetics and dosimetric eval-uation,” Int. J. Cancer 50, 984-991 (1992).
19V. K. Langmuir. B. W. Wessels. H. L. Mendonca, E. D. Yorke, and L.Montilla. “Comparisons of sectioned micro-TLD dose measurementswith predicted dose from “‘I-labeled antibody,” Med. Phys. 19, 1213-1218 (1992).
20D. M. Goldenberg. S. A. Gaffar, S. J. Bennett, and J. L. Beach. “Ex-perimental radioimmunotherapy of a xenografted human colonic tu-mor (GW-39) producing carcinoembryonic antigen,” Cancer Res. 41,4354-4360 (1981).
21R. M. Sharkey, M. J. Pykett, J. A. Siegel, E. A. Alger. F. J. Primus,and D. M. Goldenberg, “Radioimmunotherapy of the GW-39 humancolonic tumor xenograft with 131I-labeled murine monoclonal antibodyto carcinoembryonic antigen,” Cancer Res. 47, 5672-5677 (1987).
2 2J. M. Esteban, J. Schlom, F. Momex, and D. Colcher, “Radio-immunotherapy of athymic mice bearing human colon carcinomas withmonoclonal antibody B72.3: Histological and autoradiographic studyof effects on tumors and normal organs,” Eur. J. Cancer Clin. Oncol.23, 643-655 (1987).
2 3J. R. Zalcberg, C. H. Thompson, M. Lichtenstein. and I. F. C.McKenzie, “Tumor immunotherapy in the mouse with the use of“‘I-labeled monoclonal antibodies,” J. Natl. Cancer Inst. 72, 697-704(1984).
24B. W. Wessels, M. H. Griffith, E. W. Bradley, and B. Sibinski, “Dosi-metric measurements and radiobiological consequences of radioimmu-notherapy in tumor bearing mice, ” in Fourth International Radiophar-maceutical Dosimetry Symposium, edited by A. T. Schlafke-Stelson andE. E. Watson (Oak Ridge Associated Universities, Oak Ridge, TN1968), pp. 446-457.
25B. W. Wessels, R. L. Vessella, D. F. Palme II, J. M. Berkopec, G. K.Smith, and E. W. Bradley, “Radiobiological comparison of externalbeam irradiation and radioimmunotherapy in renal cell carcinoma xe-nografts,” Int. J. Radiat. Oncol. Biol. Phys. 17, 1257-1263 (1989).
26D. J. Buchsbaum, R. K. Ten Haken, D. B. Heidom. T. S. Lawrence, A.A. Glatfelter, V. H. Terry, D. M. Guilbault, Z. Steplewski, and A. S.Lichter, “A comparison of “‘I-labeled monoclonal antibody 17-1Atreatment to external beam irradiation on the growth of LS174T hu-man colon carcinoma xenografts,” Int. J. Radiat. Oncol. Biol. Phys. 18,1033-1041 (1990).
27D. J. Buchsbaum, P. G. Brubaker, D. E. Hanna, A. A. Glatfelter, V. H.Terry, D. IM. Guilbault, and Z. Steplewski, “Comparative binding andpreclinical localization and therapy studies with radiolabeled humanchimeric and murine 17-1A monoclonal antibodies,” Cancer Res.(Suppl.) 50, 993s-999s (1990).
28W. P. Neacy, B. W. Wessels, E. W. Bradley, S. Kovandi, T. Justice, S.Danskin, and H. Sands, “Comparison of radioimmunotherapy (RIT)and 4 MV external beam radiotherapy of human tumor xenografts inathymic mice,” J. Nucl. Med. 27, 902-903 (1986).
29M. H. Griffith, E. D. Yorke, B. W. Wessels, G. L. DeNardo, and W. P.Neacy, “Direct dose confirmation of quantitative autoradiography withmicro-TLD measurements for radioimmunotherapy,” J. Nucl. Med.29, 1795-1809 (1988).
30P. L. Roberson, D. J. Buchsbaum, D. B. Heidom, and R. K. TenHaken, “Three-dimensional tumor dosimetry for radioimmunotherapyusing serial autoradiography,” Int. J. Radiat. Oncol. Biol. Phys. 24,329-334 (1992).
31P. L. Roberson, D. J. Buchsbaum, D. B. Heidom, and R. K. TenHaken, “Variations in 3-D dose distributions for “‘Iodine-labeledmonoclonal antibody,” Antib. Immunoconj. Radiopharm. 5, 397-402(1992).
32F. Buchegger, A. Pelegrin, B. Delaloye, A. Bischof-Delaloye, and J. -P.Mach, “Iodine-131-labeled MAb F(ab’)2 fragments are more efficientand less toxic than intact anti-CEA antibodies in radioimmunotherapyof large human colon carcinoma grafted in nude mice,” J. Nucl. Med.31, 1035-1044 (1990).
33F. Buchegger, C. Pfister, K. Foumier, F. Prevel, M. Schreyer, S. Car-rel, and J. -P. Mach, “Ablation of human colon carcinoma in nudemice by 131I-labeled monoclonal anti-carcinoembryonic antigen anti-body F(ab’)2 fragments,” J. Clin. Invest. 83, 1449-1456 (1989).
34F. Buchegger, A. Vacca, S. Carrel, M. Schreyer, and J. -P. Mach,“Radioimmunotherapy of human colon carcinoma by 131I-labelledmonoclonal anti-CEA antibodies in a nude mouse model,” Int. J. Can-cer 41, 127-134 (1988).
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

565 Buchsbaum, Langmuir, and Wessels: Experimental radioimmunotherapy 565
35R. M. Sharkey, K. S. Weadock, A. Natale, L. Haywood, R. Aninipot,R. D. Blumenthal, and D. M. Goldenberg, “Successful radioimmuno-therapy for lung metastasis of human colonic cancer in nude mice,” J.Natl. Cancer Inst. 83, 627-632 (1991).
36T. Yokota, D. E. Milencic, M. Whitlow. and J. Schlom, “Rapid tumorpenetration of a single-chain Fv and comparison with other immuno-globulin forms,” Cancer Res. 52, 3402-3408 (1992).
37J. Schlom, A. Molinolo, I. F. Simpson, K. Siler, M. Roselli, G. Hinkle,D. P. Houchens, and D. Colcher, “Advantage of dose fractionation inmonoclonal antibody-targeted radioimmunotherapy,” J. Natl. CancerInst. 82, 763-771 (1990).
38Y. C. Lee, L. C. Washburn, T. T. H. Sun, B. L. Byrd, J. E. Crook, andZ. Steplewski, “Radioimmunotherapy of human colorectal carcinomaxenografts using 90Y-labeled monoclonal antibody CO17-IA preparedby two bifunctional chelate techniques,” Cancer Res. SO, 4546-4551(1990).
3 9L. C. Washburn, T. T. H. Sun, Y. -C. C. Lee, B. L. Byrd, E. C.Holloway, J. E. Crook, J. B. Stubbs, M. G. Stabin, M. W. Brechbiel, O.A. Gansow, and Z. Steplewski, “Comparison of five bifunctional che-late techniques for v-labeled monoclonal antibody CO17-1A,” Nucl.Med. Biol. 18, 313-321 (1991).
4 0L. C. Washburn, Y. -C. C. Lee, T. T. H. Sun, B. L. Byrd, E. C.Holloway, J. E. Crook, and Z. Steplewski, “Radioimmunotherapy ofSW 948 human colorectal carcinoma xenografts with repeated injec-tions of 90Y-labeled monoclonal antibody CO17-1A.” Antib. Immuno-conjug. and Radiopharm. 4, 729-734 ( 1991).
41R. M. Sharkey, F. A. Kaltovich, L. B. Shih, I. Fand, G. Govelitz, andD. M. Goldenberg, “Radioimmunotherapy of human colonic cancerxenografts with 90Y-labeled monoclonal antibodies to carcinoembry-onic antigen,” Cancer Res. 48, 3270-3275 (1988).
42R. R. Buras. B. G. Beatty, L. E. Williams, P. M. Wanek, J. B. Harris,R. Hill, and J. D. Beatty, “Radioimmunotherapy of human colon can-cer in nude mice,” Arch. Surg. 125, 660-664 (1990).
43R. R. Buras, J. Y. C. Wong, J. A. Kuhn, B. G. Beatty, L. E. Williams,P. M. Wanek, and J. D. Beatty, “Comparison of radioimmunotherapyand external beam radiotherapy in colon cancer xenografts,” Int. J.Radiat. Oncol. Biol. Phys. 25, 473-479 ( 1993).
“J. A. Kuhn, B. G. Beatty, J. Y. C. Wong, J. M. Esteban, P. M. Wanek,F. Wall, R. R. Bums, L. E. Williams, and J. D. Beatty, "Interferonenhancement of radioimmunotherapy for colon carcinoma,” CancerRes. 51, 2335-2339 (1991).
45C. S. Heacock, A. M. Blake, C. J. D’Aleo, and V. L. Alvarez, “Use ofan yttrium-90 labeled antibody for the treatment of human colon can-cer xenografts in nude mice,” Synthesis and Applications of Isotopi-tally Labelled Compounds, 783-786 (1989).
46D. J. Buchsbaum, T. S. Lawrence, P. L. Roberson, D. B. Heidorn, R.K. Ten Haken, and Z. Steplewski, “Comparison of “‘I- and90Y-labeled monoclonal antibody 17-1A for treatment of human coloncancer xenografts,” Int. J. Radiat. Oncol. Biol. Phys. 25, 629-638(1993).
47R. M. Sharkey, C. Motta-Hennessy, D. Pawlyk, J. A. Siegel, and D. M.Goldenberg, “Biodistribution and radiation dose estimates for yttrium-and iodine-labeled monoclonal antibody IgG and fragments in nudemice bearing human colonic tumor xenografts,” Cancer Res. 50, 2330-2336 (1990).
48B. A. Morton, B. G. Beatty, A. Mison, P. M. Wanek, and J. D. Beatty,“Role of bone marrow transplantation in yttrium-90 antibody therapyof colon cancer xenografts in nude mice,” Cancer Res. (Suppl.) 50,1008s-1010s (1990).
49F. M. Uckun, L. Souza, K. G. Waddick, M. Wick, and C. W. Song, “Invivo radioprotective effects of recombinant human granulocyte colony-stimulating factor in lethally irradiated mice,” Blood 75, 638-645(1990).
50R. D. Blumenthal, R. M. Sharkey, D. J. Snyder, H. J. Hansen, and D.M. Goldenberg, “Reduction of radioantibody-induced myelotoxicity inhamsters by recombinant interleukin-1,” Cancer Res. 48, 5403-5406(1988).
51F. M. Uckun, S. Gillis, L. Souza. and C. W. Song, “Effects of recom-binant growth factors on radiation survival of human bone marrowprogenitor cells,” Int. J. Radiat. Oncol. Biol. Phys. 16, 415-435(1989).
52V. S. Gallicchio, B. C. Hulette, M. J. Messino, C. Gass. M. W. Bie-schke, and M. A. Doukas, “Effect of various interleukins (IL-l, IL-2,and IL-3) on the in vitro radioprotection of bone marrow progenitors
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
(CFU-GM and CFU-MEG),” J. Biol. Response Mod. 8, 479-487(1989).
53R. Neta, S. Douches, and J. J. Oppenheim, “Interleukin 1 is a radio-protector,” J. Immunol. 136, 2483-2485 (1986).
54R. Neta, J. J. Oppenheim, and S. D. Douches, “Interdependence of theradioprotective effects of human recombinant interleukin-1, tumor ne-crosis factor, granulocyte colony-stimulating factor and murine recom-binant granulocyte-macrophage colony stimulating factor,” J. Immu-nol. 140, 108-111 (1988).
55R. Neta S. D. Douches, and J. J. Oppenheim, “Radioprotection byinterleukin-1,” in UCLA Symposia on Molecular and Cellular Biologv,edited by G. Goldstein, J. F. Bach, and H. Wigzal (Liss, New York,NY, 1986), p. 429.
56R. Neta, J. J. Oppenheim, S. D. Douches, P. C. Giclas, R. J. Imbra,and M. Karin, “Radioprotection with interleukin-1: Comparison withother cytokines,” in Progress in Immunology, edited by B. Cinader andR. G. Miller (Academic, San Diego, CA, 1986), Vol. 6, pp. 900-908.
57R. Neta and J. J. Oppenheim, “Cytokines in therapy of radiation in-jury,” Blood 72, 1093-1095 (1988).
58R. Neta M. B. Sztein, J. J. Oppenheim, S. Gills, and S. D. Douches,“The in vivo effects of interleukin 1. I. Bone marrow cells are inducedto cycle after administration of interleukin 1,” J. Immunol. 139, 1861-1866 (1987).
59R. B. Pedley, R. H. J. Begent, J. A. Boden, R. Boden, T. Adam, and K.D. Bagshawe, “The effect of radiosensitizers on radioimmunotherapy,using 131I-labelled anti-CEA antibodies in a human colonic xenograftmodel,” Int. J. Cancer 47, 597-602 (1991).
6 0V. K. Langmuir and H. L. Mendonca, “The combined use of131I-labeled antibody and the hypoxic cytotoxin SR 4233 in vitro and inviva,” Radiat. Res. 132, 351-358 (1992).
61E. P. Malaise, B. Fertil, N. Chavaudra, and M. Guichard, “Distribu-tion of radiation sensitivities for human tumor cells of specific histo-logical types: Comparison of in vitro to in vivo data,” Int. J. Radiat.Oncol. Biol. Phys. 12, 617-624 (1986).
62W. R. Redwood, T. D. Tom, and M. Strand, “Specificity, efficacy, andtoxicity of radioimmunotherapy in erythroleukemic mice,” CancerRes. 44, 5681-5687 (1984).
63W. T. Anderson-Berg, R. A. Squire, and M. Strand, “Specific radio-immunotherapy using v-labeled monoclonal antibody in erythroleu-kemic mice,” Cancer Res. 47, 1905-1912 (1987).
64O. A. Gansow, M. W. Brechbiel, G. Pippin, R. Huneke, P. Squire, andM. Strand, “Synthesis of 2-(p-SCN-benzyl)-trans-cyclohexyl-DTPA(CHX-DTPA); Use for a-particle radioimmunotherapy with Bi-212-mAb-103A in mice infected with the Rauscher leukemia virus,” J.Nucl. Med. (Suppl.) 32, 1056 (1991).
65R. M. Macklis, B. M. Kinsey, A. I. Kassis, J. L. M. Ferrara, R. W.Atcher, J. J. Hines, C. N. Coleman, S. J. Adelstein, and S. J. Burakoff,“Radioimmunotherapy with alpha-particle-emitting immunoconju-gates,” Science 240, 1024-1026 (1988).
66R. M. Macklis, W. D. Kaplan, J. L. M. Ferrara, R. W. Atcher, J. J.Hines, S. J. Burakoff, and C. N. Coleman, “Residents essay award:Alpha particle radio-immunotherapy: Animal models and clinical pros-pects,” Int. J. Radiat. Oncol. Biol. Phys. 16, 1377-1387 (1989).
67C. C. Badger, K. A. Krohn, A. V. Peterson, H. Shulman, and I. D.Bernstein, “Experimental radiotherapy of murine lymphoma with“‘I-labeled anti-Thy 1.1 monoclonal antibody,” Cancer Res. 45, 1536-1544 (1985).
68C. Nourigat, C. C. Badger, and I. D. Bernstein, “Treatment of lym-phoma with radiolabeled antibody: Elimination of tumor cells lackingtarget antigen,” J. Natl. Cancer Inst. 82, 47-50 (1990).
6 9C. C. Badger, K. A. Krohn, H. Shulman, N. Flournoy, and I. D.Bernstein, “Experimental radioimmunotherapy of murine lymphomawith 131I-labeled anti-T-cell antibodies,” Cancer Res. 46, 6223-6228(1986).
70D. A. Adams, G. L. DeNardo, S. J. DeNardo, G. B. Matson, A. L.Epstein, and E. M. Bradbury, “Radioimmunotherapy of human lym-phoma in thymic, nude mice as monitored by 31P nuclear magneticresonance,” Biochem. Biophys. Res. Commun. 131, 1020-1027 (1985).
71H. Schmidberger, D. J. Buchsbaum, B. R. Blazar, P. Everson. and D.A. Vallera, “Radiotherapy in mice with yttrium-90-labeled anti-Ly1monoclonal antibody: Therapy of the T cell lymphoma EL4,” CancerRes. 51. 1883-1890 (1991).
7 2R. A. Restock, J. L. Klein, P. Leichner, K. A. Kopher, and S. E.Order, “Selective tumor localization in experimental hepatoma by ra-

566 Buchsbaum, Langmuir, and Wessels: Experimental radioimmunotherapy 566
diolabeled antiferritin antibody,” Int. J. Radiat. Oncol. Biol. Phys. 9.1345-1350 (1983).
73J. L. Klein, T. H. Nguyen, P. Laroque, K. A. Kopher, J. R. Williams,B. W. Wessels, L. E. Dillehay, J. Frincke, S. E. Order, and P. K.Leichner, “Yttrium-90 and iodine-13 I radioimmunoglobulin therapy ofan experimental human hepatoma,” Cancer Res. 49, 6383-6389(1989).
74R. L. Vessella, V. Alvarez, R. -K. Chiou, J. Rodwell, M. Elson, D.Palme, R. Shafer, and P. Lange, “Radioimmunoscintigraphy and ra-dioimmunotherapy of renal cell carcinoma xenografts,” Natl. CancerInst. Monogr. 3, 159-167 (1987).
75R. K. Chiou, R. L. Vessella, C. Limas, R. B. Shafer, M. K. Elson, E.W. Arfman, and P. H. Lange, “Monoclonal antibody-targeted radio-therapy of renal cell carcinoma using a nude mouse model,” Cancer 61,1766-1775 (1988).
76R. L. Vessella, P. H. Lange, D. F. Palme II, R. K. Chiou, M. K. Elson,and B. W. Wessels, “Radioiodinated monoclonal antibodies in the im-aging and treatment of human renal cell carcinoma xenografts in nudemice,” in Targeted Diagnosis and Thempy, edited by J. D. Rodwell(Marcel Dekker, New York, NY, 1988), Vol. I, pp. 245-282.
77J. T. Kemshead, D. H. Jones, L. Lashford, J. Prichard, I. Gordon, F.Breatnach, and H. B. Coakham, “131-I coupled to monoclonal anti-bodies as therapeutic agents for neuroectodermally derived tumors:Fact or fiction?,” Cancer Drug Delivery 3, 25-43 ( 1986).
78N.-K. Cheung, B. Landmeier, J. Neely, A. D. Nelson, C. Abramowsky,S. Ellery, R. B. Adams, and F. Miraldi, “Complete tumor ablation withiodine-131-radiolabeled disialoganglioside GDZ-specific monoclonalantibody against human neuroblastoma xenografted in nude mice,” J.Natl. Cancer Inst. 77, 739-745 (1986).
79Y. -S Lee, D. E. Bullard, M. R. Zalutsky, R. E. Coleman, C. J. Wik-strand, H. S. Friedman, E. V. Colapinto, and D. D. Bigner, “Thera-peutic efficacy of antiglioma mesenchymal extracellular matrix131I-radiolabeled murine monoclonal antibody in a human glioma xe-nograft model,” Cancer Res. 48, 559-566 (1988).
80Y. Lee, D. E. Bullard, P. A. Humphrey, E. V. Colapinto, H. S. Fried-man, M. R. Zalutsky, R. E. Coleman, and D. D. Bigner, “Treatment ofintracranial human glioma xenografts with 131I-labeled anti-tenascinmonoclonal antibody 81C6,” Cancer Res. 48, 2904-2910 (1988).
81J. M. Schuster, P. K. Garg, D. D. Bigner, and M. R. Zalutsky, “Im-proved therapeutic efficacy of a monoclonal antibody radioiodinatedusing N-succinimidyl-3-(tri-n-butylstannyl) benzoate,” Cancer Res.51, 4164-4169 (1991).
82M. R. Zalutsky, M. A. Noska, E. V. Colapinto, P. K. Garg, and D. D.Bigner, “Enhanced tumor localization and in vivo stability of a mono-clonal antibody radioiodinated using N-succinimidyl 3-(tri-n-butylstannyl) benzoate,” Cancer Res. 49, 5543-5549 ( 1989).
83E. V. Colapinto, M. R. Zalutsky, G. E. Archer, M. A. Noska, H. S.Friedman, S. Carrel, and D. D. Bigner, “Radioimmunotherapy of in-tracerebral human glioma xenografts with 131I-labeled F(ab’)2 frag-ments of monoclonal antibody Mel-14,” Cancer Res. SO, 1822-1827(1990).
84J. A. Williams, B. W. Wessels, M. D. Wharam, S. E. Order, P. M.Wanek, J. K. Poggenburg, and J. L. Klein, “Targeting of humanglioma xenografts in vivo utilizing radiolabeled antibodies,” Int. J. Ra-diat. Oncol. Biol. Phys. 18, 1367-1375 (1990).
85M. R Zalutsky, P. K. Garg, J. M. Schuster, S. Garg, G. E. Archer, H.E. Fuchs, and D. D. Bigner, “Effective treatment of experimental hu-man neoplastic meningitis (NM) with intrathecal astatine-211 mono-clonal antibody (MAb),” J. Nucl. Med. (Suppl.) 32, 922 (1991).
86H. Bender, H. Takahashi, K. Adachi, P. Belser. S. Liang, M. Prewett,M. Schrappe, A. Sutter, U. Rodeck, and D. Herlyn, “Immunotherapyof human glioma xenografts with unlabeled, 131I-, or 125I-labeled mon-oclonal antibody 425 to epidermal growth factor receptor,” CancerRes. 52, 121-126 (1992).
87J. L. Humm, J. C. Roeske, D. R. Fisher, and G. T. Y. Chen, “Micro-dosimetric concepts in radioimmunotherapy,” Med. Phys. 20, 535-544(1993).
88R. L. Ceriani and E. W. Blank, “Experimental therapy of human breasttumors with 131I-labeled monoclonal antibodies prepared against thehuman milk fat globule,” Cancer Res. 48, 4664-4672 ( 1988).
89R. L. Ceriani, E. W. Blank, J. A. Peterson, H. Battifora, and H. Singh,“Immunotherapeutic preclinical evaluation of anti-human milk fatglobule MoAbs Mc5 and BrE-1,” Antib. Immunoconj. Radio-pharm. 3, 181-198 (1990).
90R. Senekowitsch, G. Reidel, S. Mollenstadt, H. Kriegel, and H. -W.
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
Pabst, “Curative radioimmunotherapy of human mammary carcinomaxenografts with iodine- 131-labeled monoclonal antibodies,” J. Nucl.Med. 30, 531-537 (1989).
91S. Yoneda. M. Fujisawa, J. Watanabe, T. Okabe, F. Takaku, T.Homma, and K. Yoshida, “Radioimmunotherapy of transplantedsmall cell lung cancer with 131I-labelled monoclonal antibody,” Br. J.Cancer 58, 292-295 (1988).
92P. L. Beaumier, P. Venkatesan, J. -L. Vanderheyden, W. D. Burgua, L.L. Kunz, A. R. Fritzberg, P. G. Abrams and A. C. Morgan, Jr., “ 186R eradioimmunotherapy of small cell lung carcinoma xenografts in nudemice,” Cancer Res. 51, 676-681 (1991).
93F. -M. Chen, D. K. Taylor, and A. L. Epstein, “Tumor necrosis treat-ment of ME-180 human cervical carcinoma model with 131I-labeledTNT-l monoclonal antibody,” Cancer Res. 49, 4578-4585 (1989).
94C. F M. Molthoff, H. M. Pinedo, H. M. M. Schluper, and E. Boven,“Influence of dose and schedule on the therapeutic efficacy of131I-labelled monoclonal antibody 139H2 in a human ovarian cancerxenograft model,” Int. J. Cancer 50, 471-480 (1992).
95D. V. Lightfoot, K. K. Walker, G. R. Boniface, E. L. Hetherington, M.E. Izard, and P. J. Russell, “Dosimetric and therapeutic studies in nudemice xenograft models with 153samarium-labelled monoclonal anti-body, BLCA-38,” Antib. Immunoconj. Radiopharm. 4, 319-330(1991).
96J. Schlom, K. Siler, D. E. Milenic, D. Eggensperger, D. Colcher, L. S.Miller, D. Houchens, R. Cheng, D. Kaplan, and W. Goeckeler, “Mon-oclonal antibody-based therapy of a human tumor xenograft with a“‘Lutetium-labeled immunoconjugate,” Cancer Res. 51, 2889-2896(1991).
97D. J. Buchsbaum, “Experimental radioimmunotherapy: Methods toincrease therapeutic efficacy relevant to the study of human cancer,”Antib. Immunoconj. Radiopharm. 4, 693-701 (1991).
98D. J. Buchsbaum and T. S. Lawrence, “Tumor therapy with radiola-be led monoc lona l an t ibod ies , ” An t ib . Immunocon j . Radio-pharm. 4, 245-272 (1991).
99T. A. Waldmann, “Monoclonal antibodies in diagnosis and therapy,”Science 252, 1657-1662 (1991).
100D. M. Goldenberg, R. D. Blumenthal, and R. M. Sharkey, “Biologicaland clinical perspectives of cancer imaging and therapy with radiola-beled antibodies,” Sem. Cancer Biol. 1, 217-225 (1990).
101K. Yokoyama, J. C. Reynolds, C. H. Paik, V. K. Sood, P. J. Maloney,S. M. Larson, and R. C. Reba, “Immunoreactivity affects the biodis-tribution and tumor targeting of radiolabeled anti-P97 Fab fragment,”J. Nucl. Med. 31, 202-210 (1990).
102M. Koizumi, K. Endo, Y. Watanabe, T. Saga, H. Sakahara, J. Konishi,T. Yamamuro, and S. Toyama, “Pharmocokinetics of internally labeledmonoclonal antibodies as a gold standard: Comparison of biodistribu-
tion of 7 5Se-, 111In- and 125I-labeled monoclonal antibodies in osteo-genie sarcoma xenografts in nude mice,” Cancer Res. 49, 1752-1757(1989).
103H. Sakahara, K. Endo, T. Nakashima, M. Koizumi, H. Ohta, K. Tor-izuka, T. Furukawa, Y. Ohmomo, A. Yokoyama, K. Okada, O.Yoshida, and S. Nishi, “Effect of DTPA conjugation on the antigenbinding activity and biodistribution of monoclonal antibodies againstα− fetoprotein.” J. Nucl. Med. 26, 750-755 (1985).
104S. Matzku, H. Kirchgessner, W. G. Dippold, and J. Bruggen, “Immu-noreactivity of monoclonal anti-melanoma antibodies in relation to theamount of radioactive iodine substituted to the antibody molecule,”Eur. J. Nucl. Med. 11, 260-264 (1985).
105R. Muraro, M. Kuroki, D. Wunderlich, D. J. Poole, D. Colcher, A.Thor, J. W. Greiner, J. F. Simpson, A. Molinolo, P. Noguchi, and J.Schlom, “Generation and characterization of B72.3 second generationmonoclonal antibodies reactive with the tumor-associated glycoprotein72 antigen,” Cancer Res. 48, 4588-4596 (1988).
106D. Colcher, M. F. Minelli, M. Roselli, R. Muraro, D. Simpson-Milenic,and J. Schlom. “Radioimmunolocalization of human carcinoma xe-nografts with B72.3 second generation monoclonal antibodies,” CancerRes. 48, 4597-4603 (1988).
107J. Schlom, D. Eggensperger, D. Colcher, A. Molinolo, D. Houchens. L.S. Miller, G. Hinkle, and K. Siler, “Therapeutic advantage of high-affinity anticarcinoma radioimmunoconjugates,” Cancer Res. 52, 1067-1072 (1992).
108S. M. Andrew, R. W. Johnstone, S. M. Russell, I. F. C. McKenzie, andG. A. Pietersz, “Comparison of in vitro cell binding characteristics offour monoclonal antibodies and their individual tumor localizationproperties in mice,” Cancer Res. 50, 4423-4428 (1990).

567 Buchsbaum, Langmuir, and Wessels: Experimental radioimmunotherapy 567
109D. R. McCready. C. M. Balch, I. J. Fidler. and J. L. Murray, “Lack ofcomparability between binding of monoclonal antibodies to melanomacells in vitro and localization in vivo.” J. Natl. Cancer Inst. 81, 682-687(1989).
110V. J. Philben. J. G. Jakowatz. B. G. Beatty, W. G. Vlahos, R. J.Paxton, L. E. Williams, J. E. Shively, and J. D. Bratty, “The effect oftumor CEA content and tumor size on tissue uptake of indium 111-labeled anti-CEA monoclonal antibody,” Cancer 57, 571-576 (1986).
111R. D. Blumenthal, R. M. Sharkey, R. Kashi, and D. M. Goldenberg,“Comparison of therapeutic efficacy and host toxicity of two different131I-1abelled antibodies and their fragments in the GW-39 colonic can-cer xenograft model,” Int. J. Cancer 44, 292-300 (1989).
112R. D Blumenthal, R. M. Sharkey, R. Kashi, A. M. Natale, and D. M.Goldenberg, “Influence of animal host and tumor implantation site onradioantibody uptake in the GW-39 human colonic cancer xenograft,”Int. J. Cancer 44, 1041-1047 (1989).
113T. R Shockley, K. Lin, C. Sung, J. A. Nagy, R. G. Tompkins, R. L.Dedrick, H. F. Dvorak, and M. L. Yarmush, “A quantitative analysisof tumor specific monoclonal antibody uptake by human melanomaxenografts: Effects of antibody immunological properties and tumorantigen expression levels,” Cancer Res. 52, 357-366 (1992).
114G. Rowlinson, F. Balkwill, D. Snook, G. Hooker, and A. A. Epenetos,“Enhancement by y-interferon of in vivo tumor radiolocalization by amonoclonal antibody against HLA-DR antigen,” Cancer Res. 46,6413-6417 (1986).
115F. Guadagni, J. Schlom, S. Pothen, S. Pestka, and J. W. Greiner,“Parameters involved in the enhancement of monoclonal antibody tar-geting in vivo with recombinant interferon,” Cancer Immunol. Immu-nother. 26, 222-230 (1988).
116M. Matsui, S. Yoshimura, T. Nakanishi, and S. Ferrone, “Effect oftumor size on the enhancement by y-interferon of the localization ofradiolabeled F(ab’)2 f r agmen t s of anti-intercellular adhesionmolecule-l monoclonal antibodies in human colon carcinoma cellsgrafted in nude mice,” Cancer Res. 52, 1309-1313 (1992).
117M. G. Rosenblum, L. M. Lamki, J. L. Murray, D. J. Carlo, and J. U.Gutterman, “Interferon-induced changes in pharmacokinetics and tu-mor uptake of “‘In-labeled antimelanoma antibody 96.5 in melanomapatients,” J. Natl. Cancer Inst. 80, 160-165 (1988).
118R. D. Blumenthal, R. M. Sharkey, R. Kashi, A. M. Natale, and D. M.Goldenberg, “Physiological factors influencing radioantibody uptake:A study of four human colonic carcinomas,” Int. J. Cancer 52, 1-7(1992).
119R. K. Jain and L. T. Baxter, “Mechanisms of heterogeneous distribu-tion of monoclonal antibodies and other macromolecules in tumors:Significance of elevated interstitial pressure,” Cancer Res. 48, 7022-7032 (1988).
120K. Fujimoti, D. G. Covell, J. E. Fletcher, and J. N. Weinstein, “Mod-eling analysis of the global and microscopic distribution of immuno-globulin G, F(ab’)2, and Fab in tumors,” Cancer Res. 49, 5656-5663(1989).
121R, K. Jain. “Vascular and interstitial barriers to delivery of therapeuticagents in tumors,” Cancer Metastasis Rev. 9, 253-266 (1990).
122R. K. Jain, “Haemodynamic and transport barriers to the treatment ofsolid tumours,” Int. J. Radiat. Biol. 60, 85-100 (1991).
123S. M. Andrew, J. G. Teh, R. W. Johnstone, S. M. Russell, R. H.Whitehead, I. F. C. McKenzie, and G. A. Pietersz, “Tumor localiza-tion by combinations of monoclonal antibodies in a new human coloncarcinoma cell line (LIM1899),” Cancer Res. 50, 5225-5230 (1990).
124R. D. Blumenthal, R. Kashi, R. Stephens, R. M. Sharkey, and D. M.Goldenberg, “Improved radioimmunotherapy of colorectal cancer xe-nografts using antibody mixtures against carcinoembryonic antigen andcolon-specific antigen-p,” Cancer Immunol. Immunother. 32, 303-310(1991).
125H. Sands, P. L. Jones, S. A. Shah, D. Palme, R. L. Vessella, and B. M.Gallagher, “Correlation of vascular permeability and blood flow withmonoclonal antibody uptake by human Clouser and renal cell xe-nografts,” Cancer Res. 48, 88-193 (1988).
126R. D. Blumenthal, R. M. Sharkey, R. Kashi, and D. M. Goldenberg,“Suppression of tumor vascular activity by radioantibody therapy: Im-plications for multiple cycle treatments,” Selective Cancer Therapeu-tics 7, 9-16 (1991).
127D. A. Cope, M. W. Dewhirst, H. S. Friedman, D. D. Bigner, and M. R.Zalutsky, “Enhanced delivery of a monoclonal antibody F(ab’)2 frag-ment to subcutaneous human glioma xenografts using local hyperther-mia,” Cancer Res. SO, 1803-1809 (1990).
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

An overview of imaging techniques and physical aspects of treatmentplanning in radioimmunotherapy
Peter K. LeichnerUniversity of Nebraska Medical Center, Department of Radiology, Omaha. Nebraska 68198-1045
Kenneth F. KoralThe University of Michigan Medical School, Department of Internal Medicine, Ann Arbor,Michigan 48109
Ronald J. JaszczakDuke University Medical Center, Department of Radiology, Durham, North Carolina 27710
Alan J. GreenThe Department of Clinical Oncology, The Royal Free Hospital School of Medicine, London, NW3 2PFUnited Kingdom
George T. Y. Chen and John C. RoeskeMichael Reese/University of Chicago, Center for Radiation Therapy, Chicago, Illinois 60637
(Received 18 March 1992; accepted for publication 15 December 1992)
Planar and tomographic imaging techniques and methods of treatment planning in clinicalradioimmunotherapy are reviewed. In clinical trials, the data needed for dosimetry and treat-ment planning are, in most cases, obtained from noninvasive imaging procedures. The requireddata include tumor and normal organ volumes, the activity of radiolabeled antibodies taken upin these volumes, and the pharmacokinetics of the administered activity of radiolabeled anti-bodies. Therefore, the topics addressed in this review include: ( 1) Volume determinations oftumors and normal organs from x-ray-computed tomography and magnetic resonance imaging,(2) quantitation of the activity of radiolabeled antibodies in tumors and normal organs fromplanar gamma camera views, (3) quantitative single-photon emission computed tomographyand positron emission tomography, (4) correlative image analysis, and (5) treatment planningin clinical radioimmunotherapy.
1. INTRODUCTION
Knowledge of the absorbed dose in tumors and normaltissues in clinical and experimental radioimmunotherapy(RIT) is essential for an understanding of the underlyingradiobiological principles of tumor dose-response relation-ships and normal-tissue toxicity. In clinical RIT, the doseis calculated rather than measured, and calculations areusually based on noninvasive imaging procedures. To de-velop a treatment plan for an individual patient, prospec-tive dose estimates can be made by using a tracer activity ofradiolabeled antibody to obtain phamacokinetic informa-tion prior to the administration of a larger therapeutic ac-tivity. As the pharmacokinetics depend in part on the massof antibody administered, the mass used for treatmentplanning purposes should be nearly the same as that usedfor the therapeutic administration. Additionally, dose cal-culations often require that tumor and normal organmasses be estimated. This can be done by using one ormore of the tomographic methods discussed in this review.Currently, it is impractical to determine the mass of everyorgan that can be imaged for every patient. However, it isoften feasible to compute the mass of those tumors that canbe imaged, the mass of the tumor-bearing organ and themasses of those organs that demonstrate a significant up-take of radiolabeled antibody. The dose to other organs canbe approximated by making a class dose estimate whichcan, for example, be based on tabulated values of "S"
factors. 1 This is particularly important for radionuclidesthat emit high-energy photons (e.g., 1 3 1I) which irradiatethe whole body.
For beta-particle dosimetry, knowledge of tumor andnormal organ volumes is not essential as long as the sourcevolumes are large enough so that only a negligible fractionof the energy of the contained activity escapes. For diag-nostically detectable tumors this condition is usually met.For calculations of the mean dose only the mean value ofthe concentration of activity and kinetic information arerequired. However, for calculations of the variation in localdose, knowledge of the distribution of activity in the sourcevolume is necessary. The quantitation of activity distribu-tions in tumors is an area of considerable current researchinterest.
Even after all methods of quantitation have been used,the information about the spatial distribution and temporalactivity of radiolabeled antibodies in patients is rather lim-ited. It is, therefore, necessary to interpolate and extrapo-late the available information and construct a model sothat dose calculations can be carried out. In this sense, thedose is calculated for a model rather than the patient. 2 Theoverall effort in RIT dosimetry and treatment planning isto make the model resemble the patient as much as possi-ble.
In the past decade, much work has been done to developmethodology, computer algorithms and software for quan-titative imaging and image analysis to generate the infor-mation required for dosimetry in RIT and the development
589 Med. Phys. 20 (2), Pt. 2, Mar/Apr 1993 0094-2405/93/020569-l0$01.20 © 1993 Am. Assoc. Phys. Med. 569
570 Leichner et al.: imaging techniques and treatment planning in radioimmunotherapy 570
of better models. The principal purpose of this review is tosummarize these developments so that they will becomemore readily accessible to those who have an interest in orare entering the field of radioimmunotherapy. The body ofthis review is organized into five sections: (1) volume de-terminations from computed tomography (CT) and mag-netic resonance (MR) scans, (2) activity quantitationfrom planar gamma camera views, (3) quantitative single-photon emission computed tomography (SPECT) andpositron emission tomography (PET) of radiolabeled an-tibodies, (4) correlative image analysis, and (5) treatmentplanning in RIT. The presentation of this material is in-tended for the nonspecialist and is intentionally nonmath-ematical. For an in-depth understanding of any of the top-ics covered, the reader is referred to the literature cited.
A. Volume determinations from CT and MR scans
In the context of RIT, tumor and normal organ volumecomputations are used for two purposes: dosimetry andfollowup studies of patients to assess tumor response totherapy. Although normal-organ volume computationshad been carried out by several investigators, 3-5 hepatictumor volume determinations from CT scans were devel-oped independently by Moss et al.6 and Leichner et al.7
Similar volume determinations for pheochromocytoma tu-mors were later made by Koral et al. 8 These methods werelabor intensive and slow because regions of interest (ROIs)corresponding to tumor and normal tissues were generatedmanually.
Volume computations were automated to some extentby Yang et al.9 who have described interactive computersoftware for generating ROIs in transverse CT slices ofpatients with primary hepatic cancers. This method re-quired an operator to specify lower and upper CT numbersfor boundary pixels of the liver and define a “seed pixel”within the liver for a computer search of the first boundarypixel. After the first boundary pixel was located, nearestneighboring pixels were analyzed by the computer softwarefor the same boundary condition. In this manner, a con-necting vector was specified for the first and second pixels.This process was repeated until a complete ROI was tracedand displayed on a computer graphics work station. If thecomputer went astray, the operator eliminated the incor-rect portion of the ROI interactively. Discrimination be-tween normal liver and tumor was achieved using a histo-gram method. Histograms of CT number distributionswithin each ROI were obtained. However, individual his-tograms did not contain sufficient statistical information todistinguish between tumor and normal liver. Global histo-grams were, therefore, generated by summing over individ-ual histograms. The global histograms were analyzed byfitting them to the sum of three Gaussian distribution func-tions. Threshold CT numbers for assigning volume ele-ments (voxels) to either tumor or normal tissues were de-termined in this manner. Tumor and normal liver volumeswere computed by summing over the corresponding voxels.Although the computer software was initially developedfor volume computations from CT examinations of pa-tients with primary hepatic cancers, it has been generalized
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
to include MR scans and applied to volumetric analyses ofdiverse cancers and benign lesions.10,11 Comparison of CT-based volume computations of liver tumors and normalliver with autopsy data for four patients demonstrated thatcomputations were accurate to within 2.0%-6.4%.1 2
As discussed by Udupa,1 3 volume determinations fromtransverse CT and MR slices represent only one aspect ofimage segmentation in the field of three-dimensional (3D)imaging in medicine. It is anticipated that 3D imaging willplay an important future role in improving dosimetry andtreatment planning in clinical RIT.
B. Activity quantitation from planar gamma cameraviews
The most widely used methods for quantitating tumorand normal organ uptake of radiolabeled antibodies arebased on conjugate (180-deg opposed) gamma cameraviews. Two methods have been and are used in clinicalRIT. One of these was introduced by Sorenson 14 and fur-ther developed by Thomas et al. 15,16 It requires the acqui-sition of a transmission scan and conjugate-view countrates for the quantitation of activity. This approach wasadopted by Leichner et al.7 to estimate the activity of1 3 1I-labeled antiferritin in the tumor and liver of patientswith hepatoma. In view of the large tumor and liver vol-umes and the variation of body thickness over these vol-umes, a pixel-by-pixel attenuation correction was includedin a computer program for activity calculations. Forsmaller tumors in locations where body thickness does notvary greatly, regional attenuation correction should be sat-isfactory. The same method was used by Hammond et al. 17
to quantitate the distribution of 1 3 1I-labeled F (ab’)2 frag-ments of monoclonal antibody in humans. These authorsevaluated the validity of this method in phantom studiesusing a fillable, tissue-equivalent organ-scanning phantomwith tumors and organs of various sizes. Less than 10%error was found in quantitating 1 3 1I activities in a 4-cm-diam lesion. However, in a 2-cm tumor the error wasgreater than 21%. Similar results were obtained by Earyet al.18 in a study using phantoms and dogs.
A variation of the conjugate-view method was devel-oped by Wu and Siegel.1 9 This technique also requirescount rates for opposing gamma camera views, but theneed for a transmission scan is obviated by measuring thebuildup factor. The buildup factor results from the increasein transmission under broad-beam conditions in clinicalnuclear medicine. It depends on photon energy, source ge-ometry, collimator, and other measurable parameters. Bymaking careful measurements of the buildup factor, theseauthors demonstrated improved accuracy in quantitating9 9 mTc activities, as compared to the transmission method.More recently, Siegel et al.2 0 have used the buildup factormethod to quantitate the pharmacokinetics of 131I-labeledmonoclonal antibodies in patients with B-cell lymphomas.
Although the results obtained in phantom studies havedemonstrated the validity of the conjugate-view approach,the errors in patient measurements are likely to be signif-icantly greater than phantom results indicate. In part, thisis due to the fact that intravenous administrations of cur-
571 Leichner et al.: lmaging techniques and treatment planning in radioimmunotherapy 571
rently available radiolabeled antibodies result in a systemicdistribution, with blood pool and liver activities that canpersist for days post injection. Consequently, there is asuperposition of activities that is difficult to resolve in pla-nar images. On the other hand, if the tumor-to-blood andtumor-to-normal tissue ratios are sufficiently high, mea-surement errors will be reduced. There are, however, twoadditional problems associated with planar imaging thatcan best be resolved with emission tomographic methods.As stated previously, planar gamma camera images do notprovide the volumetric information needed for dosimetry.Volumes obtained from CT and MR scans are in mostcases used in radiation absorbed-dose calculations. How-ever, CT- and MR-derived volumes need not necessarily bethe same as the volumes in which radiolabeled antibodieslocalize (localization volumes) because the physiologicaluptake of antibodies may not correspond exactly to theanatomical configuration of an organ or tumor. The secondproblem is that planar images do not provide sufficientinformation about the distribution of activity within anorgan or tumor. Therefore, only the mean value of theabsorbed dose can be calculated. This may be an overesti-mate in hypoxic or necrotic regions at the core of a tumorand an underestimate at the periphery where the dose maybe significantly higher than the mean. To improve dosim-etry in clinical RIT, it is important that improvements inquantitative emission tomography continue to be pursued.
C. Quantitative SPECT and PET imaging ofradiolabeled antibodies
The long-term goals of quantitative emission-computedtomography (ECT) include: (1) the determination of lo-calization volumes corresponding to tumors and normalorgans, (2) measurements of the distribution and range ofradiolabeled antibody activities within large tumors, and(3) the measurement of activity concentration within assmall an anatomic ROI as possible. The achievement ofthese goals is to a large extent governed by the physicalcharacteristics of the imaging system, the emission charac-teristics of radionuclides, the reconstruction algorithm em-ployed, and the method of data analysis (e.g., definition ofROIs).
Physical factors that affect quantitative SPECT havebeen discussed by Jaszczak et al.21 and perhaps the mostimportant of these are: (1) scatter and attenuation correc-tions, (2) limited spatial and energy resolutions of gammacameras, (3) septral penetration within conventional col-limators by high-energy photons (e.g., 1 3 1I), and (4) sta-tistical noise resulting from low count densities.
For SPECT, the spatial resolution is primarily deter-mined by the collimator selected and the radius of rotationused. The collimator also determines the geometric sensi-tivity or the number of gamma photons that will be de-tected and, hence, the statistical fluctuations (“noise”)that will result in the reconstructed image. The intrinsicresolution of a NaI scintillation crystal is about 3.5 mm;however, at a distance of 15 cm from the camera surface,the geometric resolution of a high-resolution collimator isapproximately 8 mm. Therefore, the resulting system res-
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
olution is about 9 mm. In general, the full-width-at-half-maximum (FWHM) of SPECT devices ranges from about7-18 mm. For PET systems, the spatial resolution rangesfrom about 6-13 mm. As a result, activity quantitation ofsmall tumors, such as metastatic lesions, by ECT methodsmay be subject to large errors.
One approach to correct for Compton scattering inSPECT is based on the method proposed by Jaszczaket a1.22 This approach requires the acquisition of two pla-nar projection data sets, one in the photopeak of the radi-onuclide and the other suitably windowed to image Comp-ton scattered photons. A fraction (ƒ) of the scatter imageis then subtracted from the photopeak image to compen-sate for Compton scatter and improve quantitation. Intheir original work, Jaszczak et al.22 imaged a 9 9 mTc linesource in air and water, and from the reconstructed pho-topeak and scatter images determined a value of ƒ=0.5.Subsequently, Koral et al. 23,24 demonstrated in phantomstudies with 99mTc and 131I as imaging agents that the valueoff depends on a number of parameters. Using 9 9 mTc anda particular algorithm and ROI, ƒ was independent ofsource location and background activity.
The Compton scatter subtraction method was employedby Green et al.2 5 in phantom and clinical studies with131I-labeled monoclonal anti-CEA. Energy windows wereset at 364 keV±10% for the photopeak and 277 keV± 18% for the scatter window. With these window set-tings, the count rates for the photopeak and scatter imageswere the same. The gamma camera employed by Greenet al. was equipped with a 400-keV high-resolution colli-mator, and the system was calibrated in a series of phan-tom studies. The reconstruction algorithm included an at-tenuation correction using the method of Chang.26 Fo rtheir gamma camera system and reconstruction algorithmused, Green et al. determined that ƒ=0.54, was optimalfor 1 3 1I which is quite close to that obtained by Jaszczaket al.22 for 9 9 mTc. In clinical studies with 1 3 1I anti-CEA,Green et al. validated scatter-corrected SPECT by estimat-ing the activity concentration in the heart obtained fromROIs and comparing it to the activity in blood samples.This yielded a correlation coefficient of 0.96. Additionally,scatter-corrected SPECT was compared with the transmis-sion conjugate-view method by measuring the activity inthe liver and spleen. Planar imaging resulted in signifi-cantly higher values than SPECT for the spleen butshowed no significant difference for the liver. This is con-sistent with the statements made earlier that the activity ina small tumor or organ is likely to be overestimated if it issurrounded by underlying and overlying activity.
SPECT quantitation of 1 3 1I has also been reported byIsrael et a1.27 who used filtered backprojection to generatetomographic slices. SPECT studies were validated in a se-ries of phantom measurements and in patients by measur-ing bladder urine concentrations. A different approach toquantitative SPECT was adopted by Denardo et al.28 whoused an empirical method of scatter correction for 123I and1 1 1In. These authors generated a post reconstruction ma-trix using a linear attenuation coefficient that varied withthe distance of pixels from the boundary. This removed
572 Leichner et al.: Imaging techniques and treatment planning in radioimmunotherapy 572
scattered photons and image counts in transverse sliceswere related to the counts from an equivalent source in air.
There is considerable interest in developing special im-age processing techniques for quantitative imaging of radi-olabeled antibodies29-31 and improved reconstruction algo-rithms to more accurately compensate for scatter,attenuation, and collimator blur.32-34 An analysis of fourintrinsic attenuation correction methods by Glick et al. 3 5
has shown that of the methods studied, those developed byBellini et a1.33 and Hawkins et al.34 have the least nonsta-tionary 3D modulation transfer functions and 3D point-spread function with minimal noise amplification. For auniform attenuation medium, these two algorithms aregood choices when post-reconstruction filtering is consid-ered. Furthermore, the intrinsic reconstruction algorithmdescribed by Hawkins et al.34 has been validated in phan-tom studies36 with nonuniform activity distributions of9 9 mTc and 1 1 1In and for 1 1 1In-labeled antibodies in the liv-ers of beagle dogs.37 Preliminary data obtained for patientswho were administered 1 1 1In- or 1 3 1I-labeled antibodieshave shown that this algorithm yields activity concentra-tions (Bq/ml) that are the same as those in patients’ tissuesamples.38 Much interest is also being shown in maximumlikelihood-expectation maximization (ML-EM) recon-struction algorithms.39,40 Recent work has demonstratedthat these techniques can result in smaller relative noisemagnitude as compared to filtered back projection3 0’31 andproduce fewer artifacts.4 1’4 3 Additionally, there are ongo-ing efforts in image reconstruction to use a priori informa-tion concerning the source.44,45 These approaches have thepotential of significantly improving quantitative SPECT inclinical studies.
Although the emphasis in this review is on recent de-velopments in imaging related to clinical RIT and radio-immunodiagnosis (RAID), quantitative SPECT has beenstudied by many investigators,46-54 and it is, in part, theirwork that has provided the foundation for the ongoingefforts discussed above.
In addition to the development of improved reconstruc-tion algorithms, progress has been made in developing bet-ter imaging systems. The resolution and sensitivity ofSPECT devices can be improved simultaneously by usingspecially designed collimators55-59 and SPECT systemshaving larger detector areas.60-65
The common denominator of all the quantitativeSPECT studies cited is careful validation of the methodol-ogy used to extract quantitative information from recon-structed images. Validation is absolutely essential becausedifferent SPECT devices and reconstruction algorithmshave a profound effect on the quality of reconstructed im-ages.
The use of PET devices in oncologic imaging has beenlimited in the past but there is growing interest in theapplication of positron emitters in the diagnosis and treat-ment of cancer. As is the case for SPECT devices, there isa variety of PET systems. Positron instrumentation hasbeen described in reviews by Brownell et al.66 a n dTer-Pogossian. 67 PET reconstruction algorithms have, forexample, been reported by Phelps et al. 68,69 The advantages
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
of PET over SPECT imaging are increased spatial resolu-tion, as discussed, and attenuation correction with a highdegree of precision. The resulting image quality is superiorto that achieved with SPECT. The growing interest in on-cologic PET imaging is, in part, related to the increasingnumber of whole-body devices and the fact that PET stud-ies have the potential to provide the physiological informa-tion for the diagnosis of cancer based on altered tissuemetabolism and to monitor the effects of therapy on me-tabolism. A detailed description of the applications of PETin oncologic imaging has recently been given by Straussand Conti.70 In the field of clinical RIT, Larson et al. 71 andPentlow et al.72 have reported PET scanning of 124I-labeled3F8 monoclonal antibody as a method of tumor dosimetryand treatment planning prior to the administration of131I-3F8 for the therapy of neuroblastoma. These authorsconclude that this technique shows promise for determin-ing the radiation-absorbed dose for 131I-3F8 RIT.
D. Correlative image analysis
Three-dimensional (3D) representations of 2D tomog-raphic data and correlative analysis of CT, MR, PET, andSPECT scans have become increasingly important in med-icine. Work in 3D rendering of bony structures carried outby Hemmy et al.73 and Herman et al.74 was based on CTscans and proved clinically useful in craniofacial surgeryand orthopedics. In this early work only bony surfaceswere visualized and soft-tissue information was lost or notused in the process of reformatting the CT data. However,subsequent investigations by Goldwasser et al.,75 Jackel,7 6
Lenz et al.,7 7 and Hoehne et al.78 have addressed the soft-ware and hardware problems of 3D displays that preservethe gray-scale information of the original data. These ef-forts have produced display systems that are generally ap-plicable to diagnostic radiology and surgical planning. Inthe past few years, computer systems for 3D displays ofmedical images have become commercially available.
Three-dimensional correlative imaging has been em-ployed by several authors in the treatment of brain tumorsand neurological disorders. For example, Schad et al.7 9
have used 3D correlative imaging in radiotherapy treat-ment planning of brain tumors. Their technique required astereotactic head holder made of wood to precisely andreproducibly localize the target volume during CT, MR,and PET imaging and radiotherapy. Magnetic resonancescans were obtained in addition to CT because of MRssuperior s o f t t i s s u e c o n t r a s t . F o r P E T i m a g i n g ,(1 8F)-2-deoxyglucose (FDG) and H2
1 5O tracers were usedto assess the rate of glucose utilization and perfusion ofbrain tumors. The target volume was defined by manuallydrawing ROIs in tomographic slices and subsequently gen-erating 3D displays of this volume and the patients’ headcontour. Others, for example, Vannier and Gayou,80 haveadvocated computer solutions for automated registrationof multimodality images because these are noninvasive andcan be applied retrospectively.
One such approach has been described by Pelizzariet al81 who generated surface models of the head based onCT, PET, and MR scans to derive the coordinate transfor-

573 Leichner et al.: Imaging techniques and treatment planning In radioimmunotherapy 573
mations required for 3D congruence of these models. Afterthe transformations were determined, volume informationcould be transferred between scans and displayed threedimensionally or in tomographic slices. As the work ofLevin et al.82 has shown, this technique can result in strik-ing 3D and 2D representations of MR and PET imagesthat are of clinical importance in planning brain surgery.Although correlative imaging has not yet been employed inthe RIT of malignant brain tumors, it is quite possible thatMR and PET imaging would be useful in assessing tumorresponse to therapy. For example, FDG and H2
1 5O PETstudies following RIT could be used to monitor changes inglucose utilization and perfusion and related to possibleanatomic changes in MR images.
Correlative CT-SPECT imaging was used by Krameret al.83 to identify anatomic sites corresponding to uptakeof 1 1 1In-labeled monoclonal anti-CEA (1 1 1In-MAb) in pa-tients with colorectal adenocarcinoma. SPECT and CTstudies of the abdomen were acquired for each patient. Inthe initial studies, 5 7Co point sources were placed at ana-tomic landmarks to provide coordinate information forsubsequent matching of CT and SPECT data sets. In laterstudies, flexible 57Co line sources were used because theseyielded information about the shape and location of thebody surface in SPECT scans and permitted matching withthe body surface in CT scans. For this reason, separateSPECT acquisitions were made for 1 1 1In-MAb and the5 7Co markers. Transaxial CT and SPECT slices were re-formatted into a common matrix size. Initial matching ofpairs of CT and SPECT slices was achieved by identifyingcoordinates belonging to anatomic landmarks (CT) andmarkers (SPECT). If necessary, CT slices were translatedand rotated until superposition of anatomic landmarks andthe corresponding 57Co markers was achieved in a “fused”image. Once the CT and SPECT studies had beenmatched, ROIs in SPECT slices representing tissue uptakeof 1 1 1In-MAb were transferred to CT slices. CorrelativeCT-SPECT imaging enabled identification of anatomicsites of tumor uptake of 1 1 1 In-MAb as well as nonspecifictissue accumulation and confirmed a small lesion detectedby CT.
Although the work of Kramer et al. was qualitative inthat quantitation of the activity of 1 1 1In-MAb was not thegoal of their investigation, it opens up the possibility ofrelating quantitative SPECT to anatomical imaging modal-ities (CT and MRI) for dosimetry and treatment planningin clinical RIT. In preliminary work, Koral et a. 84 usedfive point markers for superimposing SPECT and CT im-ages of a lymphoma RIT patient. Patient dosimetry wasbased on volumes of interest transferred from CT toSPECT after superposition had been achieved.
E. Treatment planning
Treatment planning relies on quantitative imaging, ra-diation absorbed-dose estimates, and biological input pa-rameters for the development of treatment strategies. Anexample of a biological input parameter is hematopoietictoxicity, often the dose-limiting toxicity in clinical RIT.The development of clinical protocols for the treatment of
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
hepatoma with 131I- and 9 0Y-labeled polyclonal antiferritinIgG is an example of how dosimetric and medical consid-erations can be used in clinical RIT.85,86 In a Phase I-IITrial, administered activities of “‘I-labeled antiferritinranged from 1.18 to 5.81 GBq. It was determined that anadministered activity of 1.11 GBq “saturated” most he-patomas and that larger activities did not result in in-creased tumor uptake. Additionally, an evaluation of thehematopoietic toxicity associated with the intravenous in-jection of 1 3 1I antiferritin IgG demonstrated that an activ-ity of 1.85 GBq was well tolerated by most patients. 8 7
These considerations led to a treatment regimen of admin-istering 1.11 GBq on Day 0 and 0.74 GBq on Day 5. Thetime interval between administrations was approximatelyequal to the effective half-life of 131I antiferritin IgG in thehepatoma. The second injection, therefore, “re-saturated”or maximized the activity and dose rate in the tumor andled to an increase in the integrated absorbed dose. Bonemarrow toxicity has remained a limiting factor in RIT. Ina effort to alleviate marrow suppression, Meredith et al. 8 8
used fractionation in the administration of radiolabeled an-tibodies in patients with metastatice colon cancer. Up tothree weekly fractions were used to administer a total ac-tivity of 1.33 GBq of 131I-labeled antibodies. These authorsreported only a minimal reduction in bone marrow toxicityfor this fractionation schedule and the antibody and radi-olabel used. To date, the most promising responses to RIThave been achieved by Press et al. 89 through the use oflarge adminis te red ac t iv i t ies (8 .58-22.5 GBq) of131I-labeled antibodies and autologous bone marrow trans-plantation in the treatment of refractory non-Hodgkin’slymphoma.
The development9 0 of 9 0Y-labeled antiferritin IgG wasbased on the fact that, due to their higher energy, 9 0Y betaparticles would produce a higher absorbed-dose rate and amore uniform absorbed-dose distribution than 1 3 1I betaparticles. Vriesendorp et al.91 have compared two groupsof patients with refractory non-Hodgkin’s disease whowere treated with 131I- and 9 0Y-labeled antiferritin IgG andshown that the frequency and duration of tumor responsewas significantly greater in those patients who were admin-istered y-labeled antiferritin. An obvious disadvantage isthat 90Y cannot be imaged quantitatively and that a secondradionuclide, 111 In, has to be conjugated to the same anti-body for imaging and dosimetry. A review of imaging,dosimetry, and treatment planning for 131I-labeled antifer-ritin and anti-AFP in hepatoma, 131I-labeled anti-CEA inintrahepatic biliary cancer, and 111In-labeled antiferritin inhepatoma and Hodgkin’s disease has been given by Leich-ner et al.1 0
The general requirements for treatment planning is clin-ical RIT have been discussed by DeNardo et al.92 A com-puter program and imaging methodology, specifically de-veloped for this purpose, have been described by Maceyet al.93 In this approach, a whole-body transmission imageis acquired, using a line source containing 131I, prior to theadministration of 131I-labeled antibodies. Following intra-venous infusion of 131I-labeled MoAb, serial conjugate im-ages of the whole-body, brain, chest, abdomen, and pelvis

574 Leichner et al.: Imaging techniques and treatment planning In radioimmunotherapy 574
are acquired. The activity in a tumor or normal organ iscalculated from these data by the transmission conjugate-view method, previously described. Radiation absorbed-dose calculations are made according to the MIRDschema.
A computer simulation for treatment planning, applica-ble to RIT, has been reported by Sgouros et al. 94 In thiscalculational method, it is assumed that tumor and normalorgan uptake of nonuniformly distributed radionuclides isaccurately known and that this information can be trans-ferred readily to CT images. Radiation absorbed-dose cal-culations are based on independently determined cumu-lated activities, the corresponding CT volumes, and aconvolution of the source volume cumulated activity witha point-source kernel. The electron-gamma shower (EGS)Monte Carlo code, discussed elsewhere in this volume, isused to generate point-source kernels in the form of lookuptables. The results of absorbed-dose calculations are storedin a two-dimensional dose matrix which is converted into aset of color-coded isodose contours. The contours are thendisplayed superimposed on CT images corresponding tothe target plane. As the point-source kernels are generatedfor an infinite medium of uniform composition, tissue in-homogeneities and boundary effects, such as soft-tissuebone interfaces, are not taken into account. However,methods for including these effects in absorbed-dose calcu-lations are presented in another section of this volume.
The commonality in the various approaches to treat-ment planning is that radiation absorbed-dose calculationsfor tumors and normal tissues are made as accurately aspossible within the limitations of available imaging devicesand reconstruction algorithms for quantitative ECT. Ac-curate dosimetry is essential for gaining a better under-standing of tumor dose-response relationships and assess-ments of the toxicity associated with the administration ofradiolabeled antibodies. It is anticipated that with contin-ued progress in biotechnology, immunochemistry, quanti-tative imaging and dosimetry, treatment planning in clini-cal RIT will play an increasingly important role. Tomaximize the radiation absorbed dose in tumors and re-duce normal-tissue toxicity, treatment planning may in-clude the route of administration (e.g., intravenous, intra-arterial, intraperitoneal, intrapleural, etc.) a choice ofantibodies or fragments of antibodies, and a choice of ra-dionuclides (e.g., low-energy electron or alpha emitters formicrometastases and high-energy beta emitters for largetumors). To optimize the therapy of primary and meta-static lesions it may, in fact, be advantageous to administercombinations of antibodies labeled with different radionu-clides. The number of permutations is potentially verylarge, and it will be the objective of treatment planning tooptimize RIT for each individual patient.
II. SUMMARY AND DISCUSSION
In this overview of imaging techniques and treatmentplanning in RIT, we have described the physical aspects ofthese methods based principally on the recent literature. Asummary of the steps involved in quantitative imaging andtreatment planning for macroscopic tumors that can be
Medical Physics, Vol. 20, No. 2, Pt. 2. Mar/Apr 1993
imaged using CT, MR, or ECT is given below. We recog-nize that these methods are not applicable to microme-tastases or circulating leukemia cells. However, there aremany ongoing clinical trials in RIT for which quantitativeimaging and treatment planning provide important infor-mation about tumor targeting, radiation-absorbed doses intumors and normal organs, and an assessment of responseto treatment.
A. Data acquisition and calculations prior to therapy
Radiolabeled antibody imaging using a tracer activitybefore the administration of a therapeutic activity is essen-tial to determine tumor and normal organ uptake and pro-vide a rationale for therapy. In general, at least one andpreferably two or more SPECT or PET studies should beacquired in addition to planar views to reliably determineclearance rates and cumulated activities for tumors andnormal organs. The mass of antibody used in the imagingstudies should be nearly the same as that for the therapeu-tic administration to avoid differences in pharmacokineticsdue to differences in administered antibody masses. In ad-dition to ECT studies, CT or MR scans in conjunctionwith correlative image analysis are important for volumedeterminations and a definitive identification of anatomicalstructures that show uptake of radiolabeled antibodies.
As hematopoietic toxicity is a limiting factor in RIT,information about the marrow dose is necessary for gaininga better understanding of the relationship between marrowdose and toxicity in patients who may have had prior treat-ment with chemotherapy, radiotherapy, or a combinationof both. Activity in bone marrow can be estimated fromserial gamma camera images using a method described bySiegel. 95 This should be compared with the activity in serialblood samples to estimate the fraction of blood in the mar-row for use in absorbed-dose calculations.
As the spatial resolution of imaging devices is limited,image-based dosimetry provides macroscopic informationabout absorbed-dose distributions. Additionally, the errorsin quantitating tumor and normal organ uptake of radio-labeled antibodies depend on the radiolabel used, the vol-ume, and the imaging device. In a SPECT study of111In-labeled antibodies in the livers of beagle dogs, 37 ab-solute values of percent differences between autopsy dataand computed activities ranged from 2.3% to 7.5%. How-ever, these were relatively large volumes (in the range of400 ml) and from the discussion of the FWHM of SPECTdevices it follows that for smaller volumes the percent dif-ferences will be larger. Similarly, from the discussion ofPET devices it follows that PET imaging will provide moreaccurate data than SPECT imaging of radiolabeledantibodies.71,72 With SPECT or PET, activity distributionscan be determined in sufficiently large tumors.” Neverthe-less, the local absorbed dose on the multicellular level willneed to be determined from autoradiographs or histologicmeasurements of tumor biopsies. As shown by Hui et al.96
in a study of absorbed-dose distributions in follicular lym-phoma, the local absorbed dose may vary from the averagedose by a factor of two and 70% to 80% of the tissue mayreceive less than the average dose. These data are indicative
575 Leichner et al.: lmaging techniques and treatment planning in radioimmunotherapy 575
of the variations in absorbed dose to be expected in clinicalRIT.
For photon-emitting radionuclides (e.g., 1 3 1I) “S” val-ues for tumors and tumor-bearing organs can be estimatedby at least two methods. A computer program developedby Johnson9 7 accounts for the presence of tumors usingMonte Carlo calculations. These calculations were madefor spherical tumors only, and organ distortion due to thepresence of a tumor was not taken into account. A moregeneral approach to tumor geometry was adopted byStinchcomb et al.98 who calculated “S” values for tumorsand host organs on the basis of tabulated values of thespecific absorbed fractions calculated by Berger.9 9’100 Thishad the advantage of making calculations faster than thosebased on the Monte Carlo approach. Additionally, the tu-mor was modeled as a rectangular solid with three shapeparameters which made this method more flexible, andorgan distortion was taken into account in the computa-tions. By interfacing their computations with a computerprogram 1 0 1 available for implementing the MIRD system,Stinchcomb et al.98 were thus able to compute the dose totumors and normal organs, including the tumor-bearingorgan.
After all available methods of quantitation have beenemployed and dose calculations made, medical and radio-biological considerations enter into the treatment decision.For example, in a study of v-labeled antiferritin in pa-tients with hepatoma,8 6 treatment was based on achieving acalculated minimum initial tumor dose rate of 10 cGy/h. Ifcalculations indicated that this minimum dose rate was notachievable at a given level of administered activity, patientswere entered into other protocols. In other studies, admin-istered activities were fractionated because of limited tu-mor uptake85 or in an effort to reduce marrow toxicity.” Ifmarrow toxicity is circumvented by autologous bone mar-row transplantation, second-organ toxicity may becomethe constraint in administered activity.8 9
B. Data acquisition and calculations following thetherapeutic administration
The radionuclide imaging that is feasible after the ad-ministration of a therapeutic activity of radiolabeled anti-bodies depends on the radiolabel used and the administeredactivity itself. Although it has been suggested by Clarkeet al.102 that quantitative bremsstrahlung imaging is feasi-ble for therapeutic activities of 90Y-labeled antibodies, thisis an as yet untried method. A difficulty is that if“‘In-labeled antibodies are used for treatment planning, alarge fraction of the bremsstrahlung spectrum will be ob-scured by the photopeaks and Compton scattered photonsof 111In. For radionuclides that emit beta particles and alsohave photopeaks (e.g., 1 3 1I, 6 7Cu, 1 8 6Re, 1 8 8Re) imaging isconstrained only by dead time considerations of gammacameras. This problem is more severe for 131I than for theother radionuclides mentioned because of the relativelylarge abundance of the 364-keV photons (0.82/dis) of 131I.For most commercially available large-field-of-viewgamma cameras, a total-body activity of approximately1.11-1.85 GBq of 1 3 1 I appears to be the upper limit for
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
imaging. The importance of imaging therapeutic activitieslies in monitoring therapy and testing whether scaling fromthe tracer to the therapeutic activity introduced changes inthe pharmacokinetics and hence the absorbed dose. In ad-dition to imaging, blood and urine samples are obtained todetermine clearance rates and test for immune complexes,anti-antibodies and metabolites.
Followup CT or MR scans to assess tumor response totherapy are currently employed by most investigators as anobjective means of determining this important parameter.
ACKNOWLEDGMENTS
One of the authors (PKL) acknowledges support underDOE Grant No. DE-FG02-91ER61195. Co-author KFKacknowledges support of PHS Grant No. RO1-CA38790awarded by the National Cancer Institute. Co-author RJJacknowledges support of DOE Grant No. DE-GF05-91ER60894 and PHS Grant No. RO1-CA33541 awardedby the National Cancer Institute.
1W. S. Snyder, M. R. Ford, G. G. Warner, and S. B. Watson, "'S,'Absorbed dose per unit cumulated activity for selected radionuclidesand organs,” Medical Internal Radiation Dose (MIRD) Committee,Pamphlet No. 11 (The Society of Nuclear Medicine, NY, 1975).
2R. Loevinger, “Distributed radionuclide sources,” in Radiation Dosim-etry, edited by F. H. Attix and E. Tochilin (Academic, NY, 1969), Vol.3.
3S. B. Heymsfield, T. Fulenwider, B. Nordinger, R. Barlow, P. Sones,and M. H. Kutner, “Accurate measurement of liver, kidney, and spleenvolume and mass by computerized axial tomography,” Ann. Int. Med.90, 185-187 (1979).
4J. M. Henderson, S. B. Heymsfield, J. Horowitz, and M. H. Kutner,“Measurement of liver and spleen volume by computed tomography,”Radiology 141, 525-527 (1981).
5A. A. Moss, M. A. Friedman, and A. C. Brito, “Determination of liver,kidney and spleen volumes by compted tomography: An experimentalstudy in dogs,” J. Comput. Assist. Tomogr. 5, 12-14 (1981).
6A. A. Moss, C. E. Cann, M. A. Friedman, F. S. Marcus, K. J. Resser,and W. Berninger, “Volumetric CT analysis of hepatic tumors,” J.Comput. Assist. Tomogr. 5, 714-718 (1981).
7P. K. Leichner, J. L. Klein, J. B. Garrison, R. E. Jenkins, E. L. Nick-oloff, D. S. Ettinger, and S. E. Order, “Dosimetry of 131I labeled anti-ferritin in hepatoma: A model for radioimmunoglobulin dosimetry,”Intl. J. Radiat. Oncol. Biol. Phys. 7, 323-333 (1981).
8K. F. Koral, X. Wang, J. C. Sisson, J. Botti, L. Meyer, S. Mallette, G.M. Glazer, and R. S. Adler, “Calculating radiation absorbed dose forpheochromocytoma tumors in 131-I MIBG therapy,” Int. J. Radiat.Oncol. Biol. Phys. 17, 211-218 (1989).
9N.-C. Yang, P. K. Leichner, E. K. Fishman, S. S. Siegelman, T. L.Frenkel, J. R. Wallace, D. M. Loudenslager, W. G. Hawkins, and S. E.Order “CT volumetrics of primary liver cancers,” J. Comput. Assist.Tomogr. 10, 621-628 (1986).
10P. K. Leichner, N.-C. Yang, B. W. Wessels, W. G. Hawkins, S. E.Order, and J. L. Klein, “Dosimetry and treatment planning in radio-immunotherapy,” in Frontiers of Radiation Therapy and Oncology, ed-ited by J. M. Vaeth and J. M. Meyer (Karger Verlag, Basel, Switzer-land, 1990), pp. 109-120.
11A. Rahmouni, A. Yang, C. Tempany, T. Frenkel, J. Epstein, P. Walsh,P. K. Leichner, C. Ricci, and E. Zerhouni, “Accuracy of in-vivo as-sessment of prostatic volume by magnetic resonance imaging and tran-srectal ultrasonography,” J. Comp. Assist. Tomogr. 16, 935-940(1992).
12D. S. Ettinger, P. K. Leichner, S. S. Siegelman, E. K. Fishman, J. L.Klein, and S. E. Order, “Computed tomography assisted volumetricanalysis of primary liver tumor as a measure of response to therapy,”Am. J. Clin. Oncol. 8, 413-418 (1985).
13J. K. Udupa, “Computer aspects of 3D imaging in medicine: A tuto-rial” in 3D Imaging in Medicine, edited by J. K. Udupa and G. T.Herman (CRC, Boca Raton. FL, 1991).
576 Leichner et al.: Imaging techniques and treatment planning in radioimmunotherapy 576
14J. A. Sorenson, “Quantitative measurement of radioactivity in-vivo bywhole-body counting, ” in Instrumentation in Nuclear Medicine, editedby G. J. Hine and J. A. Sorenson (Academic, New York, NY, 1974),Vol. 2.
15S. R. Thomas, H. R. Maxon, and J. G. Kereiakes, “In-vivo quantitationof lesion radioactivity using external counting methods,” Med. Phys. 3,253-255 (1976).
16S. R. Thomas, R. C. Purdom, J. G. Kereiakes, M. J. Gelfond, and H.R. Maxon. "Dose to the liver and spleen in pediatric patients under-going technetium -99m sulfur colloid scans," Radiology 133,465-467(1979).
17N. D Hammond, P. J. Moldofsky, M. R. Beardsley, and C. B. Mul-hem, Jr., “External imaging techniques for quantitation of distributionof I-131 F(ab’) fragments of monoclonal antibody in humans,” Med.Phys. 11, 778-783 (1984).
18J. F. Eary, F. L. Appelbaum, L. Durack, and P. Brown, “Preliminaryevaluation of the opposing view method for quantitative gamma cam-era imaging,” Med. Phys. 16, 382-387 (1989).
19R. K. Wu and J. A. Siegel, “Absolute quantitation of radioactivityusing the buildup factor,” Med. Phys. 11, 189-192 (1984).
20J. A. Siegel, D. M. Goldenberg, J. A. Horowitz, R. M. Sharkey, T. C.Hall, S. Murthy, H. Goldenberg, R. E. Lee, and L. C. Swayne, “Tumorand organ dosimetry for I-131 labeled LL2 (EPB-2) monoclonal anti-body in patients with B-cell lymphomas,” Antib. Immunoconj. Radiop-harm. 4, 26 (1991).
21R. J. Jaszczak, R. E. Coleman, and F. R. Whitehead, “Physical factorsaffecting quantitative measurements using camera-based single-photonemission computed tomography,” IEEE Trans. Nucl. Sci. NS-28,69-80 (1981).
2 2R. J. Jaszczak, K. L. Greer, C. E. Floyd, C. C. Harris, and R. E.Coleman, “Improved SEPCT quantification using compensation forscattered photons,” J. Nucl. Med. 25, 893-900 ( 1984).
23K. F. Koral, F. M. Swailem, S. Buchbinder. N. H. Clinthome, W. L.Rogers, and B. M. W. Tsui, “SPECT dual-energy window comptoncorrection: Scatter multiplier required for quantification,” J. Nucl.Med. 31, 90-98 (1990).
24K. F. Koral, F. M. Swailem, N. H. Clinthome, W. L. Rogers, and B.M. W. Tsui, “Dual-window compton scatter correction in phantoms:errors and multiplier dependence on energy,” J. Nucl. Med. 31, 798-799 (abst.) (1990).
25A. J. Green, S. E. Dewhurst, R. H. Begent, K. D. Bagshawe. and S. J.Riggs, “Accurate quantification of 131I distribution by gamma cameraimaging,” Eur. J. Nucl. Med. 16, 361-365 (1990).
26L. T. Chang, “A method for attenuation correction in radionuclidecomputed tomography,” IEEE Trans. Nucl. Sci. NS-25, 638-643(1978).
27O. Israel, G. Iosilevsky, D. Front, L. Bettman, A. Frenkel, S. Ish-Shalom, M. Steiner, M. Ben-Harush, and G. M. Kolodny, “SPECTquantitation of iodine-131 concentration in phantoms and human tu-mors,” J. Nucl. Med. 31, 1945-1949 (1990).
28G. L. DeNardo, D. J. Macey, S. J. Denardo, C. G. Zhang, and T. R.Custer, “Quantitative SPECT of uptake of monoclonal antibodies,”Semin. Nucl. Med. 19, 22-32 (1989).
29S. J. Cullom, L. P. Clarke, B. C. Penney, M. A. King, A. V. Heal, J. A.Madden, and M. L. Silbiger, “Importance of collimator and restorationfilter for quantitative imaging with “‘I-labeled antibody (HMFG),” J.Nucl. Med. 30, 876 (abst.) (1989).
30D. R. Gilland, R. J. Jaszczak, K. L. Greer, and R. E. Coleman, “Quan-titative SPECT reconstruction of I-123 data,” J. Nucl. Med. 32, 527-533 (1991).
31D. R Gilland, R. J. Jaszczak, T. C. Turkington, K. L. Greer, and R.E. Coleman. “Quantitative SPECT imaging with In-111.” IEEE Trans.Nucl. Sci. 32, 761-766 (1991).
32E. Tanaka, H. Toyoma, and H. Muriyama, “Convolutional image re-construction for quantitative single-photon emission computed tomog-raphy,” Phys. Med. Biol. 29, 1489-1500 (1984).
33S. Bellini, M. Piacentini, and C. Cafforio, “Compensation of tissueabsorption in emission tomography,” IEEE Trans. ASSP 27, 213-218(1979).
34W. G Hawkins, P. K. Leichner, and N. C. Yang, “The circular har-monic transform for SPECT and boundary conditions on the fouriertransform of the sinogram,” IEEE Trans. Med. Imag. 7, 135-148(1988).
35S. J. Glick, W. G. Hawkins, M. A. King, B. C. Penney, E. J. Soares,and C. L. Byrne, “The effect of intrinsic attenuation correction meth-
ods on the stationarity of the 3-D modulation transfer function ofSPECT,” Med. Phys. 19, 1105-1112 (1992).
36W. G. Hawkins, N.-C. Yang, and P. K. Leichner, “Validation of thecircular harmonic transform (CHT) algorithm for quantitativeSPECT,” J. Nucl. Med. 32, 141-150 (1991).
37P. K. Leichner. H. M. Vriesendorp, W. G. Hawkins, S. M. Quadri,N.-C. Yang, R. L. Stinson, D. M. Loundenslager, T. L. Frenkel, X.
Chen, and J. L. Klein, “Quantitative SPECT for In-111 antibodies inthe livers of beagle dogs,” J. Nucl. Med. 32, 1442-1444 (1991).
3 8P. K. Leichner, W. G. Hawkins, and N.-C. Yang, “QuantitativeSPECT in radioimmunotherapy,” Antib. Immunoconj. and Radiop-harm. 4, 25 (abst.) (1991).
39K. Lange and R. Carson, “EM reconstruction algorithms for emissionand transmission tomography,” J. Comput. Assist. Tomogr. 8, 306-316(1984).
40L. A. Schepp, and Y. Vardi, “Maximum likelihood reconstruction foremission tomography,” IEEE Trans. Med. Imag. MI-l, 113-122(1982).
41A. J. Green, R. H. J. Begent, and K. D. Bagshawe, “Maximum likeli-hood reconstruction incorporating line spread function data,” (abst.)Eur. J. Nucl. Med. 14, 226 (1988).
42B. C. Penny, N. Rajechan, C. L. Bume, and M. A. King, “Maximumlikelihood SPECT reconstruction: Use of a 2D blurring model,” J.Nuc. Med. 32, 936 (1991).
43A. J. Green, D. E. Lane, R. H. J. Begent, and K. D. Bagshawe, “A newprojector/backprojector for improved image reconstruction with highenergy gamma emitters,” (abst.) Antib. Immunoconjug. and Radiop-harm. 4, 58 (1991).
44Z. Liang, R. J. Jaszczak, and K. Greer, “On Bayesian image recon-structions from projections: Uniform and nonuniform a priori sourceinformation.” IEEE Trans. Med. Imag. 8, 227-235 (1989).
45Z. Liang, R. Jaszczak, R. Coleman, and V. Johnson, “Simultaneousreconstruction, segmentation, and edge enhancement of relativelypiecewise continuous images with intensity-level information,” Med.Phys. 18, 394-401 (1991).
46L. G. Strauss, J. H. Clorius, F. Frank, and G. Van Kaick, “Single-photon emission-computerized tomography (SPECT) for estimates ofliver and spleen volume,” J. Nucl. Med. 25, 81-85 (1984).
47W. N. Tauxe, F. Soussaline, and A. Todd-Pokropek, “Determinationof organ volume by single-photon emission computed tomography,” J.Nucl. Med. 23, 984-987 (1982).
4 8R. J. Jaszczak, F. R. Whitehead, C. B. Lim, and R. E. Coleman,“Lesion detection with single-photon emission computed tomogra-phy,” J. Nucl. Med. 23, 97-102 (1982).
49D. Osborne, R. Jaszczak, R. E. Coleman, K. Greer, and M. Lischko,“In-vivo regional quantitation of intrathoracic Tc-99m using SPECT:Concise communication,” J. Nucl. Med. 23, 446-450 (1982).
50B. Soderberg, M. Dahlborn, and J. Virgin, “Determination of organvolume by single-photon emission tomography,” J. Nucl. Med. (letter)24, 1197 (1983).
51L T. Kircos, J. E. Carey, and J. W. Keyes, “Quantitative organ visu-alization using SPECT,” J. Nucl. Med. 28, 334-341 (1987).
52K. H. Lee, H. T. H. Liu, D. C. P. Chen, M. E. Siegel, and S. Ballard,“Volume calculation by means of SPECT: Analysis of imaging acqui-sition and processing factors,” Radiology 167, 259-262 ( 1988).
53G. T. Gullberg and T. F. Budinger, “Three-dimensional reconstructionin nuclear medicine emission imaging,” IEEE Trans. Nucl. Sci. NS-21,2-20 (1974).
54A. M. Cormack, “Reconstruction of densities from their projectionswith applications in radiological physics,” Phys. Med. Biol. 18, 195-207 (1973).
55R. J. Jaszczak, L. T. Chang, and P. H. Murphy, “Single-photon emis-sion computed tomography using multi-slice fan beam collimators,”IEEE Trans. Nucl. Sci. NS-26, 610-619 (1979).
56B. M. W. Tsui, G. T. Gullberg, and E. R. Edgarton, “Design andclinical utility of a fan-beam collimator for SPECT imaging of thehead,” J. Nucl. Med. 27, 810-819 (1986).
57R. J. Jaszczak, C. E. Floyd, S. H. Mangles, K. L. Greer, and R. E.Coleman, “Cone beam collimation for single-photon emission com-puted tomography: Analysis, simulation, and image reconstruction us-ing filtered backprojection,” Med. Phys. 13, 484-489 (1987).
58E. G. Hawman and J. Hsieh, “An astigmatic collimator for high-sensitivity SPECT of the brain,” J. Nucl. Med. 27, 930 (1986).
59N. Nohara, H. Murayama, and E. Tanaka, “Single-photon emission
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

577 Leichner et al.: Imaging techniques and treatment planning In radioimmunotherapy 577
tomography with increased sampling density at central region field-of-view,” IEEE Trans. Nucl. Sci. NS-34, 359-363 (1987).
60R. J. Jaszczak, L. T. Chang, N. A. Stein, and F. E. Moore, “Whole-body single-photon emission computed tomograph using dual, large-field-of-view scintillation cameras,” Phys. Med. Biol. 24, 1123-I 143(1979).
61C. B. Lim, L. T. Chang, and R. J. Jaszczak, “Performance analysis ofthree camera configurations for single-photon emission computed to-mography,” IEEE Trans. Nucl. Sci. NS-27. 559-568 (1980).
62S. Genna and A. Smith, “The development of ASPECT, an annularsingle-crystal brain camera for high-efficiency SPECT,” IEEE Trans.Nucl. Sci. NS-35, 654-658 (1988).
63S. C Moore, M. D. Doherty, R. E. Zimmerman, and B. L. Homan,“Improved performance from modifications to the multidetectorSPECT brain scanner,” J. Nucl. Med. 25, 688-691 (1984).
64E. M. Stokley, E. Sveinsdottir, N. A. Lassen, and P. Rommer, “Asingle-photon dynamic computer-assisted tomograph (DCAT) for im-aging brain function in multiple cross sections,” J. Comput. Assist.Tomogr. 4, 230-240 (1980).
65W. L Rogers, N. H. Clinthome, and J. Stamos, “Performance evalu-ation of SPRINT, a single-photon ring tomograph for brain imaging,”J. Nucl. Med. 25, 1013-1018 (1984).
66G. L. Brownell, J. A. Correia, and R. G. Zamenhof, “Positron instru-mentation,” in Recent Advances in Nuclear Medicine, edited by J. H.Lawrence and T. F. Budinger (Grune and Stratton, New York, NY,1978).
67M. M. Ter-Pogossian, “Positron emission tomograph instrumenta-tion,” in Positron Emission Tomography (Alan R. Liss, Inc., NewYork, NY, 1985).
68M. E Phelps, E. J. Hoffman, N. A. Mullani, and M. M. Ter-Pogossian,“Application of annihilation coincidence detection to transaxial recon-struction tomography,” J. Nucl. Med. 16, 210-224 (1975).
69M. E. Phelps, E. J. Hoffman, S. C. Huang, and D. E. Kuhl, “ECAT: Anew computerized tomographic imaging system for positron-emittingradiopharmaceuticals,” J. Nucl. Med. 19, 635-647 (1978).
70L. G. Strauss and P. S. Conti, “The application of PET in clinicaloncology,” J. Nucl. Med. 32, 623-648 ( 1991).
71S. M Larson, K. S. Pentlow, N. C. Volkow, A. P. Wolf, R. D. Finn, M.C. Graham, G. D. Resta, F. Augenson, O. Mawlawi, B. Bendriem, S.D. J. Yeh, G. J. Wang, L. Birch, R. M. Lambrecht, J. Kalaigian, M.LaQuaglia, B. Kushner, and N-K. V. Cheung, “PET scanning of124I-3F8 as a novel method of tumor dosimetry during treatment plan-ning for radioimmunotherapy in a child with neuroblastoma,” Antib.,Immunoconj. Radiopharm. 4, 34 (1991).
72K. S. Pentlow, M C. Graham, R. M. Lambrecht, N-K. V. Cheung, andS. M. Larson, “Quantitative imaging of I-124 using positron emissiontomography with applications to radioimmunodiagnosis and radioim-munotherapy,” Med. Phys. 18, 357-366 (1991).
73D. C. Hemmy, D. J. David, and G. T. Herman, “Three-dimensionalreconstruction of craniofacial deformity using computed tomography,”Neurosurgery 13, 534-541 (1983).
74G. T. Herman, W. F. Vose, and W. B. Gefter, “Stereoscopic computedthree-dimensional surface displays,” Radiographics 5, 825-852 (1985).
75S. M. Goldwasser, R. A. Reynolds, and T. Bapty, “Physicians workstation with real-time performance,” Comput. Graphics Applic.5,44-57 (1985).
76D. Jackel, “The graphics PARCUM system: A 3D memory-basedcomputer architecture for processing and display of solid objects,”Comput. Graphics Forum 4, 21-32 (1985).
77R. Lenz, P. E. Danielsson, S. Cronstroem, and B. Gudmundson, “In-teractive display of 3D medical objects, ” in 3D Image Segmentation inMedicine, edited by K. H. Hoehne (Springer Verlag, Berlin, 1986).
78K. H Hoehne, R. L. Delapaz, R. Bernstein, and R. C. Taylor, “Com-bined surface display and reformating for the three-dimensional anal-ysis of tomographic data,” Invest. Radiol. 22, 658-664 ( 1987).
79L. R. Schad, R. Boesecke, W. Schlegel, G. H. Hartmann, V. Sturm, L.G. Strauss, and W. J. Lorenz, “Three-dimensional image correlation ofCT, MR. and PET studies in radiotherapy treatment planning of braintumors,” J. Comput. Assist. Tomogr. 11, 948-954 (1987).
80M.. W. Vannier and D. E. Gayou, “Automated registration of multi-modality images,” Radiology 169, 860-861 (1988).
81C. A. Pelizzari, G. T. Y. Chen, D. R. Spelbring, R. R. Weichselbaum,and C-T Chen, “Accurate threedimensional registration of CT, PET,and/or MR images of the brain,” J. Comput. Assist. Tomogr. 13,20-26 (1989).
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
82D. N. Levin. X. Hu, and K. K. Tan, “The brain: integrated three-dimensional display of MR and PET images,” Radiology 172, 783-789(1989).
83E. L. Kramer, M. E. Noz, J. J. Samger, A. J. Megibow, and G. Q.Maquire, “CT-SPECT fusion to correlate radiolabeled monoclonal an-tibody uptake with abdominal CT findings,” Radiology 172, 861-865(1989).
8 4K. F. Koral, R. K. Ten Haken, D. L. McShan. M. L. Kessler, S.Buchbinder, F. M. Swailem, I. R. Francis, M. S. Kaminski, and P. L.Wahl, “Superimposition of SPECT and CT images and transfer of ROIfor quantitation,” (abst.) J. Nucl. Med. 31, 872 (1990).
85P. K. Leichner, J. L. Klein, S. S. Siegelman, D. S. Ettinger, and S. E.Order, “Dosimetry of “‘I-labeled antiferritin in hepatoma: Specific ac-tivities in the tumor and liver,” Cancer Treat. Rep 67, 647-658 (1983).
86P. K. Leichner, N. C. Yang, T. L. Frenkel, D. M. Loudenslager, W. G.Hawkins, J. L. Klein, and S. E. Order, “Dosimetry and treatmentplanning for 90Y-labeled polyclonal antiferritin in hepatoma,” Int. J.Radiat. Oncol. Biol. Phys. 14, 1033-1042 (1988).
87D. S. Ettinger, S. E. Order, M. D. Wharam, M. K. Parker, J. L. Klein,and P. K. Leichner, “Phase I-II study of isotopic immunoglobulintherapy for primary liver cancer,” Cancer Treat. Rep. 6, 289-297(1982).
88R. F. Meredith, M. B. Khazaeli, T. Liu, G. Plott, R. H. Wheeler, C.Russell, D. Colcher, J. Schlom, D. Shochat, and A. F. LoBuglio, “Dosefractionation of radiolabeled antibodies in patients with metastatic co-lon cancer,” J. Nucl. Med. 33, 1648-1653 (1992).
89O. W. Press, J. F. Eary, C. C. Badger, P. J. Martin, F. R. Applebaum,R. Levy, R. Miller, S. Brown, W. B. Nelp, K. A. Krohn, D. Fisher, K.DeSantes, B. Porter, P. Kidd, E. D. Thomas, and I. D. Bernstein,“Treatment of refractory non-Hodgkin’s lymphoma with radiolabeledMB-1 (anti-CD37) antibody,” J. Clin. Oncol. 7, 1027-1038 (1989).
90S. E. Order, J. L. Klein, P. K. Leichner, J. Frinke, C. Lollo, and D. J.Carlo, “90Y antiferritin-a new therapeutic radiolabeled antibody,” Int.J. Radiat. Oncol. Biol. Phys. 12, 277-281 (1986).
91H. M. Vriesendorp, J. M. Herpst, M. A. Germack, J. L. Klein, P. K.Leichner, D. M. Loudenslager, and S. E. Order, “Phase I-II studies ofyttrium-labeled antiferritin treatment for endstage Hodgkin’s disease,including RTOG 87-01,” J. Clin. Oncol. 9, 918-928 (1991).
92G. L. Denardo, A. Raventos, H. H. Hines, P. O. Scheibe, D. J. Macey,M. T. Hays, and S. J. DeNardo, “Requirements for a treatment plan-ning system for radioimmunotherapy,” Int. J. Radiat. Oncol. Biol.Phys. 11, 335-348 (1985).
93D. J. Macey, G. L. DeNardo, and S. J. DeNardo, “A treatment plan-ning program for radioimmunotherapy,” in Frontiers of RadiationTherapy and Oncology, edited by J. M. Vaeth and J. M. Meyer (KargerVerlag, Basel, Switzerland, 1990), Vol. 24, pp. 109-120.
94G. Sgouros, G. Barest, J. Tekkumthala, C. Chui, R. Mohan, R. Bigler,and P. B. Zanzonico, “Treatment planning for internal radionuclidetherapy: Three-dimensional dosimetry for nonuniformly distributed ra-dionuclides,” J. Nucl. Med. 31, 1884-1891 (1990).
95J A. Siegel, “Quantitative measurements of activity in bone marrow,”Antibod. Immunoconj. Radiopharm. 3, 263-264 (1990).
96T. E. Hui, D. R. Fisher, O. W. Press, J. F. Eary, J. N. Weinstein, C. C.Badger, and I. D. Bernstein, “Localized beta dosimetry of 131I-labeledantibodies in follicular Lymphoma,” Med. Phys. 19, 97-104 (1992).
97T. K. Johnson, “MABDOS: A generalized program for internal radi-onuclide dosimetry,” Comput. Math. Prog. Biomed. 27, 159-167(1988).
98T. G. Stinchcomb, J. S. Durham, and D. R. Fisher, “Obtaining Svalues for rectangular-solid tumors inside rectangular-solid host or-gans,” Med. Phys. 18, 555-558 (1991).
99M.. J. Berger, “Energy deposition in water by photons from point iso-tropic sources,” MIRD Pamphlet No. 2, J. Nucl. Med. 9, Suppl. 1,15-25 (1968).
100M. J. Berger, “Distribution of absorbed dose. around point sources ofelectrons and beta particles in water and other media,” MIRD Pam-phlet No. 7, J. Nucl. Med. 12, Suppl. 5, l-23 (1971).
101E. E. Watson, M. Stabin, and W. E. Bolch, Documentation Package forMIRDOSE, version 2 (Oak Ridge Associated Universities, Oak Ridge,TN, 1988).
102L. P. Clarke, S. J. Cullom, R. Shaw, C. Reece, B. C. Penney, M. A.King, and M. Silbiger, “Bremsstrahlung imaging using the gammacamera: Factors affecting attenuation,” J. Nucl. Med. 33, 161-166(1992).


Radioimmunotherapy dose estimation in patients with B-cell lymphomaJ. A. SiegelCooper Hospital/University Medical Center, Camden, New Jersey 08103
D. M. GoldenbergThe Garden State Cancer Center at the Center for Molecular Medicine and Immunology, Newark,New Jersey 07103
C. C. BadgerThe Fred Hutchinson Cancer Research Center, Seattle, Washington 98104
(Received 18 March 1992; accepted for publication 28 October 1992)
Trials of radiolabeled antibody therapy in patients with B-cell lymphoma have been the mostpromising of any in radioimmunotherapy. Response rates of greater than 90% with manycomplete remissions have been reported by several groups using either low ( 185-370 MBq) orhigh (8.6-22.5 GBq) doses of I-13 l-labeled antibodies against B-cell antigens. Estimated dosesdelivered to normal organs have ranged from 0.2 to 2.2 mGy/MBq and have shown similarinterpatient variation in all series, despite differences in antibody specificity and dosimetrictechniques. Tumor doses have ranged from 0.5 to 5.4 mGy/MBq. There has been little corre-lation of tumor response with estimated tumor dose. Toxicity has been limited to bone marrowsuppression which has been greater with the higher amounts of I-131. An advantage for aparticular antibody specificity or for high dose compared to multiple low doses has yet to bedemonstrated.
Key words: lymphoma, radioimmunotherapy, dosimetry
1. INTRODUCTION
Although long-term survival is in the 40%-50% range forpatients with high grade lymphomas who have receivedaggressive third generation chemotherapy regimens, pa-tients who relapse following initial therapy and those withlow grade lymphomas are incurable with standardchemotherapy.’ Because the non-Hodgkin’s lymphomasare relatively radiosensitive, they are particularly attractivetargets for treatment with radiolabeled antibodies. In pa-tients with low grade lymphomas, remission but not curecan occur following doses of 100-250 cGy of total bodyirradiation.’ In patients with advanced disease, completeremission and long term survival can be achieved, at theexpense of substantial toxicity and cost, in up to 40% ofpatients following 10-1575 cGy of total body irradiationand chemotherapy in combination with bone marrowtransplantation (BMT).3 Thus a modest increase in radi-ation dose delivered to tumor, relative to normal tissues,could potentially result in improving long term survival inpatients with low grade lymphomas without the need forbone marrow transplantation. Similarly, in patients withadvanced lymphoma, radiolabeled antibodies used in con-junction with bone marrow support have the potential toincrease cure rates.
An additional advantage for the treatment of lymphomawith radiolabeled antibodies is the observation that unla-beled antibodies can have significant antitumor effects. Un-modified antibodies can cure experimental animals withlymphoma 4 - 6 and can induce remiss ion in t rea tedpatients.7-11 Although frequent, these responses have usu-ally been transient with the exception of a few patientstreated with anti-idiotype antibodies. The causes of the
limited effect of unmodified antibody include antigenicmodulation, the emergence of antigen negative variants,and the requirement for a host effector system. 6,12-14 Radi-ation delivered by radiolabeled antibodies can overcomethese limitations of unmodified antibodies while the intrin-sic antitumor activity of the antibody is maintained, poten-tially resulting in a synergistic antitumor effect.
II. THERAPY OF LYMPHOMA WITHRADIOLABELED ANTIBODIES
Radiolabeled antibodies have been demonstrated tohave significant antitumor effects both in experimental an-imals and in patients with lymphoma. Cure of mouse lym-phoma using either radioiodinated polyclonal or mono-clonal antibodies has been reported.15,16 Response rates inclinical trials in patients with lymphoma are the most en-couraging of any radioimmunotherapy trials. High dose(8.6-22.5 GBq) I-131-labeled antibodies against the CD37or CD20 antigens in combination with bone marrow sup-port has resulted in responses in 5/5 patients with 4 com-plete responses.17,18 Complete and partial responses to bothY-90 and I-131-labeled anti-idiotype antibodies have alsobeen observed.19,20 The use of high dose therapy is notrequired for response, since tumor regression has occurredin patients receiving 185-370 MBq of I-131-labeled Lym-1,LL2, MBl, and 1F5 antibodies.21-24 Because lymphomascan respond to infusion of unlabeled antibody, the re-sponses seen with small, as well as large, amounts of radi-onuclide may be due to deposited radiation, antitumor ef-fects of the antibody itself, or a combination of effects.
579 Med. Phys. 20 (2), Pt. 2, Mar/Apr 1993 0094-2405/93/0205794$01.20 © 1993 Am. Assoc. Phys. Med. 579
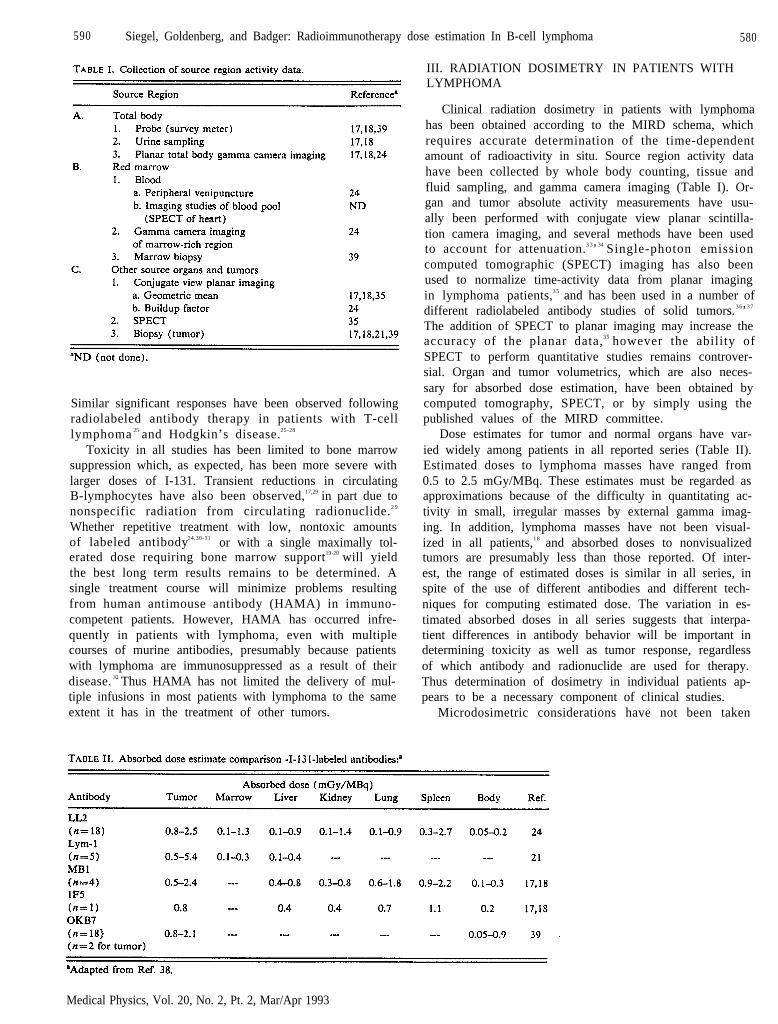
590 Siegel, Goldenberg, and Badger: Radioimmunotherapy dose estimation In B-cell lymphoma 580
Similar significant responses have been observed followingradiolabeled antibody therapy in patients with T-celllymphoma 25 and Hodgkin’s disease.25-28
Toxicity in all studies has been limited to bone marrowsuppression which, as expected, has been more severe withlarger doses of I-131. Transient reductions in circulatingB-lymphocytes have also been observed,17,29 in part due tononspecific radiation from circulating radionuclide.2 9
Whether repetitive treatment with low, nontoxic amountsof labeled antibody24,30-31 or with a single maximally tol-erated dose requiring bone marrow support19-20 will yieldthe best long term results remains to be determined. Asingle treatment course will minimize problems resultingfrom human antimouse antibody (HAMA) in immuno-competent patients. However, HAMA has occurred infre-quently in patients with lymphoma, even with multiplecourses of murine antibodies, presumably because patientswith lymphoma are immunosuppressed as a result of theirdisease. 32 Thus HAMA has not limited the delivery of mul-tiple infusions in most patients with lymphoma to the sameextent it has in the treatment of other tumors.
III. RADIATION DOSIMETRY IN PATIENTS WITHLYMPHOMA
Clinical radiation dosimetry in patients with lymphomahas been obtained according to the MIRD schema, whichrequires accurate determination of the time-dependentamount of radioactivity in situ. Source region activity datahave been collected by whole body counting, tissue andfluid sampling, and gamma camera imaging (Table I). Or-gan and tumor absolute activity measurements have usu-ally been performed with conjugate view planar scintilla-tion camera imaging, and several methods have been usedto account for attenuation.3 3’34 Single-photon emissioncomputed tomographic (SPECT) imaging has also beenused to normalize time-activity data from planar imagingin lymphoma patients,3 5 and has been used in a number ofdifferent radiolabeled antibody studies of solid tumors.3 6’3 7
The addition of SPECT to planar imaging may increase theaccuracy of the planar data,35 however the ability ofSPECT to perform quantitative studies remains controver-sial. Organ and tumor volumetrics, which are also neces-sary for absorbed dose estimation, have been obtained bycomputed tomography, SPECT, or by simply using thepublished values of the MIRD committee.
Dose estimates for tumor and normal organs have var-ied widely among patients in all reported series (Table II).Estimated doses to lymphoma masses have ranged from0.5 to 2.5 mGy/MBq. These estimates must be regarded asapproximations because of the difficulty in quantitating ac-tivity in small, irregular masses by external gamma imag-ing. In addition, lymphoma masses have not been visual-ized in all patients,1 8 and absorbed doses to nonvisualizedtumors are presumably less than those reported. Of inter-est, the range of estimated doses is similar in all series, inspite of the use of different antibodies and different tech-niques for computing estimated dose. The variation in es-timated absorbed doses in all series suggests that interpa-tient differences in antibody behavior will be important indetermining toxicity as well as tumor response, regardlessof which antibody and radionuclide are used for therapy.Thus determination of dosimetry in individual patients ap-pears to be a necessary component of clinical studies.
Microdosimetric considerations have not been taken
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

5 8 1 Siegel, Goldenberg, and Badger: Radioimmunotherapy dose estimation In B-cell lymphoma 581
into account in clinical trials of the treatment of lym-phoma. However, nonuniformity of antibody depositioncan result in substantial variation in radiation dose withinlymphomatous masses. In patients with follicular lym-phoma, preferential anti-B-cell antibody binding to cells inmalignant follicles resulted in estimated absorbed doses tofollicles (30% of tissue) that were up to twofold higherthan the mean dose, while interfollicular areas (70% oftissue) received up to twofold less than the mean. 4 0
Whether such variation is of clinical significance is un-known.
Further uncertainty in tumor and marrow radiationdoses following treatment of patients with lymphoma re-sults from the fact that tumor and hematopoietic responsesare seen as early as 24 h after infusion of labeledantibody.” In experimental animals, high dose radiationfrom either external beam or from radiolabeled antibodiesthemselves can alter subsequent uptake of radiolabeledantibody. 4 1 , 4 2 Similar changes in antibody uptake, andtherefore dose to tumor and marrow, may occur in patientsfollowing radiolabeled antibody therapy. However, directdetermination of estimated absorbed doses, and the possi-bility that these differ from doses extrapolated from tracelabeled antibody, has been limited by the difficulty in im-aging large amounts of activity. 4 3
IV. CONCLUSIONS
In summary, significant responses have been observed inpatients with lymphoma treated with several radiolabeledantibodies. Current dosimetric techniques appear to be ad-equate to conduct phase I-II trials. In trials to date, adefinite dose-response relationship has not been shown, al-though complete response is more frequent in patients re-ceiving large doses of radiolabeled antibody requiring bonemarrow support. Because of the rapid response to radia-tion, direct determination of radiation doses delivered totumor by therapeutic infusions will be particularly impor-tant in defining dose-response relationships in patients withlymphoma. The optimal antibody specificity and radionu-clide for treatment of these patients, whether microdosim-etric considerations are of importance, and whether dosesrequiring bone marrow transplantation will be needed forcure remain to be determined.
ACKNOWLEDGMENT
This work was supported in part by USPHS Grants CA39841 and CA44991 from the NIH.
1V. T. DeVita, E. S. Jaffe, P. Mauch, and D. L. Longo, “Lymphocyticlymphomas” in Cancer Principals and Practice of Oncology, edited byV. T. DeVita, S. Hellman, and S. A. Rosenberg (J. B. Lippincott.Philadelphia, PA 1989), 3rd cd., pp. 1741-1798.
2S. C. Carabell, J. T. Chaffey, D. S. Rosenthal, W. C. Moloney, and S.Hellman, “Results of total body irradiation in the treatment of ad-vanced non-Hodgkin’s lymphomas,” Cancer 43, 994-1000 ( 1979).
3F. Appelbaum, K. Sullivan, C. D. Buckner, R. A. Clift, H. J. Deeg, A.Fefer, R. Hill, J. Mortimer, P. E. Neiman, J. E. Sanders, J. Singger, P.Stewart, R. Storb, and E. D. Thomas, “Treatment of malignant lym-phoma in 100 patients with chemotherapy, total body irradiation andmarrow transplantation,” J. Clin. Oncol. 5, 1340-1347 (1987).
4C. C. Badger, C. Anasetti. J. Davis, and I. D. Bernstein, “Treatment ofmalignancy with unmodified antibody.” Pathol. Immunopathol. 6,419-434 (1987).
5M. E. Kirch and U. Hammerling, “Immunotherapy of murine leuke-mias by monoclonal antibody. I. Effect of passively administered anti-body on growth of transplanted tumor cells,” J. Immunol. 127, 805-810 (1981).
6W. W. Young and S. I. Hakomori, “Therapy of mouse lymphoma withmonoclonal antibodies to glycolipid: Selection of low antigenic variantsin vivo,” Science 211, 487-489 (1981).
7O. W. Press, F. Appelbaum, J. A. Ledbetter, P. J. Martin, J. Zarling, P.Kidd, and E. D. Thomas, “Monoclonal antibody 1F5 (anti-CD20)serotherapy of human B-cell lymphomas,” Blood 69, 584-591 ( 1987).
8G. Hale, M. J. S. Dyer, M. R. Clark, J. M. Phillips, R. Marcus, L.Riechmann, G. Winter, and H. Waldmann, “Remission induction innon-Hodgkin’s lymphoma with a reshaped human monoclonal anti-body CAMPATH-1H,” Lancet 2, 1394-1399 (1988).
9M. J. S. Dyer, G. Hale, F. G. J. Hayhoe, and H. Waldman, “Effects ofCAMPATH-I antibodies in vivo in patients with lymphoid malignan-cies: Influence of antibody isotype,” Blood 73, 1431-1439 (1989).
10R. A. Miller, R. Maloney, R. Warnke, and R. Levy, “Treatment ofB-cell lymphoma with monoclonal anti-idiotype antibody,” N. Engl. J.Med. 306, 517-522 (1982).
11T. C. Meeker, J. Lowder, R. G. Maloney, R. A. Miller, K. Thielemans,R. Warnke, and R. Levy, “A clinical trial of anti-idiotype therapy forB-cell malignancy,” Blood 65, 1349-1363 (1985).
12H. S. Shin, M. Hayden, S. Langley, N. Kaliss, and M. R. Smith,“Antibody-mediated suppression of grafted lymphoma. III. Evaluationof the role of thymic function, non-thymus-derived lymphocytes, mac-rophages, platelets, and polymorphonuclear leukocytes in syngeneicand allogeneic hosts,” J. Immunol. 114, 1255-1263 (1975).
1 3R. J. Johnson, R. F. Siliciano, and H. S. Shin, “Suppression ofantibody-sensitized cells by macrophages: Insufficient supply or activa-tion of macrophages within large tumors,” J. Immunol. 122, 379-382(1979).
14T. C. Meeker, J. Lowder, M. Cleary, S. Stewart, R. Warnke, J. Sklar,and R. Levy, “Emergence of idiotype variants during treatment ofB-cell lymphoma with antiidiotypic antibodies,” N. Engl. J. Med. 312,1658-1665 (1985).
15T. Ghose and A. Guclu, “Cure of a mouse lymphoma with radio-iodinated antibody,” Eur. J. Cancer. 10, 787-792 (1974).
16C. C. Badger, K. A. Krohn, A. V. Peterson, H. Shulman, and I. D.Bernstein, “Experimental radiotherapy of murine lymphoma with131I-labeled anti-Thy 1.1 monoclonal antibody,” Cancer Res. 45,1536-1544 (1985).
17O. W. Press, J. F. Eary, C. C Badger, P. J. Martin, F. R. Appelbaum,R. Levy, R. Miller, S. Brown, W. B. Nelp, K. A. Krohn, D. Fisher, K.DeSantes, B. Porter, P. Kidd, E. D. Thomas, and I. D. Bernstein,“Treatment of refractory non-Hodgkin’s lymphoma with radiolabeledMB-l (anti-CD37) antibody,” J. Clin. Oncol. 7, 1027-1038 (1989).
18J. F. Eary, O. W. Press, C. C. Badger, L. D. Durack, K. Y. Richter, S.J. Addison, K. A. Krohn, D. R. Fisher, B. A. Porter, D. L. Williams,P. J. Martin, F. R. Appelbaum, R. Levy, S. L. Brown, R. A. Miller, W.B. Nelp, and I. D. Bernstein, “Imaging and treatment of B-cell lym-phoma,” J. Nucl. Med. 31, 1257-1268 (1990).
19B. A. Parker, A. B. Vassos, S. E. Halpern, R. A. Miller, H. Hupf, D.G. Amox, J. L. Simoni, R. J. Starr, M. R. Green, and I. Royston,“Radioimmunotherapy of human B-cell lymphoma with 9OY-conjugated antiidiotype monoclonal antibody,” Cancer Res. 50, 1022s-1028s (1990).
20C. C. Badger, J. F. Eary, S. Brown, O. Press, J. Davis, F. Appelbaum,W. Nelp, K. Krohn, R. Miller, R. Levy, and I. D. Bernstein, “Therapyof lymphoma with I-131-labeled anti-idiotype antibodies,” Proc. Am.Assoc. Cancer Res. 28, 388 (1987).
21S. J. DeNardo, D. L. DeNardo, L. F. O’Grady, N. B. Levy, S. L. Mills,D. J. Macey, J. P. McGahan, C. H. Miller, and A. L. Epstein, “Pilotstudies of radioimmunotherapy of B-cell lymphoma and leukemia us-ing I-131 Lym-1 monoclonal antibody,” Antib. Immunoconj. Radiop-harm. 1, 17-33 (1988).
22S. J. DeNardo, G. L. DeNardo, L. F. O’Grady, E. Hu. V. M. Sytsma,S. L. Mills, N. B. Levy, D. J. Macey, C. H. Miller, and A. L. Epstein.“Treatment of B-cell malignancies with I-131 Lym-I monoclonal an-tibodies,” Int. J. Cancer Suppl. 3, 96-101 (1988).
23M. S. Kaminski, L. Fig, K. Zasadny, K. Koral, I. Francis, R. Miller, R.L. Wahl, “Phase I evaluation of 131-I MB-1 antibody radioimmunc-
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

582 Siegel, Goldenberg, and Badger: Radioimmunotherapy dose estmation In B-cell lymphoma 582
therapy (RIT) of B-cell lymphoma,” Blood 76, 355a (1990).24D. M. Goldenberg, R. M. Horowitz, R. M. Sharkey, T. C. Hall, S.
Murthy, H. Goldenberg, R. E. Lee, R. Stein, J. A. Siegel, D. O. Izon,K. Burger, L. C. Swayne, E. Belisle, H. J. Hansen, and C. M. Pinsky,“Targeting, dosimetry, and radioimmunotherapy of B-cell lymphomaswith iodine-131-labeled LL2 monoclonal antibody,” J. Clin. Oncol. 9,548-564 (1991).
25S. T. Rosen, A. M. Zimmer, R. Goldman-Leikin, L. I. Gorodon, J. M.Kazikiew, E. H. Kaplan. D. Variakojis, R. J. Marder, M. S. Dykewicz,A. Pierfies, E. A. Silverstein, H. H. Roenigk, and S. M. Spies, “Radio-immunodetection and radioimmunotherapy of cutaneous T cell lym-phomas using a 131I-labeled monoclonal antibody: An Illinois CancerCouncil study,” J. Clin. Oncol. 5, 562-573 ( 1987).
26R. E. Lenhard, S. E. Order, J. J. Spunberg, S. O. Asbell, and A. Leibel,“Isotopic immunoglobin: A new system therapy for advancedHodgkin’s disease,” J. Clin. Oncol. 3, 1296-1300 (1985).
27H. M. Vriesendorp, J. M. Herpst, P. K. Leichner, J. L. Klein, and S. E.Order, “Polyclonal 9 0yttrium labeled antiferritin for refractoryHodgkin’s disease,” Int. J. Radiat. Oncol. Biol. Phys. 17, 815-821(1989).
28H. M. Vriesendorp, S. M. Quadri, R. L. Stinson, O. C. Onyekwere, Y.Shao, J. L. Klein, P. K. Leichner, and J. R. Williams, “Selection ofreagents for human radioimmunotherapy,” Int. J. Radiat. Oncol. Biol.Phys. 22, 37-45 (1992).
29R. Stein, R. M. Sharkey, and D. M. Goldenberg, “Haematologicaleffects of radioimmunotherapy in cancer patients,” Br. J. Haematol. 80,69-76 ( 1992).
30S. J. DeNardo, D. L. DeNardo, L. F. O’Grady, N. B. Levy, G. P.Adams, and S. L. Mills, “Fractionated radioimmunotherapy of B-cellmalignancies with 1311-Lym-1,” Cancer Res. SO, 1014-1016 (1990).
31D. M. Goldenberg, R. M. Sharkey, S. Murthy, H. J. Hansen, and C. M.Pinsky, “Initial evaluation of repeated low-dose radioimmunotherapy(RAIT) using I-131-LL2 monoclonal antibody (MAb) in patientswith lymphoma,” J. Nucl. Med. 33, 863 ( 1992).
32S. B. Sutcliffe, Immunotherapy of the Lymphomas (CRC, Boca Raton,FL, 1985).
33J. F. Eary, F. R. Appelbaum, L. Durack, and P. Brown, “Preliminaryvalidation of the opposing view method for quantitative gamma cameraimaging,” Med. Phys. 16, 382-387 (1989).
34R. K. Wu and J. A. Siegel, “Absolute quantitation of radioactivity
using the buildup factor,” Med. Phys. 11, 189-192 (1984).35K. F. Koral. K. R. Zasadny, F. M. Swailem, S. F. Buchbinder. I. R.
Francis, M. S. Kaminski, and R. L. Wahl, “Importance of intra-therapy single-photon emission tomographic imaging in calculating tu-mor dosimetry for a lymphoma patient,” Eur. J. Nucl. Med. 18, 432-435 (1991).
36G. L. DeNardo, D. J. Macey, S. J. DeNardo, C. G. Zhang, and R.Custer, “Quantitative SPECT of uptake of monoclonal antibodies,”Semin. Nucl. Med. 19, 22-32 (1989).
37R. H. J. Begent, J. A. Ledermann, A. J. Green, K. D. Bagshawe, S. J.Riggs, F. Searle, P. A. Keep, T. Adam, R. G. Dale, and M. G. Glaser,“Antibody distribution and dosimetry in patients receiving radiola-beled antibody therapy for colorectal cancer,” Br. J. Cancer 60, 406412 (1989).
38J. A. Siegel, D. M. Goldenberg, R. M. Sharkey, T. C. Hall, S. Mm-thy,R. E. Lee, D. A. Pawlak, and L. C. Swaney, “Tumor and organ do-simetry for I-131-labeled LL2 (EPB-2) monoclonal antibody in pa-tients with B-cell lymphomas,” Antib. Immunoconj. Radiopharm. 4,649-654 (1991).
39D. A. Scheinberg, D. J. Strauss, S. D. Yeh, C. Divgi, P. Garin-Chesa,M. Graham, K. Pentlow, D. Coit, H. F. Oettgen, and L. J. Old, “Aphase I toxicity, pharmacology, and dosimetry trial of monoclonal an-tibody OKB7 in patients with non-Hodgkin’s lymphoma: Effects oftumor burden and antigen expression,” J. Clin. Oncol. 8, 792-803(1990).
40T. E. Hui, D. R. Fisher, O. W. Press, J. F. Eary, J. N. Weinstein, C. C.Badger, and I. D. Bernstein, “Localized beta dosimetry of 131I-labeledantibodies in follicular lymphoma,” Med. Phys. 9, 97-104 (1992).
4 1R. M. Macklis, W. D. Kaplan, J. L. Ferrara, B. M. Kinsey, A. I.Kassis, and S. J. Burakoff, “Biodistribution studies of anti-Thy 1.2 IgMimmunoconjugates: Implications for radioimmunotherapy,” Int. J. Ra-diat. Oncol. Biol. Phys. 15, 383-389 (1988).
42C. C. Badger, J. Davis, C. Nourigat, Z. M. Wu, T. E. Hui, D. R.Fisher, J. Shulman, F. R. Appelbaum, J. F. Eary, K. A. Krohn, D. C.Matthews, and I. D. Bernstein, “Biodistribution and dosimetry follow-ing infusion antibodies labeled with large amounts of 131I,” Cancer Res.51, 5921-5928 (1991).
43K. R. Pollard, A. N. Bite, J. F. Eary, L. D. Durack, and T. K. Lewel-len, “Imaging therapeutic doses of iodine-131 with a clinical gammacamera,” J. Nucl. Med. 32, 923 ( 1991).
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

Dosimetry of solid tumorsRuby F. MeredithDepartment of Radiation Oncology, University of Alabama, Comprehensive Cancer Center,Birmingham, Alabama 35233
Timothy K. JohnsonDepartment of Radiology. University of Colorado Health Sciences Center, Denver, Colorado
Gene PlottDepartment of Radiation Oncology, University of Alabama, Comprehensive Cancer Center,Birmingham, Alabama 35233
Daniel J. MaceyRadiation Physics, MD Anderson Cancer Center, Houston, Texas
Robert L. VessellaDepartment of Urology, University of Washington Medical Center, Seattle, Washington
Latresia A. WilsonDivision of Radiation Oncology, City of Hope Medical Center, Duarte, California
Hazel B. BreitzNuclear Medicine Section, Department of Radiology, Virginia Mason Medical Center,Seattle, Washington
Lawrence E. WilliamsDivision of Radiation Oncology, City of Hope Medical Center, Duarte, California
(Received 18 March 1992; accepted for publication 24 July 1992)
Dosimetry data arising from a decade of radioimmunotherapy are summarized along withtechniques utilized to arrive at the reported dose estimates. Generality of the MIRD method-ology allows it to serve as a vehicle for the calculation of solid tumor dosimetry although severallimitations exist. Nonstandard geometries of solid tumors will ultimately necessitate determina-tion of absorbed fractions for the individual tumors. Several approaches currently under inves-tigation are described. For reasons of practicality, solid tumor dosimetry estimates continue touse the assumption of homogeneous activity distribution in a source organ, accounting for eitherall radiation or only nonpenetrating radiation. As computation tools become available for in-corporating inhomogeneous cellular level data, the currently used “average dose” as an index oftumor sterilization will likely be replaced with a statistical distribution based on the number ofviable cells in the tumor volume. Estimates of a tumor control dose would be based upon a linearextension of dose coupled with a threshold dose for cell sterilization.
Key words: radioimmunotherapy, tumor dose, clinical dosimetry
I. INTRODUCTION
In the preceding decade, over 100 clinical trials have uti-lized radiolabeled antibodies against tumors.’ A variety oftumors have been treated including hepatoma, neuroblas-toma, melanoma, cancer of the ovary, breast, kidney, lung,colon, lymphoma, and other malignancies. Doses reportedhave varied widely. Some of the most recent trials reviewedby Langmuir report a tumor dose range from 2 Gy for ahepatoma patient to greater than 120 Gy fractionated de-livery for non-Hodgkins lymphoma. Dose variations arenoted among different tumor types, individual patientsgiven similar treatment for the same type of malignancyand even among multiple lesions of the same patient. Lym-phoma dosimetry has been separately reviewed by Siegeland Goldenberg.
The MIRD methodology4 serves as the framework formost solid tumor dosimetry calculations. Organ and tumorspecific radioactivity is quantitated, time-activity curvesare constructed and integrated, and cumulated activities
are multiplied by the absorbed dose constant and specificabsorbed fraction to yield estimated dose. Targeting of ra-dioactivity in a nonstandard volume positioned in a non-standard geometry, however, creates several problems dis-tinct from those encountered in normal organ dosimetry.Because published "S" tables make provision only for stan-dard organ systems as sources/targets of radiation, the fre-quently used MIRD Pamphlet No. 115 is not easily appliedto solid tumor dose estimates. For nonpenetrating radia-tion, the contribution to tumor dose may be computedassuming an absorbed fraction of unity. Determining theabsorbed fractions for penetrating radiation is not so sim-ple. MIRD Pamphlets No. 3 and No. 8 provide a partialsolution with tables of absorbed fractions for spherical andellipsoidal volumes that contain uniform distributions ofphoton emitters.6’7 Such tables allow the calculation ofdose to tumor from activity in the tumor, but fail to pro-vide estimates for other source organs that may contributeappreciably to tumor dose. The following deals with major
583 Med. Phys. 20 (2), Pt. 2, Mar/Apr 1993 0094-2405/93/020583-10$01.20 © 1993 Am. Assoc. Phys. Med. 583

584 Meredith et al.: Dosimetry of solid tumors 584
aspects of the MIRD formalism as applied to solid tumordosimetry, including calculation of dose per unit cumu-lated activity and limitations of current methodologies forestimating tumor dose. Therapeutic interventions and thetype of circulating protein that may impact tumor kineticsand dose are also discussed.
II. CLINICAL DOSE ESTIMATES
A summary of clinical dose estimates for administrationof radioimmunoconjugates is presented in Table 1.8-37 Themost outstanding feature of this compilation is the widevariation of doses even when the range of administeredactivity is taken into account. Doses have generally beencalculated by indirect quantitation since direct measure-ment of activity from biopsy specimens is uncommon andeven when available usually represents only a single timepoint during the several days of radiation delivery via ra-dioimmunoconjugates. Although most dose estimates todate have utilized the MIRD formalism with activity quan-titation by means of planar scintigraphy, the details forimplementing these methodologies varied substantially.Despite this, most of the variance in tumor dose undoubt-edly results from real differences in biological and physicalfactors. This is suggested by the fact that significant dosedifferences are reported for multiple lesions in the samepatient when identical calculation techniques, assump-tions, and the same time periods for quantitative measure-ments are used. (Table II compares the dose variation be-tween multiple lesions noted by four groups.)
Tumor dose estimates presented in Tables I and II werederived from intravenous or intra-arterial administrationof radioimmunoconjugates (with the exception of intrale-sional injection to 7 patients3 5). Radioimmunoconjugatetherapy by other routes of infusion including intrapleural,intrapericardial, intraperitoneal or intrathecal have gener-ally been used for tumor deposits too small to be quanti-tated by techniques currently used. Thus dose estimateshave not always been reported for those studies. Studies inthis category that have reported dosimetry aspects includeintrathecal 1 3 1I-antibody t r e a t m e n t o fmeningitis,3 8
neoplasticand intraperitoneal dosimetry using ther-
moluminescent dosimeters and biopsy quantitation in con-junction with gamma camera imaging methods.39 In someother studies, the choice of radionuclide precluded quanti-tative dosimetry for measurable tumors. For example, thegamma component of 125I emissions is not sufficiently en-ergetic to allow quantitation by gamma camera imaging.@Various substitute radionuclides have been used for pre-therapy imaging studies to determine localization.
No definite dose/response relationship has been estab-lished to date from the results of clinical trials. Overall, themost extensive patient experience and greatest success inclinical use of radioimmunotherapy of solid tumors hasbeen with the relatively radioresponsive lymphomas. Al-though responses vary considerably among lymphoma pa-tients, a dose/response relationship is suggested by the factthat some of the best response rates have resulted fromsuch marrow toxic levels of 1 3 1I-MB-l antibody that mar-row transplantation may be necessary for recovery from
radioimmunotherapy.’ The difficulty in determining adose/response relationship is compounded by multiple fac-tors. These include the variance of responsiveness amongmultiple lesions and between individual patients, the de-gree of dose heterogeneity within tumor masses at the cel-lular level and the limited dosimetry information reportedfrom most clinical trials.
Ill. CALCULATION OF TUMOR-ABSORBED DOSE
After time-activity curves for organ specific radioactiv-ity have been constructed and integrated as has been de-tailed by Leichner and Kwok41 the resulting cumulatedactivities must be multiplied by appropriate absorbed doseconstants and specific absorbed fractions. The degree ofsophistication applied to this portion of the problem varieswithin the medical physics community. Three generalmethods found or alluded to in the literature are outlinedbelow for dealing with the second portion of the tumordosimetry equation.
A. Method No. 1: Homogeneous distribution ofradioactivity throughout the tumor volume, onlynonpenetrating radiations contribute to tumord o s e
In this approach, the distribution of radioactivity isassumed to be uniform in the tumor and the range of theradiation emitted is less than the tumor dimensions. Theassumption of a homogeneous distribution of activitythroughout the tumor is a gross oversimplification at thecellular leve1.42,43 However, since noninvasive techniqueswith sufficient resolution to characterize the microscopicradioactivity distribution are not available, the assumptionof a uniform distribution is accepted as a first approxima-tion. This approach can be modified at a later time pendingpattern analysis of the nonuniform antibody deposition.
Two assumptions may be made about the deposition ofnonpenetrating radiation in the tumor: (1) all of the non-penetrating radiation is deposited within the tumor volume[φ (np) = 1], or (2) a fraction of the nonpenetrating radi-ation is deposited within the tumor [φ (np) < 1]. For smalltumors, the assumption of np = 1 would clearly be an over-estimation.
Because of the finite range of the beta radiation and theresultant escape of some particles, the edge of the tumorwill receive a lower dose than other locations within thelesion. If one assumes spherical tumors, a simple correctioncan be made using two geometrical corrections. 44 The cor-rections involve two factors which, when multiplied to-gether, give the average spherical lesion dose relative tothat calculated via assuming an infinitely large mediumcontaining the beta source.44 Using a 9 0Y source, the re-sultant calculations are summarized in Table III.
For example, if a 1.0-cm3 lesion were to be treated witha uniform deposition of 90Y, the actual average dose withinthat volume would only be 68% of that estimated usingstandard methods which neglect edge effects. For verysmall tumors, the correction factor is 0.36; i.e., only aboutone-third of the estimated dose would be, on the average,found in the smallest volume. Corrections are not as dra-
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
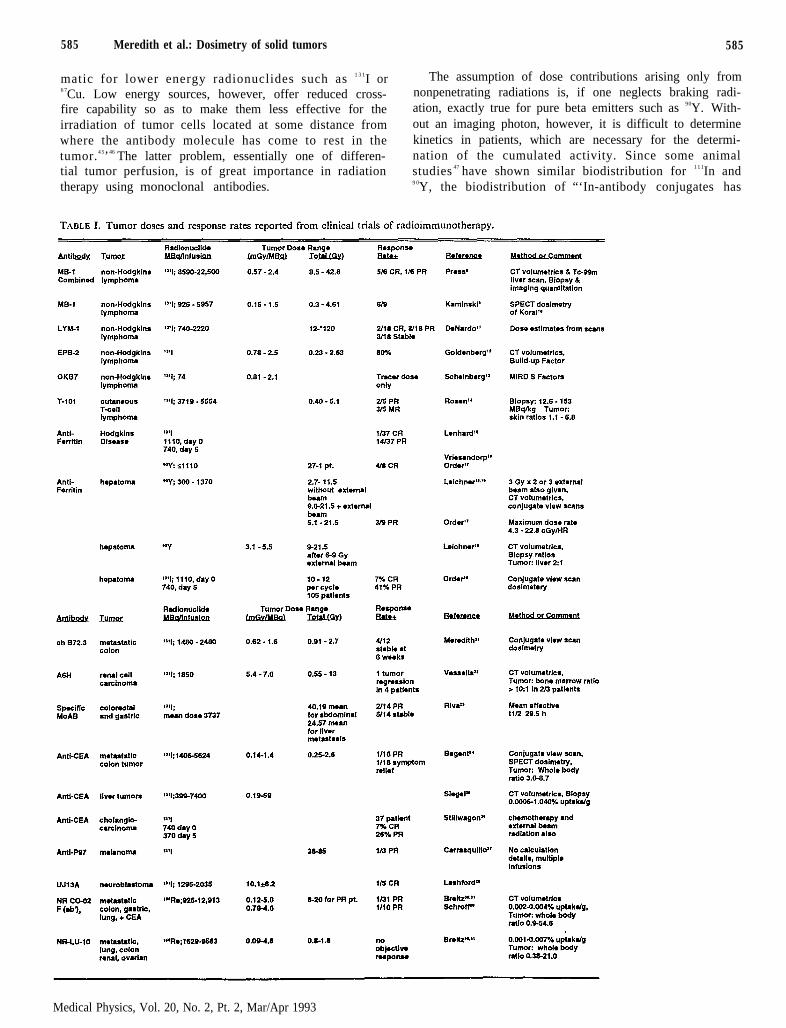
585 Meredith et al.: Dosimetry of solid tumors 585
matic for lower energy radionuclides such as 1 3 1I or The assumption of dose contributions arising only from6 7Cu. Low energy sources, however, offer reduced cross- nonpenetrating radiations is, if one neglects braking radi-fire capability so as to make them less effective for the ation, exactly true for pure beta emitters such as 90Y. With-irradiation of tumor cells located at some distance from out an imaging photon, however, it is difficult to determinewhere the antibody molecule has come to rest in the kinetics in patients, which are necessary for the determi-tumor.4 5’46 The latter problem, essentially one of differen- nation of the cumulated activity. Since some animaltial tumor perfusion, is of great importance in radiation studies 47 have shown similar biodistribution for 1 1 1In andtherapy using monoclonal antibodies. 9 0Y, the biodistribution of “‘In-antibody conjugates has
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
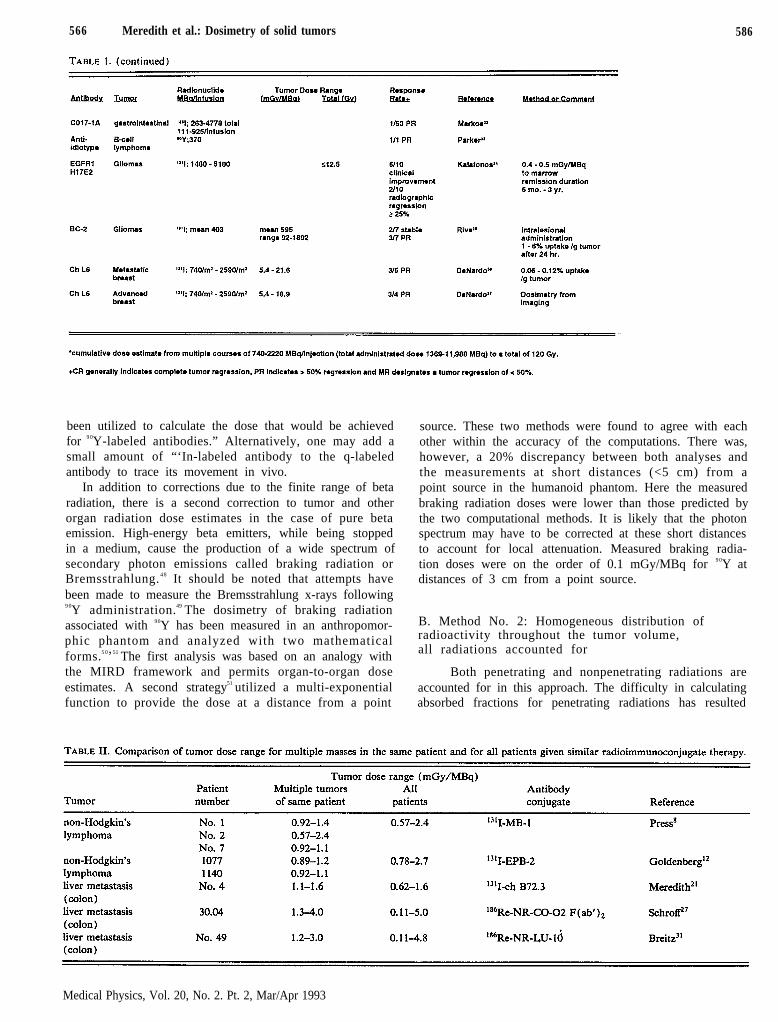
566 Meredith et al.: Dosimetry of solid tumors 586
been utilized to calculate the dose that would be achievedfor 9 0Y-labeled antibodies.” Alternatively, one may add asmall amount of “‘In-labeled antibody to the q-labeledantibody to trace its movement in vivo.
In addition to corrections due to the finite range of betaradiation, there is a second correction to tumor and otherorgan radiation dose estimates in the case of pure betaemission. High-energy beta emitters, while being stoppedin a medium, cause the production of a wide spectrum ofsecondary photon emissions called braking radiation orBremsstrahlung. 4 8 It should be noted that attempts havebeen made to measure the Bremsstrahlung x-rays following9 0Y administration.49 The dosimetry of braking radiationassociated with 90Y has been measured in an anthropomor-phic phantom and analyzed with two mathematicalforms.5 0’51 The first analysis was based on an analogy withthe MIRD framework and permits organ-to-organ doseestimates. A second strategy51 utilized a multi-exponentialfunction to provide the dose at a distance from a point
source. These two methods were found to agree with eachother within the accuracy of the computations. There was,however, a 20% discrepancy between both analyses andthe measurements at short distances (<5 cm) from apoint source in the humanoid phantom. Here the measuredbraking radiation doses were lower than those predicted bythe two computational methods. It is likely that the photonspectrum may have to be corrected at these short distancesto account for local attenuation. Measured braking radia-tion doses were on the order of 0.1 mGy/MBq for 9 0Y atdistances of 3 cm from a point source.
B. Method No. 2: Homogeneous distribution ofradioactivity throughout the tumor volume,all radiations accounted for
Both penetrating and nonpenetrating radiations areaccounted for in this approach. The difficulty in calculatingabsorbed fractions for penetrating radiations has resulted
Medical Physics, Vol. 20, No. 2. Pt. 2, Mar/Apr 1993
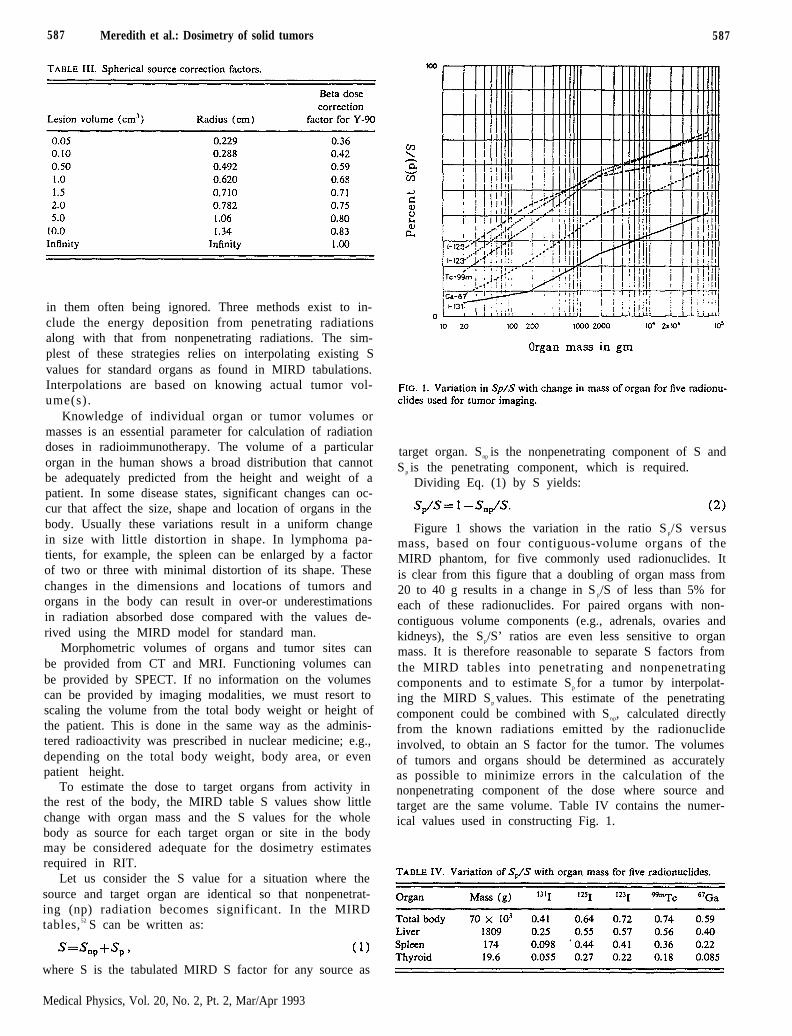
587 Meredith et al.: Dosimetry of solid tumors 587
in them often being ignored. Three methods exist to in-clude the energy deposition from penetrating radiationsalong with that from nonpenetrating radiations. The sim-plest of these strategies relies on interpolating existing Svalues for standard organs as found in MIRD tabulations.Interpolations are based on knowing actual tumor vol-ume(s).
Knowledge of individual organ or tumor volumes ormasses is an essential parameter for calculation of radiationdoses in radioimmunotherapy. The volume of a particularorgan in the human shows a broad distribution that cannotbe adequately predicted from the height and weight of apatient. In some disease states, significant changes can oc-cur that affect the size, shape and location of organs in thebody. Usually these variations result in a uniform changein size with little distortion in shape. In lymphoma pa-tients, for example, the spleen can be enlarged by a factorof two or three with minimal distortion of its shape. Thesechanges in the dimensions and locations of tumors andorgans in the body can result in over-or underestimationsin radiation absorbed dose compared with the values de-rived using the MIRD model for standard man.
Morphometric volumes of organs and tumor sites canbe provided from CT and MRI. Functioning volumes canbe provided by SPECT. If no information on the volumescan be provided by imaging modalities, we must resort toscaling the volume from the total body weight or height ofthe patient. This is done in the same way as the adminis-tered radioactivity was prescribed in nuclear medicine; e.g.,depending on the total body weight, body area, or evenpatient height.
To estimate the dose to target organs from activity inthe rest of the body, the MIRD table S values show littlechange with organ mass and the S values for the wholebody as source for each target organ or site in the bodymay be considered adequate for the dosimetry estimatesrequired in RIT.
Let us consider the S value for a situation where thesource and target organ are identical so that nonpenetrat-ing (np) radiation becomes significant. In the MIRDtables,52 S can be written as:
where S is the tabulated MIRD S factor for any source as
target organ. Snp is the nonpenetrating component of S andS p is the penetrating component, which is required.
Dividing Eq. (1) by S yields:
Figure 1 shows the variation in the ratio S p/S versusmass, based on four contiguous-volume organs of theMIRD phantom, for five commonly used radionuclides. Itis clear from this figure that a doubling of organ mass from20 to 40 g results in a change in S p/S of less than 5% foreach of these radionuclides. For paired organs with non-contiguous volume components (e.g., adrenals, ovaries andkidneys), the Sp/S’ ratios are even less sensitive to organmass. It is therefore reasonable to separate S factors fromthe MIRD tables into penetrating and nonpenetratingcomponents and to estimate Sp for a tumor by interpolat-ing the MIRD Sp values. This estimate of the penetratingcomponent could be combined with Snp, calculated directlyfrom the known radiations emitted by the radionuclideinvolved, to obtain an S factor for the tumor. The volumesof tumors and organs should be determined as accuratelyas possible to minimize errors in the calculation of thenonpenetrating component of the dose where source andtarget are the same volume. Table IV contains the numer-ical values used in constructing Fig. 1.
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

588 Meredith et al.: Dosimetry of solid tumors 588
A second dose estimation strategy, which is somewhatmore intensive computationally, uses convolution tech-niques. This is exemplified by the software program ofSgouros et al.53 Briefly, a dose-distance function (i.e., thepoint source kernel) is stored in a table. The two sources ofcode for generating point source kernels are the EGScode5 4,55 and the ETRAN code.56 Alternatively, a simple,empirical function can be solved to provide dose as a func-tion of distance.57 Lookup tables appropriate to a givenradionuclide’s decay spectrum are fashioned to account forall prominent radiations.
Each voxel of a source organ has an associated discreteamount of activity, the integral of which represents thatvoxel’s cumulated activity. For a defined target organvoxel, the distance separating it from each source organvoxel is calculated. This distance serves as an offset into thepoint source kernel lookup table, and the dose per unitcumulated activity is obtained. Absorbed dose to a targetorgan voxel is obtained by summing the contributions fromall source organ voxels. In this manner, a nonuniform ac-tivity distribution can be taken into account at the macro-scopic level.
A third strategy by which penetrating radiation contri-bution to dose can be estimated is via a Monte Carlo sim-ulation similar to the original code that generated the datafound in MIRD Pamphlets No. 5 and No. 11. An examplecan be seen in the software program of Johnson and Ves-sella termed MABDOS, an acronym for Monoclonal An-tiBody DOSimetry.58,59 The MABDOS code allows the op-erator to enter up to five tumor foci acting as sources ofand targets for radiation in the Standard Man Model. Ini-tial simulations for 131I indicate the possibility that photonsoriginating in the liver, spleen and whole body may con-tribute more than 20% of the tumor’s dose, depending onthe amount of tumor specific uptake.
The MABDOS program initiates a dosimetry session bytaking interactive input from the user. The user identifieseach source organ to be included in the dosimetry calcu-lation, and enters a series of time/activity data points as-sociated with that source organ. The question of sourceorgan identification and selection will be specific to a givenradiopharmaceutical, and dependent on its biodistributionproperties in the human body. If an organ system can beresolved on a nuclear medicine scintigram, the assumptionis made that the organ system localizes activity to a degreegreater than that of radioisotope distributed throughoutthe whole body. This qualifies it by definition as a sourceorgan. MABDOS is completely flexible in that it allowsa d o s i m e t r y t r e a t m e n t o f a n y r a d i o i s o t o p e /radiopharmaceutical complex.
A graph mode (linear, semilog, or logit) is selectedwhich initiates a display of the individual time activitycurves. Methodology (curve peeling, trapezoidal integra-tion or mathematical modeling) to fit the time/activitydata points is chosen to achieve an estimate of cumulatedactivity for each source organ.
If a tumor has been identified as a source organ, thecoronal projection of Standard Man then appears on thegraphics screen. Identifying the height of the tumor center
in the Standard Man reference frame with a mouse initiatesthe drawing of the corresponding transverse slice of Stan-dard Man. The tumor center is next defined on the trans-verse slice, thereby positioning the tumor center with co-ordinates in x, y, and z. The tumor is approximated as asphere, and the tumor radius is entered. This identifies thetumor in three dimensions; the entered radius subsequentlydeclares a volume of space in the Standard Man as repre-senting a tumor.
The source organ information, tumor geometry infor-mation (x/y/z location of center, and radius)) and se-lected isotope are uploaded to a CRAY. Beta radiation isassumed to be locally absorbed as in MIRD 11. A simula-tion of photon transport is carried out to estimate pene-trating radiation absorbed fractions. The output consists ofan S table having an additional row and column for eachidentified tumor. The "S" table is downloaded to the mi-crocomputer host where it is combined with the cumulatedactivity and generates a dose table similar to those pre-sented in the MIRD 11 tables.
There are drawbacks to both the convolution and theMonte Carlo simulation approaches. The convolution tech-nique requires that anatomic boundaries be defined forsource and target organs. Invariably this means that a se-quence of CT or MRI slices be placed on a viewing screenand borders traced. The amount of time required is sub-stantial. Although this shortcoming could be addressedwith automated edge detection by a computer, the varia-tion of human anatomy from patient to patient virtuallyprecludes current algorithms from consistently workingcorrectly. This would necessitate review by a human ob-server, with subsequent interventional correction of ana-tomic boundaries.
A second shortcoming of the convolution technique isthe use of a point dose kernel. The kernels are derived forhomogeneous media, typically water. The makeup of thehuman body, however, is exceedingly complex. An inho-mogeneous mixture of bone and soft tissue predominatesthroughout the body. Recent work by Kwok et al. indi-cates that tissue dose at a bone interface is underestimatedby 20%-40% because of the backscatter of low-energyelectrons.6 0 A solution would be to derive a point dosekernel for each voxel in the human body or Standard ManModel. The point dose kernel derivation being based on aMonte Carlo simulation leads back to the implementationof a Monte Carlo solution. The backscatter phenomenareported by Kwok et al. at a bone interface represents anadditional error that can only be replicated by MonteCarlo simulation.60 The use of convolutions are derived forhomogeneous media, and do not allow the inclusion ofdifferent media.
The shortcomings of the Monte Carlo approach areprincipally ones of computation time economy, and the useof a model rather than the patient’s own anatomy. Underthe assumption of homogeneous activity deposition, modelapplicability to an individual is reasonable since smallchanges in organ shape should not appreciably alter theabsorbed fraction.‘* With regard to the computation time,Monte Carlo solutions are by nature time-consuming, be-
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

589 Meredith et al.: Dosimetry of solid tumors 589
ing a statistical answer requiring numerous histories to re-liably estimate absorbed fractions. The MABDOS codecurrently executes in a “reasonable” amount of time on aCRAY supercomputer.61 The issues of access and expensemake this technique unattractive to many institutions. TheMonte Carlo simulation code is currently being ported toan array of INMOS transputers housed on a microcom-puter expansion card. This will hopefully obviate the needfor access to a CRAY supercomputer. A complete dosim-etry sess ion would be conducted f rom within themicrocomputer. 6 2 This could potentially deal with theproblem of execution time by using multiple processors tolinearly speed up the calculation. The cost of such a ma-chine with a modest number of transputers would be lessthan $50000.
C. Method No. 3: Inhomogeneous distribution ofradioactivity throughout the tumor volume,all radiations accounted for
While SPECT has improved the quantitation of non-uniform distribution of radioactivity at the macroscopiclevel, it is difficult to measure the microscopic inhomoge-neity that is known to exist. Microdetectors offer a methodfor determining energy deposition at a point, albeit not inan imaging format.6 3’6 4 However, the procedure is invasiveand requires that tumors be accessible for placement ofthese measuring devices. Furthermore, multiple detectorswould be required for mapping the dose distributions.With these limitations microdetectors appear inpracticalfor widespread clinical use.
Inclusion of inhomogeneous distribution information indose calculations will therefore rely mainly on animal stud-ies, cell culture models65 and sequential autoradiographs.Extrapolation from these systems is also fraught with in-accuracies but may allow estimates that are useful in di-recting clinical trials.
IV. SPECIAL CONSIDERATIONS IN TUMORDOSIMETRY
To date, human tumor uptake and clearance of radio-immunoconjugates have not been modeled with confi-dence. Thus activity versus time measurements are essen-tial for estimating cumulated radiation delivered to tumorsin this manner. Numerous proposals for altering tumoruptake and washout kinetics such as extracorporealimmunoadsorption66,67 and chimeric or engineered anti-body fragments further complicate the situation.
Most tumor dosimetry from clinical studies has in-volved administration of xenogeneic antibodies which havea relatively short circulating half-life. With the construc-tion of chimeric antibodies (using a xenogeneic variableregion linked to a human constant region), the effectivehalf-life of the administered antibody has increased severalf o l d .6 8 E a r l y r e s u l t s f r o m a d m i n i s t r a t i o n o f131I-mouse/human chimeric B72.3 have demonstrated lo-calization of activity to tumor sites persisting for longerthan 20 days.69 Since it is impractical to scan daily for theentire period of detectable localization as may be done for
patients receiving xenogeneic antibody, assumptions mustbe made for cumulated radioactivity in tumors for the in-tervals between relatively wide-spaced scanning times. Ini-tial dosimetry in these cases has been performed assuminglinear accumulation in the site of localization when thecount rate increases with time, and an exponential decreaseof 1 3 1I concentration when the count rate drops betweenmeasurements.21
Although it may seem less accurate to have intervals ofseveral days between measurements for long-lived antibod-ies, dose estimates have not been determined to be lessprecise than for antibodies that circulate for a shorter pe-riod of time where a large portion of the total cumulatedactivity may be accrued quickly. The interval betweenmeasurements may not be as important as the total numberof measurements obtained over the period of high initialactivity.
Another source of potential inaccuracy in tumor dosim-etry is the uncertainty as to when the radionuclide concen-tration in the tumor exceeds background. To minimize thechance of missing the peak by a considerable period oftime, frequent early scans are recommended even if tech-nical innovations are required in order to protect personnelfrom undue radiation exposure.
To alleviate the problem of early scanning of patientswith therapeutic doses of radiolabeled antibodies, a tracerdose is often used with linear extrapolation of results tolarger doses delivered at a later time. 8,11 Although thistechnique will be accurate if the distribution and kinetics ofthe two doses coincide, errors of dosimetry can be large ifthese parameters are not similar for all administrations. 11,70
In using this technique a verification method should beused to confirm the linear scaling from tracer dose to ther-apeutic dose. As a minimum, whole body disappearancecurves should be generated with a GM counter for thetherapeutic dose, a procedure analogous to measurementsmade for release of patients undergoing 1 3 1I therapy forthyroid disease. Alternative methods such as analysis ofplasma clearance or other parameters71 may prove to bemore reliable in predicting whole body and region of inter-est half-life of radiolabeled antibody than following thekinetics of a small preliminary dose of the same agent.However, such techniques have not been well documentedin the literature to date.
Limited information has been reported comparing therelative biologic effectiveness of radiation delivered as frac-tionated high dose rate external beam therapy, low doserate brachytherapy and at an exponentially decreasing doserate characteristic of radioimmunotherapy.72-77 Not only isit difficult to compare radioimmunotherapy with othertechniques of radiation exposure because of the many vari-ables with radioimmunoconjugate therapy, it is also diffi-cult to compare the results within radioimmunotherapytrials. As in external beam radiation where reporting of atotal dose must be clarified by dose/fraction description,radioimmunotherapy dose reporting should provide de-tails. Specifics should include the radioimmunoconjugate,amount administered, injection route, dose rate informa-tion, times of activity measurement, calculation methods
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

590 Meredith et al.: Dosimetry of solid tumors
including assumptions used for calculations, and an esti-mate of total cumulated dose. These factors may assist infurthering the field of solid tumor dosimetry and quanti-tating the probability of tumor control by various doses ofradioimmunoconjugate therapy.
V. SUMMARY
A broad range of absorbed dose estimates to solid tu-mors is reported in the literature. Most of this dose varia-tion can be traced to differences in injected activity levels,patient size, biologic behavior of the immunoconjugate andother real factors. Nevertheless, some portion of the re-ported dose range undoubtedly results from the diversity ofapproaches currently used for quantifying tumor dose. Do-simetry for parenterally administered radionuclides is cur-rently based primarily on the MIRD formalism, withquantitation of local uptake and clearance by means ofplanar imaging computational techniques. This approachto solid tumor dosimetry presents difficulties that are beingdealt with in various ways. Some of the problems associ-ated with the use of planar imaging for tumor activityquantitation, such as the inability to accurately measurevolumes or to eliminate contributions from overlying andunderlying tissue, may be alleviated by new developmentsin the area of SPECT imaging.
Although well suited for dosimetry of normal organs,the existing MIRD formalism cannot easily deal with thearbitrary geometries of solid tumors and their spatial rela-tionship to other sites of localized activity. Convolutiontechniques and Monte Carlo simulations which are underinvestigation may accommodate nonstandard tumormasses for MIRD calculations. Alternatively, one may usethe method outlined above for determining S factors forarbitrary soft tissue masses.
The resolution limits of existing nuclear imaging devicesprecludes mapping of uptake heterogeneity, which isknown to exist at the cellular level. In light of this heter-ogeneity, specification of the dose to a tumor is of ques-tionable value. As measurement and computation tech-niques are advanced to the point where nonuniformdeposition of activity can be quantitated and incorporatedinto dose estimates, the effect of radioimmunotherapy onsolid tumors might be more effectively represented as sta-tistical distributions of dose to populations of tumor cells.
Accurate models for the kinetics of immunoconjugatesin solid tumors can only be developed from extensive serialsampling of uptake and clearance using measurement tech-niques that are reasonably accurate and uniformly applied.Further definition of dose/response relationships for radio-immunotherapy of solid tumors should further stimulatedevelopment of techniques needed to achieve therapeuticefficacy.
ACKNOWLEDGMENTS
The authors wish to thank Dr. Peter Leichner, Dr.Barry Wessels, Dr. Jeffry Siegel, Dr. Virginia Langmuir,and Dr. Donald Buchsbaum for discussion and sugges-tions, and Charm Pate and Tracy Blevins for preparation
of the manuscript. This work was supported in part bygrants from the National Institutes of Health NC1 NO1CM-97611, PO1 CA43904 and 5P30 CA33572.
1S. M. Larson, “Radioimmunology: Imaging and therapy,” Cancer 67,Suppl., 1253-1260 (1991).
2V. K. Langmuir. “Radioimmunotherapy: Clinical results and dosimet-ric considerations,” Int. J. Radiat. Appl. Instrum. Part B: Nucl. Med.Biol. 19, 213-225 (1992).
3J. A. Siegel, D. M. Goldenberg, and C. C. Badgers, “Radioimmuno-therapy dose estimation in patients with B-cell lymphomas,” Med.Phys. 20, 579-582 (1993).
4R. Loevinger and M. Berman, “A revised schema for calculating theabsorbed dose from biologically distributed radionuclides,” MIRDPamphlet No. 1, revised, with a Forward by R. J. Cloutier and E. M.Smith (Society of Nuclear Medicine, New York. 1976).
5W. S. Snyder, M. R. Ford, G. G. Warner, and S. B. Watson, “S’:Absorbed dose per unit cumulated activity for selected radionuclidesand organs,” MIRD Pamphlet No. 11 (Society of Nuclear Medicine,New York, 1975).
6G. L. Brownell, W. H. Ellett, and A. R. Reddy, “MIRD Pamphlet No.3: Absorbed fractions for photon dosimetry,” J. Nucl. ‘Med. 9, Suppl. 1,28-39 ( 1968).
7W. H. Ellett and R. M. Humes, “MIRD Pamphlet No. 8: Absorbedfractions for small volumes containing photon-emitting radioactivity,”J. Nucl. Med. 12, Suppl. 5, 26-32 (1971).
8O. W. Press, J. F. Eary, C. C. Badger, P. J. Martin, F. R. Appelbaum,R. Levy, R. Miller, S. Brown, W. B. Nelp, K. A. Krohn, D. Fisher, D.DeSantes, B. Porter, P. Kidd, E. D. Thomas, and I. D. Bernstein,“Treatment of refractory non-Hodgkin’s lymphoma with radiolabeledMB-l (anti-CD37) antibody,” J. Clin. Onc. 7(8), 1027-1038 (1989).
9M. S. Kaminski, L. M. Fig, K. R. Zasadny. K. F. Koral, R. B. Del-Rosario, I. R. Francis, C. A. Hanson, D. P. Normolle, E. Mudgett, C.P. Liu, S. Moon, P. Scott, R. A. Miller, and R. L. Wahl, “Imaging,dosimetry, and radioimmunotherapy with iodine-131-labeled anti-CD37 (MB-l) antibody in B-cell lymphoma,” J. Clin. Onc. 10(11),1696-1711 (1992).
10K. Koral, K. Zasadny, and M. Fayez, “Importance of intra-therapySPECT imaging in calculating tumor dosimetry for a lymphoma pa-tient,” Eur. J. Nucl. Med. 18, 432-435 (1991).
11S. J. DeNardo, G. L. DeNardo, L. F. O’Grady, N. B. Levy, S. L. Mills,D. J. Macey, J. P. McGahan, C. H. Miller, and A. L. Epstein, “Pilotstudies of radioimmunotherapy of B cell lymphoma and leukemia using1 -131 LYM-1 monoclonal antibody,” Antib., Immunoconj. Radiop-harm. 1(1). 17-33 (1988).
12D. M. Goldenberg, J. A. Horowitz, R. M. Sharkey, T. C. Hall, S.Murthy, H. H. Goldenberg, R. E. Lee, R. Stein, J. A. Siegel, D. O.Izon, K. Burger, L. C. Swayne, E. Belisle, H. J. Hansen, and C. M.Pinsky, “Targeting, dosimetry, and radioimmunotherapy of B-cell lym-phomas with 131I-labeled LL2 (EPB-2) monoclonal antibody,” J. Clin.Oncol. 9, 548-564 (1991).
13D. A. Scheinberg, D. J. Straus, S. D. Yeh, C. Divgi, P. Garin-Chesa,M. Graham, K. Pentlow, D. Coit, H. F. Oettgen, and L. J. Old, “Aphase I toxicity, pharmacology, and dosimetry trial of monoclonal an-tibody OKB7 in patients with non-Hodgkin’s lymphoma: Effects oftumor burden and antigen expression,” J. Clin. One. 8(5), 792-803(1990).
14S. T. Rosen, A. M. Zimmer, R. Goldman-Leikin, L. I. Gordon, J. M.Kazikiewicz, E. H. Kaplan, D. Variakojis, R. J. Marder, M. S.Dykewicz, A. Piergies, E. A. Silverstein, H. H. Roenigk Jr., and S. M.Spies, “Radioimmunodetection and radioimmunotherapy of cutaneousT cell lymphomas using an 131I-labeled monoclonal antibody: An Il-linois Cancer Council study,” J. Clin. Onc. 5(4), 562-573 (1987).
15R. E. Lenhard, S. E. Order, J. J. Spunberg, S. O. Asbell, and S. A.Leibel, “Isotopic immunoglobulin: A new systemic therapy for ad-vanced Hodgkin’s disease,” J. Clin. Oncol. 3, 1296-1300 (1985).
16H. M. Vriesendorp, J. M. Herpst, P. K. Leichner, J. L. Klein, and S. E.Order, “Polyclonal 9 0yttrium labeled antiferritin for refractoryHodgkin’s disease,” Int. J. Radiat. Oncol. Biol. Phys. 17, 815-821(1989).
17S. E. Order, H. M. Vriesendorp, J. L. Klein, and P. K. Leichner, “Aphase I study of 90yttrium antiferritin: dose escalation and tumor dose,”Antib. Immunoconj. Radiopharm. 1, 163-168 (1988).
Medical Physics, Vol. 20. No. 2, Pt. 2, Mar/Apr 1993

591 Meredith et al.: Dosimetry of solid tumors 591
18P. K. Leichner, J. L. Klein. J. B. Garrison, R. E. Jenkins, E. L. Nick-oloff, D. S. Ettinger, and S. E. Order, “Dosimetry of 131I-labeled anti-fenitin in hepatoma: A model for radioimmunolglobulin dosimetry,”Int. J. Radiat. Oncol. Biol. Phys. 7, 323-333 ( 1981).
19P. K. Leichner, N. C. Yang, T. L. Frenkel, D. M. Loudenslager, W. G.Hawkins, J. L. Klein, and S. E. Order, "Dosimetry and treatmentplanning for y-labeled antiferritin in hepatoma:" Int. J Radiat. On-col. Biol. Phys. 14, 1033-1042 (1988).
20S. E. Order, G. B. Stillwagon, J. L. Klein, P. K. Leichner, S. S. Siegel-man, E. K. Fishman, D. S. Ettinger, T. Haulk, K. Kopher, K. Finney,M. Surdyke, S. Self, and S. Leibel, “Iodine-131-antiferritin, a new treat-ment modality in hepatoma: a Radiation Therapy Oncology GroupStudy,” J. Clin. Oncol. 3, 1573-1582 (1985).
21R. F. Meredith, M. B. Khazaeli, G. Plott, M. N. Saleh, T. Liu, L. F.Allen, C. D. Russell, R. A. Orr, D. Colcher, J. Schlom, D. Shochat, R.H. Wheeler, and A. F. LoBuglio, “Phase I trial of 131I-chimeric B72.3in metastatic colorectal cancer,” J. Nucl. Med. 33(l), 23-29 (1992).
22R. L. Vessella, “Radioimmunoconjugates in renal cell carcinoma,” inImmunotherapy of Renal Cell Carcinoma, edited by F. M. J. Debruyne,R. M. Bukowski, J. E. Pontes, and P. H. M. de Mulder (SpringerVerlag, Heidelberg, 1991), pp. 38-46.
23P. Riva, G. Moscatelli, S. Lazzari, M. Agostini, G. Sarti, A. Spinelli, G.Vecchietti, R. Gasperoni, D. Tirindelli, and G. Franceschi, “Systemicand locoregional administration of labelled MOABS for gastrointesti-nal cancer radioimmunotherapy: Biokinetics, pharmacokinetics anddosimetry aspects,” J. Nucl. Med. 30, 779 (1989).
24R. H. J. Begent, J. A. Ledermann, A. J. Green, K. D. Bagshawe, S. J.Riggs, F. Searle, P. A. Keep, T. Adam, R. G. Dale, and M. G. Glaser,“Antibody distribution and dosimetry in patients receiving radiola-beled antibody therapy for colorectal cancer,” Br. J. Cancer 60, 406-412 (1989).
25J. A. Siegel, D. A. Pawlyk, R. E. Lee, N. L. Sasso, J. A. Horowitz, R.M. Sharkey, and D. M. Goldenberg, “Tumor, red marrow, and organdosimetry for 131I-labeled anti-carcinoembryonic antigen monoclonalantibody,” Cancer Res. Suppl. 50, 1039-1042 ( 1990).
26G. B. Stillwagon, S. E. Order, J. L. Klein, P. K. Leichner, S. A. Leibel,S. S. Siegelman, E. K. Fishman, D. S. Ettinger, T. Haulk, K. Kopher,S. M. Brown, and K. Finney, “Multi-modality treatment of primarynonresectable intrahepatic cholangiocarcinoma with 131I anti-CBA-aRadiation Therapy Oncology Group study,” Int. J. Radiat. Oncol.Biol. Phys. 13, 687-695 ( 1987).
27J. A. Carrasquillo, K. A. Krohn, P. Beaumier, R. W. McGuffin, J. P.Brown, K. E. Hellstrom, I. Hellstrom, and S. M. Larson, “Diagnosis ofand therapy for solid tumors with radiolabeled antibodies and immunefragments,” Cancer Treat. Rep. 68, 317-328 (1984).
28L. Lashford, D. Jones, J. Pritchard, F. Breatnach, and J. T. Kemshead,“Therapeutic application of radiolabeled monoclonal antibody UJ13Ain children with disseminated neuroblastoma,” NCI Monogr. 3, 53(1987).
29R. W. Schroff, P. L. Weiden, J. Appelbaum, M. F. Fer, H. Breitz, J. L.Vanderheyden, B. A. Ratliff, D. Fisher, D. Foisie, L. G. Hanelin, A. C.Morgan, Jr., A. R. Fritzberg, and P. G. Abrams, “Rhenium-186 la-beled antibody in patients with cancer: Report of a pilot Phase Istudy,” Antib. Immunoconj. Radiopharm. 3, 99-110 ( 1990).
30H. B. Breitz, D. R. Fisher, P. L. Weiden, J. S. Durham, B. A. Ratliff,M. J. Bjom, P. L. Beaumier, and P. G. Abrams, “Dosimetry of186rhenium labeled monoclonal antibodies: Methods, prediction from99mTc-labeled antibodies and results of Phase I trials.” J. Nucl. Med.,July (1993).
31H. B. Breitz, P. L. Weiden, J. L. Vanderheyden, J. W. Appelbaum, M.J. Bjorn, M. F. Fer, S. B. Wolf, B. A. Ratliff, C. Seiler, D. C. Foisie, D.R. Fisher, R. W. Schroff, A. R. Fritzberg, and P. G. Abrams, “Clinicalexperience with 186rhenium-Iabeled monoclonal antibodies for radioim-munotherapy: Results of Phase I trials,” J. Nucl. Med. 33, 1099-1112(1992).
32A. M. Markoe, L. W. Brady, D. Woo, B. Amendola, U. Karlsson, S.Fisher, B. Micaily. M. Rackover, S. Bulova, Z. Steplewski, and H.Koprowski, “Treatment of gastrointestinal cancer using monoclonalantibodies,” in Frontiers of Radiation Thempy Oncology, edited by J.M. Vaeth and J. L. Meyer (Karger, Basel, 1990). Vol. 24, pp. 214-224.
33B, A. Parker, A. B. Vassos, S. E. Halper, R. A. Miller, H. Hupf, D. G.Amox, J. L. Simoni, R. J. Starr, M. R. Green, and I. Royston, “Ra-dioimmunotherapy of human B-cell lymphoma with 90Y-conjugated
anti-idiotype monoclonal antibody,” Cancer Res. Suppl. 50, 1022-1028(1990).
34H. P. Kalofonos, T. R. Pawlikowska, A. Hemingway, N. Courtenay-Luck, B. Dhokia, D. Snook, G. B. Sivolapenko, G. R. Hooker, C. G.McKenzie, P. J. Lavender, D. G. T. Thomas, and A. A. Epenetos,“Antibody guided diagnosis and therapy of brain gliomas using radio-labeled monoclonal antibodies against epidermal growth factor recep-tor and placental alkaline phosphatase,” J. Nucl. Med. 30, 1636-1645(1989).
35P. Riva, A.. Arista, G. Mariani, E. Seccamani, S. Lazzari, S. G. Mos-catelli, C. Sturiale, G. Sarti, G. Franceschi, A. Spinelli, G. Vecchietti,N. Riva, P. Natali, and P. L. Zardi, “Improved tumor targeting bydirect intralesional injection of radiolabeled monoclonal antibody: Aphase I study in brain glioma,” J. Nucl. Med. 32(5), 922 (1991).
36S. J. DeNardo, K. A. Warhoe, L. F. O’Grady, D. J. Macey, A. H.Gobuty, I. Hellstrom, K. E., Hellstrom, L. W. Kroger, and G. L.DeNardo, “Response to 131I chimeric MoAb L-6 radioimmunotherapyin patients with advanced metastatic breast cancer,” J. Nucl. Med.32(5), 922 (1991).
37S. J. DeNardo, K. A. Warhoe, L. F. O’Grady, G. L. DeNardo, I.Hellstrom, K. E. Hellstrom, and S. L. Mills, “Radioimmunotherapywith I-131 chimeric L-6 in advanced breast cancer,” in Breast Epithe-lial AnTigem, edited by R. L. Ceriani (Plenum, New York, 1991).
38R.. B. Richardson, J. T. Kemshead, A. G. Davies, G. E. Staddon, P. C.Jackson, H. B. Coakham, and L. S. Lashford, “Dosimetry of intra-thecal Iodine”’ monoclonal antibody in cases of neoplastic meningi-tis,” Eur. J. Nucl. Med. 17, 42-48 (1990).
39S. M. Larson, J. A. Carrasquillo, D. C. Colcher, K. Yokoyama, J. C.Reynolds, S. A. Bacharach, A. Raubitchek, L. Pace, R. D. Finn, M.Rotman, M. Stabin, R. D. Neumann, P. Sugarbaker, and J. Schlom,“Estimates of radiation absorbed dose for intraperitoneally adminis-tered iodine-131 radiolabeled B72.3 monoclonal antibody in patientswith peritoneal carcinomatoses,” J. Nucl. Med. 32, 1661-1667 (1991).
40L. W. Brady, D. V. Woo, A. Markoe, S. Dadparvar, U. Karlsson, M.Rackover, R. Peyster, J. Emrich, C. Miyamoto, Z. Steplewski, and H.Koprowski, “Treatment of malignant gliomas with 125I labeled mono-clonal antibody against epidermal growth factor receptor,” Antibody,Immunoconjug. Radiopharm. 3 (3), 169-179 (1990).
41P. Leichner and C. Kwok, “Calculation methods,” Med. Phys. 20,569-577 (1993).
42M. H. Griffith, E. D. Yorke, B. W. Wessels, G. L. DeNardo, and W. P.Neacy, “Direct dose confirmation of quantitative autoradiography withmicro-TLD measurements for radioimmunotherapy,” J. Nucl. Med.29, 1795-1809 (1988).
43G. M. Makrigiorgos, S. J. Adelstein, and A. I. Kassis, “Limitations ofconventional internal dosimetry at the cellular level,” J. Nucl. Med. 30,1856-1864 (1989).
44G. J. Hine and G. L. Brownell, Radiation Dosimetry (Academic, NewYork, NY, 1956). Chap. 16, pp. 734-735.
45L. F. Mausner and S. C. Srivastava, “Selection of radionuclides forradioimmunotherapy,” Med. Phys. 20, 503-509 (1993).
46J. L. Humm, J. C. Roeske, D. R. Fisher, and G. T. Y. Chen, “Micro-dosimetric concepts in radioimmunotherapy,” Med. Phys. 20, 535-541(1993).
47M. Roselli, J. Schlom, O. A. Gansow, A. Raubitschek, S. Mirzadeh, M.W. Brechbiel, and D. Colcher, “Comparative biodistributions ofyttrium- and indium-labeled monoclonal antibody B72.3 in athymicmice bearing human colon carcinoma xenografts,” J. Nucl. Med. 30,672-682 (1989).
48J. Orear, A. H. Rosenfeld, and R. A. Schuter, Nuclear Physics, A courseGiven by Enrico Fermi at the University of Chicago, Revised Edition,(University of Chicago, Chicago, IL, 1950). Chap. 1, pp. 43-47.
49L. M. Lamki, J. Kavanagh, M. G. Rosenblum, J. L. Murray, D. Pod-oloff, T. Burke, V. Bhadkamkar, L. Thompson, J. Shanken, J. Cun-ningham, E. E. Kim, R. T. MaGuire, and T. P. Haynie, “Intraperito-neal r ad io immuno the rapy o f ovarian cancer with90yttrium-GYK-DTPA-B72.3 antibody: Tissue distribution, pharma-cokinetics, toxicity, and bremsstrahlung imaging,” J. Nucl. Med. 31,724 (1990).
5 0L. E. Williams, J. Y. C. Wong, D. O. Findley, and B. W. Forell“Measurement and estimation of organ bremsstrahlung radiationdose,” J. Nucl. Med. 30, 1373-1377 (1989).
51M. G. Stabin, K. F. Eckerman, J. C. Ryman, and L. E. Williams,“Bremsstrahlung dosimetry component in Y-90 monoclonal antibodytherapy,” J. Nucl. Med. 29, 926 (1988).
52W. S. Snyder, M. R. Ford, and G. G. Warner, “Estimates of specific
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

592 Meredith et al.: Dosimetry of solid tumors 592
absorbed fractions for photon sources uniformly distributed in variousorgans of a heterogeneous phantom,” NM/MIRD Pamphlet No. 5,Revised.
53G. Sgouros, G. Barest, J. Thekkumthala, C. Chui, R. Mohan, R. E.Bigler, and P. B. Zanzonico, “Treatment planning for internal radio-nuclide therapy: Three-dimensional dosimetry for nonuniformly dis-tributed radionuclides.” J. Nucl. Med. 31, 1884-1891 (1990).
54R. L. Ford and W. R. Nelson, “The EGS code system,” StanfordLinear Accelerator Center Report. (210) Stanford, California ( 1978).
55D. W. O. Rogers and A. F. Bielajew, “Experimental benchmarks ofEGS,” in Monte Carlo Transport of Electrons and Photons, edited by T.M. Jenkins, W. R. Nelson and A. Rindi, (Plenum, New York, 1988).
56M. J. Berger and S. M. Seltzer, “ETRAN, Monte Carlo code system forelectron and photon transport through extended media,” ORNL doc-umentation for RSIC computer code package CCC-107 (1973).
57I.. J. Das, “An empirical method for beta-ray dosimetry at a homoge-neous plane interface,” Phys. Med. Biol. 32 (12), 1609-1613 (1987).
58T. K. Johnson and R. L. Vessella, “A generalized dosimetry schema fortumor preferential uptake of monoclonal antibodies in radionuclideimmunotherapy,” J. Nucl. Med. Suppl. 28(4), 680 ( 1987).
59T. K. Johnson, “MABDOS: A generalized program for internal radi-onuclide dosimetry,” Comput. Meth. Progr. Biomed. 27, 159-167(1988).
60C. S. Kwok, P. J. Bialobzyski, S. K. Yu, and W. V. Prestwich, “Effectof tissue inhomogeneity on dose distribution of point sources of low-energy electrons,” Med. Phys. 17(5), 786-793 (1990).
61T. K. Johnson and R. L. Vessella, “On the possibility of ‘real-time’Monte Carlo calculations for the estimation of absorbed dose in radio-immunotherapy,” Comput. Meth. Progr. Biomed. 29, 205-210 (1989).
62T. K. Johnson and R. L. Vessella, “On the application of parallelprocessing to the computation of dose arising from the internal depo-sition of radionuclides,” Comput. Phys. 3, 69-72 (1989).
63B. W. Wessels and M. H. Griffith, “Miniature thermoluminescent do-simeter absorbed dose measurements in tumor phantom models,” J.Nucl. Med. 27, 1308-1314 (1986).
64D. J. Gladstone, D. G. Chin, and L. M. Chin, “Automated data col-lection and analysis system for MOSFET radiation detectors,” Med.Phys. 18(3), 542-548 (1991).
65V. K. Langmuir and R. M. Sutherland, “Dosimetry models for radio-immunotherapy,” Med. Phys. 15, 867-873 (1988).
66J. L. Lear, R. K. Kasliwal, A. J. Feyerabend, J. P. Pratt, P. A. Bunn,D. G. Dienhart, R. Gonzalez, T. K. Johnson, D. C. Bloedow, S. W.Maddock, and S. D. Glenn, “Improved tumor imaging with radiola-beled monoclonal antibodies by plasma clearance of unbound antibodywith anti-antibody column,” Radiology 179, 509-5 12 (1991).
67T. K. Johnson, S. Maddock, R. Kasliwal, D. Bloedow, C. Hartmann,A. Feyerabend, D. G. Dienhart, D. Thickman, S. Glenn, R. Gonzalez,
J. Lear, and P. Bunn, Jr., “Radioimmunoadsorption of KC-4G3 anti-body in peripheral blood: Implications for radioimmunotherapy,” An-tib. Immunoconj. Radiopharm. 4 (4), 885-893 (1991).
68A. F. LoBuglio, R. H. Wheeler, J. Trang, A. Haynes, K. Rogers, E. B.Harvey, L. Sun, J. Ghrayeb, and M. D. Khazaeli, “Mouse/humanchimeric monoclonal antibody in man: Kinetics and immune re-sponse,” Proc. Natl. Acad. Sci. U.S.A. 86, 4220-4224 ( 1989).
69R. F. Meredith, M. B. Khazaeli, W. E. Plott, I. A. Brezovich, C. D.Russell, R. H. Wheeler, S. A. Spencer, and A. F. LoBuglio, “Compar-ison of two mouse/human chimeric antibodies in patients with meta-static colon cancer,” Antibod. Immunoconj. Radiopham. 5 (1), 75-80(1992).
7 0R. Meredith, G. Plott, I. Brezovich, M. Khazaeli, C. Russell, R.Wheeler, M. Saleh, T. Simpson, A. Haynes, L. Allen, R. Orr, T. Baker,S. Spencer, M. Hardin, M. Salter, and A. LoBuglio, “Comparativedosimetry with repeat courses of 131I-labeled murine or mouse/humanchimeric monoclonal antibodies,” Int. J. Radiat. Oncol. Biol. Phys. 19,Suppl. 1, 252 (1990).
71J. B. Slater, J. M. Frincke, D. R. Stickney, and G. A. Kirk, “The roleof CEA as a metabolic indicator to predict the pharmacokinetics of thebifunctional antibody system (BFA) in colon carcinoma,” J. Nucl.Med. 30, 905 (1989).
72J. M. Berkopec, E. Bradley, B. W. Wessels, D. F. Palme, L. Mantilla,and R. L. Vessella, “Combined external beam irradiation (XRT) andradioimmunotherapy (RIT) on renal cell carcinoma xenografts,” J.Nucl. Med. 30 (5), 406 (1989).
73L. E. Dillehay and J. R. Williams, “Radiobiology of dose-rate patternsachievable in radioimmunoglobulin therapy,” in Frontiers of RadiationTherapy and Oncology edited by J. M. Vaeth and J. L. Meyers(Karger, Basel, 1990), Vol. 23, 93-103.
74R. L. Vessella, D. F. Palme, J. M. Berkopec, M. K. Elson, B. W.Wessels, E. W. Bradley, and P. H. Lange, “Radiotherapy of humanrenal cell carcinoma (RCC) xenograft: Comparison between singlefraction monoclonal antibody (MoAb) A6H 131-iodine conjugates andsingle fraction x-ray external beam irradiation,” Am. Assoc. CancerRes. 29, 1707 (1988).
75S. J. Knox, R. Levy, R. A. Miller, W. Uhland, J. Schiele, W. Ruehl, R.Finston, P. Day-Lollini, and M. L. Goris, “Determinants of the anti-tumor effect of radiolabeled monoclonal antibodies,” Cancer Res. 50,4935-4940 (1990).
76B. W. Wessels, R. G. Vessella, D. F. Palme, J. M. Berkopec, G. K.Smith, and E. W. Bradley, “Radiobiological comparison of externalbeam irradiation and radioimmunotherapy in renal cell carcinoma xe-nografts,” Int. J. Radiat. Oncol. Biol. Phys. 17, 1257-1263 (1989).
77V. K. Langmuir and R. M. Sutherland, “Radiobiology of radioimmu-notherapy,” Antibod. immunoconj. Radiopharm. 1, 195-211 (1988).
Medical Physics, Vol. 20, No. 2. Pt. 2, Mar/Apr 1993

Dosimetry of intraperitoneally administered radiolabeled antibodiesJohn C. Roeske and George T. Y. ChenMichael Reese/University of Chicago, Center for Radiation Therapy, Department of Radiationand Cellular Oncology, University of Chicago, Chicago, Illinois 60637
A. Bertrand BrillUniversity of Massachusetts, Worcester, Massachusetts
(Received 18 March 1992; accepted for publication 24 December 1992)
Intraperitoneal and intracavitary radioimmunotherapy differ from other approaches of radio-immunotherapy in that high activity and dose gradients exist near the solution/tumor interface.Dose to tumor and normal tissue at the interface is a function of depth and is due to three majorcomponents: (1) the activity concentration of the administered radiolabeled antibody solutionas a function of time within the compartment; (2) the spatial distribution of antibody/radionuclide complex as a function of depth and time as the biomolecules bind to and permeatetumor/normal tissues; and (3) the physical characteristics of the radionuclide in relation todepth of antibody penetration. In this review, the biological and physical aspects of intraperi-toneally administered radiolabeled antibodies are discussed, and the state of experimental andcalculational studies for this site is described. Areas requiring future investigation are examined,and recommendations are made regarding the type of measurements and calculations which arerequired for accurate dosimetry.
Key words: intraperitoneal radioimmunotherapy, dosimetry, models, alpha and beta emitters
1. INTRODUCTION
Regional administration of radiolabeled antibodies fortherapeutic intent is advantageous because this approachdelivers relatively high concentrations of biologically spe-cific molecules directly to the site of the disease, thus pro-viding a high tumor-to-normal tissue (T/NT) dose ratio.Possible anatomic sites include the peritoneum forovarian 1-12 and colorectal carcinomas,13-14 the cerebral spi-nal fluid for leptomeningeal disease,15,16 the thoracic cavityfor the treatment of pleural/pericardial effusions,17,18 andwithin the tumor itself in the therapy of cystic braintumors.” In recent years, pilot studies in humans haveshown partial or complete responses to intraperitoneal ra-dioimmunotherapy (IPRIT), spurring additional interestin this technique. The dose to tumor and normal tissues isdifficult to quantify, yet an understanding of the dosimetryof radiolabeled antibodies is important in interpreting clin-ical results and in defining directions to make this type oftreatment more effective. In this review, we discuss (a) theclinical rationale for IPRIT, (b) those biological and phys-ical parameters which most strongly affect the dose distri-bution to tumor, (c) the current status of dose measure-ment and calculations for IPRIT, and (d) research goalsand future directions for IPRIT dosimetry. We focus onintraperitoneal radioimmunotherapy in the treatment ofovarian tumors spread to this site. However, the dosimetricanalysis discussed may be applied, with appropriate mod-ification, to other regions treated with a similar methodol-ogy.
Ovarian cancer is one of highest causes of mortalityamong gynecologic cancers in the western world. TheAmerican Cancer Society has estimated approximately19 000 new cases were diagnosed in 1986, of which 60% of
these will eventually die due to complications from thedisease.20 The malignancy originates in the ovaries and isgenerally detected during Stage III or IV of the disease,when it has metastasized to the surface of the peritoneum.At th is s tage , only a 10%-20% 5-year survival i spredicted. 2 0 Conventional treatment of this disease in-volves surgical debulking of the primary tumor, followedb y a r e g i m e n o f c h e m o t h e r a p y a n d / o r r a d i a t i o ntherapy2 1’2 2 to the regions at risk for spread. Because of thediffuse nature of peritoneal disease, treatment of the entireabdomen to 2500 cGy is prescribed with external beamradiation therapy.22 This dose is inadequate for gross dis-ease, but is limited by normal tissue tolerance of criticalabdominal and pelvic organs. In order to augment the ex-ternal beam dose, Au-198 colloids23 and radioactive chro-mic phosphate (P-32 colloids)24-26 have been administereddirectly into the peritoneal cavity for the treatment of ova-rian metastases. However, with lack of specificity, there isno tumor-to-normal tissue dose advantage.23-26 Thus a mo-dality is required in which a high dose of radiation is de-livered to tumor while limiting the dose to normal tissues.This is the goal of intraperitoneal radioimmunotherapy.
II. A CONCEPTUAL MODEL FOR IPRITDOSIMETRY
In principle, the dose to tumor and normal tissues maybe calculated if the concentration of radioactivity is knownin each volume element of the body as a function of time.In practice, such detailed knowledge is impossible to ob-tain. Nevertheless, the formulation of a simplified modelaids in identifying those factors which most significantlyinfluence the dose distribution and parameters which needto be measured to reliably estimate the dose.
593 Med. Phys. 20 (2). Pt. 2, Mar/Apr 1993 0094-2405/93/020593-08$01.20 © 1993 Am. Assoc. Phys. Med. 593

594 Roeske et al.: Dosimetry of radiolabeled antibodies 594
To conceptualize the biological distribution of activity,consider the following sequence of “events.” Initially, atherapeutic quantity of radiolabeled antibody is injectedinto a cavity of the body which contains the targeted ma-lignancy (i.e, peritoneal cavity). Antibody removal fromthe compartment and redistribution occurs through lym-phatic and blood circulatory systems.27-29 A fraction of theadministered antibodies will bind to antigens expressed onthe surface of tumor cells, and to a lesser degree, antigensexpressed on the surface of normal tissue cells. Because ofthe high affinity the antibody has for the antigen, penetra-tion within bulk disease may be limited to several celllayers. 2 9 At later times, activity which escapes from theperitoneal cavity into the blood may also accumulatewithin tumor through vascularization. The therapeutic ef-fect of the treatment will depend on the total dose to tumoras a function of depth, dose rate, and relative biologicaleffectiveness of the radiation.
A. Tumor and normal tissue geometry
Geometrical aspects of both tumor and normal tissue,such as size and shape, influence the dose to these tissues.There are two principle reasons why the tumor size andgeometry are important for accurate dosimetry. First, an-tibody uptake per gram of tumor is inversely proportionalto the tumor mass. Typically, the tumor to normal tissueratios for the accumulation of activity range from 0.1-8.5for large tumors, and from 2-8700 for small tumors. 4’ 6’ 7
Second, similar to external beam therapy, it is expected theshape of isodose curves within tumor will conform to theshape of the tumor. If the activity is uniformly distributedwithin tumor, the geometry will not be as critical. How-ever, for cases of nonuniform activity confined to the tu-mor periphery, as observed on tumor autoradiographs, thetumor geometry may significantly affect the degree towhich the tumor may be treated (see Sec. III C). Addi-tionally, the size of the tumor, in relation to the maximumrange of particulate radiation, will influence the degree ofdose uniformity.
Individual tumor cells or clusters of tumor cells in sus-pension in ascites define one geometrical condition. How-ever, in IPRIT of colorectal and ovarian carcinoma, thetargets are small metastases from 1 mm to 1 cm in diam-eter on the surface of the peritoneum. Lesions greater than2 cm are not considered since these are significantly moredifficult to control.8,9,11 Unlike external beam radiationtherapy, the geometry and the size distribution of the tar-get volumes are generally not well specified. Chatal et al.30
and Thedrez et al.31 have demonstrated small ovarian tu-mor nodules (<5 mm diameter) are nearly sphericalHowever, visual inspection of biopsy samples of peritonealtumor metastases shows the geometry may vary from theidealized spherical form.32 Laparoscopy may be performedprior to radioimmunotherapy to assess the volume of theresidual disease to be treated.8’9,11 This method may also beused to provide some insight into the tumor geometry.
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
FI G. 1. Schematic diagram of the initial source distribution followinginjection of radiolabeled antibody solution into peritoneal cavity. Theperitoneum is represented as a plane, and tumor extends both above andinto the peritoneal surface. Immediately following the infusion, the solu-tion is confined to the peritoneal cavity.
B. Dose components
Dose to individual tumor cells is due to radionuclideswhich decay within the maximum range of particulateemissions (alphas, betas, and Auger electrons), and poten-tially from all radionuclides which emit photon radiation.The three dose components to an arbitrary point in tumoror normal tissue include: (a) dose from solution activity,(b) dose from the radionuclide/antibody complex specifi-cally bound to the tissues, and (c) dose from activity ac-cumulating in other parts of the body after escape from theperitoneal cavity.
C. Solution activity
The dependence of dose from nuclear decays in the IPadministered solution as a function of tissue depth can beunderstood through a simple model. Consider the perito-neal cavity as semi-infinite plane, above which resides auniform solution of radiolabeled antibodies (Fig. 1). Thisapproximation is valid when the maximum range (Rm a x)of the particulate radiation (for example, Y-90-Rm a x=1.1cm) is much smaller than the radius of curvature of thesolution/tissue interface. Initially after infusion into theperitoneal cavity, most of the activity will be confined tothe peritoneal solution. Cells on the surface of the cavityreceive dose from those sources of particulate radiationwhich decay within Rm a x of the point of calculation. There-fore, these cells are irradiated from sources which decaywithin a hemisphere of radius Rmax as shown in Fig. 2.Cells deeper in the peritoneal tissue will receive a dosefrom a spherical segment which diminishes in volume withincreasing depth. Those cells which are at depths deeperthan Rm a x will not receive dose from the peritoneal sourcedistribution. The total dose which tumor and normal tis-sues receive from the solution activity will be proportionalto the number of decays within the spherical segmentabove the peritoneal surface. Hence, the critical parameterin calculating the peritoneal source component to the tu-mor dose will be the activity concentration in the perito-neal solution as a function of time.
The total quantity of radioisotope administered and theinfusion volume are parameters which are often specified inthe literature to describe the characteristics of the irradi-ating solution.1 - 1 2 For IPRIT, typical initial quantities of

595 Roeske et al.: Dosimetry of radiolabeled antibodies
FIG. 2. Diagram of the contribution of the solution activity to peritonealtumors/tissues. For cells located near the surface, the dose from solutionis due to sources which decay within a hemisphere of radius R max Cellslocated deeper within the peritoneal surface receive dose from thosesources which decay within a spherical segment. The volume of the spher-ical segment decreases with depth such that at a depth equal to themaximum range, there is no contribution of dose from the solutionactivity.
activity range from 100 to 157 mCi for I-131, and from 5 to20 mCi for Y-90 in 1.5 liters of normal saline. 11 However,in addition to the infusion volume, the total volume of fluidwithin the peritoneal cavity is crucial to provide an accu-rate estimate of the dose from the initial solution activity.
The solution activity as a function of time is a parameterwhich is potentially measurable. In theory, the peritonealfluid may be periodically sampled during therapy throughthe Tenckoff catheter. Additionally, the fluid activity mayalso be quantitated through serial conjugate views obtainedfrom a gamma camera. However, activity within surround-ing organs may obfuscate the peritoneal source distribu-tion. Another approach which is useful in determining thecumulated activity in the peritoneal fluid is through TLDmeasurements. Thermoluminescent dosimeters (TLDs)placed within the peritoneal cavity may provide a directdose measurement of the contribution of the peritonealsource distribution (see Sec. III A).
D. Tumor activity gradients
Radiolabeled antibodies accumulate preferentially intumor (Fig. 3), and can also cross react to antigens innormal tissue (nonspecific binding). Specific binding of ra-diolabeled antibodies provides the major component of thedose to the tumor cells. A critical parameter for dose esti-mation is the activity as a function of time and depth as-sociated with the tumor. When single cells in solution are
FIG. 3. Schematic diagram of the distribution of activity at time follow-ing infusion. A fraction of the activity which was originally in the in-traperitoneal solution has penetrated and bound to peritoneal tissues.
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
595
the targets, the activity as a function of time may be esti-mated through an in vivo assay. An aliquot of cells withinthe radiolabeled antibody solution is taken, spun down,and separated from the solution at various times andcounted. The production of a time activity curve may beutilized in calculating the dose to the nucleus due to theactivity on an individual cell, and if the emission has a longrange, due to the ensemble of activity from other cellswithin the volume.
The activity distributed in a solid tumor is nonuniformdue to the high affinity of the antibody, and the heteroge-neous expression of antigen.3 3’ 34 Studies by Dedrick andFlessner35 with radiolabeled serum albumin suggest thatbiological macromolecules diffuse into the parietal and vis-ceral tissues of the peritoneum to different depths, and itsconcentration versus depth is a function of both tissue typeand molecular weight. Experiments with colon carcinomaspheroids, irradiated in a solution of radiolabeled antibod-ies specific for carcinoembryonic antigen (CEA), show ac-tivity gradients are a maximum at the tumor surface withpenetration limited to l-3 cell layers.3 6
Tumor activity is often quantitated through gross bi-opsy samples. Tumor and normal tissue samples obtainedafter sufficient antibody localization have been counted in-tact in a well counter in numerous biodistribution studies.A quantity often quoted is the percent injected dose pergram of tumor (% I.D./g), which represents the percentof the injected activity which accumulates per gram oftumor. The percent injected dose per gram of tumor forintraperitoneally administered radiolabeled antibodies mayvary from 0.001% to 0.1%, or greater.6’7 This uptake is afunction of the size of the antibody (IgG, Fab’2, Fab),antibody affinity or avidity, and the mass of the tumor.3 7,3 8
While the percent injected dose/g is useful for comparisonof therapeutic effectiveness to indicate relative uptake, itprovides little information on the spatial or temporal dis-tribution of activity, which is essential for accurate tumordosimetry. Assumptions concerning the distribution of ac-tivity within the gross tissue samples must therefore bemade to utilize these data for dosimetry.
Animal experiments and tumor autoradiography mayprovide the spatial and temporal data on tumor and nor-mal tissue activity needed to calculate dose. However, aswith all animal experiments, extrapolation to man is diffi-cult and complex. Pharmacokinetic modeling, such aswork performed by Fujimori et al.39-41 and Baxter andJain, 4 2 has elucidated the distribution of activity withintumor models for intravenous administrations. These mod-els will be useful in assessing the dose from activity whichescapes into the blood and accumulates in the tumorthrough this pathway. Modifications to these calculationsmay also result in the ability to provide detailed models ofthe percolation of activity from the intraperitoneal solutioninto the tumor.
E. Physical characteristics of radionuclides
The physical characteristics of the radionuclidewhich influence the dose distribution include the half-life,energy of emissions and type of radiation. The physical

596 Roeske et al.: Dosimetry of radiolabeled antibodies 596
half-life in relation to the biological half-life of antibody dose to tumor for both clinical situations and based onremoval from the cavity will determine the fraction of dose theoretical tumor architectures and antibody source con-received from the injectate solution. If the physical half-life figurations.is long with respect to the rate of egress, the dose from thesolution may be minimal. However, if the physical half-lifeis short compared to the biological half-life, a large fraction III. CURRENT STATUS: MEASUREMENT ANDof the dose to the tumor will be from the radionuclides in CALCULATION OF TUMOR DOSE
approximately 3 days, while the time to reach a depth of
solution. Additionally, these sources will irradiate normalstructures within the cavity, and thus may provide a doselimiting criterion.
The distribution of antibody within tumor is due to mul-tiple processes.33,34 Consider a simple example in whichdiffusion is the dominating process. The time for an anti-body to uniformly infiltrate a tumor to a death of 1 mm is
A. Dose measurements
In the previous section, a conceptual model describedthe target specification and the distribution of radiolabeledantibody with respect to this target. This section will reportthe measurements and calculations of dose to tumor. Therole of each of these methods within the framework of theproposed model will be discussed.
2.5 mm is 18 days.3 4 Thus radionuclides with short halflives will decay near the periphery of the tumor, and thedose to deeper portions of the tumor from these emissionsmay be small. Longer lived radionuclides may provide amore uniform dose to tumor because a fraction of thesewill penetrate into the tumor before decaying. However,the use of a longer lived radionuclide also results in in-creased normal tissue dose.
It is also important to examine the depth of penetrationof antibody/radionuclide complex in relation to the rangeof the particulate radiation. For example, the depth dosecurve from energetic beta particles of Y-90 (Rm a x=1.1cm) is insensitive to antibody convection and diffusion onthe order of several hundred microns. The reason the depthdose curve does not vary significantly is because the depthof penetration represents a small fraction of the maximumrange (see Sec. III C). However, the microscopic depthdose distribution for alpha emitters (Rm a x<100µm) willbe strongly influenced by a penetration depth of severalhundred microns because this distance is much greaterthan the maximum range.
F. Activity throughout the body
In principle, the dose to tumor from the remainder ofthe body is negligible. For particulate emissions, only thosenormal tissues within the maximum particulate range willcontribute dose to the tumor. In the case of beta/gammaemitters such as I-131, the dose to tumor from the gammaemissions will most likely result in a constant backgrounddose. Estimates of the dose contribution from gamma emis-sions may be determined by using MIRD or image basedtreatment planning.
G. Summary of conceptual model
Measurements of dose to peritoneal tissues has been ex-plored principally through two methodologies. Direct mea-surement of dose with thermoluminescent dosimeters hasbeen investigated,8,11 where TLD chips are placed in a tubewhich is passed into the peritoneal cavity. The advantageof this technique is the cumulated dose is measured di-rectly. However, spatial resolution is limited as well asareas of access within the patient. Stewart et al. 8,11 r e -ported inserting 20-35 LiF TLD catheters into patientswith ovarian cancer at laparoscopy, prior to radioimmu-notherapy. The average nonspecific dose to the peritonealwall was estimated from these TLD readings at 374 cGy(or 2.88 cGy/mCi of I-131) for human antimouse anti-body (HAMA) negative patients, and 200 cGy (or 1.94cGy/mCi of I-131) were measured in HAMA positive pa-tients. These findings suggest that there may be increasedabsorption of I-131 in HAMA positive patients due to an-tibody dehalogenation. Y-90 labeled antibodies resulted inan average surface dose of 21.7 cGy/mCi of injectedactivity.” The variations in the absorbed dose per mCi ofinjected activity for I-131 and Y-90 are due to differencesin the effective half-life within the cavity and the energiesof the beta emissions. Within the previously discussedmodel, the TLD measurements provide a direct dose fromthe solution component at the peritoneal surface. However,no information regarding the contribution of the solutionactivity to the dose as a function of tissue depth is pro-vided.
There are several technical difficulties associated withthe use of TLDs. Dose measurements as described aboveprovide an average dose estimate and cannot differentiateeasily between dose to tumor or normal tissue. If the TLDis near the tumor mass, a high concentration of radiola-beled antibody (relative to the solution activity) on orwithin the tumor will increase the measured dose signal.Furthermore, since the peritoneal surface is convoluted,regions where the radius of curvature is of the same order
To summarize, the important parameters in estimatingthe dose to tumor are ( 1) the antibody/radionuclide solu-tion activity as a function of time; (2) the concentration ofactivity associated with the tumor as a function of time;and (3) the relative rate and depth of antibody penetrationwith respect to the half-life and range of particulate radi-ation. The following section describes the estimation of
of magnitude as the maximum range of the particulateemissions may result in a measured dose which differs fromthe average dose received by the surface. Additional infor-mation relating TLD position to the peritoneal source ge-ometry may be obtained by a CT scan. Visualization andextraction of peritoneal contours can be used to study thevariation of measured dose from the solution.
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

597 Roeske et al.: Dosimetry of radiolabeled antibodies 597
B. Activity measurements
Measurement of activity distributions within the patientas a function of time provides input information into theMIRD formalism to permit calculation of dose.5,8-12,43,44
Dose to tumor can be calculated from the quantitation of% ID/g in gross biopsy samples previously discussed. Theassumption that the activity is uniformly distributedthroughout the tumor mass is frequently made. For exam-ple, Hnatowich et al.1 0 estimated the absorbed dose froman Y-90 labeled antibody to several peritoneal tissues basedon activity measurements of tissue biopsies. Assuming thetumor associated activity decayed in place from the time ofadministration, these calculations yielded dose estimates of48 cGy/mCi for tumor. Since these measurements arebased on a 1 mCi administration of the radiolabeled anti-body, the activity required to deliver a therapeutic dose(~50Gy) is approximately 100 mCi.
There are several limitations with this type of tumordose estimate. First, as Hnatowich et al.10 discuss, the as-sumption of instantaneous uptake in the tumor results inan overestimate of the cumulated activity, and hence over-estimates the absorbed dose. This assumption results in anunderestimate of the therapeutic quantities of isotopeneeded for therapy, as in the above example. Second, ac-tivity measurements are made and normalized to the massof tissue sampled. If an average value of the percent in-jected dose per gram is used, tumors smaller or larger thanthe average tumor size will have larger and smaller valuesof the percent injected dose per gram, respectively. Thusthe dose estimates will also be inaccurate. Third, the mostsignificant limitation of these dose studies is the assump-tion that activity within the tumor is uniform. If the activ-ity is located primarily near the periphery of the tumor, theouter portions of the tumor will receive a higher dose thanthe central portions. However, while these types of calcu-lations are inaccurate, they are simple to perform and thebiological data (tumor activity) are readily available. Ad-ditionally, since these calculations provide an upper tumordose limit, they are useful in determining if the adminis-tered quantities of radiolabeled antibody provide doseswhich are within therapeutic ranges.
C. Calculation/dose modeling
IPRIT dose modeling on the multicellular scale hasbeen applied by several groups45-48 to study the distribu-tion of dose within tumor and normal tissues. Unlike ex-ternal photon beam treatment planning and modeling(where parameters of the model yield relatively accuratedose distributions), lack of detailed knowledge of the spa-tial distribution of activity on a very small geometric scaleprevents accurate calculation of dose in the peritoneum.However, modeling permits the examination of those pa-rameters which affect the isodose distribution and providesan understanding of how these parameters should be al-tered to improve the dose distribution.
The scale of dose modeling is chosen to be of the sameorder of magnitude of the maximum range of particulateradiation from the radionuclide decay. Thus distance scales
range from 50 µm for alpha particle dose calculations to 1cm for beta emissions. The source distribution is dividedinto voxels of uniform activity, and the contribution ofeach volume element to the calculation point is computedby multiplying the number of decays in the volume elementby the appropriate value of the dose point kemel. 45-50 Thedose point kernel represents the distribution of dose as afunction of radial position from a point source emitter.Details of the dose point kernel will be discussed in a sep-arate paper in this issue. Dose calculations are performedthrough a superposition process and the computation timemay be reduced by realizing the dose computation processis a convolution process when the medium is homoge-neous. This realization allows for the use of fast Fourierconvolution. 4 8
Bardies et al.45,46 modeled ovarian carcinomas as smallspherical nodules with a high uptake of radiolabeled anti-body on the surface. Both the average dose to the sphereand the dose as a function of radial position were com-puted for a number of beta emitters considered useful forradioimmunotherapy. Comparison of the average doseand dose distribution as a function of radial positionshowed that the mean absorbed dose rate within a tumor isa misleading quantity, since the dose rate varies as a func-tion of distance within the tumor. Bardies extended thecalculations to alpha emitting radionuclides to spheroids ofradii of 5-200 µm.4 6 The results of these calculationsshowed that tumor dose is highly nonuniform. The calcu-lations also showed that the optimal alpha particle energyfor small spherical cells (5 µm radius) is 2-3 MeV, whilethe optimal energy for 200 µm spheres is more than 10MeV.
Watson et al.47 presented a method for calculating thedose as a function of depth to the peritoneal surface for theplanar geometry. Dose calculations for the planar geome-try can be traced to Loevinger et al. 49 who originally pre-sented methods for calculating the dose as a function ofdepth to a planar surface from an infinite planar source.Berger 5 0 extended the work of Loevinger and tabulatedinformation of the energy dissipation of electrons and com-mon beta emitters in various media. Watson et a1. 47 devel-oped a program which uses the work of Berger49 in MIRDPamphlet No. 7 for the case when the source is uniformlydistributed over the surface in a thin layer. For volumetricactivity distributions above the plane, the contribution ofinfinitely thin layers is integrated according to the methodof Loevinger et a1.,49 and the attenuation of the emissionswithin the source distribution is taken into account. Tableswere produced for activity confined to a semi-infinite plane(intraperitoneal solution) and for activity localized on thesurface of a plane (peritoneal surface). By using the ap-propriate combination of cumulated volumetric and sur-face activities, the dose as a function of depth to a planartumor may be calculated. For each of these dose compo-nents, the dose is a maximum at the peritoneal surface, anddecreases rapidly with depth. Typically, the dose decreasesto 50% of the maximum surface dose within 0.1-0.3 R max.
Absolute (versus relative) dose calculations for in-traperitoneal administration of radiolabeled ‘antibodies
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
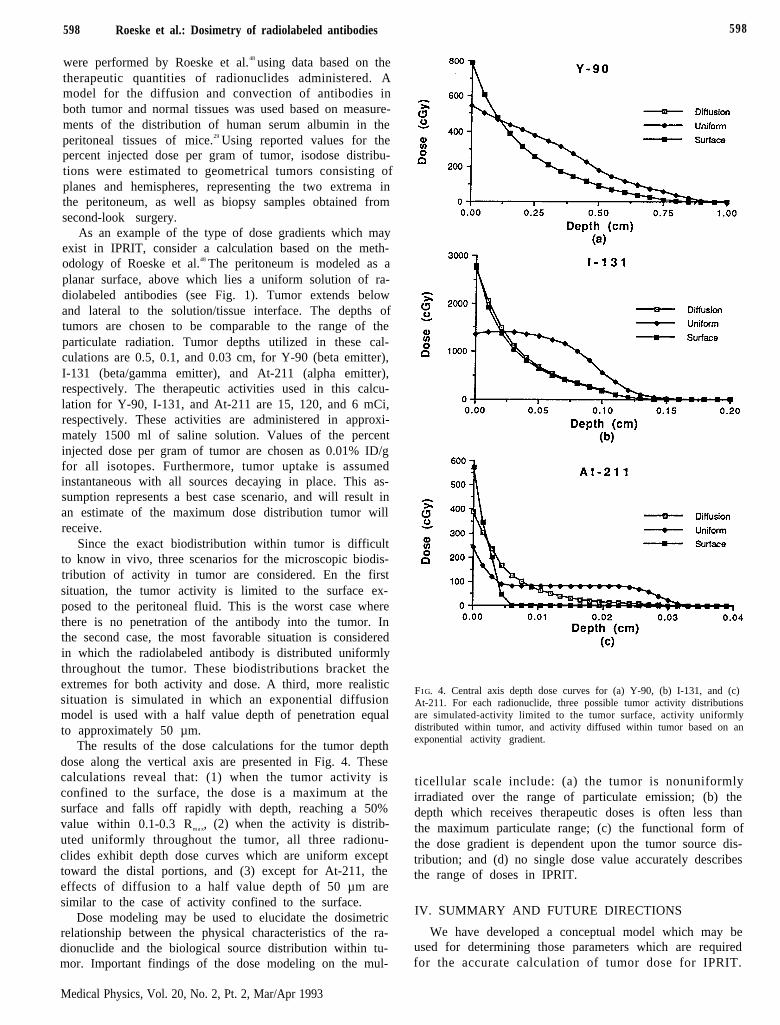
598 Roeske et al.: Dosimetry of radiolabeled antibodies 598
were performed by Roeske et al.48 using data based on thetherapeutic quantities of radionuclides administered. Amodel for the diffusion and convection of antibodies inboth tumor and normal tissues was used based on measure-ments of the distribution of human serum albumin in theperitoneal tissues of mice.29 Using reported values for thepercent injected dose per gram of tumor, isodose distribu-tions were estimated to geometrical tumors consisting ofplanes and hemispheres, representing the two extrema inthe peritoneum, as well as biopsy samples obtained fromsecond-look surgery.
As an example of the type of dose gradients which mayexist in IPRIT, consider a calculation based on the meth-odology of Roeske et al.48 The peritoneum is modeled as aplanar surface, above which lies a uniform solution of ra-diolabeled antibodies (see Fig. 1). Tumor extends belowand lateral to the solution/tissue interface. The depths oftumors are chosen to be comparable to the range of theparticulate radiation. Tumor depths utilized in these cal-culations are 0.5, 0.1, and 0.03 cm, for Y-90 (beta emitter),I-131 (beta/gamma emitter), and At-211 (alpha emitter),respectively. The therapeutic activities used in this calcu-lation for Y-90, I-131, and At-211 are 15, 120, and 6 mCi,respectively. These activities are administered in approxi-mately 1500 ml of saline solution. Values of the percentinjected dose per gram of tumor are chosen as 0.01% ID/gfor all isotopes. Furthermore, tumor uptake is assumedinstantaneous with all sources decaying in place. This as-sumption represents a best case scenario, and will result inan estimate of the maximum dose distribution tumor willreceive.
Since the exact biodistribution within tumor is difficultto know in vivo, three scenarios for the microscopic biodis-tribution of activity in tumor are considered. En the firstsituation, the tumor activity is limited to the surface ex-posed to the peritoneal fluid. This is the worst case wherethere is no penetration of the antibody into the tumor. Inthe second case, the most favorable situation is consideredin which the radiolabeled antibody is distributed uniformlythroughout the tumor. These biodistributions bracket theextremes for both activity and dose. A third, more realisticsituation is simulated in which an exponential diffusionmodel is used with a half value depth of penetration equalto approximately 50 µm.
The results of the dose calculations for the tumor depthdose along the vertical axis are presented in Fig. 4. Thesecalculations reveal that: (1) when the tumor activity isconfined to the surface, the dose is a maximum at thesurface and falls off rapidly with depth, reaching a 50%value within 0.1-0.3 Rm a x, (2) when the activity is distrib-uted uniformly throughout the tumor, all three radionu-clides exhibit depth dose curves which are uniform excepttoward the distal portions, and (3) except for At-211, theeffects of diffusion to a half value depth of 50 µm aresimilar to the case of activity confined to the surface.
Dose modeling may be used to elucidate the dosimetricrelationship between the physical characteristics of the ra-dionuclide and the biological source distribution within tu-mor. Important findings of the dose modeling on the mul-
FIG. 4. Central axis depth dose curves for (a) Y-90, (b) I-131, and (c)At-211. For each radionuclide, three possible tumor activity distributionsare simulated-activity limited to the tumor surface, activity uniformlydistributed within tumor, and activity diffused within tumor based on anexponential activity gradient.
ticellular scale include: (a) the tumor is nonuniformlyirradiated over the range of particulate emission; (b) thedepth which receives therapeutic doses is often less thanthe maximum particulate range; (c) the functional form ofthe dose gradient is dependent upon the tumor source dis-tribution; and (d) no single dose value accurately describesthe range of doses in IPRIT.
IV. SUMMARY AND FUTURE DIRECTIONS
We have developed a conceptual model which may beused for determining those parameters which are requiredfor the accurate calculation of tumor dose for IPRIT.
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

599 Roeske et al.: Dosimetry of radiolabeled antibodies 599
Based on this model and the work of those in the field,there are certain parameters which are required to providea crude dose estimate. The first quantity which is impor-tant is the concentration of antibody solution within thecavity as a function of time. This quantity is necessary notonly for tumor dosimetry, but is also the major componentin normal tissue dosimetry within the peritoneum. The so-lution activity as a function of time may be quantitated bysampling the peritoneal fluid periodically, or the dose com-ponent may be measured directly through the insertion ofTLDs. However, certain caveats must be considered in theinterpretation of TLD measurements. The use of CT todefine the patient specific geometry in relation to the TLDcatheter may be useful in this interpretation of dose mea-surements.
A second important parameter is the dose from activityassociated with tumor. At present, this quantity is oftenestimated by measuring the activity per gram of tumor at agiven time, and assuming the activity is due to the physicaldecay of isotope from t=O. This tumor dose calculationwill provide an overestimate because of the assumption ofinstantaneous uptake. Biodistribution data, such as the tu-mor activity as a function of mass and time, may be ob-tained from animal studies. However, this dose calculationis ultimately limited by the assumption of uniform activitythroughout the tumor. Nevertheless, this measurementprovides a relative measurement of dose and may be usefulin assessing if the tumor dose is within the therapeuticrange.
The above recommendations represent minimum dosi-metric requirements. However, the role of dosimetry inIPRIT is ultimately (1) to aid in the rational interpreta-tion of the therapeutic response (i.e., why one patient re-sponds favorably and another does not for the same in-j e c t e d a c t i v i t y ) a n d ( 2 ) t o s u g g e s t m e t h o d s f o roptimization. This type of detailed analysis will require themore advanced dose calculation tools developed for exter-nal beam radiation therapy such as 3-D dose calculationsand dose volume histograms. Using dose point kernels,three-dimensional dose distribution may be calculated forany specified tumor geometry and source configuration.The methods of Fujimori et al.39-41 may be applied to IPtherapy with proper modification to yield more accurateactivity gradients within tumor. These biological modelsmay also be used in conjunction with measured data, suchas the percent injected dose per gram of tumor, to provideverification of the models. Dose verification on the multi-cellular scale may be performed through microthinTLDs.51 Originally applied to quantify autoradiographs,these TLD rods are sectioned to have dimensions of 20×200×400 µm. The careful implantation of these TLDcatheters into areas of tumor and normal tissue may pro-vide an in vivo verification of the dose as a function ofdistance from the solution/tissue interface.
Methods of optimization required to make therapymore effective may be elucidated from the depth dosecurves presented in Fig. 4. Therapy will be effective only ifa uniform dose can be delivered to the tumor. This unifor-mity will not result from the proper selection of radionu-
clide energies, but will be brought about by uniform anti-body permeation throughout the tumor. Biologists andimmunologists will need to develop antibodies which havea high specificity, yet retain the ability to penetrate tumor.Since this request may be unreasonable, novel approachesto delivery will need to be developed. These methods in-clude the use of dose fractionation and the use of antibody“cocktails” in which a variety of antibodies and radionu-clides are used to provide a more uniform dose. The chal-lenge of dosimetry will be to develop methods to accuratelycalculate and verify dose distributions for these complexsource configurations.
ACKNOWLEDGMENTS
John C. Roeske gratefully acknowledges the support ofUPSHS Grant T32 CA09649. George T. Y. Chen andJohn C. Roeske wish to acknowledge the generosity of theRice Foundation, Chicago, IL and the Center for Radia-tion Therapy, Chicago, IL.
1J. Malamitsi, D. Skarlos, S. Fotiou, P. Papakostas, G. Aravantinos, D.Vassilarou, J. Taylor-Papadimitriou, K. Koutoulidis, G. Hooker, D.Snook, and A. Epenetos, “Intracavity use of two tumor associatedmonoclonal antibodies,” J. Nucl. Med. 29, 1910-1915 (1988).
2G. Rowlinson, D. Snook, A. Busza, and A. Epenetos, “Antibody-guided localization of intraperitoneal tumors following intraperitonealor intravenous administration,” Cancer Res. 47, 6528-6531 (1987).
3N. J. Finkler, M. G. Muto, A. I. Kassis, K. Weadock, S. S. Tumeh, V.R. Zurawski, and R. C. Knapp, “Intraperitoneal radiolabeled OC 125in patients with advanced ovarian cancer,” Gynecol. Oncol. 34, 339-344 (1989).
4J. F. Chatal, J. C. Saccavini, J. F. Gestin, P. Thedrez, C. Curtet, M.Kremer, D. Gurreau, D. Nolibe, P. Fumoleau, and Y. Guillard, “Bio-distribution of indium-111 labeled monoclonal antibody after intraperi-toneal injection in nude mice intraperitoneally grafted with ovariancarcinoma,” Cancer Res. 49, 3081-3086 (1989).
5A. A. Epenetos, G. Hooker, T. Krausz, D. Snook, W. Bodmer, and J.Taylor-Papadimitriou, “Antibody-guided irradiation of malignant as-cites in ovarian cancer: A new therapeutic method possessing specificityagainst cancer cells,” Obst. Gynecol. (supplement) 68, 71S-74S(1986).
6H. Haisma, K. Moseley, A. Battaile, T. C. Griffiths, and R. C. Knapp,“Distribution and pharmacokinetics of radiolabeled monoclonal anti-body OC 125 after intravenous and intraperitoneal administration ingynecologic tumors,” Am. J. Obstet. Gyncol. 159, 4218-4224 ( 1987).
7D. Colcher, J. Esteban, J. A. Carrasquillo, P. Sugarbaker, J. C. Rey-nolds, G. Bryant, S. M. Larson, and J. Schlom, “Complementation ofintracavitary and intravenous administration of a monoclonal antibody(B72.3) in patients with carcinoma,” Cancer Res. 47, 4218-4224(1987).
8J. S. Stewart, V. Hird, D. Snook, M. Sullivan, G. F. Hooker, N.Courtenay-Luck, G. Sivolapenko, M. Griffiths, M. J. Myers, H. E.Lambert, A. J. Munro, and A. A. Epenetos, “Intraperitoneal radioim-munotherapy for ovarian cancer: Pharmacokinetics, toxicity, and effi-cacy of I-131 labeled monoclonal antibodies,” Int. J. Radiat. Oncol.Biol. Phys. 16, 405-413 (1989).
9A. A. Epenetos, A. J. Munro, S. Stewart, R. Rampling, H. E. Lambert,C. G. McKenzie, P. Soutter, A. Rahemtulla, G. Hooker, G. B. Sivol-apenko, D. Snook, N. Courtenay-Luck, B. Dhokia, T. Krausz, J.Taylor-Papadimitriou, H. Durbin, and W. F. Bodmer, “Antibody-guided irradiation of advanced ovarian cancer with intraperitoneallyadministered radiolabeled monoclonal antibodies,” J. Clin. Oncol. 5,1890-1899 (1987).
1 0D. J. Hnatowich, M. Chinol, D. A. Siebecker, M. Gionet, P. W.Doherty, R. Hunter, and K. Kase, “Patient biodistribution of intraperi-toneally administered yttrium-w-labeled antibody,” J. Nucl. Med. 29,1428-1434 (1988).
11J. Stewart, V. Hird, D. Snook, M. Sullivan, M. J. Myers, and A. A.Epenetos, “Intraperitoneal I-131 and Y-90 labelled monoclonal anti-
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
600 Roeske et al.: Dosimetry of radiolabeled antibodies 600
bodies for ovarian cancer: Pharmacokinetics and normal tissue dosim-etry,” Int. J. Radiat. Oncol. Biol. Phys. 16, 405-413 (1989).
12B. G. Ward, S. J. Mather. J. H. Shepherd, K. E. Britton, M. Gra-nowska, and M L. Slevin, “Response to prospects for antibody-targeted radiotherapy of cancer,” Lancet 2, 580-581 (1986).
13D. Colcher, J. Esteban, J. A. Carrasquillo. P. Sugarbaker, J. C. Rey-nolds, G. Bryant, S. M. Larson, and J. Schlom, “Comparison of routeof administration of radiolabeled monoclonal antibodies in patientswith colorectal cancer,” J. Nucl. Med. 27(6), 902 (1986).
14P. Riva, S. Lazzari, M. Agostini, G. Sarti, G. Mosentelli, A. Pagenelli,L. Rasciti, and A. Siccardi, “The intraperitoneal administration of ra-diolabelled monoclonal antibodies for the diagnosis and therapy of co-lon cancer,” J. Nucl. Med. 29(5), 762 (1988) (Abstract).
15L. S. Lashford, A. G. Davies, R. B. Richardson, S. P. Bourne, J. A.Bullimore, H. Eckert, J. T. Kemstead, and H. B. Coakham, “A pilotstudy of I-131 monoclonal antibodies in the therapy of leptomeningealtumours,” Cancer 58, 573-583 (1986).
16W. T. Miller and A. Barrett, “Dosimetric model for antibody targetedradionuclide therapy and tumor cells in cerebrospinal fluid,” CancerRes. (Supplement) 50, 1043S-1048S (1990).
17D. Pectasides, S. Stewart, N. Courtenay-Luck, R. Rampling, A. J.Munro, T. Krausz, B. Dhokia, D. Snook, G. Hooker, H. Durbin, J.Taylor-Papadimitriou, W. F. Bodmer, and A. A. Epenetos, “Antibody-guided irradiation of malignant pleural and pericardial effusions,” Br.J. Cancer 5, 727-732 (1986).
18N. Courtenay-Luck, A. A. Epenetos, K. E. Halnan, G. Hooker, J. M.B. Hughes, T. Krausz, J. Lambert, J. P. Lavender, W. G. MacGregor,C. J. McKenzie, A. Munro, M. J. Myers, J. S. Orr, E. E. Pearse, D.Snook, B. Webb, J. Burchell, H. Durbin, J. Kemstead, and J. Taylor-Papadimitriou, “Antibody-guided irradiation of malignant lesions:Three cases illustrating a new method of treatment,” The Lancet 1,1441-1443 (1984).
19P. Riva, A. Arista, G. Mariani, E. Seccamani, S. Lazzari, G. Mosca-telli, C. Sturiale, G. Sarti, G. Franceschi, A. Spinelli, G. Vecchietti, N.Riva, P. Natali, and L. Zardi, “Improved tumour targeting by directintralesional injection of radiolabeled monoclonal antibody: A phase Istudy in brain glioma,” J. Nucl. Med. 32, 922 (1991).
20R. F. Ozols and R. C. Young, “Ovarian cancer,” Cur. Prob. Cancer 11,37-122 (1987).
21Z. Fuks, J. Yahalom, and H. Brenner, The Treatment of Carcinoma ofthe Ovary in a Radiation Therapy of Gynecologic Cancers (Alan R. Liss,New York, 1987).
22J. Horyon and T. Caputo, Gynecologic Cancer in Clinical Oncology (W.B. Saunders, New York, 1977).
23G. A. Andrews, S. Root, H. D. Kerman, and R. R. Bigelow, “Intrac-avitary colloidal radiogold in the treatment of effusion caused by ma-lignant neoplasm,” Ann. Surg. 137, 375-381 (1953).
24E. Boye, M. W. Lindegoard, E. Paus, A. Skretting, M. Davy, and E.Jacobsen, “Whole-body distribution of radioactivity after intraperito-neal administration of P-32 colloids,” Br. J. Radiol. 57, 395-402(1984).
25J. L. Currie, F. Bagne, C. Harris, D. L. Sullivan, E. A. Suruit, R. H.Wilkinson, and W. T. Creasman, “Radioactive chromic phosphate sus-pension: Studies on distribution, dose absorption and effective thera-peutic radiation in phantoms, dogs and patients,” Gynecol. Oncol. 12,193-218 (1981).
26R. J. Ott, M. A. Flower, A. Jones, and V. R. McCready, “The appli-cation of SPET to determine the radiation dose from P-32-chromicphosphate therapy of the peritoneal cavity,” Euro. J. Nucl. Med. 11,305-308 (1985).
27B. Rippe and G. Stelin, “Simulations of peritoneal solute transportduring CAPD. Application of the two-pore formalism,” Kidney Int.35, 1234-1244 (1989).
28M. F. Flessner, R. L. Dedrick, and J. S. Schultz, “Exchange of mac-romolecules between peritoneal cavity and plasma,” Am. J. Physiol.248, H15-H25 (1985).
29M. F. Flessner, J. D. Fenstermacher, R. G. Blasberg, and R. L. De-drick, “Peritoneal absorption of macromolecules studied by quantita-tive autoradiography,” Am. J. Physiol. 248, H26-H32 (1985).
30J. F. Chatal, J. C. Saccavini, J. F. Gestin, P. Thedrez, C. Curtet, M.Kremer, D. Guerrcau, D. Nobile, P. Fumoleau, and Y. Guillard, “Bio-distribution of indium-111-labeled OC 125 monoclonal antibody in-traperitoneally injected into patients operated on for ovarian carcino-mas,” Cancer Res. 49, 3087-3094 (1989).
31P. Thedrez J. C Saccavini. D. Nolibe. J. P. Simoen, D. Guerreau, I. F.Gestin, C. Curtet, M. Kremer, and J. F. Chatal, “Biodistribution ofindium-111-labeled OC 125 monoclonal antibody after intraperitonealinjection in nude mice intraperitoneally grafted with ovarian carcino-mas,” Cancer Res. 49, 3081-3086 (1989).
3 2J. Rotmensch, J. Roeske, G. Chen, C. Pelizzati, A. Montag, R.Weichselbaum, and A. L. Herbst, “Estimates of dose to intraperitonealmicrometastases from alpha and beta emitter in radioimmunotherapy,”Gynecol. Oncol. 38, 478-485 (1990).
33L. M. Cobb, “Intratumor factors influencing the access of antibody totumour cells,” Cancer Immunol. Immunother. 28, 235-240 (1989).
34R. K. Jain “Physiological barriers to delivery of monoclonal antibodiesand other macromolecules in tumors,” Cancer Res. (Supplement) 50,814S-819S (1990).
35L Dedrick and M. F. Flessner, “Pharmacokinetic considerations onmonoclonal antibodies,” Immunity Cancer 2, 429-438 ( 1989).
3 6C. A. Sutherland, J. O. Davis, G. M. Stirrat, F. Buchegger, M.Schreyer, A. Vacca, and J. P. Mach, “Penetration and binding of ra-diolabeled anti-carcinoembryonic antigen monoclonal antibodies andtheir antigen binding fragments in human colon multicellular sphe-roids,” Cancer Res. 47, 1627-1633 (1987).
37G. D. Thomas, M. J. Chappell, P. W. Dykes, D. B. Ramsden, K. R.Godfrey, J. R. M. Ellis, and A. R. Bradwell, “Effect of dose, molecularsize, affinity, and protein binding on tumor uptake of antibody orligand: A biomathematical model,” Cancer. Res. 49, 3290-3296(1989).
38L. E. Williams, R. B. Duda, R. T. Proffitt, B. G. Beatty, J. D. Beatty,J. Y. C. Wong, J. E. Shively, and R. Paxton, “Tumor uptake as a modelof tumor mass: A mathematical model,” J. Nucl. Med. 29, 103-109(1988).
39K. Fujimori, D. G. Covell, J. E. Fletcher, and J. N. Weinstein, “Mod-eling analysis of the global and microscopic distribution of Immuno-globulin G, F(ab’)2 and Fab in tumors,” Cancer Res. 49, 5656-5663(1989).
40K. Fujimori, D. G. Covell, J. E. Fletcher, and J. N. Weinstein, “Amodeling analysis of monoclonal antibody percolation through tumors:a binding site barrier,” J. Nucl. Med. 31, 1191-1198 (1990).
41K. Fujimori, D. Fisher, and J. N. Weinstein, “Integrated microscopic-macroscopic pharmacology of monoclonal antibody radioimmunocon-jugates: The radiation dose distribution,” Cancer Res. 51, 4821-4827(1991).
42L. T. Baxter and R. K. Jain, “Transport of fluid molecules in tumors:I. Role of interstitial pressure and convection,” Microvasc. Res. 48,77-109 (1989).
43M. J. Myers, A. A. Epenetos, and G. Hooker, “Practical assessment ofradiation doses using labelled antibodies for therapy,” Nucl. Med. Biol.13(4), 437-446 (1986).
44M. J. Myers, G. R. Hooker, and A. A. Epenetos, “Dosimetry of radi-olabeled monoclonal antibodies used for therapy,” in Proceedings of theFourth International Radiopharmaceutical Dosimetry Symposium (OakRidge, TN, Conf-851113, 1985).
45M. Bardies, J. Lame, M. J. Myers, and J. P. Simoen, “A simplifiedapproach to beta dosimetry for small spheres labelled on the surface,”Phys. Med. Biol. 35, 1039-1050 (1990).
46M. Bardies and M. J. Myers, “A simplified approach to alpha dosim-etry for small spheres labelled on the surface,” Phys. Med. Biol.35(11), 1551-1561 (1990).
47E. E Watson, M. G. Stabin, J. L. Davis and K. F. Eckerman, “Amodel of the peritoneal cavity for use in internal dosimetry,” J. Nucl.Med. 30, 2002-2011 (1989).
48J. C. Roeske, G. T. Y. Chen, R. W. Atcher, C. A. Pelizzari, J. Rot-mensch, D. Haraf, A. Montag, and R. R. Weichselbaum, “Modeling ofdose to tumor and normal tissue from intraperitoneal radioimmuno-therapy with alpha and beta emitters,” Int. J. Radiat. Oncol. Biol.Phys. 19(6), 1539-1548 (1990).
49R Loevinger, E. Japha, and G. Brownell, Radiation Dosimetry (Aca-demic, New York, 1958).
50M. Berger, “Distribution of absorbed dose around point sources ofelectrons and beta particles in water and other media,” MIRD Pam-phlet No. 7, J. Nucl. Med. (Supplement 5) (1971).
“M. H. Griffith, E. D. Yorke, B. W. Wessels, G. L. DeNardo, and W. P.Neacy, “Direct dose confirmation of quantitative autoradiography withmicro-TLD measurements for radioimmunotherapy,” J. Nucl. Med.29, 1795-1809 (1988).
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

Radiobiology of radiolabeled antibody therapy as appliedto tumor dosimetry
V. K. Langmuira)
Life Sciences Division, SRI International, 333 Ravenswood Avenue. Menlo Park, California 94025
J. F. FowlerDepartments of Human Oncology and Medical Physics, University of Wisconsin Clinical Cancer Center,600 Highland Avenue, Madison, Wisconsin 53792
S. J. KnoxDepartment of Radiation Therapy, Stanford University Hospital, Stanford, California 94305
B. W. WesselsDivision of Radiation Oncology and Biophysics, George Washington University Medical Center,901 23rd Street, N. W. Washington, DC 20037
R. M. SutherlandLife Sciences Division, SRI International, 333 Ravenswood Avenue, Menlo Park, California 94025
J. Y. C. WongDivision of Radiation Oncologv. City of Hope National Medical Center, 1500 East Duarte Road, Duarte,California 91010
(Received 18 March 1992; accepted for publication 24 July 1992)
This paper reviews the radiobiological aspects of radioimmunotherapy (RIT) with radiolabeledantibodies, including comparisons between RIT and external beam irradiation. The effectivenessof cell killing by radiation decreases with the dose rate and the rate of decrease is determined bythe size of the shoulder on the radiation survival curve. Tumors with poor repair capabilitiesexhibit less of a dose rate effect than tumors with good repair capabilities. Continued tumor cellproliferation during treatment occurs at very low dose rates and can contribute to the reducedeffectiveness of low dose rate radiation. Toxicity to normal tissues will determine the total doseof radiolabeled antibody that can be given and this will be influenced by the choice of both theradionuclide and the antibody. The reported enhanced effectiveness of RIT may be due tomultiple factors including selective targeting of cells responsible for tumor volume doubling,tumor surface binding rather than homogeneous binding throughout the tumor volume, target-ing of the tumor vasculature, or block of cell cycle progression in G 2. During RIT, there is lesstime for reoxygenation of hypoxic tumor cells than during a course of conventional externalbeam radiotherapy. It has not yet been determined whether this will have a detrimental effect onRIT. Probably the most important factor in the success of RIT is dose heterogeneity. Any viableportion of a tumor that is not targeted and does not receive a significant radiation dose willpotentially lead to treatment failure, no matter how high the dose received by the remainder ofthe tumor. Comparisons between RIT and external beam radiation have shown a wide range ofrelative efficacy. Tumors most likely to respond to RIT are tumors with poor repair capabilities,tumors that are susceptible to blockage in radiosensitive phases of the cell cycle, tumors thatreoxygenate rapidly, and tumors that express the relevant antigen homogeneously. From aradiobiological perspective, it appears that RIT alone is unlikely to cure many tumors and thatcombination with other treatment modalities will be essential.
I. INTRODUCTION
Most of the predictions of the radiobiological aspects ofradiolabeled antibody therapy are based on studies of con-tinuous low dose rate (LDR) or fractionated irradiationgiven by external beam. A majority of these studies weredone at dose rates that are higher than the dose ratesachieved during radioimmunotherapy (RIT) and the doserates were constant rather than exponentially decreasing,as is the case in RIT. This section will discuss what isknown about the radiobiology of LDR irradiation and RITas applied to tumor dosimetry and discuss comparisonsbetween the two. Normal tissue radiobiology, although
very important, will only be peripherally addressed herefor continuity. More complete discussions can be found inRefs. 1-5.
II. REPAIR OF RADIATION DAMAGE
In general, the effectiveness of cell killing by radiationdecreases with decreasing dose rate6 (see Fig. 1). In vitro,the dose rate effect appears to correlate best with the initialportion of the acute radiation survival curve (single frac-tion high dose rate). As the initial slope decreases, or asthe shoulder widens, the dose rate effect increases. Fromthe linear-quadratic model, this would imply that as single-
601 Med. Phys. 20 (2), Pt. 2, Mar/Apr 1993 0094-2405/93/020601-10$01.20 © 1993 Am. Assoc. Phys. Med. 601
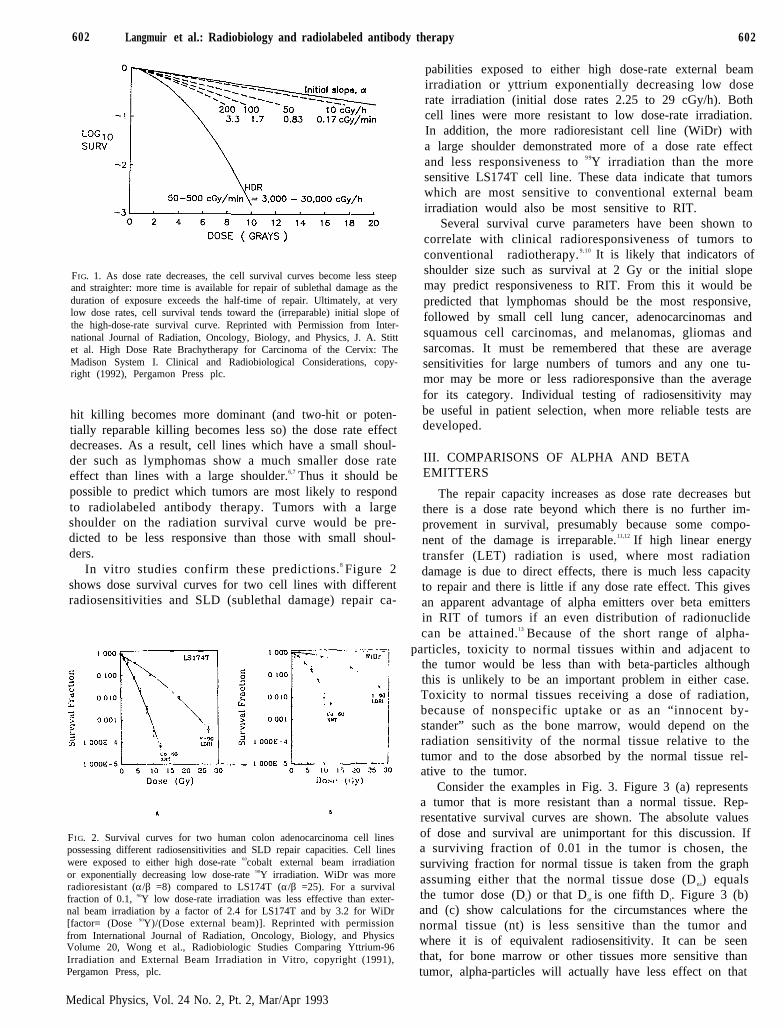
602 Langmuir et al.: Radiobiology and radiolabeled antibody therapy 602
FIG. 1. As dose rate decreases, the cell survival curves become less steepand straighter: more time is available for repair of sublethal damage as theduration of exposure exceeds the half-time of repair. Ultimately, at verylow dose rates, cell survival tends toward the (irreparable) initial slope ofthe high-dose-rate survival curve. Reprinted with Permission from Inter-national Journal of Radiation, Oncology, Biology, and Physics, J. A. Stittet al. High Dose Rate Brachytherapy for Carcinoma of the Cervix: TheMadison System I. Clinical and Radiobiological Considerations, copy-right (1992), Pergamon Press plc.
hit killing becomes more dominant (and two-hit or poten-tially reparable killing becomes less so) the dose rate effectdecreases. As a result, cell lines which have a small shoul-der such as lymphomas show a much smaller dose rateeffect than lines with a large shoulder.6,7 Thus it should bepossible to predict which tumors are most likely to respondto radiolabeled antibody therapy. Tumors with a largeshoulder on the radiation survival curve would be pre-dicted to be less responsive than those with small shoul-ders.
In vitro studies confirm these predictions.8 Figure 2shows dose survival curves for two cell lines with differentradiosensitivities and SLD (sublethal damage) repair ca-
FIG. 2. Survival curves for two human colon adenocarcinoma cell linespossessing different radiosensitivities and SLD repair capacities. Cell lineswere exposed to either high dose-rate 60cobalt external beam irradiationor exponentially decreasing low dose-rate 90Y irradiation. WiDr was moreradioresistant (α/β =8) compared to LS174T (α/β =25). For a survivalfraction of 0.1, 90Y low dose-rate irradiation was less effective than exter-nal beam irradiation by a factor of 2.4 for LS174T and by 3.2 for WiDr[factor= (Dose 90Y)/(Dose external beam)]. Reprinted with permissionfrom International Journal of Radiation, Oncology, Biology, and PhysicsVolume 20, Wong et al., Radiobiologic Studies Comparing Yttrium-96Irradiation and External Beam Irradiation in Vitro, copyright (1991),Pergamon Press, plc.
Medical Physics, Vol. 24 No. 2, Pt. 2, Mar/Apr 1993
pabilities exposed to either high dose-rate external beamirradiation or yttrium exponentially decreasing low doserate irradiation (initial dose rates 2.25 to 29 cGy/h). Bothcell lines were more resistant to low dose-rate irradiation.In addition, the more radioresistant cell line (WiDr) witha large shoulder demonstrated more of a dose rate effectand less responsiveness to 9 9Y irradiation than the moresensitive LS174T cell line. These data indicate that tumorswhich are most sensitive to conventional external beamirradiation would also be most sensitive to RIT.
Several survival curve parameters have been shown tocorrelate with clinical radioresponsiveness of tumors toconventional radiotherapy.9,10 It is likely that indicators ofshoulder size such as survival at 2 Gy or the initial slopemay predict responsiveness to RIT. From this it would bepredicted that lymphomas should be the most responsive,followed by small cell lung cancer, adenocarcinomas andsquamous cell carcinomas, and melanomas, gliomas andsarcomas. It must be remembered that these are averagesensitivities for large numbers of tumors and any one tu-mor may be more or less radioresponsive than the averagefor its category. Individual testing of radiosensitivity maybe useful in patient selection, when more reliable tests aredeveloped.
III. COMPARISONS OF ALPHA AND BETAEMITTERS
The repair capacity increases as dose rate decreases butthere is a dose rate beyond which there is no further im-provement in survival, presumably because some compo-nent of the damage is irreparable.11,12 If high linear energytransfer (LET) radiation is used, where most radiationdamage is due to direct effects, there is much less capacityto repair and there is little if any dose rate effect. This givesan apparent advantage of alpha emitters over beta emittersin RIT of tumors if an even distribution of radionuclidecan be attained.13 Because of the short range of alpha-
particles, toxicity to normal tissues within and adjacent tothe tumor would be less than with beta-particles althoughthis is unlikely to be an important problem in either case.Toxicity to normal tissues receiving a dose of radiation,because of nonspecific uptake or as an “innocent by-stander” such as the bone marrow, would depend on theradiation sensitivity of the normal tissue relative to thetumor and to the dose absorbed by the normal tissue rel-ative to the tumor.
Consider the examples in Fig. 3. Figure 3 (a) representsa tumor that is more resistant than a normal tissue. Rep-resentative survival curves are shown. The absolute valuesof dose and survival are unimportant for this discussion. Ifa surviving fraction of 0.01 in the tumor is chosen, thesurviving fraction for normal tissue is taken from the graphassuming either that the normal tissue dose (Dn t) equalsthe tumor dose (Dt) or that Dnt is one fifth Dt. Figure 3 (b)and (c) show calculations for the circumstances where thenormal tissue (nt) is less sensitive than the tumor andwhere it is of equivalent radiosensitivity. It can be seenthat, for bone marrow or other tissues more sensitive thantumor, alpha-particles will actually have less effect on that
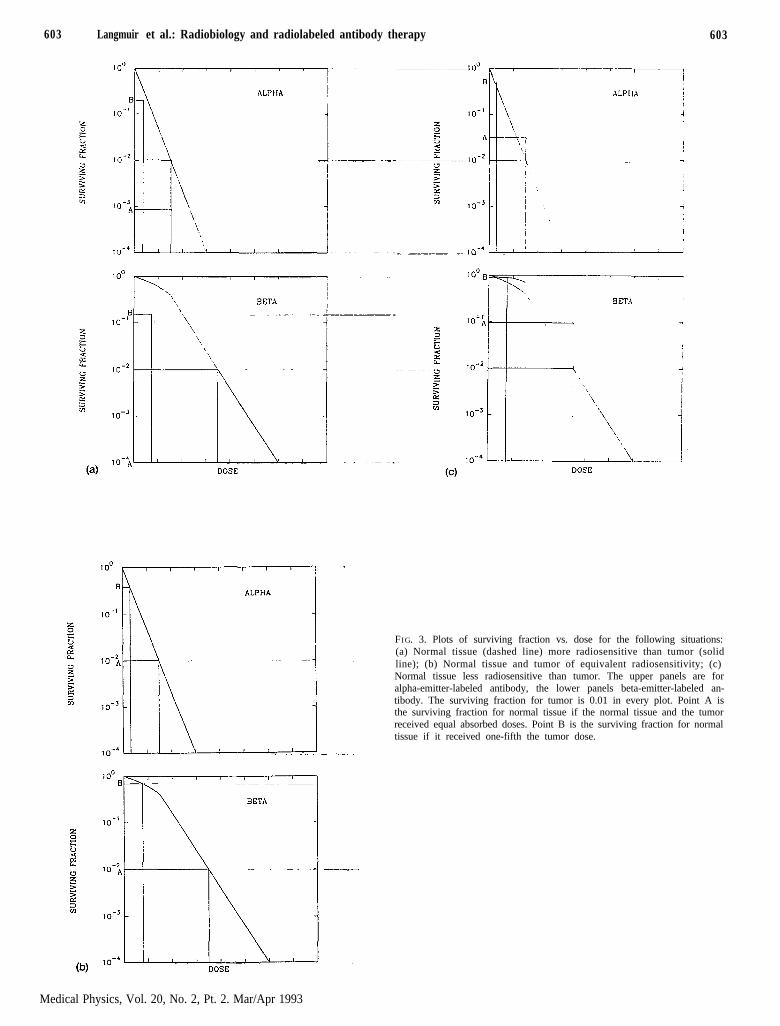
603 Langmuir et al.: Radiobiology and radiolabeled antibody therapy 603
FIG. 3. Plots of surviving fraction vs. dose for the following situations:(a) Normal tissue (dashed line) more radiosensitive than tumor (solid
line); (b) Normal tissue and tumor of equivalent radiosensitivity; (c)Normal tissue less radiosensitive than tumor. The upper panels are foralpha-emitter-labeled antibody, the lower panels beta-emitter-labeled an-tibody. The surviving fraction for tumor is 0.01 in every plot. Point A isthe surviving fraction for normal tissue if the normal tissue and the tumorreceived equal absorbed doses. Point B is the surviving fraction for normaltissue if it received one-fifth the tumor dose.
Medical Physics, Vol. 20, No. 2, Pt. 2. Mar/Apr 1993
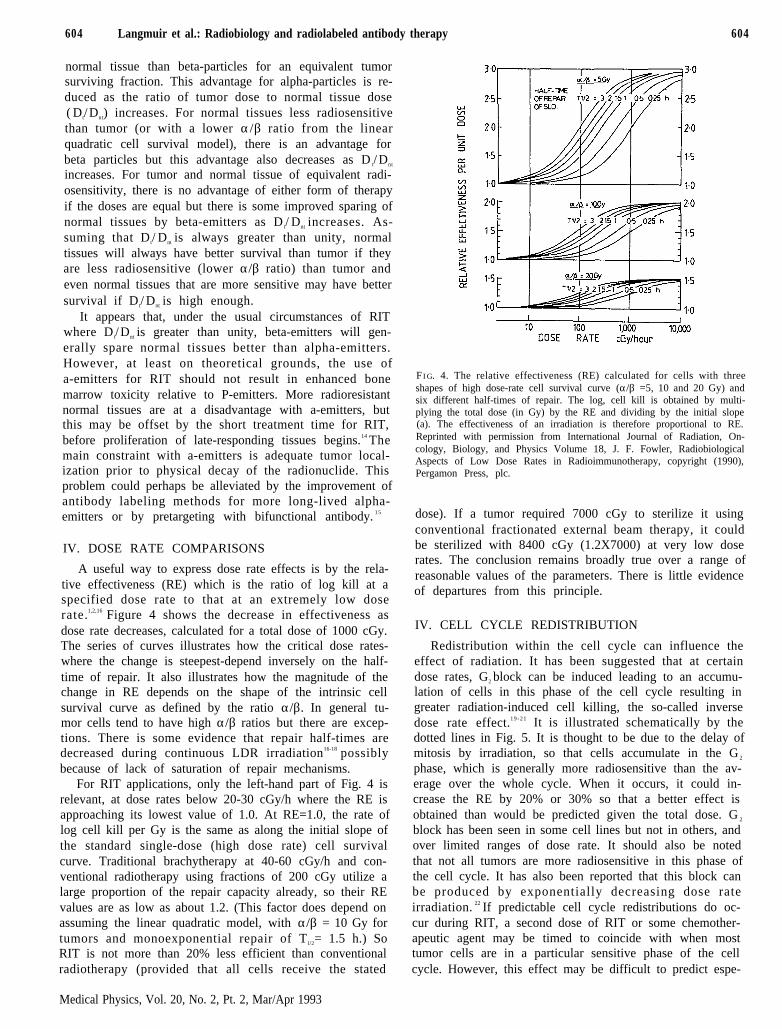
604 Langmuir et al.: Radiobiology and radiolabeled antibody therapy 604
normal tissue than beta-particles for an equivalent tumorsurviving fraction. This advantage for alpha-particles is re-duced as the ratio of tumor dose to normal tissue dose( Dt/ Dnt) increases. For normal tissues less radiosensitivethan tumor (or with a lower α/β ratio from the linearquadratic cell survival model), there is an advantage forbeta particles but this advantage also decreases as D t/ Dnt
increases. For tumor and normal tissue of equivalent radi-osensitivity, there is no advantage of either form of therapyif the doses are equal but there is some improved sparing ofnormal tissues by beta-emitters as D t/ Dnt increases. As-suming that D t/ Dnt is always greater than unity, normaltissues will always have better survival than tumor if theyare less radiosensitive (lower α/β ratio) than tumor andeven normal tissues that are more sensitive may have bettersurvival if D t/ Dnt is high enough.
It appears that, under the usual circumstances of RITwhere D t/ Dnt is greater than unity, beta-emitters will gen-erally spare normal tissues better than alpha-emitters.However, at least on theoretical grounds, the use ofa-emitters for RIT should not result in enhanced bonemarrow toxicity relative to P-emitters. More radioresistantnormal tissues are at a disadvantage with a-emitters, butthis may be offset by the short treatment time for RIT,before proliferation of late-responding tissues begins.14 Themain constraint with a-emitters is adequate tumor local-ization prior to physical decay of the radionuclide. Thisproblem could perhaps be alleviated by the improvement ofantibody labeling methods for more long-lived alpha-emitters or by pretargeting with bifunctional antibody. 1 5
IV. DOSE RATE COMPARISONS
A useful way to express dose rate effects is by the rela-tive effectiveness (RE) which is the ratio of log kill at aspecified dose rate to that at an extremely low doserate.1,2,16 Figure 4 shows the decrease in effectiveness asdose rate decreases, calculated for a total dose of 1000 cGy.The series of curves illustrates how the critical dose rates-where the change is steepest-depend inversely on the half-time of repair. It also illustrates how the magnitude of thechange in RE depends on the shape of the intrinsic cellsurvival curve as defined by the ratio α/β. In general tu-mor cells tend to have high α/β ratios but there are excep-tions. There is some evidence that repair half-times aredecreased during continuous LDR irradiation16-18 possiblybecause of lack of saturation of repair mechanisms.
For RIT applications, only the left-hand part of Fig. 4 isrelevant, at dose rates below 20-30 cGy/h where the RE isapproaching its lowest value of 1.0. At RE=1.0, the rate oflog cell kill per Gy is the same as along the initial slope ofthe standard single-dose (high dose rate) cell survivalcurve. Traditional brachytherapy at 40-60 cGy/h and con-ventional radiotherapy using fractions of 200 cGy utilize alarge proportion of the repair capacity already, so their REvalues are as low as about 1.2. (This factor does depend onassuming the linear quadratic model, with α/β = 10 Gy fortumors and monoexponential repair of T l/2= 1.5 h.) SoRIT is not more than 20% less efficient than conventionalradiotherapy (provided that all cells receive the stated
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
F I G. 4. The relative effectiveness (RE) calculated for cells with threeshapes of high dose-rate cell survival curve (α/β =5, 10 and 20 Gy) andsix different half-times of repair. The log, cell kill is obtained by multi-plying the total dose (in Gy) by the RE and dividing by the initial slope(a). The effectiveness of an irradiation is therefore proportional to RE.Reprinted with permission from International Journal of Radiation, On-cology, Biology, and Physics Volume 18, J. F. Fowler, RadiobiologicalAspects of Low Dose Rates in Radioimmunotherapy, copyright (1990),Pergamon Press, plc.
dose). If a tumor required 7000 cGy to sterilize it usingconventional fractionated external beam therapy, it couldbe sterilized with 8400 cGy (1.2X7000) at very low doserates. The conclusion remains broadly true over a range ofreasonable values of the parameters. There is little evidenceof departures from this principle.
IV. CELL CYCLE REDISTRIBUTION
Redistribution within the cell cycle can influence theeffect of radiation. It has been suggested that at certaindose rates, G2 block can be induced leading to an accumu-lation of cells in this phase of the cell cycle resulting ingreater radiation-induced cell killing, the so-called inversedose rate effect.1 9 - 2 1 It is illustrated schematically by thedotted lines in Fig. 5. It is thought to be due to the delay ofmitosis by irradiation, so that cells accumulate in the G 2
phase, which is generally more radiosensitive than the av-erage over the whole cycle. When it occurs, it could in-crease the RE by 20% or 30% so that a better effect isobtained than would be predicted given the total dose. G 2
block has been seen in some cell lines but not in others, andover limited ranges of dose rate. It should also be notedthat not all tumors are more radiosensitive in this phase ofthe cell cycle. It has also been reported that this block canbe produced by exponentially decreasing dose rateirradiation. 22 If predictable cell cycle redistributions do oc-cur during RIT, a second dose of RIT or some chemother-apeutic agent may be timed to coincide with when mosttumor cells are in a particular sensitive phase of the cellcycle. However, this effect may be difficult to predict espe-
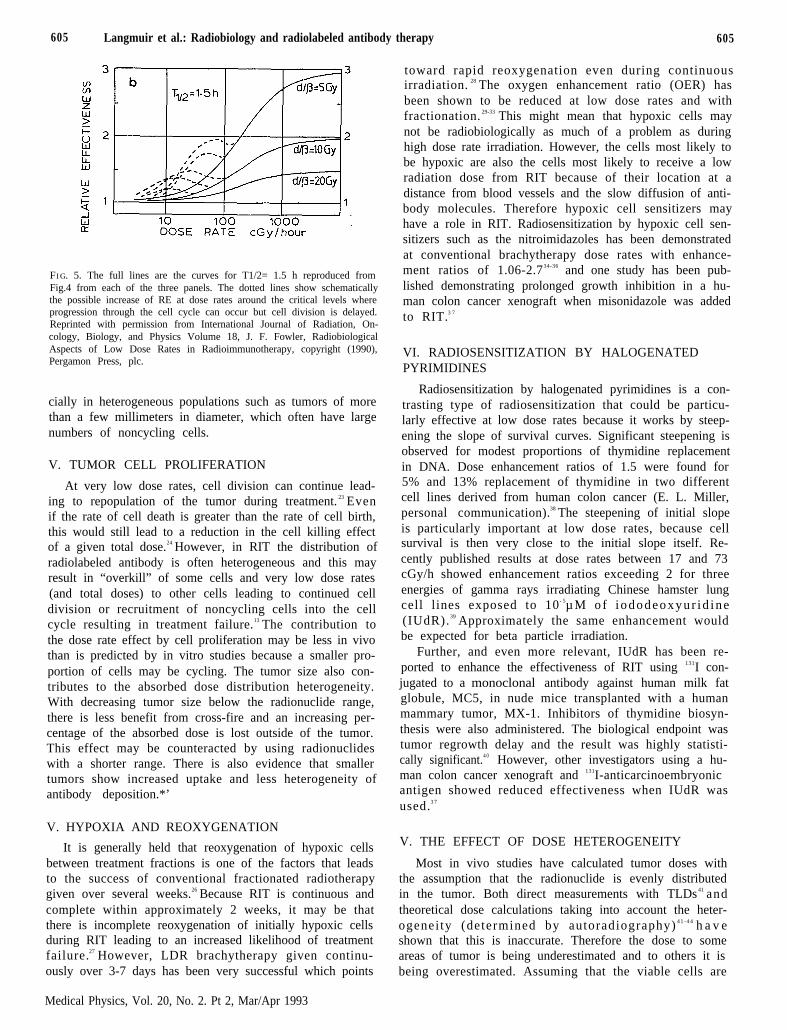
605 Langmuir et al.: Radiobiology and radiolabeled antibody therapy 605
FI G. 5. The full lines are the curves for T1/2= 1.5 h reproduced fromFig.4 from each of the three panels. The dotted lines show schematicallythe possible increase of RE at dose rates around the critical levels whereprogression through the cell cycle can occur but cell division is delayed.Reprinted with permission from International Journal of Radiation, On-cology, Biology, and Physics Volume 18, J. F. Fowler, RadiobiologicalAspects of Low Dose Rates in Radioimmunotherapy, copyright (1990),Pergamon Press, plc.
cially in heterogeneous populations such as tumors of morethan a few millimeters in diameter, which often have largenumbers of noncycling cells.
V. TUMOR CELL PROLIFERATION
At very low dose rates, cell division can continue lead-ing to repopulation of the tumor during treatment. 23 Evenif the rate of cell death is greater than the rate of cell birth,this would still lead to a reduction in the cell killing effectof a given total dose.24 However, in RIT the distribution ofradiolabeled antibody is often heterogeneous and this mayresult in “overkill” of some cells and very low dose rates(and total doses) to other cells leading to continued celldivision or recruitment of noncycling cells into the cellcycle resulting in treatment failure.13 The contribution tothe dose rate effect by cell proliferation may be less in vivothan is predicted by in vitro studies because a smaller pro-portion of cells may be cycling. The tumor size also con-tributes to the absorbed dose distribution heterogeneity.With decreasing tumor size below the radionuclide range,there is less benefit from cross-fire and an increasing per-centage of the absorbed dose is lost outside of the tumor.This effect may be counteracted by using radionuclideswith a shorter range. There is also evidence that smallertumors show increased uptake and less heterogeneity ofantibody deposition.*’
V. HYPOXIA AND REOXYGENATION
It is generally held that reoxygenation of hypoxic cellsbetween treatment fractions is one of the factors that leadsto the success of conventional fractionated radiotherapygiven over several weeks.26 Because RIT is continuous andcomplete within approximately 2 weeks, it may be thatthere is incomplete reoxygenation of initially hypoxic cellsduring RIT leading to an increased likelihood of treatmentfailure.27 However, LDR brachytherapy given continu-ously over 3-7 days has been very successful which points
toward rapid reoxygenation even during continuousirradiation. 28 The oxygen enhancement ratio (OER) hasbeen shown to be reduced at low dose rates and withfractionation. 29-33 This might mean that hypoxic cells maynot be radiobiologically as much of a problem as duringhigh dose rate irradiation. However, the cells most likely tobe hypoxic are also the cells most likely to receive a lowradiation dose from RIT because of their location at adistance from blood vessels and the slow diffusion of anti-body molecules. Therefore hypoxic cell sensitizers mayhave a role in RIT. Radiosensitization by hypoxic cell sen-sitizers such as the nitroimidazoles has been demonstratedat conventional brachytherapy dose rates with enhance-ment ratios of 1.06-2.734-36 and one study has been pub-lished demonstrating prolonged growth inhibition in a hu-man colon cancer xenograft when misonidazole was addedto RIT.3 7
VI. RADIOSENSITIZATION BY HALOGENATEDPYRIMIDINES
Radiosensitization by halogenated pyrimidines is a con-trasting type of radiosensitization that could be particu-larly effective at low dose rates because it works by steep-ening the slope of survival curves. Significant steepening isobserved for modest proportions of thymidine replacementin DNA. Dose enhancement ratios of 1.5 were found for5% and 13% replacement of thymidine in two differentcell lines derived from human colon cancer (E. L. Miller,personal communication).38 The steepening of initial slopeis particularly important at low dose rates, because cellsurvival is then very close to the initial slope itself. Re-cently published results at dose rates between 17 and 73cGy/h showed enhancement ratios exceeding 2 for threeenergies of gamma rays irradiating Chinese hamster lungcell lines exposed to 10- 5µM o f i ododeoxyu r id ine(IUdR).39 Approximately the same enhancement wouldbe expected for beta particle irradiation.
Further, and even more relevant, IUdR has been re-ported to enhance the effectiveness of RIT using 131I con-jugated to a monoclonal antibody against human milk fatglobule, MC5, in nude mice transplanted with a humanmammary tumor, MX-1. Inhibitors of thymidine biosyn-thesis were also administered. The biological endpoint wastumor regrowth delay and the result was highly statisti-cally significant.4 0 However, other investigators using a hu-man colon cancer xenograft and 131I-anticarcinoembryonicantigen showed reduced effectiveness when IUdR wasused.3 7
V. THE EFFECT OF DOSE HETEROGENEITY
Most in vivo studies have calculated tumor doses withthe assumption that the radionuclide is evenly distributedin the tumor. Both direct measurements with TLDs41 andtheoretical dose calculations taking into account the heter-ogenei ty (determined by autoradiography) 4 1 - 4 4 h a v eshown that this is inaccurate. Therefore the dose to someareas of tumor is being underestimated and to others it isbeing overestimated. Assuming that the viable cells are
Medical Physics, Vol. 20, No. 2. Pt 2, Mar/Apr 1993
606 Langmuir et al.: Radiobiology and radiolabeled antibody therapy 606
most likely to be targeted by RIT because of their proxim-ity to blood vessels, the dose to these cells is most likelybeing underestimated. However many viable cells may notbe targeted at all.
If half of the cells in a tumor (or metastatic cluster)receive no dose, they will survive and the radiobiologicaleffect is approximately the same as if only one single frac-tion of 200 cGy has been given. This is because each frac-tion of 200 cGy sterilizes about half the cells present. Thisis true no matter how great the dose delivered to those cellswhich do receive dose. If one quarter of the cells receive nodose, the effect is the same as two fractions of 200 cGy andso on. Any region of viable tumor cells that receives nodose will potentially contain enough cells (one or more) toregrow the tumor. The question of dose heterogeneity istherefore vitally important. Groups of cells which receiverather low doses are also dangerous if the cells remainclonogenic.
To overcome the problem of dose heterogeneity in RIT,additional effective treatment is necessary, possibly by us-ing external beam radiotherapy.2,45 If, for example, 90% ofthe cells in a tumor containing 1010 cells received an effec-tive dose from RIT but 10% of the cells received no dose,only one out of the ten logs of cells could have been elim-inated by RIT (assuming at least 8400 cGy to that 90%).We would then need to add 90% of a full dose of externalbeam radiotherapy in addition to RIT. If 99% of the tu-mor cells received a full dose, but 1% received no dose,then two logs could have been eliminated by RIT (assum-ing 8400 cGy to them), leaving eight logs to kill. We wouldthen need to add 80% of a full dose of external beamradiotherapy. 4 6 This picture emphasizes the real limita-tions of RIT. Dose heterogeneity is probably the largestunknown variable in both clinical and experimental tumorwork with RIT. But it also demonstrates that effective RITcan provide a useful boost dose. If it were possible to re-duce external beam doses by only 10% or 20%, many ofthe complications of radiotherapy could potentially be al-leviated.
It is necessary to emphasize that even one log of cell killis likely to lead to massive tumor shrinkage; possibly to onetenth of its original volume. Two logs of cell kill couldcause a tumor to disappear clinically (down to 1%), whichis complete remission clinically. But there would still beeight logs of cells remaining to be dealt with or else thetumor would inevitably recur.
It is also clear from the above discussion that the size oftumor is important. The larger the tumor, the more logs ofcell kill that are required to control it. Micrometastasesmay be well targeted by RIT using radionuclides of appro-priate energy. Wheldon et al.46 have made theoretical cal-culations of optimal tumor sizes for therapy with variousradionuclides and for 1 3 1I it is between 105 and 106 cells.This represents a nodule of less than l-mm diameter. Alower radiation dose would of course be required to steril-ize a micrometastasis than a tumor containing 10 10 cells.
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
VI. EXPERIMENTAL BEAM VERSUS RIT STUDIES
A final question is whether the response to exponen-tially decreasing LDR irradiation is the same as the re-sponse to constant LDR. Very few studies have addressedthis question. Differences in response may be due to theheterogeneous distribution of radionuclide in tumors withRIT or to the nature of exponentially decreasing low doserate radiation itself. There is some evidence that, in someanimal models, exponentially decreasing low dose rate ra-diation may be at least as effective as fractionatedthe rapy .4 , 4 7 - 5 1 This could be due to ( 1) the measured av-erage dose being lower than the dose that the viable tumorcells actually received, (2) a dose rate effect leading toaccumulation of cells in sensitive phases of the cell cycle,(3) a geometric effect dependent on the location of theradionuclide in the cell and the range of the radionuclide,or (4) interference with the blood supply to the tumor dueto irradiation of the endothelium leading to a tumor bedeffect.47 Several experiments have been performed usingdifferent experimental models to study the radiobiology ofRIT, and to compare the relative efficacy of RIT with doseequivalent external beam radiation. The results of thesestudies will be briefly summarized and compared here, andhave been discussed in more detail in a recent reviewpaper.5 2
Recently, five studies [Refs. 47-50 and J. A. Williams(personal communication)] have compared the efficacy ofRIT to high dose rate external beam irradiation. Althoughthese studies differed considerably in terms of the experi-mental model, design, and methodology employed, severalimportant comparisons can be made. Tables I and II sum-marize and compare these studies. The general features ofthe tumors and radioimmunoconjugates are shown in Ta-ble I and the modes or irradiation and fractionation sched-ules are shown in Table II. In all studies, RIT was com-pared to external beam irradiation, given either as a singlefraction (SF) or in multiple fractions (MF). In all but onestudy, RIT was compared to local irradiation of the tumor.Knox et al.48 utilized whole body external beam irradiationbecause of a relatively large contribution of whole bodyirradiation to the overall effect of RIT in the murine B-celllymphoma model studied. There were also important dif-ferences in the methods that were used to analyze the tu-mor response data and these have been summarized indetail in Table II.
In order to compare the results of the above studies, arelative efficacy factor was calculated for each study whichrepresented the relative efficacy of RIT compared to exter-nal beam irradiation. Relative efficacy factors were calcu-lated by using reported data for radiobiological endpointsor parameters measured as well as dosimetric data. Theactual equations used for the different studies as well as thecalculated relative efficacy factors are shown in Table II.As can be seen, the relative efficacy of RIT varied consid-erably from study to study. In a renal cell xenograft model,equivalent doses of RIT were 2.5 times more effective thanMF external beam irradiation for the inhibition of tumorgrowth, while less enhancement of efficacy was seen withSF irradiation (relative efficacy factor 1.5-1.7).47 S imi-
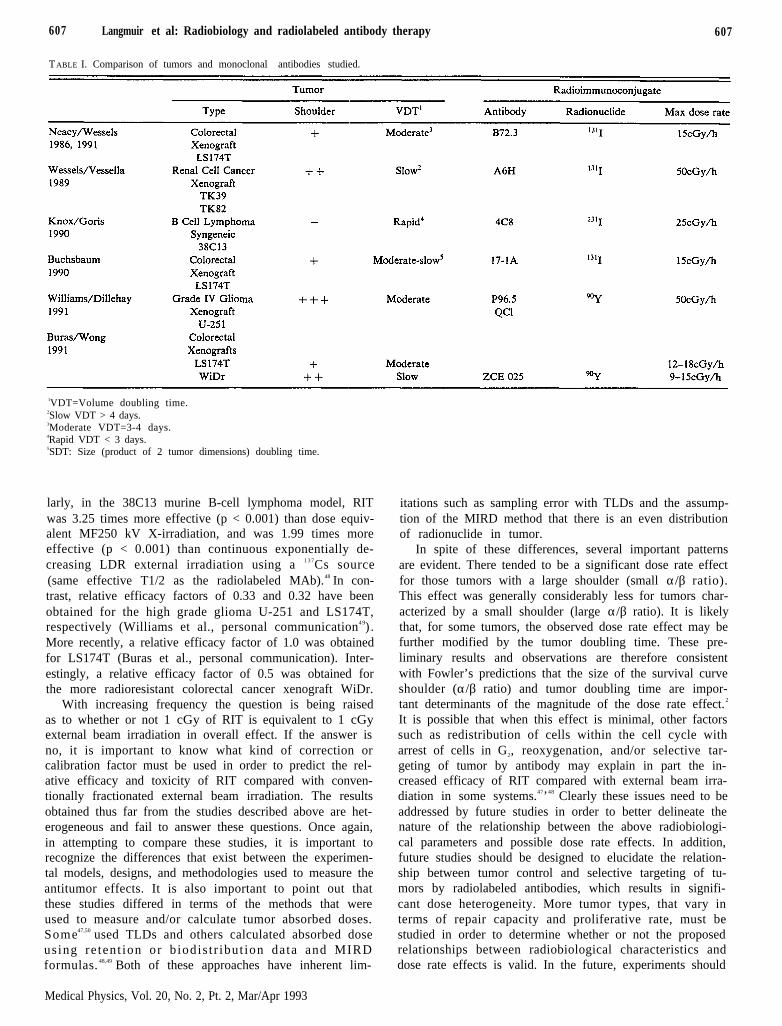
607 Langmuir et al: Radiobiology and radiolabeled antibody therapy 607
TABLE I. Comparison of tumors and monoclonal antibodies studied.
1VDT=Volume doubling time.2Slow VDT > 4 days.3Moderate VDT=3-4 days.4Rapid VDT < 3 days.5SDT: Size (product of 2 tumor dimensions) doubling time.
larly, in the 38C13 murine B-cell lymphoma model, RITwas 3.25 times more effective (p < 0.001) than dose equiv-alent MF250 kV X-irradiation, and was 1.99 times moreeffective (p < 0.001) than continuous exponentially de-creasing LDR external irradiation using a 1 3 7Cs source(same effective T1/2 as the radiolabeled MAb).48 In con-trast, relative efficacy factors of 0.33 and 0.32 have beenobtained for the high grade glioma U-251 and LS174T,respectively (Williams et al., personal communication4 9) .More recently, a relative efficacy factor of 1.0 was obtainedfor LS174T (Buras et al., personal communication). Inter-estingly, a relative efficacy factor of 0.5 was obtained forthe more radioresistant colorectal cancer xenograft WiDr.
With increasing frequency the question is being raisedas to whether or not 1 cGy of RIT is equivalent to 1 cGyexternal beam irradiation in overall effect. If the answer isno, it is important to know what kind of correction orcalibration factor must be used in order to predict the rel-ative efficacy and toxicity of RIT compared with conven-tionally fractionated external beam irradiation. The resultsobtained thus far from the studies described above are het-erogeneous and fail to answer these questions. Once again,in attempting to compare these studies, it is important torecognize the differences that exist between the experimen-tal models, designs, and methodologies used to measure theantitumor effects. It is also important to point out thatthese studies differed in terms of the methods that wereused to measure and/or calculate tumor absorbed doses.Some47,50 used TLDs and others calculated absorbed doseusing re tent ion or b iodis t r ibut ion data and MIRDformulas. 48,49 Both of these approaches have inherent lim-
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
itations such as sampling error with TLDs and the assump-tion of the MIRD method that there is an even distributionof radionuclide in tumor.
In spite of these differences, several important patternsare evident. There tended to be a significant dose rate effectfor those tumors with a large shoulder (small α/β ratio).This effect was generally considerably less for tumors char-acterized by a small shoulder (large α/β ratio). It is likelythat, for some tumors, the observed dose rate effect may befurther modified by the tumor doubling time. These pre-liminary results and observations are therefore consistentwith Fowler’s predictions that the size of the survival curveshoulder (α/β ratio) and tumor doubling time are impor-tant determinants of the magnitude of the dose rate effect.2
It is possible that when this effect is minimal, other factorssuch as redistribution of cells within the cell cycle witharrest of cells in G2, reoxygenation, and/or selective tar-geting of tumor by antibody may explain in part the in-creased efficacy of RIT compared with external beam irra-diation in some systems.47’48 Clearly these issues need to beaddressed by future studies in order to better delineate thenature of the relationship between the above radiobiologi-cal parameters and possible dose rate effects. In addition,future studies should be designed to elucidate the relation-ship between tumor control and selective targeting of tu-mors by radiolabeled antibodies, which results in signifi-cant dose heterogeneity. More tumor types, that vary interms of repair capacity and proliferative rate, must bestudied in order to determine whether or not the proposedrelationships between radiobiological characteristics anddose rate effects is valid. In the future, experiments should
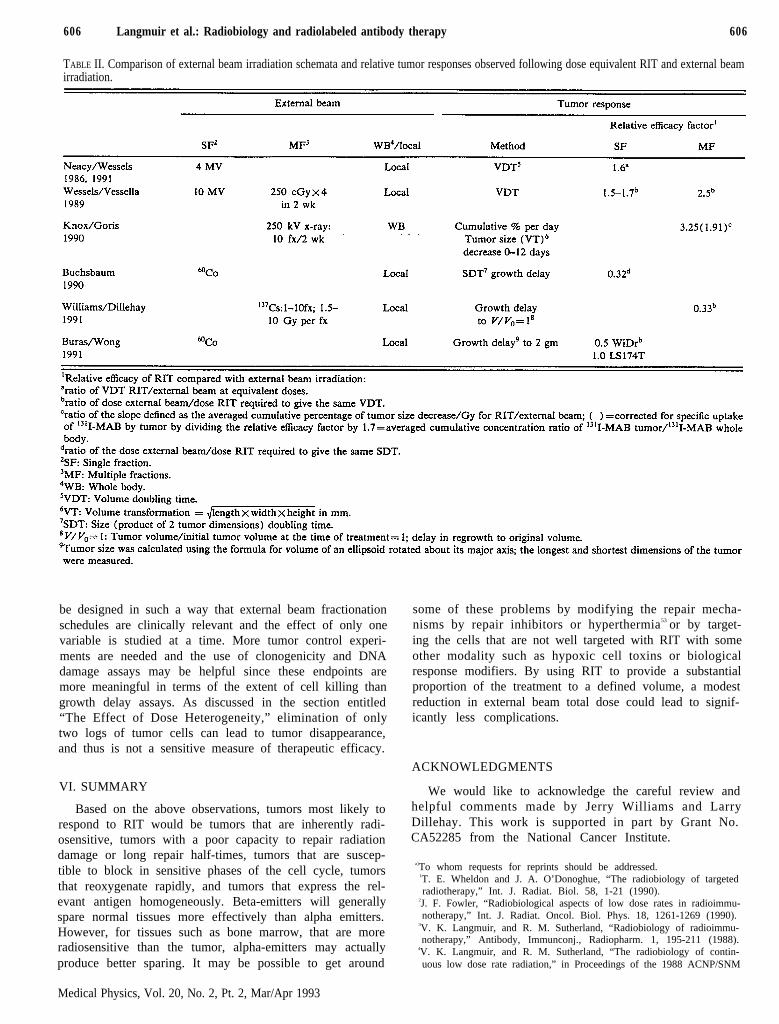
606 Langmuir et al.: Radiobiology and radiolabeled antibody therapy 606
TABLE II. Comparison of external beam irradiation schemata and relative tumor responses observed following dose equivalent RIT and external beamirradiation.
be designed in such a way that external beam fractionationschedules are clinically relevant and the effect of only onevariable is studied at a time. More tumor control experi-ments are needed and the use of clonogenicity and DNAdamage assays may be helpful since these endpoints aremore meaningful in terms of the extent of cell killing thangrowth delay assays. As discussed in the section entitled“The Effect of Dose Heterogeneity,” elimination of onlytwo logs of tumor cells can lead to tumor disappearance,and thus is not a sensitive measure of therapeutic efficacy.
VI. SUMMARY
Based on the above observations, tumors most likely torespond to RIT would be tumors that are inherently radi-osensitive, tumors with a poor capacity to repair radiationdamage or long repair half-times, tumors that are suscep-tible to block in sensitive phases of the cell cycle, tumorsthat reoxygenate rapidly, and tumors that express the rel-evant antigen homogeneously. Beta-emitters will generallyspare normal tissues more effectively than alpha emitters.However, for tissues such as bone marrow, that are moreradiosensitive than the tumor, alpha-emitters may actuallyproduce better sparing. It may be possible to get around
some of these problems by modifying the repair mecha-nisms by repair inhibitors or hyperthermia53 or by target-ing the cells that are not well targeted with RIT with someother modality such as hypoxic cell toxins or biologicalresponse modifiers. By using RIT to provide a substantialproportion of the treatment to a defined volume, a modestreduction in external beam total dose could lead to signif-icantly less complications.
ACKNOWLEDGMENTS
We would like to acknowledge the careful review andhelpful comments made by Jerry Williams and LarryDillehay. This work is supported in part by Grant No.CA52285 from the National Cancer Institute.
a)To whom requests for reprints should be addressed.1T. E. Wheldon and J. A. O’Donoghue, “The radiobiology of targetedradiotherapy,” Int. J. Radiat. Biol. 58, 1-21 (1990).
2J. F. Fowler, “Radiobiological aspects of low dose rates in radioimmu-notherapy,” Int. J. Radiat. Oncol. Biol. Phys. 18, 1261-1269 (1990).
3V. K. Langmuir, and R. M. Sutherland, “Radiobiology of radioimmu-notherapy,” Antibody, Immunconj., Radiopharm. 1, 195-211 (1988).
4V. K. Langmuir, and R. M. Sutherland, “The radiobiology of contin-uous low dose rate radiation,” in Proceedings of the 1988 ACNP/SNM
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993

609 Langmuir et al.: Radiobiology and radiolabeled antibody therapy 609
Joint Symposium on the Biology of Radionuclide Therapy (AmericanCollege of Nuclear Physicians, Washington, DC, 1989), pp. 270-284.
5S. J. Adelstein and A. I. Kassis, “Radiobiologic implications of themicroscopic distribution of energy from radionuclides,” Int. J. Radiat.Applic. Instrum. Part B: Nucl. Med. Biol. 14, 165-169 (1987).
6J. B. Mitcheli, J. S. Bedford, and S. M. Bailey, “Dose-rate effects inmammalian cells in culture III. Comparison of cell killing and cellproliferation during continuous irradiation for six different cell lines,”Radiat. Res. 79, 537-551 (1979).
7G. G. Steel, J. M. Deacon, G. M. Duchesne, A. Horwich, L. R.Kelland, and J. H. Peacock, “The dose-rate effect in human tumourcells,” Radiother. Oncol. 9, 299-310 (1987).
8J. Y. C. Wang, L. E. Williams, A. J. Demidecki, B. W. Wessels, and X.W. Yan, “Radiobiologic studies comparing yttrium-90 irradiation andexternal beam irradiation in vitro,” Int. J. Radiat. Oncol. Biol. Phys.20. 715-722 (1991).
9J. Deacon, M. J. Peckham, and G. G. Steel, “The radioresponsivenessof human tumours and the initial slope of the cell survival curve,”Radiother. Oncol. 2, 317-323 (1984).
10B. Fertil and E. P. Malaise, “Intrinsic radiosensitivity of human celllines is correlated with radioresponsiveness of human tumors: analysisof 101 published survival curves,” Int. J. Radiat. Oncol. Biol. Phys. 11,1699-1707 (1985).
11R. L. Wells and J. S. Bedford, “Dose-rate effects in mammalian cells,”Radiat. Res. 94, 105-134 (1983).
12J. B. Mitchell, J. S. Bedford, and S. M. Bailey, “Dose-rate effects inplateau-phase cultures of S3 HeLa and V79 cells,” Radiat. Res. 79,552-567 (1979).
13J. L Humm, “Dosimetric aspects of radiolabeled antibodies for tumortherapy,” J. Nucl. Med. 27, 1490-1497 (1986).
14H. D. Thames and J. H. Hendry, Fractionation in Radiotherapy (Tay-lor and Francis, London, 1987).
15D. A. Goodwin, C. F. Meares, M. J. McCall, M. McTigue, and W.Chaovapong, “Pre-targeted immunoscintigraphy of murine tumorswith indium-111-labeled bifunctional haptens,” J. Nucl. Med. 29, 226-234 (1988).
16R. G. Dale, “The application of the linear-quadratic dose-effect equa-tion to fractionated and protracted radiotherapy,” Br. J. Radiol. 58,515-528 (1985).
17G. G Steel, “Recovery kinetics deduced from continuous low-dose rateexperiments,” Radiother. Oncol. 14, 337-343 (1989).
18T. C Stephens, J. J. Eady, J. H. Peacock, and G. G. Steel, “Split-doseand low dose-rate recovery in four experimental tumour systems,” Int.J. Radiat. Biol. 52, 157-170 (1987).
19J. B. Mitchell, J. S. Bedford, and S. M. Bailey, “Dose-rate effects on thecell cycle and survival of S3 HeLa and V79 cells,” Radiat. Res. 79,520-536 (1979).
20H. B. Kal, G. W. Barendsen, R. Bakker-van Hauwe, and H. Raise,“Increased radiosensitivity of rat rhabdomyosarcoma cells induced byprotracted irradiation,” Radiat. Res. 63, 521-530 (1975).
21I. E. van Oostrum, S. Erkens-Schulze, M. Petterson, I. S. Wils, and D.H. Rutgers, “The relationship between radiosensitivity and cell kineticeffects after low- and high-dose-rate irradiation in five human tumors innude mice,” Radiat. Res. 122, 252-261 (1990).
22L. E. Dillehay and J. R. Williams, “Radiobiological characteristics ofradiolabeled immunoglobulin therapy,” in Proceedings of the 1988ACNP/SNM Joint Symposium on the Biology of Radionuclide Therapy(American College of Nuclear Physicians, Washington, DC, 1989), pp.262-269.
23W. U. Shipley, J. H. Peacock, G. G. Steel, and T. C. Stephens, “Con-tinuous irradiation of the Lewis lung carcinoma in vivo at clinically-used ‘ultra’ low-dose rates,” Int. J. Radiat. Oncol. Biol. Phys. 9, 1647-1653 (1983).
24A. Szechter, G. Schwarz, and J. M. Barsa, “Continuous and fraction-ated irradiation of mammalian cells in culture-I. The effect of growthrate,” Int. J. Radiat. Oncol. Biol. Phys. 4, 991-1000 (1978).
25L. E. Williams, R. B. Duda, R. T. Proffitt, B. G. Beatty, J. D. Beatty,J. Y. C. Wong, J. E. Shively, and R. Paxton, "Tumor uptake as a modelof tumor mass: A mathematical model," J. Nucl. Med. 29, 103-109(1988).
26R. F. Kallman, “The phenomenon of reoxygenation and its implica-tions for fractionated radiotherapy,” Radiology 105, 135-142 (1972).
27T. Nylen, H. Acker, B. Bolling, G. Holterman, and J. Carlsson, “In-fluence of ionizing radiation on oxygen profiles in different types ofmulticellular spheroids,” Radiat. Res. 120, 213-226 (1989).
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993
28H. B. Kal and G. W. Barendsen, “Effects of continuous irradiation atlow dose-rates on a rat rhabdomyosarcoma,” Br. J. Radiol. 45, 279-283(1972).
29C. C. Ling, I. J. Spiro, J. Mitchell, and R. Stickler, “The variation ofOER with dose rate,” Int. J. Radiat. Oncol. Biol. Phys. 11, 1367-1373(1985).
30Y. C. Taylor and I. M. Brown, “Radiosensitization in multifractionschedules, I. Evidence for an extremely low oxygen enhancement ra-tio,” Radiat. Res. 112, 124-133 (1987).
31B. Palcic, M. Korbelik, M. Trotter, and L. Revesz. “Oxygen enhance-ment ratio of fractionated regimens in vitro,” Radiat. Res. 117, 409-418(1989).
32J. Hall, J. S. Bedford, and R. Oliver, “Extreme hypoxia; its effect onthe survival of mammalian cells irradiated at high and low dose-rates,”Br. J. Radiol. 39, 302-307 (1966).
33I. J Spiro, C. C. Ling, R. Stickler, and J. Gaskill, “Oxygen radiosen-sitization at low dose rate,” Br. J. Radiol. Res. 58, 357-363 (1985).
34C. C. Ling, R. Stickler, M. C. Schell, and I. J. Spiro, “The effect ofhypoxic cell sensitizers at different irradiation dose rates,” Radiat. Res.109, 396-406 (1987).
35K. K. Fu, S. Hurst, A. C. Begg, and J. M. Brown, “The effects ofmisonidazole during continuous low dose rate irradiation,” in Radia-tion Sensitizers. Their Use in The Clinical Management of Cancer, ed-ited by L. W. Brady (Masson, New York, 1980), pp. 267-275.
36M Bernstein P. H. Gutin, and D. F. Deen, “Radiosensitization of theRiF-1 murin; flank tumor by desmethylmisonidazole (Ro 05 9963)during interstitial brachytherapy,” Int. J. Radiat. Oncol. Biol. Phys. 8,487-490 (1982).
3 7R. B. Pedley, R. H. J. Begent, J. A. Boden, T. Adam, and K. D.Bagshawe, “The effect of radiosensitizers on radioimmunotherapy, us-ing 131I-labelled anti-CEA antibodies in a human colonic xenograftmodel,” Int. J. Cancer 47, 597-602 (1991).
38R. Rodriguez, E. L. Miller, J. F. Fowler, and T. J. Kinsella, “Contin-uous infusion of halogenated pyrimidines,” (letter) Int. J. Radiat. On-col. Biol. Phys. 30, 1380-1382 (1991).
39R. Nath, P. Bongiorni, and S. Rockwell, “Iododeoxyuridine radiosen-sitization by low- and high-energy photons for brachytherapy doserates,” Radiat. Res. 124, 249-258 (1990).
4 0O. Santos, K. D. Pant , E. W. Blank, and R. L. Ceriani , “5-Iododeoxyuridine increases the efficacy of the radioimmunotherapy ofhuman tumors growing in nude mice,” J. Nucl. Med. 33, 1530-1534(1992).
41M. H. Griffith, E. D. Yorke, B. W. Wessels, G. L. DeNardo, and W. P.Neacy, “Direct dose confirmation of quantitative autoradiography withmicro-TLD measurements for radioimmunotherapy,” J. Nucl. Med.29, 1795-1809 (1988).
42C. S. Kwok, W. V. Prestwich, and B. C. Wilson, “Calculation of radi-ation doses for nonuniformly distributed β and γ radionuclides in softtissue,” Med. Phys. 12, 405-412 (1985).
43V K. Langmuir and R. M. Sutherland, “Dosimetry models for radio-immunotherapy,” Med. Phys. 15, 867-873 ( 1988).
44J. L. Humm and L. M. Cobb, “Nonuniformity of tumor dose in radio-immunotherapy.” J. Nucl. Med. 31, 75-83 (1990).
45B. Wessels and R. Rogus, “Radionuclide selection and model absorbeddose calculations for radiolabeled tumor associated antibodies,” Med.Phys. 11, 638-645 (1984).
46T. E. Wheldon, J. A. O’Donoghue, T. E. Hilditch, and A. Barrett,“Strategies for systemic radiotherapy of micrometastases using anti-body targeted 131I,” Radiother. Oncol. 11, 133-142 (1988).
47B. W. Wessels, R. L. Vessella, D. F. Palme, J. M. Berkopec, G. K.Smith, and E. W. Bradley, “Radiobiological comparison of externalbeam irradiation and radioimmunotherapy in renal-cell carcinoma xe-nografts,” Int. J. Radiat. Oncol. Biol. Phys. 17, 1257-1263 (1989).
48S. J. Knox, R. Levy, R. A. Miller, W. Uhland, J. Schiele, W. Ruehl, R.R. Finston, P. Day-Lollini, and M. L. Goris, “Determinants of theantitumor effect of radiolabeled monoclonal antibodies,” Cancer Res.so, 4935-4940 (1990).
49D. J. Buchsbaum, R. K. Ten Haken, D. B. Heidorn, T. S. Lawrence, A.A. Glatfelter, V. H. Terry, D. M. Guilbault, Z. Steplewski, and A. S.Lichter, “A comparison of 131I-labeled monoclonal antibody 17-1Atreatment to external beam irradiation on the growth of Ls174T hu-man colon carcinoma xenografts,” Int. J. Radiat. Oncol. Biol. Phys. 18,1033-1041 (1990).
50W. P. Neacy, B. W. Weasels, E. W. Bradley, S. Kovandi, T. Justice, S.Danskin. and H. Sands, “Comparison of radioimmunotherapy (RIT)

610 Langmuir et al.: Radiobiology and radiolabeled antibody therapy 610
and 4 MV external beam radiotherapy of human tumor xenografts inathymic mice (Abst.),” J. Nucl. Med. 27, 902-903 (1986).
51B. W. Wessels, “Current status of animal radioimmunotherapy,” Can-cer Res. (suppl) 50, 970s-973s (1990).
52S. J. Knox, M. L. Goris, and B. W. Wessels, “Overview of comparative
studies of radioimmunotherapy vs. external beam radiation” Radioth.Oncol. 23, Ill-117 (1992).
53C. C. Ling and E. Robinson, “Moderate hyperthermia and low doserate irradiation,” Radiat. Res. 114, 379-384 (1988).
Medical Physics, Vol. 20, No. 2, Pt. 2, Mar/Apr 1993