Andrew Kong, MD
The Deep Sulcus Sign1
APPEARANCE
The deep sulcus sign (1) is seen on chest radiographs
obtainedwith the patient in the supine position. It represents
lucency ofthe lateral costophrenic angle extending toward the
hypo-chondrium. The abnormally deepened lateral costophrenic an-gle
may have a sharp, angular appearance (Figure).
EXPLANATION
When the patient is in the supine position, air in the
pleuralspace (pneumothorax) collects anteriorly and basally
withinthe nondependent portions of the pleural space; when
thepatient is upright, the air collects in the apicolateral
location.If air collects laterally rather than medially, it
abnormallydeepens the lateral costophrenic angle and produces the
deepsulcus sign.
DISCUSSION
Air enters the pleural space by crossing any of its
boundaries,such as the chest wall, mediastinum, lung, or diaphragm
(2).Recognition of a pneumothorax depends on the volume of airin
the pleural space and the position of the body. The deepsulcus sign
is a useful clue in the diagnosis of pneumothorax inneonates or in
critically ill patients such as those who haveundergone major
trauma or are in intensive care units (2,3).These patients are
least capable of communicating that theyare experiencing dyspnea
and pleuritic chest pain, which arethe typical symptoms of
pneumothorax.
The visceral pleural line, which is visible as a thin
curvilinearopacity along the lung and is separated from the chest
wall byair in the apical pleural space in the upright patient, is
com-
monly not identifiable on radiographs of supine patients un-less
there is a sizable pneumothorax. Approximately 30% ofpneumothoraces
are undetected on supine radiographs (3).The deep sulcus sign of
pneumothorax may be present follow-ing severe chest injury (4). It
is important that the lateralcostophrenic angles are included on
the radiograph, as failureto diagnose pneumothorax may be
life-threatening because ofthe risk of tension. This is also
important in the intensive caresetting for procedures such as
insertion of a subclavian centralvenous catheter and for the use of
positive pressure ventila-tion.
In addition to the deep sulcus sign, other clues may suggestthe
presence of a pneumothorax on supine radiographs (2,5,6):(a)
relative lucency in the hypochondrial region or the entire
Index terms:Pneumothorax, 66.73Signs in Imaging
Published online10.1148/radiol.2282020524
Radiology 2003; 228:415416
1 From the Department of Radiology, The Queen Elizabeth
Hospital,Woodville Rd, Woodville, South Australia 5011, Australia.
ReceivedMay 7, 2002; revision requested July 10; revision received
July 30;accepted August 15. Address correspondence to the author
(e-mail:[email protected]). RSNA, 2003
A trainee (resident or fellow) wishing to submit a manuscriptfor
Signs in Imaging should first write to the Editor for approvalof
the sign to be prepared, to avoid duplicate preparation of thesame
sign.
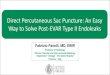
Supine chest radiograph of a neonate illustrates the deep sulcus
signwith abnormal deepening and lucency of the left lateral
costophrenicangle (). Findings on right lateral decubitus chest
radiograph (notshown) confirmed the presence of a pneumothorax on
the left side.
Signs in Imaging
415
Ra
dio
logy
hemithorax; (b) depression of an ipsilateral hemidiaphragm;(c)
double-diaphragm appearance due to air outlining of theanterior
costophrenic angle and aerated lung outlining thediaphragmatic
dome; (d) improved sharpness of the cardio-mediastinal border due
to anteromedial collection of air, whichmay appear as a lucency;
(e) increased sharpness of the peri-cardial fat pads; (f) visible
inferior edge of a collapsed lowerlobe or of the undersurface of
the heart due to air in the pleuralspace; (g) band of air in the
minor fissure bounded by twovisceral pleural lines; or (h) visible
lateral edge of the rightmiddle lobe due to medial retraction in
the presence of ante-rior pneumothorax.
Further evaluation with lateral decubitus radiography maybe
helpful, but computed tomography is more sensitive forconfirming
the presence of a pneumothorax in supine patients
(6). False-positive cases of the deep sulcus sign have
beendescribed in patients with chronic obstructive pulmonary
dis-ease, in which hyperaeration of the lungs deepens the
lateralcostophrenic angle (1).
References1. Gordon R. The deep sulcus sign. Radiology 1980;
136:2527.2. Grainger RG, Allison DJ, Adam A, Dixon AK. Diagnostic
radiology.
New York, NY: Churchill Livingstone, 2001; 254257.3. Brant WE,
Helms CA. Fundamentals of diagnostic radiology. Balti-
more, Md: Williams & Wilkins, 1994; 503506.4. Camassa N,
Boccuzzi F, Troilo A, DEttorre E. Pneumothorax in
severe chest injuries. Radiol Med (Torino) 1988; 75: 156159.
[Ital-ian]
5. Armstrong P, Wilson AG, Dee P, Hansell DM. Imaging of
diseases ofthe chest. St Louis, Mo: Mosby, 2000; 770771.
6. Tocino I, Armstrong J. Trauma to the lung. In: Taveras J,
ed.Radiology. Philadelphia, Pa: Lippincott-Raven, 1996; 18.
416 Radiology August 2003 Kong
Ra
dio
logy